
Submitted:
21 November 2024
Posted:
22 November 2024
You are already at the latest version
Abstract
Background/Objectives: Women with polycystic ovarian syndrome (PCOS) are at higher risk for pregnancy complications. The PCOS population is heterogeneous, with different phenotypes linked to varying risks of adverse outcomes. However, literature on pre-conceptional hyperandrogenism is limited and based on small sample sizes. Methods: This multi-institutional retrospective cohort study included pregnant patients diagnosed with PCOS with or without pre-conceptional hyperandrogenism. Utilizing the TriNetX platform, one-to-one propensity score matching was conducted to adjust for factors such as age at pregnancy, race, chronic diseases (e.g., diabetes and hypertension), and body mass index. Exclusion criteria included multiple pregnancies and patients who received assisted reproductive technology, oral contraceptives, or spironolactone. 571 patients with PCOS and pre-conceptional hyperandrogenism and 13,465 patients with PCOS without hyperandrogenism were identified. Post-propensity matching, each cohort consisted of 564 patients. Results: Pregnant women diagnosed with PCOS and pre-conceptional hyperandrogenism showed a higher risk of adverse maternal and neonatal outcomes compared to those diagnosed with PCOS but without hyperandrogenism. There was a higher incidence of large for gestational age (6.6% vs. 3.9%, OR = 1.73, 95% CI [1.007-2.972], p-value = 0.045) and preterm birth (10.3% vs. 5.9%, OR = 1.844, 95% CI [1.183-2.876], p-value = 0.006), but had no significant increase in the risk of gestational hypertension, preeclampsia/eclampsia, gestational diabetes, missed abortion, intrauterine growth restriction, placenta abruption, or cesarean section. Conclusions: Women with PCOS and pre-conceptional hyperandrogenism face a greater risk of pregnancy complications. Further studies are needed to clarify the results and mechanisms and determine whether treatment improves outcomes.
Keywords:
polycystic ovarian syndrome
; pre-conceptional hyperandrogenism
; pregnancy outcome
; large for gestational age
; preterm labor
1. Introduction
Polycystic ovary syndrome (PCOS) is the most prevalent endocrine and metabolic disorder among women, with its prevalence ranging from 6.8% to 13% among women of reproductive age [1]. According to the Rotterdam consensus criteria, PCOS is diagnosed when at least two out of three of the following features are present: polycystic ovaries, oligo- or anovulation, and clinical or biochemical hyperandrogenism [2]. Previous meta-analyses and systematic reviews have suggested that women with PCOS exhibit a significantly increased risk of pregnancy complications, including gestational hypertension, preeclampsia, gestational diabetes (GDM), and preterm delivery [3-5]. Recent large population-based studies with controlled confounders have been conducted to improve the limitations of previous research. These studies were often conducted with sample sizes that reduced statistical power and the ability to generalize findings [6-9]. These studies have reported women with PCOS have an increased risk of preterm birth, GDM, and preeclampsia compared to women without PCOS [7-9]. While the precise pathophysiology of pregnancy complications in women with PCOS remains unclear, it is believed that several features associated with PCOS itself may play direct roles. These include hyperandrogenism, obesity, insulin resistance, infertility treatments, and placental dysfunction [10,11].
The risk of adverse pregnancy outcomes may vary among different phenotypes of PCOS [10,12]. Hyperandrogenism may contribute to abnormal placental morphology and alterations in early trophoblast invasion and placentation, potentially increasing the likelihood of obstetric and perinatal complications [12-14]. Some studies have found that PCOS with hyperandrogenism is associated with worse maternal and neonatal outcomes compared with patients with PCOS without hyperandrogenism[11,12,15], while other studies have reported conflicting results [16]. However, most of these studies had a small sample size and did not account for confounding factors such as chronic diseases, assisted reproductive technology (ART), or body mass index (BMI). Therefore, the aim of our study was to compare pregnancy outcomes between mothers diagnosed with PCOS with and without pre-conceptional hyperandrogenism, utilizing the TriNetX system for a population-based study.
2. Materials and Methods
2.1. Database Description
This study is a retrospective observational analysis using comprehensive, de-identified datasets from TriNetX, a global federated network for health research. TriNetX grants access to a wide range of electronic medical records, including demographics, diagnoses (coded of International Classification of Diseases, Tenth Revision, Clinical Modification, ICD-10-CM), procedures (coded in International Classification of Diseases, Tenth Revision, Procedure Coding System, ICD-10-PCS, or Current Procedural Terminology, CPT), medications (coded in Veterans Affairs National Formulary), lab values coded in Logical Observation Identifiers Names and Codes, LOINC), and genomic data, from numerous large healthcare organizations (HCOs). The participating HCOs include hospitals, primary care facilities, and specialized units, contributing data from both insured and uninsured patients. TriNetX is a rapidly expanding global network, encompassing more than 220 HCOs and 30 countries in 2022. The network has facilitated over 19,000 sponsored clinical trial opportunities and has been the foundation for over 350 peer-reviewed scientific publications. This academic-industry framework represents a secure, established, and sustainable approach to developing and maintaining research-focused data networks [17]. The TriNetX Global Collaborative network comprises 123 HCOs, with a focus on major academic institutions. Information regarding the validation of this dataset can be found in a previously published article [18]. To date, over 800 research papers utilizing data from TriNetX have been published on PubMed.
