Submitted:
06 April 2025
Posted:
08 April 2025
You are already at the latest version
Preprints on COVID-19 and SARS-CoV-2
Abstract
Background: The COVID-19 pandemic has significantly disrupted healthcare systems, including the management of emergency general surgery. Even though the pandemic ended, the new variants are continuously emerging, making it necessary to standardized the management protocols of emergency general surgery in COVID patients. Objective: This meta-analysis aims to evaluate the outcomes of emergency general surgery in COVID-19 patients compared to non-COVID-19 patients, focusing on mortality, postoperative complications, mechanical ventilation, and ICU admissions. Methods: A systematic search of PubMed, Embase, Cochrane Library, Scopus, and Web of Science databases was conducted, including studies published between December 2019 and the present. Observational studies, cohort studies, case-control studies, and randomized controlled trials reporting outcomes of emergency general surgery in adult patients with and without COVID-19 were included. A random-effects meta-analysis model was employed, and heterogeneity was assessed using the I² statistic. Publication bias was evaluated using funnel plot. Results: The analysis included 10 studies encompassing 7559 patients (3118 COVID19 group, 4441 non-COVID19 group). COVID-19 group patients demonstrated significantly higher mortality having odds ratio (OR) of 3.0036 (95% CI: 2.4263, 3.7184) and risk ratio (RR) of 2.8333 (95% Cl: 2.3127, 3.4712). Conclusion: Emergency general surgery in COVID-19 patients is associated with worse outcomes, including increased mortality, higher complication rates, and increased ICU admissions. These findings highlight the need for tailored perioperative strategies for COVID patients to mitigate risks.
Keywords:
COVID-19
; Corona virus
; Emergency general surgery
; Appendicitis
; Acute cholecystitis
; Pandemic
1. Introduction
The emergence of COVID-19 has imposed unprecedented challenges on global healthcare systems. First reported from Wuhan, China, in December 2019, it spread rapidly around the world and a global pandemic was declared by World Health Organization in March 2020 [Lescure FX et al., 2020; Machhi J et al., 2020; Tadesse S, Muluye W, 2020; Brown WA et al., 2021]. Most COVID-19 patients developed mild-moderate upper respiratory tract symptoms (fever, cough & fatigue) [Huang C et al., 2020; Rodriguez-Morales AJ et al., 2020; Brown WA et al., 2021]. However, in about 8-15% of patients it progresses to a more severe illness with respiratory failure, acute respiratory distress syndrome, multiple organ failure and death [Machhi J et al., 2020; Stawicki SP et al., 2020; Brown WA et al., 2021].
With its rapid spread and high morbidity and mortality rates, the pandemic has strained resources, disrupted routine medical care, and led to significant delays or modifications in the delivery of surgical services [Abate et al., 2020]. Emergency general surgery (EGS) represents a critical component of healthcare, often involving life-threatening conditions such as appendicitis, bowel obstruction, or perforation, which demand immediate intervention. The intersection of COVID-19 and EGS has introduced unique clinical complexities, including concerns about viral transmission, altered patient physiology, and resource limitations.
Early reports suggest that COVID-19 patients undergoing surgery face a higher risk of adverse outcomes, including elevated mortality and complication rates [Abate et al., 2020; Collaborative Covids, 2020; Doglietto F et al., 2020; Brown WA et al., 2021]. These findings underscore the need for a comprehensive understanding of the pandemic's impact on surgical practice to inform clinical decision-making and resource allocation during future crises. Although, the pandemic is ended, but its new variants are emerging. This makes it necessary to formulate a strategy of managing these patients in emergency surgical conditions, both pathological emergencies and traumatic emergencies.
This meta-analysis aims to evaluate the outcomes of emergency general surgery in COVID-19 patients, comparing them to non-COVID-19 patients. By synthesizing data from available studies, this analysis seeks to provide evidence-based insights into the perioperative risks and challenges associated with managing these patients.
2. Methods
This section outlines the systematic approach undertaken for the meta-analysis to ensure the inclusion of robust, high-quality studies. The methodology adheres to Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines and focuses on rigorously evaluating outcomes of emergency general surgery in COVID-19 patients.
A comprehensive literature search was conducted across five databases: PubMed, Embase, Cochrane Library, Scopus, and Web of Science. The search spanned publications from December 2019, when COVID-19 was first identified, to the present. Both MeSH terms and free-text keywords were used to ensure broad coverage of relevant studies. Key search terms included:
- COVID-19-related terms: “COVID-19,” “SARS-CoV-2,” “coronavirus infection”
- Surgical terms: “emergency surgery,” “urgent surgery,” “general surgery”
- Outcome measures: “mortality,” “complications,” “postoperative outcomes,” “ICU admission,” “mechanical ventilation”
The search was limited to English-language publications involving human subjects. Any paper without associated data, like abstracts, editorials and opinions, were excluded. The inclusion criteria were all adult patients (≥18 years) admitted with the diagnosis of emergency general surgery condition, whether undergoing emergency general surgery or managing conservatively, during pandemic with or without confirmed COVID-19 diagnosis via Polymerase Chain Reaction (PCR) testing or clinical evaluation. Randomized controlled trials (RCTs), cohort studies, case-control studies, or case series with comparative groups (COVID-19 positive vs. COVID-19 negative patients) were selected.
The exclusion criteria were studies involving elective surgeries, non-surgical interventions, or pediatric patients (<18 years), non-comparative studies, reviews, commentaries, and abstracts without associated data, and duplicate studies across different databases.
