Submitted:
26 November 2024
Posted:
27 November 2024
You are already at the latest version
Abstract
(1) Background: Home health care (HHC) services guarantee good patient care and family support. Understanding how we can better help our informal caregivers (IC) by understanding their needs and the burden they experience is crucial; (2) Methods: A cross-sectional study was conducted from June to September 2024 at (HHC) facility in Riyadh, Saudi Arabia. The 22-item Zarit Burden Interview (ZBI-22) was used to assess the caregiver burden (CB). IC from patients with specific diseases (palliative, cancer, chronic, and dementia) and other factors were studied to identify any association with informal caregiver burden (ICB); (3) Results: Significant CB was defined as ZBI ≥ 21. Total IC (384) participants: 119 (dementia) patients, 104 (chronic), 83 (palliative) and 78 (cancer). The total mean of the ZBI-22 score among IC was 31.66, representing a significant CB. The mean by groups was chronic (38.28), dementia (34.97), cancer (25.21), and palliative patients (22.94). Other variables, such as the duration of care, education level, relationship with the patient, and unemployment, were associated with CB (p-value < 0.05); (4) Conclusions: The caregivers' characteristics and the patient’s disease were associated with significant CB. More interventions from healthcare workers to support the IC are essential to release their burden.
Keywords:
Informal caregiver burden
; Zarit scale
; Saudi Arabia
; Home Health Care
; Palliative
; Cancer
; Dementia
; Chronic
1. Introduction
Population aging is a phenomenon all over the world, even though the Kingdom of Saudi Arabia as a relatively young average population comparing with other developed countries is following the same trend. This is supported by the United Nations state report that recently showed the percentage of elderly individuals in KSA will witness a sharp increase in the next three decades (5.6% in 2017 to 23% by 2050) [1,2]. According to this scenario, there will be a high potential to lead to an increased prevalence of comorbidities such as chronic diseases, cancer, dementia, and as consequence patients under palliative care and hence will require close and constant monitoring of such individuals [3].
According to these facts, it is essential to be aware that the increment of patients institutionalized will be more frequent. Some research suggests that most people over sixty-five years old want to live in their houses for as long as possible. Additional support is necessary through the HHC services to avoid institutionalization and keep individuals in their homes [4].
HHC consists in a system of qualified practitioners who provide care to patients in their homes, such as nurses, physicians, occupational therapists, dietitians, and social services [5]. The purpose of HHC services is to promote an optimal level of well-being for the patients, to help and support them to improve and maximize independence in their daily activities, and to assist in their needs to avoid hospitalization or admission to long-term facilities [6,7,8]. In Saudi Arabia, the first HHC program was established in 1991 by the King Faisal Specialized Hospital and was only for terminal cancer patients. Later, in 1995, the Ministry of National Guard Health Affairs (MNGHA) established the HHC program to reduce the length of hospital stays [9]. Our HHC services are provided according to patients' interventions regardless there is or not family support. The HHC work schedule is from 7 a.m. to 23 p.m., seven days a week. The only exception is the palliative and cancer patients, where specialized services are provided only five days a week by an interdisciplinary team of physicians and nurses.
As mentioned before, with the growing elderly population and considering their home environment and strong Middle East culture of “taken care of your own”, informal caregivers have an essential role in providing a wide range of care [10]. An IC care to a person who is incapacitated or disabled and includes family members and friends who provide care to their dear ones without any financial benefits [11]. Even though providing informal care can be described as fulfilling and rewarding, it may also be burdensome and time-consuming and affect the informal caregiver's life on many levels, socially, economically, physically, and mentally [12,13,14].
This study aimed to perform a cross-sectional investigation to assess the burden of informal caregivers from patients under HHC of NGHA and compare the burden according to the specific comorbidities of care recipients (palliative, cancer, chronic, and dementia). The focus is to contribute to strengthening efforts to support each group by adapting specific programs to ensure that they will help and decrease their burden.
Before selecting the tool for interviewing informal caregivers, a literature review was carefully done, and all factors, including patients' age, population of care receivers, items of questions, validity, and internal consistency, were considered. One tool that covered all the qualities of this study was found.
The Zarit Burden Interview 22-item (ZBI-22) short Arabic version was used to assess the informal caregiving burden. Initially developed to measure the burden of caregivers of dementia patients, it has been one of the most commonly used measures of CB. It has demonstrated adequate construct validity and high internal reliability. The ZBI has been widely validated, extensively studied, and is easy to use [15]The survey was part of a comprehensive understanding of the impact of the constantly rising burden on informal caregivers. Thus, translating valid and reliable tools for measuring caregiver burden is crucial. The results are expected to provide a factual evidenccome base for measuring and improving the quality of the HHC program in NGHA of Saudi Arabia and similar HHCs all over the country.
2. Materials and Methods
2.1 Study Design and Setting
This study is a cross-sectional survey on informal care. It uses the Arabic version of the Zarit Burden Interview (ZBI), a short version of 22 questions, to assess the burden of informal caregivers. The study was conducted within the HHC program of National Guard Health Affairs in King Abdulaziz Medical City in Riyadh, one of the largest hospitals in the central region of Saudi Arabia, which receives cases from all social and economic classes.
2.2. Participants and Data Collection
The entire population enrolled in the HHC program who were available during the home visit and willing to participate in the study survey. The inclusion criteria comprised all informal caregivers (not paid ones) aged equal or above 18, male and female, Arabic speakers, only one caregiver per patient, and a literate person taking care of the patient continuously for a minimum of 4 weeks. This selection ensured that only respondents who had been leading informal care for more than 4 weeks for patients with and highly dependent on care were gathered, as well as all patients with one of these comorbidities (palliative, cancer, chronic, or dementia). All caregivers want to participate in the survey. From a total population of 1080 patients, 415 met the criteria, but only 384 completed the survey. Caregivers who did not meet the eligibility criteria were excluded. Three hundred eighty-four respondents completed the questionnaire on informal care.
