
Submitted:
20 December 2024
Posted:
23 December 2024
You are already at the latest version
Abstract
Introduction: Population aging poses an unprecedented global challenge, giving rise to significant social, economic, and health-related complexities. The continuous growth in the older adult pop-ulation, coupled with the feminization of aging and the gender gap in healthcare access, under-scores the imperative to reformulate existing strategies for addressing aging. Current approaches often fall short in adequately addressing the unique characteristics of female aging. Methodology: A structured literature review was conducted as a data collection strategy. The search was conducted in May 2024, utilizing the Scopus, Web of Science, and PubMed databases. Ultimately, 157 articles were included in the review. Results: Information and Communication Technologies (ICTs) have emerged as a promising avenue for enhancing the quality of life of older adults. By providing as-sistance with daily tasks, stimulating cognitive function, facilitating social interaction, and miti-gating the detrimental effects of isolation and loneliness, ICTs empower older adults to maintain their independence. However, a persisting gender gap, which ICTs have not fully addressed, re-mains a significant challenge. Conclusions: To ensure the efficacy of strategies aimed at promoting healthy aging, it is imperative to democratize access to ICTs and bridge the existing gender gap. Consequently, novel technological solutions must be developed, adopting a person-centered ap-proach. This will facilitate the creation of a society where all older adults can enjoy fulfilling, healthy, and active lives, while simultaneously eliminating the inequalities faced by older women.
Primary objective: To assess the importance, need, and implementation of ICTs for improving older adults' health.
Secondary objectives: 1. To evaluate the applicability of a gender perspective. 2. To assess the potential of ICTs to improve quality of life and general well-being.
Keywords:
active ageing
; digital
; feminisation of ageing
; ICTs
; loneliness
; older adults
; technology
; women's health
1. Introduction
Population ageing is a global phenomenon resulting from technological advances and biomedical research [1,2], which poses a crucial challenge for today's societies [3,4]. In turn, increased life expectancy has led to an increase in the prevalence of chronic non-communicable diseases and in the number of older adults suffering from unwanted loneliness [5]. Thus, one of the current challenges is to ensure that the increase in life expectancy is accompanied by effective management of chronic conditions, both in terms of prevention and early diagnosis and treatment [6]. In addition, it is essential to address the social circumstances associated with ageing, with the aim of improving the quality of life of older adults [7] and reducing or mitigating the growing sense of unwanted loneliness that affects a significant part of this population [8].
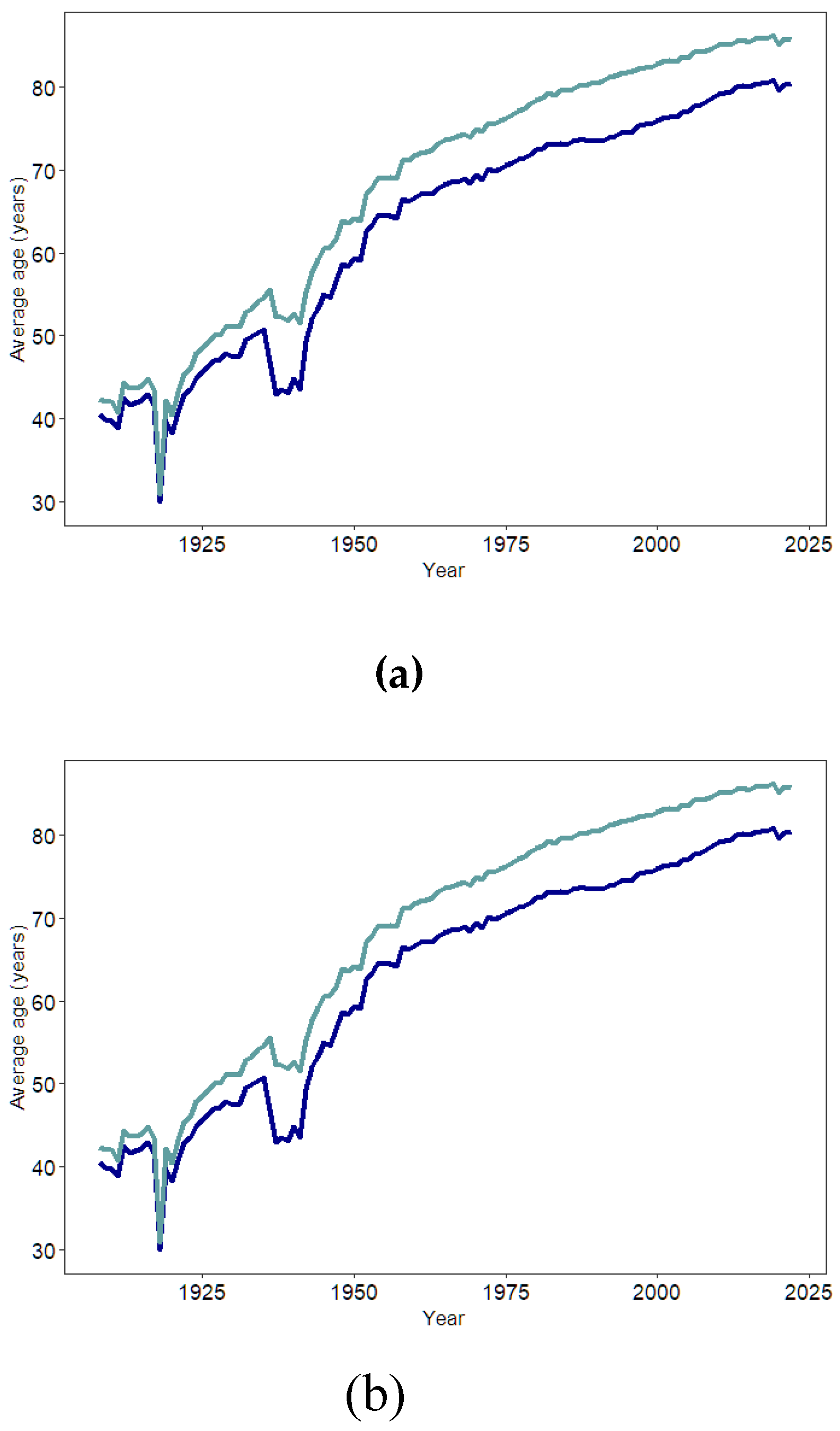
Ageing is a biological, psychological and social phenomenon [9], characterised by the deterioration and reduction of the physiological, biochemical and physical functions of the organism as a consequence of increasing chronological age [10]. The National Statistics Institute (NSI) defines life expectancy as “the average number of years that a person of a given age would expect to continue to live, if the age-specific mortality pattern observed at the time of estimation were to be maintained”. This concept is paralleled by population ageing or “an increase in the population aged 60 and over, while the population of young people aged 15 and under is declining” [11]; an indicator that reflects the health, social and economic conditions of a country [12]. Globally, there is a rapid increase in the proportion of older people, with 1 in 6 of the world's population expected to be over 60 years of age by 2030. This growth will continue over time, causing the number of people aged 80 and over to triple between 2020 and 2050, reaching 426 million [13]. Specifically, in Spain, the rapid increase in the life expectancy of Spanish adults (Figure 1 a) is also supported by predictions for the coming years (Figure 1 b) [14]. During the year 2024, the number of older adults in Spain reached 20.15%, with a projected increase of 30.5% in the coming years, which will support the inversion of the population pyramid [15]. This will lead to an overcapacity of care services for older adults, if they suffer from chronic non-communicable diseases that could have been prevented [16]. It is therefore essential to achieve the development of chronologically, but not biologically, ageing populations by maintaining healthy and active states [2].
Improvements in health systems, public health initiatives and increased health awareness have not been able to eliminate the gender gap in life expectancy [17]. However, although women live longer than men, their inclusion in the world of work [18], and the incorporation of unhealthy habits (previously ingrained only in men), have led to a stagnation in women's life expectancy, and with it, a narrowing of the gender gap (Figure 1 c) [12]. However, it has been determined that this gender gap will not disappear completely due to chromosomal composition [10], the effects of which become more pronounced as we age [17]. As a result of the loss of Y chromosome information in the male sex, males have a higher mortality risk [10] and thus a shorter life expectancy [15].
Figure 1.
(a) Evolution of life expectancy in Spain from 1908 to 2022 by biological sex (NSI). Despite the significant increase in the average age of both sexes, and the narrowing of the gender gap in recent decades, women's life expectancy continues to be higher. (b) Projection of life expectancy in Spain up to 2070 (NSI). In addition, estimates of the evolution of life expectancy at birth show that it will continue to be higher for women. (c) Evolution of the gender gap in Spain (INE). Over the years, the gender gap in life expectancy between men and women has narrowed, with a limited stagnation observed in recent years (NSI).
Figure 1.
(a) Evolution of life expectancy in Spain from 1908 to 2022 by biological sex (NSI). Despite the significant increase in the average age of both sexes, and the narrowing of the gender gap in recent decades, women's life expectancy continues to be higher. (b) Projection of life expectancy in Spain up to 2070 (NSI). In addition, estimates of the evolution of life expectancy at birth show that it will continue to be higher for women. (c) Evolution of the gender gap in Spain (INE). Over the years, the gender gap in life expectancy between men and women has narrowed, with a limited stagnation observed in recent years (NSI).
In Spain, life expectancy at age 65 is among the highest in Europe (Figure 2 a) and the world, with figures of 19.2 years for men and 23.2 years for women [19], revealing notable variations both geographically (Figure 2 b) and by gender. Population ageing is particularly pronounced in the north-west of the country, specifically in the autonomous communities of Asturias, Castilla y León and Galicia, where the proportion of people over 65 exceeded 20% in 2023. In contrast, the autonomous communities of Ceuta, Melilla and Murcia, had the lowest rates of population ageing, at around 19% [20]. At the same time, all the Autonomous Communities show a dominance of the female population in the older age group (Figure 2 c), representing a generalised trend.
2. Materials and Methods
A structured literature review was conducted as a data collection strategy. The search was conducted in May 2024, utilizing the Scopus, Web of Science, and PubMed databases. An initial filter was applied to limit results to publications from 2019 onwards, ensuring access to the most recent literature. The search terms were keywords that initially yielded over 11,000 results for some queries. To refine the search, combinations of two and three terms were employed using the Boolean operator "AND" to logically connect concepts. Additional filters, beyond the publication year, included document type (articles and reviews only), publication status (published or in press), and species (humans only).
Search data was entered into an Excel spreadsheet (Microsoft Corporation, Redmond, WA) according to the database consulted and the specific search terms used. Upon completion of the search, the findings were filtered in multiple phases. Phase I involved eliminating duplicate records identified by the search engines. In Phase II, titles were screened for relevance and alignment with the study's central theme. Phase III involved a review of abstracts, followed by a full-text review in Phase IV.
The initial search yielded 247 articles, which were reduced to 122 after the various filtering phases. A secondary search of the references in the most relevant articles added 36 articles (without a publication year restriction). Ultimately, 157 articles were included in the review.
