
Submitted:
16 December 2024
Posted:
17 December 2024
You are already at the latest version
Abstract
Background/Objectives: Recent researches on Mortality rate (MR) Vs Bionomic functionality (BF) in the territory of the province of Monza and Milan led to the knowledge of the state of the environment of each municipality. This study verifies the need for an anamnesis capable of highlighting the presence of Cumulative Environmental Stress (ECS) and verifies the differences between smoking and non-smoking patients in their relationship with the living environment. Methods: Two questionnaires collected the patients' responses. Their evaluation is based on the cumulative impact of stress due to an incorrect Cumulative Wrong Relationships (cWR), detected through Physio-Environmental parameters (Wrong Relationships (WR-Phys)) increased by the stress due to the Wrong Relationships "Psychosocial" environment (WR-PSoc). These tables were tested in the Pneumology department of the Vimercate Hospital (Monza-Brianza) in 70 lung cancer patients. cWR receives a further cumulative impact from the bionomic conditions of the landscape unit where the patient lives, measurable by BF, leading to ECS. Results: All cases present a high ECS (above the norm), so a correlation emerges between the disease and the patient-environment relationship. An indication of morbidity is related to ECS levels. Smoker and ex-smoker patients differ from non-smoker in oncological histotypes independently from BF levels, and the ECS values of smoker are higher due to the heavy WR-PSoc factors. Conclusions: The examined patients present a high ECS, so, the distorted human-environment relationship is also accompanied by severe illnesses. Anamnesis’ extension to environmental parameters is to be suggested, also as a prevention factor.
Keywords:
environmental anamnesis
; lung cancer
; cumulative Wrong Relationships (cWR)
; bionomic functionality (BF)
; environmental cumulative stress (ECS)
1. Introduction
The main responses of scientists to the environmental crisis, and its dangerous influence on the alteration of health, both of natural systems and of the human body, are the concepts of Sustainability and Planetary Health. These concepts need the help of ecology and medicine, which remain mostly reductionist, thus limiting their ability to fight the crisis. The systemic turning point [1,2,3] due to the paradigm shift in science can overcome this impasse by proposing new updating disciplines, such as the Biological Integrated Landscape Ecology, recently renamed Bionomy/Landscape Bionomics (LB) [4,5,6].
Landscape Bionomics updates the key critical principles of traditional ecology by recognizing (a) that the environment or, better, the Life on Earth is organized in a hierarchy of six interrelated and integrated space-time-information levels; each human organism is ontologically an integrated part of the hierarchy. Each level performs the intrinsic processes of life (birth, nourishment, growth, development, reproduction, death, etc.) properly following its proper space-time-information scale (complex living systems), (b) the territorial/landscape level represents the usual contest for the human person’s growth, life, and activities and (c) that it is possible to define a state of health for every level. The check of bionomic principles' ability to evaluate, in a very synthetic way, the state of health of a territorial/landscape unit and relate it to the incidence of human diseases has begun with encouraging results, finding other correlations in addition to the conventional ones [4,6,7,8].
However, a patient's anamnesis does not usually concern environmental parameters. As underlined in the preliminary study [8] on the need for a history of Cumulative Environmental Stress (ECS) in the patient, it would instead be necessary to expand the patient’s anamnesis in this sense. Note once again that a patient's organism is interrelated with two life systems: one internal (genome, cells, organs) and the other external (ecocoenotope, landscape unit, ecoregion) as expressed in Figure 1.
2. Materials and Methods
The impact assessment of the man/environment relationship concerning health is based -firstly- on the cumulative impact of the stress due to an improper man-environment relationship (cWR), detected through physio-environmental parameters (WR-Phys.) increased by the impacts of the stress due to the "Psycho-social" environment (WR-PSoc.) (Figure 2 A). Secondly, cWR receives a further cumulative impact from the bionomic conditions of the landscape unit where the patient lives, synthetically measured by the bionomic parameter of the Bionomic Functionality (BF) (Figure 2 B), leading to his/her Environmental Cumulative Stress (ECS) calculated by the ratio of cWR and BF.
To obtain cWR, two summary questionnaire tables were prepared to record the patient's responses. These tables were tested in the Pulmonology department of the Vimercate Hospital (province of Monza-Brianza, Lombardy, Northern Italy) with the collaboration of 70 lung cancer patients. All patients gave consent before completing the questionnaire. The first (Figure 3) investigates the history of their improper relationships with the physical and natural environment (WR-Phys), while the second (Figure 4) concerns the evaluation of stress due to the psychological and social environment (WR-PSoc).
The answers to all the questions also require a series of specifications and examples, able to guide the detection of patient responses, given that only some of them have the same level of cultural education. The present research was carried forward thanks to the assistants who helped the patients answer the questionnaires correctly. A seminar was held precisely before the start of the surveys.
Biological Territorial Capacity of Vegetation (BTC) is based on the concept of resistance stability, the type of vegetation community, its metabolic data and level organization. BTC measured in Mcal/m2/year [4,6,9].
The human habitat (HH), that is the % of the territory totally managed by humans in each municipality analysed [10].
It was possible to build the simplest mathematical model of bionomic normality, available for the first framing of the dysfunctions of landscape units.
The curve green represents the normal condition (BTCnorm), while BTCsurv is the surveyed value in the examined territory.
The BTCsurv was analysed for each municipality of residence of each patient and was compared to the BTCnorm (1) (given by the equation of the second-degree polynomial curve) [Figure 5].
BTCnorm = 0.0007x2 – 0.1518x + 8.85 (where x is HH=%LU)
The ratio BTCsurv/BTCnorm is the Bionomic Functionality (BF). Below normal values of bionomic functionality (BF = 1.15-0.85), with a tolerance interval of 0.15 from the curve of normality, we can register three levels of abnormal BF: altered (BF = 0.85-0.65), dysfunctional (BF = 0.65-0.45) and degraded (BF < 0.45). The vertical bars divide the main types of landscapes, from Forest-Natural (high BTC natural) to Dense-Urban: each of them may present an environmental syndrome [Figure 5, Table 1]. So, BF=1.0 corresponds to the value expressing the correct relationship (normality in scientific meaning) [6].
Previous studies have highlighted an inverse correlation between mortality rate (MR, ten years average) and BF [Figure 6] and were conducted in the province of Monza and Brianza (55 municipalities), 8 in the NE periphery of Milan and 9 sectors of the city of Milan [11].
Table 1 shows the ranges for the various calculated parameters, starting from the optimal state (normal) up to the maximum impairment.
2.1. Ethical considerations, data source and analysis.
Data used in this study are anonymous and each patient gave written consent to complete the questionnaire.
Human participants were involved in this research; the study was conducted in accordance with the Declaration of Helsinki. Our study was approved by the local institution, Vimercate Hospital, ASST-Brianza, according to the legal requirements concerning observational studies (Resolution 0000135, February 27, 2023).
For data analysis and correlation significance, Pearson analysis was employed to investigate the statistical relationship between the outcome variables and the covariances. The trend equations were based on Microsoft Excel.
3. Results
Table 2 summarizes the global results obtained for WR-Phys, WR-PSoc and cWR as mean, standard deviation, maximum value, and minimum value. The cWr is the cumulative value obtained from the physio-environmental questionnaire and the psycho-social questionnaire. The BF represents the bionomic functional values of BF for LU in the province of Monza and Brianza. The indicated ECS is obtained as the average of the value obtained from the ratio between cWR and BF for each patient.
The distribution of patients examined in the five ECS classes [Table 1, Figure 7]. As it can be seen, this distribution does not follow a classical Gaussian curve but is completely shifted towards a high ECS, leaving the first two classes empty (or almost empty).
The ECS values for each patients, no patients have an ECS ≤ 25 (normal value) [Figure 8].
The subdivision of lung cancers according to histotype is summarized in Figure 9. Note that our 70 patients present histotypes very near the known general averages: Adenocarcinoma=60%, Squamous carcinoma 25%, Small-cell carcinoma=5%, Other=10%.
This section may be divided by subheadings. It should provide a concise and precise description of the experimental results, their interpretation, as well as the experimental conclusions that can be drawn.
Adenocarcinoma is confirmed as the most frequent form and even higher in percentage in non-smokers [Figure 10].
