
Submitted:
21 November 2024
Posted:
22 November 2024
You are already at the latest version
Abstract
Background/Objectives: Autism Spectrum Disorders (ASD), attention deficit hyperactivity disorder (ADHD), and Tourette Syndrome (TS) are neurodevelopmental disorders (NDD) with overlapping symptoms suggesting a partially shared genetic factor. This study investigates the prevalence of connective tissue-related conditions in individuals with ASD, ADHD, or TS. Methods: A questionnaire was administered to families of 120 individuals with ASD, ADHD, or TS, collecting sociodemographic data and examining 10 types of disorders affecting various organs and systems. Statistical analyses were performed using STATA 16.0, with a significance level set at 5%. Results: Among the 120 cases, 48 had ASD, 36 had ADHD, and 36 had TS. Flat feet were significantly more common in individuals with ASD (52.1%; OR 7.20; p<0.001), ADHD (52.8%; OR 6.73; p=0.001), and TS (38.9%; OR 3.70; p=0.034) compared to controls (13.6%). Hypersensitivity was more frequent in individuals with ASD (56.3%; OR 5.90; p=0.001), ADHD (50.0%; OR 4.11; p=0.011), and TS (58.3%; OR 5.35; p=0.003) compared to controls (18.2%). Myopia and ptosis were more common in ADHD (30.6%). There was a possible trend towards orthodontic device use in TS (OR 3.20; p=0.076). Flat feet and hypersensitivity were also common in fathers (31.0% and 36.4%, respectively), mothers (31.0% and 15.2%), and patients (43.8% and 55%). Conclusions: These results suggest common aetiopathogenetic factors, with connective tissue anomalies potentially underlying different clinical phenotypes. Further studies are warranted.
Keywords:
Autism Spectrum Disorder
; Attention Deficit Hyperactivity Disorder
; neurodevelopmental disorders
; Tourette syndrome
1. Introduction
Autistic Spectrum Disorders (ASD), Attention Deficit/Hyperactivity Disorder (ADHD), and Tourette Syndrome (TS) are neurodevelopmental disorders (NDD) that typically emerge during childhood and persist throughout life. These conditions manifest in diverse ways, leading to impairments in personal, social, academic, and occupational functioning [1,2]. The aetiopathogenesis of these disorders is thought to involve a complex interplay of genetic, epigenetic, and environmental factors. Extensive research into the heritability of NDDs suggests that a substantial proportion of phenotypic variance can be attributed to genetic influences [3,4]. Notably, certain genes associated with ASD have also been implicated in ADHD and TS [4].
Although ASD, ADHD, and TS are traditionally viewed as distinct conditions, differences in the timing of abnormal neurodevelopment and, more importantly, the neural circuits involved distinguish these disorders [5]. However, emerging evidence indicates that they may share partially overlapping genetic factors [4,6]. Specific genes and genetic regions have been identified that appear to contribute to a shared genetic predisposition for ASD, ADHD, and TS [4]. This genetic overlap is further supported by the significant symptomatological similarities among these disorders, which include attentional difficulties, impulsivity, repetitive or ritualistic behaviours, deficits in communication and social interaction, obsessive traits, anxiety disorders, and abnormalities in sensory processing [2,4,7].
Moreover, ASD, ADHD, and TS seem to exhibit overlapping neuropathological mechanisms. These disorders share features such as long-range underconnectivity and short-range overconnectivity in brain networks, reflecting similar patterns of neural dysfunction [8]. Consequently, it has been hypothesised that ASD, ADHD, and TS may represent a spectrum of related neurodevelopmental disorders, collectively termed "abnormal connectivity spectrum disorders” [9].
A broader perspective on the central and peripheral connectivity alterations characterising NDDs has been proposed through the "Connectivome Theory" [10]. This theory underscores the role of connective tissue in various organs, highlighting its multifunctional properties, including structural support, connection, nourishment, regulation, and modulation among different cellular elements.
The primary objective of this study is to examine the prevalence of pathologies associated with connective tissue alterations in individuals diagnosed with ASD, ADHD, or TS and to compare these findings with those from a healthy control group. A secondary aim is to evaluate whether these symptoms are observed at a significant rate among the parents of affected individuals.
2. Materials and Methods
The questionnaire (see Appendix), designed to investigate symptoms associated with connective tissue disorders, was administered to the families of 120 individuals diagnosed with NDD, specifically ASD, ADHD, and TS, as well as to a control group attending the Child and Adolescent Neuropsychiatry Outpatient Clinics at the University Hospital of Verona, Italy. The questionnaire gathered sociodemographic data and assessed the presence of 10 symptom categories in both the patients and their parents. These categories included:
Striae rubrae, skin irregularities, or redness;
Excessive sweating of the hands and feet;
Back pain, transient muscle pain in the limbs, or chronic fatigue;
Hip dysplasia, scoliosis, or kyphosis;
Flat feet;
Constipation, diarrhoea, or alternating bowel patterns;
Heartburn, gastroesophageal reflux, or hiatal hernia;
Use of orthodontic appliances;
Tactile, visual, auditory, olfactory, or gustatory hypersensitivity;
Myopia or drooping eyelids, including unilateral or bilateral ptosis.
The same questionnaire was also administered to a control group comprising 44 families with typically developing, healthy children attending the clinic. The data collection period spanned from December 2019 to January 2022. Parents or caregivers actively participated in the study by responding to structured questionnaires, contributing to the data acquisition.
The study was approved by the Ethical Committee of the University Hospital of Verona under the following codes: CESC 2243 (Paediatric Clinic, University Hospital of Verona) and CESC 2242 (Child and Adolescent Neuropsychiatry Outpatient Clinics, University Hospital of Verona). Written informed consent was obtained from each participant's parents.
Statistical Analysis
Continuous Gaussian variables were summarised as mean values with standard deviations (S.D.). Categorical variables were described using counts and percentages.
The presence of symptoms was compared across controls, TS, ASD, and ADHD groups using logistic regression models. In these models, the dependent variable was the presence of the symptom, while case-control status served as the independent variable. Age and sex were included as covariates to adjust the estimates.
