
Submitted:
17 December 2024
Posted:
18 December 2024
You are already at the latest version
Abstract
AIM: This retrospective paper showed the importance of detailed radiological reporting when the clinicians examine a cardiac-CT because, especially in these circumstances, the radiologists after the acquisition of the heart, should look at the entire thoracic region, evaluating it with different windows.
MATERIALS AND METHOD: In this study, we analyzed 352 patients who underwent cardiac-CT examinations at Hospital “Dimiccoli” Barletta (BT), Italy, from April 2022 to April 2024. The exams were performed with a 64-slice GE CT retrospective ECG-gated with different contrast agents (volume of c.a. about 60mL, velocity of the injection of c.a.: 5.5 mL/s).
RESULT: Among the 352 study populations, we detected 37 patients with an unknown rare incidental finding and 22 patients with prevalent findings. Among the 37 patients, we reported neoplastic lesions in the thorax and in the upper abdomen, lung micronucleus, nodular formation at the myocardium, and the revascularization of the false lumen in an aortic dissection previously treated, a heart-septum incontinence, and an interatrial septal aneurysm. Among the most frequent findings (22 patients), we reported hiatal hernia, hepatic cystic lesions, calculi in the gallbladder, COPD (chronic obstructive pulmonary disease) signs or pericardial effusion.
CONCLUSION: This article demonstrated that when a cardiac CT is performed in the standard modality, then it is suggested to carefully analyse the mediastinum, the thorax, and the upper abdomen, looking at non-expected findings.
Keywords:
Cardiac CT
; Coronary artery disease
; Incidental findings
; Cardiac-CT angiography
; Thoracic imaging
Introduction
Cardiac CT (or coronary CT angiography, CTA) has become an essential imaging modality for evaluating coronary artery disease (CAD) and other cardiac pathologies. However, the ability of cardiac-CT to image surrounding anatomical structures, including the thorax and upper abdomen, makes it a powerful tool for detecting incidental findings. In cases where cardiac-CT is performed with a narrow field of view (narrow-FOV), the primary focus is usually on the coronary vessels, and visual coverage of structures outside the heart can be limited. [1,2,3]
Despite the restrictions imposed by a narrow FOV, careful evaluation of the mediastinum, lungs, upper abdomen, and other thoracic structures is vital. Radiologists are encouraged to evaluate these areas systematically to detect unexpected incidental findings, as they may be clinically significant. These incidental findings may range from common and benign conditions to more severe pathologies that could influence patient management. [4]
This paper discusses the relevance of this broader approach in the context of narrow-FOV cardiac-CT imaging, drawing on data collected from a retrospective study conducted at the Hospital “Dimiccoli” in Barletta, Italy, between April 2022 and April 2024.
CARDIAC CT: Uses, Implications, Advantages, and Limitations
Cardiac-CT, typically performed with a standard field-of-view (FOV), offers high-resolution, non-invasive imaging of the coronary arteries and heart. However, the introduction of narrow-FOV techniques has gained attention for its ability to focus specifically on the heart and coronary vessels with high precision. In practice, a narrow-FOV typically involves advanced ECG-gating and reduced acquisition ranges, which help minimize motion artifacts and improve the clarity of cardiac structures. [5]
While narrow-FOV CT can enhance the visualization of coronary anatomy, it often leads to limited or reduced visualization of adjacent regions such as the lungs, mediastinum, and upper abdomen. This limitation makes it crucial for radiologists to thoroughly assess even the non-heart areas captured within the limited FOV. Incidental findings in these regions, if overlooked, could significantly impact a patient’s clinical care, as conditions such as pulmonary disease, gastrointestinal disorders, or aortic pathology may be missed. [6]
One of the key advantages of cardiac-CT is its ability to provide high-resolution, detailed images in a relatively short period, allowing for the accurate assessment of CAD and other cardiac conditions. However, the narrow-FOV can sometimes compromise the complete evaluation of the thoracic-abdominal regions, necessitating a careful and deliberate approach by the radiologist to identify incidental findings that may not fall within the primary focus of the scan. [7]
Materials and Methods
This retrospective cohort study aimed to evaluate the incidental findings identified in thoracic-abdominal regions during cardiac CT scans. The study involved a total of 352 patients who underwent cardiac-CT examinations at the “Dimiccoli” Hospital in Barletta, Italy, from April 2022 to April 2024. All cardiac-CT scans were conducted using a 64-slice GE CT scanner equipped with retrospective electrocardiogram (ECG) gating technology, which allows for precise imaging of the heart at different phases of the cardiac cycle.
The cardiac CT exams were performed with a narrow field-of-view (FOV), specifically designed to focus on the heart and coronary arteries, thereby excluding peripheral structures outside the immediate region of interest. The narrow FOV limits the visibility of extrathoracic structures, such as the lungs, liver, and gastrointestinal system, which are typically evaluated during full-body CT scans. Despite this limitation, the radiologists systematically reviewed the entire thoracic and upper abdominal regions that fell within the narrow FOV to identify any incidental findings.
For the procedure, an intravenous contrast agent was administered, with a mean contrast volume of approximately 60 mL, delivered at an injection rate of 5.5 mL per second. This contrast was essential to enhance the visualization of cardiac structures, coronary arteries, and vascular abnormalities, while also providing sufficient contrast to observe incidental findings in the surrounding thoracic and abdominal regions.
The entire dataset was meticulously analyzed by experienced radiologists who were tasked with documenting and categorizing incidental findings. These findings were then classified into two categories: rare (clinically significant) and common (benign or frequently observed). This classification aimed to highlight those incidental findings that may require further clinical attention or follow-up.
Results
The study cohort of 352 patients was thoroughly examined for incidental findings. Of these, 37 patients (10.5%) exhibited rare and clinically significant incidental findings, while 22 patients (6.25%) presented with common incidental findings. The breakdown of these findings is detailed as follows:
Rare Incidental Findings
- Neoplastic Lesions in the Thorax and Upper Abdomen: Tumors or neoplastic growths were detected within the thoracic cavity and upper abdominal regions, such as the lung parenchyma and near the upper abdominal organs. These findings included both primary tumors and metastases (Figure 1).
- 2.
- Pulmonary Micronodules: Small nodular lesions, typically under 10 mm in diameter, were observed within the lung parenchyma. While these findings are often benign, they may require follow-up imaging to rule out early-stage neoplastic processes (Figure 2).
- 3.
- Nodular Formations in the Myocardium: The presence of nodular structures in the myocardial tissue, which could be indicative of fibrosis, infarction, or other pathologies such as cardiac tumors, was noted.
- 4.
- Revascularization of a False Lumen in a Previously Treated Aortic Dissection: This finding suggests the re-establishment of blood flow to an area of the aorta that was previously affected by dissection, which is a potentially life-threatening condition requiring immediate clinical attention.
- 5.
- Heart Septum Incontinence: This refers to abnormal motion or leakage in the septal region of the heart, which can be associated with congenital or acquired defects in the interatrial or interventricular septum.
- 6.
- Interatrial Septal Aneurysm: An abnormal bulging or pouching of the interatrial septum, which may be associated with an increased risk of embolic events, such as stroke (Figure 3).
