
Submitted:
14 December 2024
Posted:
16 December 2024
You are already at the latest version
Abstract
Introduction: Infantile fibrosarcoma is a malignant tumor of fibroblastic origin, typical in early childhood, locally aggressive, and characterized by molecular alterations that activate tyrosine kinase signaling, primarily the ETV6::NTRK3 fusion. In recent years, a series of fusions different from the classic one have been described, including NTRK1, RAF1, and BRAF. In this paper, we present a case of IFS with a novel EVI5::BRAF fusion. Methods: We received a humeral surgical resection specimen. After macroscopic carving, tumor samples were collected, processed, and stained with hematoxylin-eosin. Various immunohistochemical and molecular techniques were applied to sections of the non-decalcified tumor. Results: We observed a spindle cell neoplasm growing in intertwined fascicles within a fibrous stroma, without the formation of immature osteoid matrix. Weak and focal immunoreactivity for S100 was observed. SATB2 exhibited diffuse and intense staining, with focal expression of osteonectin and negativity for caldesmon, smooth muscle actin, desmin, GFAP, SOX10, MelanA, panTRK, and HMB45. The Ki67 index was 7%, and the tumor harbored an EVI5::BRAF genetic fusion. Conclusions: To the best of our knowledge, the EVI5::BRAF fusion has not yet been described in BRAF fusions in IFS. Nevertheless, further studies are needed to define the prognostic features of these emerging BRAF sarcomas.
Keywords:
Infantile intraosseous fibrosarcoma
; BRAF translocation
; EVI5::BRAF fusion
Introduction
Pediatric mesenchymal tumors encompass a heterogeneous group of benign and malignant pathologies, both de novo (90%) and associated with hereditary syndromes (10%). Soft tissue sarcomas are more common in children than in adults, with an incidence that increases with age, from 0.9 cases per-100,000 person-years in children under 10 years old to 18.2 cases per 100,000 person-years. In children under 15 years old, the most common sarcoma is rhabdomyosarcoma (95-97% of cases), while the remaining 3-5% includes both low-grade tumors (rarely metastatic or locally aggressive) and high-grade tumors [1].
This group includes both typical pediatric sarcomas as well as other “adult-type” sarcomas that can appear in childhood. One of the typical pediatric tumors, infantile fibrosarcoma (IFS), is a malignant tumor of fibroblastic origin, typical in early childhood, locally very aggressive, characterized by molecular alterations that activate tyrosine kinase signaling, primarily the ETV6::NTRK3 fusion. Despite its local aggressiveness, metastases are infrequent (8-15%), and the 10-year survival rate is 90% with surgical and chemotherapeutic treatment. Local recurrence occurs in 25-40% of cases with affected margins. These tumors exhibit a poorly characteristic immunohistochemical profile, with variable expression of CD34, S100, smooth muscle actin, and desmin. PanTRK may be positive in cases where mutations are present [1].
In recent years, a series of IFS with fusions different from the classic one have been described, involving other tyrosine kinase genes, including NTRK1, NTRK2, RET, MET, and RAF1 [1]. Among these new fusions is BRAF, a gene that encodes proteins from the RAF family of protein kinases that regulate the MAP kinase/ERK signaling pathway. This pathway promotes cell proliferation and survival, and its activation induces tumorigenesis [2]. Although BRAF has functions typically associated with carcinomas, its role as an inducer of mesenchymal neoplasms has also been described. These neoplasms characteristically present a “spindle cell” or “epitheloid” pattern and are NTRK-negative [2]. This group not only includes IFS but also mandibular and central nervous system sarcomas [4,5].
Treatment consists of surgery and chemotherapy. Despite being locally aggressive, metastasis is rare (10%), and the 10-year survival rate exceeds 90%. The most relevant factor for recurrences (which occur in 25-40% of cases) is resection with clear margins, which is why surgery is often aggressive. Given that NTRK fusion is common, tyrosine kinase inhibitors are currently being studied as a future therapeutic option [1].
In this paper, we present a case of IFS with a novel EVI5::BRAF fusion, and discuss its clinical, histological, immunohistochemical, and molecular features.
Case Presentation
Clinical and Radiological Findings
A 14-year-old male experienced intense pain in his left arm after a sudden movement while descending a slide at a water park. He sought emergency care and was diagnosed with a pathological fracture of the left humerus. The patient denied any prior symptoms before the accident. An arm sling was applied by orthopedics, and 20 days later, he returned for a follow-up MRI.
