
Submitted:
26 November 2024
Posted:
27 November 2024
You are already at the latest version
Abstract
Clostridioides difficile is an urgent public health threat that affects approximately half a million patients annually in the United Sates. Despite concerted efforts aimed at the prevention of Clostridioides difficile infection (CDI), it remains a leading cause of healthcare associated infections. CDI is associated with significant clinical, social, and economic burdens. Therefore, it is imperative to provide optimal and timely therapy for CDI. We conducted a systematic literature review and offer treatment recommendations based on available evidence for the treatment and prevention of CDI.
Keywords:
C.difficile infection
; recurrent C.difficile infection
; metronidazole
; vacomycin
; fidaxomicin
; fecal microbiota transplantation
Introduction
Clostridioides difficile infection (CDI) is caused by a spore-forming, toxin-producing, anaerobic, gram-positive bacillus, originally named Bacillus difficile [1]. Since it was first discovered in 1935, this bacteria has been renamed Clostridioides difficile (C.diff) and has emerged as one of the leading causes of nosocomial infections. C. difficile causes approximately 500,000 infections and 29,000 deaths each year in the United States (US) alone [2]. Despite enormous efforts focused on preventive strategies, C. difficile remains one of five CDC-designated urgent threats [3].
Recurrent Clostridioides difficile infection (rCDI) occurs in 10% to 25% of individuals after an initial episode and up to 65% in individuals with more than one rCDI episode [4,5,6]. Recurrent CDI is more difficult to treat and is associated with significant morbidity and mortality. In the endemic setting, mortality rates range between 5 - 10% which increases to 30 - 40% in the setting of fulminant disease [7,8,9]. As such, patients with CDI have higher healthcare expenditures, contributing approximately 1.5 billion annually in overall healthcare costs in the US [10].
Given the pronounced impact of CDI on morbidity and mortality, it is of utmost importance to offer optimal and timely CDI treatment. This review focuses on the treatment of CDI in adults, including new, novel microbiota-based therapeutics.
Materials & Methods
A literature search of PUBMED was conducted using MeSH terms Clostridioides difficile and treatment management or prophylaxis of Clostridioides difficile infection (CDI) between January 2019 to September 2024. The search included specific therapeutic options such as fidaxomicin, vancomycin, metronidazole, bezlotoxumab, fecal microbiota, live biotherapeutics, tigecycline, and rifamycin. Studies published in non-English language, involving animals or children, pre-prints, and case reports were excluded. Bibliographies of included studies were further reviewed to identify other relevant studies.
Results
A total of 668 articles were identified following initial PubMed search. Articles were reviewed for relevance. Following screening, 495 articles were excluded with indications described in Figure 1. The remaining 173 articles were reviewed in-depth.
First Line Antimicrobials for the Treatment of CDI in Adults
Metronidazole
There are three widely accepted antimicrobial options for the treatment of CDI: metronidazole, vancomycin, and fidaxomicin. Although it is not an FDA approved indication, historically metronidazole was long considered a first-line therapeutic option based on a 90 - 95% success rate documented in early clinical trials [11,12,13]. However, surveillance studies have since described an increasing trend in metronidazole minimum inhibitory concentration (MIC) values for common C. difficile strains, which may contribute to the increasing number of metronidazole associated treatment failures observed over the past decade [14,15].
Based on recent evidence, metronidazole does not perform as favorably as once documented in early trials. In a large prospective, randomized, double-blind, placebo controlled trial that compared vancomycin to metronidazole treatment in 150 patients stratified by disease severity, metronidazole and vancomycin resulted in clinical cure in 90% and 98% of patients with mild disease (p=0.36) and 76% and 97% of patients with severe disease (p=0.02), respectively [16]. While vancomycin and metronidazole were equally effective in mild presentations of CDI, vancomycin was the superior choice for the treatment of severe CDI. As a result, the Infectious diseases Society of America (IDSA) and Society for Healthcare Epidemiology of America (SHEA) updated CDI treatment guidelines in 2010 to recommend against the use of metronidazole specifically for patients with severe disease due to lower clinical cure rates in this landmark trial [17].
Inferior clinical cure rates associated with metronidazole were later corroborated in two large phase 3 clinical trials. Johnson et al first demonstrated that metronidazole had a 10% lower probability of achieving clinical cure compared to patients treated with vancomycin (72.7% vs 81.1%, respectively; p=0.02) [18]. In addition, clinical success rates in patients with severe disease was higher in those treated with vancomycin, but the difference was not statistically significant (p=0.059) [18]. Stevens et al later demonstrated metronidazole was inferior to vancomycin by showcasing that vancomycin use was associated with significantly lower 30-day mortality than metronidazole (RR 0.86, 95% CI 0.74-0.98) in any severity cohort [19]. This favorable response was more evident in patients with severe CDI in which vancomycin significantly reduced the risk of all cause 30-day mortality by 20% (RR 0.79, 95% CI 0.65-0.97) [19].
The mechanistic hypothesis to explain vancomycin’s improved performance compared to metronidazole include the following: (1) nearly all strains of C. difficile maintain high susceptibility to vancomycin in-vitro and (2) vancomycin achieves high fecal concentrations with mean fecal concentrations to MIC90 ratios of 500:1 to 1000:1 using an observed MIC90 of 2 mcg/mL [20,21,22,23] . In contrast, metronidazole in-vitro susceptibility is less predictable. In addition, it is efficiently absorbed, and therefore a majority of the drug is delivered from the bloodstream to the inflamed colonic mucosa. In patients with severe disease there may be a decrease in blood flow to the colon, thus decreasing colonic delivery and drug concentrations of metronidazole [16,24].
Based on this evidence, the IDSA/SHEA CDI treatment guidelines published in 2022 recommended against metronidazole for all adult patients with CDI and instead recommend vancomycin or fidaxomicin [25]. Metronidazole should only be considered in mild cases when the other two agents are unavailable. Similarly, the American College of Gastroenterology (ACG) cites that oral metronidazole can be considered for the treatment of an initial treatment non-severe CDI in low-risk patients.
Vancomycin and Fidaxomicin
The current cornerstone for the management of CDI involves treatment with one of the two FDA approved medications for CDI: vancomycin or fidaxomicin. Treatment of CDI is based on severity of the current episode and number of prior episodes. For the treatment of a first episode of non-fulminant CDI, treatment with oral vancomycin or oral fidaxomicin have demonstrated similar clinical cure rates. Two pivotal double-blind, randomized clinical trials (RCTs) reported cure rates of fidaxomicin ranging from 87 - 92%, which were similar to those reported for patients treated with vancomycin [26,27]. While fidaxomicin and vancomycin have similar efficacy with regards to clinical cure or resolution of acute diarrheal disease, many experts prefer fidaxomicin over vancomycin as it has been associated with improved sustained resolution of disease, a shorter time to resolution of diarrhea, and most importantly, a lower recurrence rate. Fidaxomicin has demonstrated a relative risk reduction of recurrence of approximately 40 -50% in clinical trials which included patients with first or second episodes of CDI [6,26,27,28,29].
Certain pharmacokinetic, pharmacodynamic and microbiological characteristics may explain the favorable results for fidaxomicin with respect to CDI recurrence. Fidaxomicin is the most potent anti-C. difficile agent with an MIC range of 0.004-1 mcg/mL [23]. Additionally, fidaxomicin can achieve high fecal concentrations several magnitudes above reported MICs and with fecal concentration to MIC90 ratios of 5000:1 based on an MIC90 of 0.25 mcg/mL [30]. Furthermore, fidaxomicin has been shown to exhibit a prolonged post-antibiotic effect and has a narrower antimicrobial spectrum to mitigate disruption to the normal gut microbiome [26]. While clinical cure rates of fidaxomicin and vancomycin are similar, IDSA/SHEA CDI treatment guidelines preferentially recommend fidaxomicin for the treatment of a first episode of non-fulminant CDI. Comparatively, the ACG recommends either vancomycin or fidaxomicin based on comparable efficacy data and lower cost associated with vancomycin [31]. A comparison of IDSA/SHEA and ACG treatment recommendation for CDI is in Table 1.
Despite successful initial treatment with fidaxomicin or vancomycin, recurrent CDI can occur in 10 - 25% of patients after an initial episode and up to 65% in patients after a first recurrence [2,4,5,6]. Two randomized clinical trials evaluated clinical efficacy of fidaxomicin 200 mg twice daily and vancomycin 125 mg four times daily for 10 days stratified by number of CDI episodes. While both trials included patients with either no prior episode or 1 episode of CDI in the past 3 months, approximately 85% of patients were enrolled with primary CDI versus approximately 15% with rCDI [26,32]. Given the small number of patients in the rCDI subgroup, both studies were underpowered to detect a difference in recurrence rates amongst patients with a history of 1 prior CDI. A significant reduction in rCDI with fidaxomicin was only found in patients with no prior CDI episode (i.e. primary CDI). In patients with 1 prior CDI episode, only a non-significant trend towards lower recurrence rates was associated with fidaxomicin [26,32]. Results of these studies suggest fidaxomicin is optimally beneficial for recurrence prevention in patients with no prior CDI but can also be considered for patients with one prior episode given trends towards lower recurrence. Data from RCTs for fidaxomicin in patients with multiple episodes of recurrence is limited.
Guery et al compared an extended-pulsed fidaxomicin regimen (200 mg twice daily on days 1-5, then once daily on alternate days on days 7 to 25) to vancomycin 125 mg four times daily on days 1-10. This study included patients with up to two prior CDI episodes; however, only 5.6% of patients in this subgroup were ultimately enrolled. The primary endpoint was sustained clinical cure 30 days after end of treatment. Extended-pulsed fidaxomicin was superior to standard dose vancomycin for sustained clinical cure (70% (124/177) extended pulsed fidaxomicin vs 59% (106/179) vancomycin (OR 1.62 95% CI 1.04-2.54, p=0.030)[6]. Recurrence of CDI at day 90 was also lower in the fidaxomicin group (6% (11/177) vs 19% (34/176), OR 0.29 (95CI 0.14-0.60; p=value 0.00073)[6]. While the number of patients with two previous CDI episodes was limited, this study does demonstrate potential benefit of a fidaxomicin extended pulsed regimen in this subpopulation.
In addition to fidaxomicin, other guidelines recommended options for the treatment of second or subsequent recurrence include oral vancomycin therapy using a tapered and pulsed regimen (eg. 125 mg four times daily for 10 – 14 days, 2 times per day for a week, once per day for a week, and then every 2 or 3 days for 2 to 8 weeks). This dosing regimen is based on limited evidence and largely supported by one RCT. In this trial, most patients had a history of 4 to 5 episodes (range 2 to 9) prior to randomization. Patients received a 6-week oral vancomycin taper or 14 days of oral vancomycin followed by fecal transplantation enema. There was no difference in rCDI in the cohort receiving the fecal transplant enema or tapered oral vancomycin course [56.2% (9/16) fecal transplant vs 41.7% (5/12) vancomycin taper] [33].
Based on available evidence, antimicrobial treatment recommendations for recurrent CDI include standard dose fidaxomicin, extended-pulsed fidaxomicin, standard dose vancomycin, or vancomycin tapered and pulsed (see Table 1). Fidaxomicin can be considered as the preferred therapeutic option for an initial CDI episode or first recurrence. For second recurrences, fidaxomicin extended-pulsed or vancomycin tapered and pulsed regimens can be considered. Given limited data for fidaxomicin in multiple recurrences, one should consider vancomycin pulsed and tapered regimens for 3 or more recurrences in addition to adjunctive or microbiota-based therapies discussed below.
For rCDI, the choice between therapeutic options often depends on the antibiotic used for the first episode [34]. For example, if the first episode of CDI was treated with a standard course of oral vancomycin, the first rCDI would be treated with standard fidaxomicin or a vancomycin tapered and pulsed regimen. In addition, risk factors for recurrence such as age greater than 65 years, concomitant systemic antibiotics for non-CDI indication, comorbidities, and severe infection should be taken into account. Guery et al demonstrated that an extended pulsed regimen of fidaxomicin has lower recurrence rates compared to vancomycin and was particularly advantageous for patients at high risk of recurrence [6]. Patients were included in this study if they were aged 60 years or older, and many presented with concomitant risk factors for rCDI such as severe CDI, history of 1 or 2 prior CDI episodes, concomitant systemic antibiotics for a condition other than CDI, and documented cancer in their medical history [6]. If patient compliance allows, an extended pulsed regimen of fidaxomicin could be preferentially considered for patients at highest risk for recurrence.
