
Submitted:
27 November 2024
Posted:
28 November 2024
You are already at the latest version
Abstract
Posterior fixation is usually performed to restore spinal stability and decompress the spinal canal for unstable thoracolumbar burst fractures. This study compared the trunk and lower extremity joint kinematics of patients who underwent posterior fixation surgery after thoracolumbar fractures with healthy subjects. The optical motion capture was used to record the joint kinematics during walking. The trunk, hip, knee, and ankle joint angles and excursions in sagittal, frontal, and transverse planes were calculated, averaged, and compared between patients and control groups. The patients' group had significantly reduced hip extension and increased total excursion in the frontal plane, where the mean differences were 7.0º in hip extension and 4.2º in total excursion. In the ankle joint, dorsiflexion was significantly reduced with increased plantarflexion, and internal rotation was also increased in the patients’ group. However, there were no differences in knee joint kinematics. The patient exhibited more upright trunk position during the walking than the control group, where both peak trunk flexion and extension were significantly different, possibly indicating a stiffer trunk movement. This study provides fundamentals of the joint kinematics of the trunk and lower extremities after posterior surgical operation for thoracolumbar fracture, which may help to evaluate the surgical outcomes.
Keywords:
Gait analysis
; trunk
; lower extremity
; posterior fixation
; thoracolumbar fracture
1. Introduction
Thoracolumbar fractures are the most common spinal injuries and are mostly associated with motor vehicles and falls [1,2]. Posterior fixation and fusion techniques are usually performed to restore spinal stability and decompress the spinal canal for unstable thoracolumbar burst fractures. There was no significant difference was identified between the fixation with and without fusion [3,4]. Most of the previous studies have reported clinical complications and radiographic and functional outcomes of short or long-segment posterior fixation techniques for thoracolumbar burst fractures [5,6,7]. Kanna et al. [5] found that posterior fixation efficiently restored the radiological parameters such as kyphosis angle and anterior and posterior vertebral height in patients with severe unstable thoracolumbar fractures. Liang et al. [8] also showed the clinical effects of long-segment pedicle instrumentation for treating thoracolumbar fractures. Clinically, the visual analogue scale and Oswestry disability index are used to assess functional outcomes [3,6].
Clinical gait analysis is often used to quantify gait abnormalities in patients who underwent surgeries. Haddas et al. [9] performed gait analysis after surgical correction in patients with severe kyphosis from ankylosing spondylitis. Yagi et al. [10] assessed gait patterns in patients with adult spinal deformities (ASD) and the effect of corrective spinal surgery on gait. Mahaudens et al. [11] compared pre- and post-surgery conditions in thoracolumbar scoliosis patients. The effect of decompression surgery on lumbar spinal stenosis was evaluated through the three-dimensional (3D) motion analysis [12,13,14]. However, only one study assessed the gait parameters of patients who underwent posterior fixation and fusion surgery after thoracolumbar burst fractures [2]. They reported that characteristics of patients undergoing short and long-segment fusion are similar to those of healthy matched controls, but slight differences were observed on pelvic and hip excursions. This study was limited to assessing movement patterns of the lower extremity. To fully understand the effect of posterior fixation on the gait patterns, the lower extremity and the trunk joint movement patterns should be assessed by gait analysis. In this study, we investigated the lower extremities and trunk joint kinematics of patients who underwent posterior fixation surgery after thoracolumbar fractures and compared them against healthy subjects.
2. Materials and Methods
2.1. Participants
We recruited nine male patients (age, 42.9 ± 8.1 years; height, 170.5 ± 4.7 cm; weight, 79.0 ± 13.1 kg) who had posterior fixation after traumatic thoracolumbar burst fracture at the National Trauma and Orthopaedics Research Center with the same team. One patient underwent short-segment fixation, while the remaining seven underwent long-segment (LS). LS fixation is typically chosen for patients with more severe fractures, such as those involving adjacent structure distraction, dislocation, or complete burst fracture [15]. It was previously reported that either short or long fixation had less effect on the gait parameters [2] and radiological parameters [15]. Study inclusion was limited to neurologically intact patients with no lower extremity dysfunction or changes. Nine healthy male people (age 43.7 ± 6.3 years; height, 173.5 ± 3.6 cm; weight, 75.2 ± 8.7 kg) were also recruited with the same age, height, and weight. The study was approved by the Institutional Review Board of the Mongolian National University of Medical Science, and informed consent was obtained from all subjects. All research was performed in accordance with the relevant guidelines and regulations.
