Submitted:
17 February 2025
Posted:
18 February 2025
You are already at the latest version
Abstract
Conventional hernia repair using static flat meshes is often associated with complications casused by extensive dissection, implant fixation, and poor biological response. The Stenting & Shielding (S&S) Hernia System offers a novel solution designed for dissection-free, fixation-free hernia repair. The S&S Hernia System has been evaluated in a porcine model, focusing on procedural simplicity, device retention and regenerative properties. The experimental study involved 10 pigs, each implanted with two S&S devices. Follow-up assessments included ultrasound, laparoscopic examinations, and histological analyses over a period ranging from 4 weeks to 8 months post-implantation. The S&S Hernia System, made from medical-grade polypropylene-based thermoplastic elastomer (TPE), features a rayed 3D scaffold and an oval shield connected by a mast. Delivered and positioned intraabdominally without dissection, the device transforms into a self-retaining scaffold to obliterate the hernia defect. Primary outcomes included ease of delivery, visceral adhesion formation, and device retention, ensuring no dislocation. Secondary outcomes evaluated histological evidence of tissue regeneration, including the development of connective tissue, muscles, vessels, and nerves within the scaffold. Immunohistochemistry was used to detect tissue growth factors promoting regeneration of the abdominal wall's typical components. All 20 implanted devices remained securely in place without dislocation. Transient adhesion bands were observed in two shields at 1 month but resolved by 3 months. No visceral adhesions were detected at the time of animal sacrifice. Histological analyses demonstrated tissue regeneration within the scaffold, while immunohistochemistry confirmed the presence of growth factors supporting regeneration. Overall, the S&S Hernia System showed promising results in a porcine model, with no dislocation and evident regenerative potential. Its rapid, dissection-free delivery and compliance with abdominal wall dynamics simplify the procedure while minimizing adhesions. These findings warrant further clinical investigation to validate its application in human patients.
Keywords:
Introduction
- The hernia defect often remains patent post-repair, increasing the risk of recurrence. [15]
- Placement typically necessitates extensive tissue dissection, raising the risk of iatrogenic injuries, edema, and delayed recovery.
- Provide fixation-free deployment without tissue dissection.
- Permanently obliterate the hernia defect.
- Assure dynamic compliance with abdominal wall movements.
- Act as a regenerative scaffold, promoting the development of newly formed connective tissue, muscles, vessels, and nerves to restore the integrity of the abdominal wall barrier.
Material and Methods
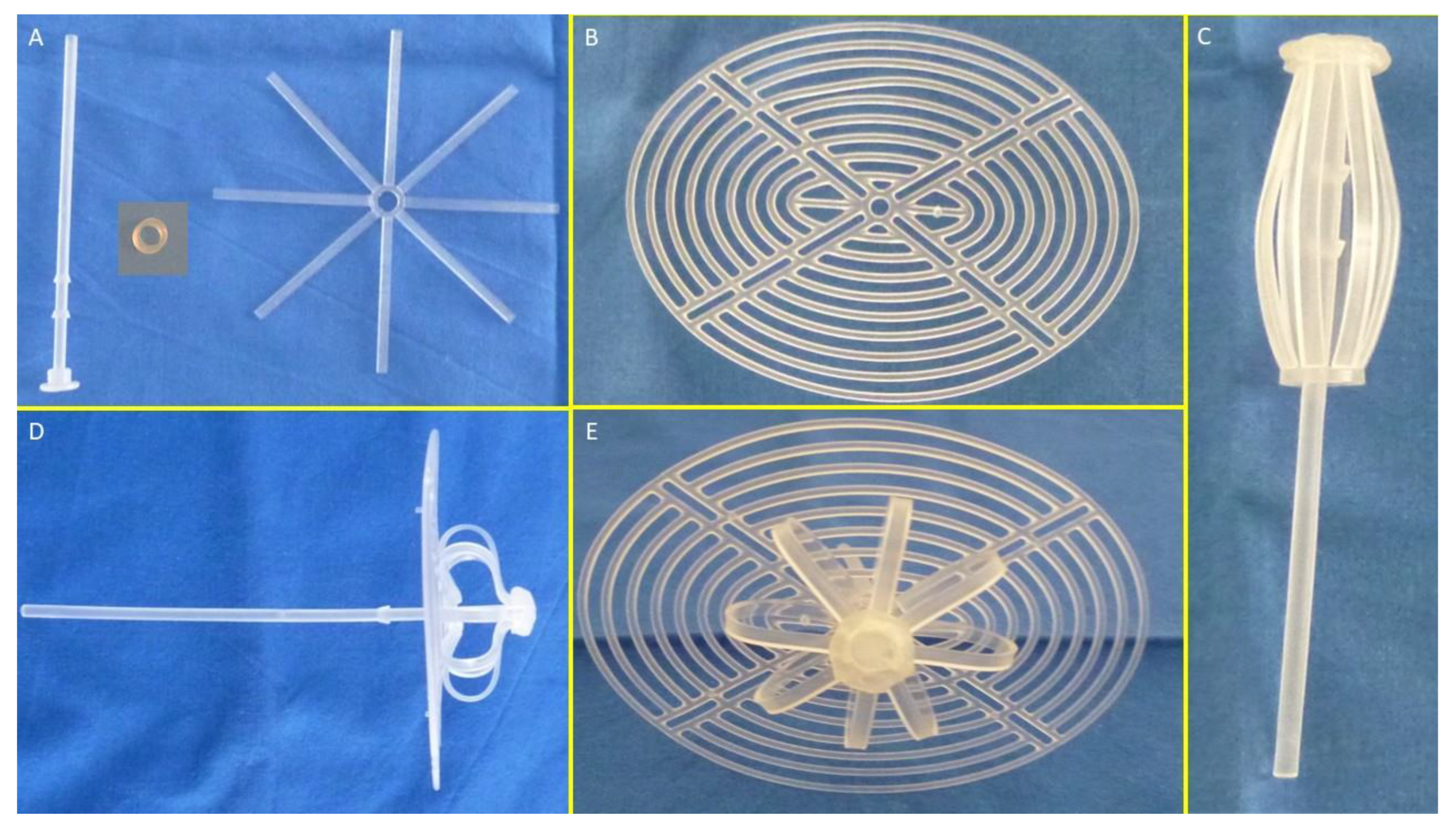
- Mast element: Equipped with a button-like distal end and two conic stops.
