
Submitted:
17 December 2024
Posted:
18 December 2024
You are already at the latest version
Abstract
The blood-brain barrier (BBB) plays a crucial role in regulating the transport of solutes and essential nutrients into the brain. It maintains the homeostasis of the brain microenvironment, regulates nutrient transport, and prevents pathogens and neurotoxic substances from entering brain tissue. In recent years, increasing research has shown that BBB dysfunction plays a significant role in the pathophysiology of schizophrenia. Additionally, various MRI-based neuroimaging techniques have gradually been applied to study BBB permeability in schizophrenia. They may offer boundless potential for the in vivo assessment of brain structure and neurovascular function status, along with the evaluation of treatment efficacy in future schizophrenia patients. This article aims to synthesize evidence from postmortem, serum and cerebrospinal fluid biomarker, and neuroimaging studies, highlighting the alterations in BBB permeability among schizophrenia patients and their potential links to neuroinflammation and other factors. Moreover, it intends to deepen the understanding of schizophrenia pathophysiology, explore the BBB as a therapeutic target, and provide a basis for new antipsychotic drug development.
Keywords:
Schizophrenia
; Blood-brain barrier
; Neuroimaging
; MRI
; ASL
1. Introduction
Schizophrenia (SZ) is a psychiatric disorder characterized by evolving clinical symptoms and treatment challenges, affecting approximately 24 million people worldwide. It commonly manifests in adolescence or early adulthood, often with a gradual onset. Major clinical symptoms include delusions, hallucinations, affective blunting, social withdrawal, and cognitive deficits[1]. Despite decades of research on the pathophysiological basis of schizophrenia, its fundamental pathogenic mechanisms remain unclear.
Genome-wide association studies (GWAS) indicate that schizophrenia has a polygenic basis, including some rare variants with significant effects[2] and hundreds of common genetic variants with small effects[3]. Genetic risk is more predictive of schizophrenia when adverse factors are present early in development. Therefore, schizophrenia is a complex disorder, with its onset and progression arising from the combined influence of genetic susceptibility and environmental factors[4,5]
The brain is well-known as a high-energy and high-oxygen-demanding organ. To meet these requirements, it requires substantial blood supply, resulting in the synchronous development of vascular and neural networks[6]. The total surface area of microvessels in the brain is approximately 150–200 cm²/g of tissue, equivalent to about 15–20 m² for the entire adult brain, forming a dense vascular network supplying blood flow to all brain regions[7]. Given the lack of regenerative ability in neurons, maintaining the stability of the central nervous system (CNS) environment is crucial for both optimal synaptic transmission and safeguarding neuronal health and integrity. Consequently, the brain vasculature varies from other body regions because of the existence of the blood-brain barrier (BBB), which is seen as the brain’s primary safeguard against potentially noxious substances. Recently, the BBB has emerged as a key dynamic interface for the brain and a key focus in the research on the pathogenesis of various CNS disorders.
Current studies have revealed that alterations in blood-brain barrier (BBB) function are central to the pathophysiology of many central nervous system (CNS) diseases, including stroke, demyelinating diseases, epilepsy, and dementia. However, the role of the BBB in psychiatric disorders has received relatively scant attention. With the progress in understanding the pathophysiological mechanisms of these disorders and the ongoing improvement for detecting BBB impairment, research in this field has gradually increased. In this review, the authors aim to explore the evidence for BBB impairment in SZ, from autopsy studies, cerebrospinal fluid and blood biomarkers , as well as the neuroimaging research. Moreover, the mechanisms including CLDN5 protein and neuroinflammation that lead to BBB permeability alterations in SZ are analyzed, along with the reciprocal impacts of antipsychotic drugs on BBB permeability. This review endeavors to deepen the comprehension regarding the role of BBB permeability alterations in schizophrenia's pathogenesis, diagnosis, and treatment.
2. Structure and Function of the Blood-Brain Barrier
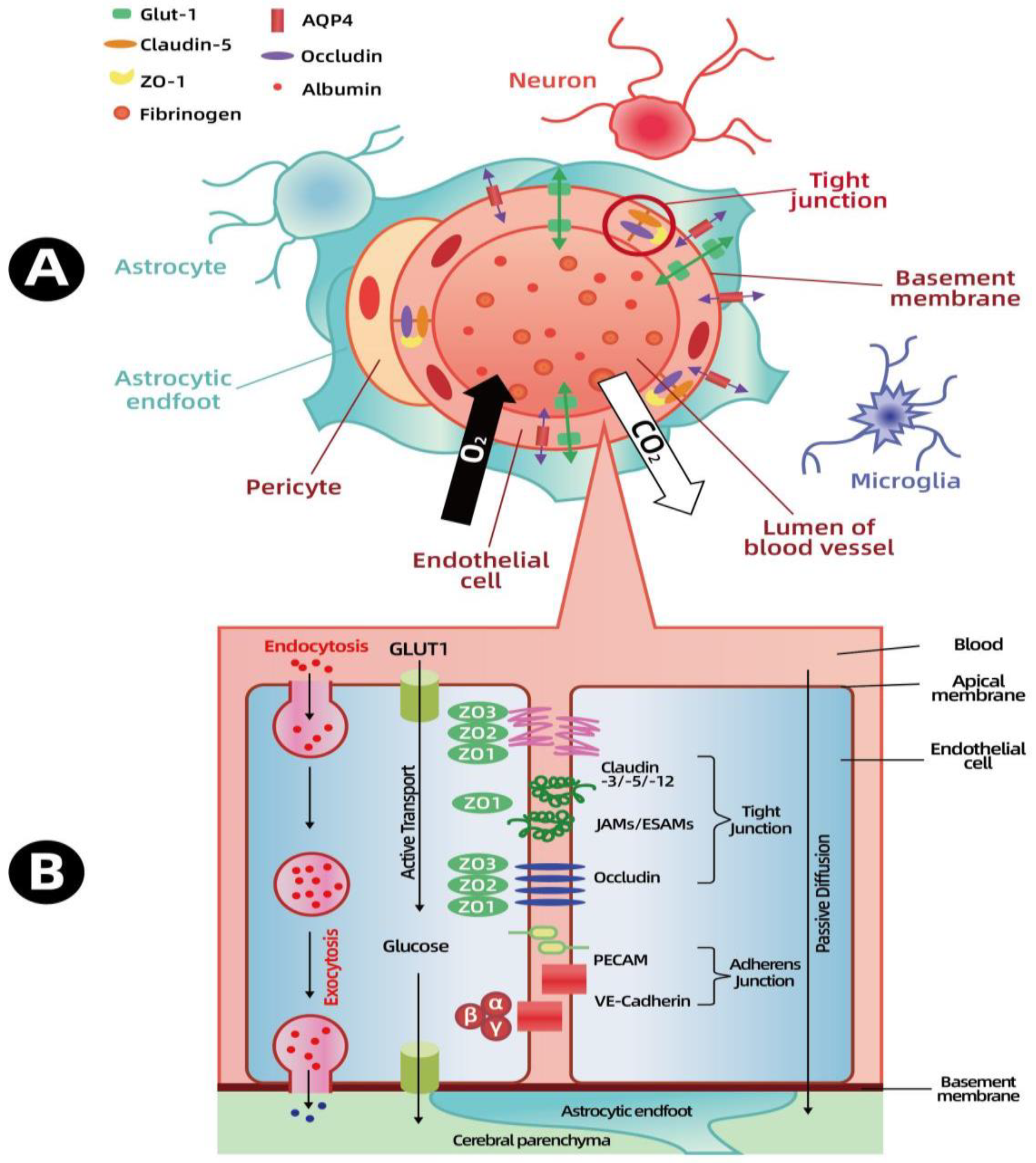
The BBB, which surrounds the central nervous system, is among the few highly selective and tightly regulated barriers, demonstrating the brain's critical role in cognitive function, homeostasis, and the coordination of peripheral organ functions. The BBB, a part of the neurovascular unit (NVU), represents a complex structure comprising diverse cell types , including neurons, astrocytes, microglia, pericytes, and brain microvascular endothelial cells (see Figure 1A). The cell types within the NVU cooperate to ensure a steady blood supply to the brain, a process termed autoregulation. Whenever neuronal activation results in augmented metabolic demand, cerebral blood flow promptly increases[8]. In the process of fulfilling such functions, the BBB is of essential significance in maintaining the brain’s microenvironmental homeostasis. By means of tight junctions among endothelial cells, receptor- and transporter-mediated protein and peptide transportation, and transcytosis across endothelial cells, the BBB regulates the interchange of ions and nutrients between the blood and the brain. It also protects vulnerable neural tissue from potentially hazardous blood-borne substances such as pathogens, immune cells, and bradykinin[9]. Additionally, brain endothelial cells secrete approximately 200 milliliters of new interstitial fluid daily, contributing to maintain an optimal ionic environment essential for normal neural function[10]
The junctional complexes, which encompass adherens junctions and tight junctions, are located within the gaps between brain microvascular endothelial cells. Alongside the basement membrane, pericytes, and astrocyte end-feet which form the glial limiting membrane, these complexes construct the blood-brain barrier (BBB), confining its permeability[6]. Adherens junctions consist of cadherin and catenin proteins spanning the endothelial cell gaps. Catenins further bind to cytoskeletal proteins, linking cells and regulating intercellular connections. Although the exact role of adherens junctions remains not fully understood, they are believed to contribute to maintaining cell polarity, providing stability, promoting endothelial cell survival, and responding to stimuli via interactions with cadherin or catenin proteins and the actin cytoskeleton[11]. Unlike adherens junctions distributed throughout all vascular beds, tight junctions are significantly enriched in the cerebral microvascular endothelium. Tight junctions span the intercellular spaces and interact with tight junction proteins on adjacent endothelial cells at the "contact points" , thereby sealing the intercellular space [12]. The binding of tight junction proteins hinders the flow of solutes and ions between the blood and the brain, thus forming a dynamic and highly regulatable barrier system. Tight junctions are mainly composed of claudins and occludin, which are connected to the actin cytoskeleton through zonula occludens (ZO) proteins [13]. The presence of tight junctions restricts the intercellular permeability and maintains cell polarity by achieving the asymmetric distribution of membrane components [14].