2.2. Experimental Setup and Data Processing
The gait analysis was performed at 18.1±2.5 months after surgery. The Optitrack motion capture system with ten cameras (Optitrack, NaturalPoint, Inc, USA), and 43 reflective markers were used to record the trunk and lower extremity movements during walking at a sampling rate of 100 Hz, where the markers were attached to anatomical landmarks according to the previous studies [16,17]. The markers were attached to the lower extremity (bilateral anterior superior iliac spines, posterior superior iliac spines, lateral/medial femoral condyles, lateral/medial malleolus, 1st/2nd/5th of metatarsus, posterior surface of calcaneus, four tracking markers on left/right thigh and shank) and the upper body (right/left acromion, deepest point of incisura jugularis, xiphoid process, C7 vertebra, T2 vertebra, T7 vertebra, and L1, L3 and L5 vertebra). Subjects walked at their comfortable walking speed along a 6 m walkway after multiple trails.
The recorded optical marker data were exported to the Visual 3D software (C-Motion, Inc, USA) to develop a musculoskeletal model, where the 3D joint kinematics were calculated. The 3D trunk angle was calculated as the orientation of the thorax relative to the pelvis segment (Figure 1) [18]. After the experiment, walking data were trimmed to one full gait cycle (right heel strike to the next right heel strike). The trunk, hip, knee, and ankle joint angles in sagittal (SP), frontal (FP), and transverse plane (TP) were calculated, averaged, and compared between patients and control groups. Total excursion motion was estimated according to the previous studies [19,20]. A statistical difference between the two groups was determined using an individual T-test.
3. Results
The joint angles and total excursion motion in each anatomical plane are presented in Table 1. The hip, knee, ankle, and trunk joint angles in SP, FP, and TP for the control group are shown in Figure 2. The total excursion of the hip, knee, ankle, and trunk in SP were 35.3±3.5º, 57.6±4.6º, 30.5±4.3º and 3.2º ±1.3º (Figure 2).
The hip, knee, ankle, and trunk joint angles in SP, FP, and TP for the patient group are shown in Figure 3. The total excursion of the hip, knee, ankle, and trunk in SP were 33.3±6.1º, 58.5±6.6º, 35.8±5.5º and 3.1±1.0º (Figure 3).
The patients' group had significantly reduced hip extension (p=0.02) and increased total excursion in FP (p<0.05), where the mean differences were 7.0º in hip extension and 4.2 º in total excursion. In the ankle joint, dorsiflexion was significantly reduced (p=0.03) with increased plantarflexion (p=0.03), and internal rotation was also increased (p=0.02) in the patients’ group (Figure 4). Reductions were more prominent in dorsiflexion (6.4º) than plantarflexion (5.3º). However, there were no differences in knee joint kinematics (Table 1). The results showed compensatory extension of the hip and dorsiflexion of the ankle due to the stiffer upper body for patients with posterior fixation during walking. The patient exhibited more upright trunk position during the walking than the control group, where both peak trunk flexion and extension were significantly different (p<0.05), possibly indicating a stiffer trunk movement. Moreover, patients tended to have more right rotation of the trunk than healthy subjects (p=0.04).
4. Discussion
The LS fixation is the stiffest and provides more stability to manage thoracolumbar burst fractures with good clinical and radiological outcomes [21]. After surgery, we expected the upper body stiffening due to posterior fixation would affect joint kinematics. Our results showed that patients who underwent surgery had more upright trunk positions with higher hip extension and ankle dorsiflexion when compared to healthy subjects. Specifically, statistical difference was observed during hip extension in SP, hip total excursion in SP, ankle dorsiflexion and plantarflexion in SP, ankle internal rotation in TP, trunk flexion and extension in SP, and trunk right rotation in TP, respectively. The main changes were shown in the trunk, hip, and ankle joints in the SP after surgery. It could be explained by patients with stiffened upper body to compensate by having more hip flexion and ankle plantarflexion while walking.
