
Submitted:
25 November 2024
Posted:
26 November 2024
You are already at the latest version
Abstract
Background: Multiple markers were investigated to predict adverse outcomes post-cardiac surgery. Platelet-activating factor has a potential involvement in the hematologic and cardiovascular dysfunctions noted during and subsequent to extracorporeal circulation and coronary artery bypass grafting. The objective of our study was to assess Platelet-activating factor and CRP levels and their influence on mortality and morbidity following major heart surgery. Methods: We selected 87 patients that underwent major cardiac surgery between 2021 and 2022 at our institution. We gathered demographical data and unfavorable events after surgery. We investigated a composite outcome comprising three combined outcomes: mortality, renal failure, and stroke, using univariate and multivariate analysis. Results: The study population consisting of 87 individuals with a mean age of 64.9 years old was divided into 4 groups based on CRP levels: normal values (0-10 mg/l), mild increase (10-40 mg/l), moderate increase (40-200mg/l) and severe in-creased (>200 mg/l) levels. There was no significant difference between the 4 CRP groups except higher PAF levels (4939 ±2166.3 pg/ml) and lower baseline LVEF (43.6±6.9%) in group 4 with severely increased CRP values. We also found a significant positive correlation between preoperative PAF levels and post-operative CRP levels (r=0.72, p=0.0001). ROC curve analysis showed that both PAF and CRP can predict post-operative mortality with a good sensitivity and specificity. CRP values > 80 mg/l and PAF values > 5000 pg/ml were associated with combined outcome of: stroke, acute kidney failure and death HR=2.45 (95%CI 0.48-18.3) and HR = 2.62 (95%CI 0.37-20.0) respectively. Conclusions: Preoperative PAF and postoperative CRP are predictors of unfavorable prognosis after major cardiac surgery. C-reactive protein > 80 mg/l and Platelet-activating facotr > 5000 pg/ml were associated with the outcome of: stroke, acute kidney failure and death.
Keywords:
major cardiac surgery
; platelet-activating factor
; C-reactive protein
; cardiopulmonary bypass
1. Introduction
Preoperative risk assessment in cardiac surgery is essential for evaluating a patient's eligibility for the procedure and identifying markers for adverse outcomes. To ensure a successful outcome, the anesthesiologists must collect adequate information, comprehend the patients' clinical condition, and refine their overall strategy depending on preoperative findings [1,2]. Multiple markers were investigated [3] to predict adverse outcomes post-cardiac surgery. However, this strategy should avoid superfluous tests that lack predictive value for outcomes, incur significant costs for the medical department, or postpone the surgical procedure [4].
Platelet-activating factor (PAF) is a potent phospholipid mediator initially identified for its capacity to induce platelet aggregation and vasodilation. PAF plays a primary role in inflammatory responses and the initiation of thrombotic processes, additionally it promotes the pathogenesis of severe sepsis. Bacterial endotoxins can stimulate PAF synthesis, leading to significant hypotension and organ damage [5]. These lipid mediators are important components of inflammatory and coagulation pathways. Its presence also suggests a potential involvement in the hematologic and cardiovascular dysfunctions noted during and subsequent to extracorporeal circulation [6] and coronary artery bypass grafting [7-10].
Tissue damage resulting from cardiac surgery and myocardial necrosis induces an inflammatory response, evidenced by elevated levels of C-reactive protein [11-12]. Under these conditions, PAF interacts with several proteins, including C-reactive protein, which indicate systemic inflammation, positioning PAF as a potential therapeutic target for managing these diseases. The CRP levels during hospitalization correlate with the severity of the inflammatory response [13], and may be associated to PAF levels.
Several experimental studies have demonstrated the multilevel interaction between CRP and PAF: Filep et al. [13] indicated that CRP inhibited PAF-induced platelet aggregation in a dose- and time-dependent manner, whereas Sato et al. [14] revealed an enhanced inflammatory activity of PAF mediated by CRP.
The primary objective of our study was to assess the influence of Platelet-activating factor and CRP levels on mortality and morbidity following major heart surgery. Additionally, the relationship between platelet activation factor and postoperative CRP was investigated.
2. Materials and Methods
This retrospective descriptive study was conducted on patients with major cardiac surgery at Niculae Stancioiu Heart Institute Hospital in Cluj-Napoca and center and approved by the “Iuliu Hatieganu” University of Medicine Ethics Committee (approval number 259 on 28 September 2023). Patients who underwent major cardiac surgery procedures necessitating general anesthesia and cardiopulmonary bypass between 2021 to 2022, were included in the study. The inclusion criteria consisted of: age older than 18 years, patients who underwent open cardiac surgery, and the availability of data in the hospital registry system. Unstable individuals who underwent emergency procedures, minimally invasive and transcatheter procedures, and patients with incomplete information in the database, were excluded from this study. The data gathered from the patients included demographic information such as gender, age, sex, weight, height, body mass index (BMI), heart disease diagnosis, left ventricular ejection fraction pre- and post-surgery, type of surgery, diabetes mellitus status, duration of mechanical ventilation, stay in intensive care unit, total stay in the hospital, =laboratory tests: hematocrit, white blood cells, platelet count, preoperative platelet activation factor (PAF), creatinine, postoperative C-reactive protein. Blood samples of PAF were collected before surgery and serum was prepared by centrifugation. PAF levels were measured in plasma using PAF Elisa Kit with the colorimetric detection method, the color intensity being inversely related to the quantity of PAF extracted from the samples. The study was performed in compliance with the Declaration of Helsinki and Good Clinical Practice Guidelines. The necessity for patient consent was exempted due to the retroactive nature of the data analysis.
