Submitted:
10 December 2024
Posted:
11 December 2024
You are already at the latest version
Abstract
How to determine suitable animal models of anxiety disorders and post-traumatic stress disorders (PTSD) for screening anxiolytic drugs and linking preclinical and clinical research is a crucial issue. This review paper provides background knowledge and critical determination to the animal models for discussing this issue. Moreover, this article analyzes the characteristics, properties, advantages, and disadvantages of various animal models of anxiety disorders and PTSD. It offers an overview of the pathophysiology, treatments, prevalence, and symptoms of anxiety disorders in the clinics. Furthermore, it comprehensively discusses pharmacological treatments and neural mechanisms, as well as the types and properties of the animal models of anxiety disorders in shaping and testing anxiety behaviors. In light of the previous literature discussion, we can understand the different functions of the animal models of anxiety disorders and PTSD to help us link preclinical and clinical research. Animal models are used in advanced drug discovery programs, specifically in psychiatry and neuroscience research. The challenge for the future will be to keep pace with developing the appropriate animal models of anxiolytic drugs to improve the translation of large datasets obtained to clinics.
Keywords:
animal model
; anxiety disorders
; anxiolytic drugs
; post-traumatic stress disorders
; preclinical and clinical research
1. Introduction
Depending on the diagnosis of the Diagnostic and Statistical Manual of Mental Disorders (DSM), anxiety disorders are characterized by excessive fear, anxiety, and related disturbances [1]. Anxiety disorders present heterogenous categories that include generalized anxiety disorder, panic disorder, agoraphobia, conduct disorder, social anxiety disorder (SAD), illness anxiety disorder, bereavement, separation anxiety disorder, selective mutism, obsessive-compulsive disorder (OCD), trauma- and stressor-related disorders, post-traumatic stress disorder (PTSD), and acute stress disorder (ASD) [1,2,3]. Although the nosology of anxiety disorders reveals a phenotypical discrepancy in the human model, it is difficult to dissociate the biomarkers and behavioral mechanisms from the various anxiety disorders in the animal model [4,5]. Thus, it is challenging to determine the animal models most appropriate for evaluating the neural mechanisms.
Accordingly, the role of an animal model of anxiety disorders offers the potential for screening current and developing novel anxiolytic drugs [6,7]. Moreover, the most suitable and appropriate animal models are effectively utilized in understanding the behavioral and neural mechanisms of anxiety disorders via anxiogenic and anxiolytic drugs to modulate their symptoms, and the present findings can be applied in the development of novel anxiolytic medicines. Therefore, the determination of animal models of anxiety disorder is key to novel pharmacological treatments. However, it appears that researchers often do not know how to choose the validated and most appropriate animal models for specific anxiety disorders in the experimental procedures or consider the sexual differences, in part because they do not always understand the advantages and disadvantages of each model. Furthermore, researchers may struggle to determine which model has superior reliability and validity to fit their experimental purposes and link with the human models in the clinic.
The review paper addresses the abovementioned issues and offers some insights and implications for selecting ideal animal models of anxiety disorders. First, we comprehensively introduce the prevalence, symptoms, pathophysiology, and treatments of anxiety disorders, including generalized anxiety disorders (GAD), panic disorder, agoraphobia, PTSD, SAD, ASD, separation anxiety disorder, and OCD [1,8]. Although OCD, PTSD, and ASD are excluded from the conventional anxiety disorders in DSM-5, this review paper still discusses OCD, PTSD, and ASD. Second, this study examines numerous anxiolytic drugs and their mechanisms in the brain. For example, common anxiolytic drugs are always involved in the brain GABA system [6,9] or contribute to selective serotonin reuptake inhibitors (SSRIs) via the brain serotonin system [10,11]. Therefore, these distinct mechanisms may help alleviate anxiety disorder symptoms. Third, it also examined anxiolytic substances related to nonclassical neurotransmitters that act via other systems (besides classical neurotransmitters or neuropeptides) to alleviate anxiety symptoms. For example, compounds such as cannabidiol [12] and melatonin [13] were found to reduce the behaviors of anxiety disorders in animal models. Fourth and finally, this review paper analyzes the characteristics, properties, advantages, and disadvantages of various animal models of anxiety disorders, providing some suggestions as to how and when to use these animal models to build up or test anxiety disorders and PTSD, which animal models and test anxiety disorders are best for testing compounds with a specific mechanism of action.
In conclusion, this review paper aims to offer background knowledge and critical determination for screening anxiolytic drug discovery. Moreover, it can promote linking the animal model of anxiety disorders in preclinical research and clinical human studies.
2. Characteristics, Pathophysiology, and Treatments of Anxiety Disorders in the Clinic
2.1. Prevalence and Symptoms of Various Anxiety Disorders in the Clinic
In 2017, the World Health Organization reported that the total estimated number of people with anxiety disorders in the world was 264 million [14]. Moreover, it was separated by regions and showed the prevalence of anxiety disorders. For example, the African region was 10 %; the Eastern Mediterranean region was 12%; the European region was 14%; the region of the Americas was 21%; the South-East Asia region was 23%; the Western Pacific region was 20% [14]. According to the DSM-5 descriptions of anxiety disorders in clinical aspects, the essential symptoms of many anxiety disorders vary widely [1,8]; anxiety disorders are shown to be heterogeneous and exhibit diverse phenotypes in humans [2,8]. For example, the major anxiety disorders can be separated into eight phenotypical categories. The present and discussed anxiety disorders include GAD, panic disorder, agoraphobia, PTSD, SAD (i.e., social phobia), ASD, separation anxiety disorder, and OCD.
According to the DSM-5 [1], the major symptoms of GAD are chronic, excessive anxiety, and worry about various domains, including school and work performance. GAD has a 12-month prevalence of 0.9–2.9% in adults and adolescents in the United States. The major symptoms of panic disorder include recurrent unexpected panic attacks, and individuals with panic disorder are persistently concerned with and worried about further panic attacks, potentially changing their behaviors in maladaptive ways. Panic disorder has a 2–3% prevalence rate for adolescents and adults in the United States. The major symptoms of agoraphobia are intense fear or anxiety induced by an extendable range of surroundings in real or anticipated exposure; the 12-month prevalence of agoraphobia is nearly 1.7% for adolescents and adults in the United States. The major symptoms of PTSD include intrusions and avoidance of memories associated with traumatic events. The critical features of PTSD vary. Some patients encounter fear-based reexperiencing, emotional, and behavioral symptoms. Others feel anhedonic or dysphoric mood states, and negative cognitions may be most distressing. In some cases, arousal and reactive-externalizing symptoms are prominent; however, others produce dissociative symptoms predominate. Particularly, some individuals exhibit combinations of these symptom patterns. The 12-month prevalence of PTSD is 3.5% in the United States. The major symptoms of SAD include fear and anxiety about, or avoidance of, social interactions and social surroundings when they involve the possibility of being scrutinized; the 12-month prevalence of SAD is approximately 7% in the United States. The major symptoms of ASD, which follow one or more traumatic events, include the development of anxiety lasting from three days to one month after the event(s). The prevalence of ASD is less than 20% (that does not involve interpersonal assault) in the United States. The critical features of separation anxiety disorder are excessive fear or anxiety concerning separation from home or attachment figures. The 12-month prevalence of separation anxiety disorder in the United States is about 0.9–1.9% for adults, 4% in children, and 1.6% in adolescents. The major symptoms of OCD are, as the name implies, obsessions and compulsions; obsessions are chronic and repetitive thoughts, images, or urges, whereas compulsions are persistent behaviors and mental acts. The 12-month prevalence of OCD is about 1.2% in the United States. In descending order of prevalence among adults, the three most common of these eight anxiety disorders are ASD, SAD, and PTSD. The diversity of the eight disorders’ major symptoms is shown in Table 1.
2.2. Pathophysiology of Anxiety Disorders in the Clinic
A growing body of evidence showed that the dorsomedial prefrontal cortex, insula, and amygdala were involved in anxiety disorders [15,16,17,18]. The threat circuit concerning the projections between the dorsomedial prefrontal cortex and amygdala induces the activation and coupling of the dorsomedial prefrontal cortex-amygdala circuit for healthy people when they experience fear, threat, and aversive stimuli; however, anxiety disorders enhance the activations in the dorsomedial prefrontal cortex-amygdala circuit when exposing to the situation related to the danger and aversive stimuli [19]. Threat stimuli are positively associated with coupling the dorsomedial prefrontal cortex and amygdala in hyperactivation [16,17]. Therefore, the dysfunction of the dorsomedial prefrontal cortex-amygdala circuit contributes to the pathophysiology of various anxiety disorders.