Smokers and ex-smoker patients differ from no smokers in oncological histotype independently from BF levels [Table 3]. ECS value of smokers is higher: this difference is due to the substantial diversity of WR-PSoc and, therefore, a greater psychosocial fragility. Furthermore, smokers get sick even living in a "better" environment, i.e., with a higher BF than non-smokers (+5%). Therefore, non-smokers and ex-smokers are more sensitive to the state of the environment of their Landscape Units (LU), as shown by the WR-Phys/WR-PSoc ratios: 1.17 for smokers vs. 1.46 for non-smokers (+ 25%) and 1.6 for ex-smokers (+ 37%).
4. Discussion
Over the years, we have witnessed a change in lung neoplastic pathology, with the transition from predominantly squamous cell neoplasms found mostly in the main bronchial tracts and heavy smoking patients [12], to neoplasms predominantly in the peripheral bronchial tracts, especially adenocarcinomas, often found in Non-Smoking. [13,14,15].
The results of previous studies demonstrate a possible link between environmental alterations (i.e. pm 2.5 or lack of natural forests) and the development of lung cancers [16]. Results of several epidemiological studies have shown higher risks for lung cancer in association with various measures of air pollution [17,18] and suggested an association mainly in non-smokers [19,20] and never-smokers [21,22]
The Vimercate Hospital is in the center of the catchment area of the province of Monza-Brianza, effectively united with the city of Milan (Italy). Research on the environmental history of this territory has been being conducted by Ingegnoli since 2011: these studies [6,11] show a clear correlation between the mortality rate (MR) and the bionomic functionality (BF) of the 72 municipalities understood as landscape units (LU), that is between the alteration of the environment (regardless of pollution) and the alteration of human health.
The prevalence of adenocarcinoma is confirmed in our sample, which is even greater in non-smokers than in smokers, as has been known in the literature [13].
As shown in Table 3, ex-smokers maintain similarities with smokers in the frequencies of cancer histotypes (52.4 and 55.2% of adenocarcinoma vs. 80% of non-smokers (difference of approximately 32.5%)).
Regarding the other parameters examined, ex-smokers and non-smokers have complete overlap: Wr-Phys., Wr-PSoc., cWR, BF ed ECS.
Smokers and ex-smoker patients differ from no smokers in oncological histotype independently from BF levels [Table 3] and the ECS value of smokers is higher: this difference is due to the substantial diversity of WR-PSoc and, therefore, a greater psychosocial fragility. In addition, smokers get sick regardless of the environment in which they live.
The smoking habit seems to have irreversibly affected the histotype of lung cancer with no apparent difference between active and former smokers.
In particular, the importance of environmental history is underlined, verifying that the values of environmental stress, psychosocial stress and the consequent cWr are significantly increased in patients who have developed a lung neoplastic disease. Given that the first evaluation class corresponds to normality (12-25) [Table 1], no patient shows a good relationship with the environment: all cancer patients present high environmental stress.
From a practical point of view, high cWr values found in the population without evidence of disease could lead to more in-depth and closer clinical-instrumental checks, for preventive purposes.
The previous studies have demonstrated a significant impairment of BF values in the patients' areas of residence.
An Ethological Alarm Signal leads to environmental stress, which can be chronic. An alarming meaning registers all the environmental alterations, which remain memorized within our cells. To reach this goal the ethological process must be innate and unconscious because to de-codify environmental signals we must reduce emotions.
Stressors simultaneously activate (i) neurons in the hypothalamus, which secrete CRH (Corticotropin-releasing hormone), and (ii) adrenergic neurons. These responses potentiate each other. The final effect of the activation of neurons that secrete CRH is the increase in cortisol levels, while the net effect of adrenergic stimulation is to increase in plasma levels of catecholamine (Dopamine, norepinephrine, and epinephrine).
The negative feedback exerted by cortisol can limit an excessive reaction, which is dangerous for the organism. However, when the stress becomes chronic, the circadian rhythm of melatonin/cortisol is altered. Plasma cortisol levels bring to a dominance of the Th2 immune circuit, with the production of typical interleukin (e.g., IL-4, IL- 5, IL- 13) and the circuit Th17 [23]. Note that the Th2 immune response is not available to counteract viral infections, neo-plastic cells, and auto-immune syndromes, which need a Th1 response. So, the premature death risk increases.
The results of the present studies show that consciousness and sub-consciousness and biological development of man can be affected even just by the effects and/or the reverberation of the anomalies in the structure, function, and behavior of the surrounding environment, and that all of us perceive, process, and react to all these anomalies even before the bionomic quality and efficiency of that surrounding is known. So, morbidity is linked not only to good environmental conditions but to our modality of interaction with the environment, our modality of living within the environment, even if it is altered, independently from pollution and type of energy supply or recycling of materials, etc.
STUDY LIMITATION:
The present questionnaires are in review, as they must be upgraded and/or implemented. The possibility of developing this anamnesis also depends on academic updating in medicine, biology, and the natural and environmental sciences. Only developing an integrated biological discipline, such as Landscape Bionomic, allows for effective environmental stress detection.
To obtain the ECS it is essential to have the BF of the patients' area of residence, previously assessed by the ecologist specialist. The BF obtained remains valid for approximately 15-20 years [8].
The small number of patients studied limits the evaluation regarding smokers and non-smokers.
5. Conclusions
Extending the anamnesis to macro-scale environmental parameters is likely to be suggested, as a high ECS found in patients monitored or treated for minor syndromes can push doctors to extend the analyses for prevention.
Medical prevention should be updated, extending the anamnesis to environmental factors, which, as we have said, are complex and linked in a system of cumulative impacts.
Author Contributions
Conceptualization, V.I.; methodology, V.I., L.B., S.P. and P.S.; software, V.I.; formal analysis, V.I.; data curation, S.R., C.B., M.C.S., R.R., C.M., S.A., R.M., S.A.A., M.P. and M.S.C..; writing—original draft preparation, V.I..; writing—review and editing, V.I., S.P. and P.S.; supervision, V.I. and L.B.. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki, and approved by the Institutional Review Board, Vimercate Hospital, ASST-Brianza, according to the legal requirements concerning observational studies (Resolution 0000135, February 27, 2023).
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
The datasets analyzed during the current study are available from the corresponding author on reasonable request.
Acknowledgments
All nurses and healthcare support workers in the Pulmonology department of the Vimercate Hospital for their assistance to the patients.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Agazzi, E. Science, Methaphysics, Religion; Franco Angeli, 2014; ISBN 9788891718280.
- Agazzi, E. Systemic Thinking. In: Matthews, M.R. (Eds) Mario Bunge: A Centenary Festschrift. Springer 2019, 219–240. [CrossRef]
- Ulivi, L. The Systemic Turn in Human and Natural Sciences A Rock in The Pond. Contemp. Syst. Think. 2019, 205.
- Ingegnoli, V. Landscape Ecology: A Widening Foundation; Springer-Verlag Berlin and Heidelberg GmbH & Co. KG, Ed.; 2002; ISBN 978-3-540-42743-8.
- Ingegnoli, V. Bionomia Del Paesaggio. L’ecologia Del Paesaggio Biologico-Integrata per La Formazione Di Un “Medico” Dei Sistemi Ecologici.; 2011; ISBN 9788847020405.
- Ingegnoli, V. Landscape Bionomics Biological-Integrated Landscape Ecology; Springer Milano, 2015; ISBN 978-88-470-5225-3.
- Ingegnoli Vittorio, E.G. Covid-19 Incidence and Its Main Bionomics Correlations in the Landscape Units of Monza-Brianza Province, Lombardy. J. Environ. Sci. Public Heal. 2020, 4, 349–366. [CrossRef]
- Ingegnoli, V.; Lombardo, F.; Torre, G. La; Lenzi, A. Environmental Alteration Leads to Human Disease : A Planetary Health Approach; Sustainable Development Goals Series; Springer International Publishing: Cham, 2022; ISBN 978-3-030-83160-8. [CrossRef]
- Baltimore D., Dulbecco R., Jacob F., Levi- Montalcini R., Ingegnoli V. Landscape Ecology. Landsc. Ecol. 2001, IV, 489–508.
- Ingegnoli, V. Importance of the Btc Function in the Environment-Health Relationships. 2024, [preprint], 17.
- Ingegnoli, V.; Giglio, E. Complex Environmental Alterations Damages Human Body Defence System: A New Bio-Systemic Way of Investigation. WSEAS Trans. Environ. Dev. 2017, 13, 170–180.
- U.S. National Cancer Institute and World HealthOrganization. The Economics of Tobacco and TobaccoControl. National Cancer Institute Tobacco ControlMonograph21. NIH Publication. Bethesda, MD, U.S. 2016.