For fulminant CDI, patients are treated with higher dose oral vancomycin plus intravenous metronidazole and vancomycin rectal enema if an ileus is present [25,31]. Fidaxomicin clinical trials excluded patients with life-threatening or fulminant CDI. In the absence of supportive data, fidaxomicin is not recommended for the treatment of fulminant CDI. While studies comparing standard dose vancomycin (i.e. 125 mg four times daily) to high dose vancomycin (i.e. 500 mg four times daily) suggest there is no difference in clinical cure rates, these studies excluded patients who presented with fulminant CDI [22,35,36]. Rather, this recommendation is based out of prudency. An ileus reduces gastrointestinal motility and delays GI transit of oral medications. Additionally, profuse diarrhea with higher stool frequency can reduce the contact time of vancomycin in the colon [21]. Therefore, patients with an ileus in the setting of profuse diarrhea may benefit from high doses of oral vancomycin. Similarly, there is limited data to support the use of rectal vancomycin for patients with an ileus. Given the severity and urgency of fulminant CDI, rectal vancomycin and intravenous metronidazole are recommended to ensure therapeutic concentrations within the inflamed colon [25].
Alternative Antimicrobial Therapies
Rifaximin
Rifaximin, a non-absorbable rifamycin, is currently indicated for the treatment of traveler’s diarrhea and reducing the recurrence of hepatic encephalopathy. Since it displays potent activity against C. difficile and achieves high colonic concentrations because of its poor absorption, rifaximin has been explored as a treatment option for other GI infections like CDI [37]. Rifaximin has been most studied as an adjunctive or “follow-on” agent after vancomycin treatment in patients with rCDI.
The IDSA/SHEA guidelines recommend a standard course of oral vancomycin followed by rifaximin in patients with >1 recurrence [25]. This is largely based on a small RCT in which patients received rifaximin 400 mg three times daily for 20 days after standard CDI therapy with vancomycin or metronidazole. Recurrent CDI occurred in 5 of 33 (15%) patients given rifaximin and 11 of 35 (31%) patients given placebo (p=0.11), which was not statistically significant due to small sample size [38]. While there was a numerical reduction in rCDI, the difference was not significant. While rifaximin may be promising, it has not been definitively proven as effective. Lastly, results of these trials cannot be extrapolated to patients treated with fidaxomicin. As the standard of care treatment changes from metronidazole and vancomycin to fidaxomicin (an anti-CDI therapy associated with lower recurrence rates), the benefit of rifaximin may be even less impressive.
One concern associated with the use of rifaximin is the potential for resistance. C. difficile isolates with elevated MICs >256 and isolates developing high MICs during rifaximin therapy have been reported with resistance rates ranging from approximately 30 to 50% [37]. In the absence of a definitive demonstration of benefit and concerns for resistance ACG suggests further randomized trials, including cost-benefit analyses, are needed. Therefore, ACG does not currently recommend its routine use [31].
Another consideration for rifaximin is its effect on the gut microbiome. In addition to potent activity against C. difficile, it is more potent than fidaxomicin and vancomycin against gram-negative anaerobic bacteria such as Bacteroides spp. As a result, gut dysbiosis is further exacerbated, thus increasing the risk of recurrence [39]. Given paucity of data, concerns for resistance, and propensity to disrupt the gut flora it may be more beneficial to explore alternative options for patients with >1 recurrence such as monoclonal antibodies or microbiota-based therapies in addition to standard-of-care antibiotics.
Tigecycline
Tigecycline, a tetracycline derivative, is a broad-spectrum antibiotic that is active against various gram-positive and gram-negative aerobic and anaerobic bacteria including C. difficile, Bacteroides fragilis, Prevotella spp., and multidrug resistant bacteria [40]. As a result, it can have a significant impact on the gut microbiome and subsequently increase the risk of rCDI.
Both IDSA/SHEA and ACG guidelines describe tigecycline as an alternative agent with suggested efficacy in the treatment of C. difficile, but do not recommend its routine use. There are no RCTs to-date that have evaluated the safety or efficacy of tigecycline for the treatment of CDI. The current evidence to support the use of tigecycline is limited to retrospective and observational studies in severe or fulminant CDI [41,42,43,44]. A meta-analysis of 4 studies that included patients with severe CDI and treated with tigecycline as monotherapy (45/186, 24.12%) or in combination with other antibiotics (141/186, 75.88%) reported a pooled clinical cure rate of 79% (95% CI 73 – 84.5%) [40]. While tigecycline may be a promising agent, the authors of the meta-analysis acknowledged the lack of RCTs and heterogeneity of included studies and suggested further studies are needed to elucidate the role of tigecycline in the treatment of CDI. A phase 2 clinical trial was started in 2011 to specifically address this question but was discontinued due to slow enrollment rate.
While there is insufficient evidence to support the universal use of tigecycline, it may be considered as part of a salvage regimen in patients with severe or fulminant CDI based on a retrospective study that demonstrated higher clinical cure rates for patients treated with tigecycline compared to standard antibiotics for severe or fulminant CDI (75.6% vs 53.3%, respectively; p=0.02). In this study, a majority of patients (84.6%) received tigecycline after failure with vancomycin plus metronidazole, thus suggesting its role as salvage therapy [44]. In the absence of RCTs, risk may outweigh potential benefit of tigecycline in the setting of non-salvage therapy.
Adjunctive Treatment
Bezlotoxumab
Bezlotoxumab is a monoclonal antibody that binds to C. difficile toxin B and is administered as a single dose of 10 mg/kg based on actual body weight infused over 1 hour in conjunction with standard-of-care antibiotics [45]. It is not an antibiotic and therefore is not indicated for the treatment of CDI and should not be used as monotherapy. Rather it received approval in 2016 as an adjunctive agent to standard-of-care-antibiotics to reduce rCDI in adults and pediatric patients 1 year of age and older.
Bezlotoxumab was originally studied in two double-blind, randomized, placebo-controlled phase 3 trials, MODIFY I/II, in which 2559 patients were treated with placebo or bezlotoxumab. Administration of bezlotoxumab occurred anywhere between one day prior to the initiation of standard-of-care antibiotics and up to day 14 of antibiotic therapy. Distribution of standard-of-care antibiotics included 46.7% metronidazole, 47.7% vancomycin and 3.6% fidaxomicin [46]. Nearly half of the study participants had 1 or more prior CDI episodes. Recurrence within 12 weeks of bezlotoxumab infusion occurred in 16.5% (129/781) of patients receiving bezlotoxumab versus 26.6% (206/773) of patients in the placebo group (p<0.0001). This corresponds to a number needed to treat (NNT) of 10 to prevent a single recurrence [46]. Notably, the choice of antibiotic therapy for CDI did not influence bezlotoxumab efficacy.
A post-hoc analysis later investigated bezlotoxumab efficacy in patients with the following risk factors for recurrence: age > 65 years, history of CDI, immunocompromised, severe CDI, and ribotype 027/078/244. In this post hoc analysis 1554 patients were included, and the majority (75.6%) had at least 1 pre-specified risk factor for rCDI. There was no difference in initial cure rates in the bezlotoxumab and placebo group for patients with at least 1 risk factor and in patients with no risk factors [47]. However, bezlotoxumab reduced the rates of rCDI amongst patients with any of the five pre-specified risk factors. The absolute reduction in rCDI associated with bezlotoxumab increased with the number of risk factors present: -14.2%, -14.2% and 24.8% for those with 1, 2 and 3 or more risk factors, respectively (95% CI excluded 0 for all comparisons) [47]. Results from this study suggest that bezlotoxumab is particularly effective in patients who are at high risk of recrudescence of disease which include those who are 65 years or older, have a history of CDI, or are infected with hypervirulent ribotypes 027/078/244.
A second post hoc analysis evaluated the timing of bezlotoxumab administration with respect to antibiotic treatment initiation for CDI. In 1554 patients included in this analysis, 649 (41.8%), 469 (30.1%), and 436 (28.1%) received an infusion at 0 – 2, 3-4, and > 5 days after initiation of anti-CDI therapy. Rate of clinical cure and the time to resolution of diarrhea were similar in all groups irrespective of timing of administration (range 77.8 to 81.4% bezlotoxumab vs 77.8 to 81.7% placebo)[48]. Results of this study suggest bezlotoxumab can be administered at any point during antibiotic therapy for CDI.
Based on available evidence, bezlotoxumab can be considered for patients with one or more of the following risk factors for rCDI: age > 65, history of CDI, immunocompromised, severe CDI, prior CDI, or presence of a hypervirulent C. difficile strain. This coincides with current CDI guideline recommendations. ACG specifically recommends the addition of bezlotoxumab for patients who are at high risk of recurrence. IDSA/SHEA recommends the addition of bezlotoxumab in patients with a CDI episode within the past 6 months for first or multiple recurrences and for patients at high risk for CDI recurrence for primary CDI.
When considering the addition of bezlotoxumab, safety considerations should be made. While adverse events (AEs) in clinical trials were generally mild with symptoms of nausea, headache, fatigue, dizziness, and pyrexia occurring in similar rates between bezlotoxumab and placebo (7.5% and 5.9%, respectively) the package insert does provide additional AEs and mortality rates for patients with congestive heart failure (CHF). In patients with a history of CHF, a serious reaction of heart failure occurred in 12.7% of bezlotoxumab treated patients compared with 4.8% of patients in the placebo arm. In these same patients, the mortality rate was higher in the bezlotoxumab group compared to placebo (19.5% vs 12.5%, respectively) [45]. Furthermore, patients with CHF were more likely to report increased treatment-emergent adverse events (83.9% vs 12.5%, respectively) and serious adverse events (53.4% vs 38%, respectively) [31]. While there is no absolute contraindication to the use of bezlotoxumab, it may be best to avoid bezlotoxumab in patients with CHF out of prudency.
Microbiota Restoration Therapies for the Prevention of CDI
Fecal Microbiota Transplantation (FMT)
Fecal Microbiota Transplantation (FMT) was first used in the 4th century in China to treat patients with severe diarrhea and food poisoning [49]. It was first reported in medical literature in 1958 when it was successfully used for treatment of pseudomembranous colitis. The practice of FMT gained traction following the landmark open-label randomized trial in Netherlands in 2013. This study showed that duodenal infusion of donor feces preceded by a short vancomycin regimen and bowel lavage ( 13/16, 81% cured) was superior to vancomycin alone (4/13, 31%) or vancomycin and bowel lavage (3/13, 23%) in patients with recurrent CDI [50].
Over the years, several studies have shown benefits of FMT in many conditions, including recurrent CDI, inflammatory bowel disease and metabolic syndrome. A Cochrane systematic analysis conducted to assess safety and efficacy of FMT in recurrent CDI in adults showed superior efficacy of FMT over other treatment modalities. This systematic analysis included six randomized trials including 320 participants from Canada, Italy, Netherlands and the United States. These trials excluded immunosuppressed individuals. The pooled results from the six studies showed the use of FMT with recurrent CDI resulted in a higher rate of resolution of recurrent CDI compared to other controls with a risk ratio of 1.92, confidence interval (CI) 1.36 to 2.71 with statistical significance. The follow up time period after treatment with FMT was 8-18 weeks. The number needed to treat for an additional benefit outcome was only 3. The amount of stool, type of donor, route of administration, number of administrations varied across the studies. The commonly reported mild adverse events in the FMT group were abdominal pain, bloating and diarrhea. The authors were not able to draw conclusion about safety as the number of serious adverse events were small [51]. Accordingly, the IDSA guidelines (2021), recommends using FMT after at least two recurrences, if appropriate antibiotics have failed [25].
At a patient-level, outcome of FMT is influenced by donor and recipient related factors, such as microbiota richness, underlying disease state and genetic make-up of an individual. In addition, FMT protocols regarding recipient preparation to administration of the product also influence the final outcome of FMT. It is a well-accepted practice to administer oral vancomycin before FMT for recurrent CDI, for priming the recipient’s gut for FMT. However, there is lack of standardization for other factors like bowel cleansing regimen, number of fecal infusions, amount of infused feces and route of delivery. Based on limited evidence, for recurrent CDI, higher cure rates were achieved with repeated FMT compared to single infusion[52].