Various studies have noted that the compensation mechanism for walking differs between patients who underwent surgery and healthy individuals. Yagi et al. [10] found that compensatory flexion of the hip and pelvic posterior shift for ASD patients. Mahaudens et al. [11] also noted that the range of motions increases in unaffected joints in spinal fusion for adolescent idiopathic scoliosis.
Although few studies have reported gait parameters in patients after posterior fixation and fusion for thoracolumbar fracture, similar trends were observed for lower extremity joint angles. Oken et al. [2] reported that pelvic and hip excursions in the SP differed slightly between control and patients who underwent posterior fixation and fusion surgery. Similar to this study, the present study showed a difference in hip and trunk rotation in the SP, which may explain why the posterior fixation method leads to a more upright trunk position. Then, the pelvis is more anterior tilted, and the hip is more extended during walking.
The study has several limitations. First, a few participants were recruited due to difficulty finding patients because gait analysis was performed about 18 months after surgery. Previous studies have shown that lower extremity gait parameters did not change significantly between 1 and 2 years after spinal surgery. We only investigated joint kinematics, but comprehensive gait analysis should include kinetics [11]. Various daily activities should be analyzed in addition to walking further to elucidate the effect of posterior fixation on the trunk. Furthermore, few gait studies are available regarding patients with a posterior fixation for thoracolumbar fracture, which makes comparison and interpretation difficult.
Our results showed differences in trunk and lower extremity kinematics between patients with posterior fixation and healthy people. Patients who underwent surgery tended to have a more upright trunk than healthy people. This study provides fundamentals of the joint kinematics of the trunk and lower extremities after a posterior surgical operation for a thoracolumbar fracture, which may help evaluate the surgical outcomes and plan further reconstruction surgery if needed.
Author Contributions
Conceptualization, B.K. and B.B.; methodology, B.K., B.B and G.D.; software, B.K.; formal analysis, B.K. and B.B.; investigation, B.K., G.D; resources, B.B. and M.S.; data curation, B.K.; writing—original draft preparation, B.B.; writing—review and editing, B.K. and M.S.; visualization, B.K. and B.B.; supervision, G.D and M.S.; project administration, B.K; funding acquisition, B.K. and B.B. All authors have read and agreed to the published version of the manuscript.
Funding
This work was supported by the Mongolian University of Science and Technology (mfund-05/2022) and the “Mongolia-Japan Engineering Education Development” project (J24C16), Mongolia.
Institutional Review Board Statement
The study was conducted according to the guidelines of the Declaration of Helsinki and approved by the Institutional Review Board of the Mongolian National University of Medical Sciences.
Informed Consent Statement
Informed content was obtained from all subjects involved in the study.
Data Availability Statement
Data are contained within the article.
Acknowledgments
The authors would like to thank all participants.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Aebi, M. Classification of thoracolumbar fractures and dislocations. Eur. Spine J. 2009, 19, 2–7. [Google Scholar] [CrossRef] [PubMed]
- Oken, F.; Yildirim, O.; Oken, O.; Gulcek, M.; Yavuzer, G.; Ucaner, A. Short or long fusion after thoracolumbar burst fractures does not alter selected gait parameters: a preliminary study. J. Orthop. Res. 2011, 29, 915–918. [Google Scholar] [CrossRef] [PubMed]
- Tian, N.-F.; Wu, Y.-S.; Zhang, X.-L.; Wu, X.-L.; Chi, Y.-L.; Mao, F.-M. Fusion versus Nonfusion for Surgically Treated Thoracolumbar Burst Fractures: A Meta-Analysis. PLOS ONE 2013, 8, e63995. [Google Scholar] [CrossRef] [PubMed]
- McLain, R.F. The Biomechanics of Long Versus Short Fixation for Thoracolumbar Spine Fractures. Spine 2006, 31, S70–S79. [Google Scholar] [CrossRef] [PubMed]
- Kanna, R.M.; Shetty, A.P.; Rajasekaran, S. Posterior fixation including the fractured vertebra for severe unstable thoracolumbar fractures. Spine J. 2015, 15, 256–264. [Google Scholar] [CrossRef] [PubMed]
- Jeon, C.-H.; Lee, H.-D.; Lee, Y.-S.; Seo, J.-H.; Chung, N.-S. Is It Beneficial to Remove the Pedicle Screw Instrument After Successful Posterior Fusion of Thoracolumbar Burst Fractures? Spine 2015, 40, E627–E633. [Google Scholar] [CrossRef]
- Leduc, S.; Mac-Thiong, J.-M.; Maurais, G.; Jodoin, A. Posterior pedicle screw fixation with supplemental laminar hook fixation for the treatment of thoracolumbar burst fractures. . 2008, 51, 35–40. [Google Scholar]
- Liang, J.Z.; Corso, N.; Turner, E.; Zakhor, A. Image Based Localization in Indoor Environments. 2013 4th International Conference on Computing for Geospatial Research & Application (COM.Geo). LOCATION OF CONFERENCE, United StatesDATE OF CONFERENCE; pp. 70–75.
