
Submitted:
14 December 2024
Posted:
16 December 2024
You are already at the latest version
Abstract
Background/Objectives:
Immunisation with hepatitis B vaccine is the most effective means of preventing acute HBV infection.
However, whether primary vaccination of infants confers lifelong immunity remains controversial. Therefore, ongoing surveillance of vaccine recipients is required.
Methods: A longitudinal study was carried out based on LongAn county, one of the five clinical trial centres for hepatitis B immunization in China in the 1980s. Serum samples were collected and tested for HBV serological markers and DNA.
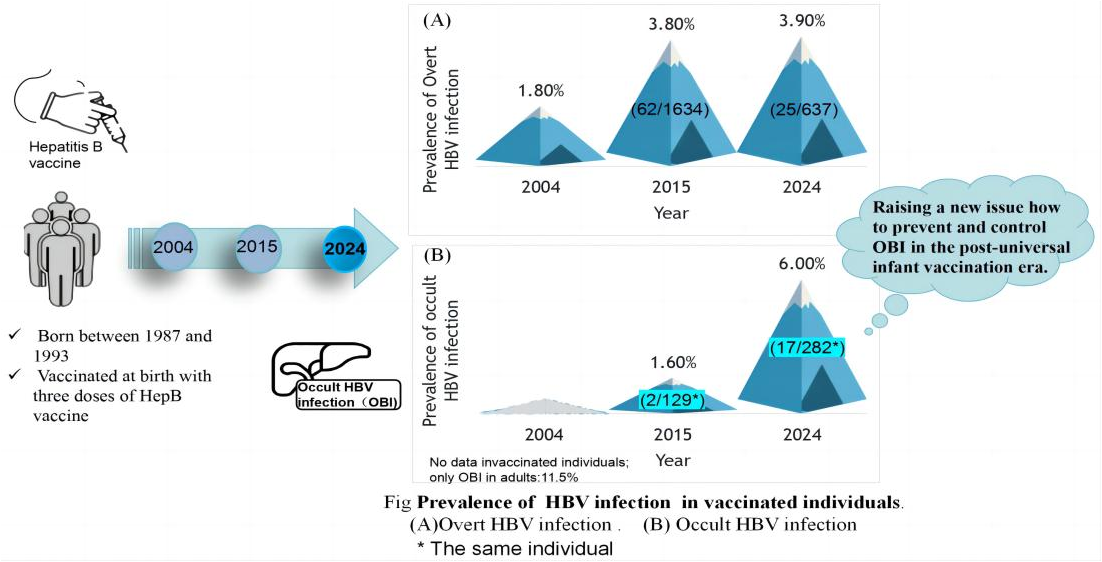
Results: A total of 637 subjects born in 1987-1993 were recruited, including 503 males and 134 females. The total prevalence of HBsAg was 3.9%. The prevalence in females (8.2%) was significantly higher than in males (2.8%) (p=0.004). The prevalence of anti-HBc in females (46.3%) was also significantly higher than in males (41.7%) (p=0.021). The prevalence of anti-HBs was 42.7% and did not differ significantly between males (41.7%) and females (46.3%) (p=0.347). Compared to data from surveillance over the last ten years, the positivity rate of HBsAg had not increased. The positivity rate of anti-HBs decreased significantly (p=0.049) while that of anti-HBc increased significantly (p=0.001). The prevalence of occult HBV infection (OBI) in 2024 (6.0%) was significantly higher than in 2017 (1.6%) (p=0.045). Subjects diagnosed with OBI in 2015 maintained occult infection in 2024.
Conclusions: Neonatal HBV vaccination maintained effective protection at least 37 years. However, the prevalence of OBI is increasing with age in those vaccinated at birth, raising a new issue how to prevent and control OBI in the post-universal infant vaccination era.
Keywords:
Hepatitis B virus (HBV)
; Occult HBV infection
; Hepatitis B vaccine
; Vaccination
; Prevalence
1. Introduction
Despite global immunization programmes, persistent infection with hepatitis B virus (HBV) remains a major public health problem. The infection, which may lead to acute and chronic liver diseases, including cirrhosis and hepatocellular carcinoma (HCC) [1], is transmitted perinatally, horizontally between children in infancy, and via the percutaneous route [2]. More than two billion people, one-third of the world’s population alive today, have been infected with HBV and approximately 257 million remain persistently infected[3]. Regarding HBV-related HCC, it is estimated that the number of associated deaths was 192,000 in 2019, an increase from 156,000 in 2010 [4].
The first hepatitis B vaccine was licensed in 1981 [5] and immunization has become the most effective means of preventing acute infection by HBV [6]. In 1992, the World Health Organization set a goal for all countries to introduce the hepatitis B vaccine into the national Expanded Program on Immunization (EPI) by 1997 [7]. Globally, the prevalence of chronic HBV infection among children below 5 years of age fell from 4.7% to 1.3% over two decades [8]. A remarkable reduction in HBV-related diseases was been observed in Italy in the first three decades of universal vaccination [9]. Universal vaccination of newborns has reduced the incidence of HCC in Asia, compared to the pre-vaccination era [10]. However, whether immunization of neonates provides lifelong protection remains contentious, because immunity to HBV may deteriorate over time. Individuals with high initial levels of HBV immunity may experience a faster rate of decline of antibody titres [11]. Therefore, ongoing surveillance of vaccine recipients is needed to determine whether primary hepatitis B vaccination can confer lengthy, or even lifelong, protection [6].
Meanwhile, more and more evidence reveals that occult HBV infection (OBI) may occur in individuals vaccinated at birth [12]. These individuals may be those born to HBsAg-negative mothers [13] or those born to mothers who were positive for HBsAg, despite hepatitis B immunoglobulin being administered at birth [14]. OBI may become overt after several years [15]. It has been reported that OBI is associated with the development of HCC [16,17].
Prior to the advent of immunization against HBV, around 17.2 % of the adult population LongAn, a county in Guangxi, China, were carriers of HBsAg [18]. LongAn hosts one of the five clinical trials of hepatitis B immunization in China and, between 1986 and 1996, all newborn infants in these trials were vaccinated according to a 0-, 1-, and 6-month schedule using a 10 μg dose of plasma-derived HBV vaccine, regardless of the mother’s HBV infection status [19]. Our surveillance ten years ago revealed that the HBsAg and anti-HBc positivity rates in LongAn county had increased, 22–28 years after immunization. Anti-HBs positivity and geometric mean concentration of antibody decreased significantly in the years after vaccination [20]. We also found later that a few individuals vaccinated at birth had become persistently infected with HBV [21]. Has the prevalence of HBsAg in this vaccinated cohort increased since then? Here, we report our surveillance data.
