
Submitted:
08 December 2024
Posted:
09 December 2024
You are already at the latest version
Abstract
Background: The prevalence of sexual dysfunctions varies from 35.5% to over 80% among post-partum women. Controversy exists regarding risk factors for female sexual dysfunction (FSDs) in the postpartum period. It remains unclear whether the breastfeeding types contribute to the development of FSDs differently. Aims: The primary goal of this meta-analysis is to explore the role of baby-feeding practices in developing sexual dysfunctions in women. Methods: We con-ducted a systematic literature search using the biomedical databases Scopus, CINAHL, Embase, Web of Science, and PubMed/Medline. We looked for peer-reviewed original studies written in English, Polish, and Arabic and published from January 2000 to June 2023. We included publica-tions that reported scores in sexuality domains assessed with the Female Sexual Dysfunction Index (FSFI) and any sexuality-related issues during postpartum. FSFI scores were combined in a meta-analysis using the random-effects inverse-variance model. Other findings were synthesized with a narrative review. Results: Nineteen articles met the eligibility criteria for systematic review and meta-analysis. Sexual dysfunctions were detected in all women, irrespective of the feeding type. Better overall sexual functioning was reported among women using complementary feeding than among those who breastfeed exclusively or use baby bottles: 22.16, 95% CI: 21.68 – 22.65, 21.61, 95% CI: 20.27 – 22.95, and 20.18, 95% CI -20.93 – 61.30, respectively. Slight lower scores were reported in all FSFI subscales in exclusively breastfeeding women compared to those using the complementary method. Conclusion: Breastfeeding females experience difficulties in sexual life during the postpartum period, irrespective of the feeding type. The most important aspects of the postpartum period that should be considered in the future are early diagnosis and prevention of sexual dysfunctions in all breastfeeding females.
Keywords:
Sexual dysfunctions
; sexuality
; sexual health
; breastfeeding
; lactation
; postpartum
; meta-analysis
; women’s health
1. Introduction
According to the World Health Organization (WHO), good sexual health encompasses "physical, emotional, mental, and social well-being in relation to sexuality" [1]. DSM-V defines sexual dysfunction as "a clinically significant disturbance in a person's ability to respond sexually or to experience sexual pleasure" [2]. A disturbance in female sexual life is regarded as a female sexual dysfunction (FSD) [3].
The prevalence of sexual dysfunctions differs across the studies between 20% and almost 50% [4,5,6,7,8]. Among postpartum women, the rate varies from 35.5% to over 80% [9,10]. A considerable heterogeneity in reporting the prevalence could be linked with methodological differences across the studies. The projects use different questionnaires, cover various populations, and assess sexual health at different time points since delivery. Moreover, psychological and sociocultural aspects could hinder the research. Controlling for confounders is another issue in reporting the precise prevalence of FSDs. For example, the mode of delivery and breastfeeding seem to be the most important biological factors influencing sexual health after birth [11,12]. However, the data regarding the occurrence of sexual dysfunction among breastfeeding women are ambiguous and vary from 20 to 80% [10,12,13].
After childbirth, women may experience a disturbance in any aspect of sexual function [14]. The divergence from pre-pregnancy sexuality can happen at psychosexual and biological levels. The disruption can appear in any female sexual response cycle described by Basson [15] and lead to decreased desire, reduced frequency of sexual intercourse, lack of lubrication, pain, and other issues [16,17]. In postpartum, the most common types of dysfunctions are decreased lubrication (85.6%), followed by loss of desire (69.7%), and pain disorders (62.9%) [9].
Multiple factors account for changes in sexual behavior and physical discomfort during intercourse [14,18,19]. The causes include hormonal shifts, adjustment to a new social role, physical traumas during birth, and breastfeeding. A single dysfunction can be caused by an interplay between the systems of the human body and the environment [20]. For example, dyspareunia is more common in women who had vaginal delivery compared to those with elective cesarian [18]. Dyspareunia is also associated with decreased estrogen levels and increased prolactin concentrations in breastfeeding women, which lead to vaginal dryness [21,22]. Moreover, hormonal changes can result in loss of desire associated with estrogen release, drop in androgens, fatigue, and sleep deprivation [15,23,24]. The hypothalamic-pituitary-adrenal and hypothalamic-pituitary-gonadal axes work differently in the postpartum compared to the pre-pregnancy period, and fluctuations in corresponding hormones can amplify the effect of individual hormonal shifts [20].
It remains unclear whether breastfeeding contributes to the development of FSDs. Dyspareunia, problems with lubrication, and low libido have been extensively studied [9]. However, while some publications highlight a higher prevalence of pain during intercourse in nursing mothers compared to non-breastfeeding females [25,26], others do not report any notable difference in the occurrence rate of this dysfunction. Similarly, controversy exists over a change in desire and sexual satisfaction after giving birth and vaginal atrophy [12,27]. Lev-Sagie et al. reported a high prevalence of postpartum atrophy (up to 62%) but did not confirm the correlation of dyspareunia with vaginal atrophy [28].
The prevention of FSD is challenging due to the lack of clear guidelines on defining a threshold for disorders [29]. The absence of the ideal diagnostic tools hinders timely counseling of women about dealing with fluctuations in the frequency and quality of sexual activity [30]. Still, many symptoms remain subjective, and women may treat deviations as a norm. As a result, FSD cases may be underreported. These factors complicate the identification of women at risk for disturbances in sexual health postpartum. The introduction of the Female Sexual Function Index (FSFI) helped to unify the assessment of sexual health and research in this field. The survey measures sexual function in six domains: desire, arousal, lubrication, orgasm, satisfaction, and pain [31]. However, the tool provides diagnostic criteria only for the overall sexual dysfunction and desire hypoactive disorders.
The existing literature has many systematic reviews (SRs) examining postpartum FSDs. Still, the findings contradict each other due to methodological differences and ethical concerns at a particular study site. The studies focus on types of delivery, complications during childbirth, and psychosocial determinants of FSDs. Research on sexual health in breastfeeding women lacks an explicit stratification of the study participants by baby-feeding type [26,32,33]. Authors classify the mothers by either breastfeeding or non-breastfeeding. However, a complete list of criteria defining infant feeding practice includes breastfeeding, exclusive, predominant feeding, and bottle-feeding [34]. Another limitation of available research is the small sample size: the number of participants rarely exceeds 500 women. SR and meta-analysis (MA) may help to overcome the limitations of original studies. The proposed SR and MA will be the first study examining the relationship between breastfeeding types and FSDs.
2. Materials and Methods
2.1. Objectives
The primary goal of this MA is to explore the role of baby-feeding practices in developing sexual dysfunctions in women. The secondary objectives are as follows:
1. Calculate pooled mean scores of FSFI total and its subscales according to different types of breastfeeding.
2. Summarize other issues with sexuality in breastfeeding women.
2.2. Methodology
This review and MA focused on sexual health in generally healthy breastfeeding women. The publication was prepared following the 2020 Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) checklist, which is available as an online Supplementary file 1. The study protocol was registered in PROSPERO (CRD 42023411053). The methodology of the SR and MA was also published elsewhere [35].
2.2.1. Study Design and Data Source
The study focused on the relationship between infant feeding style and FSD, as well as other possible disturbances in sexual health that may appear during the lactation period. The study explored pooled scores in total FSFI and its domains among mothers practicing various types of baby feeding. These findings were used to conduct a meta-analysis. We also sought information on other issues related to sexuality and systematically reviewed the data.
A systematic literature search was conducted in the biomedical databases Scopus, CINAHL, Embase, Web of Science, and PubMed/Medline by D.S. and the Principal Investigator (K.Z.). We looked for peer-reviewed original studies written in English, Polish, and Arabic and published from January 2000 to June 2023. The inception date corresponds to the first mention of the FSFI tool. Key terms were searched in the "title/abstract", "MeSH terms", or "keywords" fields. The last literature search was performed on 27 May 2023. The detailed search strategy is available online in Supplementary Table S1.
2.2.2. Eligibility Criteria
The study analyzed females of reproductive age, starting from 15 years old, who reported at least one sexuality-related issue within two years of childbirth. For the MA, we focused on the studies reporting the mean and standard deviations (mean±SD) of total scores in FSFI or its domains. The publications were deemed eligible if they reported a type of breastfeeding, time since delivery, and the age of the participants.
We included the publications that reported findings about participants free from mental, psychological, and neurological disorders, organic pathologies of the central nervous system and reproductive organs, cerebrovascular and endocrine diseases, and any conditions that could affect sexual health (e.g., diabetes mellitus, systemic mastocytosis). We did not include studies assessing women who had pregnancies with severe fetal abnormalities and sexual dysfunctions known before conception.
We excluded dissertations, protocol papers, reviews, case studies, editorial letters, conference posters, and presentations. We considered randomized-control trials, cohort, and cross-sectional studies.
2.2.3. Selection Process
Records matching the search strings were uploaded to the systematic review software Covidence (Veritas Health Innovation, 2021, https://www.covidence.org) for automatic deduplication and blinded screening. Four reviewers (S.A., A.A., M.A., and E.H.) screened titles and abstracts independently by voting "yes", "no", or "maybe" in the software. In case of any disagreements, D.S. and K.Z. discussed whether the paper met the eligibility criteria. The same process was applied to evaluate the full texts of the publications. The results of the literature screening were automatically generated and presented with a PRISMA flowchart (Figure 1).
2.2.4. Data Collection Process
The team members extracted data into a pre-defined Microsoft Excel spreadsheet. D.S. created the spreadsheet and approved it by K.Z. Four separate reviewers (H.A., M.A., R.A., and H.A.) performed the data extraction. Once the template was filled in, D.S. verified the entered data.
The table consisted of two tabs. The first section included information about FSFI scores in breastfeeding females. In this part, the data items included general information about the article: first author's name, year of publication, publication title, country of conduct of a study, and authors' conflicts of interest. The extracted data also included details about the methodology and study cohort: study design, aims/objectives, inclusion and exclusion criteria, the number of participants in each feeding group, age of participants, and time since delivery expressed as mean ± SD. The final set of variables consisted of time since delivery as mean ± SD, breastfeeding type, FSFI domain, score (mean), and score (SD).
The second part of the data extraction table covered other issues relevant to sexual health during the lactation period. This section had the same data items for the general characteristics of the publications, methodology, and study cohort as the first part of the table. The variables corresponding to sexual health consisted of time since delivery, condition type (e.g., resumption of intercourse, vulvovaginal atrophy), the number of participants with an issue, breastfeeding characteristics, and measures of associations.
While collecting the data, we observed variability in reporting time since delivery. To ensure uniform presentation of data, the findings were converted in days since giving birth. The authors also classified feeding methods differently. The following infant feeding styles were reported in the publications: exclusive, formula, breastfeeding plus formula, breastfeeding plus complementary feeding, breastfeeding with no further specification, non-exclusive without further specifications, predominant, complementary, mixed, and artificial. The primary investigator, an obstetrics and gynecology doctor, grouped the identified feeding practices into three methods: exclusive, formula, and breastfeeding with complimentary. This classification is similar to the one proposed by the WHO [34].