2.2. Study Protocol, and Patient Selection
For our study, we utilized data from the Global Collaborative Network, which comprises 120 prominent HCOs covering more than 141 million individuals. A total population of 147,303,377 patients from these 120 HCOs was identified. The cohort was queried in TriNetX on June 13, 2024. Patients were included if they were aged 18 to 45 years old, experienced a pregnancy between January 1, 2000, and December 31, 2022, and were diagnosed with PCOS either with pre-conceptional hyperandrogenism or without pre-conceptional hyperandrogenism.
2.3. Cohort Definitions
The study included pregnant females aged 18 to 45 years with medical records containing specific ICD-10-CM codes (Z33.1, Z32.01, Z34) between January 1, 2000, and December 31, 2022, who were previously diagnosed with PCOS (ICD-10-CM E28.2) before pregnancy. To ensure the specificity of the PCOS diagnosis, women were excluded if they had any of the following conditions: pituitary adenoma (ICD-10: D35.2), pituitary gland disorders (ICD-10: E22, E23), adrenal gland disorders including Cushing’s syndrome and congenital adrenal hyperplasia (ICD-10: E24, E25, E27), suprarenal tumor (ICD-10: C74), galactorrhea (ICD-10: N64.3), Turner syndrome (ICD-10: Q96), or thyroid disease (ICD-10: E00-E07).
Two separate study populations were defined: pregnant patients diagnosed with PCOS with pre-conceptional hyperandrogenism, and pregnant patients diagnosed with PCOS without pre-conceptional hyperandrogenism. Hyperandrogenism was defined as patients with a record containing the ICD-10 code E28.1 (Androgen excess) or having total testosterone levels ≥ 60 ng/dL or free testosterone levels ≥ 0.84 ng/dL within 6 months before pregnancy. To minimize the chance of including potential hyperandrogenic patients, those who used combined estrogen-progestin oral contraceptives (COCs) or spironolactone within 18 months prior to pregnancy were excluded from the non-hyperandrogenism group.
Patients with multiple pregnancies (ICD-10: O30, O31) and those who had undergone ART procedures (ICD-10: O09.81, CPT 1008937, 58974, 58970) were also excluded. Body mass index (BMI) data within one year prior to pregnancy was required and obtained from the most recent laboratory records provided by the TriNetX system.
2.4. Propensity Score Matching
For propensity score matching, we utilized the TriNetX built-in algorithm, which employed 1:1 nearest-neighbor matching with a caliper of 0.1 standard deviations. We included approximately 21 covariates and characteristics for matching, encompassing factors such as age at pregnancy, race (White, Black or African American, Asian, American Indian or Alaska Native, Native Hawaiian or Other Pacific Islander, Unknown Race, and other race), chronic diseases including diabetes mellitus (ICD-10: E08-E13), hypertensive diseases (ICD-10: I10-I16), ischemic heart diseases (ICD-10: I20-I25), cerebrovascular diseases (ICD-10: I60-I69), systemic lupus erythematosus (SLE) (ICD-10: M32), Chronic kidney disease (CKD) (ICD-10: N18), Recurrent pregnancy loss (ICD-10: N96), previous cesarean section history (ICD-10-PCS 10D00Z1), and BMI (TNX Curated 9083; TNX Curated lab terms standardize and harmonize multiple LOINC codes into one term).
2.5. Outcome Measurement
The primary outcomes in this study were adverse pregnancy outcomes, including GDM (ICD-10: O24.4, O24.9), gestational hypertension (ICD10: O13, O16), preeclampsia (ICD 10: O14)/eclampsia (ICD 10: O15), placental abruptio (ICD 10: O45), placenta previa (ICD10-O44), cesarean section (ICD-10: O82, ICD-10-PCS10D00Z0, 10D00Z1, 10D00Z2, and SNOMED-CT code 11466000), intrauterine growth restriction (IUGR) (ICD-10: Z36.4, O36.5), large for gestational age (LGA) (ICD-10: O36.6), preterm delivery (ICD-10: O60), induction of labor (SNOMED 31208007), instrumental delivery (ICD10: O66.5, ICD-10-PCS 10D07Z3, ICD-10-PCS ,10D07Z4, SNOMED 236974004, SNOMED 302383004, SNOMED 61586001, ICD-10-PCS 10D07Z6), Shoulder dystocia (ICD-10 O66.0), dysfunction labor (ICD-10 O66.4, O66.9) and spontaneous abortion (ICD-10: O03). In the study, only data attributed to the mother were used. Data attributed to the newborn were not used, as these are considered highly sensitive data according to the TriNetX Data Privacy principles.
