
Submitted:
20 December 2024
Posted:
20 December 2024
You are already at the latest version
Abstract
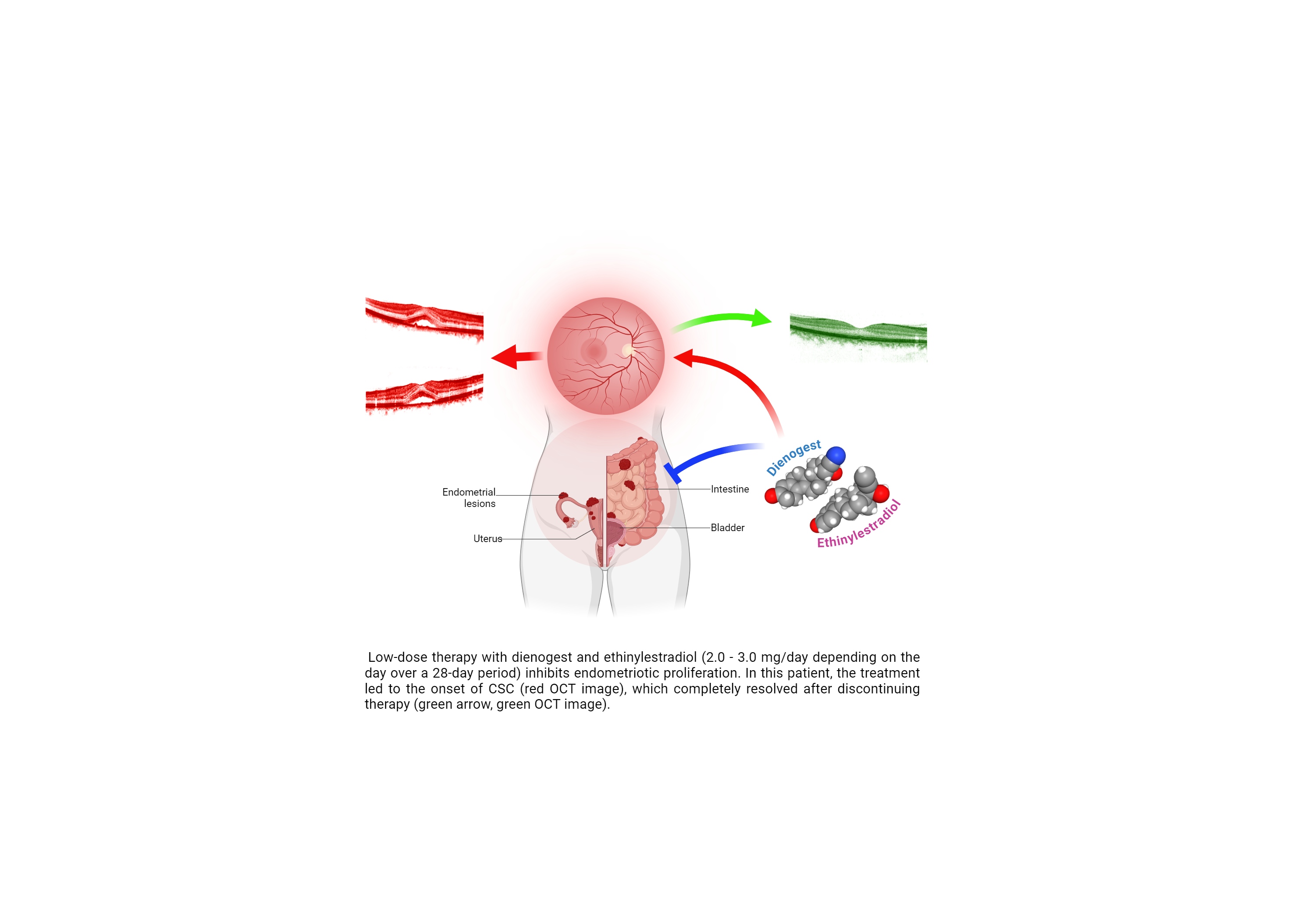
Endometriosis afflicts 10% of women in their reproductive years and nearly half of women with infertility and its etiology is not yet clear. Pharmacological therapy is generally based on progestins like progestogen. This drug binds to progesterone receptors with many known side effects. Here we described the case of a 33-year-old woman surgically treated for endometriosis continued with drug therapy based on estradiol valerate and dienogest. Approximately 21 months after treatment, she reported ocular symptoms with vision alteration, diplopia and metamorphopsia related to central serous chorioretinopathy (CSC). After discontinuation of combined progestin-based treatment, CSC fully subsided. Semeiological, clinical and laboratory approaches were adopted; urinary steroids were measured. A slight increase in prolactinemia in the absence of macro-prolactinemia was reported. Steroidal profile appeared without abnormalities, without abnormalities, although a slight alteration of estrogens balance was noted. Considering the pharmacodynamics of dienogest versus selective progesterone receptor modulators, it can be assumed that patients clinical events are related to specific-site-response of steroids that bind the progesterone receptor. Dienogest may have induced the CSC, as a not yet characterized side effect of the drug. Undoubtedly, further specific studies are needed concerning the metabolic and pharmacodynamic aspects that cannot be exhaustively covered here.
