Submitted:
09 December 2024
Posted:
10 December 2024
You are already at the latest version
Abstract
Background: Obesity is affecting 33.2% of the adult Bulgarians. Scarce information is available about the affected people’s attitudes toward their weight condition. The aim of this study was to explore the perceptions about obesity of affected adults. Methods: This was a home-based, tablet assisted, face-to-face interview. It included people aged 25-64 y/o with a BMI > 25.0 kg/m2. Results: Overall 704 respondents participated (344 overweight; 360 with obesity). >50% of them reported attempts to reduce their overweight. Only 6% in the overweight group and 16% in the obese group perceived their condition as worrisome. One third of the obese people considered their state as temporary. The alarm for being overweight / obese was the worsening overall physical condition in males, and the growing size of clothes females. A need for urgent reduction of body weight was perceived by 12% of the overweight and 40% of the obese respondents. The reasons for being overweight were rated as lack of physical activity (checked by 52%), sedentary lifestyle (51%), stress/depression (41%), excessive consummation of carbohydrates (34%), overconsump-tion generally (33%), poor quality of food products (28%). Fifty-six % of the respondents had first consulted a medical doctor about overweight. Most respondents selected diet without physical activity for weight reduction. Forty-eight percent would try drugs approved for weight reduction. Conclusion: Many people with overweight / obesity had unreal self-perception and a very low motivation for taking active measures. These discrepancies offer great opportunities for better public education and structured active strategies.
Keywords:
obesity
; interview
; perceptions
; attitudes
; discrepancies
Keywords: obesity; interview; perceptions; attitudes; discrepancies
1. Introduction
Obesity is a contemporary health epidemic whose magnitude is constantly growing. More than 1 billion people are affected worldwide and their number will on the rise in future decades [1]. More and more people are living in a better environment than that some 20-30 years ago, they are consuming more calories and moving a lot less. On the other side of the problem is the food industry which is processing more and more foods and relies mainly on inborn human instincts such as appetite, satiety and reward. The sequelae of obesity however include many unfavourable conditions and human diseases. Obesity incurs both human and economic costs to the whole society [2].
It is typical for the medical doctor’s way of thinking to consider obesity as a common disease, that could be treated by lifestyle changes and by simply prescribing drugs [3, 4]. However, the situation seems far more complex. First, the affected person should regard his/her condition as a disease, not as a minor or cosmetic problem. Second, lifestyle changes require deeply founded motivation and strong patient’s will to take place. Awareness and incentives need a lot of work on both sides – the patient’s one and the medical specialist’s one. And third, drugs used to treat obesity are still very few, with prices that are above the average of much more common medications.
Very few is known about the perceptions of people with overweight / obesity of their condition. Those perceptions are the result of personal believes and character traits, sources and magnitude of available information, family support, financial factors and many others [5-7].
Obesity is a common health condition in Bulgaria. According to the 2012 National Representative Epidemiologic Survey 33.2% of the adult Bulgarians had obesity (28.3% of females and 38.8% of males) while overweight was registered in 37.0% of the whole sample – in 32.5% of females and in 42.2% of the males [8]. Sixty-two percent of the participants had an abnormal waist circumference (63.2% of females and 61.6% of males) [9]. Almost no information is available about the affected people’s attitudes toward their personal condition, the way they gather information about it and their personal perceptions about the need for urgent action and the ways they might further proceed. The medical community is in desperate need of more detailed information about the concerns, fears and hopes of those with overweight/obesity to properly guide management and treatment decisions.
The aim of this study was to explore the perceptions of and attitudes toward obesity in Bulgarian adults with overweight or obesity.
2. Materials and Methods
2.1. Study Design and Ethical Standards
This study was a questionnaire-based survey primarily conceived as a marketing tool to explore the different segments of people with obesity. According to local regulations there is no need for ethical approval of questionnaire-based surveys. The ethical standards approved by the European Society for Opinion and Marketing Research were strictly followed. All respondents were volunteers and gave their informed consent prior to initiation of any procedures. Their personal data were properly blinded. The marketing research agency doing the field work was certified as an operator of personal data by the Bulgarian authorities.
First, a pilot (target) group completed a qualitative survey to better formulate the research questions. The interview duration was 3 hours and it covered a number of topics: free & leisure time, attitudes towards “good health” & “healthy weight losing”, sources of information related to weight loss. The results were used to structure the computer-based questionnaire for the large study group.
As a second step the actual quantitative home-based interview was completed using computerized tablets. All eligible subjects took part in this in-home, tablet assisted, face-to-face interview with a median length of ~ 25 min. They first gave their informed consent for data collection, analysis and storing. The in-home interviews were performed between Jan 20th and Feb 5th, 2022.
2.2. Participants
All participants were male & female volunteers aged 25-59 years. The following inclusion criteria were used: 1/ Age between 25 and 59 years; 2/ BMI ≥ 25.0 kg/m2; 3/ Household monthly income above the Bulgarian average [≥ 2400 BGN ≈ ≥1200 Euro for the pilot group and ≥ 3000 BGN ≈ ≥1500 Euro for the actual survey participants]. The respondents were divided in 2 cohorts based on their age: 25-39 y/o and 40-59 y/o. Their body mass index was calculated based on self-reported height and weight during the recruitment and following interview. The income criterion was introduced to select participants able to afford more expensive diets, food supplements or drugs typically used in the management of obesity.