2. Materials and Methods
2.1. Study Population
As mentioned above, LongAn hosts one of the five clinical trials of hepatitis B immunization in China. In order to evaluate the efficacy of vaccination, a serial study has been carried out in LongAn county since the early 1990s. The candidate study subjects for this study were those who born between 1987 and 1993 and vaccinated at birth with three doses of HepB vaccine, and who came for our evaluation at least once in the last ten years and provided serum samples. Doctors from local town hospitals and village clinics dispensed notice to all candidate study subjects. Those subjects who are willing to attend our visit became be our study subjects. Each study subject completed a one-page questionnaire at that visit and provided a 3 mL sample of blood by venepuncture for testing for serological markers of HBV and HBV DNA.
Informed consent in writing was obtained from each individual. The study protocol conforms to the ethical guidelines of the 1975 Helsinki Declaration and has been approved by the Guangxi Institutional Review Board.
2.2. Qualitative Assays of HBV Serological Markers
Sera were tested for HBV serological markers (including hepatitis B surface antigen (HBsAg), hepatitis B surface antibody (anti-HBs), hepatitis B e antigen (HBeAg)), antibodies to the hepatitis B e antigen (anti-HBe), and antibodies to the hepatitis B core antigen (anti-HBc), using enzyme immunoassays (WANTAI BioPharm, Beijing, China). Quality control for the measurements was performed in accordance with the protocols provided by the manufacturer.
2.3. Quantitative Assays of Anti-HBs and HBsAg
Serum anti-HBs and HBsAg concentrations were quantified by the Maccura i6000, using HBsAg and HBsAb Quantitative Kits (Maccura Biotechnology Co., Ltd, Chendu, China). The Maccura i6000 is a fully automated chemiluminescence immunoassay (CLIA) system designed for high-throughput testing in clinical laboratories. According to protocols provided by the manufacturer, positive and negative cutoffs were calculated with the positive and negative controls as required by the diagnostic kits. The dynamic range of the kit for HBsAg is 0.05 IU/mL~250 IU/mL. The dynamic range of the kit for anti-HBs is 4 mIU/mL~1000 mIU/mL.
2.4. Measurement of Serum Viral Loads
Serum HBV DNA concentrations were quantified by real-time polymerase chain reaction (PCR) using commercial reagents (Sansure Biotech Inc., Hunan, China) in an ABI Prism 7500sequence detection system (Applied Biosystems, Foster City, CA, California, USA), with a dynamic range of 30 -5×109 IU/mL. To avoid the effect of cross-contamination on the results, negative and blank controls were included in each assay. The positive test result was repeated three times.
To confirm OBI, HBV genomic DNA was extracted from 200 μL of serum samples using QIAamp DNA Mini kits (QIAGEN GmbH, Hilden, Germany) and eluted in 50 μL of distilled water. To amplify the pre-S, polymerase and X regions, first round PCR was carried out in a 50 μL reaction using primers LSOB1 (nt 2739-2762, 5′-GGCATTATTTGCATACCCTTTGG-3′) and MDN5R (nt1794-1774, 5′-ATTTATGCCTACAGCCTCCT-3′) with 5 min hot start followed by 30 cycles of 94°C for 30 s, 50°C for 30 s and 72°C for 90 s. Second round PCR was carried out on 5 μL of the first round products in a 50 μL reaction using primers LSBI1 (nt 2809–2829, 5′-TTGTGGGTC ACCATATTCTT-3′) and XSEQ1R (nt1547–1569, 5′-CAGATGAGAAGGCACAGACGGGG-3′), with the same amplification protocol as the first round. Products from the second round were confirmed by agarose gel electrophoresis
2.5. Statistical Methods
Categorical data were evaluated by χ2 or Fisher’s exact tests, depending on the absolute numbers included in the analysis, and quantitative data were analyzed by the independent sample t test or Mann-Whitney U test. HBV DNA concentrations were set at 30 IU/mL for those with undetectable values. All P values were 2-tailed, and P <0.05 was considered to be significant. All statistical analyses were performed using the SPSS software (ver.16.0; Chicago, IL, USA).
3. Results
3.1. General Characteristics of the Study Subjects
The 637 subjects in the study were recruited from the Long An cohort, including 503 males and 134 females. The average age was 34.0 ± 2.0 (Mean ± SD) years. The average ages of the males and females were 34.0 ± 2.0 and 34.0±1.9, respectively. The total prevalence of HBsAg was 3.9% ((95% CI (confidence interval): 2.4-5.4)). The prevalence of HBsAg in females (8.2%) was significantly higher than that in males (2.8%) (p=0.004). The total prevalence of anti-HBc was 43.3% (95% CI: 39.7-47.3). The prevalence of HBc in females (46.3%) was also significantly higher than that in males (41.7%) (p=0.021). The total prevalence of anti-HBs was 42.7% (95% CI: 38.9-46.5). However, there is no significantly different in its prevalence between males (41.7%) and females (46.3%) (p=0.347). Clearly, the prevalence of HBsAg corresponds to the prevalence of anti-HBc (Table 1).
3.2. Trend in the Prevalence of HBsAg and the Positive Rates and Levels of Anti-HBs, According to Age
The highest prevalence of HBsAg in males (3.6%) was seen in the age group of 36 while that in females (18.8%) was in the age group of 30. The prevalence of HBsAg varies with age and it can be seen that the prevalence of HBsAg increase with age in males but not in females (Figure 1).
The highest prevalence of anti-HBs positivity in males (52.5%) was seen in the age group of 36 while that in females (68.8%) was in the age group of 30. The prevalence of anti-HBs positivity varies with age and it can also be seen that the prevalence of anti-HBs positive increases with age in males but not in females. The levels of anti-HBs corresponded to the positive rates of anti-HBs in males but not in females (Figure 2). These data suggested that using the positive rate or titer of anti-HBs to determine the protection period of HepB vaccination may not helpful.
3.3. Trend in the Prevalence of Anti-HBc According to Age
The highest prevalence of anti-HBc in males (51.8%) was seen in the age group of 36 while that in females (68.8%) was in the age group of 30. The prevalence of anti-HBc varies with age. However, no trend was seen in either males or females (Figure 3).
3.4. Characteristics of Subjects Positive for HBeAg
We found 17 subjects to be positive for HBeAg but negative for HBsAg. Eleven of them were positive for anti-HBs. In order to determine whether these subjects were OBI, we tested for HBV DNA using qPCR. It was surprising that only one of them was positive for HBV DNA, with a low viral load of 80 IU/ml. Clearly, only one of these subjects was OBI (Table 2).