Data were collected during June and September 2024 using the Arabic Version of the short 22-item ZBI-22 questionnaire for measuring the ICB, obtained from Mapi Research Trust, Lyon, France (https://eprovide.mapi-trust.org/). It is widely used, and data from numerous studies demonstrate internal consistency, with Cronbach`s alpha values above 0.8 [16].
When asked to participate, the participants were properly and meticulously informed regarding the survey to ensure the precision of the data collection. The survey was sent through the caregiver's WhatsApp to avoid bias. We avoided a face-to-face interview with a nurse familiar with and working at the HHC program of the Ministry of National Guard Health Affairs in Riyadh. Before sending the link through WhatsApp, we called the patient's caregiver and explained the study and the confidentially, and after obtaining their consent, the link was sent. Automatically, the answers go to Google Drive. Before concluding the survey, all answers must be completed, and you cannot leave any answer without a response before sending the link.
2.3. Measurements
The survey was composed of 2 sections. The first section included sociodemographic details of the participants, such as age, gender, education level, marital status, employee status, relationship with the care recipient, and the time since caregiving. Section two of the survey was the ZBI-22 questionnaire that included the impact of caregiving on distinct aspects (caregiver´s physical health, psychological well-being, finances, social life, and the relationship between the caregiver and patient.) Each question is scored on a five-point Likert scale: never (0), rarely (1), sometimes (2), quite frequently (3), and nearly always (4). Total scores range from 0 to 88. The cut-off values were 0-20 little or no burden, 21-40 mild to moderate burden, 41-60 moderate to severe burden, and 61-88 severe burden [17]. The scale permits a prompt evaluation and provides a significant understanding of the informal caregiver´s burden, facilitating profitable data collection and analysis.
The survey was identical for all informal caregivers. The only way to differentiate each group was by the order of the first question.
Before sending the survey, the group each participant belongs to according to the patient's disease (palliative, cancer, chronic, or dementia) was selected. The survey takes around 5 minutes to answer.
2.4. Statistical Analysis
All categorical data obtained from the survey were calculated and presented as numbers and percentages. Continuous data was presented as means, standard deviation, median, and quartiles. As appropriate, inferential statistics, such as the t-test and chi-square test, were used to compare variables. Multivariable logistic regression analysis was used to identify any association between burden scores, patient condition, and informal caregiver characteristics.
All data were entered and analyzed through SAS 9.4 (SAS Institute Inc., Cary, NC, USA).
2.5. Ethical Considerations
The Department Research Committee of NGHA reviewed and approved ethical approval. Respondents were informed that participation was voluntary and that all information and data would remain confidential and anonymous. Respondents needed to provide written informed consent at the start and end of the survey.
3. Results
3.1. Questionnaire
3.1.1. Sociodemographic Characteristics of Study Participants
First: The information regarding our sample (n=384), informal caregivers` sociodemographic characteristics, is in (Table 1). The mean (SD) age of informal caregivers was 52.3 (11.49) years, ranging from 19 to 85 years. Regarding the type of care recipients' according to their morbidity, 21.6% were palliative, 20.3% had cancer, 27.1 % had a chronic disease, and 31% had dementia. On average, informal caregivers provided care for more than 3 years (41.7%). Half (50%) of the respondents had a general level of education degree, and less than one-third (27.3%) had jobs. More than half (69.3%) of the participants were female, and the majority (75%) were married. Regarding the relationship with the patients, more than half of them lent care to their parents (58.1%).
3.1.2. The ZBI-22 tool
Second: The prevalence of burden among caregivers was reported by the ZBI-22 questionnaire tool by mean and frequency. The total ZBI-22 score ranged from 0 to 88. The mean ZBI-22 score was (31.66). Using the ZBI-22 cutoff score of 21, (74.48%) had significant CB (286 ≥ 21). Regarding the individual items of ZBI, the highest score was for the question, "Do you feel your relative is dependent upon you?" with a mean (SD) of 2.5 (1.13). The lowest score was for the question, "Do you feel that your relative currently affects your relationship with other family members or friends in a negative way?" with a mean (SD) of 0.9 (1.10). Details of ZBI-22 item characteristics are presented in (Table 2), all questions 22 of the short version with respective means and standard deviation for the sample (n=384).
3.2. Informal Caregiver Burden
From (Figure 1) it is possible to see the frequency and compare the difference in ICB according to the recipient's disease.
3.3. Bivariate Analysis (ZBI-22) with Significant (P-Value > 0.05)
The relationship between CB and the studied variables in bivariate analysis is described in (Table 3). We are considerate, as from other studies conducted, the Yes (there is a burden) (ZBI-22 scored ≥ 21) with a total of 286, and No (there is no Burden (ZBI-22 scored < 21) with a total of 98. The caregiver's age was significant to the CB (p-value 0.0003). The oldest persons had the highest burden compared with the youngest ones. The bivariate analysis for factors associated with CB revealed that the caregivers taking care of patients with chronic (32.9%) and dementia (35.3%) disease had a high burden (ZBI-22 score ≥ 21) compared with those under palliative (15.7%) and cancer (16.1%) disease. The duration of care reveals that the caregivers with a short duration of caregiving of < 1 year (26.2%) had less burden compared to those with > 3 years (44.4%). Regarding the education level (p-value 0.0113), those with general education (51.7%) had more burden comparatively than those caregivers with university education (39.2%). Also, the fact that the caregivers had a job impacts the caregiver's burden, and it is possible that those working had less burden (20.3%) compared with those unemployed (79.7%). Gender also represents females as a higher burden (76.2%). The relationship with the patient's husband/wife demonstrates a significance (p-value < 0.0001) with ICB. Marital status was not significantly associated with the CB (p-value > 0.05).
