
Submitted:
12 December 2024
Posted:
12 December 2024
You are already at the latest version
Preprints on COVID-19 and SARS-CoV-2
Abstract
Background: Studies have highlighted long-term respiratory muscle dysfunction in COVID-19 survivors, although the underlying risk factors remain unclear. This single-center study assessed respiratory muscle function and individual associated factors at follow-up in patients hospitalised with COVID-19 and related acute respiratory failure.
Methods: Data were collected for consecutive patients, aged ≥18 years, at the post-COVID outpatient service of Hospital Policlinico in Modena (Italy) in the time frame of 3 to 6 months after discharge. Data were analysed using single and multiple logistic regression model. Correlation between MIP/MEP, hand-grip values and lung function were further explored.
Results: Out of 223 patients (mean age 67 years, 69% male) 121 (54.3%) exhibited MIP or MEP dysfunction which was found to be associated with use of non-invasive ventilation (OR=1.93 [1.08–3.52], p=0.03) and female gender (OR=1.96 [1.1–3.57], p=0.03) as indipendent risk factors. A positive correlation was observed between MIP dysfunction and hand-grip strength (p=0.03 and 0.01), whereas both MIP and MEP were significantly associated with FEV1, FVC, TLC, and DLCO.
Conclusions: Respiratory muscle dysfunction is consistently prevalent and parallels peripheral muscle weakness and lung fuction level in patients at follow up after severe COVID-19. The need for non-invasive ventilation during the acute phase and female gender might represent risk factors. MIP/MEP assessment should be recommended to observe respiratory muscle dysfunction in severe post-COVID survivors.
Keywords:
post-COVID
; Maximal Inspiratory Pressure (MIP)
; Maximal Expiratory Pressure (MEP)
; Hand-Grip Strength
; Lung function
; Non-invasive ventilation
1. Introduction
The Coronavirus disease 2019 (COVID-19) pandemic was declared on March 11, 2020 from the World Health Organization (WHO) and had an unprecedented impact on global health in terms of morbidity and mortality. Beyond 7,065,880 deaths confirmed in September 2024,[1] it is known that the symptoms of COVID-19 can range from asymptomatic to life threatening.[2] People experience a wide range of symptoms including fever, dry cough, shortness of breath, muscle pain, and fatigue, although most infections are not severe and people are able to recover at home without hospital treatment. Where the novel Coronavirus causes severe illness, the commonest clinical presentation is bilateral pneumonia leading to hypoxemia with acute respiratory failure. Individuals getting moderate to severe respiratory failure require hospital admission with need of respiratory support, such as oxygen therapy and/or non-invasive ventilation (NIV).
A significant proportion of patients post COVID-19, particularly those with severe acute disease, may experience persistent symptoms with poor quality of life following recovery from the viral infection. Increasing evidence of post-COVID long-term effects following hospitalisation has been reported in literature. Clusters of symptoms including dyspnea, fatigue, muscle pain, and sleep disturbances have been frequently described and indicated new disability.[3,4]
Considering that SARS-CoV-2 is a virus spreading to multiple organs other than lungs, it has been proposed that the COVID-related cytokine storm may cause dysfunction to the respiratory muscles (RM), especially the diaphragm.[5,6] On the other hand, critical illness myopathy is associated with prolonged mechanical ventilation and patient immobilisation that are risk factors for complications such as peripheral muscle weakness and RM dysfunction.[7,8] Skeletal muscle is one of the most involved organs in COVID-19. Myalgia and fatigue are the third most reported symptoms (after fever and cough) in people with symptomatic infection.[9]
The relationship between COVID-19 and changes in RM and the resulting functional implications have not been yet completely understood in individuals without pre-existing conditions associated with RM dysfunction. In this study, we aimed to explore: 1) long-term RM function in patients previously hospitalised for COVID-19; 2) factors associated with RM dysfunction, and association of MIP/MEP levels with the follow up variables.
2. Materials and Methods
Study Design
We established a post-COVID follow up service at the Outpatient Department of Hospital Policlinico in Modena (Italy), for patients admitted with COVID-19 since the first wave of the pandemic. The primary setting that provided patient assessment was a multidisciplinary referral centre for post-Acute COVID syndrome at the Infectious Disease Unit and secondly, at the Respiratory Unit. We aimed to follow up all patients in-person after discharge and collected data also to identify people presenting with any persistent symptom. This study is an observational single-centre cohort study that has been designed and carried out in those patients who attended the service solely 3 to 6 (three-to-six) months after discharge. All visits were conducted into an optimal time window.
Participants
All consecutive patients referred to the post-COVID service between June 2020 and October 2021, aged ≥18 years, with a minimum 7-day length of hospital stay, were systematically included. Exclusion criteria were pre-admission diagnosis of chronic conditions potentially affecting RM function such as asthma, COPD, ILD, coronary artery disease and/or chronic heart failure, cardiomyopathies, and neuromuscular diseases. Nursing home residents were excluded due to difficulty of attending follow up appointments. Patients not able to perform lung function test and hand-grip test were also excluded.
Procedures
Variables and Outcomes
Variables
Variables collected at follow up included: age; sex; smoking status (never, previous, or current); pre-admission Body Mass Index (BMI); respiratory support (Non-Invasive Ventilation (NIV); high-flow nasal cannula (HFNC) oxygen therapy; intubation); use of Dexamethasone; use of any other systemic corticosteroid; use of Tocilizumab; O2 at discharge; length of stay in hospital (LOS) and in Intensive Care Unit (ICU); time from discharge to follow up; pulmonary function parameters, DLCO, MIP and MEP; skeletal muscle strength of the hand; and dyspnea scale. Data collection was completed by patient clinical records (case notes and electronic records) and drug prescription charts. All data entered into a specific database.
Outcomes
The primary aim was to explore the prevalence of Maximal Inspiratory Pressure (MIP) and Maximal Expiratory Pressure (MEP) dysfunction in COVID-19 survivors, according to the age-adjusted lower threshold from Lista-Paz 2023.[13] The secondary outcomes were: 1) MIP/MEP dysfunction related risk factors; 2) association of MIP/MEP levels with the follow up variables. The peripheral muscle dysfunction was defined as reduction in dominant hand grip strength under 25th percentile (age- and sex-adjusted value).[14] The lung volume reduction was defined either as restrictive pattern (TLC <90% of predicted value) or reduced lung diffusion capacity (DLco <80% of predicted value). A self-reported symptom of dyspnea according to mMRC scale score ≥ 1 indicated the presence of breathlessness.[15] Outcomes were assessed up to last data entry using systems of prospective follow-up and electronic health records.
