
Submitted:
10 December 2024
Posted:
11 December 2024
You are already at the latest version
Abstract
Background/Objectives: Early pediatric cochlear implantation positively impacts early language outcomes. The Teenager and Young Adults Cochlear Implant (TAYACI) study investigates long-term outcomes of early implantation and factors influencing variability among cochlear implant (CI) users. This article outlines participants’ background, early language outcomes, and multidisciplinary study protocol. Methods and Materials: Individuals aged 12-22 received CIs before 30 months of age, followed-up at the same hearing implant center, and adhered to a standard school curriculum were invited to participate. Out of 109 eligible CI users, 50 participated; 46 agreed to undergo clinical assessments, while four completed questionnaires only. Results: The mean age at 1st CI was 15.63 months (SD=6.0). All but one communicated with spoken language(s). Participants attended mainstream schools and had highly educated parents. Over half (56%) had received Auditory Verbal Therapy in early childhood. Earlier implantation correlated with better language understanding one year post-CI. Conclusions: Earlier implantation was associated with better early language outcomes, with parental education level and early family-centered intervention likely contributing. Future Sub-Studies will investigate multidisciplinary long-term effects of pediatric cochlear implantation in adolescents.
Keywords:
cochlear implants
; adolescents
; young adults
; long-term outcomes
; baseline characteristics
; language understanding
; study design
1. Introduction
Cochlear implantation is a successful treatment for congenital and pre-lingual permanent severe-to-profound sensorineural hearing loss (SNHL). Most children with typical cognitive development who receive cochlear implants (CIs) at a young age, typically during infancy, are expected to acquire spoken language through listening and primarily follow a standard school curriculum [1,2]. Furthermore, long-term educational outcomes as well as quality of life are positively influenced by earlier age at CI (<18 months) [3]. However, the population is heterogeneous and the hearing ability and spoken language development with CI vary, despite early age at implantation. The understanding of which factors that affect this variation are only beginning to emerge [4]. There is a need to not only understand the outcomes in early childhood, but also the complexity of long-term CI intervention outcomes. This would preferably be studied in population-based cohorts, in order to adopt more specific and tailor-made guidelines and recommendations in the hearing care system [5].
Older school-aged children and adolescents are in transitional phases of development, moving from childhood through adolescence into adulthood. Little is known about how CI users navigate these developmental stages while simultaneously continuing to adapt their listening abilities with CIs, in complex listening and learning environments with varying amount of support. Only a few large-scale studies have investigated the long-term cognitive skills in children with CI [1,2,6]. For school-aged children, previous research findings show that early age at 1st CI affects speech recognition and speech, and may indirectly also affect cognitive skills like reading and language abilities [2,4]. Long-term outcomes after pediatric CI are particularly sparse related to finer linguistic competence, general well-being, and listening skills in more complex listening conditions. In addition, it is also unclear how the chronic electrical stimulation in the inner ear and the CI procedure itself affects vestibular function over time, and manifests in teenagers and young adults who received CIs at an early age.
In our group’s cross-sectional and longitudinal clinical studies, we demonstrated that age at 1st CI is a critical factor for early spoken language development but does not significantly influence speech recognition [7,8,9]. However, some of these findings were based on retrospective analyses, lacked control groups, or included children who were too young to participate in certain assessments. Limited clinically-based genetic screening was conducted, and assessment of basic auditory skills was not always performed. In addition, we have previously not included multilingual participants in our studies, although around 30 % of all children who receive CIs at the Hearing Implant Center (HIC), Karolinska University Hospital use several languages for communication [10]. Multilingual cohorts are generally understudied in the literature, which is problematic from many perspectives, especially in relation to health-care equity [11,12]. Another demographic factor that is known to influence early language development is the socioeconomic level of the family [13], which may also affect long-term outcomes in teenagers and young adults.
Approximately 0.2% of all newborns in Sweden are born with hearing loss, with 0.04% of them have a severe-to-profound bilateral SNHL [14]. The population of individual with prelingual deafness who use CI is highly heterogeneous, partly due to variations in the duration of auditory deprivation or reduced hearing experience before undergoing CI surgery [15]. Although the Universal Newborn Hearing Screening (UNHS) system was not fully implemented across all regions of Sweden until 2008, its adoption has since led to a gradual reduction in the age at which most children with congenital or prelingually acquired deafness receive their 1st CI. During the time period 2018-2023, 39,3% (n=328) of all Swedish children with prelingual deafness received the 1st CI before 12 months of age [16]. Previously, in the time period of 2000-2011, which is the birth years of the participants in the present follow-up study, the mean age at 1st CI was somewhat older. During this time period, only 14,9% (n=424) of all Swedish infants recieved a CI before 12 months [16]. Other hearing care factors have also changed in the Swedish system gradually. Today, children recieve simultaneous bilateral CIs, or develop listening and spoken language through bimodal hearing, using a combination of a unilateral CI and hearing aid. Furthermore, Family-Centered Early Intervention (FCEI) options, like Auditory Verbal Therapy (AVT) [17], have been introduced on a national basis since around 2005. These advancements, particularly the introduction of early preventive interventions, have resulted in better opportunities for children born deaf to develop listening skills and spoken language on par with their chronological aged peers with typical hearing [9].
There is solid support in previous research that early implantation has positive effects on linguistic and cognitive development [1,31,32]. Albeit shown by our previous work that implantation before nine months is ideal [9], the large variability in the linguistic performance of children growing up with CI can not fully be explained by age at implant [4]. For example, differences in executive functions could be related to the variability in linguistic performance. The development of executive functions is closely linked to linguistic development [44,45], and studies have shown differences in the relationship between executive functions and language in individuals with CI compared to peers with typical hearing [46,47]. When it comes to higher linguistics skills, such as understanding metaphors, research in individuals with CIs is still scarce. A handful of studies has found difficulties with metaphor comprehension in individuals with CI [48,49,50]. There is, however, further need to explore both metaphor comprehension and executive functions, and their relationship, in early implanted individuals.
Hearing, a fundamental part of verbal communication, shows large outcome variability after cochlear implantation in children [12]. A hallmark of hearing is the recognition of speech. Studies show conflicting results regarding the impact of early implantation on speech recognition in quiet conditions [1,7,23,24], whereas it is widely accepted that children with CI’s are more susceptible to noisy conditions than children with typical hearing [6,7]. Little is known, however, about long-term performance in children with an early age at CI surgery, specifically in more naturally occurring and complex listening environments, in which they spend much time communicating and learning. An example of a complex listening environment is a condition in which a listener wants to understand speech in the presence of masked speech. We are aware of a few studies measuring performance for such conditions in children with CIs at 6 and 9 years of age [25,26] but not in teenagers and young adults with early implantation. Misurelli et al. [25,26] observed large variability in performance for children using implants in conditions with interfering speech. The source of this variability is poorly understood. Another example of an important auditory ability that may aid daily life communication is sound localization. We and others have shown that horizontal sound localization accuracy is better with bilateral than with unilateral CIs [7,27]. Sound localization seems to develop gradually after bilateral input is provided despite relatively late and/or sequential implantation [28], but simultaneous implantation allows higher accuracy in children aged 7-10 years [29]. It is unknown if the benefit of simultaneous implantation is maintained into adolescence and early adulthood, a question we address in this study.
The inner ear balance (vestibular) organ functions as a complex inertial sensor which detects the head movements/positions and adjusts the muscle activity in the trunk, limbs, neck and eyes for an optimal gaze stabilization and body posture during movements and stance. The vestibular organ consists of two otolith organs (sacculus and utriculus, activated by linear accelerations) and three semicircular canals (activated by angular accelerations). Accumulated clinical evidence has revealed a vestibular deficit in DHoH children with high prevalence [30], and a potential detrimental effect of cochlear implantation on vestibular function [31,32]. Moreover, the presence of a vestibular impairment, especially in the form of a bilateral vestibular loss, has been shown to alter the motor development of young children [33], and the motor proficiency in school-aged/teenaged CI recipients [34,35]. Impaired gaze stabilization, reading difficulties [36], acquisition of protective fall reactions [37], and cognitive abilities [38] have also been associated to vestibular failure in developmental age. The impact of vestibular impairment on the motor abilities, hearing, speech and cognitive function of early CI recipients grown up to school/teenage is still debated and in need of further investigation [39,40,41].