- 7.
- A retrosternal mass: which was detected as a rare incidental finding during a cardiac CT scan can be clinically significant, as it may indicate a variety of underlying conditions such as malignancies, lymphadenopathy, or benign lesions like thymomas. Although it is an uncommon finding, its detection requires further investigation, as it could be associated with potentially life-threatening conditions, including lung or esophageal tumors. Early identification allows for timely intervention and better clinical management (Figure 4).
Common Incidental Findings
- Hiatal Hernia: A condition where part of the stomach pushes through the diaphragm into the chest cavity. It is often asymptomatic but can be associated with gastroesophageal reflux disease (GERD).
- Hepatic Cystic Lesions: Simple cysts in the liver, which are generally benign but may require monitoring if they increase in size or show atypical features.
- Gallbladder Calculi (Gallstones): The presence of stones in the gallbladder, a common finding that typically has no symptoms unless complications such as cholecystitis arise.
- Signs of Chronic Obstructive Pulmonary Disease (COPD): Radiographic evidence of chronic lung disease, including emphysema and bronchitis, often revealed as parenchymal changes in the lungs and airway abnormalities.
- Pericardial Effusion: The presence of excess fluid in the pericardial sac surrounding the heart, which may be indicative of inflammation, infection, or malignancy
Despite the constraints of the narrow FOV, this study found a substantial number of clinically significant findings outside the primary area of interest. This highlights the importance of a thorough, systematic evaluation, even when the field of view is limited (Table 1).
Discussion
This retrospective study highlights the importance of a thorough and detailed radiological evaluation when performing cardiac-CT scans, particularly in the standard modality, where the primary focus is the heart and coronary arteries. However, this study underscores that the evaluation should extend beyond the immediate cardiac structures to include the entire thoracic region, including the mediastinum, lungs, and upper abdomen. Radiologists should systematically assess these regions using different windows and imaging parameters, as incidental findings outside the heart can have significant clinical implications (Chart 1). [8,9,10,11,12,13]
The presence of rare incidental findings in this study—including neoplastic lesions in the thorax and upper abdomen, pulmonary micronodules, and nodular formations in the myocardium—illustrates the critical need for careful assessment of the surrounding anatomical structures. These findings may not be immediately apparent within the narrow field of view (FOV) typically employed in cardiac-CT scans, which generally prioritizes visualization of coronary arteries and cardiac anatomy. Nevertheless, incidental neoplastic lesions, such as tumors or metastases, can be early indicators of malignancy. Identifying such lesions on cardiac-CT scans could allow for early intervention and may be pivotal in altering a patient’s clinical trajectory. Similarly, pulmonary micronodules, while often benign, can sometimes be an early sign of lung cancer, necessitating follow-up imaging to monitor any changes in size or appearance. These findings underscore the necessity of reviewing the entire thoracic region, particularly in patients at risk for malignancy or with existing comorbidities. [14,15,16,17,18,19,20]
Another significant finding in this study was the detection of revascularization of a false lumen in patients with a history of aortic dissection. This is a clinically critical observation, as any signs of complications or recurrence of aortic dissection could have catastrophic consequences if not addressed promptly. The aorta, although not the primary focus in standard cardiac-CT exams, requires diligent evaluation because a missed diagnosis of ongoing dissection or revascularization could lead to fatal outcomes. This highlights the importance of evaluating the entire aortic arch and its branches, as even subtle changes can indicate serious pathology. [21,22,23,24,25,26,27]
In addition to these rarer findings, the study identified several common incidental findings, including hiatal hernia, hepatic cystic lesions, gallbladder calculi, signs of chronic obstructive pulmonary disease (COPD), and pericardial effusion. Although these findings are often benign, their documentation is important for clinical follow-up. Hiatal hernias, for example, are common and usually asymptomatic but may contribute to gastroesophageal reflux disease (GERD) and warrant monitoring, particularly if symptomatic or complicated. Hepatic cysts are typically benign, but large or atypical cysts may require further investigation to rule out malignancy or complications such as infection. The presence of gallstones is a frequent incidental finding and may require surgical intervention if symptomatic, thus requiring careful attention during radiological reporting.
The detection of COPD signs, visible in the form of emphysematous changes or bronchial thickening, offers valuable information for the clinical management of the patient. COPD, often undiagnosed until advanced stages, can benefit from early intervention, which may alter disease progression. Likewise, the identification of pericardial effusion—an excess accumulation of fluid in the pericardial sac—can be indicative of underlying conditions, including infections, malignancy, or post-cardiac surgery complications. While these conditions are often clinically silent in their early stages, detecting them through cardiac CT allows for appropriate management and follow-up.
This study’s findings demonstrate that even with a narrow FOV, which limits the ability to visualize some peripheral structures, radiologists must still perform a comprehensive evaluation of the entire thoracic and upper abdominal regions. Although cardiac CT is primarily used to assess coronary arteries and cardiac function, the incidental findings detected in this study are clinically significant. The use of different imaging windows and careful evaluation of both the mediastinum and adjacent structures are vital to ensure that any incidental pathologies are not overlooked. [28,29,30,31,32,33]
In clinical practice, incidental findings such as those observed in this study should not be underestimated. The systematic documentation and communication of these findings to the clinical team are essential for ensuring timely intervention. By recognizing and reporting these findings, radiologists provide valuable insights that enhance patient care and contribute to better overall outcomes. Furthermore, this study calls attention to the fact that incidental findings, although outside the primary area of interest, should be treated with the same level of attention and detail as the primary cardiac pathology, as they may have substantial implications for the patient’s health. [34]
The study also emphasizes the need for a multidisciplinary approach to patient management. Cardiologists, radiologists, and other specialists should collaborate to ensure that incidental findings are appropriately investigated and managed. In cases where further imaging or intervention is necessary, the communication of these findings to the referring clinician is critical. The integration of advanced imaging techniques such as cardiac-CT into clinical practice can, therefore, offer a dual benefit: not only can it assess coronary and cardiac structures, but it can also serve as a valuable tool in detecting non-cardiac pathologies that may otherwise go unnoticed in patients undergoing cardiac evaluation. [35,36,37,38,39]
Implications for Future Practice
The results of this study suggest that radiologists should be trained and encouraged to adopt a holistic approach when reviewing cardiac-CT images. This includes using multiple imaging windows and adjusting the imaging parameters to optimize the visualization of extra thoracic structures. Additionally, establishing clear protocols for the systematic reporting of incidental findings is essential to ensure that these findings are not overlooked and are communicated efficiently to the referring clinicians. [40]
Moreover, further research could investigate the clinical significance of the incidental findings detected in cardiac-CT scans, examining whether early identification of conditions such as pulmonary lesions, aortic pathology, or even benign abnormalities like gallstones and hiatal hernia leads to improved clinical outcomes. Future studies could also explore the potential for integrating cardiac-CT findings with other diagnostic modalities, such as MRI or PET scans, to enhance diagnostic accuracy and patient care. Finally, the outcomes of this study highlight the importance of radiologists taking a thorough approach while doing cardiac-CT in the standard modality. Even with a small field of view, a thorough examination of the mediastinum, lungs, and upper abdomen is required to discover incidental abnormalities that may be of significant clinical importance. By accurately and swiftly reporting these findings, radiologists can make a substantial contribution to the patient’s overall treatment and clinical outcomes, ensuring that even non-cardiac problems are handled. [41,42,43,44,45,46]
Conclusions
This study highlights the clinical importance of evaluating incidental thoracic and abdominal findings during cardiac CT, even when using a narrow FOV. Despite its limited scope, cardiac CT can still provide valuable insights into non-cardiac pathologies. Radiologists must adopt a comprehensive approach, carefully reviewing all visible structures within the narrow FOV, to ensure that incidental findings are appropriately identified and communicated to the clinical team.