- Rayed structure: Eight rays connected by a central ring.
- Assembly ring: Secures the mast and rayed structure.
- 3D oval shield plate: Dimensions: 10×8 cm; central ring for attachment.
Operational Steps
- 1.
- Assembly and Preparation:
- ○
- The mast, rayed structure, and assembly ring are assembled into a cylindrical compound. (Figure 1 C)
- ○
- The shield plate is loosely attached to the mast for laparoscopic delivery.
- ○
- The conic enlargements of the mast that serve as stops, secure the shield and the 3D scaffold in its final position preventing the shield from slipping backwards. (Figure 1 D – E)
- ○
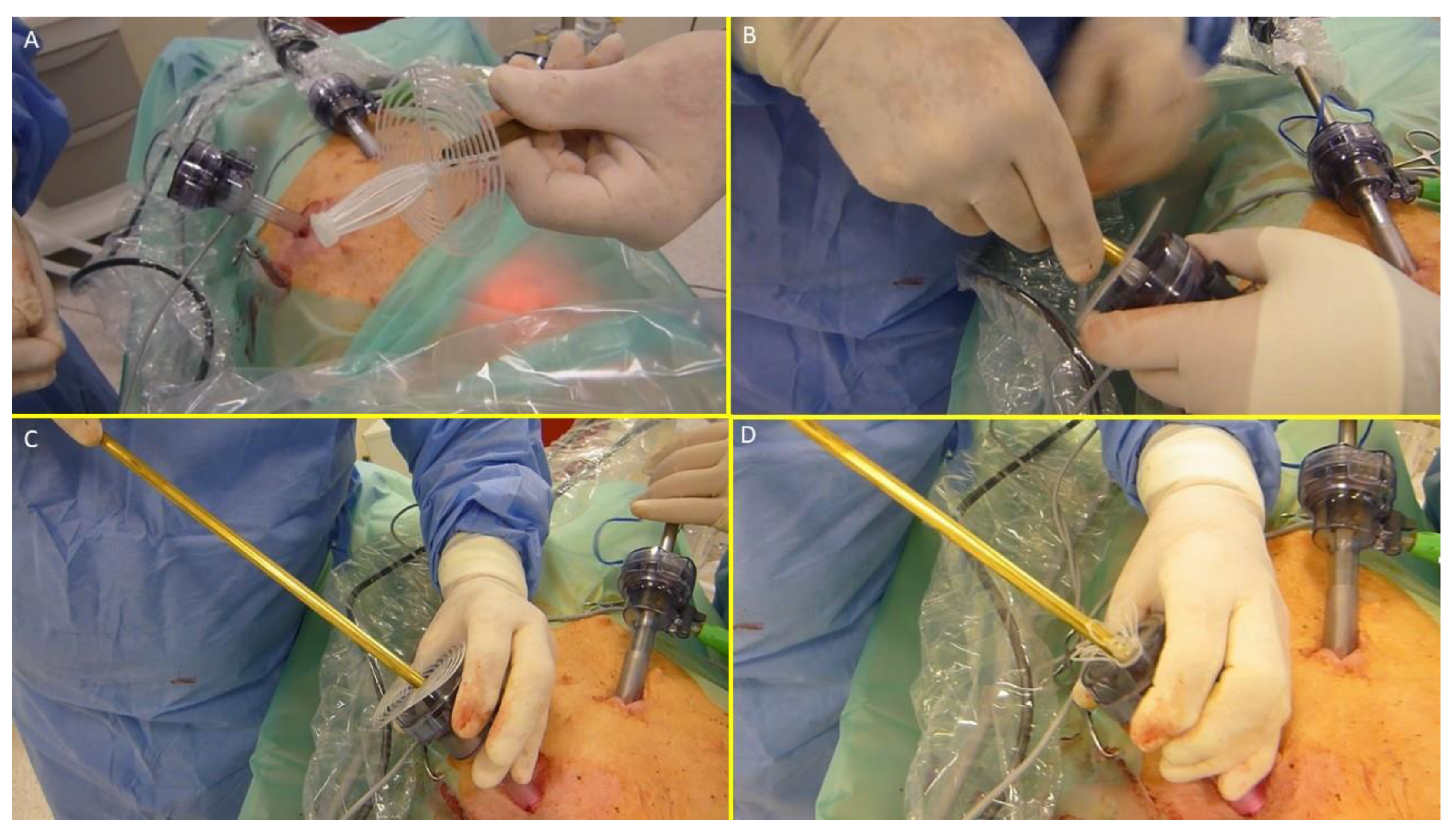
- The prepared device, held by the forceps inserted in the metallic tube, is intended to be introduced into a trocar channel to be delivered into the abdominal cavity. (Figure 2 A – E)
- 2.
