
Submitted:
10 December 2024
Posted:
11 December 2024
You are already at the latest version
Abstract
Childhood abuse can have long-lasting consequences and be a risk for mental health. This review aimed to explore the recent studies on equine-assisted psychotherapy (EAP), which uses equines in therapy to help young people recover from adverse childhood experiences. Five relevant data-bases were utilized in the search of full-text articles published between January 2000 and August 2024 - addressing the incorporation of equines in therapeutic activities of young people (between 6 and 25 years old) who have experienced abuse, violence, or psychological trauma. The search excluded articles that lacked well-defined treatment programs or focused on physical treatments and limited the results to scholarly journals. The initial search yielded 537 articles, of which 27 were extracted. Following a detailed examination, 18 were excluded, leaving 9 works for further analysis. All authors agree that EAP holds much promise for youth with a history of trauma or abuse, however, a lack of methodological rigor was found across the publications collected, including inconsistencies in the concepts used; the variability in participants, designs, and settings of the programs; minimal use of randomization or control groups; and lack of reliability. The implications for future research are discussed, including the need to address discrepancies in the program’s descriptions and reporting outcomes.
Keywords:
childhood trauma
; psychological recovery
; adverse childhood experiences
; horses in psychotherapy
; human-horses interaction
; equine-assisted therapy
; Youth mental health
1. Introduction
Currently, there is a significant issue with children and adolescents experiencing trauma-related health problems, behavioral problems, and psychological distress at an alarming rate [1]. The development of the brain and regulatory systems is not complete until the end of adolescence, which makes youth who are exposed to psychological trauma or adverse childhood experiences (ACEs) more likely to develop lifelong health issues [2]. Enduring adverse events at childhood, such as neglect or abuse, can have a great impact on youth's development, leading to long-term mental and emotional issues [3,4,5,6]. If left untreated, these issues can lead to significant impairments and have long-lasting negative effects [7,8,9]. ACEs are not punctual, often are chronic and repetitive, and associated with an increased risk of substance use [7,10], anger, insecure attachments [11], delinquency, revictimization [12], impaired cognitive functions and increased vulnerability to mood disorders [13], with the emergence of depression, anxiety [14], or posttraumatic stress disorder (PTSD) [15]. When these events occur within the family or social environment, they can significantly disrupt the child's physical or psychological development [16].
Although there are some treatment methods, effectively involving children and adolescents in therapy after psychological trauma can be challenging. Despite the rising popularity of mind/body experiential approaches used as therapies (such as mindfulness programs, adventure-based activities, music, or theatre), most behavioral therapies are talk-based. Talk therapies are simply not efficacious for children or young people who may be unable to verbally process their feelings or cannot deal with emotional intimacy, making it difficult to encourage children to engage and positively participate in-office therapy [17,18].
The challenges presented by verbal-based psychotherapeutic interventions are becoming so evident that new approaches of therapy and interventions are being developed. Eckshtain and colleagues [17], highlighted the need for treatment development and research to improve both immediate and long-term benefits on youth depression psychotherapy. In their meta-analysis, Weisz et al. [18], reported that psychotherapy interventions for mental health problems are becoming less successful, and the average benefit from youth treatment has not increased over the past fifty years. All this data suggests that new psychotherapeutic strategies may be needed. As such, new perspectives of Animal-Assisted interventions have experienced a surge in interest, as an alternative therapy to psychological treatment and are currently frequently used to address trauma sequelae [19]. In the following section, relevant terms are briefly explained for a better understanding of the content. However, the terminology used to describe the use of animals, including horses, for treatment, therapy, or education is evolving. It is important to note that the pace of this evolution has not matched the rapid growth and diversification of the sector. Indeed, recent studies have indicated the necessity for further research into the standardization of terminological terms [20,21].
In recent years, the use of horses in services aiming to improve human health has evolved greatly. While initially, horses were used mostly on medical and therapeutic interventions in persons with disabilities or physical illnesses (e.g., [22,23]), the practice has evolved into a new, different focus, with results suggesting recovering mental health, and wellness [7,9,24,25]. Research is beginning to show that along with other non-talk-based interventions, connecting with animals is not only recreational but can be therapeutic [26]. Activities and interaction with horses can be particularly efficient for mental health recovery, especially for individuals who do not respond to other interventions or treatments [6,9,27,28,29,30,31,32,33]. The various goal-oriented and structured interventions that intentionally incorporate equines in health, education, and human service, are called equine-assisted services (EAS) [21]. Therefore, here we use the term EAS when referring to the different varieties of equine programs.
The practice of EAS can take on several different terms and forms. While often referred to as therapeutic riding, equine-assisted learning (EAL), equine-assisted therapy (EAT), or hippotherapy [7,23,24], each approach has its own methods and goals, where the animal's presence, which can be a donkey, mule, or horse, and its interactions, are used to achieve different goals, whether educational, physical, or psychological [34]. Therapeutic riding programs typically center around the skill of riding, catering to individuals with disabilities, and emphasize fun and social interactions [35]. EAL primarily focuses on education, using horses as a tool for facilitating learning [36]. EAT programs, often called hippotherapy [20,22], involve a health therapist and utilizes equines as a tool to rehabilitate and foster physical or psychological insights.
Among EAT, equine-assisted psychotherapy (EAP) is a form of experiential therapy, where a selected equine, is included in sessions designed to achieve therapy goals for psychiatric or psychological issues [37]. While other approaches, such as EAL or equine-assisted mental health (EAMH) also involve equines in mental health support, their goals differ from those of EAP. As a rule, EAP aims to address treatment goals, and, like other forms of psychotherapy, it is a purposeful and conventional treatment for general psychopathology symptoms [38,39], therefore, it includes a credentialed mental healthcare professional [40]. In addition, EAP often involves some traditional psychotherapeutic techniques such as the therapist asking the client questions to facilitate introspection, encouraging positive play activities, aiding in skill acquisition, teaching communication skills, and supporting empathy development. Some models and certification programs have been established [34, in which the protocols may be based on mounted, or unmounted activities. As it is in therapeutic riding programs, mounted programs prioritize activities such as riding, driving, or vaulting, incorporating groundwork only as complementary activities, through leading, or tacking the equine as pre, or post-mounted activities. In ground-based programs, grooming, leading and observing the animal, are the focus, despite in some circumstances it may incorporate riding at the end of the programs. EAGALA Model (Equine-Assisted Growth and the Learning Association), e.g., advocates for an approach to EAS where horses (normally) are kept at liberty and never ridden. This model, closely related to the holistic method of Gestalt therapy techniques, was designed to enable working with horses at freedom, allowing the animal to decide when, if, and how they want to interact with a client [19]. During the EAP sessions, specifically, therapy is based on the reciprocal exchange of interactions between the client and the equine, and therapists rely on their intervention on the ability of the equines to act as social facilitators, to reduce the client's arousal and ease into the conversation [41]. Being hypothesized that recovery depends on the therapeutic alliance potentially created [8].
Other literature reviews have focused on the efficacy of EAS in psychological outcomes overall. Kendall et al [34], and Lentini and Knox [42], reviewed the efficacy of EAS, but they included individuals from quite different populations, from autistic to those suffering physical pain, with widely different needs and difficulties. Cantin and Marshal-Lucette [43], and Anestis et al. [44], focused on people with mental health and behavioral disorders but included all groups and ages. Anestis and colleagues concluded that the studies they collected failed to provide evidence that EAS would be superior to the mere passage of time, and did not justify its utilization in the treatment of mental disorders [44]. Also, Wilkie et al. [45], conducted a meta-analysis research and concluded that designs on this topic still had flawed methodologies, or the research supporting this practice was still descriptive. However, more recently, Staudt and Cherry [46], after reviewing the efficacy of EAS, in both youth and adults, despite agreeing with the several gaps in the studies collected, including confounding terms, and ignoring knowledge of long-term or continuous effects, suggested it as promising for treating trauma/ PTSD symptoms. Also, Haig and Skinner, in 2022 [47], suggested in their review the use of EAS as a promising approach for youth, however, they focused specifically on learning goals and EAL.
Empirical research suggests the positive impact equines may have on mental health, but there is a lack of focus on the effects of EAS, as a therapeutic approach in young people recovering from trauma or ACEs [8]. Given the increase in the number of young individuals and parents seeking complementary, alternative, and efficacious models of therapy, it has become imperative to accurately evaluate the efficacy of such Programs.
The main goal of this review is to analyze the findings, identify gaps in the knowledge, and clarify concepts that can be drawn from the empirical literature that has emerged in the last few years, on the effectiveness of EAP practices, for young people who have suffered from unfavorable environmental conditions, such as abuse or continuous trauma. We specifically concentrate on those who have experienced physical, emotional, and sexual abuse or abandonment, but do not have any disabilities. A scoping review design was considered the most appropriate methodology to understand and summarize the existing literature on the use of EAP in trauma recovery of youth.
