
Submitted:
20 December 2024
Posted:
23 December 2024
You are already at the latest version
Abstract
Pharmaceutical pollution of surface waters has emerged as a significant environmental health concern worldwide. In this study, we investigated the presence and concentration of pharmaceuticals in aquatic environments within Vhembe District Municipality, South Africa. To achieve this, grab samples of water were collected from various locations across the Thulamela Local Municipality, encompassing rivers, streams, and dams. A targeted solid-phase extraction method with ultra-high-pressure liquid chromatography coupled with quadrupole time-of-flight mass spectrometry (UHPLCQTOF) was used to screen, detect, and quantify 99 pharmaceutical compounds in the collected water samples. The findings revealed the presence of a range of pharmaceutical compounds, including the antiretrovirals nevirapine and lopinavir, the anticonvulsant/anti-epileptic carbamazepine, and the analgesic and antipyretic acetaminophen. The central nervous system stimulant caffeine was also detected in various water bodies across the region. The presence and concentrations of the pharmaceuticals varied across different water bodies, with nevirapine present at nine sites out of 21 (up to 166 ng/L), lopinavir at two sites (up to 42 ng/L), carbamazepine at one site (21 ng/L) and acetaminophen at two sites with the highest concentration of 427 ng/L. Caffeine was present at 15 sites (up to 975 ng/L). This study provides valuable insights into pharmaceutical pollution in surface water resources from one of South Africa's rural areas, Vhembe District Municipality in Limpopo Province.
Keywords:
Water quality
; Emerging contaminants
; Aquatic environments
; Pharmaceutical pollution
; Rural water resources
; Environmental health
; Vhembe district
1. Introduction
South Africa is situated in the southern African subregion, where the human immunodeficiency virus and acquired immunodeficiency syndrome (HIV/AIDS) are most prevalent on the continent. According to the Statistics South Africa 2022 mid-year report, the country has an estimated population of 60.6 million, with the total number of people suffering from HIV infection estimated to be approximately 8.45 million [1]. South Africa has the world's largest antiretroviral (ARV) treatment program, where approximately 5.55 million people were on ARV treatment in 2021 [2]. The Vhembe District Municipality, where the present study was conducted, is part of the Limpopo Province, and it is the northernmost part of the country, sharing a border with Zimbabwe in the north, Botswana in the northwest, and Mozambique in the southeast [3]. Limpopo is the fifth most populated province in South Africa, with a population estimated at 5 941 439 people in 2022; it comes after Gauteng (16 098 571), KwaZulu Natal (11 538 325), Western Cape (7 212 142) and Eastern Cape (6 676 691) [1]. Available data from the fifth South African National HIV Prevalence, Incidence, Behaviour, and Communication Survey conducted in 2017 shows that the HIV/AIDS epidemic prevalence in people aged 15 – 49 years varies from one province to another: the most populated provinces, Gauteng, KwaZulu Natal, and Western Cape, recorded a prevalence of 17.6%, 27% (the highest prevalence) and 12.6% (the lowest prevalence) respectively. The least populated province, the Northern Cape (1 308 734 people), recorded the second-lowest HIV prevalence of 13.9% [4].
There are over 20 ARVs available for HIV treatment worldwide; the most used in South Africa include lamivudine, stavudine, didanosine, zidovudine, tenofovir, lopinavir, abacavir, ritonavir, nevirapine, emtricitabine and efavirenz [5,6]. Most of these ARVs have been detected in aquatic environments in Gauteng, KwaZulu Natal, Western Cape, and Eastern Cape at quantifiable levels, sometimes up to micrograms per litre [7,8,9,10,11,12,13]. However, little is known about ARV concentrations in aquatic environments in other parts of the country, including Vhembe District Municipality in Limpopo Province. Although Limpopo is the fifth most populated province in the country, its HIV prevalence was 17.2% in 2017, which is comparable to the prevalence of HIV in the Gauteng Province (17.6%), the most populated province [4]. The number of HIV patients on ART in Limpopo Province was counted at 296,000 people, while it was 1 248,000 people in KwaZulu Natal and 896,000 in Gauteng [4].
In their study, Robson et al. [14] investigated the presence of the ARV efavirenz in three rivers that feed the Nandoni Dam in the Vhembe District Municipality, the Dzindi, Mvudi and Luvuvhu Rivers. Efavirenz was present in the water from all three rivers at concentrations varying from 1.6 ng/L (Luvuvhu River) to 10.3 ng/L (Mvudi River). This was a once-off sampling conducted in 2016; since then, no other sampling has been conducted to show the situation of pharmaceutical pollution in the region. Since South Africa is the leading country in ART worldwide, it is important to monitor the levels of pharmaceuticals in aquatic environments across the country, as it is done for other chemicals, such as metals and pesticides. This will help implement measures to prevent further water pollution and ensure that future generations have clean water, as highlighted by Goals 6 and 14 of the 2030 United Nations’ Sustainable Development Goals (SDGs) [15].
Pharmaceuticals and other chemical pollutants enter surface water mostly via inefficient pathogen and micropollutant removal from wastewater treatment works (WWTWs) [16,17,18]. Although there is some information on the levels of heavy metals, pesticides, and nutrients in the rivers around the Vhembe District Municipality [19,20,21], there is currently insufficient information on the levels and types of pharmaceuticals in these rivers [14]. As discussed previously, most of the studies on the presence of pharmaceuticals in South African waters have focused on the Gauteng and KwaZulu Natal provinces, where major rivers, dams and WWTWs’ effluents, have shown the presence of diverse types of pharmaceuticals, including ARVs and antibiotics [7,8,9,10,12,13,18,22,23,24]. This is understandable, as KwaZulu Natal is the second most populated province in South Africa after Gauteng and the one with the highest HIV prevalence. In contrast, Limpopo is among the least populated provinces with a lower HIV prevalence [4]. In the Vhembe District, 89.7% of the population lives in rural areas [25]; they mostly use pit latrines and wastewater treatment is mostly done in oxidation ponds [26]. Around Thohoyandou Town, there are currently three public hospitals and nine WWTWs, including a treatment plant, Thohoyandou WWTP (biological process), and eight oxidation ponds. Recently, WWTWs in this area were found to be inefficient in removing chemicals, such as metals and pesticides, mainly because the technology or infrastructure is outdated and sometimes unable to accommodate the excessive amounts of wastewater in the region [26]. Thus, the surface waters in this area receive seepage from pit latrines, oxidation ponds, and solid waste disposal sites [25,26], carrying diverse types of chemicals and their metabolites, including pharmaceuticals.
Recent laboratory studies have shown that some ARVs used in ART in South Africa may affect fish health at their current levels in the Gauteng and KwaZulu Natal surface waters [27,28]. This raises concerns that uncontrolled levels of ARVs in surface water in the Vhembe district could have profound implications not only for the exposed fish and other non-target aquatic organisms but also for water users downstream of the local wastewater treatment plants. Previous studies in this region have shown that local communities sometimes utilise water directly from rivers, streams, and dams [29,30] and are at risk of exposure to ARVs and other pharmaceuticals. The contamination of surface water affects human life and chronically exposes aquatic wildlife species inhabiting these waters [31]. In 2016, efavirenz, an ARV used in South Africa, was detected in the Mvudi River in the Vhembe District, with a 10.3 ng/L concentration [14]. A laboratory exposure study of efavirenz (10.3 ng/L and 20.6 ng/L) showed liver damage and a decline in the health of adult Oreochromis mossambicus [14]. Another study using the same concentrations showed efavirenz’s capacity to cause physical deformities in O. mossambicus larvae at such low concentrations [32]. This is concerning for aquatic life in the rivers of the Vhembe District Municipality, as pharmaceutical levels in water are expected to continue increasing as the country strives to reach the 90-90-90 HIV treatment goals, according to the World Health Organization (WHO) [33].
Another alarming fact is that ARVs are believed to have endocrine-disrupting properties, enabling them to interfere with the normal function of the endocrine system in vertebrates [31,34]. Thus, the presence of ARVs in surface waters may have an additive detrimental effect on other EDCs in the water. Therefore, it is important to monitor the presence, levels, and effects of ARVs in all South African aquatic environments, as it is done for other known EDCs. This study reports on the state of pharmaceutical pollution in Vhembe District Municipality surface waters, where ARVs and other commonly used pharmaceuticals were screened from rivers, streams and dams near the region's main hospitals, clinics, and WWTWs.
2. Materials and Methods
2.1. Study Area and Sampling Sites
In the Vhembe District Municipality, where this study was conducted, water samples were primarily collected in areas with informal settlements within the Nzhelele River catchment, Thulamela Local Municipality, around Thohoyandou town, one of the four towns in the Vhembe District Municipality [25]. The Thulamela Local Municipality (Figure 1) is the most populated in the Vhembe District, with a population of 618 462, which forms 47.7% of the Vhembe District’s population [1].
2.2. Samples Collection, Extraction, and Quantification
Grab water samples were collected using sterilized 1L Schott bottles from different sites covering major rivers, streams, and dams in the Thulamela Local Municipality, focusing on nearby hospitals, clinics, and WWTWs, as shown on the map in Figure 2 and Table 1. The collected water samples were kept in a large cooler box away from sunlight and delivered to the laboratory for analysis on the same day of collection. The samples were then stored for extraction and analysis at -20℃.
Extraction and analysis were conducted at a South African National Accreditation System (SANAS) certified laboratory, Protechnik Laboratories (Pty) Ltd. (ISO/IEC 17025:2017 (T0032)). The targeted solid-phase extraction method used is a slight modification of Ferrer and Thurman's method [35]; it was modified and validated by Wood et al. [22]. Ultra-high-pressure liquid chromatography coupled to quadrupole time-of-flight mass spectrometry (UHPLCQTOF) was used to quantify the pharmaceuticals. In total, 98 pharmaceuticals commonly used in South Africa and caffeine, as listed in Table A1 (Annexure A), were targeted. The instrument’s quantification limits were between 3 ng/L and 10 ng/L. The reference standards (≥ 97% purity) used in this analysis were purchased from Sigma-Aldrich in Johannesburg, South Africa. Dimethyl sulfoxide (DMSO) was used as a solvent for the target compounds at 1 mg/mL and as a dilution for the standard solutions at 10 µg/mL. The prepared solutions were stored at -20℃ until use.
The Ferrer and Thurman [35] extraction method was used with a few modifications: 500 mL of each water sample was filtered through a 1 mm glass-fibre syringe-driven filter before extraction with the Smart Prep Extraction System (Horizon USA). Solid phase extraction (SPE) cartridges (Oasis LB, 6 cc, 500 mg, Waters, Milford, MA, USA) conditioned with 4 mL of methanol and 6 mL of HPLC-grade water were loaded with 500 mL of the filtered sample at a flow rate of 10 mL/min. The SPE cartridges were dried under nitrogen for 3 min and eluted twice with 5 mL of methanol in 500 mL DMSO containing 13C3 caffeine (1 mg/mL). The eluates were then dried under a gentle stream of nitrogen to remove methanol. Samples were extracted at 18 ± 0.5℃) in a dedicated area, and the extracts were stored at - 20℃ until analysis. Figure 3 and Figure 4 below show the calibration curves for caffeine and abacavir used as standards for this study.