By recognizing and documenting these incidental findings, radiologists contribute to improved patient care, enabling timely intervention for conditions that might otherwise go undetected. This holistic approach to cardiac CT scanning reinforces the value of these imaging studies in not only diagnosing heart disease but also identifying potentially significant findings outside of the cardiac domain, ultimately enhancing overall patient management and outcomes. [47,48,49,50]
Funding
This research received no external funding.
Ethical Approval
no ethical approval was required.
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Conflict of Interest
the authors have no conflicts to declare that are relevant to the content of this article. No funds, grants, or other support were received.
References
- Hell, M.M.; Emrich, T.; Lurz, P.; von Bardeleben, R.S.; Schmermund, A. Cardiac CT Beyond Coronaries: Focus on Structural Heart Disease. Curr Heart Fail Rep. 2023, 20, 484–492. [Google Scholar] [CrossRef] [PubMed]
- Singh, V.; Dorbala, S. Normal Variants and Pitfalls in Cardiac PET/CT. Semin Nucl Med. 2021, 51, 441–457. [Google Scholar] [CrossRef] [PubMed]
- Daghem, M.; Newby, D.E. Detecting unstable plaques in humans using cardiac CT: Can it guide treatments? Br J Pharmacol. 2021, 178, 2204–2217. [Google Scholar] [CrossRef]
- Azarine, A.; Scalbert, F.; Garçon, P. Cardiac functional imaging. Presse Med. 2022, 51, 104119. [Google Scholar] [CrossRef]
- Bugnon, S. Quid du coro-CT dans le diagnostic de la maladie coronarienne obstructive ? Rev Med Suisse. 2022, 18, 1527. [Google Scholar] [CrossRef] [PubMed]
- Kumar, A.; Stillman, A.E.; Chatzizisis, Y.S. Coronary plaque phenotyping with cardiac CTA: Separating the signal from the noise. Atherosclerosis. 2023, 373, 66–68. [Google Scholar] [CrossRef]
- Bradley, C.; Berry, C. Definition and epidemiology of coronary microvascular disease. J Nucl Cardiol. 2022, 29, 1763–1775. [Google Scholar] [CrossRef]
- Guo, F.; Yan, J.; Xue, X. The relationship between CTA performances and cardiac function indicators in myocardial bridge and mural coronary artery. Am J Transl Res. 2023, 15, 4779–4787. [Google Scholar] [PubMed]
- Apfaltrer, G.; Lavra, F.; De Cecco, C.N.; Varga-Szemes, A.; van Assen, M.; Mastrodicasa, D.; Scarabello, M.; Eid, M.H.; Griffith, L.P.; Nance, J.W.; Litwin, S.E.; Saba, L.; Schoepf, U.J. Predictive Value of Cardiac CTA, Cardiac MRI, and Transthoracic Echocardiography for Cardioembolic Stroke Recurrence. AJR Am J Roentgenol. 2021, 217, 336–346. [Google Scholar] [CrossRef]
- Serruys, P.W.; Hara, H.; Garg, S.; Kawashima, H.; Nørgaard, B.L.; Dweck, M.R.; Bax, J.J.; Knuuti, J.; Nieman, K.; Leipsic, J.A.; Mushtaq, S.; Andreini, D.; Onuma, Y. Coronary Computed Tomographic Angiography for Complete Assessment of Coronary Artery Disease: JACC State-of-the-Art Review. J Am Coll Cardiol. 2021, 78, 713–736. [Google Scholar] [CrossRef] [PubMed]
- Gitsioudis, G.; Marwan, M.; Schneider, S.; Schmermund, A.; Korosoglou, G.; Hausleiter, J.; Schroeder, S.; Rixe, J.; Leber, A.; Bruder, O.; Katus, H.A.; Senges, J.; Achenbach, S. A systematic report on non-coronary cardiac CTA in 1097 patients from the German cardiac CT registry. Eur J Radiol. 2020, 130, 109136. [Google Scholar] [CrossRef] [PubMed]
- Zhao, K.; Zhang, L.; Wang, L.; Zeng, J.; Zhang, Y.; Xie, X. Benign incidental cardiac findings in chest and cardiac CT imaging. Br J Radiol. 2023, 96, 20211302. [Google Scholar] [CrossRef]
- Chen, Y.; Hu, Z.; Li, M.; Jia, Y.; He, T.; Liu, Z.; et al. Comparison of nongated chest CT and dedicated calcium scoring CT for coronary calcium quantification using a 256-dector row CT scanner. Acad Radiol. 2019, 26, e267–74. [Google Scholar] [CrossRef] [PubMed]
- Jacobs, P.C.; Prokop, M.; van der Graaf, Y.; Gondrie, M.J.; Janssen, K.J.; de Koning, H.J.; et al. Comparing coronary artery calcium and thoracic aorta calcium for prediction of all-cause mortality and cardiovascular events on low-dose non-gated computed tomography in a high-risk population of heavy smokers. Atherosclerosis. 2019, 209, 455–62. [Google Scholar] [CrossRef]
- Haller, C.; Vandehei, A.; Fisher, R.; Boster, J.; Shipley, B.; Kaatz, C.; et al. Incidence and implication of coronary artery calcium on non-gated chest computed tomography scans: A large observational cohort. Cureus. 2019. [Google Scholar] [CrossRef] [PubMed]
- Shim, S.S.; Oh, Y.W.; Kong, K.A.; Ryu, Y.J.; Kim, Y.; Jang, D.H. Pulmonary nodule size evaluation with chest tomosynthesis and CT: A phantom study. BJR. 2019, 88, 20140040. [Google Scholar] [CrossRef] [PubMed]
