
Submitted:
16 December 2024
Posted:
17 December 2024
You are already at the latest version
Abstract
Background/Objectives: Whole-body cryotherapy (WBC) is widely recognized for its analgesic and anti-inflammatory effects. Despite growing interest in its therapeutic potential, the impact of WBC on functional performance, pain perception, sleep quality and quality of life among indi-viduals with multiple sclerosis (MS) remains underexplored. This study aimed to assess the ef-fects of a 10-session WBC protocol on functional and psychological parameters in patients with MS and compare them with individuals without neurological disorders. Methods: A total of 73 participants, divided into two groups: non-neurological individuals (non-MS, n=43) and patients with MS (MS, n=30), underwent 10 WBC sessions (-120 °C to -130 °C) over two weeks. Assess-ments included the Numerical Rating Scale (NRS), 30-Second Chair Stand Test (30CTS), Timed-Up-and-Go Test (TUG), and Pittsburgh Sleep Quality Index, WHOQOL-Bref conducted pre-treatment, post-treatment, and at 10-day follow-up. Results: In the MS group, significant im-provements were observed post-treatment in NRS, 30CTS, WHOQOL-1, and PSQI. However, only CTS and WHOQOL-3 maintained improvements during follow-up. In the non-MS group, statis-tically significant improvements were observed post-treatment across most parameters, except for NRS and WHOQOL-3, with most effects diminishing by follow-up. No deterioration in any assessed parameters was observed in either group. Conclusions: WBC demonstrates potential benefits for managing MS symptoms, particularly pain and sleep quality, with no observed dete-rioration in parameters and some effects emerging only during follow-up, underscoring its safety and the need for further research on long-term outcomes.
Keywords:
whole-body cryotherapy
; cryostimulation
; multiple sclerosis
; pain
; functional status
; sleep quality
1. Introduction
Multiple sclerosis (MS) is a chronic neuroinflammatory disease of the central nervous system, marked by demyelination, neuronal damage, and a range of disabling physical and cognitive impairments, which collectively impose a substantial socioeconomic and individual burden globally. MS manifests with a broad spectrum of symptoms, including fatigue, cognitive impairment, gait and mobility challenges, spasticity, bladder and bowel dysfunction, visual disturbances, sensory deficits, pain, and emotional disturbances such as depression and anxiety,[1] highlighting the complexity of its management and the need for individualized therapeutic approaches. Among the numerous symptoms of MS, pain has gained increasing recognition as a significant and multifaceted aspect of the disease, contrary to the earlier belief that MS is a painless condition.[2] Pain in MS, according to pathophysiological mechanisms, is classified into three categories: nociceptive pain (including pain from optic neuritis, musculoskeletal pain due to postural issues, low back pain, migraines, tension-type headaches, and treatment-related pain); neuropathic pain (NP), presenting as persistent limb pain, Lhermitte’s sign, or trigeminal neuralgia; and mixed pain, such as painful tonic spasms and spasticity-related pain. [2,3].
Another significant issue among individuals with MS is poor sleep quality, affecting over 50% of patients [4,5]. Sleep disturbances in this population can stem directly from the disease’s effects on the central nervous system, including demyelination and neuroinflammatory processes, or indirectly from related symptoms such as pain, spasticity, fatigue, and depression. These disturbances often lead to worsened quality of life (QoL) and increased disease burden [5].
MS significantly affects both physical and psychological well-being, contributing to reduced functionality and social participation. According to research, individuals with MS report consistently lower QoL compared to the general population, with factors such as fatigue, depression, and mobility impairments playing a prominent role in this decline [6]. The multifaceted impact of MS symptoms, including their cyclical interplay—where worsening of one symptom, such as pain or fatigue, exacerbates others—underscores the importance of a holistic approach to treatment.
Symptomatic treatment remains a cornerstone of MS care, aiming to alleviate the disease burden and improve patients’ QoL. Over the past few decades, advancements in MS therapies have transformed the treatment landscape. The pharmacological approach is effective in reducing relapse frequency and delaying disability progression but may not fully address all aspects of disease activity and its effectiveness is significantly limited in more progressive forms of MS, highlighting the need for complementary approaches in MS management [7]. Moreover, the side effects and limitations of long-term pharmacological treatments, such as increased risk of infections and systemic adverse effects, underscore the necessity of exploring complementary and non-pharmacological therapies [8].
Non-pharmacological approaches have gained increasing attention as essential components of comprehensive MS management. Rehabilitation, in particular, is increasingly recognized as a cornerstone of care, offering significant benefits for maintaining and improving functional status, fatigue, as well as enhancing quality of life in individuals with MS [9,10,11,12]. However, the growing complexity of MS symptoms highlights the need to explore and implement innovative solutions that address unmet therapeutic needs and complement existing treatments [13,14]. These strategies, which most frequently include physiotherapy, exercise programs, cognitive-behavioral therapy, and lifestyle interventions, aim to address symptoms that remain unresponsive to pharmacological treatments [15].
In Poland, WBC has been widely adopted as a therapeutic intervention, with the national health fund reimbursing approximately 650,000 WBC sessions annually over the past decade [16]. Of these, an estimated 14,000 sessions were administered to individuals with MS, while the majority were utilized by patients with osteoarthritis (OA) and other musculoskeletal conditions.
In recent years, there has been a growing interest in the application of WBC among patients with MS, primarily due to its potential anti-inflammatory and antioxidative effects [17]. Studies suggest that WBC may reduce pro-inflammatory cytokines, such as TNF-α and IL-1β, while increasing levels of anti-inflammatory cytokines like IL-10 [18]. These mechanisms are particularly significant in the context of MS, an autoimmune disease characterized by chronic inflammation, which plays a significant role in disease progression. This therapeutic approach holds promise as a complementary strategy to address inflammation-driven symptoms in MS management. Although WBC has demonstrated benefits in conditions such as rheumatoid arthritis, fibromyalgia, ankylosing spondylitis, depression, anxiety, sleep disorders, post-exercise muscle soreness, post-COVID syndrome, and obesity [19], research on its effects in neurological conditions like MS exists but remains limited.
This study aimed to evaluate the impact of WBC on functional performance, pain perception, and sleep quality in patients with MS, comparing the outcomes with those in a non-neurological population.
To the best of our knowledge, this is the first study to evaluate the effects of WBC on pain and sleep quality in patients with MS. Additionally, it incorporates a follow-up phase to explore the longevity of these effects, providing a comprehensive perspective on the intervention’s impact. By investigating these effects, the study seeks to broaden the understanding of WBC’s role in MS management and highlight its potential as a complementary therapeutic tool for improving the quality of life in diverse patient populations. In addition, correlation analyses were performed to examine the interplay between various outcomes, offering a more holistic perspective on the potential interconnected effects of WBC.
2. Materials and Methods
2.1. Participants
The study recruited participants from the Creator Rehabilitation Center in Łódź, divided into two groups: those without neurological disorders (non-MS n=43) and patients diagnosed with MS (MS n=30) (Figure 1).
Patients from the MS group had been previously diagnosed with MS by a neurologist and are under regular care at a neurology outpatient clinic. The non-MS group consisted of individuals recruited among patients referred for WBC due to OA, serving as a comparison group to highlight differences between those with and without neurological conditions. The demographic and baseline characteristics of the study participants (n = 73) are detailed in Table 1, with a comparison between non-MS group (n = 43) and MS group (n = 30) [Table 1].
The data encompass factors such as gender distribution, education level, employment status, comorbidities, lifestyle habits, and prior exposure to cryotherapy, providing a thorough overview of the study population.
Inclusion criteria required patients to have a referral for WBC from a medical doctor, no contraindications for the therapy, an age range of 18 to 85 years, no neurological disorders in WBC1 group and a confirmed diagnosis of MS in WBC2 group and written consent to participate. Exclusion criteria included health conditions that contraindicate participation in WBC sessions, EDSS<6, ongoing involvement in other physiotherapy treatments during the study period, and significant lifestyle or physical activity changes during or right before WBC treatment period. The protocol and procedures were followed according to the Helsinki Declaration and were approved by the Ethics Committee of the Medical University of Lodz, Poland, RNN/97/23/KE. The data were collected face to face.
2.2. Study Design
Participants underwent a series of 10 consecutive WBC sessions, excluding weekends. The cryotherapy process took place in a specialized chamber with two sections. The procedure involved an initial adaptation phase of 30 seconds in a atrium at -60°C, followed by 2 minutes in the main chamber. The temperature in the main chamber started at -120°C on the first day and decreased by 2°C every other day, reaching -130°C by the last session. After the main chamber exposure, participants returned to the atrium for an additional 30 seconds. Whole procedure lasted for 3 minutes. The chamber was cooled using liquid nitrogen. To ensure safety, participants wore protective gear: gloves, knee-high socks, wooden clogs, a headband or hat for ear coverage, and a surgical mask. Each session was immediately followed by a 30-minute supervised exercise routine, primarily on a cycle ergometer, to promote rewarming and enhance therapeutic benefits (Figure 2).