The mechanism of action of FMT in recurrent CDI remains unclear. Potential mechanisms that have been proposed include restoration of microbial ecology and favorable changes in microbial-derived metabolites. Restoration of microbial ecology implies increase in microbial diversity which results in increase in the colonization resistance against C.difficile. Microbial metabolites that are known to play an important role in CDI pathology are bile acids and short-chain fatty acids (SCFAs). Primary bile acids (PBA) promote C.difficile germination and secondary bile acid inhibit spore germination. In individuals with recurrent CDI, there is excess of PBA and diminished secondary bile acids. Following FMT, there is restoration of bile acid composition that resembles that of healthy donors. Another metabolite, SCFAs are known to protective against C.difficile, i.e., higher the level, more protection against CDI and their levels are restored following FMT. Other less studied mechanisms of FMT are immune-mediated and epigenetic-related mechanism [53]
Given the limited understanding of the mechanism of action of FMT, there is variability in regulating its use globally. For instance, in USA and Canada FMT is an investigational drug which can be used either to treat recurrent CDI and in the context of clinical trial for other diseases. While in certain countries in EU, it is considered a tissue transplant and a regulated medicinal product in the United Kingdom. Despite this variability, the FDA in USA has published extensive guidelines regarding screening of FMT donors and requires submission of details of specific chemistry, manufacturing and control of the product before administration [54]. With these regulations in place, feces for FMT can be obtained from stool banks, the largest being OpenBiome that collects, screens and stores stool from health donors.
FMT is an effective and relatively safe option for individuals with recurrent CDI and has an evolving role in treating chronic conditions like inflammatory bowel diseases.
Novel Live Biotherapeutic Products
Although FMT is generally safe, it is associated with some risk. The FDA has issued a safety alert regarding the potential for transmission of serious or life-threatening infections with pathogenic and multi-drug-resistant organisms with the use of FMT [55,56]. This underscores the need for a rigorous and standardized approach to donor qualification, pathogen screening, and application of quality control measures to reduce the risk of transmission.
Based on a clear need for standardization of manufacturing and administration processes, there has been new development around standardized microbiota restoration therapies in capsule and enema form. In comparison to FMT methodologies that involve infusion of whole stool, newer live biotherapeutics products (LBP) provide a smaller, more refined consortium of key bacteria with a standardized and consistent composition, concentration, and screening process for infectious organisms [57]. The recent US Food and Drug Administration (FDA) approval of LBPs has expanded patient access for microbiota restoration therapies beyond FMT. Similar to FMT, the aim of LBPs is to reconstitute the microbiome and achieve engraftment in which healthy bacteria replicate in the recipient colon to create an inhibitory environment for C. difficile growth. Real-world experience with new LBPs for the prevention of rCDI will help inform its place in therapy over the next few years. The following section will review the new biotherapeutics for the prevention of rCDI: fecal microbiota, live-jslm; fecal microbiota spores, live-brpk; and VE303.
Fecal Microbiota, Live-jslm (RebyotaTM)
First in the new class of LBPs for CDI is rectal live-jslm fecal microbiota suspension, previously known as RBX260 in clinical trials. Rectal live-jslm received FDA approval for the prevention of rCDI following antibiotic treatment for recurrent CDI. The product is administered rectally as a single 150 mL dose to be administered by a licensed healthcare provider 24 to 72 hours after the last dose of antibiotics [58]. No bowel preparation is required prior to administration. The use of bowel preparation was not studied in clinical trials to help simplify the administration process and improve patient experience [59]. Rectal live-jslm is a fecal microbiota suspension derived from healthy human stool samples that undergoes a panel screen for transmissible pathogens. In contrast to FMT in which whole stool samples are administered, fecal microbiota (FM), live-jslm provides a smaller, more refined consortium of key bacteria with consistent make-up. Each 150 mL dose contains between 1x108 and 5x1010 colony-forming units (CFU) of fecal microorganisms per mL, including more than 1x105 CFU/mL of Bacteroides, that is suspended with a solution of polyethylene glycol (PEG) 3350 and 0.9% sodium chloride in a predefined ratio [55,57]. FM, live-jslm is stored either in an ultracold freezer (-60°C to 90°C) or in a refrigerator (2°C to 8°C) if administered within 5 days [58]. Prior to administration, healthcare personnel should ensure the suspension is warmed to room temperature. For minimization of cramping and expulsion, patients should be instructed to remain in a left-sided prone or knee-chest position for up to 15 minutes post administration.
A safety concern with FMT was the lack of a standardized approach to donor qualification and pathogen screening processes. FM, live-jslm, however, was developed under the FDA’s Investigational New drug program with the intent to meet the stringent requirements for approval as an FDA regulated drug product to reduce rCDI. As a result, stool donors for FM, live-jslm undergo a rigorous screening process with routine blood and stool testing to identify pathogens such as HIV, hepatitis A/B/C, syphilis, SARS-CoV-2, enteropathogenic Escherichia coli, Shiga toxin producing E. coli, norovirus, rotavirus, adenovirus, vancomycin-resistant enterococci, methicillin-resistant Staphylococcus aureus, and other antibiotic resistant bacterial strains [60].
FM, live-jslm was approved based on data from the PUNCH CD trial series. First, in the series was PUNCH CD which was first published in March 2016. The objective of this study was to evaluate the safety and durability of FM, live-jslm in patients with at least two rCDI episodes or at least 2 severe episodes requiring hospitalization. Of the 188 reported AEs, the most cited were mild to moderate in severity, primarily GI, and all self-limited: diarrhea 24%, flatulence 14%, abdominal pain and cramping 13%, and constipation 13% [61]. Twenty serious adverse events were reported but were found to be unrelated to the study drug. Resolution of CDI-associated diarrhea at 8 weeks for patients receiving either 1 or 2 doses occurred in 27/31 (87.1%) study participants [61]. Of the 14 patients who received a second dose and were available for follow-up, 78.6% (11/14) were considered treatment successes. Therefore, in all 31 patients included in this study, 87.1% (27/31) experienced resolution of CDI-associated diarrhea. The results of PUNCH CD illustrated the short-term safety of FM, live-jslm and demonstrated similar efficacy to those reported for FMT.
In October 2022, results from PUNCH CD2, a phase 2b randomized, placebo-controlled trial, were published. Eligible patients included those with at least 3 episodes of rCDI and received at least two courses of CDI directed antibiotic therapy. Following a 24 to 48 hour wash out period after antibiotic therapy, patients received a single dose of FM, live-jslm and were eligible to receive a second dose if rCDI was suspected less than 8 weeks after receiving the first dose Study participants were randomized into one of the following treatment groups: 2 doses of FM, live-jslm, 2 doses of placebo, or 1 dose of FM, live-jslm followed by 1 dose of placebo. Non-responders were eligible to receive up to 2 doses of FM, live-jslm in an open label part of the study. In the final intention to treat (ITT) analysis, clinical cure at 8 weeks occurred in 56.8% (25/44) of patients who received one dose of FM, live-jslm and 43.2% (19/44) of patients who received one dose of placebo (p=0.201) [62]. Across all analyses, 2 doses of FM, live-jslm were not associated with improved treatment success. The combined efficacy for all patients who received at least 1 dose of FM, live-jslm, which included blinded or open-label administration, was 88.8%. Treatment related AEs were similar across all groups during the 24 month follow up period [62]. Although the clinical trial did not meet its pre-defined primary endpoint for treatment success observed at 8 weeks after the receipt of 2 doses, clinically meaningful and a statistically significant difference was found between 1 dose compared to placebo. As a result, a single dose regimen was pursued in the phase 3 clinical trial, Punch CD3.
The Punch CD3 trial was a randomized, double-blind, placebo-controlled trial that compared 1 dose of FM, live-jslm (n=180) to placebo (n=87) for treatment success at 8 weeks defined as the absence of C. difficile infectious diarrhea. The study included patients who had one or more rCDI episodes. If treatment failure was noted within 8 weeks of study treatment, participants were able to receive an open-label treatment of FM, live-jslm. This study used a Bayesian primary analysis that combined results from the placebo and 1-dose arm of Punch CD2 with those from matching arms of the Punch CD3 trial. Based on the Bayesian analysis integrating Punch CD2 trial data, treatment success occurred in 70.6% FM, live-jslm vs 57.5% placebo (13.1% treatment difference) with posterior probability of superiority of 0.991, exceeding the prespecified cutoff of 0.975 [60]. Of the patients with documented success at 8 weeks, 92.1% experienced sustained clinical resolution at 6 months. 65 study participants (n=41 FM, live jslm; n=24 placebo), with treatment failure received a dose of open-label FM-live, jslm. Notably, 53.7% (22/41) of participants who received 2 doses of FM-live jslm were deemed treatment successes within 8 weeks and of these responders 86% (19/22) exhibited sustained clinical response at 6 months. Overall, 83.6% (148/177) who received blinded FM-live jslm achieved treatment success by their second dose. During the 6-month follow-up period, a higher rate of AEs was reported in patients who received FM-live, jslm compared to placebo (100/180, 55.6% vs 39/87, 44.8%, respectively) [60]. However, the difference was largely driven by mild adverse events which mainly occurred during the first 2 weeks after treatment. Punch CD3 demonstrated superiority of FM-live, jslm compared to placebo with sustained clinical response up to 6 months with no reported serious AEs.
Given the similarities between Punch CD2 and Punch CD3 that allowed for a Bayesian modeling approach, Feuerstadt and colleagues aimed to identify patient and treatment characteristics that may have impacted the safety and efficacy of FM, live-jslm. The goal of this study was to help inform real-world clinical decision making. FM, live-jslm significantly reduced rCDI in patients without T2DM, CKD, and CHF as well as those who received oral vancomycin courses >14 days. The most robust reductions of rCDI were observed in patients with a 3-day antibiotic wash out period (24% (95%CI 1.3 – 46.5) and participants with > 4 previous CDI episodes (20.8, 95% CI 3.3 – 38.0) [59]. While FM-live-jslm can be administered within 24 to 72 hours of completing standard of care antibiotics based on FDA approved labeling, an antibiotic wash-out period of at least 3 days may suggest optimal clearance of antibiotics within the system to prevent unintended harm to microbiota-based therapies.
Across all 3 trials of Punch CD, Punch CD2, and Punch CD3, FM-live-jslm was demonstrated to have a positive benefit-risk profile for the prevention of rCDI. However, the following patients were excluded from the trial series: immunocompromised, prior FMT, pregnancy, other concurrent infections, gastrointestinal comorbidities (eg. Irritable bowel syndrome (IBS), inflammatory bowel disease (IBD), celiac disease), and liver cirrhosis. Although it may be necessary to exclude these populations in early trial designs, these patient groups would have the most to benefit from LBPs like FM, live-jslm. Addressing this concern, Punch CD3-OLS was recently published in May 2024. This study was a prospective, phase 3, open-label study designed to assess the 6-month AE rate of FM, live-jslm in patients previously excluded from the prior Punch CD trials. Secondarily, it evaluated treatment success at 8 weeks and sustained clinical response for up to 6 months. Study participants included individuals with GI comorbidities (ie. ulcerative colitis, Crohn’s disease, IBD, IBS, GERD), mild to moderate immunocompromising conditions, and renal and urinary comorbidities. Overall, 793 patients were enrolled in which approximately half were > 65 years of age. Results of this study demonstrated an 8-week symptom resolution rate of 73.8% and a 91% sustained clinical response at 6 months with FM-live, jslm, which are comparable to the Punch CD3 RCT [63]. Majority (121/151, 80%) of the individuals with treatment failure at week 8 elected to receive a second dose of FM, live-jslm. Following the second dose, 55.4% of patients achieved treatment success [63]. Similar to previous trials, AEs were mild to moderate and resolved with time. Punch CD3-OLS provided safety and efficacy data in a “real-world” population at higher risk for rCDI.
FM, live-jslm has consistently demonstrated to be safe and effective across several randomized controlled trials amongst patients with one or more recurrences of CDI, including complex patients such as those who are immunocompromised. Success rates are largely comparable to the ranges reported for FMT. However, unlike FMT, FM, live-jslm is manufactured under standardized processes and is an FDA approved drug product. Based on long term safety and efficacy, it can be considered as an alternative to FMT in patients with at least 1 recurrence. While FDA labeling suggests it can be administered as early as 1 day after completion of standard of care antibiotics, in the absence of bowel preparation it may be prudent to wait 72 hours to limit lingering presence of antibiotics that may reduce its efficacy. While 1 dose of FM-live jslm was selected for phase 3 studies, a second dose may be considered for treatment failures after symptom recurrence within 8 weeks of first dose.
Fecal Microbiota Spores, Live-brpk (VowstTM)
Fecal microbiota spores, live (FMSL)-brpk, previously referred to as SER-109 in clinical trials, is another novel FDA approved LBP indicated to prevent rCDI following standard of care antimicrobial treatment. FMSL-brpk is the first capsulated and orally administered fecal microbiota based LBP that is composed of primarily live, purified Firmicute spores [64]. A reduction of Firmicute spp. and their key metabolites is one mechanism believed to facilitate CDI recurrence. A reduction of Firmicute spp. in the gut microbiome leads to an increase in primary BAs, promoting favorable conditions for C. difficile spore germination. As a result, the administration of live purified firmicute spores is thought to resist and limit the C. difficile life cycle [65].