Keywords:
Endometriosis
; PR
; chorioretinopathy
; CSC
; dienogest
1. Introduction
Currently, endometriosis has a prevalence of approximately 10%, and from the knowledge in our possession is a multifactorial pathology, whose etiology is not fully clarified [1] Endometriosis is characterized by endometrial glands and stroma in location outside the endomyometrium. It occurs in as many as 10% of women in their reproductive years and in nearly half of women with infertility. It is a common cause of dysmenorrhea, and pelvic pain, and may present as a pelvic mass filled with degenerating blood (chocolate cyst) [2]. It is frequently multifocal and may involve tissue in the pelvis (ovaries, pouch of Douglas, uterine ligaments, tubes, and rectovaginal septum), less frequently in more remote sites of the peritoneal cavity and about the umbilicus and uncommonly lymph nodes, lungs, and even heart, skeletal muscle, or bone [3,4]. Three possibilities (not mutually exclusive) have been invoked to explain the origin of these dispersed lesions. First, the regurgitation theory, currently the most accepted, proposes menstrual backflow through the fallopian tubes with subsequent implantation. Indeed, menstrual endometrium is viable and survives when injected into the anterior abdominal wall; however, this theory cannot explain lesions in the lymph nodes, skeletal muscle or lungs. Second, the metaplastic theory proposes endometrial differentiation of coelomic epithelium, which is the origin of the endometrium itself [5,6]. This theory too, cannot explain endometriotic lesions in the lungs or lymph nodes. Third, the vascular or lymphatic dissemination theory has been invoked to explain extrapelvic or intranodal implants. Conceivably, all pathways are valid in individual instances. The clinical manifestations of endometriosis depend on the distribution of the lesions. Extensive scarring of the oviducts and varies often produces discomfort in the lower abdominal quadrants and eventually causes sterility [7,8]. Pain on defecation reflects rectal wall involvement and dyspareunia (painful intercourse) and dysuria reflect involvement of the urine and bladder serosa, respectively. In almost all cases, there is severe dysmenorrhea and pelvic pain as a result of intrapelvic bleeding and periuterine adhesions [9]. Current treatments for endometriosis comprehend conservative surgery and fertility treatment, alongside hormone therapy, generally in combination with pain relievers [10]. Therapeutic choices are different, also based on patients clinical situation and include: hormonal contraceptives that can help to control the hormones responsible for the buildup of endometrial tissue [11]; gonadotropin-releasing hormone (Gn-RH) agonists and antagonists, typically in combination with a low dose of estrogen that block the production of ovarian-stimulating hormones, limiting estrogen levels [12]; progestin therapy that can stop the menstrual periods and the progression of endometrial formation and aromatase inhibitors with progestin to reduce the amount of estrogen [13,14]. Progestin-based therapy is chosen for long-treatment of endometriosis and the first selection is represented by dienogest. It is an oral progestin that has been investigated systematically in Europe and Japan for the treatment of endometriosis in different clinical assets: from dose-ranging and placebo-controlled to active comparator-controlled, and long-term trials performed. Based on these studies, dienogest in monotherapy has received approval for the treatment of endometriosis in Europe, Australia, Singapore and Japan [15]. Pharmacologically, dienogest grants the positive effects of both the 19-norprogestin and the progesterone derivative classes. When administered continuously, dienogest induces a hypoestrogenic, hypergestagenic local endocrine environment, leading to a decidualization of endometrial tissue with consequent atrophy of the endometriotic lesions. Animal studies suggest that dienogest may also lower plasma estradiol exposures via apoptosis of granulose cells in the ovary [16]. Many studies in vitro and in animals show that dienogest has a direct inhibitory effect on the proliferation of endometrial-like tissue that is independent of progesterone receptor binding [17,18]. Another important mechanism of action for dienogest is inhibition of angiogenesis, which is important in endometriotic lesions: the molecular mechanisms at the basis of this process continue to be explored [19,20]. Dienogest has been investigated as a long-term treatment of endometriosis in two large trials (Europe and Japan), evaluating efficacy, change in quality of life, safety, and tolerability. During the long-term study, laboratory parameters, vital signs, and body weight remained within range. Adverse effects treatment-related developed in 16.1% of women, including breast discomfort (4.2%), nausea (3.0%), and irritability (2.4%). The maximal intensity of treatment-related adverse events was mild or moderate in 92.5% of cases. The most reported treatment-related adverse event was metrorrhagia (71.9%), followed by headaches (18.5%) and constipation (10.4%). None of the treatment related adverse events was rated as serious [21,22]. Currently, many mechanisms and possible negative implications of dienogest remains poorly explored; in this study we presented the case of 33-years-old treated for endometriosis with endometriosis treated with estradiol valerate/dienogest after surgical intervention. The patient developed central serous chorioretinopathy (CSC) during progestins treatment, with a complete regression after dienogest stop.
2. Materials and Methods
2.1. Anamnesis and Diagnosis
This study presented a 33-year-old female patient diagnosed with polyp of the uterus body and endometriosis cysts of the left ovary. The patient underwent resectoscopic and laparoscopic polypectomy surgery by removal of endometriosis cysts. The surgery was conducted in the first instance with the positioning of anterior and posterior ibere valves with subsequent dilation by Hegar of increasing number up to 10. Through the insertion of the resector it was possible to visualize regular cervical canal, regular isthmus, morphologically regular uterine cavity occupied by endometrial polyp with left lateral implantation, regular and in-situ osti, hyperplastic endometrium. The intervention then continued with removal of the endometrial polyp by means of a bipolar loop and slicing technique and with removal of portions of endometrium. At this point a uterine manipulator is positioned with induction of pneumoperitoneum by means of a Verres needle and subsequent introduction of three-way optics in the left iliac fossa, right iliac fossa and suprapubic seat. In this context they were visualized: the uterus affected by the presence of voluminous node of fundic myoma, the right ovary regular in shape and size, the left appendage deformed by the presence of a massive cyst of about 8 cm.
The perforation of the cyst causes leakage of dense liquid to "chocolate" that is aspirated. The cyst is then removed by stripping of the cystic wall and the tubal patency is subsequently verified by salpinge-kromoscopy. In this phase is highlighted tubal patency preserved on the left and obstacle at the isthmic level on the right. Endometriosis foci are also observed at the abdominal wall and perivesical peritoneum, on which diathermocoagulation is performed and excision of the affected area. An intramural myoma node with a diameter of about 5 cm at the level of the uterine bottom is identified; regularity of the Douglas hollow, of the vesicular-uterine fossa and of the annexes is observed. Myomectomy was then performed. An incision of the uterine wall was then made at the myoma, highlighting the capsule of the myoma and its cleavage plane and proceeding to its enucleation.
2.2. Pharmacological Treatment and Instrumental Exams
Histopathological examination of intraoperative findings confirms the diagnosis of endometriosis on biopsy fragments of prevesical peritoneum. The subsequent pharmacological treatment of endometriosis involved the administration of estradiol valerate/dienogest at low dosage over a 28-day cycle (see Table 1). The treatment with estradiol valerate in association with dienogest orally provides different dosages depending on the day of the month completing a cycle of 28 days as shown in Table 1. This treatment continued for 21 months, with the appearance of ocular symptoms such as: diplopia, blurred vision and in general metamorphopsia.
The optical coherence tomography (OCT) was performed and serous fluid from the choroid was infiltrated with detachment localized between the Inner/outer Photoreception layer and the retinal pigmented epithelium (see Figure 2). This clinical picture led to the diagnosis of CSC.
2.3. Clinical Biochemistry
Clinical and haematological tests were carried out. Serum prolactin was dosed after interruption of pharmacologycal therpay and the steroidal profile was then determined on a 24h urine sample using the gas chromatography method coupled to mass spectrometry (GC-MS), according to Shackleton et al. [23,24], to further deepen the metabolic condition.
To investigate patients metabolic balance, the ratio of the steroids was investigated. In particular, the ratio of concentrations of etiocholanolone [Et] and androsterone [An] and its reciprocal was considered and compared with reference values reported by Rousson V. et al. [25], to understand the equilibrium of the androgen pathway.
In the same way, the balance between testosterone biosynthesis pathways was evaluated considering the ratio of pregnanediol (P2) to the sum of Et and An.
Furthermore, estrogen levels were evaluated through the ratio between estrone (E1) and the sum of 17β-estradiol (E2) and estriol (E3). Reference value in normal conditions for this ratio was not considered by Rousson in his work, thus, as part of our work, we analyzed with GC-MS technique, the urine of 36 healthy women with age comprised between 30 and 40 years, reporting E1 and its relationship with the sum of the concentrations of E2 and E3.