- Haddas, R.; Xu, M.; Lieberman, I.; Yang, J. Finite Element Based-Analysis for Pre and Post Lumbar Fusion of Adult Degenerative Scoliosis Patients. Spine Deform. 2019, 7, 543–552. [Google Scholar] [CrossRef] [PubMed]
- Yagi, M.; Ohne, H.; Konomi, T.; Fujiyoshi, K.; Kaneko, S.; Takemitsu, M.; Machida, M.; Yato, Y.; Asazuma, T. Walking balance and compensatory gait mechanisms in surgically treated patients with adult spinal deformity. Spine J. 2016, 17, 409–417. [Google Scholar] [CrossRef] [PubMed]
- Mahaudens, P.; Detrembleur, C.; Mousny, M.; Banse, X. Gait in thoracolumbar/lumbar adolescent idiopathic scoliosis: effect of surgery on gait mechanisms. Eur. Spine J. 2010, 19, 1179–1188. [Google Scholar] [CrossRef] [PubMed]
- Loske, S.; Nüesch, C.; Byrnes, K.S.; Fiebig, O.; Schären, S.; Mündermann, A.; Netzer, C. Decompression Surgery Improves Gait Quality in Patients with Symptomatic Lumbar Spinal Stenosis; Elsevier Inc., 2018; Vol. 18; ISBN 0-00-000026-4.
- Kuwahara, W.; Deie, M.; Fujita, N.; Tanaka, N.; Nakanishi, K.; Sunagawa, T.; Asaeda, M.; Nakamura, H.; Kono, Y.; Ochi, M. Characteristics of thoracic and lumbar movements during gait in lumbar spinal stenosis patients before and after decompression surgery. Clin. Biomech. 2016, 40, 45–51. [Google Scholar] [CrossRef] [PubMed]
- Lamas, V.; Gueugnon, M.; Fournel, I.; Grelat, M.; Maillefert, J.-F.; Ornetti, P.; Martz, P. Dynamic global sagittal alignment in patients with lumbar spinal stenosis: Analysis of the effects of decompression surgery on gait adaptations. Gait Posture 2021, 88, 272–279. [Google Scholar] [CrossRef] [PubMed]
- Borkhuu, B.; Batochir, B.; Sonomjamts, M.; Tsevegmid, E.; Lkhagvasuren, N. Long Versus Short-segment Stabilization in Patients with Traumatic Thoracolumbar Fractures. Ortop. Traumatol. Rehabil. 2023, 25, 173–179. [Google Scholar] [CrossRef] [PubMed]
- Jan, S.V.S. Color Atlas of Skeletal Landmark Definitions; Churchill Livingstone/Elsevier, 2007; ISBN 0-443-10315-1.