Data Analysis
A priori sample size calculation on the primary outcome was based on the reported prevalence of MIP/MEP dysfunction among critically ill patients ranging 50-80%. 16-18] Assuming α = 0.05 and power of 85 and a margin of error of 5%, a sample size of 223 patients was suitable for assessing the primary outcome. Data were displayed as median and interquartile range (IQR) for continuous variables and numbers and percentages for dichotomous variables. Continuous variables were compared by Student’s t-test or Mann-Whitney test as appropriate. Categorical variables were expressed as numbers and percentages (%) and compared by χ2 test or Fisher’s exact test across the groups. The association with MIP/MEP dysfunction was analysed using a univariate single logistic regression model and a multiple logistic regression model to explore independent associations for selected variables. Sensitivity analysis was used to examine the correlation between the values of MIP and MEP (expressed as % of predicted values) and hand-grip values and pulmonary function parameters (namely TLC, FEV1, FVC and DLCO). Pearson’s R or Spearman correlation coefficient were used as appropriate. Statistical analysis was performed using SPSS package ver.25.0 (IBM Corp., Armonk-NY, USA) and GraphPad Prism version 8.0 (GraphPad Software, Inc., La Jolla, Ca, USA) unless otherwise indicated.
3. Results
Between June 2020 and October 2021, 719 participants with COVID-19 were assessed at the follow up service. Of these, 496 were excluded based on the study criteria, missing data and follow up time not ranging within 3-6 months. The study included 223 patients. The time from discharge to follow up was 4 ±1.1 months (mean±SD). Demographic and clinical variables are shown in Table 1. Overall, the mean age was 67 years with a greater proportion of men (69%). The mean BMI was 30. On admission, conventional oxygen therapy (COT) was used in 24%, HFNC oxygen therapy in 27%, NIV in 33%. Intubation rate was 16% (36/223). Missing data accounted for less than 3% of the dataset.

Table 1.
Sample characteristics and hospital admission factors of patients attending follow up by MIP/MEP dysfunction.
Table 1.
Sample characteristics and hospital admission factors of patients attending follow up by MIP/MEP dysfunction.
| Overall n = 223 (100) | MIP/MEP abnormal values * n=121 (54.2) |
MIP/MEP normal values * n=102 (45.8) |
p value | |
|---|---|---|---|---|
| Demographics | ||||
| Age, years [IQR] | 67 (57 – 75) | 67 (59 – 74) | 65 (55 – 75) | 0.11 |
| Male gender, no. [%] | 153 (68.6) | 76 (62.8) | 77 (75.5) | 0.04 |
| Ethnicity | ||||
| Caucasian, n [%] | 218 (97.8) | 118 (97.5) | 100 (98) | 0.99 |
| Black, n [%] | 4 (1.8) | 2 (1.7) | 2 (2) | 0.99 |
| Asian, n [%] | 1 (0.4) | 1 (0.8) | 0 (0) | 0.99 |
| Smoking history | ||||
| Current smoker, no. [%] | 2 (0.9) | 1 (0.8) | 1 (1) | 0.99 |
| Former smoker, no. [%] | 88 (39.5) | 51 (42.1) | 37 (36.2) | 0.41 |
| Non-smoker, no. [%] | 133 (59.6) | 69 (57) | 64 (62.7) | 0.41 |
| BMI (pre-admission), median [IQR] | 30 (27 – 34) | 30 (27 – 34) | 30 (27 – 34) | 0.64 |
| BMI >30, no. [%] | 121 (54.3) | 68 (56.2) | 53 (52) | 0.21 |
| Outcomes | ||||
| LOS, days [IQR] | 14 (10 – 21) | 15 (11 – 23.5) | 13 (9 – 19.3) | 0.14 |
| Respiratory support | ||||
| HFNC, no. [%] | 60 (26.9) | 32 (26.4) | 28 (27.5) | 0.88 |
| NIV, no. [%] | 74 (33.2) | 48 (39.7) | 26 (25.5) | 0.03 |
| Intubation/MV, no. [%] | 36 (16.1) | 21 (17.4) | 15 (14.7) | 0.72 |
| Use of Tocilizumab | 150 (67.3) | 79 (65.3) | 71 (69.6) | 0.47 |
| Use of Dexamethasone | 67 (30) | 37 (16.6) | 30 (13.4) | 0.88 |
| Use of other corticosteroids (oral/IV) | 134 (60.1) | 73 (60.3) | 61 (59.8) | 0.99 |
| O2 at discharge, no. [%] | 32 (14.3) | 19 (15.7) | 13 (12.75) | 0.57 |
| Follow up | ||||
| Dyspnea grade (mMRC), median [IQR] | 0 (0 – 1) | 0 (0 – 1) | 0 (0 – 1) | 0.09 |
| Dyspnea as mMRC ≥ 1, no. [%] | 67 (30) | 39 (32.2) | 28 (27.5) | 0.46 |
| FEV1/FVC, % [IQR] | 82 (78 – 85.7) | 81.8 (78.7 – 86.3) | 82.1 (78.1 – 85.1) | 0.78 |
| TLC, %pred [IQR] | 105 (94 – 116) | 101 (91.5 – 113) | 107.5 (96.8 – 117) | 0.06 |
| TLC <90%pred, no. [%] | 38 (17) | 27 (22.3) | 11 (10.8) | 0.03 |
| DLCO, %pred [IQR] | 77 (67 – 87) | 75 (64.5 – 86) | 79.5 (68 – 92.3) | 0.02 |
| DLCO <80%pred, no. [%] | 128 (57.4) | 77 (63.6) | 51 (50.5) | 0.06 |
| MIP, %pred [IQR] | 84 (66 – 104) | 68 (58 – 73) | 102 (90 – 120) | <0.0001 |
| MEP, %pred [IQR] | 82 (62 – 93) | 65 (54 – 72) | 96 (88 – 101) | <0.0001 |
| Reduced strength in dominant hand, no. [%] | 60 (26.9) | 40 (33.1) | 20 (19.6) | 0.034 |
| Reduced strength in right hand, no. [%] | 68 (30.5) | 46 (38) | 22 (21.6) | 0.01 |
| Reduced strength in left hand, no. [%] | 77 (34.5) | 46 (38) | 31 (30.4) | 0.26 |
Abbreviations: BMI, body mass index; LOS, Length of stay; mMRC, modified Medical Research Council; FEV1, Forced Expiratory Volume in 1 Second; FVC, Forced Vital Capacity; TLC, Total Lung Capacity; DLCO, Diffusing capacity of the Lungs for Carbon monoxide; MIP, Maximal Inspiratory Pressure; MEP, Maximal Expiratory Pressure *Lista-Paz A et al. Arch Bronconeumol 2023; 59(12):813-820. [13].
