
Submitted:
22 November 2024
Posted:
25 November 2024
You are already at the latest version
Abstract
Objectives: This study aims to explore perspectives and opinions from healthcare professionals and people at risk of type 2 diabetes mellitus (T2DM) to inform the design of PREDIABETEXT, a new digital multifaceted intervention to prevent T2DM. Methods: in this qualitative study, we purposefully recruited 15 healthcare professionals (doctors and nurses) working in primary healthcare centers in Mallorca (Spain), and 15 of their patients at risk of T2DM (HbA1c 6%-6.4%, and/or fasting plasma glucose 110-125 mg/dl). We collected the data through semi-structured phone interviews, using an interview guide aimed at gathering participants’ views about the two PREDIABETEXT proposed co-interventions (educational intervention targeted to professionals and delivered as an online training course, and; behavioral intervention targeted to patients and delivered using SMS short text messages). The interviews were audio-recorded, verbatim transcribed and analyzed using a thematic analysis approach. Results: Primary healthcare professionals valued a prediabetes training course for standardizing care and supporting diabetes prevention. They preferred a blended format with content on early detection, intervention, and monitoring. They perceived SMS reminders to their patients as potentially useful for reinforcing guidelines and improving care. Patients, who faced challenges maintaining a healthy diet and exercise routine, viewed SMS as potentially motivational and informative, offering suggestions on content, format, and frequency to enhance its intended benefits. Conclusions: This qualitative study provided valuable insights from primary care professionals and patients that will inform the user-centered design of the PREDIABETEXT intervention.
Keywords:
diabetes mellitus
; digital health
; prediabetic state
; primary health care
1. Introduction
Type 2 diabetes mellitus (T2DM) is a prevalent and chronic condition affecting approximately 4 million individuals in Spain [1]. Those with T2DM face a heightened susceptibility to severe complications, including but not limited to blindness, lower-limb amputations, kidney disease, and cardiovascular issues, all of which significantly diminish both their quality of life and life expectancy. The associated complications of T2DM pose a substantial financial burden on the Spanish National Health System (NHS), accounting for an annual direct cost of €5.1 billion, equivalent to 8% of the total NHS expenditure. Additionally, there are €1.5 billion in expenses related to diabetes-induced complications. Beyond the financial toll, T2DM complications exert an impact on an individual's ability to work throughout their productive years, leading to labor productivity losses amounting to approximately €2.8 billion in Spain [2]. Importantly, T2DM and its risk factors disproportionately affect socioeconomically vulnerable populations in Spain, with a prevalence rate of 9.3% in the lowest socio-economic status (V to VI) compared to 4.5% in the upper class (I and II) [3].
Prediabetes, as defined by the National Institute for Health and Care Excellence (NICE) [4] and the Working Group of the Spanish Diabetes Society [5], refers to an HbA1c level ranging from 6% to 6.4% or fasting plasma glucose levels of 110-125 mg/dl, or both. It affects approximately 7.3% of the global population [6]; however, in Spain, the prevalence is notably higher, around 13-15% [1]. Prediabetes presents a substantial risk for progressing to diabetes, with an annualized conversion rate ranging from 5% to 10%, and a comparable proportion returning to normoglycemia [7]. Moreover, individuals with prediabetes face an elevated risk of developing cardiovascular diseases [8].
For those with prediabetes, lifestyle modification emphasizing a healthy diet and increased physical activity stands as the primary strategy for diabetes prevention, demonstrating a relative-risk reduction of 40-70% [7]. Not surprisingly, recommendations aimed at promoting T2DM prevention through healthy lifestyles are now widely integrated into clinical practice guidelines [9]. However, implementing interventions to support such modifications in the healthcare setting remains a considerable challenge, due to numerous barriers, both at the patient and healthcare professional levels. On the patient side, the acceptance of lifestyle interventions is influenced not only by intrapersonal factors such as personality but also by external determinants related to healthcare professionals and the environment[10]. Regarding healthcare professionals, their involvement in lifestyle-based prevention programs is generally suboptimal, primarily due to a lack of confidence in the programs' effectiveness, deficient communication skills, inadequate training in brief counseling techniques, and limited organizational support [11].
Identifying highly implementable and effective interventions that promote healthy lifestyles among individuals with prediabetes is therefore very much needed. Digital health interventions have the potential to be a low cost, highly scalable, and sustainable strategy for health systems for improving health at the population level. However, there is a lack of evidence-based, digital health interventions to promote lifestyle changes in people with prediabetes [12,13]. Crucially, the design of these interventions needs to take close consideration of users’ views and preferences [14].
As part of a wider project [15], we set up to design a multifaceted intervention (targeted at primary care patients and healthcare professionals) to prevent T2DM. It was considered of utmost importance to meaningfully involve patients and healthcare providers in the design of this intervention to ensure its acceptability, optimize its potential impact, and facilitate its implementation in Spanish primary healthcare centers.