In addition to endothelial cells, pericytes, astrocytes, and the basement membrane (BM) are also essential elements in maintaining the function and integrity of the blood-brain barrier (BBB). The presence of astrocytic end-feet encircling blood vessels is a distinctive characteristic of the brain vasculature, emerging during the development of the BBB. Astrocytes can partly activate the barrier function of endothelial cells and are significant in BBB maintenance. Studies have indicated that the existence of astrocytes is one of the prerequisites for the formation and maturation of tight junctions (TJs) between brain endothelial cells[15,16]. Moreover, astrocytes secrete several regulatory factors ,including TGF-β, GDNF, bFGF, and IL-6[17].The basement membrane is a specialized extracellular matrix. Its biological activity is vital for the growth, development, differentiation, and functional maintenance of endothelial cells. Composed mainly of fibronectin (FN), type IV collagen, laminin (LN) linked to collagen, and proteoglycans, the basement membrane helps to position cells and establishes connections among endothelial cells, astrocytes, and pericytes. It also functions as an additional barrier to solute movement prior to entering neural tissue [18].. Damage to the basement membrane gives rise to dysregulation of tight junction protein expression on endothelial cells,leading to changes in blood-brain barrier permeability[19].
Pericytes are mural cells embedded in the basement membrane and surround the blood vessels of the central nervous system (CNS) during embryonic development. They are essential for the establishment of the blood-brain barrier (BBB) and are attracted to endothelial cells by the paracrine signaling of platelet-derived growth factor β (PDGFβ) and its receptor (PDGFRβ). Indeed, PDGFβ and PDGFRβ knockout mice die at the embryonic stage, exhibiting tight junction dysfunction and enhanced vascular permeability as a result of the absence of pericyte coverage. Pericytes modulate BBB permeability by governing the expression of tight junction proteins and adherens junction proteins. In addition, pericytes can engage in immune responses with macrophage-like activity. They express scavenger receptors, and cultured pericytes possess the capacity to phagocytose large molecules like polystyrene beads.Unfortunately,the role of pericytes in psychiatric disorders has not been thoroughly investigated thusfar[20,21,22]
3. Methodology-Based Studies on Blood-Brain Barrier Permeability in Schizophrenia
3.1. Post-Mortem Studies
Postmortem studies have been progressively carried out, mainly centering on structural and morphological abnormalities, alterations in molecular marker expression, gene expression patterns and immunological abnormalities. However, these studies are frequently constrained by small sample sizes, inadequate control group matching, potential confounding impacts of medications, variations in sample preservation conditions, and biases arising during brain tissue processing, all of which could detrimentally affect the results.
Structural and Morphological Anomalies: In the prefrontal cortex and visual cortex of patients with schizophrenia, morphological distinctions in capillaries and NVU (neurovascular unit) cell types have been noted, along with endothelial cell vacuolation, astrocytic endfoot thickening, and basal membrane thickening [23].Subsequent studies have found that a decrease in capillary density correlates with the negative symptoms of schizophrenia [24]. Structural abnormalities of varying extents have also been witnessed in the brains of schizophrenia patients under antipsychotic treatment, such as reduced capillary diameter, extracellular matrix deposition, perivascular edema, and endothelial cell vacuolation [25].However, this particular study only encompassed three patients on antipsychotic treatment. Other studies have pointed to abnormalities in other NVU components, particularly astrocytes. A diminished number of oligodendrocytes surrounding capillaries in the prefrontal cortex of schizophrenia patients has been reported [26]. Moreover, a decreased quantity of glial fibrillary acidic protein (GFAP)-positive astrocytes around blood vessels has been observed in the prefrontal cortex , hippocampus ,and anterior cingulate cortex of schizophrenia patients [27,28]. The extent to which these anomalies influence blood-brain barrier function remains unclear.
Altered Expression of Molecular Markers: A study employed immunohistochemical techniques to assess P-glycoprotein expression in the brains of 13 patients with schizophrenia and 9 healthy controls. They found no substantial differences in the the density of P-glycoprotein-expressing capillaries in most regions; however, a decreased capillary density was observed in the habenula of schizophrenia patients. Neurons in the habenula also express P-glycoprotein, and schizophrenia patients showed a reduced density of P-glycoprotein-expressing neurons[29]. Another study reported a significant reduction of claudin-5 in the hippocampus of schizophrenia patients. Moreover, the mRNA and protein levels of claudin-5, claudin-12, and ZO-1 were found to be associated with the age of onset and the duration of schizophrenia [30].
Gene Expression Abnormalities: A study performed single-nucleus RNA sequencing on midbrain tissues from 15 psychiatric patients and 14 healthy controls. The results indicated no alterations in the relative abundance of major blood-brain barrier (BBB) cell types associated with schizophrenia, nor were there any alterations in subpopulations linked to the disorder. However, 14 differentially expressed genes were identified in BBB cells of schizophrenia patients compared to controls, including previously implicated schizophrenia-related genes such as FOXP2 and PDE4D. These transcriptional changes were restricted to ependymal cells and pericytes, suggesting that such alterations are not widespread in schizophrenia [31]
Considering the diverse causes and symptom presentations in schizophrenia (SZ), researchers utilized a statistical approach to analyze gene expression variability. Their analysis revealed a general increase in gene expression variability across SZ brains, with VEGFA emerging as the most variably expressed gene compared to controls [32]. This discovery provides a unifying explanation for the inconsistent findings across studies regarding VEGF's involvement in SZ. The variability in VEGF expression among individuals with SZ suggests it may play distinct roles at different stages of the disease.
BAI3 (Brain-specific Angiogenesis Inhibitor 3) plays a critical role in the process of angiogenesis[33].Recent postmortem findings revealed a male-specific decrease in hippocampal BAI3 expression among SZ patients, based on an analysis of 104 SZ cases and 174 controls[34] ..
Immunological Abnormalities: A postmortem study quantitatively evaluated the presence of lymphocytes in the brain parenchyma of schizophrenia patients. The study detected significant infiltration of CD3+ T lymphocytes and CD20+ B lymphocytes in the hippocampal region in residual and paranoid schizophrenia, but no correlation with disease duration was observed [35]. Another study, which partially concurs with these findings, investigated IgG levels in the brain parenchyma of schizophrenia patients. It showed elevated IgG levels in the temporal cortex surrounding the hippocampus and in the hippocampus itself compared to controls, suggesting increased BBB permeability in these regions. Additionally, blood-brain barrier dysfunction in schizophrenia patients was more conspicuous in older and male individuals [36]。
A study categorized schizophrenia (SZ) postmortem cases into high-inflammation and low-inflammation subtypes based on inflammatory cytokine transcript levels in brain tissue. The SZ-high-inflammation group displayed significantly elevated midbrain ICAM and macrophage marker CD163 expression compared to controls, while no differences were observed in the SZ-low-inflammation group[37]. Further analysis of dorsolateral prefrontal cortex (DLPFC) endothelial transcripts revealed altered expression of key blood-brain barrier (BBB) markers in the SZ-high-inflammation group, including increased CDH5 and OCLN and decreased ABCG2.Additionally,SZ-high-inflammation samples exhibited increased ICAM1 expression and a higher number of CD163+ macrophages. These findings suggest that neuroinflammation, endothelial dysfunction, increased BBB permeability, and greater peripheral macrophage infiltration are associated with the high-inflammation SZ subtype. Importantly, ICAM and other BBB gene expressions in cultured brain endothelial cells were not affected by therapeutic doses of antipsychotics[38].
SERPINA3 has anti-angiogenic and anti-inflammatory effects on endothelial cells, and its expression is increased in the cerebral cortex of SZ patients in postmortem analyses [39]. Recent studies have verified the elevated expression of SERPINA3 in SZ patients, with even higher levels observed in the high-inflammation SZ group. Immunostaining revealed that blood vessel-associated astrocytes are the primary source of increased SERPINA3 expression in the high-inflammation SZ group. This upregulation may constitute a compensatory response to chronic inflammation in SZ patients[40] . SERPINA3 inhibits the catalytic activity of leukocyte elastase, an enzyme that cleaves ICAM1 and facilitates leukocyte adhesion to endothelial cells. Therefore, the increased SERPINA3 expression in blood vessel-associated astrocytes of the high-inflammation SZ group may act in concert with CD163+ CNS infiltration [38].
