
Submitted:
18 November 2024
Posted:
20 November 2024
You are already at the latest version
Abstract
Objectives
To evaluate the index density (Id) of the percentage of biopsy positive cores (BPC), Id-BPC, as a prognostic factor of prostate cancer (PCa) progression after predicting unfavorable pathology in patients treated with robot-assisted radical prostatectomy (RARP) eventually associated with extended pelvic lymph node dissection.
Design
Data from 1047 patients undergoing RARP were collected between January 2013 and December 2021.
Methods
Id-BPC was defined as the ratio of BPC (%) to prostate volume (mL). Unfavorable pathology in the surgical specimen was defined as tumor grade group greater than 1 and/or non-organ confined disease. Disease progression was defined as biochemical recurrence and/or loco-regional recurrence and/or metastatic occurrence. Associations with the risk of unfavorable pathology and disease progression were evaluated by logistic regression and Cox proportional hazards model (univariate and multivariate analysis), respectively.
Results
Unfavorable pathology was detected in 930 (88.8%) cases. Disease progression occurred in 160 (15.3%) patients after a mean (95% CI) follow-up of 89.0 (86.6-91.3) months. After adjusting for all clinical variables, patients with higher Id-BCR were more likely to have unfavorable pathology in the surgical specimen (odds ratio = 1.566; 95% CI: 1.029 – 2.383; p < 0.001). As Id-BCR increased, patients were more likely to experience disease progression, even when adjusting for clinical variables (hazard ratio = 1.587; 95% CI: 1.306 – 1.929; p < 0.0001), as well as unfavorable pathology (hazard ratio = 1.365; 95% CI: 1.166 – 1.597; p < 0.0001). The impact of Id-BPC on PCa progression was stronger than that of BPC, particularly after predicting unfavorable pathology.
Conclusions
Id-BCR is an independent prognostic factor of unfavorable pathology and disease progression in PCa patients undergoing surgical treatment with curative intent. As Id-BPC increases, patients have a higher probability of experiencing unfavorable pathology in the surgical specimen and disease progression. Id-BCR is a clinical marker of PCa biology.
Keywords:
prostate cancer
; robot-assisted radical prostatectomy
; extended pelvic lymph node dissection
; pelvic lymph node invasion
; biochemical recurrence
; prostate cancer progression
; prostate biopsy
; percenta
1. Introduction
Prostate cancer (PCa) is a growing concern among aging men [1,2]. To address the most common form of presentation, clinical non-metastatic PCa, the European Association of Urology (EAU) and the National Comprehensive Cancer Network (NCCN) have developed guidelines that offer valuable options for management. Depending on the clinical risk class, options may include monitoring strategies such as active surveillance (AS) or watchful waiting (WW), or active treatment like surgery, most frequently performed with robot-assisted radical prostatectomy (RARP) approach eventually associated with extended pelvic lymph node dissection (ePLND), and radiation therapy (RT) [1,2,3]. Although clinical risk classes provide valuable information about a disease's prognosis, it's essential to understand that risk groups are not homogeneous. As such, it's crucial to make further efforts within each class to detect patient subsets that may have indolent or aggressive disease, avoiding over-treatment, which patients may come to regret in the future [1,2,4,5]. Although molecular biology holds significant potential in identifying prognostic subgroups, it has yet to become commonly utilized in routine clinical practice. Conversely, multiparametric resonance imaging (mpMRI) is useful in diagnosing diseases, but its reproducibility is lacking and its ability to accurately stage diseases remains uncertain [6,7]. Therefore, the applications of validated nomograms remain an essential tool for stratifying low- and intermediate-risk patients and predicting the risk of unfavorable disease and pelvic lymph node invasion (PLNI) [1,2]. These nomograms rely on standard clinical parameters that are widely available in urological centers during PCa diagnosis [1,2]. Briganti's 2012 nomogram, which employs basic standard parameters, has proven highly effective in predicting unfavorable disease. Although the updated nomogram incorporates mpMRI parameters, its accuracy is heavily operator-dependent and varies across multicenter studies [1,2,6,8,9]. One of the most powerful parameters is the percentage of biopsy-positive cores (BPC), which is particularly useful for determining the risk of PLNI [1,2,8]. BPC provides valuable information on PCa biology, including tumor load after prostate biopsy, along with basal PSA, tumor grade, and stage [1,2,10]. However, the potential of tumor density within the organ being investigated as a parameter for defining cancer biology has yet to be explored. This study endeavors to investigate the index density of BPC (Id-BPC), defined as the ratio of BPC to prostate volume (PV), as a potential clinical marker of PCa biology. Id-BPC was evaluated as a predictor of the likelihood of unfavorable pathology in the surgical specimen, as well as a prognostic factor of disease progression following RARP for clinical PCa with curative intent.
2. Materials and Methods
The reporting of this study conforms to the Strengthening the Reporting of Observational Studies in Epidemiology statement (Supplementary Material 1).
2.1. Selection of the Investigated Patient Population
Between January 2013 and December 2021, a total of 1047 operated PCa patients who had follow-up data available were selected. Data were collected prospectively and evaluated retrospectively. All patients provided informed consent that was approved by the Institutional Review Board. Inclusion criteria consisted of at least 12 systematic prostate biopsy cores; 3 to 5 target biopsy cores for each PI-RADS > 3 lesions detected in Patients undergoing mpMRI before prostate biopsy; the measurement of prostate volume through transrectal ultrasound (TRUS) methods at the time of PCa diagnosis. Patients who had undergone androgen deprivation or previous active treatment were excluded. Following recommendations, RARP was eventually performed alongside ePLND, which followed a standard anatomical template that included external iliac, obturator, Cloquet’s, and Marcille’s regions [11]. The choice to perform ePLND was made considering the EAU risk class and nomograms to estimate the risk of lymph node extension of the disease. Surgical procedures were performed by five experienced urologists.
2.2. Evaluation of Clinical, Pathological, and Follow-Up Factors
During clinical assessments, patient age (years), body mass index (BMI; kg/m2), physical status, PSA (ng/mL), PV (mL), BPC (%), tumor grade, and stage were all evaluated. For each case, the ratios of BPC and PSA to PV, measured by TRUS methods, were calculated, and the resulting relative densities were reported as Id-BPCD (%/mL) and PSA density (PSAD, ng/ml2), respectively. The surgical specimens were assessed by a dedicated pathologist for tumor grade, stage, and surgical margins status, while pelvic lymph nodes were counted and assessed for PLNI. The RARP and ePLND procedures have been previously described [11,12]. Tumors were graded according to the International Society of Urological Pathology (ISUP) system and staged using the TNM system [1,2]. Physical status was evaluated preoperatively using the American Association of Anesthesiologists (ASA) score system [11,12]. Patients were followed by recommendations [1,2]. In case of persistence/recurrence of PSA, imaging modalities were considered to restage the disease and plan further treatments, performed in a multidisciplinary setting involving urologists, radiation oncologists, and oncologists, to optimize recommendations while taking the patient's issues into account [1,2].