3.1.1. Prevalence of MIP/MEP Dysfunction and Related Risk Factors
Reduction in MIP or MEP was found in 54.2% of patients (Table 1). In the multiple logistic regression model, MIP or MEP dysfunction showed positive association with use of NIV (p = 0.03) and female gender (p = 0.03) (Table 2).
Table 2.
Raw and independent association between clinical variables and MIP/MEP dysfunction at follow-up according to Lista-Paz A et al 2023.[13].
Table 2.
Raw and independent association between clinical variables and MIP/MEP dysfunction at follow-up according to Lista-Paz A et al 2023.[13].
| Univariable | Multivariable | |||||
|---|---|---|---|---|---|---|
| Parameter | OR | 95% Confidence Interval | p value | OR | 95% Confidence Interval | p value |
| Age | 1.02 | 0.99 – 1.04 | 0.12 | |||
| Female sex | 0.54 | 0.3 – 0.98 | 0.04 | 0.51 | 0.28 – 0.91 | 0.03* |
| Smoking status (active/former) | 1.19 | 0.91 – 1.55 | 0.20 | |||
| BMI | 1.01 | 0.96 – 1.07 | 0.64 | |||
| BMI ≥ 30 kg/m2 | 1.19 | 0.7 – 2 | 0.53 | |||
| Hospital length of stay | 1.01 | 0.99 – 1.03 | 0.15 | |||
| HFNC | 0.95 | 0.52 – 1.93 | 0.87 | |||
| NIV | 1.79 | 1.01 – 3.22 | 0.04 | 1.93 | 1.08 – 3.52 | 0.03* |
| Intubation/MV | 1.22 | 0.59 – 2.54 | 0.59 | |||
| Use of Dexamethasone | 1.06 | 0.59 – 1.6 | 0.85 | |||
| Use of other corticosteroids | 1.02 | 0.6 – 1.75 | 0.94 | |||
| Use of Tocilizumab | 0.82 | 0.47 -1.44 | 0.49 | |||
Association is shown through odds ratio (OR) and 95%CI. Abbreviations: OR, odds ratio; IQR, InterQuartile Range; HFNC, high-flow nasal cannula oxygen therapy; NIV, non-invasive ventilation; MV, mechanical ventilation; BMI, body mass index.
3.1.2. Correlation Between MIP/MEP, Peripheral Muscle Function, Lung Function, and Dyspnea
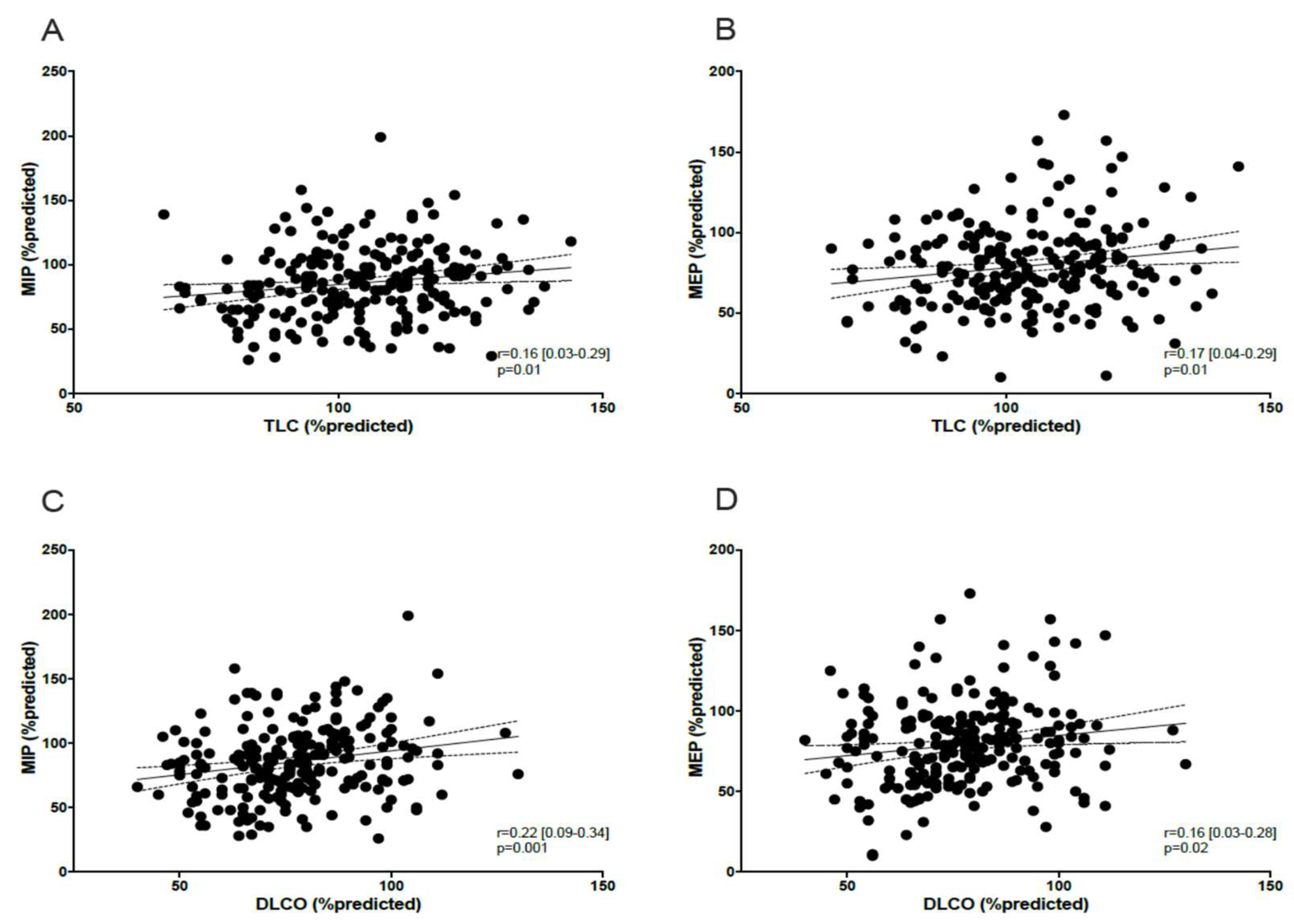
Reduction in dominant hand grip strength (in kg) was observed in 27% of patients (Table 1). Using the Pearson correlation coefficient test, right and left hand grip strength was associated with MIP dysfunction (p = 0.03 and 0.01, respectively) (Figure 1). None of the patients showed obstructive pattern on spirometry (FEV1/FVC <0.7). Restrictive pattern (TLC <90% pred) was observed in 17% of patients and reduced lung diffusing capacity (DLCO <80% pred) was found in 57.4% (128 participants). All patients presenting restrictive pattern on spirometry showed reduction in DLCO. MIP and MEP were significantly correlated with lung function level (Figure 2) and DLCO (Figure 3). mMRC ≥ 1 grade was reported in 67/223 patients (30%) (Table 1), and no association was found with RM dysfunction.