2. Materials and Methods
2.1. Information Sources
In this study, we conducted a scoping review using the analytical methodology recommended by the Prisma declaration [48], to identify full-text articles that explored the use of EAP for youth who have experienced adverse environments or continuous psychological trauma. We limited our search to articles written in English and published between January of 2000 and August 2024. We searched five online databases which were Scopus, PubMed (NCBI), ScienceDirect, Web of Science, and ProQuest. Additionally, we examined the reference sections of the included articles to identify any other relevant studies for inclusion.
2.2. Search Strategy and Eligibility Criteria
The searches were carried out from September to November 2024. To ensure our search was comprehensive, we used several keywords and refined results for "youth" OR "at risk" OR "neglect" OR "behavioral" OR "abuse" OR "violence" OR "trauma" AND ("adaptive riding" OR "adapted riding" OR "equine" OR "horse" OR "equine assisted psychotherapy" OR "equine facilitated psychotherapy" OR "equine facilitated therapy" OR "therapeutic riding" OR " horse riding" OR "hippotherapy" AND PUBYEAR = 2000 to 2024 AND (LIMIT-TO ( DOCTYPE , "ar" ). We excluded articles that were unrelated to the relationship between humans and horses and those that focused only on physical treatment using horses. We also filtered our search to include only scholarly journals and articles, excluding conference abstracts, book chapters, short communications, and reviews.
Inclusion and exclusion criteria for the study are summarized in Table 1.
2.3. Study Selection, Data Extraction and Analysis
We developed the research question according to the PICOS strategy outlined and updated by Higgins et al [49], to determine the relevance of published articles. The Population, Interventions, Comparisons, Outcomes, and Study design are described in Figure 1. The intervention of interest was the limited range of EAP, as defined in the following section, on the Concept of EAP. After identifying potential articles using the PICOS strategy, the three authors, IPF, KO, and SA, independently reviewed the articles in full to determine their eligibility and quality. Conflicts that arose during the review process were communicated and mutually resolved. The utilization of the PICOS strategy and PRISMA guidelines ensured that the selection and analysis of the articles were comprehensive, transparent, and consistent.
2.4. Risk of Bias Assessment
This review aimed to focus on high-quality research studies that offer insights into the benefits and limitations of EAP, as a therapeutic intervention, particularly in the treatment of young people who have experienced psychological trauma or neglect. We deemed it crucial in the understanding of the mechanisms through which EAP may be effective, to consider the quality of the studies, therefore we detached qualitative/ descriptive studies and instead focused on experimental or quasi-experimental reports that used quantitative assessments, that provided details about the interventions, session duration, number of sessions, and the protocols used.
3. Results
After conducting the initial search, the findings were reported in the PRISMA Flow Diagram (Figure 2). A total of 537 research articles published between 2000 and August 2024 were found, after removing duplicates. We then applied the selection criteria described previously to narrow down the number of studies included in the review. From this process, we extracted 27 publications (Table 2) that appeared to meet the inclusion criteria (Table 1). We carefully examined the complete texts of the 27 selected works in detail. By excluding studies that did not meet these criteria, we could ensure that the conclusions drawn from the review are valid and reliable.
3.1. Study Selection
Initially, we conducted a broad search but narrowed it down to a specific study design. We included the studies that provided EAS to at-risk youth overall, under the assumption that some participants in these study samples may have faced traumatic experiences. However, some of the studies were designed to improve learning skills (EAL) rather than for therapeutic purposes [36,50,51,52,53] or consisted of counseling interventions [30]. Consequently, we had to exclude research studies that investigated the impact of EAS on mental health support or emotional issues in youth that did not clearly include ACEs, psychological trauma (n=4), or treatment goals (n=6) (see Table 2), and therefore could not be considered EAP.

Table 2.
Basic characteristics of the 27 studies extracted and examined. It is organized by articles in which the Program purpose was clearly to recover psychosocial outcomes, from those not clearly to recover. Abbreviations: PPSU: problematic parental substance use.
Table 2.
Basic characteristics of the 27 studies extracted and examined. It is organized by articles in which the Program purpose was clearly to recover psychosocial outcomes, from those not clearly to recover. Abbreviations: PPSU: problematic parental substance use.
| Authors and Year | Reference | Issue | Type of Intervention | ||
| 1 | 1 | Bachi et al., 2011 | [57] | NEGLET (RESIDENTS) | TREATMENT |
| 2 | 2 | Coffin, 2019 | [62] | TRAUMA | TREATMENT |
| 3 | 3 | Gibbons et al., 2017 | [58] | ABUSE/VIOLENCE | TREATMENT |
| 4 | 4 | McCullough et al., 2015 | [61] | VIOLENCE | TREATMENT |
| 5 | 5 | Mueller and McCullough, 2017 | [15] | TRAUMA | TREATMENT |
| 6 | 6 | Schultz et al., 2007 | [60] | ABUSE /VIOLENCE | TREATMENT |
| 7 | 7 | Kemp et al., 2014 | [12] | ABUSE | TREATMENT |
| 8 | 8 | Signal et al., 2013 | [59] | ABUSE | TREATMENT |
| 9 | 9 | Tsantefski et al., 2017 | [56] | NEGLET (PPSU) | TREATMENT |
| 10 | 10 | Roberts and Honzel, 2020 | [56] | TRAUMA | MORE THAN 1 TREATMENT |
| 11 | 1 | Carlsson et al., 2015 | [54] | ABUSE/ REJECTION | TREATMENT |
| 12 | 2 | Carlsson, 2017 | [55] | ABUSE /REJECTION | TREATMENT |
| 13 | 3 | Craig, 2020 | [16] | ACEs | TREATMENT |
| 14 | 4 | Craig et al., 2020 | [16] | ACEs | TREATMENT |
| 15 | 5 | Dunlop and Tsantefski, 2018 | [19] | NEGLET (PPSU) | TREATMENT |
| 16 | 6 | Kesner and Pritzker, 2008 | [29] | NEGLET/ ABUSE | TREATMENT |
| 17 | 7 | Weiss-Dagan et al., 2022 | [33] | NEGLET (RESIDENTS) | TREATMENT |
| 18 | 1 | Cagle-Holtcamp et al., 2019 | [13] | AT RISK | NOT TREATMENT |
| 19 | 2 | Frederick et al., 2015 | [50] | AT RISK | NOT TREATMENT |
| 20 | 3 | Hemingway et al., 2015 | [51] | AT RISK | NOT TREATMENT |
| 21 | 4 | Ho et al., 2017 | [52] | AT RISK | NOT TREATMENT |
| 22 | 5 | Hood and Wilson, 2020 | [31] | AT RISK | NOT TRAUMA |
| 23 | 6 | Kaiser et al., 2006 | [35] | AT RISK | NOT TRAUMA |
| 24 | 7 | Pendry et al., 2018 | [36] | BEHAVIORAL ISSUES | NOT TREATMENT |
| 25 | 8 | Trotter et al., 2008 | [30] | AT RISK | NOT TREATMENT |
| 26 | 9 | Hoagwood et al., 2022 | [26] | ANXIETY | NOT TRAUMA |
| 27 | 10 | Punzo et al., 2022 | [32] | MENTAL ILNESS | NOT TRAUMA |
3.2. Quality of Selected Studies
As depicted in Table 3, from the 17 studies published concerning the value of EAP in therapeutic settings, 7 publications relied upon qualitative assessments only. Regarding their low quality and risk of bias, these studies were excluded from further analysis. These works studied children [19,29], or adolescents [11,16,33,54,55] previously exposed to ACEs. Most of these studies had small participant samples (MEAN= 15.6 ± 8.0), unclear and unstandardized session durations and numbers, and the protocols were based on clients' demands, or not specified, except for three studies that followed the EAGALA [19] or a standardized protocol of therapeutic horseback riding [29,33].
Out of the 10 studies that met the rigorous scientific criteria of: (1) including a control group (20%) [15,37]; (2) presentation of comparative pre- and post-therapy results (100%); and (3) utilizing standardized outcome measures (quantitative), one additional report was excluded for including complementary types of therapy (n=1) 4]. The remaining 9 studies were included in this review. Details of these articles are displayed in Table 4.
3.3. Patient and Intervention Characteristics
A total of 315 participants, from the 9 studies were included in the quantitative analysis study, each one with 11 to 63 participants (MEAN= 35 ± 16.0), with mean ages of 11.44 ± 1.2 years old. Most of the studies encompassed adolescent participants, except for Tsantefski et al.'s [56] investigation, which exclusively assessed children below 13 years of age. The subjects' gender distribution was relatively uniform, with 135 boys and 141 girls included in the analyses. However, gender information was not specified in the report by Bachi et al. [57]. All studies were conducted with horses (100%), and in almost all studies the young participants have been self-selected, not randomly assigned, except for Mueller and McCullough's [15] who quasi-randomized participants to treatment, and Gibbons et al. [58] study, whose participants were randomly assigned to experimental or wait-list control groups.