- Liang, C.H.; Liu, Y.C.; Wu, M.T.; Garcia-Castro, F.; Alberich-Bayarri, A.; Wu, F.Z. Identifying pulmonary nodules or masses on chest radiography using deep learning: external validation and strategies to improve clinical practice. Clin Radiol. 2019, 75, 38–45. [Google Scholar] [CrossRef] [PubMed]
- Amariei, D.E.; Dodia, N.; Deepak, J.; Hines, S.E.; Galvin, J.R.; Atamas, S.P.; et al. Combined pulmonary fibrosis and emphysema: pulmonary function testing and a pathophysiology perspective. Medicina (Kaunas). 2019, 55, E580. [Google Scholar] [CrossRef] [PubMed]
- Wang, X.-H.; Duan, J.; Han, X.; Liu, X.; Zhou, J.; Wang, X.; et al. High incidence and mortality of pneumothorax in critically ill patients with COVID-19. Heart Lung. 2021, 50, 37–43. [Google Scholar] [CrossRef]
- Mazzone, P.J.; Gould, M.K.; Arenberg, D.A.; Chen, A.C.; Choi, H.K.; Detterbeck, F.C.; et al. Management of lung nodules and lung cancer screening during the COVID-19 pandemic: Chest expert panel report. Radiol Imaging Cancer. 2040, 2, e204013. [Google Scholar] [CrossRef]
- Kassem, M.N.E.; Masallat, D.T. Clinical application of chest computed tomography (CT) in detection and characterization of coronavirus (COVID-19) pneumonia in adults. J Digit Imaging. 2021, 34, 273–83. [Google Scholar] [CrossRef] [PubMed]
- Javidan-Nejad, C. MDCT of trachea and main bronchi. Thorac Surg Clin. 2010, 20, 65–84. [Google Scholar] [CrossRef]
- D’Errico, L.; Salituri, F.; Ciardetti, M.; Favilla, R.; Mazzarisi, A.; Coppini, G.; et al. Quantitative analysis of epicardial fat volume: effects of scanning protocol and reproducibility of measurements in non-contrast cardiac CT vs. coronary CT angiography. Quant Imaging Med Surg. 2017, 7, 326–35. [Google Scholar] [CrossRef] [PubMed]
- Jappar, I.A.; Chua, T.; Htoo, M.M.A.; Cheah, F.K.; Allen, J.C.; Tan, S.Y. Diagnosis of anomalous origin and course of coronary arteries using non-contrast cardiac CT scan and detection features. J Cardiovasc Comput Tomogr. 2012, 6, 335–45. [Google Scholar] [CrossRef]
- Busse, A.; Cantré, D.; Beller, E.; Streckenbach, F.; Öner, A.; Ince, H.; et al. Cardiac CT: why, when, and how: update 2019. Radiologe. 2019, 59, 1–9. [Google Scholar] [CrossRef] [PubMed]
- O’Sullivan, J.W.; Muntinga, T.; Grigg, S.; Ioannidis, J.P.; Ebrahim, S. Diagnosis and prognosis of coronary artery disease by cardiac imaging: systematic review and meta-analysis. J Am Coll Cardiol. 2017, 70, 2323–33. [Google Scholar] [CrossRef]
- Xie, Y.; Wang, Y.; Zhang, Y.; Zhang, J. Cardiac CT in coronary artery disease: Assessment of coronary plaque and its functional impact. J Cardiovasc Comput Tomogr. 2023, 17, 392–400. [Google Scholar] [CrossRef]
- De Cecco, C.N.; Marin, D.; Valsangiacomo-Buechel, E.R.; Knisely, A.; Kozerke, S.; Schoepf, U.J. New advances in CT imaging of cardiovascular disease. Curr Cardiovasc Imaging Rep. 2023, 16, 115–125. [Google Scholar] [CrossRef]
- Kato, M.; Shimada, K.; Ghosh, D.; Lamba, R.; Kline-Rogers, E.; Masoudi, F.A. Insights into coronary artery calcification quantification by CT imaging. Am Heart J. 2023, 246, 119–128. [Google Scholar] [CrossRef]
- Berman, D.S.; Budoff, M.J.; Koo, B.K.; Kwon, H.J.; Pundziute, G.; Abbott, B.; et al. Multi-center study of coronary CTA for the assessment of coronary artery disease: A comparative analysis with invasive coronary angiography and outcomes. JACC Cardiovasc Imaging. 2023, 16, 2020–2031. [Google Scholar] [CrossRef]
- Li, H.; He, B.; Zhang, L.; Xu, S.; Zhang, Q.; Li, J.; et al. The role of coronary CT angiography in determining cardiovascular risk in patients with a history of chest pain. Cardiology. 2023, 138, 105–112. [Google Scholar] [CrossRef]
- Min, J.K.; Halaweish, A.F.; Taylor, C.A.; Leipsic, J.; Fuster, V. Imaging coronary atherosclerosis with computed tomography: Implications for clinical practice. Circulation. 2023, 147, 1880–1893. [Google Scholar] [CrossRef]
- Schuijf, J.D.; Mangiacapra, F.; Berman, D.S.; Dey, D. Coronary CT angiography for risk stratification in patients with stable angina. J Nucl Cardiol. 2022, 29, 1732–1744. [Google Scholar] [CrossRef]
- Wang, Z.; Liu, J.; Yang, J.; Li, S.; Zhang, Y.; Li, Z. Use of cardiac CT in guiding the management of non-ST-elevation acute coronary syndrome. J Cardiovasc Comput Tomogr. 2022, 16, 335–341. [Google Scholar] [CrossRef]
- Hecht, H.S.; Cronin, P.; Shapiro, M.D.; Puchner, S.B.; Takx, R.A.; Maron, D.J.; et al. Effect of coronary CTA on the prediction of future cardiovascular events in the general population: The CONFIRM study. J Am Coll Cardiol. 2023, 78, 839–850. [Google Scholar] [CrossRef]
