
Submitted:
26 November 2024
Posted:
28 November 2024
You are already at the latest version
Abstract
Effective cancer therapies must address the tumor microenvironment (TME), a complex network of tumor cells and stromal components, including endothelial, immune, and mesenchymal cells. Durable outcomes require targeting both tumor cells and the TME while minimizing systemic toxicity. Interleukin-2 (IL-2)-based therapies have shown efficacy in cancers such as metastatic melanoma and renal carcinoma but are limited by severe side effects.
Innovative IL-2-based immunotherapeutic approaches include immunotoxins, such as antibody-drug conjugates, and immunocytokines, antibody-cytokine fusion proteins that enhance tumor-specific delivery. These strategies activate cytotoxic CD8+ T lymphocytes and Natural Killer (NK) cells, eliciting a potent Th1-mediated anti-tumor response. Modified IL-2 variants with reduced Treg cell activity further improve specificity and reduce immunosuppression. Additionally, IL-2 conjugates with peptides or anti-angiogenic agents offer improved therapeutic profiles.
Combining IL-2-based therapies with immune checkpoint inhibitors (ICIs), anti-angiogenic agents, or radiotherapy has demonstrated synergistic potential. Preclinical and clinical studies highlight reduced toxicity and enhanced anti-tumor efficacy, overcoming TME-driven immune suppression. These approaches mitigate the limitations of high-dose soluble IL-2 therapy, promoting immune activation and minimizing adverse effects.
This review critically explores advances in IL-2-based therapies, focusing on immunotoxins, immunocytokines, and IL-2 derivatives. Emphasis is placed on their role in combination strategies, showcasing their potential to target the TME and improve clinical outcomes effectively.
Keywords:
IL-2
; immunotoxins
; immunocytokines
1. Introduction
Cancer therapies have been revolutionized by the use of immune checkpoint inhibitors (ICI) both as alone treatments and in combination with other approaches [1,2,3,4,5,6,7,8,9,10]. Initially applied for patients with metastatic melanoma and metastatic renal cell carcinoma, these therapies have since been extended to other cancer types, achieving excellent results and, in some cases, definitive cures [1,4,8]. However, it became apparent that a significant portion of the patients did not respond to ICI [11,12,13,14]. Among the various potential reasons for this, two critical factors must be considered: the inhibitory role of the TME on immune cells and its proactive role in promoting carcinogenesis and tumor progression [15,16,17,18,19,20].
Of note in 2011, Hanahan and Weinberg [21] redefined and highlighted several new key hallmarks of cancer, including enabling characteristics that were initially postulated in 2000 [22]. Of particular importance are three hallmarks that play fundamental roles in tumor dynamics: “evading immune destruction”, “tumor-promoting inflammation”, and “immune orchestration of angiogenesis”. These characteristics underscore the essential and dual role of the immune system in neoplastic diseases.
Immune cells, particularly innate immune cells such as macrophages and natural killer (NK) cells, can exhibit potent anti-tumor activities, including phagocytosis and cytotoxic functions. [23,24,25]. However, at the same time, macrophages and NK cells upon interactions with the tumor and TME, can become protumor effectors with low cytotoxic capacities and display immunosuppressive and pro-angiogenic behaviors [26,27,28].
In this context, Hanahan recently suggested new emerging characteristics of tumor cells: “unlocking phenotypic plasticity,” “non-mutational epigenetic reprogramming,” “polymorphic microbiomes,” and “senescent cells”, making the study of malignant tumor growth even more complex and intricate [29]. However, increasing experimental data have begun to clarify the protumor or antitumor roles played by different types of immune or stromal cells, in particularly in promoting or suppressing tumor growth, reinforcing or inhibiting metastasis and contributing to therapy.
Hanahan defined “unlocking phenotypic plasticity” as a potential new hallmark of cancer, referring specifically to malignant cells. However, from the point of view of the immune cells in the TME, it appears that these cells can also exhibit high plasticity in both their phenotype and function. Indeed, as a result of tumor signaling and the release of soluble factors or extracellular vesicles, immune cells can become highly plastic, altering their phenotype and function. These alterations, induced by interactions with cancer, stromal and endothelial cells, as well as cytokines/chemokines in the TME, can lead to impairment of cytotoxic activities, the development of immunosuppressive features and, in many cases, the acquisition of pro-angiogenic activities.
Among these factors, cytokines play a crucial role in shaping the cancer-induced immune cycle by prompting various processes such as tumor antigen expression, antigen presentation, priming and activation of immune cells, recruitment of effector immune cells to the tumor site, and ultimately facilitating cancer cells elimination within the TME [30]. On the other hand, proinflammatory cytokines might have both protumor or antitumor effects. For IL-2, several lines of evidence have shown that this cytokine serves as a crucial regulator for the activation of helper/regulatory T cells, cytotoxic T cells and NK cells, influencing their proliferation, differentiation, and contributing to both pro- and anti-inflammatory immune responses. Some specific cytokines are identified as promising cancer immunotherapies. They function by adjusting the immune response against cancer cells and by directly displaying anti-cancer effects, including inhibiting proliferation and promoting apoptosis. Cytokines have a substantial track record as anticancer treatments, starting from the 1970s, when interferon (IFN)-α and IL-2 were the first cytokines utilized in cancer therapy [30]. Among the various types of immunotherapies, cytokine therapy, shows high promise in cancer treatment. IL-2 treatment has shown significant efficacy in metastatic melanoma, renal cancer, and advanced non-Hodgkin’s lymphoma. However, following these early advancements, the clinical translation of these molecules has been significantly restricted due to their broad and diverse biological effects across various cell types. These characteristics, combined with suboptimal pharmacokinetics, such as short half-lives, have impeded the effective systemic administration of cytokines, primarily due to severe dose-limiting toxicities [31]. In fact, severe adverse reactions, such as vascular leakage syndrome, underscore the need for careful administration under the supervision of an oncologist in a hospital setting. To address these challenges, novel engineering strategies been developed to broaden the therapeutic range, extend the duration of pharmacokinetic effects, improve tumor-specific targeting, and minimize adverse effects, thereby enhancing the overall efficacy of the therapy [31]. Herein, we focus on discussing the impact and relevance of anti-cancer immune effectors induced by IL-2 immunotoxins (IT), IL-2 immunocytokines and IL-2 derivatives or variants in different combined therapies.
2. Main Features of IL-2 and Tumor Specific Targeting of IL-2
Since its discovery in 1976 and the subsequent understanding of its vital role as a lymphocyte T-cell growth factor, the cytokine IL-2 was approved in the 1990s for use in patients with advanced stage cancer, including renal cell carcinoma and later for metastatic melanoma. IL-2 is a 15.5 kDa glycoprotein involved in immune response [32,33,34]. IL-2 exerts its function by interacting with IL-2 receptors (IL-2R) [34,35,36]. The IL-2R is comprised of three different subunits: IL2Rα (CD25), IL2-Rβ (CD122) and IL-2Rγ (CD132). The strongest binding affinity is observed when IL-2 binds to the trimeric IL-2Rαβγ complex, though it can also bind to the dimeric IL-2Rβγ [37,38]. This implies that the lymphocytes expressing the trimeric form of the IL-2R will respond promptly to 10-100 folds lower amount of IL-2 than cell population expressing the dimeric βγ IL-2R. Indeed, regulatory CD4+ T cells and activated T cells display high CD25 expression and respond to IL2 very efficiently [39,40]. On the other hand, CD8+ memory T cells and NK cells, which express IL-2Rβγ+, require higher doses of IL-2 than regulatory T cells. Upon binding to IL-2R, the signal transduction cascade is initiated through the heterodimerization of the β and γ subunits, leading to the activation of Janus kinases (JAK1 and JAK3) and the subsequent phosphorylation of the β chain. This activation recruits and phosphorylates STAT transcription factors, primarily STAT5, which dimerize, translocate to the nucleus, and bind to DNA to promote the transcription of genes responsible for T and NK cell activation and proliferation. This signaling pathway also engages downstream PI3K/AKT/mTOR and MAPK/ERK pathways [37,38,41,42].
High-dose IL-2 regimens have shown considerable efficacy, inducing potent cytolytic responses and expansion of CD8+ T and NK cells in approximately 10% of patients. However, a substantial portion of patients experienced severe adverse effects. Among these, is vascular leak syndrome (VLS) and severe pulmonary edema, attributed to direct endothelial cell action inducing vasodilation, as well as fever, hypotension, cytopenia and organ dysfunction [43,44,45,46,47]. Both innate and adaptive immunity influence VLS onset, with NK cells contributing and Treg cells mitigating severity [48,49,50,51]. While systemic IL-2 administration for cancer has resulted in toxicity, local application, particularly intratumoral administration, shows promise [52,53,54]. However, it is evident that IL-2 can play a dual role in anti-tumor immunity. On one hand, it can trigger the generation of anti-tumor cytotoxic effector cells, such as CD8+ T cell antigen specific lymphocytes and NK cells, on the other hand, it can stimulate the immunomodulatory function of Treg cells, leading to the inhibition and exhaustion of the anti-tumor immune response. Notably, the use of low doses of IL-2 preferentially activates Treg cells, resulting in the inhibition and weakening of anti-cancer cytolytic responses [55,56,57,58,59].
Additionally, the half-life and the efficacy of IL-2 should be enhanced. It is crucial that these modified properties of IL-2 do not lead to increased vascular toxicity or heightened immunoregulatory effects [60,61]. The features of chimeric cytokines such as IL-2 and IL-15 have been extensively described in recent studies [62]. Indeed, the generation of several mutated IL-2 as well as the pegylation or production of IL-2 prodrugs can increase the half-life and the efficacy of IL-2 as detailed summarized [62]. The primary challenge to address is targeting IL-2 to the tumor to prolong its effect at this specific site; this to limit IL-2 interaction with the α-chain of IL-2R on endothelial and pulmonary cells which can lead to severe, life-threatening effects [63,64,65,66]. The solution of this issue lies in targeting the tumor with IL-2 in association with of an anti-tumor specific antibody generating an immunocytokine.
A detailed list of immunocytokines is reported by Ren et al. [67,68,69,70,71,72,73] and some of these immunocytokines will be discussed later on in this review. It is important to note that the antibody can be directed either to tumor cells or to components of the TME, such as mesenchymal stromal cells or tumor-associated fibroblasts. This targeting could enhance the local immune response by activating effector cells, such as CD8+ T cells and NK cells. Additionally, IL-2 can be part of a fused IT, as described in the next paragraph [62,74,75].
3. IL-2 Immunotoxins as Antibody-Drug Conjugates to Target and Fight Cancer Cells
The targeting of a tumor with a cytotoxic drug is one of the easiest ways to kill proliferating tumor cells [76,77,78]. This targeting is more specific when the cytotoxic drug is linked to a molecule able to recognize mainly the tumor cell [79]. This is achieved using antibody-drug conjugates (ADC) or proteins generated by molecular engineering, which are composed of a toxin and an antibody fragment capable of interacting with a tumor- specific or tumor-associated antigen [80,81,82,83,84]. In this way, the protein carrying the toxin can enter into the tumor cell, allowing the toxin to specifically kill the cell [85,86,87]. For example, it has been shown that a fusion protein, composed of the truncated diphtheria toxin, IL-2 and an anti-CCR4 antibody generating a bispecific IL2-CCR4 IT, can be used for the treatment of cutaneous T-cell lymphoma (CTCL) [88]. CTCL can indeed express good levels of IL-2Rα and CCR4 antigens, making these two receptors the optimal targets for delivering this IT. Importantly, this complex has demonstrated significant efficacy in prolonging the survival of mice bearing a CTCL tumors. Notably, it was found that this IT was more effective than the anti-CD30 ADC, Brentuximab-Vedotin. Interestingly, the combo of this ADC with the IT has been shown to produce a stronger anti-CTCL response than using either the ADC or the IT alone (Figure 1).