2.3. Assessment Protocol
Participants were evaluated at three points during the study: before the first cryotherapy session (T1), after completing the series of 10 sessions on the final treatment day (T2), and 10 days after the final session (T3). The clinical impact was assessed using the following scales and tests.
2.3.1. Numerical Rating Scale (NRS) for Pain Assessment
NRS is a widely utilized tool for subjective pain assessment, allowing patients to rate their pain intensity on a scale from 0 (no pain) to 10 (worst possible pain). Furthermore, its ease of administration—requiring patients to either verbalize or mark their pain level—ensures wide applicability [20]. Its simplicity makes it particularly suitable for clinical and research settings, including the evaluation of pain in patients with chronic and inflammatory conditions. As highlighted by Hawker et al., the NRS has demonstrated strong validity and reliability in diverse populations, where pain intensity plays a crucial role in determining functional status and treatment efficacy. Its sensitivity to change makes it an essential measure for assessing treatment outcomes and monitoring pain over time [21].
2.3.2. The World Health Organization Quality of Life-BREF (WHOQOL-BREF)
The WHOQOL-BREF is a widely utilized instrument designed to assess quality of life across multiple domains (physical, psychological, social, and environmental) [22]. As highlighted in recent studies, this tool is particularly suitable for patients with chronic conditions, including neurological disorders like MS. It provides insights into how diseases impact day-to-day functioning and overall life satisfaction. Its user-friendly structure, consisting of 26 items rated on a 5-point Likert scale, allows for efficient data collection in both clinical and research settings [23].
2.3.3. Pittsburgh Sleep Quality Index (PSQI)
PSQI is a validated instrument for assessing subjective sleep quality, with a global score >5 typically indicating poor sleep [24]. It assesses seven components, including subjective sleep quality, latency, duration, habitual efficiency, disturbances, use of sleeping medication, and daytime dysfunction. The global PSQI score, ranging from 0 to 21, differentiates between “good” and “poor” sleepers [25]. However, no standardized cut-off score has been firmly established for individuals with MS [26]. Recent studies, including those on populations with chronic conditions, underscore the PSQI’s reliability and validity for evaluating sleep quality [26].
2.3.4. 30-Second Chair Stand Test (30CTS)
30CST is a widely used functional assessment to evaluate lower limb strength, balance, and fall risk, particularly useful in individuals with chronic neurological conditions such as MS [27] Participants sit in an armless chair approximately, with their feet flat on the ground and arms crossed over their chest. After receiving the start command, they transition from a seated to a standing position and back as many times as possible within 30 seconds. The total number of successful repetitions is recorded [28]. The 30CST has a good sensitivity to detect changes in functional performance over time [29], making it an excellent tool for tracking the effects of interventions like cryotherapy.
2.3.5. Timed Up and Go (TUG)
The TUG test is a widely used and simple assessment tool for evaluating mobility, functional movement, and fall risk. In the TUG test, participants are required to rise from a seated position in a sturdy chair, walk three meters at a normal pace, turn around, return to the chair, and sit back down. Timing begins when the participant initiates movement and ends upon sitting [30] .This test provides insight into dynamic balance, gait speed, and the overall functional ability of individuals, making it a valuable measure for various populations, including those with neurological or musculoskeletal disorders [31].
2.4. Data Analysis
Statistical analyses were performed using Statistica version 13.1 software (StatSoft). The distribution of the variables was calculated using Shapiro-Wilk test. The statistical analysis was performed by Mann–Whitney U-test t for two independent variables or Kruskal-Wallis ANOVA for more than two independent variables. The effect size, measuring the differences between the results inside the groups and between groups, was determined by Cohen’s d; the value is defined as the difference between two means divided by a standard deviation for the data. Effect sizes were recorded as small (d=0.2), medium (d=0.5), and large (d=0.8). Spearman’s correlation coefficient was used to assess the relationship between the results of WHOQOL-bref test results and quality of sleep. For all analyses, significant differences were accepted at the level of p < 0.05.
3. Results
In this research, we aimed to evaluate the impact of WBC on MS patients in comparison to neurologically healthy population by focusing on the observed changes rather than the baseline results. However, it is important to note that the MS group exhibited poorer initial outcomes in 30CTS, PSQI, WHOQOL-bref domains 1, 2 and 3, while non-MS group in NRS, TUG and WHOQOL-bref domain 4. All of the results are listed in Table A1 and Table A2 in Appendix A (Appendix A).
3.1. Changes in Test Results Before WBC, After 10 Sessions and After 10 Days from Last Session
In general, the changes in the results were greater and more often significant after cryotherapy rather than in follow-up te The results obtained in follow-up were only slightly better than before 10 WBC sessions (Table 2).
3.1.1. Numerical Rating Scale (NRS):
In non-MS group, the changes in pain perception after cryotherapy were not statistically significant (Δ = -0.74, p = 0.081, d=0.30). At follow-up the results also showed no statistical significance, but the effect size was moderate (Δ = -0.44, p = 0.515, d=64). Conversely, in the MS group, the reduction in pain after cryotherapy was statistically significant (Δ = -0.93, p = 0.031, d = 0.38). However, this effect did not persist at follow-up (Δ = -0.12, p = 1.00, d=0.66).
3.1.2. 30-Second Chair Stand Test (30CTS):
Both groups experienced significant improvement in lower-limb strength and endurance post-treatment. In non-MS group, the changes were statistically significant (Δ = 1.02, p = 0.020, d = 0.23). At follow-up, there was no significant change (Δ = -0.22, p = 0.475, d=0.11). In MS patients, the improvement was greater and statistically significant with moderate effect size (Δ = 2.30, p = 0.001, d = 0.48), and a smaller, but still significant, improvement was maintained at follow-up (Δ = 2.00, p = 0.038, d = 0.22).
3.1.3. Timed Up and Go (TUG):
The non-MS group demonstrated significant improvement in functional mobility post-treatment (Δ = -0.62, p = 0.002, d = 0.39), but no statistically significant changes were observed at follow-up (Δ = -0.12, p = 0.155, d=0.36). For MS patients, neither the immediate (Δ = -0.30, p = 0.157, d=0.12) nor follow-up results (Δ = 0.07, p = 0.953, d=0.03) showed statistical significance.
3.1.4. WHOQOL Quality of Life Domains:
- Somatic domain: Both groups improved post-treatment. In non-MS, the improvement was statistically significant and medium-sized (Δ = 5.07, p = 0.004, d = 0.41), with no significant effect at follow-up (Δ = 1.19, p = 0.075, d=0.42). Similarly, MS group experienced significant improvements (Δ = 6.43, p = 0.001, d = 0.40), but these did not persist at follow-up (Δ = 0, p = 0.726, d=0.58).
- Psychological domain: Statistically significant improvements were observed in non-MS (Δ = 3.97, p = 0.010, d = 0.31). In MS, the changes were not significant post-treatment (Δ = 0, p = 0.793, d=0).
- Social domain: Improvements were not statistically significant for non-MS group (Δ = 2.52, p = 0.265, d=0.17) but were significant for MS, however only at the follow-up (Δ = 8.33, p = 0.028, d = 0.42).
- Environmental domain: Statistically significant changes were observed in non-MS post-treatment (Δ = 3.85, p = 0.025, d = 0.29), but these were not seen in MS patients at any stage.
3.1.5. Pittsburgh Sleep Quality Index (PSQI):
The improvements in sleep quality were statistically significant in both groups post-treatment. For non-MS group, the changes were modest (Δ = -0.83, p = 0.041, d = 0.28), with no significant follow-up improvement (Δ = -0.11, p = 0.674, d=0.28). For MS, sleep quality improved significantly after cryotherapy (Δ = -1.40, p = 0.011, d = 0.40), but no significant effects were maintained at follow-up (Δ = -1.37, p = 0.183, d=1.08).
The most significant changes were observed immediately following the therapy, with a notable decline in the persistence of these improvements after 10 days, particularly among MS patients. Figure 3 presents the percentages of changes after 10 WBC sessions and in follow-up after 10 days in non-MS group, and Figure 4 the same in MS group.
