Submitted:
17 December 2024
Posted:
18 December 2024
You are already at the latest version
Abstract
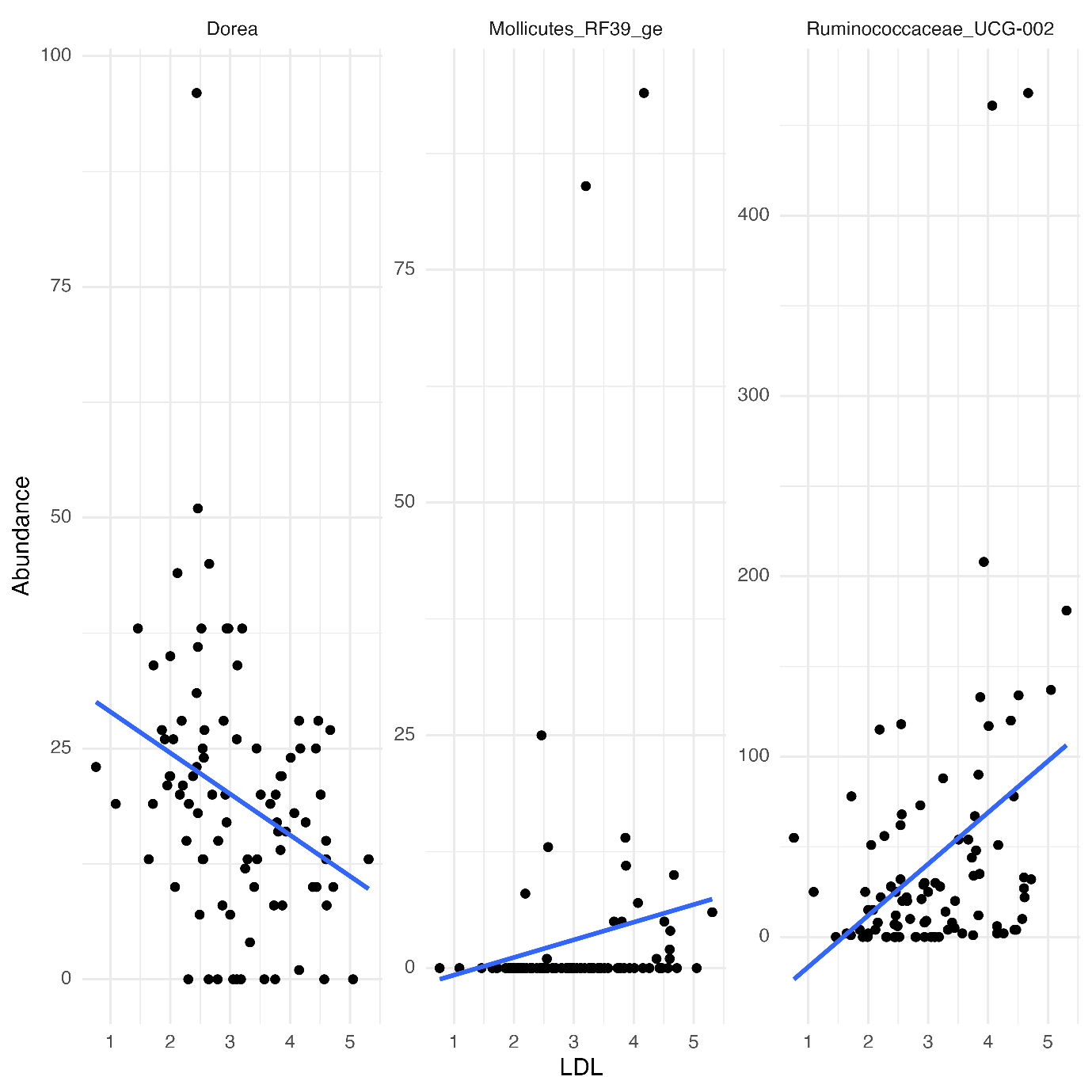
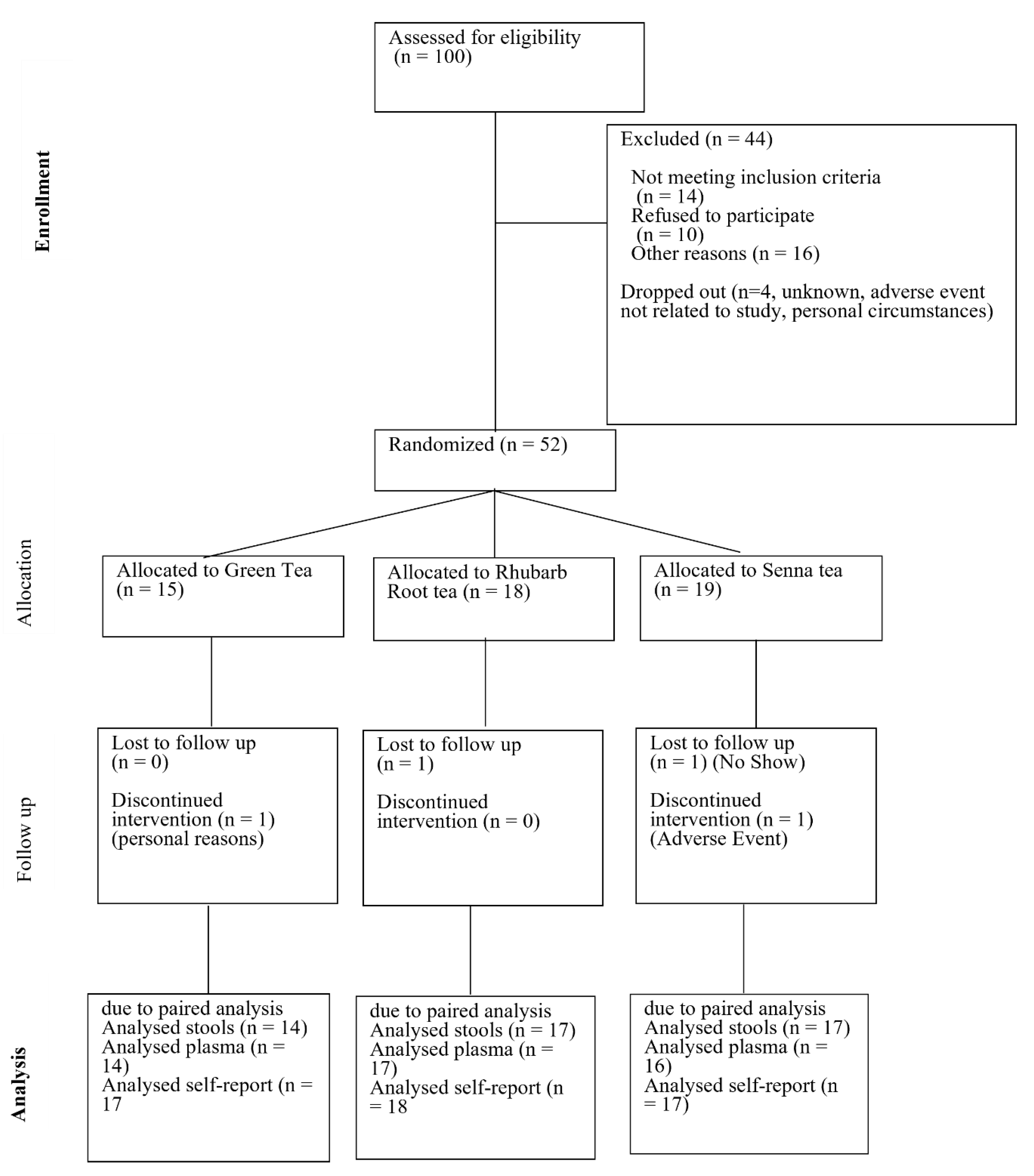
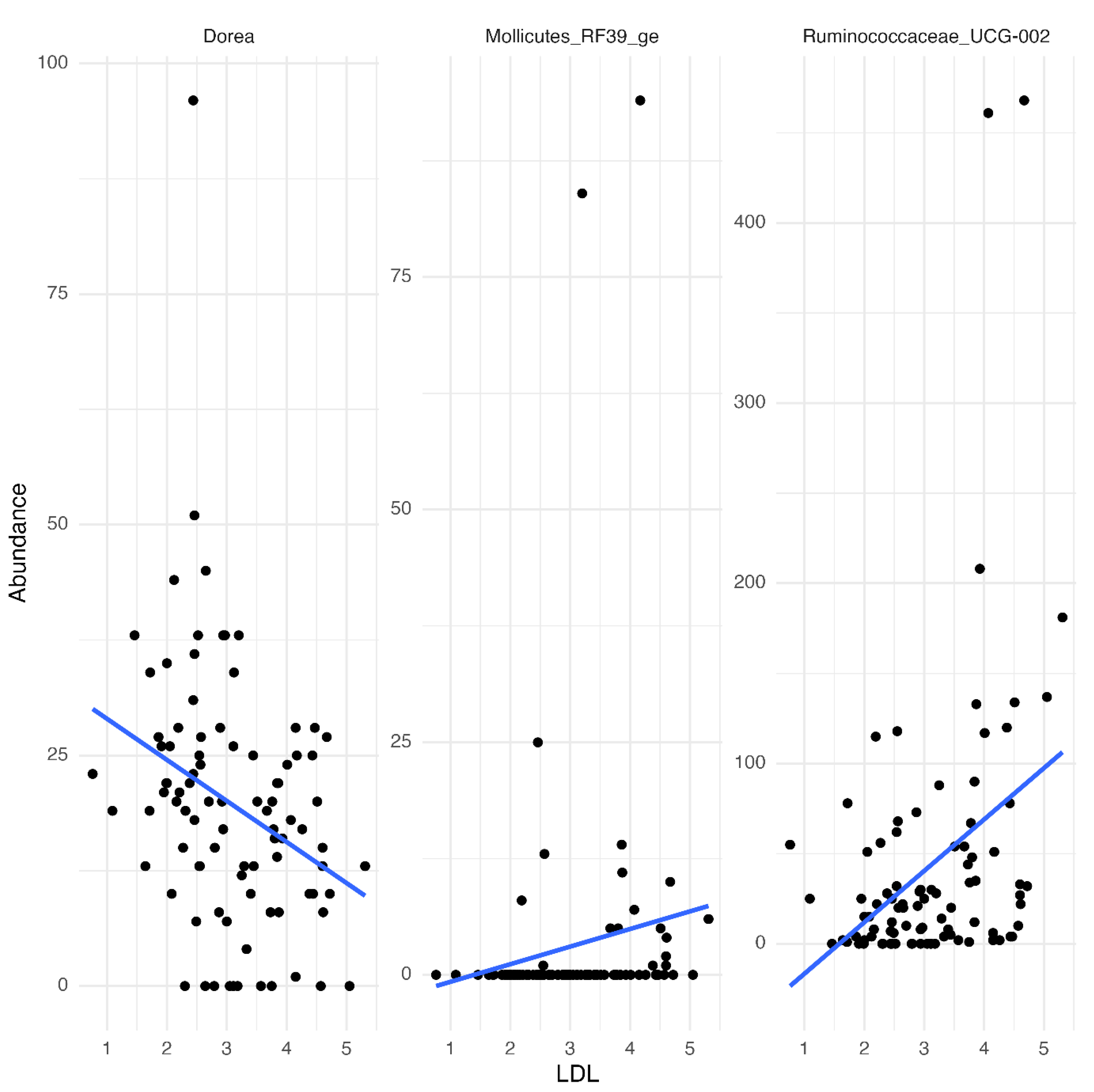
Background/Objectives: Cardiovascular diseases remain a leading cause of mortality and morbidity. The widespread use of herbs and medicinal plants in traditional medicine has garnered increasing recognition as a valuable resource for increasing wellness and reducing the onset of disease. Several epidemiologic and clinical studies have shown that altering blood lipid profiles and maintaining gut homeostasis may protect against cardiovascular diseases. Methods: A randomized, active-controlled parallel human clinical trial (n = 52) with three herbal tea infusions (green (Camellia sinensis) tea with rhubarb root, green tea with senna, and active control green tea) daily for 21 days in a free-living healthy adult cohort was conducted, to assess the potential for health benefits in terms of plasma lipids and gut health. Paired plasma samples were analyzed using Afinion lipid panels (total cholesterol, LDL (Low- Density Lipoprotein) cholesterol, HDL (High-Density