
Submitted:
04 December 2024
Posted:
05 December 2024
You are already at the latest version
Abstract
Introduction: Risk factors, a 75 year old concept, are instrumental in the management of the general population. Newer biomarkers can explain residual risk and protection from risk. The population needs a new platform to make more comprehensible the importance of managing risk. Biologic age, the number of years left to live, is the platform that will get the attention of patients.
Method: Risk factor odds ratios are used to approximate the years lost to the modifiable risk; calculating a biologic age. Newer biomarkers confirm the predication and can be used to explain the pleomorphic properties of medications and unrealized risk. The biomarkers represent repair, inflammation, immune function, hematologic, clotting factors, metabolic-nutritional, organ maintenance, anthropomorphic, environmental, endothelial function, sleep, co-morbidities, frailty, and the electromagnetic.
Results: A six step method of patient management using biologic age, and biomarkers is presented.
Conclusions: Knowledge of risk factors and therapies to improve risk has increased over the last 75 years. Biologic age is more appropriate in explaining the significance of this knowledge. Appropriate counseling with utilization of Hs-CRP, circulating stem cells, number of co-morbidities, frailty, ECG, pulse wave velocity will improve compliance and personalize care. The six-minute walk should be incorporated into the vital signs due to prognostic significance.
Keywords:
Risk Factors
; Biologic Age
; Biomarkers
; Odds Ratio
; Integrated Risk
; Inflammation
; Repair
; pleomorphic Medications and Unrealized Risk
1. Introduction
The era of risk factors began over 75 years ago in Framingham, Massachusetts. The study was funded to determine the cause of vascular disease, myocardial infarction, strokes, peripheral vascular disease, and other afflictions. By recording health data on the 5209 volunteers (roughly half of the population) risk factors, mortality, and morbidity for vascular disease was recorded. The study Included risk factors of age, sex, glucose intolerance, total serum cholesterol, cigarette smoking, educational level, systolic and diastolic blood pressure, body mass index, physical activity index, pulse pressure, and electrocardiographic left ventricular hypertrophy [1]. Other risk factors were added as discovered over the decades.
Of the thousands of Framingham studies, the study by Terry illustrates the usefulness of risk factors in counseling patients. Their objective was to examine whether midlife cardiovascular risk factors predict survival and survival free of major comorbidities to the age of 85 [2]. Table 1 is from their paper with permission demonstrates the power of risk factors. Age of death of the population studied is represented in Figure 1 again with permission.
The study further demonstrated for men with no risk factors the probability of reaching 85 was 37% whereas if 4 or more risk factors were present the chance fell to 2%. In females the chances were much better, respectively 65% and 14%. Clearly, risk factors can predict the probability of mortality. In order of importance, glucose intolerance is particularly deadly followed by smoking, hypertension, and total cholesterol. The odds ratios are respectively 0.3, 0.47, 0.57, and 0.89. A favorable odds ratio of 2.0 demonstrates the female advantage. Rare patients still escape the prediction with 2% of males and 14% of females reaching 85 despite having 4 risk factors; therefore, other protective factors must be present. These rare patients are a hazard to the general population, demonstrating risk factors failed to predict dire events. The general population believes they too may escape the predicted morbidity and mortality. Risk factors have lost their significance warranting a new approach.
Over the past 75 years patients have been identified and inundated with messages of life style modifications and medications. If risk factors are musical notes, patients have tone deafness. Risk factors have to be replaced by something that is more tangible and understood by all. The concept is described by a previously traditional history and exam documentation. ”The patient appears (older, younger, or stated) age.” Chronological age correlates with your birthday. Biologic age correlates with how long you have to live.
Based on Arias expectation of life [3], a 50 year old male has an expected life time of 30 years. If he has no risk factors his biologic age is identical to his true age. If he has all 4 independent risk factors his expected life expectancy is reduced to 30 years times the odds ratio of the risk factors. Table 2 life expectancy is the source of 30 years selected for the above patient. Life expectancy with risk factors is calculated as (30 years)(0.3)(0.47)(0.57)(0.89) = 2.15 years. At a chronological age of 50, his biologic age is 74.3 with estimated 2.15 years to live.