2.3. Model Description and Assumptions, Study Design, and Evaluation of Endpoints
The clinical factor investigated was the Id-BPC. The clinical model, depicted in Figure 1, was based on the following assumptions. Firstly, variations in PV are associated with tumor variations. Secondly, a constant BPC that correlates with variation in PV resulted in different tumor densities. Therefore, as PV increases, tumor densities decrease. For instance, tumors with a BPC of 10% could occur in a PV of 30 mL (Id-BCP = 0.33), 60 mL (Id-BPC = 0.16), or 90 mL (Id-BPC = 0.11). However, tumor load density is higher in the former case, where aggressive tumor biology should be expected when evaluating the surgical specimen. Thirdly, high tumor load densities should predict unfavorable pathology in the surgical specimen and PCa progression. We evaluated the Id-BPCD as a continuous variable and related it to unfavorable pathology in the surgical specimen and disease progression. Unfavorable pathology in the surgical specimen was defined as including unfavorable tumor grade (ISUP > 1) and/or non-organ confined disease (extracapsular extension (ECE) or seminal vesicle invasion (SVI)) and/or PLNI. Thus, PCa progression was defined as the occurrence of biochemical recurrence/persistence and/or local recurrence and/or distant metastasis.
2.4. Statistical Methods
Continuous variables were measured by medians with interquartile ranges (IQR). Categorical factors were assessed by frequencies (%). Differences in the distributions of clinical factors between favorable and unfavorable pathology were assessed by chi-squared and Mann-Whitney tests. The association of clinical variables with the risk of unfavorable pathology was evaluated by a logistic regression model (univariate and multivariate analysis). Time elapsed between surgery and the clinical outcome of interest (disease progression) or last follow-up was measured as time to event occurrence. The Cox proportional hazards method (univariate and multivariate analysis) was used to estimate the association of clinical factors with the risk of PCa progression. In multivariable model analysis, the Wald forward method was computed to select significant predictive models. Finally, unadjusted Kaplan-Meier estimator curves of factors associated with the risk of disease progression were eventually displayed. The software used to perform the analysis was IBM-SPSS version 26. All tests were two-sided, and p < 0.05 was considered an index of statistical significance.
3. Results
3.1. Patient Population Demographics and Risk of Unfavorable Pathology in the Surgical Specimen
The study population included 1047 patients who underwent RARP with associated ePLND in 666 subjects. The median (IQR) count of lymph nodes was 25 (19 – 31). Clinical demographics of the PCa population stratified by unfavorable versus favorable pathology are described in Table 1. Among the surgical specimens with unfavorable pathology, detected in 930 cases (88.8%), extra-prostatic extension (pT3) occurred in 224 cases (24.1%) of which 122 (13.1%) with SVI and PLNI in 56 (6%). Only one case (0.1%) exhibited ISUP grade group 1. Unfavorable pathology resulted in a higher rate of positive surgical margins (27.1%) than in controls (10.3%). The distributions of pathology ISUP grade groups were as follows: grade 1 in 118 (11.3%), grade 2 in 409 (39.1%), grade 3 in 295 (28.2%), and grade 4/5 in 264 (25.2%) cases. Patients with unfavorable pathology were older, had smaller prostates, higher PSA levels, and unfavorable tumor features related to grade and stage. They were also associated with higher BPC and Id-BPC. The population was distributed according to the EAU risk classes: 297 (28.4%) at low risk, 527 (50.3%) at intermediate risk, and 223 (21.3%) at high risk. Table 2 illustrates the association of clinical factors with the risk of unfavorable pathology, indicating that patients with higher Id-BPC had a greater likelihood of unfavorable pathology in the surgical specimen, regardless of unfavorable tumor grade and stage.
3.2. Clinical Risk Factors of Prostate Cancer Progression after Robotic Surgery
The mean (95% CI) follow-up was 89.0 (86.6-91.3) months. Overall, PCa recurrence occurred in 160 (15.3%) cases, as reported in Table 3. Recurrent patients tended to have higher Id-BPC and PSA levels and undifferentiated cancers eventually associated with locally advanced stage. Deaths occurred in 14 (1.3%) patients, including 6 (0.6%) due to PCa. Radiation therapy was administered to 172 (16.5%) patients, with salvage intent in 73 (7.0%). Additionally, 172 (16.4%) follow-up patients were under androgen blockade.
3.3. The Prognostic Impact of Id-BPC on PCa Progression after Predicting Unfavorable Pathology in the Surgical Specimen
The prognostic impact of Id-BPC on PCa progression after predicting the risk of unfavorable pathology in the surgical specimen is reported in Table 4. The results indicate that patients with higher Id-BPC have a higher likelihood of unfavorable pathology in the surgical specimen (odds ratio = 1.566; 95% CI: 1.029 – 2.383; p < 0.001) even after adjusting for other clinical variables. Therefore, patients with increasing Id-BPC are more likely to experience disease progression, accounting for both clinical variables (hazard ratio = 1.587; 95% CI: 1.306 – 1.929; p < 0.0001) and unfavorable pathology (hazard ratio = 1.365; 95% CI: 1.166 – 1.597; p < 0.0001). Interestingly, BPC showed a lower impact on predicting unfavorable pathology and PCa progression compared to Id-BPC, as shown in the reference table. Figure 2 displays the Kaplan-Meyer risk curves of PCa progression stratified by unfavorable versus favorable pathology in the surgical specimen. Figure 3 and Figure 4 present the distribution of Id-BPC for unfavorable versus favorable pathology and PCa progression versus non-progression, respectively.
