
Submitted:
03 December 2024
Posted:
04 December 2024
You are already at the latest version
Abstract
BACKGROUND With a progressively aging global population, the prevalence of Parkinson’s Disease and dementia will increase, thus multiplying healthcare burden worldwide. Sensing technology can complement current measures used for symptom management and monitoring. The aim of this umbrella review is to provide future researchers with a synthesis of current methodologies and metrics for use of sensing technologies for the management and monitoring of activities and behavioral symptoms in older adults with neurodegenerative disease. This is of key importance when considering the rapid obsolescence of and potential for future implementation of these technologies into real-world healthcare settings. METHODS Seven medical and technical databases were searched for systematic reviews (2018-2024) which met inclusion/exclusion criteria. Articles were screened independently using Rayyan. PRISMA guidelines, the Cochrane Handbook for Systematic Reviews, and the Johanna Briggs Institute Critical Appraisal Checklist for Systematic Reviews were utilized for assessment of bias, quality, and research synthesis. A narrative synthesis combines the study findings. RESULTS After screening 1458 articles, 9 systematic reviews were eligible for inclusion, synthesizing 402 primary studies. This umbrella review reveals that use of sensing technologies for observation and management of activities and behavioral symptoms is promising, however diversly applied, heterogenous in methods used, and currently challenging to apply within clinical settings. CONCLUSIONS Human Activity and Behavioral Recognition requires true interdisciplinary collaborations between engineering, data science, and healthcare domains. Standardization of metrics, ethical AI development, and a culture of research-friendly technology and support are the next crucial developments needed for this rising field.
Keywords:
dementia
; Parkinson’s Disease
; human activity recognition
; sensing technology
; wearables
; sensors
; non-motor symptoms
; behavioral and psychological symptoms
; systematic review
1. INTRODUCTION
Currently there are almost one billion people over the age of 60 years worldwide. [1] Increased age is associated with increased prevalence of neurological diseases such as Parkinson’s disease (PD) and dementia, which affect 15% of the current population. [1,2,3] PD prevalence is increasing faster than any other neurological disorder worldwide [3] and dementia is estimated to affect 139 million people globally by 2050 [2]. In addition, these diseases cost global economies trillions of dollars each year. [1,2] Sensing technologies, such as wearables, are one available solution which can help address limitations and challenges of aging, however, also introduce complex topics such as the suitability of biometric applications within real-world healthcare scenarios. [4]
1.1. Physical Activity Metrics
Physical activity metrics such as step counts, energy expenditure, awake vs. sleep time, and intensity of various classified activities (light, moderate, vigorous), are the most studied digital biomarkers regarding activities. [5] Accuracy challenges of commercial wearables, such as Fitbit, in detection of physical activity biomarkers is well documented and previous studies conclude that beyond use for measurement of step counts in healthy individuals, researchers should use discretion when employing the devices for healthcare decisions. [5,6] Regardless of this, activity is a highly researched metric and decreased overall physical activity is associated with increased mortality risk in older adults. [7] Additionally, reduced capacity of ADLs is associated with increased severity of behavioral symptoms [7], making both key biomarkers for older persons with neurological diseases. This umbrella review defines activities using metrics for physical activity and functional activities of daily living (ADL) such as transitions, sitting, lying, standing, and sedentary activities.
1.2. Behavioral Symptoms of PD and Dementia
Although PD has classically been categorized and diagnosed based on the presence of cardinal motor-symptoms, such as slowness of movements (bradykinesia), rigidity and resting tremor, behavioral symptoms are currently being investigated as an important tool within both the prodromal (10-20 years prior to emergence of motor symptoms) and diagnostic stages (pre-motor and motor).[8] These behavioral symptoms go largely undiagnosed and are under-managed over disease progression. These symptoms can include constipation (50-60%), sleep disorders (60-90%), depression (35%), anxiety (40%), apathy (25-40%), hallucinations (33-42%), fatigue, pain (85%), orthostatic hypotension, urinary incontinence and dementia.[8,9] Likewise, behavioral and psychological symptoms of dementia, also referred to as neuropsychiatric symptoms, effect up to 90% of people with dementia over the course of the illness and include agitation, anxiety, apathy, euphoria, depression, hallucinations, and sleep disturbances.[10] This review focuses on behavioral symptoms which are most commonly measured with sensing technology and associated with a diagnosis of PD or dementia, for example; agitation, anxiety, apathy, depression, and sleep disturbances. Recent studies have shown that the use of sensing technologies, such as actigraphy and machine learning predictive models for behavioral symptoms are feasible and show positive correlations with traditional outcome measures for symptoms such as apathy and agitation. [11,12,13,14]
1.3. Human Activity and Behavioral Recognition in People with PD or Dementia
Human activity recognition (HAR) is a fast-growing field rooted within engineering and computer science. The field has changed rapidly over the last ten years, requiring a cutting-edge and broader approach.[15] A scoping review by Huhn et al. (2022) concluded that use of wearables in research has increased exponentially from 2013-2020, and has included almost 11 million total participants.[16] Combined with other technologies such as Internet of Things (IoT) and Artificial Intelligence (AI), HAR can give high accuracy, precision, and recall of activity classification. [17] HAR is classically defined as a process which identifies and classifies human activities over time based on measurements made by digital sensing devices, wearables, or non-wearables. [18] Gupta et al. (2022) further defines HAR as “the art of identifying and naming activities” and expands the traditional definition to include behavioral symptoms such as agitation, sleep disturbance, pain, and apathy. [19] Common sensors utilized for HAR include accelerometer, gyroscope, magnetometer, radar-sensors (wireless), and Global Positioning Systems (GPS).
According to the Cochrane Handbook for Systematic Reviews [20] an umbrella review, or an overview of reviews, should “use systematic methods to identify multiple systematic reviews on a related research question with the goal to extract and analyze results across outcomes”. We chose to conduct an umbrella review as there is a need to synthesize existing literature to inform future practice and research at this pivotal point in the field of HAR. We found that many systematic reviews and surveys have been published, especially within the last 5 years, regarding the use of sensing technologies for management and observation of activity and behavioral symptoms [21,22,23,24,25]. We chose to narrow this umbrella review to people of advanced age (>65 years) and with neurodegenerative disease (PD or dementia), as these populations continue to grow at unprecedented rates, presenting healthcare systems with immediate challenges to which these sensing technologies and techniques could be a viable solution.
1.4. Research Questions
- What are the current methods, sensing technologies, and AI techniques being used for activity and behavioral symptom recognition in older people with PD or dementia?
- Are statistical analyses and study protocols within the studies heterogeneous and/or reproducible?
- What gaps and possibilities exist in bringing research related to the use of sensing technologies for management and monitoring of human activity and behavioral symptoms into real-world settings and clinical practice for older adults with PD or dementia?
2. METHODS
This umbrella review follows standards set by Cochrane and the Johanna Briggs Institute Critical Appraisal Checklist for Systematic Reviews (JBI) [26] for methodology and reporting guidelines. We in addition use the rationale and guidelines for conducting an umbrella review provided by Choi et al. (2023).[27] To identify relevant and clinically useful studies for the purposes of classifying non-motor symptoms (i.e.: agitation, apathy, sleep disturbance) and functional activities of daily living in persons with PD or dementia, we have excluded systematic reviews primarily focused on gait and pure motor functions. In collaboration with the University of Bergen Medical Library, we developed a working search strategy, including PICO and inclusion/exclusion criteria, which are detailed in Table 1 and Table 2.
2.1. Search Strategy
Initial searches were conducted between September 15 – October 31, 2023, using both MeSH terms and free-text words such as: “wearable electronic devices” OR “sensor technology” OR “fitness track*” AND “complex chronic diseas*” OR “dementia” AND “human activity recognition” OR “activity recognition” AND “aged” OR “older adult*” AND “systematic review” OR “review”. The final systematic search was conducted in Medline Ovid, Embase Ovid, Web of Science, Cochrane Library, Epistemonikos, the Institute of Electrical and Electronics Engineers (IEEE Xplore), and ACM Digital Library databases on October 31, 2023. Restrictions included: publication date January 1, 2018 to 2024. Articles before 2018 were not included as we considered that there has been a substantial amount of newly investigated technologies over the last 5-year period, exacerbated by the pandemic and recent growth within the wearable industry [16], including research conducted using both research-grade and commercial wearables. A complete list of search terms for each database can be found within the supplemental material (Appendix 1).
In accordance with regulations set by the International Prospective Register of Systematic Reviews (PROSPERO), protocol registration was completed prior to data extraction of included articles and accepted in PROSPERO December 9, 2023 (CRD42023487121). Duplicates were removed using EndNote, and Rayyan [28,29] was used as a screening tool. Four reviewers (LDB, LG, MP, LS) conducted an independent, blind screening using Rayyan based on title and abstract from October 27 – November 10, 2023. An unblinded assessment of full-text articles identified as “conflicts” within Rayyan was conducted by four researchers (LDB, LG, BM, MP) between the dates of November 10 – December 10, 2023. PRISMA guidelines [30] were used for reporting of inclusions and study selection processes.
2.2. Data Extraction
Data was extracted by two researchers (LDB, LG). Disagreements were settled by discussion and resolved by a third party (BM) if agreement was not reached. Data was recorded in MS Excel spreadsheets and included categories for: author, date of publication, journal type, methods, technologies, primary articles within each systematic review (behavioral symptoms), AI, algorithms, statistical methods, thresholds, traditional measures as validators to digital biomarkers, aims, results, outcomes, datasets, and gaps in research or future directions.
