
Submitted:
12 December 2024
Posted:
13 December 2024
You are already at the latest version
Abstract
The aim was to determine the influence of a complex intervention based on pharmacotherapeutic follow-up (PTF) and the application of therapeutic education (TE) protocols on the clinical and educational parameters of patients at cardiovascular risk (CVR) attending community pharmacies (CP).
Keywords:
community pharmacy
; pharmacist
; pharmacotherapeutic follow-up
; therapeutic education
; cardiovascular risk prevention
; professional pharmaceutical services
1. Introduction
According to the World Health Organisation (WHO), cardiovascular disease (CVD) is the leading cause of mortality worldwide [1], and the identification and control of cardiovascular risk factors (CVRFs), such as hypertension (HT), diabetes mellitus (DM), dyslipidaemia, obesity and smoking, among others, remains the best strategy for prevention. Numerous studies point to the importance of patient involvement for optimal disease control, both in terms of adherence to treatment and the acquisition of healthy habits aimed at controlling/reducing CVRFs [2,3,4].
There are numerous publications on CVR in community pharmacy (CPs), aimed at identifying and/or controlling risk factors as a whole or in isolation [5,6,7], and some studies have shown that in patients over 60 years of age with a medium to low level of education, HT, dyslipidaemia, diabetes II and obesity were the most common CVRFs, with an insufficient level of knowledge about their CVR and CVRFs [8]. There are also many articles describing the health benefits of pharmacotherapeutic follow-up (PTF) in these patients [9,10,11]. There is a precedent for comparing the responses of CVR patients who receive PTF with those who receive health education, demonstrating the better outcomes of the former [12]. However, it is more difficult to find papers describing a complex intervention that includes PTF and the use of specific therapeutic education (TE) protocols in this group of patients.
The main aim of TE is not only to inform, but more importantly to educate patients in the skills, knowledge and behaviors needed to self-manage their chronic conditions and treatments over time [13]. It needs to be clear and concise to enable them and/or their carers to manage treatment and prevent complications, and it needs to be delivered by trained health professionals [14]. Health education programs have a significant positive impact on attitudes and behaviors regarding global health [15]. Therefore, it is important to apply TE protocols to patients with chronic diseases, as the behavior and attitude of the individual is crucial to their engagement with their disease and proper adherence to treatment. The approach of different types of interventions related to the patient's educational and psychoeducational needs and aimed at improving knowledge about their disease can bring health benefits. In addition, when patient PTF is carried out, which aims to optimise the effects of pharmacotherapy to minimise possible adverse outcomes [16], a complex intervention is obtained aimed at helping the patient to understand the impact of the disease on their health, the reason for each of the medications they are taking, and the importance of correctly adhering to dosage guidelines. This protocolised intervention makes it possible to identify the patient's lifestyle, dietary habits, level of knowledge about their medication and compliance with dosage guidelines, and to assess their CVRFs and degree of CVR. And this work can be carried out in the CP, since frequent contact with the patients each time they come to collect their medication allows the pharmacist to offer and provide this type of service [17].
The aim of our research was to test the influence of a complex intervention over 6-month based on the PTF and the application of TE protocols on the clinical and educational parameters of patients.
2. Materials and Methods
2.1. Population Studied, Sample Size and Sampling Method
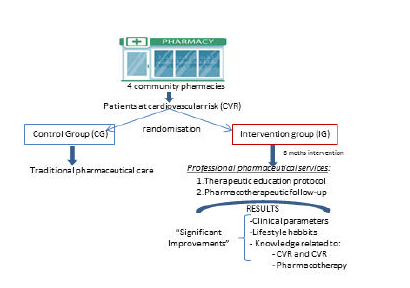
The study was carried out in patients seen daily in four Spanish CPs; two in Seville and two in Badajoz. Patients were selected for randomisation in two time slots (morning and afternoon). Those who met the inclusion criteria were invited to participate in the study when they went to the pharmacy to collect their medication. They were given information about the procedure to be followed, and those who agreed to participate had to sign the informed consent form by making an appointment with the research pharmacist.
Patients over 18 years of age, with CVRFs and pharmacological treatment for at least one of them, and/or with a history of CVD and/or obesity and/or smoking, without cognitive changes that hindered communication and understanding, were included. Pregnant women and patients who did not agree to participate after receiving the required information were excluded. Allocation to the intervention (IG) and control (CG) groups was randomised by an external person.
The initial sample size was n=100 (25 patients/pharmacy). A difference of p<0.050 or greater in favour of IG in CVR reduction after the follow-up period (6 months) was considered clinically relevant. Based on previous studies of similar characteristics and duration, a standard deviation of the change in population CVR of 0.56 was assumed. Finally, values for significance level (α = 5%) and power (β = 80%) were chosen that are commonly used in randomised controlled trials of the same type [9,18]. Using Altman's nomogram with these data would require a sample size of ≈40 for each group, giving a total of 80 patients. This size was confirmed by exact calculation using the TrialSize package in RStudio. In anticipation of potential dropouts during follow-up, a total of 100 patients were selected, with 50 patients assigned to each group (CG and IG).
2.2. Treatment Groups
Control Group (CG): Patients in this group received usual care from the participating pharmacies.
- (a)
- An initial interview at time 0 (t0) using a validated questionnaire, previously published by our group to obtain information on patient demographics, pathologies, hygiene and health habits, weight control, diet and eating habits, pharmacotherapy, allergies and drug alerts, use of natural medicine, food supplements, vitamins or infusions was conducted [8]. The interview was repeated after 6 months (t6). Their perception of the effectiveness of their treatment and their experience with pharmacotherapy at t0 and t6 were also analysed.
- (b)
- Patient knowledge of CVR and CVRFs was assessed using a validated questionnaire with a series of multiple-choice questions (http://dx.doi.org/10.1016/j.aprim. 2016.01.005) [19]. Based on the score obtained, patients were classified into two categories: adequate (> 6 points) or inadequate (< 6 points) knowledge. The difference in patient knowledge between the initial and final interviews was assessed.
- (c)
- Compliance with pharmacological treatment was assessed at t0 and t6 using the Morisky-Green-Levine test [20].
- (d)
- The following parameters were recorded: systolic blood pressure (SBP) and diastolic blood pressure (DBP) in mmHg, HbA1c: Glycosylated hemoglobin (HbA1c), total cholesterol (TC), cholesterol-High density lipoprotein (c-HDL), cholesterol-low density lipoprotein (c-LDL) triglycerides (TG) in mg/dl and body mass index (BMI) values at t0 and t6 for comparison of results.
- (e)
- The degree of CVR at t0 and t6 was recorded using the SCORE table [21].
Intervention group (IG): Patients in this group received a specific intervention from the participating community pharmacies.