3. Results
The diagnostic evidence obtained from the anatomical-pathological examination of the intraoperative findings confirmed the diagnostic hypotheses, based on the gynecological semeiotic, of endometriosis. Surgical treatment allowed the removal of several endometriosis foci including those at the bladder peritoneum.
Estradiol valerate/dienogest treatment provided clinical evidence to contain and subsequently abolish the symptoms reported by the patient in the perioperative period, summarized in the total absence of heavy menstrual bleeding (HMB) and pelvic pain.
After 21 months from the beginning of drug treatment, the patient began to report ophthalmologic symptoms, as regards the visual functionality of the right eye. The most evident signs were those related to diplopia and metamorphopsia.
Optical coherence tomography of the right eye showed a macular thickening due to a serus neuroretinal detachment. The photograph (in two sections) reported in Figure 1a an increased value of 371 µm of foveal thickness at the level of the central zone. This value returned to the norm (259 µm) after 15 days of discontinuation of drug therapy based on estradiol valerate/dienogest (see Figure 1b).
The morphology of the retinal layers and the increased BMO-MRW values led to the diagnosis of CSC, which regressed with complete resolution of the visual symptomatology in a progressive way after 15 days of discontinuation of the aforementioned drug therapy. Possible correlation between progestin therapy and the onset of CSC was investigated. The hematochemical and hematological condition, which did not provide any significant evidence, was therefore examined in depth. An increase in prolactinemia (41.2µg/L) in the absence, however, of macro-prolactinemia (estimated monomer/total ratio of 72%) was observed.
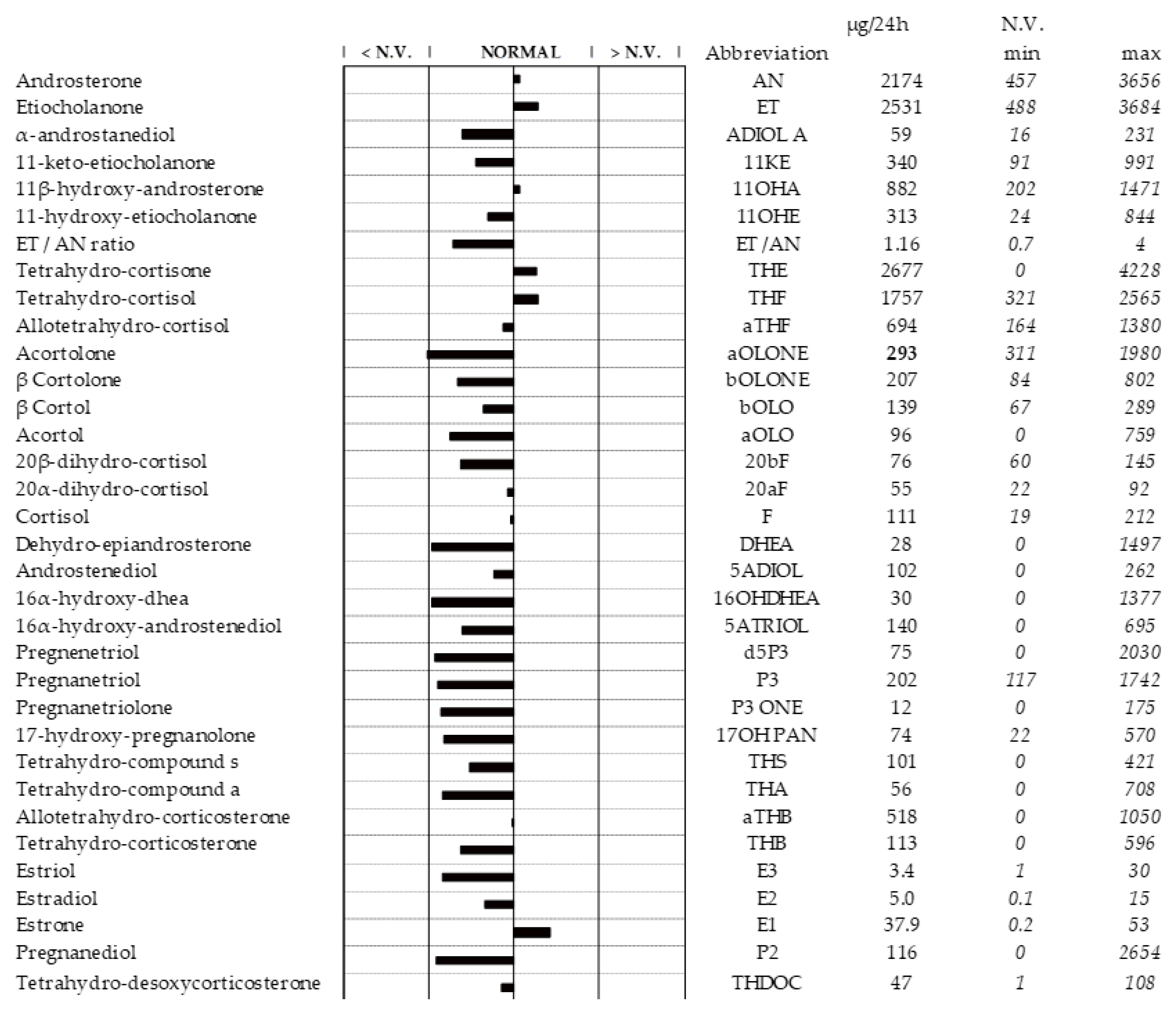
Apparently, the steroid profile was in the norm, although some variations were highlighted. (See Figure 2).
Figure 2.
This figure shows the patients steroid profile in sample of 24h urine. Minimum and maximum ranges have been obtained from subject with ages comprised between 18 and 55 years. For comments see the text.
Figure 2.
This figure shows the patients steroid profile in sample of 24h urine. Minimum and maximum ranges have been obtained from subject with ages comprised between 18 and 55 years. For comments see the text.
All ratio values to evaluate the functionality of some enzymes and their metabolic flow according to specific pathway, for a better understanding of urinary steroid profile, were reported in Table 2.
[An]/[Et] ratio and its reciprocal were respectively 0.859 and 1.164 and fell within the range of normal values.
Concerning testosterone biosynthesis balance, P2 to the sum of Et and An ratio showed a slight decrease compared to the lower limit of normality (0.025 < 0.0376).
When considering estrogens balance, references values for the ratio of E1 and the sum of the concentrations of E2 and E3 obtianed from 36 healthy women were reported in Table 3.
Patients estrogens ratio was 4.51, above the calculated reference value.
4. Discussion
Patients steroid profile led to some potentially relevant considerations on the physio pathological mechanisms that had a partial clinical response in the patient.