3.5. Comparison of the Prevalence of HBsAg, Anti-HBs and Anti-HBc from the Same Subject, Previously and Currently (2024)
Among 637 subjects, the HBsAg status (positive or negative) of 98.9% (95%CI: 98.1-99.7) subjects remains unchanged. One subject alone became positive for HBsAg, while 6 subjects underwent seroconversion of HBsAg from positive to negative. The difference between the rate of becoming positive for HBsAg and the rate of seroconversion of HBsAg from positive to negative was not significant (p=0.070). It was noted that one of the 6 subjects was positive for HBsAg in 2009, 2017 and 2019 and another was positive for HBsAg in 2017, 2019 and 2020. Clearly, the positivity rate of HBsAg had not increased (Table 3).
Most of the subjects (90.4%, 95% CI: 88.1-92.7) maintained their anti-HBs status. The percentage of those who became negative for anti-HBs (5.5%) was significantly higher than that of those who became positive for anti-HBs (4.1%) (p=0.049), suggesting that the rate of anti-HBs positivity is decreasing with age (Table 3).
The anti-HBc status of 71.3% (67.8-74.8) subjects of the 637 subjects remains unchanged. However, the percentage of subjects who became anti-HBc positive (24.6%) was significantly higher than that of those who became anti-HBc negative (4.1%) (p=0.001), suggesting that the positivity rate of anti-HBc is increasing with age (Table 3).
3.6. Comparison of Occult Infection Between Subjects Recruited in 2017 and 2024
We tested for HBV DNA in 282 subjects from 2024 and 129 subjects from 2017, respectively. The total prevalence of OBI in 2017 and 2024 were 1.6% (95% CI: -0.6-3.8) and 6.0% (3.2-8.8), respectively. The difference in the prevalence of OBI between 2017 and 2024 is significant (p=0.045), suggesting that the prevalence of OBI in those vaccinated at birth is increasing with age.
It is noted that 84.2% (95% CI: 67.8-100.6) of OBI occurred in those who were anti-HBc positive, more than half of them (9/16) were positive for anti-HBs and some had high levels of anti-HBs, suggesting that anti-HBs may not prevent occult HBV (Table 4 and Table 5).
Viral loads in the subjects with OBI were low, except for one subject whose viral load was 4.1 x104 IU/ml. The viral loads of 89.5% (17/19) subjects were less than 103 IU/ml.
4. Discussion
To our knowledge, this is the first study comparing long-term efficacy of vaccination against hepatitis B in the same individuals at different time points. The major findings are that the prevalence of OBI is increasing with age. The rate of anti-HBc positivity is increasing with age and the rate of anti-HBs positivity is decreasing with age. The positivity rate of HBsAg had not increased. The prevalence of anti-HBc positivity corresponds to that of both HBsAg and OBI. Using the positive rate or titer of anti-HBs to determine the protection period of HepB vaccination may not helpful. Anti-HBs may not prevent occult HBV. A strength of this study is that comparing the long-term efficacy of vaccination in the same person at different time points may avoid sampling bias and yield reliable results. A weakness of the study is that there are fewer females than males because we failed to contact them, which may prevent stratification analysis. According to custom in Long An county, female must move to live with her husband in other village or town or county, which resulted in losing contact details.
There have been many studies evaluating the long-term efficacy of HepB vaccination. They found that the titer or levels of anti-HBs decrease with ages[22,23,24] . The longest period of protection by HepB vaccination is 35 years[25]. In this study, we found that the prevalence of HBsAg did not increase significantly, compared to that in 2015, although the prevalence of anti-HBc doubled[20] , suggesting that the protection period of HepB vaccination was at least 37 years.
It has been reported that, despite HepB vaccination and passive protection with hepatitis B immunoglobulin (HBIG), OBI is common in children and adolescents in high-risk groups [12,26]. This may occur in anti-HBs-positive young adults after neonatal HepB vaccination[27] . It was more common in those born to HBsAg-positive mothers [28,29]. However, these are all cross-sectional studies and could not determine whether the prevalence of occult infection increases or decreases. In this study, we are the first to show that the prevalence of OBI in those vaccinated at birth increased significantly, compared to data from the same subjects in 2015.
The factors involved in the development of OBI, despite vaccination and prophylaxis with HBIG, remain obscure. One potential factor is the presence of mutations in the region of the HBV genome encoding the surface protein, these may lead to failure to detect of HBsAg and apparent HBsAg negativity [30]. However, we reported previously that five of six subjects with OBI did not have unusual amino acid substitutions in or around the major antigenic region of HBsAg (the “a” determinant) [31]. Pollicino et al. did not find any relevant pre-S deletion mutations in their occult HBV isolates and found that these isolates could replicate normally and produce HBsAg. They proposed that host, rather than viral, factors are responsible for OBI [32]. A potential host factor is the gut microbiota, which may contribute to the immune response leading to suppressed virus replication and the development of occult hepatitis B[33].
Occult HBV can be transmitted and develop as an overt infection [15,34] . It has been implicated in the development of chronic liver diseases, including cirrhosis and HCC [17,35]. It may also reactivate in the face of immunosuppression, even leading to the development of fulminant hepatitis [36]. We previously reported that the prevalence of OBI in those without vaccination in LongAn county was 11.5% [31]. Although the prevalence of OBI among adults against hepatitis B at birth is lower than 11.5%, it is increasing with age, raising a new issue how to prevent and control OBI in the post-universal infant vaccination era.
Anti-HBc develops during acute HBV infection and may be maintained life-long. Thus, the serological status of anti-HBc alone is compatible with resolved acute infection, as well as overt or occult chronic HBV infection [37]. Studies from high prevalence areas confirm the potential for waning immunity to allow breakthrough infections to occur. Although chronic HBV infections after vaccination are rare, the prevalence of anti-HBc has been seen to increase with time [8]. In this study, we found that OBI occurred most frequently in subjects who were anti-HBc positive, especially those with anti-HBc alone. We also found that the prevalence of anti-HBc is increasing. Therefore, the risk of occult HBV should no longer be neglected in vaccinated populations.