The objective of this study was to explore primary healthcare patients’ and providers’ perspectives regarding the design of PREDIABETEXT, a new multifaceted digital health intervention to prevent T2DM by supporting lifestyle changes in people at risk of T2DM based on: i) the use of a system comprising mobile health (mHealth) technology integrated with electronic health records to send automated, tailored brief text messages, and; ii) the provision of education to primary healthcare workers about T2DM prevention and management of pre-diabetes.
2. Materials and Methods
2.1. Study Design
2.2. Participant Selection and Recruitment
- -
- Healthcare professionals: We included primary healthcare physicians and nurses working in health centres in Mallorca (Spain). We recruited participants through our network of coordinators from primary care centers. They were purposefully sampled to ensure heterogeneity in terms of gender, age, and professional background (nurse or doctor).
- -
- Patients: We included adult (>18 years old) patients with prediabetes (HbA1c: 6%-6.4%, fasting plasma glucose: 110-125 mg/dl, or both). We used purposeful sampling to ensure diversity in terms of patients' age and gender. Participant recruitment was assisted by the previously recruited professionals.
2.3. Data Collection
Data were collected through 30 semi-structured interviews (15 with healthcare professionals and 15 with patients), conducted telephonically by an experienced post-doctoral female qualitative researcher (SMM) in April 2021. This number of interviews allowed us to reach data saturation.
The topic guide for the healthcare professional’s interviews (online supplemental appendix 1) covered three main areas: general perceptions concerning a new potential online educational intervention about clinical management of people at risk of developing T2DM; perceptions about the text messaging intervention targeted to patients, and; barriers and facilitators for large-scale implementation within the Balearic Islands Health Service.

ONLINE APPENDIX 1.
Topic guide for the healthcare professional’s semi-structured interviews.
| INTRODUCTION Summary of the Interview Plan (objectives, duration, rules) Brief Project Overview PROFESSIONAL EDUCATIONAL INTERVENTION • What do you think about the idea of receiving a course on prediabetes? (Relevant, necessary, useful, etc.) • What format of training would you prefer? (In-person -preferred schedule-, blended, online) • How would you like to receive the content? (Videos, case studies, scientific articles, text documents, etc.) • What topics do you consider important to include? (Epidemiology, diagnostic criteria, preventive measures -diet and physical activity-, pharmacology in prediabetes, behaviour modification, others) • What difficulties do you think might arise for the acceptance of this training? • What elements could facilitate the acceptance of training on this topic? ACCEPTABILITY AND PERCEIVED UTILITY OF AN INTERVENTION TO PROMOTE HEALTH LIFESTYLE BEHAVIOUR FOR PREDIABETES WITHIN THE PORTFOLIO OF SERVICES OF THE HEALTH SYSTEM OF THE BALEARIC ISLANDS • Overall, what do you think about the idea of sending text messages to your patients to help them manage their lifestyles to prevent diabetes? • What impact/response do you think these messages could have on your patients? What usefulness do you see in this type of intervention? • What content do you think would be necessary to include in these messages? (Diet, exercise, others) • PERSONALIZATION: Based on the information in medical records, how could we personalize (age, gender, socioeconomic status, physical activity questionnaire, predimed, postal code or Medea...), based on which variables could personalization be done? BARRIERS AND FACILITATORS FOR THE IMPLEMENTATION AND INCORPORATION OF THE INTERVENTION WITHIN THE PORTFOLIO OF SERVICES OF THE HEALTH SYSTEM OF THE BALEARIC ISLANDS • What possible impact could implement this service on a large scale have, as part of the IBSALUT service portfolio? • What barriers or difficulties do you think could arise for the implementation of this service? • Any other comments or suggestions that you think we should take into account when designing this messaging service? |
The topic guide for the patient interviews (online supplemental appendix 2) covered three main areas regarding the text messaging component of the PREDIABETEXT intervention: barriers and facilitators for the adoption of a healthier lifestyle behavior to prevent T2DM; acceptability and perceived utility of the personalized text messaging system to support behavior change, and; suggestions to optimize the proposed text messaging intervention. We applied the topic guide with flexibility, allowing the exploration of other topics during the interview and subsequent interviews.
ONLINE APPENDIX 2.