To address issues of separation and potential convergence difficulties caused by the low prevalence of certain symptoms, Firth's penalised maximum likelihood method was employed in the logistic regression analyses [11,12].
Statistical analyses were conducted using the STATA 16.0 software package (www.stata.com). A significance threshold of 5% was applied for all statistical tests.
3. Results
A total of 164 participants were included in the study. Of these, 44 (26.8%) were healthy controls, while the remaining 120 (73.2%) were cases: 48 (29.3%) with ASD, 36 (22.0%) with ADHD, and 36 (22.0%) with TS. The mean age of the cases was 10.1 years (S.D.: 3.6), compared to 9.5 years (S.D.: 2.5) for the controls.
The control group was evenly distributed by sex, with 22 males (50.0%) and 22 females (50.0%). In contrast, most cases were male, comprising 110 participants (91.7%).
The analysis presented in Table 2 demonstrates that flat feet are significantly more prevalent among individuals with ASD (52.1%), ADHD (52.8%), and TS (38.9%) compared to the control group (13.6%), indicating a strong association with the NDD under investigation. Heartburn, gastro-oesophageal reflux, and hiatus hernia are notably more frequent in individuals with TS (27.8%) relative to the other groups. Similarly, the use of orthodontic appliances is more common in subjects with TS (41.7%) compared to the other cohorts. Hypersensitivity is markedly more prevalent in individuals with ASD (56.3%), ADHD (50.0%), and TS (58.3%) compared to controls (18.2%), further supporting a strong correlation with the NDD included in the study. Additionally, myopia and ptosis are observed more frequently in individuals with ADHD (30.6%) compared to the other groups (Table 1, Figure 1).
The analysis in Table 2 indicates that individuals with ASD exhibit a lower tendency to experience back pain, transient muscle pain in the limbs, and chronic fatigue (OR 0.25; 95% CI: 0.053–1.16; p = 0.076). The data also reveal a strong association between flat feet and various NDD, including ADHD (OR 6.73; 95% CI: 2.097–21.63; p = 0.001), ASD (OR 7.20; 95% CI: 2.438–21.23; p < 0.001), and TS (OR 3.70; 95% CI: 1.107–12.34; p = 0.034). Additionally, there is a potential trend towards increased use of orthodontic appliances in TS (OR 3.20; 95% CI: 0.887–11.51; p = 0.076).
A significant association between hypersensitivity and NDD was also identified. Individuals with hypersensitivity demonstrate a higher propensity for ADHD (OR 4.11; 95% CI: 1.385–12.19; p = 0.011), ASD (OR 5.90; 95% CI: 2.160–16.12; p = 0.001), and TS (OR 5.35; 95% CI: 1.738–16.47; p = 0.003), confirming a robust association between hypersensitivity and these disorders. Finally, the analysis revealed a significant association between myopia or ptosis and ADHD (OR 13.12; 95% CI: 1.859–92.56; p = 0.01).

Table 3.
The table presents a comparative analysis of the percentage distribution of symptoms among all patients, their fathers, and their mothers, alongside the statistical significance of the observed associations.
Table 3.
The table presents a comparative analysis of the percentage distribution of symptoms among all patients, their fathers, and their mothers, alongside the statistical significance of the observed associations.
| Symptoms | Overall patients with NDD |
Father’s patients | Mother’s patients | Statistical analysis | ||||||
| Total n. (ASD+ADHD + TS) | % | n. | % | . | % | O.R. | p-value | p-overall | ||
| Totals (n.) | 120 | |||||||||
| Striae roubre / Skin irregularities / Reddened skin | absent | 109 | 90.8 | 15 | 13.8 | 7 | 6.4 | 2.44 | 0.206 | 0.330 |
| present | 11 | 9.2 | 5 | 45.5 | 0 | 0.0 | ||||
| Excessive sweating of hands and feet | absent | 97 | 80.8 | 11 | 11.3 | 10 | 10.3 | 1.49 | 0.480 | 0.299 |
| present | 23 | 19.2 | 4 | 17.4 | 2 | 8.7 | ||||
| Mal di schiena / dolori muscolari transitori agli arti / stanchezza cronica | absent | 104 | 86.7 | 28 | 26.9 | 21 | 20.2 | 1.7 | 0.341 | 0.353 |
| present | 16 | 13.3 | 6 | 100.0 | 5 | 31.6 | ||||
| Back pain / transient muscle pain in the limbs / chronic fatigue | absent | 110 | 91.7 | 21 | 19.1 | 19 | 17.3 | 2.08 | 0.283 | 0.862 |
| present | 10 | 8.3 | 3 | 30.0 | 3 | 30.0 | ||||
| Flat foot | absent | 62 | 51.7 | 5 | 8.1 | 4 | 4.5 | 8.3 | <0.001 | <0.001 |
| present | 58 | 48.3 | 18 | 31.0 | 18 | 31.0 | ||||
| Constipation/diarrhoea / abdominal discomfort | absent | 103 | 85.8 | 23 | 22.3 | 8 | 7.8 | 3.01 | 0.041 | 0.302 |
| present | 17 | 14.2 | 8 | 47.1 | 4 | 23.5 | ||||
| Heartburn / gastroesophageal reflux / hiatal hernia | absent | 101 | 84.2 | 33 | 32.7 | 25 | 24.8 | 1.68 | 0.344 | 0.389 |
| present | 19 | 15.8 | 9 | 47.4 | 6 | 31.6 | ||||
| Heartburn / gastroesophageal reflux / hiatal hernia | absent | 84 | 70.0 | 23 | 27.4 | 10 | 11.9 | 1.48 | 0.372 | 0.109 |
| present | 36 | 30.0 | 12 | 33.3 | 10 | 27.8 | ||||
| Tactile, visual, auditory, olfactory or gustatory hyper sensoriality | absent | 54 | 45.0 | 8 | 14.8 | 3 | 5.6 | 3.31 | 0.006 | <0.001 |
| present | 66 | 55.0 | 24 | 36.4 | 10 | 15.2 | ||||
| Myopia or drooping eyelids / unilateral or bilateral eyelid ptosis | absent | 100 | 83.3 | 28 | 28.0 | 26 | 26.0 | 1.27 | 0.635 | 0.059 |
| present | 20 | 16,7 | 9 | 45,0 | 6 | 30,0 | ||||
Legend: ASD, Autism Spectrum Disorder; ADHD, Attention Deficit Hyperactivity Disorder; NDD, neurodevelopmental disorders; O.R, odds ratio; TS, Tourette Syndrome.