To quantify the 98 targeted pharmaceutical compounds and caffeine, ultra-high-pressure liquid chromatography coupled with quadrupole time-of-flight mass spectrometry (UHPLCQTOF) was used. Each extracted sample was injected three times in its mass spectral acquisition mode. The first injection was a full-scan mode-targeted screening, which resulted in the formation of unfragmented pseudo-molecular ions. This was followed by a second injection, untargeted screening, targeting highly abundant ions that were automatically fragmented, generating tandem mass spectra (auto MS/MS). In the third injection, all low-abundance ions missed in the second injection were targeted and fragmented. A fixed collision energy was applied to all detected ions to ensure that all low-abundance ions were fragmented. The full details of the extraction and quantification methods used in this study have been previously described by Wood et al. [22].
2.3. Data Processing and Analysis
The target pharmaceuticals were identified and confirmed using the Agilent Personal Compound Database Library (PCDL) Manager software package. The software is part of the Agilent MassHunter suite for mass spectrometry analysis. Its advanced data mining and processing options allow quick and accurate detection and confirmation of targeted or unknown compounds. The software can combine multiple chemical libraries, which allows quick comparison of the results from chemical screening against a vast collection of chemicals. This study integrated three chemical libraries (METLIN, Veterinary Drugs and Forensics Toxicology libraries) into one compound database to identify and confirm the targeted pharmaceuticals. Results and reports from the analysis produced in CSV files using MassHunter Qual software were processed, sorted, filtered, and presented in Microsoft Excel.
3. Results
Ninety-eight pharmaceuticals and caffeine were targeted during analysis (Table A1), and only six pharmaceuticals and caffeine were detected in the Vhembe District Municipality aquatic environments. These pharmaceuticals represent five classes of the most consumed medicines in the country: ARVs for HIV treatment, anticonvulsant/antiepileptic, analgesic/antipyretic, antibiotics, and antifungals. The presence and concentrations of the detected pharmaceuticals varied across different water bodies, as shown in Table 2. The most prevalent drug was nevirapine, detected at nine sites at the highest concentration of 166 ng/L. Acetaminophen was detected at two sites only, with the highest concentration of 427 ng/L. Caffeine was detected at 15 sampling sites, with 975 ng/L being its highest quantifiable concentration.
The sites that showed the presence of two or more pharmaceuticals were site 1 at the joint of the Nzhelele River and Mutshedzi River, site 7 in the stream below the Siloam Hospital oxidation ponds, site 20 in the Tshikhwikhwikhwi River outflow from the Mutshedzi Dam below the Phadzima Clinic, and site 21 in the Mvudi River below the Thohoyandou WWTW and oxidation ponds (Table 1 and Figure 2).
The site with the most pharmaceuticals was the stream Mutangwi, which passes below the oxidation ponds near the Siloam Hospital (site 7) and flows into the Nzhelele River (Figure 2). Five pharmaceuticals were detected here; these were nevirapine (166 ng/L), lopinavir (42 ng/L), fluconazole (outside the instrument calibration range), sulfamethoxazole (below the instrument LQ), and carbamazepine (21 ng/L) as shown in Table 2. This stream receives effluent from the oxidation ponds via groundwater and possible overflow.
The sampling site in the Mvudi River (site 21) was below the WWTW and oxidation ponds in Thohoyandou (Figure 2). It showed the presence of nevirapine (7 ng/L), clindamycin (below the instrument LQ), carbamazepine (below the instrument LQ), and the highest acetaminophen concentration in this study (427 ng/L). The Mvudi River is one of the tributaries of the Luvuvhu River; its water feeds Nandoni Dam (Figure 2), one of the drinking water sources in Thohoyandou.
The Nzhelele River (site 1), after joining with the Mutshedzi River, also showed levels of nevirapine at 109 ng/L and lopinavir (non-quantifiable, < 10 ng/L). The Nzhelele River is one of the main rivers in Limpopo Province; one of its tributaries is the Mutshedzi River, on which the Mutshedzi Dam is situated. It is worth mentioning that nevirapine was also detected in the Mutshedzi Dam water (site 3 on the map in Figure 2) but under the instrument LQ (10 ng/L). Below the Mutshedzi Dam, in the Tshikhwikhwikhwi River flowing from the dam, near the Phadzima Clinic (site 20), nevirapine, as well as clindamycin, were also detected at non-quantifiable levels. However, at this site, acetaminophen was present at 292 ng/L (Table 2 and Figure 2).
4. Discussion
The present study examined the situation of pharmaceutical pollution since 2019 in the Vhembe District Municipality surface waters, focusing on ARVs, as a previous study conducted in this area in 2016 revealed the presence of the ARV efavirenz in the Mvudi River water in this district with the highest concentration of 10.3 ng/L [14]. Robson et al. [14] studied only three rivers: Mvudi, Dzindi and Luvuvhu. The present study screened for pharmaceuticals in most rivers, streams, and dams in the Thulamela Local Municipality, the most populated area in the Vhembe District Municipality. Among the detected pharmaceuticals, only a few, including the antiretrovirals nevirapine and lopinavir, anticonvulsant/anti-epileptic carbamazepine, and analgesic and antipyretic acetaminophen, were quantifiable at least at one study site. Most of the present study's pharmaceutical compounds and caffeine have previously been detected nationwide but at varying concentrations in different water bodies.
Caffeine was detected at 15 sites, varying from 94 to 975 ng/L concentrations. This was not surprising, as this lifestyle substance is common in different water bodies worldwide, including South Africa [7,8,13,22,31,38]. Studies have shown that the caffeine removal rate is high (up to 86.40%), and the levels in WWTWs’ effluents are much lower than those in influents [8,13]. This implies that caffeine levels in the environment may be a result of direct human pollution from pit latrines, raw sewage, or WWTWs not coping with high loads of wastewater in highly populated areas [18]. Therefore, the levels of caffeine in the Vhembe District Municipality waters are not surprising as previous studies showed that pit latrines are common in this region, and wastewater treatment is mostly done in oxidation ponds, which are inefficient at removing most chemicals [26].
Caffeine is a known central nervous system stimulant which, consumed in high quantities, can have negative effects on cognitive function [39]. Although many studies have reported the presence of caffeine in surface water around the world, there is still insufficient information on its potential effects on non-target aquatic biota. However, only a few studies have investigated the potential effects of caffeine on the environment. One study has shown that caffeine may cause a significant change in the brain and liver phase I biotransformation enzyme ethoxy resorufin-O-demethylase (EROD) activity in fish, Prochilodus lineatus, exposed to up to 30 µ/L of caffeine for 168 hours [40]. Two other studies have shown that caffeine at current concentrations in aquatic environments is not yet a health concern for fish [41,42]. However, at concentrations higher than those in the environment, effects on fish were observed, including impaired reproduction in Ceriodaphnia dubia and inhibited growth in Pimephales promelas exposed to 44 mg/L and 71 mg/L of caffeine for 7 days, respectively [41]. Skeletal deformations and reduced growth were also observed in Neotropical catfish larvae, Rhamdia quelen, exposed to 16 mg/L caffeine for 30 days [42]. Therefore, there is some evidence that increasing caffeine in the world’s aquatic environments may hurt aquatic biota soon; biomonitoring programs and guideline measures are needed for this compound. It is important to note that caffeine has recently been detected in marine water and marine biota (seaweed and invertebrates) on the coast of Camps Bay in Cape Town, South Africa [43]. In Europe, environmental scientists have suggested classifying caffeine as a high-priority emerging environmental pollutant [44,45].
As mentioned above, this study followed Robson et al. [14], who detected the ARV efavirenz in the Mvudi River in Vhembe District Municipality at a low ng/L level. Thus, we expected to find efavirenz in the water samples collected in this area; however, it was surprising that efavirenz was not detected in any of the water samples. Instead, nevirapine not detected by Robson et al. [14] was present at quantifiable levels in the Mvudi River (7 ng/L). Nevirapine was present at 9 of the 30 sites screened in Vhembe District Municipality; its highest concentration was 166 ng/L in a small stream near the Shiloam Hospital oxidation ponds. The presence of nevirapine in Vhembe District Municipality waters confirms what has been previously stated by various studies across the country that this compound is one of the most common pharmaceuticals in the environment [18,22,24,46,47]. A decade ago, Nevirapine was among the first pharmaceuticals detected in South African waters [11]. Since then, it has occurred at varying concentrations in different water bodies. Nevirapine concentration in the present study was lower compared to the concentrations reported from the Roodeplaat Dam and the Hartbeesspruit River in Gauteng Province, where the highest concentrations were 1.48 μg/L [11] and 1.3 μg/L [18] respectively. Both water bodies are situated near major WWTWs in the Province. The Rietvlei Nature Reserve rivers, also in Gauteng, showed the presence of nevirapine up to 227 ng/L [48]. This was the first time nevirapine was reported in the waters of Vhembe District Municipality. Although Wood et al. [22] reported that nevirapine was the most commonly occurring pharmaceutical in South African waters, up to 379 ng/L, rivers in rural areas such as the Thulamela Local Municipality were not investigated. The only previous studies which investigated the presence of pharmaceuticals in the Vhembe District were by Robson et al. [14] in Mvudi, Dzindi and Luvuvhu rivers and Wooding et al. [48] in Albasini Dam, but nevirapine was not detected.
Nevirapine is a non-nucleoside reverse transcriptase inhibitor (NNRTI) ARV, which is mainly used as a first-line treatment for HIV in adults and to prevent the transmission of HIV-1 from pregnant mothers to children [49]. Until recently, NVP was the first choice of first-line ARVs in developing countries because it is affordable and has proven to be efficient in decreasing HIV-related deaths in burdened countries [33]. However, as both nevirapine and efavirenz have been associated with serious undesired effects (such as liver toxicity) in patients with HIV [50,51,52], the WHO has been discouraging their use [6,53]. However, in developing countries, including South Africa, the two ARVs are still used, as they are more affordable than the other ARVs [47,54]. Research on the behaviour of these two pharmaceuticals during South African WWTWs’ processes has shown that these ARVs are partially resistant to the process, and some of their metabolites resulting from the treatment may still be bioactive [16,55,56]. Additionally, many WWTWs nationwide are in poor state and struggle to cope with the heavily loaded influent in highly populated areas [18]. Consequently, efavirenz and nevirapine are still commonly detected in aquatic environments across South Africa [17,18,24,47].