3.2. Correlations Between the Quality of Life and Quality of Sleep After Cryotherapy
Spearman’s correlation test, as highlighted in Table 3, identified a relationship between the results of WHOQOL-Bref questionnaire results and PSQI obtained directly after cryotherapy in non-MS patients (Table 3).
There was positive and small relationship between the results of WHOQOL 3 questionnaire results and PSQI but the result was not statistically significant (r=0.25; p>0.05). Correlation was also observed between the results of WHOQOL and PSQI obtained in follow-up in non-MS patients. Also here, the strong and positive relationship (r=0.68; p<0.05) was between WHOQOL 3 and PSQI. There was positive and small relationship between the results of WHOQOL 2 questionnaire results and PSQI but the result was not statistically significant (r=0.22; p>0.05). In MS patients there were not observed any significant correlations. However, there was negative and moderate relationship between WHOQOL 1 and WHOQOL 2 and PSQI in follow-up results.
3.3. Correlations Between the Number of Cryotherapy Sessions in the Past and Obtained Test Results
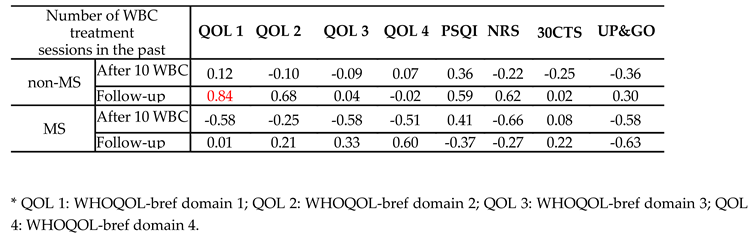
There was observed a relationship between the number of cryotherapy sessions in the past and the obtained results in the tests after cryotherapy, but mainly in MS group and the results were not statistically significant. However, there was observed a relationship between the number of cryotherapy sessions in the past and the obtained results in the tests in follow-up in both, non-MS and MS patients, as presented in Table 4.
In MS group, it what was observed that there was a negative and moderate relationship between the results after cryotherapy of WHOQOL-Bref 1, 2 and 3 and the number of sessions in the past. Also, a negative and moderate correlation was observed between NRS and TUG test in MS group. No correlation or very small was observed only in WHOQOL 2 and 30CTS results in MS group. However, while analysing the results obtained in follow-up it can be observed, that the correlations changed into positive and moderate in WHOQOL 3 and 4 and in 30CTS in MS group. It means that in the longer period of time, more frequent cryotherapy sessions can positively influence some aspects of the QOL and physical health.
In non-MS group, the only positive and small correlation can be observed between PSQI and the number of sessions in the past, but the result is not statistically significant. However, if analysing the results obtained in follow-up it can be also observed, that the correlations changed and more relationships exist. The strong and positive relationship can be observed in WHOQOL 1 results and the number of sessions in the past with p<0.05. Also, moderate and positive relationship was observed between WHOQOL 2, PSQI and NRS and the number of sessions in the past with p>0.05.
4. Discussion
We investigated the effects WBC on pain, functional status, sleep quality and quality of life in patients with MS compared to those without any neurological conditions non-MS), including a follow-up to assess the durability of these effects. While the benefits of WBC are well-documented in localized musculoskeletal conditions like OA, its impact on systemic and neurologically-driven symptoms in MS remains less understood.
WBC has repeatedly demonstrated analgesic effects, not only among healthy athletes but also in various medical conditions [32,33,34], including OA. In a study by Chruściak et al. among OA patients pain perception and its frequency and the number of taken analgesic medications were reduced [35]. However, to our knowledge, no studies have evaluated the impact of a series of cryotherapy sessions on pain in patients with MS. In this study, we aimed to examine the impact of cryostimulation on pain management and we found that while WBC may offer pain relief for patients with OA, its effects are more pronounced and statistically significant in individuals with MS. This reduction in pain may be attributed to the anti-inflammatory and neuromodulatory effects of cryotherapy, highlighting its potential as a valuable non-pharmacological intervention for managing chronic pain.
In patients with MS, sit-to-stand performance has been linked to lower-limb strength, spasticity, trunk control, and balance [29,36]. In our study, 30CST was used to assess the impact of WBC on functional performance in both MS patients and individuals without neurological conditions and the 30CST results highlighted notable differences between the non-MS and MS groups. In the non-MS group, the increase in repetitions post-intervention was statistically significant, indicating a positive effect of cryotherapy on lower-limb strength. However, the magnitude of improvement was smaller compared to the MS group, where the change was also statistically significant but more pronounced.
The improvement observed in the 30CST for individuals with MS after WBC can be attributed to several key mechanisms. In MS patients, WBC appears to reduce fatigue and pain through its anti-inflammatory and neuromodulatory effects [37]. These changes may facilitate better neuromuscular coordination and muscle activity, allowing significant improvement in muscle strength and endurance tasks, such as repeated sit-to-stand movements. In contrast, the non-MS group also showed statistically significant improvement in the 30CST, but the changes were less pronounced, possibly reflecting the more localized effects of WBC on nociceptive pain.
Interestingly, in the TUG test, statistically significant improvements were observed only in the non-MS group. This may reflect the nature of the task, which incorporates both sitting-to-standing and walking. For individuals with OA (non-MS group), pain relief and reduced stiffness in joints likely contributed to improved mobility. In contrast, MS patients showed improvements in TUG performance that were not statistically significant, potentially due to the persistent neurological impairments, such as reduced balance and motor control, which are less immediately responsive to cryostimulation.
Although there are no studies using these two tests to evaluate strength and functional state in MS patients undergoing WBC, existing research, such as study by Radecka et al., has shown improvements in functional outcomes through other measures. A series of 20 WBC sessions led to decreased fatigue, improved gait speed, and increased hand grip strength. These changes are attributed to adaptive modifications in bioelectrical muscle activity, as assessed through surface electromyography (sEMG)[38].
A positive impact of WBC on functional status has been demonstrated in two studies using a more comprehensive tool – the Rivermead Motor Assessment (RMA). In the study conducted by Miller et al., MS patients were divided into two groups based on their levels of fatigue: low-fatigue and high-fatigue. Both groups demonstrated statistically significant improvements after 10 sessions of WBC, particularly in RMA sections 1 (gross motor function) and 3 (arm movements)[39]. The improvements were especially pronounced in the high-fatigue group, highlighting the potential of cryotherapy to address fatigue-related limitations in functional abilities
Pawik et al. compared functional outcomes in MS patients divided into three groups: one undergoing WBC, another combining cryotherapy with structured physical exercise, and a third group participating only in a physical exercise program. While all groups showed improvements in functional status, the combined approach of cryotherapy and exercise yielded the most significant enhancements in RMA [40]. This finding underscores the additive benefits of integrating physical activity with cryotherapy to maximize functional recovery and mobility in patients with MS.
Another common challenge faced by patients with MS are sleep disturbances. It is worth noting that our initial findings pointed to poorer sleep quality in the MS group compared to the non-MS group, emphasizing the unique challenges faced by individuals with MS. While therapies such as melatonin supplementation, cognitive-behavioral therapy, chronotherapy, non-invasive brain stimulation, as well as complementary methods such as yoga, Tai Chi, and acupuncture have been explored for improving sleep in MS patients [41], WBC could offer a novel and complementary approach, addressing sleep disturbances linked to other symptoms. Until now, the impact of WBC on sleep disturbances in individuals with MS had not been examined; however, its effects have been explored in other populations, highlighting its potential in this area. For example, research by Douzi et al. has shown that WBC can improve sleep quality in healthy individuals. A study conducted with physically active men reported that evening, post workout, 3-min-WBC sessions improved the subjective sleep quality and the morning form state, objective sleep quality by reducing the number of movements during sleep, enhanced the pain relief, and parasympathetic nervous activity during the deep sleep (slow wave sleep) [42]. Given that sleep disturbances are prevalent among individuals with MS, these findings suggest that WBC may offer a promising non-pharmacological approach to ameliorate sleep-related issues in the MS population.
While no studies to date have specifically examined the effects of WBC on sleep quality in MS patients, the improvements observed in our findings align with the broader benefits of WBC reported in other contexts. The statistically significant improvement in the MS group may be attributed to the complex interplay between these factors, particularly given the greater symptom burden in this population.
The lack of comparable studies underscores the novelty of our findings and highlights the potential of WBC as an adjunct therapy for addressing sleep disturbances in MS patients. Further research is required to explore these effects more comprehensively and to identify mechanisms that could explain the observed differences between the MS and non-MS groups.