- (a)
- A baseline interview at time 0 (t0) was conducted using the same questionnaire as described for CG patient [8] to obtain the necessary information from them. Patients underwent a complex intervention in this group based on the PTF and TE, with bimonthly interviews to evaluate their progress: t2 (2 months after the first interview), t4 (4 months) and t6 (final interview).
- (b)
- In this way, the same items described above for CG patients were assessed every two months: b), c), d) and e).
The PTF was carried out according to the methodology proposed in the Guide for professional pharmaceutical care services in community pharmacy [16], in order to determine the need, effectiveness and safety of the medicines received by the patient, to detect and prevent possible treatment problems and, if necessary, to try to resolve them in collaboration with the prescribing physician (return interview). In addition, a TE protocol previously used by our working group in a specialised CVR unit was applied and adapted to patients assessed in community pharmacies [22]. These were divided into three type of interventions: a) Related to the patient's educational and psychoeducational needs, with 11 categories covering healthy habits, disease management skills, disease knowledge and experience, outcome expectations, cognitive and communication function, and level of knowledge about the medication use process; b) Related to the management of pharmacotherapy, with only one category assessing the patient's experience with their medication. c) Related to the use of pharmacotherapy, consisting of the 6 categories that make up the PTF (2 for necessity, 2 for efficacy and 2 for safety) and one more to determine the causes of non-adherence.
The bi-monthly interventions assessed the percentage of patients who started or maintained healthy habits, the percentage who increased their knowledge of CVR and CVRF, and those who improved their adherence to treatment. In some cases, an additional intervention was needed, and follow-up interviews were also conducted with patients whose doctor made a change after the pharmaceutical intervention.
Pharmacy consultation: Patients selected and randomised to the IG and CG groups were scheduled for an initial interview at the pharmacy consultation in the personalised care area during pharmacy opening hours, two days a week. The contents of the questionnaires were recorded in Microsoft® Excel® 2013 software for prior database creation and subsequent statistical processing. To avoid personal bias, the interviewing pharmacist was the same in all pharmacies.
2.3. Evaluation of the Intervention
A randomised, longitudinal, prospective, unblinded, controlled clinical trial was conducted. The duration of the work was from January 2018 to July 2021 (due to the COVID-19 pandemic, the procedure was extended by 6 months).
The variables related to the objective of the project were determined in the CG at the start time (t0) and at the end time (t6). In the IG, these parameters were determined at each of the bi-monthly appointments:
- -
- Mean value of decrease in SBP and DBP values obtained according to the protocol blood pressure monitor calibrated and validated with cuffs adaptable to the arm circumference of each patient.
- -
- Mean values of decrease in lipid profile values: TC, c-LDL, TG. Roche Laboratories COBAS b101® devices were used, Accu-Chek Safe-T-Pro Plus® lancets were used to perform the punctures, and medical supplies (gauze, 96º alcohol and cotton wool) were provided by each pharmacy.
- -
- Average reduction in HbA1c levels using COBAS b101® devices and the above materials.
- -
- Average BMI reduction and patients reaching normal weight [24]. Patients' weight and height were measured using mechanical scales in each pharmacy, calibrated and validated with an integrated altimeter.
- -
- Percentage reduction of sedentary patients according to WHO criteria [25].
- -
- Percentage reduction in the number of patients who smoke, by assessing the number of patients who managed to reduce their consumption of cigarettes/day.
- -
- Percentage of patients achieving clinical control targets for better CVR prevention of the following parameters SBP, DBP, TC, c-LDL, c-HDL, TG, HbA1c, defined for each patient according to their clinical condition.
- -
- Level of knowledge achieved by the patient about CVR, CVRFs between t0 and t6.
- -
- Average level of medication adherence: Percentage of patients who improved their adherence at the end of the study (t6).
- -
- The pharmacotherapy profile of the patients was assessed.
- -
- The type and number of educational interventions required for each patient were assessed only in the IG.
At the end of this intervention period, a CG-IG comparison was performed to evaluate the difference in the results obtained between t0 and t6 in the patients of each group.
2.2. Statistical Analysis
The free and open-source software RStudio, version 1.1.414 - © 2009-2018 RStudio, Inc. was used. Within this integrated development environment (IDE), after the usual work of debugging and resolving inconsistencies in the data, most of the calculations and tables were obtained using the compareGroups version 4.0 package. Data archived in Excel were exported to RStudio software. All results were expressed as means and standard deviations for continuous variables and frequencies and percentages for categorical variables. Continuous variables were analysed using Student's t-test for two samples, while categorical data were analysed using Pearson's chi-squared test. A p-value < 0.05 was considered statistically significant.
3. Results
3.1. Sociodemographic Characteristics of the Sample
Of the initial 100 patients, 15 dropped out of the study for reasons such as change of address, lack of interest or illness of a close relative. The sample was reduced to 85 patients (41 in CG and 44 in IG) distributed among the four pharmacies.
The gender distribution in both groups, the mean age of the sample, the level of education and the type of living arrangements are shown in Table 1. Although the sample was initially evenly split between men and women, after the losses, women predominated in the CG (56.1%) and men in the IG (59.1%).
3.2. Prevalence of CVRFs and CVR Value
Table 2 shows the percentages and baseline values (t0) of the different CVRFs, as well as the level of prevention and the CVR value CG and IG.
The remaining CVRFs of the two groups at baseline (t0), weight level, BMI, level of physical activity and tobacco consumption are shown in Table 3.
3.3. Level of Individual Patient Knowledge of CVR and CVRFs
Using the test to assess patients' knowledge of their CVR and CVRFs [19], the mean of the total number of adequately answered questions was 4.3±1.46, corresponding to an inadequate level of knowledge.
3.4. Adherence to Pharmacotherapy
The overall mean of patients' adherence to prescribed medication was 72.4% according to the Morisky-Green test [20].
3.5. Prevalence of Pharmaceutical Interventions Related to Educational and Psychoeducational Needs and the Patient's Pharmacotherapy
The list of all the interventions carried out following the application of the protocols described in section 2.2. of “treatment groups” in the material and methods is presented in the Appendix A(Tables A.1., A.2, A.3) at the end of the article. The first column indicates the category evaluated, the second column lists each of the items corresponding to the interventions related to the problems identified in the patients of this category, and the third column shows the number and percentage of interventions carried out.
From the results showed in these tables, it was confirmed that 100% of the intervention patients had to be trained in the CVR knowledge category (Table A.1). It was also necessary to explain the importance of 'Physical activity' to improve the clinical condition (50.0%), to use motivational interviewing to help the patient feel able to initiate and maintain this healthy habit in the long term (52.1%), and to explain the frequency, duration and intensity required to achieve the desired results in 60.4% of patients (Table A.1). As for the category of "heart healthy diet", 66.7% of patients needed to be given an idea of the impact of certain foods and/or ingredients (salt, sugar, fats, alcoholic drinks...) on their pathology, and motivational interviewing was necessary for 60.40%. In addition, 68.8% were offered a list of heart-healthy foods (Table A.1).