The target (pilot) group consisted of four online group discussions, each with 6 participants - 2 participants with BMI 25-27 kg/m2 plus 4 participants with BMI >27.0 kg/m2 respectively. The home-based interview group (quantitative survey) included people aged 25-64 y/o with a ratio of ≈ 50/50 male/female, all of them with a BMI > 25.0 kg/m2. The survey covered the top 6 cities in Bulgaria (Sofia, Plovdiv, Varna, Burgas, Stara Zagora, Blagoevgrad) with a 1,3 million inhabitants (34% of the country population). 360 thousand of them (28% of the cities’ population) were registered having higher household income. 170 thousand of the latter (47% of the cities’ population with higher income) had a BMI ≥ 25,0 kg/m2 per based on previous surveys with 17% being in the BMI stratum of 25,0-29,9 kg/m2. The sample of participants was distributed on a random basis throughout six of Bulgaria's largest cities. A randomly selected street within the city, along with a randomly selected starting address, served as a nest. Interviewers systematically visited every address, engaged with a household member and ensured that they addressed the relevant sections of the questionnaire at the designated location. From the approximately 4000 addresses visited, a total of 704 effective interviews were collected.
2.3. Questionnaire
The patients’ questionnaire was specifically designed for this study. It included and introductory part with screening questions, followed by 4 sections covering all topics of interest: Awareness of the health condition, Overweight and the patient’s path, Attitudes towards losing weight & using information channels, and Additional demographic data. The questionnaire is available in Appendix 1.
2.4. Statistical Analysis
The sample size computation was based additionally on published data about the prevalence of obesity and overweight in the general Bulgarian population – status 2012 [8]. The expected representative sample size was calculated to be around 0.4% of the target population (N=700).
All analyses were performed on an IBM SPSS 19.0 for Windows platform (SPSS Corp., Chicago, IL). Descriptive statistics (means, medians, standard deviations and quartiles) and frequency analysis were performed. The different shares of patients were presented in percentages. The total sample was subdivided according to BMI (25.0–26.9; 27.0-29.9, and BMI≥30.0 kg/m2). Appropriate graphs were built. Statistical significance was set as p≤0.05.
3. Results
3.1. Demographic Profile of the Respondents
The survey achieved a sample size of N=704, distributed in two equal clusters - people with BMI 25,0-29,9 and BMI ≥ 30 kg/m2, randomly selected in each cluster. At least 50% of the participants had made attempts to reduce the overweight within the last 2-3 years.
The capital Sofia was represented by 48 % of the participants, while the second large city, Plovdiv – by 16%, and the third one, Varna – by 15%. The remaining three cities participated with 8%, 7% and 6% of the survey respondents. Table 1 summarizes the sample structure and profile in total and stratified to BMI.
3.2. Overall Health and Concomitant Diseases – the Participants’ Evaluation
The patients’ overall health evaluation was predominantly good or moderate, as shown in Figure 1.
As Figure 1 shows the overall health perception considerably worsened with BMI≥30. About 37% of all participants reported concomitant chronic illnesses, two at average. Their prevalence in decreasing order was blood pressure (66%), hypercholesterolemia (28%), osteoarthritis (27%), depressive disorders (16%), dysglycemia (14%0, heart disease (13%), type 2 diabetes (10%), sleep apnoea/snoring (8%), kidney disease (5%), liver disease (2%) and others (12%). Adults 55-64 y/o (N=154) showed both the highest rates of obesity (60% with BMI>30 kg/m2) and chronic illness (68%).
3.3. Self-Perception of Overweight / Obesity and the Urgency to Lose Weight
The attitudes of the respondents toward their problem of overweight/obesity are displayed in Figure 2.
Figure 2 underlines the fact, that 1/3 of the obese people considered their state as temporary, while the big majority – as permanent. Females and respondents 55-64 y/o were more inclined to consider their overweight as permanent, not temporary.
The alarm for being overweight / obese was the worsening overall physical condition in males, while females had noted the growing size of their clothes.
The patients’ views about their need to urgently reduce body weight is reflected in Figure 3.
3.4. Perceived Reasons for Being Overweight / Obese
The reasons for being overweight were rated by the respondents in the following order: lack of physical activity (checked by 52%), sedentary lifestyle (51%), stress/depression (41%), excessive consummation of carbohydrates (34%), overconsumption generally (33%), poor quality of food products (28%), hormonal changes (24%) and genetic predisposition (21%). Table 2 summarizes the different reported reasons for obesity / overweight by subcategories of BMI.
The interaction between obesity and chronic illnesses was perceived in both directions. Twenty-nine percent tended to explain their chronic diseases with overweight /obesity, while another large proportion shared the belief that obesity is a result of the chronic diseases.
3.5. Preferred Information Sources About Overweight / Obesity
Of note, 56% of the respondents had first consulted a medical doctor about overweight, 27% had consulted a fitness instructor and 26% had consulted a nutritionist. When asked if the medical specialist (doctor) had paid attention to their weight condition, only 32% of the total sample and 49% of the people with obesity gave a positive answer. This showed the low commitment of medical specialists to the problem of overweight / obesity.
On the other hand, only 67% of the whole study sample used different sources to get informed about weight loss. 42% approached friends and relatives to get informed about approaches toward overweight, while 26% and 25% had consulted a medical doctor or social media, respectively. A nutritionist had been approached by 13% and a gym instructor – by 8%. For the obese respondents, the medical doctor was considerably more trusted than social media, though equally used. The younger the people, the less addressing a doctor. GP is the main specialist consulted by now (in 39%), followed by the endocrinologists (29%), nutritionists (14%) and cardiologists (13%). Ten percent had consulted another specialist, mainly fitness instructors and dieticians. Once deciding to lose weight only 22% (32% of those with BMI≥30 kg/m2) had consulted a medical doctor, while 55% of the whole sample would proceed on their own. Table 3 shows a list of different medical specialists that were most trusted for weight reduction.