4. Discussion
The 10-year mortality rate for clinically treated PCa varies between 1.2% and 13.7%, depending on prognostic risk classes. The Cambridge Prognostic Groups (CPG) risk classification, which includes 5 clinical risk classes defined by basal PSA levels, tumor grades, and stages, seems to provide the most accurate definition of these risk classes. However, this system overlooks BPC as a crucial prognostic factor in stratifying low to intermediate-risk classes [1,2,13,14]. The 15-year PCa-specific mortality rate after radical prostatectomy (RP) ranged from 2.2% to 12% as reported by the randomized Protect trial from England and an uncontrolled study conducted in North America, respectively. Additionally, the former study highlighted that there was no difference in disease-specific mortality between the monitored (AS) and actively treated groups (RP, RT), while the latter emphasized the need for new clinical markers specifically associated with PCa's lethal biology [4,15]. Biochemical recurrence is a crucial endpoint for evaluating PCa patients treated with curative intent. The EAU has developed and validated prognostic risk classes of biochemical recurrence by considering PSA dynamics, such as PSA doubling time (PSA-DT) after RP or interval to biochemical failure (IBF) after RT, as well as tumor grade groups at biopsy or pathology, based on the chosen curative intent modality [16,17]. Based on a meta-analysis of the EAU biochemical risk classes, it has been found that atypical PSA dynamics (short PSA-DT or IBF) and high-tumor grades are unfavorable prognostic factors, increasing the risk of PCa-specific mortality after RP. Only short IBF is linked to PCa-specific mortality after curative RT [16]. Currently, the occurrence of PCa biochemical recurrence in approximately 25% of RP-treated patients does not necessarily lead to disease-specific death, ranging from 1.2% to 13%. However, the high velocity of PSA post-operative dynamics and unfavorable tumor grades and stages are considered unfavorable prognostic factors for disease progressing to metastases, leading to lower cancer-specific survival rates. Nevertheless, the tumor load density of positive biopsy cores has not been investigated as a prognostic factor of disease progression. Our study revealed that the Id-BPC is a more powerful prognostic factor than BPC alone in the PCa progression. As the Id-BPC increased, patients were more likely to experience disease progression, while those with low id-BPC were less susceptible to such progression. Notably, even after accounting for other significant factors related to unfavorable pathology, the Id-BPC remained an independent predictor of unfavorable prognosis following surgical treatment with curative intent, as per EAU risk classes These findings are groundbreaking and have significant implications for both basic science and clinical practice. In PCa patients treated with RARP eventually associated with ePLND, analyzing surgical specimens is crucial for predicting disease prognosis. The pathological ISUP tumor grade system remains the most reliable prognostic factor of BCR after RP with curative intent. As ISUP grade groups increase, patients are more likely to experience BCR [18]. Tumor extension within the prostate and/or to loco-regional lymph nodes is also pivotal, since extra-prostatic extension (pT3a), seminal vesical invasion (pT3b), and PLNI (pN1) disease are unfavorable prognostic factors that impair the natural history of the treated disease with curative intent [19,20]. As such, unfavorable pathology, including ISUP grade groups greater than 1 and/or non-organ confined disease (pT3a, pT3b, pN1), represents the best way to identify potential disease progression [1,2,18,19,20]. Each validated nomogram incorporates the BPC, which is crucial in calculating the final risk score [1,2,8,9]. While the BPC is already an important parameter in assessing unfavorable tumor pathology to predict PLNI, the influence of the Id-BPC has yet to be assessed. In our study, patients with higher Id-BPC were more prone to unfavorable pathology in the surgical specimen, including non-indolent tumors for non-organ confined disease and/or tumor grade groups greater than one. As Id-BPC increased, patients were more likely to have unfavorable pathology, while a decrease in Id-BPC was often associated with indolent disease in the surgical specimen. It's noteworthy that Id-BPC was a stronger predictor of unfavorable pathology in the surgical specimen than BPC. Clinical studies have shown that there's a clear correlation between prostate volume and PCa biology. A pioneering study revealed that PSAD was positively linked to the risk of PCa in men undergoing prostate biopsy. Patients with higher PSAD were more likely to have cancer detection in smaller prostate sizes than those with benign prostatic hyperplasia (BPH) [21]. A large study including 939 subjects undergoing prostate biopsies found that cancer detection rates were significantly higher for small prostates (61% for PV < 30 mL) and lower for large prostates (37% for PV > 50 mL) [22]. An early study that analyzed a new prostate volume model, defined as the ratio of the volume of the transition zone to the volume of the peripheral zone of the prostate (PV index), showed that patients with low PV index were more likely to have positive cores associated with high tumor loads and grades. Interestingly, the risk of PCa was increased by small prostates, predominantly represented by peripheral zone volume, and decreased by large prostates, sustained by large transitional zone volumes and associated with the presence of chronic prostatic inflammation [23,24]. A dated trial, which analyzed 325 patients treated with surgery, discovered that PSAD served as a powerful predictor of unfavorable pathology in the surgical specimen and biochemical recurrence Specifically, patients with higher PSAD levels were more likely to have unfavorable pathology and experience BCR. This was particularly true for patients with smaller prostates, as they tended to have higher PSAD, a greater likelihood of unfavorable disease, and BCR. Interestingly, the researchers suggested that PSAD could potentially serve as a correcting factor for PSA produced by benign epithelium [25]. Another large study conducted in North America investigated 1602 PCa patients treated with RP and found that smaller prostates were more likely to have unfavorable disease and BCR. The researchers, while hypothesizing that low PV may be related to low androgen levels, concluded that PV was an impacting variable that should be included in nomograms useful for clinical practice [26]. These findings emphasize the importance of understanding prostate growth biology in aging males and provide insights into the results of our study. Our research has shown that the Id-BCR is a significant and independent clinical prognostic factor for disease progression, particularly in cases of unfavorable tumor pathology, in a large series of patients from all EAU risk classes surgically treated with curative intent. So far, Id-BPC has been able to trace the main steps of PCa’s natural history. Our findings suggest that high tumor load densities are underpinned by local factors, promoting exponential growth rates and expanding locally by invading the prostatic capsule and seminal vesicles, which increases the likelihood of progression to nearby regional lymph nodes. These patterns are sustained by tumors that are either highly undifferentiated or invasive, exhibiting high frequencies of dynamic genetic mutations. Unfavorable tumor grade and/or stage merely scratches the surface of these complex phenomena. In theory, higher tumor load densities in small prostates may indicate an unfavorable microenvironment, where lower testosterone densities are to be expected than in larger prostates, which are predominantly sustained by benign hyperplasia, as demonstrated by clinical investigations on this topic [27].
The results of our study could have clinical implications. Id-BCR could represent a valuable clinical parameter for clustering PCa patients into prognostic risk classes, where tumor under grading and/or under staging can challenge managing treatment options. As Id-BPC increased, patients were more likely to have unfavorable pathology in the surgical specimen and experience disease progression. Conversely, as Id-BCR decreased, subjects were more likely to have indolent disease in the surgical specimen and less likely to experience disease progression. To select appropriate treatments for patients, effective clinical markers are necessary to assess the aggressive PCa biology. Although BPC remained an effective predictor of PCa natural history in our study, Id-BCR showed greater potential in predicting unfavorable pathology. Therefore, it could be included in new nomograms for predicting the risk of unfavorable pathology and as an effective clinical prognostic factor for disease progression. Tumor load density should be considered when planning clinical investigative studies on the subject. The next step could be categorizing the variable to find an appropriate cut-off value for selecting a subset of patients at increased risk for both unfavorable pathology and disease progression.
While our study has some limitations, it also has notable strengths. One limitation is that it was a retrospective study with procedures performed by multiple surgeons. PSA-DT and extension of cancer involvement within each core were not evaluated because they were not available in all cases. Additionally, PV was not always evaluated at our institution, and Id-BPC was not evaluated for PCa-specific mortality. However, the data collection was prospective and the procedures were performed by experienced surgeons. Furthermore, the investigated factor was evaluated in a large case series that was operated on in a single tertiary referral center. Finally, Id-BPC was assessed for unfavorable pathology and disease progression, which is a stronger endpoint than BCR.