This indicates that the combination of these two drugs can enhance the therapeutic response in this murine model [89]. It is of note, that the IT can target not only CTCL cells but also the infiltrating Treg cells decreasing their immunosuppressive effects. This is an example of how an IL-2 IT can influence the anti-tumor response. Some recent data indicated that the CCR4-IL2 bispecific IT has a favorable safety profile in rats and minipigs animal models, suggesting its possible future use in human clinical trials [90].
However, it is important to consider that IL-2 based IT may also interact with anti-tumor effector cells. In this context, it has been shown that Denileukin Difititox (DD), which is composed of IL-2 fused to diphtheria toxin can enhance the anti-tumor immunity by interacting with the IL-2Rαβγ trimeric form selectively expressed on Treg cells, leading to their depletion [91,92]. These findings have been challenged by some observations indicating that DD administration in cynomolgus monkeys can lead to significant and long-lasting depletion of peripheral blood CD16+CD8+NKG2A+CD3- NK cells, beside a strong but transient elimination of peripheral Treg cells [93]. However, this depletion can be considered an unwanted side effect, as activated NK cells are important anti-tumor effectors. Interestingly, co-administration of DD and IL-15 has been shown to prevent DD-induced NK cell depletion both in vitro and in vivo, without affecting the strong depletion of Treg cells. This protective effect is attributed to the interaction of IL-15 with IL-2Rβγ on NK cells [91,92]. Taken together, these findings suggest that the use of IL-2-based IT should be thoroughly analyzed, with consideration given to the potential use of other factors, such as IL-15, to modulate their effects.
4. Immunotherapy Using Combined Tumor Microenvironment-Targeted IL-2 Cytokine
It quickly became evident that new biotechnological tools were needed for the clinical application of IL-2 to overcome important negative factors in cancer therapy. As a result, various IL-2 immunocytokines, which consist of IL-2 fused to antibodies targeting different tumor or TME antigens, have been developed and evaluated in tumor mouse models, yielding encouraging results [93,94,95,96,97,98,99,100,101,102,103]. Antibody-cytokine protein fusion combinations show promise in enhancing efficacy, when used in combination with other treatments at the appropriate time. While pro-inflammatory immunocytokines, including IL-2, can trigger side effects, these are generally of low intensity and can be managed through careful dosing and infusion strategies. Various cytokines such as TNF-α, IL-12, and IL-2 have been employed as they can stimulate different immune cell subsets [104,105,106,107,108,109,110]. By fusing IL-2 with antibodies targeting tumor-associated antigens, researchers aimed to localize cytokine activity to the TME, employing diverse targeting strategies and modulating pharmacokinetic properties with different antibody formats [111]. Clinical studies using IL-2 immunocytokines, particularly in combination setting with other biopharmaceuticals, have demonstrated efficacy in inducing anti-tumor immune responses mediated by CD8+ T cells, NK cells, and macrophages (https://www.clinicaltrials.gov), as recently reviewed by Raeber et al. [112].
Diverse tumor or tumor stroma antigens has been targeted with IL-2 immunocytokine including carcinoembryonic antigen (CEA), CD20, CD30, disialoganglioside 2 (GD2), epithelial cell adhesion molecule (EpCAM), fibroblast activation protein α(FAP), extracellular matrix (ECM) proteins preferentially expressed in the tumor vasculature, such as extra domain A of fibronectin (A-FN), extra domain B of fibronectin (B-FN), and tenascin-C. The selection of ECM tumor proteins is based on the fact that some isoforms are highly expressed in the TME while they are either absent or weakly expressed in healthy tissues [113,114]. An alternative approach to using IL-2 TME specific therapy is the targeting of IL-2 to CTLs and NK cells via NKG2D surface molecule. For this purpose, a mutant moiety of IL-2, which lacks the binding capacity to CD25, was developed. This construct is formed by using a virally high-affinity encoded NKG2D ligand, known as orthopoxvirus major histocompatibility complex class I like protein (OMCP) [115]. It was shown that OMCP-mutIL-2 in a Lewis lung carcinoma mouse model was effective in inducing a strong NK cell-mediated therapeutic responses.
One of the most studied IL-2 immunocytokines has been L19-IL-2, targeting the neoangiogenesis tumor-specific B-FN isoform. L19-IL-2 has been evaluated in various tumor contexts in mouse models, where it has shown promising results in combination with other anti-tumor therapies. For example, when combined with anti-CTLA-4 ICIs or another immunocytokine consisting of L19 fused with TNF-α, it led to complete tumor eradication in teratocarcinoma and colon carcinoma mouse models [98]. Similarly, complete remission was achieved in the treatment of B-cell lymphoma in a xenograft mouse model with L19-IL-2 in combination with rituximab (anti-CD20 monoclonal antibody, mAb) [96]. Additionally, Cazzamalli et al. reported interesting preclinical data showing that L19-IL-2, in combination with a small molecule-drug conjugate selectively targeting cancer cells expressing carbonic anhydrase IX, exhibited high specificity and efficacy [116].
Other interesting preclinical results involving L19-IL-2 demonstrated its cooperation with various chemotherapeutics, as well as its effectiveness when intratumorally injected in melanoma and sarcoma mouse models [99]. Building on these promising findings, a phase II clinical trial was initiated for advanced melanoma patients, testing a single injection of L19-IL-2 either alone or in combination with L19-TNF [117].
Concerning IL-2 immunocytokines combined with anti-angiogenic treatments, the critical role of the cell surface heparan sulfate proteoglycan syndecan-1 (SDC1, CD138) in neovascularization, vasculogenic mimicry (VM), and tumor progression is well established. Its ectodomain could be made soluble through the action of the ADAM17 enzyme, and it acts as a coreceptor for several angiogenic molecules (VEGF, FGF-2 and others) or it could be physically associated with VEGFR-2 [118,119]. In xenograft melanoma model, it has been demonstrated that the combination of L19-IL-2 with anti-SDC1 OC-46F2 mAb resulted in complete inhibition of melanoma growth for up to three months after tumor injection in 71% of the treated mice [96]. More recently, in an ovarian carcinoma model, it has been confirmed that SDC1 and tumor angiogenic B-FN isoform play pivotal roles in VM and that combined treatment using L19-IL2 and an anti-SDC1 46F2SIP antibody was effective in reducing the expression of EMT markers and loss of cancer stemness traits, which were correlated with the inhibition of VM in mice [119].
However, several research groups have made significant efforts to obtain compounds with modified IL-2 binding capacity, i.e. specifically by designing sequences that retain binding to the IL-2Rβ and IL-2Rγ (CD122 and CD132, respectively), while abolishing binding to IL-2Rα (CD25), with the goal of minimizing toxicity. Levin and colleagues developed an engineered IL-2, referred to as a “superkine”, which has an enhanced binding affinity for the IL-2βR [120], leading a superior induction of CTL with minimal activation of Treg cells. Similarly, Sun et al. constructed an IL-2 immunocytokine comprising a tumor-targeting antibody with a super mutant IL-2 (sumIL-2), which has enhanced binding to CD122 and weak binding to CD25 [121]. The sumIL-2 is incorporated in place of one Fab of an anti-EGFR mAb, resulting in the construct Erb-sumIL2. Importantly, the combination of PD-L1 ICI with sumIL-2 therapy has shown a synergistic effect in controlling advanced tumors.
Another different strategy was developed by the Doberstein team [122]. Indeed, it has been made an IL-2 with high binding affinity for CD122 and low binding affinity for CD25 conserving the same amino acid sequence of wild-type (WT) IL-2. This IL-2 has been conjugated to multiple releasable polyethylene glycol (PEG) chains (a total of six chains), which effectively rendered this new prodrug IL-2 an IL-2Rβ agonist. This design, named Bempegaldesleukin (or NKTR-214), leverages the molecular location of the PEG molecules to achieve selective stimulation of CD122, enhancing its therapeutic potential [122].
As of 2023, no IL-2 enhanced compounds had been approved for the treatment of cancer patients, with the exception of NKTR-214. NKTR-214 completed phase 3 studies but failed to meet its primary endpoints in both metastatic melanoma (PIVOT IO-001 trial) and advanced renal cell carcinoma (PIVOT-09) [111].
Klein and colleagues developed an IL-2 variant (IL-2v) immunocytokine that lacks IL-2Rα binding capacity. This IL-2v is fused with a mAb that is specific to CEA or FAP, and it contains an inert Fc domain that does not have the ability to activate FcγR-bearing cells [101,123]. The IL2v part is derived through structure-based mutation of key residues in the CD25 subunit of IL2R to prevent binding to IL-2Rα while preserving its affinity for IL-2R. Notably, both compounds used in combination therapy demonstrated superior activity compared to conventional IL-2-based immunocytokines. These engineered compounds were able to trigger and reinforce NK cell and CD8+ effector T cell activation via IL-2Rβγ both in the periphery and within the TME. Furthermore, they synergized with anti-PD-L1 ICI therapy, as well as with trastuzumab and cetuximab chemotherapies, enhancing the overall anti-tumor response [101,123].
The in vivo anti-cancer immune response of FAP-IL2v in various combination immunotherapies was investigated in both xenograft and syngeneic murine tumor models. FAP is low expressed or absent in healthy adult tissues but is highly expressed on cancer-associated fibroblasts and pericytes in the majority of human epithelial cancers.
When combined with different therapeutic antibodies able to trigger antibody dependent cellulare cytotoxicity (ADCC), such as the anti-EGFR antibody cetuximab, FAP-IL2v significantly extended the median survival compared to single-agent treatments of BALB-neuT genetically engineered mice that spontaneously developed breast tumors. Notably, mice that responded to this therapy showed increased tumor infiltration by CD3+ T cells, NK cells, and CD68+ macrophages, highlighting the enhanced immune response facilitated by the combination therapy [123].
5. Therapeutic Relevance of Enhancing Effector Cytolytic CD8+ T Cell Responses Induced by the Combination of Immunocytokine IL-2 with PD-1 Cis-Targeting
A key objective in cancer immunotherapy is the activation of non-exhausted, functional cytolytic CD8+ T effector responses, alongside the activation of NK effector cells. T cell exhaustion is often associated with the expression of markers such as PD-1, TIM-3, and CD39, which limit effective anti-tumor immunity [124,125,126,127]. A promising therapeutic strategy to overcome T cell exhaustion was demonstrated with the experiments reported by Klein’s group [128]. Indeed, it has been developed an IL-2v immunocytokine targeting PD-1 in cis (named PD1-IL-2v) and directed to the FAP tumor stroma antigen [128]. The IL-2v variant avoids binding to CD25, thus limiting Treg cell expansion and reducing the immunosuppressive effects commonly observed with WT IL-2 therapy. Importantly, this modification enhanced the functional activation of the stem-like CD8+ T cells (TCF1+ PD-1+), a subset critical for durable immune responses. This effect is mediated by strong STAT5 phosphorylation, which boosts the activation of these T cells.
