Submitted:
09 December 2024
Posted:
11 December 2024
You are already at the latest version
Abstract
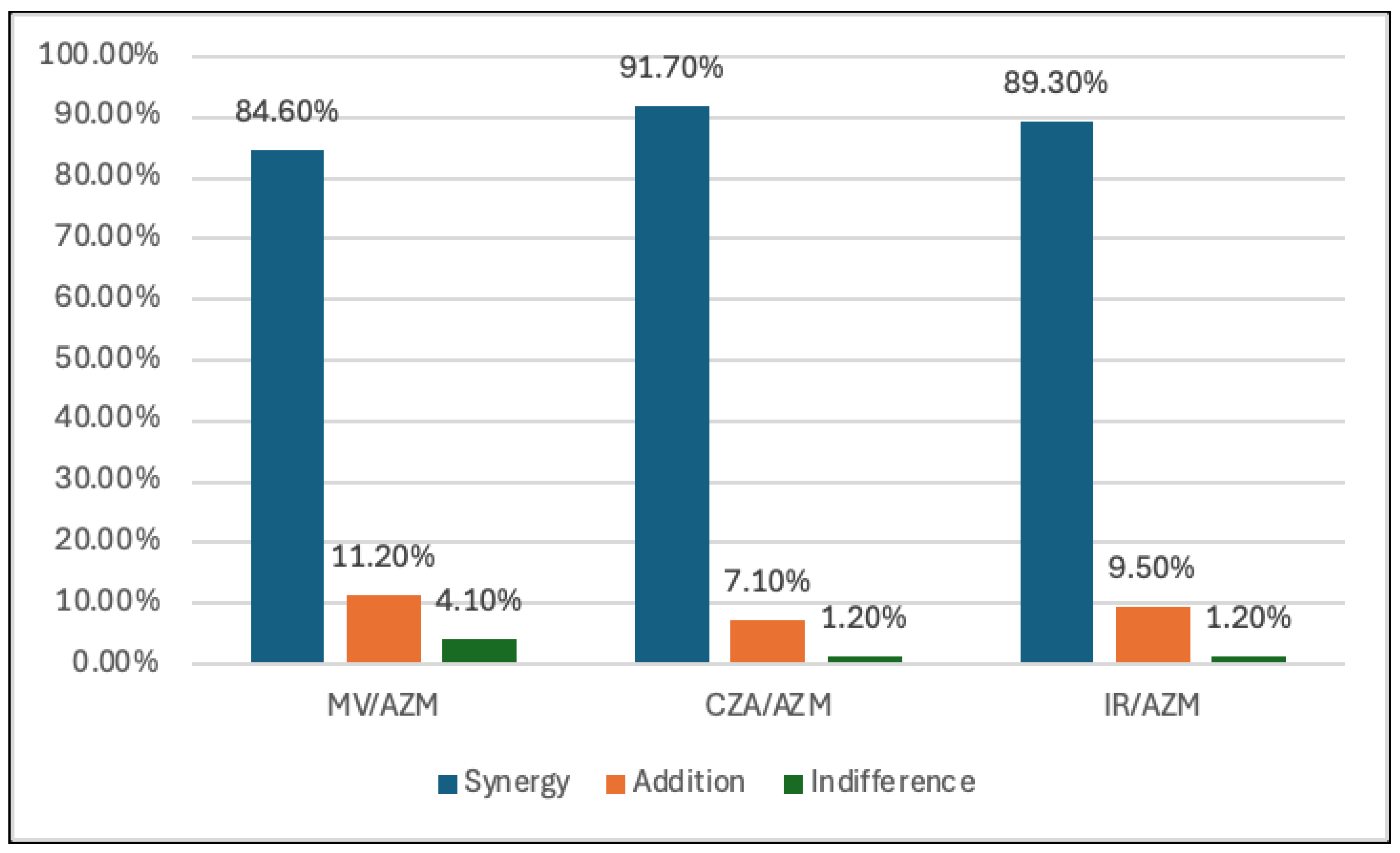
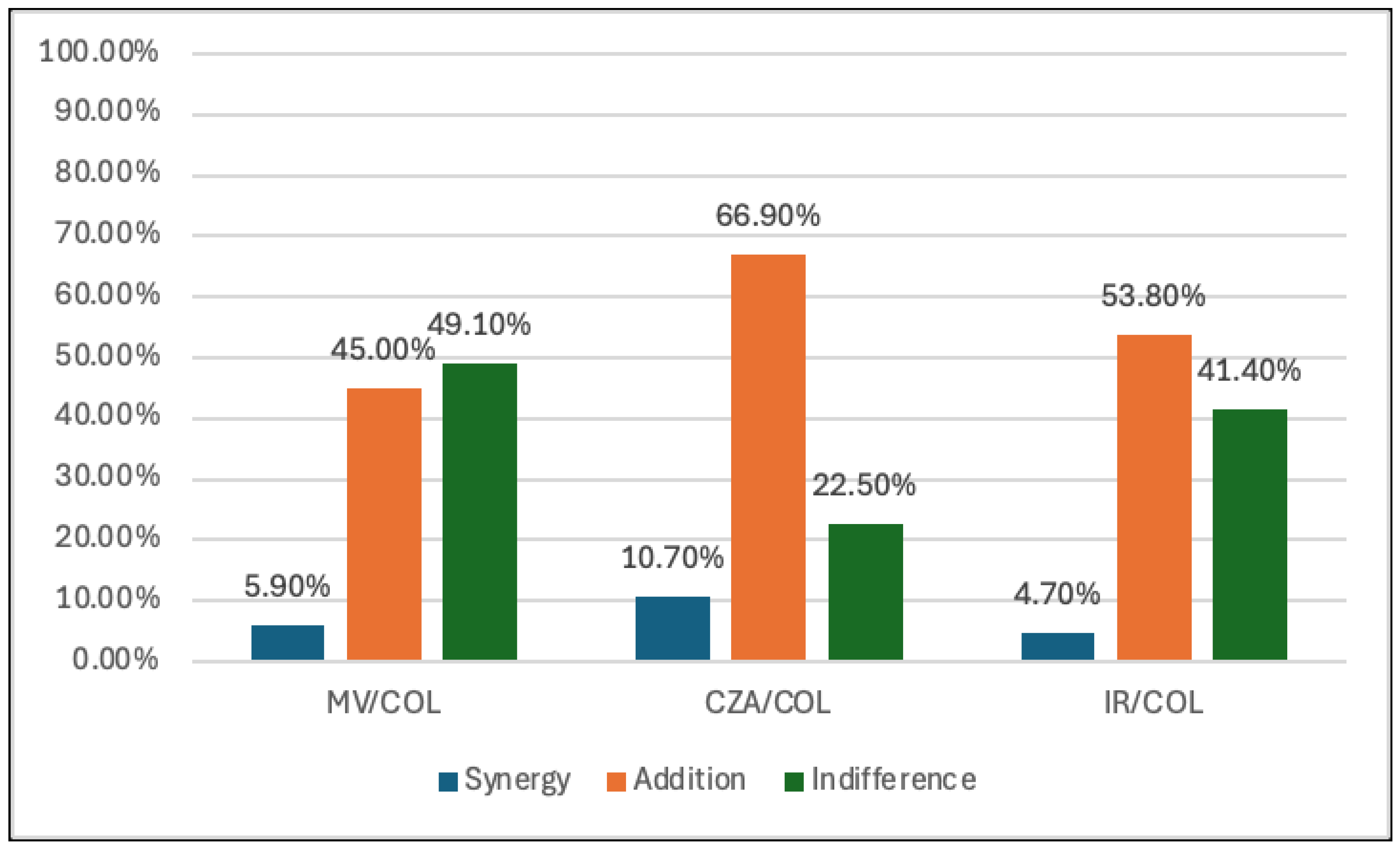
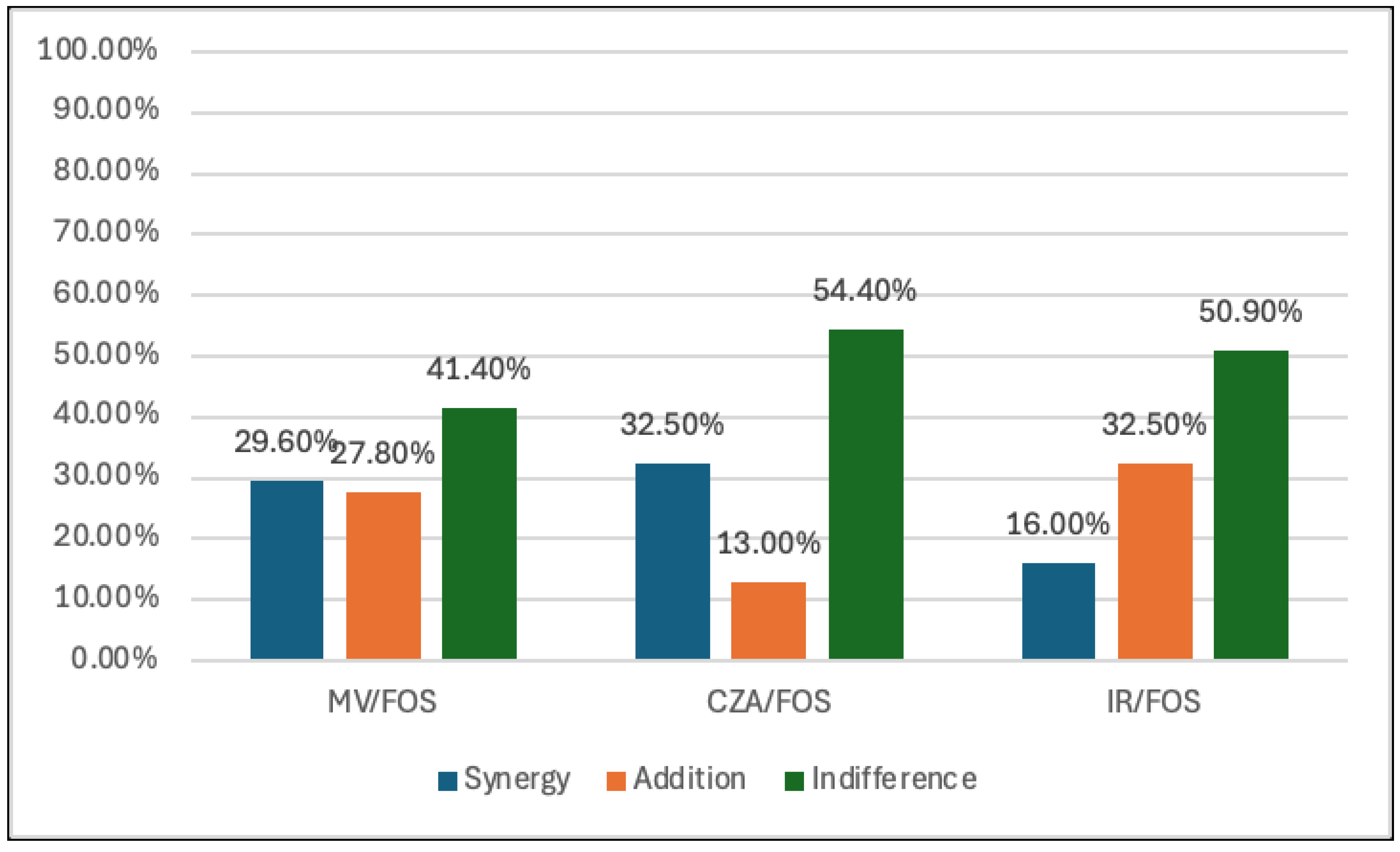
Τhe objective of this study was to assess the in vitro synergy between the new antibacterial agents CZA, M/V and I/R combined with aztreonam (AZM), colistin (COL) and fosfomycin (FOS) against MBL producing Klebsiella pneumoniae strains. This was done to identify the most effective combination regimen that could offer alternative treatment options for infections caused by MBL carbapenemase-producing Klebsiella pneumoniae.A total of 169 MBL-producing Klebsiella pneumoniae single clinical isolates (89 NDM, 66 NDM+KPC and 14 VIM) were included in the study, collected between 1 March 2023 and 30 September 2024. Of these, 86 were isolated from urine, 45 from blood, 27 from wound cultures and 11 from bronchoalveolar secretions. the strongest synergistic effects were observed with the combination of AZM plus CZA, MV, and IR, followed by combinations of FOS plus CZA, MV, and IR, suggesting promising therapeutic options for MBL-producing CRKP infections. Additionally, COL-based combinations with CZA, MV, and IR provided a better additive effect, emphasizing the need for tailored therapeutic strategies.
Keywords:
1. Introduction
2. Materials-methods:
3. Statistical Analysis
4. Results
5. Discussion
5.1. Aztreonam and Combinations
5.2. Fosfomycin and Combinations
5.3. Colistin and Combinations
6. Conclusions
References
- Aljeldah, M.M. Antimicrobial Resistance and Its Spread Is a Global Threat. Antibiotics 2022, 11, 1082. [Google Scholar] [CrossRef] [PubMed]
- Iftikhar, Qayum. Top ten global health threats for 2019: the WHO list. JRMI.