A female utilizing the risk reducing odds ratio of 2 for being female with the same age and risk factors would have life expectancy of 4.3 years. At age 50 her biologic age is 78.7 years with 4.3 years to live. Patients understand birthdays and years left to live. Patients also understand gambling and probabilities such as odds ratio. Odds do not predict a winner only what is more likely.
This patient may be more inclined to modify lifestyle and take risk reducing medication based on this information. Biologic age should replace risk factors in counseling patients how to manage their health status. Physicians are uncomfortable with assigning a death prediction. This is the likely reason the methodology of Terry was not adopted. Physicians are not making a death prediction only the odds of death unless lifestyle is not changed. Fate is still in the realms of the Cosmos.
Biomarkers, discovered in the last 75 years further refine risk factors, residual risk, and predict mortality [4]. Biomarkers can differentiate members of a population reaching centurion status [5]. In biologic age models, biomarkers can refine risk factors accounting for known protective and harmful factors. The testing should correlate with age, known and evolving risk factors, inflammation, repair mechanisms, life style, genetic pre-dispositions, and co-morbidities.
Longitudinal data providing predictive value of biomarkers is sparse since many of these markers are recently available and initially used in a disease model. Currently these markers at best can be used in advisory role to confirm biologic age prediction based on risk factors. As data is collected over time their predictive value will surpass a risk factor model with the markers providing a personalized prediction. Some markers have a variability being influenced by other environmental influences and may need repeated to achieve a true biomarker profile. Other markers are integrated over a lifetime and thus more predictive of years left to live.
2. Biomarkers and Longevity
The twelve categories below and roughly 30 biomarkers listed in Table 3 pales to the potential number of biomarkers which include 2 million proteins, 300 cell types of 50 trillion cells, 45/46 chromosomes, billions of base pairs, 20,000 genes, signaling hormones, vitamins, minerals, microbiome, and countless electrical impulses and imaging tests. Table 3 is a promising list; covering most biological processes of repair and protection from the environment. Nutrition, sleep, and exercise, the pillars of health, are also represented. The greater the number of co-morbidities increases biologic age [6]. Frailty is also included due to its dire prediction but is not necessarily age dependent and can occur at any age. In females frailty is more predictive than co-morbidities of advanced biologic age [6,7]. Only a handful of potential markers were selected for Table 4
3. Definitions and Realizations of Table 4
Odds = (probability of survival)/(1 - probability of survival)
Odds ratio = odds in one group/odds in unexposed group
Odds ratio approximated from Hazard Ratio - Hazard Ratio/(1+ Hazard Ratio)
Hazard ratio is the hazard rate of one group’s outcome compared to a hazard rate of a control. It represents an instantaneous rate. The separation of survival or mortality curves at a particular time.
Hazard rate is probability of death over an interval -the number of deaths over the interval by the survivors at the beginning of the interval.
The odds ratio for this study was computed from epidemiological papers listed and from the above definitions. All had appropriate confidence intervals. The populations were not identical so these findings are an approximation. The table reveals many interesting aspects of biological markers. The lower the odds ratio the more influence it has on mortality the greater the number of life expectancy years lost. The odds ratios of biologic markers and risk factors suggest the order of significance is pulse wave velocity, diabetes mellitus, less than 290 meters in the six-minute walk, smoking, ECG LVH, hypertension, waist circumference, circulating stem cells, Hs-CRP, followed by the rest.
The electrocardiogram represents integration over the entire lifespan. The changes reflect previous cardiac events and recent and past exposure to hypertension volume excess due to environmental salt, the stiffness of blood vessels from hypertension, inflammation, and nutrition stresses. Pulse wave velocity is also an integration factor over time and incorporates inflammation, nutrition, hypertension, exercise and most of the risk factors into the stiffness of blood vessels, a potent risk for mortality. Similarly, but less predictive of death are the integrative factors of co-morbidities, and coronary artery calcium.
The value of the odds ratio is directing therapy toward the biggest benefits and helps explain the pleomorphic effects of medications. The odds ratio for total cholesterol is .9 which is not particularly deadly. How can you explain the significant mortality benefit of Hmg CoA reductase inhibitor medications if cholesterol is not that deadly? The pleomorphic effects of Statins include lowering Hs-CRP and increasing circulating stem cells with odds ratio respectively of .7 and .61, targeting protective therapies. Colchicine also lowers Hs-CRP, exercise increases circulating stem cells. These therapies need to be added to patients who have residual risk. The biomarker profile of an individual patient will determine biologic age and protective medications.