A factor that contributes to the heterogeneity in individuals with CI is etiology, or the cause of SNHL or deafness. Around 30-40% of all children who are deaf or hard of hearing have additional diagnoses that may affect their outcomes [18]. Knowledge of the cause of a child’s deafness or SNHL is crucial, both for the individual, but also for health care professionals and caregivers, so they can support children and teenagers who are deaf and hard of hearing (DHoH) in optimal and efficient ways. The most common causes of deafness and SNHL are due to genetic mutations in genes that are important for the hearing pathway development and auditory functioning. Gene mutations are believed to be the cause of at least 50% of SNHL and deafness in children [16]. Thirty percent of the genetic causes of SNHL are syndromic, including examples such as Jervell and Lange-Nielsen syndrome, Waardenburg syndrome, Pendred syndrome, and Usher syndrome. Common causes of congenital and acquired SNHL in children include congenital infections, such as rubella or congenital cytomegalovirus (cCMV) infection, which alone accounts for approximately 5-20% of cases [19]. However, in the Western world, rubella is nowadays rare due to vaccination programs but cCMV infection is still very common [20]. Meningitis is now rare in Sweden due to the introduction of the pneumococcal vaccine into the national childhood vaccination program in 2009 [21]. Most newly identified Swedish children with hearing loss are nowadays tested both genetically for mutations known to cause hearing loss (GJB2), and for congenital CMV infection (not screened at birth). Hence, the cause of a child´s deafness or SNHL is known for more children, but still not for all individuals. Possible reasons why not all children have a conclusive etiology include the gradual evolution of clinical diagnosis practices over time, which have varied across different counties in the country. Additionally, all genetic mutations causing hearing loss have been identified, and the cost for extensive genetic testing in clinical settings may not be feasible for everyone. Most children born with cCMV infection experience progressive SNHL, which is currently not detected at birth during the universal newborn screening. As a result, many children with cCMV infection undergo a delayed hearing and cCMV diagnostic process. In Sweden, a retrospective CMV diagnosis can be made using a dried blood test (PKU-test) that is conducted at birth on all children and stored for potential future analysis. Identifying the cause of SNHL can provide a clearer prognosis for the child and ensure that appropriate support is offered based on the diagnosis.
Mental health and health-related quality of life (HRQoL) cover a wide and comprehensive outcome area. In this project these areas are especially related to listening experiences with CI in different environments and situations, and the participants’ wellbeing. The heterogeneity in outcomes found in this group may be related to comorbid conditions due to etiological factors and may not only influence language, hearing and social skills, but also mental health. Previous studies have mainly been based on questionnaires, where parents of children with CIs have reported on their behalf. Furthermore, few interview studies of adolescents with CIs have been conducted, and only in small groups with a large variation of age at 1st CI [51,52,53]. This may be due to the fact that it is not until present times, that individuals that were implanted at an early age have become teenagers and young adults and are able to speak for themselves.
The risk of depression and other mental health-related problems increases dramatically during adolescence, and therefore the prevention of depression during this period is especially prioritized for all adolescents [54,55]. Previous studies have reported that children with CIs have more problems with mental health than peers with typical hearing [56]. As an example, children and teenagers with CI have previously been shown to have more depressive symptoms than age-matched peers with typical hearing [57]. One of the traits known to have a protective effect against depression is higher levels of self-efficacy [58]. This factor has been investigated in parents of young children who are DHoH [59,60], but less so in the target group of the present study. Prospective multidisciplinary evaluation of higher-level cognitive skills in relation to listening skills, and HRQoL, is highly motivated. By conducting such research in a larger group of teenagers and young adults who have grown up using CIs from early childhood, and matching them with controls with typical hearing, we will gain new valuable insight. This new knowledge may contribute to understanding the specific clinical needs of subgroups and individuals with CI.
This far, there are only a few previous longitudinal, multicenter, and population-based studies that have examined children who are DHoH. However, these studies provide valuable insights into the population by addressing the sample size limitations often encountered in single-center studies. Such research has primarily been conducted in Anglo-Saxon countries like Australia and the USA. One example is the population-based Longitudinal Outcomes of Children with Hearing Impairment (LOCHI) study from Australia which has included 460 children with different types of hearing loss and deafness [61] but to our best knowledge they have not yet investigated outcomes of teenagers. At five years of age, children in the LOCHI study with severe or profound SNHL who received CI before 12 months of age, had significantly higher language scores than those who received CI at an older age [62]. In the US, the Childhood Development After Cochlear Implantation (CDaCI) study, outcomes of children with cochlear implants were compared to age-matched children with typical hearing [63]. Another US study is the Outcomes of Children with Hearing Loss (OCHL) study, examining different factors influencing language and auditory outcomes in young children with permanent, bilateral and mild to severe-to-profound SNHL [64]. The findings of these studies are highly valuable but may not be fully representative of other regions and countries worldwide.
The aim of this article is to describe the Teenagers and Young Adults with Cochlear Implants (TAYACI) study, specifically focusing on its design and approach, which includes five key study domains: language and cognition; hearing and listening; balance; etiology; and mental health and HRQoL. Additionally, the article presents the background characteristics of participants with CI and their families. Another objective was to examine their early hearing and language development in relation to the age at 1st CI. The TAYACI study is a national cohort study, with all participants being followed-up at the same CI center that serves half of Sweden’s population.
The overall two PICO-questions motivating the multi-disciplinary research program:
- How do teenagers and young adults who received their 1st CI before 30 months perform long-term in linguistics, cognition, hearing, balance, self-efficacy and health related quality of life, in comparison to age-matched controls with typical hearing?
- How do adolescents and young adults with CIs perceive their listening and communication experiences in different everyday life situations and activities (school, work, leisure), in relation to controls with typical hearing?
- Hypotheses:
- Q1: Age at 1st CI has an impact on long-term cognition, linguistics, hearing and HRQoL.
- Q1: Hearing outcomes are related to modifiable clinical parameters.
- Q1: Lower socio-economic status of families are related to poorer long-term outcome (cognition, language and HRQoL).
- Q1: Etiological factors affect balance, hearing, language, cognition and HRQoL.
- Q2: Self-perceived HRQoL is positively affected in adolescents and young adults with CI if they have acquired age-equivalent language skills and is related to better hearing.
- Q2: The overall HRQoL outcome in adolescents and young adults with CI is similar to that of age-matched controls with typical hearing (TH).
2. Material and Methods
2.1. Study Design
Cohort study with a long-term follow-up approach including quantitative and qualitative methods.
2.2. Brief Prospective Project Overview
The ongoing research program consists of five sub-studies (Sub-Study I-V) in the same cohort of individuals with CIs. Inclusion criteria: adolescents who had received their 1st CI before the age of 30 months and were followed-up at the HIC, Karolinska University Hospital, aged 12-22 years, and who follow or have followed normal school curriculum were asked to take part in Sub-Study I-V during the period 2022-2023. Participants were invited to the clinic for an extended research visit at the time point of their regular clinical appointment. The multidisciplinary research team consisted of two Principal investigators, a Speech-Language Pathologist (Sub-Study I), a clinical audiologist, an engineer and radiologist (Sub-Study II), two balance specialists (medical doctors) and a physiotherapist specialist (Sub-Study III), a medical doctor specialized in audiology (Sub-Study IV), and a teacher of the deaf (Sub-Study V). Saliva samples were taken at HIC for those with unknown cause of deafness and who specifically volunteered for this investigation (Sub-Study IV). High resolution photon-counting computer tomography was performed to estimate electrode insertion depth and scalar location. Information from previous medical records and the clinical software for cochlear implant fitting were collected and used as background material, and as predictors for hearing and language outcomes, respectively. The adolescents filled out questionnaires either before the follow-up visit or during the test occasion, with support provided if needed. Additionally, they were invited to participate in semi-structured focus group interviews or individual interviews scheduled after the follow-up visit at HIC. Caregivers of participants under 18 years of age also filled out some questionnaires.
2.3. Participants
Initially, we recruited a clinical cohort of participants with CI at the HIC, Karolinska University Hospital. Thereafter we recruited controls with typical hearing who were matched for age. Control groups were recruited for each Sub-Study (I-V), a mainly overlapping cohort. Descriptive information about controls will be shared in later publications.
A total of 135 individuals met the criteria of age at implantation <30months and were aged 12-22 years in the clinical database. Twenty-six individuals were excluded due to non-fulfillment of inclusion criteria (other curriculum). Invitations were sent to 109 individuals who were followed up at Karolinska University Hospital and met the study criteria. Twelve declined to participate, 51 accepted the invitation and the remaining 46 did not respond. One participant was incorrectly invited from start (did not meet the inclusion criteria of age at CI 1), and was therefore excluded from the study (Figure 1). The final number of participants was 50 (27 females and 23 males), aged 12-22 years (see Table 1 in results section). The majority used spoken Swedish as their primary communication mode (n=42), three participants used at least two spoken languages in their daily communication. Another four participants used spoken Swedish with sign support (n=4) and one participant primarily used sign language and some spoken Swedish (n=1). For further demographic background information and hearing characteristics see Table 1 and Table 2 (results section).
2.4. Descriptions of Material and Procedures Used in Sub-Studies (I-V)
Background information (demographics) and academic level: background information (family background, family socioeconomic status level, communication mode, school setting, reading and screen use habits), and questions about national school test results: Swedish, Mathematics and English at 6th and 9th school year level and in high-school) (www.skolverket.se). Information about early hearing background characteristics like age at CI surgery, and language outcome results after 1st CI have been collected from medical records at HIC, Karolinska University Hospital, with consent from participants. This article presents background information from medical records available at the time of data collection, as well as clinical data related to early outcomes. For an overview of the entire test battery and the specific instruments used in Sub-Study I-III and V, see Supplementary Materials (S1).