The MRI revealed a pathological fracture of the proximal humerus with angulation, located over a poorly defined lytic lesion in the proximal diaphysis, measuring approximately 17x72 mm. There was a cystic area of 13 mm in its proximal portion, cortical erosion, and intense contrast uptake. The findings suggested a differential diagnosis of fibrous dysplasia (FD), aneurysmal bone cyst (ABC), Ewing sarcoma (ES), and osteosarcoma (OS). Additionally, there was edema and contrast uptake in the adjacent musculature, which could be secondary to inflammatory changes due to the fracture, although infiltration could not be ruled out (Figure 1). Given these findings, the patient was referred to our center and was admitted for further evaluation.
A core needle biopsy (CNB) was performed. Three cores were obtained, with a diagnosis of "low-grade sarcoma." A thoracoabdominal-pelvic CT scan was performed, showing no signs of distant metastasis. After discussion in the sarcoma committee, a decision was made to proceed with radical surgery, including resection and reconstruction with a vascularized fibula graft. Medical Oncology determined that there was no indication for neoadjuvant chemotherapy (NCT) or radiotherapy (NCRT).
During surgery, 13 cm of the humerus were resected along with the coracobrachialis muscle and parts of the deltoid and brachialis anterior muscles. Intraoperative samples were sent to Pathology Department, confirming free margins. The humerus was reconstructed using a free osteocutaneous fibula flap from the right leg (intramedullary in the proximal humerus and trench technique in the distal humerus). After the surgery, the patient has been discharged without complications, with no indication for adjuvant therapy from Medical Oncology.
Macroscopic Findings
The resection specimen of the humerus measured 14 x 5.4 x 4.6 cm. After staining the margins and sectioning the specimen, a poorly defined yellowish lesion measuring 4.7 x 2.3 cm was observed within the medullary cavity, expanding into the surrounding soft tissues. The lesion was located 2.6 cm from the proximal margin, 1.7 cm from the distal margin, and 1 cm from the circumferential margin, all of which were macroscopically free of the lesion (Figure 2).
Microscopic Findings
The lesion exhibited a "fish spine" pattern in the medullary cavity, composed of atypical cells with moderate pleomorphism and medium to large size. These cells were arranged in long, highly intertwined fascicles, breaking through the cortical bone and extending into the soft tissues (Figure 3A, 3B). The nuclei were oval to elongated, hyperchromatic, granular with nuclear pseudo-inclusions, and the cytoplasm was elongated and eosinophilic (Figure 3C). An inflammatory component, predominantly mononuclear and plasmacytic, was observed between the tumor fascicles and around the blood vessels. There were 5 mitoses in 10 high-power fields (Figure 3D). No bone trabeculae, osteoid formation, or areas of necrosis were present within the lesion.
Based on the histological findings and the results of the previous biopsy, the diagnosis was oriented towards IFS. However, other diagnoses based on age, appearance and location such as low-grade osteosarcoma (LGO), inflammatory myofibroblastic tumor (IMT), malignant peripheral nerve sheath tumor (MPNST), or melanoma were also considered. Taking into account these differential diagnoses, microscopic findings and immunohistochemical stainings were crucial, in addition to next-generation sequencing (NGS).
Immunohistochemical Findings
Weak and focal immunoreactivity was observed for S100. SATB2 expressed a diffuse and intense staining, with focal expression of osteonectin and negativity for caldesmon, smooth muscle actin, desmin, GFAP, SOX10, MelanA, panTRK and HMB45. H3K27me3 was not valuable, and the Ki67 index was 7% (Figure 4 and Table 1). According to the Fédération Nationale des Centres de Lutte Contre le Cancer (FNLCC) criteria [9], the score was 4, corresponding to a G2 grade (Dedifferentiation 3/3, mitosis 1/3, and necrosis 0/2). Table 1 includes the antibodies used for diagnosis.
Fluorescence In Situ Hybridisation (FISH) and Next Generation Sequencing (NGS) Results
Given the suspicion of pediatric fibrosarcoma and the negativity for panTRK, fluorescence in situ hybridisation (FISH) was performed for BRAF gene, revealing an EVI5::BRAF fusion. This rearrangement was later studied by Next Generation Sequencing (Fig. 5), confirming the fusion.