Diabetes as a risk factor is responsible for most years of life lost, therefore increases biologic age. Sodium–glucose cotransporter 2 inhibitors decreases diabetic risk, preserves kidney function and lowers the inflammatory marker Hs-CRP. The pleomorphic favorable effect on multiple biomarkers requires utilization of this medication to decrease years lost to diabetes. Othe medications are listed in Table 5 that have favorable responses in vascular repair.
4. Method of Management of Patients
1. Determine risk factors age gender and ethnicity
- 50 old year Hispanic male with diabetes, hypertension, smoking, and elevated total cholesterol
2. Determine expected years of life chronological age with no risk factorsTable 3
- 31.9 expected years, chronological age 50 expected age at death 81.9 with no risks
3. Determine the risk factor weighted reduction of expected years due to risk factor odd ratios fromTable 1
- 31.9(.3)(.57)(.47)(.89) = 2.28 years of expected life due to risk factors biologic age is 81.9 – 2.28 = 79.6 years
4. Obtain Biomarker Panel
- Hs-Crp = 4
- Co-morbidity renal insufficiency, sleep apnea, renal insufficiency
- Six minute walk – 300 feet
- Elevated albumin to creatinine and creatinine 2.3
5. Biomarker panel confirms dire expected life of just over two years
6. Develop treatment plan
- Exercise, Hmg CoA reductase inhibitors, spironolactone, Sodium–Glucose transporter 2 Inhibitor, ARB and Clopidogrel (primary prevention due to high risk)
7. Follow-up for compliance and repeat biomarkers for improvement.
- Steady improvements of biomarkers will improve life expectancy.
5. Caveat
In the general population biomarkers are limited to Lipids, Hgba1c, blood count, comprehensive metabolic profile, urinary albumin. The other useful biomarkers are reserved for the diseased populations. For the above method to be applied, the biomarkers listed have to be obtained to confirm the health/unhealthy status of the patient. These same markers need to be followed for trends. Circulating stem cells are a powerful predictor of the effect of age and risk factors; but are generally reserved for oncology patients. Circulating stem cells have strong predictive role in the general population reflecting all of the risk factors. This testing should be made available.
6. Conclusions
Knowledge of risk factors and therapies to improve risk has increased over the last 75 years. Biologic age is more appropriate in explaining the significance of this knowledge. Odd ratio suggests which risk factors are more deadly. Biomarkers of fundamental processes such as repair and inflammation can further refine biologic age. Utilization of Hs-CRP, circulating stem cells directly reflects the risk factors. Medications can alter risk factors and processes of repair and inflammation. Selecting medications based on this knowledge should extend the biologic age. In addition, the number of co-morbidities, frailty, ECG findings, pulse wave velocity can indicate shorter biologic age. The six-minute walk with strong predictive value should be incorporated into the vital signs.
Author Contributions
Philip Houck M.D. was the sole author responsible for conceptualization, writing—original draft preparation, and review and editing. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
No patients were utilized in the review requiring Institutional Review Board Statement and approval. Ethical review and approval were not required for this study due to no utilization of patients.
Informed Consent Statement
No consent was required; not applicable for studies not involving humans.
Data Availability Statement
No new data was created.
Conflicts of Interest
The author declare no conflicts of interest.