In the “knowledge and experience about their pathologies” category (Table A.1) the most appropriate learning method had to be chosen for each individual (56.2%) in order to teach them about their condition: identification, causes, duration, consequences and appropriate control. 41.7% needed to be informed and trained about what self-management is and why it is necessary on a regular and long-term basis, and 43.8% needed information about the purpose of self-management in order to be able to assess whether the medicines they were using were effective. It is curious that the 12,5 % of patients did not want to take the medication because they considered it was a sign of aging and 6.25% was afraid to start using medication (Table A.2). In table A.3 it can be observed that 25% had an untreated medical condition and in the 29.2% the medication was not producing an adequate response. In the “medication adherence” category (Table A.3.) it should also be noted that 27.1% needed education about the importance of adherence. In addition, a careful study of these three tables gives us much useful information about the patients.
3.6. Evaluation of the Pharmaceutical Intervention
Table 4 shows the evolution of the two groups, CG and IG, after 6 months of pharmaceutical follow-up. In the IG patients, the following results were observed: significant reduction in CVR (p<0.005), BP (p<0.05) and sedentary lifestyle (p<0.001). Knowledge of CVR and CVRFs also increased in the IG for all patients (p<0.001).
The percentage of patients achieving the target values for each of the CVRFs assessed is shown in Table 5. The control values established by the European guidelines have been taken into account according to the clinical condition of each patient, depending on whether they were diabetic or not and the level of prevention they were in. It is noteworthy that in the IG the control of SBP levels, 52.3% at t0, increased to 79.5% after the intervention reaching a difference of 27.2 %. The percentage of patients with controlled triglycerides also increased by 12.4%.
The pharmaceutical follow-up of the IG patients showed that 29.2% of the patients did not achieve the expected response (ineffectiveness), 25% had untreated pathologies (they needed treatment) and 10 % had an adverse reaction. These latter data are not shown in tables.
4. Discussion
4.1. Discussion
The community pharmacist can play an important role in the primary and secondary prevention of CVD and in the detection and control of specific CVD through patient education and counselling programmes that increase patients' knowledge about the management and safety of their treatments, reviewing their medication and monitoring clinical parameters [17]. Although systematic reviews of randomised controlled and observational studies have documented improved control of some conditions, such as HT, and a reduction in patient hospitalisations [26,27], more research is needed to quantitatively and qualitatively assess the impact of pharmaceutical interventions on CVD.
A recent study showed that the majority of patients with CVR presenting to the CP are over 60 years of age, have a medium/low level of education, a high percentage have developed hypertension, are overweight or obese, tend to be sedentary and have inadequate knowledge of their CVRFs and CVR level [8].
These results led us to apply a complex intervention based on the use of a TE protocol accompanied by PTF, which has previously been applied by our research group and shown to be effective in patients at the Specialised CVR Service of a local hospital in Seville [28].
The results show that 100% of IG patients needed to be given basic knowledge about CVR and CVRF. A high percentage who was unaware of the benefits of a heart-healthy diet and moderate physical activity were stressed the benefits of a proper diet, provided with graphic and written material to help them improve their habits, informed and helped to start moderate physical activity, and smokers were informed of the need to reduce and/or stop using tobacco.
Specific goals were set with each patient and behavioural changes to achieve these goals were encouraged at each session. More than half required motivational interviewing, which is recognised by the American Heart Association as an effective intervention for promoting health-related outcomes [29] and aims to stimulate and convince the patient of the importance of their direct involvement in achieving the desired goals and maintaining them over time.
Problems related to patients' treatments were also addressed in each interview to assess their effectiveness and to identify and/or prevent adverse effects [16]. Because pharmacists work directly with patients to assess their medication, they are more aware of the need to adhere to treatment guidelines and contribute to optimising the management of their pharmacotherapy [30]. Protocol-based monitoring is particularly beneficial in multi-morbid and polymedicated chronic patients, who are at greater risk of inadequate pharmacological treatment due to continuous transitions in care [31]. In many cases, physician intervention is required to resolve or prevent these inadequacies, creating a highly beneficial pharmacist-patient-physician relationship. Several studies have shown that the involvement of the pharmacist in the health care team responsible for the patient's care leads to improved medication efficacy and safety [32,33,34,35].
This work has shown that the combined use of specific protocols of TE and PTF in IG patients led to a significant reduction in some parameters such as SBP (p<0.05), CVR (p<0.05), sedentary lifestyle (p<0.001) and a significant improvement in knowledge of CVR and CVRF (p<0.001) after 6 months of follow-up compared to CG. In general, a higher number of IG patients achieved control values after pharmaceutical intervention for DBP, TG, HbA1c, BMI. These results, analysed in the overall sample and in each of the pharmacies where the study was conducted, show that the work of the community pharmacist can be highly relevant in helping patients to control CVRFs.
The EMDADER HTA study, carried out in Spanish pharmacies, demonstrated the beneficial results of PTF in outpatients with hypertension, with a significant increase of 19.6% in the percentage of patients achieving SBP control targets [9]. In our study, with the combined intervention of TE and PTF, this percentage increases to 27.2%, which could demonstrate the greater efficacy of the procedures used.
PTF combined with TE resulted in an overall significant improvement in the health status of IG patients. This suggests that there is an obvious need to establish broader and more effective educational interventions that are sensitive to the perceptions, attitudes and skills of individual patients, and that the community pharmacist can play a relevant role in the primary and secondary prevention of CVD.
4.2. Limitations of the Study
The number of patients was somewhat limited due to the difficulty of recruiting cv-risk patients in the community pharmacies. The reliability of the information provided by the patients could be questioned if they did not understand the questions well or did not answer them truthfully. Also, the fact that they are regular users of pharmacies could influence the results. This was minimised by the fact that the interviewer was a person outside the pharmacy staff and the same for the whole study.
5. Conclusions
The TE protocols related to the patients' educational and psycho-educational needs applied individually and combined with the PTF, were very effective in helping patients to improve their lifestyle habits, CVR and CVRF knowledge, adherence to treatments, optimisation of pharmacotherapy, and thus improving some important clinical parameters of their CVD and their health status.
Author Contributions
Conceptualization, M.M.M.; M.C.M.J. and P.R.; methodology, B.J.P.; M.M.M.; M.C.M.J.; P.R.; software, B.J.P.; formal analysis, B.J.P.; investigation, B.J.P. and M.M.M.; resources, M.M.M.; M.C.M.J.; data curation, B.J.P.; writing—original draft preparation, M.C.M.J. and P.R.; writing—review and editing, M.M.M.; M.C.M.J. and P.R..; visualization, B.J.P.; M.M.M.; M.C.M.J. and P.R.; supervision, M.M.M.; M.C.M.J. and P.R.; project administration, M.C.M.J. and P.R.