Clinically, HBeAg is an indicator of viral replication and infectivity, inflammation and the severity of disease, and the response to antiviral therapy. Seroconversion from HBeAg-positivity to an HBeAg-negative or anti-HBeAg-positive phase usually heralds the resolution of infection [38]. Although, in general, HBeAg positivity correlates with a high serum level of HBV DNA, it has been reported that low levels HBeAg and HBV DNA are not always in proportion, although very high levels of HBeAg often are correlated with high levels of HBV DNA [39]. In this study, 16 subjects who were HBsAg negative but positive for HBeAg, were found to be negative for HBV DNA. Are the levels of HBV DNA in these subjects below the limit of detection?An overall 97-100% rate of anti-HBs development at ≥10 mIU/mL could be achieved in those with a full course of primary HepB vaccination [5]. Over time, anti-HBs concentrations decline in vaccinated individuals, becoming undetectable in some [8]. However, the vaccinees with anti-HBs <10 mIU/mL or undetectable remain have a brisk anamnestic immune response to HBsAg [5,8]. In this study, we found 4.1% of subjects were negative for anti-HBs in 2017 but positive in 2024. These subjects deny having received a booster. We postulate that they may have been exposed to wild-type virus. Therefore, using the titer of anti-HBs to determine the protection period of HepB vaccination may not helpful.
In this study, we found that two subjects with OBI in 2015 and maintained occult infection in 2024. This is not in correspondence with the data from Lai’s group [40]. We also found that 15 subjects were negative for HBV DNA in 2015 but had developed OBI by 2024. Because we did not test their family members, such as their spouses, parents, brothers and sisters for HBV, the sources of their infections remain unclear. Furthermore, we did not determine the sequences of the S gene of the virus and cannot determine whether mutants are responsible for their occult infection.
In conclusion, the prevalence of OBI is increasing with age in individuals vaccinated against hepatitis B at birth. The prevalence of anti-HBc positivity corresponds to that of OBI. Neonatal HBV vaccination maintained effective protection at least 37 years in terms of the positivity rate of HBsAg and anti-HBs.
Author Contributions
Conceptualization: Fang ZL, Zhong G, Harrison TJ, Black A. Data curation: Jiang ZH, Wang XY, Chen QY. Formal analysis: Jiang ZH, Wang XY, Huang ML. Investigation: Jiang ZH, Wang XY, Chen QY, Zhang LJ, Hu LP, Huang ML, Huang YB, Hu X and Zhang WW. Methodology: Zhong G, Jiang ZH, Wang XY. Supervision: Zhong G, Fang ZL. Writing- original draft: Fang ZL. Writing-review & editing: Zhong G, Fang ZL, Harrison TJ, Black A.
Funding
This study was supported by the National Natural Science Foundation of China (Grant No. 81860595) and Guangxi Key Research and Development Project (Grant No. 2018AB59002).
Institutional Review Board Statement
The study protocol conforms to the ethical guidelines of the 1975 Helsinki Declaration and has been approved by the Guangxi Institutional Review Board.
Informed Consent Statement
Informed consent in writing was obtained from each individual.
Data Availability Statement
The data presented in this study are available within the article.
Acknowledgments
We are indebted to staff members of Long An People’s Hospital and local town hospitals in Long An county, Guangxi, who assisted in recruiting the study subjects, sample collection.
Conflicts of Interest
The authors declare that they have no conflict of interest relevant to this study.
References
- Boora S.; Sharma V.; Kaushik S.; Bhupatiraju AV.; Singh S.; Kaushik S. Hepatitis B virus-induced hepatocellular carcinoma: a persistent global problem. Braz J Microbiol. 2023, 54, 679–689. [CrossRef]
- Patel A.; Dossaji Z.; Gupta K.; Roma K.; Chandler T-M.; Minacapelli CD.; Catalano K.; Gish R.; Rustgi V. The Epidemiology, Transmission, Genotypes, Replication, Serologic and Nucleic Acid Testing, Immunotolerance, and Reactivation of Hepatitis B Virus. Gastro Hep Adv. 2023, 3, 139–150. [CrossRef]
- Hepatitis B Fact Sheet. http://www.who.int/mediacentre/factsheets/fs204/en/.2021,.
- Hsu Y-C.; Huang DQ.; Nguyen MH. Global burden of hepatitis B virus: current status, missed opportunities and a call for action. Nat Rev Gastroenterol Hepatol. 2023, 20, 524–537. [CrossRef]
- Zhao H.; Zhou X.; Zhou Y-H. Hepatitis B vaccine development and implementation. Hum Vaccin Immunother. 2020, 16, 1533–1544. [CrossRef]
- Davis JP. Experience with hepatitis A and B vaccines. Am J Med. 2005, 118 Suppl 10A, 7S-15S. [CrossRef]
- Centers for Disease Control and Prevention (CDC). Implementation of newborn hepatitis B vaccination--worldwide, 2006. MMWR Morb Mortal Wkly Rep. 2008, 57, 1249–1252.
- Scheifele DW. Will Infant Hepatitis B Immunization Protect Adults? Pediatr Infect Dis J. 2019, 38, S64–S66. [CrossRef]
- Boccalini S.; Bonito B.; Zanella B.; Liedl D.; Bonanni P.; Bechini A. The First 30 Years of the Universal Hepatitis-B Vaccination-Program in Italy: A Health Strategy with a Relevant and Favorable Economic-Profile. Int J Environ Res Public Health. 2022, 19, 16365. [CrossRef]
- Liu Y.; Liu L. Changes in the Epidemiology of Hepatocellular Carcinoma in Asia. Cancers (Basel). 2022, 14, 4473. [CrossRef]
- Phattraprayoon N.; Kakheaw J.; Soonklang K.; Cheirsilpa K.; Ungtrakul T.; Auewarakul C.; Mahanonda N. Duration of Hepatitis B Vaccine-Induced Protection among Medical Students and Healthcare Workers following Primary Vaccination in Infancy and Rate of Immunity Decline. Vaccines (Basel). 2022, 10, 267. [CrossRef]
- Wu J.; He J.; Xu H. Global prevalence of occult HBV infection in children and adolescents: A systematic review and meta-analysis. Ann Hepatol. 2024, 29, 101158. [CrossRef]
- Hsu H-Y.; Chang M-H.; Ni Y-H.; Chiang C-L.; Wu J-F.; Chen H-L.; Chen P-J.; Chen D-S. Chronologic changes in serum hepatitis B virus DNA, genotypes, surface antigen mutants and reverse transcriptase mutants during 25-year nationwide immunization in Taiwan. J Viral Hepat. 2017, 24, 645–653. [CrossRef]
- Zhou S.; Li T.; Allain J-P.; Zhou B.; Zhang Y.; Zhong M.; Fu Y.; Li C. Low occurrence of HBsAg but high frequency of transient occult HBV infection in vaccinated and HBIG-administered infants born to HBsAg positive mothers. J Med Virol. 2017, 89, 2130–2137. [CrossRef]
- Eilard A.; Andersson M.; Ringlander J.; Wejstål R.; Norkrans G.; Lindh M. Vertically acquired occult hepatitis B virus infection may become overt after several years. J Infect. 2019, 78, 226–231. [CrossRef]
- Mak L-Y.; Wong DK-H.; Pollicino T.; Raimondo G.; Hollinger FB.; Yuen M-F. Occult hepatitis B infection and hepatocellular carcinoma: Epidemiology, virology, hepatocarcinogenesis and clinical significance. J Hepatol. 2020, 73, 952–964. [CrossRef]
- Xia R.; Peng J.; He J.; Jiang P.; Yuan C.; Liu X.; Yao Y. The Serious Challenge of Occult Hepatitis B Virus Infection-Related Hepatocellular Carcinoma in China. Front Microbiol. 2022, 13, 840825. [CrossRef]
- Ding ZR. Distribution of viral hepatitis B infection in Guangsi Province. Zhonghua Liu Xing Bing Xue Za Zhi. 1982, 3, 84–87.