2.4.1. Sub-Study I: Language and Cognition
During one test session, participants were assessed on language and cognition, including executive functions, reading, lexical-semantic abilities, and metaphor comprehension (S1). Since there is no standardized test assessing metaphor comprehension in Swedish a new task was devised for this study, based on previous work by Kalandadze and colleagues [65]. The metaphor task includes multiple-choice responses as well as verbal explanation. Responses will be analyzed both quantitatively and qualitatively. Metaphor comprehension and executive functions task performance will be analyzed separately, in relation to each other, as well as in relation to lexical-semantic abilities. The total test time for the language and cognition tasks was three hours, which included two ten-minute breaks for each participant. Participants and their parents also filled out one or two questionnaires during their visit, which are included with the additional documents and questionnaires used in Sub-Study V (S1).
2.4.2. Sub-Study II: Hearing and Listening
The participants’ hearing was tested in a 2.5-hour visit including short breaks between the tests (S1). Participants were always tested in bilateral listening conditions, e.g. bilateral CIs or bimodal listening.
Hearing thresholds
Aided sound-field hearing thresholds were recorded using frequency-modulated tones with center frequencies at 0.125, 0.25, 0.5, 1, 2, 3, 4, 6 and 8 kHz for left, right, and bilateral listening conditions.
Recognition of words in quiet
Speech recognition was assessed in sound-field using a standardized and validated Swedish clinical speech audiometry test [66]. The test material consisted of phonemically balanced lists of 50 monosyllabic words.
Recognition of sentences in masking speech and spatial release from masking
An adaptive psychoacoustic task was used to estimate the 40% recognition threshold for target speech in co-located and spatially and symmetrically separated masking speech (e.g., [45,46]). Target sentences were the Swedish Hagerman sentences (female voice, [69]), whereas the masking speech consisted of four non-correlated speech signals (one male voice reading out of a novel).
Horizontal sound localization accuracy
Horizontal sound localization accuracy was measured in the frontal plane (12 sound-sources evenly distributed across ±55 degrees azimuth; 10 degrees between target sound-sources). The objective determination of overall localization accuracy was based on a rapid and reliable technique utilizing eye-gaze responses [70]. Localization performance was measured four times using four different stimuli, each of which provided various spatial cues [71].
Interaural level and time differences
A psychoacoustic test of the just noticeable difference of interaural level and time difference of a 250 Hz pure tone was administered. Headphones (HDA200, Sennheiser) were used together with the PsychoPy test suite (University of Nottingham), [72] in an adaptive 2-up-1-down 1I-2A forced choice paradigm [73].
Assessment of programming levels and objective and behaviorally assessed thresholds
The participants went through a fitting session before the language and hearing tests to ensure full technical functionality. No changes in programming levels were introduced at this occasion. The electrical comfort and threshold levels of the participants’ clinical maps were collected, and the actual electrical threshold was assessed behaviorally by means of the modified Hughson-Westlake method at three positions along the electrode array. Additionally, electrically evoked compound action potentials were measured when possible.
Spectral discrimination
A psychoacoustic test of spectral discrimination previously used in adults [74] was used to assess the peak-valley ratio (PVR) in dB at 4 and 8 frequency channels. Briefly, the sound was created by alternating the amplitude in frequency bands of a pink noise. Each sound was created in two versions where the first half of the sound had odd bands attenuated and the second half of the sound had even bands attenuated to ensure equal loudness. Each sound pair was created in 10 versions with unique frozen pink noises to make sure the subject would not be able to learn to recognize the character of the noise. One of the 10 versions were chosen randomly for each iteration. The procedure followed an adaptive staircase 2 down 1 up 3I3A forced choice paradigm, preceded by a training session.
Photon-counting computer tomography
Photon-counting computer tomography was performed in a subset of participants to reconstruct inner ear anatomy with high resolution, determine scalar location for CI electrodes, and quantify interaural asymmetries of angular insertion depth (AID).
2.4.3. Sub-Study III: Balance
The balance function has been studied at different levels.
Vestibular function: The vestibular responses (vestibular reflexes) were investigated with two modern clinical tests: the video head impulse test (vHIT) and the VEMP (vestibular evoked myogenic potentials). vHIT is the recording of eye velocity at peak of head velocity during passive head jerk rotations on the planes of semicircular canals [75]. The main measure is the gain of eye velocity on head velocity which is directly correlated to the residual function in the semicircular canals. By vHIT it is possible to obtain separately the VOR gain of each of the three semicircular canals (anterior, lateral and posterior) for the two sides. The VEMP is the recording of short latency muscle responses at cervical muscles (cervical VEMP, cVEMP) and eye muscles (ocular VEMP, oVEMP) in response to vestibular activation by impulsive air conducted sounds (AC) or skull vibrations (bone conduction, BC) [76]. cVEMP is considered a test of sacculus function and oVEMP of utricular function. By vHIT and VEMP it is possible to map in detail the function of the different parts of vestibular organ and the integrity of vestibular pathway.
Balance tests: An assessment of motor function, balance and gait, blinded to vestibular testing, was conducted by a physiotherapist using the subtest of balance from Bruininks-Oseretsky Test of Motor Proficiency (BOT-2) [39], the sections Reactive Postural Responses and Sensory Orientation from Kids-Balance Evaluation System Test (Kids-BESTest) [77], Walking 10 meters with and without head turns [78], and Head Impulse Test (HIT). In addition, self-reported physical activity, and experience of balance were measured with a self-composed questionnaire and SGPALS [79]. The aim of this testing was to ascertain possible balance and motor deviations at common clinical testing in CI recipients and to find possible associations between balance alterations and vestibular impairment. Motor pattern recording: A quantitative analysis of balance and motor functioning was conducted with inertial sensors. All participants wore a total of 7 wireless inertial sensors attached to different body parts of the kind APDM during the balance tests [80]. This was done to obtain a parametric analysis of their motor pattern. Each sensor could measure the intensity, direction, and duration of the seven body segment movements during testing. The data obtained was analyzed with machine learning and AI analysis. For the technical specifications, the protocol and the parameters used in the studies, see Supplementary Materials (S1).
2.4.4. Sub-Study IV: Etiology
The cause of deafness or sensorineural hearing loss (SNHL) was identified in 74% (n=37) of the cohort at the time of the follow-up study (see Table 1). This relatively high proportion of known diagnoses can be attributed to the early development of a clinical protocol for etiological investigation at HIC, Karolinska University Hospital, implemented at the time participants underwent CI surgery. The protocol included targeted screening for cCMVinfection and genetic testing for GJB2 mutations (connexin 26), two of the most common causes of deafness and SNHL. Additionally, the HIC collaborated with referring local audiological clinics and conducted parental interviews during the cochlear implant investigation. These interviews gathered information on the child’s general health and any family history of hearing loss, facilitating the identification of hereditary causes. The thirteen participants with an unknown diagnosis were offered a clinical diagnostic investigation, including a genetic test panel (saliva sample), and all agreed to participate. Through this procedure, we hope to determine the etiology for the majority of participants with CI, facilitating subgroup analyses of different etiologies in relation to various outcomes in Sub-Studies I-V. This effort will contribute new insights to the literature on how balance, hearing, language performance, mental health, and HRQoL may be influenced by different etiological factors.
2.4.5. Sub-Study V: Mental Health and Health-Related Quality of Life
To investigate mental health and HRQoL, a mixed-model design was employed, integrating both quantitative (questionnaires) and qualitative (focus groups, individual semi-structured interviews, and text analysis) methods (S1). Participants received questionnaires along with a document containing demographic questions on the first day of testing, with responses collected on the second day. This processallowed participants to provide feedback on the instruments and seek clarification about any questions that arose while completing the questionnaires.
All participants were informed that they would receive a separate invitation to join a focus group shortly after their on-site assessments. For those unable or unwilling to participate in focus groups, individual semi-structured interviews were offerered as an alternative. These interviews were analyzed using content analysis [81].
2.5. Statistics
Statistical analysis was done using JASP (version 0.19.0) and RStudio (version 2022.07.2+576). The baseline characteristics, socioeconomic status, and retrospective outcomes of the study group are summarized using descriptive statistics at the group level. Spearman’s rank correlation analyses were performed to examine the relationship between age at 1st CI and language understanding after one year with CI. In future manuscripts, the selection of appropriate statistical methods will depend on the sample sizes of control groups and the data distribution in each Sub-Study (I–V). These methods may include tests for group differences, correlations with additional factors, and, where feasible, regression analyses.
3. Results
3.1. Representativeness of Study Sample
To assess whether the participants were representative of the broader population, we analyzed previously collected clinical data on receptive vocabulary for those who agreed to participate (n=50) and those who declined or did not respond to the invitation (n=58). Data for Peabody Picture Vocabulary Test PPVT (3 and 4) [82,83] were available for 42 of 50 (84%) of the participants at a mean age of 10.0 years (SD=1.0 years) and 36 of the 58 (62%) non-participants at a mean age of 10.1 years (SD = 0.9 years). The analysis revealed no differences in receptive vocabulary outcomes (p = 0.30, independent samples t-test) (Figure 2a) or age at implantation (p = 0.65, independent samples t-test) (Figure 2b) between participants and non-participants.