2.3. Risk of Bias (Quality) Assessment
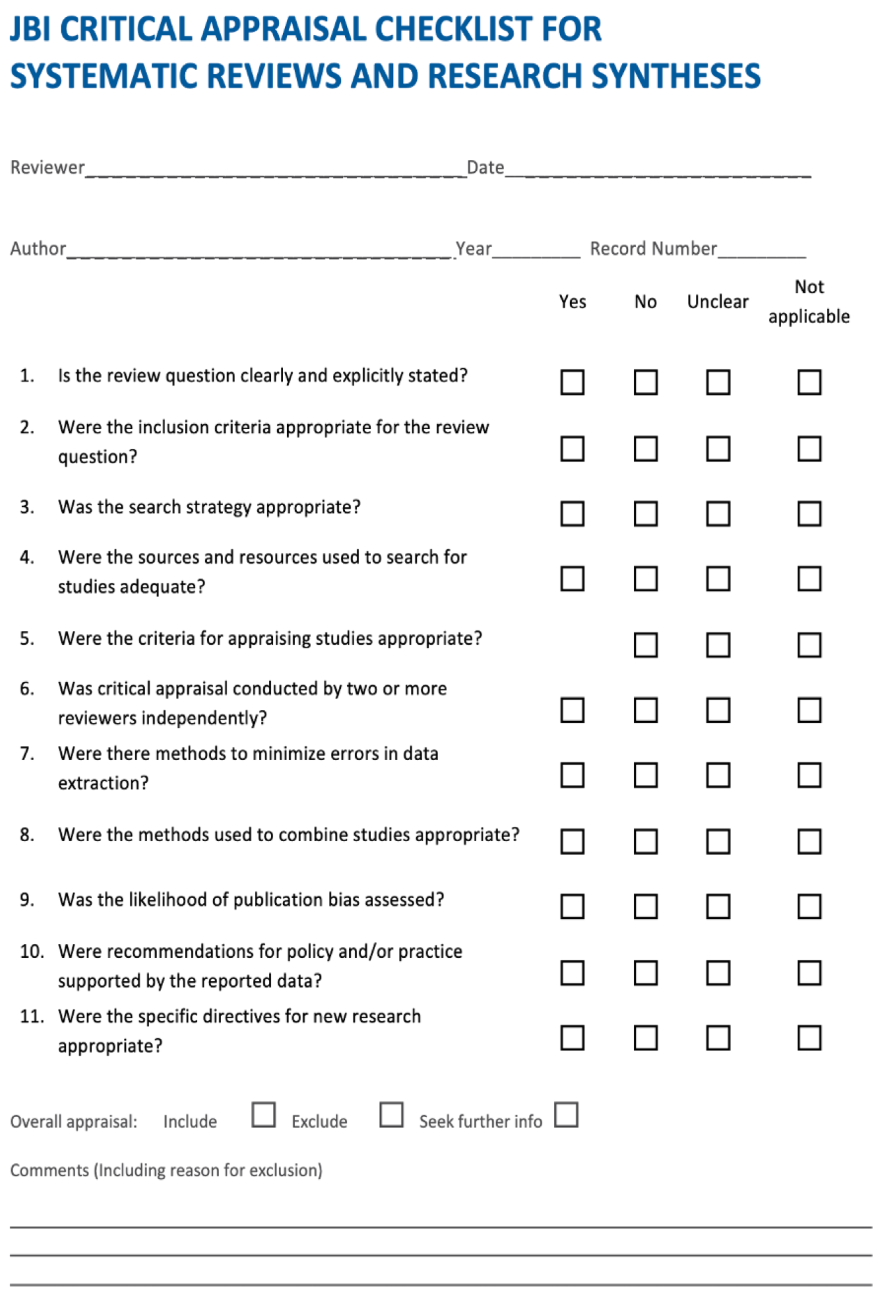
Assessment of risk and bias was conducted using the JBI Critical Appraisal Checklist for Systematic Reviews and Research Syntheses. [26] The JBI consists of eleven total questions, resulting in an overall appraisal decision for: 1) inclusion, 2) exclusion, 3) seek further info (Appendix 2). The results of the assessment were used to inform data extraction and synthesis and as assessment for the overall decision and quality for inclusions (Appendix 3). Three reviewers (LG, BM, MP) were involved in the quality assessments. Disagreements between reviewers were resolved by discussion and if agreement was not reached, a fourth researcher (LDB) settled all disputes.
2.4. Data Synthesis
50% of all systematic reviews do not incorporate meta-analysis for various reasons [31,32] and none of the included systematic reviews offered a meta-analysis. Meta-analysis was therefore not possible in this umbrella review due to heterogeneity of metrics and analyses used within the included systematic reviews, and a narrative synthesis of the included articles was subsequently conducted. Comprised content from the articles was grouped according to:
- Type of journal (technical vs. medical), authors, country, year, number & demographics of participants, study setting (real world vs. laboratory)
- Relevancy to HAR used for digital phenotyping and/or classification of behavioral symptoms
- Sensors, devices, AI, datasets, gold standard outcome measures, biomarkers, validation
- Reproducibility (i.e.: transparency and clarity of algorithms and technical details, inclusion of important demographic details such as age and diagnosis)
- Inclusion of ethical considerations, data protection
- Future recommendations from studies
- Studies conducted for an advanced stage of disease or end-of-life
- Consent procedure (informed vs. presumed)
3. RESULTS
A total of 1458 articles were identified and after removal of duplicates (n=392), 1066 articles were independently reviewed based on title and abstract. Two additional systematic reviews were identified by snowballing and full text review was conducted on a total of 20 articles. Articles were excluded based on the following reasons: not a true systematic review, focus on diagnosis of disease, HAR used for only motor symptoms of PD, fall prevention or prediction specific, did not include persons with PD or dementia, focused on commercial app development, study featured sensing technology for telehealth purposes, and one article did not meet the critical appraisal tool standards and was therefore excluded. A total of 1058 articles were excluded, resulting in 9 included high quality systematic reviews; Figure 1 presents the PRISMA flow diagram, detailing the process, including reasons for exclusion.
3.1. Included Systematic Review Characteristics
In total, within the nine included systematic reviews (Table 3), 402 individual primary studies were assessed. The included systematic reviews represent research from eleven countries. Most of the nine included systematic reviews offered evidence for a combination of management of activities and behavioral symptoms. We provide a summary of the included 9 systematic reviews in Table 3. As recommended by Faulkner et al. (2021)[33], this umbrella review sought to describe the primary studies in a more meaningful way. We therefore provide the reader a detailed summary (Appendix 6-7) of 28 primary studies within the total 402 individual primary studies assessed which were focused on the growing research topic of behavioral symptoms such as agitation, apathy, and sleep disturbances to enhance knowledge of metrics and methods used for measurement of these less researched digital biomarkers for future studies. Within the 9 included systematic reviews we identified 10 overlapping primary studies.
Sample sizes for the primary studies ranged between 1-2063 participants. The included systematic review by Morgan et al. (2020) [34] found that approximately 68% of publications had less than 50 participants and similarly, Esquer-Rochin et al. [35] stated that studies using existing databases included an average of 10 or less participants, and an average of 40 participants where ad-hoc datasets were utilized. Mean ages of included participants ranged from 22 to 95 years; five of the nine studies did not include a summary of mean age. All included systematic reviews included people with dementia, Alzheimer's disease, or PD as a primary or secondary diagnosis.
3.2. Sensing Technology, Devices, and Current Use in Research
All of the 9 included systematic reviews combined findings for accelerometry for detection of both activities and behavioral symptoms [34,35,36,37,38,39,40,41,42]. In addition, non-wearables [34,35], pressure sensors [35,40], robots [35], smart devices [34], GPS [35,37] triaxial sensors (including accelerometer, gyroscope and magnetometer) [34,35,40,41] and ambient home sensors [34,36,39] also made the stage; combining multiple wearable sensors (wrist and low back placement being the most common) and video or diary input for analysis and confirmation of data (i.e.: agitation events) was noted regarding efforts for classification of activities and behavioral symptoms [34,39,40] (Table 3).
Included systematic reviews by McArdel (2023)[37] and Breasail et al. (2021)[38] describe the use of sensing technologies to measure volume, intensity, pattern and variability of physical activity in persons with dementia, both stating that this is currently the most common use of accelerometry (actigraphy) within this population of patients. In agreeance with the included systematic review from Mughal et al. (2022) [41], we found that motor symptoms of PD are well studied and that research on sensing technologies for detection of behavioral symptoms is currently growing. An example of this primary research focus of motor symptoms of PD within our findings is the review by Sica et al. (2021) [42] who investigated home monitoring possibilities for persons with PD using sensing technologies, however included only one primary study dedicated to behavioral symptoms within their review, emphasizing the need for more synthesized literature on this topic. (Appendix 6-7)
3.3. Traditional Outcome Measures
Traditional “gold standard" assessment tools most frequently used within the included systematic reviews were Cohen-Mansfield Agitation Inventory (agitation) [43], Mini-Mental Status Exam (cognition) [44], Unified PD rating scale (staging of disease and function) [45], Montreal Cognitive Assessment (cognition) [46] and the Neuropsychiatric Inventory (behavioral symptoms) [[47]. This umbrella review had similar findings to Khan et al. (2018) (43% did not include traditional assessments) [40] and found that 22% of the included systematic reviews did not include information regarding gold standard assessment comparisons and that 67% included some information, but was incomplete. Digital biomarkers within the studies were also vast, with the most utilized being physical activity parameters such as sleep vs. wake time, step counts, activity counts, intensity of activities (low-high), activity amplitude, sedentary time, and classification of activities of daily living such as upright posture, sitting, standing, and walking (Table 3). Sleep disturbance and agitation were the most investigated behavioral symptoms.
3.4. Study Protocols and Methods
The protocols for data collection using the sensing technologies varied greatly from several hours to as long as one year, the most common metric being 7 days [36,37,38,39] followed by 48-72 hours [36,37,39,41]. In 33% of the included systematic reviews [34,39,40], the protocol was either not mentioned, or not given in full description for each study. Statistical analyses, protocols, and methods used within the articles investigated in the systematic reviews were heterogeneous and subsequently, meta-analysis was not possible or performed. A summary of statistical analyses utilized within the included primary studies, concentrated on articles covering behavioral symptoms, is provided in the supplementary materials (Appendix 6-7).
3.5. AI and Algorithms
A wide range of algorithms and AI techniques are mentioned in the included studies, among which are: fuzzy logic, time-frequency analysis, forward feature selection, random forest, k-nearest neighbors, support vector machines, artificial and deep neural networks [34,38,39,41]. Support vector machines were the most prevalent across all studies, while 55% of the studies [33,35,36,37,41] did not provide information on algorithms/AI for extracting activity/behavior information from sensor data. The systematic review by Sica et al. (2021) [42] provides a robust synthesis of AI, signal processing information, and performance validity of the included primary studies, reporting that algorithm based classification methods using digital biomarkers for bradykinesia, transitions (turning), gait and tremor resulted in moderate to high accuracy and validity compared to corresponding symptom diaries, and reflected upon the potential of AI and digital biomarker-based algorithms in efforts to enhance meaningful data gathered using commercial devices in a real-world setting. [42]
3.6. Datasets
One [35] out of the nine included systematic reviews highlighted current datasets that were used within simulated, laboratory-based studies. Esquer-Rochin et al. included a total of 104 primary articles within their systematic review, providing a thorough description of current datasets.[35] Of the existing mentioned datasets, ADNI, PD Telemonitoring, AZTIAHO, Parkinson’s dataset and Daphnet, include participants that have a diagnosis of Alzheimer’s or PD. [35] Three others additionally include older adults, OASIS, CASAS, and PUCK, however details of the demographics are not clearly stated. [35] Only 2 out of the 15 total datasets were directly applicable to use for HAR for persons with PD or dementia. [35] A description of all included datasets can be found in Appendix 4.
3.7. Quality & Bias Assessment
We conducted a critical appraisal of quality and potential biases using the Johanna Briggs Institute (JBI) Critical Appraisal Checklist for systematic reviews and found a score of eight out of eleven (moderate-good) for all included studies, except for Anderson et al. 2020, where only 6 out 11 questions were answered with a “yes”. A detailed list of questions on the JBI and conducted review can be found in the supplementary materials (Appendix 3-4). We excluded the umbrella review by Andersson et al. (2020) based upon its JBI score. Assessment scores were most affected because the studies did not provide a clear statement as to whether a critical appraisal was performed, and what tools were used.