The other ARV detected in the water from the Vhembe District Municipality is lopinavir, which has also been previously detected in different aquatic environments around the country. Abafe et al. [56] previously detected lopinavir (up to 3.8 µg/L) in WWTWs’ inflow and effluent in the eThekwini Municipality in KwaZulu-Natal. However, lopinavir was not detected in the surface water samples in the area. The highest concentration of lopinavir (38.45 µg/L) was detected in the Gauteng Province in the Pienaar River, near a WWTW [18]. The same study also reported different ARVs, including nevirapine and lopinavir, in the Olifantsfontein River System and Gauteng, with a higher total concentration than other river systems in the country. Lopinavir was one of the common pharmaceuticals at the sites investigated by Horn et al. [18] in the Gauteng Province with a frequency of 77%. Previously, Wood et al. [22], in their national screening of pharmaceuticals in South African waters, also detected lopinavir at most of the investigated sites (36 occurrences) with the highest concentration of 859 ng/L. However, it is important to note that the screening of the above two studies mainly focused on the Roodeplaat Dam system and included only major rivers and dams around the country.
Lopinavir is a protease inhibitor ARV, mainly prescribed in combination with ritonavir, another ARV protease inhibitor, to increase its bioavailability for the treatment of HIV [57]. Recently, during the coronavirus disease 2019 (COVID-19) pandemic, lopinavir and ritonavir were among the many other drugs used to treat the virus [58]. This may explain the detection of lopinavir in WWTWs’ effluent and, consequently, its detection in water bodies around WWTWs and hospitals/clinics, as discussed above. In addition, the classic wastewater treatment technique, activated charcoal, used in South Africa, is inefficient in removing many of the ARVs, including lopinavir, from WWTWs’ influent [16,18,55]. Czech et al. [57] investigated the potential effects of lopinavir’s predicted no-effect concentration (PNEC) in ng/L in aquatic animals and revealed a possible high chronic toxicity.
As discussed previously, nevirapine is known to cause liver injury in humans [50,51,52]. In contrast, lopinavir combined with ritonavir has been suspected to contribute to inhibiting endothelial cell function and cardiovascular complications in patients receiving ARV treatment [59,60]. In aquatic environments, some ARVs have also shown the potential to harm non-target aquatic animals, such as fish. Recent results from a few laboratories experimental studies have shown that the NNRTI ARVs nevirapine and efavirenz can cause physical deformities in larval stages and liver toxicity in Oreochromis mossambicus at environmental concentrations [14,28,32]. There is no information on the potential effects of protease inhibitors ARVs such as lopinavir on fish. Although ARVs occur at lower concentrations (ng/L) in Vhembe district waters, in other parts of the country, such as Gauteng Province, the concentrations are higher and increasing as more people are put on ARV treatment. This means that in the waters of Vhembe District Municipality, the occurrence and concentrations of ARVs and other commonly consumed pharmaceuticals will also continue to increase. Therefore, as previously recommended by various studies, there is a need to monitor human pharmaceutical occurrences in WWTWs’ effluents and surface waters around the country.
This study detected the analgesic and antipyretic acetaminophen/paracetamol with the highest concentrations at two sites in the Tshikhwikhwikhwi and Mvudi Rivers. The Tshikhwikhwikhwi River is situated in the vicinity of a clinic, the Phazima Clinic, and there is also a WWTW nearby. In contrast, the Mvudi River is near the Thohoyandou WWTW and Thohoyandou oxidation ponds, as shown on the map in Fig. 2. Acetaminophen is one of the over-the-counter drugs which are overused globally, resulting in its occurrence in aquatic environments around the world [24,45]. In South Africa, previous studies have shown the presence of acetaminophen in different water bodies around the country at varying concentrations. Acetaminophen was detected in the Umgeni and Msunduzi rivers in Kwa-Zulu Natal Province up to 58700 ng/L [9,61]. It was also detected in the Eerste River in Western Cape [13], in the ocean water (0.09 – 0.10 ng/L), and in invertebrates and seaweed collected at the coast of Cape Town [43]. Acetaminophen was also detected in drinking water in some parts of the world, including South Africa [45,62]. The ubiquitous presence of this compound in waters around the world can be explained by its easy accessibility as an over-the-counter medication, resulting in overuse and poor removal from wastewater at WWTWs [45,63,64].
Acetaminophen current concentrations in the environment are believed to be safe for humans [65]; however, little is known about how this drug may affect aquatic biota. Madikizela et al. [66] were able to quantify and determine the hazard quotient of acetaminophen in the Klip River in Gauteng Province at 0.432 µg/L. They showed that at this concentration, which is a little bit higher than the concentrations detected in water from Vhembe District in the present study, the acetaminophen hazard quotient was < 1. This means that there are no health concerns for aquatic biota at this concentration in Vhembe District Municipality waters. However, as acetaminophen's predicted no-effect concentration (PNEC) is estimated at 9200 ng/L [67], there is already a problem in South African waters as concentrations are increasing. In the Umgeni and Msunduzi rivers in KwaZulu Natal, concentrations are above the PNEC [61,67]. Developed countries have proposed guidelines on the acceptable levels of acetaminophen in drinking water; for example, in Europe, the suggested acceptable level of acetaminophen in drinking water is < 71 µg/L and in the US, in Minnesota State, it is ≤ 200 µg/L [63,68]. It is time that South Africa and other African countries also take steps to protect our aquatic environments by establishing guidelines for emerging pollutants of concern, such as acetaminophen.
The anticonvulsant/anti-epileptic carbamazepine was detected at three sites but was only quantifiable at one site, in a small stream below the Siloam Hospital oxidation ponds, at low ng/L levels. Many studies worldwide have shown that carbamazepine’s occurrence in aquatic environments is becoming common [45]. In South Africa, carbamazepine had been previously detected in surface water in Umgeni River water in Kwa-Zulu Natal up to 1.65 µ/L [9], in Hartbeespoort Dam water up to 95 ng/L and the Jukskei River up to 74 ng/L both in Gauteng Province [69]; in Western Cape waters [13] and in the Swartkops River in Eastern Cape from 36576.2 ng/L [12]. Carbamazepine was also detected in seawater at the coast of Cape Town up to 0.14 ng/L [43]. This shows that carbamazepine is present in surface water around the country, including in Vhembe District Municipality. Its occurrence may increase in the future as its consumption increases.
The common detection of carbamazepine in rivers worldwide may be explained by its resistance to WWTWs’ treatment with a low removal rate of 10% [12,70,71]. However, there is good news as a recent study in South Africa using a water-soluble protein extracted from a plant (Moringa stenopetala) has shown a high removal rate of carbamazepine from wastewater (80 – 86%); this is a potential opportunity that needs to be investigated further to reduce this drug from wastewater [72].
Carbamazepine's presence in surface water is a concern as it can interfere with human thyroid hormones' function [73,74]. Thyroid hormones in teleost fish regulate physiological processes, including reproduction and development [75]. Thus, carbamazepine in surface water may be a health risk to fish health. A few studies have shown that this compound may harm aquatic life. A study by Fraz et al. [76] exposed zebra fish adults to 10 µg/L of carbamazepine in a chronic exposure (6 weeks); the results showed effects on reproduction not only in the exposed adult fish but also in the offspring up to the F4 generation. This is overly concerning and shows that carbamazepine effects in South African aquatic environments should be investigated further, as the concentrations observed in some parts of the country are > 1 µg/L.
The other detected pharmaceuticals worth mentioning are the antibiotics clindamycin and sulfamethoxazole. Clindamycin was detected at two sites together with nevirapine, acetaminophen and carbamazepine, while sulfamethoxazole was detected only at one site, but both drugs were not quantifiable. Sulfamethoxazole is one of the most commonly detected antibiotics in surface water worldwide and one of the widely investigated pharmaceuticals in aquatic environments [24,45,77]. Although it was under the LOQ in the present study, sulfamethoxazole has been previously detected and quantified in water bodies around the country since a decade ago. In KwaZulu Natal, sulfamethoxazole was found in the Umgeni and Msunduzi Rivers at concentrations varying from 3.68 µg/L to 6.01 µg/L [7,8,9]. In their national screening of pharmaceuticals in South African surface waters, Wood et al. [22] reported that sulfamethoxazole was one of the most common drugs in waters across South Africa at a concentration of up to 252 ng/L. As mentioned, this screening focused more on the Roodeplaat Dam System in Gauteng Province. In the Eastern Cape, sulfamethoxazole was found in river water up to 6968 ng/L [12]. It was also among the pharmaceuticals detected in Cape Town’s seawater and aquatic biota (invertebrates and seaweed) tissues [43].
Sulfamethoxazole is one of the medications prescribed to HIV patients for the prevention of opportunistic infections such as TB [78]; thus, in African surface waters, it commonly occurs alongside ARVs at high levels compared to elsewhere in the world as its occurrence in each region mirrors its consumption [24,45]. Previous studies have shown that sulfamethoxazole is not entirely removed by the activated sludge process mainly used in different WWTWs in South Africa; this may explain why it occurs at higher levels in surface water across the country [13,48,55].
Sulfamethoxazole effects on aquatic biota have been investigated, and available information shows that in a mixture of other xenobiotic compounds in water, sulfamethoxazole may affect fish through the hypothalamic-pituitary-thyroid axis [79]. This can negatively affect gametogenesis, gonad development, ovulation and egg fertilisation rate [75]. Madureira et al. [80] exposed male and female zebrafish to a mixture of pharmaceuticals, including sulfamethoxazole, at their environmental concentrations, and a decrease in mature gametes in both male and female fish were observed. Nibamureke et al. [27] investigated the effects of a mixture of sulfamethoxazole, trimethoprim and nevirapine on adult fish, Oreochromis mossambicus, in a laboratory chronic exposure. The environmentally relevant concentration detected in the Umgeni River in KwaZulu Natal, 3.68 µg/L, was used. The adult female fish exposed to the mixture showed significant histopathological changes in the gonads. Thus, sulfamethoxazole levels in South African surface waters should be monitored, and WWTWs around the country need to be upgraded to cope with the high load of pollutants that are emerging concerns [62].
Contrary to sulfamethoxazole, the antibiotic clindamycin had never been detected in South Africa's surface water. Wood et al. [22] previously conducted a nationally targeted and non-targeted screen of pharmaceutical compounds in South African waters, but clindamycin was not detected at any of the investigated sites. However, the study did not cover small streams and rivers in rural Limpopo Province that were covered in the present study, which may explain why clindamycin had not been detected before. This shows that pollutant monitoring in aquatic environments in developing countries should not leave out rural areas as these often lack proper wastewater treatment works. Consequently, these areas experience direct upload of pollutants into local small streams and rivers from households, pit latrines, waste dumping sites or seepage from malfunctioning local WWTWs such as oxidation ponds [26,61].
Although clindamycin is only available on a doctor’s prescription, it is one of the commonly used and prescribed antibiotics designed to treat various infections, such as septicaemia, Gram-positive infections and anaerobic infections. Clindamycin possesses both bacteriostatic and bactericidal properties depending on the concentration and the site of infection [81]. After oral administration, clindamycin is metabolised in the liver and its concentration peaks in blood plasma within 60 minutes. With a half-life of three hours, Clindamycin is excreted mainly through the urine as a mixture of active and inactive metabolites [81]. Clindamycin was previously detected in aquatic environments in Germany, and it is believed to be resistant to WWTWs’ removal process, which may explain its presence in the environment [77]. Given that this was the first time this drug was detected in South African waters and was present only at two sites, more studies are needed to investigate its occurrence and potential effects in South African aquatic environments.