5. Conclusions
Id-BCR proved to be a valuable and independent prognostic factor in predicting disease progression in PCa patients surgically treated with curative intent. The study found that higher levels of Id-BPC were associated with a higher likelihood of unfavorable pathology in the surgical specimen and disease progression. Therefore, Id-BCR serves as an important clinical marker of PCa biology.
Ethics Approval and Consent to Participate
The study was conducted in accordance with the Declaration of Helsinki and approved by the Institutional Review Board of Azienda Ospedaliera Universitaria Integrata of Verona. Written informed consent was obtained from all subjects involved in the study.
Consent for Publication
Written informed consent was obtained from all subjects involved in the study.
Author Contributions
ABP provided the study design and conception, the manuscript's drafting, and the statistical analyses. A Bianchi and SG provided the manuscript's drafting, analyses, and interpretation of data. ES, SC, F Montanaro, A Baielli, FA, DB, GMP, and AF carried out data collection. RR, AV, MB, VDM, F Migliorini, MAC, and AA provided supervision and critical revision of the manuscript for important intellectual contents. All authors read and approved the final version of the manuscript.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Conflicts of Interest Statement
The authors declare no conflict of interest.
Availability of Data and Materials
The data presented in this study are available on request from the corresponding author. The data are not publicly available due to ethical reasons.
Abbreviations
| AS: active surveillance |
| ASA: Association of Anesthesiologists |
| BMI: body mass index |
| BPC: percentage of biopsy-positive cores |
| EAU: European Association of Urology |
| ECE: extracapsular extension |
| ePLND: extended pelvic lymph node dissection |
| IBF: interval to biochemical failure |
| Id-BPC: index density of percentage of biopsy-positive cores |
| IQR: interquartile ranges |
| ISUP: International Society of Urological Pathology |
| mpMRI: multiparametric resonance imaging |
| NCCN: National Comprehensive Cancer Network |
| PCa: prostate cancer |
| PLNI: pelvic lymph node invasion |
| PSAD: PSA density |
| PSA-DT: PSA doubling time |
| PV: prostate volume |
| RARP: robot-assisted radical prostatectomy |
| RP: radical prostatectomy |
| RT: radiation therapy |
| SVI: seminal vesicle invasion |
| TRUS: transrectal ultrasound |
| WW: watchful waiting |
References
- Mottet, N.; Cornford, P.; van den Bergh, R.C.N.; Briers, E.; Eberli, D.; De Santis, M.; Gillessen, S.; Grummet, J.; Henry, A.M.; et al.; Expert Patient Advocate (European Prostate Cancer Coalition/Europa UOMO) EAU - EANM - ESTRO - ESUR - ISUP - SIOG Guidelines on Prostate Cancer. Available online: https://uroweb.org/guidelines/prostate-cancer (accessed on 18 December 2023).
- Schaeffer, E.; Srinivas, S.; Adra, N.; An, Y.; Barocas, D.; Bitting, R.; Bryce, A.; Chapin, B.; Cheng, H.H.; D’Amico, A.V.; et al. Prostate Cancer, Version 4.2023, NCCN Clinical Practice Guidelines in Oncology. Available online: https://www.nccn.org/professionals/physician_gls/pdf/prostate.pdf (accessed on 18 December 2023).
- Antonelli, A.; Sodano, M.; Peroni, A.; Mittino, I.; Palumbo, C.; Furlan, M.; Carobbio, F.; Tardanico, R.; Fisogni, S.; Simeone, C. Positive Surgical Margins and Early Oncological Outcomes of Robotic vs Open Radical Prostatectomy at a Medium Case-Load Institution. Minerva Urology and Nephrology 2016, 69, 63–68. [Google Scholar] [CrossRef] [PubMed]
- Hamdy, F.C.; Donovan, J.L.; Lane, J.A.; Metcalfe, C.; Davis, M.; Turner, E.L.; Martin, R.M.; Young, G.J.; Walsh, E.I.; Bryant, R.J.; et al. Fifteen-Year Outcomes after Monitoring, Surgery, or Radiotherapy for Prostate Cancer. New England Journal of Medicine 2023. [Google Scholar] [CrossRef] [PubMed]
- Wallis, C.J.D.; Zhao, Z.; Huang, L.-C.; Penson, D.F.; Koyama, T.; Kaplan, S.H.; Greenfield, S.; Luckenbaugh, A.N.; Klaassen, Z.; Conwill, R.; et al. Association of Treatment Modality, Functional Outcomes, and Baseline Characteristics With Treatment-Related Regret Among Men With Localized Prostate Cancer. JAMA Oncol 2022, 8, 50. [Google Scholar] [CrossRef] [PubMed]
- Oderda, M.; Diamand, R.; Albisinni, S.; Calleris, G.; Carbone, A.; Falcone, M.; Fiard, G.; Gandaglia, G.; Marquis, A.; Marra, G.; et al. Indications for and Complications of Pelvic Lymph Node Dissection in Prostate Cancer: Accuracy of Available Nomograms for the Prediction of Lymph Node Invasion. BJU Int 2021, 127, 318–325. [Google Scholar] [CrossRef]
- Chandrasekar, T.; Denisenko, A.; Mico, V.; McPartland, C.; Shah, Y.; Mark, J.R.; Lallas, C.D.; Fonshell, C.; Danella, J.; Jacobs, B.; et al. Multiparametric MRI Is Not Sufficient for Prostate Cancer Staging: A Single Institutional Experience Validated by a Multi-Institutional Regional Collaborative. Urol Oncol 2023, 41. [Google Scholar] [CrossRef]
- Briganti, A.; Larcher, A.; Abdollah, F.; Capitanio, U.; Gallina, A.; Suardi, N.; Bianchi, M.; Sun, M.; Freschi, M.; Salonia, A.; et al. Updated Nomogram Predicting Lymph Node Invasion in Patients with Prostate Cancer Undergoing Extended Pelvic Lymph Node Dissection: The Essential Importance of Percentage of Positive Cores. Eur Urol 2012, 61, 480–487. [Google Scholar] [CrossRef]
- Gandaglia, G.; Ploussard, G.; Valerio, M.; Mattei, A.; Fiori, C.; Fossati, N.; Stabile, A.; Beauval, J.-B.; Malavaud, B.; Roumiguié, M.; et al. A Novel Nomogram to Identify Candidates for Extended Pelvic Lymph Node Dissection Among Patients with Clinically Localized Prostate Cancer Diagnosed with Magnetic Resonance Imaging-Targeted and Systematic Biopsies. Eur Urol 2019, 75, 506–514. [Google Scholar] [CrossRef]