- Deployment:
- ○
- All procedures are planned to be performed laparoscopically.
- ○
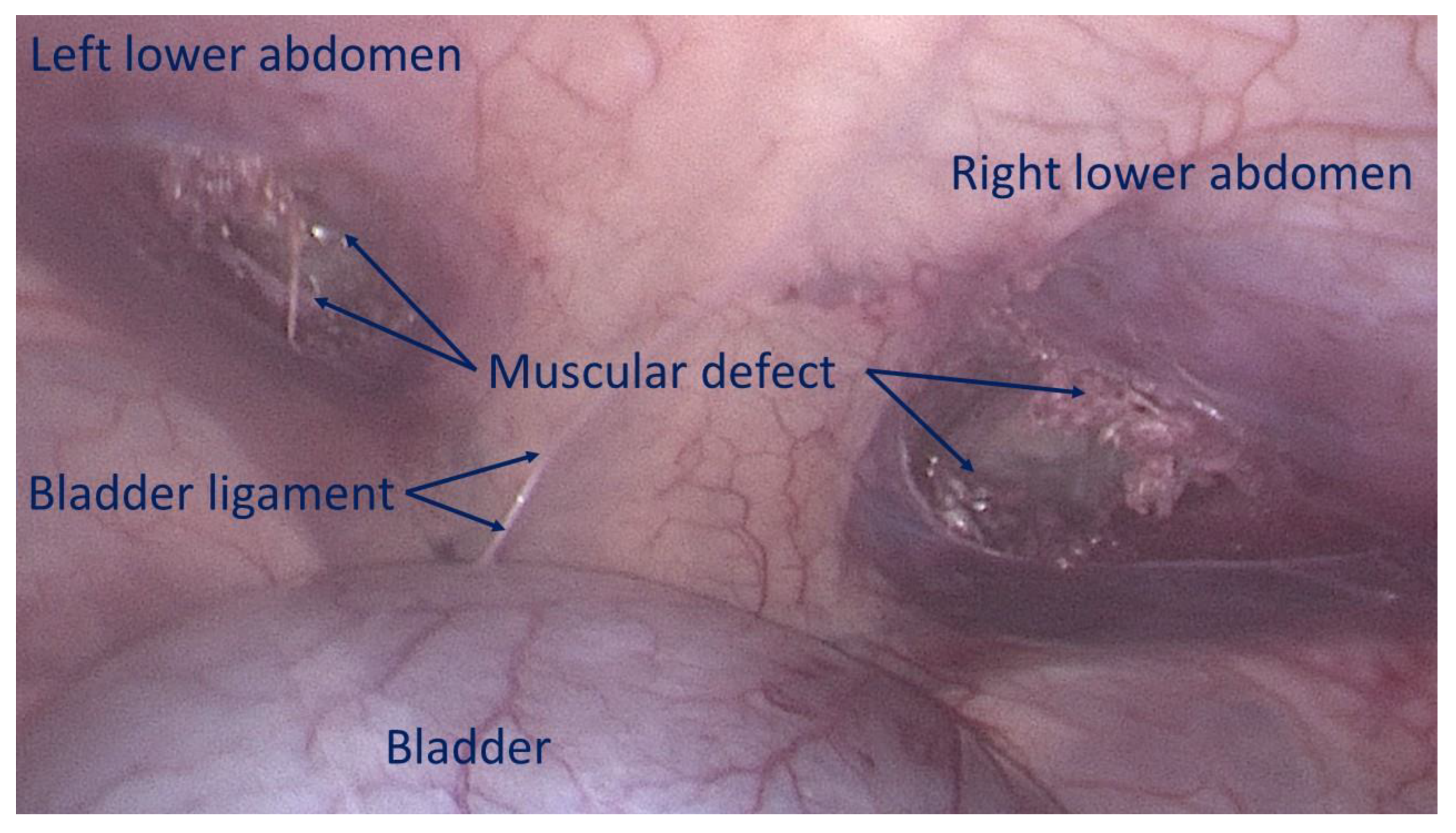
- The first step involves creating a defect in the lower abdominal wall musculature of the pig. Depending on the anatomical aspect of the swine, the defects were made using electrocautery bilaterally either in the lower part of the rectus muscle or in the lower medial aspect of the lateral abdominal musculature to achieve a ca. 3,5 cm wide opening. (Figure 3)
- ○
- The device was compounded by inserting the grip of a laparoscopic forceps into an 8 mm metallic tube. Additionally, the branches of the forceps firmly held the mast of the 3D scaffold in a restrained mode along with the loose shield. (Figure 4A)
- ○
- ○
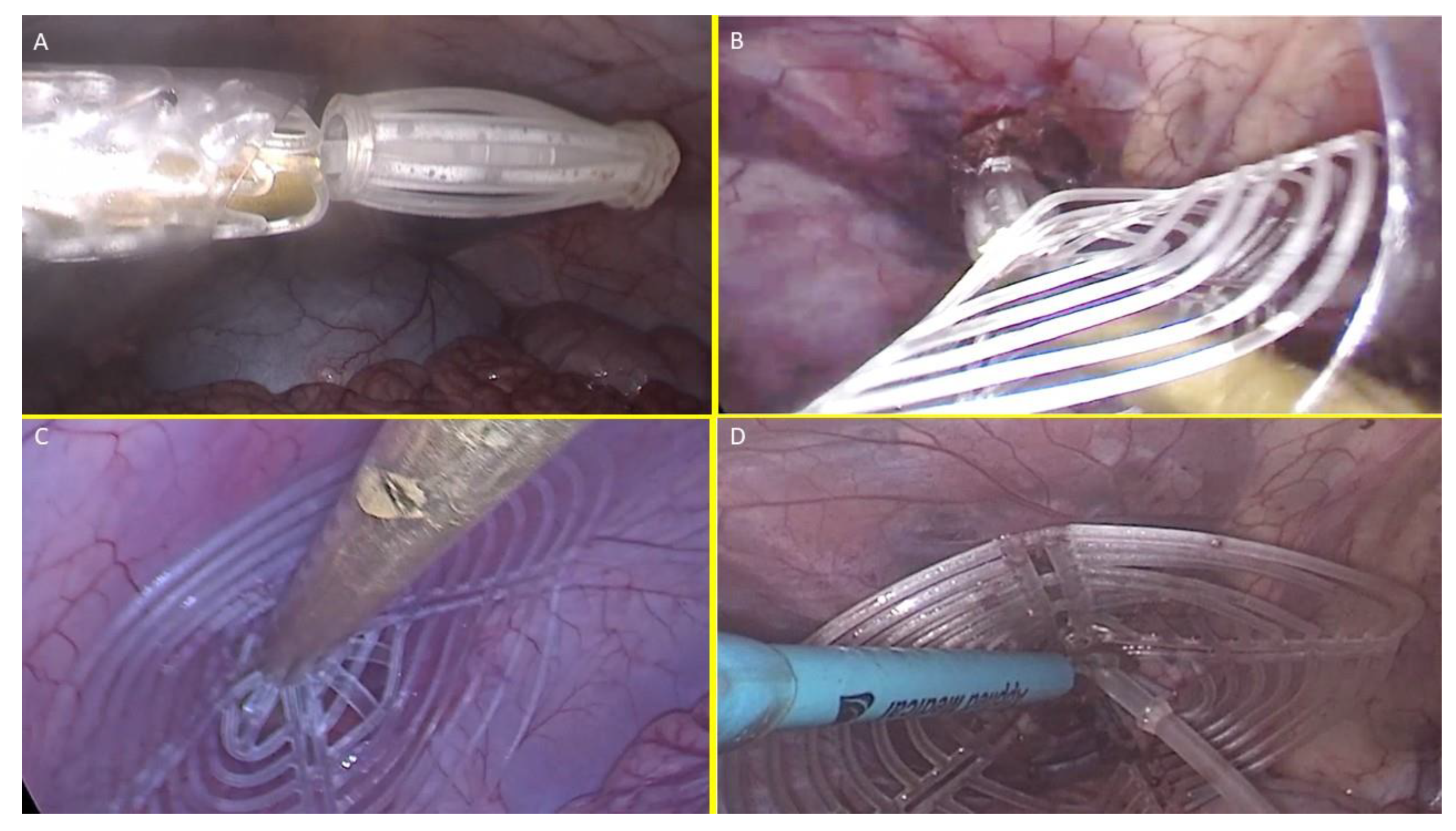
- At this stage the device is approached and introduced into the defect. (Figure 5B)
- ○
- Then, with a combined maneuver, the metallic tube was pushed to slide the shield forward along the central mast while simultaneously the forceps pulled the proximal edge of the mast backward. This allowed the shield to surpass the two conic stops of the mast
- 3.
- Securing the Device:
- ○