The final parameter assessed in our study was the QoL (WHOQOL-BREF), which revealed notable differences between the non-MS and MS groups. Right after ten sessions of WBC we observed a greater improvement in QoL (WHOQOL-BREF) among non-MS paparticipants, with statistically significant improvements in domains 1 (somatic), 2 (psychological), and 4 (environmental), while domain 3 (social) showed improvement without reaching statistical significance. At the same time (T2), among patients with MS, QoL improved significantly only in the somatic domain (domain 1), with the other domains remaining unchanged. Notably, the somatic domain in MS participants demonstrated a greater degree of improvement compared to non-MS participants. Interestingly, during the follow-up examination, the improvements observed in the non-MS group began to return toward baseline values. In contrast, among MS patients, there was a trend toward improvement in the remaining domains, with a notable and statistically significant enhancement (p = 0.028) in domain 3 (social). These findings may suggest that the time frame between the intervention and assessment might have been insufficient to capture broader changes, or that patients with MS may require more than functional improvements to observe changes in other aspects of life beyond the somatic domain. Moreover, while the effects of WBC on QOL may diminish over time in non-MS participants, the benefits for MS patients could emerge more gradually, particularly in domains beyond the somatic. This warrants further investigation into the mechanisms driving these differences and the potential long-term benefits of WBC in MS.
To the best of our knowledge, this is the first study to evaluate the effects of WBC on QoL in patients with MS using the WHOQOL-Bref questionnaire. Previous research, such as Szczepańska-Gieracha et al. [43], has demonstrated significant improvements in WHOQOL-bref after 10 sessions of WBC in patients with spinal pain syndromes and peripheral joint diseases. Vitenet et al. [44] documented improvements in QoL of fibromyalgia patients measured with the Medical Outcome Study Short Form-36 (MOS SF-36), particularly in health-related QoL, further reinforcing the potential of WBC to enhance the QoL in diverse clinical populations. These findings underscore the need for further research to explore the mechanisms underlying these effects and to establish standardized approaches to assess and optimize WBC protocols in different patient populations.
It is important to consider that most symptoms in MS are interconnected, where the worsening of one aspect can significantly impact others. For instance, pain and spasticity may exacerbate fatigue, while cognitive impairment and depression can further diminish overall quality of life. This relationship highlights the necessity for a holistic approach in managing MS symptoms [45].
A noteworthy and valuable trend emerged in our study, regarding the relationship between the number of previous cryotherapy sessions and outcomes, particularly during the follow-up period. While no significant correlations were observed immediately post-intervention, the follow-up analysis revealed a positive influence of past sessions on several parameters in both MS and non-MS groups. These observations suggest that the frequency of cryotherapy sessions could play a critical role in amplifying and sustaining therapeutic effects, particularly over extended periods.
Importantly none of the assessed parameters, in both groups, demonstrated any deterioration throughout the study period. This finding suggests that WBC is not only a potentially effective intervention but also a safe one, with no adverse impact on the physical, functional, or psychological state of participants. Such results underline the stability and tolerability of cryotherapy, making it a promising adjunctive therapy for improving various aspects of health without posing additional risks.
Regardless of the promising findings of this study, several limitations should be considered when interpreting the results. The study focused on a specific subgroup of patients with low to moderate levels of disability, predominantly women, which may limit the generalizability of the findings. As MS is a highly heterogeneous condition, encompassing a wide range of symptoms, further research is needed to explore the effects of WBC on other dimensions of the disease that were not captured in this study. Moreover, the assessment was conducted using a limited set of tools, and more comprehensive evaluations—particularly for complex aspects like sleep quality—would require the integration of additional, multidimensional tools to provide a fuller understanding. Despite these limitations, this study demonstrates that WBC is a well-tolerated therapy, with no adverse events or complaints reported among the participants.
6. Conclusions
The findings of this study suggest that WBC may offer meaningful benefits in managing symptoms associated with MS, particularly in areas such as pain relief and sleep quality. These results indicate that the benefits of WBC could be especially evident when applied in a cyclical manner, highlighting the potential value of repeat interventions. Notably, while some effects of WBC were observed immediately after therapy, others appeared over time, as demonstrated by the delayed improvements in certain WHOQOL-Bref domains among MS patients during follow-up. Importantly, no deterioration in the assessed parameters was observed in either group, which aligns with existing evidence supporting the safety of WBC as a non-invasive therapeutic approach. These observations underline the need for further exploration into the long-term effects of WBC and its role in symptom management for MS. Future research could benefit from longer follow-up periods and a broader range of assessments to better understand both the delayed and transient effects of WBC, as well as its potential to address the unique needs of different patient populations.
Author Contributions
Conceptualization, E.M. and E.Z-N.; methodology, E.M. and E.Z-N; software, E.Z-N and A.L.; validation, E.M., E.Z-N., Ł.K.; formal analysis, E.Z-N and A.L.; investigation, E.Z-N. and Ł.K.; resources, Ł.K.; data curation, A.L.; writing—original draft preparation, E.Z-N. and A.L.; writing—review and editing, E.M.; visualization, E.Z-N.; supervision, E.M.; project administration, E.M. and E.Z-N.; funding acquisition, E.M. All authors have read and agreed to the published version of the manuscript.
Funding
This study was supported by a grant from the Medical University of Lodz (Grant No. 503/6-127-05/503-51-001-19).
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki and approved by the Ethics Committee of the Medical University of Lodz, Poland, RNN/97/23/KE.
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Acknowledgments
We would like to express our deepest gratitude to all the patients who participated in this study for their cooperation and commitment, often adjusting their personal schedules to support the research process. Our sincere thanks go to the members of the Neurorehabilitation Student Scientific Association (Medical University of Łódź) for their invaluable assistance and dedication, with special recognition to Jan Górski and Piotr Karolczyk for their extraordinary involvement. Finally, we would like to thank the staff of the Creator Rehabilitation Center in Łódź for their unwavering support and assistance, which greatly contributed to the successful execution of this study.
Conflicts of Interest
The authors declare no conflicts of interest.
Appendix A

Table A1.
Outcomes at Baseline, Post-Intervention, and Follow-Up in non-MS group.
| Non-MS | BEFORE | AFTER | FOLLOW-UP | |||
|---|---|---|---|---|---|---|
| Mean±SD | Median (±95%CI) | Mean±SD | Median (±95%CI) | Mean±SD | Median (±95%CI) | |
| NRS | 4.23±2.71 | 4.00 (3.40; 5.06) |
3.49±2.33M | 3.00 (2.77; 4.21) |
2.89±1.67M | 3.00 (1.58; 3.69) |
| 30CTS | 16.00±4.61 | 16.00 (14.58; 17.42) |
17.02±4.56*S | 16.00 (15.62; 18.43) |
16.45±3.17S | 16.00 (14.32; 18.59) |
| UP&GO | 8.72±1.62 | 8,56 (8.22; 9.21) |
8.10±1.56**M | 7,83 (7.62; 8.58) |
8.15±1.56M | 7,75 (7.10; 9.20) |
| WHOQOL 1 |
63.87±13.55 | 64,29 (59.70; 68.04) |
69.94±11.44**M | 67,85 (65.41; 72.45) |
69.16±8.64M | 71,43 (63.35; 74.96) |
| WHOQOL 2 |
69.57±13.16 | 70,83 (65.52; 73.62) |
73.55±12.92**M | 70,83 (69.57; 77.52) |
74.62±11.7M | 79,17 (66.76; 82.48) |
| WHOQOL 3 | 71.90±16.27 | 75.00 (66.89; 76.90) |
74.42±14.01S | 75.00 (70.10; 78.73) |
71.97±9.33S | 75.00 (65.70; 78.24) |
| WHOQOL 4 | 64.32±14.05 | 65,63 (59.99; 68.64) |
68.17±12.37*M | 71,88 (64.36; 71.97) |
67.33±13.43S | 65,63 (58.31; 76.35) |
| PSQI | 6.07±3.41 | 5.00 (5.02; 7.12) |
5.23±2.5*M | 5.00 (4.46; 6.00) |
5.18±1.89S | 5.00 (3.91; 6.45) |
Table A2.