Similarly, the murine PD-1-IL-2v (muPD-1-IL-2v) also induced more potent CD8+ T cell effectors in the C57/BL6 model in syngeneic pancreatic ductal adenocarcinoma model Panc02 [128]. This CD8+ T cell effector population can induce GM-CSF production, as well as higher concentration of granzyme B. It is notable that GM-CSF is a cytokine involved in dendritic cell activation and in potentiating T cell cytotoxic effector functions [129]. Interestingly, the highest therapeutic efficacy of muPD-1-IL-2v was further demonstrated in several in vivo mouse models, such as MCA205 tumor, B16-F10-OVA and RipTag5 pancreatic neuroendocrine tumors refractory to ICI [130]. Furthermore, Tichet et al. showed that muPD1-IL-2v was able to induce remarkable tumor regression and increased survival in combination with anti-PD-L1 [128]. Notably, this therapeutic combo generated and expanded polyfunctional effector memory CD8+ TILs with significantly higher levels of granzyme B, IFNγ, and TNFα compared to than CD8+ TILs isolated from mice treated with only muPD1-IL2v. This IL-2v immunocytokine entered clinical trials in 2020 as both a monotherapy and in combination with anti-PD-L1 antibodies. This approach appears to be the most promising for all those patients who have developed an endogenous T cell response to the tumor. Also, it is widely accepted that, to obtain high and superior therapeutic responses, in addition to stem-like CD8+ T cell-mediated responses, innate NK-type effectors and M1-type macrophages are also necessary. Indeed, the combination treatment with the anti-PD-L1 and muPD1-IL2v supported the immune response by reprogramming tumor-associated macrophages and increasing the diversity of the immune repertoire [128]. In particular, single cell RNA sequence analyses of myeloid cells showed that, in tumor-bearing mice treated with the aforementioned combination therapy, there was a reduction in the expression of M2-like immunosuppressive markers such as Trem2, Mrc1, and CD163, alongside an upregulation of pro-inflammatory markers such as Irf1, Slamf8, IFNγ, as well as the presence of T cell chemokines like as CXCL9 and CXCL10 [128]. Furthermore, in the orthotopic glioma model with the GL261 cells, it has been reported that the combination treatment can increase stem-like PD-1+TCF-1+CD8+ T cells, as well as their progeny, PD-1+TCF-1- and effector CD8+ T cells. In this model, CD8+ T cells isolated from mice treated with the combination were less suppressive than those isolated from mice treated with the either of the two drugs alone. Again, a shift from M2 to M1 macrophages was detected. These findings suggested that, in several different mouse models, the combination of ICI and IL-2 variants can contribute concur to an optimal anti-tumor immune response [128]. Besides the effects described, it is worth to note that the combination treatment can affect the phenotype of endothelial cells present within the tumor. Indeed, these endothelial cells can directly regulate the infiltration, proliferation, and cytotoxicity of CD8+ T cells in an antigen specific manner [131,132].
6. Role of Radiotherapy in the Triggering Anti-Tumor Therapeutic Responses in Combined Tumor-Targeted IL-2 Treatments
Recent research has shown a growing interest in investigating the synergistic effects of combining radiotherapy (RT) with tumor-targeted IL-2 treatments to eradicate tumors. Indeed, the relationship between RT and the modulation of the immune system response have revealed novel regulatory pathways [133,134]. These include the concept of radiation-induced tumor equilibrium (RITE), which serves as a starting point to discuss the mechanistic influence of immune-checkpoint therapies on the efficacy of RT [133,134].
Traditionally viewed as a local therapy, RT directly damages DNA in tumor cells [135]. RT usually induces the release of danger signals and consequently chemokines that recruit inflammatory cells into the TME, including antigen-presenting cells that activate cytotoxic T-cell function. However, RT also has the capability to attract immunosuppressive cells into the TME [136]. Consequently, it has been shown that RT exhibits both immunostimulatory and immunosuppressive properties, owing to the inherent sensitivity of immune cells to its effects [137,138].
Concerning immunostimulatory effects, localized RT can provoke systemic immune responses [139] by inducing the expression of tumor-associated antigens and generating new tumor antigens that can activate antitumor immune responses. This helps counter the tumor's suppression of antigen presentation. For example, the expression of MHC-I, a critical antigen recognized by CD8+ antigen specific T cells, is often decreased on tumor cells [140]. RT can effectively increase MHC-I expression, facilitate dendritic cell maturation and leukocyte infiltration of tumors [141], reduce the presence of Treg cells within tumors, expand T-cell populations, and enhance T cell migration. Moreover, RT has demonstrated the capability to convert non-immunogenic tumors into immunogenic ones, either partially or completely [142]. Previous studies using IL-2 immnocytokine, such as L19-IL-2, have shown that it can synergize with RT to achieve tumor rejection and immune-mediated protection effect in a colon carcinoma mouse model [143,144,145]. Additionally, RT can manage local tumor progression when combined with anti-PD1/PDL1 or anti-CTLA4 ICI, immunocytokines, dendritic cell vaccines, and Toll-like receptor antagonists. These therapeutic combinations improve the overall survival (OS) and elicits specific immune responses against cancer [146]. Some recent preclinical and clinical research has demonstrated that the combination of RT’s immunosuppressive and immunostimulatory properties can lead to abscopal effects [147] and potentially a "radio-memory" effect, wherein the synergistic action of combo treatments produces enhanced outcomes [148].
Investigating whether the "radio-memory" effect [149] extends beyond anti-PD1/PDL1 ICI to other forms of immune therapy, such as IL-2, is a critical step in understanding the broader implications of RT-induced immune responses in cancer treatment. For instance, in patients with malignant pleural effusion who had previously received RT for non-small-cell lung cancer within 18 months, intrapleural infusion of IL-2 or cisplatin demonstrated potential evidence of a radio-memory effect [149].
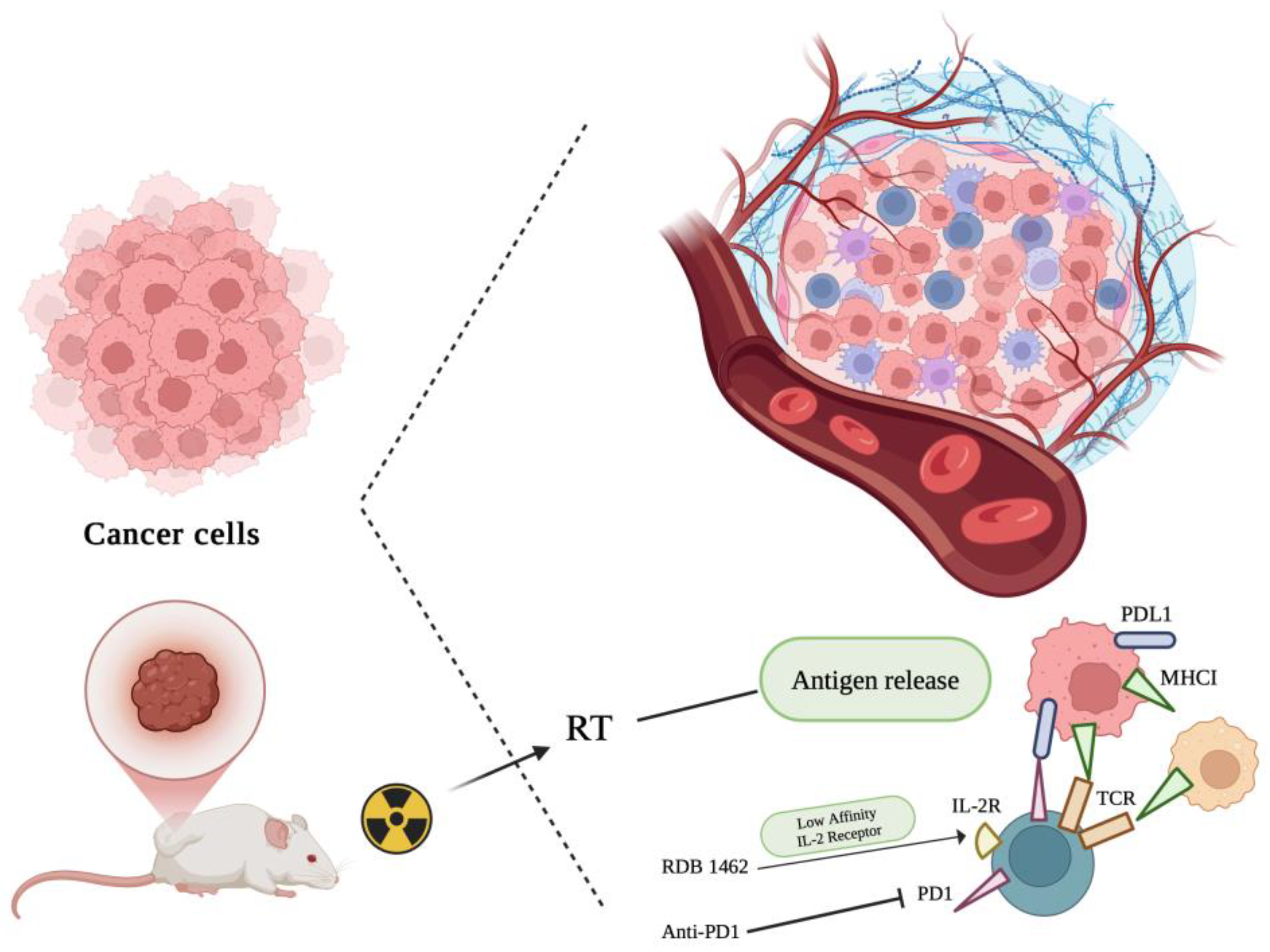
More recently, other studies have examined the critical role of IL-2 in synergistic immunotherapeutic strategies involving RT. In particular, a modified IL-2-based treatment has shown promising results when combined with RT to amplify immune responses. Gadwa and colleagues demonstrated that combining RT with PD1-IL2v, an IL-2 variant targeting intermediate-affinity IL-2 receptors (IL-2Rβγ), significantly enhanced immune activation; The lymphocytes involved are mainly CD8+ T cells and NK cells, while a concomitant reduction of the suppressive function of Treg cells was detected [150]. This combination showed effective tumor control and reduced metastasis, leveraging the immune system's response to control distant tumors via an "abscopal effect". In a parallel investigation, He et al. focused on an engineered IL-2 variant, RDB 1462, which binds selectively to IL-2Rβγ, promoting antitumor activity while minimizing the induction of Tregs [151]. Their findings revealed that combining high-dose RT with RDB 1462 significantly improved survival and suppressed primary and metastatic tumor growth in mouse models. Moreover, this combination therapy enhanced CD8+ memory T cells and NK cell activation, while diminishing Treg and MDSCs. The precise timing of IL-2 administration before RT was crucial in maximizing therapeutic efficacy and immune response [151]. These findings demonstrate that IL-2, particularly in its engineered forms, holds substantial promise when paired with RT to enhance anti-tumor immunity. By targeting specific IL-2 receptor subunits, these treatments can potentially overcome immune suppression within the TME and improve the therapeutic outcomes of RT and other immunotherapies. Further clinical investigations are warranted to optimize this approach for broader cancer treatment strategies (Figure 2).
7. Conclusions
The integration of IL-2 immunocytokines into cancer therapy marks a promising breakthrough, overcoming the challenges associated with traditional IL-2 treatment. While high-dose IL-2 has shown efficacy in specific cancers, the severe toxicities have limited a broader use. The targeted delivery of IL-2 through immunotoxin and immunocytokines, in combination with checkpoint inhibitors, chemotherapy, radiotherapy, and anti-angiogenic agents, has significantly enhanced anti-tumor responses while reducing toxicity. These strategies capitalize on the dual activation of innate and adaptive immune responses, effectively counteracting immune suppression and improving tumor clearance.