- Wang F.; Shen L.; Cui F.; Zhang S.; Zheng H.; Zhang Y.; Liang X.; Wang F.; Bi S. The long-term efficacy, 13-23 years, of a plasma-derived hepatitis B vaccine in highly endemic areas in China. Vaccine. 2015, 33, 2704–2709. [CrossRef]
- Li H.; Li GJ.; Chen QY.; Fang ZL.; Wang XY.; Tan C.; Yang QL.; Wang FZ.; Wang F.; Zhang S.; et al. Long-term effectiveness of plasma-derived hepatitis B vaccine 22-28 years after immunization in a hepatitis B virus endemic rural area: is an adult booster dose needed? Epidemiol Infect. 2017, 145, 887–894. [CrossRef]
- Wang X.; Chen Q.; Li H.; Wang C.; Hu L.; Yang Q.; Ren C.; Liu H.; Zheng Z.; Harrison TJ.; et al. Asymptomatic hepatitis B carriers who were vaccinated at birth. J Med Virol. 2019, 91, 1489–1498. [CrossRef]
- Asamoah Sakyi S.; Badu Gyapong J.; Krampah Aidoo E.; Effah A.; Koffie S.; Simon Olympio Mensah O.; Arddey I.; Boakye G.; Opoku S.; Amoani B.; et al. Evaluation of Immune Characteristics and Factors Associated with Immune Response following Hepatitis B Vaccination among Ghanaian Adolescents. Adv Virol. 2024, 2024, 9502939. [CrossRef]
- Miao N.; Zheng H.; Sun X.; Zhang G.; Wang F. Protective effect of vaccinating infants with a 5 µg recombinant yeast-derived hepatitis B vaccine and the need for a booster dose in China. Sci Rep. 2020, 10, 18155. [CrossRef]
- Bianchi FP.; Gallone MS.; Gallone MF.; Larocca AMV.; Vimercati L.; Quarto M.; Tafuri S. HBV seroprevalence after 25 years of universal mass vaccination and management of non-responders to the anti-Hepatitis B vaccine: An Italian study among medical students. J Viral Hepat. 2019, 26, 136–144. [CrossRef]
- Bruce MG.; Bruden D.; Hurlburt D.; Morris J.; Bressler S.; Thompson G.; Lecy D.; Rudolph K.; Bulkow L.; Hennessy T.; et al. Protection and antibody levels 35 years after primary series with hepatitis B vaccine and response to a booster dose. Hepatology. 2022, 76, 1180–1189. [CrossRef]
- Wang R.; Liu C.; Chen T.; Wang Y.; Fan C.; Lu L.; Lu F.; Qu C. Neonatal hepatitis B vaccination protects mature adults from occult virus infection. Hepatol Int. 2021, 15, 328–337. [CrossRef]
- Xu L.; Wei Y.; Chen T.; Lu J.; Zhu C-L.; Ni Z.; Huang F.; Du J.; Sun Z.; Qu C. Occult HBV infection in anti-HBs-positive young adults after neonatal HB vaccination. Vaccine. 2010, 28, 5986–5992. [CrossRef]
- Lu Y.; Liu Y-L.; Nie J-J.; Liang X-F.; Yan L.; Wang F-Z.; Zhai X-J.; Liu J-X.; Zhu F-C.; Chang Z-J.; et al. Occult HBV Infection in Immunized Neonates Born to HBsAg-Positive Mothers: A Prospective and Follow-Up Study. PLoS One. 2016, 11, e0166317. [CrossRef]
- Foaud H.; Maklad S.; Mahmoud F.; El-Karaksy H. Occult hepatitis B virus infection in children born to HBsAg-positive mothers after neonatal passive-active immunoprophylaxis. Infection. 2015, 43, 307–314. [CrossRef]
- Pondé RAA. Molecular mechanisms underlying HBsAg negativity in occult HBV infection. Eur J Clin Microbiol Infect Dis. 2015, 34, 1709–1731. [CrossRef]
- Fang Z-L.; Zhuang H.; Wang X-Y.; Ge X-M.; Harrison T-J. Hepatitis B virus genotypes, phylogeny and occult infection in a region with a high incidence of hepatocellular carcinoma in China. World J Gastroenterol. 2004, 10, 3264–3268. [CrossRef]
- Pollicino T.; Raffa G.; Costantino L.; Lisa A.; Campello C.; Squadrito G.; Levrero M.; Raimondo G. Molecular and functional analysis of occult hepatitis B virus isolates from patients with hepatocellular carcinoma. Hepatology. 2007, 45, 277–285. [CrossRef]
- Liu B.; Yang H.; Liao Q.; Wang M.; Huang J.; Xu R.; Shan Z.; Zhong H.; Li T.; Li C.; et al. Altered gut microbiota is associated with the formation of occult hepatitis B virus infection. Microbiol Spectr. 2024, 12, e0023924. [CrossRef]
- Hu L-P.; Liu D-P.; Chen Q-Y.; Harrison TJ.; He X.; Wang X-Y.; Li H.; Tan C.; Yang Q-L.; Li K-W.; et al. Occult HBV Infection May Be Transmitted through Close Contact and Manifest as an Overt Infection. PLoS One. 2015, 10, e0138552. [CrossRef]
- Yip TC-F.; Wong GL-H. Current Knowledge of Occult Hepatitis B Infection and Clinical Implications. Semin Liver Dis. 2019, 39, 249–260. [CrossRef]
- Gerlich WH.; Bremer C.; Saniewski M.; Schüttler CG.; Wend UC.; Willems WR.; Glebe D. Occult hepatitis B virus infection: detection and significance. Dig Dis. 2010, 28, 116–125. [CrossRef]
- Wang Q.; Klenerman P.; Semmo N. Significance of anti-HBc alone serological status in clinical practice. Lancet Gastroenterol Hepatol. 2017, 2, 123–134. [CrossRef]
- Kramvis A. The clinical implications of hepatitis B virus genotypes and HBeAg in pediatrics. Rev Med Virol. 2016, 26, 285–303. [CrossRef]
- Chen P.; Xie Q.; Lu X.; Yu C.; Xu K.; Ruan B.; Cao H.; Gao H.; Li L. Serum HBeAg and HBV DNA levels are not always proportional and only high levels of HBeAg most likely correlate with high levels of HBV DNA: A community-based study. Medicine (Baltimore). 2017, 96, e7766. [CrossRef]
- Lai M-W.; Chang Y-L.; Cheng P-J.; Chueh H-Y.; Chang S-C.; Yeh C-T. Absence of chronicity in infants born to immunized mothers with occult HBV infection in Taiwan. J Hepatol. 2022, 77, 63–70. [CrossRef]
Figure 1.