Discussion
Among the BRAF fusions described in IFS are SEPT7::BRAF, SEPT9::BRAF, SEPT11::BRAF, ERC1::BRAF, PDE10A::BRAF, CUX1::BRAF and KIAA1549::BRAF [2,6,7,8]. Kao et al [7], in his series of infantile fibrosarcomas, describes 5 cases with BRAF fusions in patients of varying ages (from 2 days to 16 years), with 3 tumors located in the pelvis, 1 in the T6 vertebra, and another in the retroperitoneum. The tumors exhibited a 'spindle cell' morphology with few mitoses and patchy and focal expression for SMA, with an absence of expression for desmin and S100. It is important to note that these tumors are not associated with upregulation of BRAF mRNA, so immunohistochemistry of BRAF is not reliable .
EVI5 (Ecotropic Viral Integration Site 5) is a gene that enables GTPase activator activity and small GTPase binding activity, involved in the positive regulation of GTPase activity and retrograde transport from the endosome to the Golgi. It functions as a regulator of cell cycle progression by stabilizing the FBXO5 protein and promoting cyclin-A accumulation during interphase [10].EVI5 was discovered by X. Liao et al. in 1995 and defined as a common site of retroviral integration in T-cell lymphomas in mice. Since then, it has been described as a regulatory gene involved in both proliferation and metastasis in tumors such as non-small cell lung carcinoma and hepatocellular carcinoma as well as in neuroblastoma, where the chromosomal translocation may influence its origin. [14]. The EVI5::BRAF fusion has been only described in congenital melanocytic nevi [15].
Kao et al. describes that these tumors appear in unusual clinical settings, such as older age groups or intra-abdominal locations, unlike classic IFS, which is more common in the early years of life and in the extremities. Despite this, they present a similar prognosis, making it complex to determine whether they correspond to variants of IFS or distinct entities. The case reports published in recent years refer to the entity as “IFS-like with BRAF fusions”. However, in the latest classification of pediatric tumors by the WHO (2022), these tumors are considered as IFS, and BRAF fusions are included alongside the classic NTRK ones [1].
It is important to note that, although the tumor expressed both SATB2 and osteonectin, the diagnosis of LGS has been ruled out due to the cytomorphological features, lack of osteoid matrix and the absence of MDM2 amplification. All these findings have supported the IFS diagnosis considering SATB2 and osteonectin expression as an unspecific staining. Additionally, the diagnosis of IMT has been ruled out due to the aggressive local behavior of the lesion and the absence of ALK immunexpression and traslocation. IFS can also present with a prominent lymphoid inflammatory component [1].
To the best of our knowledge, EVI5::BRAF has not been described in BRAF fusions in IFS yet, making this case the first in the literature. Nevertheless, further studies are needed to define the prognostic features of these emergent BRAF sarcomas.
Author Contributions
The authors declare no conflict of interest.
Funding
This research received no funding.
References
- WHO Classification of Tumours Editorial Board. Paediatric tumours [Internet]. Lyon (France): International Agency for Research on Cancer; 2022 [cited 2024 august 15]. (WHO classification of tumours series, 5th ed.; vol. 7). Available from: https://tumourclassification.iarc.who.int/chapters/44.
- Abualola RA, Al-Zaid T. KIAA1549-BRAF Gene Fusion Spindle Cell Sarcoma With Infantile Fibrosarcoma-Like Pattern in a Pediatric Patient: A Case Report. Cureus. 2024 Jan 9;16(1):e51981. [CrossRef] [PubMed] [PubMed Central]
- Zhou P, Liu W, Zheng J, Zhang H, Luo J. Case report: Primary sarcoma of the mandible with a novel SLMAP-BRAF fusion. Front Oncol. 2024 Mar 28;14:1369046. [CrossRef] [PubMed] [PubMed Central]
