Submitted:
04 December 2024
Posted:
05 December 2024
You are already at the latest version
Abstract
Pioglitazone (ACTOS) is a thiazolidinedione for peroxisome proliferator–activated receptor γ (PPARγ) that has been well established for the second or third line treatment of type 2 diabetes mellitus. Beyond the effects on glucose metabolism, pioglitazone displays positive effects on lipid metabolism, blood pressure, endothelial function, bone density and apoptosis of cancer cells. In fact, according to in vitro experiments and preclinical studies, PPARγ ligand is currently considered a potential target for both chemoprevention and cancer therapy. PPARγ ligands are known to inhibit cancer cell proliferation and metastasis through terminal differentiation and underexpression of inflammatory mediators. Despite its anticancer properties, pioglitazone was withdrawn by the national medicine agencies of France and Germany, due to reports of increased incidence of bladder cancer. These reports were associated with European populations undergoing higher doses and longer duration of treatment. In this review we discuss the pharmacokinetics, therapeutic potential and limitations regarding the clinical use of pioglitazone, with a focus on cancer treatment.
Keywords:
pioglitazone
; cancer
; type 2 diabetes
1. Introduction
Thiazolidinediones (TZDs) are a class of oral hypoglycemic agents for the management of diabetes. TZDs are ligands for PPAR α and γ, a member of the nuclear receptor family which regulates glucose and lipid metabolism, inflammation and cell proliferation [1,2,3]. PPARs are classified into three subtypes: PPARα, PPARβ/δ, and PPARγ. Specifically, PPARα receptors are expressed in the heart, liver, skeletal muscle, while PPARγ receptors are expressed in adipose tissue. The former regulate fatty acid oxidation followed by decreased low-density lipoprotein cholesterol (LDL-C) and in-creased high-density lipoprotein cholesterol (HDL-C) levels, while the latter regulate cell differentiation, leptin expression and insulin sensitivity [4,5]. As a result, TZDs find therapeutic application in the treatment of type 2 diabetes mellitus (T2DM) as well as non-alcoholic fatty liver disease (NASH) and multiple types of cancer [6,7].
Initially approved by the FDA in 1999, pioglitazone is marketed under the brand name ACTOS by Takeda Pharmaceuticals. It has been established as a second or third-line treatment for the management of T2DM, when first-line treatment with metformin is inadequate [8,9]. In this scenario metformin is combined with sulfonylureas, glinides, alpha-glucosidase inhibitors, insulin, glucagon-like peptide-1 receptor agonist, dipeptidylpeptidase 4 inhibitors, sodium-glucose co-transporter 2 inhibitors, and thiazolidinediones, such as pioglitazone [10]. Pioglitazone is typically administered orally, with the optimal dose customized based on clinical status. According to the European Medicines Agency (EMA) recommendations, initial dose ranges from 15 to 45 mg once daily. The dose may be increased if inadequate glycemic control is achieved. Alternatively, it may need to be decreased if the patient is receiving pioglitazone along with other diabetes medications (insulin, chlorpropamide, glibenclamide, gliclazide, tolbutamide). The tablets should be administered once a day with water, either with or without food. After three to six months, patients should be evaluated and treatment discontinued if considered non-beneficial [11].
However, despite its effectiveness in enhancing glycemic control, there have been concerns raised about its safety profile, one of which is regarding increased bladder can-cer risk. Notably, indications of a higher incidence of bladder cancer among pioglitazone users prompted the French and German pharmaceutical regulators to withdraw the medication from the market in May 2011. Nevertheless, the medicine remained available throughout the rest of Europe [12].
The aim of this literature review is to thoroughly evaluate pioglitazone's safety profile and efficacy, with an emphasis on its association with bladder cancer. This re-view summarizes clinical data, epidemiological studies, and regulatory recommendations in an effort to evaluate the risk-benefit ratio of pioglitazone. Its evaluation will shed light into current clinical practice and direct future studies to explore the multiple therapeutic applications of pioglitazone.
2. Overview of Pioglitazone
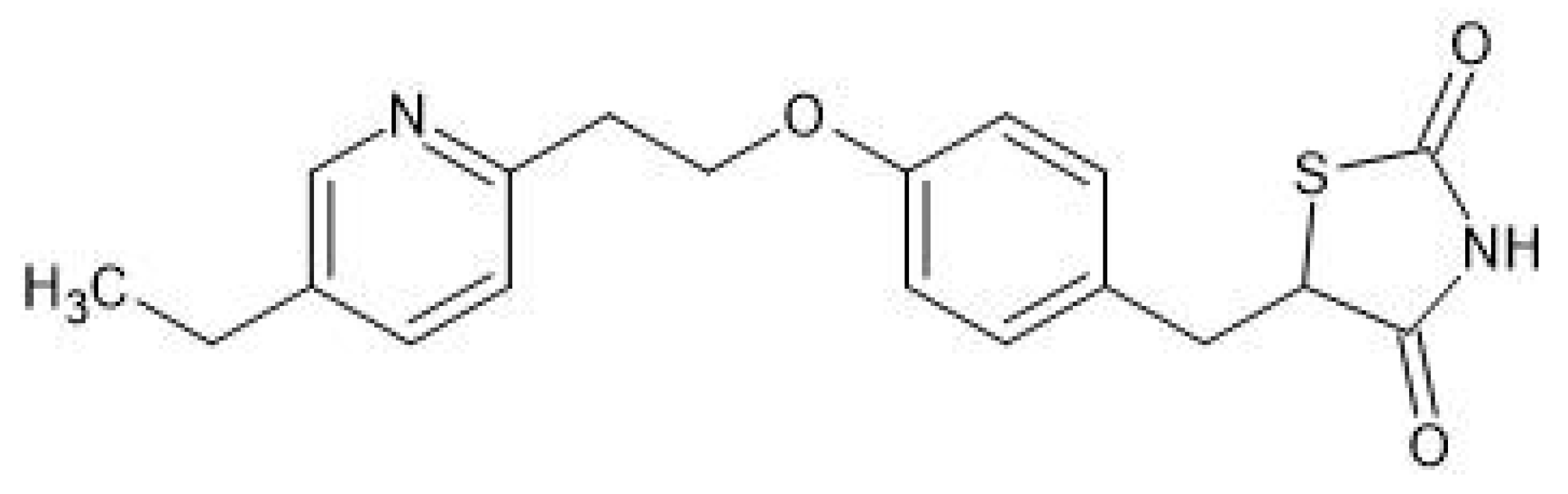
Pioglitazone, also known as 5-{4-[2-(5-Éthyl-2-pyridinyl)éthoxy]benzyl}-1,3-thiazolidine-2,4-dione based on IU-PAC, is a TZD compound derived from a pyridine derivative through nucleophilic aromatic substitution reaction with 72% yield [13]. Pioglitazone appears as needles from dimethylformamide and water, while pioglitazone hydrochloride (HCl) appears as colorless prisms from ethanol with a melting point of 183–184°C and 193–194°C, respectively [14]. The solubility of pioglitazone HCl increases with increasing temperature [15]. Low aqueous solubility and oral bioavailability can be overcome through temperature increase, cosolvents and formulation strategies such as cyclodextrins inclusion complexes or nanostructured lipid carriers (NLCs). More specifically, polyeth-ylene glycols (PEGs) are safe cosolvents for oral or parenteral pioglitazone HCl formulations. The additions of PEGs 200, 400 or 600 and temperature increase, significantly enhanced the solubility profile of pioglitazone [15]. Positive results were achieved through the addition of cyclodextrins in ethanol solution or encapsulation of pioglitazone HCl. Cyclodextrins caused a 6-fold increase in dissolution rate of pioglitazone HCl-β-cyclodextrin when compared to the pure drug, while lipid carriers achieved controlled release up to 24 h [16,17]. The latter was also observed during the administration of a newly discovered racemic compound which serves as a more thermodynamically stable and less soluble form of pioglitazone HCl [18].
The molecular structure and properties of pioglitazone have been well-characterized, providing a solid foundation for its pharmacological profile. The pharmacological activity of pioglitazone has been attributed to its hydroxy and ketone derivatives during in vivo studies on rats and dogs [13]. Similarly to other thiazolidinediones, pioglitazone activates the PPARγ receptor, increasing insulin sensitivity, without inducing insulin release from pancreatic cells. It is typically administered once a day with or without food, metabolized by the cytochrome P450 hepatic enzymes with a half-life of approximately 9 hours, and excreted in the urine. The pharmacokinetics of pioglitazone are dose and time dependent, leading to non-linear changes in plasma concentration and potential toxicity. According to clinical evidence, pioglitazone follows the same pharmacokinetic profile in healthy participants, diabetic patients and patients with renal failure, irrespective of age, gender and race. However, dose adjustment is required for patients with hepatic failure due to decreased metabolic function and by extension decreased plasma concentration [19].
Figure 1.
Chemical structure of pioglitazone.
3. Therapeutic Use of Pioglitazone
3.1. Diabetes Mellitus Type 2 (T2DM)
Thiazolidinediones (TZDs) are biguanide compounds that have been well-established for the treatment of type 2 diabetes mellitus (T2DM) [20]. Given the pathophysiology of T2DM, targeting mechanisms regulating lipid metabolism is a viable option [21]. TZDs are peroxisome-proliferator activated receptor γ (PPARγ) agonists which regulate gene expression related to the uptake, distribution and metabolism of lipids, resulting in reduced lipid levels and sensitization to insulin. However, the use of TZDs has been limited during the past years due to major safety and toxicity concerns, such as edema, cardiovascular disease, weight gain and carcinogenesis reports, as analyzed below [22].
3.2. Nonalcoholic Fatty Liver Disease (NAFLD) and Nonalcoholic Steatohepatitis (NASH)
NASH is characterized as one of the most extreme forms of NAFLD, having the potential to lead to severe and often terminal hepatic disorders such as fibrosis, cirrhosis and hepatocellular cancer [23]. Considering the association of NASH with T2DM and dyslipidemia, pioglitazone is a reasonable option against NASH in both diabetic and non-diabetic patients [24]. According to the study conducted by Della Pepa et al. (2021), pioglitazone has demonstrated positive effects against NASH even in relatively small doses. This is achieved through the increase of the peripheral and adipose tissue sensitivity to insulin, leading to the reduction of hepatic inflammation and steatosis in a glucose independent manner [25]. It is important to note several investigations of combination therapies against NASH, with the most significant one being pioglitazone combined with vitamin E [26,27].