Postoperative, the recorded variables consisted of: time of mechanical ventilation, ICU and hospital stay days, postoperative complications (e.g. hemodynamic instability, inotrope usage, arrhythmias), renal complications, infectious (sepsis, mediastinitis), severe blood lose, neurological complications: ischemic or hemoragic stroke, and mortality rate. According to CRP test, the patients were classified into normal (0 - 5 mg/l), mildly (5 - 40 mg/l), moderately (40 - 200 mg/L) or severely increased (>200 mg/l) values. We investigated a composite outcome comprising three combined outcomes: mortality, renal failure, and stroke, using univariate and multivariate analysis.
Statistical Methods
The collected data were analyzed using SPSS software version 23.0 (SPSS Inc., Chicago: IL). The data were presented with descriptive methods (frequency, percentage, mean ± standard deviation, rates in case of nominal variables). Parametric data were compared using the independent sample t-test and non-parametric data using Pearson’s chi-square for ordinal data or Mann-Whitney U test for continuous data. Comparison between multiple groups was done using the ANOVA test. Scatter plots were uses to assess association between PFA and CRP. Receiver operating curves (ROC) were used to find the sensitivity and specificity of PFA and CRP to predict mortality. Univariate regression with Cox-proportional hazards and multiple logistic regression were used to assess the effect of several variables on adverse outcomes. Odds ratios and 95% confidence intervals are given for each tested variable. P-values less than 0.05 were considered statistically significant for the test we performed. All P-values were 2-tailed.
3. Results
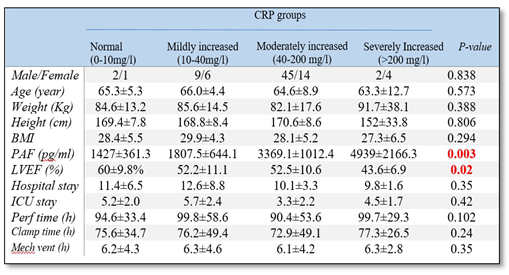
Overall, 87 patients’ data were evaluated: 61 male and 26 female with major cardiac surgery. The mean age was 64.9 years. The study population included patients that were operated for coronary artery bypass grafts, mitral or aortic valve replacements, bentall procedure, aortic aneurysm repair, atrial septal defect correction or aortic valve and ascending aorta repair. The cohort was divided into 4 groups based on CRP levels: normal values (0-10 mg/l), mild increased (10-40 mg/l), moderate increased (40-200mg/l) and severe increased (>200 mg/l) levels. Table 1 shows demographic data, preoperative and postoperative variables of the study group based on CRP levels. There was no significant difference between the 4 CRP groups in terms of perfusion time (p=0.102), clamp time (p=0.24), hours of mechanical ventilation (p=0.35), inotropic score (0.31), vasoactive-inotropic score (0.95), duration of hospital stay (p=0.35) days of stay in the intensive care unit (p=0.42). However, the group with severe increased CRP levels had higher PAF levels (p=0.003) and lower baseline left ventricular ejection fraction ( p=0.02) (Table 1).
The ANOVA test has shown that patients with increased CRP values had also increased PAF values with significant statistical differences between the 4 classes of CRP. Furthermore there was a significant positive linear correlation between preoperative PAF levels and postoperative CRP levels (r=0.72, p=0.0001) (Figure 1).
Receiver–operating characteristic (ROC) curve analysis showed that both PAF and CRP can predict post-operative mortality with a good sensitivity and specificity and an elevated AUC (area under the curve). In addition, we could assess the values of CRP and PAF that had the highest sensitivity and specificity ratio for the mortality outcome. (Figure 2a,b).
Univariate analysis showed that increased age > 65, increased BMI > 30, CRP > 80 mg/l, PAF > 5000 pg/ml and prolonged mechanical ventilation time were associated with combined outcome of stroke, acute kidney injury and death with a hazard ratio of 2.45 (95%CI 0.48-18.3) for CRP>80 mg/l and a HR of 2.62 (95%CI 0.37-20.0) for PAF > 5000 pg/ml. However in multivariate analysis we found no significant independent association between PFA, CRP, age, BMI, prolonged mechanical ventilation and the combined outcome.

Table 2.
Univariate analysis to assess predictor of combined outcome: stroke-acute kindey failure and death.
Table 2.
Univariate analysis to assess predictor of combined outcome: stroke-acute kindey failure and death.
| Variable | Odds ratio | 95% Confidence Intervals |
|---|---|---|
| Age | 1.10 | 1.02-1.19 |
| BMI | 1.75 | 0.33-9.3 |
| PAF | 2.62 | 0.37-20.0 |
| VIS | 0.89 | 0.78-0.99 |
| Clamp time >90 min | 0.34 | 0.38-3.1 |
| Perf time >180 min | 0.89 | 0.84-0.98 |
| Mech ventil | 1.85 | 0.32-10.7 |
| CRP | 2.45 | 0.48-18.3 |
Table 3.
Multivariate analysis for predictors of combined endpoint: stroke-acute kindey failure and death.
Table 3.
Multivariate analysis for predictors of combined endpoint: stroke-acute kindey failure and death.
| Variable | Odds ratio | 95% Confidence Intervals |
|---|---|---|
| Age | 0.25 | 0.03-2.56 |
| BMI | 0.48 | 0.08-2.82 |
| PAF | 0.36 | 0.01-8.9 |
| Mech ventil | 0.81 | 0.12-5.41 |
| CRP | 0.37 | 0.01-8.96 |
4. Discussion
This study shows that preoperative PAF and postoperative CRP are predictors of unfavorable prognosis after major cardiac surgery. Our findings contribute to the existing understanding of CRP as a prognostic indicator both preoperatively [15-17], and postoperatively [18] following major heart surgery. Nonetheless, the medical literature contains insufficient information regarding the predictive value of PAF in cardiovascular disease.