- The conic stops lock the shield in position. Adjustments allow tailored scaffold expansion at discretion of the surgeons. (Figure 5C)
- ○
- The redundant mast is excised after confirming stability (Figure 5D).
- Short-term (1 month): 2 pigs.
- Midterm (3–4 months): 3 pigs.
- Long-term (5–8 months): 5 pigs.
- Neo-neurogenesis: NSE (Neuron-specific Enolase, 1:100, LSBio, USA).
- Neo-angiogenesis: VEGF (1:50, R&D Systems, USA); PECAM-1 (CD31, 1:50, Dako-Agilent, USA).
- Vascular maturity: SMA (Smooth Muscle Actin, 1:100, Dako-Agilent, USA).
- Neomyogenesis: NGF (1:100, Abcam, USA).
- Neurogenesis markers: NGFRp75 (1:100, Santa Cruz Biotechnology, USA).
- 1.
- Surgical Outcomes:
- ○
- Feasibility of laparoscopic delivery without tissue dissection.
- ○
- Time required for deployment.
- ○
- Learning curve for optimal procedure time.
- ○
- Device retention within the defect.
- ○
- Ultrasound-documented tissue incorporation.
- ○
- Laparoscopic evidence of presence/absence of visceral adhesions.
- 2.
- Biological Response:
- ○
- Macroscopic ingrowth within the 3D scaffold.
- ○
- Histological evaluation of tissue integration and inflammatory response.
- ○
- Immunohistochemical detection of growth factors (e.g., VEGF, NGF) supporting vascular, muscular, and neural regeneration.