The screening process adhered to a standardized protocol. Two independent reviewers screened all titles and abstracts against the inclusion/exclusion criteria. Disagreements were resolved through consensus or consultation with a third reviewer. Studies passing the initial screening underwent full-text review to confirm eligibility. A PRISMA flowchart was created to visually represent the screening and selection process.
Data were extracted independently by two reviewers using a standardized extraction template, and discrepancies were resolved by a third reviewer. It includes study characteristics (authors, year of publication, country, study design, sample size), patient demographics (age, gender, comorbidities), surgical details (non-operative management or type of surgery performed). The primary outcome variable is 30-day mortality rate, whereas secondary variables are morbidity, mechanical ventilation and ICU admissions, along with the patients’ demography.
Risk of bias was assessed using the Newcastle-Ottawa Scale (NOS) for observational studies. Statistical analysis was performed using R packages for pooled analyses, forest plot generation, and bias evaluations with funnel plot generation. Dichotomous outcomes ie Odds ratios (OR) and risk ratio, with 95% confidence intervals (CIs) were calculated for the primary outcome. A random-effects model was employed due to the anticipated heterogeneity of included studies. Heterogeneity assessment made with I² statistic (low heterogeneity: I² < 30%, moderate heterogeneity: I² 30%-60%, high heterogeneity: I² > 60%). Publication bias assessed with funnel plot giving visual inspection for symmetry, as well as by linear regression analysis as an alternative to Egger’s Test.
This methodical approach ensures a comprehensive evaluation of emergency general surgery outcomes in COVID-19 patients, laying a foundation for robust clinical insights.
3. Results
Study Selection and Characteristics
A total of 10 studies were included in the meta-analysis, comprising 7559 patients (3118 COVID-19 group and 4441 non-COVID-19). The PRISMA flow diagram outlines the study selection process (Figure 1). The included studies spanned 8 countries and were published between 2021-2023. The majority were cohort studies, with additional contributions from one case-control study [Fernández-Martínez M et al., 2021].
Table 1 summarizes the characteristics of the included studies, including first author’s name, Country, study year, types of surgeries, and presence/absence of comparative/control group. Table 2 summarizes the demographics and outcome variables, including total number of patients, age, sex, mortality rate, morbidity rate, mechanical ventilation and ICU admission.
Outcomes Variables
Overall, COVID-19 group patients demonstrated significantly higher mortality having odds ratio (OR) of 3.0036 (95% CI: 2.4263, 3.7184) and risk ratio (RR) of 2.8333 (95% Cl: 2.3127, 3.4712). Table 2 shows the individual OR and RR of these 10 studies.
Table 3 summarizes the effect size calculated from mortality rates in 2 groups. Similarly, the odds of experiencing complications were markedly increased in COVID-19 patients (Table 2). Only 2 studies mentioned the use of mechanical ventilation due to pulmonary complications from COVID19, whereas 3 studies mentioned about ICU admissions.
The meta-analysis has yielded an estimated effect size of approximately 2.35 with a standard error of 1.29. The heterogeneity statistics indicate a very high level of variability among the studies (I² = 99.86%), suggesting that the results may not be consistent across the included studies. The forest plot (Figure 2) illustrates the individual effect sizes for each study along with the overall effect size. It illustrates the pooled odds ratios (OR) and 95% confidence intervals (CI) for mortality between COVID-19 and non-COVID-19 patients across included studies. The dashed line represents the null effect (OR = 1). The effect size (Figure 2) displays the effect sizes (Cohen’s d) for each study, along with confidence intervals.
Visual inspection of the funnel plot (Figure 3) for mortality outcomes indicated asymmetry, suggesting potential publication bias. It clearly indicates the effect size (Cohen’s d) on the x-axis and the standard error on the y-axis, making it easier to interpret the results. The results of the linear regression analysis, which serves as an alternative to Egger’s Test, indicate that the intercept is approximately 2.966, and the coefficient for the standard error (SE) is -7.864. The p-value for the SE coefficient is 0.751, which suggests that there is no significant relationship between the effect sizes and their standard errors, indicating a lack of evidence for publication bias.
4. Discussion
The COVID-19 pandemic has profoundly impacted healthcare systems globally, necessitating a reevaluation of surgical practices, especially in emergency settings. This meta-analysis, synthesizing data from 10 studies, provides compelling evidence that emergency general surgery in COVID-19 patients is associated with significantly worse outcomes compared to non-COVID-19 patients. These findings highlight the critical need for tailored strategies to optimize surgical care in the context of a pandemic or even in managing emergency general surgery in COVID-19 patients in non-pandemic period.
The findings in these studies differ, which may be due to variations in public health interventions, pandemic severity, and healthcare resources across regions. Non-Operative Management (NOM) was reported in a few studies; however, this is within the principles of surgery [Ciarleglio FA et al., 2021; Lazzati A et al., 2021; Singh C et al., 2021]. NOM may have contributed to managing patient loads effectively during the pandemic, and at the same time minimizing the risk of virus spread via the operating room [Willms AG et al., 2020]. There were NOM failure as well, leading to operative intervention, again according to the surgical principles [ Martínez Caballero J et al., 2021].