Considering the ovarian steroidogenesis (See Figure 3 A and B), the two main pathways are: the Δ4 pathway and the Δ5 pathway: the first reaction series leads to synthesis of progesterone, while the second metabolic process results in testosterone as final metabolite in the ovarian theca cells (or in Leydig cells) [26]. The most prominent step in this way of steroids biosynthesis is represented by the transport of cholesterol from the outer mitochondrial membrane to the inner membrane through the StAR (hormone-induced steroidogenic acute regulatory protein) [27]. The first limiting-rate step of steroidogenesis is the conversion of cholesterol into pregnenolone constituted by free distinct biochemical reactions: 20α-hydroxylation, 22-hydroxylation, and side-chain cleavage reaction (C–C bond cleavage of 20R,22R-dihydroxycholesterol) [28]. These facts suggest that the reactions involved in the synthesis of androstenedione (A4) and testosterone (T) are in a steady-state condition during physio-logical conditions [29]. In fact, the metabolic flux of these steroidogenic enzyme is basically unidirectional, therefore the accumulation of a product does not promote the reverse reaction [30]. Consequently, when considering the basal (after discontinuation of progestins-based therapy) steroid profile of the reported patient, it is essential to assess which pathway contributes more to the formation of Et and An, to evaluate any "asymmetries" of such metabolism. The ratio [An]/[Et] gives information about the activity of 5alpha-reductase, while its reciprocal [Et/An] tells if the way is more oriented towards androgen backdoor pathway (ABP) then classical pathway [31,32]. These ratios, respectively 1.16 and 0.859 (reported in Figure 2), fell within the range of normal values.
In general, these ratios, other than being pathological for certain diseases related to the defects of steroidogenesis, can be used as indices of evaluation of steroid metabolism.
Considering the pathways involved in testosterone biosynthesis, represented by Δ4 via progesterone or Δ5 through DHEA, the balance between these pathways could be evaluated considering the ratio of P2 to the sum of Et and An. In details, considered patient showed a slight decrease in this ratio compared to the lower limit of normality (0.025 < 0.0376). An opposite trend was observed when considering estrogen levels, evaluating the ratio between E1 and the sum of E2 and E3.
In the works of Rousson V. et al. and Bochud M. et al. E1 is not considered, not even the relationship with its metabolites E2 and E3, it is there-fore difficult to compare with E1 values or their relationship with other estrogens within reference values obtained by analyzing healthy women urine [25,33]. Shakleton et al. in their work reported E1 values but considered patients are few and by age distinction is lacking [34]. For this work, reference values for E1 to the sum of E2 and E3 were obtained analyzing the urine of 36 healthy women (see Table 3).
Patients estrogen levels above the range limit indicated a shifted equilibrium towards the precursor of E2 and E3. This typically occurs at physio-logical progesterone levels that inhibit the increase in concentration of E2 and E3 that would be the basis of pathological frameworks, like endometriosis [35]. Therefore, considering the fact that P2 levels at the time of the steroid dosing were physiological, it could be highlighted that patients steroidogenesis occurred with a metabolic flow that saw predominant progestin activity with a shift of estrogenic balance towards E1.
All this considered, the retina and the choroid present progesterone (PR), androgen (AR) and estrogen (ER) receptors [36], recalling that the progesterone receptor is a ligand-activated transcription factor and member of the nuclear receptor (NR) superfamily. All nuclear receptors have three preserved functional domains, binding respectively to DNA, N-terminal domain, and C-terminal domain, that binds to ligand [37]. When progesterone binds to its receptor, a conformational change occurs that trans-forms it into an active transcription factor. At this point a phosphorylation of the receptor occurs, but now, its role is not completely clarified.
The receptor then dimerizes to form PR-A and PR-B that are not structurally identical. These isoforms have similar activities, related to the steroid hormone-DNA interaction, but their functional activities are unique. Dimers interact with specific sequences of nuclear DNA (hormone-responsive elements) in genes that respond to progesterone. The dimeric-agonist receptor complex is combined with coactivators that bind the complex to the transcription gene [38]. Thus, the rate of gene transcription is increased or decreased. Once gene transcription is started, proteins are synthesized, and then in the cells and organs the different physiological effects are observed.
The main physiological site of action of progesterone is the uterus, although its receptor, like that of other steroid compounds, is found in different anatomical districts, including retinal tissue and choroid. It is there-fore to highlight that progestins, like dienogest, related to norethindrone and classified as an analogue of testosterone, have a decidedly important role in producing events different from their usual pharmacodynamics. Dienogest is structurally unique, presenting the molecular structure of the estrane, a cyanomethyl group in C17 that replaces the ethylene group, and an unsaturation Δ9 (see Figure 3, at half-height on the right). It is often used in combination with estradiol valerate to intervene on menopause disorders and has long since been implanted in the treatment of endometriosis, as in this case.
Focusing on the pathological manifestation linked to chorioretinopathy, one last evidence should be considered. Nielsen J. S. et al. de-scribed in 2007 the case of a 63-year-old male patient with CSC, treat-ed to full regression with mifepristone at a dose of 200mg/day [39,40]. This leads to an interesting question: can a PR modulator like mifepristone treat CSC while a progestin like dienogest may have induced it in the reported patient? Based on the observation of the presented work, the following consideration could be done: both mifepristone and dienogest bind to the PR and glucocorticoid receptor (GR), both belonging to the NR superfamily. Studies in which the affinity of dienogest for different NR, like PR, AR, ER, GR and mineralocorticoid receptor (MR) has been experimentally measured are lacking in the literature; nevertheless, Robin-Jaerschmidt et al. [41] by performing site-specific substitutions in the amino acid sequence of GR and PR through a chimerical receptor called GPn, showed that it is possible to modify the affinity of several ligands, including mifepristone, with different receptors, thus obtaining equally different response activities. It is therefore plausible a different modulation by mifepristone and dienogest on both the PR and the GR. The predominant action of the antiglucocorticoid type exercised by mifepristone [35,42] resulted in a reduction of the inflammatory process with CSC resolution, while a weak activity of dienogest on the GR, linked to a predominant progestin effect, within the already highlighted steroid profile, determined an inflammatory effect that, at that moment, was only clinically describable with the appearance of CSC and complete resolution following therapy interruption.
5. Conclusions
Mifepristone and dienogest affinity for different types of receptors should be further and deeper explored. Different pharmacodynamics and pharmacokinetics aspects need to be clarified, focusing on the under-standing of the biochemical mechanisms underlying the clinical evidence described in this work. All the clinical and biochemical information re-ported in this work can uniquely justify the pathological manifestations observed, not leading to a decisive conclusion regarding all mifepristone implication.
Author Contributions
Conceptualization, F.C. and G.M.; methodology, F.C., J.M. and S.L.; software, S.L. and S.A.; formal analysis, F.C. and M.C.; resources, M.P.P and D.T.; writing—original draft preparation, F.C. and S.A.; writing—review and editing, S.D.F.; supervision, M.P.P., G.M. and S.D.F. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki and approved by the Comitato Etico Interaziendale A.O.U. Città della Sa-lute e della Scienza di Torino – A.O. Ordine Mauriziano – A.S.L. TO1 (protocol code 14982 and date of approval 11/02/2021).