2.3. Pharmacological Treatments of Anxiety Disorders in the Clinic
It is a crucial issue how to lessen the hyperactivity and coupling of the dorsomedial prefrontal cortex-amygdala circuit, leading to severe fear and vigilance symptoms of anxiety disorders. To date, numerous pharmacological treatments have been employed in clinics for eight major types of anxiety disorders in DSM-5 (Table 2). For example, benzodiazepines (BDZs) are the GABAa receptor agonists that are underlined to inhibit the activity of postsynaptic neurons for alleviating symptoms of anxiety disorders [20]. In the clinic, almost all BDZ drugs showed non-specific anxiolytic-like effects, and all BDZs can treat all anxiety disorders, such as GAD, PD, agoraphobia, PTSD, SAD, ASD, separation anxiety disorder, and OCD; only clonazepam was used in PD but no other anxiety disorders (Table 2) [20]. SSRIs have been shown to reduce the hyperactivity of the dorsomedial prefrontal cortex-amygdala circuit, resulting in the amelioration of a variety of anxiety disorders [21]. In clinical findings, GAD can be alleviated by escitalopram, paroxetine, and sertraline [19]. The behavioral symptoms of PD and agoraphobia are alleviated by escitalopram, fluoxetine, fluvoxamine, paroxetine, citalopram, and sertraline [22]. Paroxetine and sertraline treatments alleviated PTSD’s symptoms [20]. The anxiety symptoms of SAD could be effectively reduced by escitalopram, fluvoxamine, paroxetine, citalopram, and sertraline [22]. The clinical studies of OCD showed that fluoxetine, fluvoxamine, paroxetine, and sertraline could decrease the symptoms of OCD [20]. Notably, any drugs of SSRIs cannot effectively treat the symptoms of ASD and separation anxiety disorder (Table 2). Serotonin-norepinephrine reuptake inhibitors (SNRIs) are another kind of anxiolytic drug. A previous study demonstrated that SNRIs interacted with enzymes that produce enzyme inhibitions and then it alleviated anxiety symptoms, reducing the activation of the dorsomedial prefrontal cortex-amygdala circuit [23]. Duloxetine treats GAD symptoms; however, venlafaxine treatments can reduce GAD, PD, agoraphobia, and SAD (Table 2). Tricyclic antidepressant (TCA) medicines have been demonstrated to inhibit the reuptake of serotonin and norepinephrine, and they decrease the symptoms of anxiety disorders. Especially for the mechanism of serotonin reuptake inhibitors, the TCA drugs (e.g., clomipramine and doxepine) could reduce OCD symptoms [24]. Clomipramine could decrease PD, agoraphobia, and OCD; doxepine ameliorated almost all anxiety disorders, including GAD, PD, agoraphobia, PTSD, SAD, ASD, separation anxiety disorder, and OCD; imipramine only treated PD patients (Table 2). Monoamine oxidase inhibitors (MAOIs) act to inhibit the activity of monoamine oxidase within neurons. Then, it reserved higher amounts of monoamine neurotransmitters (e.g., dopamine, norepinephrine, epinephrine, and serotonin) in the presynaptic neurons [25]. In MAOIs, phenelzine can treat PD disorders; moclobemide can ameliorate the SAD symptoms (Table 2). Pregabalin, a kind of calcium modulator, was found to act at the alpha-2-delta subunit of voltage-dependent calcium ion channels for alleviating the anxiety symptoms of GAD and SAD (Table 2). A 5-HT1A agonist, buspirone, and azapirone can effectively relieve anxiety symptoms for non-specific anxiety disorders; antihistamine hydroxyzine affiliates with histamine 1 receptors to reduce non-specific anxiety behaviors [20]. In conclusion, current anxiolytic drugs in the clinic go through different mechanisms to reduce the hyperactivity and coupling of the dorsomedial prefrontal cortex-amygdala circuit for amelioration of anxiety symptoms of anxiety disorders.
3. Anxiolytic Substances Used in Non-Clinical Studies: Pharmacological Treatments and Neural Mechanisms
3.1. Conventional Anxiolytic Substances
In the clinics, anxiolytic drugs are applied in patients with a variety of anxiety disorders; however, the same compounds are employed and tested for anxiety behaviors or anxiety activity in the animal model, which is called anxiolytic substances (but not anxiolytic drugs). This section introduces numerous anxiolytic substances to reduce anxiety activity in animal models. To our knowledge, anxiolytic substances include the categories of classical neurotransmitters, neuropeptides, and nonclassical neurotransmitters; moreover, nonclassical neurotransmitters are currently concerned and considered for developing novel medicines in anxiolytic drug discovery. As mentioned in the clinic above, the dorsomedial prefrontal cortex-amygdala hyperactivity and coupling are the essential pathophysiology for a variety of anxiety disorders [15,16,17,18]. The crucial issue is alleviating the dysfunction of the dorsomedial prefrontal cortex-amygdala circuit, which results in an anxiolytic-like effect [15,16,17,18]. This section introduces how the researcher uses animal models and a variety of anxiolytic substances to underline different neural mechanisms to reduce the dysfunction of the dorsomedial prefrontal cortex-amygdala circuit and to evaluate anxiety disorders (Table 3). For example, common anxiolytic substances that interact with classical neurotransmitter systems include benzodiazepines (BDZs) and SSRIs, as well as dopamine-, norepinephrine-, NMDAR-, and histamine-related drugs. In the animal model of anxiety disorders such as conditioning fear learning or PTSD, the neutral stimulus (i.e., conditioned stimulus) paired with aversive or threat events (i.e., unconditioned stimulus) to form the fear conditioning, and then it produced anxiety behaviors [6]. Treatment plans with BDZs are often applied in the conditioned fear learning paradigm of the animal model to assess anxiety disorders and PTSD; moreover, BDZs affiliated with GABAa receptors lead to an influx of chloride ions into the neuronal membranes, thereby inhibiting postsynaptic potentials and induce anxiolytic-like effects [26,27]. SSRIs have been applied in cue or contextually conditioned fear learning and PTSD animal models to mimic multiple anxiety-related disorders; SSRIs inhibit serotonin reuptake and increase serotonin levels in the synaptic cleft to cause anxiolytic-like effects [11,28]. Dopamine systems could be modulated using pharmacological tools to test the single prolonged stress (SPS) animal model of PTSD; it was found that D2/D3 agonists could disrupt anxiety disorders through D2/D3 receptors [29]. Some studies have examined how the norepinephrine system modulates anxiety disorders and PTSD symptoms, demonstrating that alpha-1 adrenergic receptor antagonists blunted anxiety- and PTSD-associated fear behaviors, thereby inducing anxiolytic-like effects [30,31]. NMDA receptor (NMDAR) functions were associated with anxiety disorders and PTSD; the animal study of conditioned fear learning showed that promoting NMDAR functions decreased fear symptoms [32]. Moreover, the NMDAR antagonist impaired fear extinction, whereas the NMDAR agonist facilitated the consolidation of fear extinction [32]. Histamine, which may affiliate with H3 receptors, has been shown to reduce anxiety disorders in the animal model of conditioned fear learning and isolation-induced aggressive behaviors [33]. In summary, classical neurotransmitter systems such as those cited above could modulate a range of anxiety disorders.
In contrast to the classical neurotransmitter systems, the involvement of neuropeptide systems in anxiety disorders and PTSD was relatively less common [34,35,36]. For example, previous studies showed that morphine (i.e., mu-opioid receptor agonist) attenuated PTSD symptoms in the conditioned fear learning paradigm [36,37]. Neuropeptide Y reduced anxiety behaviors and PTSD symptoms via neuropeptide Y receptors in the single-prolonged stress PTSD animal model, indicating that neuropeptide Y receptors are likely another potential mechanism for the modulation of anxiety disorders [35]. Orexin neurons have multiple functions for regulating physiological responses such as feeding, reward, and thermogenesis [38,39]; some recent studies have demonstrated that the blockade of orexin receptors may impair fear behaviors and enhance the consolidation of fear extinction [34].
Aside from the modulation of classical neurotransmitters and neuropeptide systems in anxiety disorders and PTSD, anxiolytic drugs related to nonclassical neurotransmitters were found to make essential contributions in alleviating anxiety disorders and PTSD symptoms via diverse neural mechanisms in preclinical and clinical trials. For example, pro-inflammatory cytokines can impair signaling involved in reward and the modulation of fear/anxiety, causing anxiety disorders and PTSD symptoms; inflammatory cytokines can be considered for developing novel therapeutic strategies to reduce anxiety disorders and PTSD [40]. Brain-derived neurotrophic factor (BDNF) is a protein, member of the neurotrophin family of growth factors, and has neuroprotective roles in neuronal growth; BDNF has been shown to alleviate PTSD symptoms via the BDNF-TrkB signaling pathway within neurons using the SPS PTSD animal model [41,42]. Research on glucocorticoids underlined that the hypothalamus-pituitary-adrenal gland system interferes with PTSD symptoms in the PTSD animal model [43]. Melatonin impaired contextual fear conditioning via MT1 and MT2 receptors, resulting in the amelioration of PTSD symptoms [13]. Animal models have indicated that CBD may have the potential to impair multiple anxiety disorders (e.g., generalized anxiety disorder, panic disorder, SAD, PTSD) through CB1 receptors [12]. Other studies have focused on the relationship between the blockade of ion channels and anxiety disorders and PTSD symptoms. For example, L-type calcium channel blockers such as lacidipine interfere with caffeine-induced anxiety symptoms by blocking calcium channels, thus producing anxiolytic-like effects [44]. Sodium channel blockers such as lamotrigine appear to reduce anxiety symptoms via sodium channel inhibition in the cue-conditioned fear learning paradigm [45]. In conclusion, these anxiolytic substances related to nonclassical neurotransmitters, which act through diverse neural mechanisms, have been shown to attain anxiolytic-like effects in multiple anxiety disorders and PTSD symptoms.
3.2. Current Anxiolytic Substances: Classical Neurotransmitters, Neuropeptides, and Nonclassical Neurotransmitters
Concerning the previous studies related to anxiety disorders and pharmacological treatments, a growing body of evidence has shown that various categories of anxiolytic drugs and substances (including novel drugs) could reduce anxiety disorders and PTSD symptoms [10,22,46,47]. PubMed was searched to gather data on the number of published papers with different keywords for anxiety disorders and specific anxiolytic substances (e.g., BDZs, SSRIs) for 2014–2024 (Figure 1). As Figure 1 depicts, current anxiolytic substances can be separated into classical neurotransmitter systems-related medicines (in blue bars), neuropeptide systems-related medicines (in green bars), and nonclassical neurotransmitter-related compounds (in orange bars).