3.4. Multiple Logistic Regression Analysis
Multiple logistic regression analysis (Table 4) showed that only four factors were independently associated with ICB. The CB was statistically significant for caregivers of patients with dementia compared with those with cancer and the same for caregivers without a job. Caregivers with high education levels have a significant burden compared with those with a university education. Also, the burden was substantial for those caring for spouses compared to caring for their parents.
4. Discussion
This study, conducted from a Military hospital in Riyadh, Saudi Arabia, aims to determine the prevalence of burden among different patient recipients and identify the associated risk factors. The ZBI-22 was used to assess the degree of burden. We observed that respondents who took care of chronic and dementia patients had the highest level of burden, compared with the carers who took care of cancer and palliative patients, who had the lowest level of burden. The mean ZBI-22 score in this study was 25.21 for cancer patients, similar to that reported in a study from the United Kingdom that included cancer patients, and the mean ZBI-22 score was 23 [18]. Equally, the mean ZBI-22 score was 22.94 for palliative patients, the same as in a study from palliative care in Malaysia, where the ZBI-22 mean score was 23 [19]. The ZBI scale has been used extensively in caregivers with chronic illness [20,21]. Informal care is often essential to the care provided to patients, especially those with chronic diseases. Recent studies have shown that many informal caregivers experience a substantial burden from their caregiving tasks. It has been demonstrated that caregiving amongst the elderly is an independent risk factor for morbidity and mortality [22], which supports the high level of the mean burden for chronic patients with a score of 38.29. Likewise, Gratao et al. observed a significant relationship between a caregiver´s burden and the recipient´s stage of dementia [23], which corroborates with the burden level from our study, in which the mean score was 34.97. Denno et al. concluded that as the burden of caregivers increased, the more likely they were to experience anxiety and depression [24]. Against possible expectations, palliative and cancer patients' caregivers answered lower levels of burden when compared with others. These facts could be related to the excellent support and good services provided in our HHC department (5 days a week) the palliative doctors, together with nurses going for patient visits, providing specialized care, and consequently, all these components could be associated with an excellent factor to help the informal caregivers in their tasks with close monitoring/support the patient’s needs. Also, to our knowledge, this present study was the first in Saudi Arabia, to explore the burden of informal caregivers of different patients' diseases and compare the burden between them. Evidence in the literature indicates that cultural factors influence the caregiver’s burden, with one study reporting that aspects explained 29% of the variance in burden [25]. Al-Khashan et al. asserted that home services that provide additional healthcare support to patients improve the self-confidence of the caregivers, and these frequent home visits also increase caregiver satisfaction [26]. The results will provide a basis for developing a program to teach and support this group of caregivers in their arduous work.
We detailed the results section of the response of the IC to the 22 items of the ZBI-22 to quickly identify which questions had more impact on the ICB and maybe serve as a guide for future research/interventions to minimize the ICB in our HHC department. Only 4 items out of 22 scored on average > 2 on the 0-4 scale. This may be a target for interventions dealing with ICB. Another example is the question, " Do you feel your relative is dependent upon you?" which scored an average of 2.5 on the 0-4 scale, which represents the idea that the patient depends on them, describing the feeling of the total responsibility of the total care, which causes even more anxiety for the IC. Meeting the information requirements of caregivers supporting them psychosocially may reduce their fears, stress, and, subsequently, the burden they suffer.
The caregivers' mean age in the present study was 52.3 ± 11.49 years, following those reported in previous studies [27,28,29], as the caregiver's age ranged between 43.8 and 63.1 years. In our study, older caregivers experience a higher burden than younger ones, which could be explained by the culture in Saudi Arabia, where the responsibilities increase naturally according to a person's age, which causes more physiological stress. The current study also showed that the burden was higher among participants with lower education, who were unemployed and had the most extended duration of care. Regarding the duration, time is reasonably expected for this association. In South Korea, Yoon et al. [30] reported that longer time spent providing care per day was significantly associated with caregiver burden.
The relationship between the caregiver and recipient was also a decisive factor, and as reported in previous studies, husbands and wives noticed a significant burden; the burden was more among spouses [31,32].
Females had a higher burden compared with males; studies suggest that women caregivers are usually involved in physically demanding tasks (e.g., bathing, feeding, and dressing) compared to their male counterparts, who are more likely to provide financial support [33].
Previous studies identified factors that determine the presence and degree of ICB, such as the duration of care, the education level, and whether the caregiver is employed [34,35,36,37]This study shows only four variables associated independently with significant CB: patient decease, caregivers who are unemployed, have high education, and take care of spouses; the other factors have no significant association with CB.
Many different factors can influence the CB, such as culture and beliefs, like religion. Other concepts and beliefs can affect caregiving expectations and behaviors, motivations to provide care, and different concepts of caregiver distress or burden [38]. Differences in some studies could be attributed to the various careers' socio-demographic characteristics, tools utilized, methodology, and cultural norms [39].
The present study has some significant limitations that should be acknowledged. First, the study was conducted in a single care facility. Second, the small sample size of each group of patients' diseases was due to the limited number of patients in our HHC, especially for palliative and cancer patients. Third, meaningful information about caregivers, such as social and family support, health status, health knowledge, and religious and spiritual needs, needs to be included [40,41,42].
Notwithstanding these limitations, this study strongly impacts the focus on exploring the magnitude of ICB and identifying those factors associated with a higher burden, leading to a better-targeted intervention by healthcare practitioners and researchers.
5. Conclusions
The ZBI interview, which provides a comprehensive assessment of both objective and subjective burden, was designed for caregivers of patients with dementia. Even so, it is one of the most commonly used burden measures. It has been validated in many culturally or ethnically different populations and is widely used with a wide variety of other disorders, including cancer, palliative care, and chronic illness.