References
- Dawber, T.R.; Meadors, G.F.; Moore, F. E Jr. Epidemiological approaches to heart disease: the Framingham Study. Am J Public Health Nations Health. 1951, 41, 279–81. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Terry, D.F.; Pencina, M.J.; Vasan, R.S.; Murabito, J.M.; Wolf, P.A.; Hayes, M.K.; Levy, D.; D'Agostino, R.B.; Benjamin, E.J. Cardiovascular risk factors predictive for survival and morbidity-free survival in the oldest-old Framingham Heart Study participants. J Am Geriatr Soc. 2005, 53, 1944–50. [Google Scholar] [CrossRef] [PubMed]
- Arias, E.; Heron, M.; Xu, J. United States Life Tables, 2012. Natl Vital Stat Rep. 2016, 65, 1–65. [Google Scholar] [PubMed]
- Härkänen T, Kuulasmaa K, Sares-Jäske L, et al Estimating expected life-years and risk factor associations with mortality in Finland: cohort study. BMJ Open 2020, 10, e033741. [CrossRef]
- Murata, S.; Ebeling, M.; Meyer, A.C.; et al. Blood biomarker profiles and exceptional longevity: comparison of centenarians and non-centenarians in a 35-year follow-up of the Swedish AMORIS cohort. GeroScience 2024, 46, 1693–1702. [Google Scholar] [CrossRef]
- Schoenborn, N.L.; Blackford, A.L.; Joshu, C.E.; Boyd, C.M.; Varadhan, R. Life expectancy estimates based on comorbidities and frailty to inform preventive care. J Am Geriatr Soc. 2022, 70, 99–109. [Google Scholar] [CrossRef]
- Veronese, N. Frailty as cardiovascular risk factor (and vice versa). Frailty and Cardiovascular Diseases: Research into an Elderly Population. 2020:51-4.
- Yazdanyar, A.; Aziz, M.M.; Enright, P.L.; Edmundowicz, D.; Boudreau, R.; Sutton-Tyrell, K.; Kuller, L.; Newman, A.B. Association Between 6-Minute Walk Test and All-Cause Mortality, Coronary Heart Disease-Specific Mortality, and Incident Coronary Heart Disease. J Aging Health. 2014, 26, 583–599. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Tang, Y.; Liang, P.; Chen, J.; Fu, S.; Liu, B.; Feng, M.; Lin, B.; Lee, B.; Xu, A.; Lan, H.Y. The baseline levels and risk factors for high-sensitive C-reactive protein in Chinese healthy population. Immunity & Ageing. 2018, 15, 1–8. [Google Scholar]
- Van Zant, G.; Liang, Y. The role of stem cells in aging. Experimental hematology. 2003, 31, 659–72. [Google Scholar] [CrossRef]
- Fadini, G.P.; Mehta, A.; Dhindsa, D.S.; Bonora, B.M.; Sreejit, G.; Nagareddy, P.; Quyyumi, A.A. Circulating stem cells and cardiovascular outcomes: from basic science to the clinic. Eur Heart J. 2020, 41, 4271–4282. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Patel, R.S.; Li, Q.; Ghasemzadeh, N.; Eapen, D.J.; Moss, L.D.; Janjua, A.U.; Manocha, P.; Al Kassem, H.; Veledar, E.; Samady, H.; Taylor, W.R. Circulating CD34+ progenitor cells and risk of mortality in a population with coronary artery disease. Circulation research. 2015, 116, 289–97. [Google Scholar] [CrossRef] [PubMed]
- Vasa, M.; Fichtlscherer, S.; Aicher, A.; Adler, K.; Urbich, C.; Martin, H. , et al. Number and migratory activity of circulating endothelial progenitor cells inversely correlate with risk factors for coronary artery disease. Circ Res. 2001, 89, E1–7. [Google Scholar] [PubMed]
- Heiss, C.; Keymel, S.; Niesler, U.; Ziemann, J.; Kelm, M.; Kalka, C. Impaired progenitor cell activity in age-related endothelial dysfunction. J Am Coll Cardiol. 2005, 45, 1441–8. [Google Scholar] [CrossRef] [PubMed]
- Werner, N.; Kosiol, S.; Schiegl, T.; Ahlers, P.; Walenta, K.; Link, A. , et al. Circulating endothelial progenitor cells and cardiovascular outcomes. N Engl J Med. 2005, 353, 999–1007. [Google Scholar] [PubMed]
- Cerhan, J.R.; Moore, S.C.; Jacobs, E.J.; Kitahara, C.M.; Rosenberg, P.S.; Adami, H.O.; Ebbert, J.O.; English, D.R.; Gapstur, S.M.; Giles, G.G.; Horn-Ross, P.L. A pooled analysis of waist circumference and mortality in 650,000 adults. In Mayo Clinic Proceedings 2014, 89, 335–345. [Google Scholar] [CrossRef]
- Elsevier. Stevens J, Katz EG, Huxley RR. Associations between gender, age and waist circumference. European journal of clinical nutrition. 2010, 64, 6–15.