Trend in the prevalence of HBsAg according to age.
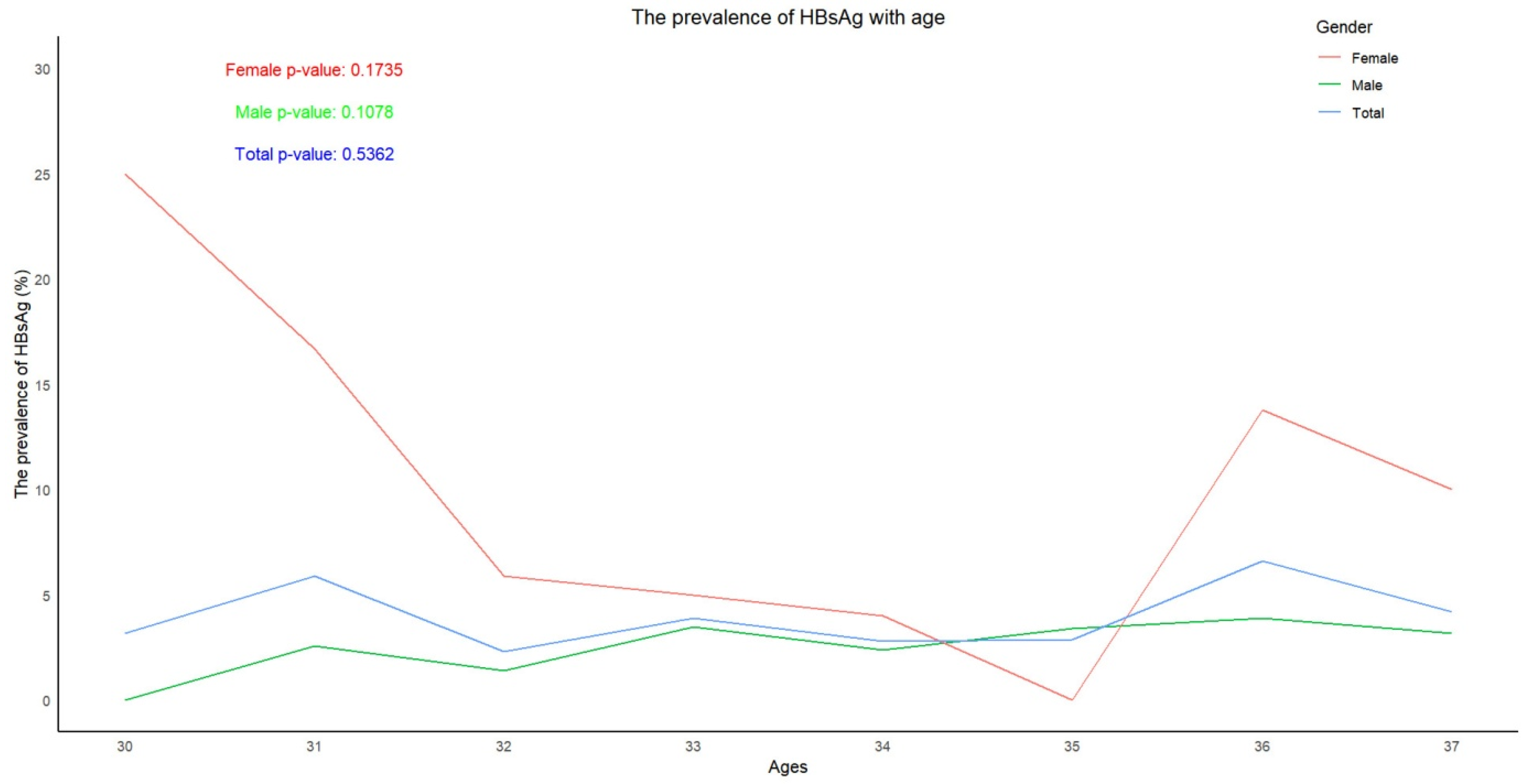
Figure 2.
Trend in the positive rates and levels of anti-HBs according to age. (A) Trend in the positive rates according to age. (B) Trend in the levels of anti-HBs according to age.
Figure 2.
Trend in the positive rates and levels of anti-HBs according to age. (A) Trend in the positive rates according to age. (B) Trend in the levels of anti-HBs according to age.