Ninety percent (90%) of the research reports offered weekly sessions, with session durations ranging from 45 minutes for the shortest to 120 minutes for the longest (MEAN= 85.3± 29.6). The most frequent period of intervention was 2 to 3 months [12,15,56,59]. The number of individual sessions varied from 8 to 26 (MEAN= 11.5 ± 4.6), except for Gibbons et al. [58] study, in which full 2-day sessions were applied. In Schultz et al. [60] study, the variation in the number of sessions each child received was enormous, so they only considered those clients receiving at least 6 sessions for analysis. The documented EAS programs varied from group sessions 15] to individual sessions [37,61] and sessions including the child's family [60]. In one study [61] the type of intervention used was not specified. Three studies (30%) used EAGALA methods: Schultz et al. [60 worked with children who had experienced intra-family violence and were diagnosed with a variety of disorders; Signal's group [59] presented an extension of Kemp et al.'s [12] study as a treatment for victims of sexual or physical abuse.
3.4. Synthesized Findings
The nine studies included in this review reported beneficial psychological effects of EAP on youth exposed to trauma or neglect (Table 4). Bachi and colleagues [57] investigated the effect of EAP in at-risk adolescents living in a residential treatment facility. Not all the participants in Bachi’s program have been previously abused, but adolescents in residential treatment facilities are generally defined as having severe personal or adjusting needs and experiencing abandonment or neglect [5]. The adolescents from their treatment group (N= 14) learned to handle and ride a horse, and that had an impact on the 4 parameters they measured, improving self-esteem, self-efficacy, trust, and communication skills. Nevertheless, the researchers found no significant differences when they were compared with the non-active adolescents (Controls, N=15), after 7 months of treatment. The relatively small sample (N=29) may have limited the extent to which differences between groups could be detected. The Coffin program [62] aimed to provide an alternative therapy for Aboriginal youth in the areas of grief, loss, and trauma. After the 8-week Gestalt Program ended, the young clients reported less frequent sleepless nights due to worrying, from baseline and fewer incidences of anger. Gibbons et al. [58] reported several significant benefits of using Join-Up® Model, for two days, in young Guatemalan victims of abuse or violence, including improvements in emotion regulation and decrease in aggression, and self-reported leadership (p= 0.016). Within this study, the young participants were randomly assigned to treatment or control groups, and besides using multiple and complete evaluation instruments, their results were based on participants’ self-reports, and on mentors and parents’ perceptions.
Through developing activities with horses- a simple task like grooming was suggested to aid teens feel secure in talking about their problems, gaining confidence, and reducing anxiety [60]. The studies collected have suggested that the therapeutic approach, using EAGALA methods was effective when working to alleviate trauma symptoms from violence [60] or abuses [12,59]. While kemp et al. [12] reported on the efficacy of the EAGALA, regarding trauma and anxiety symptoms, the Signal group [59] proved that 10 weeks of intervention significantly decreased depression level scores (p<0.05), changing from potentially impairing depressive symptomology (i.e., warranting professional intervention with attendant elevated risks for self-harm/suicide) to ‘normal’ or minimal scores. Sexually abused children and adolescents may have trouble with physical contact and proximity. EAP deepening of the children’s affective experience, by incorporating the horse, may have provided a connection to the trauma experiences that otherwise would be difficult to achieve. Schultz et al. [60], also tested the efficacy of the EAGALA method, by determining changes in Global Assessment of Functioning (GAF) scores in children and adolescents, victims of violence or abuse. Their study has demonstrated a quick response to EAP, especially in the younger children, and in those with worse experiences of abuse and neglect. Yet, this was the only outcome measure of their study.
McCullough et al. [61], results suggest that EAP can be effective in lowering PTSD symptomatology in traumatized children. However, they did not specify the type of intervention they used, and EAP treatment effects were multimodal, with several different modes of occurrences at the same time. Mueller and McCullough's [15], results point out a statistically significant therapy effect (p< 0.001), on PTSD symptoms in both groups tested: office-based and EAP, but with no differences between treatment groups. Also, despite EAP allowing adolescents to develop a strong relationship with horses, the authors [15], did not find significant changes in the HABS questionnaire responses through intervention points, where item issues like security, commitment, responsiveness, and affection were addressed. Tsantefski et al. [56], showed positive effects on the psychological well-being of children exposed to parents’ substance use. Their results were determined by parents' and teachers' survey responses about children’s behaviors and attention difficulties. Parents observed reductions in emotional problems: such as anxiety and somatic complaints (p=0.007) and both parents and teachers reported a significant reduction in hyperactivity (p=0.05).
4. Discussion
The objective of this scoping review was to scrutinize the literature that integrates EAP into therapeutic interventions for youth who have encountered psychological trauma, abuse, and emotional distress. The review comprised nine studies, with diverse research designs, conducted on children, adolescents, or young adults (aged 6-25 years old). By conducting this review, we identified and examined the available research, and key characteristics or factors related to EAS, and specifically to EAP, to shed light on the effectiveness for this specific population. We also identified and analyzed the multiple gaps in the existing literature. The summarized findings indicated that introducing horses into the therapeutic process of such vulnerable children, adolescents, or young adults fosters unique benefits, such as enhanced welfare by promoting a general improvement across multiple outcomes: improved well-being, by encouraging engagement [58], and reduced expression of anger and aggression. Moreover, EAP has been observed to ameliorate sleep [62], and mood, specifically by decreasing depression [59], stress, and anxiety [12,15,56]. Additionally, the incorporation of equines in therapy has been suggested as increasing the perception of social support, self-esteem, and trust [57], fostering personal growth, empathy, and the development of social competencies [56].
The authors unanimously agree upon the unique therapeutic potential of horses. Owing to their remarkable presence, the literature claims that horses are capable of eliciting emotions, which is believed to be the basis of initiating a therapeutic process that yields psychological and emotional benefits. In contrast to other animals used in Animal-Assisted Services, like cats and dogs, horses are not predators. Their large size coupled with their instinctive fearfulness, as a prey characteristic, may have a profound effect on vulnerable youth [7,63], who can identify with the horse's need for safety.
Most models reviewed in this study focused on the response of children and adolescents to the body language exhibited by horses. The sessions benefit from the horse's sensitivity to pick up on the young client’s intention, which can be deciphered by the therapist or equine specialist present. During the intervention, the mental health professionals usually employ structured activities, while the young client deals with the horses, in either group or individual settings. Later, the psychological competences acquired from horse interactions can be applied to everyday life situations [17].
Regarding adolescents who have experienced negative social stigma and trauma, horses may offer unique opportunities to address emotional and behavioral load. The act of caring for another living being (whereas their own needs have been partly or wholly unheeded), may help these individuals process their own emotions and experiences, ultimately leading to a sense of internal strength and empowerment [15,61]. Furthermore, as suggested by Kemp et al. [12], for sexually abused children and adolescents, EAP may provide opportunities to work with touch and physical contact without the ethical concerns that are present in traditional therapy. Touching and being touched by horses may feel safer and less threatening than human touch, allowing patients to work with physical contact in a therapeutic and healing way [12,59].
4.1. Models and the Diversity of Protocols in Psychotherapy with Equines
In the psychotherapy approach, the interplay between the body and the mind is considered crucial in bringing about healing and restoration [6]. EAP offers a unique therapeutic setting where clients can address emotional and psychological issues through nonverbal communication with the horses [60], where attachment and connection behaviors are the focus.
Most of EAP approaches here examined aimed to explore equine-human interactions to achieve therapeutic outcomes and all are person-centered. The interventions entail the interactions between the horse and the adolescents in an open and unrestrained environment, as experimented by Coffin [62] and Gibbons et al. [58], to help develop a bond. By connecting with horses, the young clients can learn body language, and horsemanship techniques, while also increasing awareness of their own body.
All articles here reviewed, have been developed incorporating natural horsemanship techniques and most used ground-based works, such as EAGALA or Parelli techniques (see Table 3). In EAP, professionals tend to avoid the inclusion of riding in their interventions [12,30,50,58,62]. According to the authors, standing side-a-side with the animal, at “eye level” can be of utmost importance, conducing to relaxation, openness, and confidence. However, certain practitioners prefer to incorporate it after the young client has learned to lead the horse from the ground (e.g., [15]). Some models of EAP here reviewed have been established solely based on riding [29,33]. According to Bachi [57], the healing aspects of riding are especially significant aspects for adolescents’ victims of abandonment or neglect. Often used with at-risk youth, it was described in most intervention goals, decreasing anger [35] helping relaxation [33], and being helpful to regulate emotions [26,32,36].