3. Health in Older Adults
The persistently greater longevity of women is a global pattern of feminisation of old age, characterised by a greater number of women [10,21] who, despite living longer than men, must face major shortcomings in quality standards [17,28,30]. Although older adults are generally perceived as frail, dependent and vulnerable, these are, in general, stereotypes and prejudices that associate old age with illness [22]. While it is true that, in older adults, health is conditioned by the circumstances experienced; specifically by factors that are not only physical and physiological, but mainly by intersectional, psychosocial, economic and cultural factors [23,24,25,26], which are determinants during ageing [27]. In turn, evolutionary theories also point to reproduction as an important factor predisposing women to greater oxidative damage [28]. Thus, women's increased reproductive strain, combined with the less advantageous economic, cultural and educational situations they have faced throughout history [29], has a cumulative negative impact on women's lives [30,31]. As a result, despite living longer, older women often experience a poorer quality of life, and higher rates of poverty, loneliness and dependency [17,28,32].
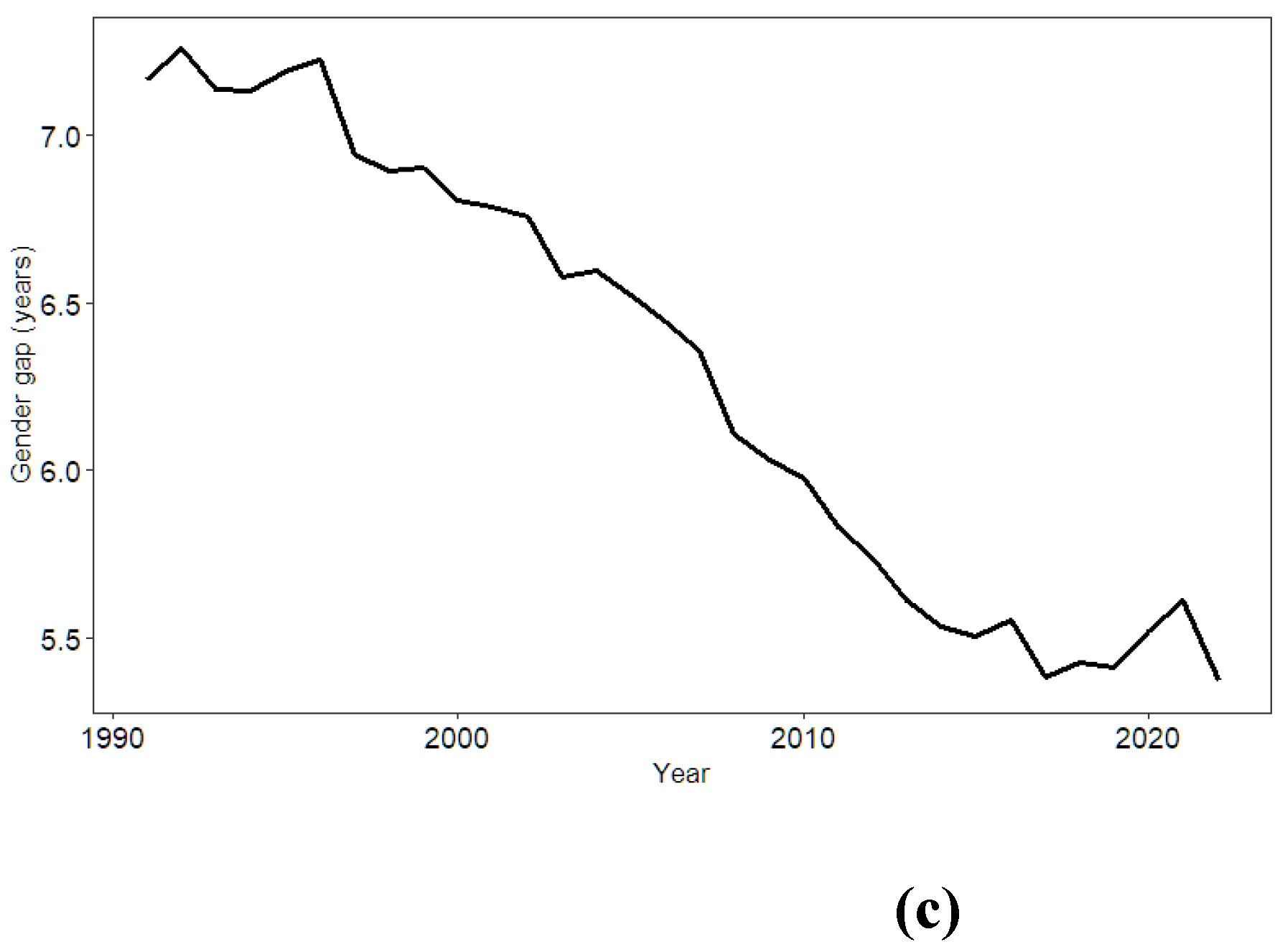
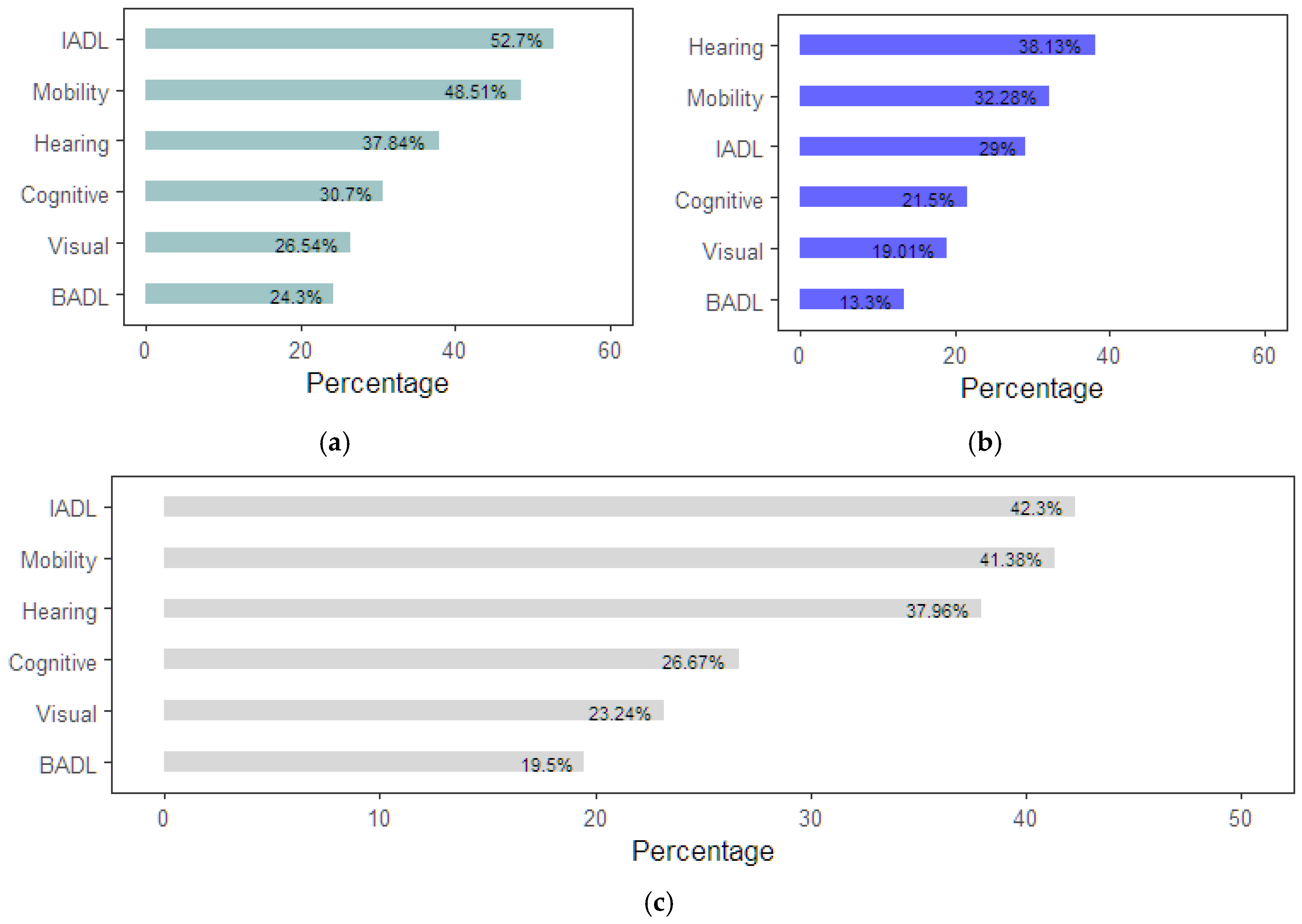
In turn, senescence increases susceptibility to disease, morbidity and mortality rates [33]. It produces highly variable clinical sequelae such as reduced skeletal muscle, skin and bone mass and strength, alterations in insulin signalling, increased adipose tissue and other immunological effects [34]; leading to increased prevalence of chronic non-communicable diseases [35]. These diseases have a multi-level impact on the lives of older adults and their families [36,37], reducing their economic, emotional and psychological well-being, leading to increased dependency and increased need for treatment or hospitalisation. Furthermore, on a global scale, non-communicable chronic diseases exhibit substantial gender disparities, as illustrated in Figure 3. [17]. In men, diseases leading to premature mortality such as cancer and heart disease are common [38,39]. However, in women, acute diseases predominate, with chronic conditions and daily symptoms that significantly affect their quality of life [38,39,40], such as osteoarthritis, osteoporosis, autoimmune diseases, fractures, vision loss, depression and dementia [41], which manifest themselves alarmingly after menopause [39,42]. As a result of diseases arising during ageing in Spanish older adults, mobility problems (41.38%), hearing impairment (37.96%), cognitive impairment (26.67%) and visual impairment (23.24%) are common in older adults (Figure 4 c). These problems predominate in the female population (Figure 4 a), with the exception of hearing impairment, which is more common in men (Figure 4 b) [43].
However, despite clear gender differences in chronic non-communicable diseases, these have not traditionally been studied and researched, even though men and women differ in disease pathophysiology, clinical manifestation, prognosis and consequences [44,45]. Thus, when men and women have the same disease, women are more likely to be diagnosed later, and thus more likely to suffer more severe consequences [39]. This is due to the lower sensitivity and specificity of traditional tests, as the diagnostic criteria used are based on the presentation of typical symptoms in males [45,46]. Therefore, the social and health bias that has existed in all societies, including biomedical research [47] and the lower inclusion of women in bio-health studies, has resulted in less use of preventive procedures by women. As a result, there is less information on the characteristics of women's mode of illness and, with it, gaps in knowledge about the determinants of women's health [40,46].
Figure 3.
Global gender disparities in the health of older adults. In women, diseases that significantly affect quality of life are common [38,39,40], while in men, diseases that lead to premature mortality predominate [38,39].