The manufacturing process for FMSL-brpk is quite rigorous and first involves a donor screening process that includes a detailed past medical history, physician examination, and comprehensive laboratory testing [64]. Healthy donor stool then undergoes testing for transmissible pathogens and undergoes processing compliant with good manufacturing processes. During the purification process, the fecal matter undergoes treatment with high concentrations of ethanol to selectively kill non-Firmicutes spores, including pathogenic bacteria. Following ethanol treatment, the fecal matter undergoes filtration to remove solids and residual ethanol to isolate the firmicutes spores. The rigorous manufacturing process for FMSL-brpk results in an inactivation of several potential pathogens, fungi, parasites, and viruses including SARS-CoV-2, and results in a standardized combination of Firmicutes spores with each capsule containing 1x106 and 3x107 Firmicutes spore colony forming units [64].
The product is supplied as capsules and recommended to be stored in the original packaging at room temperature (2° to 25°C) [66]. The dosage of FMSL-brpk is 4 capsules orally once daily for 3 consecutive days on an empty stomach. Prior to taking the first dose, the patient is instructed to complete antibacterial treatment for rCDI 2 to 4 days. In order to flush out any residual antibiotics within the patient’s gastrointestinal system that may impair FMSL-brpk activity, patients should drink 296 mL (10 oz) of magnesium citrate on the day before and at least 8 hours prior to taking the first dose of FMSL-brpk. For patients with impaired renal function, polyethylene glycol electrolyte solution may be used as an alternative [66]. Except for small amounts of water, patients should not eat or drink for at least 8 hours prior to administration of the first dose.
The safety and efficacy of FMSL-brpk was evaluated in the ECOSPOR trial series. Early in the trial series was ECOSPOR, a phase 2, randomized double-blind, placebo-controlled trial that included patients who had > 3 episodes of CDI within 9 months. Patients were randomized to receive a single dose of FMSL-bprk (n=59) or placebo (n=30). rCDI up to 8 weeks after treatment, safety, engraftment and bile acid changes were analyzed. No significant difference in rCDI between FMSL-brpk and placebo was identified (44.1% vs 53.3 %, respectively; RR 1.2, 95% CI 0.8 – 1.9) [67]. However, in a pre-planned analysis by age stratum, FMSL-brpk significantly reduced recurrence in those age > 65 years (45.2% vs 80%, respectively, RR 1.77; 95% CI 1.11 – 2.81). Notably, no benefit was shown in those aged <65 years. FMSL-brpk was generally well tolerated with AEs occurring at similar rates in the study and placebo group. GI based AEs were most commonly reported. Engraftment was assessed by evaluating the number of dose species in stool samples. Those receiving FMSL-brpk had more spore forming Firmicutes spp. compared to placebo throughout the 8-week follow-up (p<0.001). Additionally, to measure the impact of FMSL-brpk on non-dose species, the amount of Bacteroides was assessed, and a greater abundance of Bacteroides was found in the group receiving FMSL-brpk (p=0.04)[67]. To understand the relationship between engraftment and non-recurrence, authors evaluated the relationship between engraftment and abundance of secondary BAs. Although not significant, secondary BA levels were higher in those with no recurrence receiving FMSL-brpk compared to those with documented recurrence within 8 weeks (p=0.08). Notably, factors associated with non- recurrence were early engraftment of FMSL-brpk (p<0.05) and increased secondary BAs (p<0.0001)[67]. ECOSPOR provided a strong mechanistic basis for the administration of live, purified firmicutes through the demonstration that early engraftment with FMSL-brpk was associated with reduced rCDI rates and a minimal AE profile.
Two phase 3 trials assessed the therapeutic efficacy of FMSL-brpk: ECOSPOR III and ECOSPOR IV. ECOSPOR III included 182 patients who had 3 or more episodes of CDI within 12 months. The primary efficacy endpoint was CDI recurrence up to 8 weeks after treatment initiation. FMSL-brpk was found to be superior to placebo in reducing rCDI: 12% vs 40%, respectively; difference 28%; RR 0.31 95% CI 0.18-0.58; p<0.001) [65]. Similar results were observed irrespective of the initial antibiotic used to treat CDI. While not statistically significant, FMSL-brpk led to less frequent rCDI when stratified by age: age <65 years: RR 0.24, 95%CI 0. 07 – 0.78 and age > 65 years: RR 0.36; 95% CI 0.18- 0.72 [65]. AEs related or possibly related to thes tudy drug or placebo occurred in slightly more than half of the patients in each group, a majority of which were mild to moderate GI disorders (eg. flatulence, abdominal pain, constipation, diarrhea) [65].
In a secondary analysis of ECOSPOR III with an extended follow up through 24 weeks, the rate of rCDI nearly doubled compared to the 8 week follow up results, but were still significantly improved in the FMSL-brpk group (21.3% FMSL-brpk vs 47.3% placebo, RR 0.46; 95% CI 0.30 – 0.73; p<0.001) [68]. Overall, FMSL-brpk demonstrated durable efficacy with reduced rCDI rates and was well tolerated through 24 weeks.
In a post hoc analysis, rates of rCDI through week 8 were analyzed for the following subgroups: Charlson comorbidity index score categories (0, 1-2, 3-4, >5); baseline creatinine clearance (>30, 30-50, >50 to 80, > 80 mL/min); number of CDI episodes (3 and >4); exposure to non-CDI targeted antibiotics; and acid suppressing medications at baseline. Across all subgroups, FMSL-brpk was associated with a lower relative risk of CDI recurrence compared to placebo irrespective of baseline characteristics[69]. Results from this post-hoc analysis illustrate the potential benefit of FMSL-brpk for complex, and at-risk patients for rCDI.
ECOSPOR IV was an open label, single-arm, phase 3 trial conducted in 2 cohorts. Cohort 1 included patients from ECOSPOR III trial who had experienced CDI recurrence within 8 weeks after treatment with FMSL-brpk or placebo. Cohort 2 were de novo patients with at least 1 CDI recurrence. The primary endpoint was safety tolerability up to 24 weeks after dosing. The secondary endpoint was CDI recurrence up to 4, 8,12, and 24 weeks after dosing. The overall incidence of treatment-emergent AEs was 54% , but similar to previous trials most were mild to moderate and gastrointestinal: diarrhea (22.8%), flatulence (7.6%), abdominal pain (6.8%), urinary tract infection (4.9%) and fatigue (4.6)% [70]. Notably none of the urinary tract infections were caused by species included in FMSL-brpk. With respect to efficacy, 8.7% of patients on cohort 1 and 8.1% in cohort 2 had recurrent CDI. The rate of CDI recurrence remained low throughout the 24 weeks, achieving a sustained clinical response rate of 86.3% (95% CI 81.6 – 90.2%) [70]. An analysis by select baseline characteristics demonstrated low rate of CDI recurrence irrespective of age, CDI-antibiotic treatment, sex, or number or prior CDI episodes. ECOSPOR IV confirmed durability of response and safety of FMSL-brpk through 24 weeks.
The FDA approval of FMSL-brpk was largely based on the results of ECOSPOR III which demonstrated a significant reduction of rCDI in patients at increased risk for CDI recurrence and hospital admission which included patients age > 65 years, immunocompromised, malignancy, and GI disorders. While ECOSPOR IV was primarily designed to assess tolerability, results of this trial further supported the approval of FMSL-brpk through its demonstration of durable efficacy and minimal AE profile through 24 weeks. Compared to traditional FMT where routes of delivery vary from nasogastric tube, nasojejunal tube, colonoscopy or retention enema, FMSL-brpk offers a non-invasive, convenient route of oral administration which may be a more comfortable option for microbiota-based therapies to some patients.
VE303
VE303 is a defined consortium product composed of 8 nonpathogenic, nontoxigenic, and commensal strains of Clostridia selected for their ability to provide colonization resistance to C. difficile. Under current good manufacturing processes, it is produced from pure, clonal bacterial cell banks to create a standardized drug product in powdered form intended for oral administration. Unlike FMT, the manufacturing process of VE303 bypasses the need to source directly from donor fecal material of inconsistent composition. VE303 is not currently an FDA approved product, but in May 2023, the US FDA granted Fast Track designation to VE303 for the prevention of rCDI.
VE303 first demonstrated promise in VE303-002, a double-blind placebo-controlled trial. The study included patients with 1 or more prior CDI episodes within 6 months of randomization and included patients with primary CDI at high risk for recurrence defined as age >75 years or age >65 years with at least 1 of the following prespecified risk factor for recurrence: kidney dysfunction, regular use of a proton pump inhibitor, or history of CDI > 6 months previously [71]. This trial was a dose-finding study in which study participants were divided into 3 groups: high dose VE303 (8.0x109 CFs), low dose (1.6 x 109 CFUs), or placebo. VE303 was administered within 24 hours after completing antibiotic treatment. The most robust difference in CDI recurrence was in the high dose VE303 group compared to placebo, 13.8% (4/29) vs 45.5% (10/22), respectively (ARR 30.5%, 90% CI 11% to 52%)[71]. Most patients experienced sustained cure through 24 weeks with only 2 CDI recurrences reported, suggesting a durable effect. No significant difference was found between low dose VE303 and placebo. All recurrences occurred by day 11 in the high dose group. VE303 was generally well tolerated with most treatment related AEs being mild in intensity and primarily gastrointestinal (eg. diarrhea, abdominal pain, flatulence, and vomiting). Importantly, no bacterial infection or AEs of interest were noted in this study. Authors suggested that the absolute risk reduction of 30.5% in the high-dose VE303 group favors comparably to other CDI therapeutic options including FMT (28%), bezlotoxumab (10%), and FM-jslm (12.3%)[71]. The results of VE303-002 are promising and provide the rationale for pursuing high dose VE303 002 in the larger scale phase 3 trial which is still undergoing recruitment.
The phase 3 trial of VE303, RESORATIiVE303, is designed to assess the safety and recurrence rate of CDI at week 8 among study participants who undergo a 14-day treatment with either VE303 or placebo. Results of this trial could lead to changes in the management of CDI by providing a new oral option for CDI.

Table 2.
FDA approved microbiota restoration therapies.
| Fecal microbiota, live-jslm (RebyotaTM) | Fecal microbiota spores, live-brpk (VowstTM) | |
|---|---|---|
| Route | Rectal enema | Oral capsule |
| Dose | Single dose of 150 mL rectally | 4 capsules orally once daily for 3 days |
| Antibiotic wash out period | Administered 24 to 72 hours after CDI antibiotic therapy discontinuation | First dose administered 24 to 72 hours after CDI antibiotic therapy discontinuation |
| Administration | Thaw by placing product in refrigerator (2-8°C) for 24 hours. Patient should empty their bladder and bowel, if possible, prior to administration Keep the patient in the left-side positive or knee-chest position for up to 15 minutes after administration to minimize cramping and expulsion |
Prior to the first dose, patient should drink 296 mL (10 oz) of magnesium citrate (or polyethylene glycol for patients with renal dysfunction) on the day before and at least 8 h prior to taking the first dose Should be administered before the first meal on an empty stomach |
| Storage | Ultracold freezer (-60° to -90°C) -OR- Refrigerator (2° to 8°C) for up to 5 d (including thaw time) **do not freeze after thawing** |
Original packaging at 2° to 25° C **do not freeze** |
Other Preventative Strategies
Over the years, multiple strategies have been deployed to prevent the emergence of C.difficile. The scope of these strategies vary from impact at an individual-level to impact at a population-level. Population based strategies include- establishing antimicrobial stewardship programs and infection prevention programs. The latter relies on non-pharmaceutical based strategy and aims at curtailing the spread of CDI between infected and healthy individuals by isolating infected individuals through established procedures in healthcare settings. In this section, we will discuss pharmaceutical-based strategies to prevent C.difficile infection.
Antimicrobial Stewardship
Antimicrobial Stewardship programs (ASP) aim at ensuring judicious use of antimicrobials across healthcare settings. These programs formulate policies and procedures to optimize use of antimicrobials. The benefits of ASP include improving the local microbial ecology and preventing emergence of multi-drug resistant organisms and C.difficile infection (CDI) at an individual level. Judicious use of antimicrobials results in retention of microbial diversity and increase in colonization resistance against C.diffcile. At our own institution, we have seen an impressive reduction in healthcare acquired CDI as our appropriate antimicrobial usage improved over the years. Over a period of 7 years, i.e., from 2016 through 2023, we saw a 44.1% (1.36 to 0.76) reduction in CDI Standard Infection Ratio (SIR) or a 44.3% (69 cases to 44 cases) reduction in absolute number of CDI cases. At the same time, we saw a 9% improvement in appropriate usage of our broad-spectrum antimicrobials.