Given that both flat feet and hypersensitivity were found to be more prevalent in each NDD under investigation, we performed a familial analysis across the entire cohort of parents. Flat feet were common (OR 8.3) among fathers (31.0%), mothers (31.0%), and patients (43.8%; p < 0.001). The symptom of tactile, visual, auditory, olfactory, or gustatory hypersensitivity was more frequent (OR 3.31) among fathers (36.4%) compared to mothers (15.2%), and it was associated with a high prevalence of the symptom in patients (55%; p = 0.006).
4. Discussion
In our study, we identified a strong association between flat feet, hypersensitivity, and the neuropsychiatric conditions of ASD, ADHD, and TS. The use of orthodontic appliances was more frequent in individuals with TS, and myopia or ptosis was notably prevalent in those with ADHD. Additionally, flat feet and hypersensitivity were more common among the parents affected by the NDD under investigation.
Specifically, flat feet were notably more prevalent in individuals with ASD (52.1%), ADHD (52.8%), and TS (38.9%) compared to the control group (13.6%). The aetiology of flat feet can be either congenital or acquired. However, determining the precise cause of paediatric flat feet is complex, as it may occur in isolation or as part of a broader syndrome [13]. For example, certain congenital disorders, such as Ehlers-Danlos syndrome, can present with both flat feet and NDDs due to underlying connective tissue abnormalities [14]. In connective tissues, elastic fibres play a crucial role in the extracellular matrix, contributing to the elasticity and resilience of tissues. These fibres give connective tissues their elasticity and resilience [15]. Although no direct evidence links flat feet to alterations in the extracellular matrix, the structural integrity of the foot is mainly dependent on connective tissues, primarily composed of extracellular matrix components.
In our study, we observed that hypersensitivity was significantly more prevalent in individuals with TS (58.3%; OR 5.35, 95% CI 1.738-16.47), ASD (56.3%; OR 5.9, 95% CI 2.160-16.12), and ADHD (50.0%; OR 4.11, 95% CI 1.385-12.19) compared to controls (18.2%). In the context of ASD, hypersensitivity refers to an increased sensitivity to stimuli such as sound, light, touch, taste, and smell. Research has suggested that this heightened sensitivity is associated with abnormalities in glial cells, which may disrupt the development of the myelin sheath, leading to delays in response times [16,17]. There is a substantial body of literature supporting the association between sensory alterations and ASD [10] [18,19,20]. Tactile and auditory hypersensitivity has been identified as a predictor for an ASD diagnosis [21]. Moreover, connective tissue plays a crucial role in the structure and function of the outer, middle, and inner ear and the central auditory pathways.
In our study, myopia and ptosis were more prevalent in subjects with ADHD (30.6%; OR 13.12, 95% CI 1.859-92.56) compared to those with TS (13.9%), ASD (8.3%), and controls (2.3%). Previous studies have not identified a significant association between myopia and ptosis [22]. However, individuals with ASD often exhibit defects in oculomotor activity and the pupillary sphincter response to the light reflex [23] and frequently display refractive deficits [24]. The most common ocular issues in ASD include difficulties with eye alignment (convergence insufficiency) and refractive errors [20]. The connective tissue in the eyes plays a crucial role in supporting the blood vessels and nerves that comprise the retina [25]. Additionally, the corneal-scleral framework primarily comprises connective tissue [25,26].
The use of orthodontic appliances was more common in individuals with TS (41.7%) compared to other groups and controls (OR 3.20, 95% CI 0.887-11.51). Orthodontic appliances (oral orthotics, occlusal splints) have been investigated as potential treatments for reducing tics in individuals with TS. Several studies have explored using customised oral splints and dental orthodontic devices to manage tics [27]. In recent years, reports have suggested that dental orthodontic devices, typically used for treating temporomandibular joint (TMJ) disorders, may also effectively reduce tics when worn by individuals with TS [28].
Family history is strongly associated with the risk of ASD. The individual risk of ASD increases with closer genetic relationships [3]. A reanalysis of a previous study on the familial risk of ASD estimated that 83% of the risk could be attributed to genetic factors, suggesting that genetics play a pivotal role in the development of ASD [29]. In the familial analysis of our study, which included patients diagnosed with ASD, ADHD, and TS, flat feet were observed frequently in fathers (31%), mothers (31%), and patients (48.3%). Sensory hypersensitivity, which was commonly observed in patients (55%), was more prevalent in fathers (24%) compared to mothers (10%). Myopia and ptosis, which were present in 16.7% of the patients, were more frequent in fathers (45%) than in mothers (30%).
In the context of ASD, ADHD, and TS, abnormalities in connective tissue may represent a shared underlying factor. This hypothesis is supported by emerging research that underscores the interconnectedness of these NDD through physical manifestations [30]. In ASD, ADHD, and TS, abnormalities in connective tissue may represent a shared underlying factor. This hypothesis is supported by emerging research that highlights the interconnectedness of these NDD through physical manifestations [31].
Several limitations may affect the validity and generalisability of the present study. The small sample size for each NDD subgroup and the gender imbalance may introduce bias in the results. Clinic-based recruitment could lead to selection bias, and the control group may not represent the general population. Additionally, reliance on self-reported questionnaires without evaluating their reliability and validity may result in recall bias. The subjective nature of some symptoms also lacks clinical verification. The use of multiple testing increases the risk of false positives. The study does not account for all potential confounders, and its cross-sectional design prevents the establishment of causal inferences. Finally, while the familial analysis suggests a genetic component, it is limited by the absence of genetic testing.
5. Conclusions
In conclusion, the study identified significant associations between certain NDDs and physical symptoms, such as flat feet and sensory hypersensitivity. These symptoms were also frequently observed in parents, suggesting a strong familial component. This finding implies that overlapping aetiological factors may manifest in various ways, with connective tissue abnormalities potentially serving as a common underlying factor. Further research is required to confirm and expand upon these findings.