Considering the clinical findings, patients with depression have an approximate 85% rate with anxiety disorders; however, patients with anxiety disorders have an almost 90% rate to be comorbid with depression [48]. Therefore, anxiety disorders are highly comorbid with depression. Interestingly, SSRI antidepressant drugs were featured in the most published articles, with 1,874 papers. The conventional anxiolytic drugs, BDZs, were ranked second, with 1,303 papers. These findings indicate that anxiety disorders and major depression disorders seemingly share similar neural mechanisms; moreover, the present evidence was supported by the clinical data that anxiety disorders were found to be comorbid with major depression disorders [48]. Concerning the neural mechanism of anxiolytic disorders, researchers see serotonin systems as offering greater potential than GABA systems, especially during 2014–2024. Inflammation cytokines were ranked third, appearing in 1,045 published papers in connection with anxiety disorders. Administering inflammatory cytokines may induce fear, anxiety disorders, and PTSD, which is related to the inflammation system. Accordingly, the inflammation system is an alternative consideration for developing anxiolytic drugs. BDNF was ranked fourth, with 892 published papers. BDNF, a novel treatment in anxiety disorders and PTSD that is currently in the preclinical phase of animal models, goes through the BDNF-TrkB signaling conductions to alleviate anxiety disorders and PTSD symptoms. D2/D3 receptors via the dopamine system were ranked fifth, with 744 published papers; dopamine antagonism may alleviate anxiety disorders and PTSD symptoms. The other anxiolytic substances associated with classical neurotransmitters had fewer published papers, including 485 for norepinephrine, 330 for NMDA, and 100 for histamine. Neuropeptides morphine, neuropeptide Y, and orexins appeared in even fewer papers, reflecting their novelty as pharmacological treatments; very likely, more studies involving them will be published soon. The anxiolytic substances related to nonclassical neurotransmitters, including glucocorticoid, melatonin, cannabidiol, L-type-calcium channel blockers, and sodium channel blockers, appeared in the fewest publications, suggesting ample room for their development as novel and promising pharmacological anxiolytic treatments.
4. Types and Properties for Animal Models of Anxiety Disorders
A previous study has suggested that the animal models of anxiety disorders could divided into the models based on unconditioned responses and conditioned responses [49]. However, the present review paper does not follow this division for the animal models of anxiety disorders. Based on experimentation and statistical hypothesis testing, the experimental variables can be divided into independent and dependent variables [50]. The independent variable is defined as the causes of behaviors for individuals or groups; however, the dependent variable is viewed as the effect of behaviors for individuals or groups [50]. Therefore, you manipulate independent variables to affect the outcome of an experiment. Dependent variables represent the outcome of the experiment.
In the present animal models, we define the animal models for testing anxiety disorders as consisting of independent and dependent variables. Independent variables can be manipulated to shape various animal models of anxiety disorders as well as PTSD (i.e., it is like a cause for behaviors). Alternatively, another kind of anxiety disorder in the animal models belongs to the dependent variables (i.e., it is like an effect of behaviors), and these kinds of anxiety behaviors are not able to be manipulated. Instead, animal models of this type can be used to test for various anxiety responses in anxiety disorders and PTSD. Suitable animal models of anxiety disorders and PTSD should be selected based on requirements of face, predictive, and constructive validities [51]. Face validity refers to whether it is obvious on the surface that the tested behaviors and symptoms of the animal model are comparable to the symptoms in humans. Predictive validity means that the anxiolytic drugs can effectively alleviate symptoms and behaviors. Finally, constructive validity indicates that an anxiety disorder in an animal model shares the same brain mechanism as in humans. In addition to considerations of these three validity types, animal models of anxiety disorders and PTSD should be considered in light of their characteristics, advantages, disadvantages, when to use them, and usage frequencies.
4.1. Shaping an Animal Model of Anxiety Disorders and PTSD
Determining a suitable and shaping animal model for anxiety disorders and PTSD is a crucial issue. The review paper offers numerous types and properties of developed animal models (see Table 4A: Shaping anxiety models). For example, anxiety disorders and PTSD of fear conditioning were continuously used in building up a reliable and valid animal model. Fear conditioning models of this type can be separated into cue stimulus [52] and contextual stimulus [53] (conditioned stimulus, CS) to pair with footshock-induced stress (unconditioned stimulus, US); thus, the animal models could induce fear behavior to mimic anxiety responses. The cue model has advantages, including clear-cut stimulus as well as excellent face, predictive, and constructive validities [52].
In contrast, the contextual model was designed to apply a complex contextual stimulus that combined different environmental stimuli to pair with footshock stress [53]. Accordingly, the contextual stimulus is very similar to the environmental stimulus. Thus, the contextual model has the advantage of being very similar to natural, environmentally induced PTSD or anxiety disorders. However, because the context is a complex stimulus that is not easy to manipulate, the context itself may bring disadvantages. Regardless of their disadvantages, cue and contextual models were often used in research on anxiety disorders and PTSD. Moreover, both models are used very often in the animal models for PTSD and anxiety disorders.
SPS is another kind of animal model for PTSD [54]. The SPS PTSD animal model has three stages for manipulating PTSD behaviors. For example, the animal should be restrained for 2 hours and then forced to swim test for 20 minutes. After recovering for 15 minutes, animals were exposed to ether until loss of consciousness. The advantages of this model are long-term, stable stress, excellent face, and predictive and constructive validities. Its disadvantages are long-term stress treatments and manipulations because the real condition of PTSD is likely very short-term, and its symptoms are overwhelmingly stressor-induced. Thus, this SPS model of PTSD may not be ideal due to concerns about validity and reliability. Moreover, this model of SPS is firstly considered for application in inducing the symptoms of PTSD in the animal model.
Another animal model used to test anxiety and depression behaviors is learned helplessness [55,56]. This experimental procedure is designed so that animals are exposed to uncontrolled stressors through behavioral responses. The advantages of this model include effective and easy stressor manipulation. However, this model can also be used to test depression behaviors; thus, its findings cannot be differentiated between anxiety and depression tests—this is its chief disadvantage. This model has rather fewer legitimate opportunities for application in anxiety tests.
The restraint stress model [57] induces immobility in mice by placing them into well-ventilated 50 mL Falcon tubes for 2 hours per day over 21 consecutive days. This animal model is easy to conduct but is also used to test depression behaviors. Thus, its results cannot be clearly differentiated for anxiety and depression behaviors. Another animal model, inescapable tail shock, is designed to test PTSD fear behavior [58,59]. The animal would experience uncontrolled and inescapable tail shock, causing them acute stress. It is easy to conduct, but because it is also employed in testing depression behaviors, it suffers from the same disadvantages that affect the two previous models, namely the difficulty in differentiating results for anxiety and depression. For the underwater trauma model [60], animals are held underwater for 30 seconds to induce severe stress. The advantage of this model is that it is easy to manipulate to shape stressors and develop the PTSD model. However, because its face, predictive, and constructive validities remain in doubt, it is seldom used in the animal model of PTSD. Under the social isolation model [10], the animal is raised alone with no companion. This model is easily conducted to produce stress; however, the long-term conduction time is its disadvantage. A related model, social defeat, requires that animals be exposed to a trained aggressor conspecific for 6 hours per day for 5 or 10 days [61]; the advantage of this model is easy conduction. Early-life stress is designed to use maternal separation and a trauma event to mimic PTSD symptoms [60]; the advantages of this model are good face, predictive, and constructive validities, but this model requires conducting a chronic procedure of stress, which constitutes its chief disadvantage. Finally, predator-based stress [60] uses predators or predator-related stimuli (such as a predator’s urine) to induce the trauma event; its advantage is the ease of conduction.
4.2. Testing Anxiety and PTSD Behaviors
The testing animal models of anxiety disorders and PTSD served as the dependent variables are different than the previous descriptions of shaping the animal models of anxiety and PTSD (see Table 4B: Testing anxiety behaviors). In these examples, the open field test (OFT) and elevated plus maze test (EPMT) are the most popular models for testing anxiety behaviors.
The OFT measures time spent and crossing trials in the center area of the task [62,63]. Increased (decreased) time spent and more (fewer) crossing trials in the center area indicate lower (higher) anxiety responses. Note that preclinical scientists with expertise in the field of anxiety would not use this test except to control for adverse drug effects. Alternatively, the OFT also tests locomotion activity; thus, its disadvantage is the competition between locomotion and anxiety behaviors, which cannot be clearly differentiated. On the other hand, the time spent by the animal in the central part of the open arena in some situations may result from changes in spontaneous locomotor activity; therefore, the results of this test should be interpreted with caution.
The EPMT, another popular animal model [62], measures time spent in the open arm of a maze to indicate the strength of anxiety responses. The advantages of the EPMT are that the animals can rest in the crossing area between the open and closed arms. However, the disadvantages of the EPMT are that the animal sometimes stays longer in the crossing area, leading to errors of measurement for anxiety behaviors. The elevated zero maze and x-maze tests are similar to the EPMT, albeit with different shapes. The elevated zero maze test is designed in the shape of a circle with two sets of open arms and two sets of closed arms; however, it lacks the crossing area [61]. Thus, the advantage of the elevated zero maze test is its lack of a crossing area, which enforces animals’ decisions. However, conflicts arise from time spent in the open and closed arms; the elevated x-maze task tests the open arm time and total time ratio. Its face, predictive, and constructive validities are good [64,65]. The light–dark box test assesses activity and time spent in the brightly lit and dark apparatus compartments based on the animals’ innate desire to explore novel areas [62]; the advantage is easy conduction. The startle response test pairs a conditioned stimulus with a footshock to induce startle responses that serve as anxiety responses [7]. This model of startle responses has good face, predictive, and constructive validities for anxiety disorders; however, this model is limited to the anxiety behaviors related to a cue with footshock conditioning. In the marble burying test of anxiety responses, animals with previous stress are placed in the test cage; the depth of marble burying is tested up to 2/3 of the depth with bedding [66]. It appears to offer excellent face, predictive, and constructive validities for anxiety disorders; however, because digging behavior is a species-typical reaction to stress, it should be considered for use only in the specific species of animals that are prone to such behavior. The defensive shock-prod burying test is designed such that animals encounter an electrical probe with connecting to a shock source, and then it measures the depth to which the prod is buried [67]. Face, predictive, and constructive validities are good for anxiety disorders in the defensive shock-prod burying test; however, sometimes, animals do not touch the electrical probe, which thus cannot induce anxiety behaviors. The grooming test uses stressors to induce grooming behaviors, including novel environments, predator exposure, and bright light [7]. Simple conduction is its advantage; however, it has questionable face, predictive, and constructive validities. The social interaction test is designed such that two animals are placed in the test environment for 5 or 10 minutes while the duration and frequency of all social interactions—including sniffing, flowing, chasing, toughing, and biting—is recorded [7]; higher scores indicate lower anxiety behaviors. Accessible design and easy conduction are its advantages; the disadvantages are limited applicability to SAD. The Suok task simultaneously measures anxiety, vestibular, and neuromuscular deficits through an unstable rod with novelty [68]; the threats of height, loss of balance, and novelty are presented to analyze anxiety and assess animal exploration. This model may have face validity; however, competition among several behaviors has occurred in the Suok test, constituting a notable disadvantage. The stress-induced hyperthermia test is based on the evolutionarily important role of hyperthermia, which increases body temperature in response to encountering stressors [7]. This model is applicable across many species, including humans. Its disadvantages are due to testing errors from numerous confounding factors. The hole-board test assesses head-dipping behaviors [69]; more head-dips represent less anxiety and more explorations. This model enjoys easy preparation and conduction; however, there are doubts about its face, predictive, and constructive validities. The rat exposure test is dependent on the animals’ natural defensive “avoidance” behavioral responses to signs of potential danger [7]; defensive behaviors include stretch-attend posture, stretch approach, freezing, burying, and hiding. This model enjoys easy conduction; however, there are variances for different species in the present model. The novel object test measures the approach-avoidance behaviors of the animals in response to novel stimuli [70]; longer spent time in exploration for a novel object indicates lower anxiety behaviors. This model has excellent face, predictive, and constructive validities. However, the disadvantages are that this model is also applied in the recognitive function, and it is confused with recognition tests.