3.2. Peripheral and Cerebrospinal Fluid Markers
The gold standard for assessing BBB permeability in humans is the cerebrospinal fluid (CSF) to serum albumin ratio (QAlb). This test evaluates BBB permeability by comparing the concentration of albumin in CSF and blood. Albumin concentration in CSF is typically about 200 times lower than in blood; thus, an elevated QAlb indicates increased albumin leakage from blood into CSF due to barrier damage. This test has been utilized in several psychiatric studies to assess BBB dysfunction [41]. In a study involving 63 psychiatric patients and 4100 controls, some psychiatric patients (14 with major depressive disorder and bipolar disorder, and 14 with schizophrenia) showed abnormal CSF reflecting altered BBB permeability, primarily characterized by increased QAlb levels [42]. BBB dysfunction is also observed in various forms of dementia, including Alzheimer’s disease and frontotemporal dementia, with elevated QAlb levels reported in these patients [43]. A recent study compared 104 first-episode psychosis (FEP) patients with 104 healthy controls regarding CSF white blood cell (WBC) counts, total protein, IgG index, and CSF/serum albumin ratio. The results demonstrated increased CSF/serum albumin and CSF/serum IgG ratios in schizophrenia patients compared to controls. More patients in the psychosis group had CSF WBC > 3 cells/µl compared to controls, along with elevated serum leukocyte counts and neutrophil-to-lymphocyte ratios. This suggests that increased BBB permeability, elevated CSF WBC levels, and enhance peripheral inflammation are present when comparing a large sample of psychosis patients to healthy controls[44] . Reduced levels of vitamin B12 and folate can increase homocysteine levels, potentially contributing to BBB alterations. Using this as a basis, researchers analyzed routine CSF and blood parameters in a cohort of first-episode psychosis (FEP) patients to investigate the relationship between vitamin B12/folate deficiency and BBB disruption. The study found that 17.1% (38/222) of patients had elevated CSF/serum albumin ratios (QAlb), 29.3% (62/212) had white matter lesions, and 17.6% (39/222) exhibited reduced vitamin B12 or folate levels. However, no statistically significant association was identified between vitamin deficiency and QAlb changes [45]. In subsequent research, the relationship between CSF changes and C-reactive protein (CRP) levels was analyzed. Among the cohort, 41.4% of patients had elevated CRP levels, but no significant association was found between CRP and QAlb changes [46]. However, analyzing QAlb has limitations, as its elevation may be caused by other factors, including a reduced CSF production rate, increased subarachnoid space flow resistance, or impaired outflow due to arachnoid villi blockage. Additionally, this method is invasive and less practical for schizophrenia patients. Furthermore, QAlb is not a specific indicator and is vulnerable to influences such as CSF production and circulation, making it an unreliable measure of BBB permeability.
The calcium-binding peptide S100β is mainly produced by astrocytes and oligodendrocytes and is abundantly expressed in neurons and meninges in the brain. In healthy individuals, S100β is scarcely detectable in serum. Consequently, elevated serum S100β concentrations have been used to associate central nervous system (CNS) disorders, such as traumatic brain injury, with BBB dysfunction [47]. A growing number of studies have reported elevated S100β levels in the blood, cerebrospinal fluid (CSF), and brain tissues of schizophrenia patients [48,49]. Moreover, plasma S100β levels positively correlate with negative symptoms[50,51] and cognitive deficits [52] associated with schizophrenia. A meta-analysis revealed that S100β concentration positively correlates with positive symptoms and is related to the course of psychosis, suggesting the possibility that BBB permeability increases as the psychiatric disorder progresses [47]. However, it remains unclear whether the increase in S100β directly reflects enhanced BBB permeability or merely indicates increased production and/or secretion of glial cells or glial degeneration [53]. Additionally, S100β has been found to be secreted by adipose tissues outside the CNS, casting doubt on the interpretation and validity of S100β as a marker for BBB permeability[54] .
Molecules associated with neurodegeneration, such as spectrin breakdown products 120 (SBDP120), 145 (SBDP145), and 150 (SBDP150), claudin, occludin, and ubiquitin C-terminal hydrolase-L1 (UCHL1), have been reported to be related to the blood-brain barrier (BBB). A study evaluated the levels of these peripheral biomarkers in healthy controls and two groups of schizophrenia patients (one receiving typical and atypical antipsychotic treatments and the other receiving only atypical antipsychotic treatment). The results showed that in schizophrenia patients treated with atypical antipsychotics, the levels of SBDP145 and cullin (a ubiquitin ligase) were significantly higher than those in the control group. In the combined treatment group, SBDP150 levels were lower than those in the control group (p = 0.022). Levels of claudin, occludin, and UCHL1 were similar between the two groups. Among patients receiving combined treatment, SBDP145 levels positively correlated with the total SAPS scores and SAPS delusion subscores. This study represents the first investigation examining the relationship between schizophrenia and BBB damage through the measurement of SBDP145, SBDP150, UCHL1, cullin, occludin, and claudin [55]
The endothelial glycocalyx (GLX) serves as a protective layer in the blood-brain barrier (BBB), and its degradation can lead to BBB dysfunction.A study utilized immunoblotting to measure 11 GLX biomarkers in the peripheral blood of first-episode schizophrenia patients and healthy controls.Compared to healthy controls, three GLX biomarkers were significantly elevated in patients.Moreover, the increase in GLX biomarkers was associated with symptom severity.This study demonstrated the potential of GLX molecules as immunoneuropsychiatric biomarkers for the early diagnosis of psychosis,Further research is needed to explore the role of GLX in the early detection of psychotic disorders[56]
3.3 Neuroimaging Studies
In previous studies, neuroimaging has primarily focused on structural brain changes in schizophrenia patients, with consistent findings across multiple studies. Numerous studies have confirmed volume reductions in the medial temporal lobe (related to memory) and the left posterior superior temporal gyrus (involved in auditory processing and language), as well as ventricular enlargement in schizophrenia patients [57]. However, using neuroimaging techniques to evaluate BBB changes in schizophrenia patients are limited, and a few early studies were hindered by small sample sizes, difficulties in result interpretation, and technical limitations. A magnetic resonance imaging (MRI) study using a 7T scanner reported changes in the volume of small arteries and arterioles in the brain's vasculature, suggesting widespread microvascular abnormalities throughout the brain [58], potentially explaining the reduced gray matter volumes associated with schizophrenia. This study was based on previous findings of cerebral blood flow (CBF) and cerebral blood volume (CBV) abnormalities in schizophrenia [59]. Given the focus on smaller blood vessels, these findings may be relevant to BBB function. Advances in dynamic contrast-enhanced magnetic resonance imaging (DCE-MRI), a technique for quantitatively assessing BBB permeability, may facilitate the detection of subtle BBB abnormalities. A recent study utilizing this technology compared structural MRI and DCE-MRI data from 29 schizophrenia patients and 18 controls. The results revealed that schizophrenia patients exhibited higher Ktrans values bilaterally in the thalamus compared to healthy controls. The mean Ktrans value in the thalamus was significantly positively correlated with disease duration and symptom severity. Subregional analysis of the thalamus demonstrated pronounced BBB disruption in the pulvinar nucleus, particularly in the medial and lateral thalamic nuclei. Furthermore, Ktrans values across the whole brain, thalamus, and thalamic subregions were negatively correlated with their respective volumes [60].
Arterial Spin Labeling (ASL) perfusion imaging is a non-invasive technique for measuring cerebral blood flow. ASL magnetically labels water protons in arterial blood before they enter the target tissue, enabling the calculation of Kw (water exchange rate), Psw (water permeability surface area product), and CBF (cerebral blood flow) after imaging to assess water exchange across the blood-brain barrier (BBB). Water, as an abundant endogenous tracer that cannot freely pass through the BBB and has a relatively small molecular weight, can detect subtle BBB damage at early stages of disease progression. This provides a more direct and sensitive imaging marker for the BBB during the initial phases of disease. Due to its sensitivity, non-invasiveness, short scan time, and high repeatability, ASL has become a key technique for studying BBB permeability. Various ASL-related sequences, such as Intrinsic Diffusivity Encoding of Arterial Labeled Spin (IDEALS), Multi-TE ASL, Diffusion-weighted ASL, Magnetization Transfer Weighted ASL, Contrast-enhanced ASL, and Phase-contrast ASL, have been developed and widely applied in studies involving animals, healthy populations, stroke, Alzheimer's disease (AD), small vessel disease, obstructive sleep apnea (OSA), multiple sclerosis (MS), tumors, and other conditions. Recently, researchers employed DP-ASL technology to measure water exchange (Kw) between brain capillaries and neurons in schizophrenia patients to evaluate changes in BBB permeability. Meanwhile, brachial artery flow-mediated dilation was used to assess peripheral vascular endothelial cell health, exploring the relationship between whole-brain Kw and endothelial function. The study revealed a significantly reduced mean whole-brain Kw in the patient group, with decreased neurovascular water exchange in the right parietal lobe, particularly in the supramarginal gyrus and postcentral gyrus. Additionally, reduced Kw in the right superior corona radiata and angular gyrus was associated with negative symptoms. Schizophrenia patients (SSD) also exhibited significantly impaired peripheral vascular endothelial cell function; in the healthy control (HC), 94% of brain regions showed a positive correlation between Kw and peripheral endothelial function, whereas in the SSD group, 52% of brain regions displayed a negative correlation [61]. Studies on DP-ASL and DCE-MRI have made real-time, in vivo observation of BBB permeability possible, though the mechanisms of Kw and Ktrans may differ. Reduced Kw may mainly reflect impaired water transport across neurovascular units, indicating subtle early changes in the BBB, potentially related to aquaporin-4 (AQP-4) function. In contrast, Ktrans may represent abnormal passive permeability of water or macromolecules through the endothelium.