- Lewis, C.L.; Sahrmann, S.A. Effect of posture on hip angles and moments during gait. Man. Ther. 2014, 20, 176–182. [Google Scholar] [CrossRef] [PubMed]
- Dambadarjaa, B.; Khuyagbaatar, B.; Bayartai, M.-E.; Purevsuren, T.; Shambaljamts, T.; Kim, Y.H. Kinematic comparison between people with and without low back pain during functional activities. J. Mech. Sci. Technol. 2024, 38, 1–7. [Google Scholar] [CrossRef]
- Malone, A.; Meldrum, D.; Bolger, C. Gait impairment in cervical spondylotic myelopathy: comparison with age- and gender-matched healthy controls. Eur. Spine J. 2012, 21, 2456–2466. [Google Scholar] [CrossRef] [PubMed]
- Khuyagbaatar, B.; Tumurbaatar, M.; Tsenkherjav, K.; Purevsuren, T.; Shambaljamts, T.; Kim, K.; Danjkhuu, T.; Danaa, G.; Kim, Y.H. Kinematic Comparison of Snatch and Clean Lifts in Weightlifters Using Wearable Inertial Measurement Unit Sensors. Phys. Act. Heal. 2024, 8, 1–9. [Google Scholar] [CrossRef]
- Aly, T.A. Short Segment versus Long Segment Pedicle Screws Fixation in Management of Thoracolumbar Burst Fractures: Meta-Analysis. Asian Spine J. 2017, 11, 150–160. [Google Scholar] [CrossRef]
Figure 1.
Marker set and joint angle definition. Red dots represent markers attached to the modeled segment positions.
Figure 1.
Marker set and joint angle definition. Red dots represent markers attached to the modeled segment positions.
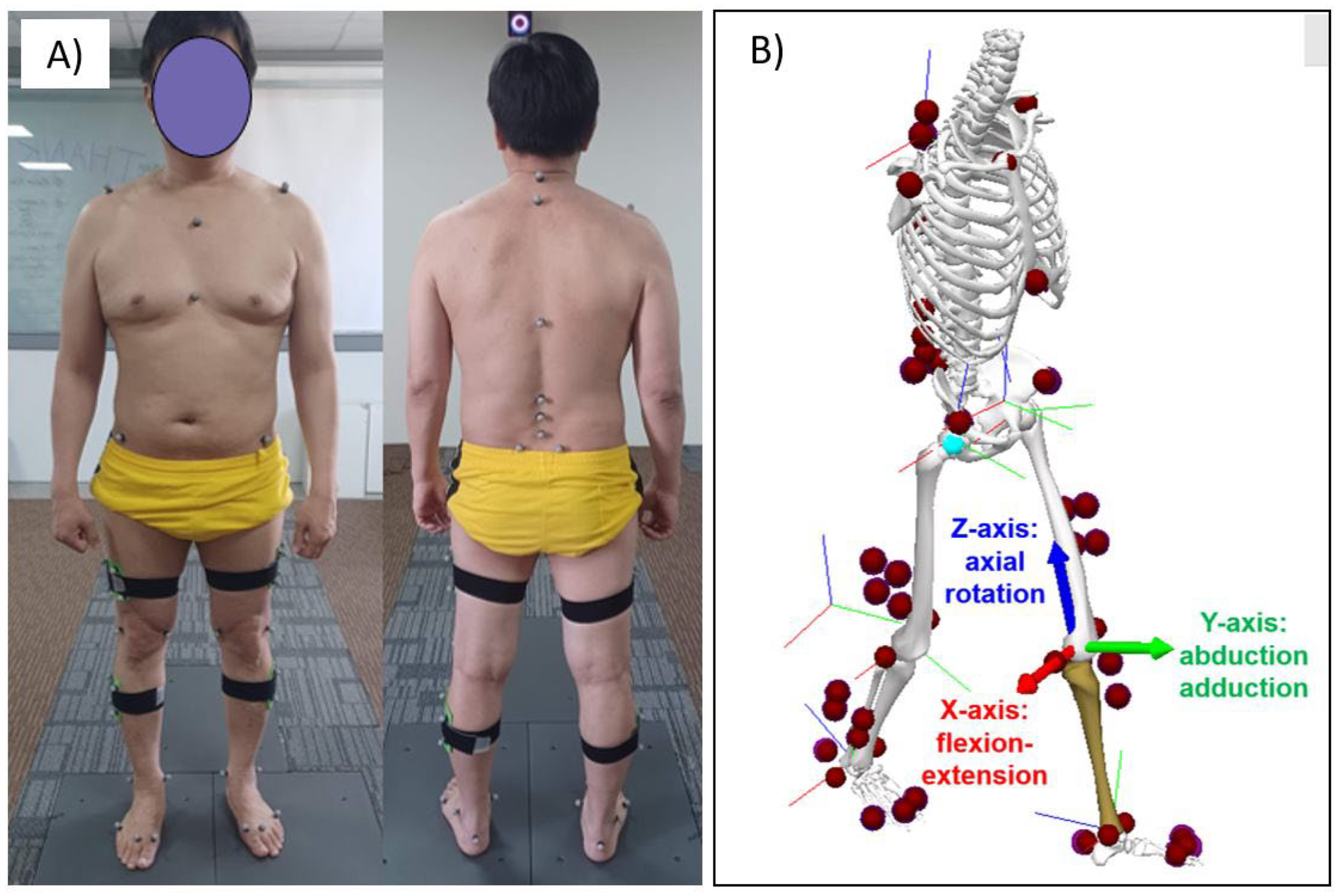
Figure 2.