Author Contributions
Conceptualisation, L.Z. and M.L.C.; methodology, G.D.G.; software, G.D.G; validation, L.Z. and M.Z.; formal analysis, G.D.G.; investigation, L.Z., and M.L.C.; resources, L.Z.; data curation, M.Z., and E.R.; writing—original draft preparation, M.Z.; writing—review and editing, A.S., M.L.C., and E.R.; visualisation, A.S., and E.R..; supervision, L.Z. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
The study was approved by the Ethical Committee of the University Hospital of Verona: CESC 2243 (Peditric clinic, University Hospital of Verona) and CESC 2242 (Child and Adolescent Neuropsychiatry Outpatient Clinics, University Hospital of Verona).
Informed Consent Statement
Written informed consent was obtained from each participant’s parents.
Data Availability Statement
Data is unavailable due to privacy and ethical restrictions.
Acknowledgments
We thank Professor Antonio Maria Persico for helpful discussion.
Conflicts of Interest
The authors declare no conflicts of interest.
Appendix A
Questionnaire used for the study, in English language and Italian language.
Paediatric Laxity Questionnaire
Subject's gender
- Male
- Female
Subject's diagnosis
- Autism,
- ADHD,
- Tourette's syndrome,
- Control
How many brothers does the subject have?
How many sisters does the subject have?
Has the child or their parents had high blood pressure on two or three occasions?
Has the child or their parents had varicose veins, vasculitis, or haemorrhoids?
Has the child or their parents had stretch marks, skin discolouration, or unexplained reddened skin?
Has the child or their parents had excessive sweating of the palms and/or soles of the feet?
Has the child or their parents had joint inflammation or rheumatism (bursitis, tenosynovitis, etc.)?
Has the child or their parents had dislocations, subluxations, or luxation of one or more joints on more than one occasion?
Has the child or their parents had joint pain involving 1 to 3 large joints for more than 3 months?
Has the child or their parents had back pain, transient muscle aches in the limbs (e.g., growing pains), or symptoms of chronic fatigue?
Has the child or their parents had hip dysplasia, scoliosis, or a curved spine?
Has the child or their parents had inguinal, umbilical, or abdominal hernias, or herniated discs?
Has the child or their parents had flat feet?
Has the child or their parents had constipation, diarrhoea, or alternating bowel habits?
Has the child or their parents had heartburn, gastro-oesophageal reflux, or a hiatus hernia?
Has the child or their parents had rectal or uterine prolapse, or urinary or faecal incontinence?
Has the child or their parents worn or wear orthodontic appliances?
Has the child or their parents had hypersensitivity to touch (feeling tags on trousers, discomfort with a belt, feeling of tight trousers), sight (perception of bright lights, glare), hearing (perception of reverberations, amplified noises), smell (heightened perception of odours, dysosmia), or taste?
Has the child or their parents had a diagnosis of myopia or drooping eyelids (ptosis), either unilateral or bilateral? Has the child or their parents had any immune or autoimmune diseases? (e.g. type 1 diabetes, coeliac disease, thyroiditis, rheumatoid arthritis, Crohn's disease, polyneuropathy, multiple sclerosis, etc.)
Has the child or have the parents had, or do they currently have, any immune or autoimmune diseases? (e.g. type 1 diabetes, coeliac disease, thyroiditis, rheumatoid arthritis, Crohn's disease, polyneuropathies, multiple sclerosis, etc.)
Questionario lassità pediatrica (Italian version)
Genere del soggetto
- Maschio
- Femmina
Patologia del soggetto
- Autismo
- ADHD
- Sindrome di Tourette
- Controllo
Quanti fratelli ha il soggetto?
Quante sorelle ha il soggetto?
Il bambino o i genitori hanno presentato o presentano ipertensione arteriosa in due o tre rilevazioni?
Il bambino o i genitori hanno presentato o presentano vene varicose, vasculiti o emorroidi?
Il bambino o i genitori hanno presentato o presentano striae rubre, smagliature e segni cutanei, cute arrossata senza apparente causa?
Il bambino o i genitori hanno presentato o presentano un eccesso di sudorazione ai palmi delle mani e/o alle piante dei piedi?
Il bambino o i genitori hanno presentato o presentano infiammazioni o reumatismi articolari (borsiti, tenosinoviti, ecc.)?
Il bambino o i genitori hanno presentato o presentano dislocazioni, sublussazioni o lussazioni di una o più articolazioni in più di una occasione?
Il bambino o i genitori hanno presentato o presentano dolore articolare coinvolgente da 1 a 3 grosse articolazioni lamentato per più di 3 mesi?
Il bambino o i genitori hanno presentato o presentano dolore alla schiena, dolori muscolari transitori agli arti (ad es. dolori della crescita) o sintomi da affaticamento cronico?
Il bambino o i genitori hanno presentato o presentano displasia dell’anca, scoliosi o dorso curvo?
Il bambino o i genitori hanno presentato o presentano ernie inguinali, ombelicali, addominali oppure ernie discali?
Il bambino o i genitori hanno presentato o presentano piedi piatti?
Il bambino o i genitori hanno presentato o presentano stipsi, diarrea o alvo alterno?
Il bambino o i genitori hanno presentato o presentano pirosi retrosternale, reflusso gastroesofageo o ernia iatale?
Il bambino o i genitori hanno presentato o presentano prolassi rettali / uterini oppure incontinenza urinaria e/o fecale?
Il bambino o i genitori hanno utilizzato o utilizzano apparecchi ortodontici?
Il bambino o i genitori hanno presentato o presentano ipersensorialità a livello tattile (percepiscono etichette dei pantaloni, fastidio per cintura, senso di pantaloni stretti), a livello visivo (percezione di luci intense, abbagliamenti), a livello uditivo (percezione di rimbombi, rumori accentuati), a livello olfattivo (percezioni accentuate di odori, disosmie) a livello gustative?
Il bambino o i genitori hanno presentato o presentano un quadro oculistico di miopia oppure un rilievo di palpebre cadenti o ptosi palpebrale mono o bi laterale?