Outcomes at Baseline, Post-Intervention, and Follow-Up in MS group.
| MS | BEFORE | AFTER | FOLLOW-UP | |||
|---|---|---|---|---|---|---|
| Mean±SD | Median (±95%CI) | Mean±SD | Median (±95%CI) | Mean±SD | Median (±95%CI) | |
| NRS | 2.6±2.85 | 1.5 (1.54; 3.66) |
3.49±2.15*S | 0.5 (0.86; 2.47) |
0.89±1.83M | 0 (-0.52; 2.30) |
| 30CTS | 14.7±3.98 | 14.00 (13.21; 16.19) |
17.00±5.55***M | 15.5 (14.93; 19.07) |
15.56±3.71* | 16.00 (12.70; 18.41) |
| UP&GO | 8.42±2.58 | 7.96 (7.46; 9.39) |
8.17±2.51S | 7.82 (7.18; 9.06) |
8.33±3.27S | 8.20 (5.82; 10.84) |
| WHOQOL 1 | 55.83±16.95 | 55.36 (49.50; 62.16) |
62.26±15.77***M | 66.07 (56.37; 68.15) |
65.08±13.81M | 67.85 (54.47; 75.69) |
| WHOQOL 2 |
63.47±13.83 | 64.58 (58.30; 68.63) |
63.47±13.83 | 64.58 (58.31; 68.63) |
68.06±12.5S | 62.5 (58.45; 77.66) |
| WHOQOL 3 | 65.00±20.58 | 66.67 (57.32; 72.68) |
65.00±20.58 | 66.67 (57.32; 72.68) |
73.15±18.53*M | 75.00 (58.90; 87.39) |
| WHOQOL 4 | 67.19±14.33 | 65.63 (61.84; 72.54) |
67.19±14.33 | 65.63 (61.84; 72.54) |
70.14±14.41S | 68.75 (59.06; 81.21) |
| PSQI | 7.8±3.6 | 7.5 (6.45; 9.16) |
6.4±3.58**M | 6.00 (5.06; 7.73) |
4.22±2.49S | 5.00 (2.31; 6.13) |
References
- Jakimovski, D.; Bittner, S.; Zivadinov, R.; Morrow, S.A.; Benedict, R.H.; Zipp, F.; Weinstock-Guttman, B. Multiple sclerosis. Lancet 2024, 403, 183-202. [CrossRef]
- Nick, S.T.; Roberts, C.; Billiodeaux, S.; Davis, D.E.; Zamanifekri, B.; Sahraian, M.A.; Alekseeva, N.; Munjampalli, S.; Roberts, J.; Minagar, A. Multiple sclerosis and pain. Neurol Res 2012, 34, 829-841. [CrossRef]
- O’Connor, A.B.; Schwid, S.R.; Herrmann, D.N.; Markman, J.D.; Dworkin, R.H. Pain associated with multiple sclerosis: systematic review and proposed classification. Pain 2008, 137, 96-111. [CrossRef]
- Kotterba, S.; Neusser, T.; Norenberg, C.; Bussfeld, P.; Glaser, T.; Dörner, M.; Schürks, M. Sleep quality, daytime sleepiness, fatigue, and quality of life in patients with multiple sclerosis treated with interferon beta-1b: results from a prospective observational cohort study. BMC Neurol 2018, 18, 123. [CrossRef]
- Vitkova, M.; Gdovinova, Z.; Rosenberger, J.; Szilasiova, J.; Nagyová, I.; Mikula, P.; Krokavcova, M.; Groothoff, J.W.; van Dijk, J.P. Factors associated with poor sleep quality in patients with multiple sclerosis differ by disease duration. Disabil Health J 2014, 7, 466-471. [CrossRef]
- Gil-González, I.; Martín-Rodríguez, A.; Conrad, R.; Pérez-San-Gregorio, M. Quality of life in adults with multiple sclerosis: a systematic review. BMJ Open 2020, 10, e041249. [CrossRef]
- Haki, M.; Al-Biati, H.A.; Al-Tameemi, Z.S.; Ali, I.S.; Al-Hussaniy, H.A. Review of multiple sclerosis: Epidemiology, etiology, pathophysiology, and treatment. Medicine (Baltimore) 2024, 103, e37297. [CrossRef]
- Konen, F.F.; Möhn, N.; Witte, T.; Schefzyk, M.; Wiestler, M.; Lovric, S.; Hufendiek, K.; Schwenkenbecher, P.; Sühs, K.W.; Friese, M.A.; et al. Treatment of autoimmunity: The impact of disease-modifying therapies in multiple sclerosis and comorbid autoimmune disorders. Autoimmun Rev 2023, 22, 103312. [CrossRef]
- Amatya, B.; Khan, F.; Galea, M. Rehabilitation for people with multiple sclerosis: an overview of Cochrane Reviews. Cochrane Database Syst Rev 2019, 1, Cd012732. [CrossRef]
- Razazian, N.; Kazeminia, M.; Moayedi, H.; Daneshkhah, A.; Shohaimi, S.; Mohammadi, M.; Jalali, R.; Salari, N. The impact of physical exercise on the fatigue symptoms in patients with multiple sclerosis: a systematic review and meta-analysis. BMC Neurol 2020, 20, 93. [CrossRef]
- Redlicka, J.; Zielińska-Nowak, E.; Lipert, A.; Miller, E. Impact of Moderate Individually Tailored Physical Activity in Multiple Sclerosis Patients with Fatigue on Functional, Cognitive, Emotional State, and Postural Stability. Brain Sci 2021, 11. [CrossRef]
- Corrini, C.; Gervasoni, E.; Perini, G.; Cosentino, C.; Putzolu, M.; Montesano, A.; Pelosin, E.; Prosperini, L.; Cattaneo, D. Mobility and balance rehabilitation in multiple sclerosis: A systematic review and dose-response meta-analysis. Mult Scler Relat Disord 2023, 69, 104424. [CrossRef]
- Zielińska-Nowak, E.; Włodarczyk, L.; Kostka, J.; Miller, E. New Strategies for Rehabilitation and Pharmacological Treatment of Fatigue Syndrome in Multiple Sclerosis. J Clin Med 2020, 9. [CrossRef]
- Duan, H.; Jing, Y.; Li, Y.; Lian, Y.; Li, J.; Li, Z. Rehabilitation treatment of multiple sclerosis. Front Immunol 2023, 14, 1168821. [CrossRef]
- Hauser, S.L.; Cree, B.A.C. Treatment of Multiple Sclerosis: A Review. Am J Med 2020, 133, 1380-1390.e1382. [CrossRef]
- Legrand, F.D.; Dugué, B.; Costello, J.; Bleakley, C.; Miller, E.; Broatch, J.R.; Polidori, G.; Lubkowska, A.; Louis, J.; Lombardi, G. Evaluating safety risks of whole-body cryotherapy/cryostimulation (WBC): a scoping review from an international consortium. European journal of medical research 2023, 28, 387.