The term "platelet-activating factor" was first used by Benveniste and coworkers in their key 1972 publication in the Journal of Experimental Medicine [19], referring to a biochemical response produced by activated basophils that induced platelet aggregation . Platelet-activating factor, a proinflammatory mediator, has been identified as a potential contributor throughout all types of coronary artery disease[20]. Evidence indicates that the well-known signaling effects of PAF are closely related to atherosclerosis which is facilitated via multiple pathways including inflammation, endothelial dysfunction, oxidative and nitrosative stress, and platelet reactivity. PAF is a significant pro-inflammatory mediator associated with various illnesses and chronic diseases [21], including renal disorders, cerebrovascular infections, and cardiovascular diseases [22]. Changes in cardiac function, particularly the decrease in cardiac output noted in vivo following PAF infusion, may arise from either a direct effect on the heart muscle or from an indirect effect, including systemic alterations and fluctuations in pre- and afterload pressures. Moreover, modifications in cardiac function may be dependent upon the influence of PAF on coronary circulation, the conduction system, and the contractile properties of the myocardium [23].
CRP was first described by Tillet and Francis in 1930 and recognized as the prototype of acute phase plasma proteins [24]. In healthy individuals, serum CRP levels generally remain under 10 mg/l, whereas patients with inflammatory disorders have a notable elevation, ranging from 10 to 200 mg/l potentially increasing by 1000-fold or more in reaction to inflammation [25]. Increased CRP levels at admission correlate with worse outcomes in acute coronary syndrome, while peak CRP levels following acute myocardial infarction are linked to mortality, myocardial infarction, and ischemic cerebrovascular events [26].
Patients undergoing heart surgery under cardiopulmonary bypass frequently experience systemic reactions that causes postoperative morbidity and prolonged hospital stay. Elevated CRP levels have been observed in individuals undergoing cardiopulmonary bypass; however, association with increased PAF levels has not been demonstrated before. Reperfusion has been directly linked to the migration of neutrophils into the previously ischemic region [27] , their adhesion to cardiac myocytes, and activation by ischemic products [28]; furthermore, activated neutrophils liberate PAF [29]. Neutrophils have been shown to move into ischemic myocardium following both prolonged obstruction of a coronary artery branch [30,31] and subsequent reperfusion of the ischemic area [32]. Activated neutrophils generate PAF, which interacts with specific receptors on myocytes, resulting in a constant effect on transmembrane potentials that can induce arrhythmias. Reperfusion of ischemic myocardium is often linked to arrhythmias [33,34]. Our study demonstrates a positive strong correlation between PAF levels and CRP levels.
The specific binding of CRP to diverse cells, such as macrophages, neutrophil granulocytes, and platelets, together with the subsequent change of their function, has been documented previously [35-39]. The reports about the impact of CRP on platelets are however controversial. First, the enhancement of PAF-induced aggregation by CRP has been documented. On the contrary, native CRP was observed to suppress platelet activation [40,41], while other studies indicated that CRP did not alter platelet responses to diverse stimuli [42, 43].
There is growing evidence that platelet reactivity is frequently modified following infection or myocardial tissue injury [44].PAF, a very effective platelet aggregating agent, has recently been identified as a significant mediator of tissue injury and inflammation [45]. Elevated plasma and tissue concentrations of PAF have been observed in conjunction with infection or tissue damage under various conditions. Given that CRP increases in serum under similar pathological conditions, the potential interactions between PAF and CRP deserve further attention. Endogenous human CRP was demonstrated to suppress PAF-induced aggregation of washed rabbit platelets, but not of human platelets, indicating species-specific action of CRP. CRP reduced the specific binding of PAF to platelets, indicating a potential direct interaction with PAF membrane receptors.
It is noteworthy that CRP, apart from the action on platelets, has been demonstrated to inhibit the binding of PAF to human neutrophils [46].
A deeper comprehension of the mechanisms underlying inflammation and thrombosis would provide improved therapeutic developments and more personalized treatment protocols for patients undergoing cardiopulmonary bypass. It was found that CRP binds to both PAF and its metabolite and enhances PAF induced inflammation. CRP exhibits strong affinity for phosphocholine-containing lipids, hence also binding to PAF, which is a phosphocholine-containing lipid. CRP shows a positive correlation with COX-2 expression in monocytes , which may conceivably facilitate platelet activation through Thromboxane A2. In the research conducted by Sato et al., CRP was observed to bind to PAF in a concentration-dependent fashion. Both CRP and PAF seem to play significant roles in the pathogenesis of several inflammatory disorders, with CRP potentially exacerbating the pathogenesis of PAF-induced inflammatory conditions. Experimental studies support the involvement of PAF in ischemia and reperfusion injury of the heart: myocardial synthesis of PAF occurs post-myocardial infarction[47], and an intravascular release of this mediator has been identified in the blood of patients with coronary artery disease who underwent atrial pacing to assess the severity of ischemia [48]. Additionally, PAF was identified in the coronary sinus during occlusion and reperfusion injury [49].
Renal failure is a common complication following major cardiac surgery, nad is associated with prolonged hospital stays, elevated costs, and increased postoperative mortality [50]. In our study, acute kidney injury, characterized by new renal failure or exacerbation of pre-existing renal failure, was observed in 21% of patients. The incidence of this complication in the medical literature ranges from 3% to 30% owing to differing definitions of renal failure. Hobson et al. indicated that the mortality risk associated with renal failure after major cardiac surgery persists at an elevated level over a decade [51]. Nevertheless, other researchers have shown that rapid recovery of renal function following acute kidney injury correlates with increased long-term survival. The causes of renal failure post-cardiac surgery may include : cardiopulmonary bypass, renal toxicity due to drugs, volume depletion, vasoactive inotropic agents, or decreased cardiac output [52]. Improving the patient's clincial condition, stopping the use of nephrotoxic medications, and maintaining normovolemia have been identified as ways of preventing renal failure after cardiac surgery [53].