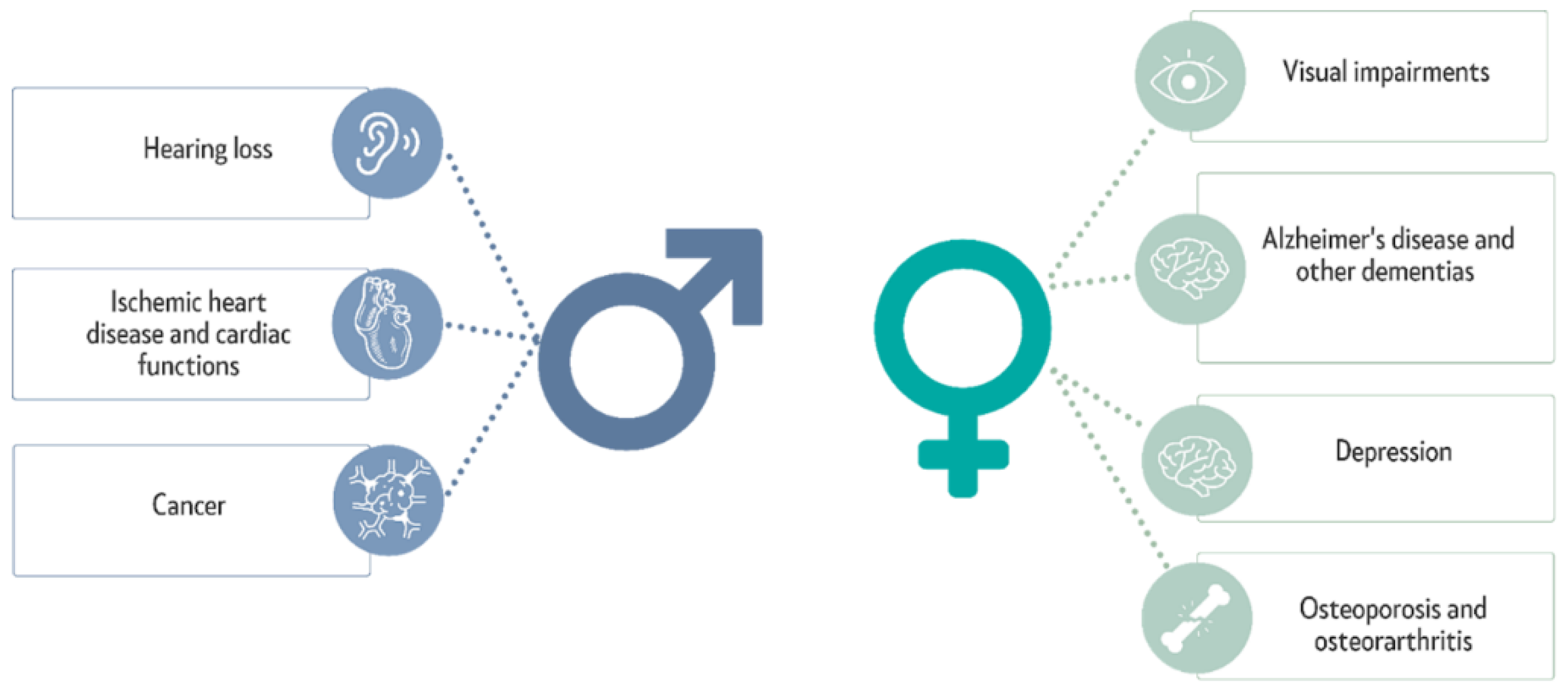
Figure 4.
Most prevalent problems in the Spanish population according to the European Health Survey in Spain 2020. (a) Problems arising from ageing in women over 65. (b) Problems arising from ageing in men aged 65 and over. (c) Problems arising from ageing in the population over 65 years of age.
Figure 4.
Most prevalent problems in the Spanish population according to the European Health Survey in Spain 2020. (a) Problems arising from ageing in women over 65. (b) Problems arising from ageing in men aged 65 and over. (c) Problems arising from ageing in the population over 65 years of age.
The impact of social and health bias is considerable in the evaluation of self-perceived health, as 28.78% of women over 75 years of age have a negative perception of their health, compared to 18.42% of men [43]. The functional deterioration caused by ageing makes it difficult for many older adults to carry out instrumental (42.29%) and basic (19.46%) activities of daily living (ADLs) [43]. This situation is aggravated by social changes in the structure and size of families and the incorporation of women into the labour market, which significantly reduce the capacity of some families to cope with the dependency situations caused by ageing. As a result, more than 40% of older adults who need help in their daily lives lack the necessary assistance to carry out some of their basic activities [43], with a significant impact on their autonomy and quality of life. It is therefore imperative to personalise and improve healthcare services for older adults in order to reduce the impact of ageing on the lives of older adults, as well as the unintentional burden placed on their families [37].
4. Healthy Ageing: Active and Social
Quality of life was defined in 1998 by the World Health Organization (WHO), [48] as “a perception of one's position in life in the context of the culture and value systems in which one lives and in relation to one's goals, expectations, standards and concerns”. While active ageing refers to “the process of optimising opportunities for health, participation and security to enhance quality of life as people age” [29]. Thus, although active ageing and quality of life are overlapping concepts, active ageing is seen as a dynamic process and quality of life as a state of being [48]. So while quality of life is influenced by personal, behavioural and economic determinants, health and social services, the physical environment and the social environment [2]; ageing can be influenced by behavioural and structural measures that shape individual experience [24].
In 2015, in the World report on ageing and health, WHO outlined the framework for action for the promotion of Healthy Ageing, highlighting the attributes that enable people to develop and maintain functional ability during the ageing process [7]. This framework for action considers 6 essential determinants: (1) determinants related to health and social services, including health promotion, disease prevention, curative services, long-term care and mental health services; (2) behavioural determinants that condition health status such as smoking, physical activity, type of diet or therapeutic adherence; (3) determinants related to personal, psychological, genetic and biological factors; (4) determinants related to the physical environment, such as safety in housing, risk of falls and absence of pollution; (5) determinants related to the social environment, such as level of social support, violence and abuse, education and literacy; (6) and economic determinants such as level of income, social protection and access to work.
The quality of life of older adults is directly linked to health, participation, and safety (2). Consequently, to promote healthy aging among this population, a per-son-centered approach must be developed (37). A person-centered approach is a philosophy and methodology that prioritizes the individual's needs, experiences, and perspectives across all domains, including health, work, education, and product or service design. Rather than focusing on general objectives or universal standards, this approach seeks to tailor solutions to the specific needs of each individual, promoting their autonomy, dignity, and well-being. This translates into research aimed at deeply understanding human experiences, developing tools and technologies adapted to individual needs, and evaluating the impact of interventions from the perspective of those involved. Additionally, for healthy aging, older adults must have access to services, employment, and volunteering opportunities, physical activity, social inclusion and participation, diet and nutrition, long-term care, accessible environments, education, and lifelong learning, including new technologies and the internet (Figure 5) [49]. It is well known that active ageing can improve the quality of life of those who practise it [2] by increasing the time of independence of older adults, enabling them to live with simple or stable chronic diseases, complex comorbidities, dementia and frailty [1]. For this, it is essential that older people maintain physical and mental health, normal cognitive function, active participation in society and good interpersonal relationships [50]. Regular physical activity helps to reduce the risk of some of the diseases associated with ageing, such as cardiovascular disease, metabolic diseases, osteoarthritis, cognitive impairment [51], mobility problems, disability and the risk of falls [52]. It also improves verbal memory, executive functioning, attention and global cognition. The evidence that neuroplasticity is preserved later in life creates a unique opportunity for cognitive interventions to delay and mitigate the onset of cognitive decline in later life. Cognitively stimulating activities are therefore recommended to delay age-related decline while increasing social contact through activities such as reading, crossword puzzles, mind games, card games or board games [51]. However, the participation of older adults is often conditioned by traditionally consolidated gender roles, resulting in differential access to resources, goods and services, which again places women at a disadvantage. These differences are accentuated by the worse economic situation faced by older women, who are more likely to have spent most of their lives in unpaid work, presenting a high risk of impoverishment and marginalisation. For this reason, for older women, access to paid work is a source of income and independence, enabling empowerment and greater participation in social support networks, greater satisfaction, self-esteem and improved mental health [53]. Thus, in order to achieve active ageing, it is imperative to understand ageing also from a gender perspective, as it raises awareness of the influence that gender has exerted (and exerts) on women's lives, and the consequences it produces at older ages; highlighting the need to promote adapted and appropriate strategies that eliminate gender inequalities and promote active, participatory and social ageing [23].
Human beings are social, compassionate and cooperative [54] by nature, requiring social relationships for their well-being and maintenance of health [55]. However, today's societies are characterised by shrinking family size and migration of family members, causing social disconnection and accentuating social isolation and loneliness in older adults [56] around the world [57]. Despite this, many older adults live alone, maintain frequent social contact, develop satisfying social relationships and are active in community organisations, so living alone is not synonymous with unwanted isolation or loneliness [22,51]. However, problems arising from physical disability, frailty, lack of independence or poor health do have a limiting effect on older adults' ability to enjoy leisure activities, as they rely on others for daily stimulation and social interactions; these factors increase social isolation and loneliness in older adults [55]. In this regard, women, due to their greater longevity and poorer living conditions, are more likely to suffer from this lack of independence, leading to a higher risk of unwanted loneliness. Therefore, the scientific community suggests that being an older woman, being unmarried, having a low economic and/or educational level, living alone, having low quality social relations and health problems are associated with a higher risk of suffering from isolation and loneliness [54].