The reviewed studies here have suggested that participating in EAP can have immediate impacts on behaviors, even after just brief periods of time. For example, Gibbons et al. [58] who evaluated at-risk Guatemalan adolescents participating in the Join-Up® Model workshop for two days, reported significant changes (p<0.05) in their attitudes, and improvements in emotion regulation. The key tools utilized in these studies were body language and interaction with horses, which were used to facilitate problem-solving activities and encourage non-aggressive, assertive responses. Bachi et al. [57] have suggested that the use of these methods can lead to a sense of mastery and increased self-efficacy; and Gibbons et al. [58] reported that the young participants exhibited better communication skills and greater evidence of compassion with others.
Despite the promising benefits reported in the collected studies, further and better research is needed, as bellow described, and the suggested results must be interpreted with caution.
4.2. Research Gaps and Limitations of the Findings
Since the last decade, better-designed experimental studies have been demanded [44], and, in the last years, an impressive boom of studies appeared, with more robust research quality in treatment programs. Nevertheless, this scoping review revealed that research on this topic is limited, and it has several limitations. Regarding the obvious differences in the outcomes measured in this review, we could not answer whether EAP intervention benefits youth exposed to ACEs or psychological trauma, as we could not standardize the type of problem, and its severity or exclude concurrent therapies, moreover, the intervention study designs were not homogenous.
Some of the studies included in this review had problems with the methodologies, containing threats to validity and generalizability; some with small sample sizes (eg. [61]: N=11; and [62]: N= 20); with participants self-selecting into the intervention, including lack of control groups, and with the only exception of Gibbons’ [58] report, when existent, no random assignment [15,57].
Most studies included in the collection did not include follow-up, except for Bachi et al. [57] study - and that compromises the integrity and generalizability of the results. Despite the within-group designs allowing for examination of baseline and ending data, without follow-up, it is unknown if benefits remained after program completion. Specifically, investigations should be conducted to explore the potential long-term impacts of EAP interventions on behavior change. In addition, the specific mechanisms by which EAP can lead to improved emotion regulation, attitudes, and communication skills among participants should be further investigated. This could include exploring the role of body language and interaction with horses, as well as other factors such as the therapeutic alliance between the participant and therapist.
In the literature described above, researchers have described the nature of EAS at a high level of generality, with a few studies describing what occurred during the intervention, and it is difficult to identify each study as EAP, EAL or activity. Many studies did not give a thorough description of the specific sequences of the steps or exercises within EAP [44,60] and did not always provide a description of the credentials of the facilitators. Any study gave a rationale for why the modality, or the Model was chosen. This gap is especially significant given the variance between models of EAP and the uncertainty that exists regarding the typical practices utilized within the therapy.
A serious gap in the literature is the absence of a systematic account of the clinical practices implemented within EAP. Objective experimental designs, measuring physiological parameters, not relying merely on perceptions or scales would allow us to better identify mechanisms of change [2]. Traumatic experiences affect many physiological systems in the body especially if experienced as children or adolescents [2,60,61]. The effect of age on treatment was also a remarkable factor affecting EAP program outcomes, Schultz [60] and Signal et al. [59] suggested their approach was more effective in reaching the youngest children.
Given that EAP is particularly novel and under-researched, it is important that attention be paid to both the theoretical foundations and clinical practices of the therapy. It is likely that failure to account for this variation may contribute to the inconsistencies that exist within literature. The potential benefits attributed to EAP and its outcomes have been incomplete in terms of the effectiveness of the interventions with studies showing no clear results for PTSD [61]. There were several limitations, and despite considering EAP may be an effective additional treatment modality for healing trauma, Mueller and McCullough [15] found no evidence that EAP was more effective than traditional office-based, trauma-focused cognitive behavioral therapy. Both works found moderate to high scores of human-animal bonding at pretest, reducing the potential impacting effect of improvement. Moreover, in Mueller and McCullough’s [15] study they found that despite higher post-traumatic stress symptoms at baseline in Controls, there were no differences between groups in the reduction of symptoms across time points. McCullough’ s group [61] also observed several participants scored increased symptomatology at post-test. This phenomenon could reflect the individuals’ emotional state, state of anxiety, heightened for novelty, perceived danger or threat nervous system activity, and most probably unrelated to the abuse, or reflect the nature of PTSD which is that of declining and flowing symptoms [65]. Healing occurs during those comparatively tranquil periods when the traumatized individual can think more clearly and thus comprehend the lessons learned from the EAP experience. This factor indicates the need for test taking at a variety of intervals and over longer time periods.
Gibbons et al. [58] and Coffin [62] mentioned their concerns about the rigor of the psychometric testing they used, considering the number of young participants who were able to fill the questionnaires, or their potential difficulties in understanding all items used. Also, Kemp et al. [12] and Tsantefski [56] presented several skills improvements, with their EAP program, but couldn’t establish whether the character of the program was acting, or if were mere novelty effects. To increase the reliability of the efficacy of their interventions, EAP should also compare with other interventional programs e.g., art or music therapy, over the same period. Moreover, in Tsantefski et al. [56] report, the parents were not blind to their child’s involvement in the program and their expectations may have influenced their perception of their child’s behavior, thus, potentially, overestimated or underestimated the effects of EAP. Then, the possibilities that participating in a new recreational activity and the presence of supportive adults may have accounted for the difference in outcomes the authors have found. Identifying gaps in the current literature can offer valuable information for clinicians and practitioners working with this population.
While standardizing the type and severity of the problem and excluding concurrent therapies may have helped address some issues, the presence of limitations in the selected studies raises questions about the underlying mechanisms and may render it difficult to assess their reliability, and the differences in outcomes.
4.3. Methodological Considerations
Many researchers have theorized about the working mechanisms in EAP and several promising interventions and model theories have been proposed across literature, as particularly beneficial in addressing the sequelae of trauma in children and adolescents.
It is right that youth who had negative interactions with grownups can view therapists, teachers, and adults in general, with apprehension; and, that EAP may offer a unique environment in which children can feel safe, secure, and supported to grow personally and socially by overcoming their fears [45]. However, it is crucial to consider some important factors and make prudent recommendations for research focusing on rational elements.
Over the past few years, the concept of psychotherapy with horses has evolved, from Karol in 2007 [39] to Frederick et al., in 2015 [50]. However, there is still a misunderstanding of terms in this field. Generally, psychotherapy with horses refers to a therapy aimed at treating mental health disorders, in which the psychodynamic work within the session is guided by a qualified therapist. In contrast, other approaches incorporate horses into mental health support, such as equine-assisted learning (EAL) or equine-assisted mental health (EAMH), which have different goals from EAP, as indicated by Bachi et al. [57].
In conducting the present scoping review, the process of selecting studies was a crucial and rigorous step, which posed certain challenges, as confusing terms have been misused by some authors. For example, Cagle-Holtcamp et al. [53] mentioned in their work that their "objectives were to determine if Equine-Assisted Learning (EAL) as a form of therapy would promote learning by creating an emotionally safe environment." However, as previously mentioned, in EAL, the goal is to teach and develop life skills and coping skills, depending on the modality and providers in the EAL program/session. The authors did not intend to address anything related to mental health recovery, past events, or traumas; therefore, this study was excluded. Another challenge was presented by Cofin [62] whose project, Nguudu Barndimanmanha, aimed to address the trauma of Aboriginal youth in the areas of grief, loss, and trauma through the evaluation of alternative therapies for a historically traumatized population. However, they called their project "Improving Social and Emotional Wellbeing in Aboriginal Youth Through EAL". The use of EAL in this context did not align with typical learning goals, but rather with therapeutic goals. Therefore, the study was included in the present review.
In this review we also highlight the significance of establishing the frequency and duration of the intervention when assessing the efficacy of EAP. By scrutinizing the specifics of the interventions, we can gain better insights into how EAP can be effective in addressing the needs of young people exposed to trauma or neglect. Standardizing interventions is crucial to ensure the study's findings are reliable and valid.
Finally, while examining the effectiveness of interventions involving horses, most studies lack detail of the horse`s role. Ewing et al. [66] emphasize that therapists conducting EAP must have horse knowledge and experience, in addition to their clinical background. Ensuring the suitability of the animal is of paramount importance. The horses used for the therapy need to be unfailing and minimally predictable. Fearfulness and aversion to horses may be therefore a relevant and impactful variable. Schultz et al. [60] put as exclusion criteria for participation the children who had an aversion to horses. in addition to trusty equines, the young participants should be assessed for their comfort around the horses, and the staff should be present to ensure safety. After all it is this deep alliance between the young teens, therapist, and the horse, the basis for the therapeutic.