In conclusion, the burden of IC had a more significant impact on patients with chronic and dementia disease than on those under cancer and palliative care. That could be addressed because of the specialized services for palliative and cancer patients. Therefore, healthcare staff must be more aware of patients and their families experiences and potential needs. Eventually, an interdisciplinary approach and collaborative visits with physicians and nurses could minimize the ICB.
In this study, we did not investigate all caregivers' essential characteristics that could lead to different burden levels. For future research, it will be crucial to consider that all caregivers had, for example, the same number of healthcare visits and the same personalized service with close monitoring to compare the burden level.
Author Contributions
Conceptualization D.C; Methodology D.C; Validation D.C; Formal analysis D.C; Investigation D.C; Writing - Original draft preparation D.C; Writing - review and editing D.C; Visualization D.C; Supervision D.C. All authors have read and agreed to the published version of the manuscript.
Funding
“This research received no external funding”.
Institutional Review Board Statement
This study was conducted in accordance with the Declaration of Helsinki and approved by the Department Research Committee of NGHA
Informed Consent Statement
“Written informed consent has been obtained from the subjects involved to publish this paper” The participants received a detailed explanation of the study’s objectives and the purpose of data collection. Additionally, all participants were volunteers, and the confidentiality of the data obtained was preserved with anonymity.
Data Availability Statement
The data presented in this study can be obtained by contacting the corresponding author if desired. Data Availability Statements are available in section “MDPI Research Data Policies” at https://www.mdpi.com/ethics.
Acknowledgments
We appreciate the support from all staff working in our home health care facility, especially to Yasser.
Conflicts of Interest
“The authors declare no conflicts of interest.”
References
- Gov.sa. https://www.my.gov.sa/wps/portal/snp/careaboutyou/elderly/!ut/p/z0/04_Sj9CPykssy0xPLMnMz0vMAfIjo8zijQx93d0NDYz8LYIMLA0CQ4xCTZwN_Ay8Qgz1g1Pz9AuyHRUB-ivojg!!/#:~:text=The%20Ministry%20provides%20the%20elderly,and%20their%20families%20through%20the. 2024 [cited 2024 Nov 19]. Elderly. Available from: https://www.my.gov.sa/wps/portal/snp/careaboutyou/elderly/!ut/p/z0/04_Sj9CPykssy0xPLMnMz0vMAfIjo8zijQx93d0NDYz8LYIMLA0CQ4xCTZwN_Ay8Qgz1g1Pz9AuyHRUB-ivojg!!/#:~:text=The%20Ministry%20provides%20the%20elderly,and%20their%20families%20through%20the.
- United Nations. World Population Ageing - Highlights. Department of Economic and Social Affairs - Population Division. 2017;((ST/ESA/SER.A/397)).
- Althabe F, Belizán JM, McClure EM, Hemingway-Foday J, Berrueta M, Mazzoni A, et al. A population-based, multifaceted strategy to implement antenatal corticosteroid treatment versus standard care for the reduction of neonatal mortality due to preterm birth in low-income and middle-income countries: The ACT cluster-randomised trial. The Lancet. 2015 Feb 14;385(9968):629–39. [CrossRef]
- Home health services [Internet]. [cited 2024 Nov 19]. Available from: https://www.medicare.gov/coverage/home-health-services.
- Ellenbecker CH, Samia L, Cushman MJ, Alster K. Chapter 13. Patient Safety and Quality in Home Health Care.
- Homecare is the solution [Internet]. [cited 2024 Nov 19]. Available from: http://www .aahomecare .org/associations/3208 /files/home%20healthcare%202%20pager .pdf.
- Wilson DR. Home health nursing: scope and standards of practice. Act Adapt Aging. 2019;43(1). [CrossRef]
- Shaughnessy PW, Hittle DF, Crisler KS, Powell MC, Richard AA, Kramer AM, et al. Improving patient outcomes of home health care: Findings from two demonstration trials of outcome-based quality improvement. J Am Geriatr Soc. 2002;50(8). [CrossRef]
- Almoajel A, Al-Salem A, Al-Ghunaim L, Al-Amri S. The Quality of Home Healthcare Service in Riyadh/Saudi Arabia. Asian Journal of Natural & Applied Sciences. 2016;5(2).
- Lang A, Edwards N, Hoffman C, Shamian J, Benjamin K, Rowe M. Broadening the patient safety agenda to include home care services. Healthc Q. 2006;9 Spec No. [CrossRef]
- Gouin JP, da Estrela C, Desmarais K, Barker ET. The Impact of Formal and Informal Support on Health in the Context of Caregiving Stress. Fam Relat. 2016;65(1). [CrossRef]
- van Exel J, Bobinac A, Koopmanschap M, Brouwer W. The invisible hands made visible: Recognizing the value of informal care in healthcare decision-making. Expert Rev Pharmacoecon Outcomes Res. 2008;8(6). [CrossRef]
- Brouwer WBF, Van Exel NJA, Van Den Berg B, Van Den Bos GAM, Koopmanschap MA. Process utility from providing informal care: The benefit of caring. Health Policy (New York). 2005;74(1). [CrossRef]
- Pendergrass A, Mittelman M, Graessel E, Özbe D, Karg N. Predictors of the personal benefits and positive aspects of informal caregiving. Aging Ment Health. 2019;23(11). [CrossRef]
- Knight BG, Fox LS, Chou CP. Factor structure of the burden interview. J Clin Geropsychology. 2000;6(4). [CrossRef]
- Arai Y, Kudo K, Hosokawa T, Washio M, Miura H, Hisamichi S. Reliability and validity of the Japanese version of the Zarit Caregiver burden Interview. Psychiatry Clin Neurosci. 1997;51(5). [CrossRef]
- M Bédard 1 DWMLSSDJALMO. The Zarit Burden Interview: a new short version and screening version. Gerontologist. 2001.