Antimicrobial use is pervasive in healthcare settings. Approximately 50% of patients in hospitals receive antimicrobials. Appropriate usage of antimicrobials is lifesaving in conditions like sepsis, which impacts 1.7 million adults in the United States annually [72]. At the same time, incidence of CDI is high at 116 cases per 100,000 persons and 56% of the CDI cases had received antimicrobials in the prior 12 weeks [73]. Therefore, as clinicians, it is helpful to know the risk associated with each class of antibiotics, so we can weigh the risk and benefits in clinical situations to harness maximum benefits of antimicrobials. Intuitively, broader spectrum antibiotics will be associated with a greater risk of CDI compared with narrower spectrum antibiotics. This is supported by a large cohort study in the inpatient setting, where carbapenems had the highest risk, followed closely by piperacillin-tazobactam and cefipime. In the same study, the lowest risk was noted with doxycycline and daptomycin[74]. Similarly, in the outpatient setting, lowest risk of CDI was with doxycycline, minocycline and tetracycline while highest risk was with clindamycin followed by cephalosporins and fluroquinolones [75]. With such granular information, clinicians can ensure responsible use of antimicrobials and prevent CDI.
Probiotics
Probiotics have been studied for primary prevention and secondary prevention of CDI. The results across various randomized controlled trials are conflicting. A Cochrane meta-analysis of 31 RCTs showed probiotics are effective in preventing primary CDI in patients receiving antimicrobials, with a number needed to benefit at 42, with moderate certainty. A post hoc subgroup analysis to explore heterogeneity of the trials, showed benefit with moderate certainty only when CDI baseline risk was more than 5% (NNTB=12). In the US hospitals, typically risk of CDI is less than 5% [76,77]. On the contrary, a multi-center study did not show a beneficial impact of probiotics on primary prevention of CDI [78]. Role of probiotics in secondary prevention is even more controversial. In a meta-analysis, use of probiotics for secondary prevention, did not reach statistical significance to make a firm conclusion[79]. In conclusion, currently available probiotics have not proven to be effective in preventing CDI. This is likely due to the heterogeneity in studies regarding setting (inpatient versus outpatient), probiotic strains, optimal dose along with our limited understanding of the mechanisms by which probiotics exert their action [77].
C. difficile Vaccine
Even though C.difficile has been designated as one of the five urgent threats by the CDC, there is currently no approved vaccine for prevention of primary CDI or recurrent CDI.
A recent phase 3, randomized, placebo-controlled trial to study the efficacy of a three-dose series (0, 1 and 6 months) of PF-06425090 in primary CDI prevention was completed. The candidate vaccine, PF-06425090 is genetically detoxified toxin C.difficile vaccine formulated with modified toxin A and toxin B. This study, also known as the CLOVER study, CLOstridium difficile Vaccine Efficacy tRial, included participants if they were 50 years of age or older and were considered at high risk for CDI. Criteria for high risk included individuals who were in a nursing home or skilled nursing facility, had healthcare exposure in the last year and had received antibiotics in the past 12 weeks. This was a large study with more than 7000 participants in each of arms, vaccine and placebo. The primary end point was the first episode of CDI 14 days or more after dose 3. Following the third dose, 17/7724 developed CDI in the vaccine arm and 25/7818 developed CDI in the placebo arm resulting in a vaccine efficacy of 31% (-38.7 to 66.6). The primary efficacy end point for vaccine efficacy of more than 20% was not met. Adverse events were similar in both groups and ranging from mild to moderate [80].
Several other vaccine candidates are in development including a toxoid-based vaccine is currently in phase 3 clinical trials. In this study, healthy adults who are within the age range of 65 years to 85 years were included. Based on the results thus far, a regimen of three doses (0, 1, 6 months) was well tolerated and induced a robust neutralizing antibody response[81]. Another potential candidate is a protein- based vaccine candidate, VLA 84 is also in the pipeline, though Phase 3 clinical trial has been put on hold for now [82].
Based on prior vaccine work, toxoid-based vaccine will not prevent transmission, hence consideration has been given to non-toxoid based vaccine candidates, such as VLA 84 [82]. At this time, the evidence for vaccine for C.difficile prevention is still in an investigational phase.
Antibiotic Prophylaxis
As the risk of rCDI significantly increases with each subsequent CDI episode, it is important to identify risk factors strongly associated with recurrence and mitigate the risk where feasible. Risk factors most associated with CDI include advanced age, immunocompromised, inflammatory bowel disease, history of prior CDI episode, and administration of systemic antibiotics [25]. While most risks cannot be modified, antibiotic use can be minimized to help prevent recurrence of CDI. However, some antibiotic courses are unavoidable and necessary; therefore, CDI prophylaxis has been pursued as the logical approach to reduce the risk of recurrence in this setting.
The IDSA/SHEA guidelines cite there is insufficient evidence to either extend the duration or restart anti-CDI treatment in the setting of systemic antibiotic therapy for non-CDI indications [25]. Alternatively, the ACG guidelines make conditional recommendations to consider long-term suppressive oral vancomycin in patients with rCDI who are ineligible to receive FMT, who relapsed after FMT, or are requiring ongoing courses of antibiotics. ACG also recommends considering oral vancomycin prophylaxis during systemic antibiotic use for patients at high risk of recurrence [31].
Data regarding C. difficile prophylaxis is largely retrospective and observational in design and therefore at high-risk for bias [83]. Additionally, these studies have heterogenous methodologies including their patient population; indications for use such as primary versus secondary prevention; prophylaxis regimens including antibiotic, dose, and duration; and follow-up requirements. Current data lacks a standardized approach to prophylaxis which limits the clinical utility of their conclusions. Furthermore, the use of antibiotics can disrupt the gut microbiome leading to a loss of diversity predisposing patients to colonization and infection with C. difficile up to 90 days from antibiotic discontinuation. As a result, retrospective, observational studies may be inherently plagued with attrition bias due to shorter follow-up periods that underestimate the rate of CDI [83].
With respect to C. difficile prophylaxis, only 2 RCTs evaluating vancomycin and fidaxomicin have been published and each one evaluated the role of antibiotics as primary prophylaxis. A more recent randomized, prospective, open-label study compared the efficacy of prophylaxis with vancomycin 125 mg once daily during the course of systemic antibiotics continued for 5 days after discontinuation versus no prophylaxis. Patients were considered for prophylaxis if they met one of the following high-risk criteria and were currently receiving systemic antibiotics: aged > 60 years or hospitalized < 30 days prior to index hospitalization and received antibiotics during that prior hospitalization. No CDI events (0/50) occurred in the oral vancomycin prophylaxis group compared to 12% (6/50) in the no prophylaxis group which was evaluated up to 3 months post discharge (p=0.03) [84]. Given concerns with oral vancomycin’s effect on the gut microbiome and the selection and overgrowth of vancomycin-resistant enterococci (VRE), authors of this study also evaluated new VRE colonization defined as isolation of VRE by perirectal swab prior to hospital discharge. No patients developed new VRE colonization. Similarly, a double-blind RCT of fidaxomicin 200 mg daily for prophylaxis of CDI in hematopoietic stem cell transplants receiving fluroquinolone prophylaxis confirmed CDI was significantly lower in fidaxomicin recipients (4.3%) than in placebo (10.7%) during the 60 day follow-up [p=0.0014] [85].
There is limited data to universally recommend antibiotic prophylaxis for either primary or secondary prevention. In the absence of long-term data, antibiotic prophylaxis may be considered on a case-by-case basis if benefit outweighs the risk. Such cases may include elderly and immunocompromised patients with prior history of CDI and are unable to receive microbiota-based therapies. Based on available RCTs, both vancomycin and fidaxomicin are promising prophylactic strategies that have reduced CDI in high-risk patients. While more evidence exists for vancomycin, fidaxomicin is a narrower spectrum agent with less disruption to the gut microbiome and is associated with a lower rate of recurrence. Additionally, previous studies have demonstrated prolonged vancomycin use may be associated with complications such as subsequent Candida spp. and enteric bacterial bloodstream infections [86]. Therefore, fidaxomicin may be the preferred option to minimize alterations to intestinal microbiota [86]. While optimal prophylactic dosing is still to be elucidated, generally one aims to use the smallest, effective dose. Based on RCTs, the most reasonable dosing options are the following: oral vancomycin 125 mg daily or fidaxomicin 200 mg daily for the duration of the systemic antibiotic course.
Conclusion and Future Directions
Since its discovery in 1935, C. difficile has become a leading cause of healthcare associated infections in the US, increasing morbidity and mortality of patients in healthcare settings. Antibiotic exposure is one such modifiable risk factor for CDI. Consequently, at a population level, effective implementation of antimicrobial stewardship program can be useful in preventing C. difficile infection. Stewardship interventions limit the use of unnecessary antimicrobials and minimizes the frequency, duration and number of antimicrobials prescribed to help reduce the risk of CDI.
Once CDI is diagnosed, it is imperative to distinguish disease severity and number of prior CDI occurrences as it can determine how it is treated (See Figure 2). In addition to standard of care antibiotics, monoclonal antibodies like bezolotoxumab have been developed to reduce rCDI and can be considered in patients with risk factors for recurrence such as >65 years, immunocompromised, severe CDI, or prior CDI in previous 6 months. Patients with 2 or more episodes of CDI are at a higher risk of recurrence, with rCDI occurring upwards of 65%. Management can be challenging in this setting as standard-of-care antibiotics for CDI can further disrupt the gut microbiome. Therefore, microbiota restoration therapies should be explored. While FMT, is the only guideline directed option, newer live biotherapeutic options have been FDA approved since guidelines were last updated. Fecal microbiota, live-jslm and fecal microbiota spores, live-brpk offer a safe, standardized, and more convenient approach to microbiota-based therapies compared to FMT. Real-world experience with these new agents will help determine its place in therapy.
To have a true impact on the huge morbidity associated with CDI and rCDI, our emphasis needs to shift from treatment strategies to prevention strategies. As our understanding of the pathogenesis of CDI evolves, we should aim to identify microbial signatures in the gut that represent an unhealthy microbiome and would predispose to CDI. If we can identify such microbial signatures early, especially in our vulnerable population, we could leverage preventive strategies like C.difficile vaccine and probiotics to prevent emergence of CDI. At this time, for both these preventive strategies, the evidence is either not definitive or in the investigational phase. However, as our understanding of the factors associated with gut dysbiosis matures, these preventive strategies (along with others) can be leveraged to reduce the C.difficile associated morbidity and ultimately eliminate C.difficile from the CDC urgent threat list.
Author Contributions
Both authors, FM and NN have contributed equally to the manuscript.
Funding
No funding was received for this work.
Acknowledgments
None.
Conflicts of Interest
The authors report no conflict of interest.
References
- Snyder, m. Further Studies on Bacillus Dificilis (Jall and O'Toole). The Journal of Infectious Diseases 1937, 60, 223-231.
- Lessa, F.C.; Mu, Y.; Bamberg, W.M.; Beldavs, Z.G.; Dumyati, G.K.; Dunn, J.R.; Farley, M.M.; Holzbauer, S.M.; Meek, J.I.; Phipps, E.C., et al. Burden of Clostridium difficile infection in the United States. N Engl J Med 2015, 372, 825-834. [CrossRef]
- Prevention, C.f.D.C.a. Antibitoic Resistance Threats in the United States 2019. US Department of Health and Human Services, Centers for Diseae Control and Prevention 2019.