2.2.5. Risk of Bias Assessment
For the quality assessment of individual studies, we used checklists developed by the Joanna Briggs Institute [36]. We selected checklists for the appraisal of analytical cross-sectional studies, cohort studies, and randomized controlled trials. Four reviewers (H.A., M.A., R.A., and H.A.) independently answered the assessment tools' questions. The principal investigator (K.Z.) and another reviewer (D.S.) checked the answers. If any disagreements arose, they were resolved by discussing them with the reviewer who initially appraised the article. Details of quality assessment are available in Supplementary Table S3.
2.2.6. Data Synthesis
As part of working on the first specific objective, we resorted to the “metafor” and “dmetar” packages in R software (version 2024.04.2-764). We conducted the MA using the random-effects inverse-variance model. Mean scores and SDs in FSFI total and its domains were combined in the MA to obtain aggregated data on the severity of FSDs. Then, we assessed between-study heterogeneity with the “m.gen” command. To detect studies causing a high level of variability (I2>75%), the “find.outliers” function was called. The identified outliers were removed from the database. Subsequently, we divided the observations into groups according to FSFI domains and feeding practices. The “metamean” function was applied again to produce the results from a dataset without outliers. To illustrate the study results, we constructed forest plots with the “meta::forest” function. Working on the second objective, we analyzed the findings from the eligible studies with a narrative approach.
2.2.7. Bias Assessment
We examined publication bias between studies included in the MA. We constructed funnel plots using the “funnel” function in R software. The graph allows for visual inspection of publication bias. Asymmetric funnel plots indicate a low precision of the effect sizes (See Supplementary Figures S8 – S15).
3. Results
3.1. Literature Search
We retrieved 5573 studies from the biomedical databases. After deduplication, 3265 publications remained for titles and abstracts screening. 126 articles were identified for full-text evaluation against the eligibility criteria. The final dataset consisted of 19 publications. Findings from nine studies were included in the MA. The remaining publications were included in the qualitative analysis of postpartum sexual health.
3.2. Characteristics of Studies Included in the Meta-Analysis
The studies included in the MA were conducted in Iran (4 publications) [37,38,39,40], Brazil (two papers) [12,41], Canada [42] and Japan [43]. The sample size ranged from 27 to 355 women (See Table 1). The age of participants was similar across the publications. The time since giving birth did not exceed six months. The classification of breastfeeding practices was not uniform across the studies. In total, we identified nine infant feeding types. Eight publications reported scores in all domains of the FSFI questionnaire. Saotome et al. considered exclusively the overall sexual dysfunction in breastfeeding women [43]. The quality of studies ranged from low to high (Supplementary Table S3).
3.3. Scores in FSFI Domains, Irrespective of Infant Feeding Practices
We analyzed pooled scores in total FSFI and its subscales irrespective of feeding practices (Supplementary Figures S1-S6). Results in the desire domain were below the clinical cut-off point for diagnosing a desire disorder: 3.08, 95% CI: [2.92; 3.24] vs 5 points on the scale. Other subscales do not have a threshold for healthy sexual functioning. However, the highest mean score was reported for the satisfaction domain (4.12, 95% CI: [3.79; 4.46]). In this subscale, the scores range between 0.8 to 6.
The FSFI scores for the overall sexual function may range between 2 and 36. In our sample, the overall score was 21.97, 95% CI [21.09;22.84].
Sexual function in women choosing distinct infant feeding methods
3.4. Scores in FSFI Subscales
3.4.1. Desire
Aggregated FSFI desire score was also calculated for 409 women breastfeeding exclusively and 122 females resorting to complementary feeding (Figure 2). The first group had slightly lower scores on desire subscale than the second one: 3.04, 95% CI: 2.81 – 3.27 vs. 3.18, 95% CI: 2.80 – 3.56. Desire is the only FSFI domain with a clinically validated cut-off point of 5 for confirming desire hypoactive disorder. Both groups met the criteria for diagnosing the dysfunction in the desire domain. No significant heterogeneity was observed among studies in both groups. The funnel plots were also symmetric, indicating the absence of publication bias.
section may be divided by subheadings. It should provide a concise and precise description of the experimental results, their interpretation, as well as the experimental conclusions that can be drawn.
3.4.2. Arousal
We did not receive enough studies reporting FSFI arousal scores among women using bottle feeding. The analysis covered 424 study participants breastfeeding exclusively and 122 females using complimentary breastfeeding (Figure 3). In the latter group, the pooled FSFI arousal score was higher than women feeding their babies only with breast milk: 4.00, 95% CI: 3.58 – 4.43 vs. 3.53, 95% CI: 3.21 – 3.85, respectively. The between-study heterogeneity was greater for publications reporting arousal scores among exclusively breastfeeding mothers (I2 =73%, p<0.01). We did not observe any publication bias in the two groups.
3.4.3. Orgasm
FSFI scores on the orgasm subscale were reported for 387 women breastfeeding exclusively and 122 females using complementary feeding (Figure 4). The pooled results for the orgasm domain were lower in the women feeding the babies solely with human milk compared to females complimenting breastfeeding: 3.56, 95% CI: 3.05 – 4.08 vs. 3.88, 95% CI: 3.60 – 4.16, respectively. Heterogeneity was high for studies reporting orgasm scores for women breastfeeding exclusively (I2=85%, p<0.01). Therefore, the results should be interpreted with caution.
3.4.4. Lubrication
The FSFI lubrication domain was assessed in 396 women breastfeeding exclusively and in 122 females using complimentary feeding (Figure 5). The pooled score was lower among exclusively breastfeeding mothers than in those using mixed feeding: 3.69, 95%CI: 3.44 – 3.93 vs. 3.91, 95%CI: 2.89 – 4.93, respectively. The between-study heterogeneity was high in both groups. However, no publication biases were seen on the funnel plots.
3.4.5. Pain
Removal of outliers resulted in omitting studies reporting scores on FSFI pain domain in women choosing complementary feeding (Figure 6). Among 507 women breastfeeding exclusively, the random-effects model produced a pooled score of 3.44, 95%CI 3.12 – 3.76. The analyzed studies were highly heterogeneous (I2=81%, p<0.01). The funnel plot was slightly asymmetric due to a possible presence of bias.
3.4.6. Satisfaction
Satisfaction was measured among 507 exclusively breastfeeding women and 74 women using complementary feeding (Figure 7). This domain had the highest score in both groups compared to other FSFI subscales. Exclusively breastfeeding women had lower scores than mothers using complementary feeding: 4.04, 95%CI: 3.67 – 4.42 vs 4.52, 95%CI: 0.23 – 8.82. Heterogeneity was high among studies reporting data for the exclusive breastfeeding group (I2=81%, p<0.01). In the second group, heterogeneity was moderate. However, only 2 studies were included in the analysis. These results complicate the generalizability of findings beyond the analyzed studies.
3.4.7. Overall Sexual Function
Overall sexual functioning was reported in studies examining FSDs in three groups of women: exclusively breastfeeding, using complementary feeding, and giving only bottles to the babies (Figure 8). Each group included 535, 175, and 188 examinees, respectively. Sexual dysfunction was detected in all women, irrespective of the feeding type. Better sexual functioning was reported among women using complementary feeding than among those who breastfeed exclusively or use baby bottles: 22.16, 95%CI: 21.68 – 22.65, 21.61, 95%CI: 20.27 – 22.95, and 20.18, 95%CI -20.93 – 61.30, respectively.
Significant inter-study heterogeneity was detected among studies reporting FSFI scores among exclusively breastfeeding women (I2=89%, p<0.01) and those who bottle feed (I2=82%, p=0.02). The funnel plots did not show publication bias in all three groups.
3.5. Description of Studies Included in a Systematic Review
3.6. Resumption of Sexual Intercourse
Four studies focused on the resumption of sexual intercourse in breastfeeding women. Alum et al. reported that 82% of exclusively breastfeeding women from Uganda resumed intercourse before 6 weeks postpartum [44]. Among Spanish women, 23.10% of nursing mothers were engaged in sexual activity within the same period [51]. In another study, 28.3% of breastfeeding Iranian women returned to sexual activity within one month of giving birth [27]. The publication did not provide information on whether a baby feeding type was associated with the resumption of intercourse. In a sample of Swedish women, 75.3% of breastfeeding participants returned to sexual activity within 3 months of childbirth. In the same study, over 90% of nursing mothers had sex within 6 months of the delivery [46]. According to Signorello et al., breastfeeding females resumed sexual activity 0.8 weeks earlier than non-breastfeeding women [50].
Change in sexuality was explored in four studies [15,27,47,49]. These changes included reduced desire, satisfaction, lack of vaginal lubrication, difficulty in reaching orgasm, and overall decreased sexual functioning. The studies used ad hoc questionnaires to assess postpartum sexual functioning. Rezai et al. and Salamon et al. examined sexual health with FSFI but the studies did not report scores in the domains [47,49]. Therefore, these studies were not included in the meta-analysis. According to Rezai et.al., exclusive breastfeeding was a risk factor for sexual dysfunction: aOR: 2.47; 95% CI: 1.21 - 5.03 [47]. Salamon et al. did not compare sexual issues between different feeding styles, but the study confirmed a higher risk of FSD in breastfeeding women compared to non-breastfeeding: aOR: 2.24; 95% CI: 1.03 - 4.85 [49]. Heidari et al. did not observe any significant difference between breastfeeding and bottle-feeding women on sexual desire and satisfaction before and after pregnancy [27]. Both groups of women did not have a notable difference in experiencing orgasm before conception and after the delivery. O’Malley et al., compared vaginal lubrication and loss of interest in sexual activity between breastfeeding and non-breastfeeding women [45]. At 6 months postpartum, breastfeeding was associated with change in these two domains.
Two authors looked for a relationship between breastfeeding and pain during intercourse [48,50]. Rosen et al. modeled change in dyspareunia levels up to 24 months postpartum. The study did not confirm the impact of breastfeeding on the dyspareunia trajectory postpartum [48]. Signorello et al. identified breastfeeding as a strong predictor of pain at the first postpartum intercourse, at 3 and 6 months after delivery: OR: 2.2; 95% CI: 1.4 - 3.2, OR: 2.7; 95% CI: 1.8 – 4.1, and OR: 4.4; 95% CI: 2.7 - 7.0 [50]. A single study explored an incidence of vulvovaginal atrophy in breastfeeding and non-breastfeeding women. The disorder was more common in breastfeeding than in non-breastfeeding women [28].
4. Discussion
Breastfeeding is crucial for the healthy development of newborns, both biologically and psychologically. From the maternal point of view, Stone and Smith define breastfeeding as a “sexual and reproductive health right” [52]. Regrettably, the postpartum period may be associated with the occurrence of sexual disorders [53]. Breastfeeding may further intensify the disorder due to both biological reasons arising from hormonal changes and fatigue resulting from frequent waking at night [19]. However, the presented study does not provide clear results in this regard.