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
Not applicable.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Saunders, P.T.K.; Horne, A.W. Endometriosis: Etiology, pathobiology, and therapeutic prospects. Cell 2021, 184, 2807–2824. [Google Scholar] [CrossRef] [PubMed]
- Zondervan, K.T.; Becker, C.M.; Koga, K.; Missmer, S.A.; Taylor, R.N.; Vigano, P. Endometriosis. Nat Rev Dis Primers 2018, 4, 9. [Google Scholar] [CrossRef] [PubMed]
- Bourgioti, C.; Preza, O.; Panourgias, E.; Chatoupis, K.; Antoniou, A.; Nikolaidou, M.E.; Moulopoulos, L.A. MR imaging of endometriosis: Spectrum of disease. Diagn Interv Imaging 2017, 98, 751–767. [Google Scholar] [CrossRef]
- Mechsner, S.; Weichbrodt, M.; Riedlinger, W.F.; Bartley, J.; Kaufmann, A.M.; Schneider, A.; Kohler, C. Estrogen and progestogen receptor positive endometriotic lesions and disseminated cells in pelvic sentinel lymph nodes of patients with deep infiltrating rectovaginal endometriosis: a pilot study. Hum Reprod 2008, 23, 2202–2209. [Google Scholar] [CrossRef] [PubMed]
- Sourial, S.; Tempest, N.; Hapangama, D.K. Theories on the pathogenesis of endometriosis. Int J Reprod Med 2014, 2014, 179515. [Google Scholar] [CrossRef] [PubMed]
- Lamceva, J.; Uljanovs, R.; Strumfa, I. The Main Theories on the Pathogenesis of Endometriosis. Int J Mol Sci 2023, 24. [Google Scholar] [CrossRef] [PubMed]
- Nisenblat, V.; Bossuyt, P.M.; Farquhar, C.; Johnson, N.; Hull, M.L. Imaging modalities for the non-invasive diagnosis of endometriosis. Cochrane Database Syst Rev 2016, 2, CD009591. [Google Scholar] [CrossRef]
- Parasar, P.; Ozcan, P.; Terry, K.L. Endometriosis: Epidemiology, Diagnosis and Clinical Management. Curr Obstet Gynecol Rep 2017, 6, 34–41. [Google Scholar] [CrossRef]
- Jamieson, D.J.; Steege, J.F. The prevalence of dysmenorrhea, dyspareunia, pelvic pain, and irritable bowel syndrome in primary care practices. Obstet Gynecol 1996, 87, 55–58. [Google Scholar] [CrossRef]
- Alkatout, I.; Mettler, L.; Beteta, C.; Hedderich, J.; Jonat, W.; Schollmeyer, T.; Salmassi, A. Combined surgical and hormone therapy for endometriosis is the most effective treatment: prospective, randomized, controlled trial. J Minim Invasive Gynecol 2013, 20, 473–481. [Google Scholar] [CrossRef]
- Vannuccini, S.; Clemenza, S.; Rossi, M.; Petraglia, F. Hormonal treatments for endometriosis: The endocrine background. Rev Endocr Metab Disord 2022, 23, 333–355. [Google Scholar] [CrossRef] [PubMed]
- Rzewuska, A.M.; Zybowska, M.; Sajkiewicz, I.; Spiechowicz, I.; Zak, K.; Abramiuk, M.; Kulak, K.; Tarkowski, R. Gonadotropin-Releasing Hormone Antagonists-A New Hope in Endometriosis Treatment? J Clin Med 2023, 12. [Google Scholar] [CrossRef]
- Chandra, V.; Kim, J.J.; Benbrook, D.M.; Dwivedi, A.; Rai, R. Therapeutic options for management of endometrial hyperplasia. J Gynecol Oncol 1015, 27, e8. [Google Scholar] [CrossRef] [PubMed]
- Pavone, M.E.; Bulun, S.E. Aromatase inhibitors for the treatment of endometriosis. Fertil Steril 2012, 98, 1370–1379. [Google Scholar] [CrossRef] [PubMed]
- Schindler, A.E. Dienogest in long-term treatment of endometriosis. Int J Womens Health 2011, 3, 175–184. [Google Scholar] [CrossRef]
- Sasagawa, S.; Shimizu, Y.; Nagaoka, T.; Tokado, H.; Imada, K.; Mizuguchi, K. Dienogest, a selective progestin, reduces plasma estradiol level through induction of apoptosis of granulosa cells in the ovarian dominant follicle without follicle-stimulating hormone suppression in monkeys. J Endocrinol Invest 2008, 31, 636–641. [Google Scholar] [CrossRef] [PubMed]
- Okada, A.; Sato, T.; Ohta, Y.; Buchanan, D.L.; Iguchi, T. Effect of diethylstilbestrol on cell proliferation and expression of epidermal growth factor in the developing female rat reproductive tract. J Endocrinol 2001, 170, 539–554. [Google Scholar] [CrossRef] [PubMed]
- Katsuki, Y.; Takano, Y.; Futamura, Y.; Shibutani, Y.; Aoki, D.; Udagawa, Y.; Nozawa, S. Effects of dienogest, a synthetic steroid, on experimental endometriosis in rats. Eur J Endocrinol 1998, 138, 216–226. [Google Scholar] [CrossRef] [PubMed]
- Tatsumi, H.; Kitawaki, J.; Tanaka, K.; Hosoda, T.; Honjo, H. Lack of stimulatory effect of dienogest on the expression of intercellular adhesion molecule-1 and vascular cell adhesion molecule-1 by endothelial cell as compared with other synthetic progestins. Maturitas 2002, 42, 287–294. [Google Scholar] [CrossRef] [PubMed]
- Horie, S.; Harada, T.; Mitsunari, M.; Taniguchi, F.; Iwabe, T.; Terakawa, N. Progesterone and progestational compounds attenuate tumor necrosis factor alpha-induced interleukin-8 production via nuclear factor kappa B inactivation in endometriotic stromal cells. Fertil Steril 2005, 83, 1530–1535. [Google Scholar] [CrossRef] [PubMed]
- Petraglia, F.; Hornung, D.; Seitz, C.; Faustmann, T.; Gerlinger, C.; Luisi, S.; Lazzeri, L.; Strowitzki, T. Reduced pelvic pain in women with endometriosis: efficacy of long-term dienogest treatment. Arch Gynecol Obstet 2011, 285, 167–173. [Google Scholar] [CrossRef] [PubMed]
- Momoeda, M.; Harada, T.; Terakawa, N.; Aso, T.; Fukunaga, M.; Hagino, H.; Taketani, Y. Long-term use of dienogest for the treatment of endometriosis. J Obstet Gynaecol Res 2009, 35, 1069–1076. [Google Scholar] [CrossRef] [PubMed]
- C. Shackleton, O.J. Pozo, J. Marcos, GC/MS in Recent Years Has Defined the Normal and Clinically Disordered Steroidome: Will It Soon Be Surpassed by LC/Tandem MS in This Role?, Journal of the Endocrine Society. 2 (2018) 974–996. [CrossRef]
- Schiffer, Lina et al. “Human steroid biosynthesis, metabolism and excretion are differentially reflected by serum and urine steroid metabolomes: A comprehensive review.” The Journal of steroid biochemistry and molecular biology vol. 194 (2019): 105439. [CrossRef]
- V. Rousson, D. Ackermann, B. Ponte, M. Pruijm, I. Guessous, C.H. D’Uscio, G. Ehret, G. Escher, A. Pechère-Bertschi, M. Groessl, P.-Y. Martin, M. Burnier, B. Dick, M. Bochud, B. Vogt, N.A. Dhayat, Sex- and age-specific reference intervals for diagnostic ratios reflecting relative activity of steroidogenic enzymes and pathways in adults, PLOS ONE. 16 (2021) e0253975. [CrossRef]
- Wickenheisser, Jessica K et al. “Human ovarian theca cells in culture.” Trends in endocrinology and metabolism: TEM vol. 17,2 (2006): 65-71. [CrossRef]
- Clark, B J et al. “The purification, cloning, and expression of a novel luteinizing hormone-induced mitochondrial protein in MA-10 mouse Leydig tumor cells. Characterization of the steroidogenic acute regulatory protein (StAR).” The Journal of biological chemistry vol. 269,45 (1994): 28314-22.