The hip, knee, ankle, and trunk joint angles in the control group.
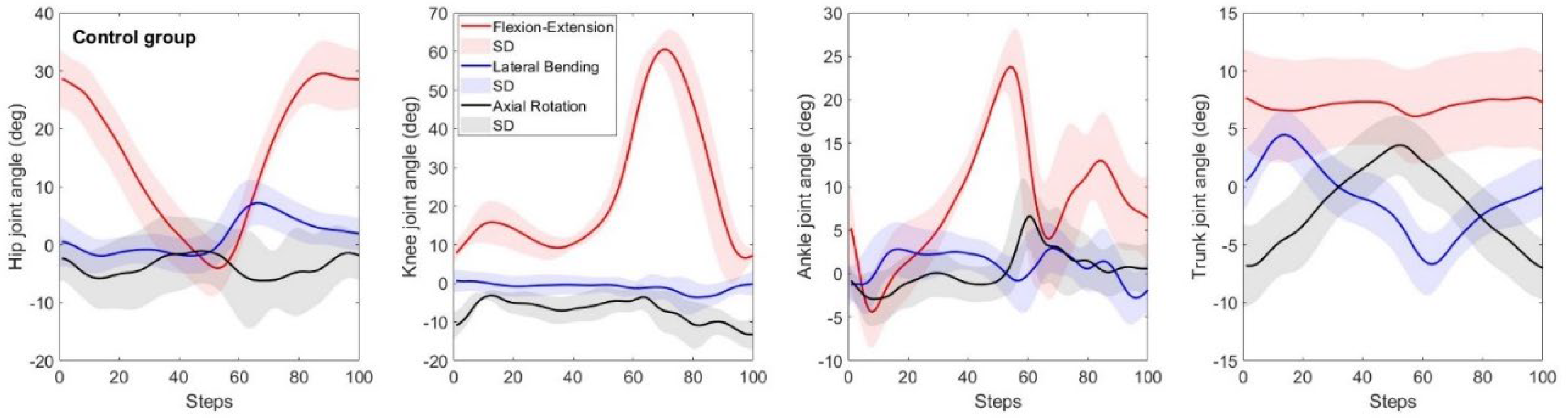
Figure 3.
The hip, knee, ankle, and trunk joint angles in the patients group.