Certain central nervous system diseases, including epilepsy, are associated with upregulation of P-glycoprotein function, which may represent a compensatory mechanism triggered by blood-brain barrier permeability damage. A PET study attempted to quantify the function of blood-brain barrier transporters in vivo. The authors used radiolabeled verapamil ([¹¹C]) as a probe to assess P-glycoprotein function and distribution in a small sample of schizophrenia patients. Compared to healthy controls, decreased uptake of [¹¹C]verapamil was observed in the temporal cortex, basal ganglia, and amygdala, indicating enhanced P-glycoprotein activity [62].
4. Mechanistic Studies on Blood-Brain Barrier Abnormalities in Schizophrenia
Currently, research into the mechanism of blood-brain barrier injury remains at the exploratory stage. In recent years, numerous studies have predominantly centered on neuroinflammation, dysfunctions of the neurovascular unit, and tight junction leakage, among other aspects.
The BBB and immune response in schizophrenia: As a part of the pathophysiology of schizophrenia, neuroinflammation is increasingly regarded as a significant factor in the pathogenesis of schizophrenia. Human and animal studies have shown that schizophrenia-related neuroinflammation can disrupt neurovascular function, leading to impaired blood-brain barrier function.[63] , and its main pathways involve microglial activation and proliferation (MAP), upregulation of matrix metalloproteinases (MMPs), upregulation of pro-inflammatory cytokines, and activation and apoptosis of astrocytes.
Excessive microglial activation is associated with the pathophysiology of schizophrenia. Postmortem studies of the brains of schizophrenia patients consistently demonstrate elevated microglial activation, including increased HLA-DR immunoreactivity in multiple regions, particularly the dorsolateral prefrontal cortex, superior temporal cortex, and anterior cingulate cortex, compared with healthy controls [64,65]. In the hippocampal regions of some schizophrenia patients, the enrichment of CD3+ T lymphocytes, CD20+ B lymphocytes, and HLA-DR-expressing microglia has been observed[35]. Excessive microglial activation disrupts the tight junction proteins of BBB endothelial cells and increases BBB permeability through various mechanisms, including the activation of inducible nitric oxide synthase, promotion of reactive oxygen species (ROS) synthesis, induction of COX2 expression within the neurovascular unit, and upregulation of pro-inflammatory cytokines and matrix metalloproteinases. Increased BBB permeability may, in turn, enhance interactions between innate brain immunity and peripheral adaptive immunity, perpetuating microglial activation and pro-inflammatory cytokine synthesis in the brain through a positive feedback loop [63].
Matrix metalloproteinase-9 (MMP9) is a 92 kDa protein that belongs to the family of zinc- and calcium-dependent endopeptidases. Studies have found elevated concentrations of MMP9 and tissue inhibitors of metalloproteinases (TIMP) in schizophrenia patients [66,67]. The primary mechanism by which MMP9 negatively impacts the central nervous system (CNS) likely involves its participation in immune-inflammatory responses. This includes the activation and regulation of various cytokines and chemokines, leading to the disruption of the blood-brain barrier (BBB). The resulting BBB breakdown allows leukocytes to infiltrate brain tissue, thereby exacerbating the adverse effects of neuroinflammation on the brain. However, the relationship between MMP9 upregulation, lipid peroxidation, and BBB disruption in schizophrenia patients remains uncertain.
Due to the enhanced "immune privilege" status conferred by the blood-brain barrier (BBB), alterations in BBB components such as cell adhesion molecules and vascular endothelial growth factors (VEGF) may increase the infiltration of peripheral immune cells into the brain. A few studies have examined BBB components in the peripheral blood of patients, and several have shown that untreated acute schizophrenia patients exhibit increased peripheral concentrations of endothelial cell adhesion molecules, such as P-selectin and L-selectin, in their serum and plasma compared to controls [68,69]. Changes in vascular endothelial growth factor (VEGF), intercellular adhesion molecule-1 (ICAM-1), and vascular cell adhesion molecule-1 (VCAM-1) levels have also been observed in schizophrenia patients [70]. A recent study reported elevated serum VEGF levels in schizophrenia patients, which were associated with structural abnormalities in the prefrontal cortex [71]. The accumulation of vascular endothelial factors may contribute to increased transendothelial migration of inflammatory mediators, facilitating the aggregation of peripheral immune cells in the central nervous system and thereby inducing a neuroinflammatory state. This condition can lead to endothelial cell activation, subsequently resulting in abnormal BBB permeability.
A study has shown that the levels of pro-inflammatory cytokines in the blood and cerebrospinal fluid of schizophrenia patients are significantly elevated, with cytokine levels decreasing after the resolution of psychotic symptoms. Neuroinflammation activates microglial cells, which subsequently secrete cytokines such as interleukin (IL)-1α, IL-1β, IL-6, and tumor necrosis factor (TNF)-α, thereby impairing the endothelial function of the blood-brain barrier (BBB)[72]. The primary mechanisms by which pro-inflammatory cytokines contribute to BBB disruption may include inducing the expression of intercellular adhesion molecule-1 (ICAM-1) and vascular cell adhesion molecule-1 (VCAM-1) on the luminal surface of BBB endothelial cells, thereby promoting the transendothelial migration of lymphocytes and monocytes; causing oxidative damage to endothelial cells by impairing mitochondrial oxidative metabolism in vascular endothelial cells; and directly damaging the tight junctions of endothelial cells.
Astroglia regulate cerebral blood flow and volume as well as BBB permeability, among many other critical functions [73]. Therefore, in schizophrenia, there is a recorded reduction in the number of astroglia within functionally significant regions, including the subgenual cingulate, anterior, dorsolateral, and prefrontal cortices, along with the hippocampus and corpus callosum[65].Aquaporin 4 (AQP4), a bidirectional water channel predominantly expressed at the perivascular endfeet of astrocytes, is crucial for BBB development, integrity, and intracerebral water homeostasis. A significant reduction in AQP4 expression in the deep layers of the anterior cingulate cortex in schizophrenia patients has been confirmed [74]. Reduced AQP4 expression may impair astrocyte-endothelial interactions, resulting in neurovascular dysfunction and increased BBB permeability [75]. The pathological mechanism by which altered AQP4 expression impacts glial cell function and damages the BBB in schizophrenia patients requires further investigation.
A comprehensive review of the aforementioned studies suggests that neuroinflammation may contribute to the behavioral and cognitive symptoms of schizophrenia through multiple mechanisms. These mechanisms include disrupting the integrity of the blood-brain barrier (BBB), reducing cerebral blood flow, and disturbing the dynamic balance of the brain's microenvironment. Furthermore, BBB disruption may exacerbate interactions between the brain's innate immune system and the peripheral adaptive immune system, leading to chronic harmful neuroimmune signaling and neuroinflammatory responses. However, many of these findings remain speculative, underscoring the urgent need for further research to elucidate the precise relationship between these mechanisms and the pathogenesis and progression of schizophrenia.
The abnormalities of the neurovascular unit in schizophrenia: Neurovascular endothelial dysfunction is intimately related to increased blood-brain barrier permeability. Studies have shown that oxidative stress and neurovascular endothelial dysfunction in schizophrenia may arise from mechanisms such as impaired cerebral blood perfusion and disturbances in the homeostasis of the brain microenvironment. Furthermore, the disruption of blood-brain barrier permeability allows harmful neuroimmune signals and neuroinflammatory responses to persist, leading to the typical cognitive, emotional, and behavioral symptoms of schizophrenia.[63]
In the prefrontal cortex and visual cortex of schizophrenia patients, studies have detected structural and morphological abnormalities in capillaries and neurovascular unit (NVU)-related cells, including a decrease in capillary density, endothelial cell degeneration, and alterations in astrocytic endfeet and basement membranes[23-25].These changes are associated with the negative symptoms of schizophrenia and antipsychotic treatment. However, the limited sample sizes in some studies demand further validation. Additionally, other NVU components, such as astrocytes, also display abnormalities [26-28].These microvascular abnormalities are relevant to the pathogenesis of schizophrenia, but the degree of their impact requires further investigation.