Topic guide for the patient interviews.
| INTRODUCTION · Summary of the interview plan (objectives, duration, norms) · Brief project presentation BARRIERS AND FACILITATORS FOR PREVENTION OF TYPE 2 DIABETES • What should you do to avoid having high blood sugar? (diet and physical activity should come out) • Among these factors, which one do you find most difficult to follow? What things help you? What works best for you? • Regarding recommendations about diet, what difficulties do you face in maintaining an appropriate diet to help control your condition? What helps you overcome or deal with these difficulties? • Regarding physical exercise, what difficulties do you encounter in maintaining a level of physical activity that helps control your blood sugar? What helps you overcome or deal with these difficulties? PERCEIVED ACCEPTABILITY AND UTILITY OF PERSONALIZED SMS MESSAGING SYSTEM TO AID IN BETTER SELF-MANAGEMENT OF YOUR CONDITION [The interviewer briefly describes the proposed text messaging system.] • In general, how do you feel about the idea of receiving text messages on your mobile phone with information that could help you manage your prediabetes? • To what extent do you think it could be useful in your daily life as a tool to address some of the problems you mentioned earlier? • Do you have access to a mobile phone? Do you foresee any issues in accessing the text messages we might send to your phone? CONSIDERATIONS TO MAXIMIZE THE UTILITY AND ACCEPTABILITY OF THE PROPOSED SYSTEM [The interviewer may present several examples of messages.] This messaging service is currently in the design phase. We would like to know any suggestions you might have to make it as useful as possible. • In general, what aspects do you think we should consider when launching this service, so that it is most positively received by patients? • Would you prefer to receive information in a format other than text messages (audio, images, or others)? • What content do you think these messages should include? • What are your preferences regarding: • Language of the messages • Frequency of the messages • Level of personalization (e.g., patient's name) • Ability for patients to personalize the type of message they receive (content, frequency, language, time of day received) • Any other ideas or suggestions? |
The interviews were digitally audio recorded and transcribed verbatim by a professional transcription company. The duration of the interviews ranged between 20–40 minutes. Then, transcripts were anonymized, imported into Atlas.ti 5.5, and checked for accuracy.
2.4. Data Analysis
Three experienced qualitative researchers (SMM, MJS, PS) analyzed the data using thematic analysis [18]. First, they went deeply into the text to identify recurring themes and significant passages. Second, they coded the data using an inductive approach (i.e., allowing themes, codes and categories to emerge from the data). They choose quotes that effectively show the data and reflect a variety of perspectives and themes relevant to the study's aims. Researchers defined frequent themes, and phrases as keywords. During the coding process, data segments that contained the main message, meaning, or theme were allocated codes, which were brief sentences or words. To find relationships and patterns and create themes, researchers classified codes into relevant groups. Finally, the three researchers reviewed and revised the themes, defined and named them.
2.5. Ethical Considerations
The study protocol was in accordance with the guidelines of the Declaration of Helsinki and was approved by the Ethics Committee of Clinical Research of the Balearic Islands (CEI-IB) in June 2021 with reference number of CEI-IB Ref No: IB4495/21PI. Prior to the interviews all the participants received the information sheets and signed the informed consent form approved by the CEI-IB.
3. Results
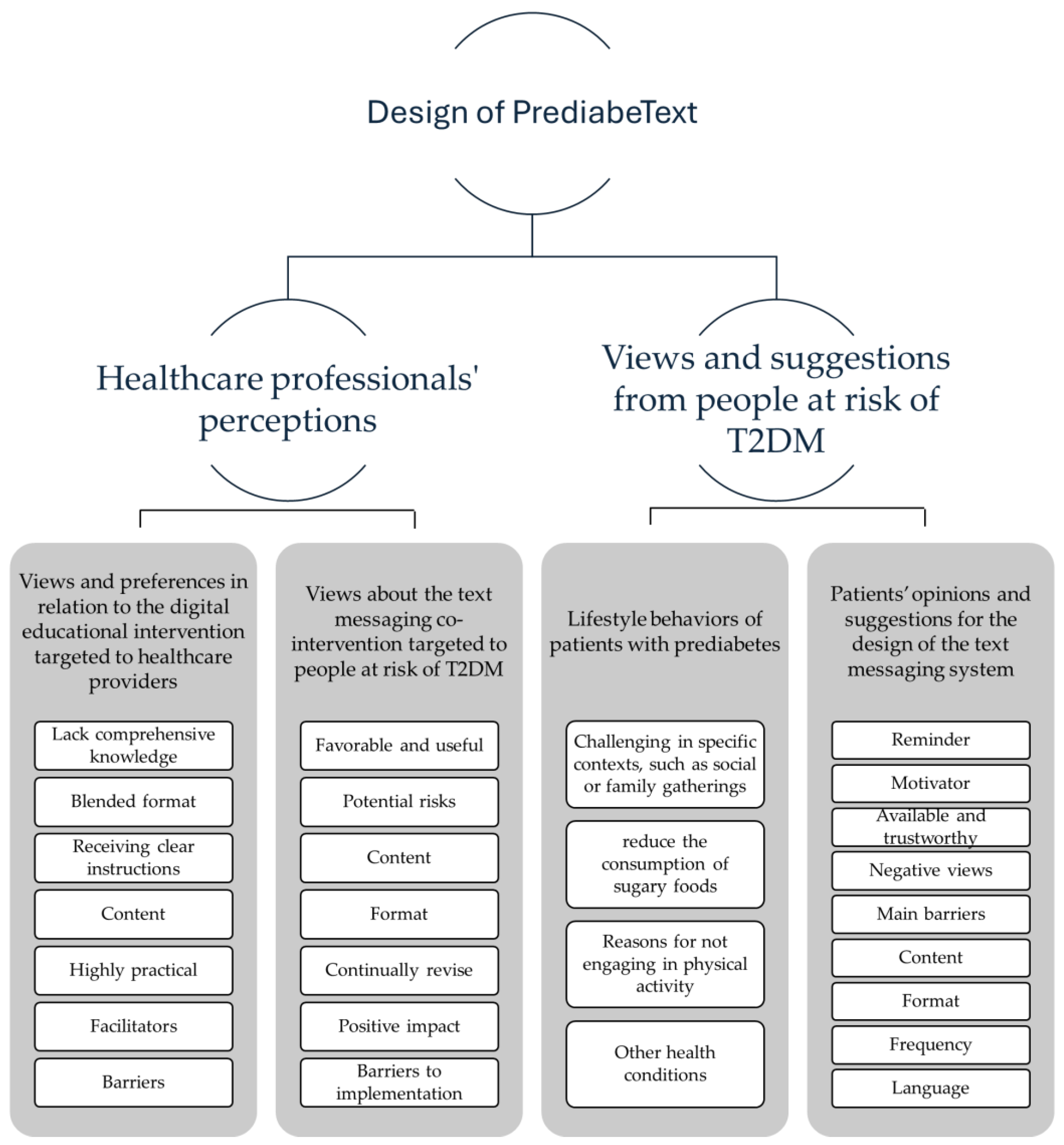
The qualitative study conducted to inform the development of the PREDIABETEX intervention engaged both healthcare professionals and patients. Figure 1 provides an overview of the main themes identified.
3.1. Healthcare Professionals' Perceptions about PREDIABETEXT