Innovations such as antibody fusion proteins, modified IL-2 variants, and bi-specific formats further optimize the targeting of the TME, improving therapeutic efficacy without inducing significant side effects. The use of PD-1-targeting IL-2 immunocytokines, in particular, has demonstrated the ability to rejuvenate exhausted T cells and enhance immune infiltration within tumors, offering substantial promise in both primary and metastatic cancer settings. Moreover, advances in cytokine engineering, including glyco-engineering and prodrug formulations, have enhanced the selectivity and cost-effectiveness of these therapies, ensuring their viability in diverse clinical contexts.
Looking ahead, continued research into IL-2 immunocytokines holds great potential for developing therapies that not only target primary tumors but also overcome metastasis and therapy resistance. As these treatments evolve, the ability to precisely modulate immune responses on demand could redefine cancer therapy, offering durable responses and improved survival outcomes for patients worldwide. Further exploration in clinical settings is crucial to unlock the full potential of IL-2 immunocytokines, ensuring their effective translation from preclinical models to routine clinical use.
Funding
This research was funded by FAR2022 and FAR2023 to L.M. from University of Insubria, Varese, Italy. L.M. and G.B. are funded by the Ministry of Health—Ricerca Corrente to IRCCS MultiMedica, Milan, Italy. G.B. is part of the PhD course in Experimental and Translational Medicine at the University of Insubria, Varese, Italy.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Sinicrope, FA. : Turk MJ. Immune checkpoint blockade: timing is everything. J Immunother Cancer. 2024 Aug 28;12(8):e009722. [CrossRef] [PubMed]
- Boutros C, Herrscher H, Robert C. Progress in Immune Checkpoint Inhibitor for Melanoma Therapy. Hematol Oncol Clin North Am. 2024 Oct;38(5):997-1010. [CrossRef] [PubMed]
- Hossain SM, Carpenter C, Eccles MR. Genomic and Epigenomic Biomarkers of Immune Checkpoint Immunotherapy Response in Melanoma: Current and Future Perspectives. Int J Mol Sci. 2024 Jun 30;25(13):7252. [CrossRef] [PubMed]
- Benhima N, Belbaraka R, Langouo Fontsa MD. Single agent vs combination immunotherapy in advanced melanoma: a review of the evidence. Curr Opin Oncol. 2024 Mar 1;36(2):69-73. [CrossRef] [PubMed]
- Tyagi S, Kumar A. Safety of immune checkpoint inhibitors: An updated comprehensive disproportionality analysis and meta-analysis. Crit Rev Oncol Hematol. 2024 Aug;200:104398. [CrossRef] [PubMed]
- Yamada K, Takeuchi M, Fukumoto T, Suzuki M, Kato A, Mizuki Y, Yamada N, Kaneko T, Mizuki N, Horita N. Immune checkpoint inhibitors for metastatic uveal melanoma: a meta-analysis. Sci Rep. 2024 Apr 3;14(1):7887. [CrossRef] [PubMed]
- Tian J, Quek C. Understanding the Tumor Microenvironment in Melanoma Patients with In-Transit Metastases and Its Impacts on Immune Checkpoint Immunotherapy Responses. Int J Mol Sci. 2024 Apr 11;25(8):4243. [CrossRef] [PubMed]
- Ghoreifi A, Vaishampayan U, Yin M, Psutka SP, Djaladat H. Immune Checkpoint Inhibitor Therapy Before Nephrectomy for Locally Advanced and Metastatic Renal Cell Carcinoma: A Review. JAMA Oncol. 2024 Feb 1;10(2):240-248. [CrossRef] [PubMed]
- Yanagisawa T, Mori K, Matsukawa A, Kawada T, Katayama S, Bekku K, Laukhtina E, Rajwa P, Quhal F, Pradere B, Fukuokaya W, Iwatani K, Murakami M, Bensalah K, Grünwald V, Schmidinger M, Shariat SF, Kimura T. Updated systematic review and network meta-analysis of first-line treatments for metastatic renal cell carcinoma with extended follow-up data. Cancer Immunol Immunother. 2024 Jan 30;73(2):38. [CrossRef] [PubMed]
- Blas L, Monji K, Mutaguchi J, Kobayashi S, Goto S, Matsumoto T, Shiota M, Inokuchi J, Eto M. Current status and future perspective of immunotherapy for renal cell carcinoma. Int J Clin Oncol. 2024 Aug;29(8):1105-1114. [CrossRef] [PubMed]
- Langouo Fontsa M, Padonou F, Willard-Gallo K. Biomarkers and immunotherapy: where are we? Curr Opin Oncol. 2022 Sep 1;34(5):579-586. [CrossRef] [PubMed]
- De Luca AJ, Lyons AB, Flies AS. Cytokines: Signalling Improved Immunotherapy? Curr Oncol Rep. 2021 Jul 16;23(9):103. [CrossRef] [PubMed]
- Tokaz MC, Baik CS, Houghton AM, Tseng D. New Immuno-oncology Targets and Resistance Mechanisms. Curr Treat Options Oncol. 2022 Sep;23(9):1201-1218. [CrossRef] [PubMed]
- D'Amico S, Tempora P, Melaiu O, Lucarini V, Cifaldi L, Locatelli F, Fruci D. Targeting the antigen processing and presentation pathway to overcome resistance to immune checkpoint therapy. Front Immunol. 2022 Jul 22;13:948297. [CrossRef] [PubMed]
- Khosravi GR, Mostafavi S, Bastan S, Ebrahimi N, Gharibvand RS, Eskandari N. Immunologic tumor microenvironment modulators for turning cold tumors hot. Cancer Commun (Lond). 2024 May;44(5):521-553. [CrossRef] [PubMed]
- Jin Y, Huang Y, Ren H, Huang H, Lai C, Wang W, Tong Z, Zhang H, Wu W, Liu C, Bao X, Fang W, Li H, Zhao P, Dai X. Nano-enhanced immunotherapy: Targeting the immunosuppressive tumor microenvironment. Biomaterials. 2024 Mar;305:122463. [CrossRef] [PubMed]
- Poggi A, Varesano S, Zocchi MR. How to Hit Mesenchymal Stromal Cells and Make the Tumor Microenvironment Immunostimulant Rather Than Immunosuppressive. Front Immunol. 2018 Feb 19;9:262. Erratum in: Front Immunol. 2018 Jun 11;9:1342. [CrossRef] [PubMed]
- Poggi A, Musso A, Dapino I, Zocchi MR. Mechanisms of tumor escape from immune system: role of mesenchymal stromal cells. Immunol Lett. 2014 May-Jun;159(1-2):55-72. [CrossRef] [PubMed]
- Chhabra Y, Weeraratna AT. Fibroblasts in cancer: Unity in heterogeneity. Cell. 2023 Apr 13;186(8):1580-1609. [CrossRef] [PubMed]
- Zhang F, Ma Y, Li D, Wei J, Chen K, Zhang E, Liu G, Chu X, Liu X, Liu W, Tian X, Yang Y. Cancer associated fibroblasts and metabolic reprogramming: unraveling the intricate crosstalk in tumor evolution. J Hematol Oncol. 2024 Sep 2;17(1):80. [CrossRef] [PubMed]
- Hanahan, D.; Weinberg, R.A. Hallmarks of cancer: the next generation. Cell. 2011 Mar 4;144(5):646-74.
- Hanahan, D.; Weinberg, R.A. The hallmarks of cancer. Cell. 2000 Jan 7;100(1):57-70.
- Molgora, M.; Bonavita, E.; Ponzetta, A.; Riva, F.; Barbagallo, M.; Jaillon, S.; Popović, B.; Bernardini, G.; Magrini, E.; Gianni, F.; Zelenay, S.; Jonjić, S.; Santoni, A.; Garlanda, C.; Mantovani, A. IL-1R8 is a checkpoint in NK cells regulating anti-tumour and anti-viral activity. Nature. 2017 Nov 2;551(7678):110-114. [CrossRef]
- Mattiola, I.; Tomay, F.; De Pizzol, M.; Gomes, R.S.; Savino, B.; Gulic, T.; Doni, A.; Lonardi, S.; Boutet, M.A.; Nerviani, A.; Carriero, R.; Molgora, M.; Stravalaci, M.; Morone, D.; Shalova, I.N.; Lee, Y.; Biswas, S.K.; Mantovani, G.; Sironi, M.; Pitzalis, C.; Vermi, W.; Bottazzi, B.; Mantovani, A.; Locati, M. The interplay of the macrophage tetraspan MS4A4A with Dectin-1 and its role in NK cell-mediated resistance to metastasis. Nat Immunol. 2019 Aug;20(8):1012-1022. [CrossRef]
- Locati, M.; Curtale, G.; Mantovani, A. Diversity, Mechanisms, and Significance of Macrophage Plasticity. nnu Rev Pathol. 2020 Jan 24:15:123-147. [CrossRef]
- Albini, A.; Bruno, A.; Noonan, D.N.; Mortara, L. Contribution to Tumor Angiogenesis From Innate Immune Cells Within the Tumor Microenvironment: Implications for Immunotherapy. Front Immunol. 2018 Apr 5:9:527. [CrossRef]
- Bassani, B.; Baci, D.; Gallazzi, M.; Poggi, A.; Bruno, A.; Mortara, L. Natural Killer Cells as Key Players of Tumor Progression and Angiogenesis: Old and Novel Tools to Divert Their Pro-Tumor Activities into Potent Anti-Tumor Effects. Cancers (Basel). 2019 Apr 1;11(4):461. [CrossRef]
- Bruno, A.; Mortara, L.; Baci, B.; Noonan, D.M.; Albini, A. Myeloid Derived Suppressor Cells Interactions With Natural Killer Cells and Pro-angiogenic Activities: Roles in Tumor Progression. Front Immunol. 2019 Apr 18;10:771. [CrossRef]
- Hanahan, D. Hallmarks of Cancer: New Dimensions. Cancer Discov. 2022 Jan;12(1):31-46. [CrossRef]
- Song, K. Current Development Status of Cytokines for Cancer Immunotherapy. Biomol Ther (Seoul). 2024 Jan 1; 32(1): 13–24. [CrossRef]
- Fu, F.; Tang, R. , Zhao X. Engineering cytokines for cancer immunotherapy: a systematic review. Front Immunol. 2023 Jul 6:14:1218082. [CrossRef]
- Malek, T.R. The biology of interleukin-2. Annu Rev Immunol. 2008;26:453-79. [CrossRef]
- Radi, H.; Ferdosi-Shahandashti, E.; Kardar, G.A.; Hafezi, N. An Updated Review of Interleukin-2 Therapy in Cancer and Autoimmune Diseases. J Interferon Cytokine Res. 2024 Apr;44(4):143-157. [CrossRef]
- Shouse, A.N.; LaPorte, K.M.; Malek, T.R. Interleukin-2 signaling in the regulation of T cell biology in autoimmunity and cancer. Immunity. 2024 Mar 12;57(3):414-428. [CrossRef]
- Waldmann, T.; Tagaya, Y.; Bamford, R. Interleukin-2, interleukin-15, and their receptors. Int Rev Immunol. 1998;16(3-4):205-26. [CrossRef]
- Waldmann, T.A. The biology of interleukin-2 and interleukin-15: implications for cancer therapy and vaccine design. Nat Rev Immunol. 2006 Aug;6(8):595-601. [CrossRef]
- Waldmann, T.A. The interleukin-2 receptor. J Biol Chem. 1991 Feb 15;266(5):2681-4.