2.6. Statistical Analysis
All statistical analyses were performed using the TriNetX Platform. Baseline characteristics of the study population were summarized using descriptive statistics. Continuous variables were reported as means with corresponding standard deviations (SDs), while categorical variables were presented as frequencies with percentages. To assess differences between cohorts, the risk difference was evaluated using a Z-test, which provided a 95% confidence interval. Additionally, the risk ratio was calculated with its corresponding 95% confidence interval. The analysis considered a time window from the date of the index event (the first pregnancy record) extending up to 270 days later.
3. Results
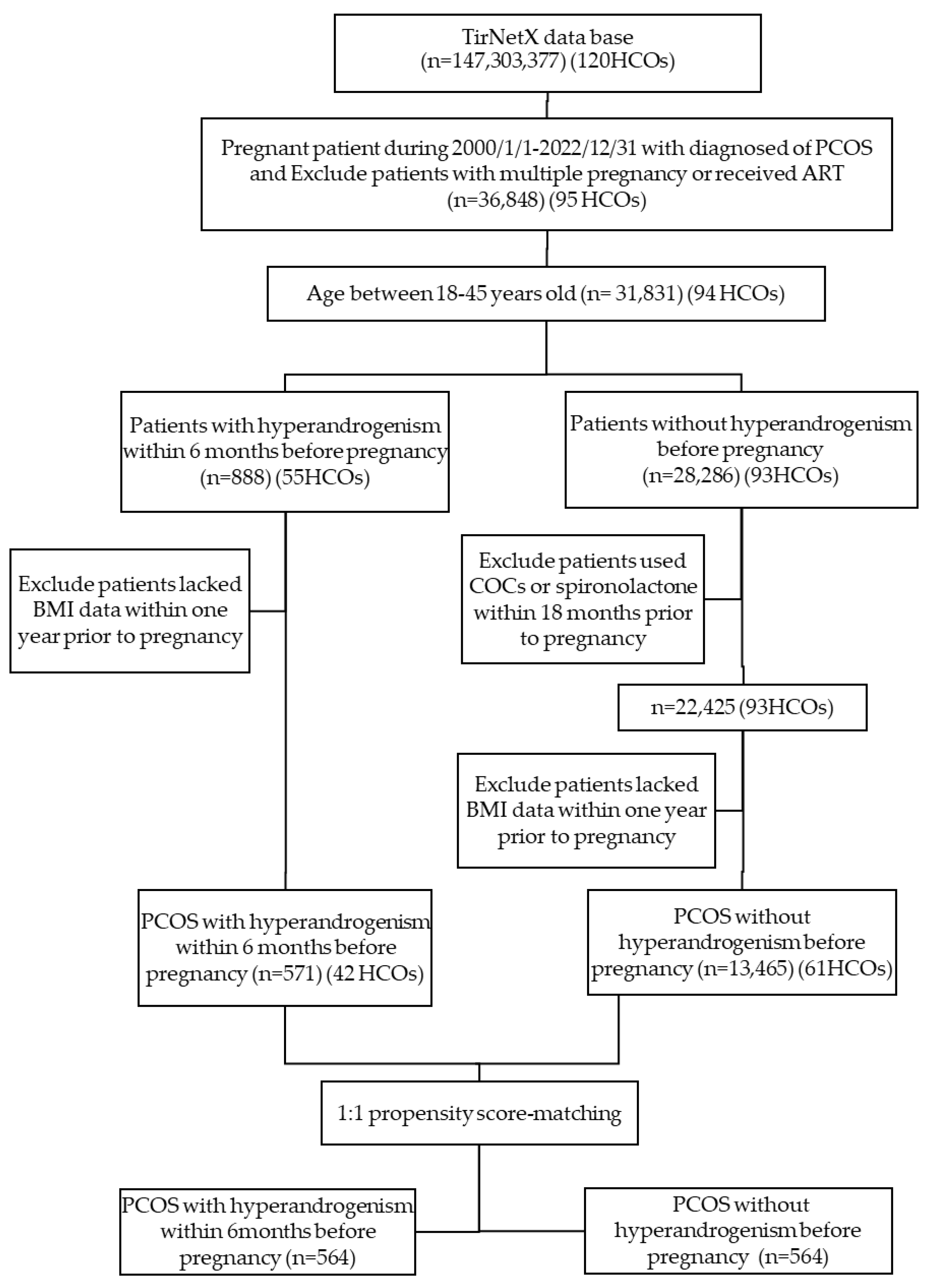
In the base population, a total of 36,848 females diagnosed with PCOS became pregnant between January 1, 2000, and December 31, 2022. Patients with multiple pregnancies or who conceived via ART were excluded. Additionally, patients outside the age range of 18 to 45 years were excluded, resulting in 31,831 patients meeting these criteria. Further exclusions were applied to patients who lacked BMI data within one year prior to pregnancy and those who used COCs or spironolactone within 18 months before pregnancy in the non-hyperandrogenism group. This refining process yielded 571 patients from 42 HCOs in the PCOS with hyperandrogenism group, and 13,465 patients from 61 HCOs in the PCOS without hyperandrogenism group. The flowchart in Figure 1 illustrates the process for selecting the study population.