Only 16% reported they could rely on their families to support their efforts for weight reduction. The closest attitude of friends and family toward their personal overweight was assessed by the respondents as accepting without interfering (57%), disapproving but not commenting (19%), ready to provide any help (19%) and even making inappropriate jokes (8%). The majority of the families of obese people were ready to interfere, unlike families of people with lower BMI.
3.6. Management of Overweight / Obesity – Knowledge and Attitudes
Asked about their awareness of methods for weight reduction most respondents selected diet without physical activity (84%), followed by exercise / physical activity only (80%), OTC drugs and supplements (77%), cosmetic procedures like lifting or massage (65%), fitness / gym-based weight loss program (60%) and surgical interventions (53%). Forty-eight percent only would try drugs approved for weight loss with 31% aware of injection therapy. 61% of the obese people were currently trying to lose weight. 78% of the total sample and 82% of those with BMI≥30 kg/m2 had ever tried to lose weight. The main reasons for not trying were feeling good enough (even with excess weight) and lack of will. Figure 4 displays the preferred method for losing weight (if ever tried) as selected by the respondents. The average of 2 methods had been tried by those wishing to lose weight.
Failure to lose the needed weight resulted in a self-blame for the lack of persistence, lack of will. Not keeping the lost kg in the course of time made many to give up trying, and accepting the overweight. Keeping the lost kilos was considered a much more substantial result than primarily losing them.
The most often considered benefits of obesity drugs were safety (73%), efficacy (69%), positive impact on CV risk factors (54%). The perceived barriers included fear of weight increase following treatment discontinuation (63%), high drug prices (48%), fear of needle injections (43%) and need for long-term use (40%). This behaviour resulted in a rather low willingness for buying expensive anti-obesity drugs – overall 14% agreed to do that including 19% of those with BMI≥30 kg/m2.
4. Discussion
Our study gathered detailed information about common believes, knowledge and attitudes toward overweight / obesity in a representative sample of the urban Bulgarian population. It included a small pilot sub-study (qualitative part) and the actual quantitative part of 704 participants with BMI ≥ 25.0 kg/m2. All of them had at least high-middle income. The overall health self-evaluation of the participants was good in about half of them with a minority reporting bad health (<7% if BMI 25.0 – 29.9 kg/m2 and 16% if BMI ≥ 30 kg/m2). Around two thirds of people with obesity (67%) perceived their condition as permanent with only one third (33%) seeing urgency for losing weight. Obese respondents expressed a wish to lose a mean of 19.2 kg which seemed quite difficult to achieve. The reported family support for these efforts to lose weight was very low (16% only), although family and friends were the preferred source for gathering information about possible approaches. Help from medical doctors was sought in only 26% of cases with nutritionist followed by endocrinologists being the preferred specialists. Of note, diet and physical activity were perceived by more than 80% as the main way to fight against obesity, however most respondents chose one single method out of both and very rarely a combined approach. At least 80% of the whole study sample had ever tried to lose weight, however mostly with a partial and temporary success. The most common perceived barriers were feeling good with overweight and lack of will. In short, this study showed that most people with overweight / obesity had unreal self-perception and a very low motivation for taking any active measures. Help received from the family or medical specialists also seemed not sufficient. These discrepancies offer great opportunities for better public education and implementation of structured strategies for fighting overweight / obesity – easier access to trusted information, specialists and management opportunities.
The first barrier in obesity management might be that most patients and a substantial proportion of healthcare practitioners do not recognize high BMI as a disease requiring special attention. In the Spanish cohort of the International ACTION-IO observation study 59% of the affected people agreed that obesity is a chronic disease [10]. As an additional obstacle 80% of them assumed complete responsibility for their own weight management, coupled with a mean delay of 6 years in first discussing this particular problem with a health care provider [10]. In the US National ACTION study 65% of the respondents recognized obesity as a disease, however only 54% worried about possible repercussions of excessive weight on their health [11]. Similarly, in our study sample a majority of the participants with a BMI≥30 kg/m2 perceived their health status as good or moderate (30%, respectively 54%).
Similar perceptions and attitudes of people with overweight / obesity were revealed in the ACTION international and national studies [12-14]. A very detailed study from Lithuania showed that most participants failed to visually recognize obesity (males more often than females) and had little knowledge about diseases associated with obesity except for heart diseases and diabetes [12]. This study corroborated our finding that a relevant part of people with obesity are not perceiving a problem at all and would not see urgency to lose weight. Of note, “low metabolism” was perceived as one of the main causes for putting weight in this Lithuanian population, rated just after “eating too much” and “exercising too little”. Younger respondents (age < 45 years) were more likely to change their lifestyle. Disappointment with their current weight was identified as the driving force for implementing weight loss strategies [12].
The perceived causes for weight gain are also poorly understood both by patients and healthcare providers. A study examining the patient’s perspective reported genetic (uncontrollable) causes for obesity in 13% of the participants while the remaining 87% emphasized the importance of controllable factors (lifestyle habits and unhealthy diet) [7]. Of note, our respondents pointed at poor quality of food, irregular meals and a sedentary lifestyle as major causes for obesity.