In conclusion, animal models have different characteristics, advantages, and disadvantages. In the following section, we provide some suggestions as to how and when to use these animal models to build up or test anxiety disorders and PTSD. Face, predictive, and constructive validities should be basic considerations when selecting the most appropriate model for the determinations.
5. Opinion from Precinical Studies to Clinical Research
This review paper sought background knowledge and critical determination for screening anxiolytic drug discovery. Moreover, it can help narrow the gaps between the animal model of anxiety disorders in preclinical research and clinical human studies. Choosing the most appropriate animal model of anxiety disorders is crucial because the best animal models could precisely target specific anxiety disorders in humans. In addition, the most suitable animal model could be fully explained and applied to anxiety disorders in clinical settings.
To summarize the information in the above tables, the animal models of fear conditioning with cue and learned helplessness models can be used for testing the brain mechanism of GAD and clinical drugs, including BDZs, SSRIs, SNRIs, TCA, calcium modulators, azapirone, and antihistamine. Fear conditioning with context, inescapable tail shock, and underwater trauma are the most appropriate animal models of anxiety disorders for testing PD with BDZs, SSRIs, SNRIs, TCA, MAOIs, azapirone, and antihistamines in the clinics. Agoraphobia was tested in fear conditioning with context and assessing anxiolytic drugs such as BDZs, SSRIs, SNRIs, TCA, azapirone, and antihistamines. PTSD can be tested by numerous animal models, including fear conditioning with cue or context, SPS, learned helplessness, restraint stress, inescapable tail shock, underwater trauma, social isolation, social defeat, early-life stress, and predator-based stress; moreover, BDZs, SSRIs, SNRIs, TCA, azapirone, and antihistamine can be tested by the mentioned models. Because of social properties, SAD was suggested using social isolation and social defeat to test BDZs, SSRIs, SNRIs, TCA, MAOIs, calcium modulators, azapirone, and antihistamines. ASD has the properties of short-term and severe stress, and thus, fear conditioning with cue or context, restraint stress, inescapable tail shock, and predator-based stress for testing BDZs, TCA, azapirone, and antihistamine. Separation anxiety disorder can be tested by the animal models of anxiety disorders, including social isolation and early-life stress, because of the social separation effect; moreover, BDZs, TCA, azapirone, and antihistamines can be tested by these animal models. OCD was suggested to use fear conditioning with the cue, learned helplessness, inescapable tail shock, and predator-based stress for tests in clinical drugs such as BDZs, SSRIs, TCA, azapirone, and antihistamines (Table 5).
Current anxiolytic substances interact with different neural mechanisms, including classical neurotransmitter, neuropeptide, and nonclassical neurotransmitter systems. The present developmental lines of anxiolytic substances may potentially attenuate multiple anxiety disorders and PTSD. The most suitable anxiolytic substances can be identified for the amelioration of multiple anxiety disorders. SSRIs were the most-reference in clinical and preclinical aspects of the current anxiolytic substances related to classical neurotransmitter systems. The conventional anxiolytic substances, BDZs, were ranked second. Anxiolytic substances related to neuropeptides may be considered for the development of novel pharmacological treatments. The nonclassical neurotransmitters (except for inflammatory cytokines and BDNF) also appeared in fewer published papers. This line of studies needs to be examined in the future.
On the other hand, multitargeted drugs can be considered to alleviate the symptoms of anxiety disorders. For example, the novel treatment combined the first three priority anxiolytic drugs, BDZ, SSRI, and anti-inflammatory cytokines. The mixed drugs might produce the optimal amelioration effects of anxiety disorders. This issue should be investigated in further study.
In summary, some suggestions can be provided on how and when to use these animal models to build up or test anxiety disorders and PTSD. For example, when the researcher wants to manipulate a stressor to induce the animal model of anxiety disorders, the researcher can use “the shaping anxiety models”. Moreover, the fear conditioning in the cue (or context) pairing with footshock or the SPS PTSD model is the appropriate animal model of anxiety disorders and PTSD. On the other hand, when the researcher wants to test anxiety behaviors, they can use the open field test or elevated plus maze test. The face, predictive, and constructive validities should be basic requirements for considering which model is most apt for the determinations.
6. Conclusions
The development of anxiolytic drugs’ discovery should be considered for which anxiety disorders and anxiolytic drugs underlined different neural mechanisms, including classical neurotransmitters, neuropeptides, and nonclassical neurotransmitter systems. Moreover, the side effects, neurotoxin, and shortages should be discussed and considered in the clinical trials. The nonclassical neurotransmitters (except for inflammatory cytokines and BDNF) appeared in far fewer published papers. Therefore, this line of studies for nonclassical neurotransmitters calls for further investigation.
The different animal models of anxiety disorders and PTSD have different characteristics, advantages, and disadvantages. We provided some suggestions on how and when to use these animal models for building up or testing anxiety disorders and PTSD. The basic requirements for consideration are face, predictive, and constructive validities. The present review contributes some clinical insights for screening novel anxiolytic drugs.
Funding
This paper was supported by funding granted to A. C. W. Huang from the National Science and Technology Council of Taiwan [NSTC 112-2410-H-431-009, NSTC 113-2923-H-431 -001 -MY3, and NSTC 113-2410-H-431 -015 -MY2].
Declaration of interest
The authors have no other relevant affiliations or financial involvement with any organization or entity with a financial interest in, or financial conflict with, the subject matter or materials discussed in the manuscript apart from those disclosed.
Reviewer disclosures
Peer reviewers on this manuscript have no relevant financial or other relationships to disclose.
Data availability
No data was used for the research described in the article.
References
- Diagnostic and statistical manual of mental disorders: DSM-5, 5th ed.; Association, A.P., Ed.; American Psychiatric Association: Washington, DC, 2013. [Google Scholar]
- Griebel, G.; Holmes, A. 50 years of hurdles and hope in anxiolytic drug discovery. Nat Rev Drug Discov 2013, 12, 667–687. [Google Scholar] [CrossRef] [PubMed]
- Stewart, A.M.; Kalueff, A.V. Anxiolytic drug discovery: what are the novel approaches and how can we improve them? Expert Opin Drug Discov 2014, 9, 15–26. [Google Scholar] [CrossRef] [PubMed]
- Calabrese, E.J. An assessment of anxiolytic drug screening tests: hormetic dose responses predominate. Crit Rev Toxicol 2008, 38, 489–542. [Google Scholar] [CrossRef] [PubMed]
- Cryan, J.F.; Sweeney, F.F. The age of anxiety: role of animal models of anxiolytic action in drug discovery. Br J Pharmacol 2011, 164, 1129–1161. [Google Scholar] [CrossRef]
