
Submitted:
12 December 2024
Posted:
13 December 2024
You are already at the latest version
Abstract
Psychoactive substance use, encompassing both legal (tobacco, alcohol) and illicit drugs (cocaine, methamphetamines, cannabis), poses a significant and escalating threat to global cardiovascular health. This comprehensive review explores the multifaceted impact of these substances on cardiovascular diseases (CVDs), which remain the leading cause of mortality worldwide. Through an analysis of recent literature, the review elucidates the pathophysiological mechanisms—including oxidative stress, systemic inflammation, autonomic dysregulation, and endothelial dysfunction—that mediate the cardiovascular toxicity of these substances. Acute and chronic cardiovascular risks are highlighted, encompassing myocardial infarction, arrhythmias, hypertension, cardiomyopathy, and cerebrovascular events. Particular attention is given to vulnerable populations, such as younger users and individuals with pre-existing CVDs, emphasizing the compounded risks associated with prolonged substance exposure. Additionally, the review identifies gaps in current research, especially regarding the chronic cardiovascular effects and optimal long-term management strategies for substance-induced CVDs. Evidence-based recommendations for prevention, diagnosis, and management are proposed, aiming to inform clinical practice and public health policies. By integrating pathophysiological insights with clinical evidence, this review seeks to advance understanding of substance-related cardiovascular risks and promote the development of targeted interventions to mitigate this growing global health challenge.
Keywords:
Psychoactive drugs
; Cardiovascular risk
; Oxidative stress
; Endothelial dysfunction
; Sub-stance-induced cardiovascular diseases
1. Introduction
Cocaine use, for instance, is strongly associated with acute coronary syndromes, arrhythmias, and chronic risks such as cardiomyopathy and heart failure [6]. Similarly, methamphetamine consumption is linked to severe hypertension, arrhythmias, and sudden cardiac death, driven by massive catecholamine release and chronic vascular damage [5].
In addition to stimulants, opioids and cannabis have demonstrated a significant relationship with adverse cardiovascular outcomes. Opioids, widely used in chronic pain management, are associated with bradycardia, hypotension, and increased risk of infective endocarditis in intravenous drug users [7,8]. These effects are mediated by interactions with mu-opioid receptors (MOR), modulating inflammatory and oxidative stress pathways, contributing to endothelial damage and arterial stiffness [8,9]. Cannabis, often perceived as a low-risk substance, significantly increases the risk of myocardial infarction and arrhythmias, particularly in individuals with pre-existing cardiovascular conditions [10,11,12,13].
Despite their legality, tobacco and alcohol remain primary contributors to the global burden of CVD. Nicotine, the addictive component of tobacco, exerts its deleterious effects through nicotinic acetylcholine receptor activation, promoting vasoconstriction, oxidative stress, and endothelial dysfunction [14,15]. Chronic exposure to tobacco exacerbates atherosclerosis, coronary artery disease, and cerebrovascular events [16]. Furthermore, exposure to secondhand smoke significantly heightens cardiovascular risk by impairing endothelial function and increasing platelet aggregation [14,17].
Alcohol consumption presents a complex relationship with cardiovascular health [18]. While moderate intake (1–2 drinks per day) may confer cardioprotective effects, such as increasing HDL cholesterol and reducing fibrinogen levels [19], excessive consumption is associated with cardiomyopathy, hypertension, and higher risks of hemorrhagic stroke [20,21]. Recent findings indicate that alcohol consumption exacerbates vascular inflammation and oxidative stress, further amplifying CVD risk in susceptible individuals [22].
Psychotropic medications, including antidepressants and antipsychotics, have drawn significant attention due to their cardiovascular side effects. Piña et al. highlight that tricyclic antidepressants (TCAs) and selective serotonin reuptake inhibitors (SSRIs) prolong the QT interval, thereby increasing the risk of life-threatening arrhythmias such as torsades de pointes [23]. Furthermore, atypical antipsychotics are closely associated with metabolic syndrome, a cluster of cardiovascular risk factors including hypertension, insulin resistance, and dyslipidemia, which substantially elevate the risk of coronary artery disease and stroke [24].
Pathophysiological Mechanisms of Drug-Induced Cardiovascular Damage
At the molecular level, cardiovascular damage induced by psychoactive substances involves sympathetic overstimulation, oxidative stress, and inflammation. Stimulants such as cocaine and methamphetamines act as sympathomimetic agents, activating adrenergic receptors and promoting vasoconstriction and ischemic injury [3]. Conversely, opioids suppress autonomic activity, leading to bradycardia and hypotension, particularly in overdose scenarios [8]. Substances like nicotine and cannabis disrupt vascular homeostasis through receptor activation, impairing autonomic regulation [11,25].
Oxidative stress and inflammation play pivotal roles in the pathogenesis of drug-induced cardiovascular damage. Chronic exposure to substances like tobacco and methamphetamines generates reactive oxygen species (ROS), which impair endothelial integrity and accelerate aterosclerosis [2,26]. Elevated levels of inflammatory markers such as C-reactive protein (CRP) are associated with increased cardiovascular risk, as observed in psychotropic medication users [23]. These findings highlight the intricate interplay of biological pathways underlying cardiovascular damage and emphasize the urgent need for targeted interventions.
Justification of the Study
Despite the growing body of evidence linking the use of legal and illicit substances to significant cardiovascular risks, there remain critical gaps in understanding the underlying mechanisms and long-term implications. Much of the existing research has adopted an observational approach, which limits the ability to establish robust causal relationships between substance use and cardiovascular events. Additionally, many studies have predominantly focused on acute effects, leaving a considerable gap in knowledge regarding chronic impacts and optimal strategies for long-term clinical management [2,27].
This review is particularly relevant given the increasing prevalence of drug use among younger populations, who are at risk of experiencing an accumulated burden of cardiovascular diseases over time. This phenomenon poses not only a public health challenge but also a global threat to well-being, further exacerbating the already alarming prevalence of cardiovascular diseases [28].
This review uniquely integrates and analyzes the cardiovascular effects of multiple psychoactive substances within a single conceptual framework, addressing gaps in the literature that often focus on individual substances, such as tobacco or alcohol. It explores under-researched mechanisms, including the interplay between oxidative stress and endothelial dysfunction in users of emerging substances like cannabis and e-cigarettes, while highlighting underrepresented populations, such as women and younger individuals. Furthermore, this work advances knowledge by synthesizing recent findings on inflammatory biomarkers and autonomic stress associated with these substances, offering a comprehensive perspective on both acute and chronic cardiovascular risks. Additionally, it identifies critical gaps in public policy and prevention strategies, particularly regarding misconceptions of “safety” associated with certain substances, emphasizing the urgent need for targeted interventions. Therefore, a review of this scope is imperative—not only to comprehensively evaluate the mechanisms and clinical studies available but also to identify critical gaps in the current literature. Such an effort will advance scientific understanding and inform improved prevention and treatment strategies. The specific objectives of this review are:
- To explore the pathophysiological mechanisms underlying drug-induced cardiovascular damage, with a focus on autonomic regulation, oxidative stress, and inflammatory pathways.
- To review the existing clinical evidence, including randomized controlled trials and meta-analyses, to assess the cardiovascular impact of substance use invulnerable populations such as young individuals and those with pre-existing cardiovascular comorbidities.
- To propose clinical and public health strategies for the prevention, diagnosis, and management of substance-related cardiovascular diseases, addressing risks associated with both legal and illicit drugs.
- To identify critical gaps in current research and suggest future directions, with particular attention to the chronic cardiovascular effects of prolonged substance use.
By synthesizing and analyzing the available evidence, this review aims to provide clinicians, researchers, and policymakers with a comprehensive understanding of the cardiovascular risks associated with substance use. This effort will support the development of more effective interventions to reduce the global burden of cardiovascular diseases attributable to substance use.
Research Objectives and PICO Questions
The central aim of this review is to analyze the impact of legal and illicit drug use on cardiovascular health, employing a framework based on the PICO model (Population, Intervention, Comparison, Outcome).
- Impact of illicit drugs on cardiovascular health: What are the effects of illicit drug use, such as cocaine, methamphetamines, and cannabis, on the incidence of severe cardiovascular events (e.g., myocardial infarction, arrhythmias, ¿heart failure) compared to non-users?
- Cardiovascular effects of legal substance use (tobacco and alcohol): How does chronic use of legal substances like tobacco and alcohol influence the development of cardiovascular diseases (e.g., hypertension, atherosclerosis, arrhythmias) compared to non-users?
- Pathophysiological mechanisms of drug-induced cardiovascular damage: What pathophysiological mechanisms—such as autonomic dysfunction, oxidative stress, inflammation, ¿and endothelial damage—are implicated in drug-induced cardiovascular damage?
- Cardiovascular risks of novel psychoactive substances: How do the risks of acute cardiovascular events, such as hypertension, arrhythmias, and cardiac diseases, ¿among users of novel psychoactive substances compare to those of traditional drug users?
Through this systematic approach, the review seeks not only to elucidate the relationships between substance use and cardiovascular outcomes but also to lay the groundwork for future research and more precise, effective intervention strategies.
2. Materials and Methods
This narrative review was conducted following the Preferred Information Elements for Systematic Reviews and Meta-Analyses (PRISMA) statement (Figure 1).
The literature search will be performed using medical header terms (MeSH) in WOS and PubMed and other relevant search engines, employing Boolean operators to identify relevant studies. The strategy is designed to obtain high-quality evidence that addresses the cardiovascular impact of psychoactive substances.