Figure 1.
Correlation between MIP/MEP and hand-grip strength.
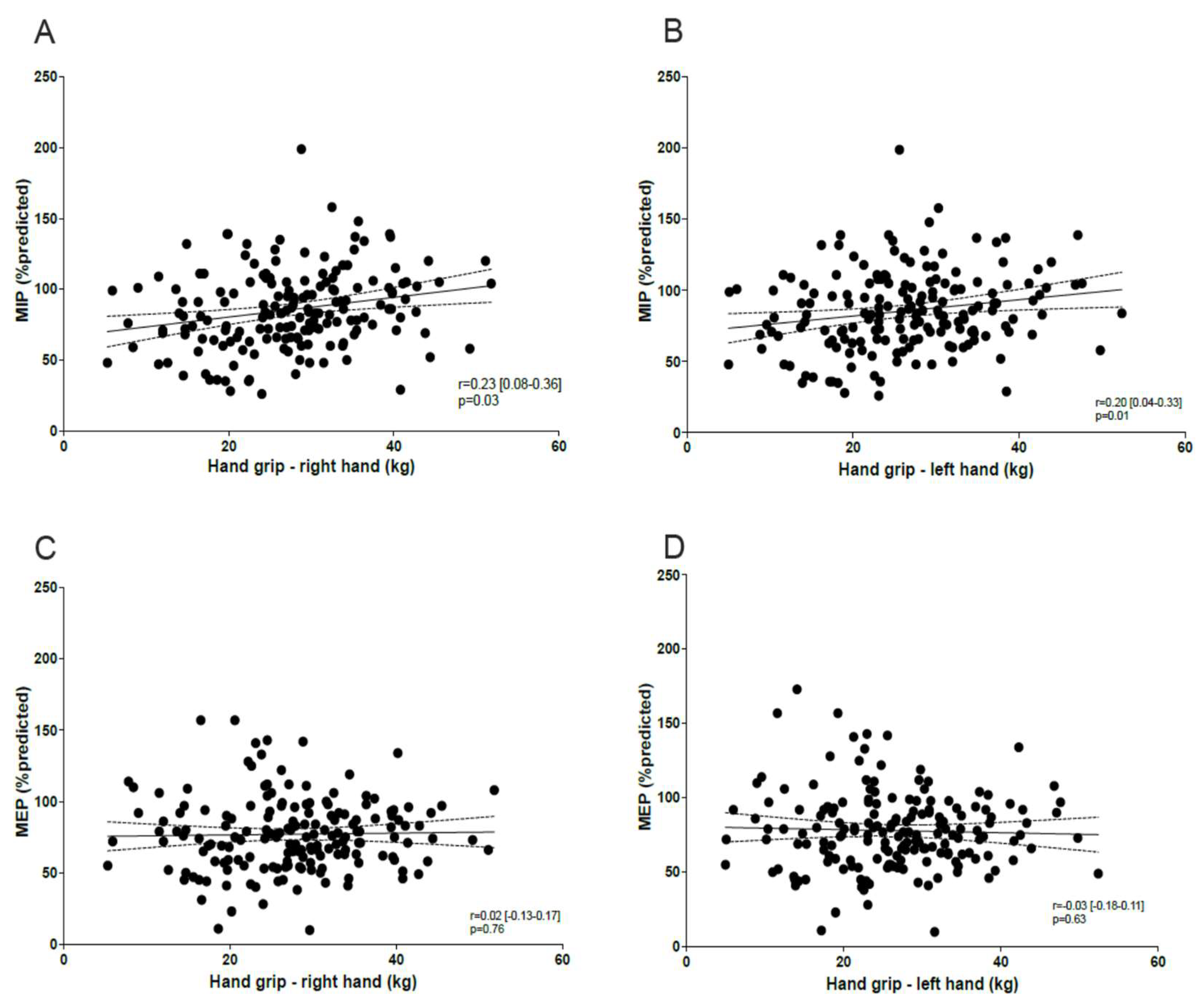
Figure 2.
Correlation between MIP/MEP and FEV1 and FVC values.
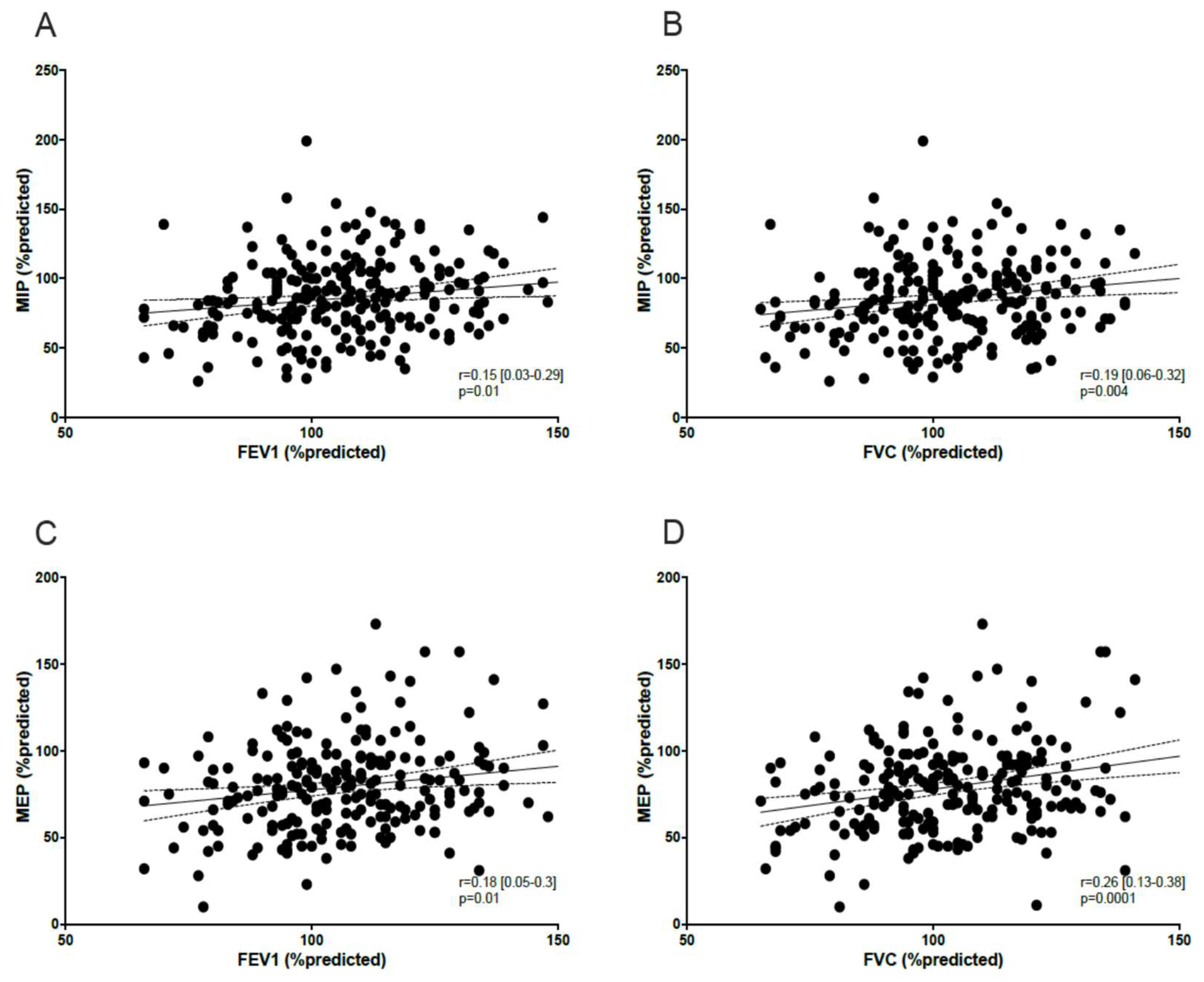
Figure 3.