5. Conclusions
The body of literature here collected suggests that EAP holds much promise and may be particularly beneficial for treating vulnerable youth with a history of trauma, abuse, and emotional distress, but also emphasizes the need for more rigorous, reliable, and validated measures in research, to shed light on psychotherapeutic assets using equines, and to better quantify its impact. The present review identified inconsistencies in concepts, methods, samples, and types of publication, making the existing data difficult for mental health professionals to develop useful guidelines and treatment recommendations. The review did not substantively address the efficacy of EAP for youth exposed to trauma.
Further research to better understand its effectiveness and to refine program models with larger, more diverse samples and true random assignment to reduce confounding variables are needed before any definitive conclusions can be made about the efficacy of EAP. These future well-designed studies could provide valuable insights into the efficacy of EAP as a treatment modality for recovering from childhood trauma.
Author Contributions
Conceptualization, IPF, and CS.; methodology, IPF, KO, and SA; validation, IPF and CS.; formal analysis. IPF, KO, and SA; investigation, IPF and KO; writing—original draft preparation, IPF.; writing—review and editing, IPF and SA; Supervision, CS.; funding acquisition, CS. All authors have read and agreed to the published version of the manuscript.
Funding
This research did not receive any specific grant from funding agencies in the public, commercial or not-for-profit sectors.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Acknowledgments
The authors thank to Andrés García-Gómez for the great help, assistance and inspiring ideas to constructing this article
Conflicts of Interest
The authors declare no conflicts of interest.
References
- World mental health report: transforming mental health for all. Geneva: World Health Organization; 2022. Licence: CC BY-NC-SA 3.0 IGO.
- Pereira-Figueiredo, I., Umeoka, E.H.L. Stress: Influences and Determinants of Psychopathology. Encyclopedia 2024, 4, 1026-1043. [CrossRef]
- Spytska, L. Psychological trauma and its impact on a person’s life prospects. Scientific Bulletin of Mukachevo State University. Series Pedagogy and Psychology 2023 9(3), 82-90.
- Roberts, H., & Honzel, N. The Effectiveness of Equine-Facilitated Psychotherapy in Adolescents with Serious Emotional Disturbances. Anthrozoös, 2020. 33:1, 133-144. [CrossRef]
- Lippard, E. T., & Nemeroff, C. B. The Devastating Clinical Consequences of Child Abuse and Neglect: Increased Disease Vulnerability and Poor Treatment Response in Mood Disorders. Am J Psychiatry 2019, 177(1), 20. [CrossRef]
- Harvey, C., Jedlicka, H., & Martinez, S. A Program Evaluation: Equine-Assisted Psychotherapy Outcomes for Children and Adolescents. Child Adolesc Social Work J. 2020 6, 665–675. [CrossRef]
- Adams, C., Arratoon, C., Boucher, J., Cartier, G., Chalmers, D., Dell, C.A., Dell, D., Dryka, D., Duncan, R., Dunn, K., Hopkins, C., Longclaws, L., MacKinnon, T., Sauve, E., Spence, S., & Wuttunee, M. The Helping Horse: How Equine Assisted Learning Contributes to the Wellbeing of First Nations Youth in Treatment for Volatile Substance Misuse. Hum Anim Interact Bull. 2015 Jul; 1(1):52-75.
- Naste, T.M., Price, M., Karol, J., Martin, L., Murphy, K., Miguel, J., & Spinazzola, J. Equine Facilitated Therapy for Complex Trauma (EFT-CT). J Child Adolesc Trauma. 2018, 11(3) 289-303. [CrossRef]
- Atherton, W., Meola, C., & Pritchard, K. Innovative Equine Facilitated Psychotherapy Intervention for Adolescent Addiction Treatment: A Pilot Study. Int J High Risk Behav Addict. 2020 9(3): e103877. [CrossRef]
- Dell, C., Chalmers, D., Bresette, N., Swain, S., Rankin, D., & Hopkins, C. A Healing Space: The Experiences of First Nations and Inuit Youth with Equine-Assisted Learning (EAL). Child & Youth Care Forum 2011, 40, 319–336. [CrossRef]
- Craig, E.A., Nieforth, L., & Rosenfeld, C. Communicating Resilience among Adolescents with Adverse Childhood Experiences (ACEs) through Equine Assisted Psychotherapy (EAP). West. J. Commun 2020b, 84(4), 400–418. [CrossRef]
- Kemp, K., Signal, T., Botros, H., Taylor, N., & Prentice, K. Equine Facilitated Therapy with Children and Adolescents Who Have Been Sexually Abused: A Program Evaluation Study. J Child Fam Stud 2014, 23(3), 558–566. [CrossRef]
- Pereira-Figueiredo, I., Sancho, C., Carro, J., López, D.E., Gómez-Nieto, R. and Castellano, O. Sex-Dependent Effects of Prenatal Stress on Learned Helplessness and Anxiety-Related Behaviours in Wistar Rats. J Behav Brain Sci, 2015, 5, 251-265. [CrossRef]
- Wrobel, A. L., Cotton, S. M., Jayasinghe, A., Diaz-Byrd, C., Yocum, A. K., Turner, A., McInnis, M. G. Childhood trauma and depressive symptoms in bipolar disorder: a network analysis. Acta Psychiatrica Scandinavica 2023 , 147(3), 286-300. [CrossRef]
- Mueller, M.K., & McCullough, L. Effects of Equine-Facilitated Psychotherapy on Post-Traumatic Stress Symptoms in Youth. J Child Fam Stud 2017, 26 (4), 1164–1172. [CrossRef]
- Craig, E.A. Equine-Assisted Psychotherapy Among Adolescents with ACEs: Cultivating Altercentrism, Expressiveness, Communication Composure, and Interaction Management. Child Adolesc Social Work J 2020b. [CrossRef]
- Eckshtain, D., Kuppens, S., Ugueto, A., Ng, M. Y., Vaughn-Coaxum, R., Corteselli, K., & Weisz, J. R. Meta-analysis: 13-year follow-up of psychotherapy effects on youth depression. J Am Acad Child Adolesc Psychiatry 2020, 59(1), 45-6. [CrossRef]
- Weisz, J. R., Venturo-Conerly, K. E., Fitzpatrick, O. M., Frederick, J. A., & Ng, M. Y. What four decades of meta-analysis have taught us about youth psychotherapy and the science of research synthesis. Annu Rev Clin Psychol 2023, 19, 79-105. [CrossRef]
- Dunlop, K., & Tsantefski, M. A space of safety: Children’s experience of equine-assisted group therapy. Child & Family Social Work 2018, 23(1), 16–24. [CrossRef]
- Mattila-Rautiainen, S., Brennan, R., Emond, N., Horne, V., Volpe, G., Arrieta, K. and Stergiou, A. A prospective international study of terminology in human-equine interactions preliminary results. HETI International Research and Practice 2023, 22(1), 13. [CrossRef]
- Rankins, E. M., McKeever, K. H., & Malinowski, K. Equids in Equine Assisted Services: A Scoping Review. J. Equine Vet. Sci 2023, 104825. [CrossRef]
- Benda, W., McGibbon, N.H., & Grant, K.L. Improvements in Muscle Symmetry in Children with Cerebral Palsy after Equine-Assisted Therapy (Hippotherapy). J Altern Complement Med 2003, 9 (6), 817–825. [CrossRef]
- Krejčí, E., Janura, M., & Svoboda, Z. The benefit of hippotherapy for improvement of attention and memory in children with cerebral palsy: A pilot study. Acta Gymnica, 2015, 45(1), 27–32. [CrossRef]
- Rothe, E.Q., Vega, B.J., Torres, R.M., Soler, S.M.C., & Pazos, R.M.M. From kids and horses: Equine facilitated psychotherapy for children. Int J Clin Health Psychol 2005, 5(2), 373–383.
- Hemingway, A., & Sullivan, K. Reducing the incidence of domestic violence: An observational study of an equine-assisted intervention. Family Process, 2022 61(2), 549–570. [CrossRef]
- Hoagwood, K., Vincent, A., Acri, M., Morrissey, M., Seibel, L., Guo, F., Flores, C., Seag, D., Peth Pierce, R., & Horwitz, S. Reducing Anxiety and Stress among Youth in a CBT-Based Equine-Assisted Adaptive Riding Program. Animals: An Open Access Journal from MDPI, 2022, 12(19), 2491. [CrossRef]
- Yorke, J., Adams, C., & Coady, N. Therapeutic Value of Equine-Human Bonding in Recovery from Trauma. Anthrozoos 2008, 21 (1), 17–30. [CrossRef]
- Burgon, H. Queen of the world: Experiences of at-risk young people participating in equine-assisted learning/therapy. J. Soc. Work Pract 2011, 165-18. [CrossRef]
- Kesner, A., & Pritzker, S. Therapeutic Horseback Riding With Children Placed In The Foster Care System. Revision. J. Consc Transform, 2008, 30, 77–87.