The perceptions and expectations of people with obesity were also very well highlighted in the ACTION-IO study [13]. It summarized data from 14502 people with obesity and showed that only 68% agreed that obesity was a disease. A median of three (mean six) years were needed for the patient to seek medical consultation and the primary reason for this delay was that most of them (81%) assumed complete responsibility for losing weight. Interestingly, most of the respondents (68%) were inclined to wait for the health care professionals to address the issue of body weight. In line with our data, most respondents in the ACTION-IO study shared the view that they “ate too much” (62%) and “exercised too little” (73%). Almost two thirds of that international study population had not tried to lose weight during the last 3 years, which is in contrast with reported attempts for losing weight in more than three fourth of our study sample [13]. The ACTION-IO study came to the conclusion that several gaps in obesity care still exist together with a misalignment between perceptions and attitudes, a finding corroborated by our data.
Another study examined nutrition knowledge and attitudes and identified self-regulation as potent predictor of weight problems [6]. Again 28.1% of the participants only correctly identified the body mass index for obesity. The participants identified poor eating self-regulation as one of the strongest causes for excessive weight. Age was also a strong predictor adding 30% more overweight/obese people per decade. Of note, respondents showed the highest knowledge score on diet and diseases (80.7%) [6]. This is very similar to our data, showing diet alone as the most popular method among those who ever tried to lose weight (58% of total sample and 84% of obese people).
Another major problem lies in the fact that even if generally perceived as a disease, obesity is not commonly treated. A systematic review exploring GP’s and nurses’ perspectives on shared weight management with their patients revealed that obesity was often not a priority and other lifestyle interventions such as quitting smoking often were seen as more important [15]. The other perspective of the same problem is reflected in a systematic review of patient’s perspectives, revealing negative experiences in consultations as a major barrier in fighting excessive weight [5].
Strengths and Limitations
Our study has some limitations. First, it included people from urban areas only with a moderate to high income. Secondly, the specific questionnaire itself and the multiple choice questions might have introduced some bias in the recorded answers and selected preferences. Thirdly, the psychological background of our respondents remained unexplored.
This study has, however, many strengths. It is the first of its kind in our country, revealing the scope of the problem as perceived by affected people. Even if correctly identifying themselves as overweight/obese these people are often satisfied with their overall health status and do not perceive any urgency for body weight reduction. However, those who wish losing weight may often harbor unrealistic expectations that may lead to severe disappointments. The causes for excessive weight are also poorly understood. The long-term management of obesity is still an enigma to the affected individuals and modern anti-obesity drugs are largely unknown.
5. Conclusions
There is a large gap between the scientific / clinical knowledge about obesity and the patients’ perspectives, attitudes and expectations. Filling this gap requires hard work both in increasing public awareness and correct knowledge and in implementing new health strategies for large-scale clinical programs fighting the epidemic of obesity. More detailed studies are still needed to better understand the incentives for both patients and healthcare professionals.
Supplementary Material
The following supporting information can be downloaded at the website of this paper posted on Preprints.org.
Author Contributions
Conceptualization, M.B.G., T.K.A., A.T K-S., M.A.B., M.G.N.; Methodology M.B.G., T.K.A., M.A.B., M.G.N.; Investigation, M.A.B. and M.B.G.; Data curation, T.K.A. and M.B.G.; Formal analysis, M.A.B., A.T.K-S., M.G.N. and M.B.G.; Funding acquisition, M.B.G.; Writing—original draft M.A.B.; Writing—review and editing, all authors. All authors have read and agreed to the submitted version of the manuscript.
Funding
This survey was sponsored by Novo Nordisk Bulgaria as a marketing study. The sponsor did not interfere either with the study design, methodology and completion or with the manuscript content.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki. Ethical review and approval were waived for this study as local regulations did not require ethical approval for questionnaire-based observational studies.
Informed Consent Statement
Informed consent was obtained from all subjects involved in the survey.
Data Availability Statement
Information available upon request to the corresponding author.
Acknowledgments
The authors would like to thank the NOEMA marketing research agency for their devoted work in building and completing this survey.
Conflicts of Interest
M.B. and M.G. have received lecture honoraria from Novo Nordisk Bulgaria. T.A. and A. K-S. are employees of Novo Nordisk Bulgaria. .
References
- Purnell, J.Q. Definitions, Classification, and Epidemiology of Obesity. [Updated 2023 May 4]. In: Feingold, K.R.; Anawalt, B.; Blackman, M.R. et al., Editors Endotext [Internet]. South Dartmouth (MA): MDText.com, Inc.; 2000-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK279167/.