The meta-analysis revealed a markedly higher postoperative mortality rate in COVID-19 patients, as reported in several other studies [Doglietto F et al., 2020; Ciarleglio FA et al., 2021; Lazzati A et al., 2021; Singh C et al., 2021; Aloyan K et al., 2021; Carrier FM et al., 2021; Prasad NK et al., 2021; Alelyani RH et al., 2022; Pratha AR et al., 2023]. This aligns with prior reports suggesting that severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) infection exacerbates perioperative risks due to factors such as hyperinflammatory states, coagulopathies, and pulmonary compromise [Saleh SK et al., 2020; Yuki K et al., 2020; Luca M et al., 2021; Aloyan K et al., 2021; Pratha AR et al., 2023; Cascella M et al., 2024]. The disproportionate impact on older adults and those with comorbidities underscores the need for heightened vigilance in these patients. Hypertension, diabetes, Chronic Obstructive Pulmonary Disease (COPD), cardiovascular disease, cerebrovascular disease and chronic renal disease were reported as major risk factors for serious events in these patients [Nandy K et al., 2020; Wang B et al., 2020; Ciarleglio FA et al., 2021; Singh C et al., 2021; Luca M et al., 2021; Prasad NK et al., 2021]. COVID-19 patients experienced a higher rate of postoperative complications, particularly respiratory complications [Doglietto F et al., 2020; Aloyan K et al., 2021]. The underlying pathophysiological mechanisms, including viral pneumonia, cytokine storm, and altered immune responses, likely contribute to this increased risk. Surgery may exacerbate these mechanisms by adding pro-inflammatory state, as well as causing additional strains on cardiorespiratory systems [Kavanagh BP, 2007; Hedenstierna G, Edmark L, 2010; Alazawi W et al., 2016; Ball L et al., 2018; Scholten R et al., 2019; Duggan M, Gerstein NS et al., 2020; Rieder M et al., 2020]. Notably, abdominal surgeries were associated with a greater complication burden, potentially due to the interplay between intra-abdominal infections and systemic inflammation. The mean hospital stay for COVID-19 patients was significantly longer [Prasad NK et al., 2021; Alelyani RH et al., 2022; Pratha AR et al., 2023]. This finding reflects the complexity of managing postoperative recovery in the presence of SARS-CoV-2 infection, compounded by the need for extended monitoring and isolation protocols. The odds of ICU admissions and mechanical ventilation were significantly higher among COVID-19 patients [Prasad NK et al., 2021]. This likely results from a combination of COVID-19-related respiratory failure, heightened perioperative complications, and resource-intensive postoperative care requirements.
The findings of this meta-analysis have several clinical implications. Surgical decision-making in COVID-19 patients should incorporate a comprehensive risk assessment, prioritizing non-surgical management where feasible or deferring procedures in stable cases until viral clearance. Given the increased need for ICU admissions and prolonged hospital stays, healthcare systems must ensure adequate resource planning during pandemics to accommodate the surgical burden [Lazzati A et al., 2021; Carrier FM et al., 2021]. Enhanced infection prevention measures, including preoperative testing and strict intraoperative protocols, are essential to minimize nosocomial transmission and optimize patient outcomes.
Strengths:
- Comprehensive and rigorous methodology adhering to PRISMA guidelines.
- Inclusion of diverse study designs across multiple geographical regions, enhancing generalizability.
- Robust statistical analyses to ensure result reliability.
Limitations:
- Markedly high heterogeneity (I² = 99.86%), likely reflecting variations in healthcare infrastructure, patient populations, and surgical practices.
- Potential publication bias, as suggested by funnel plot asymmetry.
- Limited availability of high-quality randomized controlled trials, with most data derived from observational studies.
Future Directions
- Prospective, multicenter studies to validate these findings and elucidate underlying mechanisms.
- Development of perioperative protocols tailored to COVID-19 patients, emphasizing preoperative optimization and postoperative care.
- Exploration of long-term outcomes, including quality of life and functional recovery in COVID-19 surgical patients.
5. Conclusions
This meta-analysis demonstrates that emergency general surgery in COVID-19 patients is associated with significantly higher mortality, complication rates, and healthcare resource utilization. These findings highlight the critical need for tailored perioperative strategies to mitigate risks and improve outcomes. As the world continues to grapple with COVID-19 variants, these insights are invaluable in shaping resilient and adaptive surgical practices.
Acknowledgement
The author is grateful to the Deanship of Scientific Research at Prince Sattam Bin Abdulaziz University, Alkharj, Kingdom of Saudi Arabia, for its support and encouragement in conducting the research and publishing this report.
Conflict of Interest
None.
Abbreviations
| COVID-19 | Coronavirus disease of 2019 |
| ICU | Intensive Care Unit |
| I2 | Statistical measure of inconsistency or heterogeneity between studies |
| OR | Odds ratio |
| 95% CI | 95% Confidence Interval |
| RR | Risk ratio |
| EGS | Emergency general surgery |
| PRISMA | Preferred Reporting Items for Systematic Reviews and Meta-Analyses |
| PCR | Polymerase Chain Reaction |
| RCT | Randomized controlled trial |
| NOS | Newcastle-Ottawa Scale |
| NOM | Non-Operative Management |
| SARS-CoV-2 | Severe acute respiratory syndrome coronavirus 2 |
| COPD | Chronic Obstructive Pulmonary Disease |
References
- Abate SM, Mantefardo B, & Basu B. (2020). Postoperative mortality among surgical patients with COVID-19: a systematic review and meta-analysis. Patient Safety in Surgery, 14(1), 1–14. [CrossRef]
- Alazawi W, Pirmadjid N, Lahiri R, & Bhattacharya S. (2016). Inflammatory and Immune Responses to Surgery and Their Clinical Impact. Annals of surgery, 264(1), 73–80. [CrossRef]
- Alelyani RH, Alghamdi AH, Mahrous SM, Alamri BM, Alhiniah MH, Abduh MS, et al. (2022). Impact of COVID-19 Pandemic Lockdown on the Prognosis, Morbidity, and Mortality of Patients Undergoing Elective and Emergency Abdominal Surgery: A Retrospective Cohort Study in a Tertiary Center, Saudi Arabia. International Journal of Environmental Research and Public Health, 19(23), 15660. [CrossRef]
- Aloyan K, Harutyunyan H, & Voskanyan A. (2021). Virology: Current Research Early and Late Complications after Abdominal Surgery in Patients with COVID-19 in Armenia. In Virol Curr Res (Vol. 5).