3.3. Cardiovascular Protection
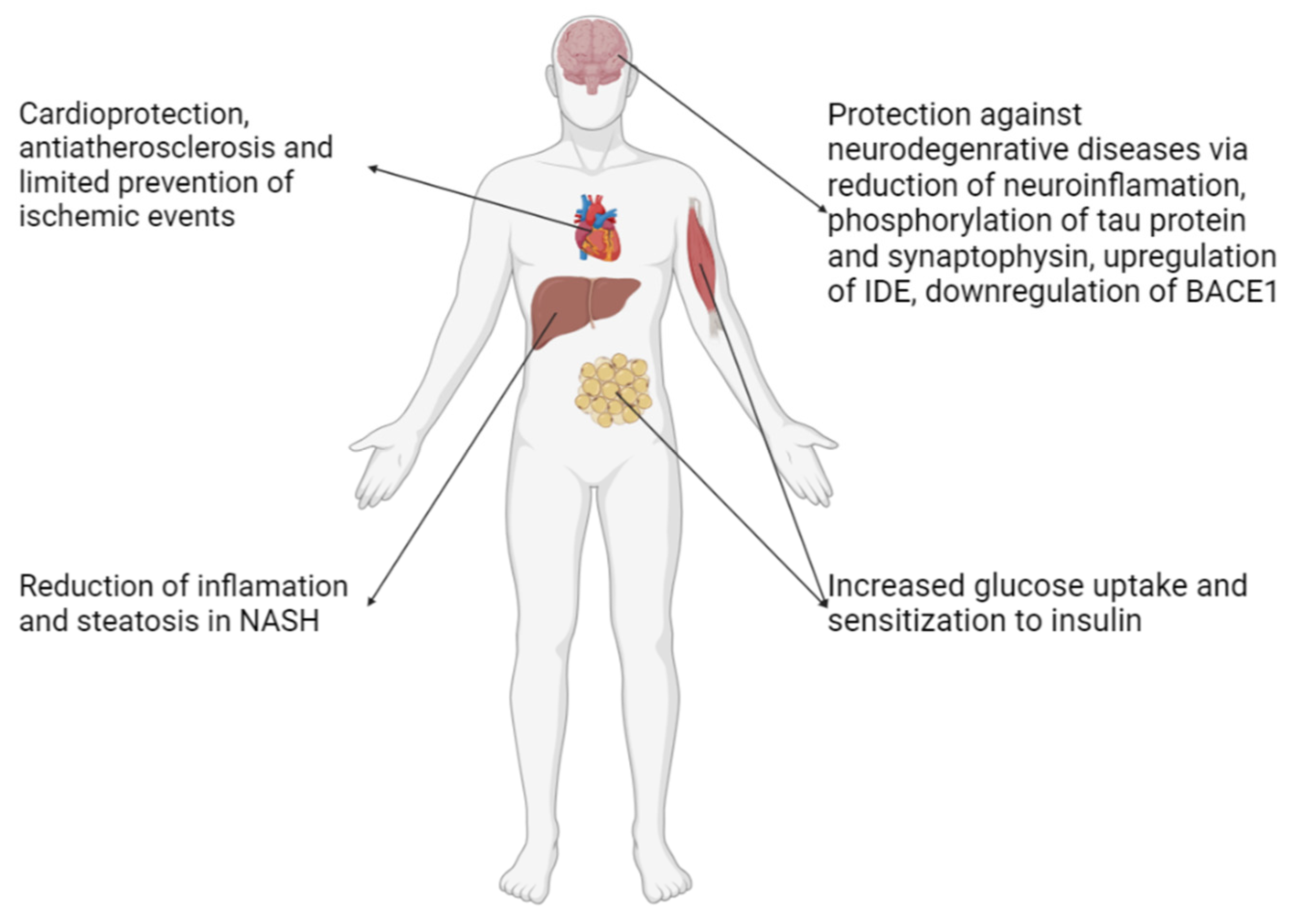
By lowering insulin resistance, TZDs can have cardioprotective and anti-atherosclerotic activity and prevent ischemic events to an extent in patients with prior history of insulin resistance [28,29,30]. Additionally, it has been noted that in murine models and in vitro studies, pioglitazone has demonstrated the capability of limiting cardiac hypertrophy in addition to arresting cardiac fibrosis and providing protection against oxidative stress [31,32].
3.4. Neurodegenerative Diseases (NDs)
There have been promising indications that PPAR-γ agonists, such as pioglitazone, possess the capability of reducing neuroinflammation as well as the concentration phosphorylated tau protein and synaptophysin, This is complemented by the elevated permeability of the blood-brain barrier [34]. Focusing on Alzheimer’s Disease (AD), given that PPARγ regulates the expression of key enzymes related to the production and metabolism of amyloid plates, the inhibition of its phosphorylation, and therefore deactivation by pioglitazone suggests favorable results [35]. The neuroprotective properties of pioglitazone that mainly stem from the anti-inflammatory effects and the mitochondrial enhancement can also be applied for Parkinson’s Disease (PD) as well as amyotrophic lateral sclerosis (ALS) in which case the effects on the muscular tissue are also of significance [36,37]. As such, based on the results of studies contacted in rodents and humans, it is evident that pioglitazone can have a positive impact in the cognition and other neurological functions of patients with NDSs [38,39].
Figure 2.
Pharmacological effect of pioglitazone on the cardiovascular and nervous system, as well as hepatic and metabolic function.
Figure 2.
Pharmacological effect of pioglitazone on the cardiovascular and nervous system, as well as hepatic and metabolic function.
3.5. Anticancer Properties
3.5.1. Overview
As established, pioglitazone has been associated with elevated risk of bladder cancer, especially in the Caucasian population to such extend that it has catalyzed its withdrawal from the French, German and Indian markets and led the Food and Drug Administration (FDA) to introduce a mandate for the providing of information regarding potential risk [40,41]. However, there have been several reports and studies that point out the antineoplastic properties of pioglitazone and the related biochemical pathways that PPARγ is implicated in. Given the pleiotropic effects of PPARγ and its agonists, we consider that investigating the exact molecular interactions will contribute to shedding some light on the mechanism of action and toxicity as well as the interactions and effects of pioglitazone and potentially suggest new applications and optimalization/personalization of interventions involving TZDs.
3.5.2. Molecular Pharmacology
PPARγ is classified as a nuclear receptor, which after binding with its ligand, translocates to the nucleus, heterodimerizes the retinoid X receptor (RXR) and acts as gene regulator via its interaction with the peroxisome proliferator response element of selected genes. The latter is related to metabolism in physiological as well as cancer cells [42]. As such, the receptor possesses the capability of affecting key cancer cell processes related to proliferation, progression, differentiation, metastasis, apoptosis etc. Activation of PPARγ receptors suppresses tumorgenicity through their interaction with insulin growth factor. Additional molecular mechanisms of therapeutic significance are summarized in Table 1.
3.6. Therapeutic Effect on Different Types of Cancer
3.6.1. Breast Cancer
According to retrospective cohort studies, there is insignificant to almost no elevated breast cancer (BC) risk related to the use of pioglitazone [64,65]. It is important to note that PPARγ levels are reduced and methylation of PPARγ promoter is in-creased in BC cells, leading to the indication of its unfavorable role in cancer proliferation. In the example of triple negative breast cancer (TNBC), pioglitazone has proven its value as an adjuvant in the combined use with doxorubicin as it decreases the inva-siveness and tendency for migration, an issue commonly associated with the use of the latter. Similar findings were also reported for the apoptosis-inducing capabilities of cisplatin during in vitro testing [49]. PPARγ facilitates major regulatory processes such as the promotion of CXCR4 and CXCR7 genes, inhibition of eIF2α, and intracellular accumulation of glucose-affecting related migration pathways [66].
3.6.2. Lung Cancer
According to clinical evidence, PPARγ agonists play a major role lung cancer progression. In fact, PPARγ agonists have been associated with differentiation, tumor size, BCL2/BAX ratio and c-MYC expression levels, in cases of non-small cell lung cancer (NSCLC), lung adenocarcinoma and squamous cell lung cancer (SCLC) [67]. Pioglitazone has demonstrated the ability to reduce NSCLC proliferation and invasiveness through downregulation and altering pathways of major significance in proliferation, apoptosis, angiogenesis and metastatic potential. Indeed, rodent studies have shown that pioglitazone has the potential to reduce tumor formation and volume [68]. Additionally, inflammation is also affected as pioglitazone inhibits prostaglandin 2 (PGE2) production while bypassing cyclooxygenase 2 (COX-2) [59]. As a chemopreventive medication, pioglitazone has proven little value considering the double-blind clinical trial conducted by Keith et al. (2019), that reported no significant alterations in the endpoints were noted other than some minor effect on lesions [69]. Chemopreventive studies were also carried out by Seabloom et al. (2017) who noted significant re-duction in adenoma formation but no noteworthy alteration to the effect of metformin when combined with it and, by a team of similar composure, who evaluated the effectiveness of pioglitazone in an aerosol form [70]. They concluded from animal tests that a dose of 150-450 μg/kg was tolerable, with limited to no adverse effects, and effective, given the reduction in adenoma formation after biochemical and histological assessments [71]. As with BC, pioglitazone has also been considered for combination therapy along with more established anticarcinogenic agents, as studied in the following cases:
- The use with EGFR Tyrosine Kinase Inhibitors such as geftinib for NSCLC as it was found that PPARγ mediated upregulation of Phosphate and Tensin homolog (PTEN) downregulated the PI3K/Akt pathway that is correlated to resistance to said TKIs [72].
- Combination of pioglitazone with clarithromycin and a relatively small dose of chemotherapeutic agent was compared against nivolumab in the ModuLung trial by Heudobler et al. (2021) [73]. This trial was terminated early due to the approval of checkpoint inhibitors as first line treatment, with the conclusion that nivolumab was superior to this combination therapy however with difference of the overall survival rate and quality of life between the two regimens being similar, the latter seems to be a viable alternative to be assessed in future trials and be considered in cases that there are few other options [73].
Granted that inactivation of PPARγ combined with increased presence of prosta-glandins is a dangerous sign as it leads to loss of control over Ras/Raf/Mek activation and NF-Κβ mediated proliferation, Kiran et al. (2022) tested pioglitazone along with COX-2 specific antagonist celecoxib on rodents. The results were coherent with the hypothesis as decrease in tumor size, alterations in tumor architecture and increase of lifespan as well as improvement of its quality were noted [74].
However, PPARγ also possesses tumor promoting effects regarding lung cancer [75], such as the case of increased tumor progression in orthotropic mice after systemic PPARγ activation in the cancer cells as well as the tumor microenvironment [59], and, as such, additional studies regarding the exact effects of pioglitazone in a clinical set-ting and risk/benefit assessment in the given context are needed.
3.6.3. Renal Cancer
It has been noted that the antidiabetic use of pioglitazone is not associated with elevation in the risk of kidney cancer [76]. Pioglitazone itself induced apoptosis in Caki cells, a model used for the study of clear cell renal cell carcinoma, as shown in Table 1 [54]. Such effects are expected considering the aforementioned as well as the elevated presence of PPARγ receptors in renal carcinoma cells. Another cell line, 769-P cells, was heavily affected in a dose-dependent manner with imminent apoptosis as the ap-plication of the molecule led to significant morphological alterations, including cell density. The suggested mechanism of apoptosis, with limited proof, in this case, was mitochondrial with membrane irregularities and release of cytochrome c. This cell line also exhibited increased sensitivity to methotrexate after treatment with pioglitazone, something that was not evident in the Vero cell line [77]. Finally, there is a lot of interest in the combination of pioglitazone with cisplatin as it showcased nephroprotective effects in rodent models by preventing tissue damage and oxidative stress and it potentiated the latter’s effects on renal adenocarcinoma cells [78].