3.1. Population Characteristics
The baseline patient characteristics of each group before and after matching are summarized in Table 1. In terms of ethnic composition, approximately 60% were White, 15% were Black or African American, and Asians comprised about 5-6% of the total. Before matching, patients in the PCOS with hyperandrogenism group were younger at the time of pregnancy (27.4 ± 4.4 years vs. 29.0 ± 4.8 years, p < 0.001), had a higher prevalence of ischemic heart diseases (1.8% vs. 0.3%, p < 0.001), cerebrovascular diseases (1.8% vs. 0.4%, p < 0.001), lower BMI (31.5 ± 7.3 vs. 32.4 ± 7.8, p = 0.016), and a lower prevalence of diabetes mellitus (2.3% vs. 6.0%, p < 0.001). After propensity score matching, 564 patients were identified in each cohort.

Table 1.
Baseline characteristics of patients before and after propensity score matching.
| Variables | Before Matching | P Value | After Matching | P Value | ||
|---|---|---|---|---|---|---|
| PCOS with hyperandrogenism (n= 571) | PCOS without hyperandrogenism (n=13,420) | PCOS with hyperandrogenism (n=564) | PCOS without hyperandrogenism (n=564) | |||
| Age, mean (SD), years | 27.4 +/- 4.4 | 29.0 +/- 4.8 | <0.001 | 27.4 +/- 4.4 | 27.4 +/- 4.4 | 0.808 |
| White | 330(58.2) | 8103(60.6) | 0.252 | 329 (58.3) | 351 (62.2) | 0.181 |
| Diabetes mellitus | 13 (2.3) | 799 (6.0) | <0.001 | 13 (2.3) | 10 (1.8) | 0.527 |
| Hypertensive diseases | 42 (7.4) | 1038 (7.8) | 0.756 | 41 (7.3) | 32 (5.7) | 0.276 |
| Ischemic heart diseases | 10 (1.8) | 45 (0.3) | <0.001 | 10 (1.8) | 0 (0) | 0.001 |
| Cerebrovascular diseases | 10 (1.8) | 48 (0.4) | <0.001 | 10 (1.8) | 0 (0) | 0.001 |
| Systemic lupus erythematosus | 0 (0) | 45 (0.3) | 0.166 | 0 (0) | 0 (0) | -- |
| Chronic kidney disease | 0 (0) | 52 (0.4) | 0.137 | 0 (0) | 0 (0) | -- |
| Recurrent pregnancy loss | 15 (2.6) | 231 (1.7) | 0.104 | 13 (2.3) | 11 (2.0) | 0.68 |
| Cesarean section | 17 (3.0) | 187 (1.0) | 0.002 | 16 (2.8) | 16 (2.8) | 0 |
| Body mass index, mean (SD), kg/m2 | 31.5 +/- 7.3 | 32.4 +/- 7.8 | 0.016 | 31.5 +/- 7.3 | 31.0 +/- 7.2 | 0.259 |
Abbreviations: PCOS, polycystic ovarian syndrome; SD, standard deviation.
Figure 1.
Patient Enrollment Algorithm. Abbreviations: HCOs, healthcare organizations; PCOS, polycystic ovarian syndrome; COCs, combined oral contraceptives; BMI, Body mass index.
Figure 1.
Patient Enrollment Algorithm. Abbreviations: HCOs, healthcare organizations; PCOS, polycystic ovarian syndrome; COCs, combined oral contraceptives; BMI, Body mass index.
3.2. Maternal and Neonatal Outcomes
The maternal and neonatal outcomes are presented in Table 2. The incidence of LGA and preterm labor was significantly higher in the PCOS cohort with hyperandrogenism compared to the cohort without hyperandrogenism, with rates of LGA (6.6% vs. 3.9%) and preterm labor (10.3% vs. 5.9%), respectively. The OR were 1.730 (95% CI 1.007-2.972, p=0.045) for LGA and 1.844 (95% CI 1.183-2.876, p=0.006) for preterm labor. Other outcomes including missed abortion, placenta previa, IUGR, GDM, gestational hypertension, preeclampsia/eclampsia, placental abruption, cesarean section, shoulder dystocia, dysfunctional labor, and instrumental delivery showed comparable in both groups.
4. Discussion
To the best of our knowledge, this is the first population-based study with the largest cohort comparing pregnancy outcomes between women diagnosed with PCOS and hyperandrogenism pre-conceptionally versus those diagnosed with PCOS without hyperandrogenism with detailed propensity score matching. The study results indicated that PCOS with hyperandrogenism was associated with worse pregnancy outcome with higher risk of preterm birth and LGA.