- Trotter, K.S., Chandler, C.K., Goodwin-Bond, D., & Casey, J. A comparative study of the efficacy of group equine assisted counseling with at-risk children and adolescents. J. Creat. Ment. Health, 2008 3(3), 254–284. [CrossRef]
- Hood, P., & Wilson, C. If You’re Hyper It Calms You Down; Young People’s Experiences of an Irish Equine Facilitated Program. J. Creat. Ment. Health. 2021, 16 (2): 153-167. [CrossRef]
- Punzo, K., Skoglund, M., Carlsson, I.M., & Jormfeldt, H. Experiences of an Equine-Assisted Therapy Intervention among Children and Adolescents with Mental Illness in Sweden - A Nursing Perspective. Issues in Mental Health Nursing 2022, 43 (12), 1080–1092. [CrossRef]
- Weiss-Dagan, S., Naim-Levi, N., & Brafman, D. Therapeutic horseback riding for at-risk adolescents in residential care. Child Adolesc. Psychiatry Ment 2022, 16 (1), 1–13. [CrossRef]
- Kendall, E., Maujean, A., Pepping, C. A., Downes, M., Lakhani, A., Byrne, J., & Macfarlane, K. A systematic review of the efficacy of equine-assisted interventions on psychological outcomes. Eur. J. Psychother. Couns 2015, 17(1), 57–79. [CrossRef]
- Kaiser, L., Smith, K., Heleski, C., & Spence, L. Effects of a therapeutic riding program on at-risk and special education children. J. Am. Vet. Med. Assoc 2006, 228, 46–52. [CrossRef]
- Pendry, P., Carr, A.M., & Vandagriff, J.L. Adolescents’ Affective and Physiological Regulation Shape Negative Behavior During Challenging Equine Assisted Learning Activities. Front Vet Sci. 2018 4; 5:300. [CrossRef]
- Bachi, K. Application of Attachment Theory to Equine-Facilitated Psychotherapy. J Contemp Psychother 43, 187–196 2013. [CrossRef]
- Kruger, K. A., & Serpell, J. A. Animal-assisted interventions in mental health: Definitions and theoretical foundations. In A. H. Fine (Ed.), Handbook on animal-assisted therapy: Theoretical foundations and guidelines for practice (2nd ed., 2006 pp. 21–38). Academic Press.
- Karol, J. Applying a traditional individual psychotherapy model to Equine-facilitated Psychotherapy (EFP): theory and method. Clin Child Psychol Psychiatry. 2007 12 (1):77-90. [CrossRef]
- Diaz, L., Gormley, M.A., Coleman, A., Sepanski, A., Corley, H., Perez, A., Litwin, A.H., Equine-assisted services for individuals with substance use disorders: a scoping review. Subst Abuse Treat Prev Policy 2022 17. [CrossRef]
- Hauge, H., Kvalem, I. L., Berget, B., Enders-Slegers, M.-J., & Braastad, B.O. Equine-assisted activities and the impact on perceived social support, self-esteem and self-efficacy among adolescents- an intervention study. Int J Adolesc Youth, 2014 19 (1), 1–21. [CrossRef]
- Lentini, J.A., Knox, M.S. Equine-facilitated psychotherapy with children and adolescents: An update and literature review. J Creativity Ment Health. 2015 10 (3), 278-305. [CrossRef]
- Cantin, A., & Marshall-Lucette, S. Examining the Literature on the Efficacy of Equine Assisted Therapy for People with Mental Health and Behavioural Disorders. Ment Health Learn Disabil Res Pract, 2011 8(1), 51–61. [CrossRef]
- Anestis, M.D., Anestis, J.C., Zawilinski, L.L., Hopkins, T.A., & Lilienfeld, S.O. Equine-related treatments for mental disorders lack empirical support: A systematic review of empirical investigations. J Clin Psychol, 2014 70(12), 1115–1132. [CrossRef]
- Wilkie, K. D., Germain, S., & Theule, J. Evaluating the Efficacy of Equine Therapy Among At-risk Youth: A Meta-analysis. Anthrozoos, 2016 29(3), 377–393. [CrossRef]
- Staudt, M., & Cherry, D. Equine-Facilitated Therapy and Trauma: Current Knowledge, Future Needs. Adv Soc Work 2017, 18, 403. [CrossRef]
- Haig, L., & Skinner, K. Use of Equine-Assisted Services to Improve Outcomes Among At-Risk and Indigenous Youth: A Scoping Review. Front. Public Health 2022, 10, 730644. [CrossRef]
- Page, M. J., Mckenzie, J.E., Bossuyt, P.M., Boutron, I., Hoffmann, T.C., Mulrow, C.D., Shamseer, L., Tetzlaff, J.M., Akl, E.A., Brennan, S.E., Chou, R., Glanville, J., Grimshaw, J.M., Hróbjartsson, A., Lalu, M.M., Li, T., Loder, E. W., Mayo-Wilson, E., Mcdonald, S., Moher, D. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews 2021. [CrossRef]
- Higgins, J.P.T., Thomas, J., Chandler, J., Cumpston, M., Li, T., Page, M.J., Welch, V.A. (editors). Cochrane Handbook for Systematic Reviews of Interventions version 6.3 (updated February 2022). Cochrane, 2022. Available from www.training.cochrane.org/handbook.
- Frederick, K., Hatz, J., & Lanning, B. Not Just Horsing Around: The Impact of Equine-Assisted Learning on Levels of Hope and Depression in At-Risk Adolescents. Community Ment Health J. 2015 ;51(7):809-17. [CrossRef]
- Hemingway, A., Meek, R., & Hill, C.E. An Exploration of an Equine-Facilitated Learning Intervention with Young Offenders. Soc. Anims2015, 23(6), 544–568. [CrossRef]
- Ho, N., Zhou, J., Fung, D., & Kua, P. Equine-assisted learning in youths at-risk for school or social failure. Cogent Education 2022 , 4: 1334430. [CrossRef]
- Cagle-Holtcamp, K., Nicodemus, M.C., Parker, J., & Dunlap, M.H. Does equine assisted learning create emotionally safe learning environments for at-risk youth? J. Youth Develop. 2019, 14(4), 232–252. [CrossRef]
- Carlsson, C., Ranta, D., & Traeen, B. Mentalizing and Emotional Labor Facilitate Equine-Assisted Social Work with Self-harming Adolescents. Child Adolesc Social Work J. 2015 32:329–339. [CrossRef]
- Carlsson, C. Triads in Equine-Assisted Social Work Enhance Therapeutic Relationships with Self-Harming Adolescents. Clinic. Soci Work J. 2017, 45(4), 320–331. [CrossRef]
- Tsantefski, M., Briggs, L., Griffiths, J., & Tidyman, A. An open trial of equine-assisted therapy for children exposed to problematic parental substance use. Health Soc Care Community 2017, 25(3), 1247–1256. [CrossRef]
- Bachi, K., Terkel, J., & Teichman, M. Equine-facilitated psychotherapy for at-risk adolescents: The influence on self-image, self-control and trust. Clin. Child Psychol. Psychiatry 2011 17(2) 298–312. [CrossRef]
- Gibbons, J., Cunningham, C., Paiz, L., Poelker, K., & Chajón, A. Now, he will be the leader of the house: An equine intervention with at-risk Guatemalan youth. Int J Adolesc Youth 2017, 22, 1–15. [CrossRef]
- Signal, T., Taylor, N., Botros, H., Prentice, K., & Lazarus, K. Whispering to horses: Childhood sexual abuse, depression and the efficacy of Equine Facilitated Therapy. Sexual Abuse in Australia and New Zealand: An Interdisciplinary Journal. 2013 5(1), 24-32.
- Schultz, P.N., Remick-Barlow, G.A., & Bobbins, L. Equine-assisted psychotherapy: A mental health promotion/intervention modality for children who have experienced infra-family violence. Health Soc Care Community 2007, 15(3), 265–271. [CrossRef]
- McCullough, L., Risley-Curtiss, C., & Rorke, J. Equine Facilitated Psychotherapy: A Pilot Study of Effect on Posttraumatic Stress Symptoms in Maltreated Youth. J. Infant Child Adolesc. Psychother 2015. 14, 158–173. [CrossRef]
- Coffin, J. The Nguudu Barndimanmanha Project-Improving Social and Emotional Wellbeing in Aboriginal Youth Through Equine Assisted Learning. Front Public Health 2019, 7. [CrossRef]
- Bennett, B., & Woodman, E. The Potential of Equine-Assisted Psychotherapy for Treating Trauma in Australian Aboriginal Peoples. Condor 2019, 121(4), 1041–1058. [CrossRef]
- Bizub, A.L., & Davidson, L. “It’s like being in another world”: Demonstrating the benefits of therapeutic horseback riding for individuals with psychiatric disability. Psychiatr. Rehabil. J. 2003, 26(4), 377–384. [CrossRef]
- Earles, J. L., Vernon, L. L., & Yetz, J.P. Equine-Assisted Therapy for Anxiety and Posttraumatic Stress Symptoms. J. Trauma. Stress 2015 28(2), 149–152. [CrossRef]
- Ewing, C., MacDonald, P., Taylor, M., & Bowers, M. Equine-Facilitated Learning for Youths with Severe Emotional Disorders: A Quantitative and Qualitative Study. Child & youth care forum 2007, 36, 59–72. [CrossRef]
Figure 1.