3.6.4. Hepatocellular Carcinoma
Assessing the preventative potential of pioglitazone, metanalytical results indicate that the use of TZDs in patients with T2DM is associated with protection against liver cancer [79]. Complimentary, rodent studies indicated prevention of liver fibrosis and carcinogenesis following cirrhosis [80]. Results originating from preclinical studies showcase pioglitazone’s anticancer properties. The increased presence of Receptor for Advanced Glycation End products (RAGE) is deemed as a negative biomarker for the progression of Hepatocellular Carcinoma which possibly indicates invasion. Pioglitazone decreased the expression of RAGE along with HMGB1, NF-κβ, and p38MAPK resulting in reduced proliferation, invasion, and metastatic potential [81]. Additionally, it was reported that metabolomic alterations triggered by pioglitazone, mostly regarding the metabolism of lipids, leading to the death of chemically induced hypoxic HepG2 cells from oxidative stress [82].
3.6.5. Colorectal Cancer
Similar to hepatocellular carcinoma, it has been indicated that TZDs reduce the risk of colorectal cancer occurrence in patients with T2DM after metanalytical assessment of about 2.5 million T2DM patients [83]. Direct effects were reported during in vitro experiments with pioglitazone and, its analog, Δ2-pioglitazone treated HCT116 and HT29 cells. There were similarities in the endpoints such as cell growth arrest and differentiation in addition to key differences in the ways those were achieved, namely arrest in the S phase when treated with the former and in the G0/G1 phase when treated with the latter [84]. Additionally, xenograft studies on rodents using HT29 and SW480 cell lines indicated antiproliferative and antimetastatic activity, towards the liver activity [85]. As an adjuvant, pioglitazone can be used in immunotherapy due to the autophagic degradation of PD-L1 mediated by PPARγ whose binding with the immunomodulatory ligand is similarly enhanced by said xenobiotic agent in the case of lung cancer [86]. Investigations in the field of pharmaceutics addressing pioglitazone’s poor solubility have shown that its combination with capecitabine, an established chemotherapeutic molecule against colorectal cancer, in the form of nanoparticles enhances its bioavailability and overall proapoptotic effect on HT29 and HCT119 cells [87].
3.6.6. Thyroid Cancer
The use of pioglitazone has been correlated with neither increased nor decreased risk of thyroid cancer according to a study comprising mostly Eastern Asian individuals [88]. A widely studied finding is the PAX8-PPARγ Fusion Protein (PPFP) and how pioglitazone alters its function. PPFP is a result of a fused gene containing the significant majority of the Paired Box Gene 8 (PAX8) transcription factor, related to thyroid development and function, gene, and the entirety of the PPARγ gene and, as such, a binding site for TZDs [89]. As evident by the imminent intracellular lipid accumulation and the expression of adipocyte-related biomarkers upon treatment, pioglitazone induces the differentiation of thyroid cancer cells into adipocytes. Moreover, it is accepted that pioglitazone blocks the interaction between PPFP and Thyroid Transcription Factor 1 (TTF-1) which otherwise leads to the severe limiting of the differentiation induction by the former via suspension of recruitment of synergistic molecules such as coactivators and corepressors [90]. Considering immunity, pioglitazone also advanced the infiltration of T cells and macrophages in the tumor microenvironment when test-ed on mice and exhibited favorable properties in a clinical setting [91]. Unfortunately, Giordano et al. (2018) in their examination of 40 thyroid cancer patients found only one tested positive for PPFP, potentially indicating that it is a rare phenomenon in these cases [92]. Finally, studies have suggested that pioglitazone and metformin have a synergistic effect against thyroid cancer, especially in the induction of apoptosis [93].
3.6.7. Glioma
As mentioned before, pioglitazone can cross the blood-brain barrier, a capability that can be utilized in the case of glioma, as it is one of the most aggressive brain malignancies. Cytotoxic activity has been confirmed as it has been reported to reduce glioma cell proliferation in vitro in the U87MG, T98G and U251MG cell lines, as well as LN-229 cells in a xenograft model [94,95]. However in another xenograft study using Gl261 cells, pioglitazone seemed to significantly alter the fate of the test subjects only when injected into the cerebrum [96]. Antineoplastic action can be by conventional, PPARγ dependent and independent pathways previously mentioned, namely alterations in the levels of cyclin D1, MMP9, N-Cadhenin and caspase 3, in addition to β-catenin inhibition as revealed by knockout studies [97,98]. Invasiveness is also affected as it was limited to C6 rat glioma cells [99]. Complimentary to this is the evident increase in the expression of the Excitatory Amino Acid Transporter 2 (EAAT2) in the same cell lines, except T98G. Lack of this transporter is commonly found in glioma cells as the resulting elevation of extracellular glutamate concentration leads to excitotoxicity, assisting in the thriving of malignant cells, as an excitatory neurotransmitter, and sets setting the field for tumor associated epilepsy (TAE). As such, by increasing EAAT2 levels in glioma cells, pioglitazone worsens the conditions for the development of glioma and potentially the associated symptoms such as TAE [100]. Glioma Stem Cells (GSC) do not seem to be immune from the effects of pioglitazone either. In vitro tests by Cilibrasi et al. (2016) involving treatment of GSCs revealed that G166, GliNS2, GBM2 and G144 (with latent effects) cells reduced their metabolic rate and alteration in the proteomic profile regarding the expression of markers related to dif-ferentiation and stemness. These changes in the behavior of the cells were not accom-panied by any alterations in their morphology [101]. Data originating from the clinic reveal a preventative relationship between pioglitazone and glioma [94]. A synergy between TZDs, with pioglitazone being the most potent of them, and statins has been suggested as there was observed a significant reduction in the population, in in vitro tests by Tapia-Perez et al. (2010) using U87 cells, even in hypoxic conditions, using the U87 and RG II cell lines [102]. Follow-up rodent model tests, also by Tapia Perez et al. (2016), revealed no significant differences in overall survival rate compared to the controls and that the only combination displaying reduction in tumor size was lovastatin/atorvastatin + pioglitazone [103]. Related to cancer care, pioglitazone has also been found to protect against radiation induced cognitive decline in patients with brain malignancy and is relatively safe for use in radiation treatment [104].
3.6.8. Hematological Malignancies
There is a great amount of interest in the potential of pioglitazone in blood cancers. Studies conducted on U937 cells, modeling Acute Myeloid Leukemia (AML) cancer cells, by Esmaeili et al. (2021) have shown in their results that pioglitazone damp-ened their survival and development capabilities, led to accumulation of cells in the G1 and pre-G1 cell cycle phases and induction of apoptosis, as indicated by the in-crease in the population of cells that test positive for Annexin-V and PI [105]. Similar targeted antiproliferative effects were also observed on HL60 (modeling Acute Pro-myelocytic Leukemia-APL), K562 (modeling Chronic Myeloid Leukemia) and Jurkat (modeling T-cell lymphoma) cells and the cell cycle of the HL60 line also demonstrated accumulation in the G1 phase and decrease of the G2 and Metaphasis populations [106]. Jurkat cells were also assessed with the combination of pioglitazone and valproic acid with optimistic results as cell cycle deregulation was noted [107]. According to in vitro studies in different types of leukemia ─AML in U937 cells, APL in Jurkat cells, ALL in SD-1, IM-9, Sup-B15, and NALM-6 cells─ the primary mode of action for pioglitazone is cell cycle arrest [108]. Adding to the above are the tests on Philadelphia chromosome positive leukemic cells by Okabe et al. (2017) that reported the antineoplastic effects of pioglitazone on cells bearing the T315I mutation while sparing nor-mal CD34 expressing cells and inducing the phosphorylation of the AMP-activated protein kinase (AMPK) [109]. The combination of pioglitazone with PI3K inhibitors can potentiate its cytotoxic effects as was observed on NB4 cells (APL) when they were treated with pioglitazone and PI3K inhibitors CAL-101 and BKM120. The suggested mechanism of synergy is the cell cycle arrest, as analyzed before, mediated by p21 [110]. However, in NALM-6 cell line experiments, where similar synergy was noted, it was found that said effects are interfered with by NF-κβ signaling and autophagy [111]. Potential synergy was also noticed in more conventional chemotherapeutics with a statistically insignificant remission rate being reported for cytarabine and daunorubicin in the clinical study conducted by Ghadiany et al. (2019) [112]. Additionally, as noted in Table 1, pioglitazone is correlated with elevated effectiveness of arsenic trioxide [113]. Adjuvant use of pioglitazone has been proven to positively in-fluence interventions utilizing BCR-ABL1 tyrosine kinase inhibitors (TKIs) in Chronic Myeloid Leukemia (CML). In vitro experiments carried out on K562 cells by Glodkowska-Mrowka et al. (2016) resulted in the eradication of leukemia stem cells, progenitors, and differentiated CML cells [114,115]. A small phase II clinical trial by Rousselot et al. (2016) involving 24 subjects treated with imatinib who were administered pioglitazone at a dosage ranging from 30mg/d to 45mg/d exhibited that about half of the patients showed response within one year, with no significant adverse effects, other than edema, higher than the rate of 23% in monotherapy with imatinib, thus suggesting correlation between the synergy of pioglitazone and favorable outcomes [116]. Additional discontinuation trials such as EDI-PIO in Brazil have raised the issue of alterations in the lipid metabolism and metabolomic profile of the patients, given the effects of pioglitazone on the adipose tissue, and the aspect of mitochondrial dysfunction that influences the proliferation of CML cells [107]. However, results, also originating from the same study, suggest that pioglitazone does not affect STAT5 expression and, therefore, the levels of downstream molecules to it such as HIF-2α, contrary to the statements of previous reports [117].
3.6.9. Pancreatic Cancer
There has been contradictory evidence regarding the association between the antidiabetic use of pioglitazone and the elevation of the risk of pancreatic cancer. As such, the effect the molecule has on pancreatic cancer occurrence, and the extent of it, is yet to be determined [118,119,120]. Nevertheless, antitumor activity has been observed in cell lines modeling pancreatic cancer including Capan-1, Apsc-1 BxPC-3, PANC-1, and MIApaCa-2. Xenograft studies involving BxPC-3 revealed that antiproliferative and antimetastatic properties as tumor size was limited along with lymph metastasis [121]. Finally, pioglitazone has been reported to enhance the anticancer effects of gemcitabine through inhibition of the NF-κβ, induction of apoptosis, and setting of the platform to include HDAC inhibitors that have proven to be helpful in the activity of PPARγ [122].