- Harding R, Gao W, Jackson D, Pearson C, Murray J, Higginson IJ. Comparative Analysis of Informal Caregiver Burden in Advanced Cancer, Dementia, and Acquired Brain Injury. J Pain Symptom Manage. 2015;50(4). [CrossRef]
- Ahmad Zubaidi ZS, Ariffin F, Oun CTC, Katiman D. Caregiver burden among informal caregivers in the largest specialized palliative care unit in Malaysia: a cross sectional study. BMC Palliat Care. 2020 Dec 1;19(1).
- Al-Rawashdeh SY, Lennie TA, Chung ML. Psychometrics of the zarit burden interview in caregivers of patients with heart failure. Journal of Cardiovascular Nursing. 2016;31(6). [CrossRef]
- Steven H. Zarit JMZ. The memory and behavior problems checklist and the burden interview. 1983.
- Schulz R, Beach SR. Caregiving as a Risk Factor for Mortality The Caregiver Health Effects Study [Internet]. Available from: www.jama.com.
- Gratao ACM, Vale F de AC do, Roriz-Cruz M, Haas VJ, Lange C, Talmelli LF da S, et al. The demands of family caregivers of elderly individuals with dementia. Revista da Escola de Enfermagem da USP. 2010;44(4).
- Denno MS, Gillard PJ, Graham GD, Dibonaventura MD, Goren A, Varon SF, et al. Anxiety and depression associated with caregiver burden in caregivers of stroke survivors with spasticity. Arch Phys Med Rehabil. 2013;94(9). [CrossRef]
- Del-Pino-Casado R, Millán-Cobo MD, Palomino-Moral PA, Frías-Osuna A. Cultural correlates of burden in primary caregivers of older relatives: A Cross-sectional Study. Journal of Nursing Scholarship. 2014;46(3). [CrossRef]
- Al-Khashan H, Mishriky A, Selim M, El Sheikh A, Binsaeed A. Home caregivers’ satisfaction with the services provided by Riyadh Military Hospital’s home support program. Ann Saudi Med. 2011 Nov;31(6):591–7. [CrossRef]
- Youngmee Kim1 RLS and DLH. Quality of life of family caregivers 5 years after a relative’scancer diagnosis: follow-up of the national quality of lifesurvey for caregivers. Psychooncology. 2012.
- Rostami M, Abbasi M, Soleimani M, Moghaddam ZK, Zeraatchi A. Quality of life among family caregivers of cancer patients: an investigation of SF-36 domains. BMC Psychol. 2023 Dec 1;11(1). [CrossRef]
- Hsu T, Loscalzo M, Ramani R, Forman S, Popplewell L, Clark K, et al. Factors associated with high burden in caregivers of older adults with cancer. Cancer. 2014;120(18). [CrossRef]
- Yoon SJ, Kim JS, Jung JG, Kim SS, Kim S. Modifiable factors associated with caregiver burden among family caregivers of terminally ill Korean cancer patients. Supportive Care in Cancer. 2014;22(5). [CrossRef]
- Lowenstein A, Gilbar O. The perception of caregiving burden on the part of elderly cancer patients, spouses and adult children. Vol. 18, Families, Systems and Health. 2000. [CrossRef]
- Doorenbos AZ, Given B, Given CW, Wyatt G, Gift A, Rahbar M, et al. The influence of end-of-life cancer care on caregivers. Vol. 30, Research in Nursing and Health. 2007.
- Depasquale N, Davis KD, Zarit SH, Moen P, Hammer LB, Almeida DM. Combining formal and informal caregiving roles: The psychosocial implications of double- and triple-duty care. Journals of Gerontology - Series B Psychological Sciences and Social Sciences. 2016;71(2). [CrossRef]
- Schwartz K, Beebe-Dimmer J, Hastert TA, Ruterbusch JJ, Mantey J, Harper F, et al. Caregiving burden among informal caregivers of African American cancer survivors. Journal of Cancer Survivorship. 2021;15(4). [CrossRef]
- Ye Ji Seo HP. Factors influencing caregiver burden in families of hospitalised patients with lung cancer. Wiley. 2019.
- Mirsoleymani S, Rohani C, Matbouei M, Nasiri M, Vasli P. Predictors of caregiver burden in Iranian family caregivers of cancer patients. J Educ Health Promot. 2017;6(1). [CrossRef]
- Lukhmana S, Bhasin SK, Chhabra P, Bhatia MS. Family caregivers’ burden: A hospital based study in 2010 among cancer patients from Delhi. Indian J Cancer. 2015;52(1). [CrossRef]
- Zarzycki M, Seddon D, Bei E, Dekel R, Morrison V. How Culture Shapes Informal Caregiver Motivations: A Meta-Ethnographic Review. Vol. 32, Qualitative Health Research. 2022. [CrossRef]
- Otis-Green S, Juarez G. Enhancing the Social Well-Being of Family Caregivers. Semin Oncol Nurs. 2012;28(4). [CrossRef]
- Yoo JS, Lee JH, Chang SJ. Family Experiences in End-of-Life Care: A Literature Review. Asian Nurs Res (Korean Soc Nurs Sci). 2008;2(4). [CrossRef]
- Lee J, Cha C. Unmet Needs and Caregiver Burden among Family Caregivers of Hospice Patients in South Korea. Journal of Hospice and Palliative Nursing. 2017;19(4). [CrossRef]
- Nathan E Goldstein 1 JCTRFSVKRJHEHB. Factors associated with caregiver burden among caregivers of terminally ill patients with cancer. J Palliat Care. 2004.
Figure 1.
Severity of burden among informal caregivers by recipients’ condition.