- Exner, M.; Bhattacharya, S.; Christiansen, B.; et al. Antibiotic resistance: what is so special about multidrug-resistant gram-negative bacteria? GMS Hyg Infect.Control. 2017, 12, 1–5. [Google Scholar]
- Algammal, A.; Hetta, H.F.; Mabrok, M.; Behzadi, P. Editorial: Emerging multidrug-resistant bacterial pathogens “‘superbugs’”: A rising public health threat. Front. Microbiol. 2023, 14, 1135614. [Google Scholar] [CrossRef] [PubMed]
- European Centre for Disease Prevention and Control. Carbapenem-resistant Enterobacteriaceae,secondupdate–26September2019 https://www.ecdc.europa.eu/en/publications-data/carbapenem-resistant-enterobacteriaceae-second-update.
- European Centre for Disease Prevention and Control 2023. Surveillance Atlas of Infectious Diseases. []. Available online: https://atlas.ecdc.europa.eu/public/index.aspx?Dataset=27&HealthTopic=4. (accessed on 10 November 2024).
- Hammoudi Halat, D.; Ayoub Moubareck, C. The Current Burden of Carbapenemases: Review of Significant Properties and Dissemination among Gram-Negative Bacteria. Antibiotics (Basel). 2020, 9, 186. [Google Scholar] [CrossRef]
- Bush, K.; Bradford, P.A. Epidemiology of β-lactamase-producing pathogens. Clin. Microbiol. Rev. 2020, 33, e00047–19. [Google Scholar] [CrossRef]
- Bakthavatchalam, YD.; Shankar, A. ; DPM, Sethuvel.; Asokan, K.; Kanthan, K.; Veeraraghavan, B. Synergistic activity of fosfomycin–meropenem and fosfomycin–colistin against carbapenem resistant Klebsiella pneumoniae: an in vitro evidence. Future Sci, 2020; 6, 461–468. [Google Scholar]
- Giacobbe, D. R.; Del Bono, V.; Trecarichi, E. M.; De Rosa, F. G.; Giannella, M.; Bassetti, M.; et al. Risk factors for bloodstream infections due to colistin-resistant KPC-producing Klebsiella pneumoniae: results from a multicenter case-control-control study. Clin. Microbiol. Infect. 2015; 21, 1106, e1–1108.e1. [Google Scholar]
- Doi, Y. Treatment options for carbapenem-resistant gram-negative bacterial infections. Clin Infect Dis. 2019, 69, S565–S575. [Google Scholar] [CrossRef]
- Shields, RK.; Nguyen, MH.; Chen, L.; Press, EG.; Potoski, BA.; Marini, RV.; et al. Ceftazidime-Avibactam Is Superior to Other Treatment Regimens against Carbapenem-Resistant Klebsiella pneumoniae Bacteremia. Antimicrob Agents Chemother. 2017, 61. [Google Scholar] [CrossRef]
- Marino, A.; Campanella, E.; Stracquadanio, S.; Calvo, M.; Migliorisi, G.; Nicolosi, A.; Cosentino, F.; Marletta, S.; Spampinato, S.; Prestifilippo, P.; et al. et al. Ceftazidime/Avibactam and Meropenem/Vaborbactam for the Management of Enterobacterales Infections: A Narrative Review, Clinical Considerations, and Expert Opinion. Antibiotics (Basel). 2023, 12, 1521. [Google Scholar]
- Biagi, M.; Lee, M.; Wu, T.; Shajee, A.; Patel, S.; Deshpande, L. M.; Mendes, R. E.; & Wenzler, E.; Wenzler, E. Aztreonam in combination with imipenem-relebactam against clinical and isogenic strains of serine and metallo-β-lactamase-producing enterobacterales. Diagnostic Microbiology and Infectious Disease. 2022, 103, 115674. [Google Scholar] [CrossRef]
- Bush, K.; Bradford, P.A. B-lactams and B-lactamase inhibitors: An overview. Cold Spring Harb. Perspect. Med. 2016, 6, a025247. [Google Scholar] [CrossRef]
- Petty, L.A.; Henig, O.; Patel, T.S.; et al. Overview of meropenem-vaborbactam and newer antimicrobial agents for the treatment of carbapenem-resistant Enterobacteriaceae Infect Drug Resist. 2018; 11, 1461–1472. [Google Scholar]