Search Strategy
A review was carried out in the PubMed and WOS (Without the term [MeSH Terms]) databases using the PICO structure, the extraction of the keywords was carried out, thus forming various combinations in English vocabulary with the respective use of Boolean operators such as the following search terms:
Clinical Trail: ((((“drugs”[Title/Abstract] AND (“addiction”[Title/Abstract] OR “abuse”[Title/Abstract] OR “dependence”[Title/Abstract] OR “consumption”[Title/Abstract] OR “use”[Title/Abstract])) OR (“alcohol”[Title/Abstract] AND (“drinking”[Title/Abstract] OR “consumption”[Title/Abstract] OR “abuse”[Title/Abstract])) OR ((“amphetamine”[Title/Abstract] OR “cocaine”[Title/Abstract] OR “heroin”[Title/Abstract] OR “marijuana”[Title/Abstract] OR “opium”[Title/Abstract] OR “psychotropic drugs”[Title/Abstract] OR “tobacco”[Title/Abstract] OR “smoking”[Title/Abstract] OR “smoke”[Title/Abstract] OR “smokers”[Title/Abstract]) AND (“addiction”[Title/Abstract] OR “abuse”[Title/Abstract] OR “dependence”[Title/Abstract] OR “consumption”[Title/Abstract] OR “use”[Title/Abstract]))) AND “2019/12/05 00:00”:”3000/01/01 05:00”[Date - Publication] AND ((“heart arrest”[Title/Abstract] OR “heart failure”[Title/Abstract] OR “heart aneurysm”[Title/Abstract] OR “arrhythmia”[Title/Abstract] OR “heart disease”[Title/Abstract] OR “vascular disease”[Title/Abstract] OR “cardiovascular disease”[Title/Abstract]) AND “2019/12/05 00:00”:”3000/01/01 05:00”[Date - Publication]) AND “2019/12/05 00:00”:”3000/01/01 05:00”[Date - Publication]) OR ((“substance related disorders/adverse effects”[MeSH Terms] OR “illicit drugs/adverse effects”[MeSH Terms] OR “designer drugs/adverse effects”[MeSH Terms] OR “synthetic drugs/adverse effects”[MeSH Terms] OR “amphetamine related disorders”[MeSH Terms] OR “amphetamines/adverse effects”[MeSH Terms] OR “alcoholism/complications”[MeSH Terms] OR “alcohol related disorders”[MeSH Terms] OR “alcohol induced disorders”[MeSH Terms] OR “cardiomyopathy, alcoholic”[MeSH Terms] OR “alcohol drinking/adverse effects”[MeSH Terms] OR “smoking/adverse effects”[MeSH Terms] OR “pipe smoking/adverse effects”[MeSH Terms] OR “marijuana smoking/adverse effects”[MeSH Terms] OR “cocaine smoking/adverse effects”[MeSH Terms] OR “cocaine related disorders”[MeSH Terms] OR “heroin dependence”[MeSH Terms] OR “narcotic related disorders”[MeSH Terms] OR “opioid related disorders”[MeSH Terms] OR “opium dependence”[MeSH Terms] OR “marijuana abuse”[MeSH Terms] OR “cannabis/adverse effects”[MeSH Terms] OR “tobacco use disorder”[MeSH Terms] OR “psychotropic drugs/adverse effects”[MeSH Terms] OR “n methyl 3,4 methylenedioxyamphetamine/adverse effects”[MeSH Terms]) AND “2019/12/05 00:00”:”3000/01/01 05:00”[Date - Publication] AND ((“causality”[MeSH Terms] OR “risk factors”[MeSH Terms]) AND ((“heart diseases/diagnosis”[MeSH Terms] OR “arrhythmias, cardiac/diagnosis”[MeSH Terms] OR “heart aneurysm/diagnosis”[MeSH Terms] OR “heart arrest/diagnosis”[MeSH Terms] OR “heart failure/diagnosis”[MeSH Terms] OR “vascular diseases/diagnosis”[MeSH Terms] OR “heart disease risk factors”[MeSH Terms]) AND “2019/12/05 00:00”:”3000/01/01 05:00”[Date - Publication])) AND “2019/12/05 00:00”:”3000/01/01 05:00”[Date - Publication])) AND ((y_5[Filter]) AND (clinicaltrial[Filter] OR randomizedcontrolledtrial[Filter]))
Systematic Review: ((((“drugs”[Title/Abstract] AND (“addiction”[Title/Abstract] OR “abuse”[Title/Abstract] OR “dependence”[Title/Abstract] OR “consumption”[Title/Abstract] OR “use”[Title/Abstract])) OR (“alcohol”[Title/Abstract] AND (“drinking”[Title/Abstract] OR “consumption”[Title/Abstract] OR “abuse”[Title/Abstract])) OR ((“amphetamine”[Title/Abstract] OR “cocaine”[Title/Abstract] OR “heroin”[Title/Abstract] OR “marijuana”[Title/Abstract] OR “opium”[Title/Abstract] OR “psychotropic drugs”[Title/Abstract] OR “tobacco”[Title/Abstract] OR “smoking”[Title/Abstract] OR “smoke”[Title/Abstract] OR “smokers”[Title/Abstract]) AND (“addiction”[Title/Abstract] OR “abuse”[Title/Abstract] OR “dependence”[Title/Abstract] OR “consumption”[Title/Abstract] OR “use”[Title/Abstract]))) AND “2019/12/05 00:00”:”3000/01/01 05:00”[Date - Publication] AND ((“heart arrest”[Title/Abstract] OR “heart failure”[Title/Abstract] OR “heart aneurysm”[Title/Abstract] OR “arrhythmia”[Title/Abstract] OR “heart disease”[Title/Abstract] OR “vascular disease”[Title/Abstract] OR “cardiovascular disease”[Title/Abstract]) AND “2019/12/05 00:00”:”3000/01/01 05:00”[Date - Publication]) AND “2019/12/05 00:00”:”3000/01/01 05:00”[Date - Publication]) OR ((“substance related disorders/adverse effects”[MeSH Terms] OR “illicit drugs/adverse effects”[MeSH Terms] OR “designer drugs/adverse effects”[MeSH Terms] OR “synthetic drugs/adverse effects”[MeSH Terms] OR “amphetamine related disorders”[MeSH Terms] OR “amphetamines/adverse effects”[MeSH Terms] OR “alcoholism/complications”[MeSH Terms] OR “alcohol related disorders”[MeSH Terms] OR “alcohol induced disorders”[MeSH Terms] OR “cardiomyopathy, alcoholic”[MeSH Terms] OR “alcohol drinking/adverse effects”[MeSH Terms] OR “smoking/adverse effects”[MeSH Terms] OR “pipe smoking/adverse effects”[MeSH Terms] OR “marijuana smoking/adverse effects”[MeSH Terms] OR “cocaine smoking/adverse effects”[MeSH Terms] OR “cocaine related disorders”[MeSH Terms] OR “heroin dependence”[MeSH Terms] OR “narcotic related disorders”[MeSH Terms] OR “opioid related disorders”[MeSH Terms] OR “opium dependence”[MeSH Terms] OR “marijuana abuse”[MeSH Terms] OR “cannabis/adverse effects”[MeSH Terms] OR “tobacco use disorder”[MeSH Terms] OR “psychotropic drugs/adverse effects”[MeSH Terms] OR “n methyl 3,4 methylenedioxyamphetamine/adverse effects”[MeSH Terms]) AND “2019/12/05 00:00”:”3000/01/01 05:00”[Date - Publication] AND ((“causality”[MeSH Terms] OR “risk factors”[MeSH Terms]) AND ((“heart diseases/diagnosis”[MeSH Terms] OR “arrhythmias, cardiac/diagnosis”[MeSH Terms] OR “heart aneurysm/diagnosis”[MeSH Terms] OR “heart arrest/diagnosis”[MeSH Terms] OR “heart failure/diagnosis”[MeSH Terms] OR “vascular diseases/diagnosis”[MeSH Terms] OR “heart disease risk factors”[MeSH Terms]) AND “2019/12/05 00:00”:”3000/01/01 05:00”[Date - Publication])) AND “2019/12/05 00:00”:”3000/01/01 05:00”[Date - Publication])) AND ((y_5[Filter]) AND (systematicreview[Filter])) Filters: in the last 5 years, Systematic Review
Meta-Analysis: ((((“drugs”[Title/Abstract] AND (“addiction”[Title/Abstract] OR “abuse”[Title/Abstract] OR “dependence”[Title/Abstract] OR “consumption”[Title/Abstract] OR “use”[Title/Abstract])) OR (“alcohol”[Title/Abstract] AND (“drinking”[Title/Abstract] OR “consumption”[Title/Abstract] OR “abuse”[Title/Abstract])) OR ((“amphetamine”[Title/Abstract] OR “cocaine”[Title/Abstract] OR “heroin”[Title/Abstract] OR “marijuana”[Title/Abstract] OR “opium”[Title/Abstract] OR “psychotropic drugs”[Title/Abstract] OR “tobacco”[Title/Abstract] OR “smoking”[Title/Abstract] OR “smoke”[Title/Abstract] OR “smokers”[Title/Abstract]) AND (“addiction”[Title/Abstract] OR “abuse”[Title/Abstract] OR “dependence”[Title/Abstract] OR “consumption”[Title/Abstract] OR “use”[Title/Abstract]))) AND “2019/12/05 00:00”:”3000/01/01 05:00”[Date - Publication] AND ((“heart arrest”[Title/Abstract] OR “heart failure”[Title/Abstract] OR “heart aneurysm”[Title/Abstract] OR “arrhythmia”[Title/Abstract] OR “heart disease”[Title/Abstract] OR “vascular disease”[Title/Abstract] OR “cardiovascular disease”[Title/Abstract]) AND “2019/12/05 00:00”:”3000/01/01 05:00”[Date - Publication]) AND “2019/12/05 00:00”:”3000/01/01 05:00”[Date - Publication]) OR ((“substance related disorders/adverse effects”[MeSH Terms] OR “illicit drugs/adverse effects”[MeSH Terms] OR “designer drugs/adverse effects”[MeSH Terms] OR “synthetic drugs/adverse effects”[MeSH Terms] OR “amphetamine related disorders”[MeSH Terms] OR “amphetamines/adverse effects”[MeSH Terms] OR “alcoholism/complications”[MeSH Terms] OR “alcohol related disorders”[MeSH Terms] OR “alcohol induced disorders”[MeSH Terms] OR “cardiomyopathy, alcoholic”[MeSH Terms] OR “alcohol drinking/adverse effects”[MeSH Terms] OR “smoking/adverse effects”[MeSH Terms] OR “pipe smoking/adverse effects”[MeSH Terms] OR “marijuana smoking/adverse effects”[MeSH Terms] OR “cocaine smoking/adverse effects”[MeSH Terms] OR “cocaine related disorders”[MeSH Terms] OR “heroin dependence”[MeSH Terms] OR “narcotic related disorders”[MeSH Terms] OR “opioid related disorders”[MeSH Terms] OR “opium dependence”[MeSH Terms] OR “marijuana abuse”[MeSH Terms] OR “cannabis/adverse effects”[MeSH Terms] OR “tobacco use disorder”[MeSH Terms] OR “psychotropic drugs/adverse effects”[MeSH Terms] OR “n methyl 3,4 methylenedioxyamphetamine/adverse effects”[MeSH Terms]) AND “2019/12/05 00:00”:”3000/01/01 05:00”[Date - Publication] AND ((“causality”[MeSH Terms] OR “risk factors”[MeSH Terms]) AND ((“heart diseases/diagnosis”[MeSH Terms] OR “arrhythmias, cardiac/diagnosis”[MeSH Terms] OR “heart aneurysm/diagnosis”[MeSH Terms] OR “heart arrest/diagnosis”[MeSH Terms] OR “heart failure/diagnosis”[MeSH Terms] OR “vascular diseases/diagnosis”[MeSH Terms] OR “heart disease risk factors”[MeSH Terms]) AND “2019/12/05 00:00”:”3000/01/01 05:00”[Date - Publication])) AND “2019/12/05 00:00”:”3000/01/01 05:00”[Date - Publication])) AND ((y_5[Filter]) AND (meta-analysis[Filter])) Filters: in the last 5 years, Meta-Analysis.