- Ball L, Costantino F, Fiorito M, Amodio S, & Pelosi P. (2018). Respiratory mechanics during general anaesthesia. Annals of translational medicine, 6(19), 379. [CrossRef]
- Brown WA, Moore EM, & Watters DAK. (2021). Mortality of patients with COVID-19 who undergo an elective or emergency surgical procedure: a systematic review and meta-analysis. Anz Journal of Surgery, 91, 33–41. [CrossRef]
- Carrier F M, Amzallag É, Lecluyse V, Côté G, Couture EJ, D’Aragon F, et al. (2021). Postoperative outcomes in surgical COVID-19 patients: a multicenter cohort study. BMC Anesthesiology, 21(1), 15. [CrossRef]
- Cascella M, Rajnik M, Aleem A, Dulebohn SC, & Di Napoli R. (2024). Features, Evaluation, and Treatment of Coronavirus (COVID-19). StatPearls Publishing. https://www.ncbi.nlm.nih.gov/books/NBK554776/.
- Chan A, Stathakis P, Goldsmith P, Smith SJ, & Macutkiewicz C. (2022). The reorganisation of emergency general surgery services during the COVID-19 pandemic in the UK: outcomes of delayed presentation, socio-economic deprivation and Black, Asian and Minority Ethnic patients. Annals of The Royal College of Surgeons of England. [CrossRef]
- Ciarleglio FA, Rigoni M, Rigoni M, Mereu L, Tommaso C, Carrara A, et al. (2021). The negative effects of COVID-19 and national lockdown on emergency surgery morbidity due to delayed access. World Journal of Emergency Surgery, 16(1), 37. [CrossRef]
- Collaborative Covids. (2020). Mortality and pulmonary complications in patients undergoing surgery with perioperative SARS-CoV-2 infection: An international cohort study. The Lancet, 396(10243), 27–38. [CrossRef]
- Doglietto F, Vezzoli M, Gheza F, Lussardi GL, Domenicucci M, Vecchiarelli L, et al. (2020). Factors Associated With Surgical Mortality and Complications Among Patients With and Without Coronavirus Disease 2019 (COVID-19) in Italy. JAMA Surgery, 155(8), 691–702. [CrossRef]
- Duggan M, & Kavanagh BP. (2007). Atelectasis in the perioperative patient. Current opinion in anaesthesiology, 20(1), 37–42. [CrossRef]
- Fallani G, Lombardi R, Masetti M, Chisari M, Zanini N, Cattaneo GM, et al. (2021). Urgent and emergency surgery for secondary peritonitis during the COVID-19 outbreak: an unseen burden of a healthcare crisis. Updates in Surgery, 73(2), 753–762. [CrossRef]
- Fernández-Martínez M, Martín-Román L, Fernández-Vázquez ML, Rey-Valcarcel C, Pérez-Díaz D, & Turégano-Fuentes F. (2021). Overall management of emergency general surgery patients during the surge of the COVID-19 pandemic: an analysis of procedures and outcomes from a teaching hospital at the worst hit area in Spain. European Journal of Trauma and Emergency Surgery, 47(3), 693–702. [CrossRef]
- Gebran A, Gaitanidis A, Argandykov D, Maurer LR, Gallastegi AD, Bokenkamp M, et al. (2022). Mortality and pulmonary complications in emergency general surgery patients with COVID-19: A large international multicenter study. The Journal of Trauma and Acute Care Surgery, 93, 59–65. [CrossRef]
- Gerstein NS, Venkataramani R, Goumas AM, Chapman NN, & Deriy L. (2020). COVID-19-Related Cardiovascular Disease and Practical Considerations for Perioperative Clinicians. Seminars in cardiothoracic and vascular anesthesia, 24(4), 293–303. [CrossRef]
- Hedenstierna G, & Edmark L. (2010). Mechanisms of atelectasis in the perioperative period. Best practice & research. Clinical anaesthesiology, 24(2), 157–169. [CrossRef]
- Huang C, Wang Y, Li X, Ren L, Zhao J, Hu Y, et al. (2020). Clinical features of patients infected with 2019 novel coronavirus in Wuhan, China. The Lancet, 395(10223), 497–506. [CrossRef]
- Lazzati A, Rousseau MR, Bartier S, Dabi Y, Challine A, Haddad B, et al. (2021). Impact of COVID-19 on surgical emergencies: nationwide analysis. 5(3). [CrossRef]
- Lescure F-X, Bouadma L, Nguyen DB, Parisey M, Wicky P-H, Behillil S, et al. (2020). Clinical and virological data of the first cases of COVID-19 in Europe: a case series. Lancet Infectious Diseases, 20(6), 697–706. [CrossRef]
- Luca M De, Sartori A, Vitiello A, Piatto G, Noaro G, Olmi S, et al. (2021). Complications and mortality in a cohort of patients undergoing emergency and elective surgery with perioperative SARS-CoV-2 infection: an Italian multicenter study. Teachings of Phase 1 to be brought in Phase 2 pandemic. Updates in Surgery, 73(2), 745–752. [CrossRef]
- Lund S, MacArthur TA, Fischmann MM, Maroun JW, Dang J, Markos JR, et al. (2021). Impact of COVID-19 Governmental Restrictions on Emergency General Surgery Operative Volume and Severity. American Surgeon, 31348211011113. [CrossRef]