3.8. Recommendations from Included Systematic Reviews
The future perspectives provided by the articles published within the technical vs. medical journals differed greatly. An example can be seen in the summary of suggestions from Esquer-Rochin et al. (2023) [35], concluding that collection of more data is the highest priority among the 104 technical primary papers included in their systematic review. In contrast, the highest-ranking future priorities within the articles published within the medical journals were ethical concerns, development of best practices for data management, and technology which is best suited to the participants and research needs (validation of technology).(Appendix 5) Included systematic reviews from Ardelean and Redolat (2023) [36] and Khan et al. (2018) [40] discuss ethical and safety issues, including unforeseen consequences of technology, and conclude that these topics should be highlighted in future research. Johansson et al. (2018) [39] emphasizes the need to take a “leap of faith” in the application of HAR and similar technologies for clinical trials and implementation into real-world settings. Breasail et al. (2021) [38] further discusses commercial vs. research grade sensing technologies and the need to best discriminate between which is most appropriate for future use in studies and real-life application, emphasizing the need to improve and validate devices and algorithms.
4. DISCUSSION
This umbrella review sought to answer several research questions and found that: 1) methods, sensing technologies, algorithms and AI techniques being used in HAR for persons with PD or dementia are diverse, and that standardization of the metrics and strategies in the field, across disciplines is a necessary step forward to allow potential application of HAR in clinical and real-life settings; 2) statistical analyses and study protocols are heterogeneous and introduce potential bias, decreasing generalization and reproducibility of study results; and 3) there are many opportunities for furthering research withing the field of HAR for persons with PD and dementia, including the topics/gaps of behavioral symptom management, use of HAR throughout the progression of disease including the end-of-life, improved data mining techniques and management of big data (minimalization), validation of technologies, and encouraging cross-collaboration and true interdisciplinary work.
The included systematic reviews by Khan [40] Mughal [41], and Ardelean [36] et al. found that the most common current use of HAR for behavioral symptoms is for detection and management of depression, apathy, agitation and sleep deprivation, however, we agree most with the systematic review by Mughal et al. (2022) [41] which stated that behavioral symptoms are often ignored and currently not well studied. We recommend a future systematic review be performed on the latest HAR methods for behavioral symptoms as a continuation and update of this topic, especially considering the rapidly evolving nature of the field.
Sample size is a common theme throughout the included systematic reviews. We will note that when it comes to the use of sensors, dataset size assessments are fourfold: unique sources (number of participants), datapoints (number of measurements), variety (number of action types), and modality (number of sensor types). Digital sensors usually generate a significant number of datapoints, from 24 per day (e.g., actigraphy measures) to approx. 8.3 million per day (e.g., 3-axis accelerometer at 32 Hz).
4.1. Underrepresentation and Ethical Considerations
Many people with dementia and other advanced neurological conditions are excluded from research based on structural discrimination, measures designed to protect them from harm (i.e.: informed consent), or inadvertently through lack of awareness of participants’ needs and difficulties. [76] Study demographics, including age and disease stage, can have a big impact on results. [77,78] In 2020 Alzheimer Europe published a report titled Overcoming ethical challenges affecting the involvement of people with dementia in research: recognizing diversity and promoting inclusive research [79]; the report states that ethics in dementia research extends from traditional standards of “do no harm” to include empowerment, rights, respect, equity and well-being and emphasizes that appropriate adaptations must be made to ensure that people with dementia have the same opportunities to take part in research. Likewise, future studies involving these vulnerable participants should consider possible unforeseen challenges and consequences of introducing these devices at later stages of disease, and acceptance should be addressed within the studies, as emphasized within the included systematic review by Johannesen et al. (2018)[39].
Khan et al. (2018)[40] brings to light the important topic of ethics related to the use of sensing technologies with vulnerable groups of patients and considers this a gap within the literature as only 7% of the included studies within their systematic review addressed ethical challenges, similar to our findings across all the included reviews. Rubeis et al. (2020) explored the “disruptive power” of AI in elderly care and identified four main risks in the use of AI and phenotypes for detecting and managing neurodegeneration in older adults: depersonalization, discrimination (including ageism), dehumanization, and disciplining (i.e.: enforcing norms) through the collection of big data.[80] The author discusses issues such as the use of AI for clinical decision making and reliance on algorithms for prediction of health outcomes, assessment of risks, and choice of appropriate interventions, which have a large impact on clinical responsibility, accountability and trust [80].
4.2. Future Directions
We identified several intersections between the medical and technical literature included in this umbrella review for future research direction: more research in real-world settings, validation of technologies for monitoring of symptoms of PD and dementia, more research conducted at late stages of neurodegenerative diseases, and adaptive technology to individual progression (precision models). Standardization of metrics, protocols, statistical methods, and use of AI and algorithms is necessary for real-life, real-time application of sensing technologies. A scoping review by Alfalahi et. al (2023) [81] introduced a novel paradigm the authors call “explainable digital phenotyping” influenced by brain, body, and social behavioral decline, based on validation of digital biomarkers and reliant on multidisciplinary co-creation combining AI and knowledge from healthcare professionals; the authors highlight the complexities of using digital sensing technologies as an unbiased data-driven approach for behavioral quantification, including the need for empirical consensus on standardization, reliability, and interpretation.
Morgan et al. (2023)[82], in agreeance with previous articles [83], describes dataset information related to “REal world Mobility Activities in PD” and details 20 total existing datasets, with only two including participants >44 years of age. The article further provides foundational research for future datasets with a detailed opened dataset named REMAP featuring transitional ADLs and participants with PD (61.25 years +-8.5).[82] Morgan et al.’s (2023)[82]results support our findings in the included systematic review by Esquer-Rochin et al. (2023)[35] that current datasets are largely unrelated to persons with PD or dementia, and future work should provide more robust datasets featuring transparent representation of older people with neurodegenerative diseases.
The included systematic review by McArdel et al. (2023)[37] revealed that over 50% of the included primary studies did not include information about validation of the technology used. Morgan et al. (2020)[34] offers the reader a future suggestion that testing the technology against itself using test-retest repeatability may be the best way to validate results in future studies. Traditional methods for validation, such as comparison to a gold-standard outcome measurement, may not correlate to the measurements taken by the device, and this may not always be a negative scenario. Measurements taken through HAR sensing methods should in theory be able to pull out details that subjective traditional outcome measures, such as the NPI, do not capture. This makes it difficult to conduct validation comparisons in the traditional sense. With the challenge of rapid obsolescence of new technologies, future studies may need to shift validation efforts away from specific device brand and model and towards characteristics of the devices that are a best fit for patient care scenarios and develop new methods for validation.
5. LIMITATIONS & STRENGTHS
This systematic umbrella review has several limitations. Gaps in the evidence are possible should the included systematic reviews not comprehensively cover the intended topic, which was found to be true in this case as most of the included reviews reported results for our topic within a broader context, encompassing both motor, activity and behavioral uses for HAR. As a result of our search results, we identified a gap in literature surrounding the topic of HAR for management and monitoring of behavioral symptoms. To address this gap, we included for the reader further analysis of the primary studies from within the included systematic reviews which were directly related to behavioral symptoms use for HAR (Appendix 6-7) in efforts to expand knowledge on this growing topic of interest. The overlap of included primary studies was assessed and reported to further reduce bias. The validity of any umbrella review depends highly on the quality of the included studies and existing systematic reviews. To assess quality and further reduce bias, three researchers performed a critical appraisal of all included reviews. As with standard systematic reviews, there is potential for missed studies, small study bias, missed outcomes, selective reporting bias, and study publication bias, which can influence results and effect the validity of the review. [84] Only 33% of the included systematic reviews deployed a search strategy including one or more technical database (i.e.: IEEE or ACM), creating potential for missed studies within the fields of engineering and data science [34,40,41]. To reduce bias between technical vs. medical literature, we included four multi-disciplinary reviewers for initial selection based on title and abstract and final full-text selection of articles. We also take into consideration that we have a narrow focus within this umbrella review on specific vulnerable groups (older adults, PD and dementia) and therefore may have missed studies which include HAR for younger participants and more general purposes. We further note, however, that by using the narrow scope of older adults, PD and dementia, we uncover true gaps within this specific and important sector. Lastly, another limitation of this umbrella review was that a meta-analysis was not possible as the included quantitative literature did not include a meta-analysis because measurements were clinically heterogeneous and used inconsistent metrics for analyses.
6. CONCLUSIONS
HAR has the potential to enrich knowledge of digital biomarkers which can help guide clinical decision making for people with PD and dementia. However, for HAR to be sustainable for real-world use in persons with neurodegenerative diseases, such as PD, a foundation of new interdisciplinary collaborations and a culture for technology complemented care is necessary. Researchers should improve knowledge and understanding of sample size relativity within the field of HAR, meaning that depending on the type of analysis employed, data quantities within smaller sample sizes might be sufficient if there are enough for both training of models and validation of technologies.
Future perspectives of HAR for monitoring activities and behavioral symptoms include the application of AI for prediction and observation, strategies for complementing knowledge and clinical differentiation of health professionals, and the empowerment of research participants encouraging ethical inclusion of participants in later stages of disease. Further accountability from the developers of the technologies used for HAR to discourage obsolescence and improve support, and more research friendly agreements with universities must be realized for future progress in this field.
7. DECLARATIONS
Author Contributions
All authors contributed to the study conception, design, development of search strategies and selection of literature based upon title and abstract. LDB and LG contributed to data extraction and analysis and LG, BM, and MP conducted bias and quality assessments. LDB wrote the manuscript, and all authors read, edited, and approved the final versions.
Funding
Funding was provided by the Western Norway Regional Health Authority (Helse Vest RHF); sponsor protocol code: F-12829-D10484.
Ethics approval and consent to participate
The review is associated with a prospective cohort study (DIPH.DEM) which was approved by the Regional Committee for Medical and Healthcare Research Ethics (REK) on October 23, 2023: 634938.
Consent for publication
Not applicable.
Availability of data and materials
Not applicable.
Acknowledgments
We would like to thank Ida Sofia Sletten, Academic Librarian at The Medical Library, University of Bergen, Norway, for assistance with search criteria and support services throughout the project. BSH thanks the Trond Mohn Research Foundation, GC Reiber, and the Norwegian Government for supporting our work at the Centre for Elderly and Nursing Home Medicine, University of Bergen, Norway.
Competing interests
The authors acknowledge that there are no conflicts of interest.
ABBREVIATIONS
| AI | Artificial Intelligence |
| BPSD | Behavioral and Psychological Symptoms of Dementia |
| GPS | Global Positioning Systems |
| HAR | Human activity recognition |
| IoT | Internet of Things |
| JBI | Johanna Briggs Institute |
| MCI | mild cognitive impairment |
| PD | Parkinson’s Disease |
APPENDIX 1. Search strategies.