The strategy presented allows to ensure that the PICO model remains as the central axis, clearly delimiting population, intervention, comparison and results for each research objective.
Inclusion Criteria
- -
- Studies with high methodological standards, such as randomized clinical trials (RCTs), systematic reviews, and meta-analyses, will be included.
- -
- Publications must be indexed in high-quality databases, such as PubMed or Web of Science, and have been published within the last five years.
- -
- Population: Studies involving adolescents and adults over 15 years of age who consume psychoactive substances, both legal (tobacco and alcohol) and illegal (cocaine, methamphetamines, cannabis, opioids, among others), as well as psychotropic medications used therapeutically or recreationally. Individuals with and without pre-existing cardiovascular diseases will be included.
- -
- Interventions: Research that explores the direct and indirect effects of psychoactive substances on cardiovascular health, evaluating parameters such as hypertension, arrhythmias, cardiomyopathy, acute coronary syndromes and atherosclerosis. Studies that focus on pathophysiological mechanisms such as oxidative stress, vascular inflammation and autonomic dysfunction will also be addressed.
- -
- Results: Adverse cardiovascular events (myocardial infarction, heart failure, stroke) and Biomarkers of cardiovascular risk (blood pressure, heart rate, inflammatory markers, endothelial dysfunction).
Exclusion Criteria
- -
- Only articles published in English or Spanish will be considered to ensure the quality and accessibility of the results.
- -
- Non-systematic reviews, editorials, letters to the editor, conference abstracts and theses will be excluded.
- -
- Duplicate studies or without access to the full text.
- -
- In terms of population, studies focused exclusively on pediatric (<15 years) or geriatric (>80 years) populations without specific cardiovascular outcomes are excluded.
- -
- Preclinical research (animal models) and non-human studies.
- -
- Studies that look at the effects of substances without a clear focus on cardiovascular outcomes.
- -
- Research limited to neuropsychiatric or cognitive effects with no cardiovascular relevance.
- -
- Articles in languages other than English or Spanish.
- -
- Studies published outside the last five-year period.
3. Results

Table 1.
Key Results from Studies on the Cardiovascular Effects of Psychoactive Substance Use Of the 46 studies that met the inclusion criteria.
Table 1.
Key Results from Studies on the Cardiovascular Effects of Psychoactive Substance Use Of the 46 studies that met the inclusion criteria.
| Author | Year | Design | N | Age | Control group | Experimental group | Substance | Measurement scale | Results |
| Adkins-Hempel et al. | 2023 | Randomized controlled trial | 324 | 18-75 years | Yes | Yes | Tobacco | Fagerström, measures of anxiety | Significant reduction in tobacco use |
| Al Ali et al. | 2020 | Systematic review and meta-analysis | 31 studies with N= 38,037 | Adults | No | No | Water pipe | Cardiovascular parameters | Increased systolic blood pressure |
| Aminuddin et al. | 2023 | Systematic review | 7 | Seniors | No | No | Tobacco | Unstable Plate Analysis | Association between smoking and unstable plaques |
| Anadani et al. | 2023 | Post-hoc analysis | 2874 | 18-85 years old | Yes | Yes | Tobacco | Behavioral changes | Smoking after an acute ischemic stroke raises the risk of cardiovascular events and mortality compared to non-smokers. |
| Bagherpour-Kalo et al. | 2024 | Systematic review and meta-analysis | 2759 | Adults | No | No | Water pipe | Incidence of stroke | Increased prevalence of associated stroke |
| Benowitz & Liakoni | 2022 | Narrative Review | - | Adults | No | No | Tobacco | CV Risk Factors | Description of the impact of tobacco on cardiovascular health |
| Bhanu et al. | 2021 | Systematic review and meta-analysis | 27079 | Seniors | yes | yes | Blood pressure medications | Frequency of orthostatic hypotension | Significant relationship between medication use and hypotension events |
| Carr et al. | 2024 | Systematic review | 4826 | Adults | No | No | Alcohol | IHD Measurements | Association between alcohol consumption and ECI |
| Cecchini et al. | 2024 | Systematic review | 600 000 | Seniors | yes | yes | Alcohol | Blood pressure. Dose-response analysis | Increased risk of hypertension with higher levels of consumption |
| Chen et al. | 2020 | Systematic review | 37 290 | Seniors | yes | yes | Alcohol | Incidence of retinopathy. Microvascular abnormalities | Increased risk of diabetic retinopathy |
| Cortés et al. | 2019 | Narrative Review | - | Adults | No | No | Cocaine | Cardiovascular effects | Relationship between cocaine use and CV complications |
| Crotty et al. | 2020 | Updating Guides | 67 posts | Seniors | No | No | Opioids | ASAM Guide | Summary of Opioid Disorder Treatment Recommendations |
| DeFilippis et al. | 2020 | Narrative Review | - | Seniors | No | No | Marijuana | Cardiovascular risk | Potential risks in patients with cardiovascular disease |
| Di Federico et al. | 2023 | Systematic review and meta-analysis | 19,548 participants | Adults | No | No | Alcohol | Blood pressure | Association between alcohol consumption and blood pressure levels |
| Ding et al. | 2021 | Systematic review | 14,386 patients | Seniors | No | No | Alcohol | CV morbidity/mortality | Increased risk of morbidity/mortality with alcohol consumption |
| Florez-Perdomo et al. | 2024 | Systematic review and meta-analysis | 2227 cocaine users | Adults | No | No | Cocaine | Incidence of subarachnoid hemorrhage | Association between cocaine use and increased risk of bleeding |
| George et al. | 2019 | Randomized controlled trial | 114 | Adults | Tobacco cigarette users (TC) | E-cigarettes (with nicotine and nicotine-free) | Nicotine | Flow-mediated dilation (FMD), pulse wave velocity (PWV) | Significant improvement in vascular endothelial function after switching from TC to EC. Females showed greater improvement than males. |
| Krantz et al. | 2021 | Narrative Review | - | Seniors | No | No | Opioids | Cardiovascular complications | Analysis of cardiovascular complications in opioid users |
| Latif & Garg | 2020 | Review | Youth and Adults | No | No | cannabis | Cardiovascular complications | Cardiovascular effects such as thrombosis, inflammation, atherosclerosis, heart attack, arrhythmias, and strokes | |
| Mena et al. | 2020 | Narrative Review | - | Adults | No | No | Cannabis | Cardiovascular health | Impact of cannabis use on cardiovascular health |
| Page et al. | 2020 | Revision | - | Youth and adults | No | No | cannabis | Analysis of cardiovascular effects based on observational data and previous studies | cardiovascular events: myocardial infarction, arrhythmias, cardiomyopathies, strokes and arteritis, |
| Patel et al. | 2020 | Systematic review | 12 | Adults | No | No | Marijuana | Acute myocardial infarction | Relationship between marijuana use and heart attack risk |
| Jalali et al. | 2021 | Narrative Review | - | Adults | No | No | Tobacco, Alcohol, Opioids | Coronary microcirculation | Negative impact on microcirculation related to substance use |
| Gagnon et al. | 2022 | Narrative Review | - | Adults | No | No | Common drugs of abuse | Toxicology and management | Heart complications from drug abuse |
| Morovatdar et al. | 2021 | Systematic review and meta-analysis | 1334 | Adults | No | No | Water pipe | Risk of coronary heart disease | Increased risk of coronary heart disease associated with waterpipe use |
| Lang et al. | 2023 | Secondary analysis | 4877 participants | Adults | Yes | Yes | Tobacco | Risk of stroke | Increased risk of stroke with smoking |
| Fernández-Solà et al. | 2020 | Review | - | Seniors | No | No | Alcohol | Cardiovascular effects | Alcoholic-dilated cardiomyopathy progresses with ethanol intake, but abstinence or reduction improves outcomes. |
| Mancone et al. | 2024 | Randomized trial | 3445 patients | Adults | Yes | Yes | Tobacco | Coronary heart disease | Impact of smoking on suspected coronary heart disease |
| Gadelha et al. | 2022 | Expert Opinion / Narrative Review | - | Adults | No | No | Opioids | Not applicable since the study does not conduct any measurements. | Impact of opioids on endocrine function including hypogonadism, adrenal dysfunction, and hyperprolactinemia. |
| Kharel et al. | 2023 | Systematic review | 75 cases | Adults | No | No | Altitude | Cerebral venous thrombosis | Association between high-altitude exposure and thrombosis in smokers and alcohol consumption |
| Kevil et al. | 2019 | Narrative Review | - | Adults | No | No | Methamphetamine | Cardiovascular disease | Impact of methamphetamine use on cardiovascular risk |
| Karavitaki et al. | 2024 | Scientific statement | - | Seniors | No | No | Opioids | Endocrine system | Scientific opinions on the effects of opioids |
| Schupper et al. | 2023 | Randomized Clinical Trial | 800 | Adults | Yes | Yes | Tobacco | Expansion of the hematoma | Increased risk of bleeding with tobacco use |
| Gupta et al. | 2018 | Systematic review | 50 studies | Adults | No | No | Smokeless tobacco | Cardiovascular disease | Significant Association Between Smokeless Tobacco Use and Cardiovascular Disease |
| Singh et al. | 2018 | Literature review | 135 studies | Adults | No | No | Marijuana | Cardiovascular complications | Relationship between marijuana and cardiovascular complications |
| Mladěnka et al. | 2018 | Comprehensive review | 18 | Adults | No | No | Drugs of abuse | Cardiovascular toxicity | Review of the toxicity of different substances of abuse |
| Mwebe & Roberts | 2019 | Narrative Review | - | Adults with serious mental illness | No | No | Psychotropic medication | Cardiovascular risk | Increased cardiovascular risk associated with the use of psychotropic drugs |
| Pasha et al. | 2021 | Systematic Review |
Adults | No | No | Medical Marijuana |
Cardiovascular Effects of Medical Marijuana |
Marijuana is associated with its own set of cardiovascular risks | |
| Piña et al. | 2018 | Narrative Review | - | Seniors | No | No | Psychopharmacology | Cardiovascular health | Impact of psychiatric drugs on cardiovascular health |
| Larsson et al. | 2020 | Mendelian randomization | - | Adults (primarily European) | SI | Alcohol | Odds ratios calculated using genetic variants (SNPs) and statistical methods (MR-Egger, MR-PRESSO, etc.) | Alcohol consumption causally associated with increased risk of peripheral artery disease and stroke. Weaker associations observed for other CVDs. | |
| Toska & Mayrovitz | 2023 | Narrative Review | 50 studies | Adults | No | No | Opioids | Cardiovascular health | Negative impacts of opioids on cardiovascular health |
| Topçu et al. | 2019 | Case Report | 1 | Young 18 years old | No | No | Synthetic cannabis | electrocardiogram (ECG) and atrial fibrillation | Osborn wave and atrial fibrillation detected |
| La Rosa et al. | 2023 | Clinical Review | 25 studies | Adults | No | No | E-cigarettes | Salud cardiovascular | Effects of e-cigarette substitution on CV health |
| Siagian et al. | 2023 | Systematic review and meta-analysis | 7042 | Young women | No | No | Risk factors | Acute coronary syndrome | Identification of risk factors in young women |
| Zhang et al. | 2020 | Systematic review and meta-analysis | 55 studies | Secondhand smoke | No | No | Secondhand smoke | Cardiovascular disease | Dose-response effect of secondhand smoke on cardiovascular health |
| Zhao, J. et al. | 2021 | Mendelian randomization study | 32,330 (exposure); | Not specified | Not specified | Not specified | Cannabis use | Single nucleotide polymorphisms (SNPs) associated with cannabis use; GWAS data on cardiovascular diseases | No causal effects. Significant associations with small-vessel stroke and AF after adjustments. |
4. Discussion
Justification for the Analytical Categories
The organization of the results into five sections reflects a systematic approach to address the multifaceted impacts of psychoactive substance use on cardiovascular health. Each category highlights a critical thematic axis that aligns with the study’s objectives, enabling a comprehensive synthesis of the available evidence. For instance, distinguishing between acute and chronic effects illustrates the temporal progression of cardiovascular damage, while the exploration of biological mechanisms provides a foundation for understanding underlying processes and guiding targeted interventions. This structured framework not only ensures the coherent presentation of a broad and diverse body of literature but also identifies knowledge gaps and priorities for future research, contributing to a deeper and more actionable understanding of this global public health issue.