- Machhi J, Herskovitz J, Senan AM, Dutta D, Nath B, Oleynikov MD, et al. (2020). The Natural History, Pathobiology, and Clinical Manifestations of SARS-CoV-2 Infections. Journal of Neuroimmune Pharmacology, 15(3), 359–386. [CrossRef]
- Martínez Caballero J, González González L, Rodríguez Cuéllar E, Ferrero Herrero E, Pérez Algar C, Vaello Jodra V, et al. (2021). Multicentre cohort study of acute cholecystitis management during the COVID-19 pandemic. European journal of trauma and emergency surgery : official publication of the European Trauma Society, 47(3), 683–692. [CrossRef]
- McGuinness MJ, & Harmston C. (2021). The effect of national public health interventions for COVID-19 on emergency general surgery in Northland, New Zealand. Anz Journal of Surgery, 91(3), 329–334. [CrossRef]
- Nandy K, Salunke AA, Pathak SK, Pandey A, Doctor C, Puj K, et al. (2020). Coronavirus disease (COVID-19): A systematic review and meta-analysis to evaluate the impact of various comorbidities on serious events. Diabetes and Metabolic Syndrome: Clinical Research and Reviews, 14(5), 1017–1025. [CrossRef]
- Pratha AR, Pustela MK, Kaniti VK, Shaik S, & Pecheti T. (2023). Retrospective analysis of outcome of COVID positive patients undergoing emergency surgeries for acute general surgical conditions. International Surgery Journal, 10(3), 432–436. [CrossRef]
- Prasad NK, Çınar S, Lake R, Englum BR, Turner DJ, Siddiqui T, et al. (2021). Increased complications in patients who test COVID-19 positive after elective surgery and implications for pre and postoperative screening. American Journal of Surgery. [CrossRef]
- Rieder M, Goller I, Jeserich M, Baldus N, Pollmeier L, Wirth L, et al. (2020). Rate of venous thromboembolism in a prospective all-comers cohort with COVID-19. Journal of Thrombosis and Thrombolysis, 50(3), 558–566. [CrossRef]
- Rodriguez-Morales AJ, Cardona-Ospina JA, Gutiérrez-Ocampo E, Villamizar-Peña R, Holguin-Rivera Y, Escalera-Antezana JP, et al. (2020). Clinical, laboratory and imaging features of COVID-19: A systematic review and meta-analysis. Travel Medicine and Infectious Disease, 34, 101623. [CrossRef]
- Sá AF, Lourenço SF, da Silva Teixeira R, Barros F, Costa APN, & Lemos P. (2021). Urgent/emergency surgery during COVID-19 state of emergency in Portugal: a retrospective and observational study. Revista Brasileira De Anestesiologia, 71(2), 123–128. [CrossRef]
- Saleh SK, Oraii A, Soleimani A, Hadadi A, Shajari Z, Montazeri M, et al. (2020). The association between cardiac injury and outcomes in hospitalized patients with COVID-19. Internal and Emergency Medicine, 15(8), 1415–1424. [CrossRef]
- Scholten R, Leijtens B, Hannink G, Kamphuis ET, Somford MP, & van Susante JLC. (2019). General anesthesia might be associated with early periprosthetic joint infection: an observational study of 3,909 arthroplasties. Acta Orthopaedica, 90(6), 554–558. [CrossRef]
- Singh C, Kaman L, Shah A, Thakur UK, Ramavath K, Jaideep B, et al. (2021). Surgical outcome of COVID-19 infected patients: experience in a tertiary care hospital in India. International Surgery Journal, 8(3), 899–903. [CrossRef]
- Stawicki SP, Jeanmonod R, Miller AC, Paladino L, Gaieski DF, Yaffee AQ, et al. (2020). The 2019-2020 novel coronavirus (severe acute respiratory syndrome coronavirus 2) pandemic: A joint american college of academic international medicine-world academic council of emergency medicine multidisciplinary COVID-19 working group consensus paper. Journal of Global Infectious Diseases, 12(2), 47–93. [CrossRef]
- Tadesse S and Muluye W. (2020) The Impact of COVID-19 Pandemic on Education System in Developing Countries: A Review. Open Journal of Social Sciences, 8, 159-170. [CrossRef]
- Tarim IA, Derebey M, Ozbalci GS, Ozsay O, Yüksek MA, Buyukakincak S, et al. (2021). The impact of the COVID-19 pandemic on emergency general surgery: a retrospective study. Sao Paulo Medical Journal, 139(1), 53–57. [CrossRef]
- Wang B, Li R, Lu Z, & Huang Y. (2020). Does comorbidity increase the risk of patients with COVID-19: evidence from meta-analysis. Aging (Albany NY), 12(7), 6049–6057. [CrossRef]
- Willms AG, Oldhafer KJ, Conze S, Thasler WE, von Schassen C, Hauer T, et al. (2020). Appendicitis during the COVID-19 lockdown: results of a multicenter analysis in Germany. [CrossRef]
- Yuki K, Fujiogi M, & Koutsogiannaki S. (2020). COVID-19 pathophysiology: A review. Clinical Immunology, 215, 108427. [CrossRef]
Figure 1.
PRISMA Flow Diagram.