Results
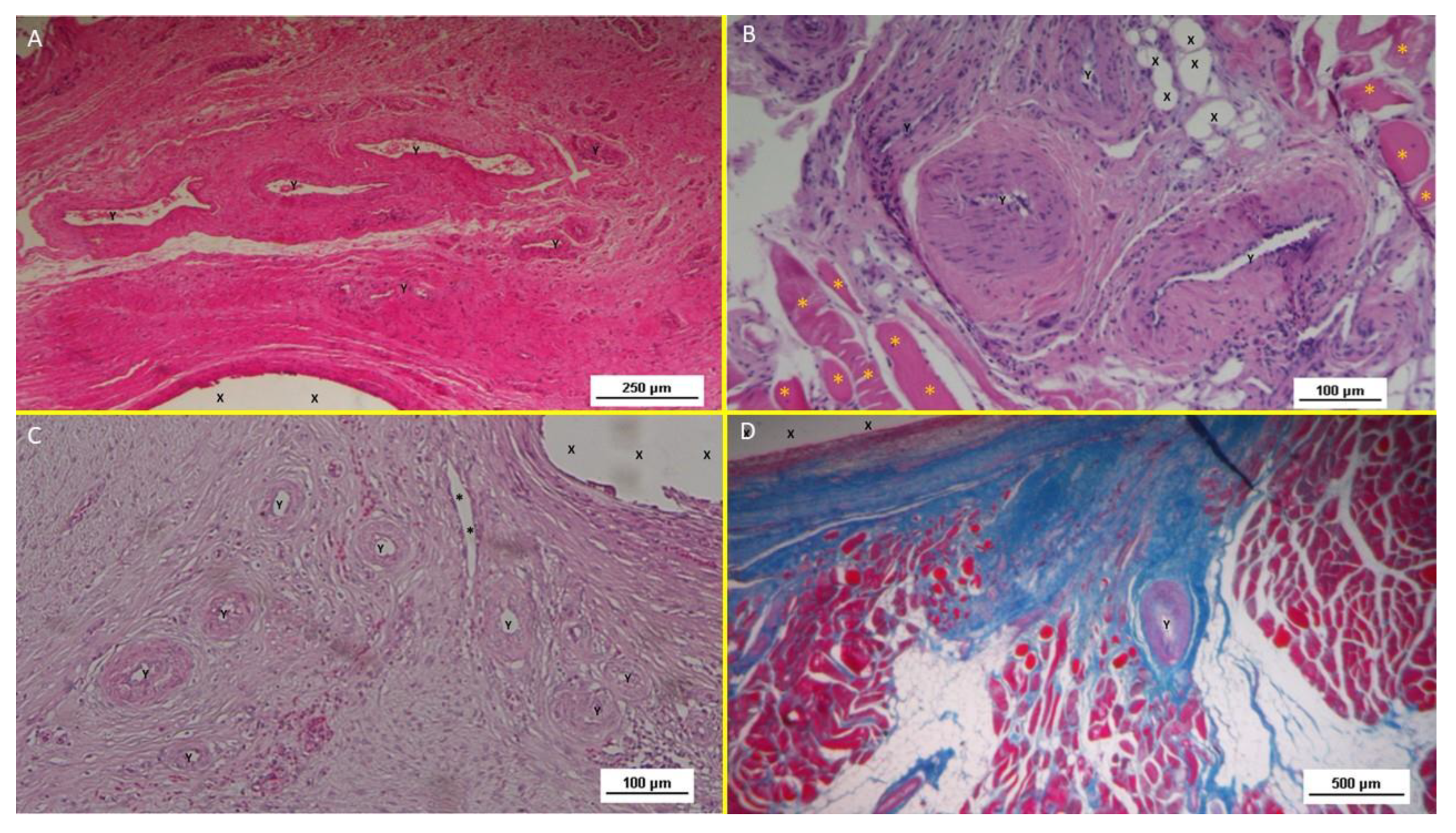
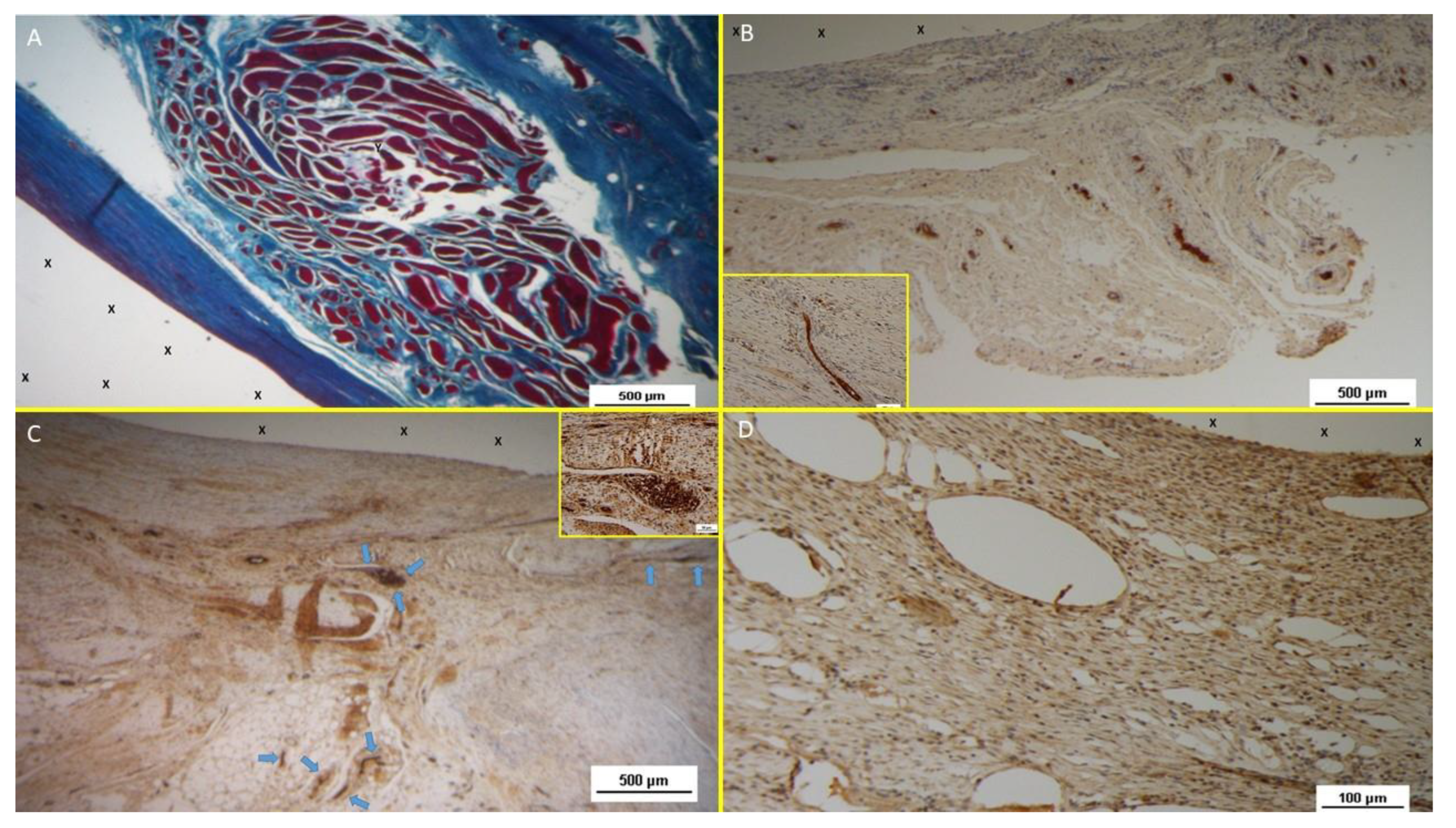
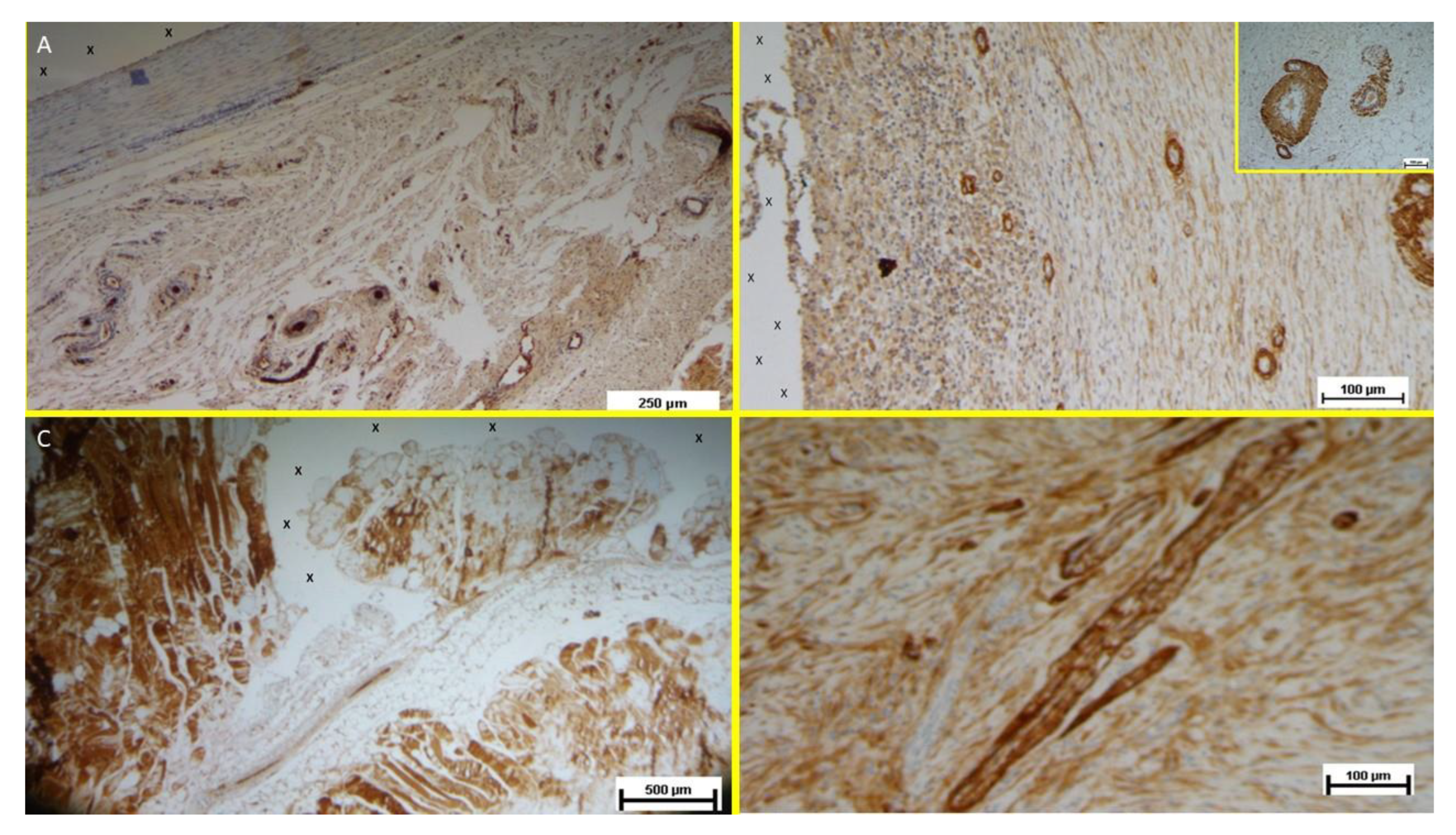
- Vascular Growth Factors: Early VEGF-induced neovascularization (Figure 11 D) transitioned to a predominance of CD31-positive endothelial cells in the midterm, along with SMA-driven vascular maturation (Figure 12 A). Long-term specimens exhibited further SMA-mediated structural thickening, with complete vascular development (Figure 12 B).