Correlation between MIP/MEP and TLC and DLCO values.
4. Discussion
In this cohort study of 223 patients hospitalised with severe COVID-19, we found MIP or MEP dysfunction in 54.2% of participants at follow-up ranging from 3 to 6 months, excluding those with pre-existing pulmonary, cardiac, and neuromuscular comorbidities.
The study adds to evidence base evaluating RM function in COVID-19 survivors.[19,20,21] One previous study found a reduction of MIP and MEP in 49.1% and 22.8% respectively among slightly younger patients at 1 month from hospital discharge,[19] and no correlation was observed with use of corticosteroids or severe COVID. That population was characterised by 30% of severe cases without underlying pulmonary and cardiovascular disease. Correspondingly, we also did not find any association with glucocorticoid therapy and/or illness severity or intubation. Another study demonstrated greater decrease of MIP (27%) than MEP at the same timepoint in patients who presented higher intubation rate (40%) and pre-admission lung disease (29%).[20] A multicentric study showed MIP reduction even 30 months following hospitalisation for severe COVID-19 in younger patients, after excluding chronic diseases that lead to RM dysfunction.[21] Whilst the authors did not report data on intubation or mechanical ventilation, these findings were associated with prolonged hospital stay and age. Our findings are consistent with previous data on medium- and long-term outcomes regarding RM dysfunction in individuals exposed to severe COVID-19 but without underlying RM-affecting diseases.
As MIP has a strong relationship with strength of the diaphragm that is the major inspiratory muscle, a few studies also included diaphragm ultrasound measurements following ICU admission due to COVID-19. One study, considering inspiratory muscle normal thresold level as MIP > 70% predicted, confirmed that mechanically ventilated COVID-19 survivors had overall dysfunction at 3 (48%) and 6 (24%) months but not any specific diaphragm dysfunction.[8] Contrastingly, one complex study demonstratred a diaphragm dysfunction in 80% of patients not requiring mechanical ventilation, at 15 months.[22] Another study showed a significant reduction in diaphragm contractility in COVID-19 survivors.[23] The persistence of MIP reduction in our population highlights the substantial impact of severe COVID-19 on inspiratory muscle function, even in the absence of prolonged mechanical ventilation or other established contributors to RM impairment.
This impairment is likely to be linked to a combination of factors, including systemic inflammation, microvascular damage, and critical illness myopathy. Additionally, mechanisms such as ventilator-induced diaphragm dysfunction and oxidative stress may further impair contractility and strength. Unlike MEP, MIP appears particularly vulnerable due to the diaphragm’s central role in respiration and its heightened sensitivity to systemic and illness-related factors.
We also found that MIP/MEP dysfunction was associated with the use of NIV as an independent risk factor. Prolonged NIV use may contribute to diaphragmatic deconditioning, promoting long-term impairment as a result. Interestingly, the number of patients with reduced MIP or MEP exceeded those requiring NIV (33%) or intubation (16%). Whilst ICU admission and mechanical ventilation, which can lead to critical illness myopathy,[8,24] may explain RM dysfunction in some severe COVID-19 cases, the persistence of MIP reduction in non-hospitalised patients or those requiring no respiratory support, as observed in our study, requires further investigation. Evidence on RM dysfunction in survivors, regardless of mechanical ventilation status, remains inconclusive. Factors such as ageing and its associated decline in respiratory muscle performance may also play a role.[25]
In our study, mechanical ventilation was not associated with RM dysfunction, whereas NIV was—a difference that may be attributed to survivorship bias. Many intubated patients did not survive, excluding the most severe cases from follow-up analysis, whereas in contrast NIV patients, unless under therapeutic ceiling, were more likely to survive and be included. This overrepresentation of NIV patients amplifies its apparent statistical association with RM dysfunction, underscoring the need for cautious interpretation of these findings.
We also found that female gender was an independent risk factor for reduced MIP or MEP. This finding is in line with recent literature showing that females had a marked reduction in MIP,[21] even in women not admitted to hospital for COVID at 5 months following discharge.[26] Although the role of gender shoud be further clarified, Hennigs et al [26] and Steinbeis et al [27] demonstrated that all patients with RM dysfunction were also symptomatic at follow up. RM reduction was associated with dyspnea and fatigue after 3-8 months, irrespective of hospitalisation, admission to ICU, or need for oxigen.[27] Nonetheless, when we assessed breathlessness, the prevalence of mMRC score ≥1 (as clinically symptom presence) was 30% and not to be related to RM dysfunction. These findings of dyspnea are consistent with literature on large populations of post-COVID patients, showing a prevalence ranging from 20% to 43% in the time frame of 2-8 months follow up.[28,29,30,31,32]
We also found that hand-grip strength was lower in 27% of patients, similarly to the study of Johnsen et al. (28%) who reported a prevalence of 28% at 3 months, regardless of hospitalisation, though a higher prevalence among admitted patients (32%).[33] In contrast, Godoy et al. observed only 14% of reduced hand-grip strength at 4 months,[34] while Hussain et al. reported a prevalence of 24% among ICU-admitted patients after 1 year.[35] Unlike these studies, our cohort excluded patients with relevant comorbidities. Although we cannot confirm normal hand-grip strength prior to hospitalisation, the observed changes in peripheral muscle strength were likely due to to SARS-CoV-2 infection. In addition, both right and left hand-grip strength were associated with MIP dysfunction in our cohort, suggesting a relationship between peripheral and respiratory muscle function. Whilst the lack of association between MEP and skeletal muscle strength might seem controversial, our findings highlight that peripheral muscle function and RM function are related each other, which is in line with data reporting parallel dysfunction in older healthy individuals.[36] In addition, one previous study showed that both older age and obesity were linked to low muscle quality index - including hand-grip strength as a component - and concomitant reduction of MIP/MEP at 3 months after admission for COVID-19.[37] These data further support the interrelationship between peripheral and respiratory muscle dysfunction in post-COVID.