Il bambino o i genitori hanno presentato o presentano malattie immunitarie e/o autoimmunitarie? (es. diabete di tipo 1, celiachia, tiroiditi, artrite reumatoide, morbo di Crohn, polineuropatie, sclerosi multipla, etc.)
References
- Morris-Rosendahl, D.J.; Crocq, M.A. Neurodevelopmental disorders-the history and future of a diagnostic concept. Dialogues Clin Neurosci 2020, 22, 65–72. [Google Scholar] [CrossRef]
- Huisman-van Dijk, H.M.; Schoot, R.; Rijkeboer, M.M.; Mathews, C.A.; Cath, D.C. The relationship between tics, OC, ADHD and autism symptoms: A cross- disorder symptom analysis in Gilles de la Tourette syndrome patients and family-members. Psychiatry Res 2016, 237, 138–146. [Google Scholar] [CrossRef]
- Xie, S.; Karlsson, H.; Dalman, C.; Widman, L.; Rai, D.; Gardner, R.M.; Magnusson, C.; Sandin, S.; Tabb, L.P.; Newschaffer, C.J.; et al. The Familial Risk of Autism Spectrum Disorder with and without Intellectual Disability. Autism Res 2020, 13, 2242–2250. [Google Scholar] [CrossRef]
- Yang, Z.; Wu, H.; Lee, P.H.; Tsetsos, F.; Davis, L.K.; Yu, D.; Lee, S.H.; Dalsgaard, S.; Haavik, J.; Barta, C.; et al. Investigating Shared Genetic Basis Across Tourette Syndrome and Comorbid Neurodevelopmental Disorders Along the Impulsivity-Compulsivity Spectrum. Biol Psychiatry 2021, 90, 317–327. [Google Scholar] [CrossRef]
- Hollander, E. Obsessive-compulsive disorder and spectrum across the life span. Int J Psychiatry Clin Pract 2005, 9, 79–86. [Google Scholar] [CrossRef]
- Darrow, S.M.; Grados, M.; Sandor, P.; Hirschtritt, M.E.; Illmann, C.; Osiecki, L.; Dion, Y.; King, R.; Pauls, D.; Budman, C.L.; et al. Autism Spectrum Symptoms in a Tourette's Disorder Sample. J Am Acad Child Adolesc Psychiatry 2017, 56, 610–617.e611. [Google Scholar] [CrossRef]
- Petti, T.; Gupta, M.; Fradkin, Y.; Gupta, N. Management of sleep disorders in autism spectrum disorder with co-occurring attention-deficit hyperactivity disorder: update for clinicians. BJPsych Open 2023, 10, e11. [Google Scholar] [CrossRef]
- Lau-Zhu, A.; Fritz, A.; McLoughlin, G. Overlaps and distinctions between attention deficit/hyperactivity disorder and autism spectrum disorder in young adulthood: Systematic review and guiding framework for EEG-imaging research. Neurosci Biobehav Rev 2019, 96, 93–115. [Google Scholar] [CrossRef]
- Kern, J.K.; Geier, D.A.; King, P.G.; Sykes, L.K.; Mehta, J.A.; Geier, M.R. Shared Brain Connectivity Issues, Symptoms, and Comorbidities in Autism Spectrum Disorder, Attention Deficit/Hyperactivity Disorder, and Tourette Syndrome. Brain Connect 2015, 5, 321–335. [Google Scholar] [CrossRef]
- Zoccante, L.; Ciceri, M.L.; Gozzi, L.A.; Gennaro, G.D.; Zerman, N. The "Connectivome Theory": A New Model to Understand Autism Spectrum Disorders. Front Psychiatry 2021, 12, 794516. [Google Scholar] [CrossRef]
- Heinze, G.; Puhr, R. Bias-reduced and separation-proof conditional logistic regression with small or sparse data sets. Stat Med 2010, 29, 770–777. [Google Scholar] [CrossRef]
- Heinze, G.; Schemper, M. A solution to the problem of separation in logistic regression. Stat Med 2002, 21, 2409–2419. [Google Scholar] [CrossRef]
- Lee, J.S.; Kim, K.B.; Jeong, J.O.; Kwon, N.Y.; Jeong, S.M. Correlation of foot posture index with plantar pressure and radiographic measurements in pediatric flatfoot. Ann Rehabil Med 2015, 39, 10–17. [Google Scholar] [CrossRef]
- Pezaro, S.; Brock, I.; Buckley, M.; Callaway, S.; Demirdas, S.; Hakim, A.; Harris, C.; High Gross, C.; Karanfil, M.; Le Ray, I.; et al. Management of childbearing with hypermobile Ehlers-Danlos syndrome and hypermobility spectrum disorders: A scoping review and expert co-creation of evidence-based clinical guidelines. PLoS One 2024, 19, e0302401. [Google Scholar] [CrossRef]
- Kielty, C.M.; Sherratt, M.J.; Shuttleworth, C.A. Elastic fibres. J Cell Sci 2002, 115, 2817–2828. [Google Scholar] [CrossRef]
- Hitoglou, M.; Ververi, A.; Antoniadis, A.; Zafeiriou, D.I. Childhood autism and auditory system abnormalities. Pediatr Neurol 2010, 42, 309–314. [Google Scholar] [CrossRef]
- Gage, N.M.; Siegel, B.; Callen, M.; Roberts, T.P. Cortical sound processing in children with autism disorder: an MEG investigation. Neuroreport 2003, 14, 2047–2051. [Google Scholar] [CrossRef]