Stroke continues to be a severe complication following cardiac surgical procedures, with an incidence reaching up to 6% [54]. Prior research has sought to determine predictors of stroke following major cardiac surgery. Limited large-scale prospective studies exist regarding the incidence of stroke and its related risk factors [55]. Prior research in the medical literature has suggested that the cause of stroke following cardiac surgery is multifactorial: Age beyond 70 years is one of the most frequently cited independent predictors of stroke [56], history of vertebral events, hypertension, diabetes, peripheral arterial disease, prior cardiac surgery,endocarditis, CBP time longer than 2 hours, and high transfusion reguirements all were demonstrated to be risk factor for stroke [57]. Advanced age is not considered a direct cause of stroke; instead, it serves as an indicator of advanced atherosclerosis [58]. The incidence of stroke in our study was 1.15%.
Several risk factors have been identified as predictors of mortality after major cardiac surgery. Age and sex have been linked to elevated mortality in some research, primarily focusing on coronary artery by-pass procedures [59]. Prolonged cardiopulmonary bypass time and aortic-cross clamp time as well as prolonged mechanical ventilation have also been associated with increased mortality [60-62]. Our study confirmed that age >65, BMI>30, and prolonged mechanical ventilation time were associated with negative outcomes. Furthermore, our investigation reveals that both preoperative PAF and postoperative CRP serve as predictors for death/stroke/AKI, demonstrating superior predictive capability compared to the above mentioned predictors, as evidenced by their odds ratios.
Despite logistic regression being a robust analytical technique for binary outcomes, the results from univariate and multiple logistic regressions often exhibit discrepancies. A covariate may exhibit a substantial influence in univariate analysis yet play no role in the multiple logistic regression model. Our current investigation showed a significant association between PAF, CRP levels and adverse outcomes after major cardiac surgery, with hazard ratios > 2; however it does not demonstrate an independent prognostic significance of PAF and CRP for morbidity and mortality. Conversely, our findings underscore the significance of other clinical characteristics including age, BMI, mechanical ventilation duration, together with PAF and CRP, all of which, together were associated with poorer prognosis.
Whether PAF and CRP serve as a markesr or plays a role in the mechanisms of atherothrombosis continues, necessitating further investigation. The development of selective, high affinity PAF receptor inhibitors might convey therapeutic benefits in ischemia, thrombosis and arrhythmias that occur after cardiopulmonary bypass in major cardiac surgery.
Limitations
The main limitation is the small sample size of patients in our study. A higher number would have indicated a more robust correlation among PFA, CRP, and death.
The association between PAF, CRP, and the adverse composite outcome, significantly decreased in the adjusted model. It is possible that other significant prognostic factors have not been accounted for. The prognostic value of platelet-activating factor requires validation in prospective studies with meticulous adjustment for relevant clinical variables.
5. Conclusions
Preoperative PAF and postoperative CRP are predictors of unfavorable prognosis after major cardiac surgery. Patients with elevated CRP levels also showed increased PAF values, revealing a significant positive correlation between preoperative PAF levels and postoperative CRP levels. CRP > 80 mg/l and PAF > 5000 pg/ml were associated with highest odds ratio for the combined outcome of stroke, acute kidney disease and death.
Author Contributions
Conceptualization, EP, A.S., G.C.; methodology, A.S., A.G.S., N.T.; software, A.S., G.C.; validation, EP, A.S., ADB, ICB, RMP, G.C.; formal analysis, A.S., G.C.; investigation, A.S., A.G.S., N.T.; resources, A.S., A.G.S., N.T.; data curation, EP, A.S., A.G.S., N.T., G.C.; writing—original draft preparation, A.S., G.C.; writing—review and editing, EP,ADB, ICB, RMP, A.G.S., N.T.,G.C. visualization: EP, A.S., ADB, ICB, RMP, A.G.S., N.T.G.C.; supervision, EP,A.S.,ICB; project administration, A.S.; funding acquisition, A.S. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki and approved by the Ethics Committee of the “Iuliu Hatieganu” University of Medicine” Cluj-Napoca, Romania (approval number 259 on 28 September 2023).
Informed Consent Statement
Informed consent was waived because of the retrospective nature of the study, and the analysis used anonymous clinical data.
Data Availability Statement
Data supporting the reported results can be found in Mega cloud through the following link: https://mega.nz/fm/YFERRRoC.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Bernard, N.A., Williams, R.W. and Spencer, E.M. Preoperative Patient Assessment: A Review of Literature and Recommendations. Annals of the Royal College of Surgeons of England 1994, 76, 293–297. [Google Scholar]
- Van Klei, W.A., Grobbee, D.E., Rutten, C.L., Hennis, P.J., Knape, J.T., Kalkman, C.J., et al. Role of History and Physical Examination in Preoperative Evaluation. European Journal of Anaesthesiology 2003, 20, 612–618. [Google Scholar] [CrossRef]
- Johnson, R.K. and Mortimer, A.J. Routine Preoperative Blood Testing: Is It a Necessary? Anaesthesia 2002, 57, 914–917. [Google Scholar] [CrossRef] [PubMed]
- Krishnammurthy, A. , Dutta, D., Phililps, J. and Methal, N. (2007) Are We Still Performing too Many Blood Tests? Quality and Safety in Health Care, 16, 400.
- Ishii S, Kuwaki T, Nagase T, Maki K, Tashiro F, Sunaga S, Cao WH, Kume K, Fukuchi Y, Ikuta K, Miyazaki J, Kumada M, Shimizu T. Impaired anaphylactic responses with intact sensitivity to endotoxin in mice lacking a platelet-activating factor receptor. J Exp Med. 1998 Jun 01;187(11):1779-88.
- Won Song, S. , Yi, G.J., Lee, S., Nam Youn, Y., Young Sul, S. and Jong Yoo, K. (2008) Perioperative Indicators of Stress Response and Postoperative Inflammatory Complications in Patients Undergoing Off-Pump Coronary Artery Bypass Surgery.