Ovid MEDLINE(R) and Epub Ahead of Print, In-Process, In-Data-Review & Other Non-Indexed Citations and Daily <1946 to October 30, 2023>
Date: 31.10.2023
1 (activity recognition or behavior recognition or behaviour recognition or wearable* or non-wearable* or non wearable* or nonwearable* or sensor or sensors or sensing technolog* or fitness track* or activity track* or smart phone* or smartphone* or digital device* or smartwatch* or smart watch* or internet of things or IoT or ubiquitous sensing or pervasive sensing or unobtrusive sensing or actigraph* or acceleromet*).ti,ab,kf. 279731
2 Wearable Electronic Devices/ or Fitness Trackers/ or "Internet of Things"/ or Digital Technology/ or Actigraphy/ or Accelerometry/ 22143
3 1 or 2 282869
4 (dementia* or Alzheimer* or lewy body or lewy-body or mild cognitive impairment* or Parkinson*).ti,ab,kf. 407094
5 exp Dementia/ or exp Parkinsonian Disorders/ 294719
6 4 or 5 455490
7 (Systematic review or scoping review or metaanalys* or metaanalyz* or meta-analys* or meta-analyz* or meta analys* or meta analyz*).ti,ab,kf. 445495
8 "Systematic Review"/ or Meta-Analysis/ 325679
9 7 or 8 481452
10 3 and 6 and 9 172
11 limit 10 to yr="2018 -Current" 144
Results: 144
Embase <1974 to 2023 October 30>
Date: 31.10.2023
1 (activity recognition or behavior recognition or behaviour recognition or wearable* or non-wearable* or non wearable* or nonwearable* or sensor or sensors or sensing technolog* or fitness track* or activity track* or smart phone* or smartphone* or digital device* or smartwatch* or smart watch* or internet of things or IoT or ubiquitous sensing or pervasive sensing or unobtrusive sensing or actigraph* or acceleromet*).ti,ab,kf. 312756
2 wearable sensor/ or wearable computer/ or motion sensor/ or sensor/ or exp smartphone/ or exp smart watch/ or digital technology/ or "internet of things"/ or accelerometry/ or actimetry/ 144812
3 1 or 2 336544
4 (dementia* or Alzheimer* or lewy body or lewy-body or mild cognitive impairment* or Parkinson*).ti,ab,kf. 569433
5 exp dementia/ or exp Parkinson disease/ 596015
6 4 or 5 712239
7 (Systematic review or scoping review or meta-analys* or meta-analyz* or meta analys* or meta analyz* or metaanalys* or metaanalyz*).ti,ab,kf. 553739
8 "systematic review"/ or exp meta analysis/ 565000
9 7 or 8 703746
10 3 and 6 and 9 318
11 limit 10 to yr="2018 -Current" 261
Results: 261
Cochrane Library
Date: 31.10.2023
ID Search Hits
#1 ("activity recognition" OR "behavior recognition" OR "behaviour recognition" OR wearable* OR (non NEXT wearable*) OR nonwearable* OR "sensor" OR "sensors" OR (sensing NEXT technolog*) OR (fitness NEXT track*) OR (activity NEXT track*) OR (smart NEXT phone*) OR smartphone* OR (digital NEXT device*) OR smartwatch* OR (smart NEXT watch*) OR "internet of things" OR "IoT" OR "ubiquitous sensing" OR "pervasive sensing" OR "unobtrusive sensing" OR actigraph* OR acceleromet*):ti,ab,kw 23963
#2 [mh ^"Wearable Electronic Devices"] OR [mh ^"Fitness Trackers"] OR [mh ^"Internet of Things"] OR [mh ^"Digital Technology"] OR [mh ^"Actigraphy"] OR [mh ^"Accelerometry"] 1704
#3 #1 OR #2 23986
#4 (dementia* OR Alzheimer* OR "lewy body" OR "lewy-body" OR ("mild cognitive" NEXT impairment*) OR Parkinson*):ti,ab,kw 38178
#5 [mh "Dementia"] OR [mh "Parkinsonian Disorders"] 15520
#6 #4 OR #5 38487
#7 #3 AND #6 1059
#8 #3 AND #6 with Cochrane Library publication date Between Jan 2018 and Dec 2023, in Cochrane Reviews 3
Results: 3
Epistemonikos
Date: 31.10.2023
(advanced_title_en:("activity recognition" OR "behavior recognition" OR "behaviour recognition" OR wearable* OR "non-wearable" OR "non-wearables" OR "non wearable" OR "non wearables" OR nonwearable* OR "sensor" OR "sensors" OR "sensing technology" OR "sensing technologies" OR "fitness tracking" OR "fitness tracker" OR "fitness trackers" OR "activity tracking" OR "activity tracker" OR "activity trackers" OR "smart phone" OR "smart phones" OR smartphone* OR "digital device" OR "digital devices" OR smartwatch* OR "smart watch" OR "smart watches" OR "internet of things" OR "IoT" OR "ubiquitous sensing" OR "pervasive sensing" OR "unobtrusive sensing" OR actigraph* OR acceleromet*) OR advanced_abstract_en:("activity recognition" OR "behavior recognition" OR "behaviour recognition" OR wearable* OR "non-wearable" OR "non-wearables" OR "non wearable" OR "non wearables" OR nonwearable* OR "sensor" OR "sensors" OR "sensing technology" OR "sensing technologies" OR "fitness tracking" OR "fitness tracker" OR "fitness trackers" OR "activity tracking" OR "activity tracker" OR "activity trackers" OR "smart phone" OR "smart phones" OR smartphone* OR "digital device" OR "digital devices" OR smartwatch* OR "smart watch" OR "smart watches" OR "internet of things" OR "IoT" OR "ubiquitous sensing" OR "pervasive sensing" OR "unobtrusive sensing" OR actigraph* OR acceleromet*)) AND (advanced_title_en:(dementia* OR Alzheimer* OR "lewy body" OR "lewy-body" OR "mild cognitive impairment" OR "mild cognitive impairments" OR Parkinson*) OR advanced_abstract_en:(dementia* OR Alzheimer* OR "lewy body" OR "lewy-body" OR "mild cognitive impairment" OR "mild cognitive impairments" OR Parkinson*)) [Filters: classification=systematic-review, protocol=no, min_year=2018, max_year=2024]
Publication year: 2018-2024
Publication Type: Structured summary:
Results: 0
Publication Type: Broad synthesis
Results: 6
Publication Type: Systematic review
Results: 121
Total results: 127
Web of Science Core Collection
Date: 01.11.2023
Entitlements:
- WOS.SCI: 1945 to 2023
- WOS.AHCI: 1975 to 2023
- WOS.ESCI: 2018 to 2023
- WOS.SSCI: 1956 to 2023
(TS=("activity recognition" OR "behavior recognition" OR "behaviour recognition" OR "wearable*" OR "non-wearable*" OR "non wearable*" OR "nonwearable*" OR "sensor" OR "sensors" OR "sensing technolog*" OR "fitness track*" OR "activity track*" OR "smart phone*" OR "smartphone*" OR "digital device*" OR "smartwatch*" OR "smart watch*" OR "internet of things" OR "IoT" OR "ubiquitous sensing" OR "pervasive sensing" OR "unobtrusive sensing" OR "actigraph*" OR "acceleromet*")) AND TS=("dementia*" OR "Alzheimer*" OR "lewy body" OR "lewy-body" OR "mild cognitive impairment*" OR "Parkinson*" ) AND (TS=("Systematic review" OR "scoping review" OR "meta-analys*" OR "meta-analyz*" OR "meta analys*" OR "meta analyz*" OR "metaanalys*" OR "metaanalyz*" OR "survey*" ) OR (TI=("review")))
7:32 PM | Timespan: 2018-01-01 to 2024-12-31 (Publication Date)
Results: 465
IEEE Explore: Digital Library
Date: 01.11.2023
("All Metadata":dementia* OR "All Metadata":Alzheimer* OR "All Metadata":"lewy-body" OR "All Metadata":"lewy body" OR "All Metadata":mild cognitive impairment* OR "All Metadata":Parkinson*) AND ("All Metadata":"Systematic review" OR "All Metadata":"scoping review" OR "All Metadata":meta-analys* OR "All Metadata":meta-analyz* OR "All Metadata":meta analys* OR "All Metadata":meta analyz* OR "All Metadata":"metaanalys* OR "All Metadata":"metaanalyz* OR "All Metadata":review OR "All Metadata":survey*)"activity recognition" OR "behavior recognition" OR "behaviour recognition" OR wearable* OR non-wearable* OR non wearable* OR nonwearable* OR sensor* OR sensing technolog* OR fitness track* OR activity track* OR smart phone* OR smartphone* OR digital device* OR smartwatch* OR smart watch* OR "internet of things" OR IoT OR "ubiquitous sensing" OR "pervasive sensing" OR "unobtrusive sensing" OR actigraph* OR acceleromet*
Filters Applied:
2018 – 2024
Results: 70
ACM Digital Library
Association for Computing Machinery
Date: 25.10.2023
(Title:("activity recognition" OR "behavior recognition" OR "behaviour recognition" OR wearable* OR non-wearable* OR non wearable* OR nonwearable* OR sensor* OR sensing technolog* OR fitness track* OR activity track* OR smart phone* OR smartphone* OR digital device* OR smartwatch* OR smart watch* OR "internet of things" OR IoT OR "ubiquitous sensing" OR "pervasive sensing" OR "unobtrusive sensing" OR actigraph* OR acceleromet*) OR Abstract:("activity recognition" OR "behavior recognition" OR "behaviour recognition" OR wearable* OR non-wearable* OR non wearable* OR nonwearable* OR sensor* OR sensing technolog* OR fitness track* OR activity track* OR smart phone* OR smartphone* OR digital device* OR smartwatch* OR smart watch* OR "internet of things" OR IoT OR "ubiquitous sensing" OR "pervasive sensing" OR "unobtrusive sensing" OR actigraph* OR acceleromet*) OR Keyword:("activity recognition" OR "behavior recognition" OR "behaviour recognition" OR wearable* OR non-wearable* OR non wearable* OR nonwearable* OR sensor* OR sensing technolog* OR fitness track* OR activity track* OR smart phone* OR smartphone* OR digital device* OR smartwatch* OR smart watch* OR "internet of things" OR IoT OR "ubiquitous sensing" OR "pervasive sensing" OR "unobtrusive sensing" OR actigraph* OR acceleromet*))
AND (Title:(dementia* OR Alzheimer* OR "lewy-body" OR "lewy body" OR mild cognitive impairment* OR Parkinson*) OR Abstract:(dementia* OR Alzheimer* OR "lewy-body" OR "lewy body" OR mild cognitive impairment* OR Parkinson*) OR Keyword:(dementia* OR Alzheimer* OR "lewy-body" OR "lewy body" OR mild cognitive impairment* OR Parkinson*))
AND (Title:("Systematic review" OR "scoping review" OR review OR survey) OR Abstract:("Systematic review" OR "scoping review" OR review OR survey) OR Keyword:("Systematic review" OR "scoping review" OR review OR survey))
Results: 388
Appendix 2. Johanna Briggs Institute (JBI) bias and quality assessment.
Appendix 3.JBI quality assessment for systematic reviews.