Lipoprotein) cholesterol, triglycerides, and non-HDL cholesterol) and paired stools were analysed by 16S rRNA amplicon sequencing was used to determine bacterial diversity within the gut microbiome. Results: participants who provided fasted bloods before and after the in-tervention (n=47) the consumption of herbal rhubarb root tea and green tea significantly lowered total cholesterol, LDL-cholesterol, and non-HDL cholesterol (p < 0.05) in plasma after 21 days of daily consumption when compared with concentrations before the intervention. No significant change was observed in senna tea group. Participants who provided stool samples, across the different experimental groups (n=48), no significant differences in overall microbial composition between pre- and post-intervention was observed, even at the genus level. This suggests that, while specific bacterial genera correlate with LDL-cholesterol changes, the broader microbial commu-nity structure remains stable across the intervention period, unaffected by these other confounding factors. Diet and BMI was maintained in each of the three groups. Conclusions: it was found that drinking a cup of rhubarb root herbal or green tea infusion for 21 days produced beneficial effects on lipid profiles and maintained gut eubiosis without observable adverse effects in a healthy human cohort. More studies are needed to fully understand the effects of rhubarb root and green tea in fatty acid metabolism and gut microbial composition.
Keywords:
1. Introduction
2. Materials and Methods
2.1. Subjects
2.2. Sample Size Calculation
2.3. Study Design: Dose, and Type of Herbal Teas
2.4. Anthropometric Measures
2.5. Food Recall and Stool Consistency
2.6. Collection, Preparation of Blood Samples and Analysis
2.7. Collection, Preparation of Stool Samples and Analysis
3. Results and Discussion
4. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
References
- Pan, S.-Y. , et al, Tea and tea drinking: China’s outstanding contributions to the mankind. Chinese Medicine 2022, 17, 27. [Google Scholar] [CrossRef] [PubMed]
- Tang, G.-Y. , et al, Health Functions and Related Molecular Mechanisms of Tea Components: An Update Review. International Journal of Molecular Sciences 2019, 20, 6196. [Google Scholar] [CrossRef] [PubMed]