- N. Strushkevich, F. Mackenzie, T. Cherkesova, I. Grabovec, S. Usanov, H.-W. Park, Structural basis for pregnenolone biosynthesis by the mitochondrial monooxygenase system, Proceedings of the National Academy of Sciences. 108 (2011) 10139–10143. [CrossRef]
- M.S. Breen, D.L. Villeneuve, M. Breen, G.T. Ankley, R.B. Conolly, Mechanistic Computational Model of Ovarian Steroidogenesis to Predict Biochemical Responses to Endocrine Active Compounds, Annals of Biomedical Engineering. 35 (2007) 970–981. [CrossRef]
- Hall, P F. “Cytochromes P-450 and the regulation of steroid synthesis.” Steroids vol. 48,3-4 (1986): 131-96. [CrossRef]
- Dhayat, Nasser A et al. “Urinary steroid profiling in women hints at a diagnostic signature of the polycystic ovary syndrome: A pilot study considering neglected steroid metabolites.” PloS one vol. 13,10 e0203903. 11 Oct. 2018. [CrossRef]
- W.L. Miller, R.J. Auchus, The Molecular Biology, Biochemistry, and Physiology of Human Steroidogenesis and Its Disorders, Endocrine Reviews. 32 (2011) 81–151. [CrossRef]
- Murielle Bochud, Belen Ponte, Menno Pruijm, Daniel Ackermann, Idris Guessous, Georg Ehret, Geneviève Escher, Michael Groessl, Sandrine Estoppey Younes, Claudia H d’Uscio, Michel Burnier, Pierre-Yves Martin, Antoinette Pechère-Bertschi, Bruno Vogt, Nasser A Dhayat, Urinary Sex Steroid and Glucocorticoid Hormones Are Associated With Muscle Mass and Strength in Healthy Adults, The Journal of Clinical Endocrinology & Metabolism, Volume 104, Issue 6, June 2019, Pages 2195–2215. [CrossRef]
- Cedric H.L. Shackleton,Mass spectrometry in the diagnosis of steroid-related disorders and in hypertension research, The Journal of Steroid Biochemistry and Molecular Biology, Volume 45, Issues 1–3,1993,Pages 127-140,ISSN 0960-0760. [CrossRef]
- Islam MS, Afrin S, Jones SI, Segars J. Selective Progesterone Receptor Modulators-Mechanisms and Therapeutic Utility. Endocr Rev. 2020 Oct 1;41(5):bnaa012. [CrossRef] [PubMed] [PubMed Central]
- Ciloglu, E.; Unal, F.; Dogan, N.C. The relationship between the central serous chorioretinopathy, choroidal thickness, and serum hormone levels. Graefes Arch Clin Exp Ophthalmol 2018, 256, 1111–1116. [Google Scholar] [CrossRef]
- Leonhardt, S.A.; Edwards, D.P. Mechanism of action of progesterone antagonists. Exp Biol Med (Maywood) 2002, 227, 969–980. [Google Scholar] [CrossRef]
- Sitruk-Ware, R. New progestogens: a review of their effects in perimenopausal and postmenopausal women. Drugs Aging 2004, 21, 865–883. [Google Scholar] [CrossRef]
- Nielsen, J. S., Weinreb, R. N., Yannuzzi, L., & Jampol, L. M. Mifepristone treatment of chronic central serous chorioretinopathy. Retina (Philadelphia, Pa.). 27 (2007), 119–122. [CrossRef]
- Nielsen, Jared S MD*†; Jampol, Lee M MD*. Oral mifepristone for chronic central serous chorioretinopathy. Retina 31(9):p 1928-1936, October 2011. [CrossRef]
- C. Robin-Jagerschmidt, J.-M. Wurtz, B. Guillot, D. Gofflo, B. Benhamou, A. Vergezac, C. Ossart, D. Moras, D. Philibert, Residues in the Ligand Binding Domain That Confer Progestin or Glucocorticoid Specificity and Modulate the Receptor Transactivation Capacity, Molecular Endocrinology. 14 (2000) 1028–1037. [CrossRef]
- F. Cadepond, Phd, A. Ulmann, Md, Phd, E.-E. Baulieu, Md, Phd, RU486 (MIFEPRISTONE): Mechanisms of Action and Clinical Uses, Annual Review of Medicine. 48 (1997) 129–156. [CrossRef]
Figure 1.
This figure shows the optical coherence tomography (OCT) of the female patient: (a) This figure represents the infiltration of serous fluid from the choroid causing a small detachment of the Inner/outer Photoreception layer; (b) Reabsorption of serous fluid and resolution of detachment after interruption of treatment with estradiol valerate/dienogest.
Figure 1.
This figure shows the optical coherence tomography (OCT) of the female patient: (a) This figure represents the infiltration of serous fluid from the choroid causing a small detachment of the Inner/outer Photoreception layer; (b) Reabsorption of serous fluid and resolution of detachment after interruption of treatment with estradiol valerate/dienogest.