- Antonelli, A.; Vismara Fugini, A.; Tardanico, R.; Giovanessi, L.; Zambolin, T.; Simeone, C. The Percentage of Core Involved by Cancer Is the Best Predictor of Insignificant Prostate Cancer, According to an Updated Definition (Tumor Volume up to 2.5 Cm3): Analysis of a Cohort of 210 Consecutive Patients with Low-Risk Disease. Urology 2014, 83, 28–32. [Google Scholar] [CrossRef] [PubMed]
- Sebben, M.; Tafuri, A.; Shakir, A.; Pirozzi, M.; Processali, T.; Rizzetto, R.; Amigoni, N.; Tiso, L.; De Michele, M.; Panunzio, A.; et al. The Impact of Extended Pelvic Lymph Node Dissection on the Risk of Hospital Readmission within 180 Days after Robot Assisted Radical Prostatectomy. World J Urol 2020, 38, 2799–2809. [Google Scholar] [CrossRef]
- Porcaro, A.B.; Rizzetto, R.; Bianchi, A.; Gallina, S.; Serafin, E.; Panunzio, A.; Tafuri, A.; Cerrato, C.; Migliorini, F.; Antoniolli, S.Z.; et al. American Society of Anesthesiologists (ASA) Physical Status System Predicts the Risk of Postoperative Clavien–Dindo Complications Greater than One at 90 Days after Robot-Assisted Radical Prostatectomy: Final Results of a Tertiary Referral Center. Journal of Robotic Surgery 2022, 1–7. [Google Scholar] [CrossRef]
- Gnanapragasam, V.J.; Bratt, O.; Muir, K.; Lee, L.S.; Huang, H.H.; Stattin, P.; Lophatananon, A. The Cambridge Prognostic Groups for Improved Prediction of Disease Mortality at Diagnosis in Primary Non-Metastatic Prostate Cancer: A Validation Study. BMC Med 2018, 16, 31. [Google Scholar] [CrossRef] [PubMed]
- Parry, M.G.; Cowling, T.E.; Sujenthiran, A.; Nossiter, J.; Berry, B.; Cathcart, P.; Aggarwal, A.; Payne, H.; Van Der Meulen, J.; Clarke, N.W.; et al. Risk Stratification for Prostate Cancer Management: Value of the Cambridge Prognostic Group Classification for Assessing Treatment Allocation. BMC Med 2020, 18. [Google Scholar] [CrossRef] [PubMed]
- Stephenson, A.J.; Kattan, M.W.; Eastham, J.A.; Bianco, F.J.; Yossepowitch, O.; Vickers, A.J.; Klein, E.A.; Wood, D.P.; Scardino, P.T. Prostate Cancer–Specific Mortality After Radical Prostatectomy for Patients Treated in the Prostate-Specific Antigen Era. Journal of Clinical Oncology 2009, 27, 4300–4305. [Google Scholar] [CrossRef] [PubMed]
- Van den Broeck, T.; van den Bergh, R.C.N.; Arfi, N.; Gross, T.; Moris, L.; Briers, E.; Cumberbatch, M.; De Santis, M.; Tilki, D.; Fanti, S.; et al. Prognostic Value of Biochemical Recurrence Following Treatment with Curative Intent for Prostate Cancer: A Systematic Review. Eur Urol 2019, 75, 967–987. [Google Scholar] [CrossRef]
- Tilki, D.; Preisser, F.; Graefen, M.; Huland, H.; Pompe, R.S. External Validation of the European Association of Urology Biochemical Recurrence Risk Groups to Predict Metastasis and Mortality After Radical Prostatectomy in a European Cohort. Eur Urol 2019, 75, 896–900. [Google Scholar] [CrossRef]
- Pierorazio, P.M.; Walsh, P.C.; Partin, A.W.; Epstein, J.I. Prognostic Gleason Grade Grouping: Data Based on the Modified Gleason Scoring System. BJU Int 2013, 111, 753–760. [Google Scholar] [CrossRef]
- Magi-Galluzzi, C.; Evans, A.J.; Delahunt, B.; Epstein, J.I.; Griffiths, D.F.; van der Kwast, T.H.; Montironi, R.; Wheeler, T.M.; Srigley, J.R.; Egevad, L.L.; et al. International Society of Urological Pathology (ISUP) Consensus Conference on Handling and Staging of Radical Prostatectomy Specimens. Working Group 3: Extraprostatic Extension, Lymphovascular Invasion and Locally Advanced Disease. Modern Pathology 2011, 24, 26–38. [Google Scholar] [CrossRef]
- Berney, D.M.; Wheeler, T.M.; Grignon, D.J.; Epstein, J.I.; Griffiths, D.F.; Humphrey, P.A.; van der Kwast, T.; Montironi, R.; Delahunt, B.; Egevad, L.; et al. International Society of Urological Pathology (ISUP) Consensus Conference on Handling and Staging of Radical Prostatectomy Specimens. Working Group 4: Seminal Vesicles and Lymph Nodes. Modern Pathology 2011, 24, 39–47. [Google Scholar] [CrossRef]
- Benson, M.C.; Seong Whang, I.; Pantuck, A.; Ring, K.; Kaplan, S.A.; Olsson, C.A.; Cooner, W.H. Prostate Specific Antigen Density: A Means of Distinguishing Benign Prostatic Hypertrophy and Prostate Cancer. Journal of Urology 1992, 147, 815–816. [Google Scholar] [CrossRef]
- Jiang, J.; Colli, J.; El-Galley, R. A Simple Method for Estimating the Optimum Number of Prostate Biopsy Cores Needed to Maintain High Cancer Detection Rates While Minimizing Unnecessary Biopsy Sampling. J Endourol 2010, 24, 143–147. [Google Scholar] [CrossRef]
- Porcaro, A.B.; Novella, G.; Molinari, A.; Terrin, A.; Minja, A.; De Marco, V.; Martignoni, G.; Brunelli, M.; Cerruto, M.A.; Curti, P.; et al. Prostate Volume Index and Chronic Inflammation of the Prostate Type IV with Respect to the Risk of Prostate Cancer. Urol Int 2015, 94, 270–285. [Google Scholar] [CrossRef] [PubMed]
- Porcaro, A.B.; Tafuri, A.; Sebben, M.; Novella, G.; Processali, T.; Pirozzi, M.; Amigoni, N.; Rizzetto, R.; Shakir, A.; Mariotto, A.; et al. Prostate Volume Index and Prostatic Chronic Inflammation Predicted Low Tumor Load in 945 Patients at Baseline Prostate Biopsy. World J Urol 2020, 38, 957–964. [Google Scholar] [CrossRef] [PubMed]
- Freedland, S.J.; Wieder, J.A.; Jack, G.S.; Dorey, F.; deKernion, J.B.; Aronson, W.J. Improved Risk Stratification for Biochemical Recurrence after Radical Prostatectomy Using a Novel Risk Group System Based on Prostate Specific Antigen Density and Biopsy Gleason Score. J Urol 2002, 168, 110–115. [Google Scholar] [CrossRef] [PubMed]
- Freedland, S.J.; Isaacs, W.B.; Platz, E.A.; Terris, M.K.; Aronson, W.J.; Amling, C.L.; Presti, J.C.; Kane, C.J. Prostate Size and Risk of High-Grade, Advanced Prostate Cancer and Biochemical Progression After Radical Prostatectomy: A Search Database Study. Journal of Clinical Oncology 2005, 23, 7546–7554. [Google Scholar] [CrossRef]
- Porcaro, A.B.; Amigoni, N.; Tafuri, A.; Rizzetto, R.; Shakir, A.; Tiso, L.; Cerrato, C.; Lacola, V.; Zecchini Antoniolli, S.; Gozzo, A.; et al. Endogenous Testosterone as a Predictor of Prostate Growing Disorders in the Aging Male. Int Urol Nephrol 2021, 53, 843–854. [Google Scholar] [CrossRef]
Figure 1.