The current MA identified sexual dysfunction in the overall sample of postpartum women, irrespective of the feeding type. Women breastfeeding exclusively had lower scores in all FSFI domains (desire, arousal, orgasm, lubrication, and satisfaction) than the women choosing complementary feeding. The findings are in line with the recent research by Sun et al., who reported a high incidence of sexual dysfunctions in both groups [53]. According to Fuentealba-Torres et al., sexual dysfunction was present in 58.3% of breastfeeding females, and it was connected to a low quality of life [12]. In the presented sample, the total FSFI score was 21.97, 95% CI [21.09;22.84]. Clinicians use a score of 26.55 out of 36 to differentiate between women with and without sexual dysfunction. The results imply that the participants experienced difficulties in sexual life during the postpartum period, irrespective of the feeding type. The reason for this might be hormonal changes that still occur even when the breasts are stimulated infrequently [54]. It remains unclear whether the concentration of hormones is the same in mothers breastfeeding exclusively or complementary. In formula-feeding mothers, FSDs may occur due to the fatigue that women experience because of the necessity to wake up frequently to prepare the infant's food [55]. Mariman et al. did not find any difference in the level of fatigue between mothers who are exclusively breastfeeding and mothers who bottle-feed [55].
The exclusively breastfeeding mothers had slightly lower scores on desire subscale than mothers using complementary feeding: 3.04, 95% CI: 2.81 – 3.27 vs. 3.18, 95% CI: 2.80 – 3.56. Both groups met the criteria for diagnosing the dysfunction in the desire domain. The results are in line with the research performed by Kayner al. on 121 lactating females with lactation amenorrhea who predominantly reported low desire [56]. Desire is mainly connected with the psychological aspect of sexuality [58]. In line with Basson's theory, we can hypnotize that women are less willing to have sexual intercourse when they experience vaginal atrophy connected with exclusive lactation[28,57].
In the presented study, the FSFI arousal score was higher in females complementing breastfeeding compared to women feeding solely with human milk: 4,95% CI: 3.58 – 4.43 vs 3.53, 95% CI: 3.21 – 3.85, respectively. Arousal is the biological effect of desire that depends on genital and hormonal well-being [58]. Changes that occur during lactation may influence these systems. Moreover, sexual arousal relates also to sexual desire, which can influence the final biological effect. The same biological aspect may play a role in the ability to reach the orgasm among exclusively breastfeeding women. The pooled results for the orgasm domain were lower in the women feeding the babies solely with human milk compared to females complimenting breastfeeding: 3.56, 95% CI: 3.05 – 4.08 vs. 3.88, 95% CI: 3.60 – 4.16, respectively. The presented results are in line with Fuentealba-Torres et al., who reported that breastfeeding females had high levels of sexual dysfunction in arousal (83%) and orgasmic domain (76.3%) [12].
The pooled score for the lubrication domain was lower among exclusively breastfeeding mothers than those using mixed feeding: 3.69, 95% CI: 3.44 – 3.93 vs. 3.91, 95% CI: 2.89 – 4.93, respectively. Vaginal lubrication is mostly connected with the level of estrogens that is lower in breastfeeding females – especially in those resorting to exclusive lactation [59]. High levels of prolactin produced by stimulation of the breasts inhibit estrogen secretion, leading to vulvovaginal atrophy, dryness, and subsequent dyspareunia.
The MA revealed lower scores on the satisfaction subscale in exclusively breastfeeding women compared to mothers using complementary feeding: 4.04, 95%CI: 3.67 – 4.42 vs 4.52, 95% CI: 0.23 – 8.82. On the other hand, Fuentealba-Torres et al. reported that among all FSFI domains, sexual satisfaction was low only in 50.9% of participants being less predisposed to decrease than other domains reaching 70-80% of cases [12]. Supposedly, this domain also addresses the theory of Basson, where sexual intercourse is only a part of all aspects of sexual satisfaction involving relational dimensions such as mutuality, interpersonal closeness, romance, cohabitation, and expression of feelings [60,61].
In traditional societies, sexuality is a taboo topic and is studied in the social and medical context [44]. Early return to sexual activity has a protective effect against extramarital affairs and sexually transmitted diseases. However, early initiation of sexual contact is associated with unwanted pregnancies, genital trauma, and puerperal infection. The presented study highlights the most important aspects of female sexuality in the postpartum period that should be considered in future management, starting with simple things like asking questions about the occurrence of possible sexual dysfunctions. Some of them, like vaginal atrophy, can be managed with simple vaginal treatment [62].
Limitations
The meta-analysis possesses limitations that should be considered and addressed in future similar works:
- The search strategy did not yield a sufficient number of publications reporting sexual dysfunctions among women resorting to bottle-feeding. Therefore, we did not calculate pooled scores in individual sexuality domains for this group of women.
- The initial analysis revealed a high heterogeneity index. To address significant between-study variability, we identified and removed outliers. Omitting studies with extreme values may reduce the generalisability of the study findings beyond the results of this work.
- Since the number of included studies was low, we could not adjust the findings for time since delivery. However, this information could provide valuable insight into the dynamics of sexual functioning in the postpartum period.
Strengths
- The work was prepared in accordance with the PRISMA guidelines and registered in the PROSPERO database.
- The research compiled aggregate scores across all areas of sexual functioning using the FSFI scale. Earlier systematic reviews and meta-analyses focused on overall sexual health data. Nevertheless, understanding changes within each domain is crucial for creating effective counseling approaches for couples expecting a baby.
- The FSFI scores were calculated separately for each type of feeding practice. The findings reflect a possible relationship between hormonal changes in lactating women and their sexual function postpartum.
- No significant publication biases were detected across the studies. The funnel plots were symmetric in all subgroups, indicating that the studies had similar effect sizes.
- The systematic review covered other possible changes in sexual health in breastfeeding females. The findings revealed a range of issues women face in the postpartum period that require attention from healthcare specialists.
5. Conclusions
Breastfeeding females experience difficulties in sexual life during the postpartum period irrespective of the feeding type. The prevalence of sexual dysfunctions (both as the pool score and in all domains) is slightly higher in patients exclusively breastfeeding. The most important aspects of female sexuality in the postpartum period that should be considered in the future are early diagnosis and prevention of sexual dysfunctions in all breastfeeding females.
Supplementary Materials
The following supporting information can be downloaded at: Preprints.org, Table S1. Search strategy; Table S2. PRISMA 2020 checklist; Table S3. Quality assessment of individual studies; Figure S1. Arousal in Postpartum Women; Figure S2. Desire in postpartum women; Figure S3. Orgasm in postpartum women; Figure S4. Lubrication in postpartum women; Figure S5. Pain in postpartum women; Figure S6. Satisfaction in Postpartum Women; Figure S7. Overall sexual function in postpartum women; Figure S8. Funnel plots exploring publications bias in studies reporting arousal (A), desire (B), orgasm (C), lubrication (D), pain (E), satisfaction (F), and overall sexual function (G); Figure S9. Funnel plots depicting publication bias for studies on arousal in women choosing (A) exclusive and (B) complimented breastfeeding; Figure S10. Funnel plots depicting publication bias for studies on desire in women choosing (A) exclusive and (B) complimented breastfeeding; Figure S11. Funnel plots depicting publication bias for studies on orgasm in women choosing (A) exclusive and (B) complimented breastfeeding; Figure S12. Funnel plots depicting publication bias for studies on lubrication in women choosing (A) exclusive and (B) complimented breastfeeding; Figure S13. Funnel plots depicting publication bias for studies on pain in women choosing (A) exclusive and (B) complimented breastfeeding; Figure S14. Funnel plots depicting publication bias for studies on satisfaction in women choosing (A) exclusive and (B) complimented breastfeeding; Figure S15. Funnel plots depicting publication bias for studies on overall FSFI score in women choosing (A) exclusive, (B)complimented breastfeeding, and (C) bottle feeding;
Author Contributions
Conceptualization, K.Z., D.S.; methodology, D.S., Y.S.; software, Y.S.; validation, K.Z., S.A; formal analysis, Y.S; investigation, S.A., A.A., M.A., E.H., H.A., M.A, R.A. and H.A.; resources, K.Z, Y.S.; data curation, D.S.; writing—original draft preparation, K.Z., D.S.; writing—review and editing, K.Z., D.S.; visualization, Y.S; supervision, K.Z.; project administration, Y.S.; funding acquisition, K.Z. All authors have read and agreed to the published version of the manuscript.
Funding
This work was supported and funded by the Summer Research Grant Number G00004754 (08-MAY-2024) awarded by the United Arab Emirates University.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
No new data were created for this study.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- WHO. Sexual Health and Well-Being. Available online: https://www.who.int/teams/sexual-and-reproductive-health-and-research-(srh)/areas-of-work/sexual-health#:~:text=WHO%20defines%20sexual%20health%20as,of%20disease%2C%20dysfunction%20or%20infirmity (accessed on day month year).
- American Psychiatric Association Diagnostic and Statistical Manual of Mental Disorders; American Psychiatric Association: Arlington, VA, 2013; p. 423; ISBN 0-89042-555-8.