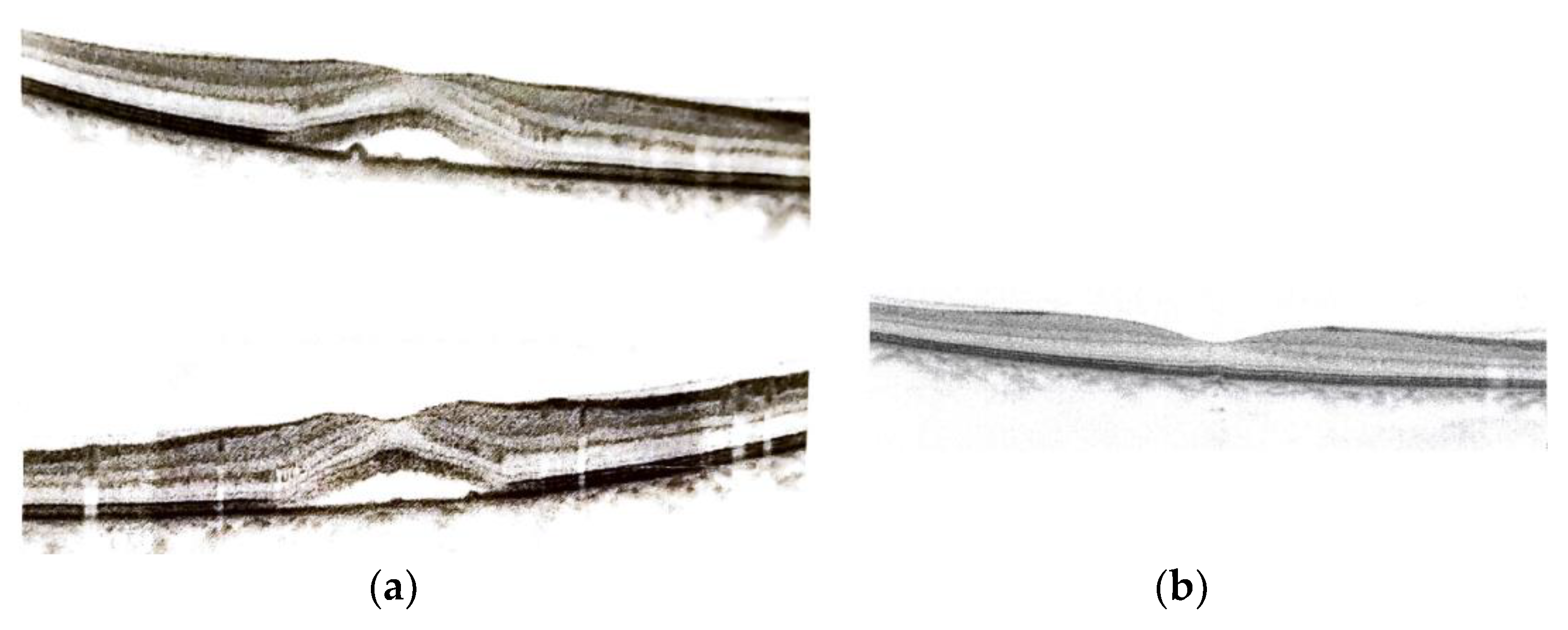
Figure 3.
This figure shows the ovarian theca cells and granulosa cells steroidogenesis (A). The excretion of steroids involved in endometriosis pathway (B). Abbreviation: cytochrome b5 (b5); cytochrome P450 oxidoreductase (POR); ferredoxin (FDX); ferredoxin reductase (FDXR); hexose-6-phosphate dehydrogenase (H6PDH); PAPS synthase 2 (PAPSS2); steroidogenic acute regulatory protein (StAR).
Figure 3.
This figure shows the ovarian theca cells and granulosa cells steroidogenesis (A). The excretion of steroids involved in endometriosis pathway (B). Abbreviation: cytochrome b5 (b5); cytochrome P450 oxidoreductase (POR); ferredoxin (FDX); ferredoxin reductase (FDXR); hexose-6-phosphate dehydrogenase (H6PDH); PAPS synthase 2 (PAPSS2); steroidogenic acute regulatory protein (StAR).
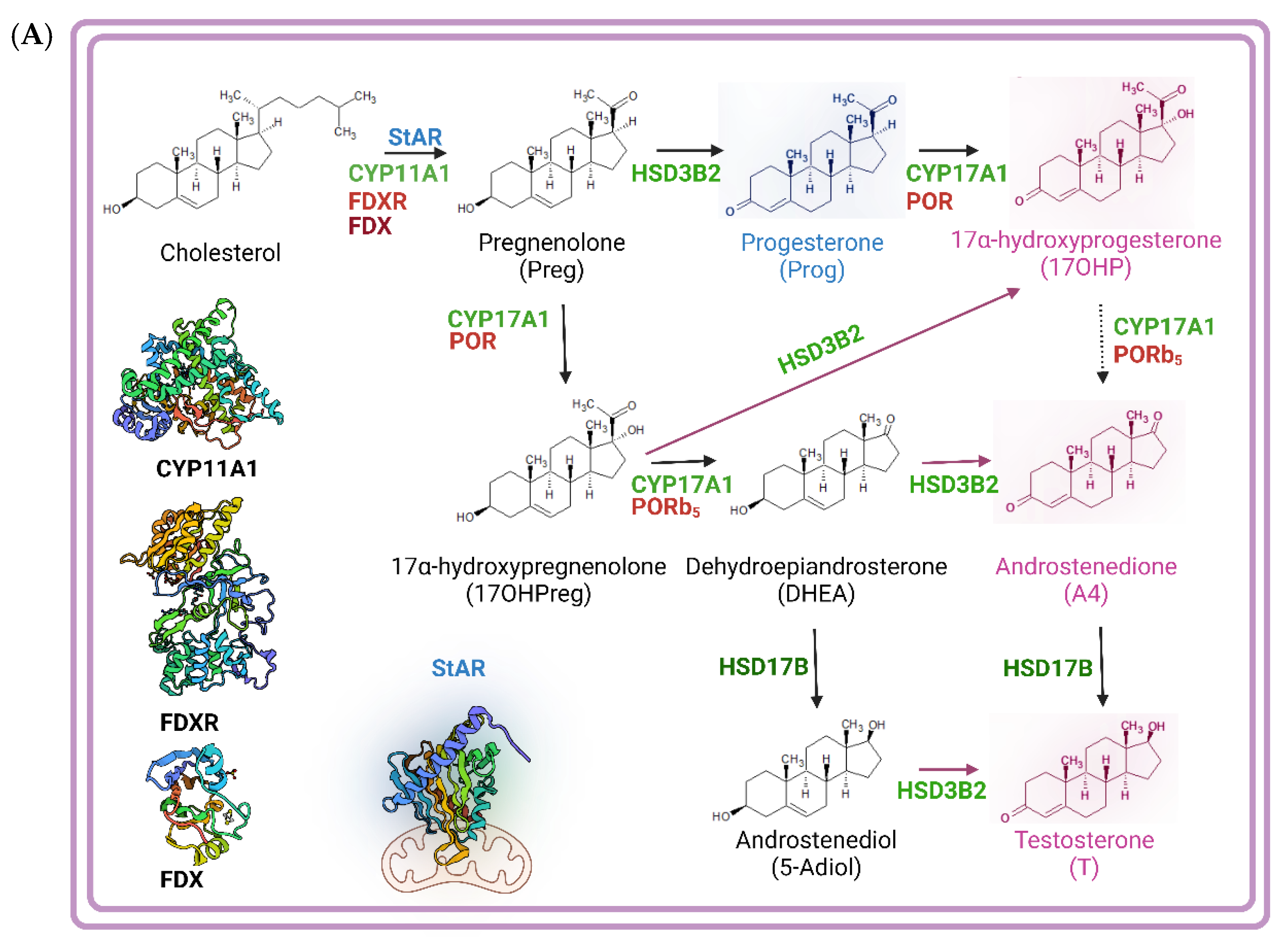
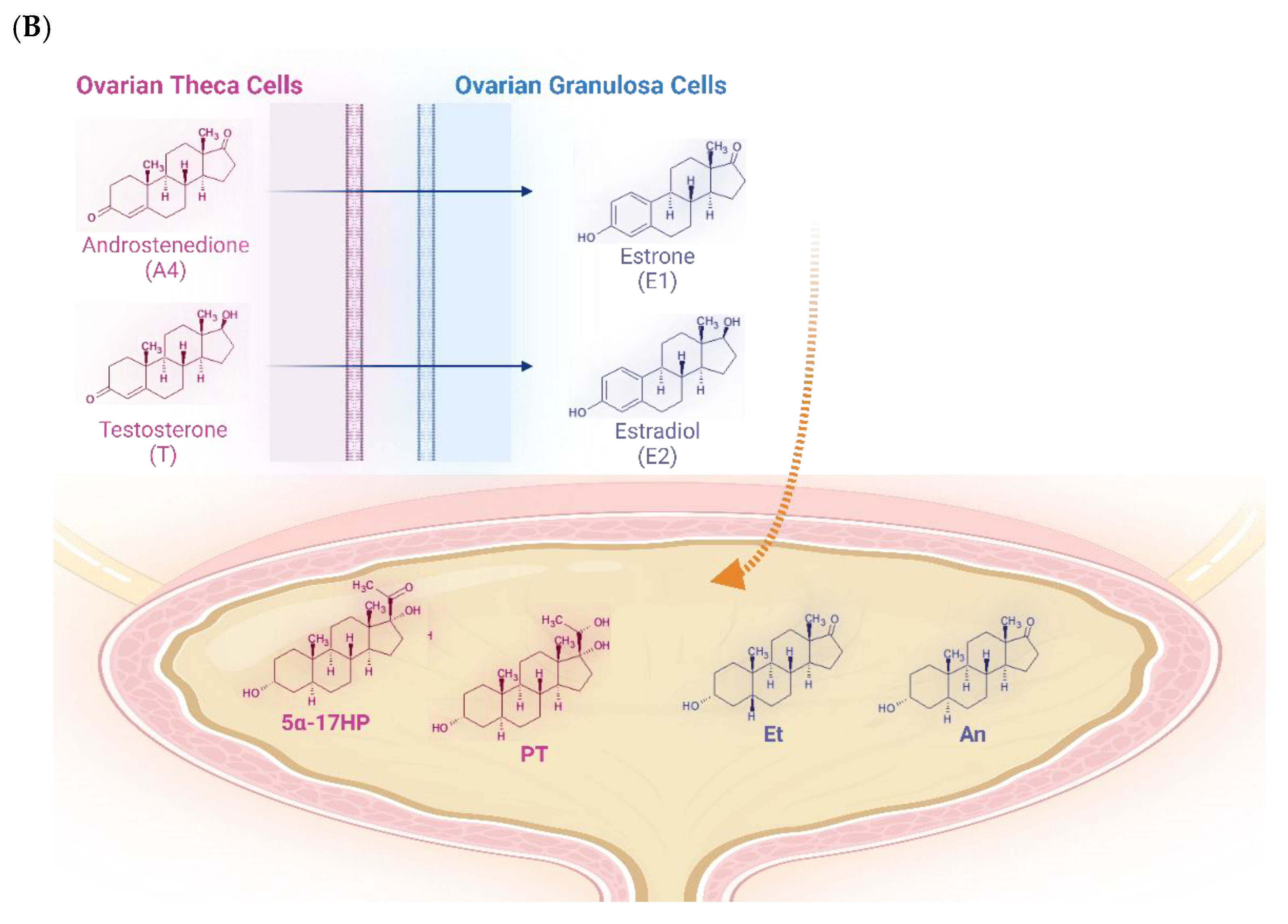

Table 1.
Composition of estradiol valerate/dienogest tablets depending on the days of the month.
| Day number | Estradiol valerate [mg] | Dienogest [mg] |
|---|---|---|
| 1-2 | 3.0 | 0.0 |
| 3-7 | 2.0 | 2.0 |
| 8-17 | 2.0 | 3.0 |
| 18-24 | 2.0 | 3.0 |
| 25-26 | 1.0 | 0.0 |
| 27-28 | 0.0 | 0.0 |
Table 2.
Diagnostic ratios of urinary steroid metabolites.
| Enzymes and pathways | Ratios | Value | Range |
|---|---|---|---|
| 17β-hydroxysteroid dehydrogenase (HSD17B) | 0.917 | 0.366 – 2.580 | |