We also found a mild reduction in DLCO in 57% of patients. This was expected as a potential residual lung damage following extensively acute lung involvement. Our findings are in line with previous studies. A systematic review confirmed that reduced DLCO was the most frequent residual functional abnormality with a prevalence of 39% at 6 months after recovery.[38] One study showed a higher prevalence of DLCO reduction (76.5%) in 30-day follow up,[19] whereas another reported comparable rates to our findings in patients treated with HFNC, NIV or intubation at 6 months. In contrast, a lower prevalence (29%) was found in patients requiring only COT.[31] We also observed that DLCO was reduced in patients showing restrictive pattern on spirometry (17%), in line with literature data.[27] Additionally, MIP/MEP values were globally associated with the lung function parameters (FEV1, FVC, TLC, and DLCO) at follow up. However, the impact of these findings in people without chronic diseases potentially affecting pulmonary function remains poorly understood. Generally, published research in COVID-19 survivors showed that DLCO is the most accurate respiratory functional parameter,[19,27,31,38,39,40] which should be monitored in post-COVID population.
It is worth noting that our study is single-centre. The population included is reflective of the wider post-COVID populations during the first waves of the pandemic [2,41] but might not reflect those of different contexts.
Further limitations of note were that we did not collect imaging data examining extension of lung abnormalities such as chest CT that could explore the relationship with functional data, and real-time diaphragm ultrasound in patients with MIP dysfunction. Nonetheless, excluding patients with pre-existing respiratory/cardiac or neuromuscular diseases helped to better evaluate the impact of the viral pneumonia on RM function, lung function, and dyspnea in absence of potential confounding factors.
5. Conclusions
The study assessed RM strength in COVID-19 survivors and showed that most people had RM dysfunction at follow up. Whilst the direct effect of SARS-CoV-2 on RM needs further research, these findings support the introduction of MIP/MEP measurement as screening for RM dysfunction at post-COVID follow up, regardless of symptoms, and consideration of RM training [42] in patients identified as having moderate to severe dysfunction.[25,43]
Author Contributions
Alessia Verduri: Conceptualisation; Data curation; Methodology; Investigation; Supervision; Writing – original draft; Writing – review and editing. Roberto Tonelli: Formal analysis; Method-ology; Software; Validation; Writing – review and editing. Pierluigi Donatelli: Data curation; Writing – review and editing. Jonathan Hewitt: Methodology; Supervision; Writing – review and editing. Giovanni Guaraldi: Writing – review and editing. Jovana Milić: Writing – review and editing. Valentina Ruggieri: Project administration; Writing – review & editing. Cristina Mussini: Writing – review and editing. Enrico Clini: Methodology; Supervision; Validation; Writing – review and editing. Bianca Beghé: Methodology; Supervision; Writing – review and editing. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
Ethical review and approval were waived for this study due to the retrospective anonymised data analysis.
Informed Consent Statement
Not applicable.
Data Availability Statement
The dataset used and analysed during the study is available from the corresponding author on reasonable request and with ethical permission.
Acknowledgements
The Authors thank Ms. Elisabetta Adami for lung function and MIP/MEP measurements.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- World Health Organisation. Coronavirus disease (COVID-19) situation reports. Available from: https://www.who.int/emergencies/diseases/novel-coronavirus-2019/situation-reports Accessed: 29th September 2024.
- Huang C, Wang Y, Li X, Ren L, Zhao J, Hu Y, Zhang L, Fan G, Xu J, Gu X, Cheng Z, Yu T, Xia J, Wei Y, Wu W, Xie X, Yin W, Li H, Liu M, Xiao Y, Gao H, Guo L, Xie J, Wang G, Jiang R, Gao Z, Jin Q, Wang J, Cao B. Clinical features of patients infected with 2019 novel coronavirus in Wuhan, China. Lancet 2020; 395(10223): 497-506. [CrossRef]
- COVID-19 rapid guideline: managing the long-term effects of COVID-19. National Institute for Health and Care Excellence (NICE), Scottish Intercollegiate Guidelines Network (SIGN) and Royal College of General Practitioners (RCGP). NICE guideline [NG188] Published: Last updated: 11 November 2021. https://www.nice.org.