- Lokau, J.; Petasch, L.M.; Garbers, C. The soluble IL-2 receptor α/CD25 as a modulator of IL-2 function. Immunology. 2024 Mar;171(3):377-387. [CrossRef]
- Malek, T.R.; Castro, I. Interleukin-2 receptor signaling: at the interface between tolerance and immunity. Immunity. 2010 Aug 27;33(2):153-65. [CrossRef]
- Liao, W.; Lin, J.X.; Leonard, W.J. Interleukin-2 at the crossroads of effector responses, tolerance, and immunotherapy. Immunity. 2013 Jan 24;38(1):13-25. [CrossRef]
- Raeber, M.E.; Sahin, D.; Boyman, O. Interleukin-2-based therapies in cancer. Sci Transl Med. 2022 Nov 9;14(670):eabo5409. [CrossRef]
- Rokade, S.; Damani, A.M.; Oft, M.; Emmerich, J. IL-2 based cancer immunotherapies: an evolving paradigm. Front Immunol. 2024 Jul 24;15:1433989. [CrossRef]
- Oppenheim, M.H.; Lotze, M.T. Interleukin-2: solid-tumor therapy. Oncology. 1994 Mar-Apr;51(2):154-69. [CrossRef]
- Hashimoto, M.; Ramalingam, S.S.; Ahmed, R. Harnessing CD8 T cell responses using PD-1-IL-2 combination therapy. Trends Cancer. 2024 Apr;10(4):332-346. [CrossRef]
- Krieg, C.; Létourneau, S.; Pantaleo, G.; Boyman, O. Improved IL-2 immunotherapy by selective stimulation of IL-2 receptors on lymphocytes and endothelial cells. Proc Natl Acad Sci U S A. 2010 Jun 29;107(26):11906-11. Epub 2010 Jun 14. Erratum in: Proc Natl Acad Sci U S A. 2012 Jan 3;109(1):345. [CrossRef]
- Puri, R.K.; Rosenberg, S.A. Combined effects of interferon alpha and interleukin 2 on the induction of a vascular leak syndrome in mice. Cancer Immunol Immunother. 1989;28(4):267-74. [CrossRef]
- Edwards, M.J.; Miller, F.N.; Sims, D.E.; Abney, D.L.; Schuschke, D.A.; Corey, T.S. Interleukin 2 acutely induces platelet and neutrophil-endothelial adherence and macromolecular leakage. Cancer Res. 1992 Jun 15;52(12):3425-31.
- Siddall, E.; Khatri, M.; Radhakrishnan, J. Capillary leak syndrome: etiologies, pathophysiology, and management. Kidney Int. 2017 Jul;92(1):37-46. [CrossRef]
- Kang, S.; Kishimoto, T. Interplay between interleukin-6 signaling and the vascular endothelium in cytokine storms. Exp Mol Med. 2021 Jul;53(7):1116-1123. [CrossRef]
- van Hinsbergh, V.W.; van Nieuw Amerongen, G.P. Endothelial hyperpermeability in vascular leakage. Vascul Pharmacol. 2002 Nov;39(4-5):171-2. [CrossRef]
- Park, S.; Lee, S.; Kim, D.; Kim, H.; Kwon, Y.G. CU06-1004 as a promising strategy to improve anti-cancer drug efficacy by preventing vascular leaky syndrome. Front Pharmacol. 2023 Aug 30;14:1242970. [CrossRef]
- Den Otter, W.; Jacobs, J.J.; Battermann, J.J.; Hordijk, G.J.; Krastev, Z.; Moiseeva, E.V.; Stewart, R.J.; Ziekman, P.G.; Koten, J.W. Local therapy of cancer with free IL-2. Cancer Immunol Immunother. 2008 Jul;57(7):931-50. [CrossRef]
- Jackaman, C.; Bundell, C.S.; Kinnear, B.F.; Smith, A.M.; Filion, P.; van Hagen, D.; Robinson, B.W.; Nelson, D.J. IL-2 intratumoral immunotherapy enhances CD8+ T cells that mediate destruction of tumor cells and tumor-associated vasculature: a novel mechanism for IL-2. J Immunol. 2003 Nov 15;171(10):5051-63. [CrossRef]
- Jacobs, J.J.; Sparendam, D.; Den Otter, W. Local interleukin 2 therapy is most effective against cancer when injected intratumourally. Cancer Immunol Immunother. 2005 Jul;54(7):647-54. [CrossRef]
- Spolski, R.; Li, P.; Leonard, W.J. Biology and regulation of IL-2: from molecular mechanisms to human therapy. Nat Rev Immunol. 2018 Oct;18(10):648-659. [CrossRef]
- Wang, F.; Wang, S.; He, B.; Liu, H.; Wang, X.; Li, C.; Peng, P.; Zhao, J.; Zang, Y. Immunotherapeutic strategy based on anti-OX40L and low dose of IL-2 to prolong graft survival in sensitized mice by inducing the generation of CD4+ and CD8+ Tregs. Int Immunopharmacol. 2021 Aug;97:107663. [CrossRef]
- Marchetti, G.; Meroni, L.; Molteni, C.; Bandera, A.; Franzetti, F.; Galli, M.; Moroni, M.; Clerici, M.; Gori, A. Interleukin-2 immunotherapy exerts a differential effect on CD4 and CD8 T cell dynamics. AIDS. 2004 Jan 23;18(2):211-6. [CrossRef]
- Sockolosky, J.T.; Trotta, E.; Parisi, G.; Picton, L.; Su, L.L.; Le, A.C.; Chhabra, A.; Silveria, S.L.; George, B.M.; King, I.C.; Tiffany, M.R. , Jude K.; Sibener L.V.; Baker D.; Shizuru J.A.; Ribas A.; Bluestone J.A.; Garcia K.C. Selective targeting of engineered T cells using orthogonal IL-2 cytokine-receptor complexes. Science. 2018 Mar 2;359(6379):1037-1042. [CrossRef]
- Horton, B.L.; D'Souza, A.D.; Zagorulya, M.; McCreery, C.V.; Abhiraman, G.C.; Picton, L.; Sheen, A.; Agarwal, Y.; Momin, N.; Wittrup, K.D.; White, F.M.; Garcia, K.C.; Spranger, S. Overcoming lung cancer immunotherapy resistance by combining nontoxic variants of IL-12 and IL-2. JCI Insight. 2023 Oct 9;8(19):e172728. [CrossRef]
- Bentebibel, S.E.; Diab, A. Cytokines in the Treatment of Melanoma. Curr Oncol Rep. 2021 ;23(7):83. 18 May. [CrossRef]
- Rojas, G.; Relova-Hernández, E.; Pérez-Riverón, A.; Castro-Martínez, C.; Diaz-Bravo, O.; Infante, Y.C.; Gómez, T.; Solozábal, J.; DíazBravo, A.B.; Schubert, M.; Becker, M.; Pérez-Massón, B.; Pérez-Martínez, D.; Alvarez-Arzola, R.; Guirola, O.; Chinea, G.; Graca, L.; Dübel, S.; León, K.; Carmenate, T. Molecular reshaping of phage-displayed Interleukin-2 at beta chain receptor interface to obtain potent super-agonists with improved developability profiles. Commun Biol. 2023 Aug 9;6(1):828. [CrossRef]
- Ren, Z.; Zhang, X.; Fu, Y.X. Facts and Hopes on Chimeric Cytokine Agents for Cancer Immunotherapy. Clin Cancer Res. 2024 May 15;30(10):2025-2038) Indeed, the generation of several.
- Baars, J.W.; de Boer, J.P.; Wagstaff, J.; Roem, D.; Eerenberg-Belmer, A.J.; Nauta, J.; Pinedo, H.M.; Hack, C.E. Interleukin-2 induces activation of coagulation and fibrinolysis: resemblance to the changes seen during experimental endotoxaemia. Br J Haematol. 1992 Oct;82(2):295-301. [CrossRef]
- Miller, J.D.; Clabaugh, S.E.; Smith, D.R.; Stevens, R.B.; Wrenshall, L.E. Interleukin-2 is present in human blood vessels and released in biologically active form by heparanase. Immunol Cell Biol. 2012 Feb;90(2):159-67. [CrossRef]
- Locker, G.J.; Kapiotis, S.; Veitl, M.; Mader, R.M.; Stoiser, B.; Kofler, J.; Sieder, A.E.; Rainer, H.; Steger, G.G.; Mannhalter, C.; Wagner, O.F. Activation of endothelium by immunotherapy with interleukin-2 in patients with malignant disorders. Br J Haematol. 1999 Jun;105(4):912-9. [CrossRef]
- Baars, J.W.; Hack, C.E.; Wagstaff, J.; Eerenberg-Belmer, A.J.; Wolbink, G.J.; Thijs, L.G.; Strack van Schijndel, R.J.; van der Vall, H.L.; Pinedo, H.M. The activation of polymorphonuclear neutrophils and the complement system during immunotherapy with recombinant interleukin-2. Br J Cancer. 1992 Jan;65(1):96-101. [CrossRef]
- Davis, C.B.; Gillies, S.D. Immunocytokines: amplification of anti-cancer immunity. Cancer Immunol Immunother. 2003 May;52(5):297-308. [CrossRef]
- Sondel, P.M.; Hank, J.A.; Gan, J.; Neal, Z.; Albertini, M.R. Preclinical and clinical development of immunocytokines. Curr Opin Investig Drugs. 2003 Jun;4(6):696-700.