- Lucasti, C.; Vasile, L.; Sandesc, D.; et al. Phase 2, Dose-ranging study of relebactam with imipenem-cilastatin in subjects with complicated intra-abdominal infection. Antimicrob Agents Chemother. 2016, 60, 6234–6243. [Google Scholar] [CrossRef] [PubMed]
- Haidar, G.; Clancy, CJ.; Chen, L.; et al. Identifying spectra of activity and therapeutic niches for ceftazidime-avibactam and imipenem-relebactam against carbapenem-resistant Enterobacteriaceae. Antimicrob Agents Chemother. 2017, 61, e00642–17. [Google Scholar] [CrossRef] [PubMed]
- Vardakas, K.Z.; Athanassaki, F.; Pitiriga, V.; Falagas, M.E. Clinical relevance of in vitro synergistic activity of antibiotics formultidrug-resistant Gram-negative infections: A systematic review. J. Glob. Antimicrob. Resist. 2019, 17, 250–259. [Google Scholar] [CrossRef] [PubMed]
- Laishram, S.; Pragasam, A.K.; Bakthavatchalam, Y.D.; Veeraraghavan, B. An update on technical, interpretative and clinical relevance of antimicrobial synergy testing methodologies. Indian J. Med. Microbiol. 2017, 35, 445–468. [Google Scholar] [CrossRef]
- Pillai, S.K.; Moellering, R.C.; Eliopoulos, G.M. Antimicrobial combinations. In Antimicrobials in Laboratory Medicine, 5th ed.; Lippincott Williams & Wilkins: Philadelphia, PA, USA. 2005; pp. 365–435. [Google Scholar]
- Bai, Y.; Liu, B.; Wang, T.; Cai, Y.; Liang, B.; Wang, R.; Liu, Y.; Wang, J. In vitro activities of combinations of rifampin with other antimicrobials against multidrug-resistant Acinetobacter baumannii. Antimicrob Agents Chemother. 2015, 2015 59, 1466–1471. [Google Scholar] [CrossRef]
- Falcone, M.; Daikos, GL.; Tiseo, G.; Bassoulis, D.; Giordano, C.; Galfo, V.; Leonildi, A.; Tagliaferri, E.; Barnini, S.; Sani, S.; et al. Efficacy of Ceftazidime-avibactam Plus Aztreonam in Patients With Bloodstream Infections Caused by Metallo-β-lactamase-Producing Enterobacterales. Clin Infect Dis. 2021, 72, 1871–1878. [Google Scholar] [CrossRef]
- Brauncajs, M.; Bielec, F.; Malinowska, M.; Pastuszak-Lewandoska, D. Aztreonam Combinations with Avibactam, Relebactam, and Vaborbactam as Treatment for New Delhi Metallo-β-Lactamase-Producing Enterobacterales Infections—In Vitro Susceptibility Testing. Pharmaceuticals. 2024, 17, 383. [Google Scholar] [CrossRef]
- Biagi, M.; Wu, T.; Lee, M.; Patel, S.; Butler, D.; Wenzler, E. Searching for the Optimal Treatment for Metallo- and Serine-β-Lactamase Producing Enterobacteriaceae: Aztreonam in Combination with Ceftazidime-avibactam or Meropenem-vaborbactam. Antimicrob Agents Chemother. 2019, 63, e01426–19. [Google Scholar] [CrossRef]
- Taha, R.; Kader, O.; Shawky, S.; Rezk, S. Ceftazidime-Avibactam plus aztreonam synergistic combination tested against carbapenem-resistant Enterobacterales characterized phenotypically and genotypically: a glimmer of hope. Ann Clin Microbiol Antimicrob. 2023, 22, 26. [Google Scholar] [CrossRef]
- Wu, Y.; Yu, W.; Chu, X.; Zhang, J.; Jia, P.; Liu, X.; Zhu, Y.; Xu, Y.; Yang, Q. Effect of ceftazidime-avibactam combined with different antimicrobials against carbapenem-resistant Klebsiella pneumoniae. Microbiol Spectr. 2024, 12, e0010724. [Google Scholar] [CrossRef]
- Jayol, A.; Nordmann, P.; Poirel, L.; Dubois, V. Ceftazidime/avibactam alone or in combination with aztreonam against colistin-resistant and carbapenemase-producing Klebsiella pneumoniae. J Antimicrob Chemother. 2018, 73, 542–544. [Google Scholar] [CrossRef]