3.7. Immunotherapy
PPARγ immunomodulatory effects have long been known and have been multiple studies seeking to assess the significance of said effects in cancer. A study conducted on mice hosting solid Ehrlich carcinoma cells by El-Sisi et al. (2014) concluded that pioglitazone administration led to a statistically important reduction in tumor size and TNF-α amount, increase of peripheral neutrophil and splenic T- lymphocyte populations, increase of splenic T-lymphocyte activity, CD4+/CD8+ ratio and Immunoglobin G (IgG) levels, indicating elevated immune response. Similar results, although to a varying extent and except peripheral neutrophil counts, were also obtained from co-administration with doxorubicin [123]. Immunomodulation is a property that can be exploited in the context of immunotherapy. An example of it is the use of PPARγ agonists to reprogram T cells, however there were no specific reports on pioglitazone [124].
4. Discussion
Concerns have been raised regarding the elevated risk of bladder cancer which has been reported since 2012. This can be attributed to overexpression of PPARγ which are present in the urinary bladder and several other tissues. This adverse event is prevalent especially in cases of prolonged pioglitazone administration, indicating a time-dependent and dose-dependent pharmacological profile. However, analysis does not suggest a strong dose-dependence relationship, since bladder cancer risk can be at-tributed to comorbidities and administration of antidiabetic drugs, such as metformin. Existing studies suggest a slightly but significantly elevated risk of bladder cancer as-sociated with pioglitazone administration in a time- and dose-dependent manner [40]. Due to the structure of these studies, there is no conclusive data regarding the risk-benefit ratio of pioglitazone. Up to date, there is no study that proves the direct cause-effect relationship between pioglitazone and bladder cancer [41].
Similar concerns have been raised regarding the association of metformin with risk of bladder cancer. While metformin does not decrease bladder cancer risk, it im-proves clinical parameters such as recurrence-free survival (RFS), progression-free survival (PFS) and cancer-specific survival (CSS) [125]. Although no effect was reported between overall survival (OS) and bladder cancer, studies show a positive outlook [126]. Another meta-analysis conducted in bladder cancer patients showed neither a protective nor a harmful effect of metformin exposure [127]. Few reports indicate decreased bladder cancer risk in metformin users versus never-users. However, the link between metformin and bladder cancer risk is not clear due to co-administration of other drugs and small proportion of metformin users versus never-users [128]. Overall, meta-analyses show no association of metformin with bladder cancer risk. Considering that these studies are limited to T2DM or bladder cancer patients, a consensus cannot be drawn regarding the risk of bladder cancer in the general population.
5. Conclusions
Based on the aforementioned, it is safe to assume that pioglitazone, as well as other TZDs, possess antineoplastic agents properties. PPARγ receptors, being implicated in multiple pathways, lead to diverse results in tumors. Although in vitro studies have been carried out with positive results, the adverse events presented indicate that additional studies are required in order to fully assess the risk to benefit ratio in an evidence based manner.
Author Contributions
Conceptualization, M.V., S.C.D., C.T. and N.P.N.; investigation, M.V., S.C.D., C.T. and N.P.N.; writing—original draft preparation, M.V., S.C.D., C.T. and N.P.N.; writing—review and editing, M.V., S.C.D., C.T. and N.P.N.; supervision, N.P.N. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Acknowledgments
Figure 1 was created using ACD/ChemSketch, version 2021.2.0 (Advanced Chemistry Development, Inc., Canada; www.acdlabs.com, 2022). Figure 2 was created using https://biorender.com. URL accessed on 25 October 2024.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Rangwala, S. M.; Lazar, M. A. Peroxisome Proliferator-Activated Receptor γ in Diabetes and Metabolism. Trends in Pharmacological Sciences 2004, 25, 331–336. [Google Scholar] [CrossRef] [PubMed]
- Olefsky, J. M. Treatment of Insulin Resistance with Peroxisome Proliferator–Activated Receptor γ Agonists. Journal of Clinical Investigation 2000, 106, 467–472. [Google Scholar] [CrossRef] [PubMed]
- Spiegelman, B. M. PPAR-Gamma: Adipogenic Regulator and Thiazolidinedione Receptor. Diabetes 1998, 47, 507–514. [Google Scholar] [CrossRef] [PubMed]
- Szychowski, K. A.; Leja, M. L.; Kaminskyy, D. V.; Kryshchyshyn, A. P.; Binduga, U. E.; Pinyazhko, O. R.; Lesyk, R. B.; Tobiasz, J.; Gmiński, J. Anticancer Properties of 4-Thiazolidinone Derivatives Depend on Peroxisome Proliferator-Activated Receptor Gamma (PPARγ). European Journal of Medicinal Chemistry 2017, 141, 162–168. [Google Scholar] [CrossRef]
- Towfighi, A.; Ovbiagele, B. Partial Peroxisome Proliferator-Activated Receptor Agonist Angiotensin Receptor Blockers. Cerebrovascular Diseases 2008, 26, 106–112. [Google Scholar] [CrossRef]
- Davidson, M. A.; Mattison, D. R.; Azoulay, L.; Krewski, D. Thiazolidinedione Drugs in the Treatment of Type 2 Diabetes Mellitus: Past, Present and Future. Critical reviews in toxicology 2018, 48, 52–108. [Google Scholar] [CrossRef]
- Mantovani, A.; Byrne, C. D.; Scorletti, E.; Mantzoros, C. S.; Targher, G. Efficacy and Safety of Anti-Hyperglycaemic Drugs in Patients with Non-Alcoholic Fatty Liver Disease with or without Diabetes: An Updated Systematic Review of Randomized Controlled Trials. Diabetes & Metabolism 2020, 46, 427–441. [Google Scholar] [CrossRef]
- Takada, N.; Genda, K. Pioglitazone (Actos, Glustin). Drug Discovery in Japan 2019, 169–181. [Google Scholar] [CrossRef]
- Devchand, P. R.; Liu, T.; Altman, R. B.; FitzGerald, G. A.; Schadt, E. E. The Pioglitazone Trek via Human PPAR Gamma: From Discovery to a Medicine at the FDA and Beyond. Frontiers in Pharmacology 2018, 9. [Google Scholar] [CrossRef]
- Marín-Peñalver, J. J.; Martín-Timón, I.; Sevillano-Collantes, C.; Cañizo-Gómez, F. J. del. Update on the Treatment of Type 2 Diabetes Mellitus. World Journal of Diabetes 2016, 7, 354. [Google Scholar] [CrossRef]
- European Medicines Agency. (2024). Actos: EPAR - Product Information. Retrieved from https://www.ema.europa.eu/en/documents/product-information/actos-epar-product-information_en.pdf.
- Schernthaner, G.; Currie, C. J.; Schernthaner, G.H. . Do We Still Need Pioglitazone for the Treatment of Type 2 Diabetes? A Risk-Benefit Critique in 2013. Diabetes Care 2013, 36, 155–161. [Google Scholar] [CrossRef] [PubMed]
- Tanis, S. P.; Parker, T. T.; Colca, J. R.; Fisher, R. M.; Kletzein, R. F. Synthesis and Biological Activity of Metabolites of the Antidiabetic, Antihyperglycemic Agent Pioglitazone. Journal of Medicinal Chemistry 1996, 39, 5053–5063. [Google Scholar] [CrossRef] [PubMed]
- Al-Majed, A.; Bakheit, A. H. H.; Abdel Aziz, H. A.; Alharbi, H.; Al-Jenoobi, F. I. Pioglitazone. Profiles of Drug Substances, Excipients and Related Methodology 2016, 379–438. [Google Scholar] [CrossRef]
- Shahla Soltanpour; Fatemeh Zohrabi; Zahra Bastami. Thermodynamic Solubility of Pioglitazone HCl in Polyethylene Glycols 200, 400 or 600+Water Mixtures at 303.2 and 308.2K—Data Report and Modeling. Fluid Phase Equilibria 2014, 379, 180–184. [Google Scholar] [CrossRef]
- Beloshe, S. P.; Chougule, D. D.; Shah, R. R.; Ghodke, D. S.; Pawar, N. D.; Ghaste, R. P. Effect of Method of Preparation on Pioglitazone HCl-β-Cyclodextrin Inclusion Complexes. Asian Journal of Pharmaceutics 2010, 4, 168–172. [Google Scholar] [CrossRef]
- Faiz, S.; Arshad, S.; Kamal, Y.; Imran, S.; Mulazim Hussain Asim; Mahmood, A. ; Inam, S.; Hafiz Muhammad Irfan; Riaz, H. Pioglitazone-Loaded Nanostructured Lipid Carriers: In-Vitro and In-Vivo Evaluation for Improved Bioavailability. Journal of Drug Delivery Science and Technology 2023, 79, 104041–104041. [Google Scholar] [CrossRef]
- Zhang, C.; Matzger, A. J. A Newly Discovered Racemic Compound of Pioglitazone Hydrochloride Is More Stable than the Commercial Conglomerate. Crystal Growth & Design 2017, 17, 414–417. [Google Scholar] [CrossRef]
- Eckland, D.; Danhof, M. Clinical Pharmacokinetics of Pioglitazone. Experimental and Clinical Endocrinology & Diabetes 2000, 108, 234–242. [Google Scholar] [CrossRef]
- Taylor, S. I.; Yazdi, Z. S.; Beitelshees, A. L. Pharmacological Treatment of Hyperglycemia in Type 2 Diabetes. Journal of Clinical Investigation 2021, 131. [Google Scholar] [CrossRef]