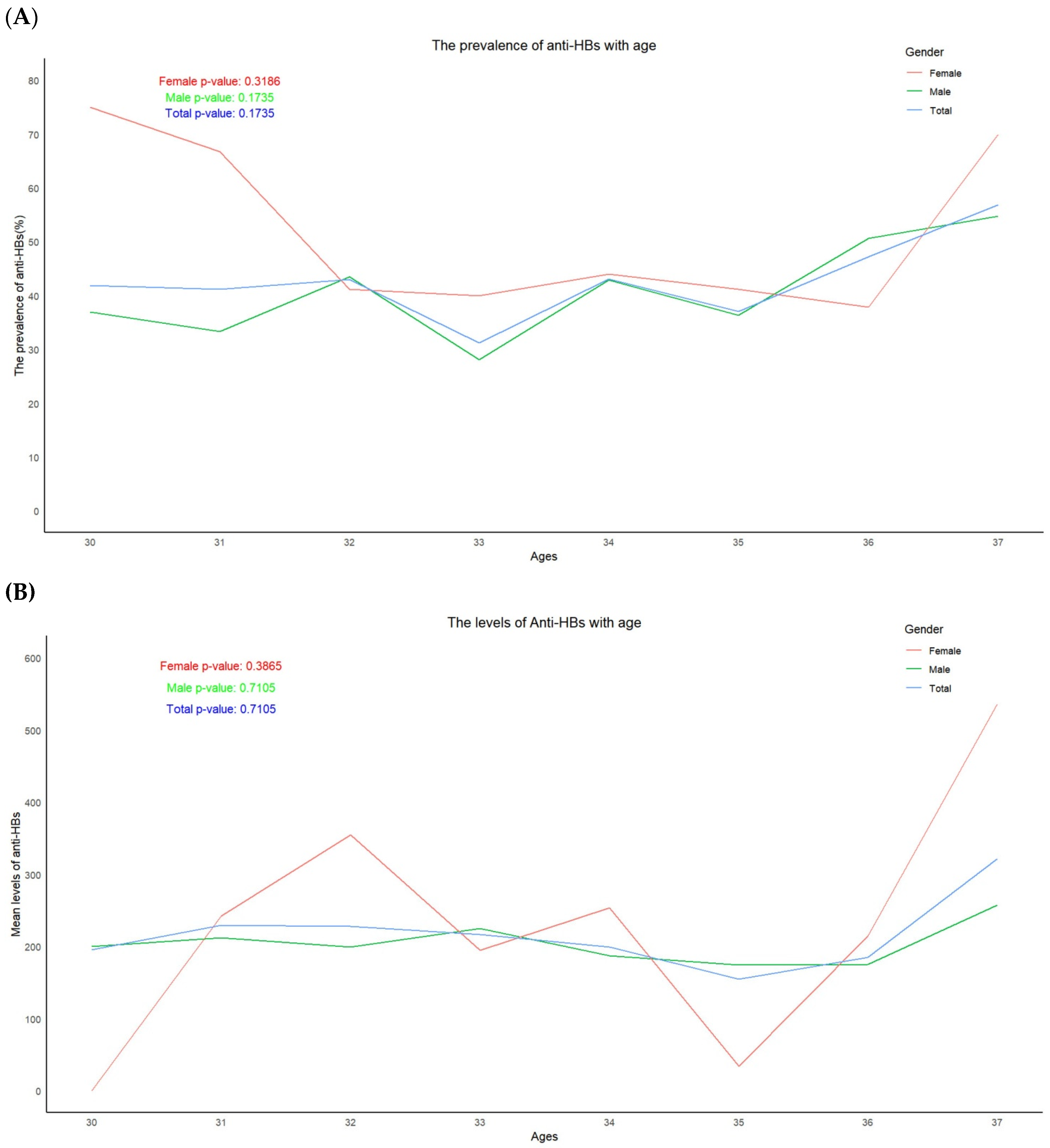
Figure 3.
Trend in the prevalence of anti-HBc according to age.
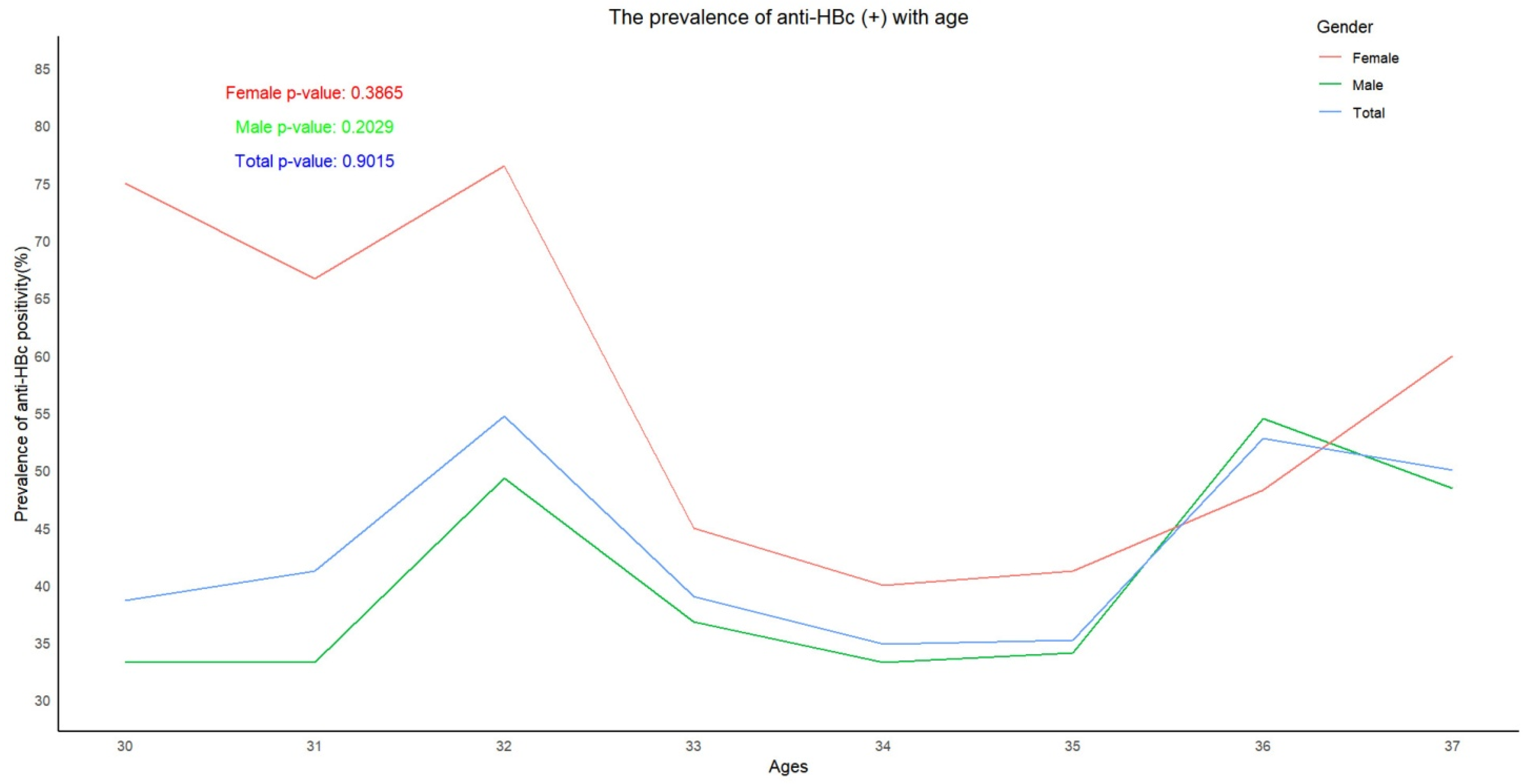

Table 1.