3.2. Characteristics of Participants with CI and Their Families
Descriptive background data on group (n=50) is presented in Table 1 and Table 2, with focus on hearing-related factors, etiology status at the time of recruitment, and family characteristics.
The educational level of the participants’ parents may be somewhat higher than expected in the population (Table 1). According to population-based data, the proportion of highly educated individuals has increased significantly since 2000, rising from 16% to 30%, while the number of those with lower education levels has declined, except among immigrant groups [84]. In 2021, it was estimated that 52% of women and 39% of men aged 25–64 had completed post-secondary education [84]. Educational attainment is notably higher in larger cities, and among individuals aged 45 and older, suggesting that Swedish adults commonly continue their university education later in life.
3.3. Early Follow-Up Procedures and Habilitation Actions After First CI
The participants with CI come from different parts of Sweden (29 from the capital area and 21 from other regions). They have been followed-up by the same multidisciplinary cochlear implant team at HIC, Karolinska University Hospital, on a regular basis with a standardized protocol. An educational audiologist has investigated the speech recognition, an speech-language pathologist has assessed spoken language abilities, and an engineer has controlled and mapped their CI(s) at the same occasions. Furthermore, they have sometimes met audiologists (MD) to discuss medical- and aetiological issues and more rarely a social worker to discuss questions related to insurance and support actions in the local hearing care after surgery etc. After initial investigation, surgery, and first fitting, post-operative evaluations were performed 6 months after surgery, and then every 6 months until the children were four years. Thereafter, they have been assessed at the same center on an annual basis until 17 years of age. All participants except one have received some sort of Family-Centered Early Intervention (FCEI) in their local hearing care team. Twenty-eight families had received Auditory Verbal Therapy (AVT) on a regular basis (at least two sessions per month during the first year after initial CI-fitting), while 22 families had received unspecified FCEI services, with a more auditory oral or total communication approach, and with unclear frequency and intensity (see Table 2). It was a clear dominance of AVT provided in the capital area (n=22), and only six families who received AVT in other regions.
3.4. Language Understanding After One Year with First CI
In our previous retrospective study, we found that earlier ages at 1st CI were associated with better language understanding in the early years [9]. In this study, we investigated whether the same pattern holds for the current cohort. Language development is regularly assessed at the HIC, Karolinska University Hospital to evaluate outcomes after cochlear implantation. We present data on language understanding using the third version of the Reynell Developmental Language Scales (RDLS-III) 12 months post-implantation, a tool that evaluates receptive and expressive language abilities in children aged 0–7 years [85] (see Figure 3). A validated Swedish version of the comprehension section was used, with results comparable to English norms for children aged 2.5–3.4 years. Due to the narrower age range in the Swedish study, we used validated English data for comparisons. RDLS-III scores 12 months post implant were available for 43 participants (see Figure 3). A Spearmans rank correlation was computed (n =42, excluding one participant who was younger than the lowest possible RDLS-III score). No correlation was found between chronological age and RDLS-III age equivalent score (r = .214, p = .173) or between age at 1st CI and RDLS-III age equivalent score (r = .238, p = .128). However, a positive correlation was found between age at 1st CI and the differences between age and RDLS-III age equivalent score (mean = 6; range = -9.6 to 19.4) (r = .851 p <.001). This suggests that in our cohort at 12 months post implantation, a lower age at 1st CI was associated with test performance closer to age-expected levels.
Note: RDLS-III= Reynell Developmental Language Scales III, * <21 months (1:9 years) is the lowest possible score of RDLS-III, 20 months was used for this score.
4. Discussion
The main motivation for conducting the inter-professional TAYACI study is the limited in-depth knowledge in international literature regarding long-term effects of age at cochlear implantation in deaf adolescents and young adults, who were implanted in early childhood, especially outside Anglo-Saxon areas and countries like the US and Australia. This study examines specific aspects, including executive functioning, linguistic abilities including metaphor comprehension, hearing and balance outcomes, self-perceived HRQoL, mental health and self-efficacy among individuals with CIs from different parts of the country. Notably, 51% of all eligible CI users (n=109) consented to participate, and this group did not differ in outcomes compared to those who declined or did not respond to the invitation.
The early language understanding of the study cohort (see Figure 3 for RDLS-III scores at one year post 1st CI) seems to align with the results of previous studies [1,9,62] indicating that early age at implantation is beneficial for initial linguistic development. We believe that our study protocol can contribute with new knowledge regarding if this relationship between linguistic development and age at implantation continues to be present as the individuals growing up with CI enter adulthood. The multidisciplinary approach also offers the possibility to study a multitude of other factors that may contribute to linguistic development, beyond age at implantation.
The outcomes of this project will not only provide new insights into the long-term effects of age at 1st CI but also shed light on the own experiences and perspectives of young people who have grown up with CI, through a combination of collecting quantitative and qualitative data. There is also potential for conducting interdisciplinary data analyses on topics such as executive functioning, etiology, mental health, HRQoL and listening in noise among individuals with CI who received CI early in life. Such analyses may enhance our current understanding of reciprocal effects and reveal subgroup differences within the cohort, and contribute with new knowledge that may expalin some of the yet unknown variability in individuals with CI.
One limitation of the TAYACI study is that it is not a prospective longitudinal design, and its participants are not fully representative of the broader population of adolescents who use CIs. This is evident in factors such as limited diversity in socio-economic status (e.g., parental education levels) and the low participation of individuals from multilingual and multicultural backgrounds. Additionally, the study excludes data from individuals with severe and multiple disabilities who presumably were unable to complete the tests used in the Sub-Studies. However, the study includes participants from different regions of the country, ensuring broad geographical representation, as well as individuals with additional diagnoses who were able to complete the assessments and questionnaires. Overall, the cohort captures some characteristics commonly observed in the broader population of individuals with pre-lingual SNHL or deafness who use CI.
The current cohort reflects characteristics commonly observed in the broader population of individuals with pre-lingual SNHL or deafness who use CIs. Another limitation is the lack of comprehensive hearing background data in the medical records, particularly regarding age at diagnosis, which was only available for 27 participants (54%).
5. Conclusions
Early age at 1st CI influence early language outcome after one year with CI. The anticipated outcomes of this multidisciplinary study program include an improved understanding of the long-term impacts of early CI in a cohort of young people who were implanted before the age of 30 months. This includes new insights into cognition, linguistic abilities, hearing, vestibular function, etiological factors, mental health, and HRQoL. Furthermore, the TAYACI study will gain insight into the participating adolescent CI users´ own experiences of living with CI. Importantly, the findings will help identify clinical parameters that can be tailored to maximize benefits for individual CI users, offering critical decision support for clinicians, CI users, and their families in optimizing outcomes.
Supplementary Materials
The following supporting information can be downloaded at the website of this paper posted on Preprints.org, Description of specific materials used in Sub-Study I-V and references, S1.
Author Contributions
Conceptualization, U.L, E.K, F.A., L.V; methodology, U.L, M.D.S., A.P., F.A., M.E., L.V., N.K., S.G., E.K..; software, U.L., M.D.S., F.A; formal analysis, U.L., M.D.S., F.A., M.E.; investigation, M.D.S., A.P, F.A., M.E., N.K., S.G, E.K., L.V.; resources, U.L., E.K., F.A., L.V.; data curation, U.L., M.D.S., A.P., F.A.; writing—original draft preparation, U.L..; writing—review and editing, M.D.S., A.P, F.A., M.E., L.V., N.K., S.G, E.K.; visualization, U.L., M.D.S., F.A.; supervision, U.L., E.K., L.V.; project administration, U.L., E.K., M.D.S, F.A., A.P., L.V.; funding acquisition, U.L., E.K., F.A., L.V. All authors have read and agreed to the published version of the manuscript.
Funding
The project has been funded by Hörselforskningsfonden, the Foundation for the Promotion and Development of Clinical Research at Karolinska Institute, and Stiftelsen Tysta skolan.
Institutional Review Board Statement
The study was approved by the Regional Ethical Review Board in Umeå (Dnr: 2021-04345, date: 21st December 2021).
Informed Consent Statement
Written informed consent was obtained from all participants.
Data Availability Statement
The dataset presented in this article is not readily available due to participants’ lack of consent for its dissemination.
Acknowledgments
The authors would like to express their gratitude to the team members at the Hearing Implant Center at Karolinska University Hospital for their invaluable contributions to the data collection process. We also extend our thanks to the Scientific Center for Advanced Pediatric Audiology (SCAPA) at Karolinska Institute and the Foundation for the Promotion and Development of Clinical Research at Karolinska Institute. Additionally, UL, AP and M.D.S. would like to thank Bergmangårdarna for the opportunity to spend time at Dämba for analyses and writing. Our sincere appreciation goes to the adolescents with cochlear implants and their families for their participation.
Conflicts of Interest
The authors declare no conflicts of interest. The funders had no role in the design of the study; in the collection, analyses, or interpretation of data; in the writing of the manuscript; or in the decision to publish the results.