- Aslan, E.; Fynes, M. Female Sexual Dysfunction. Int. Urogynecol. J. 2008, 19, 293–305. [Google Scholar] [CrossRef] [PubMed]
- Zheng, J.; Skiba, M.A.; Bell, R.J.; Islam, R.M.; Davis, S.R. The Prevalence of Sexual Dysfunctions and Sexually Related Distress in Young Women: A Cross-Sectional Survey. Fertil. Steril. 2020, 113, 426–434. [Google Scholar] [CrossRef] [PubMed]
- McCabe, M.P.; Sharlip, I.D.; Lewis, R.; Atalla, E.; Balon, R.; Fisher, A.D.; Laumann, E.; Lee, S.W.; Segraves, R.T. Incidence and Prevalence of Sexual Dysfunction in Women and Men: A Consensus Statement from the Fourth International Consultation on Sexual Medicine 2015. J. Sex. Med. 2016, 13, 144–152. [Google Scholar] [CrossRef] [PubMed]
- Nicolosi, A.; Laumann, E.O.; Glasser, D.B.; Moreira, E.D.; Paik, A.; Gingell, C. Sexual Behavior and Sexual Dysfunctions after Age 40: The Global Study of Sexual Attitudes and Behaviors. Urology 2004, 64, 991–997. [Google Scholar] [CrossRef]
- Starc, A. Female Sexual Function and Dysfunction: A Cross-National Prevalence Study in Slovenia. Acta. Clin. Croat. 2018, 57, 52–60. [Google Scholar] [CrossRef]
- Khani, A. Female Sexual Dysfunction: Prevalence and Risk Factors. J. clin. diagn. res. 2013. [Google Scholar] [CrossRef]
- Khalid, N.N.; Jamani, N.A.; Abd Aziz, K.H.; Draman, N. The Prevalence of Sexual Dysfunction among Postpartum Women on the East Coast of Malaysia. J. Taibah. Univ. Med. Sci. 2020, 15, 515–521. [Google Scholar] [CrossRef]
- Khajehei, M.; Doherty, M.; Tilley, P.J.M.; Sauer, K. Prevalence and Risk Factors of Sexual Dysfunction in Postpartum Australian Women. J. Sex. Med. 2015, 12, 1415–1426. [Google Scholar] [CrossRef]
- Dabiri, F.; Yabandeh, A.P.; Shahi, A.; Kamjoo, A.; Teshnizi, S.H. The Effect of Mode of Delivery on Postpartum Sexual Functioning in Primiparous Women. Oman. Med. J. 2014, 29, 276–279. [Google Scholar] [CrossRef]
- Fuentealba-Torres, M.; Cartagena-Ramos, D.; Fronteira, I.; Lara, L.A.; Arroyo, L.H.; Arcoverde, M.A.M.; Yamamura, M.; Nascimento, L.C.; Arcêncio, R.A. What Are the Prevalence and Factors Associated with Sexual Dysfunction in Breastfeeding Women? A Brazilian Cross-Sectional Analytical Study. BMJ Open 2019, 9, e025833. [Google Scholar] [CrossRef]
- Kouéta, F.; Dao, L.; Dao, F.; Djekompté, S.; Sawadogo, J.; Diarra, Y.; Kam, K.L.; Sawadogo, A. Factors Associated with Overweight and Obesity in Children in Ouagadougou (Burkina Faso). Cahiers Santé 2011, 21, 227–231. [Google Scholar] [CrossRef] [PubMed]
- Banaei, M.; Moridi, A.; Dashti, S. Sexual Dysfunction and Its Associated Factors After Delivery: Longitudinal Study in Iranian Women. Mater. Sociomed. 2018, 30, 198–203. [Google Scholar] [CrossRef] [PubMed]
- O’Malley, D.; Higgins, A.; Smith, V. Exploring the Complexities of Postpartum Sexual Health. Curr. Sex. Health. Rep. 2021, 13, 128–135. [Google Scholar] [CrossRef]
- Rahmani, A.; Fallahi, A.; Allahqoli, L.; Grylka-Baeschlin, S.; Alkatout, I. How Do New Mothers Describe Their Postpartum Sexual Quality of Life? A Qualitative Study. BMC Womens Health 2023, 23, 477. [Google Scholar] [CrossRef] [PubMed]
- Buster, J.E. Managing Female Sexual Dysfunction. Fertil. Steril. 2013, 100, 905–915. [Google Scholar] [CrossRef]
- Gutzeit, O.; Levy, G.; Lowenstein, L. Postpartum Female Sexual Function: Risk Factors for Postpartum Sexual Dysfunction. Sex. Med. 2020, 8, 8–13. [Google Scholar] [CrossRef]
- Florkiewicz-Danel, M.; Zaręba, K.; Ciebiera, M.; Jakiel, G. Quality of Life and Sexual Satisfaction in the Early Period of Motherhood-A Cross-Sectional Preliminary Study. J. Clin. Med. 2023, 12. [Google Scholar] [CrossRef]
- Clephane, K.; Lorenz, T.K. Putative Mental, Physical, and Social Mechanisms of Hormonal Influences on Postpartum Sexuality. Curr. Sex. Health. Rep. 2021, 13, 136–148. [Google Scholar] [CrossRef]
- Worsley, R.; Santoro, N.; Miller, K.K.; Parish, S.J.; Davis, S.R. Hormones and Female Sexual Dysfunction: Beyond Estrogens and Androgens—Findings From the Fourth International Consultation on Sexual Medicine. J. Sex. Med. 2016, 13, 283–290. [Google Scholar] [CrossRef]
- Nappi, R.E.; Di Ciaccio, S.; Genazzani, A.D. Prolactin as a Neuroendocrine Clue in Sexual Function of Women across the Reproductive Life Cycle: An Expert Point of View. Gynecol. Endocrinol. 2021, 37, 490–496. [Google Scholar] [CrossRef]
- Rupp, H.A.; James, T.W.; Ketterson, E.D.; Sengelaub, D.R.; Ditzen, B.; Heiman, J.R. Lower Sexual Interest in Postpartum Women: Relationship to Amygdala Activation and Intranasal Oxytocin. Horm. Behav. 2013, 63, 114–121. [Google Scholar] [CrossRef] [PubMed]
- McBride, H.L.; Olson, S.; Kwee, J.; Klein, C.; Smith, K. Women’s Postpartum Sexual Health Program: A Collaborative and Integrated Approach to Restoring Sexual Health in the Postpartum Period. J. Sex. Marital. Ther. 2017, 43, 147–158. [Google Scholar] [CrossRef] [PubMed]
- Alligood-Percoco, N.R.; Kjerulff, K.H.; Repke, J.T. Risk Factors for Dyspareunia After First Childbirth. Obstet. Gynecol. 2016, 128, 512–518. [Google Scholar] [CrossRef] [PubMed]
- Alp Yılmaz, F.; Şener Taplak, A.; Polat, S. Breastfeeding and Sexual Activity and Sexual Quality in Postpartum Women. Breastfeed. Med. 2019, 14, 587–591. [Google Scholar] [CrossRef]
- Heidari, M.; Merghati Khoei, E.; Kiani Asiabar, A.; Khoei, E.M.; Heidari, M. What Happens To Sexuality Of Women During Lactation Period? A Study From Iran. PaK. J. Med. Sci. 2009, 25, 938–943. [Google Scholar]
- Lev-Sagie, A.; Amsalem, H.; Gutman, Y.; Esh-Broder, E.; Daum, H. Prevalence and Characteristics of Postpartum Vulvovaginal Atrophy and Lack of Association With Postpartum Dyspareunia. J. Low. Genit. Tract. Dis. 2020, 24, 411–416. [Google Scholar] [CrossRef]
- Parameshwaran, S.; Chandra, P.S. The New Avatar of Female Sexual Dysfunction in ICD-11—Will It Herald a Better Future? J. Psychosexual Health 2019, 1, 111–113. [Google Scholar] [CrossRef]
- Grussu, P.; Vicini, B.; Quatraro, R.M. Sexuality in the Perinatal Period: A Systematic Review of Reviews and Recommendations for Practice. Sex. Reprod. Health 2021, 30, 100668. [Google Scholar] [CrossRef]
- Neijenhuijs, K.I.; Hooghiemstra, N.; Holtmaat, K.; Aaronson, N.K.; Groenvold, M.; Holzner, B.; Terwee, C.B.; Cuijpers, P.; Verdonck-de Leeuw, I.M. The Female Sexual Function Index (FSFI)—A Systematic Review of Measurement Properties. J. Sex. Med. 2019, 16, 640–660. [Google Scholar] [CrossRef]
- Triviño-Juárez, J.; Romero-Ayuso, D.; Nieto-Pereda, B.; Forjaz, M.J.; Oliver-Barrecheguren, C.; Mellizo-Díaz, S.; Avilés-Gámez, B.; Arruti-Sevilla, B.; Criado-Álvarez, J.; Soto-Lucía, C.; et al. Resumption of Intercourse, Self-reported Decline in Sexual Intercourse and Dyspareunia in Women by Mode of Birth: A Prospective Follow-up Study. J. Adv. Nurs. 2018, 74, 637–650. [Google Scholar] [CrossRef]
- McDonald, E.; Gartland, D.; Small, R.; Brown, S. Dyspareunia and Childbirth: A Prospective Cohort Study. BJOG 2015, 122, 672–679. [Google Scholar] [CrossRef] [PubMed]
- WHO. Indicators for Assessing Infant and Young Child Feeding Practices Definitions and Measurement Methods. Available online: https://www.who.int/publications/i/item/9789240018389 (accessed on 5 October 2024).
- Smetanina, D.; Awar, S. Al; Khair, H.; Alkaabi, M.; Das, K.M.; Ljubisavljevic, M.; Statsenko, Y.; Zaręba, K.T. Risk of Sexual Dysfunctions in Breastfeeding Females: Protocol for a Systematic Review and Meta-Analysis. BMJ Open 2023, 13, e074630. [Google Scholar] [CrossRef] [PubMed]
- Porritt, K.; Gomersall, J.; Lockwood, C. JBI’s Systematic Reviews. AJN, Am. J. Nurs. 2014, 114, 47–52. [Google Scholar] [CrossRef] [PubMed]
- Aghababaei, S.; Refaei, M.; Roshanaei, G.; Rouhani Mahmoodabadi, S.M.; Heshmatian, T. The Effect of Sexual Health Counseling Based on REDI Model on Sexual Function of Lactating Women with Decreased Sexual Desire. Breastfeed. Med. 2020, 15, 731–738. [Google Scholar] [CrossRef]
- Banaei, M.; Torkzahrani, S.; Ozgoli, G.; Azad, M.; Mahmoudikohani, F.; PormehrYabandeh, A. Addressing the Sexual Function of Women During First Six Month After Delivery: Aquasi-Experimental Study. Mater. Sociomed. 2018, 30, 136. [Google Scholar] [CrossRef]
- Malakoti, J.; Zamanzadeh, V.; Maleki, A.; Farshbaf Khalili, A. Sexual Function in Breastfeeding Women in Family Health Centers of Tabriz, Iran, 2012. J. Caring. Sci. 2013, 2, 141–146. [Google Scholar] [CrossRef]
- Mesbahi, A.; Mohammad-Alizadeh-Charandabi, S.; Ghorbani, Z.; Mirghafourvand, M. The Effect of Intra-Vaginal Oxytocin on Sexual Function in Breastfeeding Mothers: A Randomized Triple-Blind Placebo-Controlled Trial. BMC Pregnancy Childbirth 2022, 22, 62. [Google Scholar] [CrossRef]
- Holanda, J.B. de L.; Richter, S.; Campos, R.B.; Trindade, R.F.C. da; Monteiro, J.C. dos S.; Gomes-Sponholz, F.A. Relationship of the Type of Breastfeeding in the Sexual Function of Women. Rev. Lat. Am. Enfermagem. 2021; 29. [Google Scholar] [CrossRef]
- Cappell, J.; Bouchard, K.N.; Chamberlain, S.M.; Byers-Heinlein, A.; Chivers, M.L.; Pukall, C.F. Is Mode of Delivery Associated With Sexual Response? A Pilot Study of Genital and Subjective Sexual Arousal in Primiparous Women With Vaginal or Cesarean Section Births. J. Sex. Med. 2020, 17, 257–272. [Google Scholar] [CrossRef]
- Saotome, T.T.; Yonezawa, K.; Suganuma, N. Sexual Dysfunction and Satisfaction in Japanese Couples During Pregnancy and Postpartum. Sex. Med. 2018, 6, 348–355. [Google Scholar] [CrossRef]
- Alum, A.C.; Kizza, I.B.; Osingada, C.P.; Katende, G.; Kaye, D.K. Factors Associated with Early Resumption of Sexual Intercourse among Postnatal Women in Uganda. Reprod. Health. 2015, 12, 107. [Google Scholar] [CrossRef]
- O’Malley, D.; Higgins, A.; Begley, C.; Daly, D.; Smith, V. Prevalence of and Risk Factors Associated with Sexual Health Issues in Primiparous Women at 6 and 12months Postpartum; A Longitudinal Prospective Cohort Study (the MAMMI Study). BMC Pregnancy Childbirth 2018, 18. [Google Scholar] [CrossRef] [PubMed]
- Rådestad, I.; Olsson, A.; Nissen, E.; Rubertsson, C. Tears in the Vagina, Perineum, Sphincter Ani, and Rectum and First Sexual Intercourse after Childbirth: A Nationwide Follow-Up. Birth 2008, 35, 98–106. [Google Scholar] [CrossRef] [PubMed]
- Rezaei, N.; Azadi, A.; Sayehmiri, K.; Valizadeh, R. Postpartum Sexual Functioning and Its Predicting Factors among Iranian Women. Malays. J. Med. Sci. 2017, 24, 94–103. [Google Scholar] [CrossRef] [PubMed]
- Rosen, N.O.; Dawson, S.J.; Binik, Y.M.; Pierce, M.; Brooks, M.; Pukall, C.; Chorney, J.; Snelgrove-Clarke, E.; George, R. Trajectories of Dyspareunia From Pregnancy to 24 Months Postpartum. Obstet. Gynecol. 2022, 139, 391–399. [Google Scholar] [CrossRef] [PubMed]
- Salamon, N.; Mohd Hashim, S.; Ahmad, N.; Wahab, S.; Malaysia, K.; Yaakob Latiff, J.; Tun Razak, B.; Lumpar, K.; Kesihatan Bandar Miri, K.; Kesihatan Malaysia, K. Sexual Dysfunction Among Women At Four To Six Months Postpartum: A Study In A Primary Care Setting. Malays. J. Public Health Med. 2020, 20, 235–243. [Google Scholar] [CrossRef]
- Signorello, L.B.; Harlow, B.L.; Chekos, A.K.; Repke, J.T. Postpartum Sexual Functioning and Its Relationship to Perineal Trauma: A Retrospective Cohort Study of Primiparous Women. In Proceedings of the American Journal of Obstetrics and Gynecology; Mosby Inc., 2001; Vol. 184, pp. 881–890.