PICOS strategy (Participants, Interventions, Comparisons, Outcomes, and Study design) used in the review process.
Figure 1.
PICOS strategy (Participants, Interventions, Comparisons, Outcomes, and Study design) used in the review process.
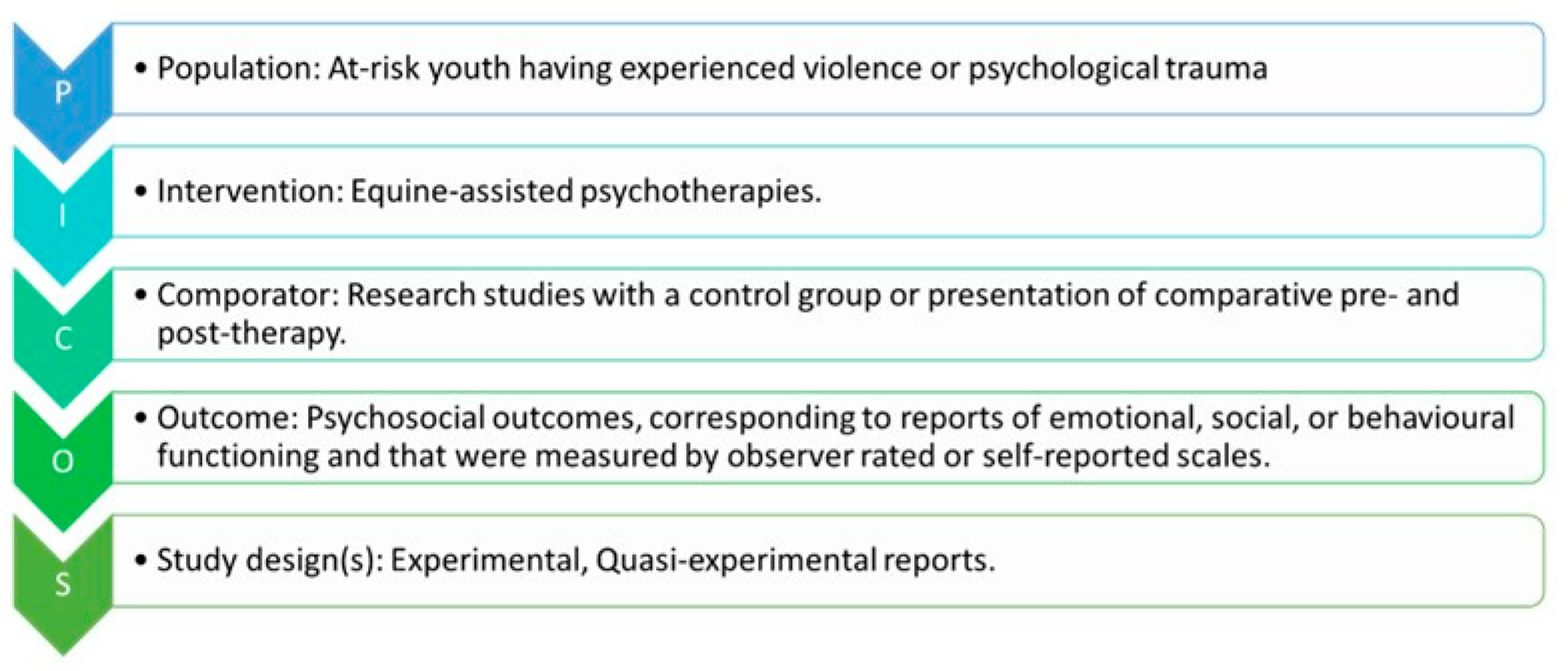
Figure 2.
PRISMA flow Diagram with the different stages of the review process. Initially, 537 research articles were identified across 5 databases and other registers after removing duplicates. Following the application of selection criteria, 27 publications were considered eligible for further examination. Ultimately, 9 publications were selected for analysis after detailed review.
Figure 2.
PRISMA flow Diagram with the different stages of the review process. Initially, 537 research articles were identified across 5 databases and other registers after removing duplicates. Following the application of selection criteria, 27 publications were considered eligible for further examination. Ultimately, 9 publications were selected for analysis after detailed review.

Table 1.
Eligibility criteria for the study.
| Inclusion Criteria | Exclusion Criteria | ||
|---|---|---|---|
|
Participants |
youth aged 6-25 that had experienced continuous psychological trauma or abandonment as children (ACEs) and had any reported intellectual disability (IQ >70). Incorporating living equines. |
Youth that did not suffer ACEs or psychological trauma With intellectual disability, physical condition, or lifelong neurological disorders (such as cerebral palsy or autism spectrum disorders). Not using specifically equines |
|
|
Program/ Intervention |
Including a set of activities with a particular long-term aim. Under the oversight of a mental health professional. Goals focus on psychosocial recovery, related to emotional, social, or behavioral functioning. Promotes at least one psychosocial measure (depression, emotional deregulation, etc.) |
Not a set of activities in a well-defined program. Delivered with no informed presence or oversight of a mental health professional. Focused on physical treatment or recreational horse riding, or the outcome evaluation did not include measures of psychosocial recovery. Used a combination of therapies or programs. |
|
|
Outcome Evaluation |
Studies that were measured using some form of quantitative analyses (observer-rated, or self-reported scales with numerical scales. Studies with a control group or presentation of comparative pre- and post-therapy results with clearly defined inclusion and exclusion criteria for the study groups and controls. |
Studies without quantitative measures. |
|
|
Type of Article |
Original research studies published in peer-reviewed journals in English. |
Original research studies not published in English. Gray literature (not peer-reviewed articles: conference abstracts, opinion pieces, etc.). Book chapters, short communications, and reviews. |
Table 3.
Characteristics of the 17 studies screened which involved EAP interventions for children and young people exposed to trauma. All studies explicitly mentioned “body language” or “natural Horsemanship”, being EAGALA the intervention model choice in 4 of the studies, with some using variations and mounted activities. Groundwork and riding were the most typical interventions, used in 7 studies, followed by groundwork in 6 studies; 2 studies used only riding, while 2studies did not specify the type of activities involved. Abbreviations: ADOL: adolescents; CH: children; ADU: adults; G: Ground; R: Riding; QUA: quantitative; QL: qualitative, EXP: experimental.
Table 3.
Characteristics of the 17 studies screened which involved EAP interventions for children and young people exposed to trauma. All studies explicitly mentioned “body language” or “natural Horsemanship”, being EAGALA the intervention model choice in 4 of the studies, with some using variations and mounted activities. Groundwork and riding were the most typical interventions, used in 7 studies, followed by groundwork in 6 studies; 2 studies used only riding, while 2studies did not specify the type of activities involved. Abbreviations: ADOL: adolescents; CH: children; ADU: adults; G: Ground; R: Riding; QUA: quantitative; QL: qualitative, EXP: experimental.