- Raaschou-Nielsen, O.; Andersen, Z.J.; Beelen, R.; Samoli, E.; Stafoggia, M.; Weinmayr, G.; Hoffmann, B.; Fischer, P.; Nieuwenhuijsen, M.J.; Brunekreef, B.; et al. Air Pollution and Lung Cancer Incidence in 17 European Cohorts: Prospective Analyses from the European Study of Cohorts for Air Pollution Effects (ESCAPE). Lancet Oncol. 2013, 14, 813–822. [CrossRef]
- Gabrielson E. Worldwide trends in lung cancer pathology. Respirology 2006; 11: 533–38. [CrossRef]
- Schuller HM. Mechanisms of smoking-related lung and pancreatic adenocarcinoma development. Nat Rev Cancer 2002; 2: 455–63. [CrossRef]
- Zeng, Q.; Vogtmann, E.; Jia, M. man; Parascandola, M.; Li, J. bin; Wu, Y. ling; Feng, Q. fu; Zou, X. nong Tobacco Smoking and Trends in Histological Subtypes of Female Lung Cancer at the Cancer Hospital of the Chinese Academy of Medical Sciences over 13 Years. Thorac. Cancer 2019, 10, 1717–1724. [CrossRef]
- Pope III CA, Burnett RT, Thun MJ, et al. Lung cancer, cardiopulmonary mortality, and long-term exposure to fi ne particulate air pollution. JAMA 2002; 287: 1132–41. [CrossRef]
- Cesaroni G, Badaloni C, Gariazzo C, et al. Long-term exposure to urban air pollution and mortality in a cohort of more than a million adults in Rome. Environ Health Perspect 2013; 121: 324–31. [CrossRef]
- Raaschou-Nielsen O, Andersen ZJ, Hvidberg M, et al. Lung cancer incidence and long-term exposure to air pollution from traffi c. Environ Health Perspect 2011; 119: 860–65. [CrossRef]
- Yorifuji T, Kashima S, Tsuda T, et al. Long-term exposure to traffi c-related air pollution and mortality in Shizuoka, Japan. Occup Environ Med 2010; 67: 111–17. [CrossRef]
- Beelen R, Hoek G, van den Brandt PA, et al. Long-term exposure to traffi c-related air pollution and lung cancer risk. Epidemiology 2008; 19: 702–10. [CrossRef]
- Raaschou-Nielsen O, Bak H, Sorensen M, et al. Air pollution from traffi c and risk for lung cancer in three Danish cohorts. Cancer Epidemiol Biomarkers Prev 2010; 19: 1284–91. [CrossRef]
- Bottaccioli F, B.A.G. Psyco Neuro Endocrine Immunology and Science of the Integrated Care - The Manual; Milano.; Edra, 2020; ISBN 9788821449222.
Figure 1.
As set out in the logical scheme, a medical doctor (MD) must repair the damage caused by environmental syndromes to human health, leading to most diseases. He must act considering the co-presence of two life systems internal and external to the organism, to arrive at integrated therapies.
Figure 1.
As set out in the logical scheme, a medical doctor (MD) must repair the damage caused by environmental syndromes to human health, leading to most diseases. He must act considering the co-presence of two life systems internal and external to the organism, to arrive at integrated therapies.
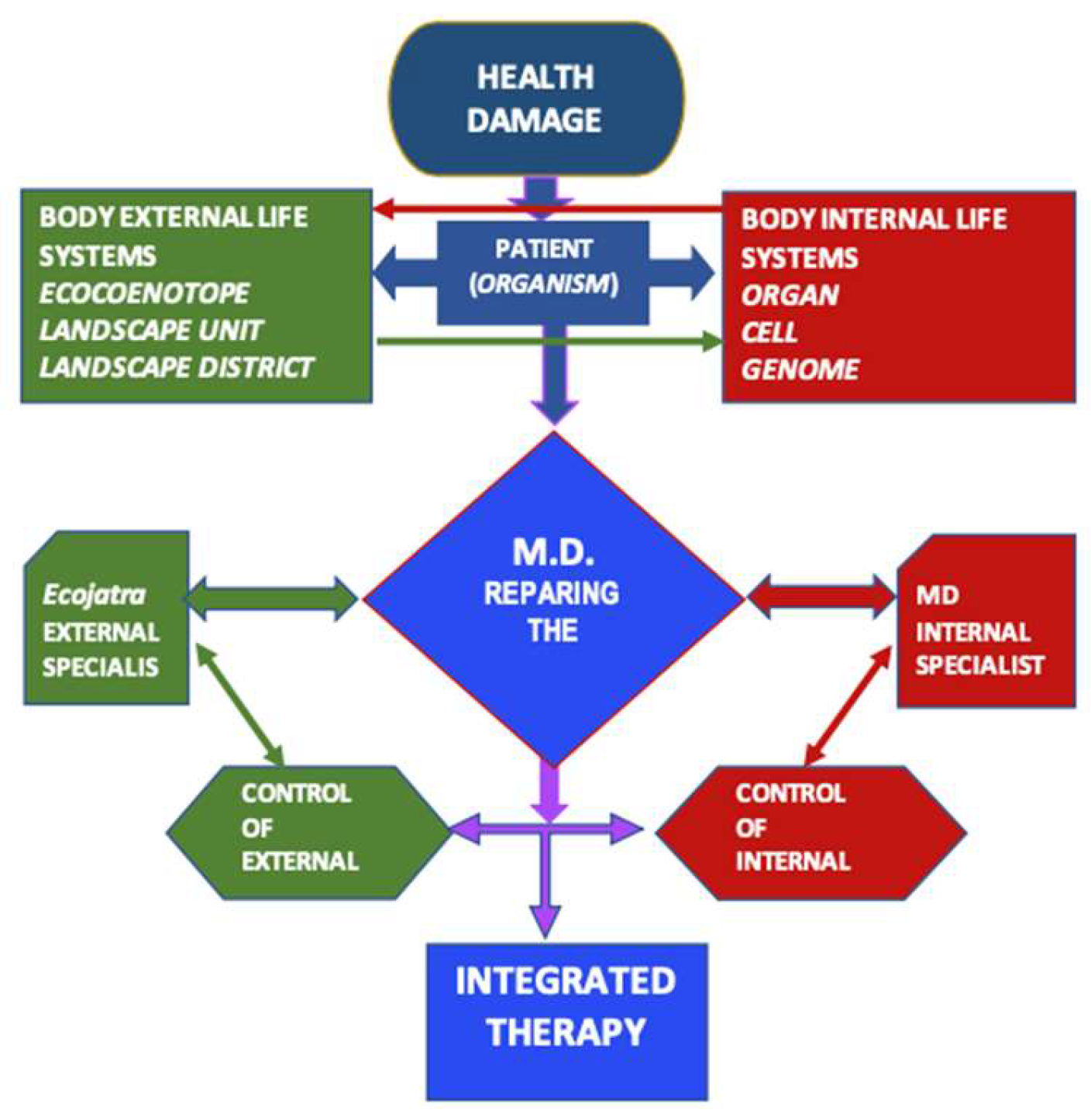
Figure 2.
Diagram of the relationships between man and the environment necessary to propose specific indicators that can be developed into two integration scales: patient scale and ecologist scale.
Figure 2.
Diagram of the relationships between man and the environment necessary to propose specific indicators that can be developed into two integration scales: patient scale and ecologist scale.