- Adefegha, S.A., G. Oboh, and O.O. Oluokun, Chapter 11 - Food bioactives: the food image behind the curtain of health promotion and prevention against several degenerative diseases, in Studies in Natural Products Chemistry, R. Atta ur, Editor. 2022, Elsevier. 391-421.
- Coimbra, S. , et al, Green tea consumption improves plasma lipid profiles in adults. Nutrition Research 2006, 26, 604–607. [Google Scholar] [CrossRef]
- Witkowski, M. L. Weeks, and S.L. Hazen, Gut Microbiota and Cardiovascular Disease. Circulation Research 2020, 127, 553–570. [Google Scholar] [CrossRef] [PubMed]
- Xu, R. , et al, Effect of green tea consumption on blood lipids: a systematic review and meta-analysis of randomized controlled trials. Nutr J 2020, 19, 48. [Google Scholar] [CrossRef] [PubMed]
- Yuan, F. , et al, Effects of green tea on lipid metabolism in overweight or obese people: A meta-analysis of randomized controlled trials. Molecular Nutrition & Food Research 2018, 62, 1601122. [Google Scholar]
- Liu, Y.-C. -Y.Li, and L. Shen, Modulation effect of tea consumption on gut microbiota. Applied Microbiology and Biotechnology 2020, 104, 981–987. [Google Scholar] [CrossRef] [PubMed]
- Bond, T. and E. Derbyshire, Tea Compounds and the Gut Microbiome: Findings from Trials and Mechanistic Studies. Nutrients 2019, 11.