In general, all the pharmaceuticals reported in the present study, except for clindamycin, have been previously reported in different water bodies around the country and at higher concentrations compared to this study. As these pharmaceuticals were detected in surface waters near hospitals, clinics and WWTWs/oxidation ponds, there is a need for improved waste management practices at hospitals/clinics as well as maintenance of existing WWTWs/ oxidation ponds in Vhembe District Municipality to reduce the upload of pharmaceutical waste into rivers and streams. Public awareness programs to educate the population on the best practices for disposing of unused pharmaceuticals are also needed to mitigate pharmaceutical pollution effectively. Lastly, continued monitoring of pharmaceutical pollution and research are also essential to understanding the long-term potential effects of these emerging contaminants on the environment. The environmental presence of some of these pharmaceuticals, including acetaminophen, sulfamethoxazole and carbamazepine, is believed to be a health risk around the world [45]. In developed countries, it has been suggested that these three pharmaceuticals be added to the ‘watch list’ for pollutants of emerging concern in the environment [63,68,82].
5. Conclusions
Pharmaceutical pollution in South African aquatic environments is a reality that needs to be addressed by all stakeholders. This study contributes valuable insights into pharmaceutical pollution in Vhembe District Municipality waters. Pharmaceuticals such as the ARVs nevirapine and lopinavir, the anticonvulsant/anti-epileptic carbamazepine, as well as the analgesic and antipyretic acetaminophen detected in the Vhembe District Municipality waters are a potential threat to the health of aquatic animals and humans in the area. Thus, continued monitoring of pharmaceutical pollution in aquatic environments around the country and research is essential to understanding the long-term potential effects of these emerging contaminants on the environment. This study shows that small rivers and streams in rural areas should be included in studies investigating the occurrence, fate, and effects of pollutants of emerging concern in the country.
Supplementary Materials
The following supporting information can be downloaded at the website of this paper posted on Preprints.org, Figure S1: Map of sampling sites; Table S1: Water Analysis Results.
Author Contributions
Conceptualization, Irene Barnhoorn; Data curation, Uwineza Marie Clémentine Nibamureke; Formal analysis, Uwineza Marie Clémentine Nibamureke; Funding acquisition, Irene Barnhoorn; Investigation, Uwineza Marie Clémentine Nibamureke; Methodology, Irene Barnhoorn; Project administration, Irene Barnhoorn; Resources, Irene Barnhoorn; Software, Uwineza Marie Clémentine Nibamureke and Irene Barnhoorn; Supervision, Irene Barnhoorn; Visualization, Uwineza Marie Clémentine Nibamureke; Writing – original draft, Uwineza Marie Clémentine Nibamureke; Writing – review & editing, Uwineza Marie Clémentine Nibamureke and Irene Barnhoorn. Both authors approved the published version of the manuscript.
Funding
This research was funded by the University of Venda Research and Publication Funds (Project number: RPC SMNS/17/ZOO/03) and the National Research Foundation (NRF) Postdoctoral Grant to U.M.C. Nibamureke (Grant Number: PSTD230504102593).
Data Availability Statement
The necessary data and Supplementary Materials have been included in the manuscript. Any other information needed will be provided on request.
Acknowledgements
The authors want to acknowledge Dr. Timoty Wood's help with water analyses at Protechnik Laboratories, Pretoria, South Africa.
Conflicts of Interest
The authors declare no conflicts of interest. The funders had no role in the study's design, in the collection, analyses, or interpretation of data, in the writing of the manuscript, or in the decision to publish the results.
Appendix A

Table A1.
List of pharmaceuticals/compounds tested in this study.
| Compound name |
|---|
| 1. Lamivudine |
| 2. Method pyrazinamide |
| 3. Chlorothiazide |
| 4. Theophylline |
| 5. Chloroquine phosphate |
| 6. Azathioprine |
| 7. Methotrexate |
| 8. Amoxicillin |
| 9. Metoprolol |
| 10. Tartrate |
| 11. Methocarbamol |
| 12. Methylparaben (Methyl parahydroxybenzoate) |
| 13. Erythromycin |
| 14. Prednisone |
| 15. Benzylpenicillin |
| 16. Fluoxetine |
| 17. Hydrochloride |
| 18. Ketoprofen |
| 19. Valsartan |
| 20. Cholecalciferol |
| 21. Taurine |
| 22. Zalcitabine |
| 23. Emtricitabine |
| 24. Famotidine |
| 25. Abacavir |
| 26. Cyclosporin A |
| 27. Cefotaxime |
| 28. Oseltamivir |
| 29. Chloramphenicol |
| 30. Diphenhydramine |
| 31. Hydrochloride |
| 32. Chlorhexidine |
| 33. Prednisolone |
| 34. Clarithromycin |
| 35. Cloxacillin |
| 36. Naproxen |
| 37. Diclofenac sodium salt |
| 38. Lovastatin |
| 39. Metformin |
| 40. Hydrochloride |
| 41. Tenofovir |
| 42. Ethionamide |
| 43. Hydrochlorothiazide |
| 44. Lidocaine |
| 45. Doxycycline hyclate |
| 46. Lamotrigine |
| 47. Guaifenesin |
| 48. Azithromycin |
| 49. Labetalol |
| 50. Hydrochloride |
| 51. Dextromethorphan hydrobromide monohydrate |
| 52. Indinavir |
| 53. Lansoprazole |
| 54. Ketoconazole |
| 55. Clotrimazole |
| 56. Praziquantel |
| 57. Gemfibrozil |
| 58. Isoniazid |
| 59. Metronidazole |
| 60. Cimetidine |
| 61. Ranitidine |
| 62. Hydrochloride |
| 63. Didanosine |
| 64. Stavudine |
| 65. Trimethoprim |
| 66. Ofloxacin |
| 67. Metoclopramide |
| 68. Hydrochloride |
| 69. Chlorpheniramine maleate |
| 70. Omeprazole |
| 71. Nevirapine |
| 72. Enalapril |
| 73. Maleate |
| 74. Carvedilol |
| 75. Tetracycline |
| 76. Hydrochloride |
| 77. Loperamide |
| 78. Rifampicin |
| 79. Lopinavir |
| 80. Gentamicin |
| 81. Ethambutol |
| 82. Acyclovir |
| 83. Acetaminophen |
| 84. Gabapentin |
| 85. Zidovudine |
| 86. Aspartame |
| 87. Fluconazole |
| 88. Sulfamethoxazole |
| 89. Clindamycin |
| 90. Hydrocortisone |
| 91. Carbamazepine |
| 92. Loratadine |
| 93. Chlorpropamide |
| 94. Flucloxacillin |
| 95. Indomethacin |
| 96. Atorvastatin |
| 97. Ritonavir |
| 98. Efavirenz |
| 99. Caffeine |
References
- Statistics South Africa (Stats SA) Statistical Release P0302: Mid-Year Population Estimates 2022. Department: Statistics South Africa 2022; https://www.statssa.gov.za/publications/P0302/P03022022.pdf (accessed September 30, 2024).
- UNAIDS (The Joint United Nations Programme on HIV/AIDS) UNAIDS Data 2022. Available online: https://www.unaids.org/en/resources/documents/2023/2022_unaids_data (accessed on 30 September 2024).
- Department of Cooperative Governance and Traditional Affairs PROFILE: VHEMBE DISTRICT MUNICIPALITY 2; 2020; https://www.cogta.gov.za/ddm/wp-content/uploads/2020/11/vhembeoctober-2020.pdf.
- Simbayi, L.C.; Zuma, K.; Zungu, N.; et al. South African National HIV Prevalence, Incidence, Behaviour and Communication Survey, 2017. Available online: https://repository.hsrc.ac.za/handle/20.500.11910/13760 (accessed on 26 August 2022).
- Venter, W.D.F.; Kaiser, B.; Pillay, Y.; Conradie, F.; Gomez, G.B.; Clayden, P.; Matsolo, M.; Amole, C.; Rutter, L.; Abdullah, F.; et al. Cutting the Cost of South African Antiretroviral Therapy Using Newer, Safer Drugs. South African Medical Journal 2016, 107, 28–30. [Google Scholar] [CrossRef]
- World Health Organization Consolidated Guidelines on HIV Prevention, Testing, Service Delivery and Monitoring: Recommendations for a Public Health Approach. World Health Organization 2021, 592.
- Agunbiade, F.O.; Moodley, B. Pharmaceuticals as Emerging Organic Contaminants in Umgeni River Water System, KwaZulu-Natal, South Africa. Environ Monit Assess 2014, 186, 7273–7291. [Google Scholar] [CrossRef]
- Matongo, S.; Birungi, G.; Moodley, B.; Ndungu, P. Pharmaceutical Residues in Water and Sediment of Msunduzi River, KwaZulu-Natal, South Africa. Chemosphere 2015, 134, 133–140. [Google Scholar] [CrossRef]
- Matongo, S.; Birungi, G.; Moodley, B.; Ndungu, P. Occurrence of Selected Pharmaceuticals in Water and Sediment of Umgeni River, KwaZulu-Natal, South Africa. Environmental Science and Pollution Research 2015, 22, 10298–10308. [Google Scholar] [CrossRef]
- Schoeman, C.; Mashiane, M.; Dlamini, M.; Okonkwo, O. Quantification of Selected Antiretroviral Drugs in a Wastewater Treatment Works in South Africa Using GC-TOFMS. J. Chromatogr. Sep. Tech. 2015, 6, 272. [Google Scholar] [CrossRef]
- Wood, T.P.; Duvenage, C.S.J.; Rohwer, E. The Occurrence of Anti-Retroviral Compounds Used for HIV Treatment in South African Surface Water. Environ Pollut 2015, 199, 235–243. [Google Scholar] [CrossRef]
- Vumazonke, S.; Khamanga, S.M.; Ngqwala, N.P. Detection of Pharmaceutical Residues in Surface Waters of the Eastern Cape Province. International Journal of Environmental Research and Public Health 2020, Vol. 17, Page 4067 2020, 17, 4067. [Google Scholar] [CrossRef]
- Archer, E.; Holton, E.; Fidal, J.; Kasprzyk-Hordern, B.; Carstens, A.; Brocker, L.; Kjeldsen, T.R.; Wolfaardt, G.M. Occurrence of Contaminants of Emerging Concern in the Eerste River, South Africa: Towards the Optimisation of an Urban Water Profiling Approach for Public- and Ecological Health Risk Characterisation. Science of The Total Environment 2023, 859, 160254. [Google Scholar] [CrossRef]
- Robson, L.; Barnhoorn, I.E.J.; Wagenaar, G.M. The Potential Effects of Efavirenz on Oreochromis Mossambicus after Acute Exposure. Environ Toxicol Pharmacol 2017, 56, 225–232. [Google Scholar] [CrossRef]
- United Nations The Future Is Now: Science for Achieving Sustainable Development (GSDR 2019) | Department of Economic and Social Affairs. Available online: https://sdgs.un.org/publications/future-now-science-achieving-sustainable-development-gsdr-2019-24576 (accessed on 26 September 2023).