- Lindly, O.J.; Chan, J.; Fenning, R.M.; Farmer, J.G.; Neumeyer, A.M.; Wang, P.; Swanson, M.; Parker, R.A.; Kuhlthau, K.A. Vision care among school-aged children with autism spectrum disorder in North America: Findings from the Autism Treatment Network Registry Call-Back Study. Autism 2021, 25, 840–853. [Google Scholar] [CrossRef]
- Guimarães-Souza, E.M.; Joselevitch, C.; Britto, L.R.G.; Chiavegatto, S. Retinal alterations in a pre-clinical model of an autism spectrum disorder. Mol Autism 2019, 10, 19. [Google Scholar] [CrossRef]
- Longo, R.; Allegrini, F.; Gusson, E.; Morbio, R.; Di Gennaro, G.; Gozzi, L.A.; Marchini, G.; Zoccante, L. Visual-motor involvement in autism spectrum disorder: could the stereopsis deficit affect motor coordination? Front Psychiatry 2023, 14, 1130185. [Google Scholar] [CrossRef]
- Jussila, K.; Junttila, M.; Kielinen, M.; Ebeling, H.; Joskitt, L.; Moilanen, I.; Mattila, M.L. Sensory Abnormality and Quantitative Autism Traits in Children With and Without Autism Spectrum Disorder in an Epidemiological Population. J Autism Dev Disord 2020, 50, 180–188. [Google Scholar] [CrossRef]
- Chou, W.P.; Chen, Y.L.; Hsiao, R.C.; Lai, Y.H.; Yen, C.F. Bidirectional associations between hyperopia, myopia, astigmatism, and strabismus, and attention-deficit/hyperactivity disorder in children: a national population-based cohort study. Braz J Psychiatry 2023, 45, 397–404. [Google Scholar] [CrossRef]
- Johnson, C.R.; DeMand, A.; Lecavalier, L.; Smith, T.; Aman, M.; Foldes, E.; Scahill, L. Psychometric properties of the children's sleep habits questionnaire in children with autism spectrum disorder. Sleep Med 2016, 20, 5–11. [Google Scholar] [CrossRef]
- Ikeda, J.; Davitt, B.V.; Ultmann, M.; Maxim, R.; Cruz, O.A. Brief report: incidence of ophthalmologic disorders in children with autism. J Autism Dev Disord 2013, 43, 1447–1451. [Google Scholar] [CrossRef]
- Asif, M.I.; Kalra, N.; Sharma, N.; Jain, N.; Sharma, M.; Sinha, R. Connective tissue disorders and eye: A review and recent updates. Indian J Ophthalmol 2023, 71, 2385–2398. [Google Scholar] [CrossRef]
- Sridhar, M.S. Anatomy of cornea and ocular surface. Indian J Ophthalmol 2018, 66, 190–194. [Google Scholar] [CrossRef]
- Bennett, S.M.; Hindin, J.S.; Mohatt, J.; Bauer, C.; Schild, J.; Falk, A.; Specht, M.; Woods, D.; Walkup, J. Proof of Concept Study of an Oral Orthotic in Reducing Tic Severity in Tourette Syndrome. Child Psychiatry Hum Dev 2022, 53, 953–963. [Google Scholar] [CrossRef]
- Murakami, J.; Tachibana, Y.; Akiyama, S.; Kato, T.; Taniguchi, A.; Nakajima, Y.; Shimoda, M.; Wake, H.; Kano, Y.; Takada, M.; et al. Oral splint ameliorates tic symptoms in patients with tourette syndrome. In Mov Disord; United States, 2019; Volume 34, pp. 1577–1578.
- Sandin, S.; Lichtenstein, P.; Kuja-Halkola, R.; Hultman, C.; Larsson, H.; Reichenberg, A. The Heritability of Autism Spectrum Disorder. Jama 2017, 318, 1182–1184. [Google Scholar] [CrossRef]
- Csecs, J.L.L.; Iodice, V.; Rae, C.L.; Brooke, A.; Simmons, R.; Quadt, L.; Savage, G.K.; Dowell, N.G.; Prowse, F.; Themelis, K.; et al. Joint Hypermobility Links Neurodivergence to Dysautonomia and Pain. Front Psychiatry 2021, 12, 786916. [Google Scholar] [CrossRef]
- Zoccante, L.; Zaffanello, M.; Di Gennaro, G. Editorial: The "Connectivome Theory": psyche, soma and the systemic involvement of connective tissue in neurodivergence. Front Psychiatry 2024, 15, 1436796. [Google Scholar] [CrossRef]
Figure 1.
The bar graph illustrates the percentage prevalence of symptoms among children in the control group and those with neurodevelopmental disorders (NDD), including Autism Spectrum Disorder (ASD), Attention Deficit/Hyperactivity Disorder (ADHD), and Tourette Syndrome (TS). The categories are colour-coded as follows: ASD (orange), ADHD (green), TS (yellow), and controls (blue). Legend: ASD, Autism Spectrum Disorders; ADHD, attention deficit hyperactivity disorder; TS, Tourette Syndrome.
Figure 1.
The bar graph illustrates the percentage prevalence of symptoms among children in the control group and those with neurodevelopmental disorders (NDD), including Autism Spectrum Disorder (ASD), Attention Deficit/Hyperactivity Disorder (ADHD), and Tourette Syndrome (TS). The categories are colour-coded as follows: ASD (orange), ADHD (green), TS (yellow), and controls (blue). Legend: ASD, Autism Spectrum Disorders; ADHD, attention deficit hyperactivity disorder; TS, Tourette Syndrome.