| PARTICIPANTS | STUDY | TREATMENT INTERVENTION | ||||||||||||||
| Authors | N | Gender | Ages | Age categories | Control | Intervention | Number of sesions | Duration in min | Type | Design | ||||||
| 1 | Bachi et al., 2011 | 29 | NO SPECIFY | 14- 18 | ADOL | YES | DEPENDS | WEEKLY | 14 - 26 | 50 | G+R | INDIVIDUAL | QUA | INCLUDED | ||
| 2 | Coffin, 2019 | 20 | 15 girls, 5 boys | 11- 16 | ADOL | NO | Gestalt | WEEKLY | 6-10 | 45-50 | G | DEPENDS | QUA | INCLUDED | ||
| 3 | Gibbons et al., 2017 | 37 | 14 girls, 23 boys | 15- 23 | ADO+ ADU | YES | Join-Up® | 2 DAYs | all day | all day | G | INDIVIDUAL | EXP | INCLUDED | ||
| 4 | McCullough et al., 2015 | 11 | 5 girls, 6 boys | 10- 18 | CH + ADOL | NO | NO SPECIFY | WEEKLY | 8 | 90-120 | NO SPECIFY | NO SPECIFY | QUA | INCLUDED | ||
| 5 | Mueller and McCullough, 2017 | 54 | 9 girls, 45 boys | 10- 18 | CH + ADOL | YES | NO SPECIFY | WEEKLY | 10 | 120 | G+R | GROUP | QUA | INCLUDED | ||
| 6 | Schultz et al., 2007 | 63 | 26 girls, 37 boys | 4- 16 | SEPARATED | NO | EAGALA | WEEKLY | 19 | NO SPECIFY | G | INDIVIDUAL | QUA | INCLUDED | ||
| 7 | Kemp et al., 2013 | 30 | 24 girls, 6 boys | 8 -17 | SEPARATED | NO | EAGALA | WEEKLY | 9- 10 | 90 | G | GROUP | QUA | INCLUDED | ||
| 8 | Signal et al., 2013 | 30 | 24 girls, 6 boys | 8- 17 | SEPARATED | NO | EAGALA | WEEKLY | 9- 10 | 90 | G | GROUP | QUA | INCLUDED | ||
| 9 | Tsantefski et al., 2017 | 41 | 24 girls, 7 boys | 7- 13 | CHILD | NO | HORSEMANSHIP | WEEKLY | 12 | 120 | G+R | GROUP | QUA | INCLUDED | ||
| 10 | Roberts and Honzel, 2020 | 37 | 9 girls, 25 boys | 12- 17 | ADOL | NO | NO SPECIFY | WEEKLY | 8 | 60 | G+ R | GROUP | QUA | EXCLUDED | ||
| 1 | Carlsson et al., 2015 | 12 | girls | 14- 21 | ADOL | NO | DEPENDS | NO SPECIFY | NO SPECIFY | NO SPECIFY | G+R |
INDIVIDUAL |
QL | EXCLUDED | ||
| 2 | Carlsson, 2017 | 12 | girls | 14 - 21 | ADOL | NO | DEPENDS | NO SPECIFY | NO SPECIFY | NO SPECIFY | G+R |
INDIVIDUAL |
QL | EXCLUDED | ||
| 3 | Craig, 2020a | 11 | girls | 13 - 17 | ADOL | NO | NO SPECIF | NO SPECIFY | DEPENDS | DEPENDS | NO SPECIFY |
INDIVIDUAL |
QL | EXCLUDED | ||
| 4 | Craig et al., 2020b | 12 | girls | 13 - 17 | ADOL | NO | TUTORING | 2 X WEEK | NO SPECIFY | 180 or plus | G+R |
INDIVIDUAL |
QL | EXCLUDED | ||
| 5 | Dunlop and Tsantefski, 2018 | 33 | 18 girls, 15 boys | 7- 13 | CHILD | NO | EAGALA | WEEKLY | 9 | 120 | G | GROUP | QL | EXCLUDED | ||
| 6 | Kesner and Pritzker, 2008 | 14 | 6 girls, 8 boys | 5- 17 | CH + ADOL | NO | RIDING | WEEKLY | 10 | 45-60 | R | INDIVIDUAL | QL | EXCLUDED | ||
| 7 | Weiss-Dagan et al., 2022 | 19 | boys | 14- 19 | ADOL | NO | RIDING | WEEKLY | 6 | 60 | R | INDIVIDUAL | QL | EXCLUDED | ||
Table 4.
Results of included studies in the scoping review. Abbreviations: + positive results; > Significant improvement/increase; < Significant decrease; = did not significantly change; OSIQ- Offer self-image questionnaire; SDQ- Strengths and Difficulties Questionnaire; YLLSD -Youth Leadership Life Skills Development Scale; TRIM- Transgression-related interpersonal motivations inventory; NBAS- Normative Beliefs about Aggression Scale; ERQ Emotion Regulation Questionnaire: CERQ - Cognitive Emotion Regulation Questionnaire; CBC- Child Behaviour Checklist; CRIES-13 - Children’s revised Inventory of Events; HABS- Human-Animal Bond Scale; GAF- Global Functioning Scale.
Table 4.
Results of included studies in the scoping review. Abbreviations: + positive results; > Significant improvement/increase; < Significant decrease; = did not significantly change; OSIQ- Offer self-image questionnaire; SDQ- Strengths and Difficulties Questionnaire; YLLSD -Youth Leadership Life Skills Development Scale; TRIM- Transgression-related interpersonal motivations inventory; NBAS- Normative Beliefs about Aggression Scale; ERQ Emotion Regulation Questionnaire: CERQ - Cognitive Emotion Regulation Questionnaire; CBC- Child Behaviour Checklist; CRIES-13 - Children’s revised Inventory of Events; HABS- Human-Animal Bond Scale; GAF- Global Functioning Scale.
| AUTHORS AND YEAR | ISSUE |
EVALUATION PROTOCOL | METHODS AND OUTCOME MEASURE/S |
RESULTS of EAP | LIMITATIONS or STRONG POINTS |
||
| 1 | Bachi et al., 2011 |
NEGLET (RESIDENTS) |
At 3 points: pre-EAP, post-EAP, after 1-year questionnaires. |
Self-image: OSIQ. Self-control using a schedule (UNP). Trust (Seven items from Children’s Interpersonal Trust Scale) |
|
Trend of + change in 4 research parameters. Trend of > general life-satisfaction vs Control group. > level of improved self-control and trust. > level of self-image among both groups. |
Sessions varied from 14 to 26. Gender is not specified. Type of intervention is not specified. One-year follow-up. |
| Student’s Life Satisfaction Scale adjusted for adolescents. | |||||||
| 2 | Coffin, 2019 | BEHAVIORAL ISSUES |
At 2 points: pre and post-EAP. |
“Body check"- to promote self-awareness and self-regulation | + in the self-reported data for worry-related sleeplessness. |
Not rigorous psychometric testing |
|
| SDQ. | + in incidences of anger. | ||||||
| Tool to assess changes in social and emotional wellbeing. | |||||||
|
Gibbons et al., 2017 |
ABUSE or VIOLENCE |
At 3 points: pre-EAP, midpoint, post-EAP. |
YLLSD 30-item self-report (Smith et al., 2005) TRIM (McCullough, 1998) NBAS (Huesmann & Guerra, 1997) ERQ (Gross & John, 2003) CERQ (Garnefski et al., 2001) Mentor Evaluations and CBC (Ladd & Profilet, 1996) |
Multiple benefits reported: > Self-reported leadership + emotion regulation, < aggression, and interpersonal response to threat. =TRIM scores. |
Evaluations based on participants, mentors at the school and parents. Random assignment. Multiple psychometric instruments. |
||
| 3 | |||||||
| 4 | McCullough et al., 2015 | VIOLENCE |
At 3 points: pre-EAP, midpoint, post-EAP (Week 10). |
CRIES-13 (2005) Attachment: HABS (Terpin, 2004) |
Multimodal EAP treatment effects working in multiple directions. | Results not conclusive. Small sample size. Does not specify the type of intervention. |
|
| 5 | Mueller and McCullough, 2017 | TRAUMA |
At 3 points: pre-EAP, Week 1, mid-EAP, Week 5, post-EAP, Week 10. |
CRIES-13 (2005) Attachment: HABS (Terpin, 2004) |
< Post-traumatic stress symptoms in both groups. EAP group did not < more than the control group in PTSD symptoms. = Across the HABS items and across the 3 item points. Positive Correlation between 10 HABS scores and the change in PTSD symptoms. |
Quasi-randomization. | |
| 6 |
Schultz et al., 2007 |
VIOLENCE/ABUSE |
At 2 points: pre-EAP and post-EAP. |
Scores on the Children’s Global Functioning (GAF) Scale |
> in GAF scores (greatest in youngest and those with worst history of abuse). |
Analysis divided into three age categories. GAF scores the only outcome measure. |
|
| 7 |
Kemp et al., 2013 |
ABUSE |
At 3 points: pre-EAP; pre-EAP, after in-clinic counselling; post-EAP. |
Children’s Depression Inventory (Kovacs, 2003) or Beck Depression Inventory; Child Behaviour Checklist Trauma; Symptom Checklist; Beck Anxiety Inventory (Beck et al. 1996) |
= in Time 1 and Time 2 assessments. > in functioning from Time 2 to Time 3 in all psychometric measures. |
Analysis divided into age categories. Scales adapted to each age group. |
|
| 8 |
Signal et al., 2013 |
SEXUAL ABUSE |
At 3 points: pre-EAP; pre-EAP, after in-clinic counselling; post-EAP. |
Beck Depression Inventory Children’s Depression Inventory (Kovacs, 2003) |
> Depressive symptomatology. |
Analysis divided into age categories. Scales adapted to each age group. Compares Efficacy Across Groups and Ethnicity. |
|
|
9 |
Tsantefski et al., 2017 |
NEGLET (PPSU) |
At 2 points: baseline and post-EAP. |
(25-item SDQ) behaviours |
Parents observed < in emotional problems: as anxiety and somatic complaints. < in hyperactive behaviours and attention difficulties. Teachers reported = in difficult behaviour and < in hyperactivity. |
Results are based only on parents’ and teachers’ perceptions. |
|
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