- Wood, T.P.; Basson, A.E.; Duvenage, C.; Rohwer, E.R. The Chlorination Behaviour and Environmental Fate of the Antiretroviral Drug Nevirapine in South African Surface Water. Water Res 2016, 104, 349–360. [Google Scholar] [CrossRef]
- Archer, E.; Petrie, B.; Kasprzyk-Hordern, B.; Wolfaardt, G.M. The Fate of Pharmaceuticals and Personal Care Products (PPCPs), Endocrine Disrupting Contaminants (EDCs), Metabolites and Illicit Drugs in a WWTW and Environmental Waters. Chemosphere 2017, 174, 437–446. [Google Scholar] [CrossRef]
- Horn, S.; Vogt, T.; Gerber, E.; Vogt, B.; Bouwman, H.; Pieters, R. HIV-Antiretrovirals in River Water from Gauteng, South Africa: Mixed Messages of Wastewater Inflows as Source. Science of The Total Environment 2022, 806, 150346. [Google Scholar] [CrossRef]
- Edokpayi, J.N.; Odiyo, J.O.; Popoola, O.E.; Msagati, T.A.M. Assessment of Trace Metals Contamination of Surface Water and Sediment: A Case Study of Mvudi River, South Africa. Sustainability 2016, Vol. 8, Page 135 2016, 8, 135. [Google Scholar] [CrossRef]
- Nibamureke, U.M.C.; Barnhoorn, I.E.J.; Wagenaar, G.M. Health Assessment of Freshwater Fish Species from Albasini Dam, Outside a DDT-Sprayed Area in Limpopo Province, South Africa: A Preliminary Study. Afr J Aquat Sci 2016, 41, 297–308. [Google Scholar] [CrossRef]
- Seshoka, M.F.; van Zijl, M.C.; Aneck-Hahn, N.H.; Barnhoorn, I.E.J. Endocrine-Disrupting Activity of the Fungicide Mancozeb Used in the Vhembe District of South Africa. Afr J Aquat Sci 2021, 46, 100–109. [Google Scholar] [CrossRef]
- Wood, T.P.; Du Preez, C.; Steenkamp, A.; Duvenage, C.; Rohwer, E.R. Database-Driven Screening of South African Surface Water and the Targeted Detection of Pharmaceuticals Using Liquid Chromatography - High Resolution Mass Spectrometry. Environmental Pollution 2017, 230, 453–462. [Google Scholar] [CrossRef]
- Rimayi, C.; Chimuka, L.; Gravell, A.; Fones, G.R.; Mills, G.A. Use of the Chemcatcher® Passive Sampler and Time-of-Flight Mass Spectrometry to Screen for Emerging Pollutants in Rivers in Gauteng Province of South Africa. Environ Monit Assess 2019, 191, 1–20. [Google Scholar] [CrossRef]
- Madikizela, L.M.; Ncube, S.; Chimuka, L. Analysis, Occurrence and Removal of Pharmaceuticals in African Water Resources: A Current Status. J Environ Manage 2020, 253, 109741. [Google Scholar] [CrossRef]
- Department of Water and Sanitation (DWS) Water and Sanitation on Growing Economy in Limpopo | South African Government. Available online: https://www.gov.za/news/media-statements/water-and-sanitation-growing-economy-limpopo-14-mar-2022 (accessed on 30 August 2024).
- Edokpayi, J.N.; Odiyo, J.O.; Popoola, O.E.; Msagati, T.A.M. Evaluation of Contaminants Removal by Waste Stabilization Ponds: A Case Study of Siloam WSPs in Vhembe District, South Africa. Heliyon 2021, 7, e06207. [Google Scholar] [CrossRef]
- Nibamureke, U.M.C.; Wagenaar, G.M. Histopathological Changes in Oreochromis Mossambicus (Peters, 1852) Ovaries after a Chronic Exposure to a Mixture of the HIV Drug Nevirapine and the Antibiotics Sulfamethoxazole and Trimethoprim. Chemosphere 2021, 274. [Google Scholar] [CrossRef]
- Nibamureke, U.M.C.; Barnhoorn, I.E.J.; Wagenaar, G.M. Nevirapine in African Surface Waters Induces Liver Histopathology in Oreochromis Mossambicus: A Laboratory Exposure Study. Afr J Aquat Sci 2019, 44, 77–88. [Google Scholar] [CrossRef]
- Fouché, P.; Vlok, W.; Roos, J.; Luus-Powell, W.; Jooste, A. Establishing the Fishery Potential of Lake Nandoni in the Luvuvhu River, Limpopo Province Report to the WATER RESEARCH COMMISSION; 2013.
- Traoré, A.N.; Mulaudzi, K.; Chari, G.J.E.; Foord, S.H.; Mudau, L.S.; Barnard, T.G.; Potgieter, N. The Impact of Human Activities on Microbial Quality of Rivers in the Vhembe District, South Africa. Int J Environ Res Public Health 2016, 13. [Google Scholar] [CrossRef]
- Archer, E.; Wolfaardt, G.M.; van Wyk, J.H. Pharmaceutical and Personal Care Products (PPCPs) as Endocrine Disrupting Contaminants (EDCs) in South African Surface Waters. Water SA 2017, 43, 684–706. [Google Scholar] [CrossRef]
- Kowlaser, S.; Barnhoorn, I.; Wagenaar, I. Developmental Abnormalities and Growth Patterns in Juvenile Oreochromis Mossambicus Chronically Exposed to Efavirenz. Emerg Contam 2022, 8, 83–89. [Google Scholar] [CrossRef]
- WHO (World Health Organization) HIV Treatment and Care: WHO HIV Policy Adoption and Implementation Status in Countries: Factsheet. Available online: https://iris.who.int/handle/10665/326035 (accessed on 24 June 2024).
- Jeannot, R.; Sabik, H.; Sauvard, E.; Dagnac, T.; Dohrendorf, K. Determination of Endocrine-Disrupting Compounds in Environmental Samples Using Gas and Liquid Chromatography with Mass Spectrometry. J Chromatogr A 2002, 974, 143–159. [Google Scholar] [CrossRef]
- Ferrer, I.; Thurman, E.M. Analysis of 100 Pharmaceuticals and Their Degradates in Water Samples by Liquid Chromatography/Quadrupole Time-of-Flight Mass Spectrometry. J Chromatogr A 2012, 1259, 148–157. [Google Scholar] [CrossRef]
- Encyclopedia Britannica Limpopo | Wildlife, Parks & Nature Reserves | Britannica. Available online: https://www.britannica.com/place/Limpopo (accessed on 30 September 2024).
- The Local Government Handbook: South Africa Municipalities of South Africa: Limpopo Municipalities. Available online: https://municipalities.co.za/provinces/view/5/limpopo (accessed on 26 August 2024).
- Styszko, K.; Proctor, K.; Castrignanò, E.; Kasprzyk-Hordern, B. Occurrence of Pharmaceutical Residues, Personal Care Products, Lifestyle Chemicals, Illicit Drugs and Metabolites in Wastewater and Receiving Surface Waters of Krakow Agglomeration in South Poland. Sci Total Environ 2021, 768. [Google Scholar] [CrossRef]
- Fiani, B.; Zhu, L.; Musch, B.L.; Briceno, S.; Andel, R.; Sadeq, N.; Ansari, A.Z.; Fiani, B.; Zhu, L.; Musch, B.L.; et al. The Neurophysiology of Caffeine as a Central Nervous System Stimulant and the Resultant Effects on Cognitive Function. Cureus 2021, 13. [Google Scholar] [CrossRef]
- Santos-Silva, T.G.; Montagner, C.C.; Martinez, C.B.R. Evaluation of Caffeine Effects on Biochemical and Genotoxic Biomarkers in the Neotropical Freshwater Teleost Prochilodus Lineatus. Environ Toxicol Pharmacol 2018, 58, 237–242. [Google Scholar] [CrossRef]
- Moore, M.T.; Greenway, S.L.; Farris, J.L.; Guerra, B. Assessing Caffeine as an Emerging Environmental Concern Using Conventional Approaches. Arch Environ Contam Toxicol 2008, 54, 31–35. [Google Scholar] [CrossRef] [PubMed]
- dos Santos, J.A.; Quadra, G.R.; Almeida, R.M.; Soranço, L.; Lobo, H.; Rocha, V.N.; Bialetzki, A.; Reis, J.L.; Roland, F.; Barros, N. Sublethal Effects of Environmental Concentrations of Caffeine on a Neotropical Freshwater Fish. Ecotoxicology 2022, 31, 161–167. [Google Scholar] [CrossRef] [PubMed]
- Ojemaye, C.Y.; Pampanin, D.M.; Sydnes, M.O.; Green, L.; Petrik, L. The Burden of Emerging Contaminants upon an Atlantic Ocean Marine Protected Reserve Adjacent to Camps Bay, Cape Town, South Africa. Heliyon 2022, 8, e12625. [Google Scholar] [CrossRef]
- Vieira, L.R.; Soares, A.M.V.M.; Freitas, R. Caffeine as a Contaminant of Concern: A Review on Concentrations and Impacts in Marine Coastal Systems. Chemosphere 2022, 286, 131675. [Google Scholar] [CrossRef] [PubMed]
- Wilkinson, J.L.; Boxall, A.B.A.; Kolpin, D.W.; Leung, K.M.Y.; Lai, R.W.S.; Galban-Malag, C.; Adell, A.D.; Mondon, J.; Metian, M.; Marchant, R.A.; et al. Pharmaceutical Pollution of the World’s Rivers. Proc Natl Acad Sci U S A 2022, 119, e2113947119. [Google Scholar] [CrossRef]
- Mosekiemang, T.T.; Stander, M.A.; de Villiers, A. Simultaneous Quantification of Commonly Prescribed Antiretroviral Drugs and Their Selected Metabolites in Aqueous Environmental Samples by Direct Injection and Solid Phase Extraction Liquid Chromatography - Tandem Mass Spectrometry. Chemosphere 2019, 220, 983–992. [Google Scholar] [CrossRef]
- Adeola, A.O.; Forbes, P.B.C. Antiretroviral Drugs in African Surface Waters: Prevalence, Analysis, and Potential Remediation. Environ Toxicol Chem 2022, 41, 247–262. [Google Scholar] [CrossRef]
- Wooding, M.; Rohwer, E.R.; Naudé, Y. Determination of Endocrine Disrupting Chemicals and Antiretroviral Compounds in Surface Water: A Disposable Sorptive Sampler with Comprehensive Gas Chromatography – Time-of-Flight Mass Spectrometry and Large Volume Injection with Ultra-High Performance Liquid Chromatography–Tandem Mass Spectrometry. J Chromatogr A 2017, 1496, 122–132. [Google Scholar] [CrossRef]
- Antunes, A.M.M.; Godinho, A.L.A.; Martins, I.L.; Justino, G.C.; Beland, F.A.; Marques, M.M. Amino Acid Adduct Formation by the Nevirapine Metabolite, 12-Hydroxynevirapine--a Possible Factor in Nevirapine Toxicity. Chem Res Toxicol 2010, 23, 888–899. [Google Scholar] [CrossRef]