| Authors | Q1 | Q2 | Q3 | Q4 | Q5 | Q6 | Q7 | Q8 | Q9 | Q10 | Q11 | Total | Overall appraisal |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Alt Muphy et al. 2018 | y | y | y | y | y | y | u | y | y | y | y | 10 | include |
| Ardelean et al. 2023 | y | y | y | y | y | u | u | y | y | y | y | 9 | include |
| Ardle et al. 2023 | y | y | y | y | y | y | u | y | y | y | y | 10 | include |
| Breasail et al. 2021 | y | y | y | y | y | y | y | y | y | y | y | 11 | include |
| Khan et al. 2018 | y | y | y | y | y | y | y | y | y | y | y | 11 | include |
| Morgan et al. 2020 | y | y | y | y | y | y | y | y | y | y | y | 11 | include |
| Mughal et al. 2022 | y | y | y | y | y | u | u | y | u | y | y | 8 | include |
| Sica et al. 2021 | y | y | y | y | y | y | y | y | y | y | y | 11 | include |
| Anderson et al. 2020 | y | u | y | u | y | u | u | u | y | y | y | 6 | exclude |
| Esquer-Rochin et al. 2023 | y | y | y | y | y | u | u | y | u | y | y | 8 | include |
JBI critical assessment; Q: question, Y: Yes, N: No, U: Unclear, PA: partially.
Appendix 4.Datasets and applicability to HAR for persons with PD or dementia.
| Dataset | Description | Applicable to HAR for persons with PD or dementia |
|---|---|---|
| ADNI | MRI images of patients with Alzheimer's disease | No |
| OASIS | MRI images (ages 18-96 years) | No |
| CASAS | Low-level sensor data of older adults ADLs; consists of Kyoto, Aruba and Multi-resident datasets featuring 20 participants (undefined). Demographics of datasets are: an older woman, her children and grandchildren; 2 participants | Yes |
| PUCK | Sensory data from environmental sensors and wearables about activities of daily living in older adults | Unclear |
| PAMAP2 | Acceleration, orientation, angular rates related to ADLs | Unclear |
| ARAS and ADL | ADLs collected from binary sensors | Unclear |
| PD Telemonitoring | Voice samples of people with PD | No |
| AZTIAHO | Voice samples of people with Alzheimer's disease | No |
| Tsanas et al.'s data set | Data related to dexterity and speech | Unclear |
| Parkinsons data set | Voice samples of people with PD | No |
| mPower Project | Vowel recordings of participants | No |
| Daphnet | Freezing of gait in persons with PD | Yes |
| Freiburg Groceries | Images of groceries | No |
| Labled faces in the wild | Facial images of people | No |
| UK DALE and Sztyler | Recordings of domestic appliance-level electricity/whole-house demand | No |
*Esquer-Rochin et al. (2023).
Appendix 5.Future Work Recommendations from Systematic Review
APPENDIX 6-7. See attached excel file
| Included systematic reviews | Future work recommendations |
|---|---|
| Johansson et al. 2018, Ardle et al. 2023, Khan et al. 2018, Ardelean et al. 2023 |
Furthering investigation of clinometric properties of the measurements derived from wearables to improve standardization of data protocols |
| Johansson et al. 2018, Mughal et al. 2020, Breasail et al. 2023 |
Development of patient-specific algorithms for precision medicine focused digital solutions |
| Ardelean et al. 2023 | Gender comparisons |
| Ardle et al. 2023, Breasail et al. 2023, Ardelean et al. 2023 |
More longitudinal research to see changes over time |
| Ardle et al. 2023, Johansson et al. 2018 | Stronger association between measures derived from HAR and clinically meaningful outcomes. |
| Ardle et al. 2023 | Improvement of devices used to collect data |
| Ardle et al. 2023, Johansson et al. 2018, Breasail et al. 2023, Khan et al. 2018 |
Effectiveness and ecological validity of wearables |
| Ardle et al. 2023, Sica et al. 2021, Ardelean et al. 2023, Breasail et al. 2023 | Development of sensing technology which is best adapted to the patient (size, cost, flexibility of software and features for users and researchers, etc.) |
| Khan et al. 2018 | Addressing ethical issues |
| Khan et al. 2018; Breasail et al. 2023 | Development of best practices for storing and accessing big data; proper data mining techniques followed by advanced machine-learning methods |
| Morgan et al. 2020, Mughal et al. 2020 | Measurement of free-living ADLs at home is relatively unexplored |
| Mughal et al. 2020 | More studies specific to behavioral symptoms of PD |
| Sica et al. 2021, Breasail et al. 2023 | Ad hoc hardware and software capable of providing real-time feedback to clinicians and patients. |
| Sica et al. 2021 | The involvement of formal and informal caregivers trained in the data collection |
| Sica et al. 2021, Mughal et al. 2020, Ardle et al. 2023 |
Sample size and choice should be justified and reported |
| Esquer-Rochin et al. 2023 | More data collection and exploring other machine learning algorithms and models |
| Esquer-Rochin et al. 2023 | Experiments in real-world settings, further validation efforts, increased sample sizes for ad hoc data |
| Esquer-Rochin et al. 2023 | Assistive IoT systems for patients suffering from late-stage dementia and adapted to progression of the disease, including end of life. |
References
- World Health Organization: WHO. (2020, February 5). Ageing. https://www.who.int/health-topics/ageing#tab=tab_1.
- World Health Organization: WHO & World Health Organization: WHO. (2023, March 15). Dementia. https://www.who.int/news-room/fact-sheets/detail/dementia.
- Emre, M. Dementia associated with Parkinson's disease. The Lancet Neurology. 2003 Apr 1;2(4):229-37.
- Stavropoulos TG, Papastergiou A, Mpaltadoros L, Nikolopoulos S, Kompatsiaris I. IoT wearable sensors and devices in elderly care: A literature review. Sensors (Basel). 2020;20(10):2826.
- St Fleur RG, St George SM, Leite R, Kobayashi M, Agosto Y, Jake-Schoffman DE. Use of Fitbit devices in physical activity intervention studies across the life course: narrative review. JMIR mHealth and uHealth. 2021 May 28;9(5):e23411.
- Feehan LM, Geldman J, Sayre EC, Park C, Ezzat AM, Yoo JY, Hamilton CB, Li LC. Accuracy of Fitbit devices: systematic review and narrative syntheses of quantitative data. JMIR mHealth and uHealth. 2018 Aug 9;6(8):e10527.
- Fukushima N, Kikuchi H, Sato H, Sasai H, Kiyohara K, Sawada SS, Machida M, Amagasa S, Inoue S. Dose-response relationship of physical activity with all-cause mortality among older adults: an umbrella review. Journal of the American Medical Directors Association. 2024 Mar 1;25(3):417-30.
- Leite Silva ABR, Goncalves de Oliveira RW, Diogenes GP, de Castro Aguiar MF, Sallem CC, Lima MPP, et al. Premotor, nonmotor and motor symptoms of Parkinson's Disease: A new clinical state of the art. Ageing Res Rev. 2023;84:101834.
- Viseux FJF, Delval A, Simoneau M, Defebvre L. Pain and Parkinson's disease: Current mechanism and management updates. Eur J Pain. 2023;27(5):553-67.
- Cerejeira J, Lagarto L, Mukaetova-Ladinska EB. Behavioral and psychological symptoms of dementia. Front Neurol. 2012;3:73.
- Au-Yeung WM, Miller L, Beattie Z, May R, Cray HV, Kabelac Z, et al. Monitoring Behaviors of Patients With Late-Stage Dementia Using Passive Environmental Sensing Approaches: A Case Series. Am J Geriatr Psychiatry. 2022;30(1):1-11.
- Avila FR, McLeod CJ, Huayllani MT, Boczar D, Giardi D, Bruce CJ, et al. Wearable electronic devices for chronic pain intensity assessment: A systematic review. Pain Pract. 2021;21(8):955-65.
- Cho E, Kim S, Heo S-J, Shin J, Hwang S, Kwon E, et al. Machine learning-based predictive models for the occurrence of behavioral and psychological symptoms of dementia: model development and validation. Sci Rep. 2023;13(1).
- Khan SS, Spasojevic S, Nogas J, Ye B, Mihailidis A, Iaboni A, et al., editors. Agitation detection in people living with dementia using multimodal sensors. 2019 41st Annual International Conference of the IEEE Engineering in Medicine and Biology Society (EMBC); 2019: IEEE.
- Kumar P, Chauhan S, Awasthi LK. Human activity recognition (har) using deep learning: Review, methodologies, progress and future research directions. Archives of Computational Methods in Engineering. 2024 Jan;31(1):179-219.
- Huhn S, Axt M, Gunga H-C, Maggioni MA, Munga S, Obor D, et al. The impact of wearable technologies in health research: scoping review. JMIR Mhealth Uhealth. 2022;10(1):e34384.
- Zhang H, Song C, Rathore AS, Huang MC, Zhang Y, Xu W. mHealth Technologies Towards Parkinson's Disease Detection and Monitoring in Daily Life: A Comprehensive Review. IEEE Reviews in Biomedical Engineering. 2021;14:71-81.
- Straczkiewicz M, James P, Onnela J-P. A systematic review of smartphone-based human activity recognition methods for health research. npj digit. 2021;4(1):148.
- Gupta N, Gupta SK, Pathak RK, Jain V, Rashidi P, Suri JS. Human activity recognition in artificial intelligence framework: a narrative review. Artif Intell Rev. 2022;55(6):4755-808.
- Chapter V: Overviews of Reviews Chapter V: Overviews of Reviews | Cochrane Training. Available at: https://training.cochrane.org/handbook/current/chapter-v (Accessed: 06 May 2024).
- Demrozi F, Pravadelli G, Bihorac A, Rashidi P. Human activity recognition using inertial, physiological and environmental sensors: A comprehensive survey. IEEE Access. 2020;8:210816-36.
- Islam MM, Nooruddin S, Karray F, Muhammad G. Human activity recognition using tools of convolutional neural networks: A state of the art review, data sets, challenges, and future prospects. Computers in Biology and Medicine. 2022;149:106060.
- Lussier M, Lavoie M, Giroux S, Consel C, Guay M, Macoir J, et al. Early detection of mild cognitive impairment with in-home monitoring sensor technologies using functional measures: a systematic review. IEEE journal of biomedical and health informatics. 2018;23(2):838-47.
- Rani GJ, Hashmi MF, Gupta A. Surface electromyography and artificial intelligence for human activity recognition-A systematic review on methods, emerging trends applications, challenges, and future implementation. IEEE Access. 2023.
- Saleem G, Bajwa UI, Raza RH. Toward human activity recognition: a survey. Neural 26. Computing and Applications. 2023;35(5):4145-82.
- Cumpston MS, McKenzie JE, Welch VA, Brennan SE. Strengthening systematic reviews in public health: guidance in the Cochrane Handbook for Systematic Reviews of Interventions. Journal of Public Health. 2022;44(4):e588-e92.
- Choi GJ, Kang H. Introduction to Umbrella Reviews as a Useful Evidence-Based Practice. J Lipid Atheroscler. 2023;12(1):3-11.
- Harrison H, Griffin SJ, Kuhn I, Usher-Smith JA. Software tools to support title and abstract screening for systematic reviews in healthcare: an evaluation. BMC medical research methodology. 2020;20:1-12.