Previous reports exploring different types of PCOS have observed an increased risk of preterm labor or delivery and preeclampsia in the hyperandrogenic phenotype [11,12,15]. Naver et al. found that women with PCOS and hyperandrogenemia had a more than two-fold increased risk of both preterm deliveries and preeclampsia compared to the background population after adjusting for BMI, age, and parity[15]. However, their study had lower case numbers (PCOS n=459, and 184 patients with hyperandrogenism) and limited matching. Another recent study with a larger sample size (PCOS n= 1715, and 854 patients with hyperandrogenism) also reported that preconception hyperandrogenism was associated with an increased risk of preeclampsia and preterm birth[12]. Both studies did not find an increased risk of LGA, however, these studies did not mention if the hyperandrogenism was treated or not before pregnancy.
Our study showed there were higher risk of preterm birth in the PCOS with hyperandrogenism group. Although the rates of preeclampsia and gestational hypertension were high in both our groups compared with the general population, our finding did not show an increased incidence in the group of patients with PCOS and hyperandrogenism, as observed in previous studies[3]. In previous studies, the frequency of preeclampsia increased with the severity of diabetes among women with pregestational diabetes mellitus[19]. Diabetes mellitus is an important confounding factor and should be included in the matching process. However, we did not match for the severity of diabetes, and further studies in this field are warranted.
We found that women with PCOS and hyperandrogenism were associated with LGA. It may be due to the slightly higher prevalence of patients with GDM in this group, although it did not reach statistical significance (13.8% vs. 10.1%, Odds ratio 1.428 (0.922, 2.05), p = 0.054). Other studies have shown that hyperandrogenism in women with PCOS is associated with more severe metabolic dysfunction, including obesity and insulin resistance[20,21]. This discrepancy may be attributed to the association of LGA and GDM[22]. Further studies are needed to explore this relationship and validate the association.
Besides, our study revealed that patients with hyperandrogenism had a comparable risk of cesarean section, which was inconsistent with findings from previous studies which were smaller sample sizes (<30 patients) and did not adjust for the background prevalence of cesarean section[3,16]. Before matching, patients in the hyperandrogenism group in our cohort also had a significantly higher prevalence of a history of cesarean section, it may lead to incorrect statistical conclusion without matching of this compound factor. Further studies are needed to validate these findings.
Our result did not show a significantly different rate of miscarriage compared to patients without hyperandrogenism. It was inconsistent to a recent systematic review that demonstrated a significantly higher rate of miscarriage in ovulatory and hyperandrogenic phenotypes, from BMI-matched spontaneous conception modes [3]. This difference may be due to our larger sample size (571 vs. 13,465) and the exclusion of patients undergoing ART in our study population. Another systematic review that investigated patients with PCOS undergoing in ART with invitro fertilization/ intracytoplasmic sperm injection (IVF/ICSI) found a higher risk of miscarriage in patients with hyperandrogenism compared to those with normal androgen levels, specifically in an Asian population[23]. Further study may focus on population with natural conception to validate this issue.
Although the majority of our study population comprised white individuals (with only 5% being of Asian descent), we observed a similar trend. We also noted that both groups of our patients had obesity (BMI: 31.5 and 32.4 kg/m2 in each group). It may be due to the fact that most patients with PCOS are obese[24]. Almost all observational findings showed a lower risk of obstetric and neonatal adverse outcomes in normal-weight women compared to overweight/obese women. Therefore, weight loss to achieve an optimal body weight before conception is suggested[25], especially in patients with PCOS and hyperandrogenism. Further study could focus on the effect of weight loss on pregnancy outcomes. Some studies have shown that metformin treatment during pregnancy can reduce androgen levels compared to no treatment and significantly decreased the incidence of GDM (from 36% to 14%)[26]. However, other studies have not shown improvement[27]. The use of metformin as a first-line drug during pregnancy is still controversial and its use should be carefully considered in specific patient groups, such as those with PCOS and hyperandrogenism, when evaluating the risk and benefit ratio[28]. Further research is needed to confirm the benefits and evaluate the effects and safety on offspring.
The main strength of the present study lies in the utilization of global registers with prospectively collected data and large sample sizes. This enabled us to control many confounding factors such as chronic disease, BMI, previous birth history and the method of conception. To minimize bias, we only included pregnant patients without ART treatment, as previous studies have suggested that pregnancies conceived through IVF/ICSI are associated with a higher risk of obstetric and perinatal complications than those conceived spontaneously[29]. This allowed us to analyze the associations of maternal hyperandrogenic PCOS with pregnancy outcomes more clearly. We also excluded patients who had used COCs within 18 months prior to pregnancy in our study design. This measure could prevent misclassification of those patients into the group without hyperandrogenism. A recent study found that pretreatment with ethinylestradiol/cyproterone acetate (EE/CPA) for three months in patients with PCOS reduces the risk of GDM, gestational hypertension, and preterm birth[30].