- Wu, P.Y.; Cheng, C.Y.; Liu, C.E.; Lee, Y.C.; Yang, C.J.; Tsai, M.S.; Cheng, S.H.; Lin, S.P.; Lin, D.Y.; Wang, N.C.; et al. Multicenter Study of Skin Rashes and Hepatotoxicity in Antiretroviral-Naïve HIVpositive Patients Receiving Non-Nucleoside Reverse-Transcriptase Inhibitor plus Nucleoside Reverse-Transcriptase Inhibitors in Taiwan. PLoS One 2017, 12. [Google Scholar] [CrossRef]
- Sulkowski, M.S.; Thomas, D.L.; Mehta, S.H.; Chaisson, R.E.; Moore, R.D. Hepatotoxicity Associated with Nevirapine or Efavirenz-Containing Antiretroviral Therapy: Role of Hepatitis C and B Infections. Hepatology 2002, 35, 182–189. [Google Scholar] [CrossRef]
- Rivero, A.; Mira, J.A.; Pineda, J.A. Liver Toxicity Induced by Non-Nucleoside Reverse Transcriptase Inhibitors. J Antimicrob Chemother 2007, 59, 342–346. [Google Scholar] [CrossRef]
- Ayele, T.A.; Worku, A.; Kebede, Y.; Alemu, K.; Kasim, A.; Shkedy, Z. Choice of Initial Antiretroviral Drugs and Treatment Outcomes among HIV-Infected Patients in Sub-Saharan Africa: Systematic Review and Meta-Analysis of Observational Studies. Syst Rev 2017, 6. [Google Scholar] [CrossRef]
- Ncube, S.; Madikizela, L.M.; Chimuka, L.; Nindi, M.M. Environmental Fate and Ecotoxicological Effects of Antiretrovirals: A Current Global Status and Future Perspectives. Water Res 2018, 145, 231–247. [Google Scholar] [CrossRef]
- Schoeman, C.; Dlamini, M.; Okonkwo, O.J. The Impact of a Wastewater Treatment Works in Southern Gauteng, South Africa on Efavirenz and Nevirapine Discharges into the Aquatic Environment. Emerg Contam 2017, 3, 95–106. [Google Scholar] [CrossRef]
- Abafe, O.A.; Späth, J.; Fick, J.; Jansson, S.; Buckley, C.; Stark, A.; Pietruschka, B.; Martincigh, B.S. LC-MS/MS Determination of Antiretroviral Drugs in Influents and Effluents from Wastewater Treatment Plants in KwaZulu-Natal, South Africa. Chemosphere 2018, 200, 660–670. [Google Scholar] [CrossRef]
- Czech, B.; Krzyszczak, A.; Boguszewska-Czubara, A.; Opielak, G.; Jośko, I.; Hojamberdiev, M. Revealing the Toxicity of Lopinavir- and Ritonavir-Containing Water and Wastewater Treated by Photo-Induced Processes to Danio Rerio and Allivibrio Fischeri. Science of The Total Environment 2022, 824, 153967. [Google Scholar] [CrossRef]
- Kaizer, A.M.; Shapiro, N.I.; Wild, J.; Brown, S.M.; Cwik, B.J.; Hart, K.W.; Jones, A.E.; Pulia, M.S.; Self, W.H.; Smith, C.; et al. Lopinavir/Ritonavir for Treatment of Non-Hospitalized Patients with COVID-19: A Randomized Clinical Trial. International Journal of Infectious Diseases 2023, 128, 223–229. [Google Scholar] [CrossRef]
- Grubb, J.R.; Dejam, A.; Voell, J.; Blackwelder, W.C.; Sklar, P.A.; Kovacs, J.A.; Cannon, R.O.; Masur, H.; Gladwin, M.T. Lopinavir-Ritonavir: Effects on Endothelial Cell Function in Healthy Subjects. Journal of Infectious Diseases 2006, 193, 1516–1519. [Google Scholar] [CrossRef]
- Istampoulouoglou, I.; Zimmermanns, B.; Grandinetti, T.; Marzolini, C.; Harings-Kaim, A.; Koechlin-Lemke, S.; Scholz, I.; Bassetti, S.; Leuppi-Taegtmeyer, A.B. Cardiovascular Adverse Effects of Lopinavir/Ritonavir and Hydroxychloroquine in COVID-19 Patients: Cases from a Single Pharmacovigilance Centre. Glob Cardiol Sci Pract 2021, 2021. [Google Scholar] [CrossRef]
- Ebele, A.J.; Abou-Elwafa Abdallah, M.; Harrad, S. Pharmaceuticals and Personal Care Products (PPCPs) in the Freshwater Aquatic Environment. Emerg Contam 2017, 3, 1–16. [Google Scholar] [CrossRef]
- Madikizela, L.M. A Journey of 10 Years in Analytical Method Development and Environmental Monitoring of Pharmaceuticals in South African Waters. South African Journal of Chemistry 2023, 77, 80–100. [Google Scholar] [CrossRef]
- Phong Vo, H.N.; Le, G.K.; Hong Nguyen, T.M.; Bui, X.T.; Nguyen, K.H.; Rene, E.R.; Vo, T.D.H.; Thanh Cao, N.D.; Mohan, R. Acetaminophen Micropollutant: Historical and Current Occurrences, Toxicity, Removal Strategies and Transformation Pathways in Different Environments. Chemosphere 2019, 236, 124391. [Google Scholar] [CrossRef] [PubMed]
- Oluwalana, A.E.; Musvuugwa, T.; Sikwila, S.T.; Sefadi, J.S.; Whata, A.; Nindi, M.M.; Chaukura, N. The Screening of Emerging Micropollutants in Wastewater in Sol Plaatje Municipality, Northern Cape, South Africa. Environmental Pollution 2022, 314, 120275. [Google Scholar] [CrossRef]
- Drew, D.; Dobreniecki, S.; Ford, E.; et al. Acetaminophen. Scoping Document: Recommendation for Anticipated Data and Human Health Risk Assessments for Registration Review; 2023; https://downloads.regulations.gov/EPA-HQ-OPP-2022-0816-0004/content.pdf.
- Madikizela, L.M.; Nuapia, Y.B.; Chimuka, L.; Ncube, S.; Etale, A. Target and Suspect Screening of Pharmaceuticals and Their Transformation Products in the Klip River, South Africa, Using Ultra-High–Performance Liquid Chromatography–Mass Spectrometry. Environ Toxicol Chem 2022, 41, 437–447. [Google Scholar] [CrossRef]
- Adegoke, O.; Dabrowski, J.M.; Montaseri, H.; Nsibande, S.A.; Petersen, F.; Forbes, P.B.C. DEVELOPMENT OF NOVEL FLUORESCENT SENSORS FOR THE SCREENING OF EMERGING CHEMICAL POLLUTANTS IN WATER Report to the Water Research Commission. Water Research Commission 2017. [Google Scholar]
- Minnesota Department of Health (MDH) Acetaminophen in Drinking Water. Available online: www.health.state.mn.us/eh (accessed on 1 October 2023).
- Rimayi, C.; Odusanya, D.; Weiss, J.M.; de Boer, J.; Chimuka, L. Contaminants of Emerging Concern in the Hartbeespoort Dam Catchment and the UMngeni River Estuary 2016 Pollution Incident, South Africa. Science of The Total Environment 2018, 627, 1008–1017. [Google Scholar] [CrossRef]
- Zhang, Y.; Geißen, S.U.; Gal, C. Carbamazepine and Diclofenac: Removal in Wastewater Treatment Plants and Occurrence in Water Bodies. Chemosphere 2008, 73, 1151–1161. [Google Scholar] [CrossRef]
- K’oreje, K.O.; Okoth, M.; Van Langenhove, H.; Demeestere, K. Occurrence and Treatment of Contaminants of Emerging Concern in the African Aquatic Environment: Literature Review and a Look Ahead. J Environ Manage 2020, 254, 109752. [Google Scholar] [CrossRef]
- Kebede, T.G.; Dube, S.; Nindi, M.M. Removal of Non-Steroidal Anti-Inflammatory Drugs (NSAIDs) and Carbamazepine from Wastewater Using Water-Soluble Protein Extracted from Moringa Stenopetala Seeds. J Environ Chem Eng 2018, 6, 3095–3103. [Google Scholar] [CrossRef]
- Aanderud, S.; Myking, O.L.; Strandjord, R.E. The Influence Of Carbamazepine On Thyroid Hormones And Thyroxine Binding Globulin In Hypothyroid Patients Substituted With Thyroxine. Clin Endocrinol (Oxf) 1981, 15, 247–252. [Google Scholar] [CrossRef]
- Aanderud, S.; Strandjord, R.E. Hypothyroidism Induced by Anti-epileptic Therapy. Acta Neurol Scand 1980, 61, 330–332. [Google Scholar] [CrossRef]
- Nugegoda, D.; Kibria, G. Effects of Environmental Chemicals on Fish Thyroid Function: Implications for Fisheries and Aquaculture in Australia. Gen Comp Endocrinol 2017, 244, 40–53. [Google Scholar] [CrossRef]
- Fraz, S.; Lee, A.H.; Pollard, S.; Srinivasan, K.; Vermani, A.; David, E.; Wilson, J.Y. Paternal Exposure to Carbamazepine Impacts Zebrafish Offspring Reproduction over Multiple Generations. Environ Sci Technol 2019, 53, 12734–12743. [Google Scholar] [CrossRef]
- Löffler, P.; Escher, B.I.; Baduel, C.; Virta, M.P.; Lai, F.Y. Antimicrobial Transformation Products in the Aquatic Environment: Global Occurrence, Ecotoxicological Risks, and Potential of Antibiotic Resistance. Environ Sci Technol 2023, 57, 9474–9494. [Google Scholar] [CrossRef]
- National Institutes of Health; Prevention, C. for D.C.; (OARAC), H.M.A. of the I.D.S. of A.P. on G. for the P. and T. of O.I. in A. and A. with H.A.W.G. of the O. of A.R.A.C. Guidelines for the Prevention and Treatment of Opportunistic Infections in Adults and Adolescents with HIV; US Department of Health and Human Services, 2024.
- Kwon, B.; Kho, Y.; Kim, P.G.; Ji, K. Thyroid Endocrine Disruption in Male Zebrafish Following Exposure to Binary Mixture of Bisphenol AF and Sulfamethoxazole. Environ Toxicol Pharmacol 2016, 48, 168–174. [Google Scholar] [CrossRef]
- Madureira, T.V.; Rocha, M.J.; Cruzeiro, C.; Galante, M.H.; Monteiro, R.A.F.; Rocha, E. The Toxicity Potential of Pharmaceuticals Found in the Douro River Estuary (Portugal): Assessing Impacts on Gonadal Maturation with a Histopathological and Stereological Study of Zebrafish Ovary and Testis after Sub-Acute Exposures. Aquatic Toxicology 2011, 105, 292–299. [Google Scholar] [CrossRef]
- Murphy, P.B.; Bistas, K.G.; Patel, P.; Le, J.K. Clindamycin. In xPharm: The Comprehensive Pharmacology Reference; StatPearls Publishing, 2024; pp. 1–4 ISBN 9780080552323.