- Deshpande, A.; Pasupuleti, V.; Thota, P.; Pant, C.; Rolston, D.D.; Hernandez, A.V.; Donskey, C.J.; Fraser, T.G. Risk factors for recurrent Clostridium difficile infection: a systematic review and meta-analysis. Infect Control Hosp Epidemiol 2015, 36, 452-460. [CrossRef]
- Czepiel, J.; Drozdz, M.; Pituch, H.; Kuijper, E.J.; Perucki, W.; Mielimonka, A.; Goldman, S.; Wultanska, D.; Garlicki, A.; Biesiada, G. Clostridium difficile infection: review. Eur J Clin Microbiol Infect Dis 2019, 38, 1211-1221. [CrossRef]
- Guery, B.; Menichetti, F.; Anttila, V.J.; Adomakoh, N.; Aguado, J.M.; Bisnauthsing, K.; Georgopali, A.; Goldenberg, S.D.; Karas, A.; Kazeem, G., et al. Extended-pulsed fidaxomicin versus vancomycin for Clostridium difficile infection in patients 60 years and older (EXTEND): a randomised, controlled, open-label, phase 3b/4 trial. Lancet Infect Dis 2018, 18, 296-307. [CrossRef]
- Juo, Y.Y.; Sanaiha, Y.; Jabaji, Z.; Benharash, P. Trends in Diverting Loop Ileostomy vs Total Abdominal Colectomy as Surgical Management for Clostridium difficile Colitis. JAMA Surg 2019, 154, 899-906. [CrossRef]
- Kwon, J.H.; Olsen, M.A.; Dubberke, E.R. The morbidity, mortality, and costs associated with Clostridium difficile infection. Infect Dis Clin North Am 2015, 29, 123-134. [CrossRef]
- Appaneal, H.J.; Caffrey, A.R.; Beganovic, M.; Avramovic, S.; LaPlante, K.L. Predictors of Mortality Among a National Cohort of Veterans With Recurrent Clostridium difficile Infection. Open Forum Infect Dis 2018, 5, ofy175. [CrossRef]
- Zimlichman, E.; Henderson, D.; Tamir, O.; Franz, C.; Song, P.; Yamin, C.K.; Keohane, C.; Denham, C.R.; Bates, D.W. Health care-associated infections: a meta-analysis of costs and financial impact on the US health care system. JAMA Intern Med 2013, 173, 2039-2046. [CrossRef]
- Teasley, D.G.; Gerding, D.N.; Olson, M.M.; Peterson, L.R.; Gebhard, R.L.; Schwartz, M.J.; Lee, J.T., Jr. Prospective randomised trial of metronidazole versus vancomycin for Clostridium-difficile-associated diarrhoea and colitis. Lancet 1983, 2, 1043-1046. [CrossRef]
- Wenisch, C.; Parschalk, B.; Hasenhundl, M.; Hirschl, A.M.; Graninger, W. Comparison of vancomycin, teicoplanin, metronidazole, and fusidic acid for the treatment of Clostridium difficile-associated diarrhea. Clin Infect Dis 1996, 22, 813-818. [CrossRef]
- Belmares, J.; Gerding, D.N.; Parada, J.P.; Miskevics, S.; Weaver, F.; Johnson, S. Outcome of metronidazole therapy for Clostridium difficile disease and correlation with a scoring system. J Infect 2007, 55, 495-501. [CrossRef]
- Brazier, J.S.; Raybould, R.; Patel, B.; Duckworth, G.; Pearson, A.; Charlett, A.; Duerden, B.I.; Network, H.P.A.R.M. Distribution and antimicrobial susceptibility patterns of Clostridium difficile PCR ribotypes in English hospitals, 2007-08. Euro Surveill 2008, 13. [CrossRef]
- Peng, Z.; Jin, D.; Kim, H.B.; Stratton, C.W.; Wu, B.; Tang, Y.W.; Sun, X. Update on Antimicrobial Resistance in Clostridium difficile: Resistance Mechanisms and Antimicrobial Susceptibility Testing. J Clin Microbiol 2017, 55, 1998-2008. [CrossRef]
- Zar, F.A.; Bakkanagari, S.R.; Moorthi, K.M.; Davis, M.B. A comparison of vancomycin and metronidazole for the treatment of Clostridium difficile-associated diarrhea, stratified by disease severity. Clin Infect Dis 2007, 45, 302-307. [CrossRef]
- Cohen, S.H.; Gerding, D.N.; Johnson, S.; Kelly, C.P.; Loo, V.G.; McDonald, L.C.; Pepin, J.; Wilcox, M.H.; Society for Healthcare Epidemiology of, A.; Infectious Diseases Society of, A. Clinical practice guidelines for Clostridium difficile infection in adults: 2010 update by the society for healthcare epidemiology of America (SHEA) and the infectious diseases society of America (IDSA). Infect Control Hosp Epidemiol 2010, 31, 431-455. [CrossRef]
- Johnson, S.; Louie, T.J.; Gerding, D.N.; Cornely, O.A.; Chasan-Taber, S.; Fitts, D.; Gelone, S.P.; Broom, C.; Davidson, D.M.; Polymer Alternative for, C.D.I.T.i. Vancomycin, metronidazole, or tolevamer for Clostridium difficile infection: results from two multinational, randomized, controlled trials. Clin Infect Dis 2014, 59, 345-354. [CrossRef]
- Stevens, V.W.; Nelson, R.E.; Schwab-Daugherty, E.M.; Khader, K.; Jones, M.M.; Brown, K.A.; Greene, T.; Croft, L.D.; Neuhauser, M.; Glassman, P., et al. Comparative Effectiveness of Vancomycin and Metronidazole for the Prevention of Recurrence and Death in Patients With Clostridium difficile Infection. JAMA Intern Med 2017, 177, 546-553. [CrossRef]
- Thorpe, C.M.; Kane, A.V.; Chang, J.; Tai, A.; Vickers, R.J.; Snydman, D.R. Enhanced preservation of the human intestinal microbiota by ridinilazole, a novel Clostridium difficile-targeting antibacterial, compared to vancomycin. PLoS One 2018, 13, e0199810. [CrossRef]
- Gonzales, M.; Pepin, J.; Frost, E.H.; Carrier, J.C.; Sirard, S.; Fortier, L.C.; Valiquette, L. Faecal pharmacokinetics of orally administered vancomycin in patients with suspected Clostridium difficile infection. BMC Infect Dis 2010, 10, 363. [CrossRef]
- Thabit, A.K.; Nicolau, D.P. Impact of vancomycin faecal concentrations on clinical and microbiological outcomes in Clostridium difficile infection. Int J Antimicrob Agents 2015, 46, 205-208. [CrossRef]
- Thorpe, C.M.; McDermott, L.A.; Tran, M.K.; Chang, J.; Jenkins, S.G.; Goldstein, E.J.C.; Patel, R.; Forbes, B.A.; Johnson, S.; Gerding, D.N., et al. U.S.-Based National Surveillance for Fidaxomicin Susceptibility of Clostridioides difficile-Associated Diarrheal Isolates from 2013 to 2016. Antimicrob Agents Chemother 2019, 63. [CrossRef]
- Fernandez, A.; Anand, G.; Friedenberg, F. Factors associated with failure of metronidazole in Clostridium difficile-associated disease. J Clin Gastroenterol 2004, 38, 414-418. [CrossRef]
- McDonald, L.C.; Gerding, D.N.; Johnson, S.; Bakken, J.S.; Carroll, K.C.; Coffin, S.E.; Dubberke, E.R.; Garey, K.W.; Gould, C.V.; Kelly, C., et al. Clinical Practice Guidelines for Clostridium difficile Infection in Adults and Children: 2017 Update by the Infectious Diseases Society of America (IDSA) and Society for Healthcare Epidemiology of America (SHEA). Clin Infect Dis 2018, 66, e1-e48. [CrossRef]
- Louie, T.J.; Miller, M.A.; Mullane, K.M.; Weiss, K.; Lentnek, A.; Golan, Y.; Gorbach, S.; Sears, P.; Shue, Y.K.; Group, O.P.T.C.S. Fidaxomicin versus vancomycin for Clostridium difficile infection. N Engl J Med 2011, 364, 422-431. [CrossRef]
- Cornely, O.A.; Crook, D.W.; Esposito, R.; Poirier, A.; Somero, M.S.; Weiss, K.; Sears, P.; Gorbach, S.; Group, O.P.T.C.S. Fidaxomicin versus vancomycin for infection with Clostridium difficile in Europe, Canada, and the USA: a double-blind, non-inferiority, randomised controlled trial. Lancet Infect Dis 2012, 12, 281-289. [CrossRef]
- Okumura, H.; Fukushima, A.; Taieb, V.; Shoji, S.; English, M. Fidaxomicin compared with vancomycin and metronidazole for the treatment of Clostridioides (Clostridium) difficile infection: A network meta-analysis. J Infect Chemother 2020, 26, 43-50. [CrossRef]
- Mikamo, H.; Tateda, K.; Yanagihara, K.; Kusachi, S.; Takesue, Y.; Miki, T.; Oizumi, Y.; Gamo, K.; Hashimoto, A.; Toyoshima, J., et al. Efficacy and safety of fidaxomicin for the treatment of Clostridioides (Clostridium) difficile infection in a randomized, double-blind, comparative Phase III study in Japan. J Infect Chemother 2018, 24, 744-752. [CrossRef]
- Venugopal, A.A.; Johnson, S. Fidaxomicin: a novel macrocyclic antibiotic approved for treatment of Clostridium difficile infection. Clin Infect Dis 2012, 54, 568-574. [CrossRef]
- Kelly, C.R.; Fischer, M.; Allegretti, J.R.; LaPlante, K.; Stewart, D.B.; Limketkai, B.N.; Stollman, N.H. ACG Clinical Guidelines: Prevention, Diagnosis, and Treatment of Clostridioides difficile Infections. Am J Gastroenterol 2021, 116, 1124-1147. [CrossRef]
- Cornely, O.A.; Miller, M.A.; Louie, T.J.; Crook, D.W.; Gorbach, S.L. Treatment of first recurrence of Clostridium difficile infection: fidaxomicin versus vancomycin. Clin Infect Dis 2012, 55 Suppl 2, S154-161. [CrossRef]
- Hota, S.S.; Sales, V.; Tomlinson, G.; Salpeter, M.J.; McGeer, A.; Coburn, B.; Guttman, D.S.; Low, D.E.; Poutanen, S.M. Oral Vancomycin Followed by Fecal Transplantation Versus Tapering Oral Vancomycin Treatment for Recurrent Clostridium difficile Infection: An Open-Label, Randomized Controlled Trial. Clin Infect Dis 2017, 64, 265-271. [CrossRef]
- Khanna, S. My Treatment Approach to Clostridioides difficile Infection. Mayo Clinic Proceedings 2021, 10.1016. [CrossRef]
- Fekety, R.; Silva, J.; Kauffman, C.; Buggy, B.; Deery, H.G. Treatment of antibiotic-associated Clostridium difficile colitis with oral vancomycin: comparison of two dosage regimens. Am J Med 1989, 86, 15-19. [CrossRef]
- Lam, S.W.; Bass, S.N.; Neuner, E.A.; Bauer, S.R. Effect of vancomycin dose on treatment outcomes in severe Clostridium difficile infection. Int J Antimicrob Agents 2013, 42, 553-558. [CrossRef]
- Ng, Q.X.; Loke, W.; Foo, N.X.; Mo, Y.; Yeo, W.S.; Soh, A.Y.S. A systematic review of the use of rifaximin for Clostridium difficile infections. Anaerobe 2019, 55, 35-39. [CrossRef]
- Garey, K.W.; Ghantoji, S.S.; Shah, D.N.; Habib, M.; Arora, V.; Jiang, Z.D.; DuPont, H.L. A randomized, double-blind, placebo-controlled pilot study to assess the ability of rifaximin to prevent recurrent diarrhoea in patients with Clostridium difficile infection. J Antimicrob Chemother 2011, 66, 2850-2855. [CrossRef]
- Finegold, S.M.; Molitoris, D.; Vaisanen, M.L. Study of the in vitro activities of rifaximin and comparator agents against 536 anaerobic intestinal bacteria from the perspective of potential utility in pathology involving bowel flora. Antimicrob Agents Chemother 2009, 53, 281-286. [CrossRef]
- Kechagias, K.S.; Chorepsima, S.; Triarides, N.A.; Falagas, M.E. Tigecycline for the treatment of patients with Clostridium difficile infection: an update of the clinical evidence. Eur J Clin Microbiol Infect Dis 2020, 39, 1053-1058. [CrossRef]
- Larson, K.C.; Belliveau, P.P.; Spooner, L.M. Tigecycline for the treatment of severe Clostridium difficile infection. Ann Pharmacother 2011, 45, 1005-1010. [CrossRef]
- Manea, E.; Sojo-Dorado, J.; Jipa, R.E.; Benea, S.N.; Rodriguez-Bano, J.; Hristea, A. The role of tigecycline in the management of Clostridium difficile infection: a retrospective cohort study. Clin Microbiol Infect 2018, 24, 180-184. [CrossRef]
- Herpers, B.L.; Vlaminckx, B.; Burkhardt, O.; Blom, H.; Biemond-Moeniralam, H.S.; Hornef, M.; Welte, T.; Kuijper, E.J. Intravenous tigecycline as adjunctive or alternative therapy for severe refractory Clostridium difficile infection. Clin Infect Dis 2009, 48, 1732-1735. [CrossRef]
- Gergely Szabo, B.; Kadar, B.; Szidonia Lenart, K.; Dezsenyi, B.; Kunovszki, P.; Fried, K.; Kamotsay, K.; Nikolova, R.; Prinz, G. Use of intravenous tigecycline in patients with severe Clostridium difficile infection: a retrospective observational cohort study. Clin Microbiol Infect 2016, 22, 990-995. [CrossRef]
- Bezlotoxumab [package insert]. Merck: 2016.