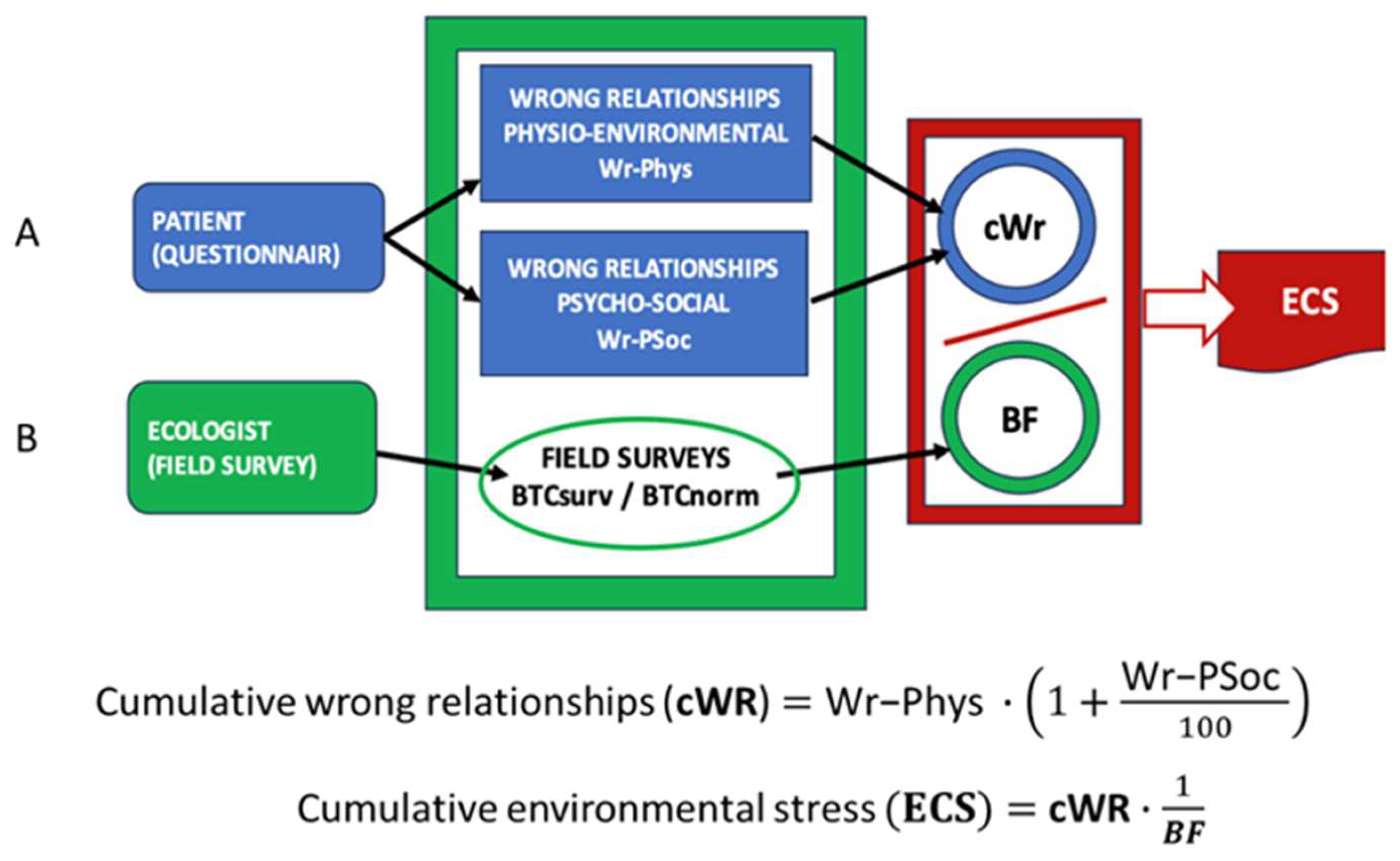
Figure 3.
Anamnesis of wrong relationships with physical environment.
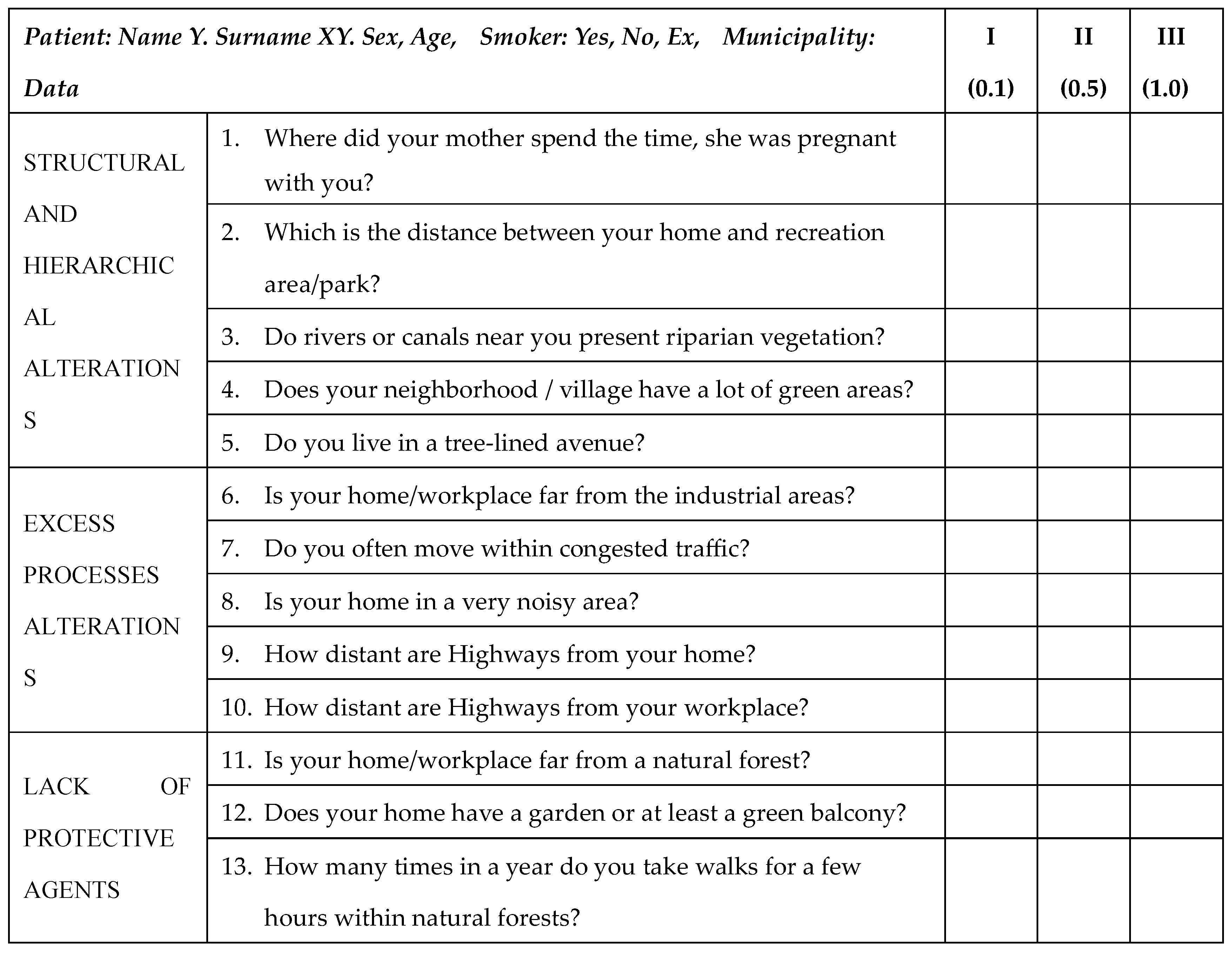
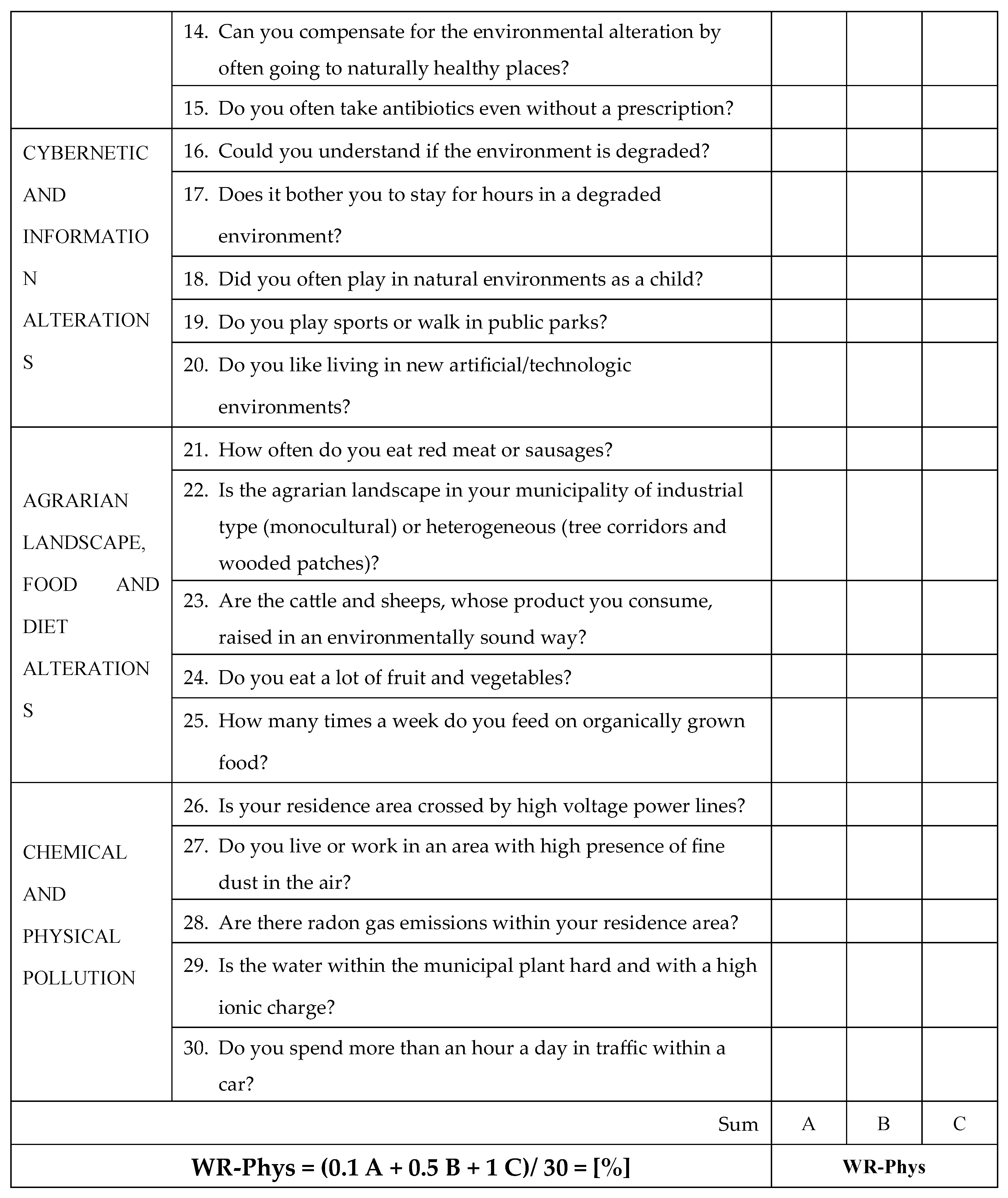
Figure 4.