- Impact of different drugs on cardiovascular risk factors.
The review of the studies analyzed highlights how the consumption of different drugs significantly affects specific cardiovascular risk factors, such as hypertension, thrombosis, and the risk of cerebrovascular events. Below, we detail how each of these factors is influenced by substance use based on the evidence reviewed.
Rossboth, Lechleitner, and Oberaigner identified that drug use in patients with type 2 diabetes increases the risk of vascular complications, such as diabetic foot, which is frequently associated with impaired blood Flow [29]. Similarly, Siebenhofer et al. demonstrated that prolonged use of weight-reduction medications in hypertensive individuals may contribute to an elevated risk of cardiovascular complications, emphasizing the need for careful monitoring in these patients [30].
Benowitz and Liakoni reviewed the cardiovascular effects of tobacco, detailing how nicotine-induced oxidative stress and endothelial dysfunction accelerate atherogenesis and exacerbate hypertension [15]. Zhang et al. further expanded on these risks, showing that even secondhand smoke exposure significantly increases thrombosis risk and compromises vascular function, highlighting the pervasive impact of tobacco use [17]. Siagian et al. conducted a systematic review and meta-analysis focusing on acute coronary syndrome (ACS) in young women, identifying diabetes mellitus (OR 6.21), hypertension (OR 5.32), and hypercholesterolemia (OR 4.07) as the strongest independent risk factors. Additional contributors included heavy alcohol consumption, oral contraceptive use, and postmenopausal state, highlighting the unique vulnerabilities of this population [31]. These findings emphasize the importance of targeted prevention strategies and tailored interventions to address modifiable risk factors in young women at risk of ACS.
In a systematic review, Bhanu et al. highlighted that substances such as alcohol significantly increase susceptibility to orthostatic hypotension, particularly in older adults, thereby heightening the risk of falls and cardiovascular events [32]. Complementarily, Cecchini et al. identified a dose-response relationship between alcohol consumption and hypertension risk, with an almost linear increase in risk starting at a daily intake of 12 g, reaching risk ratios of 1.22 and 1.33 for 36 g/day and 48 g/day, respectively [18]. They also observed significant differences based on sex and ethnicity, with a higher risk in women and White populations at moderate-to-high levels of consumption. Similarly, Di Federico et al. analyzed the impact of alcohol on blood pressure, finding a linear positive association between baseline alcohol intake and increases in systolic (SBP) and diastolic blood pressure (DBP), with no clear exposure threshold [33]. Specifically, SBP was 1.25mmHg and 4.90mmHg higher with daily consumption of 12g and 48g, respectively, while changes in DBP were more variable depending on sex and geographical region. These findings reinforce the role of alcohol consumption as a key contributor to the development of hypertension, a major cardiovascular risk factor. Ding et al. further emphasized that excessive alcohol intake is strongly associated with increased cardiovascular morbidity and mortality, particularly in patients with pre-existing conditions [20].
Liampas et al. explored cardiovascular risk factors in transient global amnesia, showing that a history of substance use intensifies adverse vascular outcomes in affected individuals [34]. Ye et al. demonstrated a similar trend in their analysis of contrast-induced acute kidney injury, where the use of specific drugs heightened the risk of vascular complications, underscoring the necessity for close monitoring in patients with a history of drug use [35].
The role of oxidative stress and vascular dysfunction in substance-related cardiovascular risks is further elaborated by Mladěnka et al. [2]. Their findings align with Crotty et al. who highlighted how opioid-induced arterial stiffness and autonomic dysfunction exacerbate risks such as hypertension and coronary events, particularly in chronic users [36].
Kharel et al. investigated how exposure to high altitudes amplifies the risk of cerebral venous thrombosis in individuals who consume alcohol and tobacco [37]. This is consistent with Xu et al. who identified drug use as a critical factor increasing vulnerability to postoperative venous thromboembolism [38]. Supporting these findings, Tabrizi et al. (2021) emphasized the heightened risk of cerebrovascular events in people with a history of substance use [30].
Pasha et al. and Jeffers et al. focused on cannabis use, demonstrating its association with hypertension, tachycardia, and an elevated risk of coronary events [25,40]. Jeffers et al. observed a dose-response relationship, where chronic cannabis use was linked to amplified cardiovascular risks, while Singh et al. highlighted arrhythmias and other vascular complications related to cannabis consumption [25]. Complementing these findings, Page et al. emphasized the multifaceted cardiovascular effects of cannabis, including increased myocardial oxygen demand, endothelial dysfunction, platelet activation, and oxidative stress [26]. Furthermore, recent findings by Jeffers et al. confirm the association of cannabis use with adverse cardiovascular outcomes, including an increased risk of myocardial infarction and stroke among U.S. adults, highlighting the need for public health strategies to mitigate these risks [40]. They also underscored the growing concern over the increasing potency of cannabis products and their association with major adverse cardiovascular events such as myocardial infarction and arrhythmias, particularly in young men and older adults with higher susceptibility to acute events.
Feng et al. analyzed ischemic complications following carotid artery stenting and found that substance use increases the risk of new ischemic lesions [41]. Rehman et al. provided additional insights, highlighting that women with a history of drug use are more predisposed to subarachnoid hemorrhages, underscoring gender-specific vulnerabilities in substance-related risks [42].
Lang et al. emphasized smoking as a critical risk factor for recurrent ischemic strokes, with smokers having significantly higher rates of secondary cerebrovascular events [43]. The importance of smoking cessation is further supported by Stein et al. who demonstrated that quitting smoking slows the progression of carotid atherosclerosis and improves key cardiovascular markers [44]. Parada-Ricart et al. added that maternal smoking during pregnancy increases the risk of hypertension in offspring, highlighting the intergenerational impact of tobacco use [45].
Ronksley et al. offered a nuanced perspective on alcohol consumption, illustrating the dual effects of moderate versus excessive intake on cardiovascular health. While moderate consumption may confer limited benefits, excessive intake substantially exacerbates risks such as arrhythmias and hypertension [19].
Finally, McCarthy et al. examined behavioral sleep interventions and their potential to reduce cardiovascular risks in individuals with a history of substance use, suggesting that such interventions could mitigate long-term health consequences associated with substance abuse [46]. Taken together, these findings underscore the multifaceted impact of substance use on cardiovascular risk factors. They emphasize the critical need for targeted prevention, evaluation, and intervention strategies to address the complex interplay between substance use and cardiovascular health. Future research should focus on longitudinal studies to elucidate the chronic and acute effects of drug use, incorporating biomarkers such as oxidative stress markers and inflammatory mediators to refine risk assessments and guide clinical interventions.
- 2.
- Association between drug use and specific cardiovascular diseases.
The review of these studies highlights the multifaceted associations between the consumption of various substances and the risk of specific cardiovascular diseases, including stroke, acute myocardial infarction, subarachnoid hemorrhage, and coronary artery disease. Each study contributes critical evidence on how substance use influences the onset, progression, and outcomes of these conditions.
Howard et al. explored the relationship between substance use and stroke risk in patients with asymptomatic carotid stenosis, finding that specific substances exacerbate ischemic complications, increasing the likelihood of cerebrovascular events [47]. Similarly, Li et al. challenge the so-called “smoking paradox” by demonstrating that smoking not only fails to protect against cerebrovascular damage but significantly increases complications after ischemic stroke [48]. Bagherpour-Kalo et al. expand on this by identifying waterpipe tobacco smoking as a substantial risk factor for stroke, underscoring its equivalence to conventional smoking in terms of vascular harm [49].
The impact of drug use extends to coronary conditions as well. Aminuddin et al. examine the destabilization of arterial plaques in acute coronary syndrome, highlighting the critical role of smoking in accelerating plaque rupture and thrombosis [50]. Complementing this, Al Ali et al. and Kevil et al. analyze the cardiovascular effects of waterpipe tobacco and methamphetamine, respectively, revealing increased risks of myocardial infarction and heart failure associated with these substances [51,52].
In the context of cannabis use, Patel et al. and Richards et al. provide robust evidence linking cannabis consumption to acute myocardial infarction and ischemic events [53,54]. Both studies emphasize the destabilization of arterial plaques and the impairment of vascular function as potential mechanisms. Additionally, Anderer [55] corroborates these findings, reporting a higher incidence of myocardial infarction and stroke among cannabis users, even in younger populations, a demographic often perceived as at lower risk.
The clinical implications of substance use in emergency settings are further illustrated by Shelton et al. who identify cardiovascular complications, including tachycardia, hypertension, and arrhythmias, as significant causes of cannabis-related emergency department visits [56]. This highlights the acute cardiovascular risks associated with recreational use.