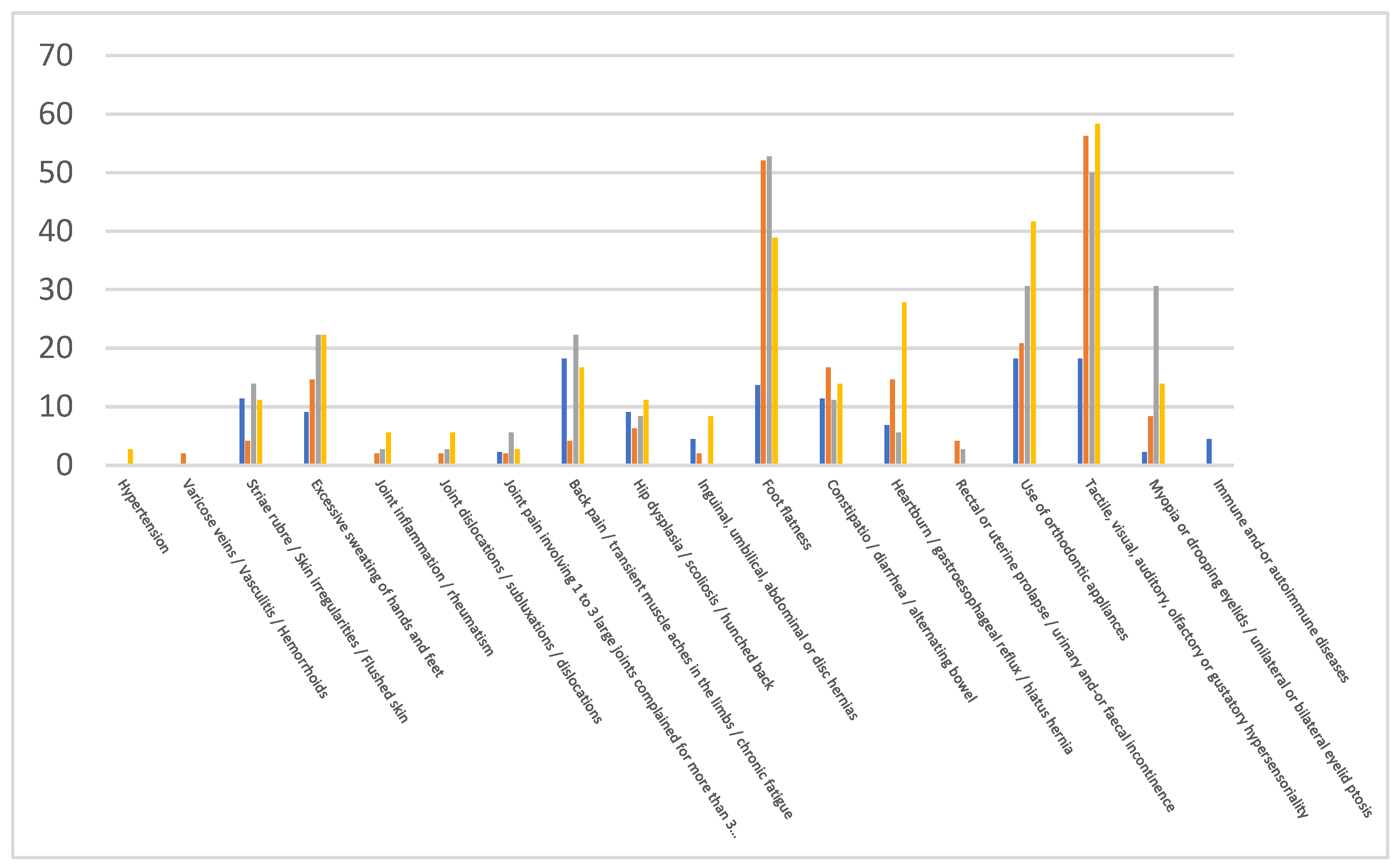
Table 1.
The table presents the prevalence of specific symptoms (expressed as percentages) among individuals with neurodevelopmental disorders (NDD), including autism spectrum disorder (ASD), Attention Deficit/Hyperactivity Disorder (ADHD), and Tourette Syndrome (TS), in comparison to the control group (last column). Additionally, it illustrates the percentage difference (Δ%) in symptom prevalence between individuals with NDD (ASD, ADHD, TS) and the control group.
Table 1.
The table presents the prevalence of specific symptoms (expressed as percentages) among individuals with neurodevelopmental disorders (NDD), including autism spectrum disorder (ASD), Attention Deficit/Hyperactivity Disorder (ADHD), and Tourette Syndrome (TS), in comparison to the control group (last column). Additionally, it illustrates the percentage difference (Δ%) in symptom prevalence between individuals with NDD (ASD, ADHD, TS) and the control group.
| NDD | ASD (%) | Δ | ADHD (%) | Δ | TS (%) | Δ | Controls (%) |
|---|---|---|---|---|---|---|---|
| Hypertension | 0.0 | 0 | 0.0 | 0 | 2.8 | 2.8 | 0.0 |
| Varicose veins / Vasculitis / Hemorrhoids | 2.1 | 2.1 | 0.0 | 0 | 0.0 | 0 | 0.0 |
| Striae rubrae / Skin irregularities / Reddened skin | 4.2 | -7.2 | 13.9 | 2.5 | 11.1 | -0.3 | 11.4 |
| Excessive sweating of hands and feet | 14.6 | 5.5 | 22.2 | 13.1 | 22.2 | 13.1 | 9.1 |
| Joint inflammation/rheumatism | 2.1 | 2.1 | 2.8 | 2.8 | 5.6 | 5.6 | 0.0 |
| Joint dislocations/subluxations/dislocations | 2.1 | 2.1 | 2.8 | 2.8 | 5.6 | 5.6 | 0.0 |
| Joint pain involving 1 to 3 large joints Complained for more than 3 months | 2.1 | -0.2 | 5.6 | 3.3 | 2.8 | 0.5 | 2.3 |
| Back pain / transient muscle pain in the limbs / chronic fatigue | 4.2 | -14 | 22.2 | 4 | 16.7 | -1.5 | 18.2 |
| Hip dysplasia/scoliosis / curved back | 6.3 | -2.8 | 8.3 | -0.8 | 11.1 | 2 | 9.1 |
| Inguinal / Umbilical abdominals or discs hernias | 2.1 | -2.4 | 0.0 | -4.5 | 8.3 | 3.8 | 4.5 |
| Flat plate | 52.1 | 38.5 | 52.8 | 39.2 | 38.9 | 25.3 | 13.6 |
| Constipation/diarrhoea/alternating bowel | 16.7 | 5.3 | 11.1 | -0.3 | 13.9 | 2.5 | 11.4 |
| Heartburn / gastroesophageal reflux / hiatal hernia | 14.6 | 7.8 | 5.6 | -1.2 | 27.8 | 21 | 6.8 |
| Rectal or uterine prolapse / urinary and/or faecal incontinence | 4.2 | 4.2 | 2.8 | 2.8 | 0.0 | 0 | 0.0 |
| Use of orthodontic appliances | 20.8 | 2.6 | 30.6 | 12.4 | 41.7 | 23.5 | 18.2 |
| Tactile / Visual / Auditory/olfactory or gustatory hyper sensoriality | 56.3 | 38.1 | 50.0 | 31.8 | 58.3 | 34.8 | 18.2 |
| Myopia or drooping eyelids / unilateral or bilateral eyelid ptosis | 8.3 | 6 | 30.6 | 28.3 | 13.9 | 11.6 | 2.3 |
| Immune and/or autoimmune diseases | 0.0 | -4.5 | 0.0 | 0 | 0.0 | 0 | 4.5 |
Legend: Red > 30%; Blue > 25%; Green > 20%. ASD, Autism Spectrum Disorders; ADHD, attention deficit hyperactivity disorder; TS, Tourette Syndrome.