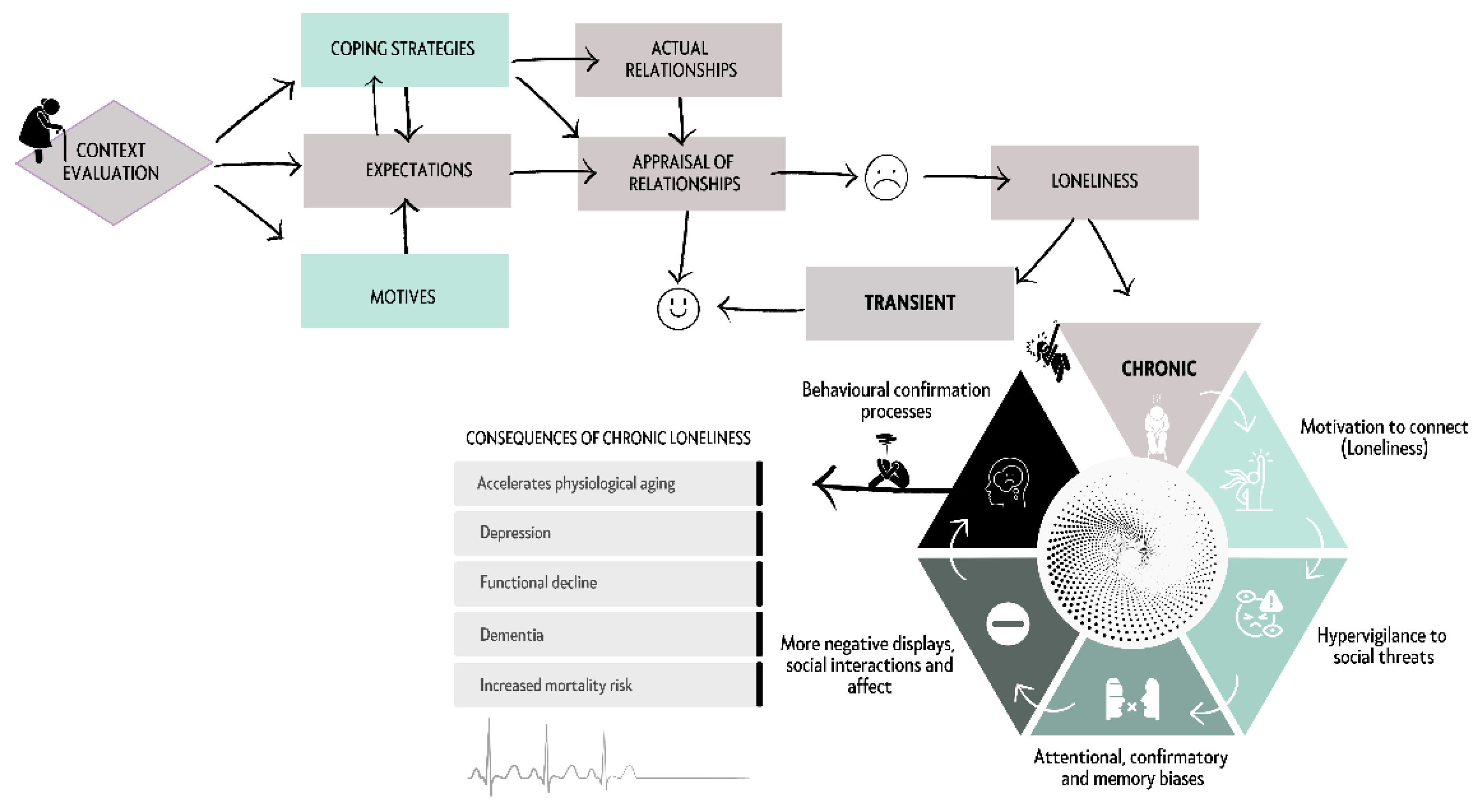
Social isolation refers to the absence of regular contact with family and friends, and of participation in social organisations [55]. Loneliness, however, refers to the perceptual experience of social isolation. Defined as the discrepancy between a person's preferred level of social contact and their actual level of social contact, it reflects a subjective state of involuntary lack of affection and closeness [58]. Loneliness, when unwanted, is a subjective source of emotional, physical and existential distress during older adults' later years [8]. Although older adults generally possess fewer tools for social reconnection [8,59], some of them develop strategies to cope with loneliness by accepting low levels of social contacts and keeping themselves occupied with solitary activities [60]. The development of loneliness is influenced by demographic variables (gender, socioeconomic status and education) and health variables (functional status, self-rated health and depressive symptoms) [61], and is triggered by events as diverse as retirement, widowhood, bereavement, mobility limitations or cognitive decline [5,8,57]. Once the feeling of loneliness has developed, depending on its duration, it can be classified into two types: transient loneliness or chronic loneliness. Transitory loneliness motivates reconnection with other people when coping strategies are successful, being able to modify expectations, evaluations or real relationships. However, when these strategies are unsuccessful, chronic loneliness occurs, leading to a snowball effect, increasing social isolation and thus producing increasingly severe health consequences (Figure 6) [58,62]. People suffering from chronic loneliness enter a vicious circle: they are often physically inactive, exhibiting harmful sedentary behaviours [63] that trigger pathologies such as high blood pressure, atherosclerosis, stroke, functional impairment, depression or dementia, which ultimately result in an increased risk of mortality [64,65].
5. Information and Communication Technologies (ICTs): A New Opportunity to Assist Older Adults
Demographic changes and increasing longevity pose serious challenges for the care of older people. While ageing at home is a desirable option for many, the reality is that there are situations where nursing homes become a necessary alternative. The choice of where to grow old is a decision conditioned not only by the person's wishes, but also by his or her needs and available resources [66]. In this regard, older adults are considered a population likely to have insufficient income and limited resources to manage unexpected changes in their lives, relying in many cases on social services and community assistance to live independently at home [67]. For them, home represents a familiar, safe and memory-laden space that provides a sense of belonging and benefits attention and memory [68]. Thus, leaving home can be a traumatic uprooting, resulting in isolation from friends and family, loss of identity, stress, anxiety, depression and accelerated cognitive decline. It is therefore particularly important that in cases of leaving home, if the decision is made to age in a nursing home, it should be easily accessible, and that it should support older adults' individuality, participation, engagement and social connectedness [69]. However, the growing demand for long-term ser-vices and the scarcity of resources are forcing a rethink of traditional care models. It is therefore imperative to develop innovative strategies that enable older people to age in a dignified and safe manner, whether at home or in residential care, combining quality care with a person-centred approach and individual needs [68]. In this scenario, technological advances create a unique opportunity through the creation of smart living environments [63], which provide a context-aware, personalised, anticipatory, adaptive, ubiquitous, transparent, accessible and gender-sensitive service [68]. New technologies are a reality in our daily lives and have become facilitators of processes, both at home and in the workplace and healthcare. Information and Communication Technologies (ICT’s) are the set of tools and resources that enable the creation, storage, processing, and transmission of information digitally. From computers and smartphones to internet networks and software, ICT has revolutionized the way we communicate, work, and live. Its scientific foundation lies in disciplines such as information theory, electronics, computer science, and telecommunications, and its impact extends to all areas of society, from scientific research to education and entertainment
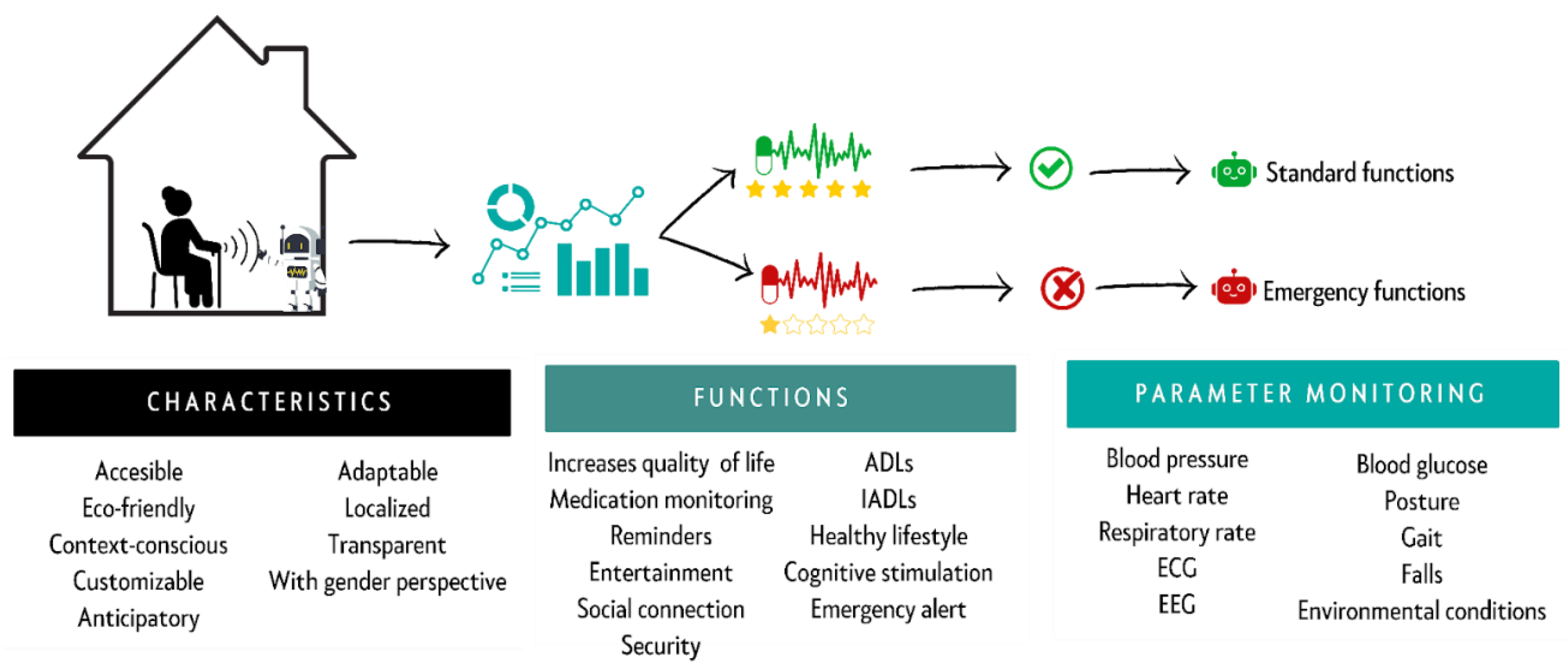
At the same time, as the years go by, older adults' need for health care increases. In many cases, they require regular medical check-ups and chronic treatments, and follow-up care is particularly important when they live alone or are frail [70]. Currently, there are many strategies used to improve the quality of life of older adults, but one of the most widely used is adapting the home to increase safety and mobility, facilitate the use of assistive devices, and maintain familiarity [60]. The implementation of ICTs within the home makes it possible to objectively assess the severity of situations faced by the older adult (Figure 7) through the use of portable sensors. These sensors, placed in different areas of the home and body regions [71], allow biomechanical and physiological data to be collected passively [72], monitoring the older adult's condition in real time. For their assessment, the scientific community recommends combining biological and environmental signals, as this improves the characterisation of the health and risk faced by older adults in their daily lives [71]. Gait parameters such as speed, cadence, stride length or sway can allow detection of health problems, postural changes and prediction of falls [73]. Analysis of activities of daily living (ADLs), behaviour, facial expressions, number of steps taken, time spent being active, number of calories consumed, energy expenditure, quality of movement or sleep is also recommended [71,73]. It is also essential to monitor body temperature, hydration level, weight, heart rate, blood pressure, oxygen saturation and glucose levels, among others. Thanks to the integration of all this information and its subsequent analysis through algorithms, deviations and patterns that are early indicators of disease can be detected, enabling early action and the adoption of measures aimed at reducing the risk to which older adults are exposed [74]. In turn, the use of ICTs enables them to improve self-management of chronic diseases [67], as by understanding their diseases, older adults can better manage them, maintaining control over their lives and being empowered [37].
ICTs are also useful in preventing, early detection and combating loneliness. However, although it is possible to detect and assess a person's loneliness through the use of sensors [63], there are a number of limitations to their application. One limitations is the difficulty in accurately tracking the activities of the older adult when living with others, in which case the use of sensors embedded in clothing, footwear, wrists, pendants or the trunk is recommended [72]. In the process of preventing and eliminating loneliness, the participation of older adults in activities that enhance their well-being and improve their quality of life is recommended [59]. In this regard, the use of the Internet can be a great ally, allowing for the maintenance and enhancement of existing relationships, as well as the forging of new social connections [54,75]. While ICTs can facilitate social connection and reduce feelings of isolation, their effectiveness depends on several factors, such as digital literacy and gender [54,61]. These difficulties were particularly noticeable at critical times of social distancing such as the Covid-19 pandemic [62], when digital contact helped to alleviate the feeling of loneliness, which was predominant among women. However, although ICTs facilitate social connection and reduce feelings of loneliness in the short term, the scientific community disagrees as to their effectiveness [59,61], concluding that, although digital technology cannot replace human contact, it can be a very useful complement in the lives of older adults to combat loneliness. Thus, it is essential to complement the use of technologies with strategies that promote face-to-face social interaction and participation in meaningful activities.