- Lebovitz, H. E. Thiazolidinediones: The Forgotten Diabetes Medications. Current Diabetes Reports 2019, 19. [Google Scholar] [CrossRef]
- Alam, F.; Islam, Md. A.; Mohamed, M.; Ahmad, I.; Kamal, M. A.; Donnelly, R.; Idris, I.; Gan, S. H. Efficacy and Safety of Pioglitazone Monotherapy in Type 2 Diabetes Mellitus: A Systematic Review and Meta-Analysis of Randomised Controlled Trials. Scientific Reports 2019, 9. [Google Scholar] [CrossRef] [PubMed]
- Zhao, Y.; Zhao, W.; Wang, H.; Zhao, Y.; Bu, H.; Takahashi, H. Pioglitazone on Nonalcoholic Steatohepatitis: A Systematic Review and Meta-Analysis of 15 RCTs. Medicine 2022, 101, e31508. [Google Scholar] [CrossRef] [PubMed]
- Wang, Z.; Du, H.; Zhao, Y.; Ren, Y.; Ma, C.; Chen, H.; Li, M.; Tian, J.; Xue, C.; Long, G.; Xu, M.-D.; Jiang, Y. Response to Pioglitazone in Non-Alcoholic Fatty Liver Disease Patients with vs. without Type 2 Diabetes: A Meta-Analysis of Randomized Controlled Trials. Frontiers in Endocrinology 2023, 14. [Google Scholar] [CrossRef] [PubMed]
- Della Pepa, G.; Russo, M.; Vitale, M.; Carli, F.; Vetrani, C.; Masulli, M.; Riccardi, G.; Vaccaro, O.; Gastaldelli, A.; Rivellese, A. A.; Bozzetto, L. Pioglitazone Even at Low Dosage Improves NAFLD in Type 2 Diabetes: Clinical and Pathophysiological Insights from a Subgroup of the TOSCA.IT Randomised Trial. Diabetes Research and Clinical Practice 2021, 178, 108984. [Google Scholar] [CrossRef]
- Mazhar, I.; Yasir, M.; Sarfraz, S. ; Gandhala Shlaghya; Narayana, S.; Mushtaq, U.; Basim Shaman Ameen; Nie, C.; Nechi, D.; Sai Sri Penumetcha. Vitamin E and Pioglitazone: A Comprehensive Systematic Review of Their Efficacy in Non-Alcoholic Fatty Liver Disease. Cureus 2023. [Google Scholar] [CrossRef]
- Sanyal, A. J.; Chalasani, N.; Kowdley, K. V.; McCullough, A.; Diehl, A. M.; Bass, N. M.; Neuschwander-Tetri, B. A.; Lavine, J. E.; Tonascia, J.; Unalp, A.; Van Natta, M.; Clark, J.; Brunt, E. M.; Kleiner, D. E.; Hoofnagle, J. H.; Robuck, P. R. Pioglitazone, Vitamin E, or Placebo for Nonalcoholic Steatohepatitis. New England Journal of Medicine 2010, 362, 1675–1685. [Google Scholar] [CrossRef]
- DeFronzo, R. A.; Inzucchi, S.; Abdul-Ghani, M.; Nissen, S. E. Pioglitazone: The Forgotten, Cost-Effective Cardioprotective Drug for Type 2 Diabetes. Diabetes and Vascular Disease Research 2019, 16, 133–143. [Google Scholar] [CrossRef]
- Kernan, W. N.; Viscoli, C. M.; Furie, K. L.; Young, L. H.; Inzucchi, S. E.; Gorman, M.; Guarino, P. D.; Lovejoy, A. M.; Peduzzi, P. N.; Conwit, R.; Brass, L. M.; Schwartz, G. G.; Adams, H. P.; Berger, L.; Carolei, A.; Clark, W.; Coull, B.; Ford, G. A.; Kleindorfer, D.; O’Leary, J. R. Pioglitazone after Ischemic Stroke or Transient Ischemic Attack. New England Journal of Medicine 2016, 374, 1321–1331. [Google Scholar] [CrossRef]
- Lee, M.; Saver, J. L.; Liao, H.-W.; Lin, C.-H.; Ovbiagele, B. Pioglitazone for Secondary Stroke Prevention. Stroke 2017, 48, 388–393. [Google Scholar] [CrossRef]
- Wei, W.-Y.; Ma, Z.G.; Xu, S.C.; Zhang, N.; Tang, Q.Z. Pioglitazone Protected against Cardiac Hypertrophy via Inhibiting AKT/GSK3βand MAPK Signaling Pathways. PPAR Research 2016, 2016, 1–11. [Google Scholar] [CrossRef]
- Bilginoglu, A. Cardiovascular Protective Effect of Pioglitazone on Oxidative Stress in Rats with Metabolic Syndrome. Journal of the Chinese Medical Association 2019, 82, 452–456. [Google Scholar] [CrossRef] [PubMed]
- Zhou, Y.; Huang, Y.; Ji, X.; Wang, X.; Shen, L.; Wang, Y. Pioglitazone for the Primary and Secondary Prevention of Cardiovascular and Renal Outcomes in Patients with or at High Risk of Type 2 Diabetes Mellitus: A Meta-Analysis. The Journal of Clinical Endocrinology & Metabolism 2019. [Google Scholar] [CrossRef]
- Alhowail, A.; Alsikhan, R.; Alsaud, M.; Aldubayan, M.; Rabbani, S. I. Protective Effects of Pioglitazone on Cognitive Impairment and the Underlying Mechanisms: A Review of Literature. Drug Design, Development and Therapy 2022, 16, 2919–2931. [Google Scholar] [CrossRef] [PubMed]
- Quan, Q.; Qian, Y.; Li, X.; Li, M. Pioglitazone Reduces β Amyloid Levels via Inhibition of PPARγ Phosphorylation in a Neuronal Model of Alzheimer’s Disease. Frontiers in Aging Neuroscience 2019, 11. [Google Scholar] [CrossRef] [PubMed]
- Zamanian, M.Y.; Terefe, E.M.; Taheri, N.; Kujawska, M.; Tork, Y.J.; Abdelbasset, W.K.; Shoukat, S.; Jade, M.; Heidari, M.; Alesaeidi, S. Neuroprotective and Anti-Inflammatory Effects of Pioglitazone on Parkinson’s Disease: A Comprehensive Narrative Review of Clinical and Experimental Findings. CNS & Neurological Disorders - Drug Targets 2023, 22, 1453–1461. [Google Scholar] [CrossRef]
- Schutz, B. The Oral Antidiabetic Pioglitazone Protects from Neurodegeneration and Amyotrophic Lateral Sclerosis-like Symptoms in Superoxide Dismutase-G93A Transgenic Mice. Journal of Neuroscience 2005, 25, 7805–7812. [Google Scholar] [CrossRef]
- Adamu, A.; Li, S.; Gao, F.; Xue, G. The Role of Neuroinflammation in Neurodegenerative Diseases: Current Understanding and Future Therapeutic Targets. Frontiers in aging neuroscience 2024, 16. [Google Scholar] [CrossRef]
- Heneka, M. T.; Fink, A.; Doblhammer, G. Effect of Pioglitazone Medication on the Incidence of Dementia. Annals of Neurology 2015, 78, 284–294. [Google Scholar] [CrossRef]
- Tang, H.; Shi, W.; Fu, S.; Wang, T.; Zhai, S.; Song, Y.; Han, J. Pioglitazone and Bladder Cancer Risk: A Systematic Review and Meta-Analysis. Cancer Medicine 2018, 7, 1070–1080. [Google Scholar] [CrossRef]
- Hashmi, A. Pioglitazone Suspension and Its Aftermath: A Wake up Call for the Indian Drug Regulatory Authorities. Journal of Pharmacology and Pharmacotherapeutics 2013, 4, 227. [Google Scholar] [CrossRef]
- Mirza, A. Z.; Althagafi, I. I.; Shamshad, H. Role of PPAR Receptor in Different Diseases and Their Ligands: Physiological Importance and Clinical Implications. European journal of medicinal chemistry 2019, 166, 502–513. [Google Scholar] [CrossRef] [PubMed]
- Yousefnia, S.; Momenzadeh, S.; Forootan, F.S.; Ghaedi, K.; Nasr-Esfahani, M.H. The Influence of Peroxisome Proliferator-Activated Receptor γ (PPARγ) Ligands on Cancer Cell Tumorigenicity. Gene 2018, 649, 14–22. [Google Scholar] [CrossRef] [PubMed]
- Wang, Y.; Lei, F.; Lin, Y.; Han, Y.; Yang, L.; Tan, H. Peroxisome Proliferator-Activated Receptors as Therapeutic Target for Cancer. Journal of Cellular and Molecular Medicine 2023, 28, 17931. [Google Scholar] [CrossRef] [PubMed]
- Chi, T.; Wang, M.; Wang, X.; Yang, K.; Xie, F.; Liao, Z.; Wei, P. PPAR-γ Modulators as Current and Potential Cancer Treatments. Frontiers in Oncology 2021, 11, 737776. [Google Scholar] [CrossRef] [PubMed]
- Jiao, X. X.; Lin, S. Y.; Lian, S. X.; Qiu, Y. R.; Li, Z. H.; Chen, Z. H.; Lu, W. Q.; Zhang, Y.; Deng, L.; Jiang, Y.; Hu, G. H. Inhibition of the Breast Cancer by PPARγ Agonist Pioglitazone through JAK2/STAT3 Pathway. Neoplasma 2020, 67, 834–842. [Google Scholar] [CrossRef]
- Kole, L.; Sarkar, M.; Deb, A.; Giri, B. Pioglitazone, an Anti-Diabetic Drug Requires Sustained MAPK Activation for Its Anti-Tumor Activity in MCF7 Breast Cancer Cells, Independent of PPAR-γ Pathway. Pharmacological Reports 2016, 68, 144–154. [Google Scholar] [CrossRef]
- Yun, S.H.; Han, S.H.; Park, J.I. Peroxisome Proliferator-Activated Receptor γ and PGC-1α in Cancer: Dual Actions as Tumor Promoter and Suppressor. PPAR Research 2018, 2018, 1–12. [Google Scholar] [CrossRef]
- Shi, J.; Zhang, W.; You, M.; Xu, Y.; Hou, Y.; Jin, J. Pioglitazone Inhibits EGFR/MDM2 Signaling-Mediated PPARγ Degradation. European Journal of Pharmacology 2016, 791, 316–321. [Google Scholar] [CrossRef]
- Vella, V.; Nicolosi, M. L.; Giuliano, S.; Bellomo, M.; Belfiore, A.; Malaguarnera, R. PPAR-γ Agonists as Antineoplastic Agents in Cancers with Dysregulated IGF Axis. Frontiers in Endocrinology 2017, 8. [Google Scholar] [CrossRef]
- Yun, S.H.; Han, S.H.; Park, J.I. Peroxisome Proliferator-Activated Receptor γ and PGC-1α in Cancer: Dual Actions as Tumor Promoter and Suppressor. PPAR Research 2018, 2018, 1–12. [Google Scholar] [CrossRef]
- Masanobu Tsubaki; Takeda, T. ; Tomonari, Y.; Kawashima, K.; Itoh, T.; Imano, M.; Satou, K.; Nishida, S. Pioglitazone Inhibits Cancer Cell Growth through STAT3 Inhibition and Enhanced AIF Expression via a PPARγ-Independent Pathway. Journal of Cellular Physiology 2017, 233, 3638–3647. [Google Scholar] [CrossRef]
- Elrod, H. A.; Sun, S.-Y. PPARγ and Apoptosis in Cancer. PPAR Research 2008, 2008, 704165. [Google Scholar] [CrossRef] [PubMed]