- Xu, L., et al., Exploring the therapeutic potential of Cassia species on metabolic syndrome: A comprehensive review. South African Journal of Botany 2024, 173, 112–136. [CrossRef]
- Thaker, K. , et al, Senna (Cassia angustifolia Vahl.): A comprehensive review of ethnopharmacology and phytochemistry. Pharmacological Research - Natural Products 2023, 1, 100003. [Google Scholar] [CrossRef]

| Catechins | Absolute | Relative (% Total Catechins) |
| (ug/ml tea infusion) | ||
| Epigallocatechin (EGC) | 8.4 ± 1.9 | 50.0 |
| Epicatechin (EC) | 5.2 ± 0.5 | 31.2 |
| Epigallocatechin gallate (EGCG) | 2.2 ± 0.2 | 12.8 |
| Epicatechin gallate (ECG) | 1.0 ± 0.2 | 6.0 |
| Total | 16.8 ± 2.5 | 100 |
| Variable | Mean | (SD) |
| Demographics | ||
| Total taking part in study [n] | 52 | |
| Gender Female [n] | 45 | |
| Gender Male [n] | 7 | |
| Age [years]* | 52.86 | 12.53 |
| Age range (min-max) [years]* | 21-71 | |
| Anthropometrics | ||
| Weight [kg]* | 82.25 | 17.66 |
| Height [cm]* | 165.68 | 8.48 |
| BMI [kg m-²] * | 29.90 | 5.83 |
| Waist circumference [cm]* | 97.13 | 15.12 |
| Hip circumference [cm]* | 112.94 | 11.94 |
| Waist to Hip ratio* | 0.86 | 0.08 |
| M | 0.93 | 0.05 |
| F | 0.85 | 0.16 |
| Lipid group | Interaction | Df | estimate | SE | t.ratio | p.value |
| Cholesterol | Green tea: Baseline - post intervention | 44 | -0.2280 | 0.1170 | -1.9410 | 0.0587 |
| Rhubarb root herbal tea: Baseline - post intervention | 44 | -0.2860 | 0.1070 | -2.6830 | 0.0102* | |
| Senna herbal tea: Baseline - post intervention | 44 | -0.1290 | 0.1100 | -1.1720 | 0.2474 | |
| Triglycerides | Green tea: Baseline - post intervention | 44 | -0.2280 | 0.1170 | -1.9410 | 0.1920 |
| Rhubarb root herbal tea: Baseline - post intervention | 44 | -0.2860 | 0.1070 | -2.6830 | 0.2503 | |
| Senna herbal tea: Baseline - post intervention | 44 | -0.1290 | 0.1100 | -1.1720 | 0.7126 | |
| HDL-Cholesterol | Green tea: Baseline - post intervention | 44 | -0.2280 | 0.1170 | -1.9410 | 0.7903 |
| Rhubarb root herbal tea: Baseline - post intervention | 44 | -0.2860 | 0.1070 | -2.6830 | 0.6207 | |
| Senna herbal tea: Baseline - post intervention | 44 | -0.1290 | 0.1100 | -1.1720 | 0.8958 | |
| LDL-Cholesterol | Green tea: Baseline - post intervention | 44 | -0.2280 | 0.1170 | -1.9410 | 0.0011** |
| Rhubarb root herbal tea: Baseline - post intervention | 44 | -0.2860 | 0.1070 | -2.6830 | 0.0006** | |
| Senna herbal tea: Baseline - post intervention | 44 | -0.1290 | 0.1100 | -1.1720 | 0.0986 | |
| Cholesterol- HDL ratio | Green tea: Baseline - post intervention | 44 | -0.2280 | 0.1170 | -1.9410 | 0.0843 |
| Rhubarb root herbal tea: Baseline - post intervention | 44 | -0.2860 | 0.1070 | -2.6830 | 0.4957 | |
| Senna herbal tea: Baseline - post intervention | 44 | -0.1290 | 0.1100 | -1.1720 | 0.1421 | |
| non HDL-Cholesterol | Green tea: Baseline - post intervention | 44 | -0.2280 | 0.1170 | -1.9410 | 0.0219** |
| Rhubarb root herbal tea: Baseline - post intervention | 44 | -0.2860 | 0.1070 | -2.6830 | 0.0112** | |
| Senna herbal tea: Baseline - post intervention | 44 | -0.1290 | 0.1100 | -1.1720 | 0.2042 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).