- Bourin, M. Animal models for screening anxiolytic-like drugs: a perspective. Dialogues Clin Neurosci 2015, 17, 295–303. [Google Scholar] [CrossRef]
- Hart, P.C.; Bergner, C.L.; Smolinsky, A.N.; Dufour, B.D.; Egan, R.J.; LaPorte, J.L.; Kalueff, A.V. Experimental Models of Anxiety for Drug Discovery and Brain Research. Methods Mol Biol 2016, 1438, 271–291. [Google Scholar] [CrossRef]
- Park, S.C.; Kim, Y.K. Anxiety Disorders in the DSM-5: Changes, Controversies, and Future Directions. Adv Exp Med Biol 2020, 1191, 187–196. [Google Scholar] [CrossRef]
- Rabow, L.E.; Russek, S.J.; Farb, D.H. From ion currents to genomic analysis: recent advances in GABAA receptor research. Synapse 1995, 21, 189–274. [Google Scholar] [CrossRef]
- Aspesi, D.; Pinna, G. Animal models of post-traumatic stress disorder and novel treatment targets. Behav Pharmacol 2019, 30, 130–150. [Google Scholar] [CrossRef]
- Heesbeen, E.J.; Bijlsma, E.Y.; Verdouw, P.M.; van Lissa, C.; Hooijmans, C.; Groenink, L. The effect of SSRIs on fear learning: a systematic review and meta-analysis. Psychopharmacology (Berl) 2023, 240, 2335–2359. [Google Scholar] [CrossRef]
- Blessing, E.M.; Steenkamp, M.M.; Manzanares, J.; Marmar, C.R. Cannabidiol as a Potential Treatment for Anxiety Disorders. Neurotherapeutics 2015, 12, 825–836. [Google Scholar] [CrossRef] [PubMed]
- Huang, F.; Yang, Z.; Li, C.Q. The Melatonergic System in Anxiety Disorders and the Role of Melatonin in Conditional Fear. Vitam Horm 2017, 103, 281–294. [Google Scholar] [CrossRef] [PubMed]
- World Health, O. Depression and Other Common Mental Disorders: Global Health Estimates; World Health Organization, 2017. [Google Scholar]
- Kirk, P.A.; Holmes, A.J.; Robinson, O.J. Threat vigilance and intrinsic amygdala connectivity. Hum Brain Mapp 2022, 43, 3283–3292. [Google Scholar] [CrossRef] [PubMed]
- Robinson, O.J.; Krimsky, M.; Lieberman, L.; Allen, P.; Vytal, K.; Grillon, C. Towards a mechanistic understanding of pathological anxiety: the dorsal medial prefrontal-amygdala 'aversive amplification' circuit in unmedicated generalized and social anxiety disorders. Lancet Psychiatry 2014, 1, 294–302. [Google Scholar] [CrossRef] [PubMed]
- Vytal, K.E.; Overstreet, C.; Charney, D.R.; Robinson, O.J.; Grillon, C. Sustained anxiety increases amygdala-dorsomedial prefrontal coupling: a mechanism for maintaining an anxious state in healthy adults. J Psychiatry Neurosci 2014, 39, 321–329. [Google Scholar] [CrossRef]
- Williams, L.M. Defining biotypes for depression and anxiety based on large-scale circuit dysfunction: a theoretical review of the evidence and future directions for clinical translation. Depress Anxiety 2017, 34, 9–24. [Google Scholar] [CrossRef]
- Giacobbe, P.; Flint, A. Diagnosis and Management of Anxiety Disorders. Continuum (Minneap Minn) 2018, 24, 893–919. [Google Scholar] [CrossRef]
- Bandelow, B. Current and Novel Psychopharmacological Drugs for Anxiety Disorders. Adv Exp Med Biol 2020, 1191, 347–365. [Google Scholar] [CrossRef]
- McCabe, C.; Mishor, Z.; Filippini, N.; Cowen, P.J.; Taylor, M.J.; Harmer, C.J. SSRI administration reduces resting state functional connectivity in dorso-medial prefrontal cortex. Mol Psychiatry 2011, 16, 592–594. [Google Scholar] [CrossRef]
- Murrough, J.W.; Yaqubi, S.; Sayed, S.; Charney, D.S. Emerging drugs for the treatment of anxiety. Expert Opin Emerg Drugs 2015, 20, 393–406. [Google Scholar] [CrossRef]
- Muscatello, M.R.; Spina, E.; Bandelow, B.; Baldwin, D.S. Clinically relevant drug interactions in anxiety disorders. Hum Psychopharmacol 2012, 27, 239–253. [Google Scholar] [CrossRef] [PubMed]
- DeVeaugh-Geiss, J. Pharmacologic therapy of obsessive compulsive disorder. Adv Pharmacol 1994, 30, 35–52. [Google Scholar] [CrossRef] [PubMed]
- Sheehan, D.V. Delineation of anxiety and phobic disorders responsive to monoamine oxidase inhibitors: implications for classification. J Clin Psychiatry 1984, 45, 29–36. [Google Scholar] [PubMed]
- Lu, C.Y.; Liu, X.; Jiang, H.; Pan, F.; Ho, C.S.; Ho, R.C. Effects of Traumatic Stress Induced in the Juvenile Period on the Expression of Gamma-Aminobutyric Acid Receptor Type A Subunits in Adult Rat Brain. Neural Plast 2017, 2017, 5715816. [Google Scholar] [CrossRef]
- Stevens, J.C.; Pollack, M.H. Benzodiazepines in clinical practice: consideration of their long-term use and alternative agents. J Clin Psychiatry 2005, 66 Suppl 2, 21–27. [Google Scholar]
- Hendriksen, H.; Olivier, B.; Oosting, R.S. From non-pharmacological treatments for post-traumatic stress disorder to novel therapeutic targets. Eur J Pharmacol 2014, 732, 139–158. [Google Scholar] [CrossRef]
- Malikowska-Racia, N.; Salat, K.; Nowaczyk, A.; Fijalkowski, L.; Popik, P. Dopamine D2/D3 receptor agonists attenuate PTSD-like symptoms in mice exposed to single prolonged stress. Neuropharmacology 2019, 155, 1–9. [Google Scholar] [CrossRef]
- Laitman, B.M.; Gajewski, N.D.; Mann, G.L.; Kubin, L.; Morrison, A.R.; Ross, R.J. The alpha1 adrenoceptor antagonist prazosin enhances sleep continuity in fear-conditioned Wistar-Kyoto rats. Prog Neuropsychopharmacol Biol Psychiatry 2014, 49, 7–15. [Google Scholar] [CrossRef]
- O'Daniel, M.P.; Petrunich-Rutherford, M.L. Effects of chronic prazosin, an alpha-1 adrenergic antagonist, on anxiety-like behavior and cortisol levels in a chronic unpredictable stress model in zebrafish (Danio rerio). PeerJ 2020, 8, e8472. [Google Scholar] [CrossRef]
- Radulovic, J.; Ren, L.Y.; Gao, C. N-Methyl D-aspartate receptor subunit signaling in fear extinction. Psychopharmacology (Berl) 2019, 236, 239–250. [Google Scholar] [CrossRef]
- Yokoyama, F.; Yamauchi, M.; Oyama, M.; Okuma, K.; Onozawa, K.; Nagayama, T.; Shinei, R.; Ishikawa, M.; Sato, Y.; Kakui, N. Anxiolytic-like profiles of histamine H3 receptor agonists in animal models of anxiety: a comparative study with antidepressants and benzodiazepine anxiolytic. Psychopharmacology (Berl) 2009, 205, 177–187. [Google Scholar] [CrossRef] [PubMed]
- Flores, A.; Saravia, R.; Maldonado, R.; Berrendero, F. Orexins and fear: implications for the treatment of anxiety disorders. Trends Neurosci 2015, 38, 550–559. [Google Scholar] [CrossRef] [PubMed]
- Serova, L.I.; Laukova, M.; Alaluf, L.G.; Pucillo, L.; Sabban, E.L. Intranasal neuropeptide Y reverses anxiety and depressive-like behavior impaired by single prolonged stress PTSD model. Eur Neuropsychopharmacol 2014, 24, 142–147. [Google Scholar] [CrossRef] [PubMed]
- RaiseAbdullahi, P.; Vafaei, A.A.; Ghanbari, A.; Dadkhah, M.; Rashidy-Pour, A. Time-dependent protective effects of morphine against behavioral and morphological deficits in an animal model of posttraumatic stress disorder. Behav Brain Res 2019, 364, 19–28. [Google Scholar] [CrossRef]
- Szczytkowski-Thomson, J.L.; Lebonville, C.L.; Lysle, D.T. Morphine prevents the development of stress-enhanced fear learning. Pharmacol Biochem Behav 2013, 103, 672–677. [Google Scholar] [CrossRef]
- Inutsuka, A.; Yamanaka, A. The physiological role of orexin/hypocretin neurons in the regulation of sleep/wakefulness and neuroendocrine functions. Front Endocrinol (Lausanne) 2013, 4, 18. [Google Scholar] [CrossRef]
- Zarrabian, S.; Riahi, E.; Karimi, S.; Razavi, Y.; Haghparast, A. The potential role of the orexin reward system in future treatments for opioid drug abuse. Brain Res 2020, 1731, 146028. [Google Scholar] [CrossRef]
- Felger, J.C. Imaging the Role of Inflammation in Mood and Anxiety-related Disorders. Curr Neuropharmacol 2018, 16, 533–558. [Google Scholar] [CrossRef]
- Andero, R.; Ressler, K.J. Fear extinction and BDNF: translating animal models of PTSD to the clinic. Genes Brain Behav 2012, 11, 503–512. [Google Scholar] [CrossRef]