- Beig Parikhani, A.; Dehghan, R.; Talebkhan, Y.; Bayat, E.; Biglari, A.; Shokrgozar, M.A.; Ahangari Cohan, R.; Mirabzadeh, E.; Ajdary, S.; Behdani, M. A novel nanobody-based immunocytokine of a mutant interleukin-2 as a potential cancer therapeutic. AMB Express. 2024 Feb 9;14(1):19. [CrossRef]
- Yen, M.; Ren, J.; Liu, Q.; Glassman, C.R.; Sheahan, T.P.; Picton, L.K.; Moreira, F.R.; Rustagi, A.; Jude, K.M.; Zhao, X.; Blish, C.A.; Baric, R.S.; Su, L.L.; Garcia, K.C. Facile discovery of surrogate cytokine agonists. Cell. 2022 Apr 14;185(8):1414-1430.e19. [CrossRef]
- Ren, B.; McKinstry, W.J.; Pham, T.; Newman, J.; Layton, D.S.; Bean, A.G.; Chen, Z.; Laurie, K.L.; Borg, K.; Barr, I.G.; Adams, T.E. Structural and functional characterisation of ferret interleukin-2. Dev Comp Immunol. 2016 Feb;55:32-8. [CrossRef]
- Boersma, B.; Poinot, H.; Pommier, A. Stimulating the Antitumor Immune Response Using Immunocytokines: A Preclinical and Clinical Overview. Pharmaceutics. 2024 Jul 24;16(8):974. [CrossRef]
- Prodi, E.; Neri, D.; De Luca, R. Tumor-Homing Antibody-Cytokine Fusions for Cancer Therapy. Onco Targets Ther. 2024 Aug 29;17:697-715. [CrossRef]
- Fabilane, C.S.; Stephenson, A.C.; Leonard, E.K.; VanDyke, D.; Spangler, J.B. Cytokine/Antibody Fusion Protein Design and Evaluation. Curr Protoc. 2024 May;4(5):e1061. [CrossRef]
- Santollani, L.; Zhang, Y.J.; Maiorino, L.; Palmeri, J.R.; Stinson, J.A.; Duhamel, L.R.; Qureshi, K.; Suggs, J.R.; Porth, O.T.; Pinney, W. 3rd.; Sari R.A.; Wittrup K.D.; Irvine D.J. Local delivery of cell surface-targeted immunocytokines programs systemic anti-tumor immunity. Nat Immunol. 2024 Oct;25(10):1820-1829. [CrossRef]
- Drago, J.Z.; Modi, S.; Chandarlapaty, S. Unlocking the potential of antibody-drug conjugates for cancer therapy. Nat Rev Clin Oncol. 2021 Jun;18(6):327-344. [CrossRef]
- Dumontet, C.; Reichert, J.M.; Senter, P.D.; Lambert, J.M.; Beck, A. Antibody-drug conjugates come of age in oncology. Nat Rev Drug Discov. 2023 Aug;22(8):641-661. [CrossRef]
- Phuna, Z.X.; Kumar, P.A.; Haroun, E.; Dutta, D.; Lim, S.H. Antibody-drug conjugates: Principles and opportunities. Life Sci. 2024 Jun 15;347:122676. [CrossRef]
- Tsuchikama, K.; Anami, Y.; Ha, S.Y.Y.; Yamazaki, C.M. Exploring the next generation of antibody-drug conjugates. Nat Rev Clin Oncol. 2024 Mar;21(3):203-223. [CrossRef]
- Tarantino, P.; Carmagnani Pestana, R.; Corti, C.; Modi, S.; Bardia, A.; Tolaney, S.M.; Cortes, J.; Soria, J.C.; Curigliano, G. Antibody-drug conjugates: Smart chemotherapy delivery across tumor histologies. CA Cancer J Clin. 2022 Mar;72(2):165-182. [CrossRef]
- Merle, G.; Friedlaender, A.; Desai, A.; Addeo, A. Antibody Drug Conjugates in Lung Cancer. Cancer J. 2022 Nov-Dec 01;28(6):429-435. [CrossRef]
- Xiao, T.; Ali, S.; Mata, D.G.M.M.; Lohmann, A.E.; Blanchette, P.S. Antibody-Drug Conjugates in Breast Cancer: Ascent to Destiny and Beyond-A 2023 Review. Curr Oncol. 2023 Jul 6;30(7):6447-6461. [CrossRef]
- Wittwer, N.L.; Brown, M.P.; Liapis, V.; Staudacher, A.H. Antibody drug conjugates: hitting the mark in pancreatic cancer? J Exp Clin Cancer Res. 2023 Oct 25;42(1):280. [CrossRef]
- Baah, S.; Laws, M.; Rahman, K.M. Antibody-Drug Conjugates-A Tutorial Review. Molecules. 2021 ;26(10):2943. 15 May. [CrossRef]
- Ruan, D.Y.; Wu, H.X.; Meng, Q.; Xu, R.H. Development of antibody-drug conjugates in cancer: Overview and prospects. Cancer Commun (Lond). 2024 Jan;44(1):3-22. [CrossRef]
- Tarantino, P.; Ricciuti, B.; Pradhan, S.M.; Tolaney, S.M. Optimizing the safety of antibody-drug conjugates for patients with solid tumours. Nat Rev Clin Oncol. 2023 Aug;20(8):558-576. [CrossRef]
- Nicolò, E.; Repetto, M.; Boscolo Bielo, L.; Tarantino, P.; Curigliano, G. Antibody-Drug Conjugates in Breast Cancer: What Is Beyond HER2? Cancer J. 2022 Nov-Dec 01;28(6):436-445. [CrossRef]
- Wang, H.; Wang, Z.; Zhang, H.; Qi, Z.; Johnson, A.C.; Mathes, D. ; Pomfret.;.A, Rubin E.; Huang C.A.; Wang Z. Bispecific human IL2-CCR4 immunotoxin targets human cutaneous T-cell lymphoma. Mol Oncol. 2020 May;14(5):991-1000. [CrossRef]
- Wang, Z.; Ma, J.; Zhang, H.; Ramakrishna, R.; Mintzlaff, D.; Mathes, D.W.; Pomfret, E.A.; Lucia, M.S.; Gao, D.; Haverkos, B.M.; Wang, Z. CCR4-IL2 bispecific immunotoxin is more effective than brentuximab for targeted therapy of cutaneous T-cell lymphoma in a mouse CTCL model. FEBS Open Bio. 2023 Jul;13(7):1309-1319. [CrossRef]
- Wang Z, Ramakrishna R, Wang Y, Qiu Y, Ma J, Mintzlaff D, Zhang H, Li B, Hammell B, Lucia MS, Pomfret E, Su AA, Washington KM, Mathes DW, Wang Z. Toxicology, pharmacokinetics, and immunogenicity studies of CCR4-IL2 bispecific immunotoxin in rats and minipigs. Eur J Pharmacol. 2024 Apr 5;968:176408. [CrossRef] [PubMed]
- Morse, M.A.; Hobeika, A.C.; Osada, T.; Serra, D.; Niedzwiecki, D.; Lyerly, H.K.; Clay, T.M. Depletion of human regulatory T cells specifically enhances antigen-specific immune responses to cancer vaccines. Blood. 2008; 112:610–618.
- Litzinger, M.T.; Fernando, R.; Curiel, T.J.; Grosenbach, D.W.; Schlom, J.; Palena, C. IL-2 immunotoxin denileukin diftitox reduces regulatory T cells and enhances vaccine-mediated T-cell immunity. Blood. 2007; 110:3192–3201.
- Yamada, Y.; Aoyama, A.; Tocco, G.; Boskovic, S.; Nadazdin, O.; Alessandrini, A.; Madsen, J.C.; Cosimi, A.B.; Benichou, G.; Kawai, T. Differential effects of denileukin diftitox IL-2 immunotoxin on NK and regulatory T cells in nonhuman primates. J Immunol. 2012 Jun 15;188(12):6063-70.
- Carnemolla, B.; Borsi, L.; Balza, E.; Castellani, P.; Meazza, R. ; Berndt A, Ferrini S.; KosmehL H.; Neri, D.; Zardi L. Enhancement of the antitumor properties of interleukin-2 by its targeted delivery to the tumor blood vessel extracellular matrix. Blood (2002) 99:1659-65. [CrossRef]
- Wagner, K.; Schulz, P.; Scholz, A.; Wiedenmann, B.; Menrad, A. The targeted immunocytokine L19-IL2 efficiently inhibits the growth of orthotopic pancreatic cancer. Clin Cancer Res. (2008) 14:4951–60. [CrossRef]
- Schliemann, C.; Palumbo, A.; Zuberbuhler, K.; Villa, A.; Kaspar, M.; Trachsel, E.; Klapper, W.; Menssen, H.D.; Neri, N. Complete eradication of human B-cell lymphoma xenografts using rituximab in combination with the immunocytokine L19-IL2. Blood (2009) 113:2275–83. [CrossRef]
- Balza, E.; Carnemolla, B.; Mortara, L.; Castellani, P.; Soncini, D.; Accolla, R.S.; Borsi, L. Therapy-induced antitumor vaccination in neuroblastomas by the combined targeting of IL-2 and TNFalpha. Int J Cancer (2010) 127:101–10. [CrossRef]
- Schwager, K.; Hemmerle, T.; Aebischer, D.; Neri, D. The immunocytokine L19-IL2 eradicates cancer when used in combination with CTLA-4 blockade or with L19-TNF. J Invest Dermatol. (2013) 133:751–8. [CrossRef]
- Pretto, F.; Elia, G.; Castioni, N.; Neri, D. Preclinical evaluation of IL2-based immunocytokines supports their use in combination with dacarbazine, paclitaxel and TNF-based immunotherapy. Cancer Immunol Immunother. (2014) 63:901–10. [CrossRef]
- Orecchia, P.; Conte, R.; Balza, E.; Pietra, G.; Mingari, M.C.; Carnemolla, B. Targeting Syndecan-1, a molecule implicated in the process of vasculogenic mimicry, enhances the therapeutic efficacy of the L19-IL2 immunocytokine in human melanoma xenografts. Oncotarget (2015) 6:37426–42. [CrossRef]
- Klein, C.; Waldhauer, I.; Nicolini, V.G.; Freimoser-Grundschober, A.; Nayak, T.; Vugts, D.J.; Dunn, C.; Bolijn, M.; Benz, J.; Stihle, M.; Lang, S.; Roemmele, M.; Hofer, T.; van Puijenbroek, E.; Wittig, D.; Moser, S.; Ast, O.; Brünker, P.; Gorr, I.H.; Neumann, S.; de Vera Mudry, M.C. , Hinton H.; Crameri F.; Saro J.; Evers S.; Gerdes C.; Bacac M.; van Dongen G.; Moessner E.; Umaña P. Cergutuzumab amunaleukin (CEA-IL2v), a CEAtargeted IL-2 variant-based immunocytokine for combination cancer immunotherapy: Overcoming limitations of aldesleukin and conventional IL-2-based immunocytokines. Oncoimmunology (2017) 6:e1277306. [CrossRef]
- Menssen, H.D.; Harnack, U.; Erben, U.; Neri, D.; Hirsch, B.; Durkop, H. Antibodybased delivery of tumor necrosis factor (L19-TNFalpha) and interleukin-2 (L19-IL2) to tumor-associated blood vessels has potent immunological and anticancer activity in the syngeneic J558L BALB/c myeloma model. J Cancer Res Clin Oncol. (2018) 144:499–507. [CrossRef]
- Mortara, L.; Balza, E.; Bruno, A.; Poggi, A.; Orecchia, P.; Carnemolla, B. Anti-cancer Therapies Employing IL-2 Cytokine Tumor Targeting: Contribution of Innate, Adaptive and Immunosuppressive Cells in the Anti-tumor Efficacy. Front Immunol 18 Dec 2018. [CrossRef] [PubMed]
- Greiner, J.W.; Morillon, Y.M. 2nd, Schlom J. NHS-IL12, a Tumor-Targeting Immunocytokine. Immunotargets Ther. 2021 ;10:155-169. 27 May. [CrossRef]
- Toney, N.J.; Gatti-Mays, M.E.; Tschernia, N.P.; Strauss, J.; Gulley, J.L.; Schlom, J.; Donahue, R.N. Immune correlates with response in patients with metastatic solid tumors treated with a tumor targeting immunocytokine NHS-IL12. Int Immunopharmacol. 2023 Mar;116:109736. [CrossRef]
- Fallon, J.; Tighe, R.; Kradjian, G.; Guzman, W.; Bernhardt, A.; Neuteboom, B.; Lan, Y.; Sabzevari, H.; Schlom, J.; Greiner, J.W. The immunocytokine NHS-IL12 as a potential cancer therapeutic. Oncotarget. 2014 Apr 15;5(7):1869-84. [CrossRef]
- Zhu, Y.; Wang, K.; Yue, L.; Zuo, D.; Sheng, J.; Lan, S.; Zhao, Z.; Dong, S.; Hu, S.; Chen, X.; Feng, M. Mesothelin CAR-T cells expressing tumor-targeted immunocytokine IL-12 yield durable efficacy and fewer side effects. Pharmacol Res. 2024 May;203:107186. [CrossRef]
- Corbellari, R.; Nadal, L.; Villa, A.; Neri, D.; De Luca, R. The immunocytokine L19-TNF eradicates sarcomas in combination with chemotherapy agents or with immune check-point inhibitors. Anticancer Drugs. 2020 Sep;31(8):799-805. [CrossRef]
- Corbellari, R.; Stringhini, M.; Mock, J.; Ongaro, T.; Villa, A.; Neri, D.; De Luca, R. A Novel Antibody-IL15 Fusion Protein Selectively Localizes to Tumors, Synergizes with TNF-based Immunocytokine, and Inhibits Metastasis. Mol Cancer Ther. 2021 May;20(5):859-871. [CrossRef]
- Inoue, M.; Tsuji, Y.; Kashiwada, A.; Yokoyama, A.; Iwata, A.; Abe, Y.; Kamada, H.; Tsunoda, S.I. An immunocytokine consisting of a TNFR2 agonist and TNFR2 scFv enhances the expansion of regulatory T cells through TNFR2 clustering. Biochem Biophys Res Commun. 2024 Feb 19;697:149498. [CrossRef]
- Zheng, X.; Wu, Y. ; Bi J, Huang Y.; Cheng Y.; Li Y.; Wu Y.; Cao G.; Tian Z. The use of supercytokines, immunocytokines, engager cytokines, and other synthetic cytokines in immunotherapy. Cell Mol Immunol. 2022 Feb;19(2):192-209. [CrossRef] [PubMed]
- Raeber, M.E.; Sahin, D.; Karakus, U.; Boyman, O. A systematic review of interleukin-2-based immunotherapies in clinical trials for cancer and autoimmune diseases. EBioMedicine. 2023 Apr;90:104539.