- Nagi, M.A. , Ahmed, H., Rezq, M.A.A.; Sangroongruangsri, S.; Chaikledkaew, U.; Almalki, Z.; Thavorncharoensap, M. Economic costs of obesity: a systematic review. Int J Obes. 2024, 48, 33–43. [Google Scholar] [CrossRef]
- Agarwal, M.; Nadolsky, K. Attitudes, Perceptions, and Practices Among Endocrinologists Managing Obesity. Endocr Pract. 2022, 28, 179–184. [Google Scholar] [CrossRef]
- Wangler, J.; Jansky, M. Attitudes, behaviours and strategies towards obesity patients in primary care: A qualitative interview study with general practitioners in Germany. Eur J Gen Pract. 2021, 27, 27–34. [Google Scholar] [CrossRef] [PubMed]
- Ananthakumar, T.; Jones, N.R.; Hinton, L.; Aveyard, P. Clinical encounters about obesity: Systematic review of patients' perspectives. Clin Obes. 2020, 10, e12347. [Google Scholar] [CrossRef] [PubMed]
- Balani, R.; Herrington, H.; Bryant, E.; Lucas, C.; Kim, S.C. Nutrition knowledge, attitudes, and self-regulation as predictors of overweight and obesity. J Am Assoc Nurse Pract. 2019, 31, 502–510. [Google Scholar] [CrossRef] [PubMed]
- Joslyn, M.R.; Haider-Markel, D.P. Perceived causes of obesity, emotions, and attitudes about Discrimination Policy. Soc Sci Med. 2019, 223, 97–103. [Google Scholar] [CrossRef] [PubMed]
- Borissova, A.-M.; Shinkov, A.D.; Vlahov, J.D.; Dakovska, L.N.; Todorov, T.C. Survey on the Prevalence of Obesity in Bulgarian population in 2012 year. J. Endocrinologia. 2015, 20, 82–92. [Google Scholar]
- Borissova, A, -M.; Shinkov, A.D.; Vlahov, J.D.; Dakovska, L.N.; Todorov, T.C. Metabolic Syndrome in Bulgarian Population in 2012 Year. J. Endocrinologia. 2015, 20, 144–152. [Google Scholar]
- Salvador, J.; Vilarrasa, N.; Poyato, F.; Rubio, M.Á. Perceptions, Attitudes, and Barriers to Obesity Management in Spain: Results from the Spanish Cohort of the International ACTION-IO Observation Study. J Clin Med. 2020, 9, 2834. [Google Scholar] [CrossRef] [PubMed]
- Kaplan, L.M.; Golden, A.; Jinnett, K.; Kolotkin, R.L.; Kyle, T.K.; Look, M.; Nadglowski, J.; O'Neil, P.M. , Parry, T.; Tomaszewski, K.J.; Stevenin, B.; Lilleøre, S.K.; Dhurandhar, N.V. Perceptions of Barriers to Effective Obesity Care: Results from the National ACTION Study. Obesity (Silver Spring). 2018, 26, 61–69. [Google Scholar] [CrossRef] [PubMed]