We interviewed 15 primary healthcare professionals, including four male (two nurses and two doctors) and eleven female (five nurses and six doctors), with a mean age of 44.4 years old (range 26-62 years). The themes identified were classified into two main categories: “Views and preferences in relation to the digital educational intervention targeted to healthcare providers”, and; “Views about the text messaging co-intervention targeted to people at risk of T2DM”.
3.1.1. Views and Preferences in Relation to the Digital Educational Intervention Targeted to healthcare Providers
Most healthcare professionals perceived significant value in implementing a prediabetes training course. They view this initiative as a means to standardize criteria and action guidelines, ultimately aiding in the prevention of diabetes. Emphasizing the importance of such a course, they noted that while they possess ample information about established diseases like diabetes, they often lack comprehensive knowledge regarding preventive measures for this condition.
“I would find it quite beneficial because, in general, it's true that we usually have more information about treating diabetes, but not so much focused on its prevention; and catching it in these early stages would be more interesting.”(Male nurse, 26 years old)
They predominantly advocated for a blended format training course, incorporating both face-to-face and online training components. Additionally, they suggested that the course should be scheduled during working hours to facilitate participation and engagement.
“(…) [An online format] it's more accessible, it's easier for professionals to get into it because they don't have to travel; you can do it in a few hours. Often, training coincides with external commitments we have related to work, so it doesn't allow us to attend”.(Female nurse, 42 years old)
Regarding the training content, they underscored the importance of receiving clear instructions about the appropriate criteria to detect and diagnose individuals considered prediabetic, as well as the appropriate measures to be taken with those patients. This encompasses discussions on the types of monitoring and guidelines that should be adhered to in their management.
“What prediabetes is, all the factors involved, which patients are at risk of developing it, so that professionals can intervene as early as possible within the procedures. This includes how to diagnose it, such as possibly standardizing the tests or determining when to conduct them, and strategies for prevention.”(Male nurse, 26 years old)
They perceived the content should highlight the need of accurately interpreting laboratory results and examining family medical history. They suggested a course format comprising a blend of visual materials like videos, clinical cases, and theoretical elements that participants could refer to periodically after completing the course. They emphasized on the need for a highly practical and straightforward format. Furthermore, they recommended the training should be short (between 1 to 2 hours).
They identified specific facilitators to maximize their engagement with the intervention, namely: infographics directly aimed at the patient; high-quality speakers; intervention delivered during working hours, and obtaining a course completion certificate.
"[we need] something very practical and feasible for us to do, let’s not complicate it with other stories that we can't do. Clear things, an algorithm, I don't know, what we have to do with these patients, what checks need to be done, tests, clear diet indications to offer them (…)”.(female doctor, 50 years old)
As potential barriers for attending the course, they identified the lack of time and motivation in the current situation, influenced by COVID-19, an excess of training offerings, and repetitive knowledge. Therefore, in order to maximize its uptake, the training should be perceived as innovative, and it should be focused practical tools.
3.1.2. Views about the text messaging co-intervention targeted to people at risk of T2DM
In general, healthcare professionals viewed the implementation of a text messaging system for prediabetic patients as favorable and useful. Most professionals perceived the messaging system as a reminder of the guidelines explained during consultations.