- Yin, J.B.; Liu, H.X.; Shi, W.; Ding, T.; Hu, H.Q.; Guo, H.W.; Jin, S.; Wang, X.L.; Zhang, T.; Lu, Y.C.; et al. Various BDNF administrations attenuate SPS-induced anxiety-like behaviors. Neurosci Lett 2022, 788, 136851. [Google Scholar] [CrossRef]
- Florido, A.; Velasco, E.R.; Monari, S.; Cano, M.; Cardoner, N.; Sandi, C.; Andero, R.; Perez-Caballero, L. Glucocorticoid-based pharmacotherapies preventing PTSD. Neuropharmacology 2023, 224, 109344. [Google Scholar] [CrossRef] [PubMed]
- Khurana, K.; Bansal, N. Lacidipine attenuates caffeine-induced anxiety-like symptoms in mice: Role of calcium-induced oxido-nitrosative stress. Pharmacol Rep 2019, 71, 1264–1272. [Google Scholar] [CrossRef] [PubMed]
- Mirza, N.R.; Bright, J.L.; Stanhope, K.J.; Wyatt, A.; Harrington, N.R. Lamotrigine has an anxiolytic-like profile in the rat conditioned emotional response test of anxiety: a potential role for sodium channels? Psychopharmacology (Berl) 2005, 180, 159–168. [Google Scholar] [CrossRef] [PubMed]
- Ragen, B.J.; Seidel, J.; Chollak, C.; Pietrzak, R.H.; Neumeister, A. Investigational drugs under development for the treatment of PTSD. Expert Opin Investig Drugs 2015, 24, 659–672. [Google Scholar] [CrossRef]
- Sartori, S.B.; Singewald, N. Novel pharmacological targets in drug development for the treatment of anxiety and anxiety-related disorders. Pharmacol Ther 2019, 204, 107402. [Google Scholar] [CrossRef]
- Tiller, J.W. Depression and anxiety. Med J Aust 2013, 199, S28–31. [Google Scholar] [CrossRef]
- Fuchs, E.; Fliugge, G. Experimental animal models for the simulation of depression and anxiety. Dialogues Clin Neurosci 2006, 8, 323–333. [Google Scholar] [CrossRef]
- Kiess, K.O. Statistical concepts for the behavioral sciences; Allyn and Bacon, Inc., 1989. [Google Scholar]
- Flandreau, E.I.; Toth, M. Animal Models of PTSD: A Critical Review. Curr Top Behav Neurosci 2018, 38, 47–68. [Google Scholar] [CrossRef]
- Lissek, S.; Kaczkurkin, A.N.; Rabin, S.; Geraci, M.; Pine, D.S.; Grillon, C. Generalized anxiety disorder is associated with overgeneralization of classically conditioned fear. Biol Psychiatry 2014, 75, 909–915. [Google Scholar] [CrossRef]
- Yu, Y.H.; Lim, Y.S.; Ou, C.Y.; Chang, K.C.; Tsai, A.C.; Chang, F.C.; Huang, A.C.W. The Medial Prefrontal Cortex, Nucleus Accumbens, Basolateral Amygdala, and Hippocampus Regulate the Amelioration of Environmental Enrichment and Cue in Fear Behavior in the Animal Model of PTSD. Behav Neurol 2022, 2022, 7331714. [Google Scholar] [CrossRef]
- Yamamoto, S.; Morinobu, S.; Takei, S.; Fuchikami, M.; Matsuki, A.; Yamawaki, S.; Liberzon, I. Single prolonged stress: toward an animal model of posttraumatic stress disorder. Depress Anxiety 2009, 26, 1110–1117. [Google Scholar] [CrossRef] [PubMed]
- Greenwood, B.N.; Fleshner, M. Exercise, learned helplessness, and the stress-resistant brain. Neuromolecular Med 2008, 10, 81–98. [Google Scholar] [CrossRef] [PubMed]
- Maier, S.F.; Watkins, L.R. Stressor controllability and learned helplessness: the roles of the dorsal raphe nucleus, serotonin, and corticotropin-releasing factor. Neurosci Biobehav Rev 2005, 29, 829–841. [Google Scholar] [CrossRef] [PubMed]
- Banagozar Mohammadi, A.; Torbati, M.; Farajdokht, F.; Sadigh-Eteghad, S.; Fazljou, S.M.B.; Vatandoust, S.M.; Golzari, S.E.J.; Mahmoudi, J. Sericin alleviates restraint stress induced depressive- and anxiety-like behaviors via modulation of oxidative stress, neuroinflammation and apoptosis in the prefrontal cortex and hippocampus. Brain Res 2019, 1715, 47–56. [Google Scholar] [CrossRef]
- Donner, N.C.; Kubala, K.H.; Hassell, J.E., Jr.; Lieb, M.W.; Nguyen, K.T.; Heinze, J.D.; Drugan, R.C.; Maier, S.F.; Lowry, C.A. Two models of inescapable stress increase tph2 mRNA expression in the anxiety-related dorsomedial part of the dorsal raphe nucleus. Neurobiol Stress 2018, 8, 68–81. [Google Scholar] [CrossRef]
- Park, H.; Rhee, J.; Park, K.; Han, J.S.; Malinow, R.; Chung, C. Exposure to Stressors Facilitates Long-Term Synaptic Potentiation in the Lateral Habenula. J Neurosci 2017, 37, 6021–6030. [Google Scholar] [CrossRef]
- Zhang, L.; Hu, X.Z.; Li, H.; Li, X.; Yu, T.; Dohl, J.; Ursano, R.J. Updates in PTSD Animal Models Characterization. Methods Mol Biol 2019, 2011, 331–344. [Google Scholar] [CrossRef]
- Campos, A.C.; Fogaca, M.V.; Aguiar, D.C.; Guimaraes, F.S. Animal models of anxiety disorders and stress. Braz J Psychiatry 2013, 35 Suppl 2, S101–111. [Google Scholar] [CrossRef]
- Karl, T.; Duffy, L.; Herzog, H. Behavioural profile of a new mouse model for NPY deficiency. Eur J Neurosci 2008, 28, 173–180. [Google Scholar] [CrossRef]
- Kraeuter, A.K.; Guest, P.C.; Sarnyai, Z. The Open Field Test for Measuring Locomotor Activity and Anxiety-Like Behavior. Methods Mol Biol 2019, 1916, 99–103. [Google Scholar] [CrossRef]
- Critchley, M.A.; Handley, S.L. Effects in the X-maze anxiety model of agents acting at 5-HT1 and 5-HT2 receptors. Psychopharmacology (Berl) 1987, 93, 502–506. [Google Scholar] [CrossRef] [PubMed]
- Handley, S.L.; McBlane, J.W. An assessment of the elevated X-maze for studying anxiety and anxiety-modulating drugs. J Pharmacol Toxicol Methods 1993, 29, 129–138. [Google Scholar] [CrossRef] [PubMed]
- Kedia, S.; Chattarji, S. Marble burying as a test of the delayed anxiogenic effects of acute immobilisation stress in mice. J Neurosci Methods 2014, 233, 150–154. [Google Scholar] [CrossRef] [PubMed]
- Yang, M.; Augustsson, H.; Markham, C.M.; Hubbard, D.T.; Webster, D.; Wall, P.M.; Blanchard, R.J.; Blanchard, D.C. The rat exposure test: a model of mouse defensive behaviors. Physiol Behav 2004, 81, 465–473. [Google Scholar] [CrossRef]
- Kalueff, A.V.; Tuohimaa, P. The Suok ("ropewalking") murine test of anxiety. Brain Res Brain Res Protoc 2005, 14, 87–99. [Google Scholar] [CrossRef]
- Kliethermes, C.L.; Crabbe, J.C. Pharmacological and genetic influences on hole-board behaviors in mice. Pharmacol Biochem Behav 2006, 85, 57–65. [Google Scholar] [CrossRef]
- Powell, S.B.; Geyer, M.A.; Gallagher, D.; Paulus, M.P. The balance between approach and avoidance behaviors in a novel object exploration paradigm in mice. Behav Brain Res 2004, 152, 341–349. [Google Scholar] [CrossRef]
Figure 1.
depicts paper numbers during 2014–2024 found by searching the PubMed database for various anxiolytic drugs and substances: BDZs, serotonin, DA, NE, NMDAR, histamine, morphine, neuropeptide Y, orexins, inflammatory cytokines, BDNF, glucocorticoid, melatonin, cannabidiol, L-type calcium channel blocker, and sodium channel blocker. The blue vertical bars are involved in classical neurotransmitter systems. The green vertical bars indicate neuropeptide systems. The orange vertical bars represent the nonclassical neurotransmitter systems. BDZs: benzodiazepines; DA: dopamine; NE: norepinephrine; NMDAR: NMDA receptor; BDNF: brain-derived neurotrophic factor.
Figure 1.
depicts paper numbers during 2014–2024 found by searching the PubMed database for various anxiolytic drugs and substances: BDZs, serotonin, DA, NE, NMDAR, histamine, morphine, neuropeptide Y, orexins, inflammatory cytokines, BDNF, glucocorticoid, melatonin, cannabidiol, L-type calcium channel blocker, and sodium channel blocker. The blue vertical bars are involved in classical neurotransmitter systems. The green vertical bars indicate neuropeptide systems. The orange vertical bars represent the nonclassical neurotransmitter systems. BDZs: benzodiazepines; DA: dopamine; NE: norepinephrine; NMDAR: NMDA receptor; BDNF: brain-derived neurotrophic factor.
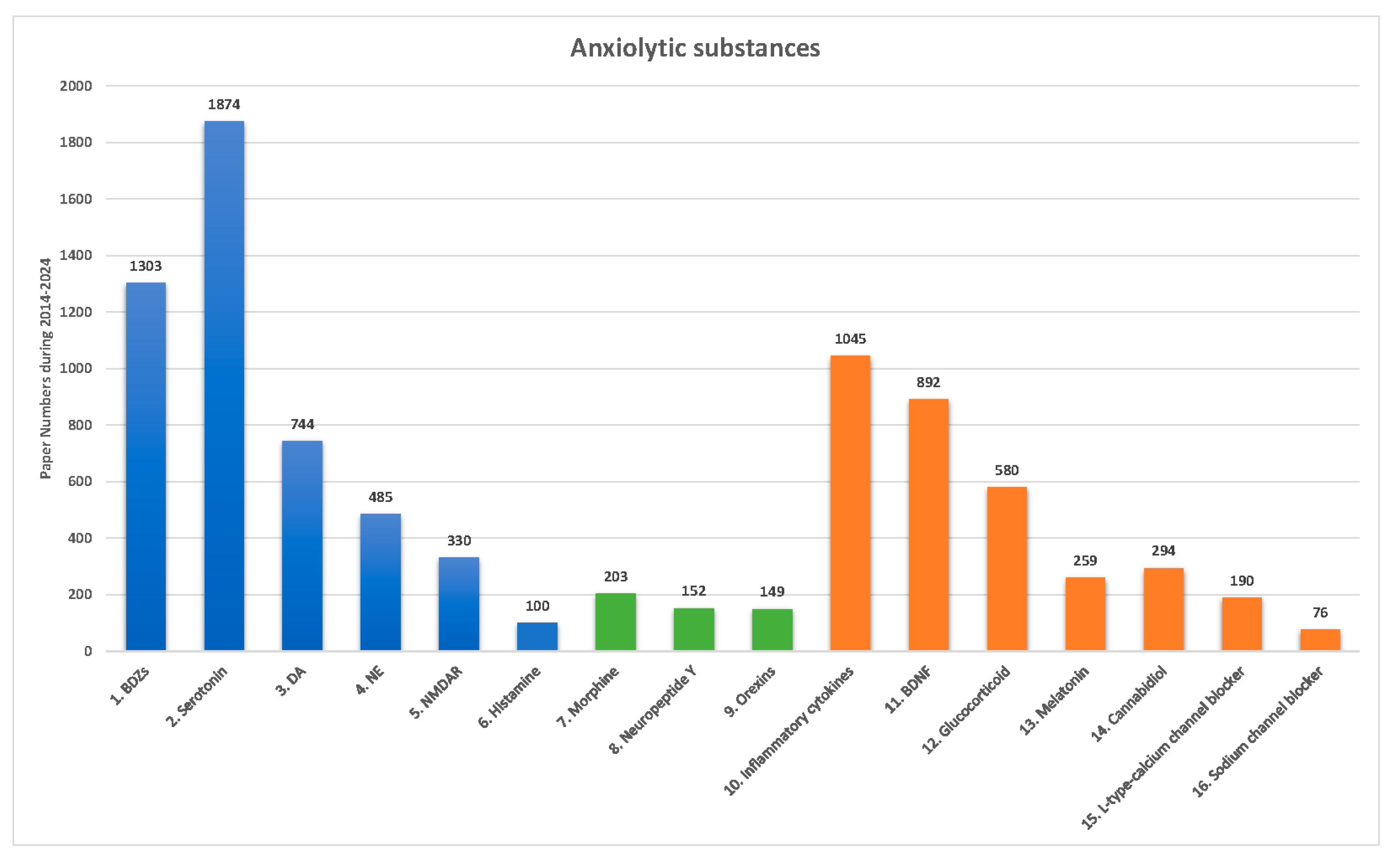

Table 1.