Funding
This research received no external funding.
Ethical considerations
This study was conducted in accordance with the Declaration of Helsinki (7th revision), http://www.wma.net. Ethics Committee was from the Hospital Virgen de Valme, Andalusian Health Service, Government of Andalusia (SAS 2433/20).
Informed Consent Statement
The privacy rights of human subjects have been observed and the written informed consent was obtained from all the volunteers who agreed to take part in the study.
Data Availability Statement
Data supporting the reported results is available from the authors on request.
Acknowledgments
The authors would like to thank the head pharmacists of the pharmacies included in the study and all the technical staff for their kind help in preparing the questionnaires and recording the values established in the protocols. The authors are grateful for the statistical analysis of the results carried out by Mr Benito Jose Velasco, Head of the Electoral Census Service of the Provincial Delegation of the National Institute of Statistics (Badajoz), for his invaluable collaboration in the statistical processing of the data.
Conflicts of Interest
The authors declare no conflicts of interest
Appendix A:

Table A.1.
Prevalence of pharmaceutical interventions related to educational and psychoeducational needs.
Table A.1.
Prevalence of pharmaceutical interventions related to educational and psychoeducational needs.
| CATEGORY EVALUATED (Problem detected) |
PHARMACEUTICAL INTERVENTIONS | FREQUENCY OF INTERVENTION n (%) |
|---|---|---|
| Physical activity (PA) | ||
| Patients do not know what PA to do | Explain and help to choose an appropriate PA | 21 (43.8%) |
| Patients do not understand the importance of doing PA | Explain the importance of PA to improve clinical condition | 24 (50.0%) |
| Patients are not motivated to engage in PA | Motivational interviewing to help start and maintain PA | 25 (52.1%) |
| Patients have limitations in carrying out PA (physical, time, scare) | Develop a specific plan according to their limitations | 11 (22.9%) |
| Patients perform PA although inappropriately | Indicate frequency, duration, and intensity for desired results | 29 (60.4%) |
| Teaching how to balance diet and medication during PA | 2 (4.17%) | |
| Inform about safety precautions for performing AP | 6 (12.5%) | |
| Heart-healthy diet (HHD | ||
| Patients are unaware of the appropriate diet for their clinical condition | Explain the effect of salt, sugar, alcoholic beverages... on their pathologies | 32 (66.7%) |
| Patients do not understand the importance of an HHD to their health condition | Motivational interviewing for the patient to initiate and maintain an HHD | 29 (60.4%) |
| Patients are not motivated to do an HHD | Development of a meal plan according to the patient's preferences and financial conditions | 11 (22.9%) |
| Patients have cultural, emotional or financial barriers | Offer a list of heart-healthy foods | 33 (68.8%) |
| Smoking | ||
| Patients do not know the consequences of smoking on their pathologies | Explain the consequences of smoking and contrast the perceived benefits | 12 (25.0%) |
| Patients think smoking 5 to 10 cigarettes is safe | To present possibilities of help: psychological support and pharmacotherapy | 6 (12.5%) |
| Patients do not know what to do to quit smoking | Teach skills needed to quit smoking depending on the phase where they are | 7 (14.6%) |
| Patients are unaware of the existence of treatments to quit smoking | Minimum intervention (3 min) at the end of the initial interview (provide written support material) | 7 (14.6%) |
| Phase of abandonment in which the patient finds himself | Insist on reducing consumption per day. Motivate towards change. Deliver support material | 2 (4.17%) |
| Smoking level (number of cigarettes per day) | Refer the patient to the specialized smoking unit for pharmacotherapy | 5 (10.4%) |
| Help improve adherence to treatment, insist on total abstinence, help recognize risk situations | To all smokers | |
| Skills and competencies to manage the disease | ||
| Patients do not know how to self-control and record their parameters | Demonstration on biochemical parameter measurement techniques | 25 (52.1%) |
| Patients do not know how to evaluate risk situations and decide what to do | Request that patients perform the techniques for measuring the parameters of their diseases | 26 (54.2%) |
| Patients do not know how to use medications because of the complexity of the dosage form | Teach them how to record the measured parameters | 26 (54.2%) |
| Explain the importance of the measures, the appropriate schedules | 24 (50.0%) | |
| Teach what to do in risky situations | 24 (50.0%) | |
| Ask the patient to teach how to use medications at home and make necessary corrections | 1 (2.08%) | |
| Teach patients how to use medicines in different dosage forms | To all interviews | |
| Knowledge about CVR | ||
| Patients do not know what cardiovascular risk is | Teach patients what CVR and CVRF are | 48 (100%) |
| Patients do not know the real cardiovascular risk | Teach patients how to estimate the risk and how important it is to know the actual CVR | 48 (100%) |
| Patients are unaware of the different CVRF they suffer from and their control objectives | Teach patients which CVRFs present and their control objectives | 48 (100%) |
| Teach patients the importance of controlling each CVRF | 48 (100%) | |
| Knowledge and experience about their pathologies | ||
| Lack of basic knowledge about the pathologies patients present | Teach about its pathologies: causes, duration, consequences and adequate control | 27 (56.2%) |
| Patients do not know what self-control is for | Teach what self-control is and the importance of doing it periodically and in the long term | 20 (41.7%) |
| Patients do not perform self-control because thinks it is not necessary | Relate the goal of self-monitoring to the effectiveness of the medications they have | 21 (43.8%) |
| Patients describe negative experiences of their own or of other people with these pathologies | Discuss the causes of negative experiences of the disease | 10 (20.8%) |
| Patients make mistaken assessment of their physiological state | Teach them how to assess their physiological state and what to do in case of imbalance | 4 (8.33%) |
| Outcome expectations | ||
| Patients do not know the natural history of their disease | Teach the natural history of the disease and when it is or is not controlled | 4 (8.33%) |
| Patients feel false expectations in the results with the use of medication or alternative therapies | Explain the expected short-, medium- and long-term outcomes with appropriate use of pharmacotherapy, lifestyle changes and non-pharmacological measures | 5 (10.4%) |
| Patients do not know what to expect now that they have a chronic illness | Explain the therapeutic goals they need to achieve for each drug and in how long | 12 (25.0%) |
| Foster and strengthen trust in the treatment and in the doctor | 4 (8.33%) | |
| Self-efficacy | ||
| Patients have low self-efficacy | Teach them during follow-up the results of their learning: illness, medications, self-control | 7 (14.6%) |
| Patients do not know how to manage their disease | Help them perceive that they are self-effective in controlling their disease | 5 (10.4%) |
| Patients have a lack of perception about its effectiveness | Teach and help them perceive that they are self-effective in controlling their disease | 1 (2.08%) |
| Cognitive and Communication Function | ||
| Patients do not prepare for the consultation and forget to discuss important things about their health condition | Teach the patient to prepare before going to appointments, writing reminders of what is important | 2 (4.17%) |
| Patients forget the guidance of the health professional at the end of the consultation | Teach them how to request a report at the end of the consultation and not be left with doubts | 2 (4.17%) |
| Patients do not know how to recognize and express their needs | Encourage the patient to call the professional when in doubt | 3 (6.25%) |
| Teach them to speak assertively with the professional about doubts and needs | 3 (6.25%) | |
| Help the patient improve their knowledge of diseases, treatments, and self-efficacy | 1 (2.08%) | |
| Risk perception | ||
| Patients do not realize the seriousness of their clinical condition | Work with patients to make them aware of their actual health condition and the risks to which they are exposed | 9 (18.8%) |
| Knowledge about the process of using medications | ||
| Patients do not know what disease each of the drugs is used for | Explain to the patient about the medication: name, for what disease, dosage, how to take it and until when, common adverse effects | 8 (16.7%) |
| Patients do not know the names of the medications they take | Teach them how to use medicines correctly: demonstration, written information | 2 (4.17%) |
| Patient do not know the correct use process | Teach the importance of using all medications correctly by relating them to their effects on disease control | 5 (10.4%) |
Table A.2.