Evaluation of psychosocial stress levels (WR-PSoc.).
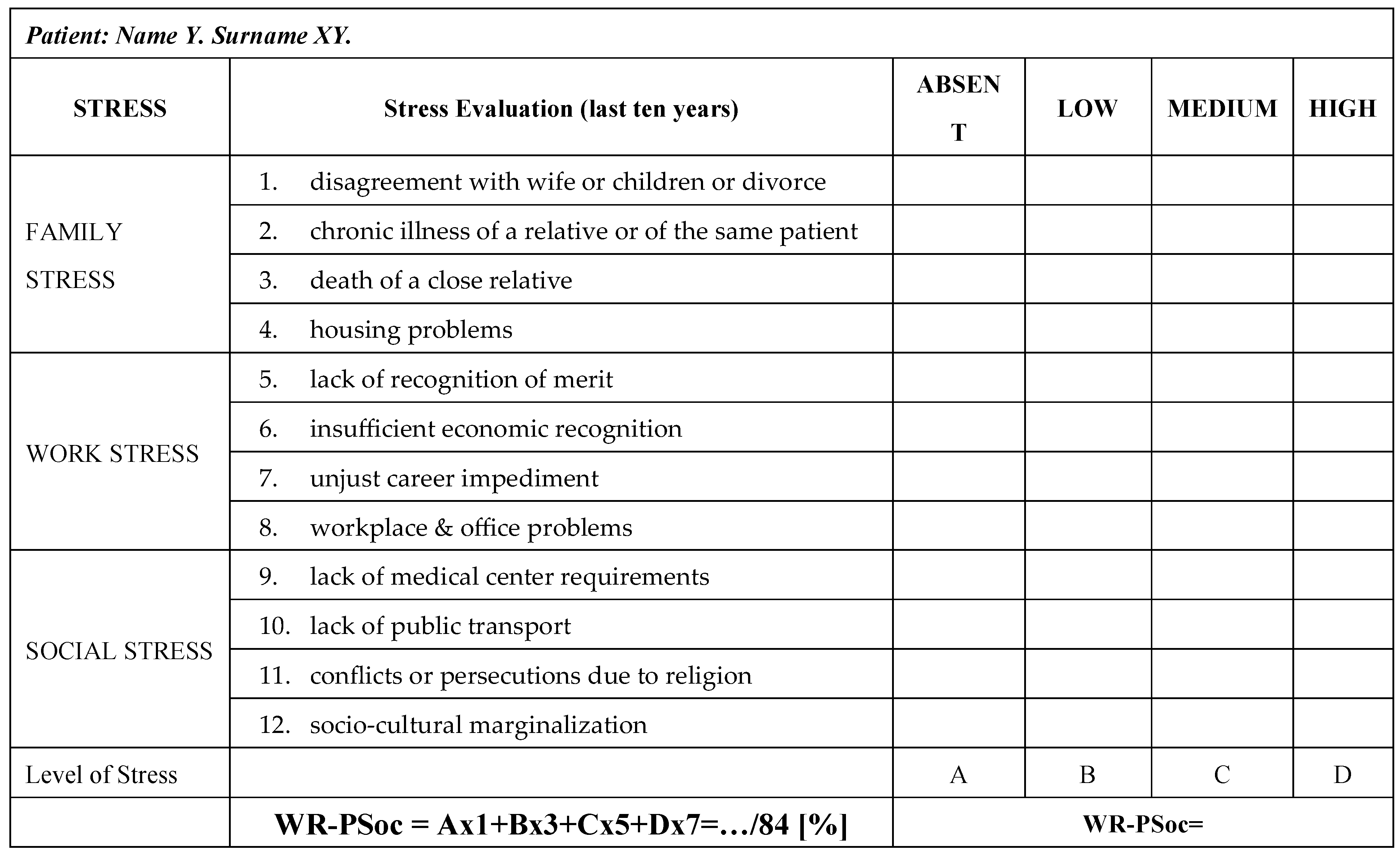
Figure 5.
The HH/BTC model, able to measure the bionomics state of a LU. Dotted lines express the BF level, that is the bionomics functionality of the surveyed LU.
Figure 5.
The HH/BTC model, able to measure the bionomics state of a LU. Dotted lines express the BF level, that is the bionomics functionality of the surveyed LU.
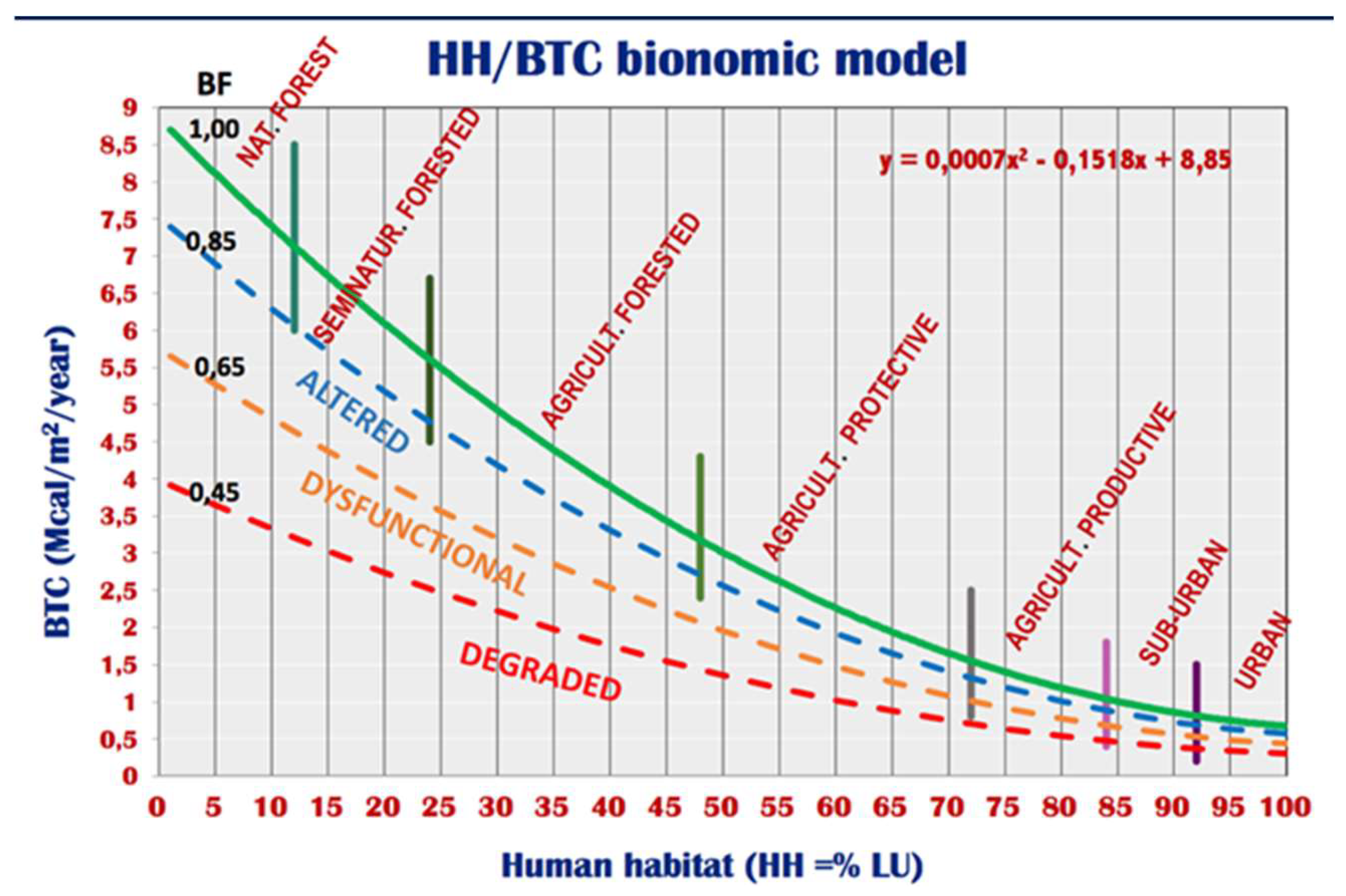
Figure 6.