The robotic assistive platforms specifically for older adults available on the market offer a multitude of services. These include medication management, memory training, various services based on ADLs and instrumental activities of daily living (IADLs), support for the management of mental health disorders, assistance in achieving a healthy lifestyle, promotion of physical activity and nutritional changes [70,76]. However, the magnitude of population ageing is such that it will require the design of new robotic platforms that are eco-friendly and environmentally friendly, capable of improving the lives of older adults without interfering with their daily lives [49]. These platforms should be customizable, allowing them to be adapted to the user's personal tastes and history, so as to enhance their use [77]. Available evidence supports that the use of ICTs in older adults produces a calming effect that reduces cortisol levels, blood pressure and heart rate, and increases oxytocin levels [78,79,80]. Thanks to ICTs, older adults can easily maintain a healthy lifestyle, thus preventing the onset of diseases, while favouring the development of multiple tasks, promoting personal autonomy, facilitating interaction with other people, reducing the level of cognitive impairment and improving their quality of life [67,70,81,82]. However, many older adults are still reluctant to accept their use, believing (wrongly) that using them makes them frail and dependent [83]. And even once accepted, they may abandon them because of difficulties in using them [8], lack of information, discomfort, interference with daily life or unwillingness to justify behaviours considered abnormal by the platforms. However, although the use of assistive robotic platforms for older adults currently causes concern and mistrust [78], their correct use will allow their usefulness to be recognised, making them allies and companions of older adults.
However, a serious design problem with current care platforms is that, although they collect information on the life context in which older adults age, their algorithms do not take into account sex and gender dimensions, which can lead to biassed, erroneous and discriminatory results for women [84]. This is a serious problem, as the feminisation of ageing is a predominant global reality, yet it continues to be neglected, negatively affecting women. In turn, although most older adults want to prevent the aggravation of their chronic problems, in some cases there are economic constraints that not only prevent them from maintaining a healthy diet, covering their medical treatments, coping with unforeseen events [37], but also make it difficult to access assistive technologies, especially among women. Therefore, providers of ICTs for older adults will need to take into consideration and adapt to the realities of the ageing population. At the same time, they should take into account that it is not possible to implement a homogeneous evaluation of the problems detected by the sensors in ICTs, if the aim is to prevent and detect early the emergency situations that older adults face in their daily lives, given the gender differences that are evident. Furthermore, it is essential to bear in mind that, although the use of these platforms has many benefits for the lives of older adults, they cannot replace human interaction, since in the final stage of their lives older adults may have needs that compromise their dignity, which are difficult to manage by means of a robotic assistive platform alone [85].
Figure 7.
General characteristics, functions and parameters monitored by the robotic assistive platforms specifically designed for older adults. The platform monitors multiple parameters of the older adult at home and after analysis, depending on the adequacy of the parameters, executes normal functions or emergency functions (such as alerting health professionals or family members, depending on the severity).
Figure 7.
General characteristics, functions and parameters monitored by the robotic assistive platforms specifically designed for older adults. The platform monitors multiple parameters of the older adult at home and after analysis, depending on the adequacy of the parameters, executes normal functions or emergency functions (such as alerting health professionals or family members, depending on the severity).
6. Conclusions: ICTs as Allies of Well-Being
Society is facing an unprecedented demographic challenge, population ageing. Driven by increasing life expectancy and low birth rates, the age transition has significant personal, social and economic impacts, producing a series of challenges that need to be addressed comprehensively. Older adults often have greater health needs, re-quiring more support in their daily lives, increasing the pressure on health and social care systems and their families. During ageing, older adults face a number of problems, which are particularly noticeable for women. In this respect, the use of ICTs specifically designed for older adults is promising, offering a multitude of benefits for older adults, as long as they are designed with gender differences in ageing in mind. New robotic assistive platforms should be able to improve the quality of life of older adults through telecare, home automation and access to leisure and cultural services, enabling older adults to achieve active ageing, staying active and independent by promoting physical activity, continuous learning, social participation, communication and social interaction; thus enabling the prevention, detection and early treatment of age-related emergencies. Therefore, the implementation of ICTs in the daily life of old-er adults is promising by enabling them to live independently at home for longer, providing them with a context-aware, personalsed, anticipatory, adaptive, ubiquitous, transparent, accessible and gender-sensitive service, in a scenario where families can-not cope alone with the dependency situation of their relatives. On the other hand, it is imperative and crucial to provide equitable access to affordable, high-quality ICTs for older adults. This can be achieved through collaborative efforts with stakeholders and decision-makers, ensuring gender parity. Moreover, the integration of an inclusive service model for older adults, coupled with adequate health insurance coverage, would facilitate the development of comprehensive intervention plans for aging-in-place seniors.
However, the utilization of ICTs also presents a range of challenges that must be addressed to guarantee that these technologies improve the quality of life of older adults. At present, two barriers still need to be eliminated: the digital divide and the gender divide. The digital divide to ensure that all older adults have access to ICTs and learn how to use them safely and effectively. And the gender gap, still persistent in assistive technology, to ensure adequate care for older women. Therefore, providers of assistive robotic platforms must design them according to the personal, economic, social, family, gender, health and independence circumstances of older adults, adapting to the differential socio-economic and health conditions of men and women. Considering that the feminisation of ageing is a global reality, and that despite the fact that women live longer, they age less well and have different needs than men.
In conclusion, population ageing is a complex phenomenon that requires a com-prehensive and multi-sectoral response, and while ICTs represent a powerful tool to address some of the challenges of ageing and improve the quality of life of older adults, it is important to use them responsibly and ethically, taking into account the specific needs and preferences of older adults. And that, while population ageing presents a number of challenges, it also offers opportunities to build a more positive and inclusive future. Harnessing the potential of ICTs by adopting a person-centred approach is therefore a unique opportunity to create a society in which all older adults can live full, healthy and active lives, and in which the inequalities faced by older women are eliminated.
A limitation of this study is the inclusion of some Spanish statistics rather than international data. However, this also presents an opportunity to expand the research to other countries with different social realities and quality of life. These future research directions will enable objective and subjective comparisons of the actual possibilities for implementing ICTs to contribute to active and healthy aging among older adults.
Author Contributions
BR: Methodology; Investigation; Writing; Original draft preparation. MIP: Methodology; Investigation; Writing; Review & editing. AMLO, AMGC & EFV: Visualization; Review & editing, MTH: Conceptualization; Methodology; Writing; Investigation; Writing—original draft; Funding acquisition; Project administration; Supervision; Validation; Visualization; Review & editing.
Funding
This research was funded by the grants from the Agencia Estatal de Investigación, Ministerio de Ciencia, Innovación y Universidades, co-funded by the European Union, Next Generation EU/PRTR Ref. Number: TED2021-130942B-C21 // MICIU/AEI /10.13039/501100011033), the “Fundación Primafrío” with the code number 39747, COST Participatory Approaches with Older Adults (PAAR-net), with the code number CA22167 and China-Spain AI Technology Joint Laboratory with Hangzhou Dianzi University.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
Not applicable.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Al-Shaqi, R.; Mourshed, M.; Rezgui, Y. Progress in ambient assisted systems for independent living by the elderly. SpringerPlus 2016, 5, 1–20. [Google Scholar] [CrossRef] [PubMed]
- Marzo, R.R.; Khanal, P.; Shrestha, S.; Mohan, D.; Myint, P.K.; Su, T.T. Determinants of active aging and quality of life among older adults: systematic review. Front. Public Heal. 2023, 11, 1193789. [Google Scholar] [CrossRef] [PubMed]
- Serrano, J.P.; Latorre, J.M.; Gatz, M. Spain: Promoting the Welfare of Older Adults in the Context of Population Aging. Gerontol. 2014, 54, 733–740. [Google Scholar] [CrossRef]
- Song, I.-Y.; Song, M.; Timakum, T.; Ryu, S.-R.; Lee, H. The landscape of smart aging: Topics, applications, and agenda. Data Knowl. Eng. 2018, 115, 68–79. [Google Scholar] [CrossRef]
- Fakoya, O.A.; McCorry, N.K.; Donnelly, M. Loneliness and social isolation interventions for older adults: a scoping review of reviews. BMC Public Heal. 2020, 20, 1–14. [Google Scholar] [CrossRef]
- Nugent, R. Preventing and managing chronic diseases. BMJ 2019, 364, l459. [Google Scholar] [CrossRef] [PubMed]
- Kemoun Ph, Ader I, Planat-Benard V, Dray C, Fazilleau N, Monsarrat P, et al. A gerophysiology perspective on healthy ageing. Ageing Res Rev. 2022 Jan 1;73:101537.
- Kotwal, A.A.; Cenzer, I.S.; Waite, L.J.; Covinsky, K.E.; Perissinotto, C.M.; Boscardin, W.J.; Hawkley, L.C.; Dale, W.; Smith, A.K. The epidemiology of social isolation and loneliness among older adults during the last years of life. J. Am. Geriatr. Soc. 2021, 69, 3081–3091. [Google Scholar] [CrossRef] [PubMed]
- Petrov, I.C. The Elderly in a Period of Transition: Health, Personality, and Social Aspects of Adaptation. Ann. New York Acad. Sci. 2007, 1114, 300–309. [Google Scholar] [CrossRef] [PubMed]
- Bronikowski, A.M.; Meisel, R.P.; Biga, P.R.; Walters, J.R.; Mank, J.E.; Larschan, E.; Wilkinson, G.S.; Valenzuela, N.; Conard, A.M.; de Magalhães, J.P.; et al. Sex-specific aging in animals: Perspective and future directions. Aging Cell 2022, 21, e13542. [Google Scholar] [CrossRef] [PubMed]
- Ismail, Z.; Ahmad, W.I.W.; Hamjah, S.H.; Astina, I.K. The Impact of Population Ageing: A Review. Iran. J. Public Heal. 2021, 50, 2451–2460. [Google Scholar] [CrossRef]
- Atance, D.; Claramunt, M.M.; Varea, X.; Aburto, J.M. Convergence and divergence in mortality: A global study from 1990 to 2030. PLOS ONE 2024, 19, e0295842. [Google Scholar] [CrossRef]
- World report on ageing and health [Internet]. [cited 2024 Jun 21]. Available from: https://www.who.int/publications/i/item/9789241565042.
- Instituto Nacional de Estadística. Evolución de la esperanza de vida al nacimiento. Brecha de género. España [Internet]. [cited 2024 Jun 26]. Available from: https://www.ine.es/ss/Satellite?blobcol=urldata&blobheader=Unknown+format&blobheadername1=Content-Disposition&blobheadervalue1=attachment%3B+filename%3DD1T1.xlsx&blobkey=urldata&blobtable=MungoBlobs&blobwhere=61%2F25%2FD1T1%2C0.xlsx&ssbinary=true.