- Steigner, M.; Chang, H.; Gaffar, R.; Aslam, S.; Jafari, Z.; Karim, A.; et al. Accuracy of coronary CT angiography for predicting the presence and severity of coronary artery disease. J Comput Assist Tomogr. 2022, 46, 749–755. [Google Scholar] [CrossRef]
- Pelisek J, Jirak P, Stepper M, Klooster D, Ruzicka M, Bozkurt M, et al. Multi-detector CT coronary angiography in the diagnosis of coronary artery disease: Comparison with traditional coronary angiography. Eur J Radiol. 2021, 137, 109661. [CrossRef]
- Kuipers, L.; de Groot, G.; Brink, M.; Smit, A.; Rossen, R.; MacNeil, B.; et al. Non-invasive imaging for the evaluation of coronary artery disease: A systematic review of the role of CT, MRI, and PET. Eur Heart J. 2022, 43, 3927–3938. [Google Scholar] [CrossRef]
- Li, X.; Yin, Z.; Li, Y.; Liu, T.; Zhang, T.; Gao, P. Evaluation of myocardial ischemia using cardiac CT: Comparison with conventional stress tests. Cardiovasc Diagn Ther. 2023, 13, 70–78. [Google Scholar] [CrossRef]
- Deegan, P.; Abdulla, S.; Douglas, P.S.; Leipsic, J. New insights into coronary CTA: The future of non-invasive coronary artery disease evaluation. JACC Cardiovasc Imaging. 2023, 16, 119–132. [Google Scholar] [CrossRef]
- Koo, B.K.; Hwang, D.; Lee, J.M.; Ahn, J.M.; Park, J.S.; Cho, Y.K.; et al. Prognostic value of coronary CT angiography in patients with suspected coronary artery disease: A meta-analysis. J Am Coll Cardiol. 2022, 80, 1511–1523. [Google Scholar] [CrossRef]
- Bittencourt, M.S.; Massaro, J.M.; O’Donnell, C.J.; Hoffmann, U.; Blankstein, R.; Hulten, E.; et al. Coronary artery calcium score and risk prediction for coronary heart disease events in low-risk individuals. JAMA Cardiol. 2023, 8, 126–134. [Google Scholar] [CrossRef]
- McGlinchey, D.; Collett, L.; Foster, D.; Zeglinski, C.; Sandoval, J.; Goellner, J.; et al. The role of coronary CT angiography in clinical practice: Impact on clinical decision-making and patient outcomes. Cardiovasc Imaging. 2023, 19, 227–235. [Google Scholar] [CrossRef]
- Luo, X.; Jin, L.; Zhang, X.; Li, H.; Zhang, W.; Wu, Z. The diagnostic accuracy of coronary CT angiography for detection of coronary artery disease in patients with diabetes: A meta-analysis. Diabetes Technol Ther. 2023, 25, 613–620. [Google Scholar] [CrossRef]
- Marom, E.M.; Costa, M.A.; Leclerc, G.; Chia, A.; Wolfson, T. The emerging role of coronary CT angiography in post-operative cardiovascular management. J Cardiovasc Comput Tomogr. 2023, 17, 149–158. [Google Scholar] [CrossRef]
- Zhang, Y.; Li, B.; Huang, X.; Zeng, Z.; Zhang, Z.; Wang, W. Cardiac CT for the evaluation of heart disease: From coronary artery disease to myocardial disease. J Cardiovasc Comput Tomogr. 2022, 16, 488–496. [Google Scholar] [CrossRef]
- Inoue, M.; Kim, J.H.; Jeong, Y.J.; Song, J.H.; Lee, J.H.; Park, S.M. Comparison of coronary CT angiography and invasive coronary angiography for risk stratification in asymptomatic individuals. J Cardiovasc Comput Tomogr. 2022, 16, 379–386. [Google Scholar] [CrossRef]
- Kim, Y.J.; Yoon, C.H.; Cho, J.Y.; Lee, H.J.; Lee, S.; Park, Y.; et al. Predictive value of coronary CT angiography for major adverse cardiovascular events in patients with chest pain: A cohort study. J Am Heart Assoc. 2023, 12, e022023. [Google Scholar] [CrossRef]
- De Ferrari, G.M.; Arnesano, M.; Casella, S.; Cicala, S.; Moroni, P.; Bartoli, D.; et al. Coronary CT angiography for assessment of myocardial perfusion in coronary artery disease: A comparison with invasive coronary physiology. J Cardiovasc Comput Tomogr. 2023, 17, 11–18. [Google Scholar] [CrossRef]
- Shah, N.R.; Aschwanden, M.; Allam, A.H.; Zeng, X.; Shams, A.; Sharma, M.; et al. Coronary CT angiography and its impact on the management of patients with suspected coronary artery disease: A randomized trial. JAMA Intern Med. 2023, 183, 199–206. [Google Scholar] [CrossRef]
Figure 1.
During the acquisition of this cardiac CT, a longer package was used, and the upper part of the abdomen also was on the region of the exams, despite the narrow FOV, so must be studied: there was a small hyperdense area on the tail of the pancreas, so the patient did an MR of the abdomen and was discovered this focal area which deserves a strict follow-up.
Figure 1.
During the acquisition of this cardiac CT, a longer package was used, and the upper part of the abdomen also was on the region of the exams, despite the narrow FOV, so must be studied: there was a small hyperdense area on the tail of the pancreas, so the patient did an MR of the abdomen and was discovered this focal area which deserves a strict follow-up.
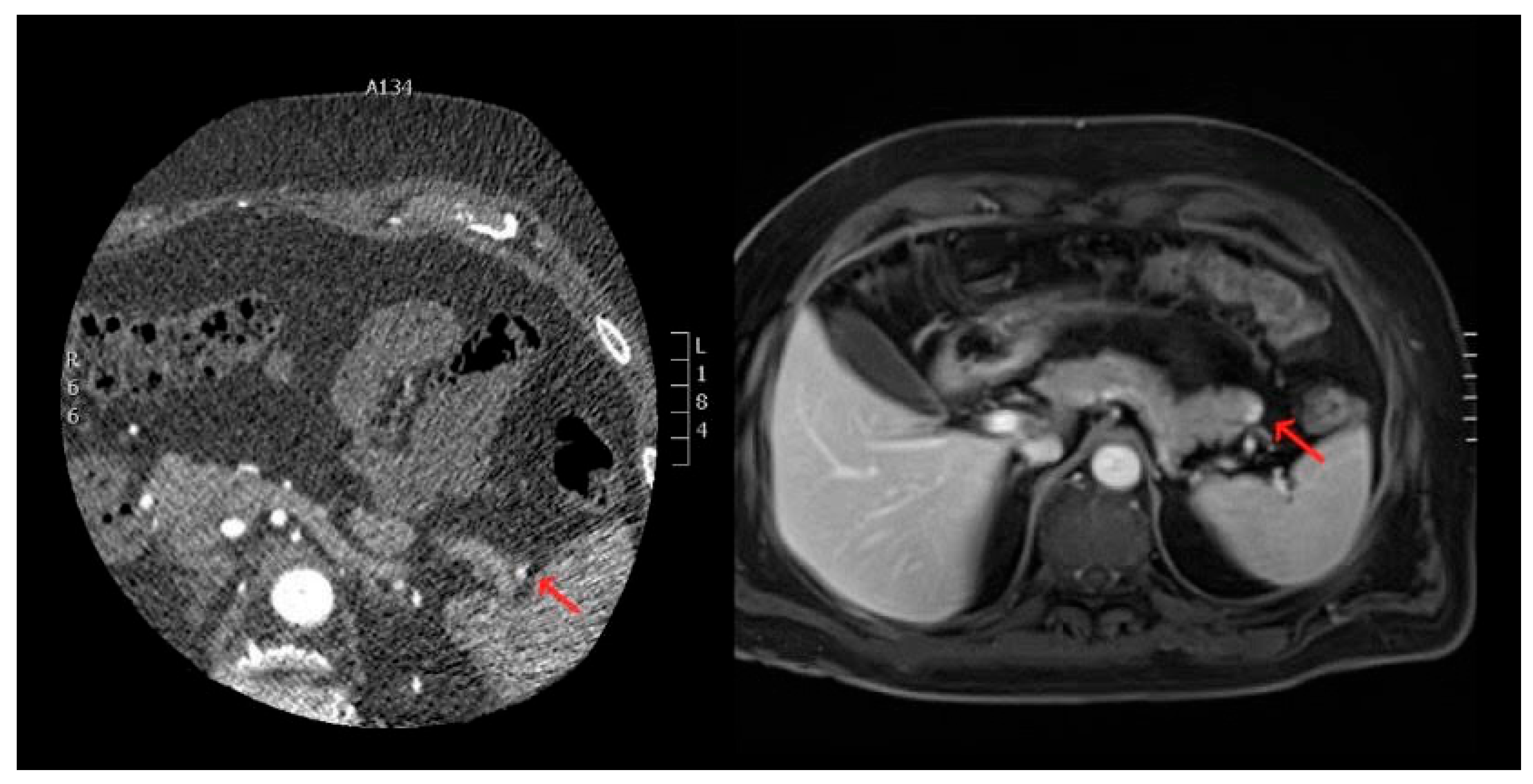
Figure 2.