- Valizadeh A, Moassefi M, Nakhostin-Ansari A, Hosseini Asl SH, Saghab Torbati M, Aghajani R, et al. Abstract screening using the automated tool Rayyan: results of effectiveness in three diagnostic test accuracy systematic reviews. BMC Medical Research Methodology. 2022;22(1):160.
- Page MJ, McKenzie JE, Bossuyt PM, Boutron I, Hoffmann TC, Mulrow CD, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. Bmj. 2021;372.
- Campbell M, McKenzie JE, Sowden A, Katikireddi SV, Brennan SE, Ellis S, et al. Synthesis without meta-analysis (SWiM) in systematic reviews: reporting guideline. bmj. 2020;368.
- Aromataris E, Fernandez R, Godfrey CM, Holly C, Khalil H, Tungpunkom P. Summarizing systematic reviews: methodological development, conduct and reporting of an umbrella review approach. Int J Evid Based Healthc. 2015;13(3):132-40.
- Faulkner, G., Fagan, M. J., & Lee, J. (2021). Umbrella reviews (systematic review of reviews). International Review of Sport and Exercise Psychology, 15(1), 73–90. [CrossRef]
- Morgan C, Rolinski M, McNaney R, Jones B, Rochester L, Maetzler W, et al. Systematic Review Looking at the Use of Technology to Measure Free-Living Symptom and Activity Outcomes in Parkinson's Disease in the Home or a Home-like Environment. J Parkinsons Dis. 2020;10(2):429-54.
- Esquer-Rochin M, Rodríguez L-F, Gutierrez-Garcia JO. The Internet of Things in dementia: A systematic review. Internet of Things. 2023;22.
- Ardelean A, Redolat R. Supporting Behavioral and Psychological Challenges in Alzheimer Using Technology: A Systematic Review. Activities, Adaptation & Aging. 2023:1-32.
- Mc Ardle R, Jabbar KA, Del Din S, Thomas AJ, Robinson L, Kerse N, et al. Using Digital Technology to Quantify Habitual Physical Activity in Community Dwellers With Cognitive Impairment: Systematic Review. J Med Internet Res. 2023;25:e44352.
- Breasail MO, Biswas B, Smith MD, Mazhar MKA, Tenison E, Cullen A, et al. Wearable GPS and Accelerometer Technologies for Monitoring Mobility and Physical Activity in Neurodegenerative Disorders: A Systematic Review. Sensors (Basel). 2021;21(24).
- Johansson D, Malmgren K, Alt Murphy M. Wearable sensors for clinical applications in epilepsy, Parkinson's disease, and stroke: a mixed-methods systematic review. J Neurol. 2018;265(8):1740-52.
- Khan SS, Ye B, Taati B, Mihailidis A. Detecting agitation and aggression in people with dementia using sensors-A systematic review. Alzheimers Dement. 2018;14(6):824-32.
- Mughal H, Javed AR, Rizwan M, Almadhor AS, Kryvinska N. Parkinson’s Disease Management via Wearable Sensors: A Systematic Review. IEEE Access. 2022;10:35219-37.
- Sica M, Tedesco S, Crowe C, Kenny L, Moore K, Timmons S, et al. Continuous home monitoring of Parkinson's disease using inertial sensors: A systematic review. PLoS One. 2021;16(2):e0246528.
- Cesana BM, Poptsi E, Tsolaki M, Bergh S, Ciccone A, Cognat E, et al. A Confirmatory and an Exploratory Factor Analysis of the Cohen-Mansfield Agitation Inventory (CMAI) in a European Case Series of Patients with Dementia: Results from the RECage Study. Brain Sci. 2023;13(7).
- Arevalo-Rodriguez I, Smailagic N, Roque IFM, Ciapponi A, Sanchez-Perez E, Giannakou A, et al. Mini-Mental State Examination (MMSE) for the detection of Alzheimer's disease and other dementias in people with mild cognitive impairment (MCI). Cochrane Database Syst Rev. 2015;2015(3):CD010783.
- Movement Disorder Society Task Force on Rating Scales for Parkinson's D. The Unified Parkinson's Disease Rating Scale (UPDRS): status and recommendations. Mov Disord. 2003;18(7):738-50.
- Nasreddine ZS, Phillips NA, Bedirian V, Charbonneau S, Whitehead V, Collin I, et al. The Montreal Cognitive Assessment, MoCA: a brief screening tool for mild cognitive impairment. J Am Geriatr Soc. 2005;53(4):695-9.
- Cummings, J. The Neuropsychiatric Inventory: Development and Applications. J Geriatr Psychiatry Neurol. 2020;33(2):73-84.
- Bankole A, Anderson M, Smith-Jackson T, Knight A, Oh K, Brantley J, et al. Validation of noninvasive body sensor network technology in the detection of agitation in dementia. Am J Alzheimers Dis Other Demen. 2012;27(5):346-54.
- Madrid-Navarro CJ, Puertas Cuesta FJ, Escamilla-Sevilla F, Campos M, Ruiz Abellan F, Rol MA, et al. Validation of a Device for the Ambulatory Monitoring of Sleep Patterns: A Pilot Study on Parkinson's Disease. Front Neurol. 2019;10:356.
- Moyle W, Jones C, Murfield J, Thalib L, Beattie E, Shum D, et al. Effect of a robotic seal on the motor activity and sleep patterns of older people with dementia, as measured by wearable technology: A cluster-randomised controlled trial. Maturitas. 2018;110:10-7.
- Cai G, Huang Y, Luo S, Lin Z, Dai H, Ye Q. Continuous quantitative monitoring of physical activity in Parkinson's disease patients by using wearable devices: a case-control study. Neurol Sci. 2017;38(9):1657-63.
- Bernad-Elazari H, Herman T, Mirelman A, Gazit E, Giladi N, Hausdorff JM. Objective characterization of daily living transitions in patients with Parkinson's disease using a single body-fixed sensor. J Neurol. 2016;263(8):1544-51.
- Bromundt V, Wirz-Justice A, Boutellier M, Winter S, Haberstroh M, Terman M, et al. Effects of a dawn-dusk simulation on circadian rest-activity cycles, sleep, mood and well-being in dementia patients. Exp Gerontol. 2019;124:110641.
- Fleiner T, Haussermann P, Mellone S, Zijlstra W. Sensor-based assessment of mobility-related behavior in dementia: feasibility and relevance in a hospital context. Int Psychogeriatr. 2016;28(10):1687-94.
- Madrid-Navarro CJ, Escamilla-Sevilla F, Minguez-Castellanos A, Campos M, Ruiz-Abellan F, Madrid JA, et al. Multidimensional Circadian Monitoring by Wearable Biosensors in Parkinson's Disease. Front Neurol. 2018;9:157.
- Mantri S, Wood S, Duda JE, Morley JF. Comparing self-reported and objective monitoring of physical activity in Parkinson disease. Parkinsonism Relat Disord. 2019;67:56-9.
- Mirelman A, Hillel I, Rochester L, Del Din S, Bloem BR, Avanzino L, et al. Tossing and turning in bed: nocturnal movements in Parkinson's disease. Movement Disorders. 2020;35(6):959-68.
- Uchino K, Shiraishi M, Tanaka K, Akamatsu M, Hasegawa Y. Impact of inability to turn in bed assessed by a wearable three-axis accelerometer on patients with Parkinson's disease. PLoS ONE. 2017;12(11):e0187616.
- Valembois L, Oasi C, Pariel S, Jarzebowski W, Lafuente-Lafuente C, Belmin J. Wrist actigraphy: a simple way to record motor activity in elderly patients with dementia and apathy or aberrant motor behavior. The Journal of nutrition, health and aging. 2015;19(7):759-64.
- van Uem JMT, Cerff B, Kampmeyer M, Prinzen J, Zuidema M, Hobert MA, et al. The association between objectively measured physical activity, depression, cognition, and health-related quality of life in Parkinson's disease. Parkinsonism Relat Disord. 2018;48:74-81.
- David R, Mulin E, Friedman L, Le Duff F, Cygankiewicz E, Deschaux O, et al. Decreased daytime motor activity associated with apathy in Alzheimer disease: an actigraphic study. Am J Geriatr Psychiatry. 2012;20(9):806-14.
- Etcher L, Whall A, Kumar R, Devanand D, Yeragani V. Nonlinear indices of circadian changes in individuals with dementia and aggression. Psychiatry Res. 2012;199(1):77-8.
- Figueiro MG, Plitnick BA, Lok A, Jones GE, Higgins P, Hornick TR, et al. Tailored lighting intervention improves measures of sleep, depression, and agitation in persons with Alzheimer's disease and related dementia living in long-term care facilities. Clin Interv Aging. 2014;9:1527-37.
- Higami Y, Yamakawa M, Shigenobu K, Kamide K, Makimoto K. High frequency of getting out of bed in patients with Alzheimer's disease monitored by non-wearable actigraphy. Geriatr Gerontol Int. 2019;19(2):130-4.
- Maglione JE, Liu L, Neikrug AB, Poon T, Natarajan L, Calderon J, et al. Actigraphy for the assessment of sleep measures in Parkinson's disease. Sleep. 2013;36(8):1209-17.
- Nagels G, Engelborghs S, Vloeberghs E, Van Dam D, Pickut BA, De Deyn PP. Actigraphic measurement of agitated behaviour in dementia. Int J Geriatr Psychiatry. 2006;21(4):388-93.
- Sringean J, Anan C, Thanawattano C, Bhidayasiri R. Time for a strategy in night-time dopaminergic therapy? An objective sensor-based analysis of nocturnal hypokinesia and sleeping positions in Parkinson's disease. J Neurol Sci. 2017;373:244-8.
- Sringean J, Taechalertpaisarn P, Thanawattano C, Bhidayasiri R. How well do Parkinson's disease patients turn in bed? Quantitative analysis of nocturnal hypokinesia using multisite wearable inertial sensors. Parkinsonism Relat Disord. 2016;23:10-6.
- Xue F, Wang FY, Mao CJ, Guo SP, Chen J, Li J, et al. Analysis of nocturnal hypokinesia and sleep quality in Parkinson's disease. J Clin Neurosci. 2018;54:96-101.
- Nakae H, Tsushima H. Analysis of 24-h physical activities of patients with parkinson's disease at home. Journal of physical therapy science. 2011;23(3):509-13.
- Alvarez F, Popa M, Solachidis V, Hernandez-Penaloza G, Belmonte-Hernandez A, Asteriadis S, et al. Behavior analysis through multimodal sensing for care of Parkinson’s and Alzheimer’s patients. Ieee Multimedia. 2018;25(1):14-25.
- Enshaeifar S, Zoha A, Markides A, Skillman S, Acton ST, Elsaleh T, et al. Health management and pattern analysis of daily living activities of people with dementia using in-home sensors and machine learning techniques. PLoS ONE. 2018;13(5):e0195605.
- Minamisawa A, Okada S, Inoue K, Noguchi M. Dementia Scale Score Classification Based on Daily Activities Using Multiple Sensors. IEEE Access. 2022;10:38931-43.
- Rostill H, Nilforooshan R, Morgan A, Barnaghi P, Ream E, Chrysanthaki T. Technology integrated health management for dementia. British Journal of Community Nursing. 2018;23(10):502-8.