- Maraki, S.; Mavromanolaki, VE.; Moraitis, P.; Stafylaki, D.; Kasimati, A.; Magkafouraki, E.; Scoulica, E. Ceftazidime-avibactam, meropenen-vaborbactam, and imipenem-relebactam in combination with aztreonam against multidrug-resistant, metallo-β-lactamase-producing Klebsiella pneumoniae. Eur J Clin Microbiol Infect Dis. 2021, 40, 1755–1759. [Google Scholar] [CrossRef] [PubMed]
- Sy, S. K.; Beaudoin, M. E.; Zhuang, L.; Löblein, K. I.; Lux, C.; Kissel, M.; Tremmel, R.; Frank, C.; Strasser, S.; Heuberger, J. A.; et al. In vitro pharmacokinetics/ pharmacodynamics of the combination of avibactam and aztreonam against MDR organisms. Journal of Antimicrobial Chemotherapy, 2016; 71, 1866–1880. [Google Scholar]
- Li, X.; Zhang, J.; Wang, J.; Long, W.; Liang, X.; Yang, Y.; Gong, X.; Li, J.; Liu, L.; Zhang, X. Activities of aztreonam in combination with several novel β-lactam-β-lactamase inhibitor combinations against carbapenem-resistant Klebsiella pneumoniae strains coproducing KPC and NDM. Front Microbiol. 2024, 15:1210313.
- Belati, A.; Bavaro, DF.; Diella, L.; De Gennaro, N.; Di Gennaro, F.; Saracino, A. Meropenem/Vaborbactam Plus Aztreonam as a Possible Treatment Strategy for Bloodstream Infections Caused by Ceftazidime/Avibactam-Resistant Klebsiella pneumoniae: A Retrospective Case Series and Literature Review. Antibiotics (Basel). 2022, 11, 373. [Google Scholar] [CrossRef] [PubMed]
- Ojdana, D.; Gutowska, A.; Sacha, P.; Majewski, P.; Wieczorek, P.; Tryniszewska, E. Activity of Ceftazidime-Avibactam Alone and in Combination with Ertapenem, Fosfomycin, and Tigecycline Against Carbapenemase-Producing Klebsiella pneumoniae. Microb Drug Resist. 2019, 25, 1357–1364. [Google Scholar] [CrossRef] [PubMed]
- Xu, C.; Chen, T.; Zhang, S.; Zhou, C.; Liao, W.; Fang, R.; Chen, L.; Zhou, T. In vitro activity of imipenem-relebactam alone and in combination with fosfomycin against carbapenem-resistant gram-negative pathogens. Diagn Microbiol Infect Dis. 2022, 103, 115712. [Google Scholar] [CrossRef] [PubMed]
- Oliva, A.; Curtolo, A.; Volpicelli, L.; Cogliati Dezza, F.; De Angelis, M.; Cairoli, S.; Dell'Utri, D.; Goffredo, BM.; Raponi, G.; Venditti, M. Synergistic Meropenem/Vaborbactam Plus Fosfomycin Treatment of KPC Producing K. pneumoniae Septic Thrombosis Unresponsive to Ceftazidime/Avibactam: From the Bench to the Bedside. Antibiotics (Basel). 2021, 10, 781.
- Fois, M.; De Vito, A.; Cherchi, F.; Ricci, E.; Pontolillo, M.; Falasca, K.; Corti, N.; Comelli, A.; Bandera, A.; Molteni, C.; Piconi, S.; et al. Efficacy and Safety of Ceftazidime-Avibactam Alone versus Ceftazidime-Avibactam Plus Fosfomycin for the Treatment of Hospital-Acquired Pneumonia and Ventilator-Associated Pneumonia: A Multicentric Retrospective Study from the SUSANA Cohort. Antibiotics (Basel). 2024, 13, 616. [Google Scholar] [CrossRef]
- Shields, RK.; Nguyen, MH.; Hao, B.; Kline, EG.; Clancy, CJ. Colistin Does Not Potentiate Ceftazidime-Avibactam Killing of Carbapenem-Resistant Enterobacteriaceae In Vitro or Suppress Emergence of Ceftazidime-Avibactam Resistance. Antimicrob Agents Chemother. 2018, 62, e01018–18. [Google Scholar] [CrossRef]
- Wang F, Zhou Q, Yang X, Bai Y, Cui J. Evaluation of ceftazidime/avibactam alone and in combination with amikacin, colistin and tigecycline against Klebsiella pneumoniae carbapenemase-producing K. pneumoniae by in vitro time-kill experiment. PLoS One. 2021, 16, e0258426.