References
- Dettman SJ, Dowell RC, Choo D, Arnott W, Abrahams Y, Davis A, et al. Long-term Communication Outcomes for Children Receiving Cochlear Implants Younger Than 12 Months: A Multicenter Study. Otology & Neurotology 2016;37:e82–95. [CrossRef]
- Geers AE, Strube MJ, Tobey EA, Pisoni DB, Moog JS. Epilogue: Factors Contributing to Long-Term Outcomes of Cochlear Implantation in Early Childhood. Ear & Hearing 2011;32:84S-92S. [CrossRef]
- Cejas I, Barker DH, Petruzzello E, Sarangoulis CM, Quittner AL. Cochlear Implantation and Educational and Quality-of-Life Outcomes in Adolescence. JAMA Otolaryngol Head Neck Surg 2023;149:708. [CrossRef]
- Marschark M, Duchesne L, Pisoni D. Effects of Age at Cochlear Implantation on Learning and Cognition: A Critical Assessment. Am J Speech Lang Pathol 2019;28:1318–34. [CrossRef]
- Hickson, L., Wong, L. Evidence Based Practice in Audiology: Evaluating Interventions for Children and Adults with Hearing Impairment. Plural Publishing; 1st Edition.; 2012.
- Ching TYC, Dillon H, Button L, Seeto M, Van Buynder P, Marnane V, et al. Age at Intervention for Permanent Hearing Loss and 5-Year Language Outcomes. Pediatrics 2017;140:e20164274. [CrossRef]
- Asp F, Mäki-Torkko E, Karltorp E, Harder H, Hergils L, Eskilsson G, et al. Bilateral versus unilateral cochlear implants in children: Speech recognition, sound localization, and parental reports. International Journal of Audiology 2012;51:817–32. [CrossRef]
- Asp F, Mäki-Torkko E, Karltorp E, Harder H, Hergils L, Eskilsson G, et al. A longitudinal study of the bilateral benefit in children with bilateral cochlear implants. International Journal of Audiology 2015;54:77–88. [CrossRef]
- Karltorp E, Eklöf M, Östlund E, Asp F, Tideholm B, Löfkvist U. Cochlear implants before 9 months of age led to more natural spoken language development without increased surgical risks. Acta Paediatr 2020;109:332–41. [CrossRef]
- Löfkvist, U., Östlund, E., Karltorp, E., Eklöf, M. Multilingual children with cochlear implants in Sweden: a longitudinal follow-up study. (In Manuscript) n.d.
- Amundsen VV, Wie OB, Myhrum M, Bunne M. The impact of ethnicity on cochlear implantation in Norwegian children. International Journal of Pediatric Otorhinolaryngology 2017;93:30–6. [CrossRef]
- Clauss-Ehlers CS, Chiriboga DA, Hunter SJ, Roysircar G, Tummala-Narra P. APA Multicultural Guidelines executive summary: Ecological approach to context, identity, and intersectionality. American Psychologist 2019;74:232–44. [CrossRef]
- Szagun G, Stumper B. Age or Experience? The Influence of Age at Implantation and Social and Linguistic Environment on Language Development in Children With Cochlear Implants. J Speech Lang Hear Res 2012;55:1640–54. [CrossRef]
- Uhlén I, Mackey A, Rosenhall U. Prevalence of childhood hearing impairment in the County of Stockholm – a 40-year perspective from Sweden and other high-income countries. International Journal of Audiology 2020;59:866–73. [CrossRef]
- Kral A, Sharma A. Developmental neuroplasticity after cochlear implantation. Trends in Neurosciences 2012;35:111–22. [CrossRef]
- Registret för hörselnedsättning för barn https://hnsb.registercentrum.se/: Registercentrum VGR; 2023-10-29. n.d.
- De Melo ME, Soman U, Voss J, Valencia MFH, Noll D, Clark F, et al. Listening and Spoken Language Specialist Auditory–Verbal Certification: Self-Perceived Benefits and Barriers to Inform Change. Perspect ASHA SIGs 2022;7:1828–52. [CrossRef]
- Cupples L, Ching TYC, Crowe K, Seeto M, Leigh G, Street L, et al. Outcomes of 3-Year-Old Children With Hearing Loss and Different Types of Additional Disabilities. Journal of Deaf Studies and Deaf Education 2014;19:20–39. [CrossRef]
- Lieu JEC, Kenna M, Anne S, Davidson L. Hearing Loss in Children: A Review. JAMA 2020;324:2195. [CrossRef]
- Kenneson A, Cannon MJ. Review and meta-analysis of the epidemiology of congenital cytomegalovirus (CMV) infection. Rev Med Virol 2007;17:253–76. [CrossRef]
- Vaccination coverage and impact of pneumococcal vaccine in Sweden. Retrieved from. 2019.
- Sarant JZ, Blamey PJ, Dowell RC, Clark GM, Gibson WPR. Variation In Speech Perception Scores Among Children with Cochlear Implants: Ear and Hearing 2001;22:18–28. [CrossRef]
- Houston DM, Miyamoto RT. Effects of Early Auditory Experience on Word Learning and Speech Perception in Deaf Children With Cochlear Implants: Implications for Sensitive Periods of Language Development. Otology & Neurotology 2010;31:1248–53. [CrossRef]
- Dunn CC, Walker EA, Oleson J, Kenworthy M, Van Voorst T, Tomblin JB, et al. Longitudinal Speech Perception and Language Performance in Pediatric Cochlear Implant Users: The Effect of Age at Implantation. Ear & Hearing 2014;35:148–60. [CrossRef]
- Misurelli SM, Litovsky RY. Spatial release from masking in children with normal hearing and with bilateral cochlear implants: Effect of interferer asymmetry. The Journal of the Acoustical Society of America 2012;132:380–91. [CrossRef]
- Misurelli SM, Litovsky RY. Spatial release from masking in children with bilateral cochlear implants and with normal hearing: Effect of target-interferer similarity. The Journal of the Acoustical Society of America 2015;138:319–31. [CrossRef]
- Lovett RES, Kitterick PT, Hewitt CE, Summerfield AQ. Bilateral or unilateral cochlear implantation for deaf children: an observational study. Archives of Disease in Childhood 2010;95:107–12. [CrossRef]
- Asp F, Eskilsson G, Berninger E. Horizontal Sound Localization in Children With Bilateral Cochlear Implants: Effects of Auditory Experience and Age at Implantation. Otology & Neurotology 2011;32:558–64. [CrossRef]
- Killan C, Scally A, Killan E, Totten C, Raine C. Factors Affecting Sound-Source Localization in Children With Simultaneous or Sequential Bilateral Cochlear Implants. Ear & Hearing 2019;40:870–7. [CrossRef]
- Verbecque E, Marijnissen T, De Belder N, Van Rompaey V, Boudewyns A, Van De Heyning P, et al. Vestibular (dys)function in children with sensorineural hearing loss: a systematic review. International Journal of Audiology 2017;56:361–81. [CrossRef]
- Jacot E, Van Den Abbeele T, Debre HR, Wiener-Vacher SR. Vestibular impairments pre- and post-cochlear implant in children. International Journal of Pediatric Otorhinolaryngology 2009;73:209–17. [CrossRef]
- Wu Q, Zhang Q, Xiao Q, Zhang Y, Chen Z, Liu S, et al. Vestibular dysfunction in pediatric patients with cochlear implantation: A systematic review and meta-analysis. Front Neurol 2022;13:996580. [CrossRef]
- Kaga K, Suzuki J, Marsh RR, Tanaka Y. INFLUENCE OF LABYRINTHINE HYPOACTIVITY ON GROSS MOTOR DEVELOPMENT OF INFANTS. Annals of the New York Academy of Sciences 1981;374:412–20. [CrossRef]
- Cushing SL, Papsin BC, Rutka JA, James AL, Gordon KA. Evidence of Vestibular and Balance Dysfunction in Children With Profound Sensorineural Hearing Loss Using Cochlear Implants. The Laryngoscope 2008;118:1814–23. [CrossRef]
- Wolter NE, Gordon KA, Campos J, Vilchez Madrigal LD, Papsin BC, Cushing SL. Impact of the sensory environment on balance in children with bilateral cochleovestibular loss. Hearing Research 2021;400:108134. [CrossRef]
- Braswell J, Rine RM. Evidence that vestibular hypofunction affects reading acuity in children. International Journal of Pediatric Otorhinolaryngology 2006;70:1957–65. [CrossRef]
- Wolter NE, Gordon KA, Papsin BC, Cushing SL. Vestibular and Balance Impairment Contributes to Cochlear Implant Failure in Children. Otology & Neurotology 2015;36:1029–34. [CrossRef]
- Van Hecke R, Danneels M, Deconinck FJA, Dhooge I, Leyssens L, Van Acker E, et al. A cross-sectional study on the neurocognitive outcomes in vestibular impaired school-aged children: are they at higher risk for cognitive deficits? J Neurol 2023;270:4326–41. [CrossRef]
- Cushing SL, Papsin BC, Rutka JA, James AL, Blaser SL, Gordon KA. Vestibular End-Organ and Balance Deficits After Meningitis and Cochlear Implantation in Children Correlate Poorly With Functional Outcome. Otology & Neurotology 2009;30:488–95. [CrossRef]