| Alternative androgen backdoor pathway vs. classic pathway | 0.859 | 0.400 – 2.100 | |
| 5α-reductase deficiency | 1.164 | 0.470 – 2.400 | |
| 17,20-lyase Δ5-pathway deficiency | 3.480 | 0.028 – 1.880 | |
| 1.980 | 0.166 – 5.510 | ||
| 1.440 | 0.0229 – 1.870 | ||
| 0.670 | 0.0097 – 0.555 | ||
| P450c17 global Δ4 vs. Δ5-pathway | 15.21 | 0.147 -6.20 | |
| 8.65 | 1.08 – 20.4 | ||
| 0.025 | 0.0376 – 1.140 |
Abbreviations: ET, etiocholanone; AN, androsterone; DHEA, dehydroepiandrosterone; 16OHDHEA, 16α-hydroxy-dehydroepiandrosterone; d5P3, Pregnenetriol; 5ADIOL, androstenediol; 5ATRIOL, androstenetriol; 11OHA, 11β-hydroxy-androsterone; P2, Pregnanediol.
Table 3.
In first column are present the analyte and the ratio referred to E1 and [E1]/{[E2]+[E3]}, then N represented the number of subjects included in the study as control and in third column is reported the reference interval obtained by 2.5th-97.5th percentiles.
Table 3.
In first column are present the analyte and the ratio referred to E1 and [E1]/{[E2]+[E3]}, then N represented the number of subjects included in the study as control and in third column is reported the reference interval obtained by 2.5th-97.5th percentiles.
| Analyte or ratio | N | Reference interval |
|---|---|---|
| E1 | 36 | 2.00 – 15.00 |
| 36 | 0.20 – 3.50 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