The tight junction leakage in schizophrenia: CLDN5(Claudin-5) is a key protein constituting the tight junctions of endothelial cells and serves as a primary transmembrane protein of the blood-brain barrier (BBB)[76]. It is a critical marker in studies of BBB structural changes, with its structure, distribution, and abnormal expression tightly associated with alterations in BBB permeability. Studies have shown that in the prefrontal cortex (non-visual cortex) of schizophrenia patients, CLDN5 mRNA expression is significantly increased while claudin-5 protein levels are decreased, with no apparent abnormalities in the visual cortex[77]. Transcriptomic analyses of the prefrontal cortex revealed that 12 out of 21 tight junction-related genes were decreased in schizophrenia patients compared to controls [78].Another study reported contrary results, finding a significant reduction in hippocampal CLDN5 levels in schizophrenia patients, with no differences observed in the orbitofrontal cortex. Additionally, the mRNA and protein levels of CLDN5, claudin-12, and ZO1 were correlated with the age of onset and duration of schizophrenia [30]. These findings suggest that BBB integrity alterations in schizophrenia might be region-specific rather than widespread across the brain, strongly closely linking changes in BBB permeability to the pathogenesis of schizophrenia. Studies in Chinese and Iranian cohorts have also identified a slight genetic association between CLDN5 and the development of schizophrenia [79,80]. Specifically, the rs10314 allele has been considered a potential risk factor for psychosis, though this association appears to be population-specific, as it was not confirmed in Japanese populations [81].Rs10314 is a single nucleotide polymorphism (SNP) that produces a protein of approximately half the mass of the wild-type CLDN5 gene, implying that individuals carrying this allele may produce lesser amounts of CLDN5 than typical individuals.The impact of this allele is particularly significant in 22q11 deletion syndrome (22q11DS), where the risk of developing schizophrenia is significantly increased compared to the general population (up to 30% in 22q11DS patients).Studies have shown a significant association between the rs10314 variant and schizophrenia diagnosis in 22q11DS, with these individuals producing only about 25% of the normal CLDN5 levels, potentially leading to increased BBB permeability [82]. The researcher subsequently focused on Pumilio-1 (PUM1), an RNA-binding protein that plays a critical role in cellular processes and is closely associated with the regulation of CLDN5.Studies have shown that under normal physiological conditions, PUM1 functions as a translational enhancer of CLDN-5. However, in rs10314-variant CLDN-5 mRNA, reduced binding affinity with PUM1 leads to translational suppression, resulting in downregulated CLDN-5 expression.In postmortem hippocampal tissues of schizophrenia patients, abnormally elevated CLDN-5 mRNA levels were observed in some individuals, yet the corresponding CLDN-5 protein expression was substantially reduced.A negative correlation was found between CLDN-5 mRNA and PUM1 levels, where patients with high CLDN-5 mRNA levels exhibited relatively lower PUM1 levels.This suggests that in these patients, PUM1's role in promoting the translation of CLDN-5 mRNA might be hampered, resulting in reduced CLDN-5 protein synthesis[83].Another study induced patient-derived stem cells to differentiate into BBB cells and found impaired BBB integrity in 22q11DS + schizophrenia patients, with markedly dysfunctional CLDN5 expression observed [84].Another study evaluated changes in serum zonulin and CLDN5 levels in schizophrenia patients. Compared to controls, schizophrenia patients exhibited significantly higher mean serum zonulin levels and reduced serum CLDN5 levels[85].In conclusion, CLDN5 may serve as a crucial intersection of genetic and environmental factors in schizophrenia and holds potential as a therapeutic target for future interventions.
5. The Relationship Between Antipsychotics and Blood-Brain Barrier Function
Common side effects of antipsychotic drugs include extrapyramidal side effects, tardive dyskinesia, cardiovascular issues, and metabolic disturbances. Currently, clinically used antipsychotics often have suboptimal therapeutic effects and poor bioavailability. However, the effects of antipsychotics on the blood-brain barrier (BBB) are generally bidirectional.On one hand, the BBB structure in the central nervous system necessitates that antipsychotic drugs cross the BBB to act on the brain. While the BBB protects the central nervous system by limiting the passage and dosage of drugs reaching the brain, it also restricts the delivery of antipsychotics to the brain. As a result, conventional formulations of antipsychotics used in clinical practice cannot efficiently deliver drugs directly to the brain [86].P-glycoprotein, expressed in astrocytes, actively pumps drugs, toxins, and other substances from the BBB back into the bloodstream, preventing harmful substances from accumulating in the brain. Certain antipsychotics, such as clozapine, act as P-glycoprotein inhibitors, increasing drug concentrations crossing the BBB to some extent and demonstrating excellent efficacy in treating schizophrenia.On the other hand, antipsychotics may negatively impact BBB permeability. One study conducted in vitro studies on the effects of antipsychotics, demonstrating that commonly used antipsychotics, such as clozapine, can cause cytotoxicity and apoptosis in BBB endothelial cells, impairing barrier function. This may underlie the pathogenesis of antipsychotic-related cerebral edema and neuroleptic malignant syndrome[87].
Furthermore, several antipsychotics, such as haloperidol, can reduce levels of inflammatory cytokines, including IL-1β, IL-6, and TNF-α, in schizophrenia patients [88]. Quetiapine, a second-generation antipsychotic, alleviates psychotic symptoms by antagonizing serotonin and dopamine receptors.A study investigating the effects of quetiapine under conditions of high BBB permeability found that quetiapine thermodynamically binds favorably to MMP-9. In human brain vascular endothelial cells, quetiapine reduced monolayer permeability. The study suggested that quetiapine might possess novel anti-inflammatory properties, and animal models confirmed its ability to significantly reduce BBB permeability by maintaining the integrity of tight junctions[89].
6. Conclusions
The blood-brain barrier (BBB) plays a crucial and complex role in normal brain function, and increasing evidence suggests that BBB disruption is implicated in the pathogenesis and progression of various neurological disorders. This paper reviews findings based on autopsy studies, serum and cerebrospinal fluid biomarkers, and neuroimaging, showing that schizophrenia patients exhibit varying degrees of BBB permeability alterations. These alterations are potentially associated with neuroinflammation, energy metabolism dysfunction, and abnormalities in tight junction proteins. However, research on BBB damage in schizophrenia remains nascent, and previous studies have multiple limitations. Autopsy-based studies often have small sample sizes and mainly reflect BBB permeability changes in the advanced stages of disease, which may bias results. Studies based on serum and cerebrospinal fluid biomarkers involve invasive procedures, making them less practical for schizophrenia patients, and markers such as QAlb and S100b are non-specific, unable to accurately reflect BBB permeability changes. Traditional DCE-MRI is highly sensitive to major BBB disruptions, capable of providing real-time, quantitative, and localized visualization of focal BBB damage. However, the relatively large molecular weight of exogenous contrast agents (e.g., Gd-DTPA, 550 Da) restricts its ability to detect subtle early-stage BBB changes. Additionally, concerns regarding the injection of exogenous agents, the risk of nephrogenic systemic fibrosis (NSF), gadolinium deposition and potential neurotoxicity, and prolonged scan times have constrained the application of DCE-MRI in psychiatric research. Another unresolved issue involves the temporal relationship between BBB damage and the timeline of schizophrenia development. Few studies have explored the structure and function of the BBB prior to the onset of psychiatric disorders, and there is scant evidence regarding the temporal progression of BBB permeability changes in relation to schizophrenia onset and course. While evidence supports BBB permeability alterations in schizophrenia, further research is needed to determine whether these changes are causativeor represent early pathophysiological outcomes. In recent years, advancements in neuroimaging have introduced arterial spin labeling (ASL) perfusion imaging, which uses endogenous water as a tracer. This non-invasive, quantitative, and localized method for assessing BBB permeability has gained wide use. ASL’s ability to detect subtle early-stage BBB damage offers a more direct and sensitive imaging biomarker for early disease stages. These studies deepen our understanding of the pathophysiological mechanisms of schizophrenia, explore the potential of the BBB as a therapeutic target, and provide a theoretical basis for developing novel antipsychotic drugs.