“prediabetics come here once every six months or once a year for the test, and of course, you give them this message, but they forget, at least for six months until they return for this. So, they stick with their own criteria and what they have understood or what we have explained to them. This [the messaging intervention] is a way, I believe, to motivate them and remind them.")(Female doctor, 30 years old
They believed that the messaging system would reinforce their work and serve as a motivational resource for patients, feeling cared for, and encouraging them to follow the recommended guidelines. This provided quality information at their fingertips, proposed innovative ideas, and incorporated electronic elements to enhance patient care.
“I think when people see that they receive things from us, they think, 'They care about me.' That's what we have to aim for, the empathy of saying, 'Oh, they care.' People love it when you care about them, don't they? Because I also love it when people care about me."(Female nurse, 62 years old)
However, healthcare professionals identified potential risks associated with the messaging intervention. Messages should not be repetitive, to prevent patients from ignoring them. It was proposed to make a pre-selection of patients who would use this service, considering that some patients do not adhere to guidelines, and others may have difficulties with new technologies. This selection should be established in consensus between the primary care microteam (doctor and nurse).
They identified specific features regarding the content of the messaging intervention that should be included to maximize its impact. They considered that messages should offer personalized information, especially regarding physical exercise based on age and the level of explanation. However, professionals also found it useful to include messages with generic information. There was a proposal to include recommendations about other diseases patients may have (e.g. obesity), although it was acknowledged that the personalization process could be increasingly challenging.
In relation to the format of the intervention, professionals highlighted the importance of including graphical elements, not just text, to attract user’s attention. The use of WhatsApp was suggested for this purpose, along with occasional calls, audio messages, or face-to-face meetings to maintain innovation in the format. Additionally, professionals believed it was crucial to continually revise the messages to fit the patients’ needs.
"(…) something that would greatly facilitate the issue is for it to be a simple system, not very complicated, easy to use,... accessible for all kinds of people, whether they are very accustomed to using mobile phones or not. And that the messages, in general, are easy to understand, do not use technical language, and can reach everyone, regardless of each person's ease of management."(Male nurse, 26 years old)
Regarding its positive impact, healthcare professionals believed that the messaging intervention could prevent the onset of multiple diseases, not only diabetes but also other related conditions. This could reduce healthcare spending and promote ongoing patient education.
“I think it's great because it surely works, and it is welcomed by patients. It could lead to a reduction in diabetes cases, which is ultimately what it's all about (…)."(Male nurse, 26 years old)
Concerning the content of the messages, professionals suggested they should focus on diet (clarification of concepts regarding the type of diet, quantities, or recommended foods), and body weight management. Additionally, it was deemed essential to include guidelines and recommendations about physical activity. Information about the consequences of developing diabetes should also be included.
Other desirable features were suggested: messages should be short, simple, and clear. Regarding the frequency of message delivery, the majority believed that messages should have been sent once a week to avoid overwhelming patients but also to regularly reinforce certain concepts. Some also suggested that the frequency should be agreed with the patients.
"I think that always must be agreed with the patient: 'Do you want us to remind you at the end of the day to see if you've exercised or not?' For example, I'm thinking. Among other things, maybe it wouldn't be necessary every day, but I believe in negotiating this aspect with the patient."(Female nurse, 51 years old)
The main barrier to implementing the system was believed to be patients not having a mobile phone or facing difficulties in handling it. Therefore, it was recommended to pre-select patients by identifying their knowledge of phone usage. One of the interviewees pointed out that one of the potential difficulties could be the issue of patient data protection and confidentiality about the diseases they have.
3.2. Views and Suggestions from People at Risk of T2DM about PREDIABETEXT
We conducted 15 semi-structured interviews with patients, consisting of seven males and eight females, with a mean age of 58.6 years (range 47-74). We classified the different themes into two main categories: “lifestyle behaviors of patients with prediabetes”, and “opinions and improvement suggestions regarding the text messaging system”.
3.2.1. Lifestyle Behaviors of Patients with Prediabetes
Most participants were unaware about being at risk of developing T2DM, and felt surprised about being questioned in relation to it. Following a healthy diet was perceived as particularly challenging in specific contexts, such as social or family gatherings; as well as during weekends.
“The diet, yeah, some weeks are tougher than others, especially on the weekends. It's like I let loose a bit psychologically on the weekends, you know? I'm like, "On the weekend, I can have a bit of, you know, pizza, and stuff like that”)(Female patient, 51 years old
A key challenge for participants was to reduce the consumption of sugary foods. They indicated they would appreciate receiving recommendations about healthy alternatives to replace the desire to consume sugary foods.
Although some of the participants felt that they were physically active, others expressed that they did not regularly engage in physical activity. Some participants perceived that, even when they did exercise, it was more out of necessity than enjoyment. Reasons for not engaging in physical activity were fatigue, lack of time, and boredom. Some mentioned that before the COVID-19 pandemic they used to exercise, but after the quarantine period, they haven't returned to the same routine.