- Wilcox, M.H.; Gerding, D.N.; Poxton, I.R.; Kelly, C.; Nathan, R.; Birch, T.; Cornely, O.A.; Rahav, G.; Bouza, E.; Lee, C., et al. Bezlotoxumab for Prevention of Recurrent Clostridium difficile Infection. N Engl J Med 2017, 376, 305-317. [CrossRef]
- Gerding, D.N.; Kelly, C.P.; Rahav, G.; Lee, C.; Dubberke, E.R.; Kumar, P.N.; Yacyshyn, B.; Kao, D.; Eves, K.; Ellison, M.C., et al. Bezlotoxumab for Prevention of Recurrent Clostridium difficile Infection in Patients at Increased Risk for Recurrence. Clin Infect Dis 2018, 67, 649-656. [CrossRef]
- Birch, T.; Golan, Y.; Rizzardini, G.; Jensen, E.; Gabryelski, L.; Guris, D.; Dorr, M.B. Efficacy of bezlotoxumab based on timing of administration relative to start of antibacterial therapy for Clostridium difficile infection. J Antimicrob Chemother 2018, 73, 2524-2528. [CrossRef]
- Wang, J.W.; Kuo, C.H.; Kuo, F.C.; Wang, Y.K.; Hsu, W.H.; Yu, F.J.; Hu, H.M.; Hsu, P.I.; Wang, J.Y.; Wu, D.C. Fecal microbiota transplantation: Review and update. J Formos Med Assoc 2019, 118 Suppl 1, S23-S31. [CrossRef]
- van Nood, E.; Vrieze, A.; Nieuwdorp, M.; Fuentes, S.; Zoetendal, E.G.; de Vos, W.M.; Visser, C.E.; Kuijper, E.J.; Bartelsman, J.F.; Tijssen, J.G., et al. Duodenal infusion of donor feces for recurrent Clostridium difficile. N Engl J Med 2013, 368, 407-415. [CrossRef]
- Minkoff, N.Z.; Aslam, S.; Medina, M.; Tanner-Smith, E.E.; Zackular, J.P.; Acra, S.; Nicholson, M.R.; Imdad, A. Fecal microbiota transplantation for the treatment of recurrent Clostridioides difficile (Clostridium difficile). Cochrane Database Syst Rev 2023, 4, CD013871. [CrossRef]
- Porcari, S.; Benech, N.; Valles-Colomer, M.; Segata, N.; Gasbarrini, A.; Cammarota, G.; Sokol, H.; Ianiro, G. Key determinants of success in fecal microbiota transplantation: From microbiome to clinic. Cell Host Microbe 2023, 31, 712-733. [CrossRef]
- Yadegar, A.; Pakpoor, S.; Ibrahim, F.F.; Nabavi-Rad, A.; Cook, L.; Walter, J.; Seekatz, A.M.; Wong, K.; Monaghan, T.M.; Kao, D. Beneficial effects of fecal microbiota transplantation in recurrent Clostridioides difficile infection. Cell Host Microbe 2023, 31, 695-711. [CrossRef]
- Carlson, P.E., Jr. Regulatory Considerations for Fecal Microbiota Transplantation Products. Cell Host Microbe 2020, 27, 173-175. [CrossRef]
- Lavoie, T.; Appaneal, H.J.; LaPlante, K.L. Advancements in Novel Live Biotherapeutic Products for Clostridioides difficile Infection Prevention. Clin Infect Dis 2023, 77, S447-S454. [CrossRef]
- Fecal Microbiota for Transplantation: Safety Alert - Risk fo Serious Adverse Events Likely Due to Transmission of Pathogenic Organisms. US Food and Drug Administration: 2020.
- Hunt, A.; Drwiega, E.; Wang, Y.; Danziger, L. A review of fecal microbiota, live-jslm for the prevention of recurrent Clostridioides difficile infection. Am J Health Syst Pharm 2024, 81, e402-e411. [CrossRef]
- fecal microbiota, live-jslm (Rebyota) [package insert]. Ferring Pharmaceuticals.
- Feuerstadt, P.; Crawford, C.V.; Tan, X.; Pokhilko, V.; Bancke, L.; Ng, S.; Guthmueller, B.; Bidell, M.R.; Tillotson, G.; Johnson, S., et al. Fecal Microbiota, Live-jslm for the Prevention of Recurrent Clostridioides difficile Infection : Subgroup Analysis of PUNCH CD2 and PUNCH CD3. J Clin Gastroenterol 2024, 58, 818-824. [CrossRef]
- Khanna, S.; Assi, M.; Lee, C.; Yoho, D.; Louie, T.; Knapple, W.; Aguilar, H.; Garcia-Diaz, J.; Wang, G.P.; Berry, S.M., et al. Efficacy and Safety of RBX2660 in PUNCH CD3, a Phase III, Randomized, Double-Blind, Placebo-Controlled Trial with a Bayesian Primary Analysis for the Prevention of Recurrent Clostridioides difficile Infection. Drugs 2022, 82, 1527-1538. [CrossRef]
- Orenstein, R.; Dubberke, E.; Hardi, R.; Ray, A.; Mullane, K.; Pardi, D.S.; Ramesh, M.S.; Investigators, P.C. Safety and Durability of RBX2660 (Microbiota Suspension) for Recurrent Clostridium difficile Infection: Results of the PUNCH CD Study. Clin Infect Dis 2016, 62, 596-602. [CrossRef]
- Dubberke, E.R.; Orenstein, R.; Khanna, S.; Guthmueller, B.; Lee, C. Final Results from a Phase 2b Randomized, Placebo-Controlled Clinical Trial of RBX2660: A Microbiota-Based Drug for the Prevention of Recurrent Clostridioides difficile Infection. Infect Dis Ther 2023, 12, 703-709. [CrossRef]
- Feuerstadt, P.; Chopra, T.; Knapple, W.; Van Hise, N.W.; Dubberke, E.R.; Baggott, B.; Guthmueller, B.; Bancke, L.; Gamborg, M.; Steiner, T.S., et al. PUNCH CD3-OLS: a phase 3 prospective observational cohort study to evaluate the safety and efficacy of fecal microbiota, live-jslm (REBYOTA) in adults with recurrent Clostridioides difficile infection. Clin Infect Dis 2024. [CrossRef]
- Blair, H.A. SER-109 (VOWST()): A Review in the Prevention of Recurrent Clostridioides difficile Infection. Drugs 2024, 84, 329-336. [CrossRef]
- Feuerstadt, P.; Louie, T.J.; Lashner, B.; Wang, E.E.L.; Diao, L.; Bryant, J.A.; Sims, M.; Kraft, C.S.; Cohen, S.H.; Berenson, C.S., et al. SER-109, an Oral Microbiome Therapy for Recurrent Clostridioides difficile Infection. N Engl J Med 2022, 386, 220-229. [CrossRef]
- Fecal microbiota spors, live-brpk (Vowst) [package insert]. Seres Therapeutics, Inc: 2023.
- McGovern, B.H.; Ford, C.B.; Henn, M.R.; Pardi, D.S.; Khanna, S.; Hohmann, E.L.; O'Brien, E.J.; Desjardins, C.A.; Bernardo, P.; Wortman, J.R., et al. SER-109, an Investigational Microbiome Drug to Reduce Recurrence After Clostridioides difficile Infection: Lessons Learned From a Phase 2 Trial. Clin Infect Dis 2021, 72, 2132-2140. [CrossRef]
- Cohen, S.H.; Louie, T.J.; McGovern, B.H. Extended Follow-up of Microbiome Therapeutic SER-109 for Recurrent Clostridioides difficile Infection-Reply. JAMA 2023, 329, 1033-1034. [CrossRef]
- Berenson, C.S.; Lashner, B.; Korman, L.Y.; Hohmann, E.; Deshpande, A.; Louie, T.J.; Sims, M.; Pardi, D.; Kraft, C.S.; Wang, E.E.L., et al. Prevalence of Comorbid Factors in Patients With Recurrent Clostridioides difficile Infection in ECOSPOR III, a Randomized Trial of an Oral Microbiota-Based Therapeutic. Clin Infect Dis 2023, 77, 1504-1510. [CrossRef]
- Sims, M.D.; Khanna, S.; Feuerstadt, P.; Louie, T.J.; Kelly, C.R.; Huang, E.S.; Hohmann, E.L.; Wang, E.E.L.; Oneto, C.; Cohen, S.H., et al. Safety and Tolerability of SER-109 as an Investigational Microbiome Therapeutic in Adults With Recurrent Clostridioides difficile Infection: A Phase 3, Open-Label, Single-Arm Trial. JAMA Netw Open 2023, 6, e2255758. [CrossRef]
- Louie, T.; Golan, Y.; Khanna, S.; Bobilev, D.; Erpelding, N.; Fratazzi, C.; Carini, M.; Menon, R.; Ruisi, M.; Norman, J.M., et al. VE303, a Defined Bacterial Consortium, for Prevention of Recurrent Clostridioides difficile Infection: A Randomized Clinical Trial. JAMA 2023, 329, 1356-1366. [CrossRef]
- Magill, S.S.; Edwards, J.R.; Beldavs, Z.G.; Dumyati, G.; Janelle, S.J.; Kainer, M.A.; Lynfield, R.; Nadle, J.; Neuhauser, M.M.; Ray, S.M., et al. Prevalence of antimicrobial use in US acute care hospitals, May-September 2011. JAMA 2014, 312, 1438-1446. [CrossRef]
- Centers for Disease Control and Prevention. 2024. Emerging Infections Programs, healthcare-Associated Infections-Community Interface Surveillance Report, Clostridioides difficile infection (CDI). 2022.
- Webb, B.J.; Subramanian, A.; Lopansri, B.; Goodman, B.; Jones, P.B.; Ferraro, J.; Stenehjem, E.; Brown, S.M. Antibiotic Exposure and Risk for Hospital-Associated Clostridioides difficile Infection. Antimicrob Agents Chemother 2020, 64. [CrossRef]
- Miller, A.C.; Arakkal, A.T.; Sewell, D.K.; Segre, A.M.; Tholany, J.; Polgreen, P.M.; Group, C.D.C.M.-H. Comparison of Different Antibiotics and the Risk for Community-Associated Clostridioides difficile Infection: A Case-Control Study. Open Forum Infect Dis 2023, 10, ofad413. [CrossRef]
- Goldenberg, J.Z.; Yap, C.; Lytvyn, L.; Lo, C.K.; Beardsley, J.; Mertz, D.; Johnston, B.C. Probiotics for the prevention of Clostridium difficile-associated diarrhea in adults and children. Cochrane Database Syst Rev 2017, 12, CD006095. [CrossRef]
- Goldenberg, J.Z.; Mertz, D.; Johnston, B.C. Probiotics to Prevent Clostridium difficile Infection in Patients Receiving Antibiotics. JAMA 2018, 320, 499-500. [CrossRef]
- Heil, E.L.; Harris, A.D.; Brown, C.; Seung, H.; Thom, K.A.; von Rosenvinge, E.; Sorongon, S.; Pineles, L.; Goodman, K.E.; Leekha, S. A Multicenter Evaluation of Probiotic Use for the Primary Prevention of Clostridioides difficile Infection. Clin Infect Dis 2021, 73, 1330-1337. [CrossRef]
- McFarland, L.V. Probiotics for the Primary and Secondary Prevention of C. difficile Infections: A Meta-analysis and Systematic Review. Antibiotics (Basel) 2015, 4, 160-178. [CrossRef]
- Donskey, C.J.; Dubberke, E.R.; Klein, N.P.; Liles, E.G.; Szymkowiak, K.; Wilcox, M.H.; Lawrence, J.; Bouguermouh, S.; Zhang, H.; Koury, K., et al. CLOVER: A Phase 3 Randomized Trial Investigating the Efficacy and Safety of a Detoxified Toxin A/B Vaccine in Adults 50 Years and Older at Increased Risk of Clostridioides difficile Infection. Clin Infect Dis 2024. [CrossRef]
- Christensen, S.; Bouguermouh, S.; Ilangovan, K.; Pride, M.W.; Webber, C.; Lockhart, S.P.; Shah, R.; Kitchin, N.; Lamberth, E.; Zhang, H., et al. A phase 3 study evaluating the lot consistency, immunogenicity, safety, and tolerability of a Clostridioides difficile vaccine in healthy adults 65 to 85 years of age. Vaccine 2023, 41, 7548-7559. [CrossRef]
- Razim, A.; Gorska, S.; Gamian, A. Non-Toxin-Based Clostridioides difficile Vaccination Approaches. Pathogens 2023, 12. [CrossRef]
- Carlson, T.J.; Gonzales-Luna, A.J. Utilizing antibiotics to prevent Clostridioides difficile infection: does exposure to a risk factor decrease risk? A systematic review. J Antimicrob Chemother 2020, 75, 2735-2742. [CrossRef]
- Johnson, S.W.; Brown, S.V.; Priest, D.H. Effectiveness of Oral Vancomycin for Prevention of Healthcare Facility-Onset Clostridioides difficile Infection in Targeted Patients During Systemic Antibiotic Exposure. Clin Infect Dis 2020, 71, 1133-1139. [CrossRef]
- Mullane, K.M.; Winston, D.J.; Nooka, A.; Morris, M.I.; Stiff, P.; Dugan, M.J.; Holland, H.; Gregg, K.; Adachi, J.A.; Pergam, S.A., et al. A Randomized, Placebo-controlled Trial of Fidaxomicin for Prophylaxis of Clostridium difficile-associated Diarrhea in Adults Undergoing Hematopoietic Stem Cell Transplantation. Clin Infect Dis 2019, 68, 196-203. [CrossRef]
- Reigadas, E.; van Prehn, J.; Falcone, M.; Fitzpatrick, F.; Vehreschild, M.; Kuijper, E.J.; Bouza, E.; European Society of Clinical, M.; Infectious Diseases Study Group on Clostridioides, d.; Study Group for, H., et al. How to: prophylactic interventions for prevention of Clostridioides difficile infection. Clin Microbiol Infect 2021, 27, 1777-1783. [CrossRef]
Figure 1.