- Benveniste J, Henson PM, Cochrane CJ: Leukocyte-dependent histamine release from rabbit platelets. The role of IgE, basophils, and a platelet-activating factor. J Exp Med 136:1365- 1377.1972 10.
- Chignard M, Le Couedic JP, Ten& M, et al: The role of platelet-activating factor in platelet aggregation. Nature 279:799- 800, 1979.
- Benveniste J: PAF-acether, an ether phospholipid with biological activity, in Karnovsky ML, Leaf A, Bolis LC (ed): Biological Membranes. New-York, NY, Liss, 1988, pp 75-85.
- Pinckard RN, Ludwig JC, MC Manus LM: Platelet-activating factors, in Gallin JI, Goldstein I, Snyderman R (ed): Inflammation. Basic Principles and Clinical Correlates. New York, NY, Raven, 1988, pp 139-167.
- Hedlund P: Clinical and experimental studies on C-reactive protein (acute phase protein). Acta Med Scand Suppl 1961, 361: 1-71.
- Balbay Y, Tikiz H, Baptiste RJ, Ayaz S, Sasmaz H, Korkmaz S: Circulating interleukin-1 beta, interleukin-6, tumor necrosis factor-alpha, and soluble ICAM-1 in patients with chronic stable angina and myocardial infarction. Angiology 2001, 52: 109-114.
- Filep JG, Hermán F, Kelemen E, Földes-Filep E. C-reactive protein inhibits binding of platelet-activating factor to human platelets. Thromb Res. 1991 Feb 15;61(4):411-21.
- Sato A, Oe K, Yamanaka H, Yokoyama I, Ebina K. C-reactive protein specifically enhances platelet-activating factor-induced inflammatory activity in vivo. Eur J Pharmacol. 2014 Dec 15;745:46-51.
- Brunetti ND, Troccoli R, Correale M, Pellegrino PL, Di Biase M: C-reactive protein in patients with acute coronary syndrome: correlation with diagnosis, myocardial damage, ejection fraction and angiographic findings. Int J Cardiol 2006, 109: 248-256.
- Tian H, Jiang X, Duan G, Chen J, Liu Q, Zhang Y, Li S, Bao X, Huang H. Preoperative inflammatory markers predict postoperative clinical outcomes in patients undergoing heart valve surgery: A large-sample retrospective study. Front Immunol. 2023 Mar 31;14:1159089. [CrossRef] [PubMed]
- Tjörvi E. Perry, Jochen D. Muehlschlegel, Kuang-Yu Liu, Amanda A. Fox, Charles D. Collard, Simon C. Body, Stanton K. Shernan, for the CABG Genomics Investigators; Preoperative C-reactive Protein Predicts Long-term Mortality and Hospital Length of Stay after Primary, Nonemergent Coronary Artery Bypass Grafting. Anesthesiology 2010, 112, 607–613. [Google Scholar] [CrossRef] [PubMed]
- Min JJ, Nam K, Kim TK, Kim HJ, Seo JH, Hwang HY, Kim KB, Murkin JM, Hong DM, Jeon Y. Relationship between early postoperative C-reactive protein elevation and long-term postoperative major adverse cardiovascular and cerebral events in patients undergoing off-pump coronary artery bypass graft surgery: a retrospective study. Br J Anaesth. 2014 Sep;113(3):391-401. Erratum in: Br J Anaesth. 2014 Nov;113(5):895. PMID: 24829443. [CrossRef] [PubMed]
- Benveniste J, Henson PM, Cochrane CG: Leukocyte-dependent histamine release from rabbit platelets: the role of IgE, basophils and a platelet-activating factor. J Exp Med 136: 1356, 1972.
- Benveniste J, Chignard M. A role for PAF-acether (platelet-activating factor) in platelet-dependent vascular diseases? Circulation. 1985 Oct;72(4):713-7. [CrossRef] [PubMed]
- Choi, B.Y.; Ye, Y.-M. Role of Platelet-Activating Factor in the Pathogenesis of Chronic Spontaneous Urticaria. Int. J. Mol. Sci. 2024, 25, 12143. [Google Scholar] [CrossRef] [PubMed]
- Barbaro, J.F. , Zvaifler N.J. Antigen induced histamine release from platelets of rabbits producing homologous PGA antibody. Proc. Soc. Exp. Biol. Med. 1966;122:1245–1247.
- Goldstein RE, Feuerstein GZ, Bradley LM, Stambouly JJ, Laurindofrm, Davenport NJ. Cardiovascular effects of platelet activat-ing factor. Lipids 26: 1250 –1256, 1991.
- Tillett WS, Francis T, Jr. Serological reactions in pneumonia with a non-protein somatic fraction of pneumococcus. J Exp Med (1930) 52:561–71.
- Calu, V.; Piriianu, C.; Miron, A.; Grigorean, V.T. Utilizing C-Reactive Protein (CRP) and CRP Ratios for Early Detection of Postoperative Complications Following Rectal Cancer Surgery. Life 2024, 14, 1465. [Google Scholar] [CrossRef] [PubMed]
- Ha, E.T.; Haessler, J.; Taylor, K.D.; Tuftin, B.; Briggs, M.; Parikh, M.A.; Peterson, S.J.; Gerszten, R.E.; Wilson, J.G.; Kelsey, K.; et al. The Relationship of Duffy Gene Polymorphism with High-Sensitivity C-Reactive Protein, Mortality, and Cardiovascular Outcomes in Black Individuals. Genes 2024, 15, 1382. [Google Scholar] [CrossRef] [PubMed]
- Engler, RL. Dahlgren MD, Peterson MA. et al: Accumulation of polymorphonuclear leukocytes during 3h experimental myocardial ischemia. Am J Physiol 1986:25I:H9.3-H]OO.