CT-scan with the use of lung-window: there is evidence of a pulmonary nodule unknown (on the left, with red arrow), and in another patient we had found a solid formation of the right ilum (on the right).
Figure 2.
CT-scan with the use of lung-window: there is evidence of a pulmonary nodule unknown (on the left, with red arrow), and in another patient we had found a solid formation of the right ilum (on the right).
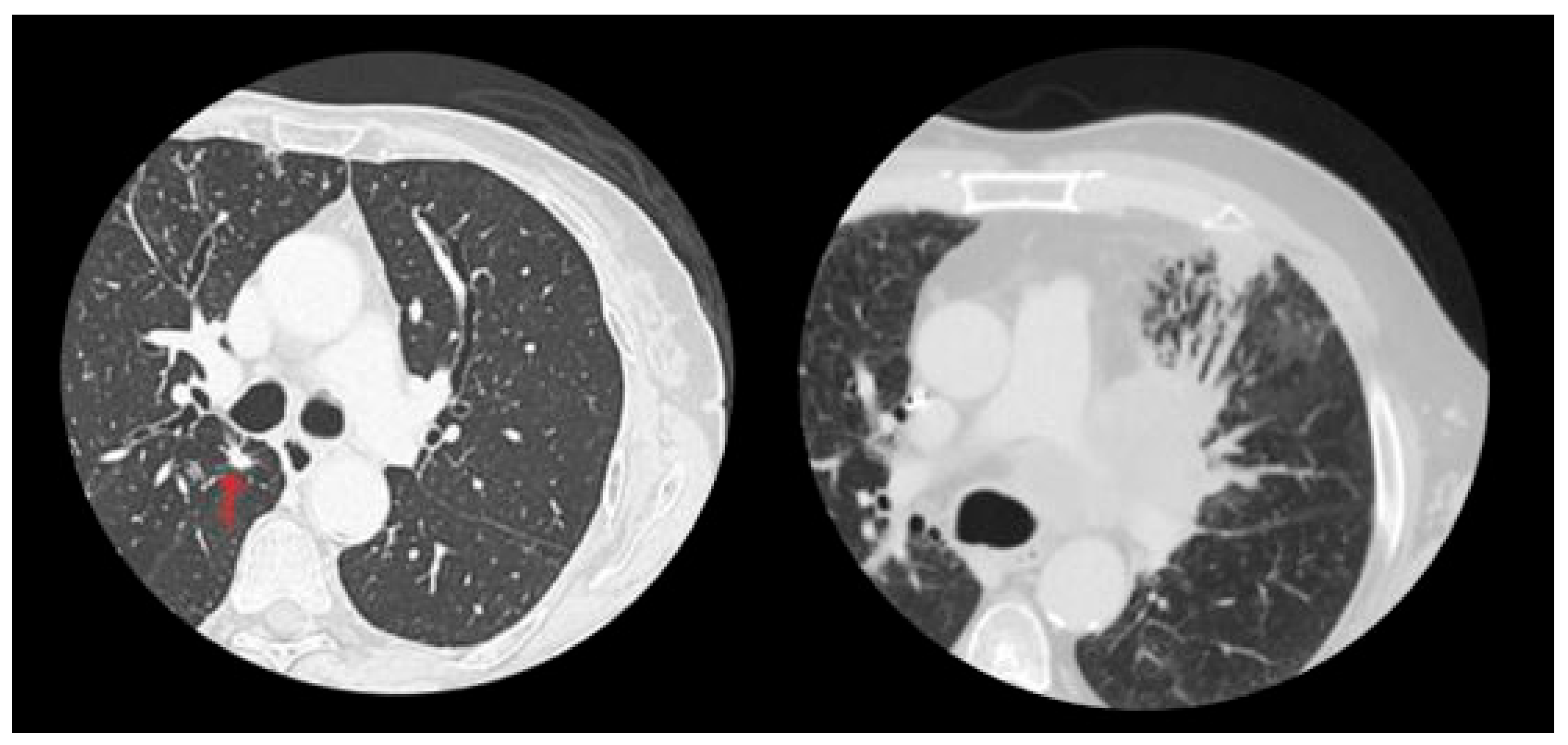
Figure 3.
Some unexpected cardiac findings, different from CAD or stenosis on the coronary arteries, are shown such as A) inter-atrial aneurism; B) inter-ventricular incontinence; C) a mass on the left ventricle; D) a rate of pericardial effusion.
Figure 3.
Some unexpected cardiac findings, different from CAD or stenosis on the coronary arteries, are shown such as A) inter-atrial aneurism; B) inter-ventricular incontinence; C) a mass on the left ventricle; D) a rate of pericardial effusion.
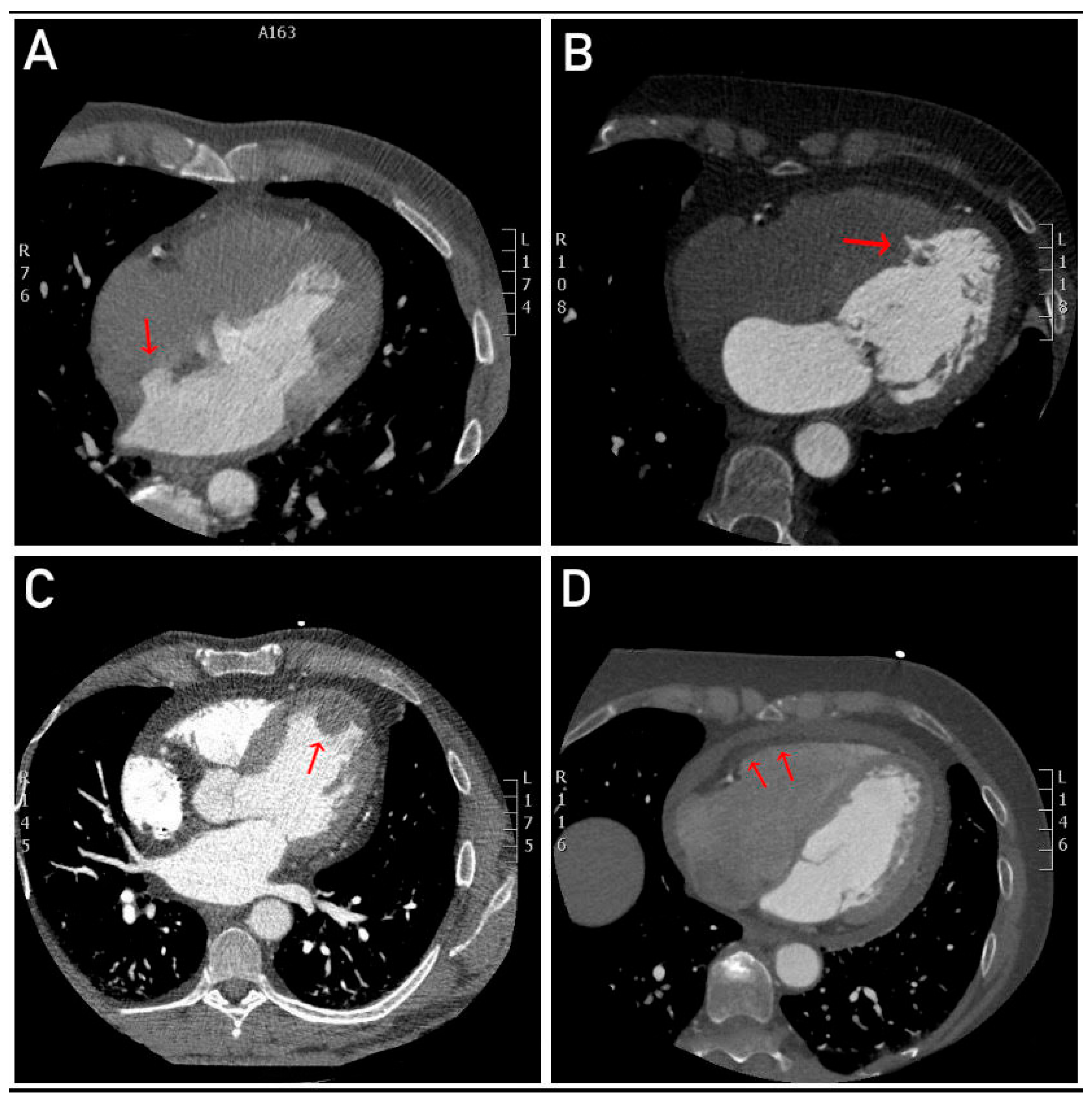
Figure 4.