- Pérez Díaz J, Ramiro Fariñas D, Aceituno Nieto P, Escudero Martínez J, Bueno López C, Castillo Belmonte AB, et al. Un perfil de las personas mayores en España, 2023 Indicadores estadísticos básicos. [Internet]. Madrid; 2023. Available from: https://envejecimientoenred.csic.es/wp-content/uploads/2023/10/enred-indicadoresbasicos2023.pdf.
- Sunzi, K.; Li, Y.; Lei, C.; Zhou, X. How do the older adults in nursing homes live with dignity? A protocol for a meta-synthesis of qualitative research. BMJ Open 2023, 13, e067223. [Google Scholar] [CrossRef] [PubMed]
- Hägg, S.; Jylhävä, J.; Biostatistics; Institutet, K.; Sweden Sex differences in biological aging with a focus on human studies. eLife 2021, 10. [CrossRef]
- Damaske S, Frech A. Women’s Work Pathways Across the Life Course. Demography. 2016 Apr;53(2):365–91.
- Esperanza de vida a los 65 años en la UE. Brecha de género. Serie 2021-2022. [Internet]. [cited 2024 Jul 1]. Available from: https://www.ine.es/jaxi/Datos.htm?path=/t00/mujeres_hombres/tablas_1/l0/&file=d01008.px.
- Instituto Nacional de Estadística. Proporción de personas mayores de cierta edad por comunidad autónoma [Internet]. 2024. Available from: https://www.ine.es/jaxi/Datos.htm?path=/t00/mujeres_hombres/tablas_2/&file=d2g5.px.
- Sampathkumar, N.K.; Bravo, J.I.; Chen, Y.; Danthi, P.S.; Donahue, E.K.; Lai, R.W.; Lu, R.; Randall, L.T.; Vinson, N.; Benayoun, B.A. Widespread sex dimorphism in aging and age-related diseases. Hum. Genet. 2019, 139, 333–356. [Google Scholar] [CrossRef]
- Jasienska, G. Costs of reproduction and ageing in the human female. Philos. Trans. R. Soc. B: Biol. Sci. 2020, 375, 20190615. [Google Scholar] [CrossRef]
- Sousa NF da S, Lima MG, Cesar CLG, Barros MB de A. Active aging: prevalence and gender and age differences in a population-based study. Cad Saúde Pública. 2018 Nov 23;34:e00173317.
- Langmann, E.; Weßel, M. Leaving no one behind: successful ageing at the intersection of ageism and ableism. Philos. Ethic- Humanit. Med. 2023, 18, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Perissinotto CM, Cenzer IS, Covinsky KE. Loneliness in Older Persons: A predictor of functional decline and death. Arch Intern Med. 2012 Jul 23;172(14):1078–83.
- Byhoff, E.; Tripodis, Y.; Freund, K.M.; Garg, A. Gender Differences in Social and Behavioral Determinants of Health in Aging Adults. J. Gen. Intern. Med. 2019, 34, 2310–2312. [Google Scholar] [CrossRef] [PubMed]
- Raparelli, V.; Norris, C.M.; Bender, U.; Herrero, M.T.; Kautzky-Willer, A.; Kublickiene, K.; El Emam, K.; Pilote, L. Identification and inclusion of gender factors in retrospective cohort studies: the GOING-FWD framework. BMJ Glob. Heal. 2021, 6, e005413. [Google Scholar] [CrossRef]
- Tadiri, C.P.; Gisinger, T.; Kautzky-Willer, A.; Kublickiene, K.; Herrero, M.T.; Norris, C.M.; Raparelli, V.; Pilote, L. Additional file 1 of Determinants of perceived health and unmet healthcare needs in universal healthcare systems with high gender equality. [CrossRef]
- World Health Organization. Active ageing: A policy framework. Madrid: World Health Organization; 2002.
- Instituto de la Mujer y Para la Igualdad de Oportunidades. Mujeres Mayores [Internet]. 2019. Available from: https://www.inmujeres.gob.es/areasTematicas/AreaSalud/Publicaciones/docs/GuiasSalud/Salud_IX.pdf Reference class.
- Ryan, C.P.; Lee, N.R.; Carba, D.B.; MacIsaac, J.L.; Lin, D.T.S.; Atashzay, P.; Belsky, D.W.; Kobor, M.S.; Kuzawa, C.W. Pregnancy is linked to faster epigenetic aging in young women. Proc. Natl. Acad. Sci. 2024, 121. [Google Scholar] [CrossRef]
- Taylor L. Women live longer than men but have more illness throughout life, global study finds. BMJ. 2024 May 2;385:q999.
- Melzer, D.; Pilling, L.C.; Ferrucci, L. The genetics of human ageing. Nat. Rev. Genet. 2019, 21, 88–101. [Google Scholar] [CrossRef] [PubMed]
- Jones, C.M.; Boelaert, K. The Endocrinology of Ageing: A Mini-Review. Gerontology 2014, 61, 291–300. [Google Scholar] [CrossRef]
- Mönninghoff, A.; Fuchs, K.; Wu, J.; Albert, J.; Mayer, S. The Effect of a Future-Self Avatar Mobile Health Intervention (FutureMe) on Physical Activity and Food Purchases: Randomized Controlled Trial. J. Med Internet Res. 2022, 24, e32487. [Google Scholar] [CrossRef] [PubMed]
- Bin Sawad, A.; Narayan, B.; Alnefaie, A.; Maqbool, A.; Mckie, I.; Smith, J.; Yuksel, B.; Puthal, D.; Prasad, M.; Kocaballi, A.B. A Systematic Review on Healthcare Artificial Intelligent Conversational Agents for Chronic Conditions. Sensors 2022, 22, 2625. [Google Scholar] [CrossRef]
- McGilton, K.S.; Vellani, S.; Yeung, L.; Chishtie, J.; Commisso, E.; Ploeg, J.; Andrew, M.K.; Ayala, A.P.; Gray, M.; Morgan, D.; et al. Identifying and understanding the health and social care needs of older adults with multiple chronic conditions and their caregivers: a scoping review. BMC Geriatr. 2018, 18, 1–33. [Google Scholar] [CrossRef] [PubMed]
- Phillips, S.P.; O’connor, M.; Vafaei, A. Women suffer but men die: survey data exploring whether this self-reported health paradox is real or an artefact of gender stereotypes. BMC Public Heal. 2023, 23, 1–10. [Google Scholar] [CrossRef]
- Carmel, S. Health and Well-Being in Late Life: Gender Differences Worldwide. Front. Med. 2019, 6, 218. [Google Scholar] [CrossRef]
- Short SE, Yang YC, Jenkins TM. Sex, Gender, Genetics, and Health. Am J Public Health. 2013 Oct;103(Suppl 1):S93–101.
- Nair, S.; Sawant, N.; Thippeswamy, H.; Desai, G. Gender Issues in the Care of Elderly: A Narrative Review. Indian J. Psychol. Med. 2021, 43, S48–S52. [Google Scholar] [CrossRef]
- Dong, L.; Teh, D.B.L.; Kennedy, B.K.; Huang, Z. Unraveling female reproductive senescence to enhance healthy longevity. Cell Res. 2023, 33, 11–29. [Google Scholar] [CrossRef]
- Encuesta Europea de Salud en España [Internet]. Instituto Nacional de Estadística; 2020. Available from: https://www.sanidad.gob.es/estadEstudios/estadisticas/EncuestaEuropea/EESE2020_inf_evol_princip_result2.pdf.
- Balistreri, C.R. New frontiers in ageing and longevity: Sex and gender medicine. Mech. Ageing Dev. 2023, 214, 111850. [Google Scholar] [CrossRef]
- Westergaard, D.; Moseley, P.; Sørup, F.K.H.; Baldi, P.; Brunak, S. Population-wide analysis of differences in disease progression patterns in men and women. Nat. Commun. 2019, 10, 1–14. [Google Scholar] [CrossRef]
- Sun TY, Hardin J, Nieva HR, Natarajan K, Cheng R fong, Ryan P, et al. Large-scale characterization of gender differences in diagnosis prevalence and time to diagnosis. medRxiv. 2023 Oct 16;2023.10.12.23296976.
- Gogovor, A.; Zomahoun, H.T.V.; Ekanmian, G.; Adisso, .L.; Tardif, A.D.; Khadhraoui, L.; Rheault, N.; Moher, D.; Légaré, F. Sex and gender considerations in reporting guidelines for health research: a systematic review. Biol. Sex Differ. 2021, 12, 62. [CrossRef]
- Development of the World Health Organization WHOQOL-BREF quality of life assessment. The WHOQOL Group. Psychol Med. 1998 May;28(3):551–8.
- Baraković, S.; Husić, J.B.; van Hoof, J.; Krejcar, O.; Maresova, P.; Akhtar, Z.; Melero, F.J. Quality of Life Framework for Personalised Ageing: A Systematic Review of ICT Solutions. Int. J. Environ. Res. Public Heal. 2020, 17, 2940. [Google Scholar] [CrossRef]
- Chi, Y.-C.; Wu, C.-L.; Liu, H.-T. Effect of a multi-disciplinary active aging intervention among community elders. Medicine 2021, 100, e28314. [Google Scholar] [CrossRef] [PubMed]
- Harmell, A.L.; Jeste, D.; Depp, C. Strategies for Successful Aging: A Research Update. Curr. Psychiatry Rep. 2014, 16, 476–476. [Google Scholar] [CrossRef]
- Barha, C.K.; Falck, R.S.; Skou, S.T.; Liu-Ambrose, T. Personalising exercise recommendations for healthy cognition and mobility in aging: time to address sex and gender (Part 1). Br. J. Sports Med. 2020, 55, 300–301. [Google Scholar] [CrossRef] [PubMed]
- Payne S, Doyal L. Older women, work and health.
- Akhter-Khan, S.C. Providing Care Is Self-Care: Towards Valuing Older People’s Care Provision in Global Economies. Gerontol. 2020, 61, 631–639. [Google Scholar] [CrossRef]
- Steptoe, A.; Shankar, A.; Demakakos, P.; Wardle, J. Social isolation, loneliness, and all-cause mortality in older men and women. Proc. Natl. Acad. Sci. 2013, 110, 5797–5801. [Google Scholar] [CrossRef] [PubMed]
- Qianqian D, Ni G, Qin H, Guicheng C, Jingyue X, L L, et al. Why do older adults living alone in cities cease seeking assistance? A qualitative study in China. BMC Geriatr [Internet]. 2022 Jun 29 [cited 2024 Jun 19];22(1). Available from: https://pubmed.ncbi.nlm.nih.gov/35768784/.