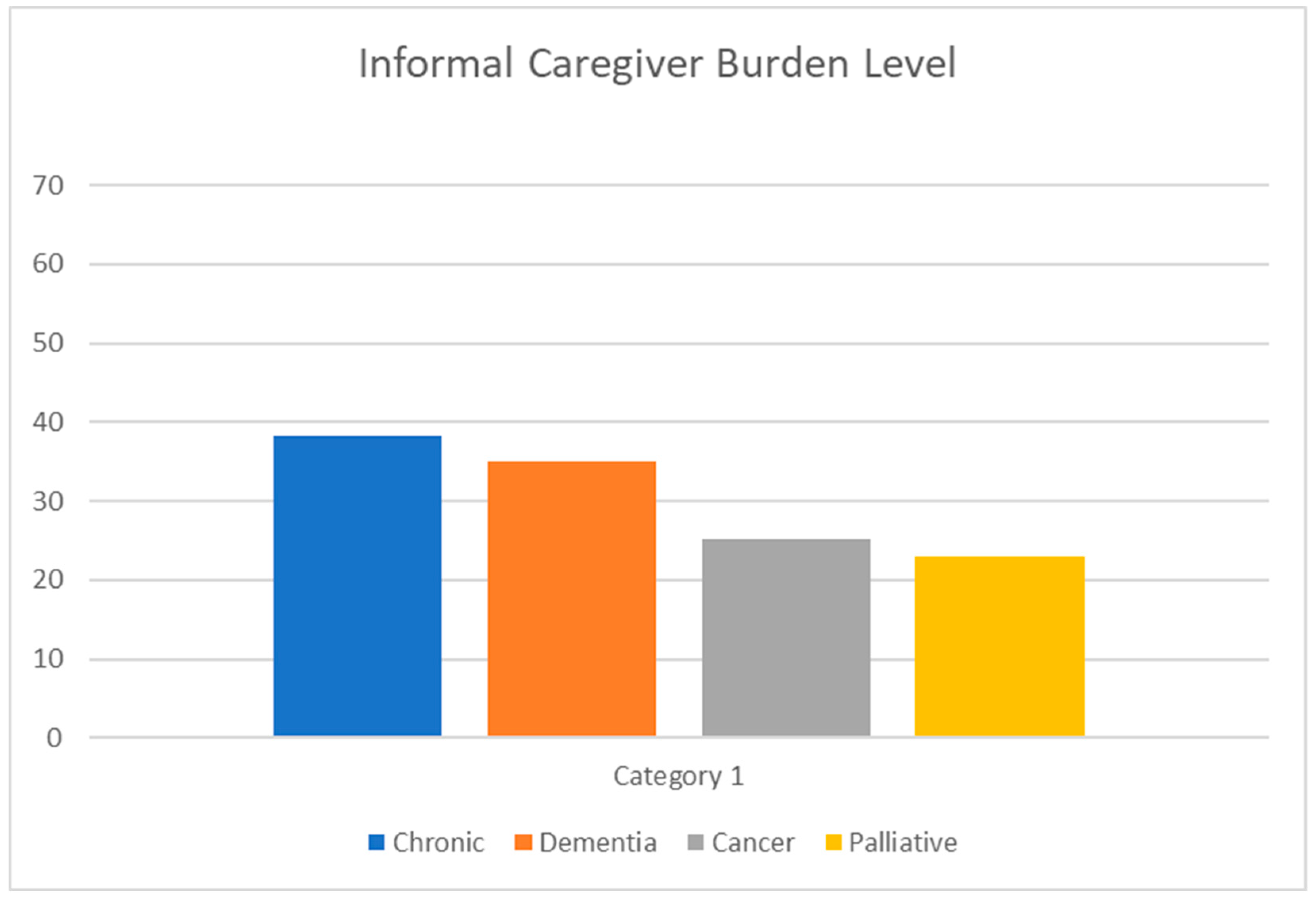

Table 1.
Sociodemographic Characteristics of Study Participants.
| VARIABLE | Category | Total |
|---|---|---|
| Age | n | 384 |
| Age | Mean (SD) | 52.3 ± 11.49 |
| Age | Median (Q1, Q3) | 53.0(45.50, 60.00) |
| Age | Min, Max | 19.0, 85.0 |
| Disease | Chronic | 104 (27.1%) |
| Disease | Dementia | 119 (31.0%) |
| Disease | Cancer | 78 (20.3%) |
| Disease | Palliative | 83 (21.6%) |
| Duration of Care | Less one year | 114 (29.7%) |
| Duration of Care | More than three years | 160 (41.7%) |
| Duration of Care | One year to three years | 110 (28.6%) |
| Education Level | General education | 192 (50.0%) |
| Education Level | High education | 28 (7.3%) |
| Education Level | University education | 164 (42.7%) |
| Employee | no | 279 (72.7%) |
| Employee | yes | 105 (27.3%) |
| Gender | Female | 266 (69.3%) |
| Gender | Male | 118 (30.7%) |
| Marital Status | Divorced | 30 (7.8%) |
| Marital Status | Married | 288 (75.0%) |
| Marital Status | Single | 60 (15.6%) |
| Marital Status | Widowed | 6 (1.6%) |
| Relationship with Patient | Brother/Sister | 50 (13.0%) |
| Relationship with Patient | Father/Mother | 223 (58.1%) |
| Relationship with Patient | Grandmother/Grandfather | 19 (4.9%) |
| Relationship with Patient | Husband/Wife | 65 (16.9%) |
| Relationship with Patient | Other | 27 (7.0%) |
* Total responses of caregivers (384).
Table 2.