Author Contributions
writing-original draft preparation,Fangsong Zhang .;writing- review and editing, Jinhong Wang. Data collection,Jianye Zhang, Xuexue Wang*, Mengyang Han*, Yi Fei
References
- Puvogel, S.; Palma, V.; Sommer, I.E.C. Brain vasculature disturbance in schizophrenia. Current opinion in psychiatry 2022, 35, 146–156. [Google Scholar] [CrossRef]
- Smeland, O.B.; Frei, O.; Dale, A.M.; Andreassen, O.A. The polygenic architecture of schizophrenia - rethinking pathogenesis and nosology. Nature reviews. Neurology 2020, 16, 366–379. [Google Scholar] [CrossRef] [PubMed]
- Ursini, G.; Punzi, G.; Chen, Q.; Marenco, S.; Robinson, J.F.; Porcelli, A.; Hamilton, E.G.; Mitjans, M.; Maddalena, G.; Begemann, M.; et al. Convergence of placenta biology and genetic risk for schizophrenia. Nature medicine 2018, 24, 792–801. [Google Scholar] [CrossRef]
- Geddes, J.R.; Verdoux, H.; Takei, N.; Lawrie, S.M.; Bovet, P.; Eagles, J.M.; Heun, R.; McCreadie, R.G.; McNeil, T.F.; O'Callaghan, E.; et al. Schizophrenia and complications of pregnancy and labor: an individual patient data meta-analysis. Schizophrenia bulletin 1999, 25, 413–423. [Google Scholar] [CrossRef]
- Feigenson, K.A.; Kusnecov, A.W.; Silverstein, S.M. Inflammation and the two-hit hypothesis of schizophrenia. Neuroscience and biobehavioral reviews 2014, 38, 72–93. [Google Scholar] [CrossRef]
- Segarra, M.; Aburto, M.R.; Hefendehl, J.; Acker-Palmer, A. Neurovascular Interactions in the Nervous System. Annual review of cell and developmental biology 2019, 35, 615–635. [Google Scholar] [CrossRef]
- Abbott, N.J.; Rönnbäck, L.; Hansson, E. Astrocyte-endothelial interactions at the blood-brain barrier. Nature reviews. Neuroscience 2006, 7, 41–53. [Google Scholar] [CrossRef]
- Muoio, V.; Persson, P.B.; Sendeski, M.M. The neurovascular unit - concept review. Acta physiologica (Oxford, England) 2014, 210, 790–798. [Google Scholar] [CrossRef]
- Abbott, N.J.; Patabendige, A.A.; Dolman, D.E.; Yusof, S.R.; Begley, D.J. Structure and function of the blood-brain barrier. Neurobiology of disease 2010, 37, 13–25. [Google Scholar] [CrossRef]
- Hladky, S.B.; Barrand, M.A. Fluid and ion transfer across the blood-brain and blood-cerebrospinal fluid barriers; a comparative account of mechanisms and roles. Fluids and barriers of the CNS 2016, 13, 19. [Google Scholar] [CrossRef]
- Wolburg, H.; Lippoldt, A. Tight junctions of the blood-brain barrier: development, composition and regulation. Vascular pharmacology 2002, 38, 323–337. [Google Scholar] [CrossRef] [PubMed]
- Tsukita, S.; Furuse, M.; Itoh, M. Multifunctional strands in tight junctions. Nature reviews. Molecular cell biology 2001, 2, 285–293. [Google Scholar] [CrossRef] [PubMed]
- Keaney, J.; Campbell, M. The dynamic blood-brain barrier. The FEBS journal 2015, 282, 4067–4079. [Google Scholar] [CrossRef] [PubMed]
- Vorbrodt, A.W.; Dobrogowska, D.H. Molecular anatomy of intercellular junctions in brain endothelial and epithelial barriers: electron microscopist's view. Brain research. Brain research reviews 2003, 42, 221–242. [Google Scholar] [CrossRef] [PubMed]
- Rubin, L.L.; Hall, D.E.; Porter, S.; Barbu, K.; Cannon, C.; Horner, H.C.; Janatpour, M.; Liaw, C.W.; Manning, K.; Morales, J.; et al. A cell culture model of the blood-brain barrier. The Journal of cell biology 1991, 115, 1725–1735. [Google Scholar] [CrossRef] [PubMed]
- Wolburg, H.; Neuhaus, J.; Kniesel, U.; Krauss, B.; Schmid, E.M.; Ocalan, M.; Farrell, C.; Risau, W. Modulation of tight junction structure in blood-brain barrier endothelial cells. Effects of tissue culture, second messengers and cocultured astrocytes. Journal of cell science, 1347. [Google Scholar] [CrossRef]
- Doyle, K.P.; Cekanaviciute, E.; Mamer, L.E.; Buckwalter, M.S. TGFβ signaling in the brain increases with aging and signals to astrocytes and innate immune cells in the weeks after stroke. Journal of neuroinflammation 2010, 7, 62. [Google Scholar] [CrossRef]
- Sorokin, L. The impact of the extracellular matrix on inflammation. Nature reviews. Immunology 2010, 10, 712–723. [Google Scholar] [CrossRef] [PubMed]
- Miller, S.W.; Palesch, Y.Y. Comments regarding the recent OAST article. Stroke 2008, 39, e14. [Google Scholar] [CrossRef] [PubMed]
- Kealy, J.; Greene, C.; Campbell, M. Blood-brain barrier regulation in psychiatric disorders. Neuroscience letters 2020, 726, 133664. [Google Scholar] [CrossRef] [PubMed]
- Pieper, C.; Marek, J.J.; Unterberg, M.; Schwerdtle, T.; Galla, H.J. Brain capillary pericytes contribute to the immune defense in response to cytokines or LPS in vitro. Brain research 2014, 1550, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Bell, R.D.; Winkler, E.A.; Sagare, A.P.; Singh, I.; LaRue, B.; Deane, R.; Zlokovic, B.V. Pericytes control key neurovascular functions and neuronal phenotype in the adult brain and during brain aging. Neuron 2010, 68, 409–427. [Google Scholar] [CrossRef]
- Uranova, N.A.; Zimina, I.S.; Vikhreva, O.V.; Krukov, N.O.; Rachmanova, V.I.; Orlovskaya, D.D. Ultrastructural damage of capillaries in the neocortex in schizophrenia. The world journal of biological psychiatry : the official journal of the World Federation of Societies of Biological Psychiatry 2010, 11, 567–578. [Google Scholar] [CrossRef]
- Kreczmanski, P.; Schmidt-Kastner, R.; Heinsen, H.; Steinbusch, H.W.; Hof, P.R.; Schmitz, C. Stereological studies of capillary length density in the frontal cortex of schizophrenics. Acta neuropathologica 2005, 109, 510–518. [Google Scholar] [CrossRef] [PubMed]
- Udriştoiu, I.; Marinescu, I.; Pîrlog, M.C.; Militaru, F.; Udriştoiu, T.; Marinescu, D.; Mutică, M. The microvascular alterations in frontal cortex during treatment with antipsychotics: a post-mortem study. Romanian journal of morphology and embryology = Revue roumaine de morphologie et embryologie 2016, 57, 501–506. [Google Scholar]
- Vostrikov, V.; Orlovskaya, D.; Uranova, N. Deficit of pericapillary oligodendrocytes in the prefrontal cortex in schizophrenia. The world journal of biological psychiatry : the official journal of the World Federation of Societies of Biological Psychiatry 2008, 9, 34–42. [Google Scholar] [CrossRef] [PubMed]
- Webster, M.J.; Knable, M.B.; Johnston-Wilson, N.; Nagata, K.; Inagaki, M.; Yolken, R.H. Immunohistochemical localization of phosphorylated glial fibrillary acidic protein in the prefrontal cortex and hippocampus from patients with schizophrenia, bipolar disorder, and depression. Brain, behavior, and immunity 2001, 15, 388–400. [Google Scholar] [CrossRef] [PubMed]
- Webster, M.J.; O'Grady, J.; Kleinman, J.E.; Weickert, C.S. Glial fibrillary acidic protein mRNA levels in the cingulate cortex of individuals with depression, bipolar disorder and schizophrenia. Neuroscience 2005, 133, 453–461. [Google Scholar] [CrossRef]
- Bernstein, H.G.; Hildebrandt, J.; Dobrowolny, H.; Steiner, J.; Bogerts, B.; Pahnke, J. Morphometric analysis of the cerebral expression of ATP-binding cassette transporter protein ABCB1 in chronic schizophrenia: Circumscribed deficits in the habenula. Schizophrenia research 2016, 177, 52–58. [Google Scholar] [CrossRef]
- Greene, C.; Hanley, N.; Campbell, M. Blood-brain barrier associated tight junction disruption is a hallmark feature of major psychiatric disorders. Translational psychiatry 2020, 10, 373. [Google Scholar] [CrossRef] [PubMed]
- Puvogel, S.; Alsema, A.; Kracht, L.; Webster, M.J.; Weickert, C.S.; Sommer, I.E.C.; Eggen, B.J.L. Single-nucleus RNA sequencing of midbrain blood-brain barrier cells in schizophrenia reveals subtle transcriptional changes with overall preservation of cellular proportions and phenotypes. Molecular psychiatry 2022, 27, 4731–4740. [Google Scholar] [CrossRef] [PubMed]
- Huang, G.; Osorio, D.; Guan, J.; Ji, G.; Cai, J.J. Overdispersed gene expression in schizophrenia. NPJ schizophrenia 2020, 6, 9. [Google Scholar] [CrossRef] [PubMed]