Prevalence of pharmaceutical interventions related to patient-centred pharmacotherapy management..
Table A.2.
Prevalence of pharmaceutical interventions related to patient-centred pharmacotherapy management..
|
CATEGORY EVALUATED (Problem detected) |
PHARMACEUTICAL INTERVENTIONS | B |
| Experience with pharmacotherapy | ||
| Patients do not know the usefulness of the prescribed medication | Listen to and acknowledge the different feelings expressed by patients | 3 (6.25%) |
| Patients are afraid to start using a drug | Pay attention to and try to assess the expectations and concerns of patients | 3 (6.25%) |
| Patients doubt the need to use one medication or add another to their treatment | To make patients understand the need of medication | 3 (6.25%) |
| Patients believe that taking more medication means that its health is getting worse | Undoing the patient's mistaken beliefs about their health status and treatment | 1 (2.08%) |
| Patients feel wrong expectations about the use of their medication | Help to understand and accept that: they have a chronic disease, which can be managed, with a necessary pharmacotherapy, with benefits and adverse reactions | 2 (4.17%) |
| Patients fear of having their medication withdrawn or their drug therapy changed | Teach patients when the medication is not being effective and needs to be changed | 2 (4.17%) |
| Patients do not want to increase the dose for fear of adverse effects | Perform negotiation methods with the patient to make changes in pharmacotherapy | 3 (6.25%) |
| Patients do want to live with the negative effects of their medication | Offer and help the patient choose alternatives that best meet their expectations and precautions | 2 (4.17%) |
| Patients fear of using several medicines for the same disease | Share with patients about more effective and/or safer medication alternatives | 1 (2.08%) |
| Patients do not want to withdraw or decrease the dose for fear of losing its beneficial effects | Respect the patient's autonomy in making their own decisions | 1 (2.08%) |
| Because of previous negative experiences, patients do not believe it should take the medication | Condescending to the decisions made by the patient | 1 (2.08%) |
| Patients do not use medication as prescribed, makes dose adjustments without valid criteria | Motivate them to make lifestyle changes to increase the effectiveness of medications | 2 (4.17%) |
| Patients do not want to take medication because it’s still does not accept the illness | Teach them about their illnesses and about the use of their medication | 3 (6.25%) |
| Patients do not want to take the medication because it is a sign of aging | Teach them the benefits of pharmacotherapy in managing their disease and preventing future complications | 6 (12.5%) |
| Patients do not like to take medication | Increase patient self-efficacy in disease control and pharmacotherapy | 1 (2.08%) |
Table A.3.
Prevalence of pharmaceutical interventions related to drug-centred pharmacotherapy management.
Table A.3.
Prevalence of pharmaceutical interventions related to drug-centred pharmacotherapy management.
|
CATEGORY EVALUATED (Problem detected) |
PHARMACEUTICAL INTERVENTIONS | FREQUENCY OF INTERVENTION n (%) |
| Unnecessary medication | ||
| There is no valid clinical indication for pharmacotherapy at this time | Inform the doctor about the need to stop the unnecessary medication | 2 (4.17%) |
| The pharmacotherapy used is to treat an avoidable adverse effect | Inform the doctor about the need to stop the unnecessary medication and correct the adverse effect | 1 (2.08%) |
| Need for pharmacotherapy | ||
| Patients have an untreated medical condition | Inform the doctor of the need to start the necessary treatment | 12 (25.0%) |
| The disease needs to add a drug to achieve synergistic effect | Inform the doctor of the need to add synergistic medication | 4 (8.33%) |
| There is a need for preventive pharmacotherapy | Inform the doctor of the need for added preventive pharmacotherapy | 7 (14.6%) |
| Ineffective medication | ||
| The medication does not produce the desired response | Inform the doctor of the need to withdraw the medication and start a new treatment | 14 (29.2%) |
| Adverse reaction | ||
| The medication is producing an adverse reaction | Inform the doctor of the need to discontinue the medication responsible for the adverse reaction or allergy | 1 (2.08%) |
| Safer medication is needed because of existing risk factors | Inform the doctor about the need to stop and switch to another, safer medication | 3 (6.25%) |
| The medication is contraindicated due to existing risk factors | Inform the doctor about the need to stop and switch to another, safer medication | 1 (2.08%) |
| Medication adherence | ||
| Patients prefer not to use medication | Assess whether the causes are related to the patient's subjective experience with their medications | 11 (22.9%) |
| Do not use medicines because they do not understand the instructions for use | Talk to patients about adherence and its benefits | 13 (27.1%) |
| Low adherence to pharmacotherapy due to forgetfulness | Simplifying the therapeutic regimen when possible | 1 (2.08%) |
| Patients are adherent only to certain medications | Teach patients to understand the use of all their medication | 2 (4.17%) |
| Patients do not have access to its medications | Associate taking their medications with a regular daily activity | 9 (18.8%) |
| Indicate to patients reminders of the times of taking the medications | 3 (6.25%) | |
| Talk to patients bout previous adverse reactions and explain how to prevent them from recurring. | 1 (2.08%) | |
| Negotiate goals for adherence to each medication and make positive reinforcement | 2 (4.17%) |
References
- World Health Organization. (Accessed on March 2021). Available online: https://www.who.int/health-topics/Cardiovascular-diseases#tab=tab_1.