- Raggi, P.; Gongora, M.; Gopal, A.; et al. Coronary Artery Calcium to Predict All-Cause Mortality in Elderly Men and Women. JACC. 2008, 52, 17–2. [Google Scholar] [CrossRef]
- Gallicchio, L.; Kalesan, B. Sleep duration and mortality: a systematic review and meta-analysis. J Sleep Res 2009, 18, 148–58. [Google Scholar] [CrossRef]
- Åkerstedt, T.; Ghilotti, F.; Grotta, A.; Bellavia, A.; Lagerros, Y.T.; Bellocco, R. Sleep duration, mortality and the influence of age. European journal of epidemiology. 2017, 32, 881–91. [Google Scholar] [CrossRef]
- Sequi-Dominguez, I.; Cavero-Redondo, I.; Alvarez-Bueno, C.; Pozuelo-Carrascosa, D.P.; Nunez de Arenas-Arroyo, S.; Martinez-Vizcaino, V. Accuracy of pulse wave velocity predicting cardiovascular and all-cause mortality. A systematic review and meta-analysis. Journal of clinical medicine. 2020, 9, 2080. [Google Scholar]
- Lee, S.H.; Lee, M.Y.; Kang, J.; Choi, H.I.; Lee, S.J.; Lee, J.Y.; Kim, B.J.; Sung, K.C.; Park, K.M. Association Between ECG Abnormalities and Mortality in a Low-Risk Population. J Am Heart Assoc. 2024, 13, e033306. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Mahemuti, N.; Zou, J.; Liu, C.; Xiao, Z.; Liang, F.; Yang, X. Urinary Albumin-to-Creatinine Ratio in Normal Range, Cardiovascular Health, and All-Cause Mortality. JAMA Netw Open. 2023, 6, e2348333. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Inoue, K.; Streja, E.; Tsujimoto, T.; Kobayashi, H. Urinary albumin-to-creatinine ratio within normal range and all-cause or cardiovascular mortality among U. S. adults enrolled in the NHANES during 1999-2015. Ann Epidemiol. 2021, 55, 15–23. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Rehman, J.; Li, J.; Parvathaneni, L.; Karlsson, G.; Panchal, V.R.; Temm, C.J. , et al. Exercise acutely increases circulating endothelial progenitor cells and monocyte-/macrophage-derived angiogenic cells. J AmColl Cardiol. 2004, 43, 2314–8. [Google Scholar]
- Laufs, U.; Werner, N.; Link, A.; Endres, M.; Wassmann, S.; Jürgens, K. , et al. Physical training increases endothelial progenitor cells, inhibits neointima formation and enhances angiogensis. Circulation. 2004, 109, 220–6. [Google Scholar]