- Nalbandian A, Sehgal K, Gupta A, Madhavan MV, McGroder C, Stevens JS, Cook JR, Nordvig AS, Shalev D, Sehrawat TS, Ahluwalia N, Bikdeli B, Dietz D, Der-Nigoghossian C, Liyanage-Don N, Rosner GF, Bernstein EJ, Mohan S, Beckley AA, Seres DS, Choueiri TK, Uriel N, Ausiello JC, Accili D, Freedberg DE, Baldwin M, Schwartz A, Brodie D, Garcia CK, Elkind MSV, Connors JM, Bilezikian JP, Landry DW, Wan EY. Post-acute COVID-19 syndrome. Nat Med 2021; 27(4):601-615. [CrossRef]
- Mittal A, Dua A, Gupta S, Injeti E. A Research Update: Significance of Cytokine Storm and Diaphragm in COVID-19. Curr Res Pharm Drug Discov 2021; 2:100031. [CrossRef]
- Cesanelli L, Satkunskiene D, Bileviciute-Ljungar I, Kubilius R, Repečkaite G, Cesanelli F, Iovane A, Messina G. The possible impact of COVID-19 on respiratory muscles structure and functions: a literature review. Sustainability 2022; 14:7446. [CrossRef]
- Cacciani N, Skärlén Å, Wen Y, Zhang X, Addinsall AB, Llano-Diez M, Li M, Gransberg L, Hedström Y, Bellander BM, Nelson D, Bergquist J, Larsson L. A prospective clinical study on the mechanisms underlying critical illness myopathy-A time-course approach. J Cachexia Sarcopenia Muscle 2022; 13(6):2669-2682. [CrossRef]
- Núñez-Seisdedos MN, Valcárcel-Linares D, Gomez-Gonzalez MT, Lazaro-Navas I, Lopez-Gonzalez L, Pecos-Martin D, Rodriguez-Costa I. Inspiratory muscle strength and function in mechanically ventilated COVID-19 survivors 3 and 6 months after intensive care unit discharge. ERJ Open Res 2023; 9(1):00329-2022. [CrossRef]
- Nasiri MJ, Haddadi S, Tahvildari A, Farsi Y, Arbabi M, Hasanzadeh S, Jamshidi P, Murthi M, Mirsaeidi M. COVID-19 clinical characteristics, and sex-specific risk of mortality: systematic review and meta-analysis. Front Med 2020; 7:459. [CrossRef]
- Miller MR, Hankinson J, Brusasco V, Burgos F, Casaburi R, Coates A, Crapo R, Enright P, van der Grinten CP, Gustafsson P, Jensen R, Johnson DC, MacIntyre N, McKay R, Navajas D, Pedersen OF, Pellegrino R, Viegi G, Wanger J; ATS/ERS Task Force. Standardization of spirometry. Eur Respir J 2005; 26(2):319-338. [CrossRef]
- Pellegrino R, Viegi G, Brusasco V, Crapo RO, Burgos F, Casaburi R, Coates A, van der Grinten CP, Gustafsson P, Hankinson J, Jensen R, Johnson DC, MacIntyre N, McKay R, Miller MR, Navajas D, Pedersen OF, Wanger J. Interpretative strategies for lung function tests. Eur Respir J 2005; 26(5):948-968. [CrossRef]
- Laveneziana P, Albuquerque A, Aliverti A, Babb T, Barreiro E, Dres M, Dubé BP, Fauroux B, Gea J, Guenette JA, Hudson AL, Kabitz HJ, Laghi F, Langer D, Luo YM, Neder JA, O'Donnell D, Polkey MI, Rabinovich RA, Rossi A, Series F, Similowski T, Spengler CM, Vogiatzis I, Verges S. ERS statement on respiratory muscle testing at rest and during exercise. Eur Respir J 2019; 53(6):1801214. [CrossRef]
- Lista-Paz A, Langer D, Barral-Fernandez M, Quintela-del-Rio A, Gimeno-Santos E, Arbillaga-Etxarri A, Torres-Castro R, Vilarç Casamitjana J, Varas de la Fuente AB, Serrano Veguillas C, Bravo Cortes P, Martin Cortijo C, Garcia Delgado E, Herrero-Cortina B, Valera JL; Fregonezi GAF, Gonzalez Montanez C, Martin-Valero R, Francin-Gallego M, Sanesteban Hermida Y, Gimenez Moolhuyzen E, Alvares Rivas J, Rios-Cortes AT, Souto-Camba S, Gonzalez-Doniz L. Maximal respiratory pressure reference equations in herlathy adults and cut-off points for defining muscle weakness. Arch Bronconeumol 2023; 59(12):813-820. [CrossRef]
- Wang Y-C, Bohannon RW, Li X, Sindhu B, Kapellusch J. Hand-grip strength: normative reference values and equations for individuals 18 to 85 years of age residing in the United States. J Orthop Sports Phys Ter 2018; 48(9):685-693. [CrossRef]
- Fletcher, CM. Standardised questionnaire on respiratory symptoms: a statement prepared and approved by the MRC Committee on the Aetiology of Chronic Bronchitis (MRC breathlessness score). Br Med J 1960; 2:1662.
- Combret Y, Prieur G, Hilfiker R, Gravier F-E, Smondack P, Contal O, Lamia B, Bonnevie T, Medrinal C. The relationship between maximal expiratory pressure values and critical outcomes in mechanically ventilated patients: a post hoc analysis of an observational study. Ann Intensive Care 2021; 11:8. [CrossRef]
- Schellekens W-J M, van Hees HWH, Doorduin J, Roesthuis LH, Scheffer GJ, van der Hoeven JG, Heunks LMA. Strategies to optimize respiratory muscle function in ICU patients. Critical Care 2016: 20:103. [CrossRef]
- Tzanis G, Vasileiadis I, Zervakis D, Karatzanos E, Dimopoulos S, Pitsolis T, Tripodaki E, Gerovasili V, Routsi C, Nanas S. Maximum inspiratory pressure, a surrogate parameter for the assessment of ICU-acquired weakness. BMC Anesthesiology 2011; 11:14. [CrossRef]
- Huang Y, Tan C, Wu J, Chen M, Wang Z, Luo L, Zhou X, Liu X, Huang X, Yuan S, Chen C, Gao F, Huang J, Shan H, Liu J. Impact of coronavirus 2019 on pulmonary function in early convalescence phase. Respir Res 2020; 21(1):163. [CrossRef]
- Fagevik Olsén M, Lannefors L, Johansson EL, Persson HC. Variations in respiratory and functional symptoms at four months after hospitalisation due to COVID-19: a cross-sectional study. BMC Pulm Med 2024; 24(1):63. [CrossRef]
- Goulart CDL, Arêas GPT, Milani M, Borges FFDR, Magalhães JR, Back GD, Borghi-Silva A, Oliveira LFL, de Paula AR, Marinho CC, Prado DP, Almeida CN, Dias CMCC, Gomes VA, Ritt LEF, Franzoni LT, Stein R, Neto MG, Cipriano Junior G, Almeida-Val F. Sex-based differences in pulmonary function and cardiopulmonary response 30 months post-COVID-19: A Brazilian multicentric study. Int J Environ Res Public Health 2024; 21(10):1293. [CrossRef]
- Regmi B, Friedrich J, Jörn B, Senol M, Giannoni A, Boentert M, Daher A, Dreher M, Spiesshoefer J. Diaphragm muscle weakness might explain exertional dyspnea 15 months after hospitalization for COVID-19. Am J Respir Crit Care Med 2023; 15;207(8):1012-1021. [CrossRef]
- Farr E, Wolfe AR, Deshmukh S, Rydberg L, Soriano R, Walter JM, Boon AJ, Wolfe LF, Franz CK. Diaphragm dysfunction in severe COVID-19 as determined by neuromuscular ultrasound. Ann Clin Transl Neurol 2021; 8(8):1745-1749. [CrossRef]
- Medrinal C, Prieur G, Bonnevie T, Gravier FE, Mayard D, Desmalles E, Smondack P, Lamia B, Combret Y, Fossat G. Muscle weakness, functional capacities and recovery from COVID-19 ICU survivors. BMC Anesthesiol 2021; 21(1):64. [CrossRef]
- Severin R, Arena R, Lavie CJ, Bond S, Phillips SA. Respiratory muscle performance screening for infectious disease management following COVID-19: a highly pressurized situation. Am J Med 2020; 133(9):1025-1032. [CrossRef]
- Hennigs JK, Huwe M, Hennigs A, Oqueka T, Simon M, Harbaum L, Körbelin J, Schmiedel S, Schulze Zur Wiesch J, Addo MM, Kluge S, Klose H. Respiratory muscle dysfunction in long-COVID patients. Infection 2022; 50(5):1391-1397. [CrossRef]
- Steinbeis F, Kedor C, Meyer HJ, Thibeault C, Mittermaier M, Knape P, Ahrens K, Rotter G, Temmesfeld-Wollbrück B, Sander LE, Kurth F, Witzenrath M, Scheibenbogen C, Zoller T. A new phenotype of patients with post-COVID-19 condition is characterised by a pattern of complex ventilatory dysfunction, neuromuscular disturbance and fatigue symptoms. ERJ Open Res 2024; 10(5):01027-2023. [CrossRef]
- Carfi A, Bernabei R, Landi F, for the Gemelli against COVID-19 Post-acute Care Study Group. Persistent symptoms in patients after acute COVID-19. JAMA 2020; 324(6):603-605.