- Jang, J. H.; Lee, T.J.; Sung, E.G.; Song, I.H.; Kim, J.Y. Pioglitazone Mediates Apoptosis in Caki Cells via Downregulating C-FLIP(L) Expression and Reducing Bcl-2 Protein Stability. Oncology Letters 2021, 22. [Google Scholar] [CrossRef] [PubMed]
- Park, J.I.; Kwak, J.Y. The Role of Peroxisome Proliferator-Activated Receptors in Colorectal Cancer. PPAR Research 2012, 2012, 1–12. [Google Scholar] [CrossRef]
- Ballav, S.; Biswas, B.; Sahu, V. K.; Ranjan, A.; Basu, S. PPAR-γ Partial Agonists in Disease-Fate Decision with Special Reference to Cancer. Cells 2022, 11, 3215. [Google Scholar] [CrossRef]
- Sun, J.; Yu, L.; Qu, X.; Huang, T. The Role of Peroxisome Proliferator-Activated Receptors in the Tumor Microenvironment, Tumor Cell Metabolism, and Anticancer Therapy. Frontiers in Pharmacology 2023, 14, 1184794. [Google Scholar] [CrossRef]
- Dicitore, A.; Caraglia, M.; Gaudenzi, G.; Manfredi, G.; Amato, B.; Mari, D.; Persani, L.; Arra, C.; Vitale, G. Type I Interferon-Mediated Pathway Interacts with Peroxisome Proliferator Activated Receptor-γ (PPAR-γ): At the Cross-Road of Pancreatic Cancer Cell Proliferation. Biochimica et Biophysica Acta (BBA) - Reviews on Cancer 2014, 1845, 42–52. [Google Scholar] [CrossRef]
- Li, H.; Weiser-Evans, M.C.M.; Nemenoff, R. Anti- and Protumorigenic Effects of PPARγin Lung Cancer Progression: A Double-Edged Sword. PPAR Research 2012, 2012, 1–12. [Google Scholar] [CrossRef]
- Hernandez-Quiles, M.; Broekema, M. F.; Kalkhoven, E. PPARgamma in Metabolism, Immunity, and Cancer: Unified and Diverse Mechanisms of Action. Frontiers in Endocrinology 2021, 12, 624112. [Google Scholar] [CrossRef]
- Jia, X.; Qian, J.; Chen, H.; Liu, Q.; Hussain, S.; Jin, J.; Shi, J.; Hou, Y. PPARγ Agonist Pioglitazone Enhances Colorectal Cancer Immunotherapy by Inducing PD-L1 Autophagic Degradation. European Journal of Pharmacology 2023, 950, 175749–175749. [Google Scholar] [CrossRef]
- Jin Young Yoo; Yang, S. -H.; Jung Eun Lee; Deog Gon Cho; Hoon Kyo Kim; Sung Hwan Kim; Il Sup Kim; Jae Taek Hong; Jae Hoon Sung; Byung Chul Son; Sang Won Lee. E-Cadherin as a Predictive Marker of Brain Metastasis in Non-Small-Cell Lung Cancer, and Its Regulation by Pioglitazone in a Preclinical Model. Journal of Neuro-Oncology 2012, 109, 219–227. [Google Scholar] [CrossRef]
- Ciaramella, V.; Ferdinando Carlo Sasso; Raimondo Di Liello; Della, M. ; Barra, G.; Viscardi, G.; Esposito, G.; Sparano, F.; Troiani, T.; Martinelli, E.; Orditura, M.; Ferdinando De Vita; Ciardiello, F.; Morgillo, F. Activity and Molecular Targets of Pioglitazone via Blockade of Proliferation, Invasiveness and Bioenergetics in Human NSCLC. Journal of Experimental & Clinical Cancer Research 2019, 38. [Google Scholar] [CrossRef]
- Tseng, C.H. Pioglitazone and Breast Cancer Risk in Female Patients with Type 2 Diabetes Mellitus: A Retrospective Cohort Analysis. BMC Cancer 2022, 22. [Google Scholar] [CrossRef] [PubMed]
- Dormandy, J.; Bhattacharya, M.; van Troostenburg de Bruyn, A.-R. Safety and Tolerability of Pioglitazone in High-Risk Patients with Type 2 Diabetes. Drug Safety 2009, 32, 187–202. [Google Scholar] [CrossRef]
- Malakouti, P.; Mohammadi, M.; Boshagh, M. A.; Amini, A.; Rezaee, M. A.; Rahmani, M. R. Combined Effects of Pioglitazone and Doxorubicin on Migration and Invasion of MDA-MB-231 Breast Cancer Cells. Journal of the Egyptian National Cancer Institute 2022, 34. [Google Scholar] [CrossRef]
- Giaginis, C.; Politi, E.; Alexandrou, P.; Sfiniadakis, J.; Kouraklis, G.; Theocharis, S. Expression of Peroxisome Proliferator Activated Receptor-Gamma (PPAR-γ) in Human Non-Small Cell Lung Carcinoma: Correlation with Clinicopathological Parameters, Proliferation and Apoptosis Related Molecules and Patients’ Survival. Pathology & Oncology Research 2012, 18, 875–883. [Google Scholar] [CrossRef]
- Lakshmi, S. P.; Reddy, A. T.; Banno, A.; Reddy, R. C. PPAR Agonists for the Prevention and Treatment of Lung Cancer. PPAR Research 2017, 2017, 1–8. [Google Scholar] [CrossRef]
- Keith, R. L.; Blatchford, P. J.; Merrick, D. T.; Bunn, P. A.; Bagwell, B.; Dwyer-Nield, L. D.; Jackson, M. K.; Geraci, M. W.; Miller, Y. E. A Randomized Phase II Trial of Pioglitazone for Lung Cancer Chemoprevention in High-Risk Current and Former Smokers. Cancer Prevention Research 2019, 12, 721–730. [Google Scholar] [CrossRef]
- Seabloom, D. E.; Galbraith, A. R.; Haynes, A. M.; Antonides, J. D.; Wuertz, B. R.; Miller, W. A.; Miller, K. A.; Steele, V. E.; Mark Steven Miller; Clapper, M. L.; M. Gerard O'Sullivan; Ondrey, F. G. Fixed-Dose Combinations of Pioglitazone and Metformin for Lung Cancer Prevention. Cancer Prevention Research 2017, 10, 116–123. [Google Scholar] [CrossRef]
- Seabloom, D. E.; Galbraith, A. R.; Haynes, A. M.; Antonides, J. D.; Wuertz, B. R.; Miller, W. A.; Miller, K. A.; Steele, V. E.; Suen, C. S.; M. Gerard O'Sullivan; Ondrey, F. G. Safety and Preclinical Efficacy of Aerosol Pioglitazone on Lung Adenoma Prevention in A/J Mice. Cancer Prevention Research 2017, 10, 124–132. [Google Scholar] [CrossRef]
- Kenneth K.W., To; William K.K., Wu; Herbert, H.F. Loong. PPARgamma Agonists Sensitize PTEN-Deficient Resistant Lung Cancer Cells to EGFR Tyrosine Kinase Inhibitors by Inducing Autophagy. European journal of pharmacology 2018, 823, 19–26. [Google Scholar] [CrossRef]
- Heudobler, D.; Schulz, C.; Fischer, J. R.; Staib, P.; Wehler, T.; Südhoff, T.; Schichtl, T.; Wilke, J.; Hahn, J.; Florian Lüke; Vogelhuber, M. ; Klobuch, S.; Pukrop, T.; Herr, W.; Held, S.; Beckers, K.; Bouche, G.; Reichle, A. A Randomized Phase II Trial Comparing the Efficacy and Safety of Pioglitazone, Clarithromycin and Metronomic Low-Dose Chemotherapy with Single-Agent Nivolumab Therapy in Patients with Advanced Non-Small Cell Lung Cancer Treated in Second or Further Line (ModuLung). Frontiers in Pharmacology 2021, 12, 599598. [Google Scholar] [CrossRef] [PubMed]
- Kiran, A.V.V.V.R.; Kumari, G. K.; Krishnamurthy, P. T. Preliminary Evaluation of Anticancer Efficacy of Pioglitazone Combined with Celecoxib for the Treatment of Non-Small Cell Lung Cancer. Investigational New Drugs 2022, 40, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Han, S. W. Anticancer Actions of PPARγ Ligands: Current State and Future Perspectives in Human Lung Cancer. World Journal of Biological Chemistry 2010, 1, 31. [Google Scholar] [CrossRef]
- Tseng, C.-H. Pioglitazone Does Not Affect the Risk of Kidney Cancer in Patients with Type 2 Diabetes. Metabolism 2014, 63, 1049–1055. [Google Scholar] [CrossRef]
- Piątkowska-Chmiel, I.; Gawrońska-Grzywacz, M.; Natorska-Chomicka, D.; Herbet, M.; Sysa, M.; Iwan, M.; Korga, A.; Dudka, J. Pioglitazone as a Modulator of the Chemoresistance of Renal Cell Adenocarcinoma to Methotrexate. Oncology Reports 2020, 43, 1019–1030. [Google Scholar] [CrossRef]
- Mahmoud, M.F.; El Shazly, S.M. Pioglitazone Protects against Cisplatin Induced Nephrotoxicity in Rats and Potentiates Its Anticancer Activity against Human Renal Adenocarcinoma Cell Lines. Food and Chemical Toxicology 2013, 51, 114–122. [Google Scholar] [CrossRef]
- Wang, F.; Zhao, S.Z.; Zhang, M.-Y.; Ma, Y.L.; Zhang, P.; Qin, H.L. Decreased Risk of Liver Cancer with Thiazolidinediones Therapy in Patients with Type 2 Diabetes: Results from a Meta-Analysis. Hepatology 2013, 58, 835–836. [Google Scholar] [CrossRef]
- Li, S.; Ghoshal, S.; Sojoodi, M.; Arora, G.; Masia, R.; Erstad, D. J.; Lanuti, M.; Hoshida, Y.; Baumert, T.; Tanabe, K.K.; Fuchs, B.C. Pioglitazone Reduces Hepatocellular Carcinoma Development in Two Rodent Models of Cirrhosis. Journal of Gastrointestinal Surgery 2019, 23, 101–111. [Google Scholar] [CrossRef]
- Yang, Y.; Zhao, L.H.; Huang, B.; Wang, R.Y.; Yuan, S.X.; Tao, Q.F.; Xu, Y.; Sun, H.Y.; Lin, C.; Zhou, W.P. Pioglitazone, a PPARγ Agonist, Inhibits Growth and Invasion of Human Hepatocellular Carcinoma via Blockade of the Rage Signaling. Molecular Carcinogenesis 2014, 54, 1584–1595. [Google Scholar] [CrossRef]
- Huang, G.; Zhang, M.; Wang, M.; Xu, W.; Duan, X.; Han, X.; Ren, J. Pioglitazone, a Peroxisome Proliferator-Activated Receptor γ Agonist, Induces Cell Death and Inhibits the Proliferation of Hypoxic HepG2 Cells by Promoting Excessive Production of Reactive Oxygen Species. Oncology Letters 2024, 27, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Hu, T.T.; Liu, Y.; Jin, P.P.; Sun, X.C. Thiazolidinediones and Risk of Colorectal Cancer in Patients with Diabetes Mellitus: A Meta-Analysis. Saudi Journal of Gastroenterology 2018, 24, 75. [Google Scholar] [CrossRef] [PubMed]
- Huber, S.; Valente, S.; Chaimbault, P.; Schohn, H. Evaluation of Δ2-Pioglitazone, an Analogue of Pioglitazone, on Colon Cancer Cell Survival: Evidence of Drug Treatment Association with Autophagy and Activation of the Nrf2/Keap1 Pathway. International Journal of Oncology 2014, 45, 426–438. [Google Scholar] [CrossRef] [PubMed]