Prevalence and symptoms of eight major anxiety disorder types as described in the DSM-5.
| Anxiety disorders | Prevalence | Symptoms |
|---|---|---|
| 1. Generalized anxiety disorder (GAD) | 0.9% and 2.9% prevalence rates for adolescents and adults in the United States. | 1. Persistent and excessive anxiety 2. Worry about school and work performance |
| 2. Panic disorder | Appropriately 2–3% for adolescents and adults in the United States. | 1. Recurrent unexpected panic attacks. 2. Persistently concerned or worried about further panic attacks. |
| 3. Agoraphobia | Approximately 1.7% for adolescents and adults in the Unites States. | 1. Significant and intense fear or anxiety induced by an extendable range of surroundings in real or anticipated exposure. |
| 4. Post-traumatic stress disorder (PTSD) | 3.5% for adults in the United States. | 1. Concern intrusions and avoidance of memories associated with the traumatic event itself. 2. The critical features of PTSD vary. 3. Some patients encounter fear-based reexperiencing, emotional, and behavioral symptoms. 4. Others feel anhedonic or dysphoric mood states, and negative cognitions may be most distressing. 5. In some cases, arousal and reactive-externalizing symptoms are prominent 6. Others produce dissociative symptoms predominate. 7. Some individuals exhibit combinations of these symptom patterns. |
| 5. Social anxiety disorder (SAD; Social phobia) | Approximately 7% in the United States. | 1. Social phobia. 2. Fearful or anxious about or avoidant of social interactions and social surroundings that involve the possibility of being scrutinized. |
| 6. Acute stress disorder (ASD) | Less than 20% (do not involve interpersonal assault) in the United States. | 1. Symptoms may vary by individuals. 2. Anxiety response for reexperiencing or reactivity to the traumatic event. 3. A dissociative or detached presentation, although these individuals typically will also display strong emotional or physiological reactivity in response to trauma reminders. 4. A strong anger response in which reactivity is characterized by irritable or possibly aggressive responses. 5. The symptoms are development at least lasting from 3 days to 1 month. |
| 7. Separation anxiety disorder | About 0.9–1.9% for adults, 4% for children, and 1.6% for adolescents in the United States. | 1. Excessive fear or anxiety concerning separation from home or attachment figures. |
| 8. Obsessive-compulsive disorder (OCD) | About 1.2% in the United States. | 1. The presence of obsessions and compulsions. 2. Obsessions are repeated, persistent thoughts, images, or urges. 3. Persistent thoughts are voluntary associated with marked distress or anxiety. 4. Compulsions are repetitive behaviors or mental acts. |
Table 2.
Pharmacological treatments for eight types of anxiety disorders in the DSM-5.
| Anxiety disorders and treatments | |||||||||
|---|---|---|---|---|---|---|---|---|---|
| Medicines | Drugs | 1. GAD | 2. PD | 3. Agoraphobia | 4. PTSD | 5. SAD | 6. ASD | 7. Separation anxiety disorder | 8. OCD |
| 1. BDZs | Alprazolam Chlordiazepoxide Clonazepam Diazepam Lorazepam Oxazepam |
V V V V V |
V V V V V V |
V V V V V |
V V V V V |
V V V V V |
V V V V V |
V V V V V |
V V V V V |
| 2. SSRIs | Escitalopam Fluoxetine Fluvoxamine Paroxetine Citalopram Sertaline |
V V V |
V V V V V V |
V V V V V V |
V V |
V V V V V |
|
|
V V V V |
| 3. SNRIs | Duloxetine Venlafaxine |
V V |
V |
V |
V |
||||
| 4. TCA | Clomipramine Doxepine Imipramine |
V |
V V V |
V V |
V |
V |
V |
V |
V V |
| 5. MAOIs | Phenelzine Moclobemide |
V |
V |
||||||
| 6. Calcium modulators | Pregabalin | V |
V |
||||||
| 7. Azapirone | Buspirone | V | V | V | V | V | V | V | V |
| 8. Antihistamine | Hydroxyzine | V | V | V | V | V | V | V | V |
Note: (V) indicates that this drug is used in the specific anxiety disorders. DSM-5: Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition. Acute stress disorder (ASD); Benzodiazepines (BDZs); Generalized anxiety disorder (GAD); Monoamine oxidase inhibitors (MAOIs); Obsessive-compulsive disorder (OCD); Panic disorder (PD); Post-traumatic stress disorder (PTSD); Serotonin norepinephrine reuptake inhibitors (SNRIs); Selective serotonin reuptake inhibitors (SSRIs); Social anxiety disorder (SAD); Tricyclic antidepressant (TCA).
Table 3.
Comparison for anxiolytic substances and animal models in specific anxiety disorders.
| Mechanism of action | Mental illness | Animal models | Neural mechanisms and effects | References |
|---|---|---|---|---|
| Classical neurotransmitters: | ||||
| 1. Agonism of GABAa receptor | Anxiety disorders and PTSD | Conditioned fear learning | 1. BDZ drugs affiliate GABAa receptor 2. Cause anxiolytic effects |
Stevens et al. (2005); Lu et al. (2017) |
| 2. Inhibition of serotonin reuptake | Anxiety-related disorders (e.g., panic disorder, generalized anxiety disorders, PTSD) | Conditioned fear learning (contextual or cue) or PTSD animal models | 1. SSRIs drugs act the inhibition of serotonin reuptake 2. Lead to anxiolytic effects |
Hendriksen et al. (2014); Heesbeen et al. (2023) |
| 3. Agonism of dopamine receptor | PTSD | PTSD animal model (single prolonged stress) | 1. D2/D3 receptor agonism 2. Lead to anxiolytic effects |
Malikowska-Racia et al. (2019) |
| 4. Antagonism of norepinephrine receptor | PTSD | Conditioned fear learning | 1. Antagonism of alpha-1 adrenergic receptor 2. Disrupt anxiety- and PTSD-associated symptoms |
Laitman et al. (2014); O’Daniel et al. (2020) |
| 5. Antagonism of NMDA receptor | Anxiety disorders and PTSD | Conditioned fear learning animal model | 1. Antagonism of NMDA receptor 2. Attenuate fear symptoms |
Radulovic et al. (2018) |
| 6. Agonism of histamine receptor | Anxiety disorders | Isolation-induced aggressive behavior; Conditioned fear learning | 1. H3 receptor agonism 2. Reduce anxiety disorders |
Yokoyama et al. (2009) |
| Neuropeptides: | ||||
| 1. Agonism of opiates | PTSD | Conditioned fear learning | 1. Opioid receptor agonism 2. Result in anxiolytic effects |
Szczytkowski-Thomson et al. (2013); RaiseAbdullahi et al. (2019) |
| 2. Activation of neuropeptide Y | PTSD | PTSD animal model (single prolonged stress) | 1. Neuropeptide Y receptor agonism 2. Reduce anxiety behaviors and PTSD symptoms |
Serova et al. (2014) |
| 3. Antagonism of orexins receptor | Anxiety disorders (e.g., phobia, panic, and PTSD) | Conditioned fear learning animal models | 1. Orexins receptor antagonism 2. Impair fear behaviors |
Flores et al. (2015) |
| Nonclassical neurotransmitters: | ||||
| 1. Activation of inflammatory cytokines | Anxiety disorders and PTSD | Multiple anxiety and PTSD animal models | 1. Activation of inflammation cytokines 2. Cause anxiety disorders and PTSD symptoms. |
Felger (2018) |
| 2. Activation of BDNF | Anxiety disorders and PTSD | PTSD animal model (single prolonged stress) | 1. Activation of BDNF via TrkB receptor 2. Attenuate anxiety disorders |
Yin et al. (2022); Andero and Ressler (2012) |
| 3. Activation of glucocorticoid | PTSD | PTSD animal models | 1. Activation of glucocorticoid receptor 2. Block anxiety disorders |
Florido et al. (2023) |
| 4. Activation of Melatonin | PTSD | Conditioned fear learning animal models | 1. Activation of melatonin receptor 2. Impairs contextual fear conditioning |
Huang et al. (2017) |
| 5. Activation of cannabidiol | Anxiety disorders (e.g., generalized anxiety disorder, panic disorder, social anxiety disorder, PTSD) | Multiple anxiety disorders animal models | 1. Agonism of CB1 receptor 2. Impair multiple anxiety disorders (including generalized anxiety disorder, panic disorder, social anxiety disorder, and PTSD) |
Blessing et al. (2015) |
| 6. Action of L-type calcium channel blocker | Anxiety disorders | Caffeine-induced anxiety symptoms | 1. Antagonism of calcium channels 2. Cause anxiolytic effects |
Khurana et al. (2019) |
| 7. Activation of sodium channel blocker | PTSD | Conditioned fear learning (i.e., cue) | 1. Antagonism of sodium channels 2. Lead to anxiolytic effects |
Mirza et al. (2005) |
Note: BDNF: Brain-derived neurotrophic factor; PTSD: post-traumatic stress disorder.
Table 4.
Various animal models of anxiety disorders and PTSD in shaping anxiety models and testing anxiety behaviors.
Table 4.