- Lutz, E.A.; Jailkhani, N.; Momin, N.; Huang, Y.; Sheen, A.; Kang, B.H. , Wittrup K.D.; Hynes R.O. Intratumoral nanobody-IL-2 fusions that bind the tumor extracellular matrix suppress solid tumor growth in mice. PNAS Nexus. 2022 Nov 3;1(5):pgac244. [CrossRef]
- Gébleux, R.; Stringhini, M.; Casanova, R.; Soltermann, A.; Neri, D. Non-internalizing antibody-drug conjugates display potent anti-cancer activity upon proteolytic release of monomethyl auristatin E in the subendothelial extracellular matrix. Int J Cancer. 2017 Apr 1;140(7):1670-1679. [CrossRef]
- Ghasemi, R.; Lazear, E.; Wang, X.; Arefanian, S.; Zheleznyak, A.; Carreno, B.M.; Higashikubo, R.; Gelman, A.E.; Kreisel, D.; Fremont, D.H.; Krupnick, A.S. Selective targeting of IL-2 to NKG2D bearing cells for improved immunotherapy. Nat Commun. 2016 Sep 21;7:12878. [CrossRef]
- Cazzamalli, S.; Ziffels, B.; Widmayer, F.; Murer, P.; Pellegrini, G.; Pretto, F.; Wulhfard, S.; Neri, D. Enhanced therapeutic activity of non-internalizing small molecule drug conjugates targeting carbonic Anhydrase IX in combination with targeted interleukin-2. Clin Cancer Res. 2018 Aug 1;24(15):3656-3667. [CrossRef]
- Weide, B.; Neri, D.; Elia, G. Intralesional treatment of metastatic melanoma: a review of therapeutic options. Cancer Immunol Immunother. (2017) 66:647–56. [CrossRef]
- Orecchia, P.; Conte, R.; Balza, E.; Petretto, A.; Mauri, P.; Mingari, M.C.; Carnemolla, B. A novel human anti-syndecan-1 antibody inhibits vascular maturation and tumour growth in melanoma. Eur J Cancer (2013) 49:2022–33. [CrossRef]
- Orecchia, P.; Balza, E.; Pietra, G.; Conte, R.; Bizzarri, N.; Ferrero, S.; Mingari, M.C.; Carnemolla, B. L19-IL2 Immunocytokine in Combination with the Anti-Syndecan-1 46F2SIP Antibody Format: A New Targeted Treatment Approach in an Ovarian Carcinoma Model. Cancers (Basel). 2019 Aug 23;11(9):1232.
- Levin AM, L Bates D.L.; Ring A.M.; Krieg C.; Lin J.T.; Su L.; Moraga I.; Raeber M.E., Bowman G.R., Novick P.; Pande V.S.; Fathman C.G.; Boyman O.; K Garcia K.C. Exploiting a natural conformational switch to engineer an interleukin-2 ‘superkine’. Nature. 2012;484(7395):529–533. [CrossRef]
- Sun, Z.; Ren, Z.; Yang, K.; Liu, Z.; Cao, S.; Deng, S.; Xu, L.; Liang, Y.; Guo, J.; Bian, Y.; Xu, H.; Shi, J.; Wang, F.; Fu, Y.-. X-; Peng H. A next-generation tumor-targeting IL-2 preferentially promotes tumor-infiltrating CD8(+) T-cell response and effective tumor control. Nat Commun. 2019;10(1):3874.
- Charych, D.H.; Hoch, H.; Langowski, J.L.; Lee, S.R.; Addepalli, M.K.; Kirk, P.B. , Sheng D.; Liu X.; Sims P.W.; VanderVeen L.A.; Ali C.F.; Chang T.K.; Konakova M.; Pena R.L.; Kanhere R.S.; Kirksey Y.M.; Ji C.; Wang Y.; Huang J.; Sweeney T.D.; Kantak S.S. Doberstein S.K. NKTR-214, an Engineered Cytokine with Biased IL2 Receptor Binding, Increased Tumor Exposure, and Marked Efficacy in Mouse Tumor Models. Clin Cancer Res. 2016 Feb 1;22(3):680-90. [CrossRef]
- Waldhauer, I.; Gonzalez-Nicolini, V.; Freimoser-Grundschober, A.; Nayak, T.K.; Fahrni, L.; Hosse, R.J.; Gerrits, D.; Geven, E.J.W.; Sam, J.; Lang, S.; Bommer, E.; Steinhart, V.; Husar, E.; Colombetti, S.; Van Puijenbroek, E.; Neubauer, M.; Cline, J.M.; Garg, P.K.; Dugan, G.; Cavallo, F.; Acuna, G.; Charo, J.; Teichgräber, V.; Evers, S.; Boerman, O.C.; Bacac, M.; Moessner, E.; Umaña, P.; Klein, C. Simlukafusp alfa (FAP-IL2v) immunocytokine is a versatile combination partner for cancer immunotherapy. MAbs. 2021 Jan-Dec;13(1):1913791. [CrossRef]
- Ziogas DC, Theocharopoulos C, Lialios PP, Foteinou D, Koumprentziotis IA, Xynos G, Gogas H. Beyond CTLA-4 and PD-1 Inhibition: Novel Immune Checkpoint Molecules for Melanoma Treatment. Cancers (Basel). 2023 ;15(10):2718. 11 May. [CrossRef] [PubMed]
- Cillo AR, Cardello C, Shan F, Karapetyan L, Kunning S, Sander C, Rush E, Karunamurthy A, Massa RC, Rohatgi A, Workman CJ, Kirkwood JM, Bruno TC, Vignali DAA. Blockade of LAG-3 and PD-1 leads to co-expression of cytotoxic and exhaustion gene modules in CD8+ T cells to promote antitumor immunity. Cell. 2024 Aug 8;187(16):4373-4388.e15. [CrossRef] [PubMed]
- Lu C, Tan Y. Promising immunotherapy targets: TIM3, LAG3, and TIGIT joined the party. Mol Ther Oncol. 2024 Feb 12;32(1):200773. [CrossRef] [PubMed]
- Poggi A, Zocchi MR. Natural killer cells and immune-checkpoint inhibitor therapy: Current knowledge and new challenges. Mol Ther Oncolytics. 2021 Nov 29;24:26-42. [CrossRef] [PubMed]
- Tichet, M.; Wullschleger, S.; Chryplewicz, A.; Fournier, N.; Marcone, R.; Kauzlaric, A.; Homicsko, K.; Deak, L.C.; Umaña, P.; Klein, C.; Hanahan, D. Bispecific PD1-IL2v and anti-PD-L1 break tumor immunity resistance by enhancing stem-like tumor reactive CD8+ T cells and reprogramming macrophages. Immunity. 2023 Jan 10;56(1):162-179.e6. [CrossRef]
- Shi Y, Liu CH, Roberts AI, Das J, Xu G, Ren G, Zhang Y, Zhang L, Yuan ZR, Tan HS, Das G, Devadas S. Granulocyte-macrophage colony-stimulating factor (GM-CSF) and T-cell responses: what we do and don't know. Cell Res. 2006 Feb;16(2):126-33. [CrossRef] [PubMed]
- Codarri Deak L, Nicolini V, Hashimoto M, Karagianni M, Schwalie PC, Lauener L, Varypataki EM, Richard M, Bommer E, Sam J, Joller S, Perro M, Cremasco F, Kunz L, Yanguez E, Hüsser T, Schlenker R, Mariani M, Tosevski V, Herter S, Bacac M, Waldhauer I, Colombetti S, Gueripel X, Wullschleger S, Tichet M, Hanahan D, Kissick HT, Leclair S, Freimoser-Grundschober A, Seeber S, Teichgräber V, Ahmed R, Klein C, Umaña P. PD-1-cis IL-2R agonism yields better effectors from stem-like CD8+ T cells. Nature. 2022 Oct;610(7930):161-172. [CrossRef] [PubMed]
- Rodig, N.; Ryan, T.; Allen, J.A.; Pang, H.; Grabie, N.; Chernova, T.; Greenfield, E.A.; Liang, S.C.; Sharpe, A.H.; Lichtman, A.H.; Freeman, G.J. Endothelial expression of PD-L1 and PD-L2 down-regulates CD8+ T cell activation and cytolysis. Eur J Immunol. 2003 Nov;33(11):3117-26. [CrossRef]
- Taguchi, K.; Onoe, T.; Yoshida, T.; Yamashita, Y.; Tanaka, Y.; Ohdan, H. Tumor endothelial cell–mediated antigen-specific T-cell suppression via the PD-1/PD-L1 pathway. Mol Cancer Res. 2020 Sep;18(9):1427-1440. [CrossRef]
- Weichselbaum, R.R.; Liang, H.; Deng, L.; Fu, Y.X. Radiotherapy and immunotherapy: a beneficial liaison? Nat Rev Clin Oncol. 2017 Jun 17;14(6):365–79.
- Liu, Y.; Jiang, X.; Wu, Y.; Yu, H. Global research landscape and trends of cancer radiotherapy plus immunotherapy: A bibliometric analysis. Heliyon. 2024 Mar;10(5):e27103.
- Wang, J.-S.; Hai-Juan Wang, H.-J.; Qian, H.-L. Biological effects of radiation on cancer cells. Mil Med Res. 2018 Jun 30;5(1):20. [CrossRef]
- Monjazeb, A.M.; Schalper, K.A.; Villarroel-Espindola, F.; Nguyen, A.; Shiao, S.L.; Young, K. Effects of Radiation on the Tumor Microenvironment. Semin Radiat Oncol. 2020 Apr;30(2):145–57.
- Herrera, F.G.; Bourhis, J.; Coukos, G. Radiotherapy combination opportunities leveraging immunity for the next oncology practice. CA Cancer J Clin. 2017 Jan 29;67(1):65–85.
- Charpentier, M.; Spada, S.; Van Nest, J.V.; Demaria, S. Radiation therapy-induced remodeling of the tumor immune microenvironment. Seminars in Cancer Biology 86 (2022) 737–747.