- Triviño-Juárez, J.M.; Romero-Ayuso, D.; Nieto-Pereda, B.; Forjaz, M.J.; Oliver-Barrecheguren, C.; Mellizo-Díaz, S.; Avilés-Gámez, B.; Arruti-Sevilla, B.; Criado-Álvarez, J.J.; Soto-Lucía, C.; et al. Resumption of Intercourse, Self-Reported Decline in Sexual Intercourse and Dyspareunia in Women by Mode of Birth: A Prospective Follow-up Study. J. Adv. Nurs. 2018, 74, 637–650. [Google Scholar] [CrossRef]
- Stone, C.; Smith, J.P. The Visibility of Breastfeeding as a Sexual and Reproductive Health Right: A Review of the Relevant Literature. Int. Breastfeed. J. 2022, 17, 18. [Google Scholar] [CrossRef]
- Sun, S.; Hamilton, F.; Dieter, A.A.; Budd, S.; Getaneh, F. The Effect of Breastfeeding on Postpartum Sexual Function: An Observational Cohort Study. Arch. Gynecol. Obstet. 2024, 1–8. [Google Scholar] [CrossRef]
- Canul-Medina, G.; Fernandez-Mejia, C. Morphological, Hormonal, and Molecular Changes in Different Maternal Tissues during Lactation and Post-Lactation. J. Physiol. Sci. 2019, 69, 825–835. [Google Scholar] [CrossRef]
- Mariman, A.; Hanoulle, I.; Pevernagie, D.; Maertens, S.-J.; Dehaene, I.; Tobback, E.; Delesie, L.; Loccufier, A.; Van Holsbeeck, A.; Moons, L.; et al. Longitudinal Assessment of Sleep and Fatigue According to Baby Feeding Method in Postpartum Women: A Prospective Observational Study. BMC Pregnancy Childbirth 2024, 24, 529. [Google Scholar] [CrossRef]
- Kayner, C.E.; Zagar, J.A. Breast-Feeding and Sexual Response. J Fam Pract 1983, 17, 69–73. [Google Scholar] [PubMed]
- Basson, R. The Female Sexual Response: A Different Model. .J Sex. Marital. Ther. 2000, 26, 51–65. [Google Scholar] [CrossRef] [PubMed]
- Brotto, L.A.; Bitzer, J.; Laan, E.; Leiblum, S.; Luria, M. Women’s Sexual Desire and Arousal Disorders. J. Sex. Med. 2010, 7, 586–614. [Google Scholar] [CrossRef]
- Battin, D.A.; Marrs, R.P.; Fleiss, P.M.; Mishell, D.R. Effect of Suckling on Serum Prolactin, Luteinizing Hormone, Follicle-Stimulating Hormone, and Estradiol during Prolonged Lactation. Obstet. Gynecol. 1985, 65, 785–788. [Google Scholar] [PubMed]
- Pascoal, P.M.; Narciso, I. de S.B.; Pereira, N.M. What Is Sexual Satisfaction? Thematic Analysis of Lay People’s Definitions. J. Sex. Res. 2014, 51, 22–30. [Google Scholar] [CrossRef] [PubMed]
- Józefacka, N.M.; Szpakiewicz, E.; Lech, D.; Guzowski, K.; Kania, G. What Matters in a Relationship—Age, Sexual Satisfaction, Relationship Length, and Interpersonal Closeness as Predictors of Relationship Satisfaction in Young Adults. Int. J. Environ. Res. Public. Health. 2023, 20, 4103. [Google Scholar] [CrossRef]
- Agarwal, S.K.; Kim, J.; Korst, L.M.; Hughes, C.L. Application of the Estrogen Threshold Hypothesis to the Physiologic Hypoestrogenemia of Lactation. Breastfeed. Med. 2015, 10, 77–83. [Google Scholar] [CrossRef]
Figure 1.
PRISMA flowchart and decision-making process for including studies in the analysis.
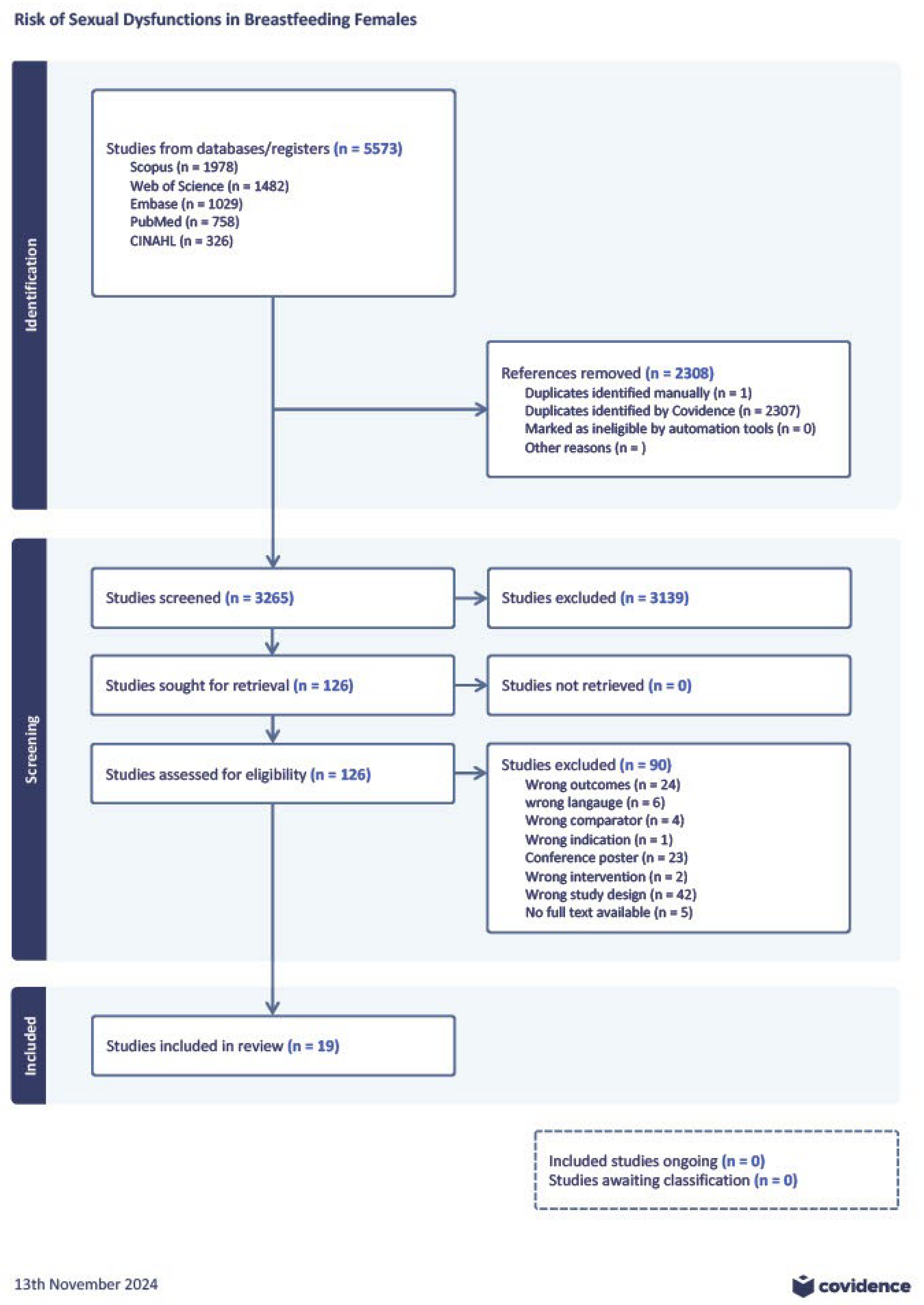
Figure 2.
Desire in women choosing (A) exclusive and (B) complimented breastfeeding.