- Zelenytė, V.; Valius, L.; Domeikienė, A.; Gudaitytė, R.; Endzinas, Ž.; Šumskas, L.; Maleckas, A. Body size perception, knowledge about obesity and factors associated with lifestyle change among patients, health care professionals and public health experts. BMC Fam Pract. 2021, 22, 37. [Google Scholar] [CrossRef] [PubMed]
- Caterson, I.D.; Alfadda, A.A.; Auerbach, P.; Coutinho, W.; Cuevas, A.; Dicker, D.; Hughes, C.; Iwabu, M.; Kang, J.H.; Nawar, R.; Reynoso, R.; Rhee, N.; Rigas, G.; Salvador, J.; Sbraccia, P.; Vázquez-Velázquez, V.; Halford, J.C.G. Gaps to bridge: Misalignment between perception, reality and actions in obesity. Diabetes Obes Metab. 2019, 21, 1914–1924. [Google Scholar] [CrossRef] [PubMed]
- Daigle, K.M.; Gang, C.H.; Kopping, M.F.; Gadde, K.M. Relationship Between Perceptions of Obesity Causes and Weight Loss Expectations Among Adults. J Nutr Educ Behav. 2019, 51, 86–90. [Google Scholar] [CrossRef] [PubMed]
- Warr, W.; Aveyard, P.; Albury, C.; Nicholson, B.; Tudor, K.; Hobbs, R.; Roberts, N.; Ziebland, S. A systematic review and thematic synthesis of qualitative studies exploring GPs' and nurses' perspectives on discussing weight with patients with overweight and obesity in primary care. Obes Rev. 2021, 22, e13151. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
Overall health self-evaluation (How would you evaluate your overall health condition?).
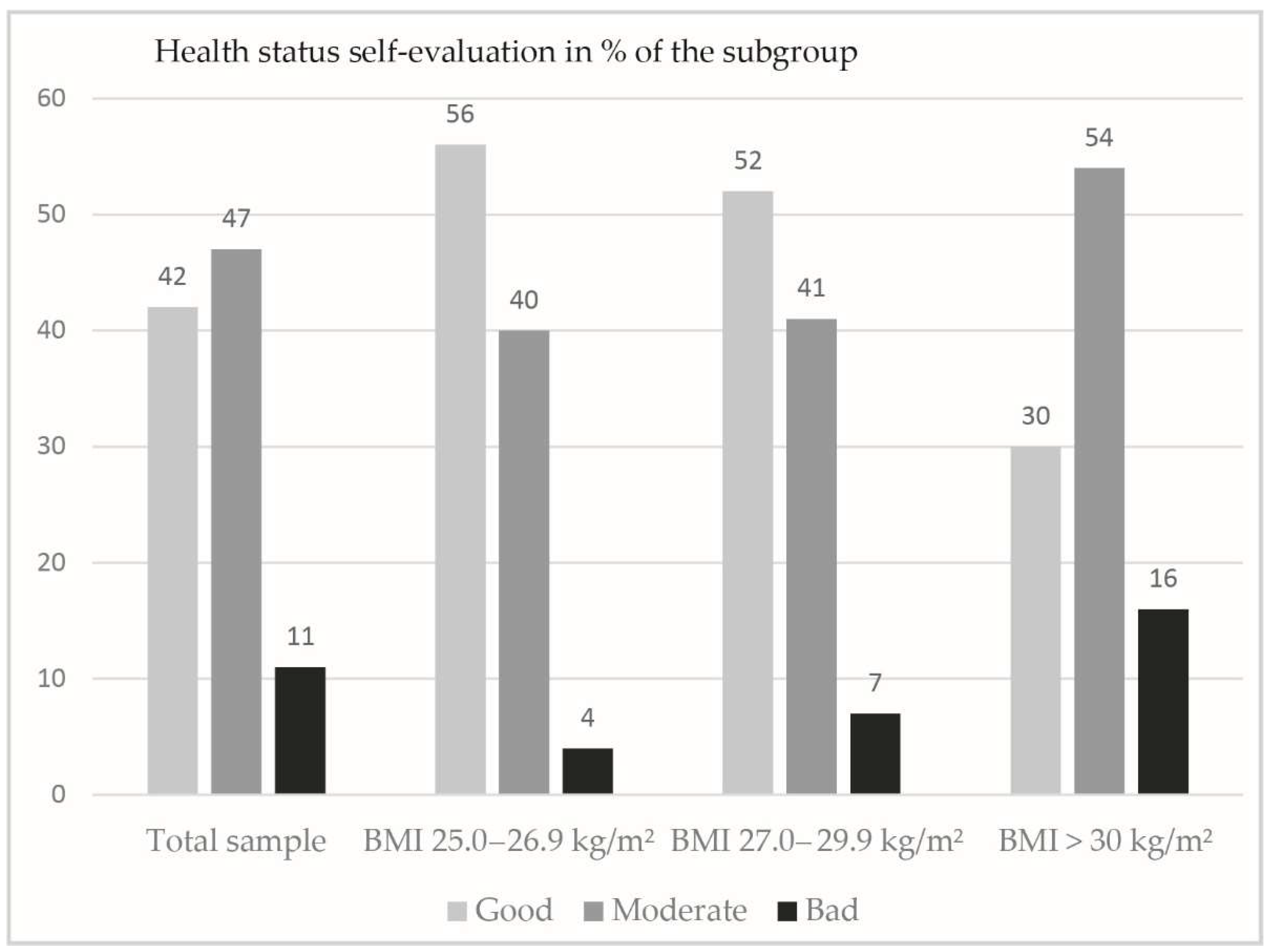
Figure 2.
The self-perception of the respondents of being overweight/obese is shown as shares in the total sample and BMI subcategories (Do you consider yourself having extra kg? How many? How many would you like to lose?).
Figure 2.
The self-perception of the respondents of being overweight/obese is shown as shares in the total sample and BMI subcategories (Do you consider yourself having extra kg? How many? How many would you like to lose?).
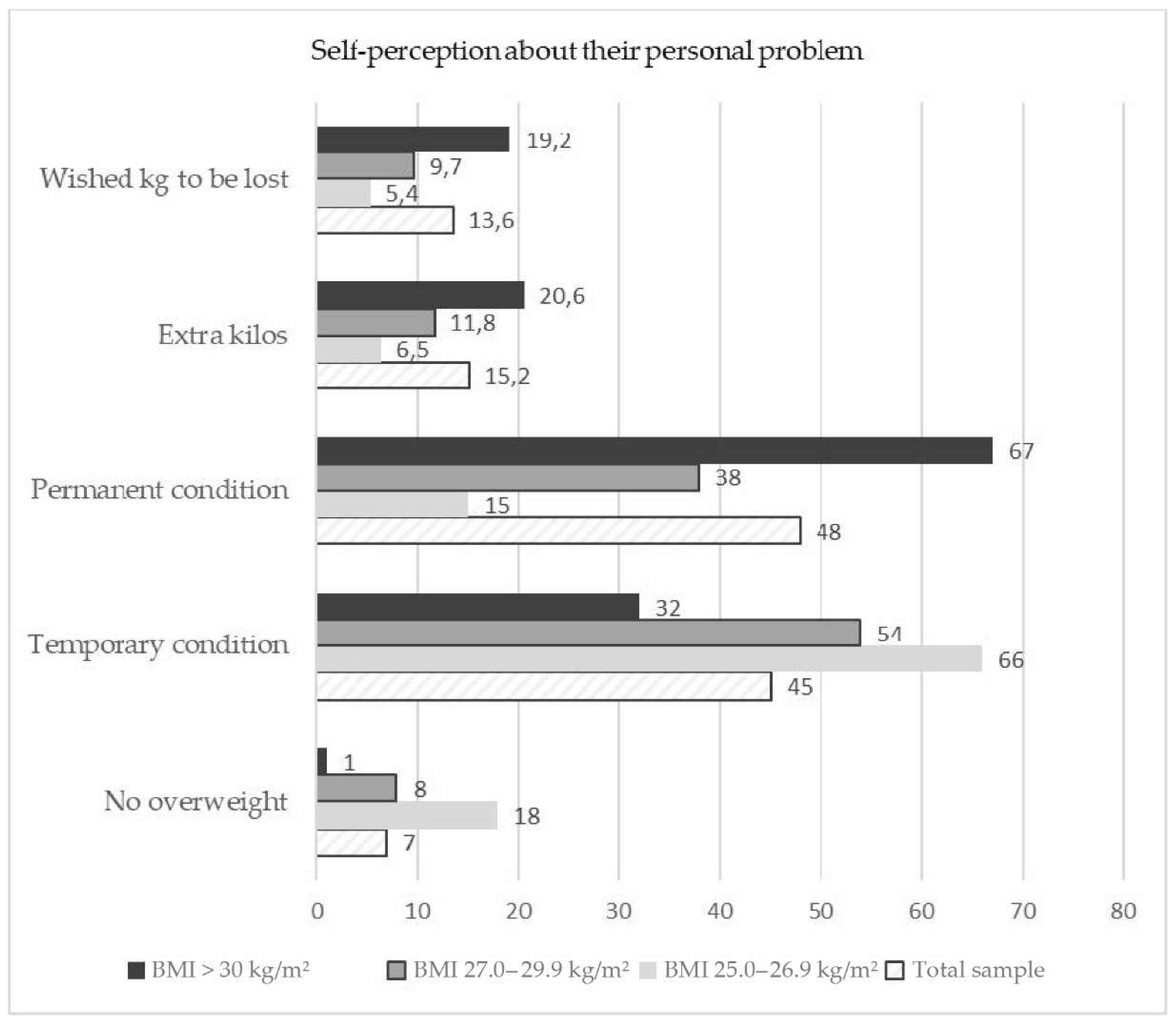
Figure 3.