- Newmyer, L.; Verdery, A.M.; Wang, H.; Margolis, R. Population Aging, Demographic Metabolism, and the Rising Tide of Late Middle Age to Older Adult Loneliness Around the World. Popul. Dev. Rev. 2022, 48, 829–862. [Google Scholar] [CrossRef] [PubMed]
- Ong, A.D.; Uchino, B.N.; Wethington, E. Loneliness and Health in Older Adults: A Mini-Review and Synthesis. Gerontology 2015, 62, 443–449. [Google Scholar] [CrossRef] [PubMed]
- Petersen, B.; Khalili-Mahani, N.; Murphy, C.; Sawchuk, K.; Phillips, N.; Li, K.Z.H.; Hebblethwaite, S. The association between information and communication technologies, loneliness and social connectedness: A scoping review. Front. Psychol. 2023, 14. [Google Scholar] [CrossRef]
- Abdi S, Spann A, Borilovic J, de Witte L, Hawley M. Understanding the care and support needs of older people: a scoping review and categorisation using the WHO international classification of functioning, disability and health framework (ICF). BMC Geriatr. 2019 Jul 22;19(1):195.
- Shah, S.G.S.; Nogueras, D.; van Woerden, H.C.; Kiparoglou, V. Evaluation of the Effectiveness of Digital Technology Interventions to Reduce Loneliness in Older Adults: Systematic Review and Meta-analysis. J. Med Internet Res. 2021, 23, e24712. [Google Scholar] [CrossRef] [PubMed]
- Akhter-Khan, S.C.; Prina, M.; Wong, G.H.-Y.; Mayston, R.; Li, L. Understanding and Addressing Older Adults’ Loneliness: The Social Relationship Expectations Framework. Perspect. Psychol. Sci. 2022, 18, 762–777. [Google Scholar] [CrossRef] [PubMed]
- Prabhu, D.; Kholghi, M.; Sandhu, M.; Lu, W.; Packer, K.; Higgins, L.; Silvera-Tawil, D. Sensor-Based Assessment of Social Isolation and Loneliness in Older Adults: A Survey. Sensors 2022, 22, 9944. [Google Scholar] [CrossRef] [PubMed]
- Kim, Y.B.; Lee, S.H. Gender Differences in Correlates of Loneliness among Community-Dwelling Older Koreans. Int. J. Environ. Res. Public Heal. 2022, 19, 7334. [Google Scholar] [CrossRef] [PubMed]
- Paquet, C.; Whitehead, J.; Shah, R.; Adams, A.M.; Dooley, D.; Spreng, R.N.; Aunio, A.-L.; Dubé, L. Social Prescription Interventions Addressing Social Isolation and Loneliness in Older Adults: Meta-Review Integrating On-the-Ground Resources. J. Med Internet Res. 2023, 25, e40213. [Google Scholar] [CrossRef]
- Benson SG, Dundis SP. Understanding and motivating health care employees: integrating Maslow’s hierarchy of needs, training and technology. J Nurs Manag. 2003;11(5):315–20.
- Chan, D.Y.L.; Lee, S.W.H.; Teh, P.-L. Factors influencing technology use among low-income older adults: A systematic review. Heliyon 2023, 9, e20111. [Google Scholar] [CrossRef]
- Cobo, A.; Villalba-Mora, E.; Pérez-Rodríguez, R.; Ferre, X.; Rodríguez-Mañas, L. Unobtrusive Sensors for the Assessment of Older Adult’s Frailty: A Scoping Review. Sensors 2021, 21, 2983. [Google Scholar] [CrossRef] [PubMed]
- Brath, H.; Kalia, S.; Li, J.M.; Lawson, A.; Rochon, P.A. Designing nursing homes with older women in mind. J. Am. Geriatr. Soc. 2022, 70, 3657–3659. [Google Scholar] [CrossRef]
- Kim, J.-W.; Choi, Y.-L.; Jeong, S.-H.; Han, J. A Care Robot with Ethical Sensing System for Older Adults at Home. Sensors 2022, 22, 7515. [Google Scholar] [CrossRef]
- Félix, J.; Moreira, J.; Santos, R.; Kontio, E.; Pinheiro, A.R.; Sousa, A.S.P. Health-Related Telemonitoring Parameters/Signals of Older Adults: An Umbrella Review. Sensors 2023, 23, 796. [Google Scholar] [CrossRef] [PubMed]
- Vavasour, G.; Giggins, O.M.; Doyle, J.; Kelly, D. How wearable sensors have been utilised to evaluate frailty in older adults: a systematic review. J. Neuroeng. Rehabilitation 2021, 18, 1–20. [Google Scholar] [CrossRef]
- Momin, S.; Sufian, A.; Barman, D.; Dutta, P.; Dong, M.; Leo, M. In-Home Older Adults’ Activity Pattern Monitoring Using Depth Sensors: A Review. Sensors 2022, 22, 9067. [Google Scholar] [CrossRef] [PubMed]
- Surianarayanan, C.; Lawrence, J.J.; Chelliah, P.R.; Prakash, E.; Hewage, C. Convergence of Artificial Intelligence and Neuroscience towards the Diagnosis of Neurological Disorders—A Scoping Review. Sensors 2023, 23, 3062. [Google Scholar] [CrossRef] [PubMed]
- Nowland R, Necka EA, Cacioppo JT. Loneliness and Social Internet Use: Pathways to Reconnection in a Digital World? Perspect Psychol Sci J Assoc Psychol Sci. 2018 Jan;13(1):70–87.
- Martinengo, L.; Jabir, A.I.; Goh, W.W.T.; Lo, N.Y.W.; Ho, M.-H.R.; Kowatsch, T.; Atun, R.; Michie, S.; Car, L.T. Conversational Agents in Health Care: Scoping Review of Their Behavior Change Techniques and Underpinning Theory. J. Med Internet Res. 2022, 24, e39243. [Google Scholar] [CrossRef] [PubMed]
- Casanova, G.; Zaccaria, D.; Rolandi, E.; Guaita, A. The Effect of Information and Communication Technology and Social Networking Site Use on Older People’s Well-Being in Relation to Loneliness: Review of Experimental Studies. J. Med Internet Res. 2021, 23, e23588. [Google Scholar] [CrossRef]
- Berridge, C. Active subjects of passive monitoring: responses to a passive monitoring system in low-income independent living. Ageing Soc. 2015, 37, 537–560. [Google Scholar] [CrossRef] [PubMed]
- Coco, K.; Kangasniemi, M.; Rantanen, T. Care Personnel's Attitudes and Fears Toward Care Robots in Elderly Care: A Comparison of Data from the Care Personnel in Finland and Japan. J. Nurs. Sch. 2018, 50, 634–644. [Google Scholar] [CrossRef] [PubMed]
- Rashid, N.L.A.; Leow, Y.; Klainin-Yobas, P.; Itoh, S.; Wu, V.X. The effectiveness of a therapeutic robot, ‘Paro’, on behavioural and psychological symptoms, medication use, total sleep time and sociability in older adults with dementia: A systematic review and meta-analysis. Int. J. Nurs. Stud. 2023, 145, 104530. [Google Scholar] [CrossRef] [PubMed]
- Oh JH, Yi YJ, Shin CJ, Park C, Kang S, Kim J, et al. [Effects of Silver-Care-Robot Program on Cognitive Function, Depression, and Activities of Daily Living for Institutionalized Elderly People]. J Korean Acad Nurs. 2015 Jun;45(3):388–96.
- Pino, M.; Boulay, M.; Jouen, F.; Rigaud, A.-S. “Are we ready for robots that care for us?” Attitudes and opinions of older adults toward socially assistive robots. Front. Aging Neurosci. 2015, 7, 141. [Google Scholar] [CrossRef]
- Van Patten R, Keller AV, Maye JE, Jeste DV, Depp C, Riek LD, et al. Home-Based Cognitively Assistive Robots: Maximizing Cognitive Functioning and Maintaining Independence in Older Adults Without Dementia. Clin Interv Aging. 2020 Jul 13;15:1129–39.
- Cirillo, D.; Catuara-Solarz, S.; Morey, C.; Guney, E.; Subirats, L.; Mellino, S.; Gigante, A.; Valencia, A.; Rementeria, M.J.; Chadha, A.S.; et al. Sex and gender differences and biases in artificial intelligence for biomedicine and healthcare. npj Digit. Med. 2020, 3, 1–11. [Google Scholar] [CrossRef]
- Gallagher A, Nåden D, Karterud D. Robots in elder care: Some ethical questions. Nurs Ethics. 2016 Jun;23(4):369–71.
Figure 2.
(a) Life expectancy at 65 in Europe. Spain is among the countries with the highest life expectancy in Europe and the world, with the feminisation of population ageing being observed in all European countries. Data obtained from the tables on life expectancy at 65 years of age in the EU, INE Series 2021-2022. (b) Geographical distribution of the population of adults over 65 years of age in Spain in 2023. The Autonomous Communities in the north of the country have the highest proportions of older adults in Spain, exceeding 20% in 2023. In contrast, Ceuta, Melilla and Murcia register the lowest figures. Source: INE. Population Structure Indicators. Results by Autonomous Community. (c) Feminisation of ageing. The higher proportion of women over 65 years of age is higher than that of men in all Spanish Autonomous Communities in 2023, producing the feminisation of ageing.
Figure 2.
(a) Life expectancy at 65 in Europe. Spain is among the countries with the highest life expectancy in Europe and the world, with the feminisation of population ageing being observed in all European countries. Data obtained from the tables on life expectancy at 65 years of age in the EU, INE Series 2021-2022. (b) Geographical distribution of the population of adults over 65 years of age in Spain in 2023. The Autonomous Communities in the north of the country have the highest proportions of older adults in Spain, exceeding 20% in 2023. In contrast, Ceuta, Melilla and Murcia register the lowest figures. Source: INE. Population Structure Indicators. Results by Autonomous Community. (c) Feminisation of ageing. The higher proportion of women over 65 years of age is higher than that of men in all Spanish Autonomous Communities in 2023, producing the feminisation of ageing.