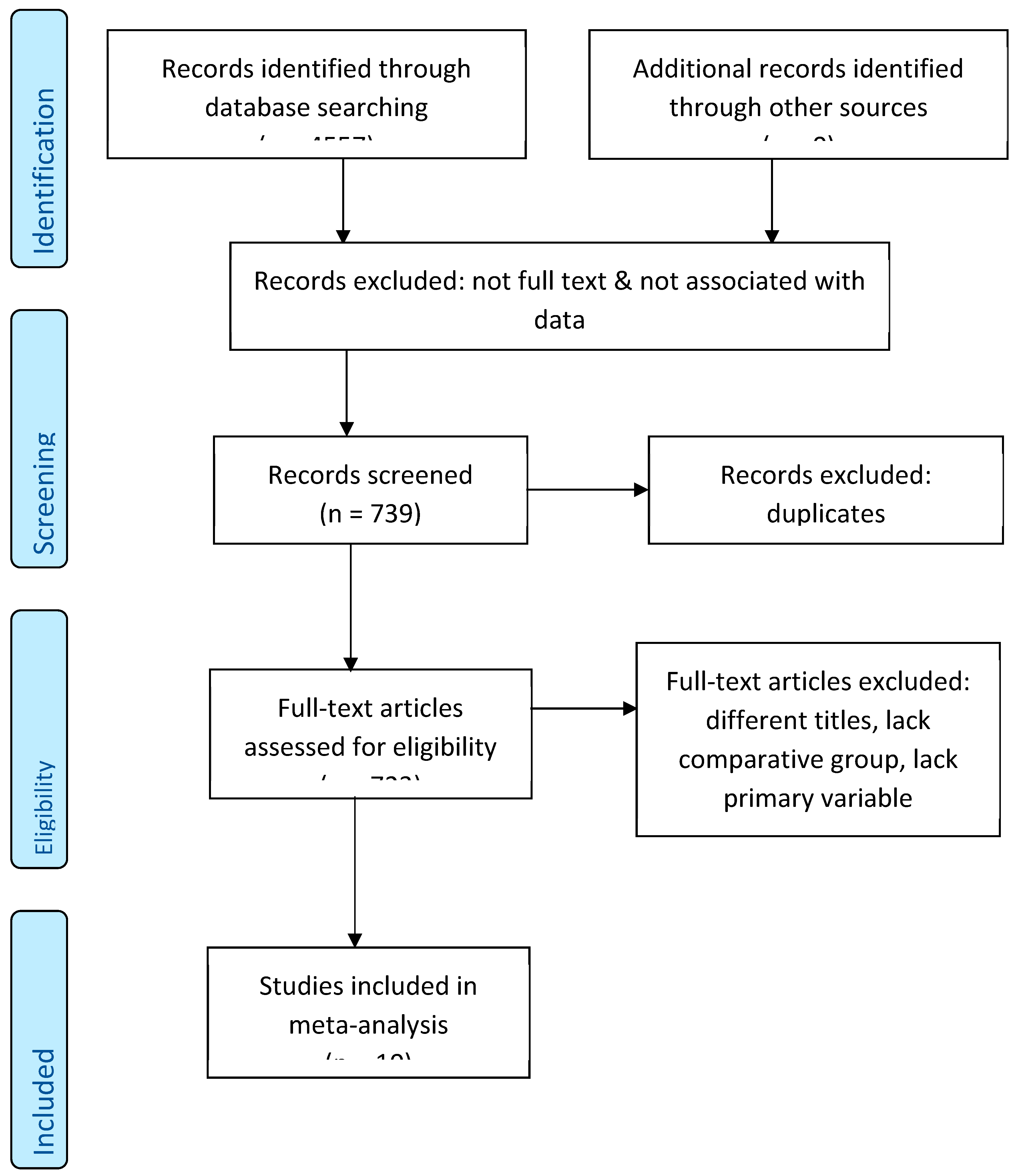
Figure 2.
Forest plot & effect size of meta-analysis.