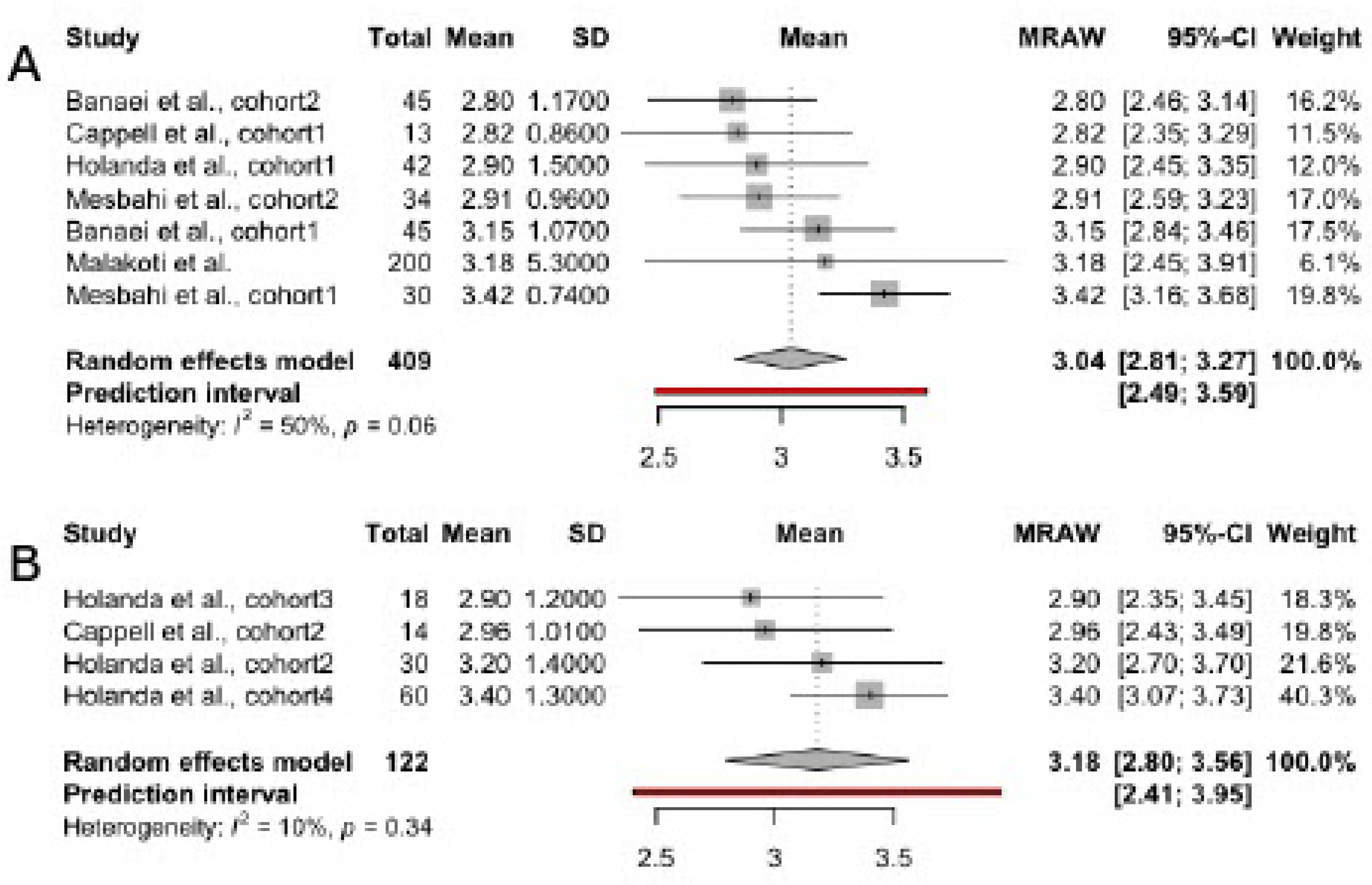
Figure 3.
Arousal in women choosing (A) exclusive and (B) complimented breastfeeding.
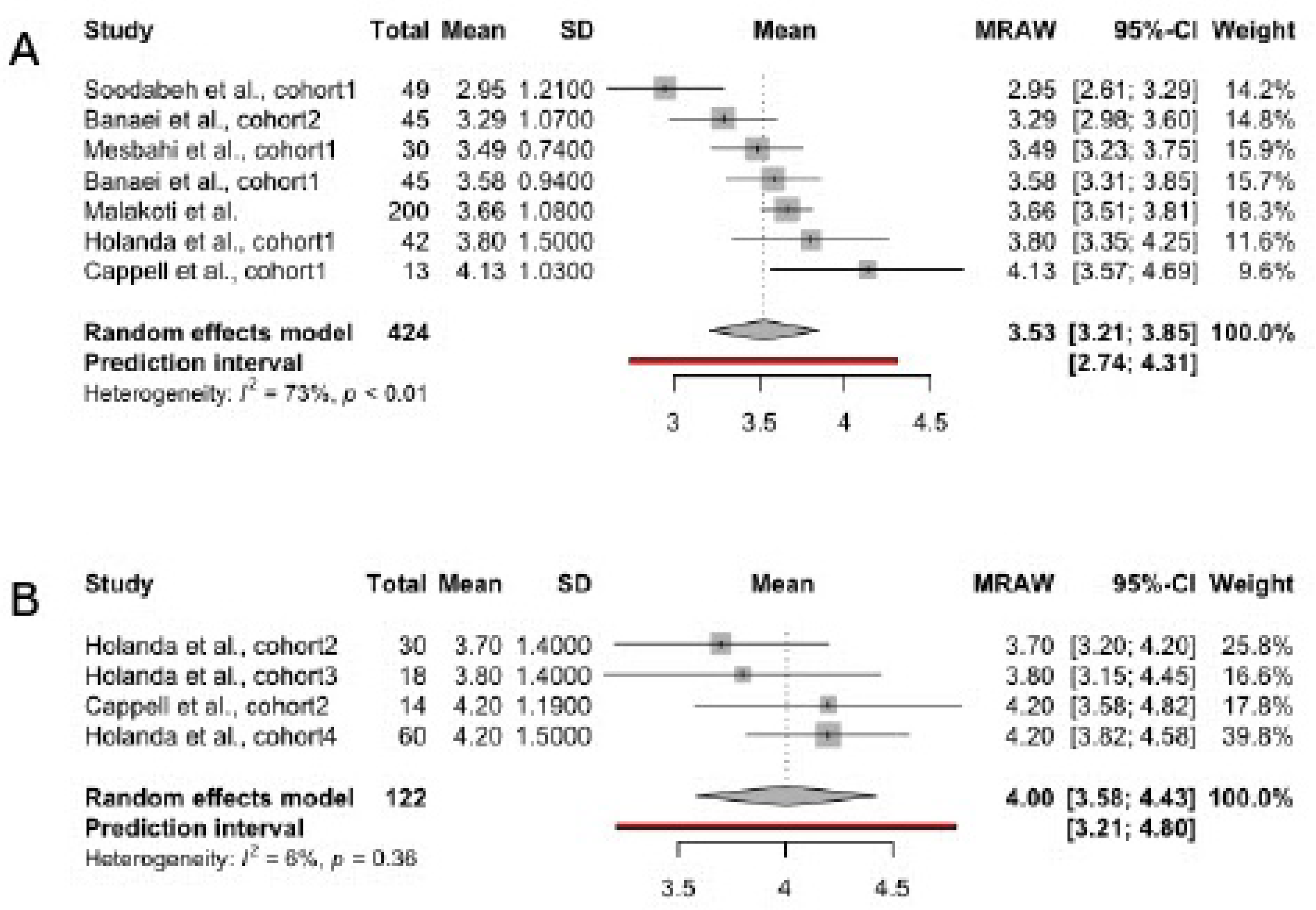
Figure 4.
Orgasm in women choosing (A) exclusive and (B) complimented breastfeeding.
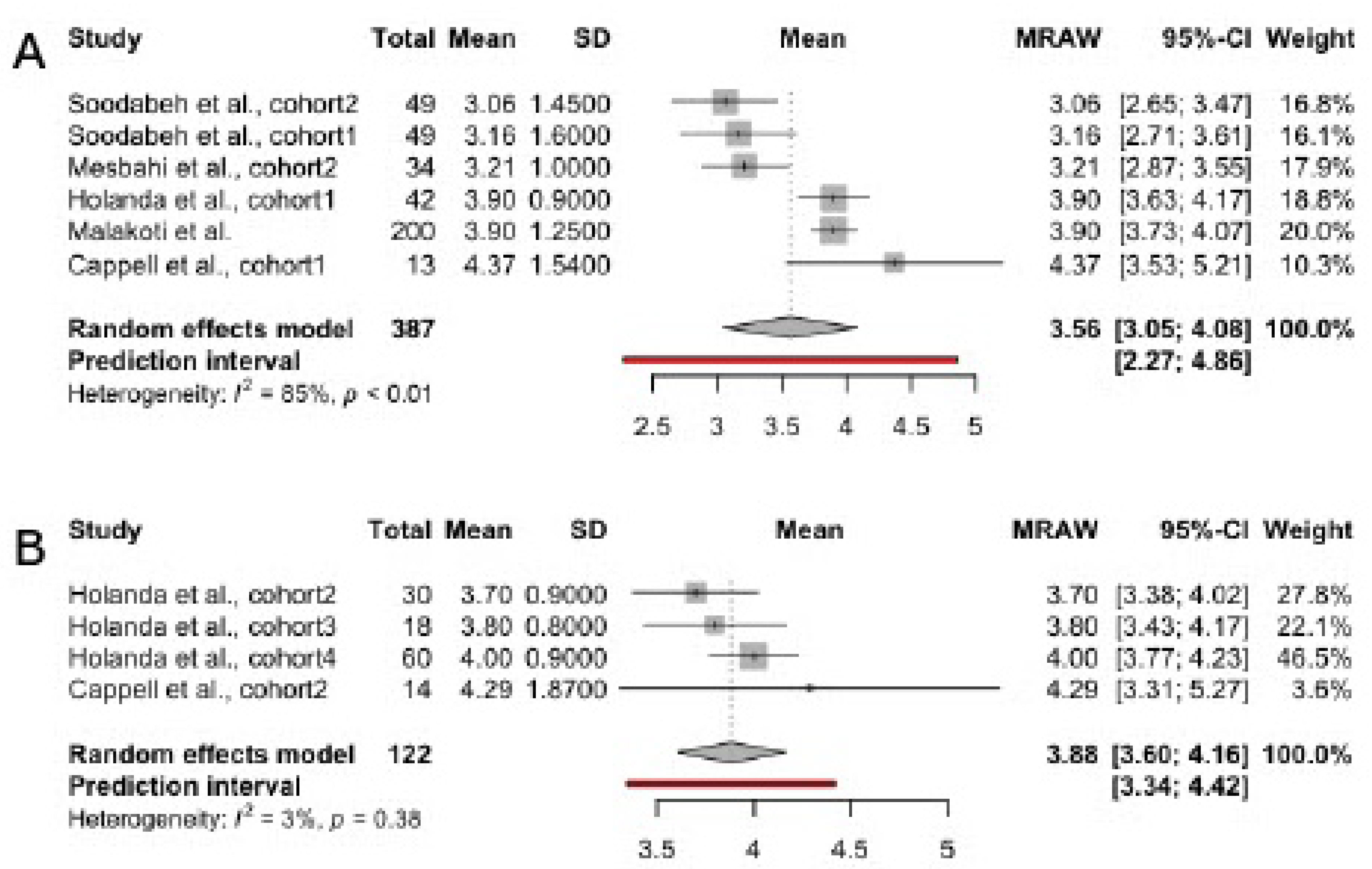
Figure 5.