- Miller, E.; Mrowicka, M.; Malinowska, K.; Mrowicki, J.; Saluk-Juszczak, J.; Kędziora, J. Effects of whole-body cryotherapy on a total antioxidative status and activities of antioxidative enzymes in blood of depressive multiple sclerosis patients. World J Biol Psychiatry 2011, 12, 223-227. [CrossRef]
- Alito, A.; Fontana, J.M.; Franzini Tibaldeo, E.; Verme, F.; Piterà, P.; Miller, E.; Cremascoli, R.; Brioschi, A.; Capodaglio, P. Whole-Body Cryostimulation in Multiple Sclerosis: A Scoping Review. J Clin Med 2024, 13. [CrossRef]
- Capodaglio, P.; Cremascoli, R.; Piterà, P.; Fontana, J.M. WHOLE-BODY CRYOSTIMULATION: A REHABILITATION BOOSTER. J Rehabil Med Clin Commun 2022, 5, 2810. [CrossRef]
- Thong, I.S.K.; Jensen, M.P.; Miró, J.; Tan, G. The validity of pain intensity measures: what do the NRS, VAS, VRS, and FPS-R measure? Scand J Pain 2018, 18, 99-107. [CrossRef]
- Hawker, G.A.; Mian, S.; Kendzerska, T.; French, M. Measures of adult pain: Visual Analog Scale for Pain (VAS Pain), Numeric Rating Scale for Pain (NRS Pain), McGill Pain Questionnaire (MPQ), Short-Form McGill Pain Questionnaire (SF-MPQ), Chronic Pain Grade Scale (CPGS), Short Form-36 Bodily Pain Scale (SF-36 BPS), and Measure of Intermittent and Constant Osteoarthritis Pain (ICOAP). Arthritis Care Res (Hoboken) 2011, 63 Suppl 11, S240-252. [CrossRef]
- Skevington, S.M.; Lotfy, M.; O’Connell, K.A. The World Health Organization’s WHOQOL-BREF quality of life assessment: psychometric properties and results of the international field trial. A report from the WHOQOL group. Qual Life Res 2004, 13, 299-310. [CrossRef]
- Pomeroy, I.M.; Tennant, A.; Mills, R.J.; Young, C.A. The WHOQOL-BREF: a modern psychometric evaluation of its internal construct validity in people with multiple sclerosis. Qual Life Res 2020, 29, 1961-1972. [CrossRef]
- Curcio, G.; Tempesta, D.; Scarlata, S.; Marzano, C.; Moroni, F.; Rossini, P.M.; Ferrara, M.; De Gennaro, L. Validity of the Italian version of the Pittsburgh Sleep Quality Index (PSQI). Neurol Sci 2013, 34, 511-519. [CrossRef]
- Fabbri, M.; Beracci, A.; Martoni, M.; Meneo, D.; Tonetti, L.; Natale, V. Measuring Subjective Sleep Quality: A Review. Int J Environ Res Public Health 2021, 18. [CrossRef]
- Jerković, A.; Mikac, U.; Matijaca, M.; Košta, V.; Ćurković Katić, A.; Dolić, K.; Vujović, I.; Šoda, J.; Đogaš, Z.; Pavelin, S.; et al. Psychometric Properties of the Pittsburgh Sleep Quality Index (PSQI) in Patients with Multiple Sclerosis: Factor Structure, Reliability, Correlates, and Discrimination. J Clin Med 2022, 11. [CrossRef]
- Tulipani, L.J.; Meyer, B.; Allen, D.; Solomon, A.J.; McGinnis, R.S. Evaluation of unsupervised 30-second chair stand test performance assessed by wearable sensors to predict fall status in multiple sclerosis. Gait Posture 2022, 94, 19-25. [CrossRef]
- Özkeskin, M.; Özden, F.; Ar, E.; Yüceyar, N. The reliability and validity of the 30-second chair stand test and modified four square step test in persons with multiple sclerosis. Physiother Theory Pract 2023, 39, 2189-2195. [CrossRef]
- Polidori, A.; Malagoli, M.; Giacalone, R.; Brichetto, G.; Monti Bragadin, M.; Prada, V. 30-Second Chair Stand and 5-Times Sit-to-Stand Tests Are Interesting Tools for Assessing Disability and Ability to Ambulate among Patients with Multiple Sclerosis. Life (Basel) 2024, 14. [CrossRef]
- Kear, B.M.; Guck, T.P.; McGaha, A.L. Timed Up and Go (TUG) Test: Normative Reference Values for Ages 20 to 59 Years and Relationships With Physical and Mental Health Risk Factors. J Prim Care Community Health 2017, 8, 9-13. [CrossRef]
- Valet, M.; Lejeune, T.; Devis, M.; van Pesch, V.; El Sankari, S.; Stoquart, G. Timed Up-and-Go and 2-Minute Walk Test in patients with multiple sclerosis with mild disability: reliability, responsiveness and link with perceived fatigue. Eur J Phys Rehabil Med 2019, 55, 450-455. [CrossRef]
- Barłowska-Trybulec, M.; Zawojska, K.; Szklarczyk, J.; Góralska, M. Effect of whole body cryotherapy on low back pain and release of endorphins and stress hormones in patients with lumbar spine osteoarthritis. Reumatologia 2022, 60, 247-251. [CrossRef]
- Klemm, P.; Hoffmann, J.; Asendorf, T.; Aykara, I.; Frommer, K.; Dischereit, G.; Müller-Ladner, U.; Neumann, E.; Lange, U. Whole-body cryotherapy for the treatment of rheumatoid arthritis: a monocentric, single-blinded, randomised controlled trial. Clin Exp Rheumatol 2022, 40, 2133-2140. [CrossRef]
- Bettoni, L.; Bonomi, F.G.; Zani, V.; Manisco, L.; Indelicato, A.; Lanteri, P.; Banfi, G.; Lombardi, G. Effects of 15 consecutive cryotherapy sessions on the clinical output of fibromyalgic patients. Clin Rheumatol 2013, 32, 1337-1345. [CrossRef]
- Chruściak, T. Subjective evaluation of the effectiveness of whole-body cryotherapy in patients with osteoarthritis. Reumatologia 2016, 54, 291-295. [CrossRef]
- Bowser, B.; O’Rourke, S.; Brown, C.N.; White, L.; Simpson, K.J. Sit-to-stand biomechanics of individuals with multiple sclerosis. Clin Biomech (Bristol) 2015, 30, 788-794. [CrossRef]
- Miller, E.; Kostka, J.; Włodarczyk, T.; Dugué, B. Whole-body cryostimulation (cryotherapy) provides benefits for fatigue and functional status in multiple sclerosis patients. A case–control study. Acta Neurologica Scandinavica 2016, 134, 420-426.
- Radecka, A.; Knyszyńska, A.; Łuczak, J.; Lubkowska, A. Adaptive changes in muscle activity after cryotherapy treatment: Potential mechanism for improvement the functional state in patients with multiple sclerosis. NeuroRehabilitation 2021, 48, 119-131. [CrossRef]
- Miller, E.; Kostka, J.; Włodarczyk, T.; Dugué, B. Whole-body cryostimulation (cryotherapy) provides benefits for fatigue and functional status in multiple sclerosis patients. A case-control study. Acta Neurol Scand 2016, 134, 420-426. [CrossRef]
- Pawik, M.; Kowalska, J.; Rymaszewska, J. The effectiveness of whole-body cryotherapy and physical exercises on the psychological well-being of patients with multiple sclerosis: A comparative analysis. Adv Clin Exp Med 2019, 28, 1477-1483. [CrossRef]
- Mogavero, M.P.; Lanza, G.; Bruni, O.; DelRosso, L.M.; Ferri, R.; Ferini-Strambi, L. Sleep counts! Role and impact of sleep in the multimodal management of multiple sclerosis. J Neurol 2023, 270, 3377-3390. [CrossRef]
- Douzi, W.; Dupuy, O.; Tanneau, M.; Boucard, G.; Bouzigon, R.; Dugué, B. 3-min whole body cryotherapy/cryostimulation after training in the evening improves sleep quality in physically active men. Eur J Sport Sci 2019, 19, 860-867. [CrossRef]
- Szczepańska-Gieracha, J.; Borsuk, P.; Pawik, M.; Rymaszewska, J. Mental state and quality of life after 10 session whole-body cryotherapy. Psychol Health Med 2014, 19, 40-46. [CrossRef]
- Vitenet, M.; Tubez, F.; Marreiro, A.; Polidori, G.; Taiar, R.; Legrand, F.; Boyer, F.C. Effect of whole body cryotherapy interventions on health-related quality of life in fibromyalgia patients: A randomized controlled trial. Complement Ther Med 2018, 36, 6-8. [CrossRef]
- Rzepka, M.; Chmiela, T.; Kaczmarczyk, A.; Krzystanek, E. Insomnia, Fatigue, Bladder Disorders and Mood Disorders among Polish Patients with Multiple Sclerosis: Cross-Sectional Study. J Clin Med 2024, 13. [CrossRef]
Figure 1.
Participants flowchart.