Table 2.
The table presents the results of the regression analysis used to assess the association between symptoms and Autism Spectrum Disorder (ASD), Attention Deficit Hyperactivity Disorder (ADHD), and Tourette Syndrome (TS).
Table 2.
The table presents the results of the regression analysis used to assess the association between symptoms and Autism Spectrum Disorder (ASD), Attention Deficit Hyperactivity Disorder (ADHD), and Tourette Syndrome (TS).
| Symptoms | O.R. | 95% C.I. | P value | ||
|---|---|---|---|---|---|
| Hypertension | ASD | 2.19 | 0.021 | 228.08 | 0.740 |
| ADHD | 1.86 | 0.011 | 306.46 | 0.812 | |
| TS | 4.90 | 0.033 | 734.81 | 0.534 | |
| Varicose veins / Vasculitis / Hemorrhoids | ASD | 3.58 | 0.069 | 185.13 | 0.526 |
| ADHD | 1.26 | 0.011 | 143.97 | 0.924 | |
| TS | 1.09 | 0.009 | 135.69 | 0.973 | |
| Striae rubrae / Skin irregularities / Reddened skin | ASD | 0.34 | 0.062 | 1.91 | 0.222 |
| ADHD | 0.81 | 0.188 | 3.45 | 0.771 | |
| TS | 0.52 | 0.107 | 2.54 | 0.419 | |
| Excessive sweating of hands and feet | ASD | 1.78 | 0.451 | 7.01 | 0.411 |
| ADHD | 2.12 | 0.523 | 8.56 | 0.293 | |
| TS | 1.79 | 0.422 | 7.62 | 0.429 | |
| Joint inflammation/rheumatism | ASD | 2.61 | 0.065 | 105.07 | 0.610 |
| ADHD | 2.43 | 0.059 | 99.60 | 0.639 | |
| TS | 3.40 | 0.082 | 141.57 | 0.520 | |
| Joint dislocations/subluxations/dislocations | ASD | 2.79 | 0.075 | 104.34 | 0.578 |
| ADHD | 3.10 | 0.071 | 134.14 | 0.557 | |
| TS | 4.82 | 0.116 | 201.07 | 0.409 | |
| Joint pain involving 1 to 3 large joints complained of for more than 3 months | ASD | 1.14 | 0.083 | 15.65 | 0.922 |
| ADHD | 1.79 | 0.151 | 21.20 | 0.645 | |
| TS | 0.90 | 0.053 | 15.23 | 0.942 | |
| Back pain / transient muscle pain in the limbs / chronic fatigue | ASD | 0.25 | 0.053 | 1.16 | 0.076 |
| ADHD | 1.21 | 0.353 | 4.12 | 0.765 | |
| TS | 0.82 | 0.211 | 3.15 | 0.769 | |
| Hip dysplasia/scoliosis / curved back | ASD | 0.91 | 0.170 | 4.92 | 0.915 |
| ADHD | 0.84 | 0.151 | 4.69 | 0.846 | |
| TS | 0.99 | 0.176 | 5.55 | 0.988 | |
| Inguinal, umbilical, abdominal or disc hernias | ASD | 0.55 | 0.060 | 5.03 | 0.596 |
| ADHD | 0.18 | 0.007 | 4.70 | 0.306 | |
| TS | 1.21 | 0.150 | 9.71 | 0.860 | |
| Flat foot | ASD | 7.20 | 2.438 | 21.23 | 0.000 |
| ADHD | 6.73 | 2.097 | 21.63 | 0.001 | |
| TS | 3.70 | 1.107 | 12.34 | 0.034 | |
| Constipation/diarrhoea/alternating bowel | ASD | 2.07 | 0.579 | 7.44 | 0.263 |
| ADHD | 1.45 | 0.325 | 6.49 | 0.625 | |
| TS | 1.85 | 0.414 | 8.28 | 0.421 | |
| Heartburn / gastroesophageal reflux / hiatal hernia | ASD | 1.92 | 0.460 | 7.98 | 0.372 |
| ADHD | 0.63 | 0.105 | 3.75 | 0.609 | |
| TS | 3.05 | 0.697 | 13.37 | 0.138 | |
| Rectal or uterine prolapse / urinary and/or faecal incontinence | ASD | 4.34 | 0.144 | 131.51 | 0.399 |
| ADHD | 2.58 | 0.068 | 97.84 | 0.609 | |
| TS | 0.71 | 0.009 | 56.36 | 0.880 | |
| Use of orthodontic appliances | ASD | 2.02 | 0.602 | 6.77 | 0.255 |
| ADHD | 2.36 | 0.650 | 8.57 | 0.192 | |
| TS | 3.20 | 0.887 | 11.51 | 0.076 | |
| Tactile, visual, auditory, olfactory or gustatory hyper sensoriality | ASD | 5.90 | 2.160 | 16.12 | 0.001 |
| ADHD | 4.11 | 1.385 | 12.19 | 0.011 | |
| TS | 5.35 | 1.738 | 16.47 | 0.003 | |
| Myopia or drooping eyelids / unilateral or bilateral eyelid ptosis | ASD | 3.18 | 0.433 | 23.37 | 0.255 |
| ADHD | 13.12 | 1.859 | 92.56 | 0.010 | |
| TS | 5.01 | 0.615 | 40.81 | 0.132 | |
| Immune and/or autoimmune diseases | ASD | 0.38 | 0.018 | 8.18 | 0.537 |
| ADHD | 0.30 | 0.010 | 9.11 | 0.488 | |
| TS | 0.38 | 0.011 | 13.29 | 0.594 | |
Legend: ADHD; ASD, Autism Spectrum Disorders; ADHD, attention deficit hyperactivity disorder; C.I., confidence interval; O-R., odds ratio; TS, Tourette Syndrome.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