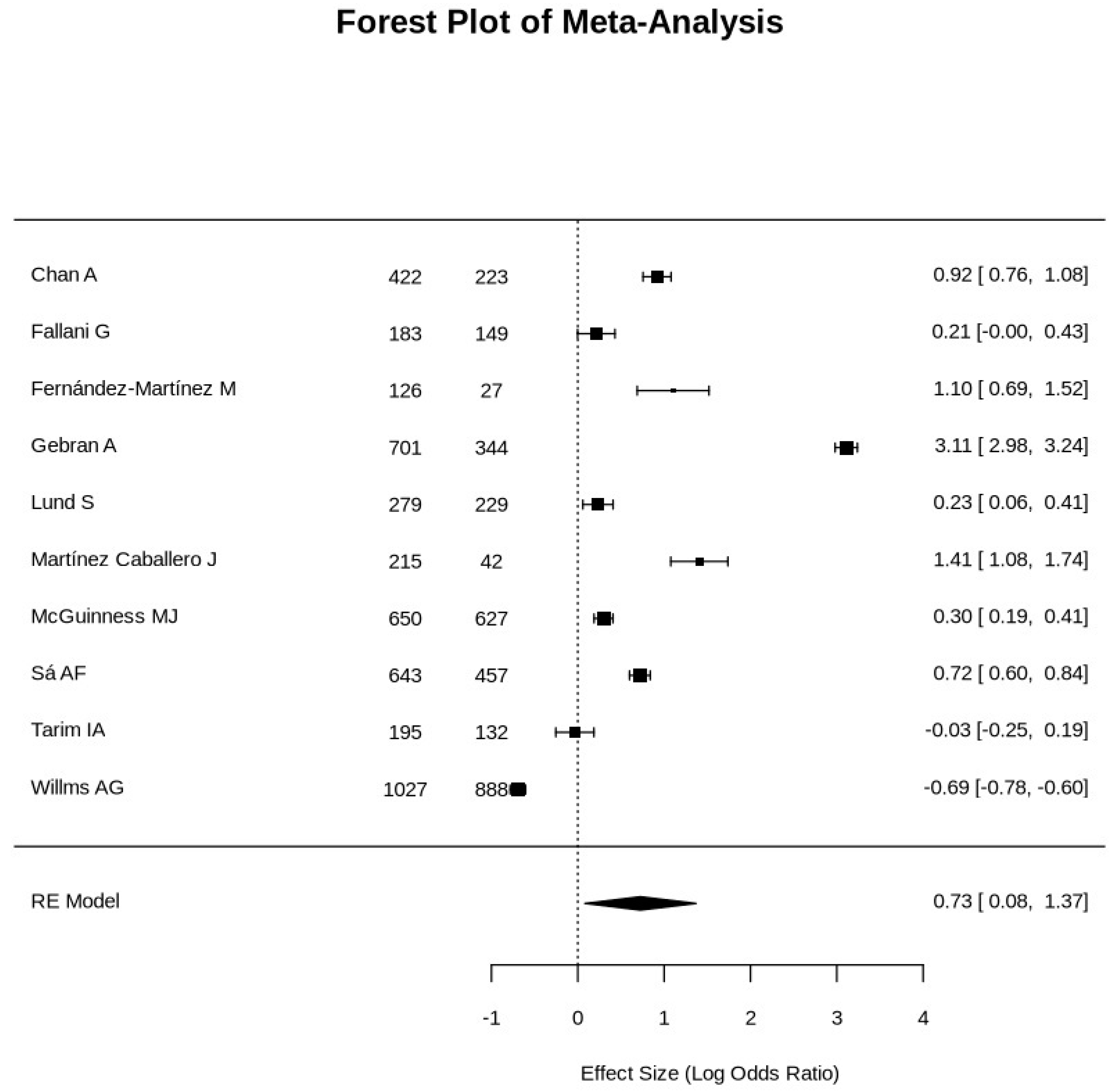
Figure 3.
Funnel plot of meta-analysis.
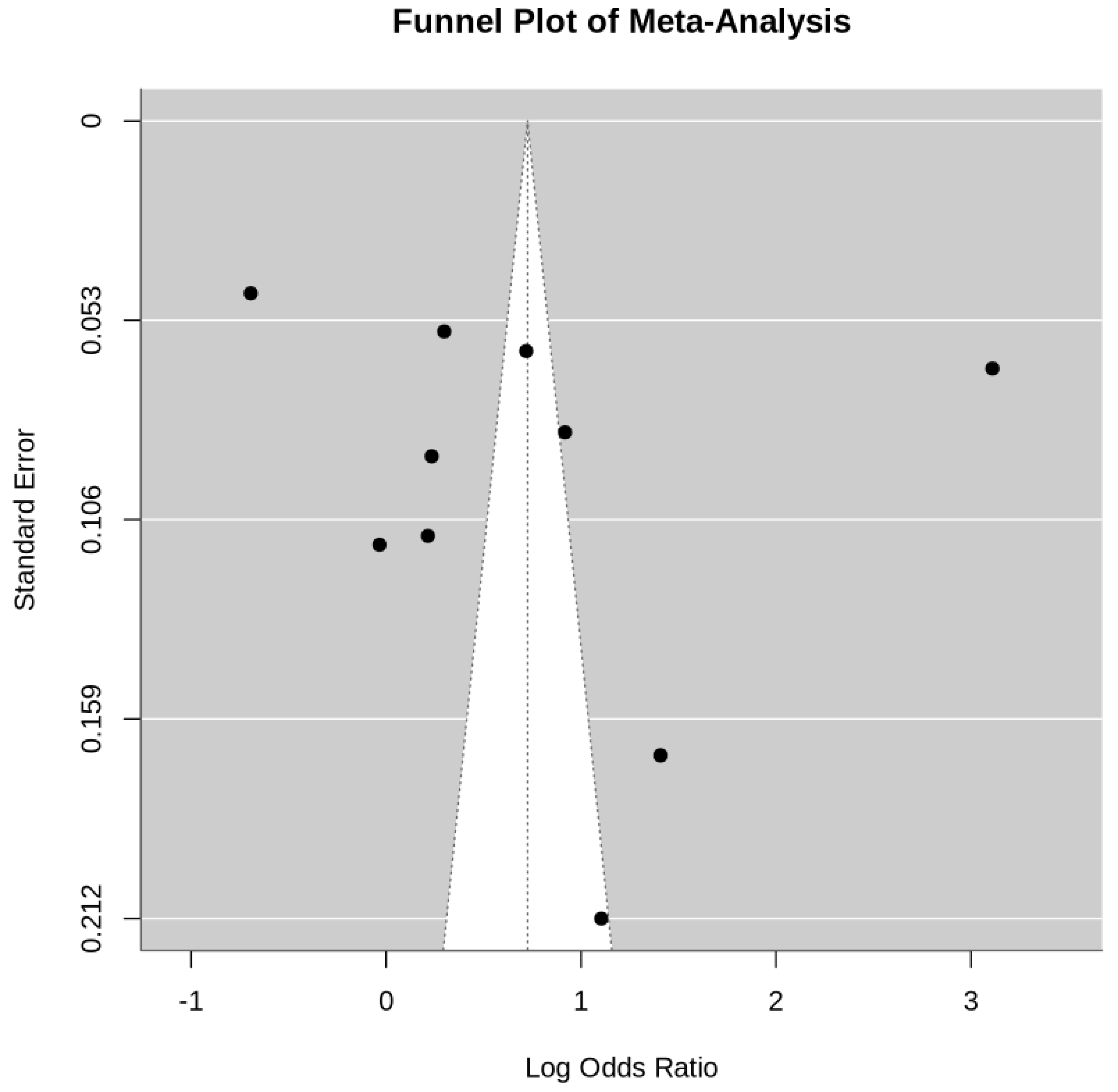

Table 1.