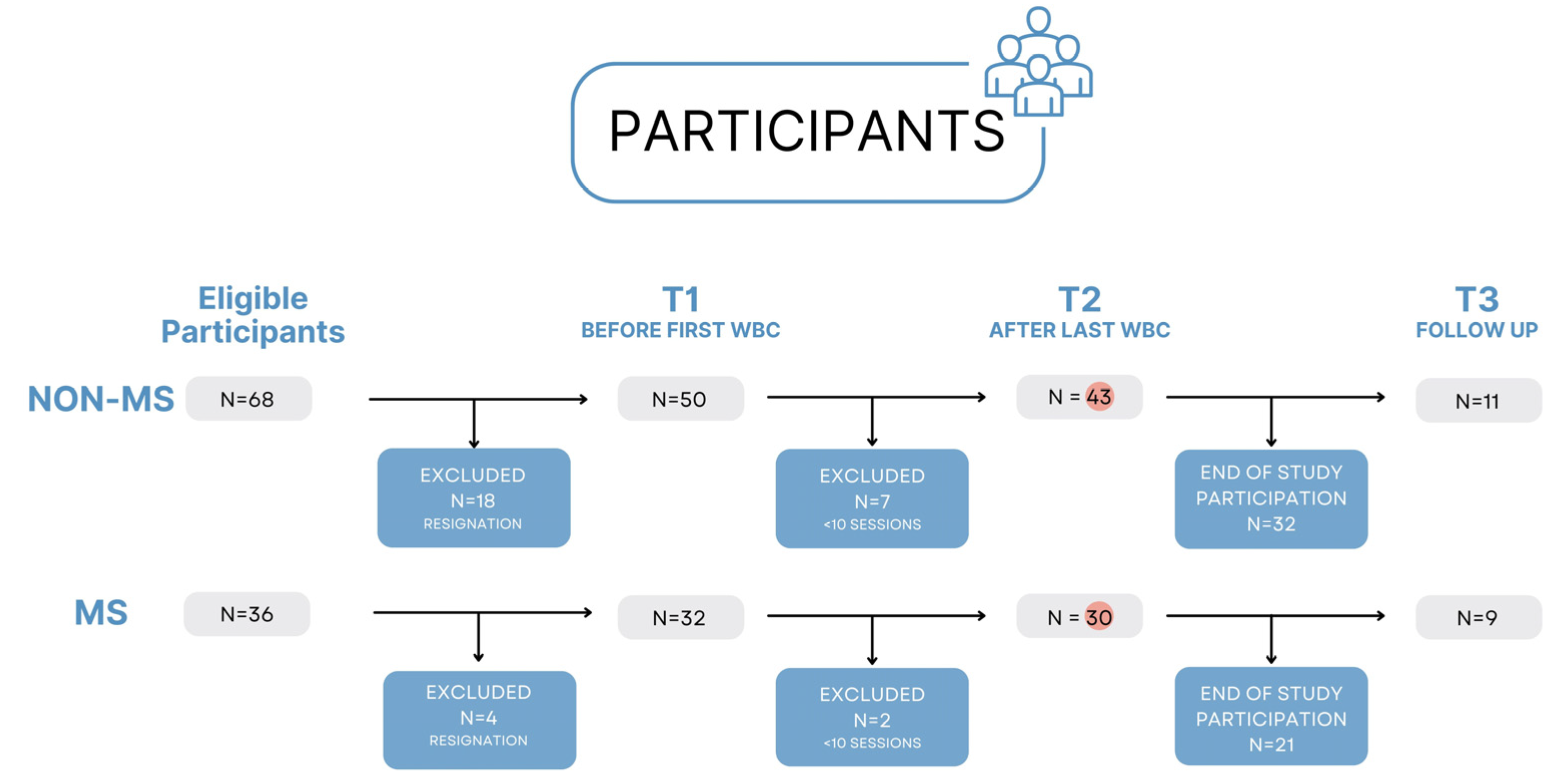
Figure 2.
Study protocol.
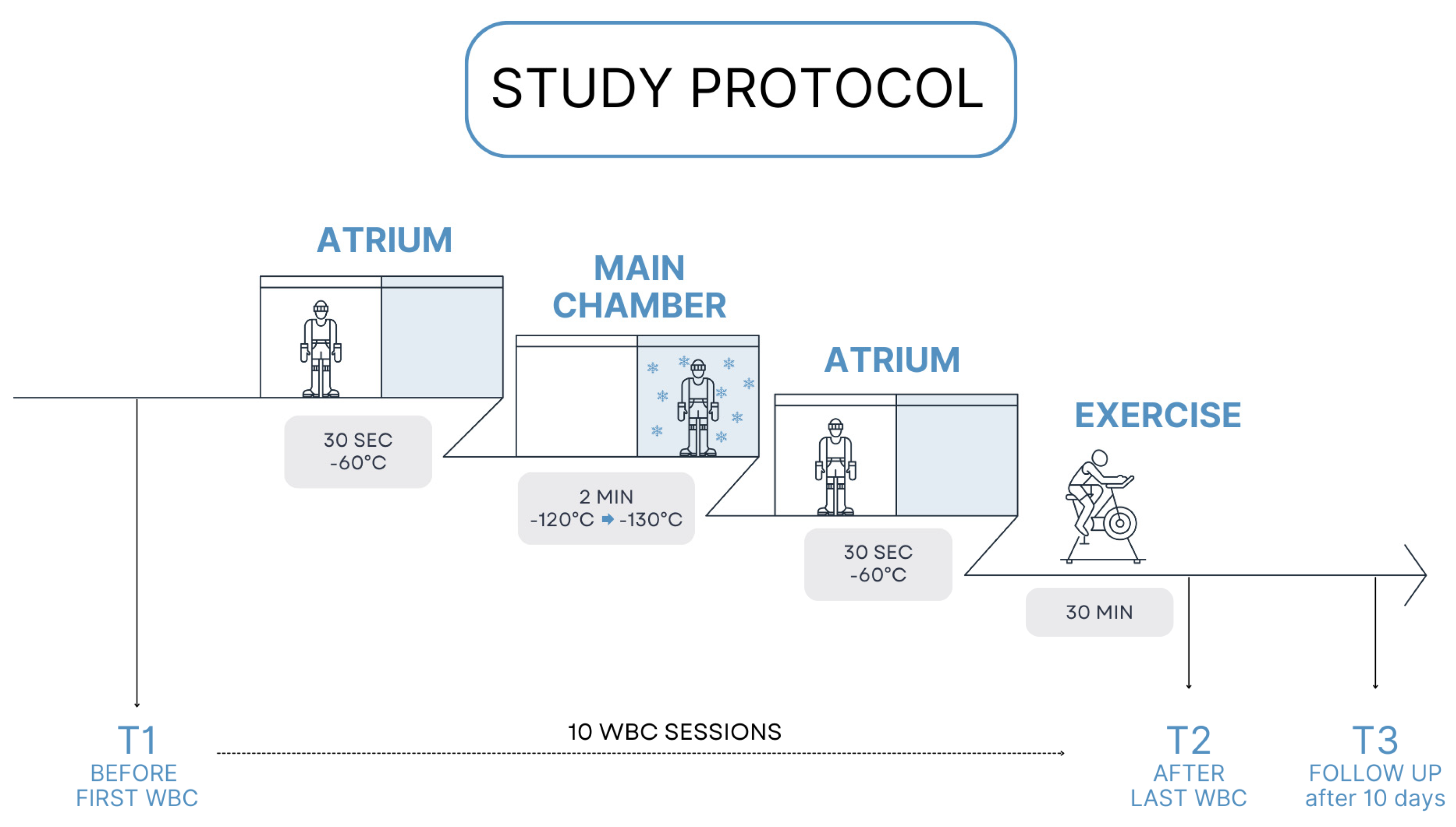
Figure 3.
Percentage of change in the results in every test in non-MS participants.
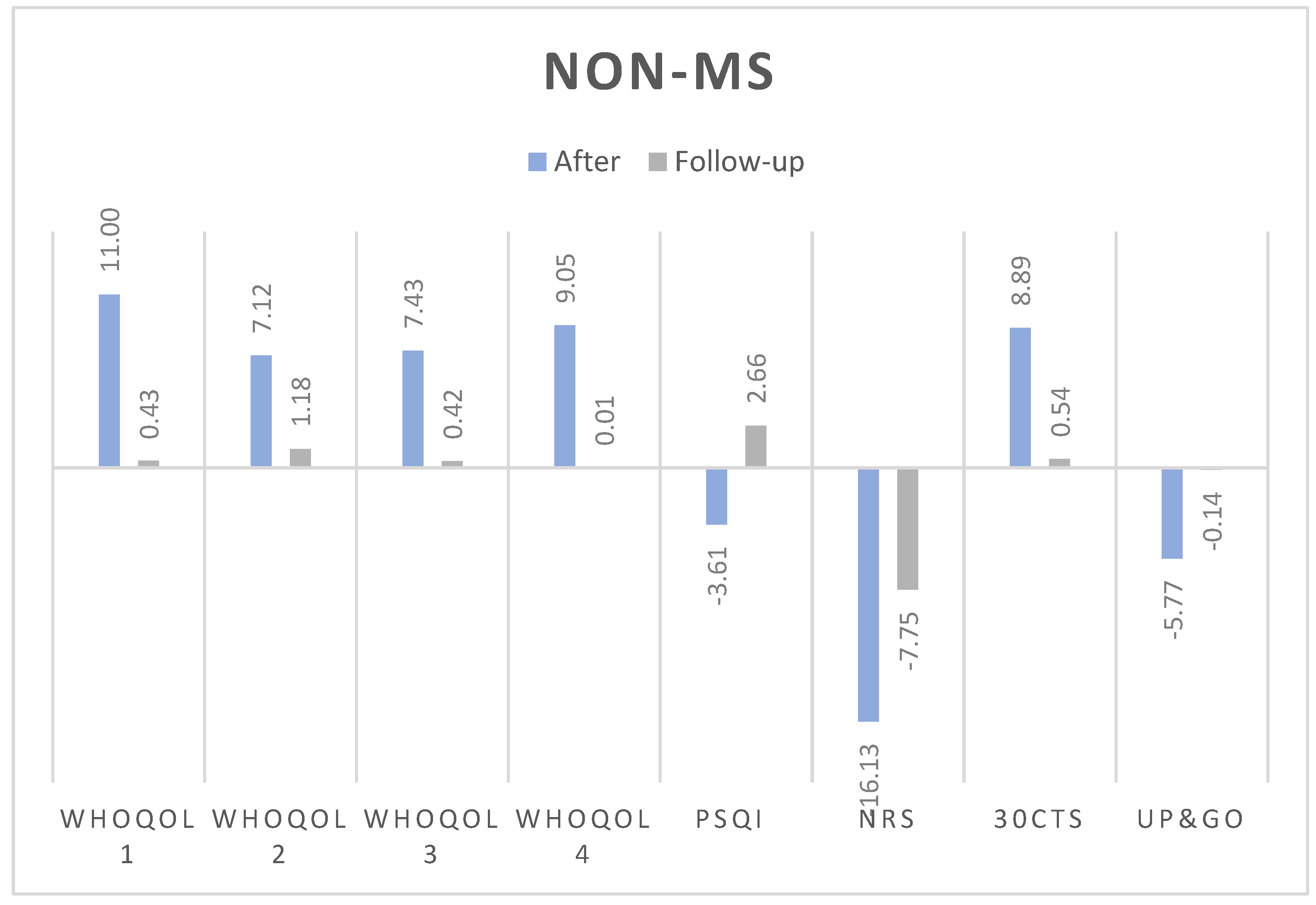
Figure 4.