- Rogers, TM.; Kline, EG.; Griffith, MP.; Jones, CE.; Rubio, AM.; Squires, KM.; Shields, RK. Mutations in ompK36 differentially impact in vitro synergy of meropenem/vaborbactam and ceftazidime/avibactam in combination with other antibiotics against KPC-producing Klebsiella pneumoniae. JAC Antimicrob Resist. 2023, 5, dlad113. [Google Scholar] [CrossRef]

| MIC range (mg/L) | Resistance n/% | |
|---|---|---|
| Aztreonam | 0.125-256 | 156 (92,3%) |
| Fosfomycin | 1-256 | 144 (85,2%) |
| Colistin | 0.125-64 | 56 (33,1%) |
| Ceftazidime/Avibactam | 0.75-256 | 169 (100%) |
| Meropenem/Vaborbactam | 9-256 | 169 (100%) |
| Imipenem/Relebactam | 3-32 | 169 (100%) |
| Drug Combination | Synergy FICI |
Additivity FICI |
Indifference FICI |
Antagonism FICI |
|---|---|---|---|---|
|
Aztreonam Aztreonam+Ceftazidime/Avibactam Aztreonam+Meropenem/Vaborbactam Aztreonam+Imipenem/Relebactam |
155(91.7%) 143(84 %) 151(89.3) |
12(7.1%) 19911.2%) 16(9.5%) |
2(1.2%) 7(4.1% 2(1.2%) |
------- ------- ------- |
|
Fosfomycin Fosfomycin+Ceftazidime/Avibactam Fosfomycin+Meropenem/Vaborbactam Fosfomycin+Imipenem/Relebactam |
55(32.5%) 50(29.6%) 27(16%) |
22(13%) 47(27.8%) 55(32.5%) |
92(54.4%) 70(41.4) 86(50.9% |
------- 2(1.2%) 1(0.6%) |
|
Colistin Colistin+Ceftazidime/Avibactam Colistin+Meropenem/Vaborbactam Colistin+Imipenem/Relebactam |
18(10.7%) 10(5.9%) 8(4.7%) |
113(66.9%) 76(45%) 91(53.8%) |
38(22.5%) 83(49.1%) 70(41.4%) |
------- ------- ------- |
| Contingency tables for pairs of drugs and/or drug combinations | p | |
|---|---|---|
| 1 | Colistin vs. Fosfomycin | <0.001 |
| 2 | Colistin vs. Aztreonam | <0.001 |
| 3 | Colistin vs. Ceftazidime/Avibactam | <0.001 |
| 4 | Fosfomycin vs. Aztreonam | 0.019 |
| 5 | Fosfomycin vs. Ceftazidime/Avibactam | <0.001 |
| 6 | Aztreonam vs. Ceftazidime/Avibactam | 0.005 |
| 7 | Ceftazidime/Avibactam+Aztreonam vs. Ceftazidime/Avibactam+Colistin | <0.001 |
| 8 | Ceftazidime/Avibactam+Colistin vs. Ceftazidime/Avibactam+Fosfomycin | <0.001 |
| 9 | Ceftazidime/Avibactam+Aztreonam vs. Ceftazidime/Avibactam+Fosfomycin | <0.001 |
| 10 | Meropenem/Vaborbactam +Aztreonam vs. Meropenem/Vaborbactam +Colistin | <0.001 |
| 11 | Imipenem/Relebactam+ Aztreonam vs. Imipenem/Relebactam+Colistin | <0.001 |
| 12 | Meropenem/Vaborbactam +Colistin vs. Ceftazidime/Avibactam+Colistin | <0.001 |
| 13 | Ceftazidime/Avibactam+Colistin vs. Imipenem/Relebactam+Colistin | <0.001 |
| 14 | Ceftazidime/Avibactam+Aztreonam vs. Meropenem/Vaborbactam +Aztreonam | 0.014 |
| 15 | Imipenem/Relebactam+Colistin vs. Meropenem/Vaborbactam +Colistin | 0.072 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).