- Cecchi R, Guptil D, Haslett N, Hristov A, Bledsoe JR, Tsai H, DeWitt J, Ferris SP. Primary CNS histiocytic sarcoma: Two case reports highlighting a novel MIGA2::BRAF gene fusion and genome-wide DNA methylation profiling results. J Neuropathol Exp Neurol. 2024 Jun 14:nlae061. [CrossRef] [PubMed]
- Zhang L, Zhang G, Zheng H, Jiang B, Ju Y, Duan Q, An L, Shi H. A rare case of primary central nervous system histiocytic sarcoma harboring a novel ARHGAP45::BRAF fusion: a case report and literature review. Brain Tumor Pathol. 2024 Jan;41(1):18-29. [CrossRef] [PubMed]
- Hughes CE, Correa H, Benedetti DJ, Smith B, Sumegi J, Bridge J. Second Report of PDE10A-BRAF Fusion in Pediatric Spindle Cell Sarcoma With Infantile Fibrosarcoma-Like Morphology Suggesting PDE10A-BRAF Fusion Is a Recurrent Event. Pediatr Dev Pathol. 2021 Nov-Dec;24(6):554-558. [CrossRef] [PubMed] [PubMed Central]
- Kao YC, Fletcher CDM, Alaggio R, Wexler L, Zhang L, Sung YS, Orhan D, Chang WC, Swanson D, Dickson BC, Antonescu CR. Recurrent BRAF Gene Fusions in a Subset of Pediatric Spindle Cell Sarcomas: Expanding the Genetic Spectrum of Tumors With Overlapping Features With Infantile Fibrosarcoma. Am J Surg Pathol. 2018 Jan;42(1):28-38. [CrossRef] [PubMed] [PubMed Central]
- Gourmel A, Rouette A, Benlimame N, El-Jalbout R, Dubé M, Théorêt Y, Piché N, Labonté S, Sinnett D, Cellot S, Dal-Soglio D, Larouche V, Tran TH. Durable Response to Trametinib in an Infant With ERC1-BRAF Infantile Fibrosarcoma-Like Tumor: A Case Report and Literature Review of BRAF-Altered Infantile Fibrosarcoma-Like Tumors. JCO Precis Oncol. 2022 Aug;6:e2200200. [CrossRef] [PubMed]
- Hettler M, Kitz J, Seif Amir Hosseini A, Guhlich M, Panahi B, Ernst J, Conradi LC, Ghadimi M, Ströbel P, Jakob J. Comparing Apparent Diffusion Coefficient and FNCLCC Grading to Improve Pretreatment Grading of Soft Tissue Sarcoma-A Translational Feasibility Study on Fusion Imaging. Cancers (Basel). 2022 Sep 5;14(17):4331. [CrossRef] [PubMed] [PubMed Central]
- The GeneCards Suite: From Gene Data Mining to Disease Genome Sequence Analyses ( Citations: 3,306) Stelzer G, Rosen R, Plaschkes I, Zimmerman S, Twik M, Fishilevich S, Iny Stein T, Nudel R, Lieder I, Mazor Y, Kaplan S, Dahary, D, Warshawsky D, Guan - Golan Y, Kohn A, Rappaport N, Safran M, and Lancet D, Current Protocols in Bioinformatics(2016), 54:1.30.1 - 1.30.33.doi: 10.1002 / cpbi.5 [PDF]. [PubMed]
- Liao X, Buchberg AM, Jenkins NA, Copeland NG. Evi-5, a common site of retroviral integration in AKXD T-cell lymphomas, maps near Gfi-1 on mouse chromosome 5. J Virol. 1995 Nov;69(11):7132-7. [CrossRef] [PubMed]
- Cai, T. , Zhou, J., Zeng, Y. et al. EVI5 is an oncogene that regulates the proliferation and metastasis of NSCLC cells. J Exp Clin Cancer Res 39, 84 (2020). [CrossRef]
- Tang J, Ou J, Xu C, Yi C, Xue F, Xu L, Lai F, Tang J, Li S, Kang T, Ding W, Wang B. EVI5 is a novel independent prognostic predictor in hepatocellular carcinoma after radical hepatectomy. Oncol Rep. 2017 Oct;38(4):2251-2258. [CrossRef] [PubMed]
- Vandepoele K, Andries V, van Roy F. The NBPF1 promoter has been recruited from the unrelated EVI5 gene before simian radiation. Mol Biol Evol. 2009 Jun;26(6):1321-32. [CrossRef] [PubMed]
- Sara Barberan Martin, Satyamaanasa Polubothu, Alicia Lopez Bruzos, Gavin Kelly, Stuart Horswell, Aimie Sauvadet, Dale Bryant, Davide Zecchin, Melissa Riachi, Fanourios Michailidis, Amir Sadri, Noreen Muwanga-Nanyonjo, Pablo Lopez-Balboa, Nicole Knöpfel, Neil Bulstrode, Alan Pittman, Iwei Yeh, Veronica A. Kinsler. Mosaic BRAF Fusions Are a Recurrent Cause of Congenital Melanocytic Nevi Targetable by MAPK Pathway Inhibition. Journal of Investigative Dermatology, Volume 144, Issue 3, 2024, Pages 593-600. [CrossRef]
Figure 1.
a) CT findings: Sagital reconstruction showing diaphyseal lytic lesion with cortical erosion, causing bone remodelation. b) MRI findings: Post contrast transverse T1 sequence showing surrounding soft tissue mass with homogeneous and intense contrast uptake.