An increase in the mortality rate MR [x 1000] is inversely correlated to the increase in landscape functionality: it goes from MR = 8.45 in unaltered landscapes (BF = 1.0) to MR = 9.45 in the dysfunctional landscape of 40% (BF = 0.60) of the normal state. Note that about 30% of the examined municipalities (but 2/3 of 2.54 million inhabitants) present a BF<0.60.
Figure 6.
An increase in the mortality rate MR [x 1000] is inversely correlated to the increase in landscape functionality: it goes from MR = 8.45 in unaltered landscapes (BF = 1.0) to MR = 9.45 in the dysfunctional landscape of 40% (BF = 0.60) of the normal state. Note that about 30% of the examined municipalities (but 2/3 of 2.54 million inhabitants) present a BF<0.60.
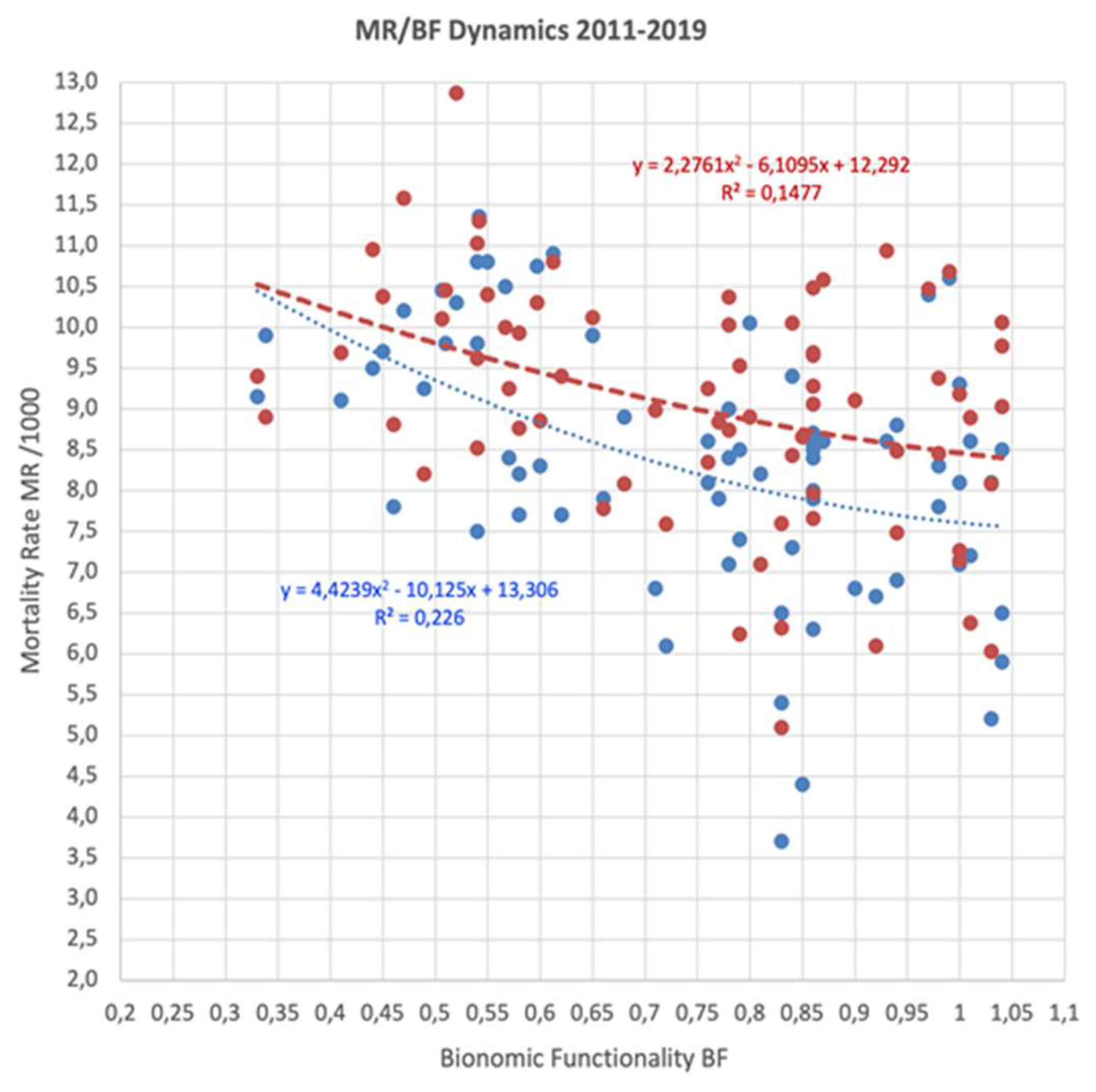
Figure 7.
The distribution of patients examined in the five ECS value classes shows a decisive shift towards the high classes. Therefore, high environmental stress is immediately found in cancer patients.
Figure 7.
The distribution of patients examined in the five ECS value classes shows a decisive shift towards the high classes. Therefore, high environmental stress is immediately found in cancer patients.