“Since we've been dealing with this pandemic and all, because I've always been big on exercising: gymnastics, running, cycling, weights, you name it, always. And now, for a year and a half or two, I've completely stopped. I'm not doing anything.”(Male patient, 47 years old).
Some participants pointed out that, apart from being at risk of developing diabetes, they also suffered from other health conditions. The need to take care of these additional health problems was an important motivation for them to improve lifestyle behaviour.
3.2.2. Patients’ Opinions and Suggestions for the Design of the Text Messaging System
The patients perceived the proposed text messaging system as potentially helpful due to three main reasons: i) the system could serve them as a reminder of the guidelines and recommendations they received during their medical consultations, ii) it could serve as a motivator to adhere to these guidelines, and iii) the system would offer readily available and trustworthy information.
Some negative views were also voiced, mostly by those participants who did not feel at risk of developing the disease, and by those who perceived text messages as an outdated technology. Two main barriers or difficulties to use the system were identified: people not using (or with low level of use of) mobile phones; and the risk of messages being ignored or dismissed if they are too frequent or with repetitive information.
In relation to the content of the messages, patients expressed a desire for information on the most suitable eating habits, including the number of calories to consume, the frequency of meals, healthy snack options, healthy recipes, detailed diets, food combinations, or suggestions for healthy foods according to seasonal variations. They also proposed that the messages should inform about the risks associated with developing diabetes.
Concerning the format, SMS text messages were perceived as appropriate vehicle, although some participants suggested complementing them with emails or WhatsApp messages, as this would allow for the inclusion of short videos, which were frequently demanded. Images, specific mobile applications, and face-to-face, group meetings were also suggested, albeit less frequently.
“The videos are good because you can just watch them, listen, pay attention if they're interesting, and that's it. No need to read anymore.”(Male patient, 69 years old)
The participants suggested that the messages should be short and specific. Most suggested that the messages should convey a positive tone, whereas some suggested framing potential consequences in a threatening manner for greater efficiency.
“Like the warning on cigarette packs, showing the potential harm with harmful images. It creates a bit more awareness.”(Female patient, 48 years old).
Participants expressed diverse opinions regarding the frequency of the messages. Some advocated for receiving one concise message daily, while others indicated that one message every two days or one to two messages per week would be enough. Regarding language, participants felt that patients should have the option to choose between Spanish or Catalan (the two official languages in the Balearic Islands).
4. Discussion
This qualitative study explored the perspectives of healthcare professionals and patients at risk of type 2 diabetes on PREDIABETEXT, a digital intervention for T2DM prevention. Professionals emphasized the value of prediabetes training to standardize care and endorsed SMS as a tool to reinforce guidelines. They suggested a blended learning format and tailored content. Patients highlighted barriers to healthy lifestyles but viewed SMS as motivating and informative. These insights will guide the user-centered design of PREDIABETEXT and similar interventions.
4.1. Comparison with Previous Literature
In our study, healthcare professionals highlighted the need for the online training to be short, focused on specific aspects of diabetes prevention, and delivered during working hours, as they identified the lack of time as a key potential barrier for its use. This is supported by a recent systematic review examining health workers’ perceptions and experiences of using mHealth technologies to deliver primary healthcare services [19], which showed that professionals valued mHealth interventions as long as they were not time-consuming.
A previous qualitative systematic review examining healthcare professionals’ perspectives on technology-assisted diabetes self-management education [20] concluded that health care professionals show high levels of acceptance towards technologies for diabetes self-management education. As in our study, previous research has also identified healthcare professionals-elicited barriers to mHealth interventions, namely older age, lower educational attainment, and lower levels of digital literacy [20]. Personalization of the intervention and the use of a patient-centered approach has also been advocated by health care professionals to facilitate optimal engagement [21].
Our findings align closely with those of a recent meta-synthesis of qualitative studies analyzing self-management experiences and perceptions of individuals with prediabetes [22]. The meta-synthesis highlighted that managing prediabetes poses significant challenges to patients' daily lives. To address these challenges, individuals require access to multiple sources of informational support and personalized guidance. It is essential to ensure that the information provided is diverse in content and tailored to the needs of different groups. Additionally, delivering information in various formats—beyond just pictures and videos—can enhance its accessibility and effectiveness [22].