Figure 1.
a) CT findings: Sagital reconstruction showing diaphyseal lytic lesion with cortical erosion, causing bone remodelation. b) MRI findings: Post contrast transverse T1 sequence showing surrounding soft tissue mass with homogeneous and intense contrast uptake.

Figure 2.
Macroscopic findings. A poorly defined yellowish lesion measuring 4.7 x 2.3 cm was observed within the medullary cavity, expanding into the surrounding soft tissues.
Figure 2.
Macroscopic findings. A poorly defined yellowish lesion measuring 4.7 x 2.3 cm was observed within the medullary cavity, expanding into the surrounding soft tissues.
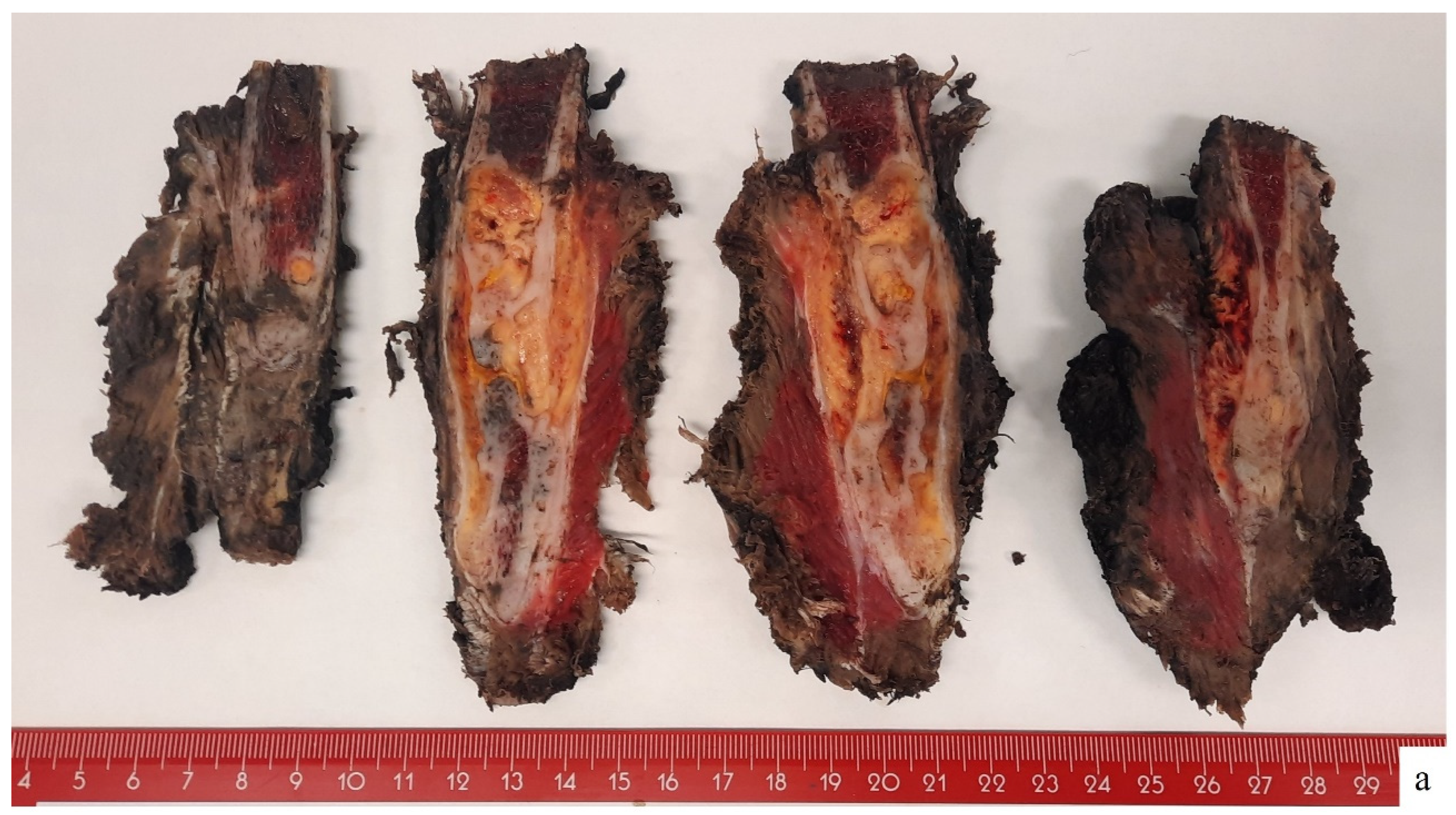
Figure 3.