- Dreyer WJ. Michael LH, West MS, et al: Neutrophil accumulation in ischemic canine myocardium. Circulation 1991:84:400-411.
- Go, LO. Murry CE. Richard VJ. et al: Myocardial neutrophil accumulation during reperfusion after reversible or irreversible ischemic injury. Am J Physiol 1988;255:H188-HI9«.
- Corr PB, Witkowski FX: Potential electrophysiologic mechanisms responsible for dysrhythmias associated with reperfusion of ischaemic myocardium. Circulation t983:68(Suppl 0:1-16-1-24.
- Manning, AS. Hearse DJ: Reperftision-induced arrhythmias: Mechanisms and prevention. J Mol Cell Cardiol 1984:16:497-518.
- Annable CR, McManus LM, Carey KD, Pinckard RN. Isolationof platelet-activating factor (PAF) from ischemic baboon myocar-dium. Federation Proc 44: 1271, 1985.
- Montrucchio G, Camussi G, Tetta C, Emanuelli G, Orzan F, Libero L, Brusca A. Intravascular release of platelet-activating factorduring atrial pacing. Lancet 2: 293, 1986.
- Ko W, Hawes AS, Lazenby WD, Calvano SE, Shin YT, Zelano JA, Antonacci AC, Isom OW, Krieger KH. Myocardial reperfusion injury. Platelet-activating factor stimulates polymorphonuclear leukocyte hydrogen peroxide production during myocardial reperfusion. J Thorac Cardiovasc Surg. 1991 Aug;102(2):297-308. [PubMed]
- Ridker PM: C-reactive protein and the prediction of cardiovascular events among those at intermediate risk: moving an inflammatory hypothesis toward consensus. J Am Coll Cardiol 2007, 49: 2129-2138.
- Vigo, C. Effect of C-reactive protein on platelet-activating factor-induced platelet aggregation and membrane stabilization. J. Biol. Chem., 260, 3418-3422, 1985.
- Mortensen, R.F. , Osmond, A.P., Lint, T.F. and Gewurz, H.Interaction of C-reactive protein with lymphocytes and monocytes: complement-de endent adherence and phagocytosis. J Immunol., 117, 774-7[1, 1976.
- Fiedel, B.A. , Simpson, R.M. and Gewurz, H. Activation of latelets b modified C-reactive protein. Immunology, s, c39-447, 1982.
- Muller, H. and Fehr, J. Binding of C-reactive protein to human polymorphonuclear leukocytes: evidence for association of binding sites with Fc receptors. J. Immunol., I36, 2202-2207, 1986.
- Buchta, R. , Pontet, M. and Fridkin, M. Binding of C-reactive protein to human neutrophils. FEBS Lett.,a, 165-168, 1987.
- Miyazawa, K. , Kiyono, S. and Inoue,K. Modulation of stimulusdependent human platelet-activation by C-reactive protein modified with active oxygen species. J. Immunol., 141, 570-574, 1988.
- Fiedel, B.A. and Gewurz, H, Effects of C-reactive protein on platelet function I. Inhibition of platelet aggregation and release reactions. J. Immunol., 116, 1289-1294, 1976.
- Fiedel, B.A. and Gewurz, H. Effects of C-reactive protein on platelet function II. Inhibition by CRP of platelet reactivities stimulated by poly-L-lysine, ADP, epinephrine, and collagen. J. Immunol., 117, 1073-1078, 1976.
- Page, C.P. processes. CRP, PAF AND PLATELETS 421 The involvement of platelets in non-thrombotic Trends Pharmacol. Sci., 2, 66-71, 1988.
- Braquet, P., Touqui, L., Shen, T. Y. and Vargaftig, B. B. Perspectives in platelet-activating factor research. Pharmacol. Rev., 3, 98-145, 1987.
- Filep, J. and Foldes-Filep, E. Effects of C-reactive protein on human neutrophil granulocytes challenged with N-formylmethionyl-leucyl-phenylalanine and platelet-activating factor. Life Sci., 44, 517-524, 1989.
- Dalmaso, B.; Silva-Junior, I.A.d.; Jancar, S.; Del Debbio, C.B. Platelet-Activating Factor Receptor (PAFR) Regulates Retinal Progenitor/Stem Cells Profile in Ciliary Epithelium Cells. Int. J. Mol. Sci. 2024, 25, 3084. [Google Scholar] [CrossRef] [PubMed]
- Margariti, A.; Papakonstantinou, V.D.; Stamatakis, G.M.; Demopoulos, C.A.; Machalia, C.; Emmanouilidou, E.; Schnakenburg, G.; Nika, M.-C.; Thomaidis, N.S.; Philippopoulos, A.I. First-Row Transition Metal Complexes Incorporating the 2-(2′-pyridyl)quinoxaline Ligand (pqx), as Potent Inflammatory Mediators: Cytotoxic Properties and Biological Activities against the Platelet-Activating Factor (PAF) and Thrombin. Molecules 2023, 28, 6899. [Google Scholar] [CrossRef] [PubMed]
- Maruyama M, Farber NE, Vercellotti GM, Jacob HS, Gross GJ. Evidence for a role of platelet activating factor in the pathogenesis of irreversible but not reversible myocardial injury after reperfusion in dogs. Am Heart J. 1990 Sep;120(3):510-20.
- Chertow GM, Levy EM, Hammermeister KE, Grover F, Daley J. Independent association between acute renal failure and mortality following cardiac surgery. Am J Med. 1998;104(4):343-348.
- Hobson CE, Yavas S, Segal MS, et al. Acute kidney injury is associated with increased long-term mortality after cardiothoracic surgery. Circulation. 2009;119(18):2444-2453.
- Swaminathan M, Hudson CCC, Phillips-Bute BG, et al. Impact of early renal recovery on survival after cardiac surgery-associated acute kidney injury. Ann Thorac Surg. 2010;89(4):1098-1104.