The prevalence of serological markers of HBV in 2024.
| Groups | Males | Females | Total | ||||||
| No | Positive | Rate (%) (95% CI△) |
No | Positive | Rate (%) (95% CI) |
No | Positive | Rate (%) (95% CI) |
|
| HBsAg | 503 | 14 | 2.8 (1.5-4.1) |
134 | 11 | 8.2 (6.1-10.3) |
637 | 25 | 3.9 (2.4-5.4) |
| Anti-HBs | 503 | 210 | 41.7 (37.9-45.5) |
134 | 62 | 46.3 (42.4-50.2) |
637 | 272 | 42.7 (38.9-46.5) |
| Anti-HBc | 503 | 207 | 41.2 (36.9-45.5) |
134 | 70 | 52.2 (43.7-60.7) |
637 | 277 | 43.5 (39.7-47.3) |
| Levels of Anti-HBs | Mean*± SD# | Mean ±SD | Mean ±SD | ||||||
| 200.9±323.2§ | 266.8±353.2 | 215.5±330.4 | |||||||
#SD: standard deviation. △CI: Confidence interval. §: IU/ml.
Table 2.
Characteristics of subjects positive for HBeAg in 2024.
| Codes | Gender | Ages | HBsAg | anti-HBs | HBeAg | anti-HBe | anti-HBc | Viral loads |
| AWL120 | M* | 33 | - | 16.428 | + | - | - | Undetectable |
| AWB133 | F# | 32 | - | - | + | - | - | Undetectable |
| ATZ196 | M | 33 | - | - | + | - | - | Undetectable |
| ATX297 | M | 34 | - | 334.995 | + | - | + | Undetectable |
| ATX289 | M | 35 | - | - | + | - | - | Undetectable |
| ATX261 | F | 33 | - | - | + | - | - | Undetectable |
| ATW230 | M | 34 | - | 190.843 | + | - | - | Undetectable |
| ATT524 | M | 37 | - | >1000.000§ | + | - | - | Undetectable |
| ATM174 | M | 33 | - | >1000.000 | + | - | + | Undetectable |
| ATL181 | M | 31 | - | - | + | - | - | 80.009△ |
| ATL143 | M | 31 | - | 78.288 | + | - | + | Undetectable |
| ATF074 | M | 32 | - | 98.957 | + | - | + | Undetectable |
| AQT182 | M | 35 | - | >1000.000 | + | - | - | Undetectable |
| APP045 | M | 35 | - | - | + | - | - | Undetectable |
| ACS020 | M | 31 | - | 482.039 | + | - | - | Undetectable |
| 09LA1043 | M | 34 | - | 35.529 | + | - | + | Undetectable |
| 09LA0167 | M | 34 | - | >1000.000 | + | - | - | Undetectable |
*Males. #Females. §IU/ml. △IU/ml.
Table 3.
Changes of the prevalence of HBsAg, anti-HBs and anti-HBc in individuals, up to 2024.
| Marker | No | Status (positive or negative) unchanged | Became positive | Became negative | |||
| No | Rate (%) (95% CI*) |
No | Rate (%) (95% CI) |
No | Rate (%) (95% CI) |
||
| HBsAg | 637 | 630 | 98.9 (98.1-99.7) |
1 | 0.2 (-0.1-0.5) |
6 | 0.9 (0.1-1.6) |
| Anti-HBs | 637 | 576 | 90.4 (88.1-92.7) |
26 | 4.1 (2.6-5.6) |
35 | 5.5 (3.7-7.3) |
| Anti-HBc | 637 | 454 | 71.3 (67.8-74.8) |
157 | 24.6 (21.3-27.9) |
26 | 4.1 (2.6-5.6) |
*CI: Confidence interval.
Table 4.
Comparison of occult infection rates between subjects recruited in 2017 and 2024.
| Groups | No | Positive | Rate (%) | 95% CI* |
| 2024 | ||||
| Negative for all serological markers | 62 | 1 | 1.6 | -1.5-4.7 |
| anti-HBc(+) only | 89 | 7 | 7.9 | 2.3-13.5 |
| anti-HBc(+) with anti-HBs(+) or anti-HBe(+) or HBeAg(+) |
104 | 7 | 6.7 | 1.9-11.5 |
| anti-HBc(-) with anti-HBs(+) or anti-HBe(+) or HBeAg(+) |
27 | 2 | 7.4 | -2.5-17.3 |
| Total | 282 | 17 | 6.0 | 3.2-8.8 |
| 2015 | ||||
| Negative for all serological markers | 53 | 1 | 1.9 | -1.8-5.6 |
| anti-HBc(+) only | 38 | 0 | 0 | 0 |
| anti-HBs(+), anti-HBc(+) | 29 | 1 | 3.4 | -3.2-10.0 |
| Total | 129 | 2 | 1.6 | -0.6-3.8 |
*CI: Confidence interval.
Table 5.
Characteristics of subjects with occult infection.
| Code | Gender | Ages | HBsAg | anti-HBs | HBeAg | anti-HBe | anti-HBc |
HBV DNA (IU/ml) |
| 09LA1051 | M△ | 34 | - | 248.835§ | - | - | + | 157.965§ |
| 09LA1073 | F# | 32 | - | - | - | - | + | 102.424 |
| 09LA3607 | M | 34 | - | - | - | - | + | 253.2 |
| ADH140* | F | 33 | - | - | - | - | - | 41192.4 |
| ADH140 | F | 33 | - | - | - | - | - | 267.372 |
| ADJ006 | F | 36 | - | 243.483 | - | - | + | 1842.646 |
| ADJ102 | M | 32 | - | - | - | - | + | 223.013 |
| ADK129 | M | 37 | - | 435.870 | - | + | + | 49.213 |
| ADK130 | M | 37 | - | - | - | + | - | 447.401 |
| AGM067 | F | 33 | - | - | - | - | + | 180.14 |
| AGM098 | M | 35 | - | - | - | - | + | 307.819 |
| AGM212 | M | 36 | - | 337.604 | - | - | + | 436.139 |
| AGZ078 | M | 36 | - | - | - | - | + | 108.223 |
| ATJ035 | M | 32 | - | 944.213 | - | - | + | 263.29 |
| ATL181 | M | 31 | - | - | + | - | - | 80.009 |
| ATW293 | M | 36 | - | - | - | - | + | 695.963 |
| ATW295* | M | 32 | - | + | - | - | + | 96.331 |
| ATW295 | M | 33 | - | 269.656 | - | - | + | 212.238 |
| ATZ238 | M | 37 | - | 595.325 | - | - | + | 65.842 |
*Samples collected in 2017. △Male. #Female. §IU/ml.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