Microscopy findings. a) The lesion occupied the medullary cavity, breaking through the cortex and extending into the surrounding soft tissues (HE; 4X). b) Diffuse 'herringbone' pattern (HE; 10X). c) Elongated and interwoven fascicles composed of atypical cells with moderate pleomorphism and medium size, with hyperchromatic nuclei and poorly defined cytoplasm. (HE;20X). d) Isolated mitoses were observed, with a notable lymphoid inflammatory component. No osteoid formation, or areas of necrosis were present within the lesion. (HE, 40X).
Figure 3.
Microscopy findings. a) The lesion occupied the medullary cavity, breaking through the cortex and extending into the surrounding soft tissues (HE; 4X). b) Diffuse 'herringbone' pattern (HE; 10X). c) Elongated and interwoven fascicles composed of atypical cells with moderate pleomorphism and medium size, with hyperchromatic nuclei and poorly defined cytoplasm. (HE;20X). d) Isolated mitoses were observed, with a notable lymphoid inflammatory component. No osteoid formation, or areas of necrosis were present within the lesion. (HE, 40X).
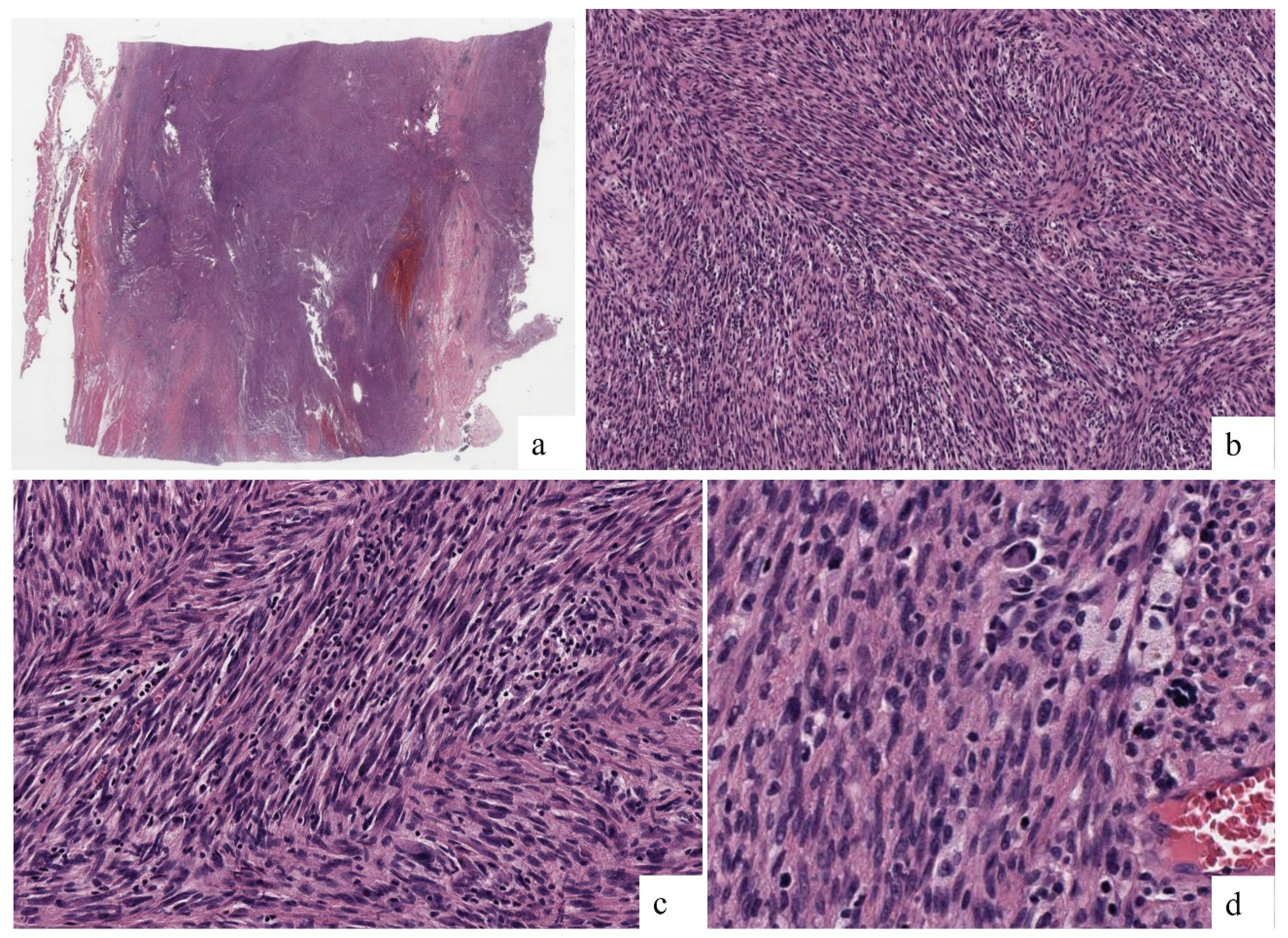
Figure 4.