- Olivero JJ, Olivero JJ, Nguyen PT, Kagan A. Acute kidney injury after cardiovascular surgery: an overview. Methodist Debakey Cardiovasc J. 2012;8(3):31-36.
- Salazar JD, Wityk RJ, Grega MA, et al. Stroke after cardiac surgery: short- and long-term outcomes. Ann Thorac Surg2001;72:1195–202.
- Stamou SC, Hill PC, Dangas G, et al. Stroke after coronary artery bypass: incidence, predictors, and clinical outcome.
- Stroke 2001;32:1508–13.
- Borger MA, Ivanov J, Weisel RD, Rao V, Peniston CM. Stroke during coronary bypass surgery: principal role of cerebral macroemboli. Eur J Cardiothorac Surg 2001;19:627–32.
- Newman MF, Wolman R, Kanchuger M, et al. Multicenter preoperative stroke risk index for patients undergoing coronary artery bypass graft surgery. Circulation 1996;94(Suppl 2):74–80.
- Head T, Daunert S, Goldschmidt-Clermont PJ. The Aging Risk and Atherosclerosis: A Fresh Look at Arterial Homeostasis. Front Genet. 2017 Dec 14;8:216.
- Kollef MH, Wragge T, Pasque C. Determinants of mortality and multiorgan dysfunction in cardiac surgery patients requiring prolonged mechanical ventilation. Chest. 1995;107:1395–401.
- Harker LA, Malpass TW, Branson HE, Hessel EA, 2nd, Slichter SJ. Mechanism of abnormal bleeding in patients undergoing cardiopulmonary bypass: Acquired transient platelet dysfunction associated with selective alpha-granule release. Blood. 1980;56:824–34.
- Floyd RD, Sabiston DC, Jr, Lee KL, Jones RH. The effect of duration of hypothermic cardioplegia in ventricular function. J Thorac Cardiovasc Surg. 1983;85:606–11.
- Hugot P, Sicsic JC, Schaffuser A, Sellin M, Corbineau H, Chaperon J, et al. Base deficit in immediate postoperative period of coronary surgery with cardiopulmonary bypass and length of stay in intensive care unit. Intensive Care Med. 2003;29:257–61.
Figure 1.
Scatter plot with line of best fit showing the association between preoperative PFA and postoperative CRP.
Figure 1.
Scatter plot with line of best fit showing the association between preoperative PFA and postoperative CRP.
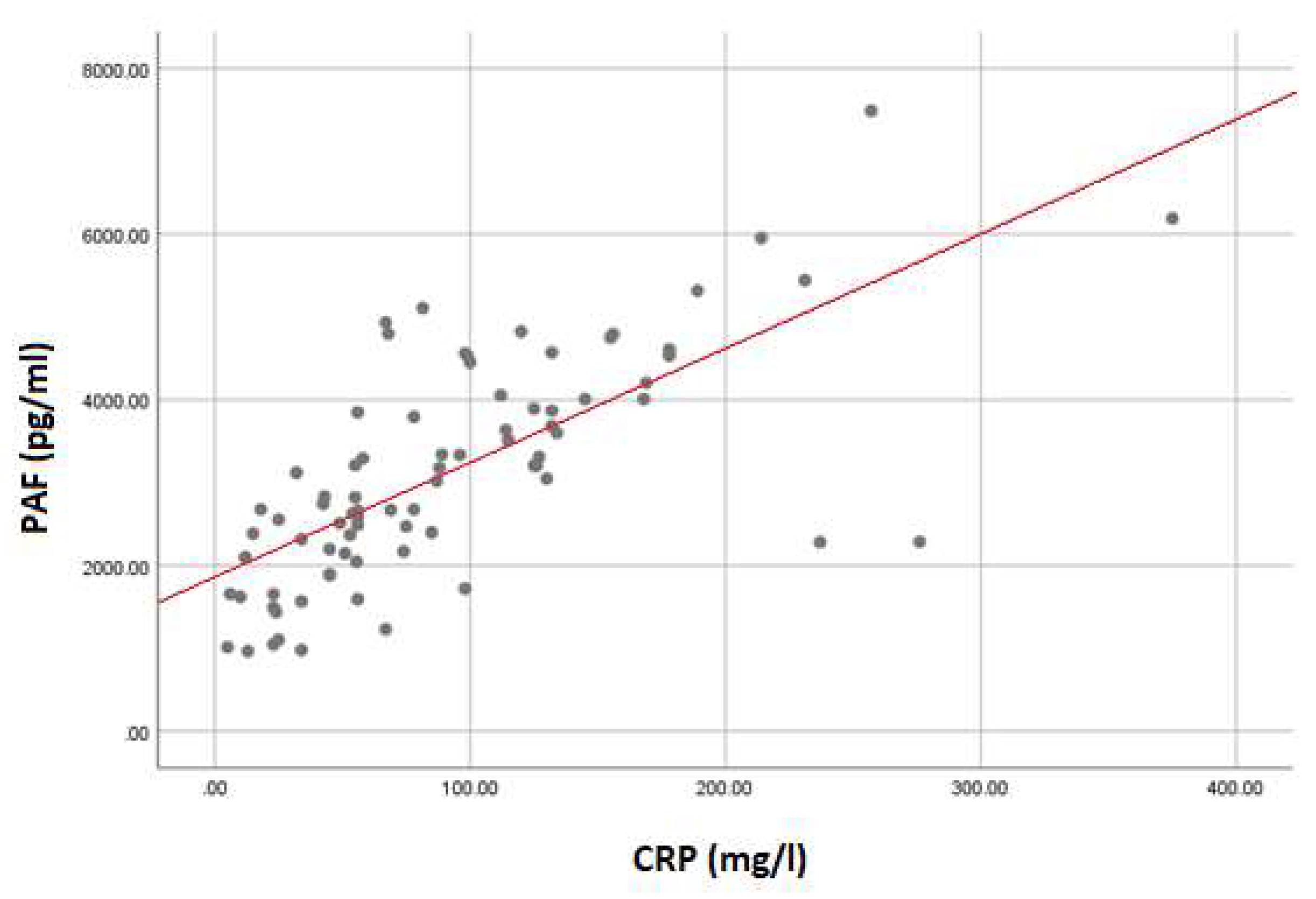
Figure 2.