- Liu, F.; Tan, A.; Yang, R.; Xue, Y.; Zhang, M.; Chen, L.; Xiao, L.; Yang, X.; Yu, Y. C1ql1/Ctrp14 and C1ql4/Ctrp11 promote angiogenesis of endothelial cells through activation of ERK1/2 signal pathway. Molecular and cellular biochemistry 2017, 424, 57–67. [Google Scholar] [CrossRef] [PubMed]
- Unroe, K.A.; Glover, M.E.; Shupe, E.A.; Feng, N.; Clinton, S.M. Perinatal SSRI Exposure Disrupts G Protein-coupled Receptor BAI3 in Developing Dentate Gyrus and Adult Emotional Behavior: Relevance to Psychiatric Disorders. Neuroscience 2021, 471, 32–50. [Google Scholar] [CrossRef] [PubMed]
- Busse, S.; Busse, M.; Schiltz, K.; Bielau, H.; Gos, T.; Brisch, R.; Mawrin, C.; Schmitt, A.; Jordan, W.; Müller, U.J.; et al. Different distribution patterns of lymphocytes and microglia in the hippocampus of patients with residual versus paranoid schizophrenia: further evidence for disease course-related immune alterations? Brain, behavior, and immunity 2012, 26, 1273–1279. [Google Scholar] [CrossRef] [PubMed]
- Goldwaser, E.L.; Swanson, R.L., 2nd; Arroyo, E.J.; Venkataraman, V.; Kosciuk, M.C.; Nagele, R.G.; Hong, L.E.; Acharya, N.K. A Preliminary Report: The Hippocampus and Surrounding Temporal Cortex of Patients With Schizophrenia Have Impaired Blood-Brain Barrier. Frontiers in human neuroscience 2022, 16, 836980. [Google Scholar] [CrossRef]
- Purves-Tyson, T.D.; Robinson, K.; Brown, A.M.; Boerrigter, D.; Cai, H.Q.; Weissleder, C.; Owens, S.J.; Rothmond, D.A.; Shannon Weickert, C. Increased Macrophages and C1qA, C3, C4 Transcripts in the Midbrain of People With Schizophrenia. Frontiers in immunology 2020, 11, 2002. [Google Scholar] [CrossRef]
- Cai, H.Q.; Catts, V.S.; Webster, M.J.; Galletly, C.; Liu, D.; O'Donnell, M.; Weickert, T.W.; Weickert, C.S. Increased macrophages and changed brain endothelial cell gene expression in the frontal cortex of people with schizophrenia displaying inflammation. Molecular psychiatry 2020, 25, 761–775. [Google Scholar] [CrossRef] [PubMed]
- Fillman, S.G.; Sinclair, D.; Fung, S.J.; Webster, M.J.; Shannon Weickert, C. Markers of inflammation and stress distinguish subsets of individuals with schizophrenia and bipolar disorder. Translational psychiatry 2014, 4, e365. [Google Scholar] [CrossRef]
- Murphy, C.E.; Kondo, Y.; Walker, A.K.; Rothmond, D.A.; Matsumoto, M.; Shannon Weickert, C. Regional, cellular and species difference of two key neuroinflammatory genes implicated in schizophrenia. Brain, behavior, and immunity 2020, 88, 826–839. [Google Scholar] [CrossRef] [PubMed]
- Shalev, H.; Serlin, Y.; Friedman, A. Breaching the blood-brain barrier as a gate to psychiatric disorder. Cardiovascular psychiatry and neurology 2009, 2009, 278531. [Google Scholar] [CrossRef] [PubMed]
- Bechter, K.; Reiber, H.; Herzog, S.; Fuchs, D.; Tumani, H.; Maxeiner, H.G. Cerebrospinal fluid analysis in affective and schizophrenic spectrum disorders: identification of subgroups with immune responses and blood-CSF barrier dysfunction. Journal of psychiatric research 2010, 44, 321–330. [Google Scholar] [CrossRef] [PubMed]
- Busse, M.; Kunschmann, R.; Dobrowolny, H.; Hoffmann, J.; Bogerts, B.; Steiner, J.; Frodl, T.; Busse, S. Dysfunction of the blood-cerebrospinal fluid-barrier and N-methyl-D-aspartate glutamate receptor antibodies in dementias. European archives of psychiatry and clinical neuroscience 2018, 268, 483–492. [Google Scholar] [CrossRef]
- Jeppesen, R.; Orlovska-Waast, S.; Sørensen, N.V.; Christensen, R.H.B.; Benros, M.E. Cerebrospinal Fluid and Blood Biomarkers of Neuroinflammation and Blood-Brain Barrier in Psychotic Disorders and Individually Matched Healthy Controls. Schizophrenia bulletin 2022, 48, 1206–1216. [Google Scholar] [CrossRef]
- Campana, M.; Löhrs, L.; Strauß, J.; Münz, S.; Oviedo-Salcedo, T.; Fernando, P.; Maurus, I.; Raabe, F.; Moussiopoulou, J.; Eichhorn, P.; et al. Blood-brain barrier dysfunction and folate and vitamin B12 levels in first-episode schizophrenia-spectrum psychosis: a retrospective chart review. European archives of psychiatry and clinical neuroscience 2023, 273, 1693–1701. [Google Scholar] [CrossRef] [PubMed]
- Campana, M.; Strauß, J.; Münz, S.; Oviedo-Salcedo, T.; Fernando, P.; Eichhorn, P.; Falkai, P.; Hasan, A.; Wagner, E. Cerebrospinal Fluid Pathologies in Schizophrenia-Spectrum Disorder-A Retrospective Chart Review. Schizophrenia bulletin 2022, 48, 47–55. [Google Scholar] [CrossRef]
- Strathmann, F.G.; Schulte, S.; Goerl, K.; Petron, D.J. Blood-based biomarkers for traumatic brain injury: evaluation of research approaches, available methods and potential utility from the clinician and clinical laboratory perspectives. Clinical biochemistry 2014, 47, 876–888. [Google Scholar] [CrossRef] [PubMed]
- Schümberg, K.; Polyakova, M.; Steiner, J.; Schroeter, M.L. Serum S100B Is Related to Illness Duration and Clinical Symptoms in Schizophrenia-A Meta-Regression Analysis. Frontiers in cellular neuroscience 2016, 10, 46. [Google Scholar] [CrossRef]
- Futtrup, J.; Margolinsky, R.; Benros, M.E.; Moos, T.; Routhe, L.J.; Rungby, J.; Krogh, J. Blood-brain barrier pathology in patients with severe mental disorders: a systematic review and meta-analysis of biomarkers in case-control studies. Brain, behavior, & immunity - health 2020, 6, 100102. [Google Scholar] [CrossRef]
- Rothermundt, M.; Missler, U.; Arolt, V.; Peters, M.; Leadbeater, J.; Wiesmann, M.; Rudolf, S.; Wandinger, K.P.; Kirchner, H. Increased S100B blood levels in unmedicated and treated schizophrenic patients are correlated with negative symptomatology. Molecular psychiatry 2001, 6, 445–449. [Google Scholar] [CrossRef]
- Rothermundt, M.; Ponath, G.; Glaser, T.; Hetzel, G.; Arolt, V. S100B serum levels and long-term improvement of negative symptoms in patients with schizophrenia. Neuropsychopharmacology : official publication of the American College of Neuropsychopharmacology 2004, 29, 1004–1011. [Google Scholar] [CrossRef]
- Chen, S.; Tian, L.; Chen, N.; Xiu, M.; Wang, Z.; Yang, G.; Wang, C.; Yang, F.; Tan, Y. Cognitive dysfunction correlates with elevated serum S100B concentration in drug-free acutely relapsed patients with schizophrenia. Psychiatry research 2017, 247, 6–11. [Google Scholar] [CrossRef] [PubMed]
- Rothermundt, M.; Falkai, P.; Ponath, G.; Abel, S.; Bürkle, H.; Diedrich, M.; Hetzel, G.; Peters, M.; Siegmund, A.; Pedersen, A.; et al. Glial cell dysfunction in schizophrenia indicated by increased S100B in the CSF. Molecular psychiatry 2004, 9, 897–899. [Google Scholar] [CrossRef] [PubMed]
- Steiner, J.; Schiltz, K.; Walter, M.; Wunderlich, M.T.; Keilhoff, G.; Brisch, R.; Bielau, H.; Bernstein, H.G.; Bogerts, B.; Schroeter, M.L.; et al. S100B serum levels are closely correlated with body mass index: an important caveat in neuropsychiatric research. Psychoneuroendocrinology 2010, 35, 321–324. [Google Scholar] [CrossRef] [PubMed]
- Yazla, E.; Kayadibi, H.; Cetin, I.; Aydinoglu, U.; Karadere, M.E. Evaluation of Changes in Peripheric Biomarkers Related to Blood Brain Barrier Damage in Patients with Schizophrenia and Their Correlation with Symptoms. Clinical psychopharmacology and neuroscience : the official scientific journal of the Korean College of Neuropsychopharmacology 2022, 20, 504–513. [Google Scholar] [CrossRef]
- Andersen, H.G.; DellaValle, B.; Bøgehave, H.; Mogensen, P.B.; Hahn, M.K.; Goth, C.K.; Sørensen, M.E.; Sigvard, A.K.; Tangmose, K.; Bojesen, K.B.; et al. Glycocalyx shedding patterns identifies antipsychotic-naïve patients with first-episode psychosis. Psychiatry research 2024, 339, 116037. [Google Scholar] [CrossRef] [PubMed]
- Mamah, D. A Review of Potential Neuroimaging Biomarkers of Schizophrenia-Risk. Journal of psychiatry and brain science 2023, 8. [Google Scholar] [CrossRef]
- Hua, J.; Brandt, A.S.; Lee, S.; Blair, N.I.S.; Wu, Y.; Lui, S.; Patel, J.; Faria, A.V.; Lim, I.A.L.; Unschuld, P.G.; et al. Abnormal Grey Matter Arteriolar Cerebral Blood Volume in Schizophrenia Measured With 3D Inflow-Based Vascular-Space-Occupancy MRI at 7T. Schizophrenia bulletin 2017, 43, 620–632. [Google Scholar] [CrossRef]
- Peruzzo, D.; Rambaldelli, G.; Bertoldo, A.; Bellani, M.; Cerini, R.; Silvia, M.; Pozzi Mucelli, R.; Tansella, M.; Brambilla, P. The impact of schizophrenia on frontal perfusion parameters: a DSC-MRI study. Journal of neural transmission (Vienna, Austria : 1996) 2011, 118, 563–570. [Google Scholar] [CrossRef] [PubMed]
- Cheng, Y.; Wang, T.; Zhang, T.; Yi, S.; Zhao, S.; Li, N.; Yang, Y.; Zhang, F.; Xu, L.; Shan, B.; et al. Increased Blood-Brain Barrier Permeability of the Thalamus Correlated With Symptom Severity and Brain Volume Alterations in Patients With Schizophrenia. Biological psychiatry. Cognitive neuroscience and neuroimaging 2022, 7, 1025–1034. [Google Scholar] [CrossRef] [PubMed]