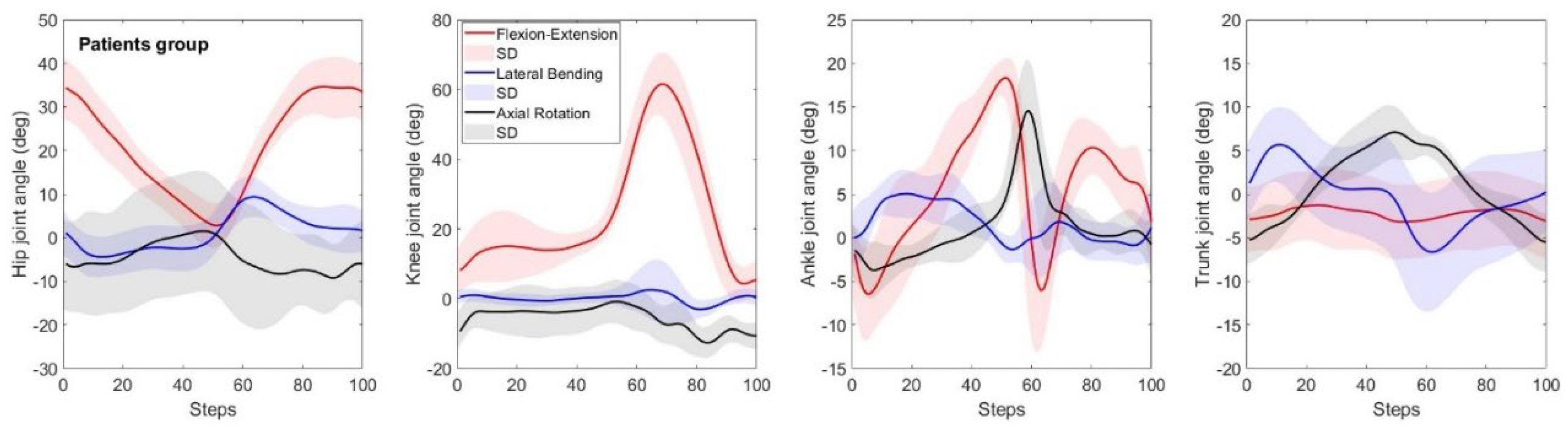
Figure 4.
The hip, knee, ankle, and trunk joint angles in between the control and patient group.
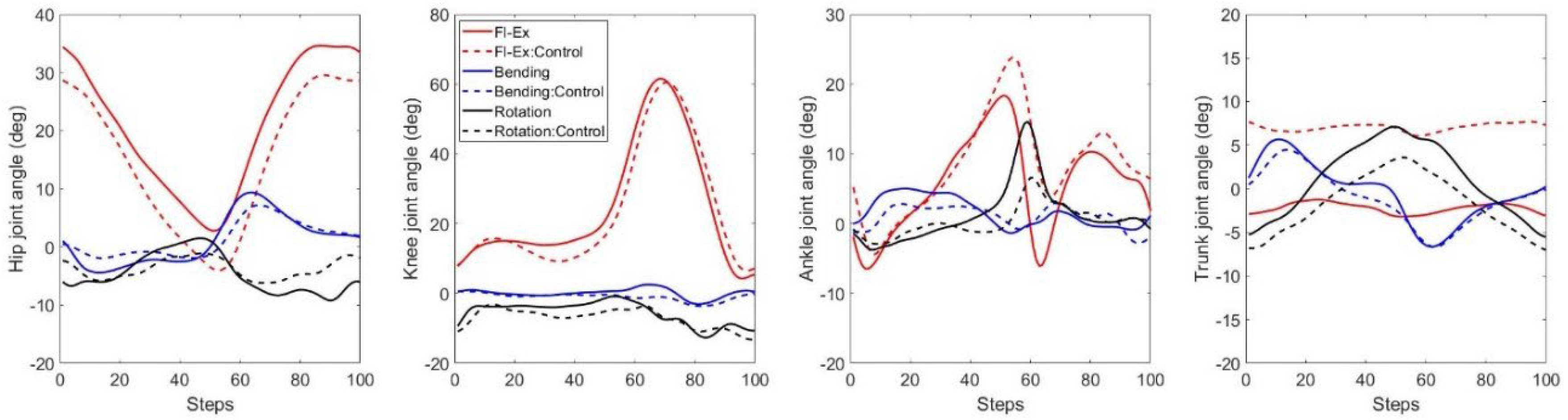

Table 1.
Hip, knee, ankle, and trunk joint angles and total excursion in SP, FP, and TP for control and patient groups.
Table 1.