Response of Informal caregivers to the ZBI-22 items.
| Item (384 Responses) | 0 (never) | 1 (rarely) | 2 (sometimes) | 3 (quite frequently) | 4 (nearly always) | Mean (SD) |
|---|---|---|---|---|---|---|
| 1. Are you afraid of what the future holds for your neighbor? | 95 (24.7%) | 75 (19.5%) | 99 (25.8%) | 98 (25.5%) | 17 (4.4%) | 1.7 ± 1.23 |
| 2. Are you ashamed of your relative’s behavior? | 201 (52.3%) | 62 (16.1%) | 65 (16.9%) | 56 (14.6%) | 0 (0%) | 0.9 ± 1.13 |
| 3. Do you feel angry or angry if you are with your relative? | 202 (52.6%) | 62 (16.1%) | 83 (21.6%) | 34 (8.9%) | 3 (0.8%) | 0.9 ± 1.08 |
| 4. Do you feel that more needs to be done than you already do for your neighbor? | 45 (11.7%) | 67 (17.4%) | 121 (31.5%) | 102 (26.6%) | 49 (12.8%) | 2.1 ± 1.19 |
| 5. Do you feel that the time you spend with your relative affects your time? | 95 (24.7%) | 91 (23.7%) | 112 (29.2%) | 68 (17.7%) | 18 (4.7%) | 1.5 ± 1.18 |
| 6. Do you feel that you are missing privacy to some degree because of your relative? | 177 (46.1%) | 72 (18.8%) | 79 (20.6%) | 50 (13.0%) | 6 (1.6%) | 1.1 ± 1.15 |
| 7. Do you feel that you can improve the level of care you provide to your relative? | 29 (7.6%) | 82 (21.4%) | 117 (30.5%) | 109 (28.4%) | 47 (12.2%) | 2.2 ± 1.12 |
| 8. Do you feel that you don't have enough money to take care of your relative in addition to the rest of your allowance? | 74 (19.3%) | 54 (14.1%) | 124 (32.3%) | 106 (27.6%) | 26 (6.8%) | 1.9 ± 1.20 |
| 9. Do you feel that you have lost control of your life since your relative’s illness? | 129 (33.6%) | 53 (13.8%) | 98 (25.5%) | 86 (22.4%) | 18 (4.7%) | 1.5 ± 1.29 |
| 10. Do you feel that your health has been affected by the result of your neighbor's care? | 130 (33.9%) | 75 (19.5%) | 114 (29.7%) | 56 (14.6%) | 9 (2.3%) | 1.3 ± 1.15 |
| 11. Do you feel that your relative is currently affecting your relationship with the rest of the family or friends negatively? | 199 (51.8%) | 70 (18.2%) | 68 (17.7%) | 45 (11.7%) | 2 (0.5%) | 0.9 ± 1.10 |
| 12. Do you feel that your relative expects to take care of him as if you are the only person who can rely on him? | 46 (12.0%) | 52 (13.5%) | 114 (29.7%) | 126 (32.8%) | 46 (12.0%) | 2.2 ± 1.18 |
| 13. Do you feel that your relative is asking for help and help more than he really needs? | 130 (33.9%) | 100 (26.0%) | 61 (15.9%) | 48 (12.5%) | 45 (11.7%) | 1.4 ± 1.37 |
| 14. Do you feel that your social life is suffering because of your care for your relative? | 137 (35.7%) | 87 (22.7%) | 81 (21.1%) | 67 (17.4%) | 12 (3.1%) | 1.3 ± 1.21 |
| 15. Do you feel the psychological pressure resulting from the distribution of attention between the care of your relative and the performance of your responsibilities towards the family or work? | 78 (20.3%) | 107 (27.9%) | 110 (28.6%) | 63 (16.4%) | 26 (6.8%) | 1.6 ± 1.18 |
| 16. Do you feel tight (uncomfortable) when you’re with your relative? | 170 (44.3%) | 63 (16.4%) | 95 (24.7%) | 48 (12.5%) | 8 (2.1%) | 1.1 ± 1.17 |
| 17. Do you feel uncomfortable inviting a friend because of your relative? | 163 (42.4%) | 70 (18.2%) | 91 (23.7%) | 48 (12.5%) | 12 (3.1%) | 1.2 ± 1.19 |
| 18. Do you feel unsure of what to do with your relative? | 131 (34.1%) | 70 (18.2%) | 108 (28.1%) | 70 (18.2%) | 5 (1.3%) | 1.3 ± 1.16 |
| 19. Do you feel you can't continue to take care of your relative? | 180 (46.9%) | 71 (18.5%) | 77 (20.1%) | 47 (12.2%) | 9 (2.3%) | 1.0 ± 1.17 |
| 20. Do you price that your relative depends on you? | 27 (7.0%) | 49 (12.8%) | 92 (24.0%) | 148 (38.5%) | 68 (17.7%) | 2.5 ± 1.13 |
| 21. In general, how much do you feel the burden of caring for your neighbor? | 117 (30.5%) | 76 (19.8%) | 117 (30.5%) | 64 (16.7%) | 10 (2.6%) | 1.4 ± 1.16 |
| 22. Would you like to leave your neighbor's care for someone else? | 193 (50.3%) | 59 (15.4%) | 76 (19.8%) | 50 (13.0%) | 6 (1.6%) | 1.0 ± 1.17 |
*Zarit Burden 22 (ZBI-22) short version in English version.
Table 3.