- Dimmeler, S.; Aicher, A.; Vasa, M.; Mildner-Rihm, C.; Adler, K.; Tiemann, M. , et al. HMG-CoA reductase inhibitors (statins) increase endothelial progenitor cells via the PI 3-kinase/Akt pathway. J Clin Invest. 2001, 108, 391–7. [Google Scholar]
- Lin, M.; Heizati, M.; Wang, L.; Nurula, M.; Yang, Z.; Wang, Z.; Abudoyreyimu, R.; Wu, Z.; Li, N. A systematic review and meta-analysis of effects of spironolactone on blood pressure, glucose, lipids, renal function, fibrosis and inflammation in patients with hypertension and diabetes. Blood Pressure. 2021, 30, 145–53. [Google Scholar] [CrossRef]
- Marumo, T.; Uchimura, H.; Hayashi, M.; Hishikawa, K.; Fujita, T. Aldosterone Impairs Bone Marrow–Derived Progenitor Cell Formation. Hypertension. 2006, 48, 490–6. [Google Scholar] [CrossRef]
- Hajsadeghi, S.; Chitsazan, M.; Chitsazan, M.; Salehi, N.; Amin, A.; Maleki, M.; Babaali, N.; Abdi, S.; Mohsenian, M. Changes of high sensitivity c-reactive protein during clopidogrel therapy in patients undergoing percutaneous coronary intervention. Research in Cardiovascular Medicine. 2016, 5, 1–6. [Google Scholar] [CrossRef]
- Klein, H.H.; Krekel, N.; Kreuzer, J.; Fichtlscherer, S.; Schirmer, A.; Paar, W.D.; Hamm, C.W. Influence of the angiotensin converting enzyme inhibitor ramipril on high-sensitivity C-reactive protein (hs-CRP) in patients with documented atherosclerosis. Clinical Research in Cardiology. 2005, 94, 336–42. [Google Scholar]
- Mubarok, M.I.; Rochmanti, M.; Yusuf, M.; Thaha, M. The Anti-Inflammatory Effect of ACE-I/ARBs Drug on hs-CRP and HDL-Cholesterol in CKD Patient. Indian Journal of Forensic Medicine & Toxicology. 2021, 15, 3743–50. [Google Scholar]
- Cassano, V.; Armentaro, G.; Magurno, M.; Aiello, V.; Borrello, F.; Miceli, S.; Maio, R.; Perticone, M.; Marra, A.M.; Cittadini, A.; Hribal, M.L. Short-term effect of sacubitril/valsartan on endothelial dysfunction and arterial stiffness in patients with chronic heart failure. Frontiers in Pharmacology. 2022, 13, 1069828. [Google Scholar] [CrossRef] [PubMed]
- Wang, D.; Liu, J.; Zhong, L.; Li, S.; Zhou, L.; Zhang, Q.; Li, M.; Xiao, X. The effect of sodium-glucose cotransporter 2 inhibitors on biomarkers of inflammation: A systematic review and meta-analysis of randomized controlled trials. Frontiers in Pharmacology 2022, 13, 1045235. [Google Scholar] [CrossRef] [PubMed]