Literature Review Flow Diagram.
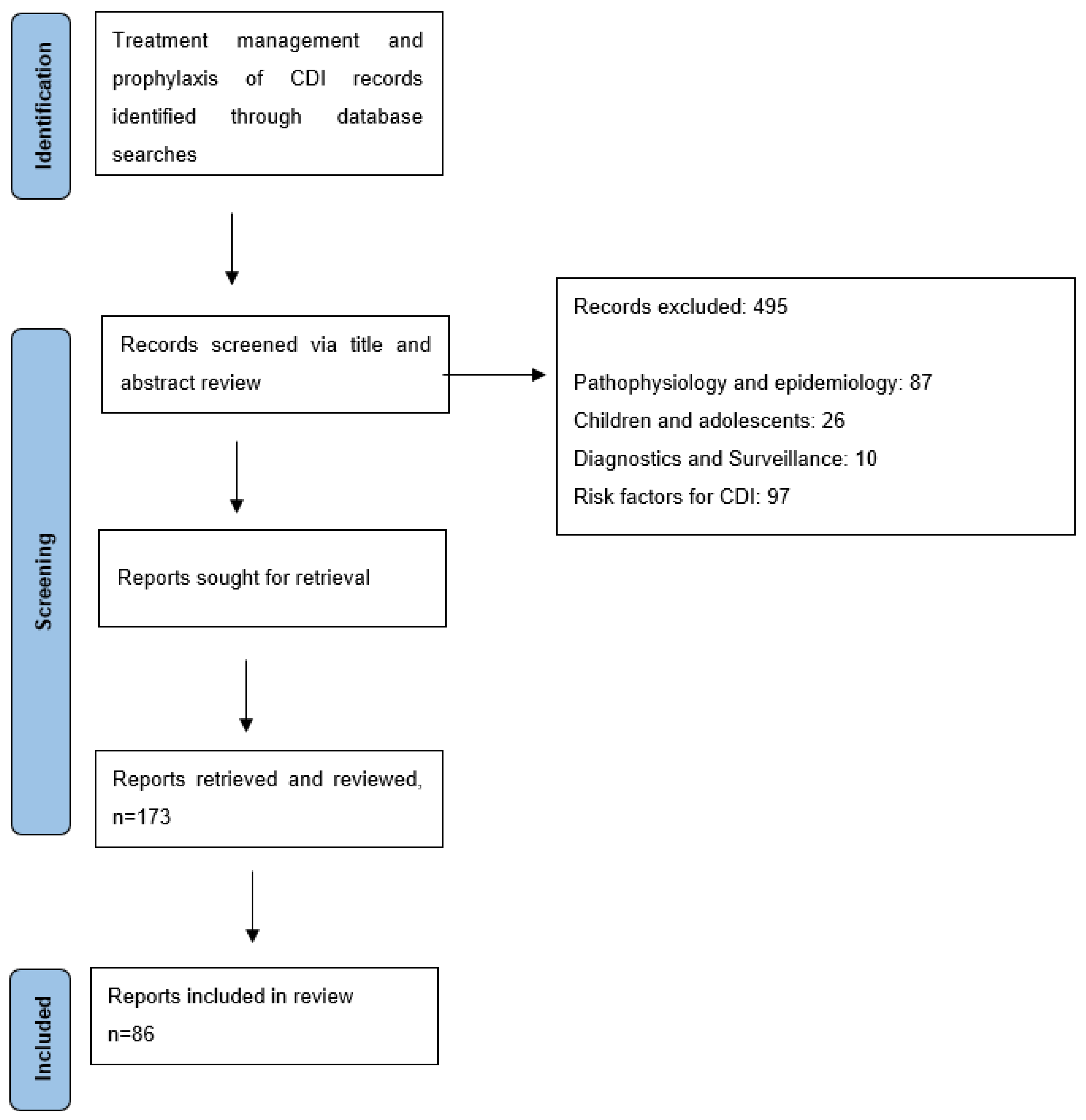
Figure 2.
Treatment Options for CDI based on Severity and Number of prior CDI Episodes.
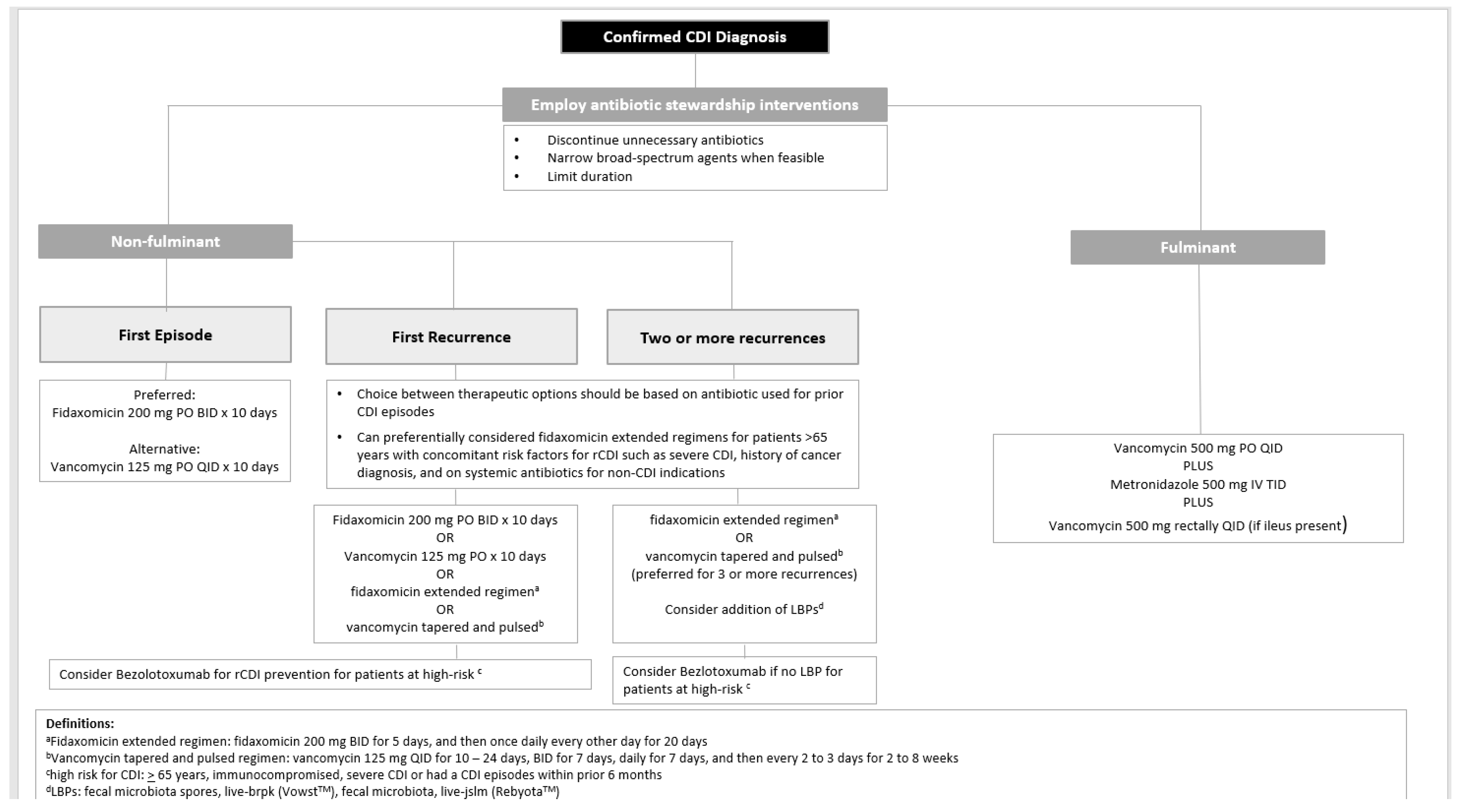
Table 1.
2017 and 2021 IDSA/SHEA and 2021 ACG Treatment Recommendations for Adult Patients with CDI.
Table 1.
2017 and 2021 IDSA/SHEA and 2021 ACG Treatment Recommendations for Adult Patients with CDI.
| IDSA/SHEA | ACG | |
|---|---|---|
| Initial CDI episode | Fidaxomicin 200 mg BID for 10 days (preferred) -OR- Vancomycin 125 mg QID for 10 days -OR- Metronidazole 500 mg TID for 10-14 days (non-severe CDI only and if vancomycin or fidaxomicin is unavailable) Adjunctive: bezlotoxumab 10 mg/kg IV oncea |
Non-Severe Vancomycin 125 mg QID for 10 days -OR- Fidaxomicin 200 mg BID for 10 days -OR- Metronidazole 500 mg TID for 10 days (low risk patientsc) Severe Vancomycin 125 mg QID for 10 days -OR- Fidaxomicin 200 mg BID for 10 days -OR- FMTd Adjunctive: bezlotoxumab 10mg/kg IV onceb |
| First recurrence | Fidaxomicin 200 mg BID for 10 days (preferred) -OR- Fidaxomicin 200 mg BID for 5 days, and then once daily every other day for 20 days (preferred) -OR- Vancomycin tapered and pulsed (eg. 125 mg QID for 10-14 days, BID for 7 days, daily for 7 days, and then every 2 to 3 days for 2 to 8 weeks) -OR- Vancomycin 125 mg QID for 10 days (if metronidazole was used for primary infection) Adjunctive: bezlotoxumab 10 mg/kg IV oncea |
Vancomycin tapered and pulsed -OR- Fidaxomicin 200 mg BID for 10 days (unless fidaxomicin was used for primary infection) Adjunctive: bezlotoxumab 10mg/kg IV onceb |
| Second or subsequent recurrence | Fidaxomicin 200 mg BID for 10 days -OR- Fidaxomicin 200 mg BID for 5 days, and then once daily every other day for 20 days -OR- Vancomycin tapered and pulsed (eg. 125 mg QID for 10-14 days, BID for 7 days, daily for 7 days, and then every 2 to 3 days for 2 to 8 weeks) -OR- Vancomycin 125 mg QID for 10 days followed by rifaximin 400 mg TID for 20 days -OR- FMT Adjunctive: bezlotoxumab 10 mg/kg IV oncea |
FMT Adjunctive: bezlotoxumab 10mg/kg IV once |
| Fulminant CDI | Vancomycin 500 QID -PLUS- Metronidazole IV 500 mg TID -PLUS- Vancomycin rectal 500 mg in 100 mL 0.9% sodium chloride QID (if ileus present) |
Vancomycin 500 QID for the first 48-72 hours, followed by 125 mg QID -PLUS- Metronidazole IV 500 mg TID -PLUS- Vancomycin rectal 500 mg in 100 mL 0.9% sodium chloride QID (if ileus present) -OR- FMTd |
a IDSA/SHEA recommends considering the addition of bezlotoxumab in patients who are age > 65 years, are immunocompromised, have severe CDI or had a CDI episodes within prior 6 months. b ACG recommends considering bezlotoxumab in patients who are age > 65 years and have one of the following risk factors for recurrence: CDI episode within prior 6 months, immunocompromised or severe CDI. cLow risk patients defined as younger outpatients with minimal comorbidities. dACG recommends considering FMT for patients with CDI refractory to antibiotic therapy particularly when deemed to be poor surgical candidate.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