- Shahid ZK, Saguna S, Ahlund C. Recognizing Long-term Sleep Behaviour Change using Clustering for Elderly in Smart Homes. 2022 IEEE International Smart Cities Conference (ISC2)2022. p. 1-7.
- Husebo BS, Heintz HL, Berge LI, Owoyemi P, Rahman AT, Vahia IV. Sensing Technology to Monitor Behavioral and Psychological Symptoms and to Assess Treatment Response in People With Dementia. A Systematic Review (vol 10, 1699, 2020). Front Pharmacol. 2020;11:1.
- Ford C, Xie CX, Low A, Rajakariar K, Koshy AN, Sajeev JK, et al. Comparison of 2 smart watch algorithms for detection of atrial fibrillation and the benefit of clinician interpretation: SMART WARS study. Clinical Electrophysiology. 2022;8(6):782-91.
- Perez MV, Mahaffey KW, Hedlin H, Rumsfeld JS, Garcia A, Ferris T, et al. Large-scale assessment of a smartwatch to identify atrial fibrillation. New England Journal of Medicine. 2019;381(20):1909-17.
- Dementia in Europe yearbook 2019. Available at: https://www.alzheimer-europe.org/sites/default/files/alzheimer_europe_dementia_in_europe_yearbook_2019.pdf (Accessed: 06 May 2024).
- Rubeis, G. The disruptive power of Artificial Intelligence. Ethical aspects of gerontechnology in elderly care. Arch Gerontol Geriatr. 2020;91:104186.
- Alfalahi H, Dias SB, Khandoker AH, Chaudhuri KR, Hadjileontiadis LJ. A scoping review of neurodegenerative manifestations in explainable digital phenotyping. npj Parkinson's Disease. 2023;9.
- Morgan C, Tonkin EL, Masullo A, Jovan F, Sikdar A, Khaire P, et al. A multimodal dataset of real world mobility activities in Parkinson's disease. Sci Data. 2023;10(1):918.
- De-La-Hoz-Franco E, Ariza-Colpas P, Quero JM, Espinilla M. Sensor-Based Datasets for Human Activity Recognition - A Systematic Review of Literature. IEEE Access. 2018;6:59192-210.
- Liberati A, Altman DG, Tetzlaff J, Mulrow C, Gøtzsche PC, Ioannidis JP, et al. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate health care interventions: explanation and elaboration. Annals of internal medicine. 2009;151(4):W-65-W-9.
Figure 1.
PRISM flow diagram of study selection process.
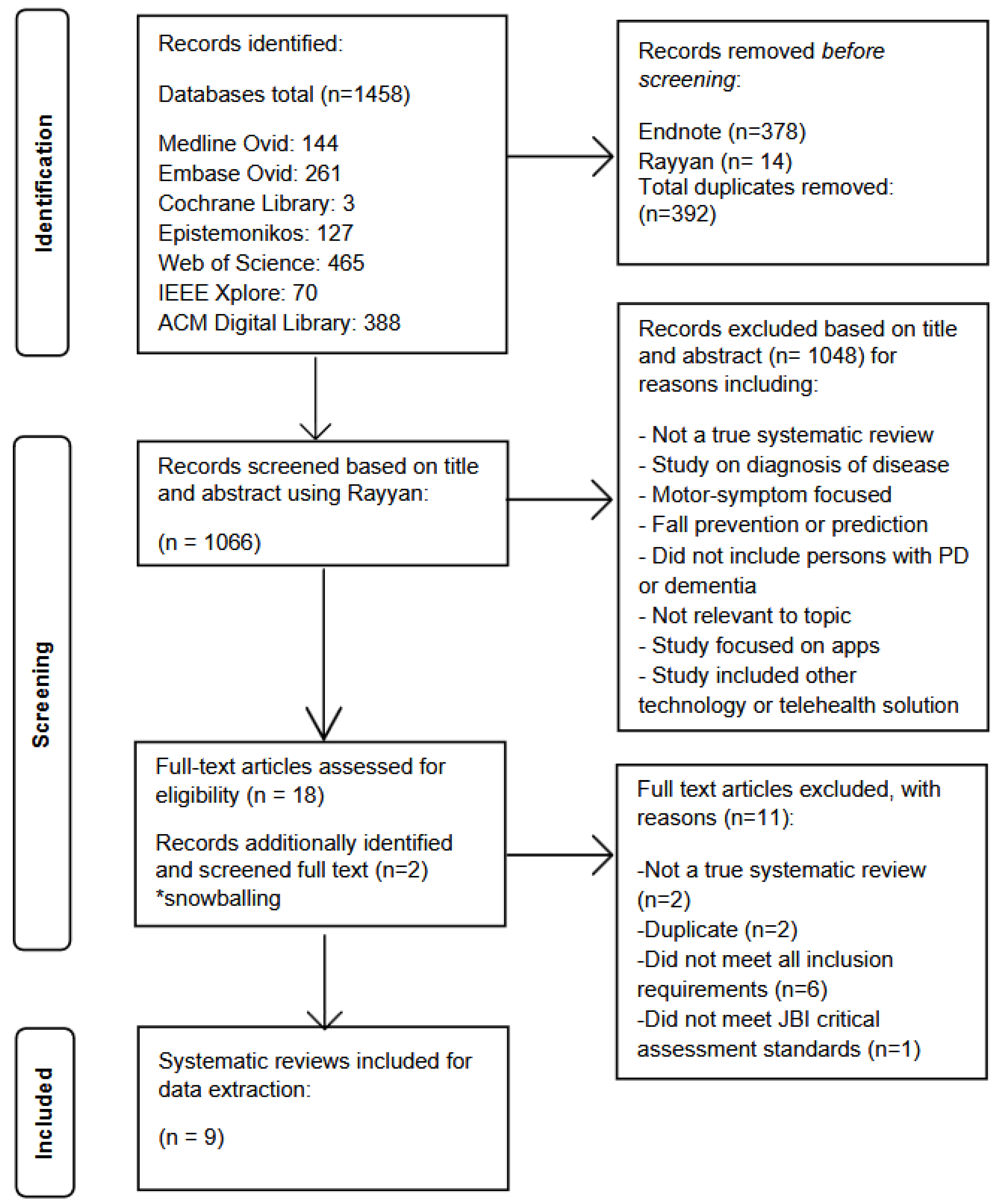
Table 1.
PICO requirements for umbrella review. .
| Population/persons | Older adults with dementia or PD |
| Intervention | Human activity and behavior recognition using sensing technology, including wearables and behavioral symptoms and/or functional activities of daily living. |
| Comparison | Current gold standard outcome measures used within current literature (i.e. Neuropsychiatric Inventory (NPI), Personal Activities of Daily Living (PADL), Polysomnography (PSG), Electrocardiography (EKG), etc.) |
| Outcome | Identification of biomarkers, movement and activity classification models, behavior identification and classification models, measurement methods for activities of daily living, knowledge of basic algorithms and AI used, and information on public datasets specific to human activity recognition (HAR) in older adults with dementia or PD. |
Table 2.
Inclusion and Exclusion criteria for umbrella review.
| INCLUSION CRITERIA | EXCLUSION CRITERIA |
|---|---|
| Systematic Reviews from medical and technical journals | Not a systematic review |
| Including people with PD or dementia, 65 years or older | People without PD or dementia and younger than 65. |
| Sensing technology used for HAR (including behavioral symptoms); sensors, wearables, radar-technology, GPS, multi-modal sensing systems. | Not specific to management or observation of activities or behaviors, gait specific, motor functions for PD specific, fall specific, apps, diagnosis of disease (early detection), non-sensor related technology. |
| Literature from the last 5 years (2018-2024) | Published before 2018 |
| English language | Not written in English |
Table 3.
Included systematic reviews; properties and characteristics.
| Authors/Year Country |
Aim and Demographics | Sensing Technology and Observation Time |
Algorithms and AI | Digital Biomarkers |
**Included Comparative Measures |
Results and conclusions |
|---|---|---|---|---|---|---|
| Ardelean and R. Redolat (2023)[36], Spain | To determine how technology can help to improve the support for behavioral and psychological challenges of dementia. Mean age 60-95 years # of participants: 9-455 # of included studies: 18 Behavioral symptoms: Behavioral and psychological symptoms of dementia (BPSD) in persons with Alzheimer’s disease |
wearable triaxial accelerometer, daysimeter (rest-activity, sleep), GPS, non-wearable actigraphy device (under mattress - sleep), wrist actimetry, mobile phone, robots 3 days, 3-4 weeks, 3 months, 1-5 years (most common 3 months) |
Not included | Psychological symptoms: depression, anxiety, apathy. Behavioral symptoms: sleep disturbances, agitation, wandering. |
MMSE, NPI, NPI-NH, CDR, IQCODE, VAS, ADL, CADS, CMAI, QUALID, FAB, DEMQOL, EQ-5D-5L, QUIS, S-MMSE, MSPSS, HDRS, FCSRT, FAST, TMT-A/B, STROOP Test, DSST, AI, NOSGER, QOL-AD, TBA, CGA, CDT, ET, STAI, HADS, NQOL, MDS, RUDAS, AS, CAM, GDS, RAID, CSDD, ACE-R, TELPI, AIFAI, WHOQOL-OLD, BARS, APADEM-NH, PSQI, AES,MDS-ADL, DAD, CERAD-NB, WMS-III, CFT, DSMT, DSST, video |
|
| Breasail et al. (2021)*[38], United Kingdom | Description of outcome measures and identification of studies that show a relationship between neurodegenerative disease and digital biomarkers. Mean age 28.3-85.5 *participants <63 years were included as healthy controls # of participants: 5-455 # of included studies: 28 Activity and behavioral symptoms: Physical activity, sedentary behavior, sleep disturbance, rest-activity patterns, motor symptoms of PD |
GPS, sensors, accelerometers 24 hrs-3 monthsmost common 7 days |
Not included | Step count, time spent in physical activity, number of bouts, MET, awake/sleep time, time spent sedentary, trip frequency, duration outside home, walking duration, aggregation of velocity data into 60s epochs, activity levels, algorithm classification of upright posture, sitting, standing, walking, walking speed cut-offs for PD, gait - motor PD, activity intensity and levels, sleep activity. |
ALSFRS-R, MoCA, PDQ, PASE, LSA |
|
|
Authors/Year Country |
Aim and Demographics |
Sensing Technology and Observation Time |
Algorithms and AI | Digital Biomarkers | Included Comparative Measures | Results and conclusions |
| Esquer-Rochin (2023)*[35], Mexico | To investigate the state of the art of the IoT in dementia. Mean age not provided. # of participants: 10-42 # of included studies: 104 Activity and behavioral symptoms: ADLs, agitation, wandering |
RF devices, Beacons GPS, Inertial devices. Smartphones glasses and watches, binary proximity sensors, ambient temperature, smart meter, video, neuroimaging devices. Length of observations not included. |
Random forest, decision trees, support vector machines, k-nearest neighbors, and (deep) neural networks. | Activities of daily living, speech/voice, location/GPS, vital signs, brain/neurological related variables, position within a room, wandering or agitation related activities. | Not included |
|
|
Authors/Year Country |
Aim and Demographics |
Sensing Technology and Observation Time |
Algorithms and AI | Digital Biomarkers | Included Comparative Measures | Results and conclusions |
| Johannson et al. (2018)[39], Sweden | Synthesis of knowledge from quantitative and qualitative clinical research using wearable sensors in epilepsy, PD (PD), and stroke. Mean age 34-71 years *1 sleep specific (non-motor) study included: mean age 67 +-9 years # of participants: 5-527 # of included studies: 56 Activity and behavioral symptoms: Physical activity metrics, walking, sleep disturbances, seizures |
accelerometry, gyroscope, wearables 1-9 days lab setting8h -7 days free-living |
Commercial algorithm (Parkinson's KinetiGraph), time-frequency mapping-Fast Fourier transformations, support vector machines, iterative forward selection algorithm, linear discriminant analysis, discriminant analysis to determine the threshold of mean duration of immobility, combined axis rotations, power spectrum area and peak power, root mean square, mean velocity, frequency, jerk. |
Step counts, energy expenditure during walking, tremor, dyskinesia, postural sway, spatiotemporal gait, medication evoked adverse symptoms, tonic-clonic seizures, non-epileptic seizures, motor seizures, sleep disturbance, upper extremity activity, walking. | Video, gait analysis, functional activities analysis, UPDRS III, CDRS, mAIMS, MBRS, GAITRite, PIGD, PDQ-39, MiniBEST, SF-36, commercial system (SAM, PAL, TriTrac RT3), commercial system (sensing stylus, Actical, ActivPAL, Vitaport and Kinesia), NIHSS, NEADL, FMA, ARAT, WMFT, stroke ULAM, MAL, MAL-26, AAUT, BBS, FIM, mRS, 6MWT |
|
|
Authors/Year Country |
Aim and Demographics |
Sensing Technology and Observation Time |