Various animal models of anxiety disorders and PTSD in shaping anxiety models and testing anxiety behaviors.
| Animal models | Characteristics | Advantages | Disadvantages | When to use | Use frequency | References |
|---|---|---|---|---|---|---|
| A. Shaping anxiety models | ||||||
|
1. Fear conditioning: Cue/footshock |
Applying a discrete cue stimulus to pair with footshock-induced stress. | Cue is a clear-cut stimulus; high face, predictive, and constructive validity. | --- | Anxiety disorders; PTSD | *** | Lissek et al. (2013) |
|
2. Fear conditioning: Context/footshock |
Applying a contextual stimulus to pair with footshock-induced stress. | A contextual stimulus mimics the environment; high face, predictive, and constructive validity. | Context is a complex stimulus combining various environmental stimuli. | Anxiety disorders; PTSD | *** | Yu et al. (2022) |
| 3. Single prolonged stress | Animals are restrained for 2 hours and then forced to swim test for 20 minutes. Following recovery for 15 minutes, animals are exposed to ether until they lose consciousness. | Stable stress; face, predictive, and constructive validity. | Require complex and long-term stress manipulations. Single prolonged stress model is complex compared to the fear conditioning model. | PTSD | *** | Yamamoto et al. (2009) |
| 4. Learned helplessness | Animals are exposed to uncontrolled stressors through behavioral responses. | Manipulate footshock to shape stressor; thus, effective and easy manipulation. | Also used to test depression behaviors. | PTSD; MDD | * | Greenwood and Fleshner (2008); Maiet and Watkins (2005). |
| 5. Restraint stress | Mice are immobilized by placing them into well-ventilated 50 mL Falcon tubes for 2 hours per day over 21 consecutive days. | Restraint mice for immobility to induce stressor; easy preparation and manipulation. | Also used to test depression behaviors. | Anxiety disorders; PTSD | * | Mohammadi et al. (2019) |
| 6. Inescapable tail shock | Animals experience uncontrolled and inescapable tail shock, leading to acute stress. | Easy manipulation for Inescapable tail shock to induce stress. | Also used to test depression behaviors. | PTSD | * | Donner et al. (2018); Park et al. (2017) |
| 7. Underwater trauma | Animals are held underwater for 30 seconds. | Easy manipulation for holding animals underwater to induce stress. | Doubt in the face, predictive, and constructive validity. | PTSD | * | Zhang et al. (2019) |
| 8. Social isolation | Animals are raised without any companion or environmental enrichment. | Easy manipulation for animals without any companion. | Long-term conduction. | PTSD | ** | Aspesi and Pinna (2019) |
| 9. Social defeat | Animals are exposed to a trained aggressor conspecific for 6 hours daily for 5 or 10 days. | Easy manipulation for exposing aggressors inducing stress. | --- | PTSD | ** | Campos et al. (2013) |
| 10. Early-life stress | Maternal separation induces trauma events. | Face, predictive, and constructive validity. | Long-term conduction. | PTSD | ** | Schoner et al. (2017); Zhang et al. (2019) |
| 11. Predator-based stress | Predators or predator-related stimuli (such as predator’s urine) produce trauma induction. | Place predator and its related stimuli to induce stress; Easy manipulation. | --- | PTSD | ** | Zhang et al. (2019) |
| B. Testing anxiety behaviors | ||||||
| 1. Open field test | Tests time spent or crossing trials in the center area of the open field task for anxiety responses. | Face, predictive, and constructive validity. | Competition between locomotion and anxiety behavior. | Multiple anxiety disorders; PTSD | *** | Karl et al. (2008); Kraeuter et al. (2019) |
| 2. Elevated zero maze test | Test is conducted in the open arm to indicate the strength of the anxiety responses. | No crossing areas, which enforces animals’ decisions. | Conflicts arise from spending time in open arms and closed arms. | Multiple anxiety disorders; PTSD | ** | Campos et al. (2013) |
| 3. Elevated plus maze test | Test is conducted in the open arm to indicate the strength of the anxiety responses. | Cross the area to take a rest. | Long-term staying in the cross area between the closed and open arms | Multiple anxiety disorders; PTSD | *** | Karl et al. (2008) |
| 4. Elevated x-maze test | Tests the open arm time/total time ratio. | Face, predictive, and constructive validity. | --- | Multiple anxiety disorders | * | Critchley and Handley (1987); Handley and McBlane (1993) |
| 5. Light-dark box test | Tests activity and time spent in both brightly lit and dark apparatus compartments using the animal’s innate desire to explore novel areas. | Assessing the activity and time in light and dark box; Easy manipulation. | --- | Multiple anxiety disorders | ** | Karl et al. (2008) |
| 6. Startle response test | Pairing a conditioned stimulus (sound or light) with a footshock induces an anxiogenic “startle” response. | Face, predictive, and constructive validity for anxiety disorders. | Limitations in the style of anxiety behaviors for a cue with footshock. | Multiple anxiety disorders; PTSD | ** | Hart et al. (2016) |
| 7. Marble burying test | Animals with previous stress are placed in the test cage and then test amounts of marble burying up to 2/3 of the depth with bedding. | Face, predictive, and constructive validity for anxiety disorders. | A digging activity for a species-typical reaction to stress (e.g., rats and mice). | Multiple anxiety disorders; PTSD | ** | Archer et al. (1987); Kedia and Chattarji (2014) |
| 8. Defensive shock-prod burying test | A familiar test cage or home cage with plentiful bedding and a hole in the wall 2 cm above the bedding. An electrical probe is connected to a shock source. Measuring the depth to which the prod is buried. | Face, predictive, and constructive validity. | Animals do not touch the electrical probe and cannot induce anxiety. | Multiple anxiety disorders | ** | Yang et al. (2004) |
| 9. Grooming test | Stressors (e.g., novel environment, predator exposure, bright light) induce grooming. |
Test grooming behavior; simple manipulation. | Questionable face, predictive, and constructive validity. | Multiple anxiety disorders; PTSD | * | Hart et al. (2016) |
| 10. Social interaction test | Two mice were in the test environment for 5 or 10 minutes and recorded the duration and frequency of all social interactions, including sniffing, following, chasing, touching, and biting. Higher scores in social interactions indicate lower anxiety behaviors. | More accessible design and manipulation. | Limitations in social anxiety disorders. | Multiple anxiety disorders; PTSD | ** | Hart et al. (2016) |
| 11. Suok test | The Suok task simultaneously tests anxiety vestibular and neuromuscular deficits by combining an unstable rod with novelty. The threats of height, loss of balance, and novelty are presented to analyze anxiety and assess animal exploration. |
Face validity. | Doubt in predictive and constructive validity. Competitions in testing for multiple behaviors. | Multiple anxiety disorders; PTSD | * | Kalueff and Tuohimaa (2005) |
| 12. Stress-induced hyperthermia test | Based on the evolutionarily important role of hyperthermia, whereby body temperature rises upon encountering stressful stimuli. | Across many species, including humans. | Testing errors from a lot of confounding factors. | Multiple anxiety disorders; PTSD | * | Hart et al. (2016) |
| 13. Hole-board test | Tests head dipping behaviors. More head dips indicate more explorations and lower anxiety. | Assessing animals’ head dipping behavior; Easy preparation and manipulation. |
Doubt in the face, predictive, and constructive validity. |
Multiple anxiety disorders | * | Kliethermes and Crabbe (2006) |
| 14. Rat exposure test | Uses animals' natural defensive “avoidance” behavioral response to signs of potential danger, such as a natural predator. Defensive behaviors include stretch-attend posture, stretch approach, freezing, burying, and hiding. | Testing the nature defensive behavior; thus, easy to use and manipulate. | Variations during different species. | Multiple anxiety disorders | * | Hart et al. (2016) |
| 15. Novel object test | Testing the approach-avoidance behaviors of mice in response to novel stimuli. Longer time in exploration for a novel object, indicating lower anxiety behaviors. | Face, predictive, and constructive validity. | Confused with recognition tests using the same task. | Multiple anxiety disorders; PTSD | * | Powell et al. (2004) |
Note: (*) numbers indicated the specific animal models’ usage frequency for anxiety disorders and PTSD; asterisks (*, **, ***) indicate relative usage frequency.
Table 5.
Choosing the best animal models for testing a variety of anxiety disorders and clinical drugs.
Table 5.
Choosing the best animal models for testing a variety of anxiety disorders and clinical drugs.
| Animal models of anxiety disorders | Clinical anxiolytic drugs | ||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Anxiety disorders |
1. Fear conditioning (Cue) |
2. Fear conditioning (Context) |
3. SPS | 4. Learned helpless ness | 5. Restraint stress | 6. Inescapable tail shock | 7. Underwater trauma | 8. Social isolation | 9. Social defeat | 10. Early-life stress | 11. Predator-based stress | Medicines | |
| 1. GAD | V | V | BDZs; SSRIs; SNRIs; TCA; Calcium modulators; Azapirone; Antihistamine | ||||||||||
| 2. PD | V | V | V | BDZs; SSRIs; SNRIs; TCA; MAOIs; Azapirone; Antihistamine | |||||||||
| 3. Agoraphobia | V | BDZs; SSRIs; SNRIs; TCA; Azapirone; Antihistamine | |||||||||||
| 4. PTSD | V | V | V | V | V | V | V | V | V | V | V | BDZs; SSRIs; SNRIs; TCA; Azapirone; Antihistamine | |
| 5. SAD | V | V | BDZs; SSRIs; SNRIs; TCA; MAOIs; Calcium modulators; Azapirone; Antihistamine | ||||||||||
| 6. ASD | V | V | V | V | V | BDZs; TCA; Azapirone; Antihistamine | |||||||
| 7. Separation anxiety disorder | V | V | BDZs; TCA; Azapirone; Antihistamine | ||||||||||
| 8. OCD | V | V | V | V | BDZs; SSRIs; TCA; Azapirone; Antihistamine | ||||||||
Note: (V) indicates that this drug is used in the specific anxiety disorders. DSM-5: Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition. Acute stress disorder (ASD); Benzodiazepines (BDZs); Generalized anxiety disorder (GAD); Monoamine oxidase inhibitors (MAOIs); Obsessive-compulsive disorder (OCD); Panic disorder (PD); Post-traumatic stress disorder (PTSD); Serotonin norepinephrine reuptake inhibitors (SNRIs); Selective serotonin reuptake inhibitors (SSRIs); Social anxiety disorder (SAD); Tricyclic antidepressant (TCA).
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