Lubrication in women choosing (A) exclusive and (B) complimented breastfeeding.
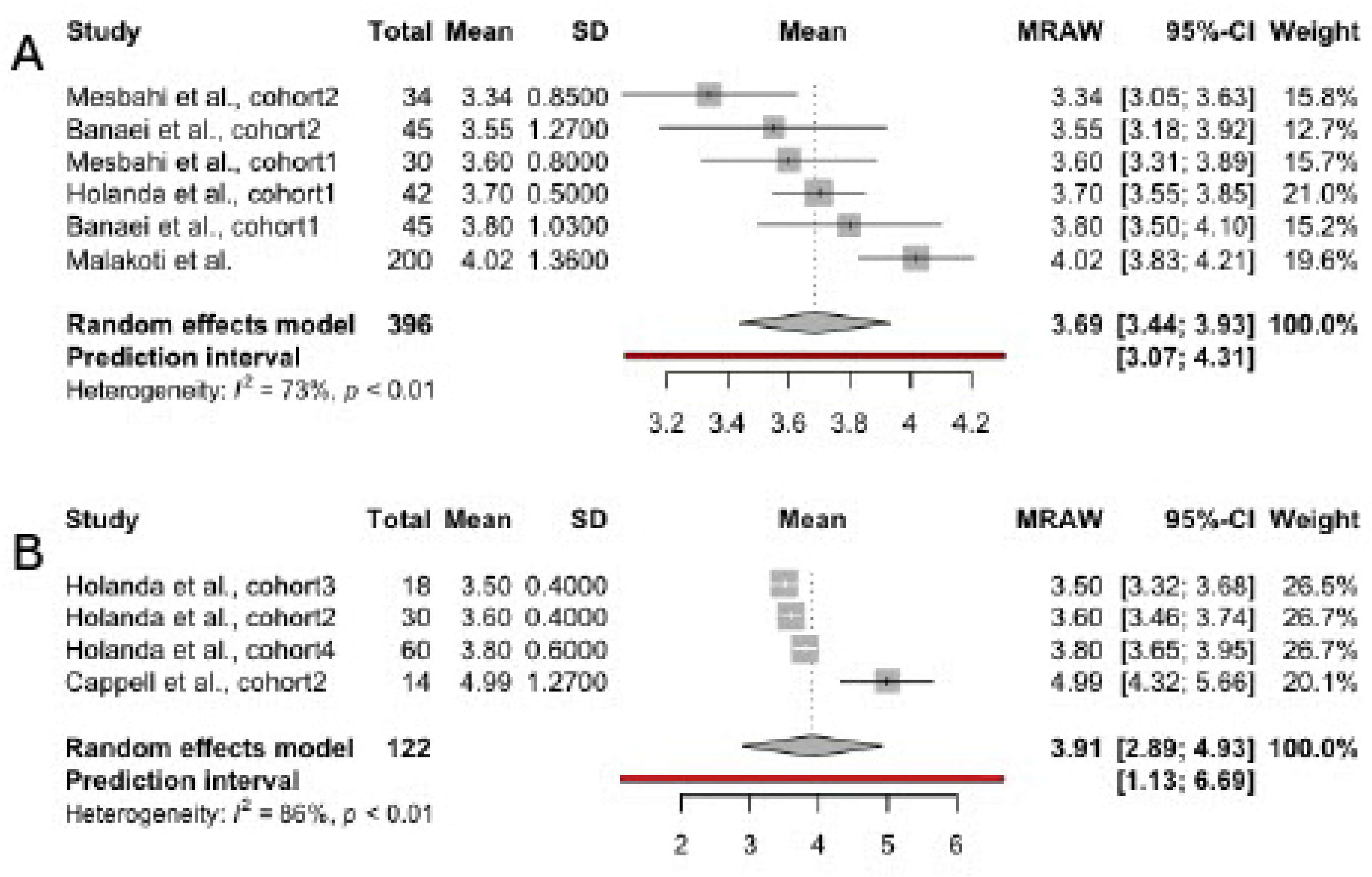
Figure 6.
Pain domain in women choosing (A) exclusive and (B) complimented breastfeeding
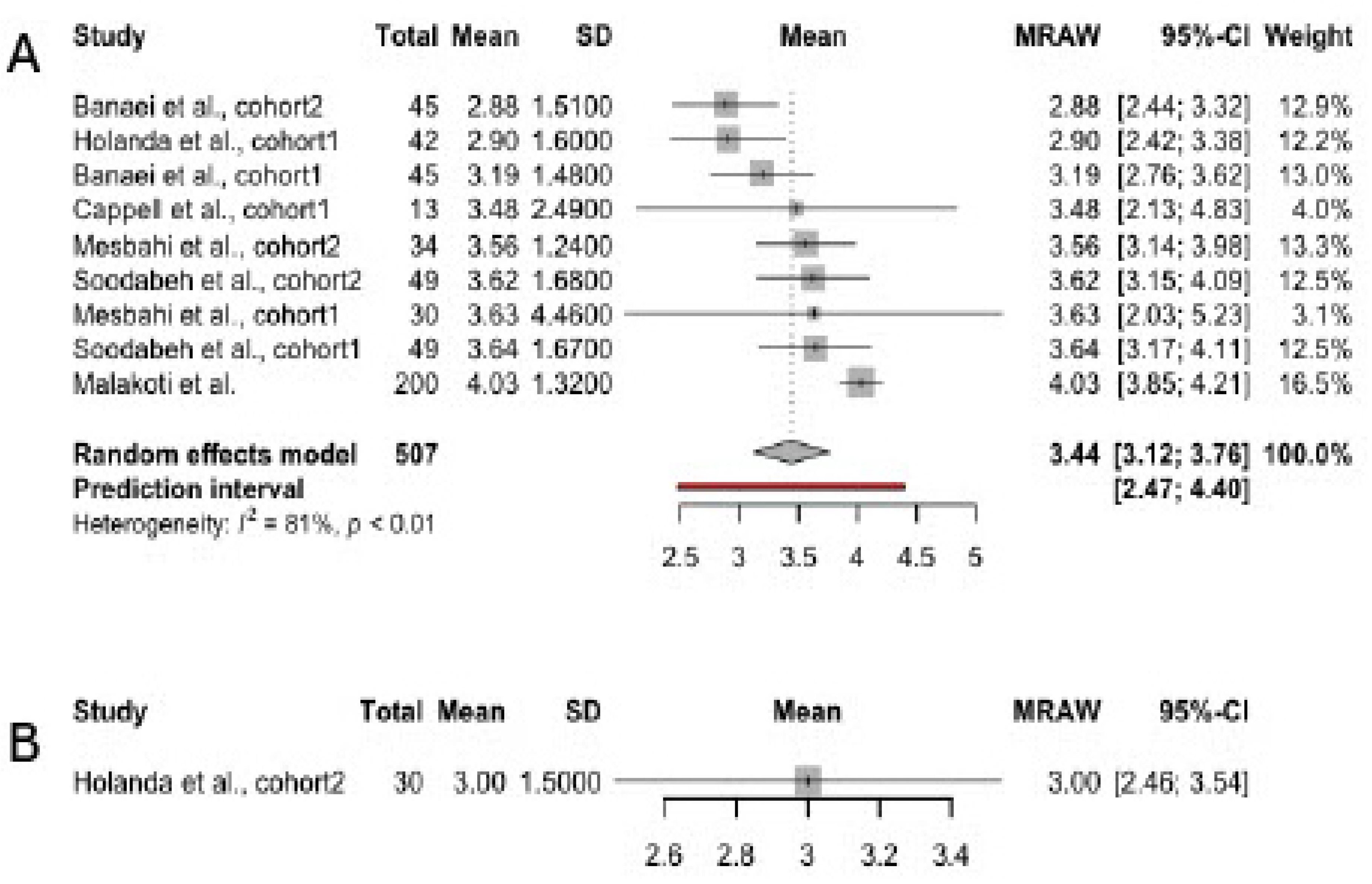
Figure 7.
Satisfaction in women choosing (A) exclusive and (B) complimented breastfeeding.
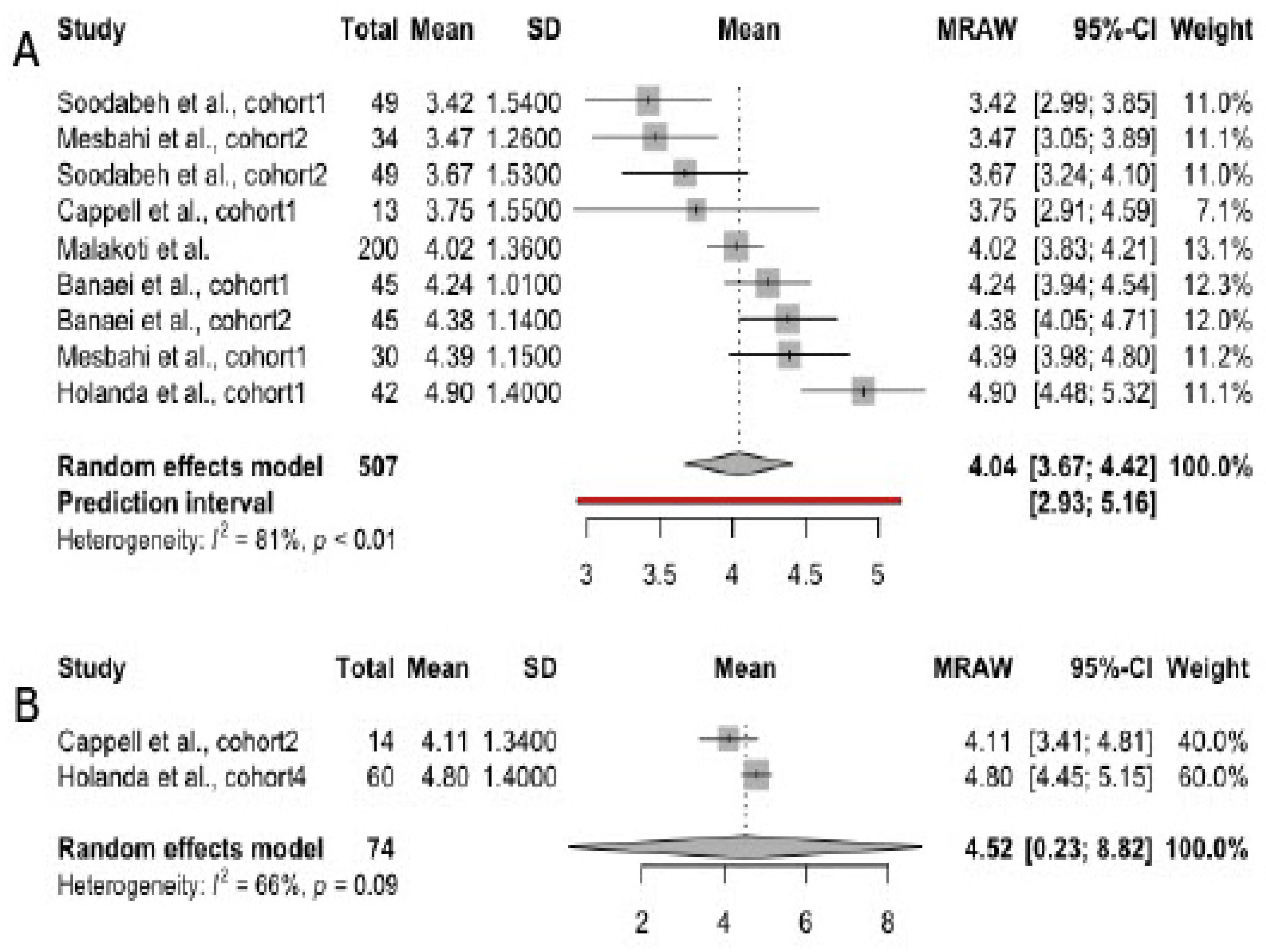
Figure 8.