Receiver–operating characteristic (ROC) curve analysis shows the sensitivity and specificity of PAF and CRP in predicting mortality after major cardiac surgery. 2a) for PAF, the area under the curve is 0.625. A value of > 3033 pg/ml predicts mortality with a sensitivity of 83% and a specificity of 53%. 2b) for CRP the area under the curve is 0.688. A value of above 80 mg/l predicts mortality with a sensitivity of 83% and a specificity of 56%.
Figure 2.
Receiver–operating characteristic (ROC) curve analysis shows the sensitivity and specificity of PAF and CRP in predicting mortality after major cardiac surgery. 2a) for PAF, the area under the curve is 0.625. A value of > 3033 pg/ml predicts mortality with a sensitivity of 83% and a specificity of 53%. 2b) for CRP the area under the curve is 0.688. A value of above 80 mg/l predicts mortality with a sensitivity of 83% and a specificity of 56%.
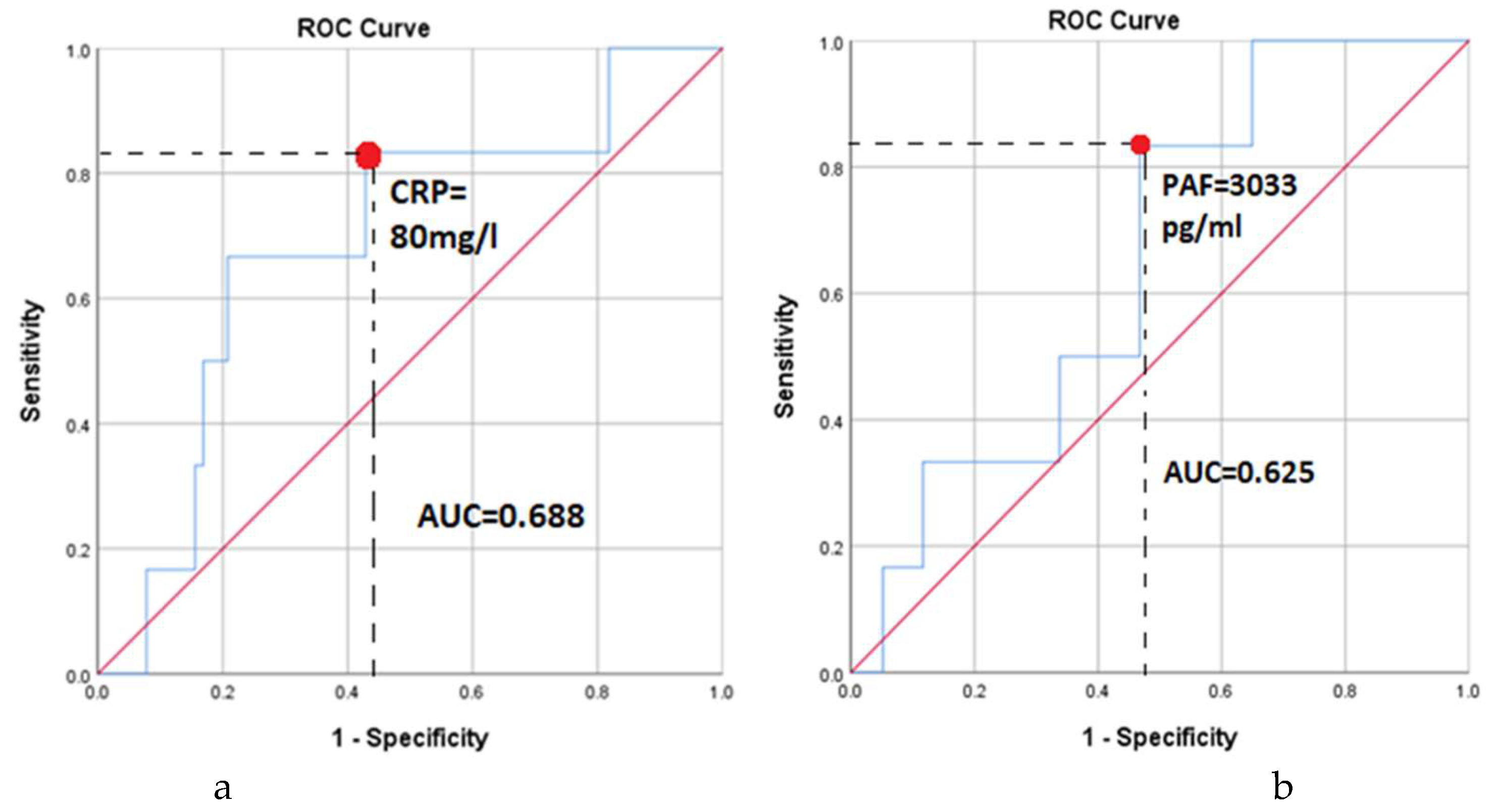
Table 1.
The study population was categorized into four CRP groups, which were compared using the one-way ANOVA test. (LVEF=left ventricular ejection fraction; perf time=cardiopulmonary bypass duration; clamp time=aortic cross-clamping duration; mech vent=mechanical ventilation duration).
Table 1.
The study population was categorized into four CRP groups, which were compared using the one-way ANOVA test. (LVEF=left ventricular ejection fraction; perf time=cardiopulmonary bypass duration; clamp time=aortic cross-clamping duration; mech vent=mechanical ventilation duration).
 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