- Suarez H, Ferreira E, Arocena S, Garcia Pintos B, Quinteros M, Suarez S, et al. Motor and cognitive performances in pre-lingual cochlear implant adolescents, related with vestibular function and auditory input. Acta Oto-Laryngologica 2019;139:367–72. [CrossRef]
- Kaga K, Shinjo Y, Jin Y, Takegoshi H. Vestibular failure in children with congenital deafness. International Journal of Audiology 2008;47:590–9. [CrossRef]
- Niparko JK. Spoken Language Development in Children Following Cochlear Implantation. JAMA 2010;303:1498. [CrossRef]
- Vlastarakos PV, Proikas K, Papacharalampous G, Exadaktylou I, Mochloulis G, Nikolopoulos TP. Cochlear implantation under the first year of age—The outcomes. A critical systematic review and meta-analysis. International Journal of Pediatric Otorhinolaryngology 2010;74:119–26. [CrossRef]
- Gooch D, Thompson P, Nash HM, Snowling MJ, Hulme C. The development of executive function and language skills in the early school years. Child Psychology Psychiatry 2016;57:180–7. [CrossRef]
- Pérez-Pereira M, Martínez-López Z, Maneiro L. Longitudinal Relationships Between Reading Abilities, Phonological Awareness, Language Abilities and Executive Functions: Comparison of Low Risk Preterm and Full-Term Children. Front Psychol 2020;11:468. [CrossRef]
- Pisoni DB, Kronenberger WG, Roman AS, Geers AE. Measures of Digit Span and Verbal Rehearsal Speed in Deaf Children After More Than 10 Years of Cochlear Implantation. Ear & Hearing 2011;32:60S-74S. [CrossRef]
- Beer J, Kronenberger WG, Pisoni DB. Executive function in everyday life: implications for young cochlear implant users. Cochlear Implants International 2011;12:S89–91. [CrossRef]
- Nicastri M, Filipo R, Ruoppolo G, Viccaro M, Dincer H, Guerzoni L, et al. Inferences and metaphoric comprehension in unilaterally implanted children with adequate formal oral language performance. International Journal of Pediatric Otorhinolaryngology 2014;78:821–7. [CrossRef]
- Gold R, Segal O. Metaphor Comprehension by Deaf Young Adults. The Journal of Deaf Studies and Deaf Education 2017;22:316–25. [CrossRef]
- Bahrami H, Faramarzi S, Amouzadeh M. A comparative study of metaphorical expression understanding between children with cochlear implants and normal children. AVR 2018:131–6. [CrossRef]
- Punch R, Hyde M. Social Participation of Children and Adolescents With Cochlear Implants: A Qualitative Analysis of Parent, Teacher, and Child Interviews. Journal of Deaf Studies and Deaf Education 2011;16:474–93. [CrossRef]
- Wheeler A, Archbold S, Gregory S, Skipp A. Cochlear Implants: The Young People’s Perspective. Journal of Deaf Studies and Deaf Education 2007;12:303–16. [CrossRef]
- Watson V, Verschuur C, Lathlean J. Exploring the experiences of teenagers with cochlear implants. Cochlear Implants International 2016;17:293–301. [CrossRef]
- Avenevoli S. Prevalence, Persistence, and Sociodemographic Correlates of DSM-IV Disorders in the National Comorbidity Survey Replication Adolescent Supplement. Arch Gen Psychiatry 2012;69:372. [CrossRef]
- Wesselhoeft R, Sørensen MJ, Heiervang ER, Bilenberg N. Subthreshold depression in children and adolescents – a systematic review. Journal of Affective Disorders 2013;151:7–22. [CrossRef]
- Hintermair Manfred. Prevalence of Socioemotional Problems in Deaf and Hard of Hearing Children in Germany. American Annals of the Deaf 2007;152:320–30. [CrossRef]
- Theunissen SCPM, Rieffe C, Kouwenberg M, Soede W, Briaire JJ, Frijns JHM. Depression in hearing-impaired children. International Journal of Pediatric Otorhinolaryngology 2011;75:1313–7. [CrossRef]
- Bandura A, Pastorelli C, Barbaranelli C, Caprara GV. Self-efficacy pathways to childhood depression. Journal of Personality and Social Psychology 1999;76:258–69. [CrossRef]
- Ambrose SE, Appenzeller M, Mai A, DesJardin JL. Beliefs and Self-Efficacy of Parents of Young Children with Hearing Loss. J Early Hear Detect Interv 2020;5:73–85.
- Cejas I, Mitchell CM, Barker DH, Sarangoulis C, Eisenberg LS, Quittner AL. Parenting Stress, Self-Efficacy, and Involvement: Effects on Spoken Language Ability Three Years After Cochlear Implantation. Otology & Neurotology 2021;42:S11–8. [CrossRef]
- Ching TYC, Dillon H, Leigh G, Cupples L. Learning from the Longitudinal Outcomes of Children with Hearing Impairment (LOCHI) study: summary of 5-year findings and implications. International Journal of Audiology 2018;57:S105–11. [CrossRef]
- Cupples L, Ching TYc, Button L, Seeto M, Zhang V, Whitfield J, et al. Spoken language and everyday functioning in 5-year-old children using hearing aids or cochlear implants. International Journal of Audiology 2018;57:S55–69. [CrossRef]
- Fink NE, Wang N-Y, Visaya J, Niparko JK, Quittner A, Eisenberg LS, et al. Childhood Development after Cochlear Implantation (CDaCI) study: Design and baseline characteristics. Cochlear Implants International 2007;8:92–112. [CrossRef]
- Moeller MP, Tomblin JB. An Introduction to the Outcomes of Children with Hearing Loss Study. Ear & Hearing 2015;36:4S-13S. [CrossRef]
- Kalandadze T, Braeken J, Brynskov C, Næss K-AB. Metaphor Comprehension in Individuals with Autism Spectrum Disorder: Core Language Skills Matter. J Autism Dev Disord 2022;52:316–26. [CrossRef]
- Lidén G, Fant G. Swedish Word Material for Speech Audiometry and Articulation Tests. Acta Oto-Laryngologica 1954;43:189–204. [CrossRef]
- Berninger E, Karlsson KK. Clinical study of Widex Senso on first-time hearing aid users. Scandinavian Audiology 1999;28:117–25. [CrossRef]
- Asp F, Reinfeldt S. Effects of Simulated and Profound Unilateral Sensorineural Hearing Loss on Recognition of Speech in Competing Speech. Ear & Hearing 2020;41:411–9. [CrossRef]
- Hagerman B. Sentences for Testing Speech Intelligibility in Noise. Scandinavian Audiology 1982;11:79–87. [CrossRef]
- Asp F, Olofsson Å, Berninger E. Corneal-Reflection Eye-Tracking Technique for the Assessment of Horizontal Sound Localization Accuracy from 6 Months of Age. Ear & Hearing 2016;37:e104–18. [CrossRef]
- Denanto FM, Wales J, Tideholm B, Asp F. Differing Bilateral Benefits for Spatial Release From Masking and Sound Localization Accuracy Using Bone Conduction Devices. Ear & Hearing 2022;43:1708–20. [CrossRef]
- Peirce J, Gray JR, Simpson S, MacAskill M, Höchenberger R, Sogo H, et al. PsychoPy2: Experiments in behavior made easy. Behav Res 2019;51:195–203. [CrossRef]
- Eklöf M, Tideholm B. The choice of stimulation strategy affects the ability to detect pure tone inter-aural time differences in children with early bilateral cochlear implantation. Acta Oto-Laryngologica 2018;138:554–61. [CrossRef]
- Stadler S, Leijon A. Prediction of Speech Recognition in Cochlear Implant Users by Adapting Auditory Models to Psychophysical Data. EURASIP J Adv Signal Process 2009;2009:175243. [CrossRef]
- McGarvie LA, MacDougall HG, Halmagyi GM, Burgess AM, Weber KP, Curthoys IS. The Video Head Impulse Test (vHIT) of Semicircular Canal Function – Age-Dependent Normative Values of VOR Gain in Healthy Subjects. Front Neurol 2015;6. [CrossRef]
- Rosengren SM, Colebatch JG, Young AS, Govender S, Welgampola MS. Vestibular evoked myogenic potentials in practice: Methods, pitfalls and clinical applications. Clinical Neurophysiology Practice 2019;4:47–68. [CrossRef]
- Dewar R, Claus AP, Tucker K, Ware R, Johnston LM. Reproducibility of the Balance Evaluation Systems Test (BESTest) and the Mini-BESTest in school-aged children. Gait & Posture 2017;55:68–74. [CrossRef]
- Kollén L, Bjerlemo B, Fagevik Olsén M, Möller C. Static and dynamic balance and well-being after acute unilateral vestibular loss. Audiological Medicine 2008;6:265–70. [CrossRef]
- Saltin B, Grimby G. Physiological Analysis of Middle-Aged and Old Former Athletes: Comparison with Still Active Athletes of the Same Ages. Circulation 1968;38:1104–15. [CrossRef]
- Liu X, Yu S, Zang X, Yu Q, Yang L. Discrimination of vestibular function based on inertial sensors. Computer Methods and Programs in Biomedicine 2022;214:106554. [CrossRef]
- Elo S, Kyngäs H. The qualitative content analysis process. J Adv Nurs 2008;62:107–15. [CrossRef]
- Dunn, L.M., & Dunn, D.M. Peabody Picture Vocabulary Test (3rd ed.). American Guidance Service,; 1997.