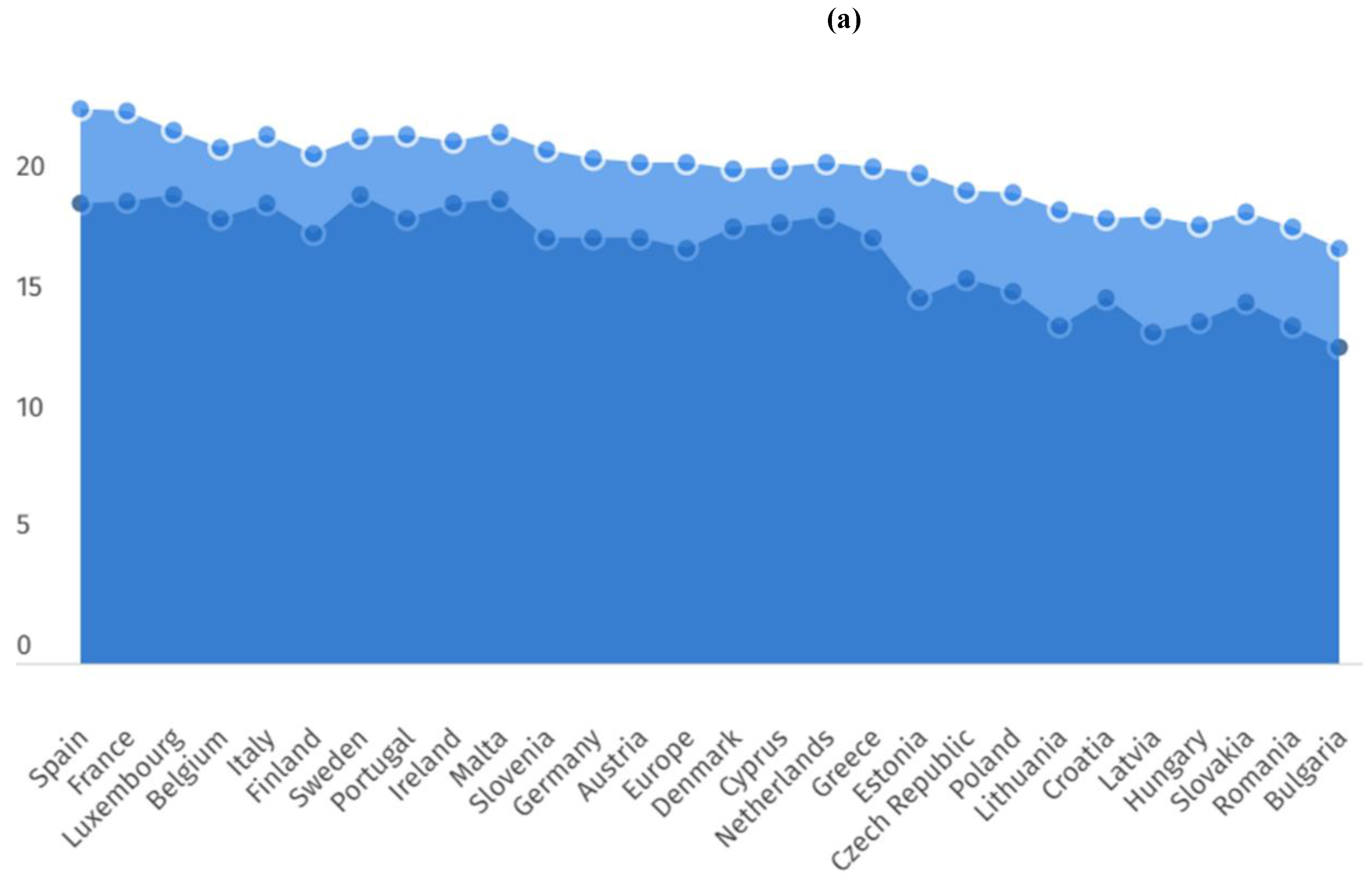
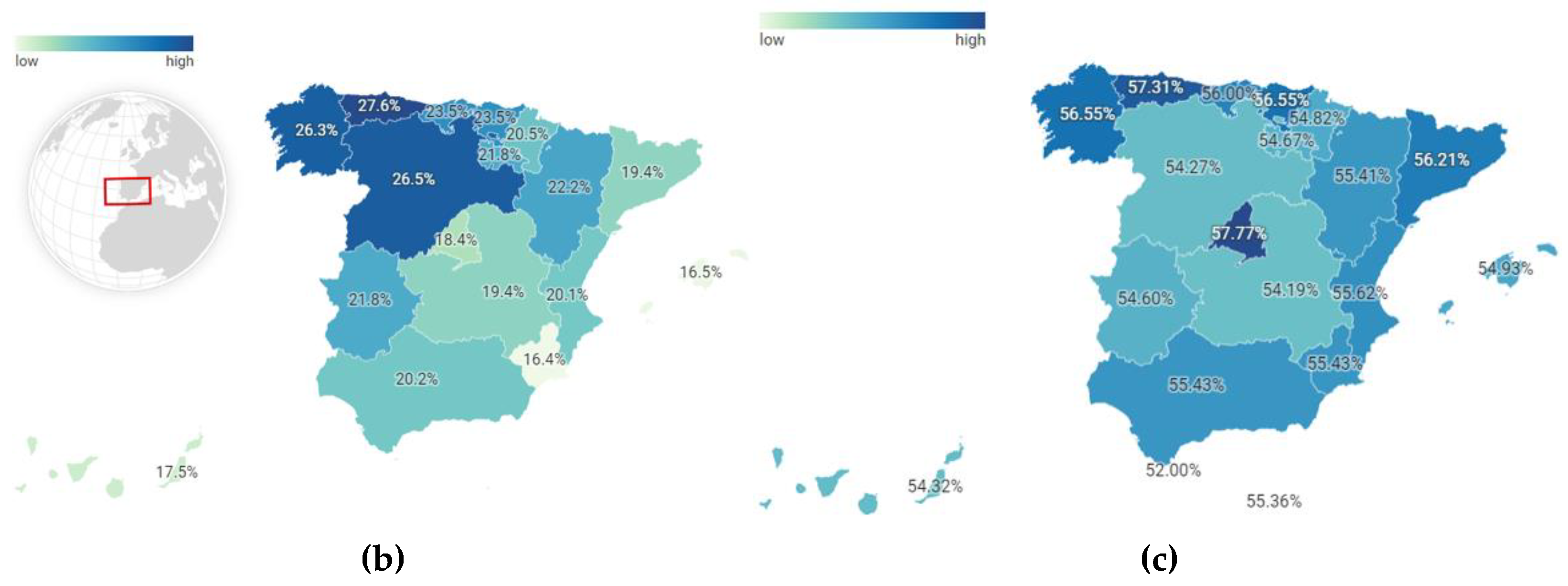
Figure 5.
Essential determinants of active ageing for older adults. To achieve active ageing, older adults must have access to services, employment and volunteering, physical activity, social inclusion and participation, diet and nutrition, long-term care, the environment and its accessibility, education and lifelong learning, including new technologies and the internet. The inequalities to which women have been subjected throughout their lives determine a new inequality in old age, making it difficult to access the tools necessary to achieve active ageing.
Figure 5.
Essential determinants of active ageing for older adults. To achieve active ageing, older adults must have access to services, employment and volunteering, physical activity, social inclusion and participation, diet and nutrition, long-term care, the environment and its accessibility, education and lifelong learning, including new technologies and the internet. The inequalities to which women have been subjected throughout their lives determine a new inequality in old age, making it difficult to access the tools necessary to achieve active ageing.
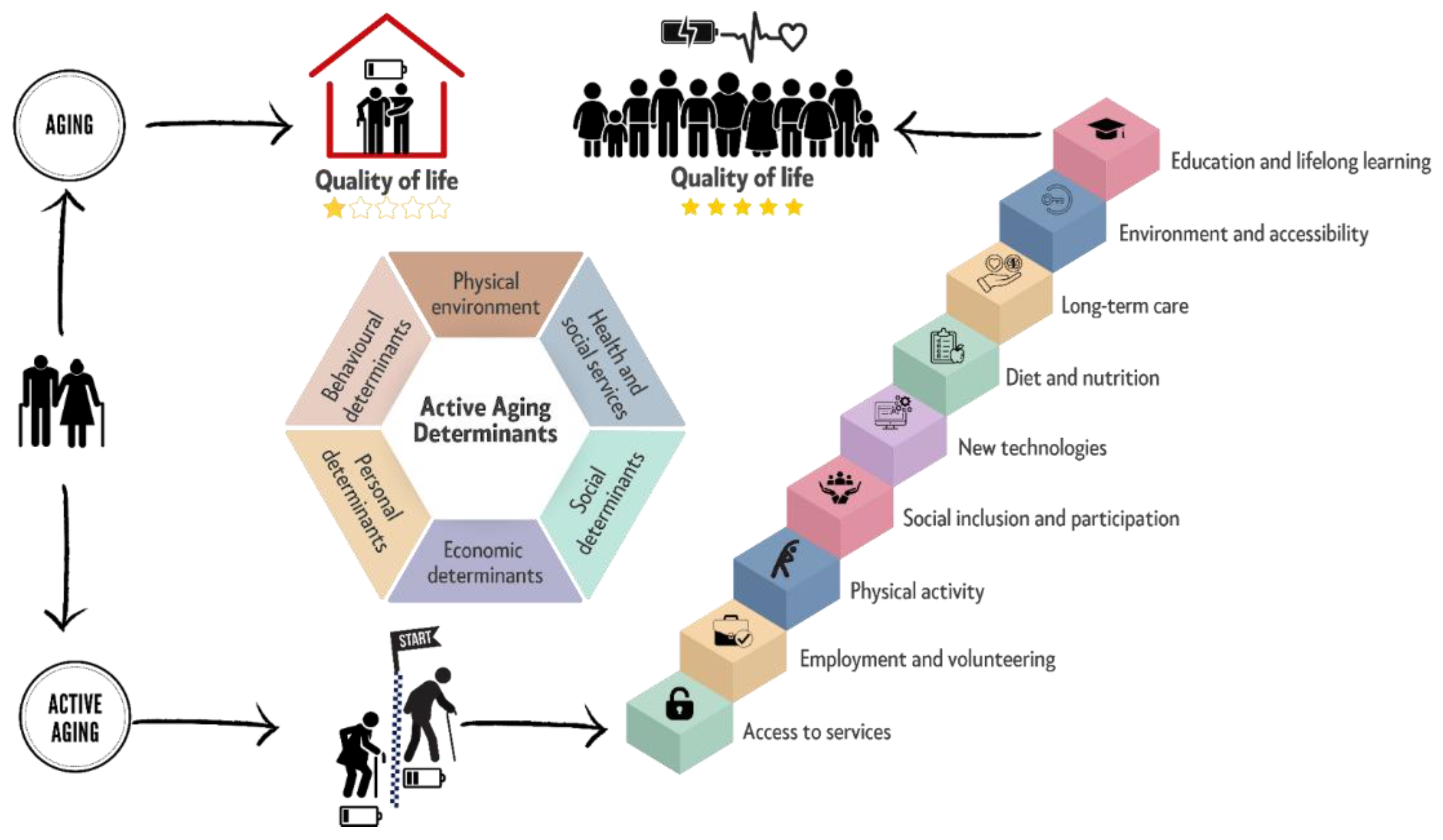
Figure 6.
Process of development of the feeling of loneliness. As a consequence of the discrepancy between the desired level of social contact and the actual level of social contact, a subjective state of involuntary lack of affection and closeness is produced. In cases where the person lacks the necessary tools to cope with the situation of loneliness, it will lead to increasing isolation until it becomes chronic. This situation is particularly serious in the case of older adults (mainly women), who have fewer tools for reconnection, so that, as a result of the situation of loneliness, they end up developing multiple pathologies that increase the risk of mortality.
Figure 6.
Process of development of the feeling of loneliness. As a consequence of the discrepancy between the desired level of social contact and the actual level of social contact, a subjective state of involuntary lack of affection and closeness is produced. In cases where the person lacks the necessary tools to cope with the situation of loneliness, it will lead to increasing isolation until it becomes chronic. This situation is particularly serious in the case of older adults (mainly women), who have fewer tools for reconnection, so that, as a result of the situation of loneliness, they end up developing multiple pathologies that increase the risk of mortality.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