- EU Commission Proposal Amending Water Directives - European Commission; 2022; European Commission, Official Journal of the European Communities 0344.
Figure 1.
Location of the Thulamela Local Municipality (red circle) in Vhembe District, Limpopo Province (blue circle), South Africa, where the study was conducted [36,37].
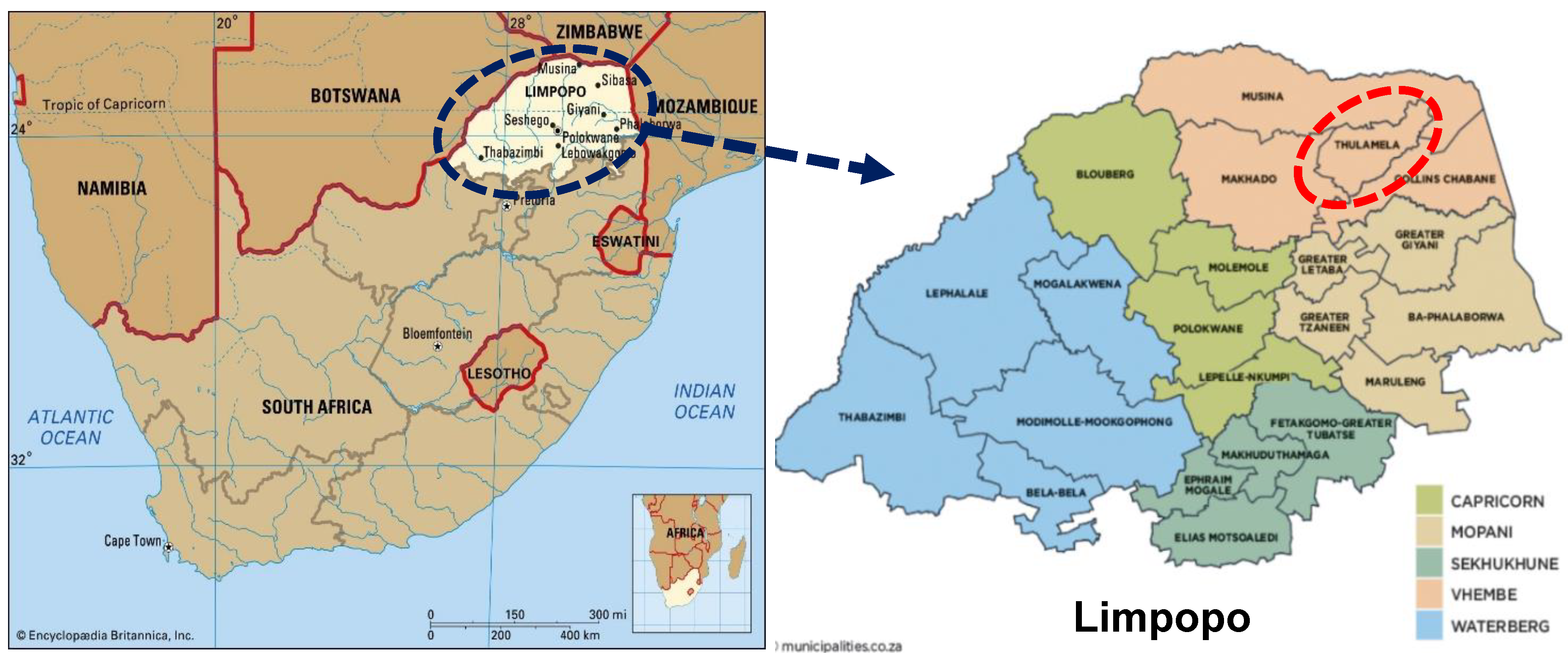
Figure 2.
Google map view of 21 sampling points from rivers, streams, and dams in Vhembe District Municipality. The sampling points were located near hospitals, clinics, and WWTWs. (Generated with Google Earth, Image © 2024 Maxa Technologies).
Figure 2.
Google map view of 21 sampling points from rivers, streams, and dams in Vhembe District Municipality. The sampling points were located near hospitals, clinics, and WWTWs. (Generated with Google Earth, Image © 2024 Maxa Technologies).
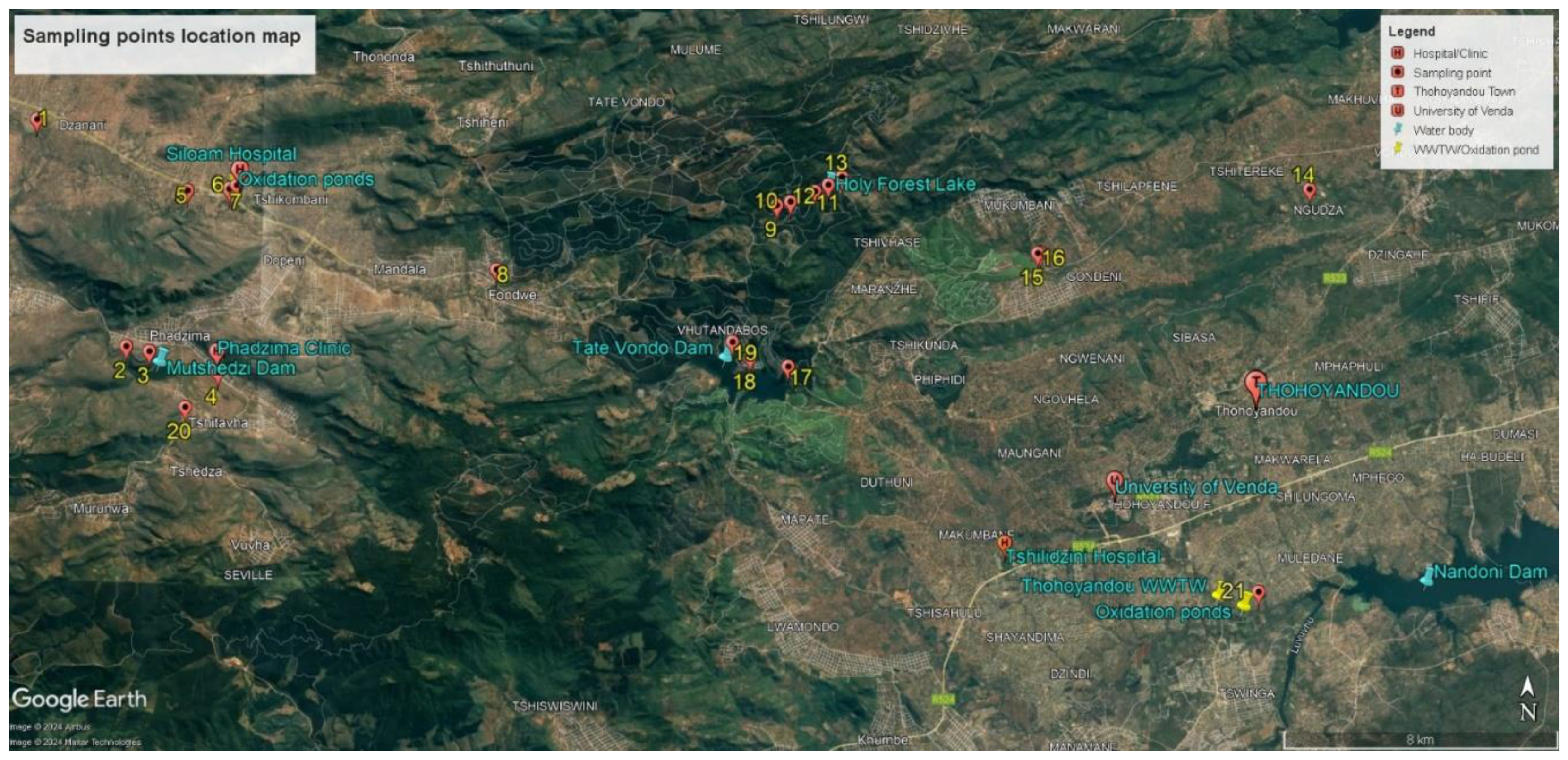
Figure 3.
The calibration curve for caffeine was used as a standard sample. Note the correlation between the change in concentrations and the signal response.
Figure 3.
The calibration curve for caffeine was used as a standard sample. Note the correlation between the change in concentrations and the signal response.
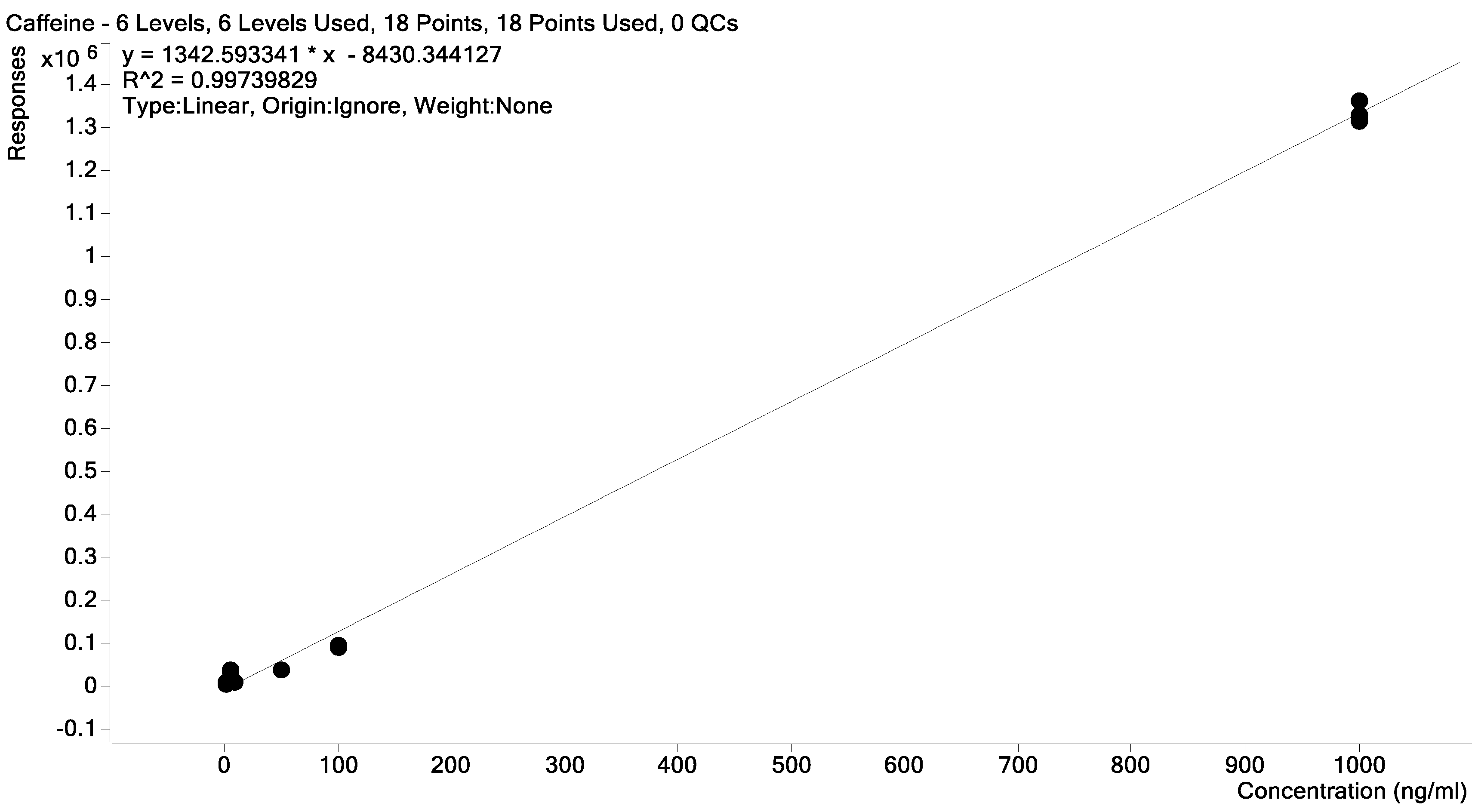
Figure 4.