Model description and assumptions of index density of percentage of biopsy positive cores (Id-tumor densities decrease. For instance, tumors with a BPC of 10% could occur in a PV of 30 mL (Id-BCP = 0.33, (A)), 60 mL (Id-BPC = 0.16, (B)), or 90 mL (Id-BPC = 0.11, (C)). However, tumor load density is higher in the former case, where unfavorable pathology in the surgical specimen and an increased risk of disease progression are expected.
Figure 1.
Model description and assumptions of index density of percentage of biopsy positive cores (Id-tumor densities decrease. For instance, tumors with a BPC of 10% could occur in a PV of 30 mL (Id-BCP = 0.33, (A)), 60 mL (Id-BPC = 0.16, (B)), or 90 mL (Id-BPC = 0.11, (C)). However, tumor load density is higher in the former case, where unfavorable pathology in the surgical specimen and an increased risk of disease progression are expected.
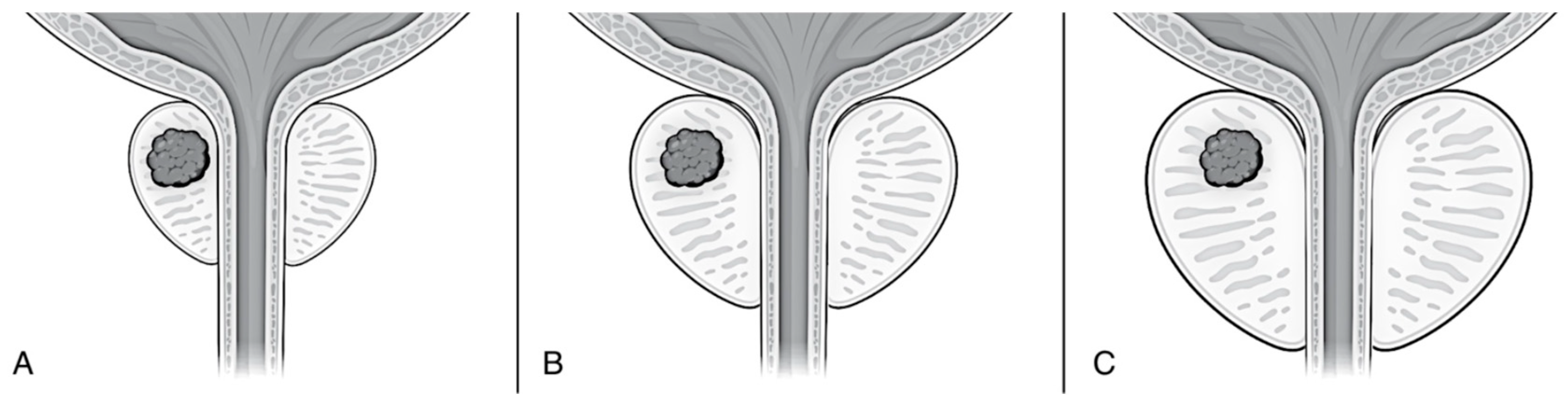
Figure 2.
Kaplan-Meyer survival risk curves of prostate cancer (PCa) progression stratified by unfavorable versus favorable pathology in the surgical specimen of 1047 patients treated with robot-assisted radical prostatectomy (RARP) eventually associated with extended pelvic lymph node dissection (ePLND). Mean survival time of PCa progression was longer for favorable pathology (101.8 months; 95% CI: 98.7 – 104.9 months) than unfavorable pathology (86.3 months; 95% CI: 83.7 – 88.9 months (Mantel-Cox log-rank test: p < 0.0001).
Figure 2.
Kaplan-Meyer survival risk curves of prostate cancer (PCa) progression stratified by unfavorable versus favorable pathology in the surgical specimen of 1047 patients treated with robot-assisted radical prostatectomy (RARP) eventually associated with extended pelvic lymph node dissection (ePLND). Mean survival time of PCa progression was longer for favorable pathology (101.8 months; 95% CI: 98.7 – 104.9 months) than unfavorable pathology (86.3 months; 95% CI: 83.7 – 88.9 months (Mantel-Cox log-rank test: p < 0.0001).
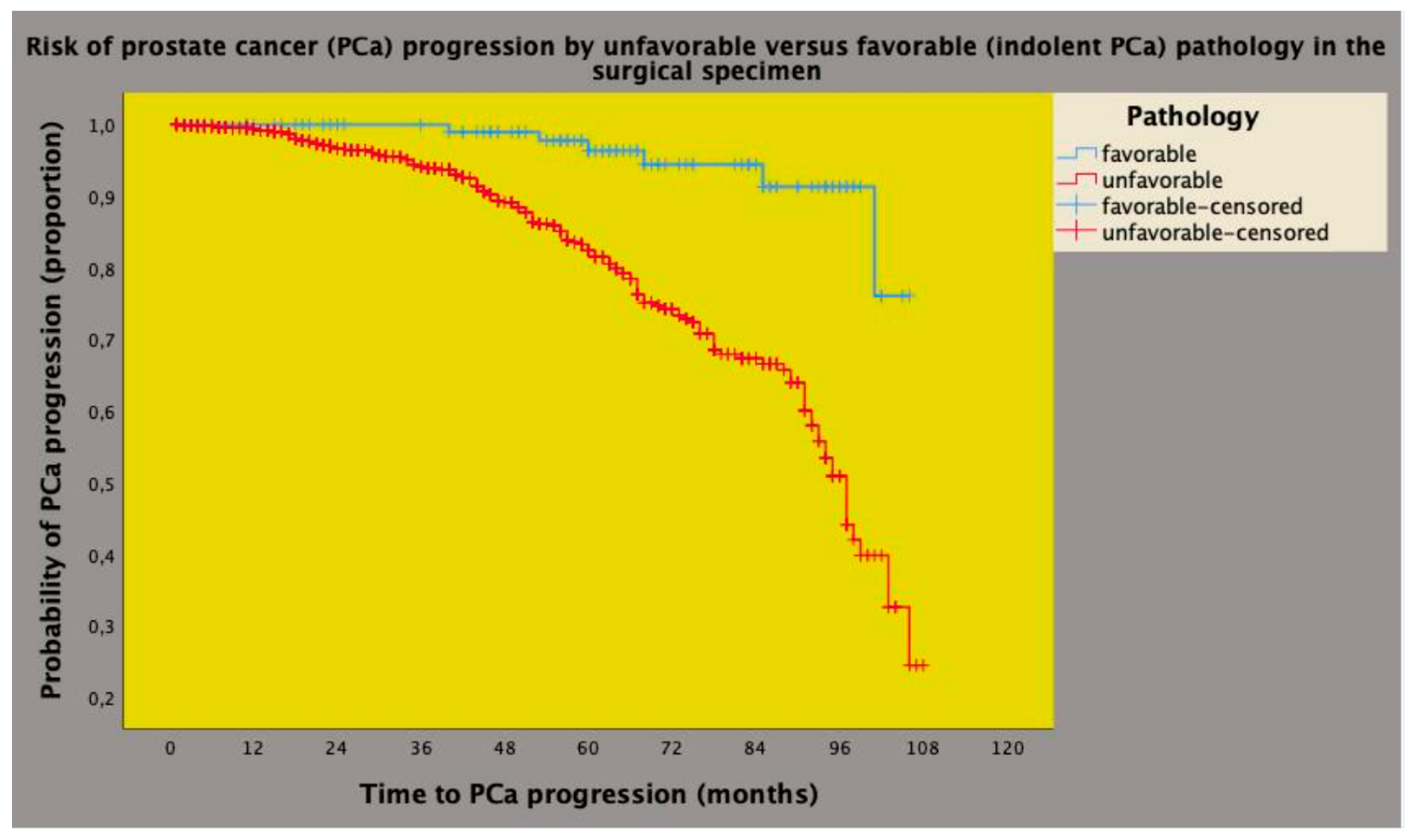
Figure 3.