- Shah AS, Wong AW, Hague CJ, Murphy DT, Johnston JC, Ryerson CJ, Carlsten C. A prospective study of 12-week respiratory outcomes in COVID-19-related hospitalizations. Thorax 2021; 76(4):402-404. [CrossRef]
- Arnold DT, Hamilton FW, Milne A, Morley AJ, Viner J, Attwood M, Noel A, Gunning S, Hatrick J, Hamilton S, Elvers KT, Hyams C, Bibby A, Moran E, Adamali HI, Dodd JW, Maskell NA, Barratt SL. Patient outcomes after hospitalization with COVID-19 and implications for follow up: results from a prospective UK cohort. Thorax 2021; 76(4):399-401. [CrossRef]
- Huang C, Huang L, Wang Y, Li X, Ren L, Gu X, Kang L, Guo L, Liu M, Zhou X, Luo J, Huang Z, Tu S, Zhao Y, Chen L, Xu D, Li Y, Li C, Peng L, Li Y, Xie W, Cui D, Shang L, Fan G, Xu J, Wang G, Wang Y, Zhong J, Wang C, Wang J, Zhang D, Cao B. 6-month consequences of COVID-19 in patients discharged from hospital: a cohort study. Lancet 2023; 401(10393):e21-e33. [CrossRef]
- Fernandez-de-las-Penas C, Martin-Guerrero JD, Pellicer-Valero OJ, Navarro-Pardo E, Gómez-Mayordomo V, Cuadrado ML, Arias-Navalón JA, Cigarán-Méndez M, Hernández-Barrera V, Arendt-Nielsen L. Female sex is a risk factor associated with long-term post-COVID related-symptoms but not with COVID-19 symptoms: the LONG-COVID-EXP-CM Multicenter Study. J Clin Med 2022; 11:413. [CrossRef]
- Johnsen S, Sattler SM, Miskowiak KW, Kunalan K, Victor A, Pedersen L, Andreassen HF, Jørgensen BJ, Heebøll H, Andersen MB, Marner L, Hædersdal C, Hansen H, Ditlev SB, Porsbjerg C, Lapperre TS. Descriptive analysis of long COVID sequalae identified in a multidisciplinary clinic serving hospitalized and non-hospitalized patients. ERJ Open Res 2021; 7(3):00205-002021.
- de Godoy CG, Schmitt ACB, Ochiai GS, Gouveia E Silva EC, de Oliveira DB, da Silva EM, de Carvalho CRF, Junior CT, D'Andre A Greve JM, Hill K, Pompeu JE. Postural balance, mobility, and handgrip strength one year after hospitalization due to COVID-19. Gait Posture 2024; 114:14-20. [CrossRef]
- Hussain N, Hansson PO, Samuelsson CM, Persson CU. Function and activity capacity at 1 year after the admission to intensive care unit for COVID-19. Clin Rehabil 2024; 38(10):1382-1392. [CrossRef]
- Shin HI, Kim DK, Seo KM, Kang SH, Lee SY, Son S. Relation between respiratory muscle strength and skeletal muscle mass and hand grip strength in the healthy elderly. Ann Rehabil Med 2017; 41(4):686-692. [CrossRef]
- González-Islas D, Robles-Hernández R, Flores-Cisneros L, Orea-Tejeda A, Galicia-Amor S, Hernández-López N, Valdés-Moreno MI, Sánchez-Santillán R, García-Hernández JC, Castorena-Maldonado A. Association between muscle quality index and pulmonary function in post-COVID-19 subjects. BMC Pulm Med 2023; 23(1):442. [CrossRef]
- Lee JH, Yim J-J, Park J. Pulmonary function and chest computed tomography abnormalities 6-12 months after recovery from COVID-19: a systematic review and meta-analysis. Respir Res 2022; 23(1):233. [CrossRef]
- Wu X, Liu X, Zhou Y, Yu H, Li R, Zhan Q, Ni F, Fang S, Lu Y, Ding X, Liu H, Ewing RM, Jones MG, Hu Y, Nie H, Wang Y. 3-month, 6-month, 9-month, and 12-month respiratory outcomes in patients following COVID-19-related hospitalization: a prospective study. Lancet Respir Med 2021; 9(7):747-754. [CrossRef]
- Lombardi F, Calabrese A, Iovene A, Pierandrei C, Lerede M, Varone F, Richeldi L, Sgalla G; Gemelli Against COVID-19 Post-Acute Care Study Group. Residual respiratory impairment after COVID-19 pneumonia. BMC Pulm Med 2021; 21(1):241. [CrossRef]
- Hewitt J, Carter B, Vilches-Moraga A, Quinn TJ, Braude P, Verduri A, Pearce L, Stechman M, Short R, Price A, Collins JT, Bruce E, Einarsson A, Rickard F, Mitchell E, Holloway M, Hesford J, Barlow-Pay F, Clini E, Myint PK, Moug SJ, McCarthy K; COPE Study Collaborators. The effect on frailty on survival in patients with COVID-19 (COPE): a multicentre, European, observational cohort study. Lancet Public Health 2020; 5(8):e444-e451. [CrossRef]
- Calvache-Mateo A, Reychler G, Heredia-Ciuró A, Martín-Núñez J, Ortiz-Rubio A, Navas-Otero A, Valenza MC. Respiratory training effects in Long COVID-19 patients: a systematic review and meta-analysis. Expert Rev Respir Med 2024; 18(3-4):207-217. [CrossRef]
- Illi SK, Held U, Frank I, Spengler CM. Effect of respiratory muscle training on exercise performance in healthy individuals. Sport Med 2012; 42(8):707-724. [CrossRef]
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