A limitation of our study was the retrospective nature of the investigation. Also, we used an administrative database, which relies on the accuracy and consistency of the individuals that coded the data. Moreover, TriNetX Platform currently provides only structured electronic medical record information, so imaging reports or medical chart will not be queryable in the Query Builder. Therefore, we could not know patients’ history of oligomenorrhea, clinical hyperandrogenism or sonography finding. Therefore, it is possible that some cases of remote diagnosis of PCOS or clinical hyperandrogenism may not have been reported. Despite the possibility of undiagnosed hyperandrogenic PCOS women being included in the control group, our results are consistent with most smaller studies. Regarding the definition of hyperandrogenism, due to the lack of free androgen index in our study cohort, we used ICD-10 codes as well as levels of free testosterone and total testosterone instead. Previous studies have also used the same definition[15,31]. Additionally, we only included testosterone levels within 6 months before pregnancy and exclude patient who use COCs within 18months before pregnancy which could better explain the association. Furthermore, the database does not provide information on parity, smoking history, or birthweight, which are potential confounding variables that we were unable to account for in our analysis. Despite these limitations, the availability of extensive data allowed for a thorough evaluation of the impact of PCOS with hyperandrogenism on pregnancy outcomes, and it was even possible to adjust for various strong confounders.
5. Conclusions
To date, this is the largest study on PCOS with pre-conceptional hyperandrogenism, which was found to be a factor linked with increased risk of preterm birth and LGA. The findings of this study highlight the importance of further research on PCOS, particularly focusing on patients with hyperandrogenism, to determine the optimal timing for screening and pretreatment before conception. By gaining a better understanding of the clinical characteristics of PCOS, we can work toward preventing maternal complications during pregnancy and delivery.
Author Contributions
Conceptualization, Ming-Jer Chen and Jui-Chun Chang ; Methodology, Wei-Szu Lin and Ching-Heng Lin; Software, Yi-Ting Chang; Supervision, Ming-Jer Chen; Validation, Yi-Ting Chang, Ming-Jer Chen and Jui-Chun Chang ; Writing – original draft, Yi-Ting Chang; Writing – review & editing, Jui-Chun Chang; All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
The Western Institutional Review Board has granted TriNetX an informed consent waiver, as the platform solely aggregates counts and statistical summaries of de-identified information. And our specific use of TriNetX for this study received approval from the institutional review board committee of Taichung Veterans General Hospital (Approval number: CE23480C, TCVGH), Date of Approval: 23 November, 2023.
Informed Consent Statement
Informed consent is not applicable as this is a retrospect decoded database analysis.
Data Availability Statement
The data for this study were collected from TriNetX, a global federated health research network that provides access to de-identified electronic medical records from various healthcare organizations. The data supporting the findings of this study are available from the corresponding author upon reasonable request.
Acknowledgments
The authors acknowledge Dr. Hsin-Hua Chen of Taichung Veterans General Hospital, Taichung, Taiwan, for his assistance in preparing the study data using the TriNetX system.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Bozdag, G.; Mumusoglu, S.; Zengin, D.; Karabulut, E.; Yildiz, B.O. The prevalence and phenotypic features of polycystic ovary syndrome: a systematic review and meta-analysis. Hum Reprod 2016, 31, 2841-2855. [CrossRef]
- Revised 2003 consensus on diagnostic criteria and long-term health risks related to polycystic ovary syndrome (PCOS). Hum Reprod 2004, 19, 41-47. [CrossRef]
- Bahri Khomami, M.; Joham, A.E.; Boyle, J.A.; Piltonen, T.; Silagy, M.; Arora, C.; Misso, M.L.; Teede, H.J.; Moran, L.J. Increased maternal pregnancy complications in polycystic ovary syndrome appear to be independent of obesity-A systematic review, meta-analysis, and meta-regression. Obes Rev 2019, 20, 659-674. [CrossRef]