Distribution of index density of percentage of biopsy positive cores (Id-BPC, %/mL), defined as the ratio of percentage of biopsy positive cores (BPC) on prostate volume (PV). Id-BPC was higher in patients with unfavorable pathology (median 0.83, interquartile range: 0.47 – 1.82) than in cases with favorable pathology (median 0.43, interquartile range: 0.28 – 1.05) in the surgical specimen and the difference was significant (odds ratio = 2.187; 95% CI: 1.541 – 3.103; p < 0.0001).
Figure 3.
Distribution of index density of percentage of biopsy positive cores (Id-BPC, %/mL), defined as the ratio of percentage of biopsy positive cores (BPC) on prostate volume (PV). Id-BPC was higher in patients with unfavorable pathology (median 0.83, interquartile range: 0.47 – 1.82) than in cases with favorable pathology (median 0.43, interquartile range: 0.28 – 1.05) in the surgical specimen and the difference was significant (odds ratio = 2.187; 95% CI: 1.541 – 3.103; p < 0.0001).
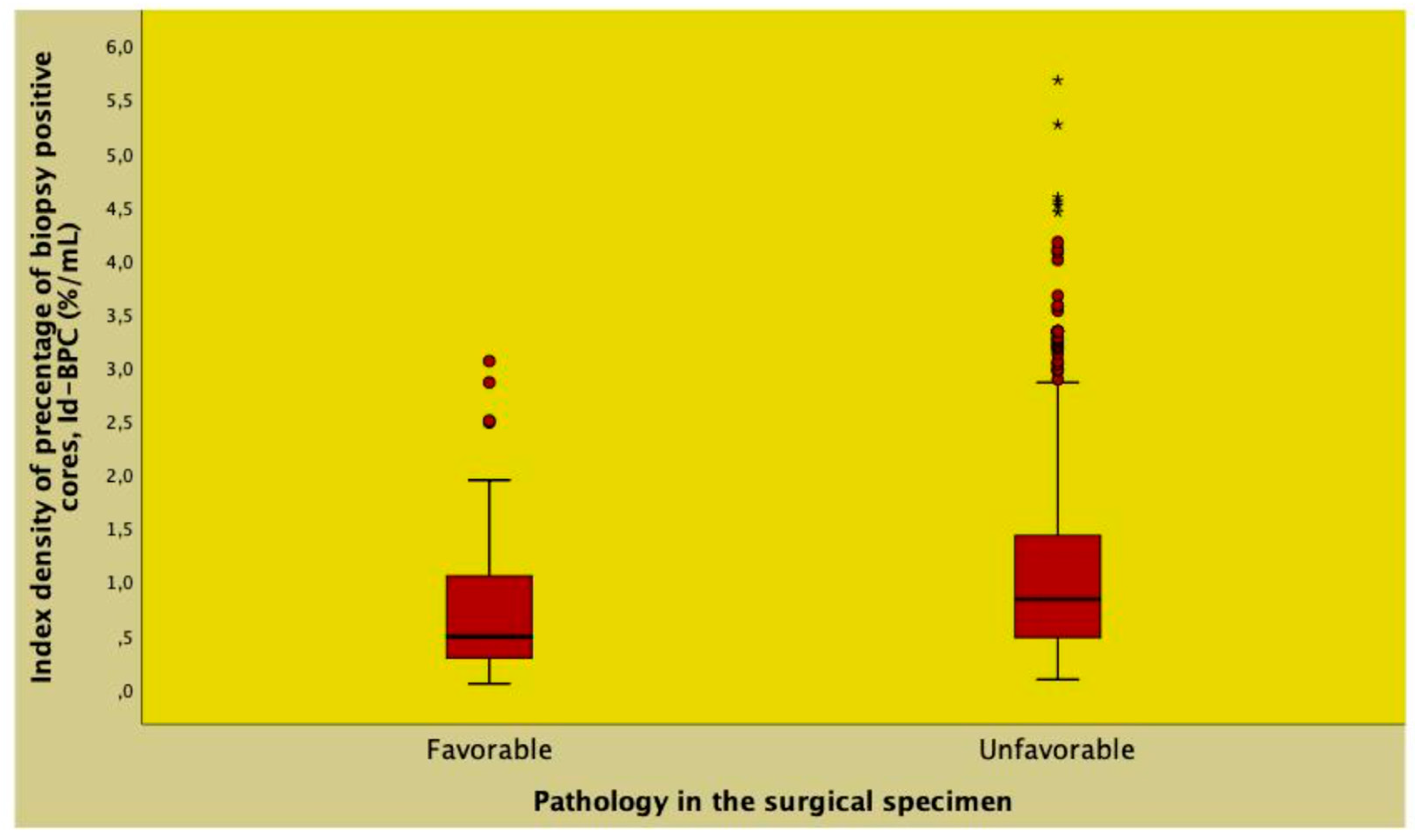
Figure 4.
Distribution of index density of percentage of biopsy positive cores (Id-BPC, %/mL), defined as the ratio of percentage of biopsy positive cores (BPC) on prostate volume (PV). Id-BPC was higher in patients experiencing prostate cancer progression (median 1.06, interquartile range: 0.57 – 1.80) than in non-progressing cases (median 0.77, interquartile range: 0.40 – 1.29) and the difference was significant (hazard ratio = 1.454; 95% CI: 1.274 – 1.697; p < 0.0001).
Figure 4.