Need for urgent reduction of body weight as perceived by the respondents (shares are shown in % of total).
Figure 3.
Need for urgent reduction of body weight as perceived by the respondents (shares are shown in % of total).
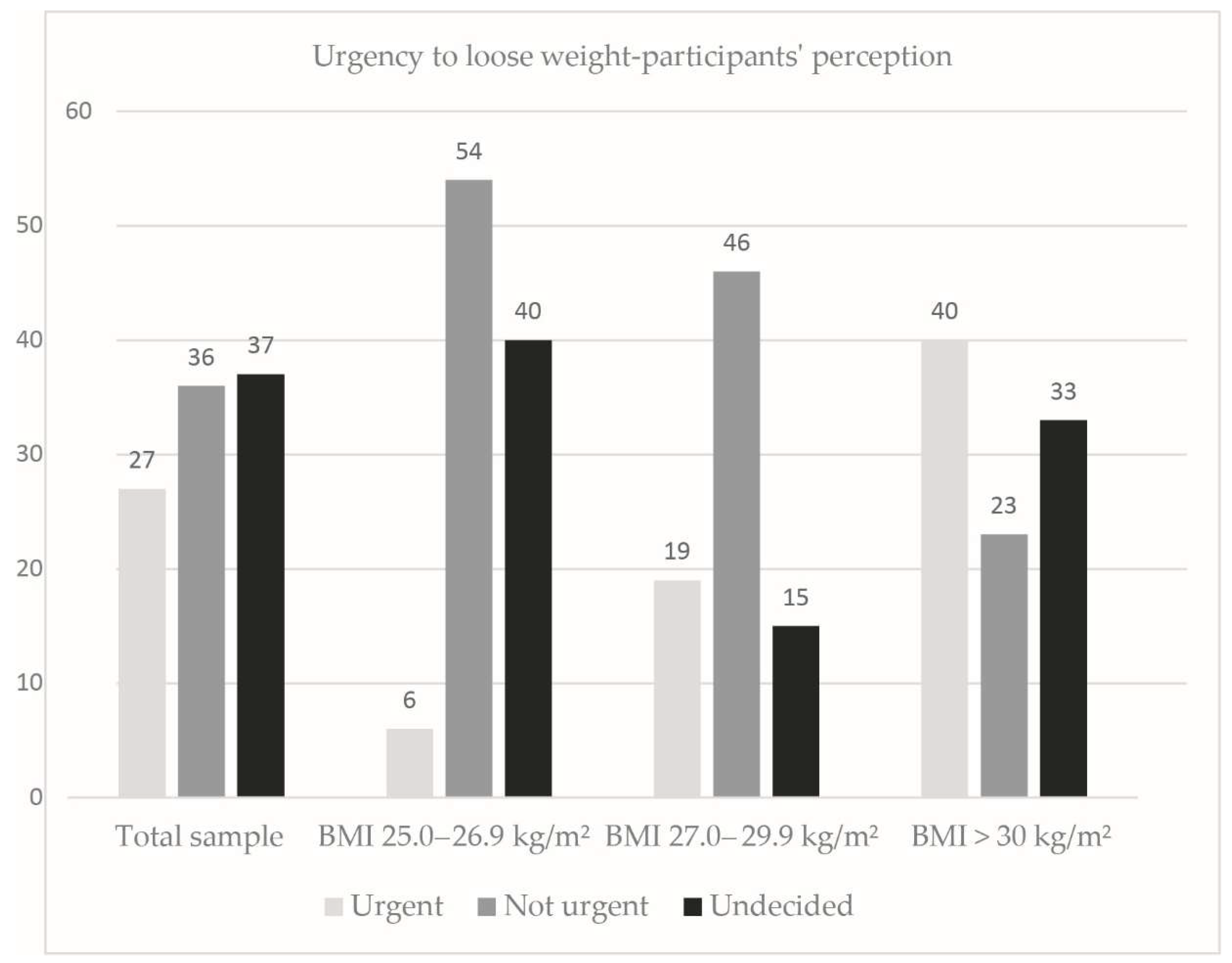
Figure 4.
Most popular methods for weight reduction among those that had ever tried.