- Goldwaser, E.L.; Wang, D.J.J.; Adhikari, B.M.; Chiappelli, J.; Shao, X.; Yu, J.; Lu, T.; Chen, S.; Marshall, W.; Yuen, A.; et al. Evidence of Neurovascular Water Exchange and Endothelial Vascular Dysfunction in Schizophrenia: An Exploratory Study. Schizophrenia bulletin 2023, 49, 1325–1335. [Google Scholar] [CrossRef] [PubMed]
- de Klerk, O.L.; Willemsen, A.T.; Bosker, F.J.; Bartels, A.L.; Hendrikse, N.H.; den Boer, J.A.; Dierckx, R.A. Regional increase in P-glycoprotein function in the blood-brain barrier of patients with chronic schizophrenia: a PET study with [(11)C]verapamil as a probe for P-glycoprotein function. Psychiatry research 2010, 183, 151–156. [Google Scholar] [CrossRef]
- Najjar, S.; Pahlajani, S.; De Sanctis, V.; Stern, J.N.H.; Najjar, A.; Chong, D. Neurovascular Unit Dysfunction and Blood-Brain Barrier Hyperpermeability Contribute to Schizophrenia Neurobiology: A Theoretical Integration of Clinical and Experimental Evidence. Frontiers in psychiatry 2017, 8, 83. [Google Scholar] [CrossRef] [PubMed]
- Steiner, J.; Mawrin, C.; Ziegeler, A.; Bielau, H.; Ullrich, O.; Bernstein, H.G.; Bogerts, B. Distribution of HLA-DR-positive microglia in schizophrenia reflects impaired cerebral lateralization. Acta neuropathologica 2006, 112, 305–316. [Google Scholar] [CrossRef] [PubMed]
- Najjar, S.; Pearlman, D.M. Neuroinflammation and white matter pathology in schizophrenia: systematic review. Schizophrenia research 2015, 161, 102–112. [Google Scholar] [CrossRef] [PubMed]
- Domenici, E.; Willé, D.R.; Tozzi, F.; Prokopenko, I.; Miller, S.; McKeown, A.; Brittain, C.; Rujescu, D.; Giegling, I.; Turck, C.W.; et al. Plasma protein biomarkers for depression and schizophrenia by multi analyte profiling of case-control collections. PloS one 2010, 5, e9166. [Google Scholar] [CrossRef] [PubMed]
- Yamamori, H.; Hashimoto, R.; Ishima, T.; Kishi, F.; Yasuda, Y.; Ohi, K.; Fujimoto, M.; Umeda-Yano, S.; Ito, A.; Hashimoto, K.; et al. Plasma levels of mature brain-derived neurotrophic factor (BDNF) and matrix metalloproteinase-9 (MMP-9) in treatment-resistant schizophrenia treated with clozapine. Neuroscience letters 2013, 556, 37–41. [Google Scholar] [CrossRef]
- Iwata, Y.; Suzuki, K.; Nakamura, K.; Matsuzaki, H.; Sekine, Y.; Tsuchiya, K.J.; Sugihara, G.; Kawai, M.; Minabe, Y.; Takei, N.; et al. Increased levels of serum soluble L-selectin in unmedicated patients with schizophrenia. Schizophrenia research 2007, 89, 154–160. [Google Scholar] [CrossRef]
- Masopust, J.; Malý, R.; Andrýs, C.; Vališ, M.; Bažant, J.; Hosák, L. Markers of thrombogenesis are activated in unmedicated patients with acute psychosis: a matched case control study. BMC psychiatry 2011, 11, 2. [Google Scholar] [CrossRef] [PubMed]
- Nguyen, T.T.; Dev, S.I.; Chen, G.; Liou, S.C.; Martin, A.S.; Irwin, M.R.; Carroll, J.E.; Tu, X.; Jeste, D.V.; Eyler, L.T. Abnormal levels of vascular endothelial biomarkers in schizophrenia. European archives of psychiatry and clinical neuroscience 2018, 268, 849–860. [Google Scholar] [CrossRef]
- Pillai, A.; Howell, K.R.; Ahmed, A.O.; Weinberg, D.; Allen, K.M.; Bruggemann, J.; Lenroot, R.; Liu, D.; Galletly, C.; Weickert, C.S.; et al. Association of serum VEGF levels with prefrontal cortex volume in schizophrenia. Molecular psychiatry 2016, 21, 686–692. [Google Scholar] [CrossRef]
- Steullet, P.; Cabungcal, J.H.; Monin, A.; Dwir, D.; O'Donnell, P.; Cuenod, M.; Do, K.Q. Redox dysregulation, neuroinflammation, and NMDA receptor hypofunction: A "central hub" in schizophrenia pathophysiology? Schizophrenia research 2016, 176, 41–51. [Google Scholar] [CrossRef]
- Serlin, Y.; Levy, J.; Shalev, H. Vascular pathology and blood-brain barrier disruption in cognitive and psychiatric complications of type 2 diabetes mellitus. Cardiovascular psychiatry and neurology 2011, 2011, 609202. [Google Scholar] [CrossRef]
- Katsel, P.; Byne, W.; Roussos, P.; Tan, W.; Siever, L.; Haroutunian, V. Astrocyte and glutamate markers in the superficial, deep, and white matter layers of the anterior cingulate gyrus in schizophrenia. Neuropsychopharmacology : official publication of the American College of Neuropsychopharmacology 2011, 36, 1171–1177. [Google Scholar] [CrossRef] [PubMed]
- Lucchinetti, C.F.; Guo, Y.; Popescu, B.F.; Fujihara, K.; Itoyama, Y.; Misu, T. The pathology of an autoimmune astrocytopathy: lessons learned from neuromyelitis optica. Brain pathology (Zurich, Switzerland) 2014, 24, 83–97. [Google Scholar] [CrossRef] [PubMed]
- Morita, K.; Furuse, M.; Fujimoto, K.; Tsukita, S. Claudin multigene family encoding four-transmembrane domain protein components of tight junction strands. Proceedings of the National Academy of Sciences of the United States of America 1999, 96, 511–516. [Google Scholar] [CrossRef]
- Nishiura, K.; Ichikawa-Tomikawa, N.; Sugimoto, K.; Kunii, Y.; Kashiwagi, K.; Tanaka, M.; Yokoyama, Y.; Hino, M.; Sugino, T.; Yabe, H.; et al. PKA activation and endothelial claudin-5 breakdown in the schizophrenic prefrontal cortex. Oncotarget 2017, 8, 93382–93391. [Google Scholar] [CrossRef] [PubMed]
- Enwright Iii, J.F.; Huo, Z.; Arion, D.; Corradi, J.P.; Tseng, G.; Lewis, D.A. Transcriptome alterations of prefrontal cortical parvalbumin neurons in schizophrenia. Molecular psychiatry 2018, 23, 1606–1613. [Google Scholar] [CrossRef]
- Sun, Z.Y.; Wei, J.; Xie, L.; Shen, Y.; Liu, S.Z.; Ju, G.Z.; Shi, J.P.; Yu, Y.Q.; Zhang, X.; Xu, Q.; et al. The CLDN5 locus may be involved in the vulnerability to schizophrenia. European psychiatry : the journal of the Association of European Psychiatrists 2004, 19, 354–357. [Google Scholar] [CrossRef]
- Omidinia, E.; Mashayekhi Mazar, F.; Shahamati, P.; Kianmehr, A.; Shahbaz Mohammadi, H. Polymorphism of the CLDN5 gene and Schizophrenia in an Iranian Population. Iranian journal of public health 2014, 43, 79–83. [Google Scholar]
- Ishiguro, H.; Imai, K.; Koga, M.; Horiuchi, Y.; Inada, T.; Iwata, N.; Ozaki, N.; Ujike, H.; Itokawa, M.; Kunugi, H.; et al. Replication study for associations between polymorphisms in the CLDN5 and DGCR2 genes in the 22q11 deletion syndrome region and schizophrenia. Psychiatric genetics 2008, 18, 255–256. [Google Scholar] [CrossRef]
- Greene, C.; Kealy, J.; Humphries, M.M.; Gong, Y.; Hou, J.; Hudson, N.; Cassidy, L.M.; Martiniano, R.; Shashi, V.; Hooper, S.R.; et al. Dose-dependent expression of claudin-5 is a modifying factor in schizophrenia. Molecular psychiatry 2018, 23, 2156–2166. [Google Scholar] [CrossRef]
- Hashimoto, Y.; Greene, C.; Hanley, N.; Hudson, N.; Henshall, D.; Sweeney, K.J.; O'Brien, D.F.; Campbell, M. Pumilio-1 mediated translational control of claudin-5 at the blood-brain barrier. Fluids and barriers of the CNS 2024, 21, 52. [Google Scholar] [CrossRef]
- Crockett, A.M.; Ryan, S.K.; Vásquez, A.H.; Canning, C.; Kanyuch, N.; Kebir, H.; Ceja, G.; Gesualdi, J.; Zackai, E.; McDonald-McGinn, D.; et al. Disruption of the blood-brain barrier in 22q11.2 deletion syndrome. Brain : a journal of neurology 2021, 144, 1351–1360. [Google Scholar] [CrossRef] [PubMed]
- Usta, A.; Kılıç, F.; Demirdaş, A.; Işık, Ü.; Doğuç, D.K.; Bozkurt, M. Serum zonulin and claudin-5 levels in patients with schizophrenia. European archives of psychiatry and clinical neuroscience 2021, 271, 767–773. [Google Scholar] [CrossRef]
- Annu; Rehman, S. ; Md, S.; Baboota, S.; Ali, J. Analyzing Nanotheraputics-Based Approaches for the Management of Psychotic Disorders. Journal of pharmaceutical sciences 2019, 108, 3757–3768. [Google Scholar] [CrossRef]
- Elmorsy, E.; Elzalabany, L.M.; Elsheikha, H.M.; Smith, P.A. Adverse effects of antipsychotics on micro-vascular endothelial cells of the human blood-brain barrier. Brain research 2014, 1583, 255–268. [Google Scholar] [CrossRef]
- Kowalski, J.; Blada, P.; Kucia, K.; Madej, A.; Herman, Z.S. Neuroleptics normalize increased release of interleukin- 1 beta and tumor necrosis factor-alpha from monocytes in schizophrenia. Schizophrenia research 2001, 50, 169–175. [Google Scholar] [CrossRef] [PubMed]
- Robinson, B.D.; Isbell, C.L.; Anasooya Shaji, C.; Kurek, S., Jr.; Regner, J.L.; Tharakan, B. Quetiapine protects the blood-brain barrier in traumatic brain injury. The journal of trauma and acute care surgery 2018, 85, 968–976. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
Composition of the Neurovascular Unit (A) ;Substance Transport Across the Blood-Brain Barrier (B).
Figure 1.
Composition of the Neurovascular Unit (A) ;Substance Transport Across the Blood-Brain Barrier (B).
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