Percentage of change in the results in every test in MS participants.
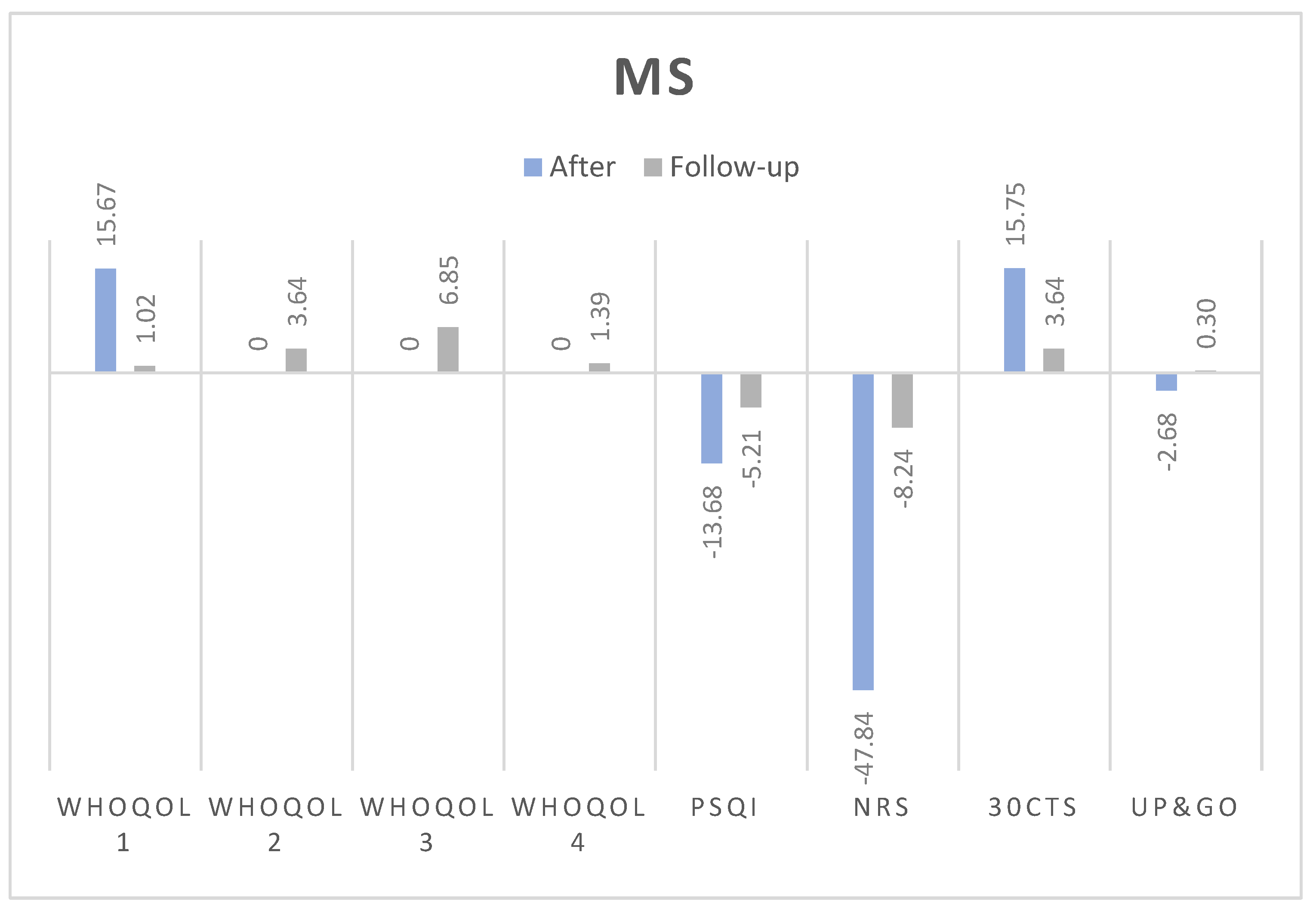
Table 1.
The demographic and baseline characteristics of the study participants.
|
All (n=73) |
NON-MS (n=43) |
MS (n=30) |
|
| Gender | |||
| Females | 62 (83.78) | 39 (88.64) | 23 (76.67) |
| Males | 11 (14.86) | 4 (9.09) | 7 (23.33) |
| Education | |||
| Primary education | 2 (2.70) | 2 (4.54) | 0 |
| Secondary education | 28 (37.84) | 21 (47.73) | 7 (23.33) |
| Higher education | 43 (58.11) | 20 (45.45) | 23 (76.67) |
| Working status | |||
| employed | 45 (60.81) | 22 (50.00) | 23 (76.67) |
| unemployed | 1 (1.35) | 0 | 1 (3.33) |
| retiree | 23 (31.08) | 19 (43.18) | 4 (13.33) |
| Disability pensioner | 4 (5.40) | 2 (4.54) | 2 (6.67) |
| Comorbidities | |||
| No | 36 (48.65) | 18 (40.91) | 18 (60.00) |
| Yes | 37 (51.35) | 25 (59.09) | 12 (40.00) |
| Smoking | |||
| No | 61 (82.43) | 36 (81.82) | 25 (83.33) |
| Yes | 12 (16.22) | 7 (18.18) | 5 (16.67) |
| Special diet | |||
| No | 64 (86.49) | 34 (77.27) | 30 (100.00) |
| Yes | 9 (12.16) | 9 (20.45) | 0 |
| Physical activity | |||
| More than 2 times per week | 33 (44.59) | 20 (45.45) | 13 (43.33) |
| 2 times per week | 15 (20.27) | 11 (25.00) | 4 (13.33) |
| 1 time per week | 13 (17.57) | 7 (15.91) | 6 (20.00) |
| 1 time per month | 3 (4.05) | 1 (2.27) | 2 (6.67) |
| No physical activity | 9 (12.16) | 4 (9.09) | 5 (16.67) |
| WBC in the past | |||
| No | 18 (24.32) | 3 (6.82) | 15 (50.00) |
| Yes | 55 (74.32) | 40 (90.91) | 15 (50.00) |
Table 2.
Changes in test results before WBC, after 10 sessions and after 10 days from last session.
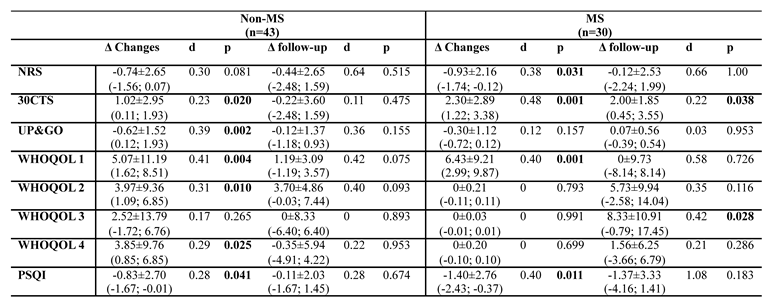
Table 3.
Correlations between the QoL and quality of sleep after 10 WBC sessions.
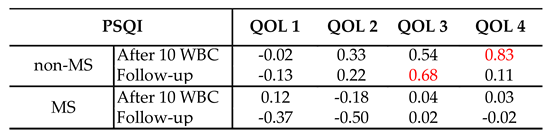
Table 4.
Correlations between the number of cryotherapy sessions in the past and obtained test results.
Table 4.
Correlations between the number of cryotherapy sessions in the past and obtained test results.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