- Kreutz, R.; Brunström M; Burnier, M.; Grassi, G.; Januszewicz, A.; Muiesan, M.L.; Tsioufis, K.; de Pinho, R.M.; Albini, F.L.; Boivin, J.M.; et al., European Society of Hypertension clinical practice guidelines for the management of arterial hypertension. Eur J Intern Med 2024; 126:1-15. [CrossRef]
- Changsieng, P.; Pichayapinyo, P.; Lagampan, S.; Lapvongwatana, P. Implementation of Self-Care Deficits Assessment and a Nurse-Led Supportive Education Program in Community Hospitals for Behavior Change and HbA1c Reduction: A Cluster Randomized Controlled Trial. J Prim Care Community Health. 2023; 14:1-9. [CrossRef]
- Vasconcelos, C.E.G.D.C., Cabral, M.M.L.G.F., Ramos, E.C.P., Mendes, R.D.C. Benefits of adding food education sessions to an exercise programme on cardiovascular risk factors in patients with type 2 diabetes. J Nutr Sci. 2021, 11;10:e59. [CrossRef]
- Rondeaux, S., Braeckman, T., Beckwé, M., Biset, N., Maesschalck, J., Duquet, N., De Wulf, I., Devroey, D., De Vriese, C. Diabetes and Cardiovascular Diseases Risk Assessment in Community Pharmacies: An Implementation Study. Int J Environ Res Public Health. 2022, 17;19(14):8699. [CrossRef]
- Macaulay, T.E.; Schaidle, S.; Wayne, N. Cardiovascular Risk Reduction by Pharmacists at the Workplace. Curr Cardiol Rep. 2020 ; 22(3):15. [CrossRef]
- Fonseca, A., Lima, T.M., Fernandez-Llimos, F., Castel-Branco, M.M., Figueiredo, I.V. Evaluation of Cardiovascular Pharmacotherapy Guideline Adherence and Risk Factor Control in Portuguese Community Pharmacy Patients. Int J Environ Res Public Health 2022 ;19(10):6170. [CrossRef]
- Buenavida, P., De la Matta, M.J., Martín, M.J., De la Puerta, R. Strategies for detecting pharmacotherapeutic and educational needs of patients with cardiovascular risk in community pharmacy. Ars Pharm 2023;64(3):192-04. [CrossRef]
- Amariles, P., Sabater-Hernández, D., García-Jiménez, E., Rodríguez-Chamorro, M.A., Prats-Más, R., Marín-Magan, F., et al. Effectiveness of Dader Method for Pharmaceutical Care on control of blood pressure and total cholesterol in outpatients with cardiovascular disease or cardiovascular risk: EMDADER-CV Randomized Controlled Trial. J Manag Care Pharm 2012; 18(4): 311-23.
- Currenti, W.; Losavio, F.; Quiete, S.; Alanazi, A.M.; Messina, G.; Polito, R.; Ciolli, F. et al. Comparative Evaluation of a Low-Carbohydrate Diet and a Mediterranean Diet in Overweight/Obese Patients with Type 2 Diabetes Mellitus: A 16-Week Intervention Study. Nutrients. 2023,16(1):95. [CrossRef]
- Al Hamarneh YN, Hemmelgarn BR, Hassan I, Jones CA, Tsuyuki RT. The Effectiveness of Pharmacist Interventions on Cardiovascular Risk in Adult Patients with Type 2 Diabetes: The Multicentre Randomized Controlled RxEACH Trial. Can J Diabetes. 2017 Dec;41(6):580-586. [CrossRef]
- Bofí Martínez, P., García Jiménez, E., Martínez Martínez, F. Comparison of health education and drug therapy monitoring interventions in patients with cardiovascular risk factors attending a community pharmacy (FISFTES-PM Study). Aten Primaria. 2015;47(3):141-8. [CrossRef]
- Chen, M.F., Wang, R.H., Hung, S.L. Predicting health-promoting self-care behaviors in people with pre-diabetes by applying Bandura social learning theory. Appl Nurs Res. 2015, 28(4):299-304. [CrossRef]
- Community Nursing Association. Chronicity Group. Health Education/Therapeutic Education. May 2014 (Accessed 21 November 2023) Available at: https://enfermeriacomunitaria.org/web/attachments/article/951/EPS.%20Educaci%C3%B3n%20Terap%C3%A9utica%20.pdf.
- Rizvi, D.S. Health education and global health: Practices, applications, and future research. J Educ Health Promot 2022,11: 262. [CrossRef]
- Pharmaceutical Care Forum. Community Pharmacy. Practical Guide to Pharmaceutical Care Services. Madrid. Ed. General Council of Official Pharmaceutical Associations; 2014. 58p.
- Pharmaceutical Care Forum. Community Pharmacy. Practical Guide to Clinical Professional Services (CPPS) in Community Pharmacy. Madrid. Ed Medea, Medical Education Agency S.L. 2024. 113p.
- Marques Santana, G. Evaluation of the effectiveness of an intervention based on the management of pharmacotherapy associated with therapeutic education in patients at cardiovascular risk (Doctoral Thesis). Seville: University of Seville; 2011. 195 p.
- Amariles, P., Pino, D., Sabater, D., Gacía-Jiménez, E., Roig, I., Faus, M.J. Reliability and external validity of a questionnaire to assess the knowledge about risk and cardiovascular disease in patients attending Spanish community pharmacies. Aten Primaria. 2016;48(9):586-95. [CrossRef]
- Morisky, D.E., Green, L.W., Levine, D.M. Concurrent and predictive validity of a self-reported measure of medication adherence. Med Care. 1986;24(1):67-74. [CrossRef]
- William McEvoy, J.; McCarthy C. P.; Bruno, R. M.; Brouwers S.; Canavan M. .D.; et al., ESC Scientific Document Group , 2024 ESC Guidelines for the management of elevated blood pressure and hypertension: Developed by the task force on the management of elevated blood pressure and hypertension of the European Society of Cardiology (ESC) and endorsed by the European Society of Endocrinology (ESE) and the European Stroke Organisation (ESO), European Heart Journal, 2024, 45 (38): 3912–4018. [CrossRef]
- Buenavida, P., De la Matta-Martín, M.J., De la Puerta, R., Martín-Calero, M.J. Design of an intervention protocol to be applied to cardiovascular risk patients cared for in the community pharmacy. Rev Esp Cien Farm. 2020;1(2):120-37.
- Gorostidi, M.; Gijón-Conde, T.; de la Sierra, A.; Rodilla, E.; Rubio, E.; Vinyoles, E. et al., Guía práctica sobre el diagnóstico y tratamiento de la hipertensión arterial en España, 2022. Sociedad Española de Hipertensión - Liga Española para la Lucha contra la Hipertensión Arterial (SEH-LELHA). [2022 Practice guidelines for the management of arterial hypertension of the Spanish Society of Hypertension]. [CrossRef]
- WHO. Obesity and overweight 2024. (Accessed 24 March 2024). Available online at: https://www.who.int/news-room/fact-sheets/detail/obesity-and-overweight.
- WHO Guidelines on physical activity and sedentary behaviour. 2022 November. (Accessed 24 March 2023). Available at: https://apps.who.int/iris/bitstream/handle/10665/336656/9789240015128-eng.pdf.