The relationship between caregiver burden and the studied variables.
| NAME OF FORMER VARIABLE | cat2 | Yes (ZBI-22 score ≥ 21) = 286 | No (ZBI-22 score < 21) = 98 | Total=384 | p-value |
|---|---|---|---|---|---|
| Age | Mean (SD) | 53.5 (10.97) | 48.8 (12.29) | 52.3 (11.49) | 0.0003 ^ |
| Age | Median (Q1, Q3) | 54.0 (48.00, 61.00) | 50.0(40.00, 57.00) | 53.0(45.50, 60.00) | 0.0003 ^ |
| Disease | Chronic | 94 (32.9) | 10 (10.2) | 104 (27.1) | <.0001 ** |
| Disease | Dementia | 101 (35.3) | 18 (18.4) | 119 (31.0) | <.0001 ** |
| Disease | Cancer | 46 (16.1) | 32 (32.7) | 78 (20.3) | <.0001 ** |
| Disease | Palliative | 45 (15.7) | 38 (38.7) | 83 (21.6) | <.0001 ** |
| Duration of Care | Less one year | 75 (26.2) | 39 (39.8) | 114 (29.7) | 0.0342 ** |
| Duration of Care | More than three years | 127 (44.4) | 33 (33.7) | 160 (41.7) | 0.0342 ** |
| Duration of Care | One year to three years | 84 (29.4) | 26 (26.5) | 110 (28.6) | 0.0342 ** |
| Education Level | General education | 148 (51.7) | 44 (44.9) | 192 (50.0) | 0.0113 ** |
| Education Level | High education | 26 (9.1) | 2 (2.0) | 28 (7.3) | 0.0113 ** |
| Education Level | University education | 112 (39.2) | 52 (53.1) | 164 (42.7) | 0.0113 ** |
| Employee | no | 228 (79.7) | 51 (52.0) | 279 (72.7) | <.0001 ** |
| Employee | yes | 58 (20.3) | 47 (48.0) | 105 (27.3) | <.0001 ** |
| Gender | Female | 218 (76.2) | 48 (49.0) | 266 (69.3) | <.0001 ** |
| Gender | Male | 68 (23.8) | 50 (51.0) | 118 (30.7) | <.0001 ** |
| Marital Status | Divorced | 21 (7.3) | 9 (9.2) | 30 (7.8) | 0.4497 ^^ |
| Marital Status | Married | 220 (76.9) | 68 (69.4) | 288 (75.0) | 0.4497 ^^ |
| Marital Status | Single | 41 (14.4) | 19 (19.4) | 60 (15.6) | 0.4497 ^^ |
| Marital Status | Widowed | 4 (1.4) | 2 (2.0) | 6 (1.6) | 0.4497 ^^ |
| Relationship with Patient | Brother/Sister | 42 (14.7) | 8 (8.2) | 50 (13.0) | <.0001 ** |
| Relationship with Patient | Father/Mother | 149 (52.1) | 74 (75.5) | 223 (58.1) | <.0001 ** |
| Relationship with Patient | Grandmother/ Grandfather | 10 (3.5) | 9 (9.2) | 19 (4.9) | <.0001 ** |
| Relationship with Patient | Husband/Wife | 62 (21.7) | 3 (3.1) | 65 (16.9) | <.0001 ** |
| Relationship with Patient | Other | 23 (8.0) | 4 (4.0) | 27 (7.0) | <.0001 ** |
| Denominator of the percentage is the total number of subjects in each group. | |||||
| *T -Test / ^ Wilcoxon rank sum test is used to calculate the P-value. | |||||
| **Chi-square test is used to calculate the P-value. | |||||
| ^^Fisher exact test is used to calculate the P-value. | |||||
Table 4.
Multivariable logistic regression modeling the relationship between caregiver burden and the studied variables.
Table 4.
Multivariable logistic regression modeling the relationship between caregiver burden and the studied variables.
| Effect | Beta | Standard Error | Odds Ratio | [95% Conf. Interval] | P-value |
|---|---|---|---|---|---|
| Age | -0.00114 | 0.0144 | 0.999 | (0.97, 1.03) | 0.9367 |
| Disease Chronic vs Dementia | 0.5697 | 0.4459 | 1.768 | (0.74, 4.24) | 0.2014 |
| Disease Cancer vs Dementia | -0.8910 | 0.4259 | 0.410 | (0.18, 0.95) | 0.0364 |
| Disease Palliative vs Dementia | -0.8242 | 0.4238 | 0.439 | (0.19, 1.01) | 0.0518 |
| Gender Female vs Male | 0.4141 | 0.3033 | 1.513 | (0.83, 2.74) | 0.1721 |
| Duration of Care More than three years vs Less one year | 0.2763 | 0.3544 | 1.318 | (0.66, 2.64) | 0.4357 |
| Duration of Care One year to three years vs Less one year | 0.2582 | 0.3596 | 1.295 | (0.64, 2.62) | 0.4727 |
| Marital Status Divorced vs Married | 0.2789 | 0.4827 | 1.322 | (0.51, 3.40) | 0.5634 |
| Marital Status Single vs Married | 0.3900 | 0.4159 | 1.477 | (0.65, 3.34) | 0.3484 |
| Marital Status Widowed vs Married | -0.4699 | 0.9956 | 0.625 | (0.09, 4.40) | 0.6369 |
| Employee Yes vs No | -0.7084 | 0.3110 | 0.492 | (0.27, 0.91) | 0.0228 |
| Education Level General education vs University education | 0.2055 | 0.2843 | 1.228 | (0.70, 2.14) | 0.4697 |
| Education Level High education vs University education | 2.0668 | 0.8001 | 7.899 | (1.65, 37.90) | 0.0098 |
| Relationship W/ Patient Brother/Sister vs Father/Mother | 0.4146 | 0.4576 | 1.514 | (0.62, 3.71) | 0.3649 |
| Relationship W/ Patient GrandMoth/GrandFath vs Father/Mother | -0.4272 | 0.5679 | 0.652 | (0.21, 1.99) | 0.4519 |
| Relationship W/ Patient Husband/Wife vs Father/Mother | 2.1022 | 0.6493 | 8.184 | (2.29, 29.22) | 0.0012 |
| Relationship W/ Patient Other vs Father/Mother | 0.2945 | 0.6099 | 1.342 | (0.41, 4.44) | 0.6293 |
*Probability modeled is Caregiver burden='Yes'.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