- Kjerulff, L.E.; Sanchez-Ramos, L.; Duffy, D. Pregnancy outcomes in women with polycystic ovary syndrome: a metaanalysis. Am J Obstet Gynecol 2011, 204, 558.e551-556. [CrossRef]
- Gilbert, E.W.; Tay, C.T.; Hiam, D.S.; Teede, H.J.; Moran, L.J. Comorbidities and complications of polycystic ovary syndrome: An overview of systematic reviews. Clin Endocrinol (Oxf) 2018, 89, 683-699. [CrossRef]
- Yu, H.F.; Chen, H.S.; Rao, D.P.; Gong, J. Association between polycystic ovary syndrome and the risk of pregnancy complications: A PRISMA-compliant systematic review and meta-analysis. Medicine (Baltimore) 2016, 95, e4863. [CrossRef]
- Farland, L.V.; Stern, J.E.; Liu, C.L.; Cabral, H.J.; Coddington, C.C.; Diop, H.; Dukhovny, D.; Hwang, S.; Missmer, S.A. Polycystic ovary syndrome and risk of adverse pregnancy outcomes: a registry linkage study from Massachusetts. Hum Reprod 2022, 37, 2690-2699. [CrossRef]
- Mills, G.; Badeghiesh, A.; Suarthana, E.; Baghlaf, H.; Dahan, M.H. Associations between polycystic ovary syndrome and adverse obstetric and neonatal outcomes: a population study of 9.1 million births. Hum Reprod 2020, 35, 1914-1921. [CrossRef]
- Valgeirsdottir, H.; Sundström Poromaa, I.; Kunovac Kallak, T.; Vanky, E.; Akhter, T.; Roos, N.; Stephansson, O.; Wikström, A.K. Polycystic ovary syndrome and extremely preterm birth: A nationwide register-based study. PLoS One 2021, 16, e0246743. [CrossRef]
- Palomba, S.; de Wilde, M.A.; Falbo, A.; Koster, M.P.; La Sala, G.B.; Fauser, B.C. Pregnancy complications in women with polycystic ovary syndrome. Hum Reprod Update 2015, 21, 575-592. [CrossRef]
- de Wilde, M.A.; Lamain-de Ruiter, M.; Veltman-Verhulst, S.M.; Kwee, A.; Laven, J.S.; Lambalk, C.B.; Eijkemans, M.J.C.; Franx, A.; Fauser, B.; Koster, M.P.H. Increased rates of complications in singleton pregnancies of women previously diagnosed with polycystic ovary syndrome predominantly in the hyperandrogenic phenotype. Fertil Steril 2017, 108, 333-340. [CrossRef]
- Christ, J.P.; Gunning, M.N.; Meun, C.; Eijkemans, M.J.C.; van Rijn, B.B.; Bonsel, G.J.; Laven, J.S.E.; Fauser, B. Pre-Conception Characteristics Predict Obstetrical and Neonatal Outcomes in Women With Polycystic Ovary Syndrome. J Clin Endocrinol Metab 2019, 104, 809-818. [CrossRef]
- Koster, M.P.; de Wilde, M.A.; Veltman-Verhulst, S.M.; Houben, M.L.; Nikkels, P.G.; van Rijn, B.B.; Fauser, B.C. Placental characteristics in women with polycystic ovary syndrome. Hum Reprod 2015, 30, 2829-2837. [CrossRef]
- Sun, M.; Maliqueo, M.; Benrick, A.; Johansson, J.; Shao, R.; Hou, L.; Jansson, T.; Wu, X.; Stener-Victorin, E. Maternal androgen excess reduces placental and fetal weights, increases placental steroidogenesis, and leads to long-term health effects in their female offspring. Am J Physiol Endocrinol Metab 2012, 303, E1373-1385. [CrossRef]
- Naver, K.V.; Grinsted, J.; Larsen, S.O.; Hedley, P.L.; Jørgensen, F.S.; Christiansen, M.; Nilas, L. Increased risk of preterm delivery and pre-eclampsia in women with polycystic ovary syndrome and hyperandrogenaemia. Bjog 2014, 121, 575-581. [CrossRef]
- Mumm, H.; Jensen, D.M.; Sørensen, J.A.; Andersen, L.L.; Ravn, P.; Andersen, M.; Glintborg, D. Hyperandrogenism and phenotypes of polycystic ovary syndrome are not associated with differences in obstetric outcomes. Acta Obstet Gynecol Scand 2015, 94, 204-211. [CrossRef]
- Palchuk, M.B.; London, J.W.; Perez-Rey, D.; Drebert, Z.J.; Winer-Jones, J.P.; Thompson, C.N.; Esposito, J.; Claerhout, B. A global federated real-world data and analytics platform for research. JAMIA Open 2023, 6, ooad035. [CrossRef]
- Topaloglu, U.; Palchuk, M.B. Using a Federated Network of Real-World Data to Optimize Clinical Trials Operations. JCO Clin Cancer Inform 2018, 2, 1-10. [CrossRef]
- Sibai, B.M.; Caritis, S.; Hauth, J.; Lindheimer, M.; VanDorsten, J.P.; MacPherson, C.; Klebanoff, M.; Landon, M.; Miodovnik, M.; Paul, R.; et al. Risks of preeclampsia and adverse neonatal outcomes among women with pregestational diabetes mellitus. National Institute of Child Health and Human Development Network of Maternal-Fetal Medicine Units. Am J Obstet Gynecol 2000, 182, 364-369. [CrossRef]
- Diamanti-Kandarakis, E.; Dunaif, A. Insulin resistance and the polycystic ovary syndrome revisited: an update on mechanisms and implications. Endocr Rev 2012, 33, 981-1030. [CrossRef]