Satisfaction in women choosing (A) exclusive, (B) complimented breastfeeding and (C) formula
Figure 8.
Satisfaction in women choosing (A) exclusive, (B) complimented breastfeeding and (C) formula
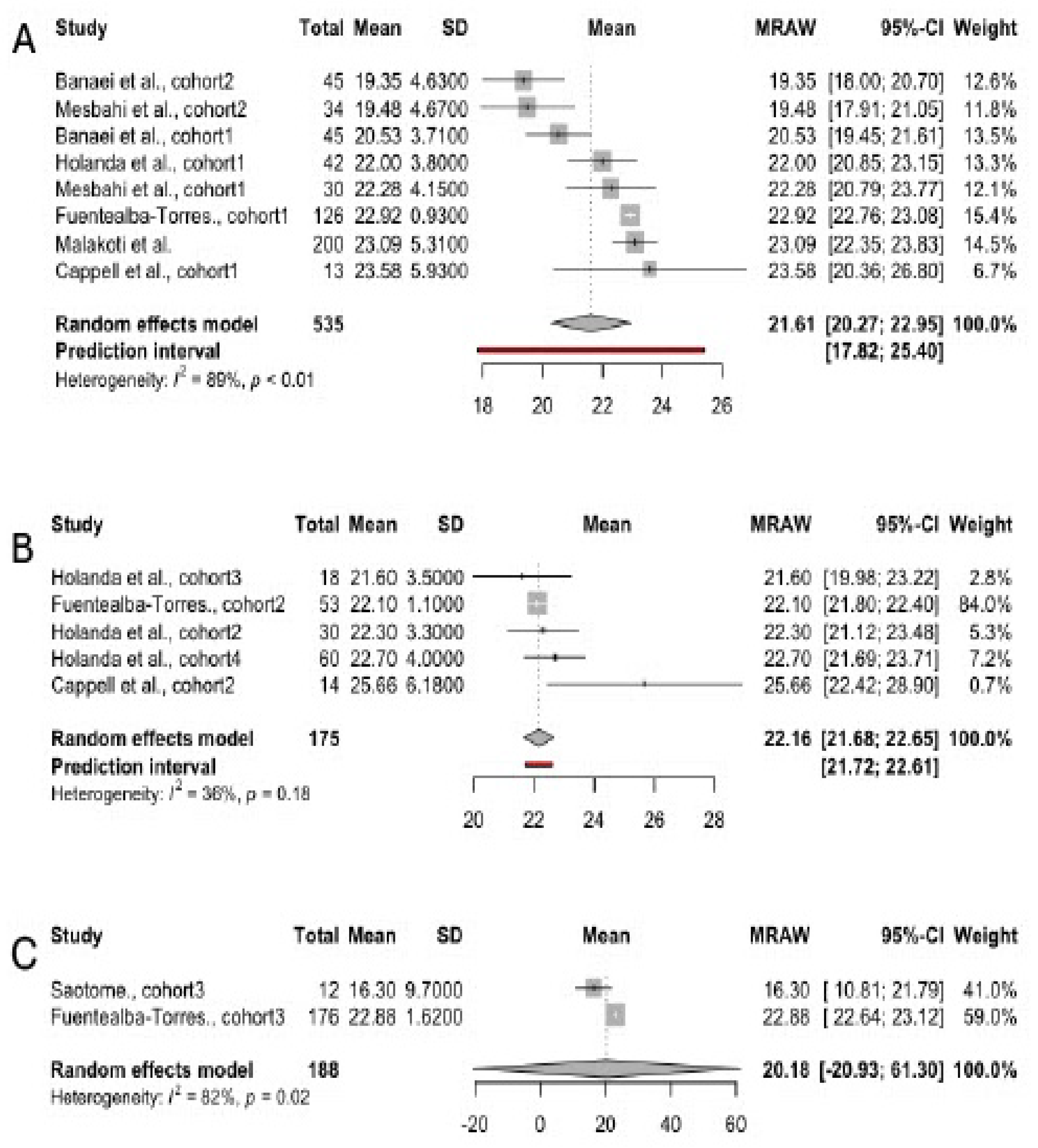

Table 1.
Characteristics of studies included in meta-analysis.
| Author, year | Country | Total sample size | Patient’s age | Time since delivery | Breastfeeding type | Studied FSFI domains |
|---|---|---|---|---|---|---|
| Soodabeh et al., 2020 [37] | Iran | 98 | 29.65±5.66 | 4.12±1.61 months | Exclusive | Total; Libido (desire); Arousal; Lubrication; Orgasm; Satisfaction; Pain |
| Banaei et al., 2018 [38] | Iran | 87 | 24.93±3.10 in the intervention group; 23.44±2.64 in the control group |
3.56±1.58 months in the intervention group; 3.56±1.80 months in the control group; |
Exclusive |
Total; Desire; Arousal; Lubrication; Orgasm; Satisfaction; Pain |
| Cappell et al., 2020 [42] | Canada | 27 | 31.45±4.35 | 310.26± 204.26 days | Exclusive; Not exclusive |
Total; Desire; Arousal; Lubrication; Orgasm; Satisfaction; Pain |
| Fuentealba-Torres et al., 2019[12] | Brazil | 355 | 26.5±6.68 | N/A | Exclusive; Predominant; Complimentary |
Total |
| Holanda et al., 2021 [41] | Brazil | 150 | 24.8±6.4 | 4.3±1.2 | Exclusive; Predominant; Complimented; Mixed | Total; Desire; Arousal; Lubrication; Orgasm; Satisfaction; Pain |
| Malakoti et al. 2013 [39] | Iran | 200 | 27.5±5.2 | 3-6 months | Exclusive | Total; Desire; Arousal; Lubrication; Orgasm; Satisfaction; Pain |
| Mesbahi et al., 2022 [40] | Iran | 64 | 31.2±5.1 in intervention group; 27.8±5.9 in control group | 4.18±1.88 months in intervention group; 3.87± 1.72 in control group | Exclusive | Total; Desire; Arousal; Lubrication; Orgasm; Satisfaction; Pain |
| Saotome et al., 2018 [43] | Japan | 84 | 32.8±4.4 | N/A | Exclusive; mixed; formula | Total |
Table 2.
Characteristics of studies included in the systematic review.
| Author, year | Country | Sample size | Age of participants | Time since delivery | Target condition | Feeding practice | Key findings |
|---|---|---|---|---|---|---|---|
| Alum et al., 2015 [44] | Uganda | 374 | Between 15 to 45 | N/A |
Resumption of sexual intercourse after 6 weeks. | Any type of breastfeeding vs. artificial feeding; Exclusive vs. non-exclusive breastfeeding. |
21.6% of participants resumed intercourse within 6 weeks after giving birth. The early resumption of intercourse was associated with socio-economic factors. |
| Heidari et al., 2009 [27] | Iran | 456 | Between 20 to 35 | 2 – 6 months | Resumption of sexual intercourse after 6 weeks; reduced desire; reduced satisfaction; Not experiencing orgasm. |
Breastfeeding vs. bottle-feeding. | Breastfeeding and bottle-feeding women did not have a significant difference in sexual health postpartum. |
| Lev-Sagie et al., 2020[28] | Israel | 329 | Between 23 to 40 | 3 – 16 weeks | Vulvovaginal atrophy. | Breastfeeding vs. non-breastfeeding (not specified) | Vulvovaginal atrophy was associated with breastfeeding status. |
| O’Malley et al., 2018 [15] | Ireland | 832 | 18 and above | 6 and 12 months | Lack of vaginal lubrication; Loss of interest in sexual activity. |
Breastfeeding vs. non-breastfeeding (not specified). | Breastfeeding and pre-existing dyspareunia were risk factors for issues in sexual health at 6 months postpartum. |
| Radestad et al., 2008 [46] | Sweden | 2342 | 15 and above | 12 months | Intercourse at: over 3 and over 6 months after giving birth. | Breastfeeding at 2 months and 6 months vs. not breastfeeding (not specified). | Breastfeeding women had 1.6 OR of resuming intercourse at over 3 months postpartum. |
| Rezaei et al., 2017[47] | Iran | 380 | 18 and above | 3 – 5 months | Total FSFI score. | Exclusive breastfeeding. |
Exclusive breastfeeding was significantly associated with sexual dysfunction (adjusted OR: 2.47, 95% CI: 1.21 – 5.03). |
| Rosen et al., 2022 [48] | Canada | 582 | 29±4.4 | Up to 2 years | Change from moderate to minimal dyspareunia. | Breastfeeding at 3 months (not specified). | Breastfeeding did not predict a dyspareunia class. |
| Salamon et al., 2020 [49] | Malaysia | 249 | 28.99±6.07 | 4 – 6 months | Overall sexual dysfunction | Breastfeeding (not specified). | Breastfeeding was a risk factor for sexual dysfunction (adjusted OR: 2.24, 95% CI: 1.03 – 4.85). |
| Signorello et al., 2001 [50] | USA | 615 | N/A | 8.1±3.5 weeks; 3 months; 6 months | Pain at the first postpartum sexual intercourse; Pain on sexual intercourse at 3 and 6 months postpartum. | Breastfeeding vs. non-breastfeeding (not specified). | Breastfeeding women were 4 times as likely to experience dyspareunia compared to non-breastfeeding mothers. |
| Triviño-Juárez et al., [51] | Spain | 552 | 32.18±5.36 | 6 weeks | Resumption of sexual intercourse at 6 weeks;Decline in sexual intercourse. | Breastfeeding (not specified). | Breastfeeding was a determinant of dyspareunia. However, nursing was not linked to the resumption of intercourse or a decline in sexual activity. |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