Algorithms and AI | Digital Biomarkers | Included Comparative Measures | Results and conclusions |
| Khan et al. (2018)[40], Canada | Identification of studies that use different types of sensors to detect agitation and aggression in persons with dementia. Mean age 74.3-85.5 years *7/13 studies included no age information # of participants: 6-110 # of included studies: 14 Behavioral symptoms: Agitation and aggression |
accelerometry, gyroscope, wearables, camera, ambient sensing modalities Timeframe not detailed for all studies; 3 hrs, 48 hrs, 5-7 days |
Rotation forest, Hidden Markov Models, Support vector machines, Bayesian Network, Time frequency analysis | agitation and aggression | CMAI, MMSE, DSM-III-R, ABS, NPI, SOAPD |
|
|
Authors/Year Country |
Aim and Demographics |
Sensing Technology and Observation Time |
Algorithms and AI | Digital Biomarkers | Included Comparative Measures | Results and conclusions |
| McArdle et al. (2023)[37], United Kingdom, New Zealand, Australia |
To understand habitual physical activity participation in people with cognitive impairment identifying: metrics used to assess activity, describe differences between people with dementia and healthy controls, and make future recommendations for measuring and reporting activity impairments. Mean age 22-84 years *majority 63-84 years # of participants: 7-323 # of included studies: 33 Activity: Physical activity metrics |
wearables, ambient home-based sensors, accelerometer (most commonly wrist worn or low back) Most common was a 7-day protocol varying from 2 days-3 months (capturing weekdays and weekends) |
Not included | Steps per day, outdoor time, activity counts, low-vigorous activity (METS), total movement intensity (mean vector magnitude of dynamic acceleration per day for total behavior, expressed relative to gravitational acceleration, time spent walking, time of day activity (day, night, etc.), relative amplitude (higher amplitude indicates stronger rhythm; rest-activity), hour to hour and day to day variability, root mean square difference, interindividual variability, intra-daily stability and variability, COV of daily activity. |
MoCA |
|
|
Authors/Year Country |
Aim and Demographics |
Sensing Technology and Observation Time |
Algorithms and AI | Digital Biomarkers | Included Comparative Measures | Results and conclusions |
| Morgan et al. (2020)[34], United Kingdom | Provide an overview of what technology is being used to test outcomes in PD in free-living participant's activity in a home environment. Mean age not provided. # of participants: N/I # of included studies: 65 Activity and behavioral symptoms: Physical activity and sleep disturbances |
Various sensing technologies 2 weeks or less (majority)10 studies- up to 1 yr3 studies- multiple measurements over time |
Not included | Tremor, gait, typing, medication on/off, sleep, physical activity, bradykinesia, dyskinesia, skin temperature, light exposure, posture, falls, activities of daily living (majority gait and motor related symptoms) | UPDRS, PDQ-8, PDSS, FIM, PSQI, NADCS |
|
|
Authors/Year Country |
Aim and Demographics |
Sensing Technology and Observation Time |
Algorithms and AI | Digital Biomarkers | Included Comparative Measures | Results and conclusions |
| Mughal et al. (2022)*[41], Pakistan, United Kingdom, Saudi Arabia, Slovakia | To present different techniques for early detection and management of PD motor and behavioral symptoms using wearable sensors. Mean age not provided. # of participants: 4-2063 # of included studies: 60 Behavioral symptoms: Sleep dysfunction, depression, impulse control, motor symptoms of PD |
Inertial sensors (IMU): triaxial accelerometers, gyroscopes, and magnetometers. Micro-electro-mechanical system (MEMS), necklace, and barometer. Cameras: Zenith and Kinect. Capacitive pressure sensor. Surface EMG. IMUs; Mechanomyography. Flex and light sensors. Ambulatory Circadian Monitoring (ACM), polysomnography. Smart toilet. EEG sensors. Timeframe information not included. |
Not included | Motor symptoms: tremor, bradykinesia, rigidity, and freezing of gait. Behavioral and other symptoms: gastrointestinal problems, sleep disfunction, impulse control disorder, depression, physical activity metrics. |
UPDRS, HY, TUG, polysomnography, EEG |
|
|
Authors/Year Country |
Aim and Demographics |
Sensing Technology and Observation Time |
Algorithms and AI | Digital Biomarkers | Included Comparative Measures | Results and conclusions |
| Sica et al. (2021)[42], Ireland | To investigate continuous PD monitoring using inertial sensors, where the focus is papers with at least one free-living data capture unsupervised (either directly or via video- tapes). Mean age not provided. # of participants: 1-172 # of included studies: 24 Activity: ADL (transitional), physical activity, and motor symptoms of PD |
accelerometer, gyroscope, magnetometers. Hours-14 days |
Artificial Neural Networks, Fuzzy logic algorithms, linear regression, and Support Vec- tor Machine, Diverse Density, Expectation Maximization version of Diverse Density, Discriminative variant of the axis-parallel hyper- rectangle, Multiple instances learning k-Nearest Neighbor and Multiple Instance Support Vector Machine. |
Gait impairments, step-counts, intensity and volume of activities, kinematics, bradykinesia, tremor, dyskinesia, and on/off state episodes. | UPDRS, PASE, symptom diaries |
|
*Published in technical journals. **Acronyms: 6MWT: 6 minute walk test; AAUT: Actual Amount of Use Test; ACE-R; Addenbrooke Cognitive Examination-Revised; ADL: Activities of Daily Living; AES: Apathy Evaluation Scale; AI: Apathy Inventory; AOAFAI: Adults and Older Adults Functional Assessment Inventory; ALSFRS-R; ALS Functional Rating Scale-Revised; APADEM-NH: Apathy Scale for Institutionalized Patients with Dementia Nursing Home version; ARAT: the Action Research Arm Test; AS: Apathy Score; BARS: Brief Agitation Rating Scale; BBS: Berg Balance Scale; CADS: Changes in Advanced Dementia care Scale; CAM: Confusion Assessment Method; CDR: Clinical Dementia Rating; CDRS: Clinical Dementia Rating Scale; CDT: Clock Drawing Test; CERAD-NB: Consortium to Establish a Registry for Alzheimer’s Disease-Neuropsychological Battery; CFT: Category Fluency Test; CGA: Comprehensive Geriatric Assessment; CMAI: Cohen-Mansfield Agitation Inventory; CSDD: Cornell Scale for Depression in Dementia; DAD: Disability Assessment for Dementia; DEMQOL: Dementia Quality of Life; DSM-III-R: the Diagnostic and Statistical Manual of Mental Disorders; DSMT: Digital Span Memory Test; EEG: electroencephalogram; EQ-5D-5L; EuroQol-5 Dimensions; ET: Emotional Thermometer; FAB: Frontal Assessment Battery; FAST: Functional Assessment Staging Test of Alzheimer’s Disease; FCSRT: Free and cue selective reminding task; FIM: Functional Independence Measure; FMA: Fugl-Meyer Assessment; FRT: Functional Reach Test; GDS: Geriatric Depression Scale; GPS: Global Positioning System; HADS: Hospital Anxiety and Depression Scale; HDRS: Hamilton Depression Rating Scale; IQCODE: Informant Questionnaire on Cognitive Decline in the Elderly; LSA: Life Space Assessment; MAL: the Motor Activity Log; MAL-26: Motor Activity Log-26; MBRS: Modified Bradykinesia Rating Scale; MDS: Modified Depression Scale; MDS-ADL: Minimum Data Set Activities of Daily Living Scale; MiniBEST: Mini Balance Evaluation Systems Test; MMSE: Mini-Mental State Examination; mRS: Modified Rankin Scale; MSPSS: Multidimensional Scale of Perceived Social Support; NADCS: Nocturnal Akinesia Dystonia and Cramp Score; NEADL: the Nottingham Extended Activities of Daily Living Questionnaire; NIHSS: the Nation Institutes of Health Stroke Scale; NOSGER: Nurses’ Observation Scale for Geriatric Patients; NPI: Neuropsychiatric Inventory; NPI-NH: Neuropsychiatric Inventory Nursing Home; NQOL: Neuro Quality of Life in Neurological Disorder; PASE: Physical Activity Scale for the Elderly; PD: Parkinson’s Disease; PIGD: Postural Instability and Gait Disorder subscore; PSQI: Pittsburgh Sleep Quality Index; QOL-AD: Quality of Life Alzheimer’s Disease; QUALID: Quality of Life Scale for Severe Dementia; QUIS: Quality of Interactions Schedule; RAID: Rating for Anxiety in Dementia; RUDAS: The Rowland Universal Dementia Assessment Scale; SF-36: Short-Form Health Survey; S-MMSE: Severe Mini-Mental State Examination; STAI: State-Trait Anxiety Inventory; S-ULAM: Stroke Upper Limb Activity Monitor; TBA: Tinetti Balance Assessment; TELPI: Test de Leitura de Palavras Irrgulares; TMT-A/B: Trail Making Test; DSST: Digital Symbol Substitution Test; UPDRS III: Unified Parkinson’s Disease Rating Scale; VAS: Visual Analog Scale (pain); WHOQOL-OLD: World Health Association Quality of Life – Older Adults module; WMFT: the Wolf Motor Function Test; WMS-III: Wechsler Memory Scale-III.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