- Muscular Growth Factors: NGF-positive elements indicated muscular development in the early stage, increasing in quantity and organization into bundles by the mid and long term (Figure 12 C).
- Nervous Growth Factors: NGFRp75-positive neural elements were initially sparse, correlating with immature nervous clusters. By the midterm, these elements increased, showing progressive myelin sheath development. Long-term specimens revealed mature nerve structures resembling human nerves (Figure 12 D).
Discussion
- Minimally invasive laparoscopic delivery without tissue dissection.
- Permanent obliteration of the hernia defect to prevent recurrence.
- An intraabdominal shield protecting neighboring areas from future herniation.
- Dynamic compliance with abdominal wall movements, preventing visceral adhesions and fostering regeneration.
Conclusions
Author Contributions
Funding
Data availability
Compliance with Ethical Standards
Human and animal right
Disclosure
References
- Amato G. State of the art and future perspectives in inguinal hernia repair. In: Inguinal Hernia: Pathophysiology and Genesis of the Disease. Cham: Springer; 2022. p. 143-163. [CrossRef]
- Kingsnorth A, LeBlanc K. Hernias: inguinal and incisional. Lancet. 2003;362:1561-71. [CrossRef]
- LeBlanc KA. Complications associated with the plug-and-patch method of inguinal herniorrhaphy. Hernia. 2001;5(3):135-8. [CrossRef]
- Klosterhalfen B, Klinge U, Schumpelick V. Functional and morphological evaluation of different polypropylene-mesh modifications for abdominal wall repair. Biomaterials. 1998 Dec;19(24):2235-46. [CrossRef]
- Klinge U, Klosterhalfen B, Muller M, Schumpelick V. Foreign body reaction to meshes used for the repair of abdominal wall hernias. Eur J Surg. 1999;65:665-73. [CrossRef]
- O’Dwyer PJ, Kingsnorth AN, Mohillo RG, Small PK, Lammers B, Horeyseck G. Randomized clinical trial assessing the impact of a lightweight or heavyweight mesh on chronic pain after inguinal hernia repair. Br J Surg. 2005;92(2):166-70. [CrossRef]
- Weyhe D, Schmitz I, Belyaev O, Grabs R, Müller KM, Uhl W, Zumtobel V. Experimental comparison of monofile light and heavy polypropylene meshes: less weight does not mean less biological response. World J Surg. 2006;30(8):1586-91. [CrossRef]
- Köckerling F, Koch A, Lorenz R, Reinpold W, Hukauf M, SchugPass C. Open repair of primary versus recurrent male unilateral inguinal hernias: perioperative complications and 1-year follow-up. World J Surg. 2016;40(4):813-25. [CrossRef]
- Amato G, Calò PG, Rodolico V, Puleio R, Agrusa A, Gulotta L, Gordini L, Romano G. The septum inguinalis: a clue to hernia genesis? J Invest Surg. 2018;31:1-9.