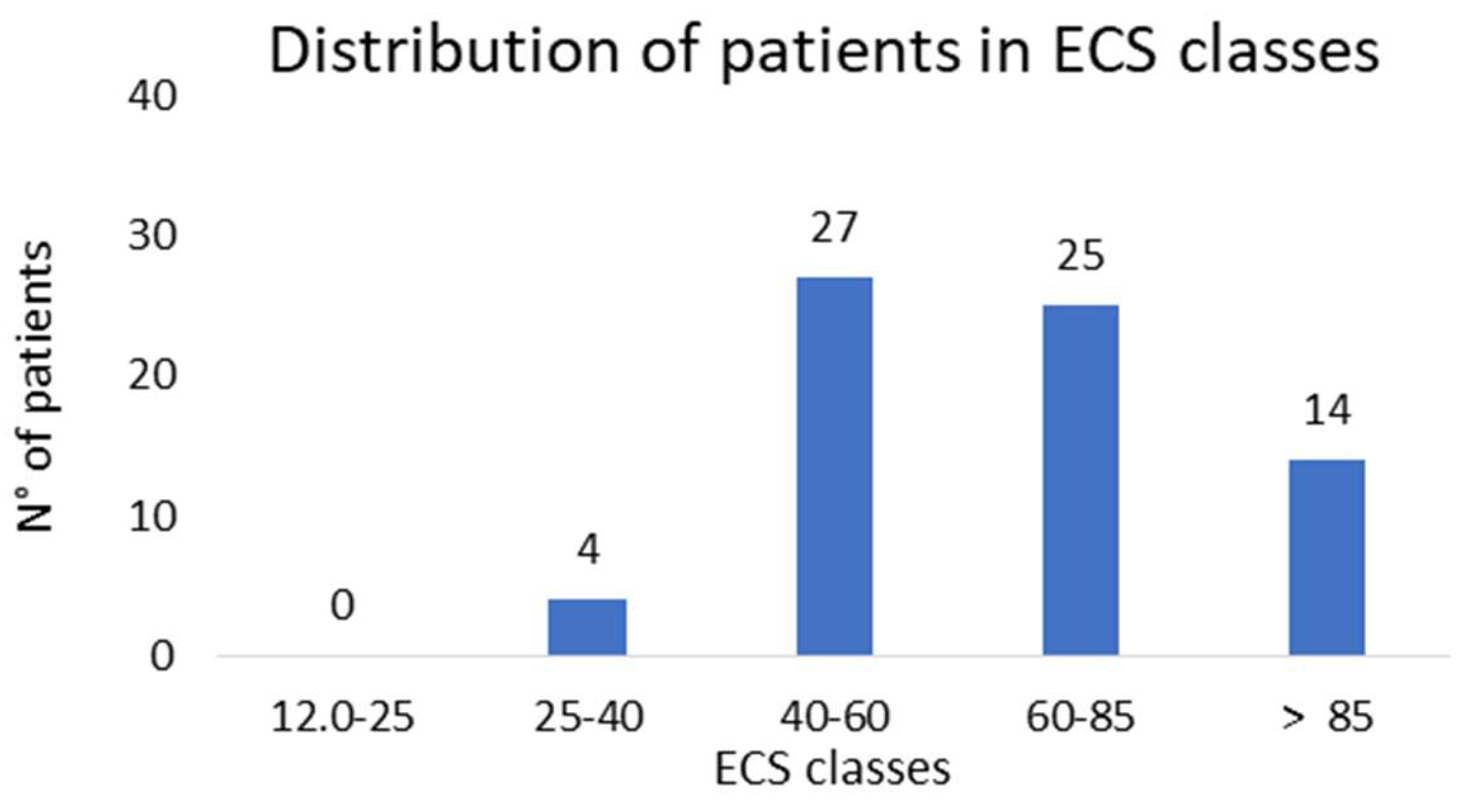
Figure 8.
Distribution of the 70-case study ECS. Note the ECS mean = 68.6 and the threshold of normality not over ECS = 25.0; note the logarithmic curve. No one case resulted within the condition of normality. Note that the BF/ECS correlation significance (Pearson) is decidedly high, equal to -3.0.
Figure 8.
Distribution of the 70-case study ECS. Note the ECS mean = 68.6 and the threshold of normality not over ECS = 25.0; note the logarithmic curve. No one case resulted within the condition of normality. Note that the BF/ECS correlation significance (Pearson) is decidedly high, equal to -3.0.
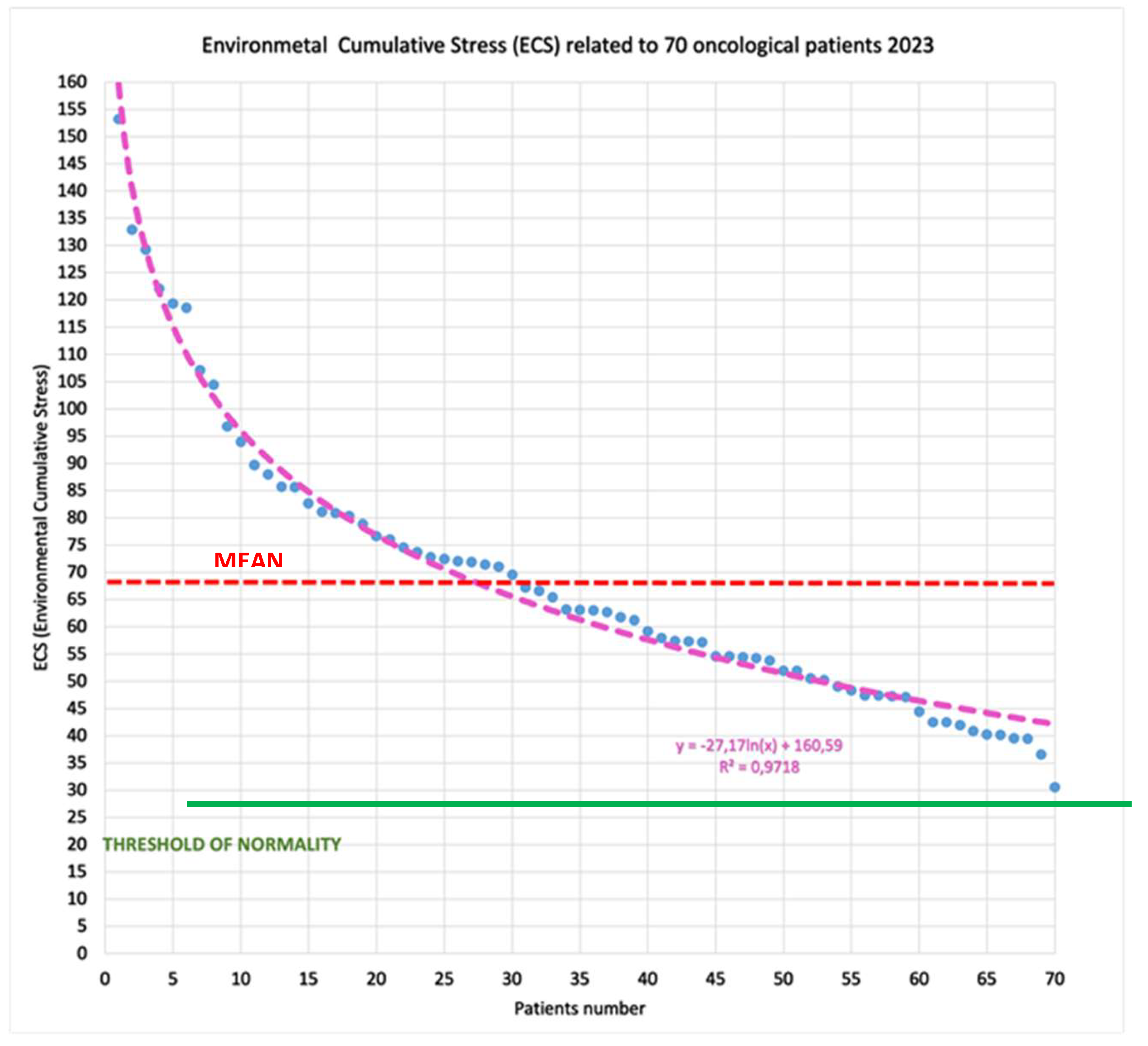
Figure 9.
The subdivision of lung tumors according to histotype.
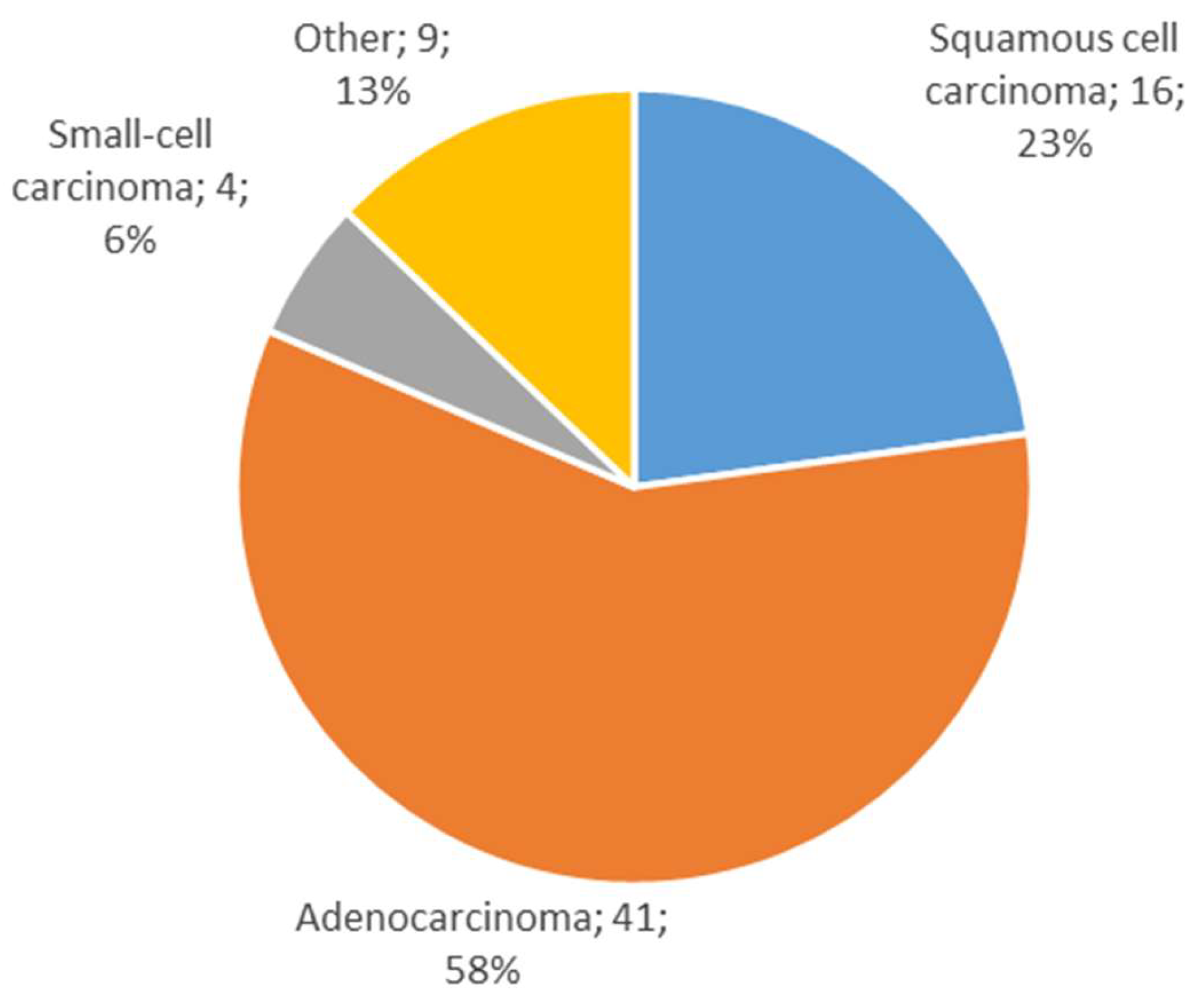
Figure 10.