- Dunn, L.M., & Dunn, D.M. Peabody Picture Vocabulary Test, Fourth Edition. Peabody Picture Vocabulary Test, Fourth Edition. Circle Pines, MN: American Guidance Service.; 2007.
- Statistikmyndigheten. Utbildningsnivån i Sverige. 2024.
- Edwards S, Garman M, Hughes A, Letts C, Sinka I. Assessing the comprehension and production of language in young children: an account of the Reynell Developmental Language Scales III. Intl J Lang & Comm Disor 1999;34:151–71. [CrossRef]
Figure 1.
Flowchart illustrating the study inclusion process.
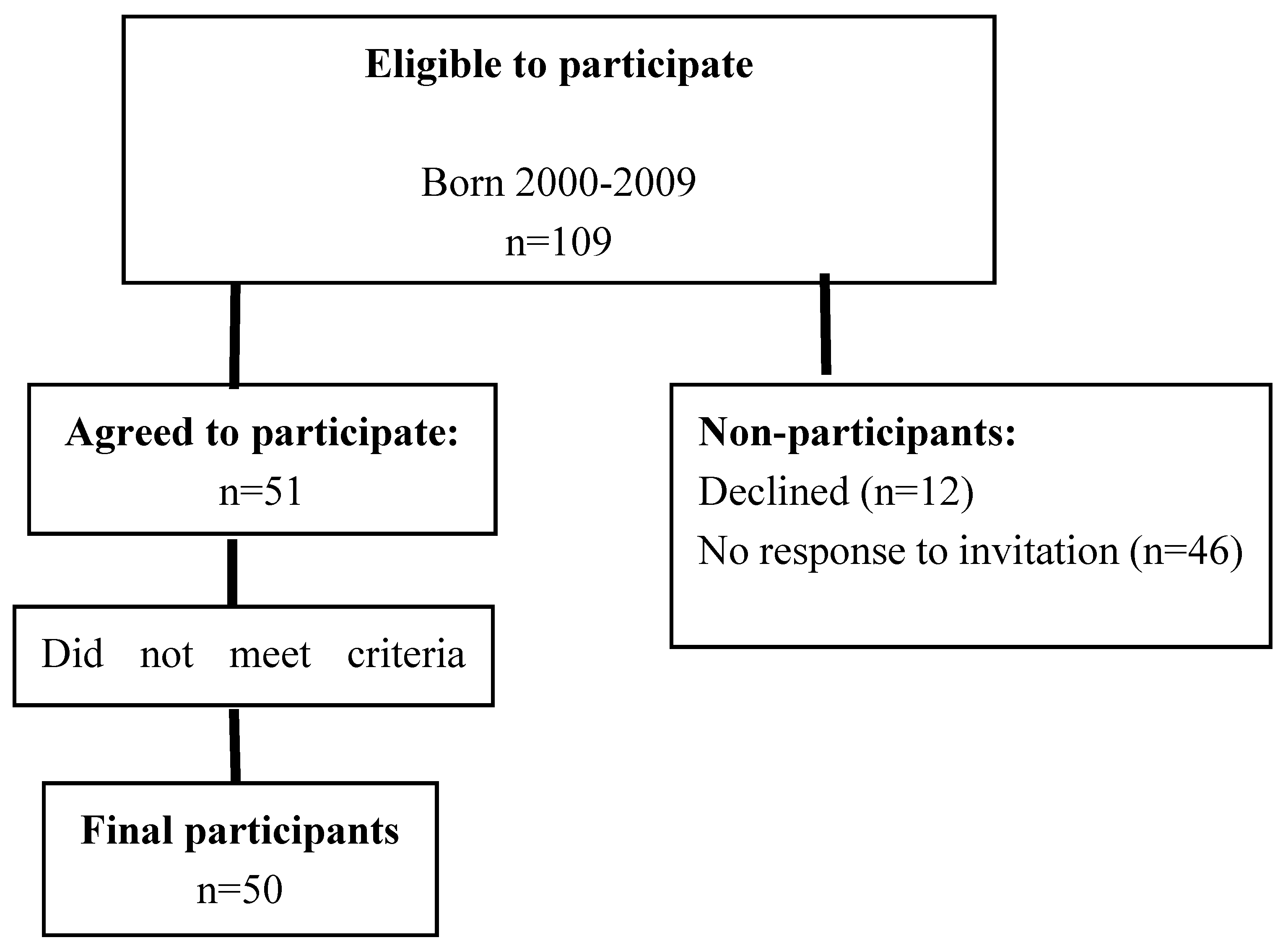
Figure 2.
Comparison of receptive vocabulary outcomes at approximately 10 years of age and age at implantation between participants and non-participants.
Figure 2.
Comparison of receptive vocabulary outcomes at approximately 10 years of age and age at implantation between participants and non-participants.
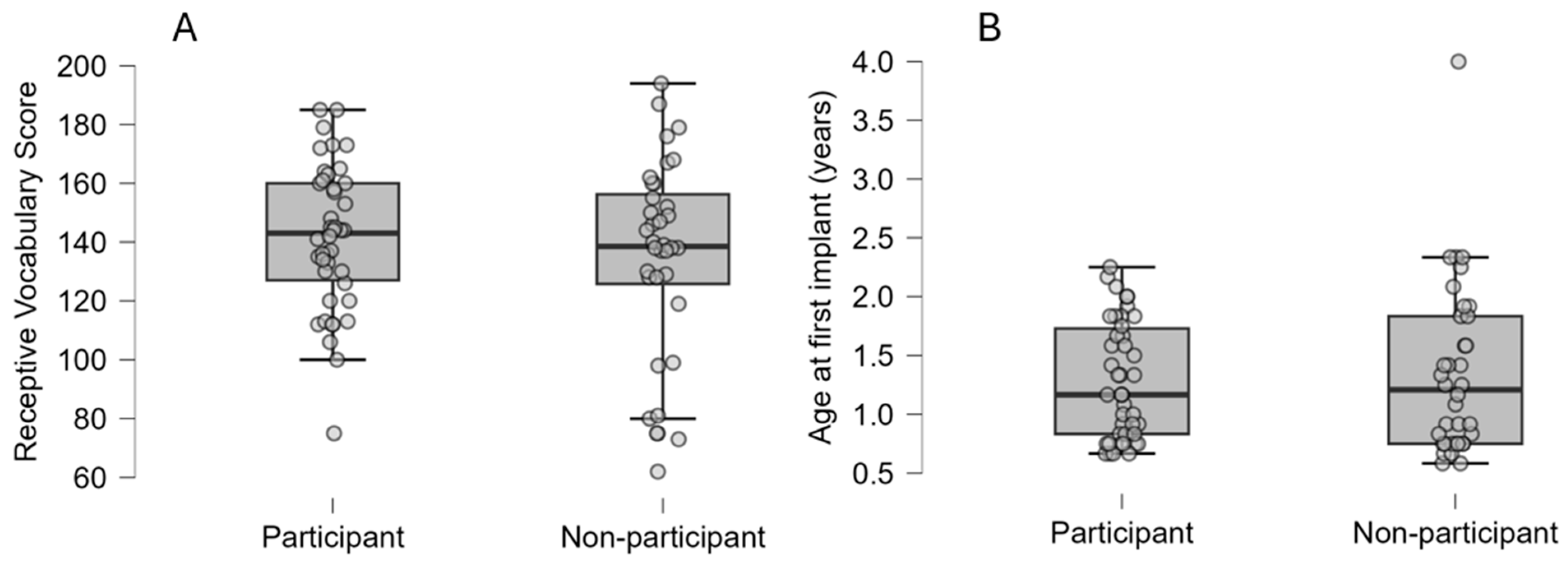
Figure 3.
Language understanding after one year with 1st CI. RDLS-III age equivalent comprehension scores (mean = 22.9 months, range = 20 – 34 months*) at one year post 1st CI (n = 43, mean age = 28.9 months, range = 19.9 - 43.4 months, mean age at 1st CI = 15.8 months, range = 7.3 - 29.3 months). Five groups are created based on age at 1st CI; CI <9 months (n = 7 , mean age = 21.3 months, mean age at 1st CI = 8.3 months), CI 9-12 months (n = 9, mean age = 23.8 months, mean age at 1st CI = 10.7 months), CI 12-18 months (n = 12, mean age = 27.9 months , mean age at 1st CI = 14.9 months), CI 18-24 months (n = 9, mean age = 34.3 months, mean age at 1st CI = 21 months), and CI >24 months (n = 6, mean age =39.2 months, mean age at 1st CI = 26 months). Dotted line illustrates expected score for age, scores above the line are higher than expected and scores below the line are lower than expected.
Figure 3.