A retrosternal mass, though rare, can indicate serious conditions like malignancies or lymphadenopathy. Its detection during cardiac CT requires further investigation to rule out life-threatening issues, enabling timely intervention and improved clinic.
Figure 4.
A retrosternal mass, though rare, can indicate serious conditions like malignancies or lymphadenopathy. Its detection during cardiac CT requires further investigation to rule out life-threatening issues, enabling timely intervention and improved clinic.
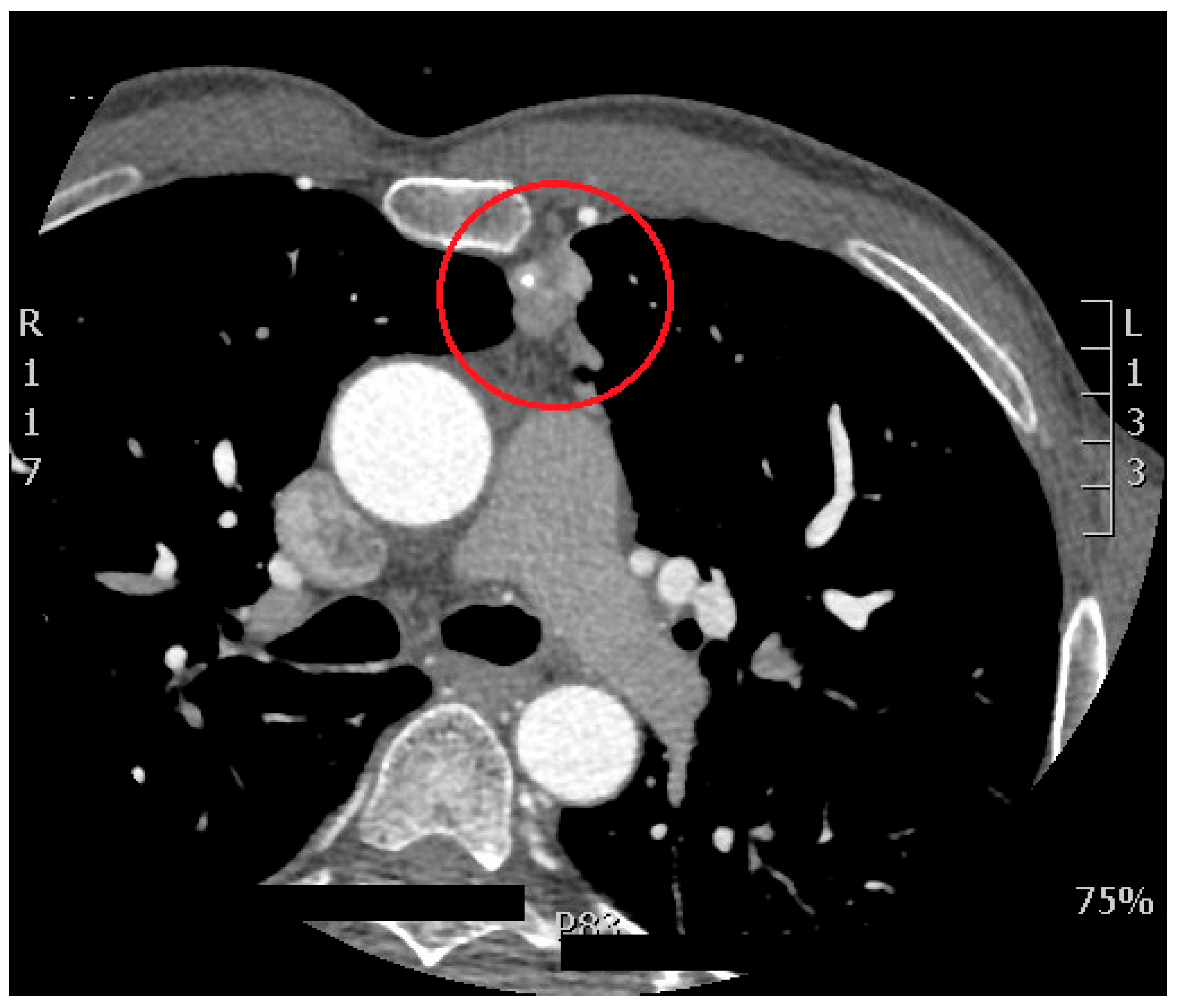
Chart 1.
The graph summarizes all the CTs and is significant because it clearly shows the percentage of patients with incidental findings on the total: it is always critical to study all the structures properly and thoroughly in the FOV. There is also the percentage of “positive” CTs displayed, which must always be a small proportion of the total.
Chart 1.
The graph summarizes all the CTs and is significant because it clearly shows the percentage of patients with incidental findings on the total: it is always critical to study all the structures properly and thoroughly in the FOV. There is also the percentage of “positive” CTs displayed, which must always be a small proportion of the total.


Table 1.
Incidental Findings in Cardiac-CT scans: This table summarizes the results of cardiac-CT scans conducted at the “Dimiccoli” Hospital in Barletta, Italy, from April 2022 to April 2024. The columns represent the following: “Month and Year” shows the time of the examinations, “Total of Exam” indicates the total number of scans performed in each month, “Type of Incidental Finding at CT Scan” lists the various incidental findings identified during the scans, and “Number of Positive Cardiac-CT” represents the number of patients who had a disease of the coronaries. The incidental findings include a variety of conditions such as pericardial effusion, pulmonary nodules, hiatal hernia, and COPD, among others. The table highlights the frequency and diversity of incidental findings, illustrating the importance of a thorough evaluation of the entire thoracic-abdominal region in cardiac CT scans.
Table 1.