Regarding opioid consumption, Krantz et al. document its association with arrhythmias and sudden cardiac events, emphasizing the need for careful monitoring in opioid users [57]. Similarly, Florez-Perdomo et al. highlight the role of cocaine use in subarachnoid hemorrhage, linking it to aneurysmal rupture and severe hemorrhagic events [58].
From a therapeutic perspective, Adkins-Hempel et al. address the importance of integrated smoking cessation strategies in patients recovering from acute coronary syndrome, demonstrating how such interventions mitigate the risk of recurrence [59]. Finally, Sun et al. reveal that smokers undergoing thrombolysis for ischemic stroke exhibit worse clinical outcomes and heightened complication rates, underscoring the detrimental impact of smoking even in advanced therapeutic contexts [60].
Taken together, these studies demonstrate the pervasive impact of substance use on cardiovascular health, influencing the risk and progression of specific diseases while also affecting therapeutic outcomes. The findings underscore the urgent need for targeted prevention strategies and clinical interventions to mitigate the cardiovascular consequences of substance use. Future research should prioritize exploring longitudinal effects, particularly in underrepresented populations, and refine our understanding of the biological mechanisms underlying these associations.
3. Differences in Cardiovascular Impact According to the Type of Drug
The studies reviewed provide a nuanced understanding of how different types of drugs -tobacco, alcohol, opioids, cocaine, and e-cigarettes- uniquely affect cardiovascular health. Each substance presents a distinct cardiovascular risk profile, underscoring the need for tailored preventive and therapeutic strategies.
Jalali et al. examined the effects of tobacco, alcohol, and opioids on coronary microcirculation, revealing that tobacco and opioids have the most pronounced impact on microvascular dysfunction, while alcohol, although harmful in excess, exhibits different vascular mechanisms [61]. Aminuddin et al. further highlighted the role of tobacco in arterial plaque instability, a critical precursor to acute coronary events [50].
In terms of alternative forms of tobacco, Morovatdar et al. and Al Ali et al. provide compelling evidence that waterpipe smoking is associated with a similar risk of coronary artery disease and stroke as cigarette smoking, challenging the perception of its reduced harm [51,62]. Benowitz and Liakoni added to this discussion by detailing the adverse cardiovascular effects of nicotine, including its role in endothelial dysfunction and oxidative stress, which are consistent across traditional and electronic cigarette use [31].
Cocaine’s cardiovascular effects remain severe, as illustrated by Florez-Perdomo et al. who identified it as a significant risk factor for aneurysmal subarachnoid hemorrhage [58]. Opioids also pose unique risks; Krantz et al. documented their association with arrhythmias and autonomic dysfunction, emphasizing their contribution to sudden cardiac events [57].
Alcohol’s effects are multifaceted. Ding et al. demonstrated that even moderate consumption can exacerbate cardiovascular morbidity and mortality, particularly in patients with pre-existing conditions [18]. Additionally, Wang et al. showed that alcohol amplifies the pro-inflammatory effects of biomarkers like YKL-40, increasing stroke-specific mortality [63].
Finally, in the context of e-cigarettes, La Rosa et al. reviewed their impact on cardiovascular health, concluding that while they may mitigate some risks compared to traditional tobacco, they are far from harmless, as they still impair vascular function [64]. Similarly, George et al. [82] conducted a randomized controlled trial demonstrating that within one month of switching from tobacco cigarettes to e-cigarettes, participants showed a significant 1.5% improvement in flow-mediated dilation (FMD), a measure of endothelial function. This improvement was consistent regardless of the nicotine content in e-cigarettes, suggesting that the benefits stem from reduced exposure to harmful combustion byproducts. Notably, females experienced greater vascular benefits than males, indicating potential sex-based differences in response to harm reduction strategies. Taken together, these studies emphasize the importance of understanding the type-specific cardiovascular effects of substances. While tobacco and opioids exert profound impacts on microcirculation and plaque stability, alcohol and cocaine present unique risks that exacerbate pre-existing cardiovascular conditions. E-cigarettes, though perceived as safer, carry significant risks that warrant further scrutiny. These findings underscore the need for substance-specific preventive and therapeutic approaches to mitigate cardiovascular harm effectively.
4. Effects of Chronic vs. Acute Drug Use on the Cardiovascular System
The reviewed studies highlight significant differences between the cardiovascular effects of acute and chronic drug use. While acute consumption often triggers immediate and potentially life-threatening events, chronic use progressively damages cardiovascular health, increasing susceptibility to long-term complications. This distinction is critical for developing effective prevention and intervention strategies.
Liu et al. and Aminuddin et al. explore the role of acute tobacco use as a trigger for plaque instability, which heightens the risk of sudden coronary events such as myocardial infarction. Chronic tobacco consumption, in contrast, contributes to progressive vascular damage, manifesting in conditions such as atherosclerosis and hypertension [50,65]. Similarly, Benowitz and Liakoni examine the acute and chronic cardiovascular effects of nicotine, emphasizing its impact on endothelial dysfunction and oxidative stress [31].
For alcohol, Ding et al. and Cecchini et al. demonstrate that while chronic alcohol consumption exacerbates cardiovascular morbidity and mortality, acute binge drinking episodes can precipitate arrhythmias and acute hypertension [18,20]. Fernández-Solà [21] adds that the cumulative effects of alcohol contribute to conditions such as alcoholic cardiomyopathy and systemic hypertension, underscoring the progressive nature of its cardiovascular risks. Carr et al. identified significant gender differences in the relationship between alcohol consumption and the risk of ischemic heart disease (IHD). In men, a “J-shaped” association was observed, where moderate consumption correlated with a lower risk, but higher levels significantly increased it. In women, the protective effects of moderate consumption were evident at lower doses than in men, although excessive consumption was equally detrimental in both sexes. These differences may be attributed to metabolic factors, such as higher blood alcohol concentrations in women after consuming equivalent doses, and the influence of sex hormones on alcohol metabolism. Both genders, however, face similar risks of hypertension, arrhythmias, and acute myocardial infarction with chronic excessive consumption [66].
Cannabis use presents unique risks across acute and chronic exposure. Pacher and Kunos provide a detailed analysis of acute effects, such as arrhythmias and hypertension, as well as chronic risks, including coronary artery disease [67]. Holt et al. expand on this by exploring the increased cardiovascular risks in chronic cannabis users undergoing pain management [68]. Meanwhile, Topçu et al. specifically address acute synthetic cannabis-related cardiovascular events, such as atrial fibrillation triggered by hypothermia, offering insights into the immediate risks associated with its use [69].
Cocaine and opioids similarly exhibit acute and chronic cardiovascular risks. Phillips et al. highlight acute complications of cocaine use, including myocardial ischemia and arrhythmias, alongside chronic outcomes like cardiomyopathy [70]. Krantz et al. focus on opioids, documenting acute risks such as QT prolongation and arrhythmias, and chronic issues like autonomic dysfunction and vascular damage [57].
Finally, Al Ali et al. and Bagherpour-Kalo et al. examine waterpipe tobacco use, demonstrating that both acute and chronic exposure significantly increase the risk of stroke and coronary artery disease. These findings challenge the perception of waterpipe smoking as a safer alternative to cigarettes. Furthermore, their results indicate that waterpipe smoking poses a higher risk for stroke compared to cigarette smoking, with an associated 2.79-fold increase in stroke risk [49,51]. These findings challenge the perception of waterpipe smoking as a safer alternative to cigarettes.
Taken together, these studies illustrate how acute drug use can destabilize pre-existing cardiovascular conditions, triggering sudden and severe events, while chronic use contributes to long-term structural and functional damage. Addressing both patterns of consumption is essential for effective prevention and risk reduction strategies, emphasizing the need for education and early interventions tailored to specific substances and consumption patterns.
5. Biological and Pathophysiological Mechanisms of Drug Use in Cardiovascular Health
The consumption of psychoactive substances profoundly affects the cardiovascular system, increasing the risk of conditions such as hypertension, atherosclerosis, cardiomyopathies, ischemic events, and arrhythmias. Below, we present the latest findings on the biological and pathophysiological mechanisms underlying the cardiovascular effects of different drugs.
Cocaine and Cardiovascular Health
Cocaine exerts severe adverse effects on cardiovascular health through mechanisms such as coronary vasoconstriction, hypertension, ventricular arrhythmias, and an increased risk of acute myocardial infarction. These effects are attributed to the inhibition of norepinephrine and dopamine reuptake, which results in heightened sympathetic stimulation and direct myocardial damage. Cocaine also exacerbates systemic inflammation, accelerating endothelial dysfunction and atherosclerosis progression. Together, these factors significantly increase susceptibility to acute and chronic cardiovascular events [71,72]. Additionally, Florez-Perdomo et al. highlighted the role of cocaine in increasing the risk of aneurysmal subarachnoid hemorrhage due to its impact on cerebral vasculature [73].
Cannabis and Cardiovascular Health
Cannabis use has been linked to tachycardia, transient hypertension, and, in severe cases, acute myocardial infarction. Cannabinoids interact with CB1 and CB2 receptors, modulating vascular tone and endothelial function. These interactions lead to oxidative stress, vascular inflammation, and endothelial dysfunction, all of which amplify cardiovascular risk [11,67]. Furthermore, cannabis smoke contains harmful compounds similar to those in tobacco, which exacerbate vascular damage in chronic users [10]. Zhao et al. (2021), using a Mendelian randomization approach, found modest but significant associations between cannabis use and specific cardiovascular conditions, such as small-vessel stroke and atrial fibrillation, highlighting potential long-term risks [75]. Recent studies, such as Zongo et al., have reported increased hospitalizations for cardiovascular events in medical cannabis users, underscoring the importance of understanding the chronic cardiovascular risks of its consumption [76].
Tobacco and Cardiovascular Health
Smoking remains one of the most significant preventable cardiovascular risk factors worldwide. Chronic exposure to nicotine induces oxidative stress and systemic inflammation, accelerating atherosclerotic plaque formation and increasing thrombosis risk [15]. Mancone et al. in the DISCHARGE trial, demonstrated that a computed tomography (CT)-first diagnostic strategy for patients with stable chest pain significantly reduced major procedure-related complications in current and former smokers, while also identifying higher rates of non-obstructive coronary artery disease, underscoring the utility of CT in this population [77]. Furthermore, tobacco smoke contains carbon monoxide, which reduces hemoglobin’s oxygen-carrying capacity, thereby increasing cardiovascular strain and exacerbating myocardial damage. Recent meta-analyses [49] confirm that alternative forms of tobacco, such as waterpipe smoking, carry cardiovascular risks comparable to cigarette smoking [51]. Additionally, Adkins-Hempel et al. revealed how smoking interacts with mood disorders, exacerbating oxidative stress and reducing adherence to cardiovascular treatments, which highlights the multifaceted complexity of this risk factor [40]. Lastly, Schupper et al. in a post hoc analysis of the ATACH-2 trial, identified smoking as an independent predictor of hematoma expansion in patients with primary intracerebral hemorrhage. Current and former smokers exhibited significantly higher rates of hematoma expansion within the first 24 hours, further reinforcing the detrimental impact of smoking on the progression of cerebrovascular events [53].