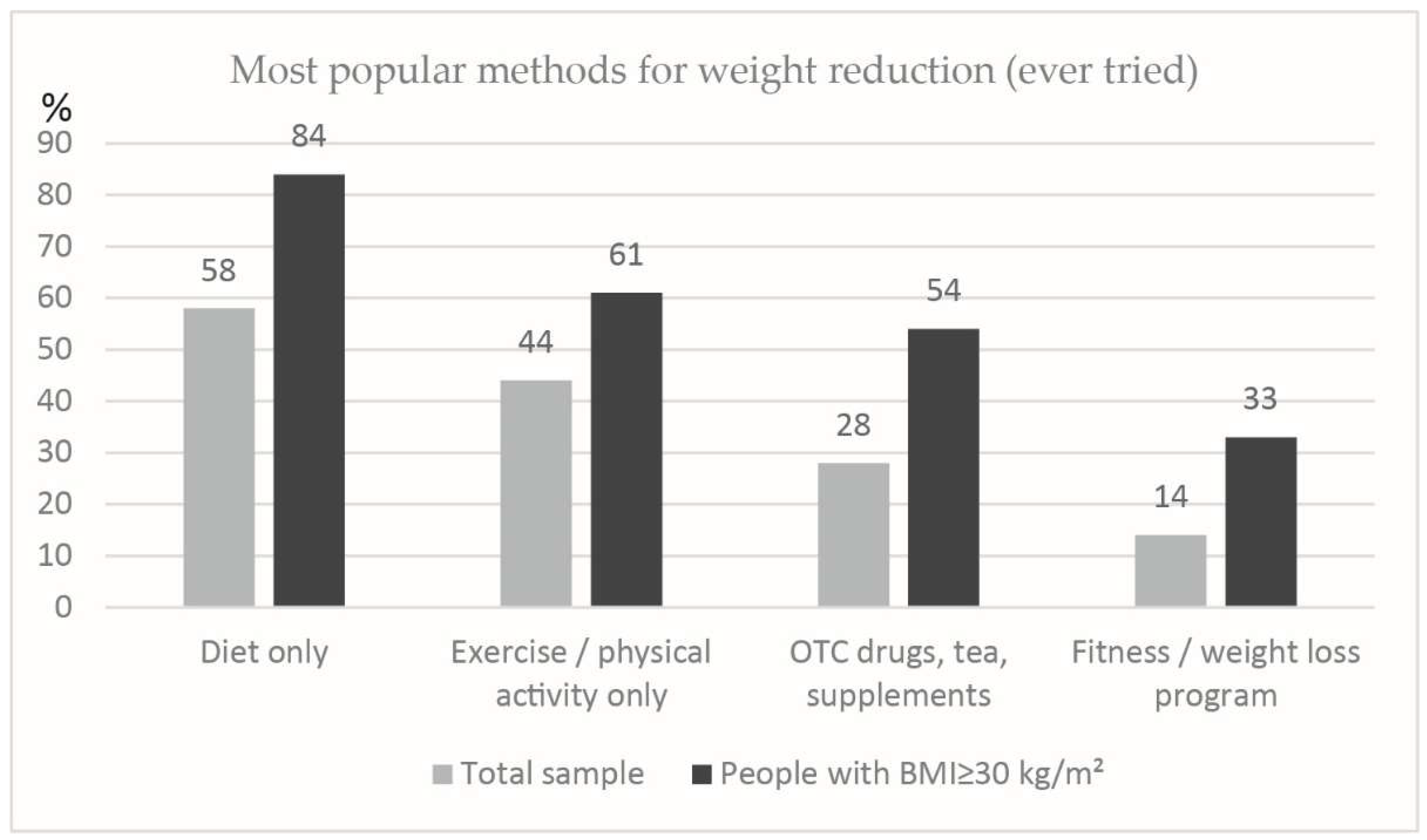

Table 1.
The sample structure and profile (as total and stratified according to BMI) are shown in %.
Table 1.
The sample structure and profile (as total and stratified according to BMI) are shown in %.
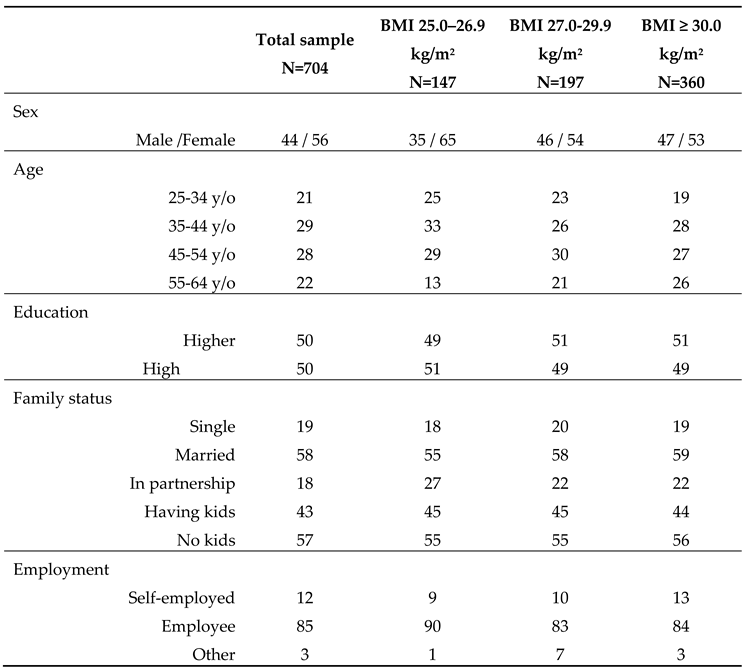
Table 2.
Differentiating reasons for overweight/obesity in BMI subcategories.
| BMI 25.0 – 26.9 kg/m2 | BMI 27.0 – 29.9 kg/m2 | BMI ≥ 30.0 kg/m2 |
|---|---|---|
|
|
|
Table 3.
Most trusted medical specialists for weight reduction.
|
Total sample N=704 |
BMI 25.0–26.9 kg/m2 N=147 |
BMI 27.0-29.9 kg/m2 N=197 |
BMI≥30.0 kg/m2 N=360 |
|
|---|---|---|---|---|
| Nutritionist | 25 | 23 | 18 | 29 |
| Endocrinologist | 17 | 14 | 11 | 21 |
| Cardiologist | 3 | 1 | 3 | 4 |
| GP | 19 | 20 | 24 | 15 |
| Other | 3 | 1 | 4 | 3 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