Incidental Findings in Cardiac-CT scans: This table summarizes the results of cardiac-CT scans conducted at the “Dimiccoli” Hospital in Barletta, Italy, from April 2022 to April 2024. The columns represent the following: “Month and Year” shows the time of the examinations, “Total of Exam” indicates the total number of scans performed in each month, “Type of Incidental Finding at CT Scan” lists the various incidental findings identified during the scans, and “Number of Positive Cardiac-CT” represents the number of patients who had a disease of the coronaries. The incidental findings include a variety of conditions such as pericardial effusion, pulmonary nodules, hiatal hernia, and COPD, among others. The table highlights the frequency and diversity of incidental findings, illustrating the importance of a thorough evaluation of the entire thoracic-abdominal region in cardiac CT scans.
| Month and year | Total of exam | Type of incidental finding at CT scan | Number of positive Cardiac-CT |
| APRIL, 2022 | 5 | - | |
| 1 patient with dyspnea on exertion | STRATUM OF PERICARDIAL EFFUSION | ||
| MAY, 2022 | 13 | 2 | |
| 1 patient with a control of stent apposition | NODULAR FORMATION AT THE MYOCARDIUM | ||
| 1 patient with epigastric pain | PULMONARY MICRONODULE AND JATAL HERNIA | ||
| 1 patient with breathlessness | PULMONARY NODULES | ||
| JUNE, 2022 | 10 | - | |
| - | - | ||
| JULY, 2022 | 13 | - | |
| 1 patient with epigastric pain | STRATUM OF PERICARDIAL EFFUSION | ||
| 1 patient with hypertension, and a previous surgical procedure on the aorta | REVASCULARIZATION OF THE FALSE LUMEN OF A PREVIOUSLY SURGICALLY TREATED AORTIC DISSECTION | ||
| AUGUST, 2022 | 6 | - | |
| 1 patient with dyspnea on exertion | RIGHT BREAST THICKENING. ON THROUGH-ABDOMEN SCANS: LITHIASIS OF THE GALLBLADDER |
||
| 1 patient with breathlessness | ON THROUGH-ABDOMEN SCANS: HYPODENSE FORMATION AT THE IVS OF THE LIVER AND RETROPERITONEAL LYMPHADENOPATHY | ||
| SEPTEMBER, 2022 | 12 | 1 | |
| 1 patient with dyspnea on exertion | STRATUM OF PERICARDIAL EFFUSION | ||
| 1 patient with epigastric pain | STRATUM OF PERICARDIAL EFFUSION AND JATAL HERNIA | ||
| OCTOBER, 2022 | 12 | 2 | |
| 1 patient with angor | RETROSTERNAL SOLID TISSUE | ||
| 1 patient with epigastric pain | CONSISTENT JATAL HERNIA | ||
| NOVEMBER, 2022 | 27 | 3 | |
| - | - | ||
| DECEMBER, 2022 | 11 | ||
| - | - | ||
| JANUARY, 2023 | 19 | 1 | |
| 1 patient with dyspnea on exertion | ON THROUGH-ABDOMEN SCANS: HYPODENSE FORMATION AT THE VS AND VIIIS OF THE LIVER | ||
| FEBRUARY, 2023 | 21 | 3 | |
| 1 patient with epigastric pain | ON THROUGH-ABDOMEN SCANS: HYPODENSE FORMATION AT THE IVS AND VIIS OF THE LIVER | ||
| MARCH, 2023 | 33 | 4 | |
| 1 patient with epigastric pain | CONSISTENT JATAL HERNIA | ||
| APRIL, 2023 | 11 | - | |
| 1 patient with dyspnea on exertion | PATENCY OF THE INTERVENTRICULAR SEPTUM | ||
| 1 patient with dyspnea | PULMONARY PARENCHYMAL THICKENING WITH SUBPLEURAL AND INTERLOBULAR THICKENING | ||
| 1 patient with epigastric pain | CONSISTENT JATAL HERNIA | ||
| 1 patient with breathlessness | COPD (CHRONIC OBSTRUCTIVE PULMONARY DISEASE) SIGN | ||
| 1 patient with occasional chest pain | INTRAMURAL ANEURYSM OF THE INTERATRIAL SEPTUM WITHOUT OBVIOUS SHUNT | ||
| MAY, 2023 | 28 | 3 | |
| 1 patient with dyspnea on exertion | COPD SIGN | ||
| 1 patient with arrhythmia and cardiovascular risk factors | CONSOLIDATIVE PULMONARY FOCUS FROM PROBABLE INFLAMMATORY OUTCOME | ||
| 1 patient with dyspnea on exertion | RIGHT VENTRICULAR LATERAL MARGIN THICKENING WITH CONSENSUAL LUNG CONSOLIDATION | ||
| JUNE, 2023 | 27 | 7 | |
| 1 patient with dyspnea on exertion | SUSPICIOUS AREA WITH CONTRAST ENHANCEMENT AT THE TAIL OF THE PANCREAS | ||
| JULY, 2023 | 12 | 2 | |
| 1 patient with dyspnea on exertion and breathlessness | COPD SIGN | ||
| 1 patient with epigastric pain | CONSISTENT JATAL HERNIA | ||
| AUGUST, 2023 | 7 | - | |
| 1 patient with epigastric pain | CONSISTENT JATAL HERNIA | ||
| SEPTEMBER, 2023 | 8 | 2 | |
| 1 patient with occasional heart palpitation | NEGATIVE T WAVE ON ECG MONITORING | ||
| OCTOBER, 2023 | 16 | 2 | |
| 1 patient with dyspnea on exertion | CYLINDRICAL AND CYSTIC BRONCHIECTASIS, 8 MM PULMONARY NODULE, AND ADDITIONAL MICRONODULES WITH LYMPHADENOPATHY (11 MM THE LARGEST SUBCARINAL) | ||
| 1 patient with occasional chest pain | ABUNDANT SHARE OF PERICARDIAL FAT | ||
| 1 patient with cardiovascular risk factors | MICRONODULE (6MM) AT THE LINGULA AND PLEURAL PLAQUES | ||
| NOVEMBER, 2023 | 10 | 1 | |
| 1 patient with dyspnea on exertion | LUNG NODULES OF ABOUT 12 AND 9 MM | ||
| 1 patient with cardiovascular risk factors, and increased phlogosis indices | PERICARDIAC PULMONARY PARENCHYMAL CONSOLIDATION | ||
| DECEMBER, 2023 | 10 | 2 | |
| 1 patient with breathlessness |
COPD (CHRONIC OBSTRUCTIVE PULMONARY DISEASE) SIGN | ||
| JANUARY, 2024 | 6 | 1 | |
| 1 patient with dyspnea on exertion |
OSTEOLYTIC LESION AT THE SOMA OF T4 | ||
| FEBRUARY, 2024 | 9 | 1 | |
| MARCH, 2024 | 14 | 3 | |
| 1 patient with epigastric pain | CONSISTENT JATAL HERNIA | ||
| APRIL, 2024 | 12 | ||
| 1 patient with dyspnea on exertion | CALCIFIC LYMPH NODE IN MEDIASTINUM |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