Immunohistochemical findings. a) Diffuse positivity for SATB2 (20X). b) Weak and focal positivity for osteonectin (20X). c) Absence of expression for smooth muscle actin (20X). d) Ki67 index was established in 7% (20X).
Figure 4.
Immunohistochemical findings. a) Diffuse positivity for SATB2 (20X). b) Weak and focal positivity for osteonectin (20X). c) Absence of expression for smooth muscle actin (20X). d) Ki67 index was established in 7% (20X).
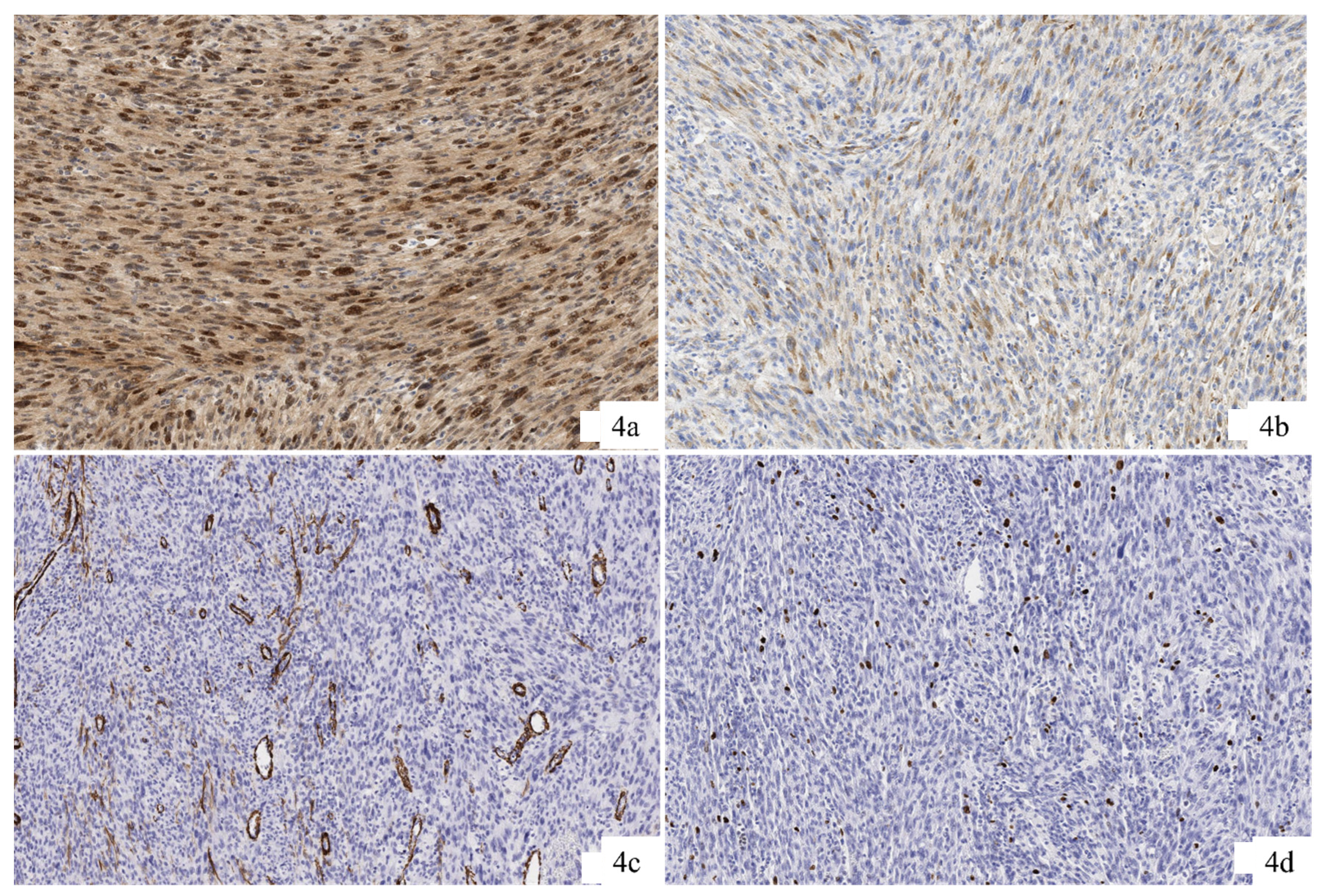
Figure 5.