Language understanding after one year with 1st CI. RDLS-III age equivalent comprehension scores (mean = 22.9 months, range = 20 – 34 months*) at one year post 1st CI (n = 43, mean age = 28.9 months, range = 19.9 - 43.4 months, mean age at 1st CI = 15.8 months, range = 7.3 - 29.3 months). Five groups are created based on age at 1st CI; CI <9 months (n = 7 , mean age = 21.3 months, mean age at 1st CI = 8.3 months), CI 9-12 months (n = 9, mean age = 23.8 months, mean age at 1st CI = 10.7 months), CI 12-18 months (n = 12, mean age = 27.9 months , mean age at 1st CI = 14.9 months), CI 18-24 months (n = 9, mean age = 34.3 months, mean age at 1st CI = 21 months), and CI >24 months (n = 6, mean age =39.2 months, mean age at 1st CI = 26 months). Dotted line illustrates expected score for age, scores above the line are higher than expected and scores below the line are lower than expected.
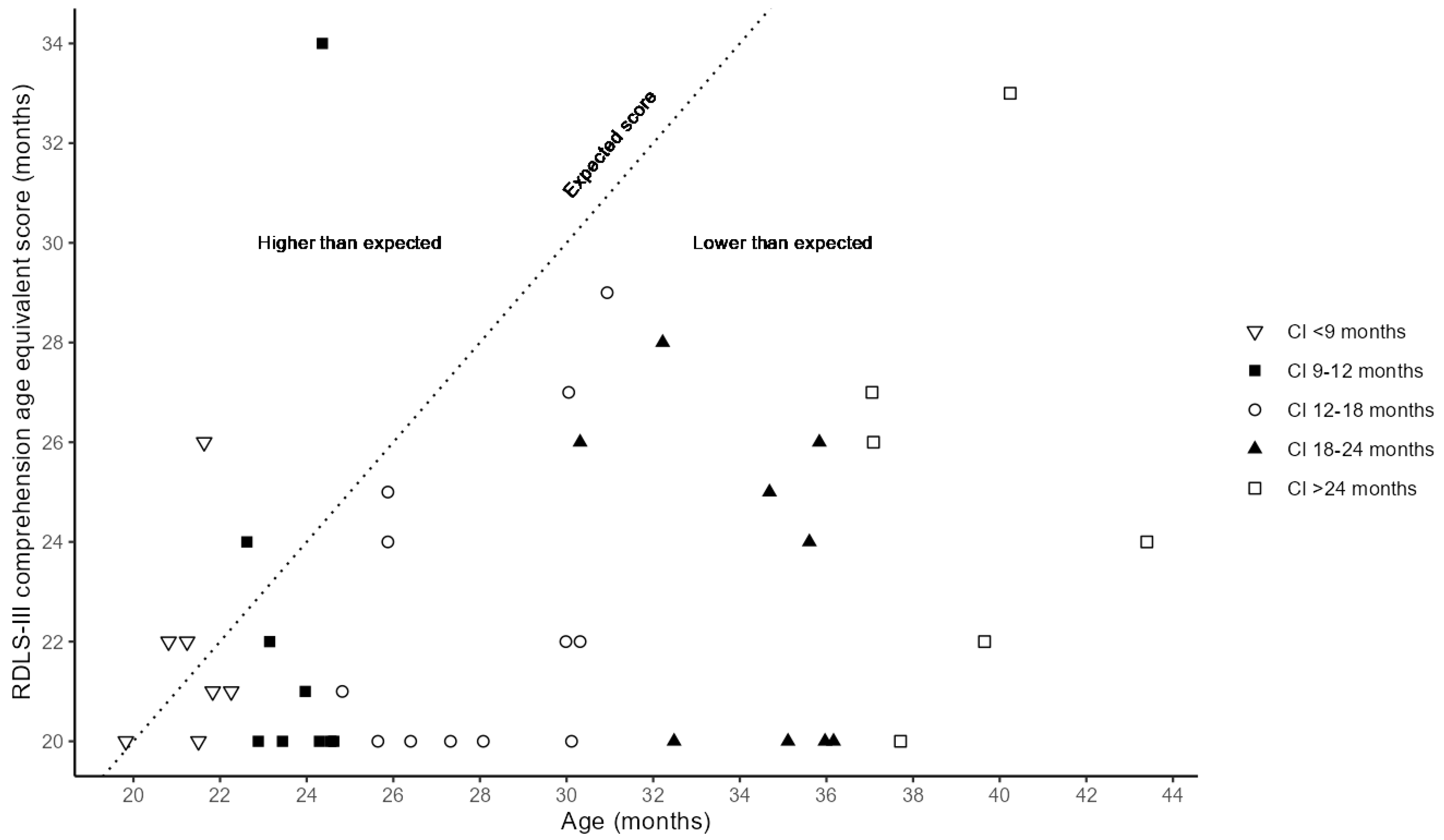

Table 1.
Background information of study participants with cochlear implants (n=50).
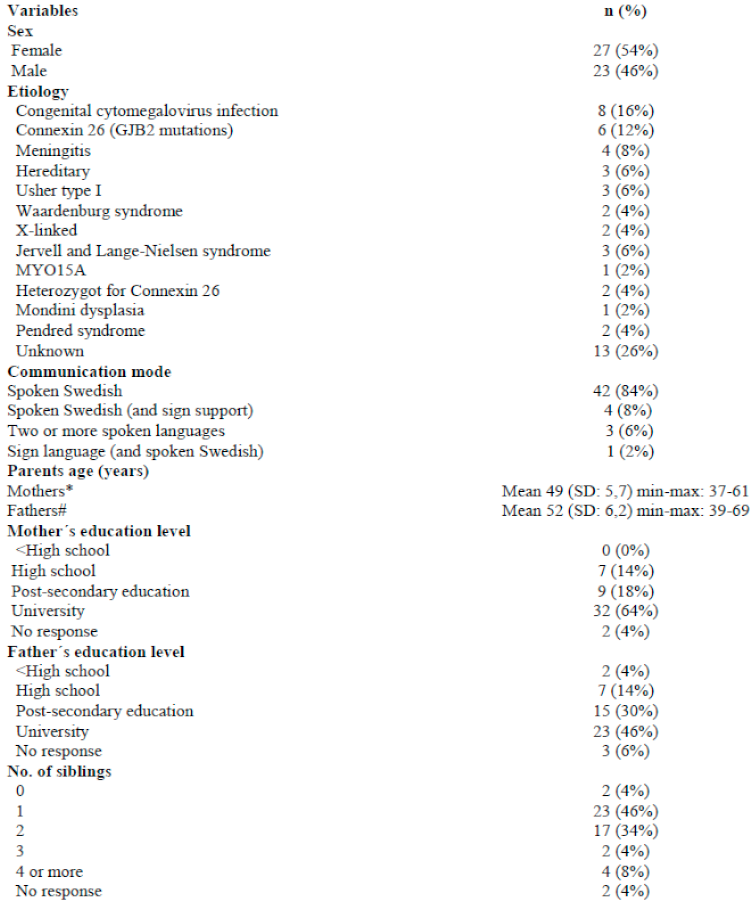 |
Notes: *missing data= n=3; # missing data= n=5.
Table 2.
Hearing diagnosis, and intervention characteristics (n=50).
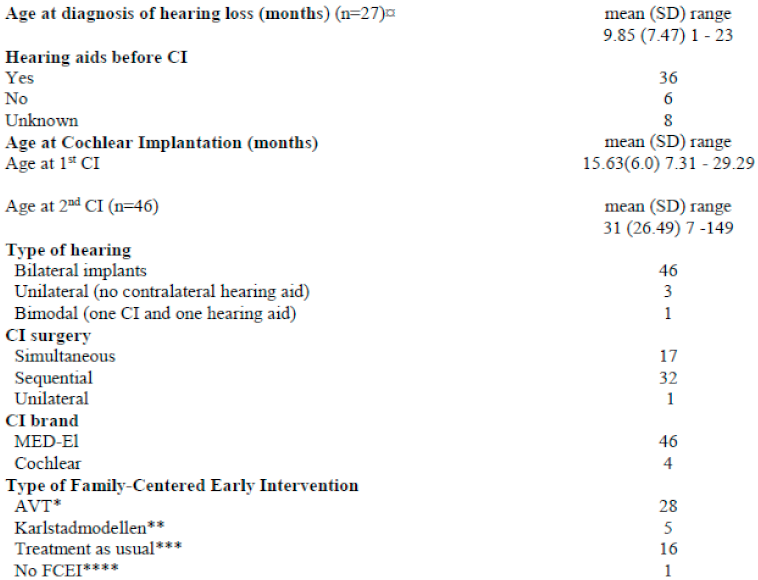 |
Notes: ¤ missing data ( n=23); *Auditory Verbal Therapy (AVT) provided at least twice per month over the course of one year by a speech-language pathologist or a teacher of the deaf trained in AVT; **Structured intervention approach focusing on the network around the child (e.g. for parents and other important caregivers like pre-school teachers) with meetings once a month to evaluate common set goals *** Unspecified Family-Centered Early Intervention (FCEI) provided on an irregular basis by a teacher of the deaf or a speech-language pathologist, ****No specific support offered for speech and language development.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