- Hattori, S. Anti-inflammatory effects of empagliflozin in patients with type 2 diabetes and insulin resistance. Diabetol Metab Syndr. 2018, 10, 93. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Durante, W.; Behnammanesh, G.; Peyton, K.J. Effects of sodium-glucose co-transporter 2 inhibitors on vascular cell function and arterial remodeling. International journal of molecular sciences. 2021, 22, 8786. [Google Scholar] [CrossRef]
Figure 1.
Age of Death in Population - with permission - Terry DF, Pencina MJ, Vasan RS, Murabito JM, Wolf PA, Hayes MK, Levy D, D'Agostino RB, Benjamin EJ. Cardiovascular risk factors predictive for survival and morbidity-free survival in the oldest-old Framingham Heart Study participants. J Am Geriatr Soc. 2005 Nov;53, 1944-50. doi: 10.1111/j.1532-5415.2005.00465.x. PMID: 16274376.
Figure 1.
Age of Death in Population - with permission - Terry DF, Pencina MJ, Vasan RS, Murabito JM, Wolf PA, Hayes MK, Levy D, D'Agostino RB, Benjamin EJ. Cardiovascular risk factors predictive for survival and morbidity-free survival in the oldest-old Framingham Heart Study participants. J Am Geriatr Soc. 2005 Nov;53, 1944-50. doi: 10.1111/j.1532-5415.2005.00465.x. PMID: 16274376.
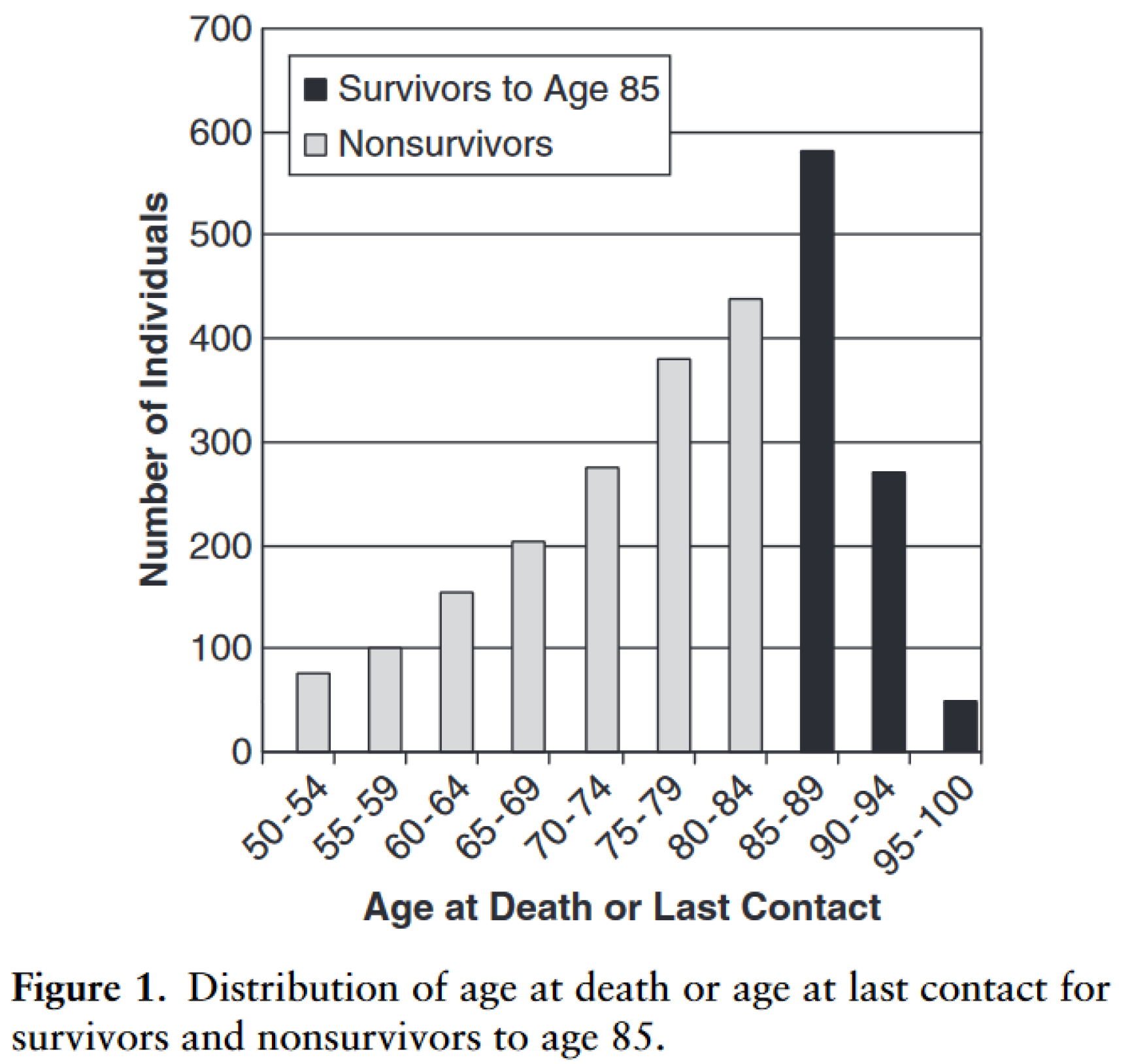

Table 1.
Odds Ratios with permission - Terry DF, Pencina MJ, Vasan RS, Murabito JM, Wolf PA, Hayes MK, Levy D, D'Agostino RB, Benjamin EJ. Cardiovascular risk factors predictive for survival and morbidity-free survival in the oldest-old Framingham Heart Study participants. J Am Geriatr Soc. 2005 Nov;53, 1944-50. doi: 10.1111/j.1532-5415.2005.00465.x. PMID: 16274376.
Table 1.
Odds Ratios with permission - Terry DF, Pencina MJ, Vasan RS, Murabito JM, Wolf PA, Hayes MK, Levy D, D'Agostino RB, Benjamin EJ. Cardiovascular risk factors predictive for survival and morbidity-free survival in the oldest-old Framingham Heart Study participants. J Am Geriatr Soc. 2005 Nov;53, 1944-50. doi: 10.1111/j.1532-5415.2005.00465.x. PMID: 16274376.
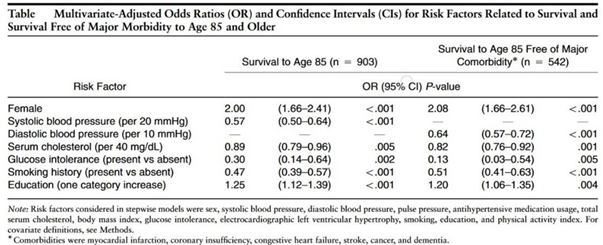 |
Table 2.
Life expectancy adapted from Arias E, Heron M, Xu J. United States Life Tables, 2012. Natl Vital Stat Rep. 2016 Nov;65, 1-65. PMID: 27906644.
Table 2.