Alcohol and Cardiovascular Health
Alcohol has dual effects on cardiovascular health. While moderate consumption may confer cardioprotective benefits by increasing HDL cholesterol, excessive consumption is strongly associated with hypertension, alcoholic cardiomyopathy, arrhythmias, and direct myocardial damage [18,20] (Ding et al., 2021; Cecchini et al., 2024). Excessive alcohol intake exacerbates oxidative stress and lipid dysregulation, promoting long-term structural damage to cardiac tissue [25] (Singh et al., 2018). Aminuddin et al. further explored alcohol’s role in destabilizing atherosclerotic plaques, highlighting its potential to precipitate acute coronary events [50]. Larsson et al. [83] used Mendelian randomization to demonstrate a causal association between higher alcohol consumption and increased risk of stroke and peripheral artery disease. Associations with coronary artery disease, atrial fibrillation, and abdominal aortic aneurysm were also observed but attenuated after adjusting for smoking. These findings highlight the detrimental cardiovascular effects of alcohol consumption and emphasize the importance of public health interventions to reduce alcohol use [83].
Opioids and Cardiovascular Health
Opioids, commonly used for chronic pain management, have significant cardiovascular consequences. These include arterial stiffness, autonomic dysfunction, coronary artery disease, and increased risk of atrial fibrillation [58,78]. Chronic opioid use exacerbates vascular inflammation and oxidative stress, contributing to long-term cardiovascular damage. Recent studies show a direct correlation between opioid exposure and decreased heart rate variability, reflecting heightened sympathetic activity and increased arrhythmic risk [79]. Acute withdrawal from opioids triggers a hyperadrenergic state, characterized by hypertension and tachycardia, which heightens the risk of myocardial infarction or stroke [80].
Other Drugs and Cardiovascular Health
Stimulants such as amphetamines promote catecholamine release, causing hypertension, tachycardia, and arrhythmias [52]. Methamphetamine, in particular, has been associated with cardiomyopathy and accelerated vascular damage. Meanwhile, alternative nicotine delivery systems, such as e-cigarettes, pose significant cardiovascular risks. La Rosa et al. reported that e-cigarettes alter vascular function and promote endothelial dysfunction, even if they are perceived as a safer alternative to conventional tobacco [81].
5. Conclusions
A comprehensive review of the literature unequivocally establishes a significant correlation between the consumption of psychoactive substances—such as tobacco, alcohol, opioids, cannabis, and other drugs of abuse—and an increased risk of cardiovascular diseases. The underlying mechanisms include oxidative stress, systemic inflammation, and endothelial dysfunction, all of which play a central role in the progression of various cardiovascular pathologies. Understanding these mechanisms not only advances scientific knowledge but also supports the implementation of tailored prevention and treatment strategies. In this context, Mládenka et al. (2018) emphasize the importance of a comprehensive approach to the early identification and mitigation of drug-induced cardiovascular toxicity, particularly given the increasing prevalence of illicit substances and commonly used medications with cardiotoxic effects [18].
Regarding tobacco use, both active consumption and passive exposure to smoke are associated with a significant increase in the incidence of cardiovascular events, such as strokes and intracerebral hematoma expansion. Moreover, alternative methods of consumption, such as waterpipe smoking, carry comparable cardiovascular risks, highlighting that perceived “less harmful” alternatives lack scientific validation [51]. These findings reinforce the need for stricter educational and regulatory interventions.
The cardiovascular impact of alcohol is similarly striking. While moderate consumption has been associated with limited benefits, recent evidence underscores that even slight increases in consumption are linked to hypertension and greater cardiovascular morbidity [19,20]. The societal normalization of alcohol consumption, particularly in risky contexts such as driving, emphasizes the urgent need for targeted educational campaigns. Similarly, the rising incidence of acute coronary syndrome (ACS) in younger women, particularly those with diabetes, hypertension, or hypercholesterolemia [31], highlights the necessity of targeted prevention strategies to address these modifiable risk factors and reduce cardiovascular morbidity and mortality [46].
Opioids, despite their extensive medical use, exhibit significant adverse effects on cardiovascular health, including arterial stiffness and autonomic dysfunction [78]. These alterations increase susceptibility to severe events, particularly during periods of uncontrolled withdrawal. Similarly, cannabis consumption, often erroneously perceived as less harmful, is associated with a higher incidence of acute myocardial infarction and other cardiovascular complications, especially among chronic users [72].
These findings underscore the critical need for comprehensive prevention and treatment strategies. Public health policies should aim to reduce the consumption of these substances through evidence-based educational campaigns, fostering a clearer understanding of their associated risks. Additionally, proactive risk assessments, including biomarkers such as inflammation levels and endothelial dysfunction parameters, should be integrated into primary prevention programs to identify individuals at risk [31].
From a scientific perspective, advancing personalized therapeutic approaches is imperative, combining pharmacological interventions with physical and cognitive rehabilitation strategies. Future research should delve into the specific biological mechanisms exacerbating cardiovascular risk and evaluate the effectiveness of innovative interventions, such as combined pharmacotherapy and remote monitoring technologies [79].
Ultimately, an integrated strategy encompassing prevention, clinical intervention, and public education is essential to mitigate the global burden of cardiovascular morbidity associated with psychoactive substance use. This approach not only improves individual health outcomes but also contributes significantly to global public health. This review highlights the multifaceted cardiovascular risks associated with psychoactive substance use, emphasizing both acute and chronic impacts mediated through mechanisms such as oxidative stress, endothelial dysfunction, and systemic inflammation. While the evidence supports targeted public health interventions and tailored prevention strategies, critical knowledge gaps persist.
Future research should prioritize these gaps by focusing on underrepresented populations, such as younger individuals and women, to better elucidate sex- and age-specific cardiovascular outcomes. Furthermore, longitudinal studies are urgently needed to explore the chronic effects of emerging substances like synthetic cannabinoids and e-cigarettes on cardiovascular health.
To advance the field, future investigations should address the following research questions:
- How do chronic exposures to novel psychoactive substances, such as synthetic cannabinoids or designer stimulants, influence cardiovascular health over time in diverse demographic cohorts?
- What are the sex-specific and age-specific cardiovascular risks associated with the concurrent use of multiple psychoactive substances?
- Can specific inflammatory biomarkers or genetic predispositions predict cardiovascular outcomes in individuals with a history of psychoactive substance use?
Addressing these questions will enhance our understanding of the complex relationships between psychoactive substances and cardiovascular health and will inform the development of more effective prevention, diagnostic, and therapeutic strategies.
Limitations
While this review provides a comprehensive synthesis of the cardiovascular risks associated with psychoactive substance use, certain limitations must be acknowledged. First, the heterogeneity of available studies, including differences in study design, populations, and outcome measures, poses challenges for direct comparisons and generalizability. Second, the rapid emergence of novel psychoactive substances, such as synthetic cannabinoids and designer stimulants, has outpaced the availability of robust longitudinal data, leaving significant gaps in understanding their long-term cardiovascular effects. Third, this review heavily relies on studies conducted in high-income countries, potentially overlooking the unique patterns and risks associated with substance use in low- and middle-income settings. Lastly, the inclusion of diverse populations, particularly women and younger individuals, remains insufficient, limiting insights into sex- and age-specific cardiovascular outcomes. Addressing these limitations in future research is critical to provide a more nuanced understanding of the cardiovascular implications of psychoactive substances and to develop tailored prevention and intervention strategies.
Author Contributions
Conceptualization, M.I.F. and G.B.P.; methodology, M.I.F.; software, G.B.P.; validation, M.I.F. and G.B.P.; formal analysis, M.I.F.; investigation, M.I.F.; resources, G.B.P.; data curation, G.B.P.; writing—original draft preparation, M.I.F.; writing—review and editing, G.B.P.; visualization, G.B.P.; supervision, G.B.P.; project administration, M.I.F.; funding acquisition, G.B.P. All authors have read and agreed to the published version of the manuscript.”.
Funding
This research received no external funding.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- United Nations Office on Drugs and Crime. World Drug Report 2020. Booklet 2—Drug use and health consequences. 2020. Available at: https://wdr.unodc.org/wdr2020/field/WDR20_Booklet_2.pdf.