- Amato G, Marasa L, Sciacchitano T, Bell SG, Romano G, Gioviale MC, Lo Monte AI, Romano M. Histological findings of the internal inguinal ring in patients with indirect inguinal hernia. Hernia. 2009;13:259-62. [CrossRef]
- Amato G, Ober E, Romano G, Salamone G, Agrusa A, Gulotta G, Bussani R. Nerve degeneration in inguinal hernia specimens. Hernia. 2011;15:53-8. [CrossRef]
- Amato G, Romano G, Salamone G, Agrusa A, Saladino VA, Silvestri F, Bussani R. Damage to the vascular structures in inguinal hernia specimens. Hernia. 2012;16(1):63-7. [CrossRef]
- Amato G, Agrusa A, Romano G, Salamone G, Gulotta G, Silvestri F, Bussani R. Muscle degeneration in inguinal hernia specimens. Hernia. 2012;16(3):327-31. [CrossRef]
- Amato G, Agrusa A, Romano G, Salamone G, Cocorullo G, Mularo SA, Marasa S, Gulotta G. Histological findings in direct inguinal hernia. Hernia. 2013;17(6):757-63. [CrossRef]
- Amato G, Agrusa A, Di Buono G, Calò PG, Cassata G, Cicero L, Romano G. Inguinal hernia: defect obliteration with the 3D dynamic regenerative scaffold Proflor™. Surg Technol Int. 2021;38:199-205. [CrossRef]
- Kilkenny C, Browne WJ, Cuthill IC, Emerson M, Altman DG. Improving bioscience research reporting: the ARRIVE guidelines for reporting animal research. PLoS Biol. 2010;8(6):e1000412. doi:10.1371/journal.pbio.1000412. [CrossRef]
- Klosterhalfen B, Klinge U, Schumpelick V. Functional and morphological evaluation of different polypropylene-mesh modifications for abdominal wall repair. Biomaterials. 1998 Dec;19(24):2235-46. [CrossRef]
- Klinge U, Klosterhalfen B, Muller M, Schumpelick V Foreign body reaction to meshes used for the repair of abdominal wall hernias. Eur J Surg 1999;65:665–673. [CrossRef]
- Zwaans WAR, Verhagen T, Wouters L, Loos MJA, Roumen RMH, Scheltinga MRM. Groin Pain Characteristics and Recurrence Rates: Three-year Results of a Randomized Controlled Trial Comparing Self-gripping Progrip Mesh and Sutured Polypropylene Mesh for Open Inguinal Hernia Repair Ann Surg. 2018 Jun;267(6):1028-1033. [CrossRef]
- Weyhe D, Schmitz I, Belyaev O, Grabs R, Müller KM, Uhl W, Zumtobel V. Experimental comparison of mono-file light and heavy polypropylene meshes: less weight does not mean less biological response. World J Surg. 2006;30(8):1586–1591. [CrossRef]
- O’Dwyer PJ, Kingsnorth AN, Mohillo RG, Small PK, Lammers B, Horeysee G. Randomized clinical trial as-sessing impact of a lightweight or heavyweight on chronic pain after inguinal hernia repair. Br J Surg 2005;92:166-70.
- Silvestre AC, de Mathia G B, Fagundes, D J, Medeiros L R, Rosa M I. Shrinkage evaluation of heavyweight and lightweight polypropylene meshes in inguinal hernia repair: a randomized controlled trial. Hernia 2011 Dec;15(6):629-34.
- Schmedt CG, Sauerland S, Bittner R. Comparison of endoscopic procedure vs Progrip and other open mesh techniques for inguinal hernia repair: a meta-analysis of randomized controlled trials. Surg Endosc. 2005;19(2):188-9. [CrossRef]
- Bay-Nielsen M, Nilsson E, Nordin P, Kehlet H; Swedish Hernia Data Base the Danish Hernia Data Base Chronic pain after open mesh and sutured repair of indirect inguinal hernia in young males. Br J Surg 2004;91:1372–1376.
- Mayer F, Niebuhr H, Lechner M, Dinnewitzer A, Köhler G, Hukauf M, Fortelny RH, Bittner R, Köckerling F. When is mesh fixation in TAPP repair of primary inguinal hernia necessary? A register-based analysis of 11,230 cases. Surg Endosc. 2016;30(10):4363-71. [CrossRef]
- Watson JT, Webb DW, Stoikes NFN, Voeller GR. Affiliations expand Fibrin Sealant: A Review of the History, Biomechanics, and Current Applications for Prosthetic Fixation in Hernia Repair. Surg Technol Int. 2015 Nov;27:140-5.
- Jeans S, Williams GL, Stephenson BM. Migration after open mesh plug inguinal hernioplasty: a review of the literature. Am Surg. 2007 Mar;73(3):207-9. [CrossRef]
- Sahu RA, Nashine A, Mudey A, Sahu SA, Prasad R. Cardiovascular stents: types and future landscape. Cureus. 2023;15(8):e43438. [CrossRef]
- Borhani S, Hassanajili S, Tafti HA, Rabbani S. Cardiovascular stents: overview, evolution, and next generation. Prog Biomater. 2018;7:175-205. [CrossRef]
- Amato G, Puleio R, Romano G, Calò PG, Di Buono G, Cicero L, Cassata G, Goetze T, Buscemi S, Agrusa A, et al. Physiologic cyclical load on inguinal hernia scaffold ProFlor turns biological response into tissue regeneration. Biology. 2023;12(4):434. [CrossRef]
- Amato G, Agrusa A, Puleio R, Micci G, Cassata G, Cicero L, Di Buono G, Calò PG, Galia M, Romano G. A regenerative scaffold for inguinal hernia repair: MR imaging and histological cross-evidence. Int J Surg. 2021;96:106170.
- Matthews BD, Pratt BL, Pollinger HS, Backus CL, Kercher KW, Sing RF, Heniford TB. Assessment of adhesion formation to intra-abdominal polypropylene mesh and polytetrafluoroethylene mesh. J Surg Res. 2003;114(2):126-32. [CrossRef]
- Turza KC, Butler CE. Adhesions and meshes: synthetic versus bioprosthetic. Plast Reconstr Surg. 2012;130(5 Suppl 2):206S-13S.



| TPE technical properties | Value | Unit | Test Standard |
|---|---|---|---|
| ISO Data | |||
| Tensile Strength | 16 | MPa | ISO 37 |
| Strain at break | 650 | % | ISO 37 |
| Compression set at 70 °C, 24h | 54 | % | ISO 815 |
| Compression set at 100 °C, 24h | 69 | % | ISO 815 |
| Tear strength | 46 | kN/m | ISO 34-1 |
| Shore A hardness | 89 | - | ISO 7619-1 |
| Density | 890 | kg/m³ | ISO 1183 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).