Life expectancy adapted from Arias E, Heron M, Xu J. United States Life Tables, 2012. Natl Vital Stat Rep. 2016 Nov;65, 1-65. PMID: 27906644.
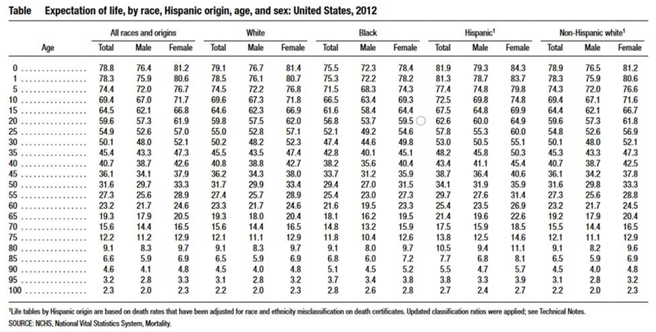 |
Table 3.
List of Biologic Processes and Biomarkers.
| Repair | Number of Progenitor cells | Type of Progenitor Cells | ||
|---|---|---|---|---|
| Inflammation and Immune Function | Hs-CRP interleukin-6 tumor necrosis factor-alpha (TNF-α) | CBC - red cell diameter width lymphocyte to neutrophil ratio | ||
| Hematologic and Clotting Factors | Clonal hematopoiesis polycythemia | clotting factors D-dimer | ||
| Metabolic Nutritional | HgbA1c glucose | albumin albuminuria | Lipids Lipoprotein a |
CBC- minimum corpuscular volume, red cell count |
| Organ Maintenance | Creatinine Cystatin C | Urinary albumin-to-creatinine ratio | liver enzymes | BNP |
| Anthropomorphic | Body Mass Index | waist circumference | ||
| Environmental Factors | Educational Status | Social Economic | Nutritional intake | Minutes of daily exercise |
| Endothelial function | Coronary Artery Calcium | Pulse Wave Velocities | endothelial progenitor cells | |
| Sleep | Quantity | Rapid Eye Movement sleep | ||
| Number of Co-Morbidities | CAD, PVD, CVD CRI, COPD, Liver disease # |
Sleep apnea | ||
| Frailty | Six-Minute Walk | Hand Grip Strength | ||
| Electromagnetic | ECG |
Table 4.
Biomarkers and All-Cause Mortality.
| Biomarker | Change with Age | Mortality Prediction | ODDs Ratio Of All Cause Mortality | Correlation With Risk Factors | Integrated over Years Lived | Ref |
|---|---|---|---|---|---|---|
| Number of Co-Morbidities | Increases | yes | .89 – men 1.0 - women |
yes | yes | [6] |
| Frailty | Not Age Dependent | yes | .84 – men .88 - women |
yes | [6,7] | |
| Six-Minute Walk distance | Decreases | yes | >414 to <290 1.0 to .37 |
[8] | ||
| Hs-CRP>2.0 | Increases | yes | .7 | yes | [9] | |
| Circulating Stem Cells | Decreases | yes | .61 | yes | [10,11,12,13,14,15] | |
| Waist Circumference | Increases | yes | .60 –men .64 - women |
yes | [16,17] | |
| Coronary Artery Calcium 400 | Increases | yes | .9 | no | yes | [18] |
| Short Sleep <7 Long Sleep |
Increases < 65 years | Yes U shaped | .9 | [19,20] | ||
| Pulse Wave Velocity | Increases | Yes | .16 | Yes | Yes | [21] |
| ECG Findings RAE LAE LVH |
No |
Yes Yes Yes |
.67 .63 .53 |
yes | yes | [22] |
Table 5.
Medications or Interventions with favorable endothelial improvement.
| Medication Intervention | Lowers Hs-CRP | Increases Stem cells | Anti-fibrotic | Ref |
|---|---|---|---|---|
| Exercise | Yes | Yes | [25,26] | |
| HMG CoA Reductase Inhibitors | Yes | Yes | [27] | |
| Aldosterone inhibitor | Yes | Yes | Yes | [28,29] |
| Clopidogrel | Yes | Yes | [30] | |
| ACEI ARB ARNI | yes | Yes | [31,32,33] | |
| Sodium–Glucose Co-transporter 2 Inhibitor | yes | Yes | [34,35,36] |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