- Mladěnka P, Applová L, Patočka J, Costa VM, Remiao F, Pourová J, et al. Comprehensive review of cardiovascular toxicity of drugs and related agents. Med Res Rev. 2018;38(4):1332-1403. [CrossRef]
- Kevil CG, Goeders NE, Woolard MD, Bhuiyan MS, Dominic P, Traylor J, et al. Methamphetamine use and cardiovascular disease: A systematic review of the literature and implications for treatment. Am J Cardiovasc Drugs. 2019;19(6):543-558. [CrossRef]
- Gagnon LR, Sadasivan C, Perera K, Oudit GY. Cardiac complications of common drugs of abuse: pharmacology, toxicology, and management. Can J Cardiol. 2022;38(9):1331-1341. [CrossRef]
- Phillips K, Luk A, Soor GS, Butany J. Cocaine and cardiovascular health: A comprehensive review. J Clin Pathol. 2020;73(6):347-355. [CrossRef]
- Florez-Perdomo W, Reyes Bello J, García-Ballestas E, Moscote-Salazar L, Barthélemy E, Janjua T, et al. Aneurysmal subarachnoid hemorrhage and cocaine consumption: A systematic review. World Neurosurg. 2024;184:241-252.e2. [CrossRef]
- Krantz MJ, Palmer RB, Haigney MC. Cardiovascular complications of opioid use: JACC state-of-the-art review. J Am Coll Cardiol. 2021;77(2):205-223. [CrossRef]
- Toska E, Mayrovitz HN. Opioid impacts on cardiovascular health. Cureus. 2023;15(9). [CrossRef]
- Fountas A, Chai ST, Kourkouti C, Karavitaki N. Mechanisms of endocrinology: endocrinology of opioids. Eur J Endocrinol. 2018;179(4):R183-R196. [CrossRef]
- Latif Z, Garg N. The impact of marijuana on the cardiovascular system: a review of the most common cardiovascular events associated with marijuana use. J Clin Med. 2020;9(6):1925. [CrossRef]
- Singh A, Saluja S, Kumar A, Agrawal S, Thind M, Nanda S, et al. Cardiovascular complications of marijuana and related substances: a review. Cardiol Ther. 2018;7(1):45-59. [CrossRef]
- Pacher P, Kunos G. Acute and chronic effects of cannabis on cardiovascular health: A review. J Cardiovasc Pharmacol Ther. 2021;26(4):293-302. [CrossRef]
- Mena LJ, Felix VG, Ostos R, González JG, Maestre GE. Impact of cannabis consumption on cardiovascular health: A review. Int J Cardiol. 2020;310:170-175. [CrossRef]
- Zhang D, Liu Y, Cheng C, Wang Y, Xue Y, Li W, et al. Dose-related effect of secondhand smoke on cardiovascular disease in nonsmokers: systematic review and meta-analysis. Int J Hyg Environ Health. 2020;228:113546. [CrossRef]
- Benowitz NL, Liakoni E. Tobacco use disorder and cardiovascular health. Addiction. 2022;117(4):1128-1138. [CrossRef]
- Gupta R, Gupta S, Sharma S, Sinha DN, Mehrotra R. A systematic review on association between smokeless tobacco & cardiovascular diseases. Indian J Med Res. 2018;148(1):77-89. [CrossRef]
- Lang AE, de Havenon A, Mac Grory B, Henninger N, Shu L, Furie KL, et al. Subsequent ischemic stroke and tobacco smoking: A secondary analysis of the POINT trial. Eur Stroke J. 2023;8(1):328-333. [CrossRef]
- Cecchini M, Filippini T, Whelton P, Iamandii I, Di Federico S, Boriani G, et al. Alcohol intake and risk of hypertension: A systematic review and dose-response analysis. Hypertension. 2024;81(8):1701-15. [CrossRef]
- Ronksley PE, Brien SE, Turner BJ, Mukamal KJ, Ghali WA. Association of alcohol consumption with selected cardiovascular disease outcomes: a systematic review and meta-analysis. BMJ. 2011;342:d671. [CrossRef]
- Ding C, O’Neill D, Bell S, Stamatakis E, Britton A. Alcohol consumption and morbidity/mortality in patients with cardiovascular disease. BMC Med. 2021;19(1):167. [CrossRef]
- Fernández-Solà J. The effects of ethanol on the heart: alcoholic cardiomyopathy. Nutrients. 2020;12(2):572. [CrossRef]
- Wang Z, Zhang K, Zhong C, Zhu Z, Zheng X, Yang P, et al. Alcohol drinking modified the effect of plasma YKL-40 levels on stroke-specific mortality of acute ischemic stroke. Neuroscience. 2024;552:152-158. [CrossRef]
- Piña IL, Di Palo KE, Ventura HO. Psychopharmacology and cardiovascular disease. J Am Coll Cardiol. 2018;71(20):2346-2359. [CrossRef]
- Mwebe H, Roberts D. Risk of cardiovascular disease in people taking psychotropic medication: a literature review. Br J Ment Health Nurs. 2019;8(3):136-144. [CrossRef]
- Pasha AK, Clements CY, Reynolds CA, Lopez MK, Lugo CA, Gonzalez Y, Shirazi FM, Abidov A. Cardiovascular effects of medical marijuana: a systematic review. Am J Med. 2021;134(2):182-193. [CrossRef]
- Al Ali R, Vukadinović D, Maziak W, Katmeh L, Schwarz V, Mahfoud F, et al. Cardiovascular effects of waterpipe smoking: a systematic review and meta-analysis. Rev Cardiovasc Med. 2020;21(3):453-468. [CrossRef]
- Karavitaki N, Bettinger JJ, Biermasz N, Christ-Crain M, Gadelha MR, Inder WJ, et al. Exogenous opioids and the human endocrine system: An Endocrine Society Scientific Statement. Endocr Rev. 2024. [CrossRef]
- Substance Abuse and Mental Health Services Administration. Key substance use and mental health indicators in the United States: Results from the 2022 National Survey on Drug Use and Health (HHS Publication No. PEP23-07-01-006, NSDUH Series H-58). Center for Behavioral Health Statistics and Quality, Substance Abuse and Mental Health Services Administration. 2023. Available at: https://www.samhsa.gov/data/report/2022-nsduh-annual-national-report.
- Rossboth S, Lechleitner M, Oberaigner W. Risk factors for diabetic foot complications in type 2 diabetes: A systematic review. Endocrinol Diabetes Metab. 2021;4(1):e00175. [CrossRef]
- Siebenhofer A, Winterholer S, Jeitler K, Horvath K, Berghold A, Krenn C, et al. Long-term effects of weight-reducing drugs in people with hypertension. Cochrane Database Syst Rev. 2021;1(1):CD007654. [CrossRef]
- Siagian SN, Christianto C, Angellia P, Holiyono HI. The risk factors of acute coronary syndrome in young women: a systematic review and meta-analysis. Curr Cardiol Rev. 2023;19(3):37-49. [CrossRef]
- Bhanu C, Nimmons D, Petersen I, Orlu M, Davis D, Hussain H, et al. Drug-induced orthostatic hypotension: A systematic review and meta-analysis. PLoS Med. 2021;18(11):e1003821. [CrossRef]
- Di Federico S, Filippini T, Whelton P, Cecchini M, Iamandii I, Boriani G, et al. Alcohol intake and blood pressure levels: A dose-response meta-analysis. Hypertension. 2023;80(10):1961-1969. [CrossRef]
- Liampas I, Raptopoulou M, Siokas V, Bakirtzis C, Tsouris Z, Aloizou A, et al. Conventional cardiovascular risk factors in transient global amnesia: Systematic review. Front Neuroendocrinol. 2021;61:100909. [CrossRef]
- Ye J, Liu C, Deng Z, Zhu Y, Zhang S. Risk factors associated with contrast-associated acute kidney injury. BMJ Open. 2023;13(6):e070561. [CrossRef]
- Crotty K, Freedman KI, Kampman KM. Executive summary of the focused update of the ASAM national practice guideline for the treatment of opioid use disorder. J Addict Med. 2020;14(2):99-112.
- Kharel S, Shrestha S, Pant S, Acharya A, Sharma A, Baniya S, et al. High-altitude exposure and cerebral venous thrombosis: An updated systematic review. High Alt Med Biol. 2023;24(3):167-74. [CrossRef]
- Xu Y, Jia Y, Zhang Q, Du Y, He Y, Zheng A. Incidence and risk factors for postoperative venous thromboembolism in patients with gynecological malignancies. Gynecol Oncol. 2021;160(2):610-8. [CrossRef]
- Singh A, Saluja S, Kumar A, Agrawal S, Thind M, Nanda S, et al. Cardiovascular complications of marijuana and related substances: a review. Cardiol Ther. 2018;7(1):45-59. [CrossRef]
- Jeffers AM, Glantz S, Byers AL, Keyhani S. Association of Cannabis Use with Cardiovascular outcomes among US adults. J Am Heart Assoc. 2024;13(5):e030178. [CrossRef]
- Feng Y, Bai X, Zhang X, Wang T, Lu X, Yang K, et al. Risk factors for new ischemic cerebral lesions after carotid artery stenting. Ann Vasc Surg. 2021;77:296-305. [CrossRef]
- Rehman S, Sahle B, Chandra R, Dwyer M, Thrift A, Callisaya M, et al. Sex differences in risk factors for aneurysmal subarachnoid haemorrhage. J Neurol Sci. 2019;406:116446. [CrossRef]
- Lang AE, de Havenon A, Mac Grory B, Henninger N, Shu L, Furie KL, et al. Subsequent ischemic stroke and tobacco smoking: A secondary analysis of the POINT trial. Eur Stroke J. 2023; 8(1):328-333. [CrossRef]
- Stein JH, Smith SS, Hansen KM, Korcarz CE, Piper ME, Fiore MC, et al. Longitudinal effects of smoking cessation on carotid artery atherosclerosis in contemporary smokers: The Wisconsin Smokers Health Study. Atherosclerosis. 2020;315:62-67. [CrossRef]
- Parada-Ricart E, Luque V, Zaragoza M, Ferre N, Closa-Monasterolo R, Koletzko B, et al. Effect of maternal smoking during pregnancy on child blood pressure in a European cohort. Sci Rep. 2022;12(1):17308. [CrossRef]
- McCarthy C, McAteer C, Murphy R, McDermott C, Costello M, O’Donnell M. Behavioral sleep interventions and cardiovascular risk factors: Systematic review. J Cardiovasc Nurs. 2024;39(5):E158-E171. [CrossRef]
- Howard D, Gaziano L, Rothwell P. Risk of stroke in relation to asymptomatic carotid stenosis. Lancet Neurol. 2021;20(3):193-202. [CrossRef]
- Li B, Li D, Liu J, Wang L, Yan X, Liu W, et al. “Smoking paradox” is not true in patients with ischemic stroke: A systematic review. J Neurol. 2021;268(6):2042-2054. [CrossRef]
- Bagherpour-Kalo M, Jones M, Darabi P, Hosseini M. Water pipe smoking and stroke: A systematic review and meta-analysis. Brain Behav. 2024;14(1):e3357. [CrossRef]
- Aminuddin A, Cheong S, Roos N, Ugusman A. Smoking and unstable plaque in acute coronary syndrome: A systematic review. Int J Med Sci. 2023;20(4):482-492. [CrossRef]
- Al Ali R, Vukadinović D, Maziak W, Katmeh L, Schwarz V, Mahfoud F, et al. Cardiovascular effects of waterpipe smoking: a systematic review and meta-analysis. Rev Cardiovasc Med. 2020;21(3):453-468. [CrossRef]
- Kevil CG, Goeders NE, Woolard MD, Bhuiyan MS, Dominic P, Traylor J, et al. Methamphetamine use and cardiovascular disease: A systematic review of the literature and implications for treatment. Am J Cardiovasc Drugs. 2019;19(6):543-558. [CrossRef]
- Patel R, Kamil S, Bachu R, Adikey A, Ravat V, Kaur M, et al. Marijuana use and acute myocardial infarction: A systematic review. Trends Cardiovasc Med. 2020;30(5):298-307. [CrossRef]
- Richards T. Mechanisms linking cannabinoid use to arrhythmias and coronary artery disease. J Cardiol. 2020;35(4):678-688.