- Takano, S.; Kubota, T.; Nishibori, H.; Hasegawa, H.; Ishii, Y.; Nitori, N.; Ochiai, H.; Okabayashi, K.; Kitagawa, Y.; Watanabe, M.; Kitajima, M. Pioglitazone, a Ligand for Peroxisome Proliferator-Activated Receptor-γ Acts as an Inhibitor of Colon Cancer Liver Metastasis. Anticancer Research 2008, 28, 3593–3599. [Google Scholar]
- Jia, X.; Qian, J.; Chen, H.; Liu, Q.; Hussain, S.; Jin, J.; Shi, J.; Hou, Y. PPARγ Agonist Pioglitazone Enhances Colorectal Cancer Immunotherapy by Inducing PD-L1 Autophagic Degradation. European Journal of Pharmacology 2023, 950, 175749–175749. [Google Scholar] [CrossRef]
- Fahima Danesh Pouya; Salehi, R. ; Yousef Rasmi; Fatemeh Kheradmand; Anahita Fathi-Azarbayjani. Combination Chemotherapy against Colorectal Cancer Cells: Co-Delivery of Capecitabine and Pioglitazone Hydrochloride by Polycaprolactone-Polyethylene Glycol Carriers. Life Sciences 2023, 332, 122083–122083. [Google Scholar] [CrossRef]
- Kushchayeva, Y.; Kushchayev, S.; Jensen, K.; Brown, R. J. Impaired Glucose Metabolism, Anti-Diabetes Medications, and Risk of Thyroid Cancer. Cancers 2022, 14, 555. [Google Scholar] [CrossRef]
- Zhang, Y.; Yu, J.; Grachtchouk, V.; Qin, T.; Lumeng, C. N.; Sartor, M. A.; Koenig, R. J. Genomic Binding of PAX8-PPARG Fusion Protein Regulates Cancer-Related Pathways and Alters the Immune Landscape of Thyroid Cancer. Oncotarget 2016, 8. [Google Scholar] [CrossRef]
- Xu, B.; O’Donnell, M.; O’Donnell, J.; Yu, J.; Zhang, Y.; Sartor, M. A.; Koenig, R. J. Adipogenic Differentiation of Thyroid Cancer Cells through the Pax8-PPARγ Fusion Protein Is Regulated by Thyroid Transcription Factor 1 (TTF-1). Journal of Biological Chemistry 2016, 291, 19274–19286. [Google Scholar] [CrossRef]
- Greco, A.; Coperchini, F.; Croce, L.; Magri, F. ; Marsida Teliti; Rotondi, M. Drug Repositioning in Thyroid Cancer Treatment: The Intriguing Case of Anti-Diabetic Drugs. Frontiers in pharmacology 2023, 14, 1303844. [Google Scholar] [CrossRef]
- Giordano, T. J.; Haugen, B. R.; Sherman, S. I.; Shah, M. H.; Caoili, E. M.; Koenig, R. J. Pioglitazone Therapy of PAX8-PPARγ Fusion Protein Thyroid Carcinoma. The Journal of Clinical Endocrinology & Metabolism 2018, 103, 1277–1281. [Google Scholar] [CrossRef]
- Ozdemir Kutbay, N.; Biray Avci, C.; Sarer Yurekli, B.; Caliskan Kurt, C.; Shademan, B.; Gunduz, C.; Erdogan, M. Effects of Metformin and Pioglitazone Combination on Apoptosis and AMPK/MTOR Signaling Pathway in Human Anaplastic Thyroid Cancer Cells. Journal of Biochemical and Molecular Toxicology 2020, 34. [Google Scholar] [CrossRef] [PubMed]
- Basilotta, R.; Lanza, M.; Casili, G.; Chisari, G.; Munao, S.; Colarossi, L.; Cucinotta, L.; Campolo, M.; Esposito, E.; Paterniti, I. Potential Therapeutic Effects of PPAR Ligands in Glioblastoma. Cells 2022, 11, 621–621. [Google Scholar] [CrossRef] [PubMed]
- Grommes, C.; Karlo, J. C.; Caprariello, A.; Blankenship, D.; DeChant, A.; Landreth, G. E. The PPARγ Agonist Pioglitazone Crosses the Blood–Brain Barrier and Reduces Tumor Growth in a Human Xenograft Model. Cancer Chemotherapy and Pharmacology 2013, 71, 929–936. [Google Scholar] [CrossRef] [PubMed]
- Lichtor, T.; Spagnolo, A.; Glick, R. P.; Feinstein, D. L. PPAR- Thiazolidinedione Agonists and Immunotherapy in the Treatment of Brain Tumors. PPAR Research 2008, 2008, 1–4. [Google Scholar] [CrossRef]
- Ching, J.; Amiridis, S.; Stylli, S. S.; Morokoff, A. P.; O’Brien, T. J.; Kaye, A. H. A Novel Treatment Strategy for Glioblastoma Multiforme and Glioma Associated Seizures: Increasing Glutamate Uptake with PPARγ Agonists. Journal of Clinical Neuroscience 2015, 22, 21–28. [Google Scholar] [CrossRef]
- Wan, Z.; Shi, W.; Shao, B.; Shi, J.; Shen, A.; Ma, Y.; Chen, J.; Lan, Q. Peroxisome Proliferator-Activated Receptor γ Agonist Pioglitazone Inhibits β-Catenin-Mediated Glioma Cell Growth and Invasion. Molecular and Cellular Biochemistry 2011, 349, (1–2). [Google Scholar] [CrossRef]
- Seufert, S.; Coras, R.; Tränkle, C.; Zlotos, D. P.; Ingmar Blümcke; Lars Tatenhorst; Heneka, M. T.; Hahnen, E. PPAR Gamma Activators: Off-Target against Glioma Cell Migration and Brain Invasion. PPAR Research 2008, 2008, 513943. [Google Scholar] [CrossRef]
- Ching, J.; Amiridis, S.; Stylli, S. S.; Bjorksten, A. R.; Kountouri, N.; Zheng, T.; Paradiso, L.; Luwor, R. B.; Morokoff, A. P.; O’Brien, T. J.; Kaye, A. H. The Peroxisome Proliferator Activated Receptor Gamma Agonist Pioglitazone Increases Functional Expression of the Glutamate Transporter Excitatory Amino Acid Transporter 2 (EAAT2) in Human Glioblastoma Cells. Oncotarget 2015, 6, 21301–21314. [Google Scholar] [CrossRef]
- Cilibrasi, C.; Butta, V.; Riva, G.; Bentivegna, A. Pioglitazone Effect on Glioma Stem Cell Lines: Really a Promising Drug Therapy for Glioblastoma? PPAR Research 2016, 2016, 1–8. [Google Scholar] [CrossRef]
- Tapia-Pérez, J. H.; Kirches, E.; Mawrin, C.; Firsching, R.; Schneider, T. Cytotoxic Effect of Different Statins and Thiazolidinediones on Malignant Glioma Cells. Cancer Chemotherapy and Pharmacology 2010, 67, 1193–1201. [Google Scholar] [CrossRef]
- Tapia-Pérez, J.H.; Preininger, R.; Kirches, E.; Reinhold, A.; Butzmann, J.; Prilloff, S.; Mawrin, C.; Schneider, T. Simultaneous Administration of Statins and Pioglitazone Limits Tumor Growth in a Rat Model of Malignant Glioma. Anticancer Research 2016, 36, 6357–6365. [Google Scholar] [CrossRef] [PubMed]
- Cramer, C.K.; Alphonse-Sullivan, N.K.; Isom, S.; Metheny-Barlow, L.J.; Cummings, T.L.; Page, B.R.; Brown, D.; Blackstock, A. W.; Peiffer, A.M.; Strowd, R.E.; Rapp, S.R.; Lesser, G.J.; Shaw, E.G.; Chan, M.D. Safety of Pioglitazone during and after Radiation Therapy in Patients with Brain Tumors: A Phase I Clinical Trial. 2019, 145, 337–344. [Google Scholar] [CrossRef] [PubMed]
- Esmaeili, S.; Salari, S.; Kaveh, V.; Ghaffari, S. H.; Bashash, D. Alteration of PPAR-GAMMA (PPARG; PPARγ) and PTEN Gene Expression in Acute Myeloid Leukemia Patients and the Promising Anticancer Effects of PPARγ Stimulation Using Pioglitazone on AML Cells. Molecular Genetics & Genomic Medicine 2021, 9, 1818. [Google Scholar] [CrossRef]
- Saiki, M.; Hatta, Y.; Yamazaki, T.; Itoh, T.; Enomoto, Y.; Takeuchi, J.; Sawada, U.; Aizawa, S.; Horie, T. Pioglitazone Inhibits the Growth of Human Leukemia Cell Lines and Primary Leukemia Cells While Sparing Normal Hematopoietic Stem Cells. International Journal of Oncology 2006, 29, 437–443. [Google Scholar] [CrossRef]
- Póvoa, V. M. O.; Delafiori, J.; Dias-Audibert, F. L.; de Oliveira, A. N.; Lopes, A. B. P.; de Paula, E. V.; Pagnano, K. B. B.; Catharino, R. R. Metabolic Shift of Chronic Myeloid Leukemia Patients under Imatinib–Pioglitazone Regimen and Discontinuation. Medical Oncology 2021, 38, 1–10. [Google Scholar] [CrossRef]
- Ryu, S.; Kim, D. S.; Lee, M. W.; Lee, J. W.; Sung, K. W.; Koo, H. H.; Yoo, K. H. Anti-Leukemic Effects of PPARγ Ligands. Cancer Letters 2018, 418, 10–19. [Google Scholar] [CrossRef]
- Okabe, S.; Tetsuzo Tauchi; Tanaka, Y. ; Kazuma Ohyashiki. Peroxisome Proliferator-Activated Receptors: Targets for the Treatment of Philadelphia Chromosome-Positive Leukemia Cells. Blood 2017, 130, 5241. [Google Scholar] [CrossRef]
- Esmaeili, S.; Yousefi, A.-M.; Delshad, M.; Davood Bashash. Synergistic Effects of PI3K Inhibition and Pioglitazone against Acute Promyelocytic Leukemia Cells. Molecular genetics & genomic medicine 2022, 11, 2106. [Google Scholar] [CrossRef]
- Mokhtari, Y.; Yousefi, A.-M.; Davood Bashash. Inhibition of PI3K Signaling Intensified the Antileukemic Effects of Pioglitazone: New Insight into the Application of PPARγ Stimulators in Acute Lymphoblastic Leukemia. Indian Journal of Hematology and Blood Transfusion 2023, 39, 546–556. [Google Scholar] [CrossRef]
- Ghadiany, M.; Tabarraee, M.; Salari, S.; Haghighi, S.; Rezvani, H.; Ghasemi, S. N.; Karimi-Sari, H. Adding Oral Pioglitazone to Standard Induction Chemotherapy of Acute Myeloid Leukemia: A Randomized Clinical Trial. Clinical Lymphoma Myeloma and Leukemia 2019, 19, 206–212. [Google Scholar] [CrossRef]
- Esmaeili, S.; Safaroghli-azar, A.; Pourbagheri-Sigaroodi, A.; Salari, S.; Gharehbaghian, A.; hamidpour, M.; Bashash, D. Activation of PPARγ Intensified the Effects of Arsenic Trioxide in Acute Promyelocytic Leukemia through the Suppression of PI3K/Akt Pathway: Proposing a Novel Anticancer Effect for Pioglitazone. The International Journal of Biochemistry & Cell Biology 2020, 122, 105739. [Google Scholar] [CrossRef]