The calibration curve from abacavir was used as a second standard to determine the limits of detection and quantification of the targeted pharmaceuticals.
Figure 4.
The calibration curve from abacavir was used as a second standard to determine the limits of detection and quantification of the targeted pharmaceuticals.
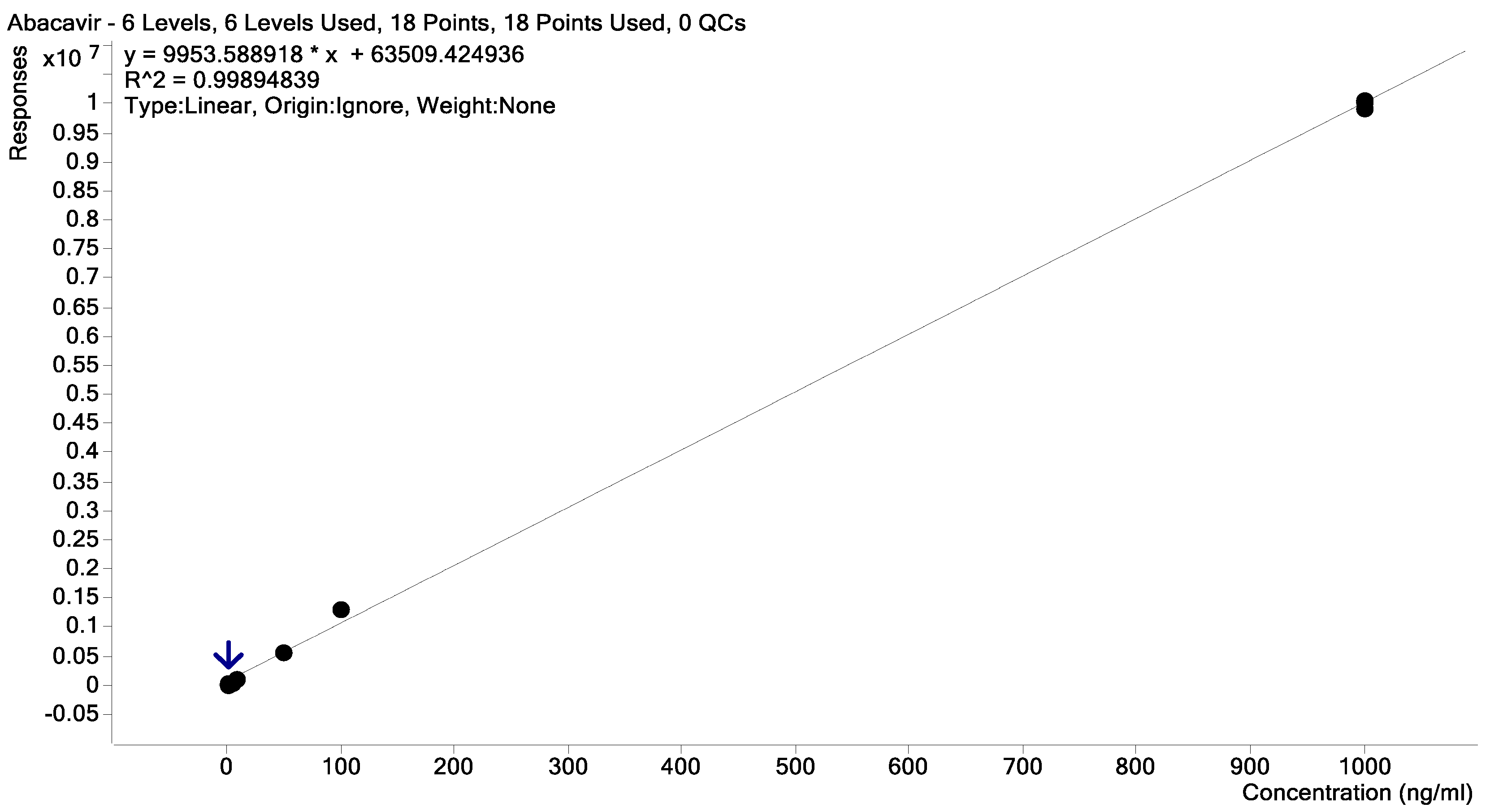
Table 1.
Sampling sites’ location in the Vhembe District Municipality, Limpopo Province.
| Sites | Location | Coordinates | Elevation |
|---|---|---|---|
| 1 | Nzhelele River after Mutshedzi River joint | 22°53ˈ10.59” S; 30°08ˈ13.90” E | 746 m |
| 2 | In the river below Mutshedzi Dam | 22°56ˈ43.30” S | 846 m |
| 3 | Mutshedzi Dam | 22°56ˈ47.30” S; 30°10ˈ14.00” E | 865 m |
| 4 | Tshiluvhadi River | 22°57ˈ18.59” S; 30°11ˈ56.26” E | 923 m |
| 5 | Nzhelele River below Shiloam Hospital oxidation ponds | 22°54ˈ15.86” S; 30°10ˈ50.53” E | 787 m |
| 6 | Next to Shiloam Hospital, receiving water from the hospital | 22°54ˈ09.21” S; 30°11ˈ40.17” E | 801 m |
| 7 | Below point 8 (stream below the oxidation ponds) | 22°54ˈ14.48’’S; 30°11ˈ32.65” E | 796 m |
| 8 | Upstream Nzhelele River at Fondwe near villages | 22°55ˈ23.17” S; 30°16ˈ08.56” E | 848 m |
| 9 | Holy Forest Lake 1 (HFL1) inflow | 22°54ˈ17.06” S; 30°20ˈ54.62” E | 1084 m |
| 10 | HFL1 | 22°54ˈ12.62” S; 30°21ˈ08.36” E | 1083 m |
| 11 | HFL1 | 22°54ˈ02.65” S; 30°21ˈ33.14” E | 1082 m |
| 12 | Before overflow HFL1 | 22°53ˈ56.05” S; 30°21ˈ47.29” E | 1085 m |
| 13 | Below the overflow HFL1 | 22°53ˈ48.50” S; 30°22ˈ00.82” E | 1081 m |
| 14 | Tshinane River inflow stream below old oxidation ponds | 22°53ˈ49.92” S; 30°29ˈ58.11” E | 585 m |
| 15 | The small stream next to the tea plantation flowing into Tshinane River | 22°54ˈ57.04” S; 30°25ˈ21.97” E | 681 m |
| 16 | Tshinane River before no 19 flows in | 22°54ˈ56.41” S; 30°25ˈ23.58” E | 676 m |
| 17 | Before the outflow of the Tate Vondo Dam | 22°56ˈ49.55” S; 30°21ˈ09.67” E | 870 m |
| 18 | Along the TateVondo Dam shores | 22°56ˈ41.48” S; 30°20ˈ29.79” E | 871 m |
| 19 | Closer to the inflow of the TateVondo Dam | 22°56ˈ26.78” S; 30°20ˈ11.44” E | 871 m |
| 20 | In the Tshikhwikhwikhwi River | 22°57ˈ39.25” S; 30°10ˈ51.63” E | 885 m |
| 21 | Below the Thohoyandou WWTW and oxidation ponds in the Mvudi River | 23°00ˈ11” S; 30°29ˈ14” E | 517 m |
Table 2.
Pharmaceuticals detected in Vhembe District Municipality waters (concentrations in ng/L).
| SITES | Caffeine | Nevirapine | Lopinavir | Acetaminophen | Fluconazole | Sulfamethoxazole | Clindamycin | Carbamazepine |
|---|---|---|---|---|---|---|---|---|
| 1 | n.d | 109 | n.q | n.d | n.d | n.d | n.d | n.d |
| 2 | 181 | n.d | n.d | n.d | n.d | n.d | n.d | n.d |
| 3 | 584 | n.q | n.d | n.d | n.d | n.d | n.d | n.d |
| 4 | 110 | n.d | n.d | n.d | n.d | n.d | n.d | n.d |
| 5 | >1000 | n.d | n.d | n.d | n.d | n.d | n.d | n.d |
| 6 | n.d | n.q | n.d | n.d | n.d | n.d | n.d | n.d |
| 7 | n.d | 166 | 42 | n.d | >1000 | n.q | n.d | 21 |
| 8 | 94 | n.d | n.d | n.d | n.d | n.d | n.d | n.d |
| 9 | >1000 | n.d | n.d | n.d | n.d | n.d | n.d | n.d |
| 10 | >1000 | n.d | n.d | n.d | n.d | n.d | n.d | n.d |
| 11 | n.d | n.d | n.d | n.d | n.d | n.d | n.d | n.d |
| 12 | >1000 | n.d | n.d | n.d | n.d | n.d | n.d | n.d |
| 13 | >1000 | n.d | n.d | n.d | n.d | n.d | n.d | n.d |
| 14 | 159 | n.d | n.d | n.d | n.d | n.d | n.d | n.d |
| 15 | >1000 | n.q | n.d | n.d | n.d | n.d | n.d | n.d |
| 16 | n.d | n.d | n.d | n.d | n.d | n.d | n.d | n.q |
| 17 | 479 | n.q | n.d | n.d | n.d | n.d | n.d | n.d |
| 18 | 217 | n.d | n.d | n.d | n.d | n.d | n.d | n.d |
| 19 | n.d | n.q | n.d | n.d | n.d | n.d | n.d | n.d |
| 20 | 690 | n.q | n.d | 292 | n.d | n.d | n.q | n.d |
| 21 | 975 | 7 | n.d | 427 | n.d | n.d | n.q | n.q |
Abbreviations: n.d = not detectable (target S/N < 3 ng/L); n.q = detected but not quantifiable by the instrument (target S/N > 3 ng/L but < 10 ng/L); >1000 = signal outside the calibration range.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