Study characteristics.
| First Author | Country | Year | Type of Surgery | Comparative/Control Group |
|---|---|---|---|---|
| Chan A | UK | 2022 | Emergency General Surgery | Present |
| Fallani G | Italy | 2021 | Emergency Abdominal Surgery | Present |
| Fernández-Martínez M | Spain | 2021 | Emergency General Surgery | Present |
| Gebran A | UK | 2022 | Emergency General Surgery | Present |
| Lund S | USA | 2021 | Emergency General Surgery | Present |
| Martínez Caballero J | Spain | 2021 | Acute Cholecystitis | Present |
| McGuinness MJ | New Zealand | 2021 | Emergency General Surgery | Present |
| Sá AF | Portugal | 2021 | Urgent/Emergency Surgery | Present |
| Tarim IA | Turkey | 2021 | Emergency General Surgery | Present |
| Willms AG | Germany | 2021 | Acute Appendicitis | Present |
Table 2.
Demographics and Outcome variables.
| First Author | Total patients Covid vs. Non-covid |
Patients’ Age (year) Covid vs. Non-covid |
Gender M:F Covid vs. Non-covid |
Mortality Rates Covid vs. Non-covid |
Morbidity Rates Covid vs. Non-covid |
Mechanical Ventilation Covid vs. Non-covid |
ICU Admission Covid vs. Non-covid |
|---|---|---|---|---|---|---|---|
| Chan A | 223, 422 | 48.6, 48.5 (Mean) | 114:109, 191:231 | 5.8%, 2.4% | 5.6%, 4.8% | Not specified | 8.5%, 7.1% |
| Fallani G. | 149, 183 | 49 (26.5-70), 44 [24-61] | 94:55, 97:86 | 6%, 4.9% | 35.6%, 18% | Not specified | Not specified |
| Fernández-Martínez M | 27, 126 | 57.5 ± 21 (total) | 91:62 (total) | 18.5%, 7% | 85.7%, 26.7% | 66%, 0 | 36%, 14% |
| Gebran A | 344, 701 | 17-70 (total) | 220:124, 406:295) | 40.1%, 2.9% | 72.7%, 0 | 23.9%, 0 | Not specified |
| Lund S | 229, 279 | 59.3, 56.7 (Mean) | 102:127, 121:158 | 5%, 4% | 25%, 29% | Not specified | Not specified |
| Martínez Caballero J | 257, 215 | 69 (52-80), 68 (50-80) (Median) | 146:111, 118:97 | 11.9%, 3.2% | 100%, 26% | Not specified | Not specified |
| McGuinness MJ | 627, 650 | 57, 57 (Median) |
327:300, 314:336 | 4%, 3% | Not specified | Not specified | Not specified |
| Sá AF | 457, 643 | 67, 63 (Median) | 261:196, 368:275 |
11.40%, 5.9% | Not specified | Not specified | Not specified |
| Tarim IA | 132, 195 | 50, 53 (Median) | 74:58, 82:113 | 3%, 3.1% | 7%, 1.5% | Not specified | Not specified |
| Willms AG | 888, 1027 | 36 ± 20, 35 ± 19 (Mean) | 468:420, 510:517 | 0.1%, 0.2% | 14.3%, 13.3% | Not specified | 4.5%, 3.9% |
Table 3.
Effect size measures.
| First Author | Effect Size (Cohen's d) |
Odds Ratio (OR) | OR, 95% CI | Risk Ratio (RR) | RR, 95% CI |
|---|---|---|---|---|---|
| Chan A | 1.383370166 | 2.5039 | 1.082, 5.7941 | 2.4167 | 1.0792, 5.4119 |
| Fallani G. | 0.68441989 | 1.2388 | 0.4778, 3.2118 | 1.2245 | 0.4975, 3.014 |
| Fernández-Martínez M | 1.666187845 | 3.0158 | 0.9191, 9.8958 | 2.6429 | 0.957, 7.2894 |
| Gebran A | 12.3839779 | 22.415 | 13.718, 36.6256 | 13.8276 | 8.8398, 21.6296 |
| Lund S | 0.697900552 | 1.2632 | 0.5433, 2.9366 | 1.25 | 0.5585, 2.7979 |
| Martínez Caballero J | 2.257458564 | 4.086 | 1.226, 13.6181 | 3.7188 | 1.2336, 11.2104 |
| McGuinness MJ | 0.744309392 | 1.3472 | 0.7377, 2.4602 | 1.3333 | 0.7454, 2.3849 |
| Sá AF | 1.133756906 | 2.0521 | 1.3258, 3.1763 | 1.9322 | 1.2942, 2.8847 |
| Tarim IA | 0.534088398 | 0.9667 | 0.267, 3.5008 | 0.9677 | 0.2779, 3.37 |
| Willms AG | 0.275966851 | 0.4995 | 0.0414, 6.0297 | 0.5 | 0.0416, 6.0162 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