- Omboni, S.; Caserini, M. Effectiveness of pharmacist's intervention in the management of cardiovascular diseases. Open Heart. 2018; 5(1):e000687. [CrossRef]
- Alabkal, R.M.; Medlinskiene, K.; Silcock, J.; Graham, A. Impact of Pharmacist-Led Interventions to Improve Clinical Outcomes for Adults with Type 2 Diabetes at Risk of Developing Cardiovascular Disease: A Systematic Review and Meta-analysis. J Pharm Pract. 2023, 36(4):888-899. [CrossRef]
- Marques Santana, G., Stiefel Garcia-Junco, P., Pamies Andreu, E., Machuca Gonzalez, M., Martin Calero, M.J. Diseño e Implementacion de un Protocolo Asistencial en una Consulta de Cardiologia. Pharm. Care Esp. 2007; 9 (Sppl): 182.
- Artinian, N.T., Fletcher, G.F, Mozaffarian, D., Kris-Etherton, P., Van Horn, L., Lichtenstein, A.H., et al. Interventions to promote physical activity and dietary lifestyle changes for cardiovascular risk factor reduction in adults. A scientific statement from the American Heart Association. Circulation. 2010; 122 (4): 406-41. [CrossRef]
- Rodríguez-Chamorro, M.A., García-Jiménez, E., Amariles, P., Rodríguez-Chamorro, A., Pérez-Merino, E.M., Martínez-Martínez, F., et al. Effect of pharmacist involvement in adherence to medications in patients with high to moderate cardiovascular risk (Study EMDADER-CV-INCUMPLIMIENTO). Aten primaria. 2011; 43(5): 245-53. [CrossRef]
- Santos-Ramos, B., Otero López, M.J., Galván-Banqueri, M., Alfaro-Lara, E.R., Vega-Coca, M.D., Nieto-Martín, M.D., Ollero-Baturone, M. Modelos de atención al paciente pluripatológico y el papel de la farmacia hospitalaria [Health care models for patients with multiple chronic conditions and the role of the hospital pharmacy/the hospital pharmacist]. Farm Hosp. 2012 ;36(6):506-17. Spanish. [CrossRef]
- Zaij S, Pereira Maia K, Leguelinel-Blache G, Roux-Marson C, Kinowski JM, Richard H. Intervention of pharmacist included in multidisciplinary team to reduce adverse drug event: a qualitative systematic review. BMC Health Serv Res. 2023 Aug 30;23(1):927. [CrossRef] [PubMed] [PubMed Central]
- Ali, S.; Salahudeen, M.S.; Bereznicki, L.R.E.; Curtain, C.M. Pharmacist-led interventions to reduce adverse drug events in older people living in residential aged care facilities: A systematic review. Br J Clin Pharmacol. 2021, 87(10):3672-3689. [CrossRef]
- Tecklenborg, S.; Byrne, C.; Cahir, C.; Brown, L.; Bennett, K. Interventions to Reduce Adverse Drug Event-Related Outcomes in Older Adults: A Systematic Review and Meta-analysis. Drugs Aging. 2020, 37(2):91-98. Erratum in: Drugs Aging. 2020 Feb;37(2):147. [CrossRef]
- Varas-Doval, R., Gastelurrutia, M.A., Benrimoj, S.I., García-Cárdenas, V., Sáez-Benito, L., Martinez-Martínez, F. Clinical impact of a pharmacist-led medication review with follow up for aged polypharmacy patients: A cluster randomized controlled trial. Pharm Pract 2020; 18 (4): 2133-40. [CrossRef]
Table 1.
Sociodemographic characteristics of the sample. Control and intervention groups (CG, IG).
| CG (n:41) | IG (n:44) | ||
|---|---|---|---|
| n (%) | n (%) | ||
| Gender | Male | 18 (43.9%) | 26 (59.1%) |
| Female | 23 (56.1%) | 18 (40.9%) | |
| Education | Primary school | 14 (34.1%) | 14 (31.8%) |
| High school | 12 (29.3%) | 11 (25.0%) | |
| Without studies | 12 (29.3%) | 8 (18.2%) | |
| University studies | 3 (7.32%) | 11 (25.0%) | |
| Living at home | In company | 38 (92.7%) | 40 (90.9%) |
| Alone | 3 (7.32%) | 5 (9.09%) | |
| Age (mean± SD) | 61.1±10.1 | 61.6±10.3 |
SD: standard deviation.
Table 2.
Prevalence of CVRFs (%): Hypertension, diabetes mellitus, and dyslipidemia. Percentage of prevention groups (%). Mean baseline values (t0) of blood pressure (BP), biochemical parameters: TC, c-HDL, c-LDL, TG, HbA1c, and cardiovascular risk (CVR) (mean ±SD). Control and intervention groups (CG, IG).
Table 2.
Prevalence of CVRFs (%): Hypertension, diabetes mellitus, and dyslipidemia. Percentage of prevention groups (%). Mean baseline values (t0) of blood pressure (BP), biochemical parameters: TC, c-HDL, c-LDL, TG, HbA1c, and cardiovascular risk (CVR) (mean ±SD). Control and intervention groups (CG, IG).
| CG (n=41) | IG (n=44) | significance | |
|---|---|---|---|
| p-valor | |||
| Hypertension | 33 (80.5%) | 39 (88.6%) | 0.458 |
| SBP | 133±19.6 | 139±19.6 | 0.162 |
| DBP | 78.2±9.69 | 81.6±11.7 | 0.153 |
| Diabetes mellitus | 19 (46.3%) | 13 (29.5%) | 0.170 |
| HbA1c1 | 6.76±1.05 | 6.75±0.79 | 0.959 |
| HbA1c2 | 5.65±0.49 | 5.67±0.51 | 0.894 |
| Dyslipidemia | 30 (73.2%) | 26 (59.1%) | 0.255 |
| TC | 167±39.2 | 169±40.1 | 0.808 |
| c-HDL | 49.4±15.7 | 51.3±14.7 | 0.552 |
| c-LDL | 85.5±30.7 | 84.1±31.2 | 0.834 |
| TG | 173±67.0 | 170±88.7 | 0.852 |
| PreventionPrimary | 29 (70.7%) | 32 (72.7%) | 1.000 |
| Secondary | 12 (29.3%) | 12 (27.3%) | 1.000 |
| CVR | 1.69±1.07 | 2.56±2.18 | 0.050 |
CVRFs: Cardiovascular risk factors; CVR: Cardiovascular Risk; SD: Standard deviation; SBP:Systolic blood pressure; DBP:Diastolic blood pressure; TC:Total Cholesterol; c-HDL:High density cholesterol; c-LDL:Low density cholesterol; TG:Triglycerides; HbA1c1:Glycosylated hemoglobin in patients diagnosed with diabetes mellitus; HbA1c2:Glycosylated hemoglobin in undiagnosed patients with diabetes mellitus.