FISH and NGS results. a) FISH shows EVI5::BRAF fusion. b) NGS shows the fusion point between the two genes.
Figure 5.
FISH and NGS results. a) FISH shows EVI5::BRAF fusion. b) NGS shows the fusion point between the two genes.
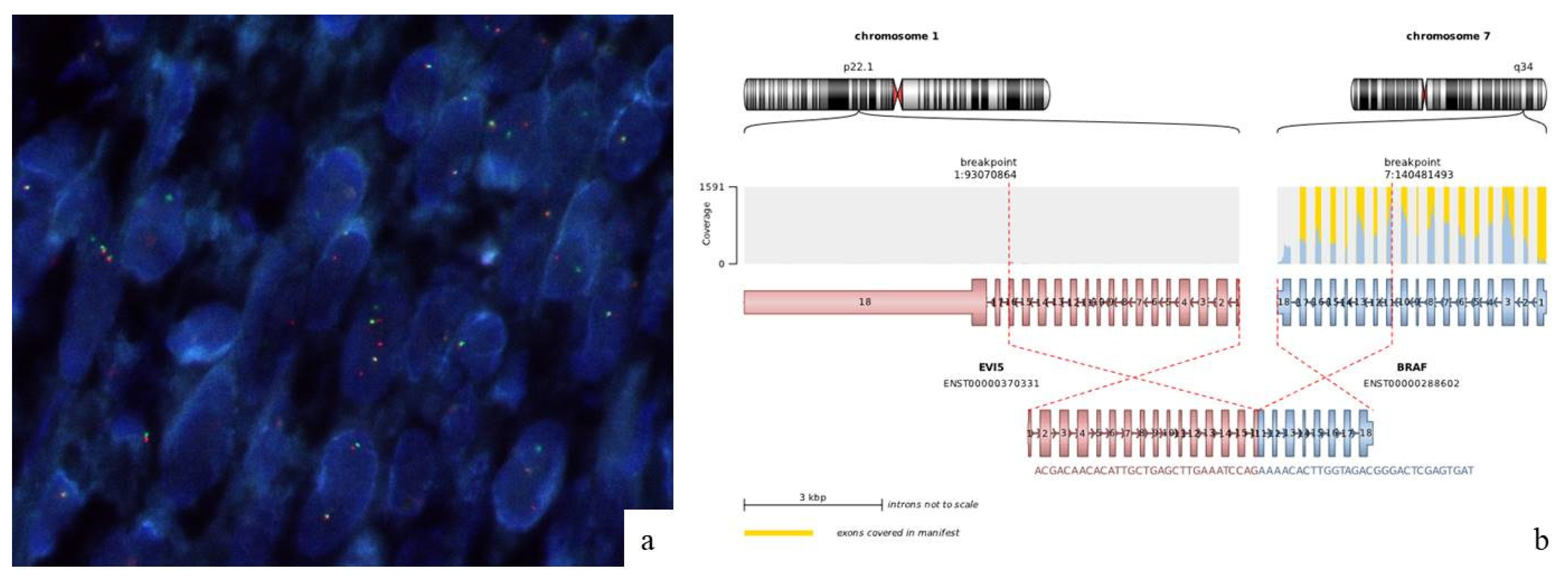

Table 1.
Main used antibodies and staining pattern.
| Antibody | Source | Clone | Staining pattern |
|---|---|---|---|
| S100 | Dako | Polyclonal | Diffuse (Nuclear) |
| SATB2 | Zeta | ZR167 | Diffuse (Nuclear) |
| Caldesmon | Dako | h_CD | Negative |
| Smooth Muscle Actin | Dako | HHF-35 | Negative |
| Desmin | Dako | D33 | Negative |
| Osteonectin | Leica | G-15-G12 | Focal (Cytoplasmic) |
| GFAP | Dako | Polyclonal | Negative |
| SOX10 | Biocare | BC34 | Negative |
| MelanA | Dako | A103 | Negative |
| HMB45 | Dako | HMB-45 | Negative |
| H3K27me3 | Gennova/Biocare | C36B11 | Not evaluable |
| Ki67 | Dako | MIB-1 | 7% |
| ALK | Dako | ALK1 | Negative |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