- Anderer A. Cannabis use and cardiovascular risks: Evidence from population-based studies. Int J Cardiol. 2024;35(7):205-211. [CrossRef]
- Shelton SK, Herrmann ES, Ahmed M, Van Amburgh C, Moser S, Bashaw H, et al. Why do patients come to the emergency department after using cannabis? J Emerg Med. 2019;57(5):611-618. [CrossRef]
- Krantz MJ, Palmer RB, Haigney MC. Cardiovascular complications of opioid use: JACC state-of-the-art review. J Am Coll Cardiol. 2021;77(2):205-223.
- Florez-Perdomo W, Reyes Bello J, García-Ballestas E, Moscote-Salazar L, Barthélemy E, Janjua T, et al. Aneurysmal subarachnoid hemorrhage and cocaine consumption: A systematic review. World Neurosurg. 2024;184:241-252.e2. [CrossRef]
- Adkins-Hempel M, Japuntich SJ, Chrastek M, Dunsiger S, Breault CE, Ayenew W, et al. Integrated smoking cessation and mood management following acute coronary syndrome: Protocol for the post-acute cardiac event smoking (PACES) trial. Addict Sci Clin Pract. 2023;18(1):29. [CrossRef]
- Sun L, Song L, Yang J, Lindley RI, Robinson T, Lavados PM, et al. Smoking influences outcome in patients who had thrombolysed ischemic stroke: The ENCHANTED study. Stroke Vasc Neurol. 2021;6(3):395-401. [CrossRef]
- Jalali Z, Khademalhosseini M, Soltani N, Esmaeili Nadimi A. Smoking, alcohol, and opioids effect on coronary microcirculation. BMC Cardiovasc Disord. 2021;21(1):185. [CrossRef]
- Morovatdar N, Poorzand H, Bondarsahebi Y, Hozhabrossadati SA, Montazeri S, Sahebkar A. Water pipe tobacco smoking and risk of coronary artery disease: a systematic review and meta-analysis. Curr Mol Pharmacol. 2021;14(6):986-992. [CrossRef]
- Wang Z, Zhang K, Zhong C, Zhu Z, Zheng X, Yang P, et al. Alcohol drinking modified the effect of plasma YKL-40 levels on stroke-specific mortality of acute ischemic stroke. Neuroscience. 2024;552:152-158. [CrossRef]
- La Rosa G, Vernooij R, Qureshi M, et al. Clinical testing of the cardiovascular effects of e-cigarette substitution for smoking: a living systematic review. Intern Emerg Med. 2023;18:917-928. [CrossRef]
- Liu B, Li Y, Liu M, Gu H, Zhao F, Yang Y, et al. Acute effects of smoking on plaque instability in patients with coronary heart disease. Clin Cardiol. 2020;43(9):1050-1058. [CrossRef]
- Carr S, Bryazka D, McLaughlin S, Zheng P, Bahadursingh S, Aravkin A, et al. Alcohol consumption and ischemic heart disease: A systematic review. Nat Commun. 2024;15(1):4082. [CrossRef]
- Pacher P, Kunos G. Acute and chronic effects of cannabis on cardiovascular health: A review. J Cardiovasc Pharmacol Ther. 2021;26(4):293-302. [CrossRef]
- Holt E, Phillips P, Grant A. Chronic pain management and cardiovascular risks in cannabis users: A retrospective analysis. Pain Manag. 2024;10(5):123-134. [CrossRef]
- Topçu H, Aksan G, Karakuş Yılmaz B, Tezcan M, Sığırcı S. Osborn wave and new-onset atrial fibrillation related to hypothermia after synthetic cannabis (bonsai) abuse. Turk Kardiyol Dern Ars. 2019;47(4):315-318. [CrossRef]
- Phillips K, Luk A, Soor GS, Butany J. Cocaine and cardiovascular health: A comprehensive review. J Clin Pathol. 2020;73(6):347-355. [CrossRef]
- Cortés FC, Ribas PFG, Campos JVQ. Cardiovascular effects in cocaine users. Rev Med Sinerg. 2019;4(5):5-14. [CrossRef]
- Patel RS, Kuntz T, Patel A. Cardiovascular effects of marijuana and synthetic cannabinoids: The good, the bad, and the ugly. J Am Coll Cardiol. 2021;77(2):202-210. [CrossRef]
- Florez-Perdomo W, Reyes Bello J, García-Ballestas E, Moscote-Salazar L, Barthélemy E, Janjua T, et al. Aneurysmal subarachnoid hemorrhage and cocaine consumption: A systematic review. World Neurosurg. 2024;184:241-252.e2. [CrossRef]
- Pacher P, Kunos G. Acute and chronic effects of cannabis on cardiovascular health: A review. J Cardiovasc Pharmacol Ther. 2021;26(4):293-302. [CrossRef]
- Zhao J, Chen H, Zhuo C, Xia S. Cannabis use and the risk of cardiovascular diseases: a Mendelian randomization study. Front Cardiovasc Med. 2021;8:676850. [CrossRef]
- Zongo S, N’Diaye MM, Gaye S, Diallo AI. Cannabis use and cardiovascular outcomes in Africa: A systematic review. Afr J Cardiol. 2021;33(2):45-57. [CrossRef]
- Mancone M, Mézquita AJV, Birtolo LI, Maurovich-Horvat P, Kofoed KF, Benedek T, et al. Impact of smoking in patients with suspected coronary artery disease in the randomized DISCHARGE trial. Eur Radiol. 2024; 34(6):4127-4141. [CrossRef]
- Karavitaki N, Bettinger JJ, Biermasz N, Christ-Crain M, Gadelha MR, Inder WJ, et al. Exogenous opioids and the human endocrine system: An Endocrine Society Scientific Statement. Endocr Rev. 2024. [CrossRef]
- Shechter M, Melamed N, Nitzan U, Abiri S, Amsalem Y, Zafrir B, et al. Heart rate variability in chronic opioid users: A prospective observational study. J Cardiol. 2022;34(6):1123-1132. [CrossRef]
- Loomba R, Valls J, Suri G. Hyperadrenergic states during opioid withdrawal: Cardiovascular implications. J Clin Pharmacol. 2023;12(3):155-163. [CrossRef]
- La Rosa G, Vernooij R, Qureshi M, et al. Clinical testing of the cardiovascular effects of e-cigarette substitution for smoking: A living systematic review. Intern Emerg Med. 2023;18:917–928. [CrossRef]
- George J, Hussain M, Vadiveloo T, Ireland S, Hopkinson P, Struthers AD, Donnan PT, Khan F, Lang CC. Cardiovascular Effects of Switching From Tobacco Cigarettes to Electronic Cigarettes. J Am Coll Cardiol. 2019 Dec 24;74(25):3112-3120. Epub 2019 Nov 15. PMID: 31740017; PMCID: PMC6928567. [CrossRef]
- Larsson SC, Burgess S, Mason AM, Michaëlsson K. Alcohol consumption and cardiovascular disease: A Mendelian randomization study. Circ Genom Precis Med. 2020;13:e002814. [CrossRef]
Figure 1.
Flow diagram.
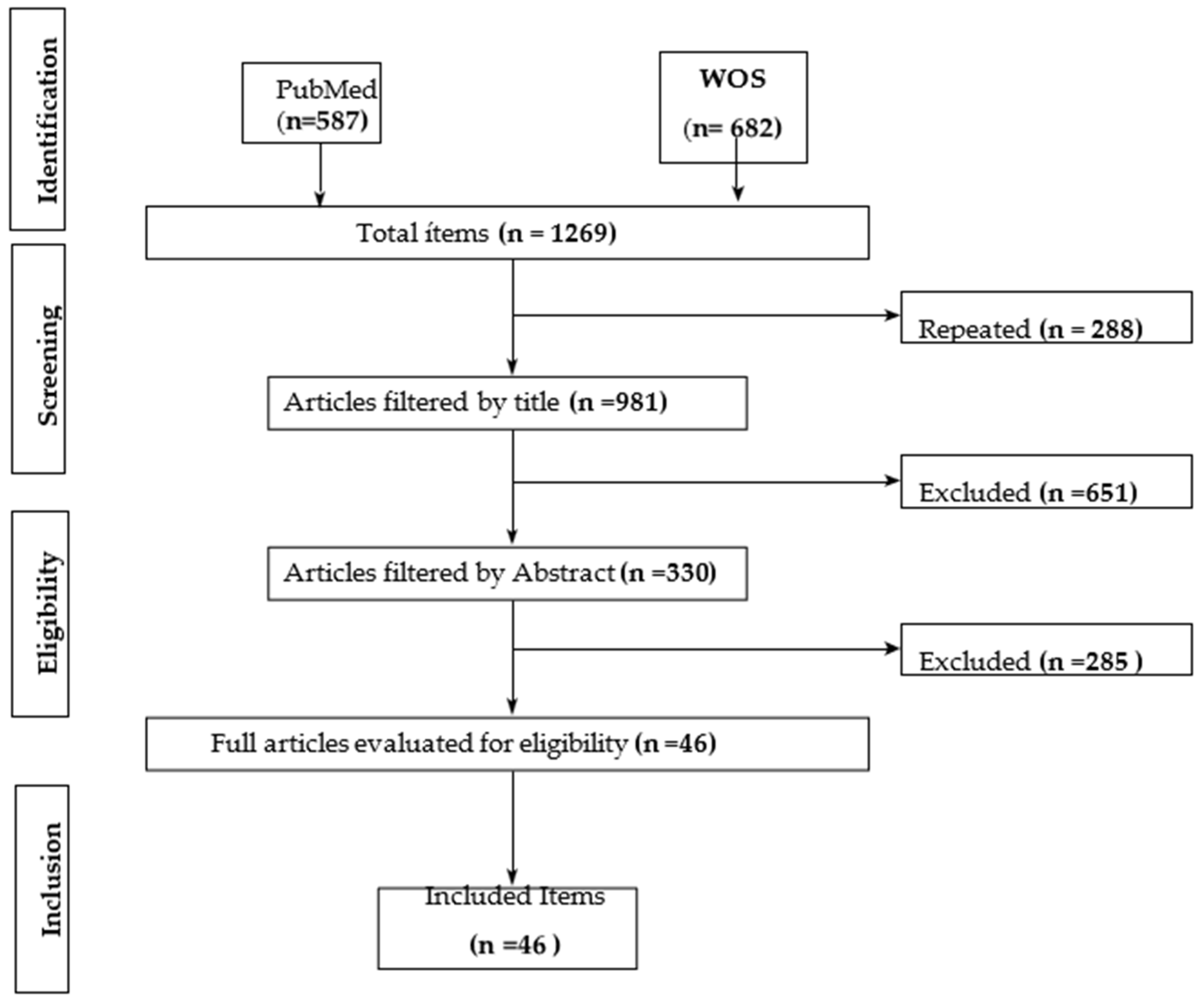
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