Histotype distribution among non-smokers A, smokers B, ex-smokers C.
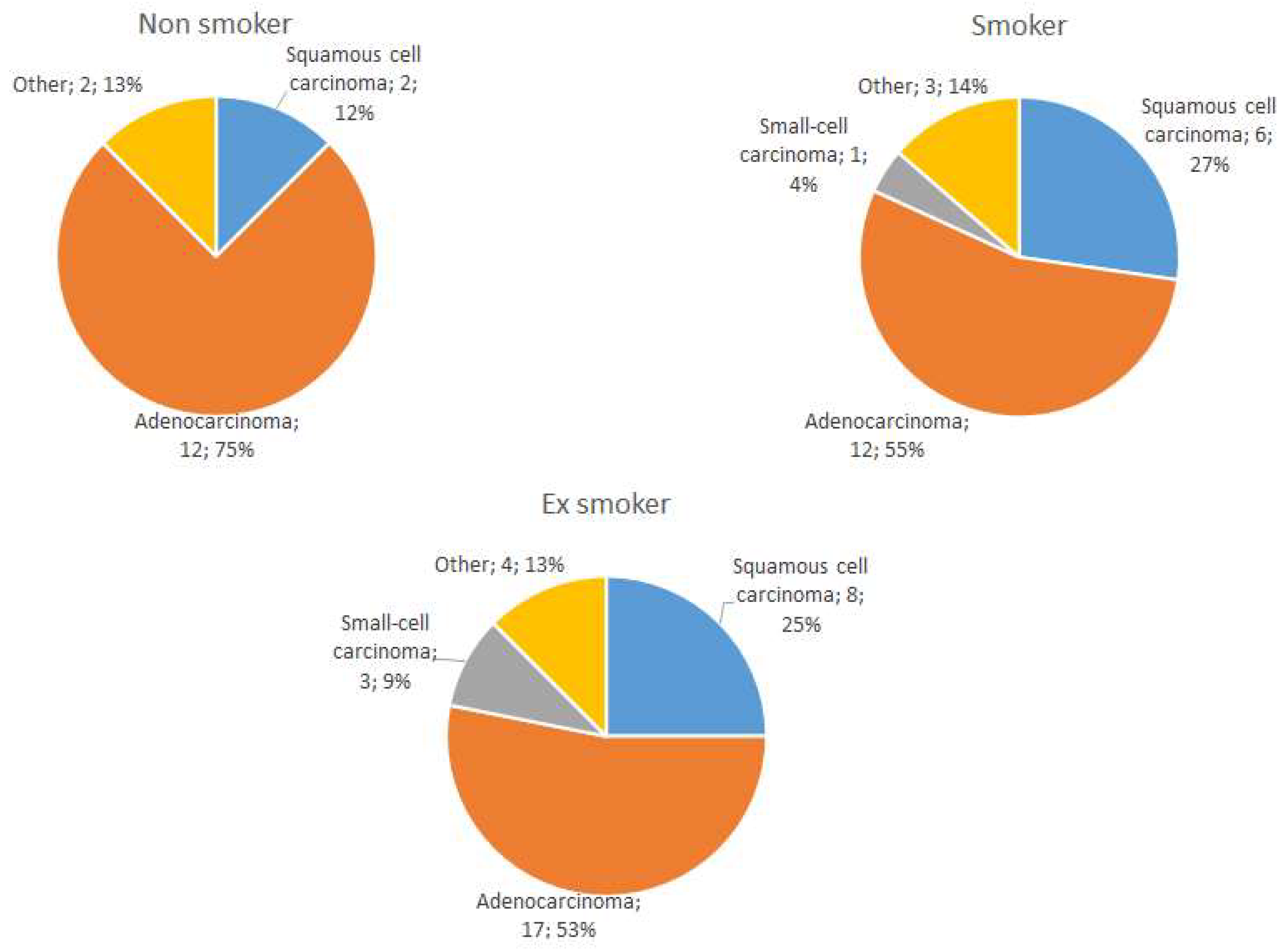

Table 1.
Summarizing the normality levels and the value ranges of the indicators considered, we will notice that they are all increasingly proportional, except BF, which behaves inversely, as indicated in equation 4 to find the Environmental Cumulative Stress (ECS) (second-degree of cumulation).
Table 1.
Summarizing the normality levels and the value ranges of the indicators considered, we will notice that they are all increasingly proportional, except BF, which behaves inversely, as indicated in equation 4 to find the Environmental Cumulative Stress (ECS) (second-degree of cumulation).
| Values | WR-Phys | WR-PSoc | cWR | BF* | ECS |
|---|---|---|---|---|---|
| Normal | 10-20 | 14-21 | 12-25 | 0.9-1.1 | 12-25 |
| Low | 20-35 | 20-30 | 25-40 | 0.7-0.9 | 25-40 |
| Medium | 35-50 | 30-40 | 40-55 | 0.5-0.7 | 40-60 |
| High | 50-65 | 40-50 | 55-70 | 0.3-0.5 | 60-85 |
| Very high | > 65 | > 50 | > 70 | 0.1-0.3 | > 85 |
| *The meaning of BF is the opposite: normal, slightly altered, altered, reduced, seriously insufficient. For both cWR and ECS, it is better to start from 25.00 with a small rounding. | |||||
Table 2.
Results of the elaboration of 70 questionnaires.
| Parameters | WR-Phys. | WR-PSoc. | cWR | BTCsurv | BF | ECS |
|---|---|---|---|---|---|---|
| Maximum Val. | 61.0 | 66.7 | 82.8 | 2.06 | 1.11 | 153.3 |
| Minimum Val. | 22.3 | 14.3 | 26.6 | 0.40 | 0.51 | 30.6 |
| Average values | 40.3 | 28.6 | 52.0 | 0.93 | 0.79 | 68.6 |
| Standard deviation | 8.14 | 12.37 | 12.35 | 0.34 | 0.15 | 25.36 |
Table 3.
Comparison among smoking patients, their oncological histotypes and their ECS factors.
| Smoking | Adenocarcinoma | Squamous carcinoma | WR Phys % | WR PSoc % | cWR | BF % | ECS |
|---|---|---|---|---|---|---|---|
| Yes | 55 | 27 | 42,49 | 36,05 | 57,79 | 82,00 | 78,75 |
| Ex | 53 | 25 | 39,49 | 24,63 | 49,21 | 81,00 | 64,16 |
| No | 75 | 12 | 39,16 | 26,75 | 49,64 | 78,00 | 61,62 |
| Normal | 60,00 | 25,00 | 20,00 | 20,20 | 24,00 | 100,00 | 24,00 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