- Glodkowska-Mrowka, E.; Manda-Handzlik, A.; Stelmaszczyk-Emmel, A.; Seferynska, I.; Stoklosa, T.; Przybylski, J.; Mrowka, P. PPARγ Ligands Increase Antileukemic Activity of Second- and Third-Generation Tyrosine Kinase Inhibitors in Chronic Myeloid Leukemia Cells. Blood Cancer Journal 2016, 6, 377. [Google Scholar] [CrossRef] [PubMed]
- Jazi, M. S.; Mohammadi, S.; Yazdani, Y.; Sedighi, S.; Memarian, A.; Mehrdad Aghaei. Effects of Valproic Acid and Pioglitazone on Cell Cycle Progression and Proliferation of T-Cell Acute Lymphoblastic Leukemia Jurkat Cells. Iranian Journal of Basic Medical Sciences 2016, 19, 779. [Google Scholar] [PubMed]
- Philippe Rousselot; Prost, S. ; Guilhot, J.; Roy, L.; Etienne, G.; Legros, L.; Charbonnier, A.; Valérie Coiteux; Pascale Cony-Makhoul; Huguet, F.; Cayssials, E.; Jean-Michel Cayuela; Relouzat, F.; Delord, M.; Bruzzoni-Giovanelli, H.; Morisset, L.; Mahon, F.; Philippe Leboulch. Pioglitazone Together with Imatinib in Chronic Myeloid Leukemia: A Proof of Concept Study. Cancer 2016, 123, 1791–1799. [Google Scholar] [CrossRef]
- Beatriz, A.; Miranda, E. C.; Oliveira, M.; Bruna Rocha Vergílio; Pavan, C. ; Marcia Torresan Delamain; Gislaine Borba Duarte; Carmino Antonio Souza; De, E. V.; Pagnano, K. B. Pioglitazone Did Not Affect PPAR-Γ, STAT5, HIF2α and CITED2 Gene Expression in Chronic Myeloid Leukemia Patients with Deep Molecular Response. Blood 2019, 134, 1637–1637. [Google Scholar] [CrossRef]
- Bosetti, C.; Rosato, V.; Buniato, D.; Zambon, A.; La Vecchia, C.; Corrao, G. Cancer Risk for Patients Using Thiazolidinediones for Type 2 Diabetes: A Meta-Analysis. The Oncologist 2013, 18, 148–156. [Google Scholar] [CrossRef]
- Wen, W.; Wu, P.; Gong, J.; Zhao, M.; Zhang, Z.; Chen, R.; Chen, H.; Sun, J. Association of Pioglitazone with Increased Risk of Prostate Cancer and Pancreatic Cancer: A Functional Network Study. Diabetes Therapy 2018, 9, 2229–2243. [Google Scholar] [CrossRef]
- Dicitore, A.; Caraglia, M.; Gaudenzi, G.; Manfredi, G.; Amato, B.; Mari, D.; Persani, L.; Arra, C.; Vitale, G. Type I Interferon-Mediated Pathway Interacts with Peroxisome Proliferator Activated Receptor-γ (PPAR-γ): At the Cross-Road of Pancreatic Cancer Cell Proliferation. Biochimica et Biophysica Acta (BBA) - Reviews on Cancer 2014, 1845, 42–52. [Google Scholar] [CrossRef]
- Ninomiya, I.; Yamazaki, K.; Oyama, K.; Hayashi, H.; Tajima, H.; Kitagawa, H.; Sachio Fushida; Fujimura, T. ; Ohta, T. Pioglitazone Inhibits the Proliferation and Metastasis of Human Pancreatic Cancer Cells. Oncology Letters 2014, 8, 2709–2714. [Google Scholar] [CrossRef]
- Koga, H. PPARγ Potentiates Anticancer Effects of Gemcitabine on Human Pancreatic Cancer Cells. International Journal of Oncology 2011, 40, 679–685. [Google Scholar] [CrossRef]
- El-Sisi, A. E.; Sokar, S. S.; Salem, T. A.; Abu, S. E. PPARγ-Dependent Anti-Tumor and Immunomodulatory Actions of Pioglitazone. Journal of Immunotoxicology 2014, 12, 308–316. [Google Scholar] [CrossRef] [PubMed]
- Saman Bahrambeigi; Morteza Molaparast; Sohrabi, F. ; Lachin Seifi; Faraji, A.; Fani, S.; Vahid Shafiei-Irannejad. Targeting PPAR Ligands as Possible Approaches for Metabolic Reprogramming of T Cells in Cancer Immunotherapy. Immunology Letters 2020, 220, 32–37. [Google Scholar] [CrossRef] [PubMed]
- Hu, J.; Chen, J.; Cui, Y.; Zhu, Y.; Ren, W.; Zhou, X.; Liu, L.; Chen, H.; Zu, X. Association of Metformin Intake with Bladder Cancer Risk and Oncologic Outcomes in Type 2 Diabetes Mellitus Patients. Medicine 2018, 97, 11596. [Google Scholar] [CrossRef] [PubMed]
- Liu, C.Q.; Sun, J.X.; Xu, J.Z.; Qian, X.Y.; Hong, S.Y.; Xu, M.Y.; An, Y.; Xia, Q.D.; Hu, J.; Wang, S.G. Metformin Use on Incidence and Oncologic Outcomes of Bladder Cancer Patients with T2DM: An Updated Meta-Analysis. Frontiers in Pharmacology 2022, 13, 865988. [Google Scholar] [CrossRef]
- Hattum, van; Max, B. ; Oddens, J. R.; Theo; Wilmink, J. W.; Molenaar, R. J. The Effect of Metformin on Bladder Cancer Incidence and Outcomes: A Systematic Review and Meta-Analysis. Bladder Cancer 2022, 8, 211–228. [Google Scholar] [CrossRef]
- Tseng, C.H. Metformin May Reduce Bladder Cancer Risk in Taiwanese Patients with Type 2 Diabetes. Acta Diabetologica 2014, 51, 295–303. [Google Scholar] [CrossRef]

Table 1.
Molecular mechanisms of pioglitazone.
| Process | Mechanism | Cancer Type |
| Proliferation & Growth | Increased expression of excitatory amino acid transporter 2 [43]. | Neuroblastoma |
| Increased activity of p-Akt and p-GSK-3β [43]. | ||
| Redifferentiation of tumor associated adipocytes [43]. | ||
| Inhibited cell growth via mTOR and STAT5 pathway tampering by retinoid X receptor agonists [44]. | Glioma | |
| Inhibited expression of estrogen receptor and aromatase via PGE2 and BRCA1 pathways [45]. | Breast cancer | |
| Inhibition of JAK2/STAT3 pathway [46]. | ||
| Increased expression of p21 and MAPK activity [47]. | ||
| Inhibited CSC proliferation due to decreased STAT5 and HIF-2α levels [48]. | Chronic myeloid leukemia | |
| Downregulated MAPK, RAS, MYC gene expression and phosphorylation of MAPK pathway proteins [49]. | Non-small cell lung cancer | |
| Apoptosis | Downregulation of BCL2 and SCD1 [43]. | Leukemia |
| Reduced expression of MEK1 and ERK phosphorylation [50]. | ||
| Downregulation of STAT3 with ERK1/2, NF-κβ and p38MAPK molecules unaffected [51,52]. | ||
| Reduced expression of Survivin [51,52]. | ||
| Increased expression of TRAIL death ligand and apoptosis inducing factor [51,53]. | ||
| Downregulation of BCLXL/BCL2 in a PPARγ and caspase-independent manner [51]. | Prostate cancer, squamous cell carcinoma | |
| Induction of apoptosis in a caspase-dependent manner assisted by downregulation of c-FLIP, leading to BCL2 downregulation and instability [54]. | Caki cells | |
| Downregulation of X-linked inhibitor of apoptosis (XIAP) and cyclooxygenase-2 (COX-2) [55]. | Colorectal cancer | |
| Upregulation of cyclinB1, CDC2, p21 and alteration of BAX/BCL2 ratio [55]. | ||
| Angiogenesis [43,44,45,56,57,58] |
Reduced expression of matrix metalloproteinase 2 (MMP2), vascular endothelial growth factor (VEGF), COX-2. | Hepatocellular carcinoma |
| Inhibition of fibroblast growth factor 2 (FGF-2) and urokinase plasminogen activator. | ||
| Apoptosis of endothelial cells. | ||
| Combined downregulation of COX-2 and VEGF when coupled with clofibric acid [44]. | Ovarian cancer | |
| Reduction of bFGF and VEGF initiated angiogenesis [59]. | Chick chorioallantoic membrane model | |
| Drug Sensitization | Reduced expression of metallothionein and endorphin connected to S273 phosphorylation [60]. | Pancreatic cancer |
| Enhanced type I Interferon activity due to inhibition of the STAT-3 pathway [58]. | ||
| Increased arsenic trioxide induced tumor toxicity through inhibition of the PI3K/AKT pathway [44]. | Leukemia | |
| Doxorubicin sensitization via modulation of P-glycoprotein [56]. | Osteosarcoma | |
| Reduced resistance to cisplatin [45]. | ||
| Cell Cycle Modification |
Increased cisplatin and oxiplatin efficacy. | Thyroid, lung, prostate, breast, kidney, esophageal and urothelial cancer |
| Inhibited EGFR/MDM2 mediated chemoresistance and PPARγ degradation [49]. | ||
| Downregulation of cyclin dependent kinase 4 (CDK4). | ||
| Upregulation of CDK inhibitors including p19, p21, p27 and rho-related GTP binding protein. | ||
| Activation of Rb protein [50,60]. | ||
| Downregulation of cyclins D, cyclin E, CDK2, CDK4, proliferating nuclear antigen and retinoblastoma protein [58]. | Breast and colorectal cancer | |
| Differentiation | Induced adipogenesis [57]. | Melanoma |
| Immunomodulation | Increased β3 and α5 integrin expression [57]. | Colorectal cancer |
| Reduced PD-L1 levels due to autophagy [61]. | Lung, colorectal cancer | |
| Bioenergetics | Reduced pyruvate oxidation and glutathione levels. | Hepatocellular carcinoma |
| ROS-induced stress mediated by HIF-1 and NF-κβ signaling. | ||
| Metastasis & Invasiveness | Downregulation of smad family member 3 (SMAD3), PDK1 and MCT-1. | Breast cancer |
| Upregulation of plasminogen activator inhibitor-1 (PAI-1). | ||
| Downregulation of NF-κβ, eIF2α, MMP9 and fibronectin [62]. | Lung cancer | |
| Upregulation of CXCR4, CXCR7, E-cadherin [46]. | ||
| Downregulation of TGF-β. | Glioma | |
| Reduced expression and invasiveness of β-cantenin [45]. | Breast cancer | |
| Downregulation of TGFβR1 and SMAD3 associated with epithelial to mesenchymal transition (EMT) [63]. | Non-small cell lung cancer | |
| Autophagy | Upregulation of HIF-1 and BNIP3 [50]. |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