- Marincola, F.M.; Jaffee, E.M.; Hicklin, D.J.; Ferrone, S. Escape of Human Solid Tumors from T–Cell Recognition: Molecular Mechanisms and Functional Significance. Adv Immunol. 2000:74:181-273. [CrossRef]
- Zeng, J.; See, A.P.; Phallen, J.; Jackson, C.M.; Belcaid, Z.; Ruzevick, J. ; DurhamN.; Meyer C.; Harris T.J.; Albesiano E.; Pradilla G.; Ford E.; Wong J.; Hammers H.-J.; Mathios D.; Tyler B.; Brem H.; Tran P.T.; Pardoll D.; Drake C.G.; Lim M. Anti-PD-1 Blockade and Stereotactic Radiation Produce Long-Term Survival in Mice With Intracranial Gliomas. Int J Radiat Oncol Biol Phys. 2013 Jun 1;86(2):343-9. [CrossRef]
- Demaria, S.; Coleman, C.N.; Formenti, S.C. Radiotherapy: Changing the Game in Immunotherapy. Trends Cancer. 2016 Jun;2(6):286-294. [CrossRef]
- Zegers, C.M.; Rekers, N.H.; Quaden, D.H.; Lieuwes, N.G.; Yaromina, A.; Germeraad, W.T.V; Wieten, L.; Biessen, E.A.L.; Boon, L.; Neri, D.; Troost, E.G.C.; Dubois, L.J.; Philippe Lambin, P. Radiotherapy combined with the immunocytokine L19-IL2 provides long-lasting antitumor effects. Clin Cancer Res. (2015) 21:1151–60. [CrossRef]
- Rekers, N.H.; Zegers, C.M.; Germeraad, W.T.; Dubois, L.; Lambin, P. Long lasting antitumor effects provided by radiotherapy combined with the immunocytokine L19-IL2. Oncoimmunology. 2015 Apr 2;4(8):e1021541. [CrossRef]
- Rekers, N.H.; Zegers, C.M.; Yaromina, A.; Lieuwes, N.G.; Biemans, R.; Senden-Gijsbers, B.L.; Losen, M.; Van Limbergen, E.J.; Germeraad, W.T.V.; Neri, D.; Dubois, L.; Lambin, P. Combination of radiotherapy with the immunocytokine L19-IL2: Additive effect in a NK cell dependent tumour model. Radiother Oncol. 2015 Sep;116(3):438-42. [CrossRef]
- Rekers, N.H.; Olivo Pimentel, V.; Yaromina, A.; Lieuwes, N.G.; Biemans, R.; Zegers, C.M.L.; Germeraad, W.T.V.; Van Limbergen, E.J.; Neri, D.; Dubois, L.J.; Lambin, P. The immunocytokine L19-IL2: An interplay between radiotherapy and long-lasting systemic anti-tumour immune responses. Oncoimmunology. 2018 Jan 16;7(4):e1414119. [CrossRef]
- Das, R.; Verma, R.; Sznol, M.; Boddupalli, C.S.; Gettinger, S.N.; Kluger, H.; Callahan, M.; Wolchok, J.D.; Halaban, R.; Dhodapkar, M.V.; Dhodapkar, K.M. Combination Therapy with Anti–CTLA-4 and Anti–PD-1 Leads to Distinct Immunologic Changes In Vivo. The Journal of Immunology. 2015 Feb 1;194(3):950–9.
- Ng, J.; Dai, T. Radiation therapy and the abscopal effect: a concept comes of age. Ann Transl Med. 2016 Mar;4(6):118–118.
- Zhao, X.; Shao, C. Radiotherapy-Mediated Immunomodulation and Anti-Tumor Abscopal Effect Combining Immune Checkpoint Blockade. Cancers (Basel). 2020 Sep 25;12(10):2762.
- Chen, D.; Song, X.; Wang, H.; Gao, Z.; Meng, W.; Chen, S.; Ma, Y.; Youda Wang, Y.; Li, K.; Yu, J.; Yue, J. Previous Radiotherapy Increases the Efficacy of IL-2 in Malignant Pleural Effusion: Potential Evidence of a Radio-Memory Effect? Front Immunol. 2018 Dec 11:9:2916. [CrossRef]
- Gadwa, J. ; Maria Amann, Thomas E Bickett, Michael W Knitz, Laurel B Darragh, Miles Piper, Benjamin Van Court, Sanjana Bukkapatnam, Tiffany T Pham, Xiao-Jing Wang, Anthony J Saviola, Laura Codarri Deak, Pablo Umaña, Christian Klein, Angelo D'Alessandro, Sana D Karam. Selective targeting of IL2Rβγ combined with radiotherapy triggers CD8- and NK-mediated immunity, abrogating metastasis in HNSCC. Cell Rep Med. 2023 Aug 15;4(8):101150. [CrossRef]
- He, K. ; Nahum Puebla-Osorio, Hampartsoum B Barsoumian, Duygu Sezen, Zahid Rafiq, Thomas S Riad, Yun Hu, Ailing Huang, Tiffany A Voss, Claudia S Kettlun Leyton, Lily Jae Schuda, Ethan Hsu, Joshua Heiber, Maria-Angelica Cortez, James W Welsh. Novel engineered IL-2 Nemvaleukin alfa combined with PD1 checkpoint blockade enhances the systemic anti-tumor responses of radiation therapy. J Exp Clin Cancer Res. 2024 Sep 2;43(1):251. [CrossRef]
Figure 1.
Schematic representation of the therapeutic action of a bispecific immunotoxin (IT) targeting CCR4 and IL-2Rα and the anti-CD30 antibody-drug conjugate (ADC) Brentuximab Vedotin in cutaneous T-cell lymphoma (CTCL). The CTCL cells expressing CCR4 (purple) and IL-2Rα (green) are the key receptors targeted by the IT (A). The IT is composed of a truncated diphtheria toxin and an anti-CCR4 antibody and IL2. This bispecific component binds to CCR4 and IL-2Rα delivering its cytotoxic payload (the truncated diphtheria toxin). In addition to targeting CTCL cells, the IT also depletes regulatory T cells (Tregs), which express IL-2Rα, enhancing the anti-tumor immune response (dashed black arrow). On the right, Brentuximab Vedotin (B), an ADC targeting the CD30 antigen expressed on CTCL, can deliver the toxic drug vedotin on tumor cells. The combination of IT and ADC therapies (red dashed arrows) leads to a synergistic effect, resulting in improved tumor suppression and survival in preclinical mouse models. Figure created with Biorender.com (accessed on 1 September 2024).
Figure 1.
Schematic representation of the therapeutic action of a bispecific immunotoxin (IT) targeting CCR4 and IL-2Rα and the anti-CD30 antibody-drug conjugate (ADC) Brentuximab Vedotin in cutaneous T-cell lymphoma (CTCL). The CTCL cells expressing CCR4 (purple) and IL-2Rα (green) are the key receptors targeted by the IT (A). The IT is composed of a truncated diphtheria toxin and an anti-CCR4 antibody and IL2. This bispecific component binds to CCR4 and IL-2Rα delivering its cytotoxic payload (the truncated diphtheria toxin). In addition to targeting CTCL cells, the IT also depletes regulatory T cells (Tregs), which express IL-2Rα, enhancing the anti-tumor immune response (dashed black arrow). On the right, Brentuximab Vedotin (B), an ADC targeting the CD30 antigen expressed on CTCL, can deliver the toxic drug vedotin on tumor cells. The combination of IT and ADC therapies (red dashed arrows) leads to a synergistic effect, resulting in improved tumor suppression and survival in preclinical mouse models. Figure created with Biorender.com (accessed on 1 September 2024).
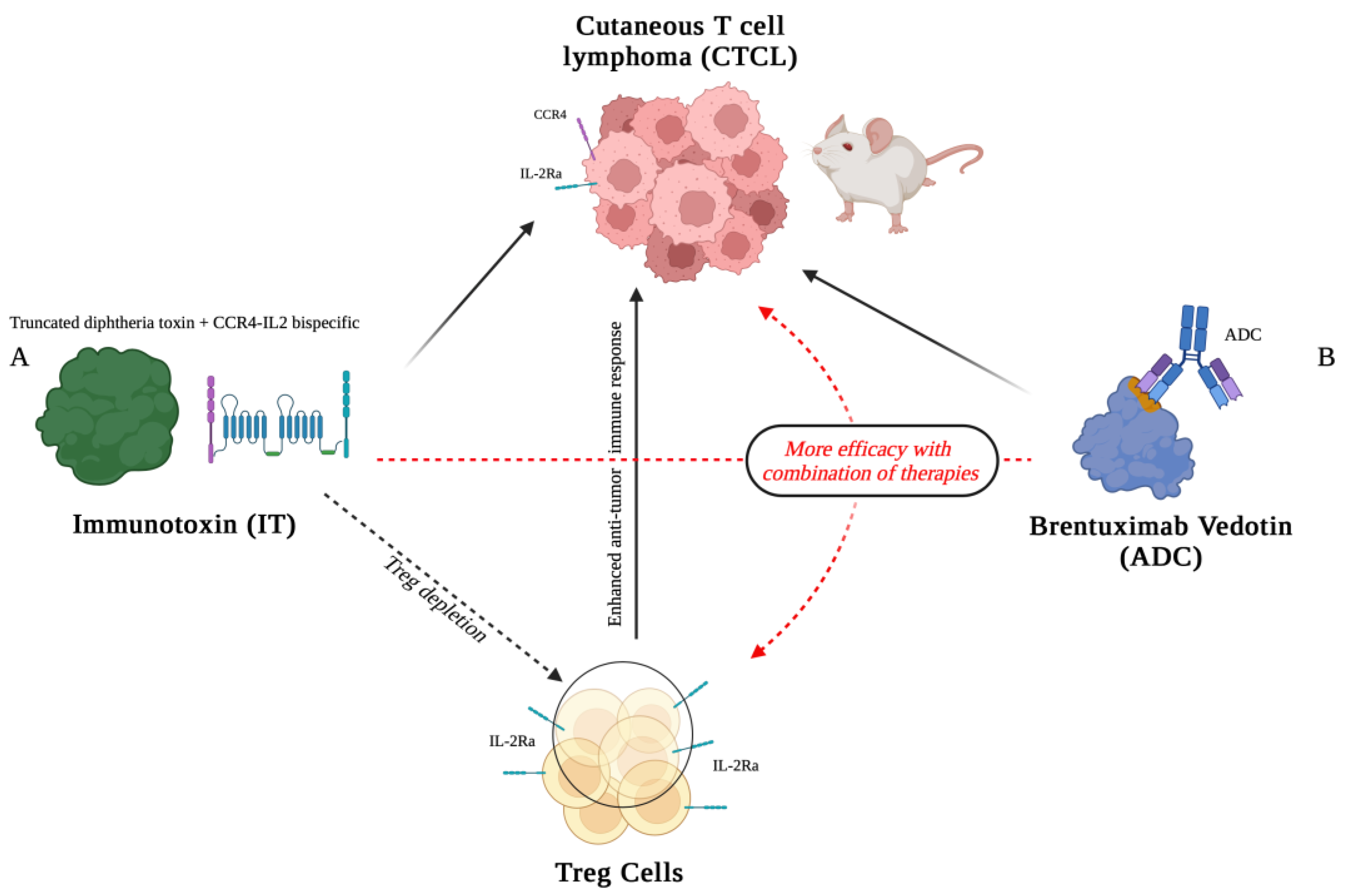
Figure 2.
Graphical representation of the effect of radiotherapy (RT) on cancer cells. Radiation induces the release of tumor antigens, which are presented by MHC-I molecules, activating the immune response. The process involves T cell receptor (TCR) recognition and interaction with immune checkpoint proteins like PD-1 and PDL1. In this context, therapeutic agents such as RDB 1462 targeting IL-2 receptor and anti-PD1 may enhance the anti-tumor immune response. Experimental mouse models have been used to study these mechanisms. Figure created with Biorender.com (accessed on 1 September 2024).
Figure 2.
Graphical representation of the effect of radiotherapy (RT) on cancer cells. Radiation induces the release of tumor antigens, which are presented by MHC-I molecules, activating the immune response. The process involves T cell receptor (TCR) recognition and interaction with immune checkpoint proteins like PD-1 and PDL1. In this context, therapeutic agents such as RDB 1462 targeting IL-2 receptor and anti-PD1 may enhance the anti-tumor immune response. Experimental mouse models have been used to study these mechanisms. Figure created with Biorender.com (accessed on 1 September 2024).
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