4.2. Strengths and Limitations
To our knowledge, this is the first study that was carried out in Spain that assesses the patients’ and healthcare providers’ perspectives and preferences about a multifaceted, digital intervention to prevent T2DM. An important strength of this study is its methodological rigor. The study meets the main trustworthiness criteria: credibility, dependability, transferability, and confirmability [23]. The analysis categories comply with the criteria of comprehensiveness, relevancy, and objectivity. Limitations to this study include the fact that we did not validate our findings with study participants and the researchers’ backgrounds may have influenced the dynamic of the interviews and subsequent findings. Despite this, consideration of reflexivity, and discussions with the rest of the research team, helped to avoid an overly narrow interpretation of the findings. In addition, the participants were a relatively homogeneous group in terms of ethnicity (white) and nationality (Spanish). Therefore, we cannot extrapolate these results to other groups. Additionally, we cannot rule out a potential selection (participation) bias, as those patients agreeing to take part in our study may be more activated toward diabetes prevention strategies than those who chose not to participate. Also, it is worth noting that this study occurred during the COVID-19 pandemic. The views and perspectives of the patients may have been influenced by the reorganization of health services that have been imposed since then, where telematics consultations are the norm rather than the exception.
4.3. Implications for Practice and Research
The results obtained in this study will be used to guide specific aspects of the design and development of the PREDIABETEXT intervention (and potentially other similar mHealth interventions). We will ensure that the interventions do not impose an increased workload on primary health care professionals. Moreover, for the text messages to be perceived as trustworthy by patients, we will ensure they are evidence based and clearly aligned with current clinical guidelines. We will involve nominated patients and healthcare providers in the development of the messages.
Supplementary Materials
The following supporting information can be downloaded at the website of this paper posted on Preprints.org, Table S1: Topic guide for the patient interviews; Table S2: Topic guide for the healthcare professional’s semi-structured interviews.
Author Contributions
Conceptualization, MJSR. and IRC.; methodology, SMM, MJSR.; data collection, SMM; validation, MJSR, RZC, MAF-dR, and NM.; formal analysis, MJSR, RZC, MAF-dR, and NM.; writing—original draft preparation, IRC and NM.; writing—review and editing, all the authors; supervision, IRC.; project administration, SMM.; funding acquisition, IRC. All authors have read and agreed to the published version of the manuscript.
Funding
The Balearic Islands Health Research Institute, IdISBa (grant SYN20/04), funded this study following a rigorous peer-reviewed funding process. The Carlos III Institute of Health provided partial support through the Network for Research on Chronicity, Primary Care, and Health Promotion (RICAPPS). MAF-dR was funded by Health Research Institute of the Balearic Islands (IdISBa), grant number FOLIUM19/05 (founded by ITS-2019-003). RZC was funded by Health Research Institute of the Balearic Islands (IdISBa), grant number FOLIUM-2023 (founded by ITS2023-057). The funding bodies had no role in the study’s design, data collection, analysis, decision to publish, or manuscript writing.
Institutional Review Board Statement
The study protocol was in accordance with the guidelines of the Declaration of Helsinki and was approved by the Ethics Committee of Clinical Research of the Balearic Islands (CEI-IB) in June 2021 with reference number of CEI-IB Ref No: IB4495/21PI.
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
Anonymized transcripts are available through the corresponding author upon request by email.
Acknowledgments
We thank all the 30 participants that agreed to take part in the telephone interview. We also thank PS who helped us with the analysis of the interviews.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Soriguer, F.; Goday, A.; Bosch-Comas, A.; Bordiú, E.; Calle-Pascual, A.; Carmena, R.; Casamitjana, R.; Castaño, L.; Castell, C.; Catalá, M.; et al. Prevalence of diabetes mellitus and impaired glucose regulation in Spain: the Di@bet.es Study. Diabetologia 2012, 55, 88–93. [Google Scholar] [CrossRef] [PubMed]
- Lopez-Bastida, J.; Goday, A.; Bosch-Comas, A.; Bordiú, E.; Calle-Pascual, A.; Carmena, R.; Casamitjana, R.; Castaño, L.; Castell, C.; Catalá, M. ;. Costs, outcomes and challenges for diabetes care in Spain. Glob. Health 2013, 9, 17. [Google Scholar] [CrossRef] [PubMed]
- Ministerio de Sanidad C y BS-PE del, S. Encuesta Nacional de Salud de España 2017. Available online: https://www.mscbs.gob.es/estadEstudios/estadisticas/encuestaNacional/encuesta2017.htm (accessed on 27 August 2019).
- Excellence, N.I.f.C. Type 2 diabetes: prevention in people at high risk. NICE guideline (PH38), 2012.
- Mata-Cases, M.; Goday, A.; Bosch-Comas, A.; Bordiú, E.; Calle-Pascual, A.; Carmena, R.; Casamitjana, R.; Castaño, L.; Castell, C.; Catalá, M. Consensus on the detection and management of prediabetes. Consensus and Clinical Guidelines Working Group of the Spanish Diabetes Society. Rev. Clin. Espanola 2015, 215, 117–129. [Google Scholar] [CrossRef] [PubMed]
- International Diabetes Federation. IDF Diabetes Atlas, 8th ed. International Diabetes Federation: Brussels, Belgium, 2017. Available online: http://www.diabetesatlas.org.