Table 3.
Prevalence of other CVRFs (%): grade of weight/obesity, sedentary lifestyle, and smoking habit. BMI values (mean±SD). Control and intervention groups (CG, IG).
Table 3.
Prevalence of other CVRFs (%): grade of weight/obesity, sedentary lifestyle, and smoking habit. BMI values (mean±SD). Control and intervention groups (CG, IG).
| CG(n=41) | IG(n=44) | significance | |
|---|---|---|---|
| n (%) | n (%) | p-valor | |
| Normal weight | 2 (4.88%) | 4 (9.09%) | 0.859 |
| Overweight grade I | 6 (14.6%) | 8 (18.2%) | |
| Overweight grade II | 11 (26.8%) | 8 (18.2%) | |
| Type I obesity | 11 (26.8%) | 13 (29.5%) | |
| Type II obesity | 6 (14.6%) | 7 (15.9%) | |
| Type III obesity | 5 (12.2%) | 3 (6.82%) | |
| Sedentariness | 21 (52.5%) | 24 (54.5%) | 1.000 |
| Ex-smoker | 17 (41.5%) | 19 (43.2%) | 0.878 |
| Smoker | 8 (19.5%) | 10 (22.7%) | |
| Non-smoker | 16 (39.0%) | 15 (34.1%) | |
| BMI (mean±SD) | 32.3±6.03 | 31.0±5.19 | 0.283 |
SD: Standard deviation; CVRFs: Cardiovascular risk factors; BMI: Body mass index.
Table 4.
Evolution of inter- and intra-group (CG and IG) comparison at baseline (t0) and final (t6) time during follow-up of biochemical parameters (CT, HDL-C, LDL-C, TG, HbA1c), body mass index (BMI) and cardiovascular risk (CVR), as well as the degree of knowledge about CVR and CVRFs (mean ±SD). Evolution of the prevalence of sedentary patients (%).
Table 4.
Evolution of inter- and intra-group (CG and IG) comparison at baseline (t0) and final (t6) time during follow-up of biochemical parameters (CT, HDL-C, LDL-C, TG, HbA1c), body mass index (BMI) and cardiovascular risk (CVR), as well as the degree of knowledge about CVR and CVRFs (mean ±SD). Evolution of the prevalence of sedentary patients (%).
| t0 | t6 | Difference | ||||||
|---|---|---|---|---|---|---|---|---|
| CG | IG | CG | IG | CG | IG | p-valor | n | |
| SBP | 133±19.6 | 139±19.6 | 130±16.8 | 130±15.5 | -2.32±12.4 | -8.84 ±16.0 | 0.038 | 85 |
| DBP | 78.2±9.69 | 81.6±11.7 | 78.2±9.83 | 80.9±21.3 | 0.02±7.52 | -0.68±18.7 | 0.818 | 85 |
| TC | 167±39.2 | 169±40.1 | 181±37.5 | 171±34.6 | 12.1±30.7 | 2.09±24.7 | 0.109 | 83 |
| c-HDL | 49.4±15.7 | 51.3±14.7 | 51.6±14.1 | 51.5±14.2 | 3.54±11.1 | 1.30±9.11 | 0.314 | 85 |
| c-LDL | 85.5±30.7 | 84.1±31.2 | 93.9±34.4 | 87.6±30.0 | 7.12±24.2 | 2.43±22.4 | 0.366 | 82 |
| TG | 173±67.0 | 170±88.7 | 177±70.5 | 159±87.2 | 2.20±58.9 | -10.30±103 | 0.497 | 83 |
| HbA1c1 | 6.76±1.05 | 6.75±0.79 | 7.03±0.98 | 6.65±0.96 | 0.27±0.76 | -0.10±0.84 | 0.222 | 31 |
| HbA1c2 | 5.65±0.49 | 5.67±0.51 | 5.64±0.46 | 5.65±0.96 | -0.03±0.31 | 0.00±0.28 | 0.777 | 52 |
| BMI | 32.3±6.03 | 31.0±5.19 | 32.1±6.30 | 30.8±5.25 | -0.21±0.89 | -0.22±1.01 | 0.980 | 85 |
| CVR | 1.69±1.07 | 2.56±2.18 | 1.69±1.00 | 1.91±1.42 | -0.07±0.46 | -0.78±1.16 | 0.003 | 61 |
| Degree of knowledge | 4.39±1.45 | 3.98±1.44 | 4.66±1.32 | 8.00±0.00 | 0.27±0.95 | 4.02±1.44 | <0.001 | 85 |
| Sedentariness (%) | 21 (52.5%) | 24 (54.5%) | 26(65.0%) | 7 (15.9%) | <0.001 | 84 | ||
Table 5.
Percentage of patients who, according to their clinical condition, reach the target figures for the control of each of the parameters related to CVRF: SBP, DBP, HDL-C, LDL-C, TG, HbA1c, BMI. Control and intervention groups (CG, IG).
Table 5.
Percentage of patients who, according to their clinical condition, reach the target figures for the control of each of the parameters related to CVRF: SBP, DBP, HDL-C, LDL-C, TG, HbA1c, BMI. Control and intervention groups (CG, IG).
| CG | CG | Difference | IG | IG | Difference | |
|---|---|---|---|---|---|---|
| n=41 | n=41 | Δ (t6-t0) | n=44 | n=44 | Δ (t6-t0 ) | |
| t0 | t6 | t0 | t6 | |||
| SBP | 26 (63.4%) | 30 (73.2%) | 9.8% | 23 (52.3%) | 35 (79.5%) | 27.2% |
| DBP | 36 (87.8%) | 36 (87.8%) | 0.0% | 34 (77.3%) | 37 (84.1%) | 6.8% |
| c-HDL | 27 (67.5%) | 31 (75.6%) | 8.1% | 33 (76.7%) | 35 (79.5%) | 2.8% |
| c-LDL | 21 (52.5%) | 15 (36.6%) | -15.9% | 21 (48.8%) | 20 (45.5%) | -3.3% |
| TG | 16 (40.0%) | 15 (36.6%) | -3.4% | 22 (51.2%) | 28 (63.6%) | 12.4% |
| HbA1c | 19 (47.5%) | 21 (51.2%) | 3.7% | 28 (65.1%) | 29 (65.9%) | 0.8% |
| BMI | 2 (4.88%) | 3 (7.32%) | 1.77% | 4 (9.09%) | 5 (11.4%) | 2.3% |
CVRFs:Cardiovascular risk factors; SBP:Systolic blood pressure; DBP:Diastolic blood pressure; c-HDL-High density cholesterol; c-LDL-Low density cholesterol; TG:Triglycerides; HbA1c-Glycosylated hemoglobin; BMI: Body Mass Index.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