- Daan, N.M.; Louwers, Y.V.; Koster, M.P.; Eijkemans, M.J.; de Rijke, Y.B.; Lentjes, E.W.; Fauser, B.C.; Laven, J.S. Cardiovascular and metabolic profiles amongst different polycystic ovary syndrome phenotypes: who is really at risk? Fertil Steril 2014, 102, 1444-1451.e1443. [CrossRef]
- He, L.R.; Yu, L.; Guo, Y. Birth weight and large for gestational age trends in offspring of pregnant women with gestational diabetes mellitus in southern China, 2012-2021. Front Endocrinol (Lausanne) 2023, 14, 1166533. [CrossRef]
- Ma, L.; Cao, Y.; Ma, Y.; Zhai, J. Association between hyperandrogenism and adverse pregnancy outcomes in patients with different polycystic ovary syndrome phenotypes undergoing in vitro fertilization/intracytoplasmic sperm injection: a systematic review and meta-analysis. Gynecol Endocrinol 2021, 37, 694-701. [CrossRef]
- Azziz, R. How prevalent is metabolic syndrome in women with polycystic ovary syndrome? Nat Clin Pract Endocrinol Metab 2006, 2, 132-133. [CrossRef]
- ACOG Committee opinion no. 549: obesity in pregnancy. Obstet Gynecol 2013, 121, 213-217. [CrossRef]
- Crisosto, N.; Echiburú, B.; Maliqueo, M.; Pérez, V.; Ladrón de Guevara, A.; Preisler, J.; Sánchez, F.; Sir-Petermann, T. Improvement of hyperandrogenism and hyperinsulinemia during pregnancy in women with polycystic ovary syndrome: possible effect in the ovarian follicular mass of their daughters. Fertil Steril 2012, 97, 218-224. [CrossRef]
- Vanky, E.; Stridsklev, S.; Heimstad, R.; Romundstad, P.; Skogøy, K.; Kleggetveit, O.; Hjelle, S.; von Brandis, P.; Eikeland, T.; Flo, K.; et al. Metformin versus placebo from first trimester to delivery in polycystic ovary syndrome: a randomized, controlled multicenter study. J Clin Endocrinol Metab 2010, 95, E448-455. [CrossRef]
- Jorquera, G.; Echiburú, B.; Crisosto, N.; Sotomayor-Zárate, R.; Maliqueo, M.; Cruz, G. Metformin during Pregnancy: Effects on Offspring Development and Metabolic Function. Front Pharmacol 2020, 11, 653. [CrossRef]
- Pandey, S.; Shetty, A.; Hamilton, M.; Bhattacharya, S.; Maheshwari, A. Obstetric and perinatal outcomes in singleton pregnancies resulting from IVF/ICSI: a systematic review and meta-analysis. Hum Reprod Update 2012, 18, 485-503. [CrossRef]
- Li, Y.; Ruan, X.; Wang, H.; Li, X.; Cai, G.; Du, J.; Wang, L.; Zhao, Y.; Mueck, A.O. Comparing the risk of adverse pregnancy outcomes of Chinese patients with polycystic ovary syndrome with and without antiandrogenic pretreatment. Fertil Steril 2018, 109, 720-727. [CrossRef]
- Escobar-Morreale, H.F.; Carmina, E.; Dewailly, D.; Gambineri, A.; Kelestimur, F.; Moghetti, P.; Pugeat, M.; Qiao, J.; Wijeyaratne, C.N.; Witchel, S.F.; et al. Epidemiology, diagnosis and management of hirsutism: a consensus statement by the Androgen Excess and Polycystic Ovary Syndrome Society. Hum Reprod Update 2012, 18, 146-170. [CrossRef]
Table 2.
Pregnancy outcomes after propensity score matching between patients with PCOS with and without pre-conceptionally hyperandrogenism.
Table 2.
Pregnancy outcomes after propensity score matching between patients with PCOS with and without pre-conceptionally hyperandrogenism.
| Outcomes | PCOS with hyperandrogenism, (n=564) | PCOS without hyperandrogenism, (n=564) | Odds ratio (95% CI) | P value |
| Missed abortion | 42 (7.4) | 38 (6.7) | 1.114 (0.706, 1.756) | 0.643 |
| Placenta previa | 16 (2.8) | 14 (2.5) | 1.147 (0.554, 2.373) | 0.711 |
| IUGR | 40 (7.1) | 39 (6.9) | 1.028 (0.650, 1.624) | 0.907 |
| LGA | 37 (6.6) | 22 (3.9) | 1.730 (1.007, 2.972) | 0.045 |
| Preterm birth | 58 (10.3) | 33 (5.9) | 1.844 (1.183, 2.876) | 0.006 |
| GDM | 78 (13.8) | 57 (10.1) | 1.428 (0.992, 2.053) | 0.054 |
| Gestational hypertension | 83 (14.7) | 67 (11.9) | 1.280 (0.906, 1.808) | 0.161 |
| Preeclampsia/eclampsia | 49 (8.7) | 45 (8.0) | 1.097 (0.719, 1.675) | 0.667 |
| Placenta abruption | 10 (1.8) | 10 (1.8) | 1 (0.413, 2.422) | 1 |
| Cesarean section | 119 (21.1) | 111 (19.7) | 1.091 (0.817, 1.458) | 0.554 |
| Shoulder dystocia | 12 (2.1) | 11 (2.0) | 1.093 (0.478, 2.498) | 0.833 |
| Dysfunctional of labor | 10 (1.8) | 10 (1.8) | 1 (0.413, 2.422) | 1 |
| Instrumental delivery | 16 (2.8) | 15 (2.7) | 1.069 (0.523, 2.183) | 0.855 |
Abbreviations: PCOS, polycystic ovarian syndrome; IUGR, intrauterine growth restriction; LGA, large for gestational age; GDM, gestational diabetes mellitus.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