- Tabak, A.G.; Herder, C.; Rathmann, W.; Brunner, E.J.; Kivimäki, M. Prediabetes: a high-risk state for diabetes development. Lancet 2012, 379, 2279–2290. [Google Scholar] [CrossRef] [PubMed]
- Selvin, E.; Steffes, M.W.; Zhu, H.; Matsushita, K.; Wagenknecht, L.; Pankow, J.; Coresh, J.; Brancati, F.L. Glycated Hemoglobin, Diabetes, and Cardiovascular Risk in Nondiabetic Adults. N. Engl. J. Med. 2010, 362, 800–811. [Google Scholar] [CrossRef] [PubMed]
- NICE. Guidance on the use of patienteducation models for diabetes. 2014, NICE technology appraisal guidance 60.
- Kolb, H.; Martin, S. Environmental/lifestyle factors in the pathogenesis and prevention of type 2 diabetes. BMC Med. 2017, 15, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Patterson, E.M.H. Provider experiences of delivering nutrition focussed lifestyle interventions for adults with metabolic syndrome and obesity: a qualitative systematic review. 2020.
- Barengo, N.C.; Valencia, P.A.D.; Apolina, L.M.; Cruz, N.A.E.; Garate, J.E.F.; González, R.A.C.; Gonzalez, C.A.C.; Rodriguez, J.A.G.; González, N.C.; Flores, M.L.A.; et al. Mobile Health Technology in the Primary Prevention of Type 2 Diabetes: a Systematic Review. Curr. Diabetes Rep. 2022, 22, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Jeem, Y.A.; Andriani, R.N.; Nabila, R.; Emelia, D.D.; Lazuardi, L.; Koesnanto, H. The use of mobile health interventions for outcomes among middle-aged and elderly patients with prediabetes: A systematic review. Int. J. Environ. Res. Public Heal. 2022, 19, 13638. [Google Scholar] [CrossRef] [PubMed]
- Yardley, L.; Morrison, L.; Bradbury, K.; Muller, I. . The Person-Based Approach to Intervention Development: Application to Digital Health-Related Behavior Change Interventions. J. Med. Internet Res. 2015, 17, e30. [Google Scholar] [CrossRef] [PubMed]
- Galmes-Panades, A.M.; Angullo, E.; Mira-Martínez, S.; Bennasar-Veny, M.; Zamanillo-Campos, R.; Gómez-Juanes, R.; Konieczna, J.; Jiménez, R.; Serrano-Ripoll, M.J.; Fiol-Deroque, M.A.; et al. Development and Evaluation of a Digital Health Intervention to Prevent Type 2 Diabetes in Primary Care: The PREDIABETEXT Study Protocol for a Randomised Clinical Trial. Int. J. Environ. Res. Public Heal. 2022, 19, 14706. [Google Scholar] [CrossRef] [PubMed]
- Braun, V.; Clarke, V. Reflecting on reflexive thematic analysis. Qual. Res. Sport Exerc. Health 2019, 11, 589–597. [Google Scholar] [CrossRef]
- Tong, A.; Sainsbury, P.; Craig, J. Consolidated criteria for reporting qualitative research (COREQ): a 32-item checklist for interviews and focus groups. Int. J. Qual. Health Care 2007, 19, 349–357. [Google Scholar] [CrossRef] [PubMed]
- Clarke, V.; Braun, V. Successful qualitative research: A practical guide for beginners. Success. Qual. Res. 2013, 1–400. [Google Scholar]
- Odendaal, W.A.; Watkins, J.A.; Leon, N.; Goudge, J.; Griffiths, F.; Tomlinson, M.; Daniels, K. Health workers' perceptions and experiences of using mHealth technologies to deliver primary healthcare services: a qualitative evidence synthesis. Cochrane Database Syst. Rev. 2020, 3, CD011942. [Google Scholar] [CrossRef] [PubMed]
- Jain, S.R.; et al. Patients' and healthcare professionals' perspectives towards technology-assisted diabetes self-management education. A qualitative systematic review. PLoS One 2020, 15, e0237647. [Google Scholar] [CrossRef] [PubMed]
- Walsh, D.M.; Moran, K.; Cornelissen, V.; Buys, R.; Cornelis, N.; Woods, C. Electronic Health Physical Activity Behavior Change Intervention to Self-Manage Cardiovascular Disease: Qualitative Exploration of Patient and Health Professional Requirements. J. Med Internet Res. 2018, 20, e163. [Google Scholar] [CrossRef] [PubMed]
- Wang, Z.; Shi, Q.; Zeng, Y.; Li, Y. Experiences and perceptions of self-management in people with prediabetes: A qualitative meta-synthesis. J. Clin. Nurs. 2023, 32, 5886–5903. [Google Scholar] [CrossRef] [PubMed]
- Elo, S.; et al. Qualitative content analysis: A focus on trustworthiness. SAGE Open 2014, 4, 2158244014522633. [Google Scholar] [CrossRef]
Figure 1.
Development of the PREDIABETEX intervention.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