Hip, knee, ankle, and trunk joint angles and total excursion in SP, FP, and TP for control and patient groups.
| Joints | Plane | Motions | Control group (°) | Patient group (°) | Mean differences (°) | p-value |
|---|---|---|---|---|---|---|
| Hip | SP | Total excursion | 35.3±3.5 | 33.3±6.1 | 2.0 | 0.468 |
| Peak flexion | 30.9±5.6 | 35.9±6.9 | 5.0 | 0.166 | ||
| Peak extension | -4.4±4.7 | 2.6±5.1 | 7.0 | 0.021 | ||
| FP | Total excursion | 10.7±2.0 | 14.9±2.0 | 4.2 | 0.002 | |
| Peak abduction | 7.5±3.7 | 9.7±4.4 | 2.2 | 0.328 | ||
| Peak adduction | -3.2±2.7 | -5.2±4.2 | 2.0 | 0.306 | ||
| TP | Total excursion | 13.1±4.0 | 14.0±7.1 | 0.9 | 0.782 | |
| Peak internal rotation | -2.7±4.6 | 1.8±13.6 | 0.9 | 0.878 | ||
| Peak external rotation | -10.4±6.3 | -12.2±9.6 | 1.7 | 0.698 | ||
| Knee | SP | Total excursion | 57.6±4.6 | 58.5±6.6 | 0.9 | 0.764 |
| Peak flexion | 62.0±4.9 | 62.1±8.8 | 0.1 | 0.984 | ||
| Peak extension | 4.5±3.5 | 3.6±5.2 | 0.9 | 0.728 | ||
| FP | Total excursion | 7.5±2.3 | 10.9±4.1 | 3.4 | 0.092 | |
| Peak abduction | 2.1±2.6 | 6.0±5.6 | 4.0 | 0.121 | ||
| Peak adduction | -5.4±2.7 | -4.8±3.3 | 0.6 | 0.712 | ||
| TP | Total excursion | 14.9±4.4 | 15.4±4.3 | 0.6 | 0.794 | |
| Peak internal rotation | 0.1±2.1 | 0.3±6.4 | 0.3 | 0.907 | ||
| Peak external rotation | -14.8±2.7 | -15.1±3.2 | 0.3 | 0.845 | ||
| Ankle | SP | Total excursion | 30.5±4.3 | 35.8±5.5 | 5.3 | 0.068 |
| Peak dorsiflexion | 25.5±4.1 | 19.0±2.5 | 6.4 | 0.005 | ||
| Peak plantarflexion | -5.1±4.1 | -10.4±4.0 | 5.3 | 0.030 | ||
| FP | Total excursion | 9.4±2.0 | 9.3±4.5 | 0.1 | 0.964 | |
| Peak inversion | 5.2±2.7 | 6.5±2.3 | 1.3 | 0.342 | ||
| Peak eversion | -4.2±2.7 | -4.1±2.3 | 0.1 | 0.949 | ||
| TP | Total excursion | 12.9±5.0 | 13.2±4.9 | 0.3 | 0.917 | |
| Peak internal rotation | 8.5±4.0 | 15.6±5.6 | 7.1 | 0.020 | ||
| Peak external rotation | -4.5±2.2 | -4.7±2.4 | 0.3 | 0.823 | ||
| Trunk | SP | Total excursion | 3.2±1.3 | 3.1±1.0 | 0.1 | 0.928 |
| Peak flexion | 8.6±4.3 | -0.9±4.5 | 9.5 | 0.002 | ||
| Peak extension | 5.5±3.7 | -3.9±3.8 | 9.4 | 0.001 | ||
| FP | Total excursion | 11.5±2.4 | 12.6±4.6 | 1.1 | 0.574 | |
| Peak right bending | 4.6±2.1 | 5.8±4.2 | 1.2 | 0.511 | ||
| Peak left bending | -6.9±2.6 | -6.8±6.9 | 0.1 | 0.978 | ||
| TP | Total excursion | 11.4±2.5 | 13.3±6.0 | 1.9 | 0.466 | |
| Peak right rotation | 3.8±2.7 | 7.4±3.1 | 3.6 | 0.040 | ||
| Peak left rotation | -7.6±2.9 | -5.9±3.3 | 1.7 | 0.330 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