Distribution of index density of percentage of biopsy positive cores (Id-BPC, %/mL), defined as the ratio of percentage of biopsy positive cores (BPC) on prostate volume (PV). Id-BPC was higher in patients experiencing prostate cancer progression (median 1.06, interquartile range: 0.57 – 1.80) than in non-progressing cases (median 0.77, interquartile range: 0.40 – 1.29) and the difference was significant (hazard ratio = 1.454; 95% CI: 1.274 – 1.697; p < 0.0001).
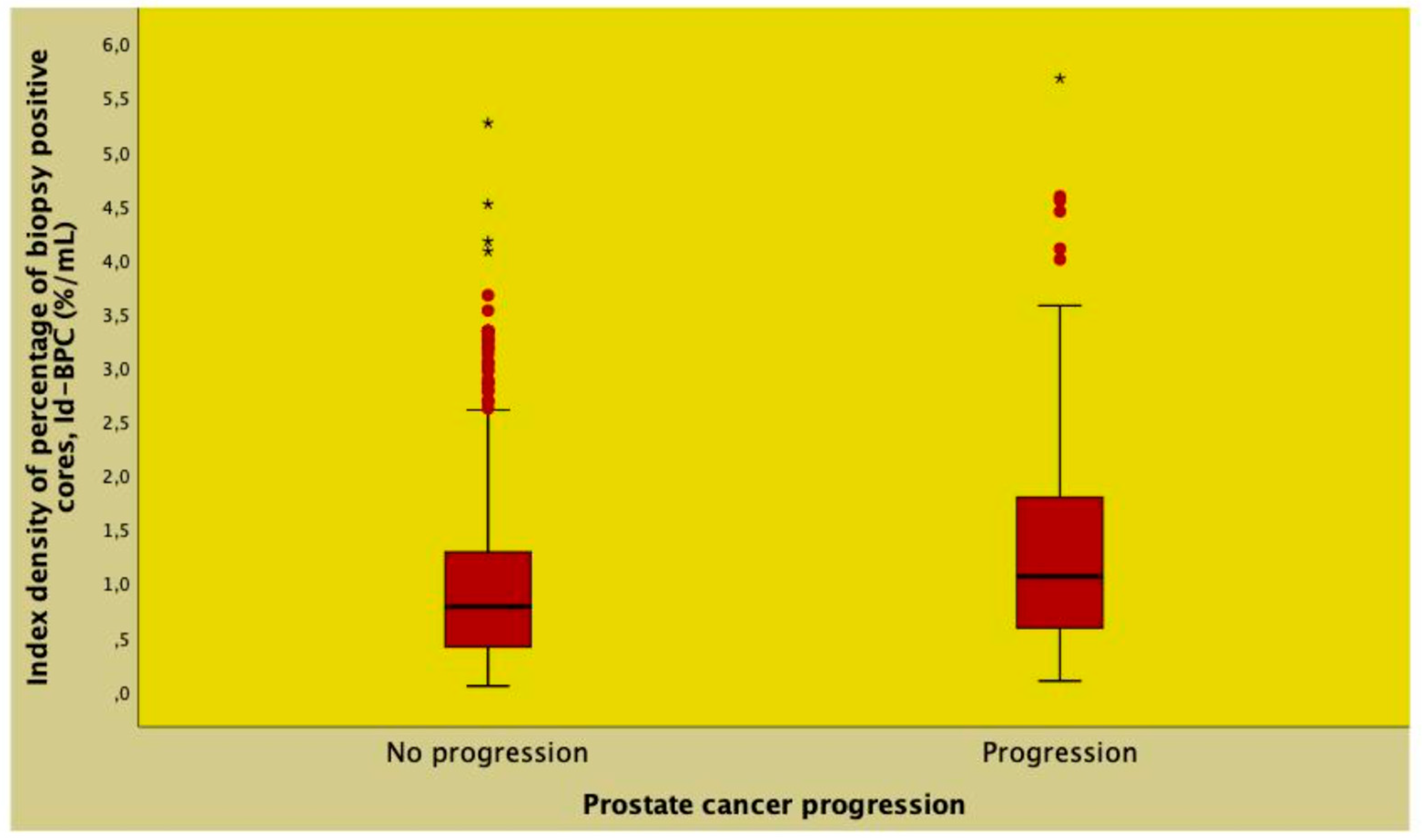

Table 1.
Distributions of clinical prostate cancer (PCa) factors according to pathological findings in 1047 patients treated with robot-assisted radical prostatectomy (RARP).
Table 1.
Distributions of clinical prostate cancer (PCa) factors according to pathological findings in 1047 patients treated with robot-assisted radical prostatectomy (RARP).
| Factors | Population | Favorable pathology | Unfavorable pathology | |
|---|---|---|---|---|
| N (%) | 1047 | 117 (11.2) | 930 (88.8) | P-value |
| Age (years) | 65 (60 - 70) | 63 (58 - 68) | 65 (60 - 70) | 0.013 |
| BMI (kg/m2) | 25.7 (23.9 - 28.1) | 25.6 (23.7 - 28.1) | 25.7 (23.9 - 28.1) | 0.939 |
| ASA 1 | 88 (8.4) | 13 (11.1) | 75 (8.1) | 0.136 |
| ASA 2 | 858 (82.0) | 98 (83.8) | 760 (81.7) | |
| ASA 3 | 101 (9.6) | 6 (5.1) | 95 (10.2) | |
| PV (mL) | 40 (30 - 50) | 42 (31.7-53) | 39 (30 - 50) | 0.020 |
| PSA (ng/mL) | 6.6 (5.0 - 9.1) | 6.1 (4.6 - 7.8) | 6.7 (5.0 - 9.3) | 0.013 |
| PSAD (ng/mL2) | 0.17 (0.11 - 0.25) | 0.13 (0.09 - 0.21) | 0.17 (0.12 - 0.26) | <0.0001 |
| BPC (%) | 31.2 (20 - 50) | 21.4 (14.2 - 35.7) | 33.3 (20 - 50) | <0.0001 |
| Id-BPC (%/mL) | 0.81 (0.43 - 1.37) | 0.48 (0.28 - 1.05) | 0.83 (0.47 - 1.42) | <0.0001 |
| ISUP 1 | 361 (34.5) | 98 (83.8) | 263 (28.3) | <0.0001 |
| ISUP 2/3 | 554 (52.9) | 19 (16.2) | 535 (57.5) | |
| ISUP 4/5 | 132 (12.6) | 0 (0.0) | 132 (14.2) | |
| cT1 | 600 (57.3) | 92 (78.6) | 508 (54.6) | <0.0001 |
| cT2/3 | 447 (42.7) | 25 (21.4) | 422 (45.4) | |
| cN0 | 990 (94.6) | 116 (99.1) | 874 (94) | 0.020 |
| cN1 | 57 (5.4) | 1 (0.9) | 56 (6) |
Legend: OR, odds ratio; CI: confidence interval; continuous variables are reported as medians (interquartile ranges) while categorical factors are described as frequencies (%); BPC, percentage of biopsy positive cores; Id-BPC: index density of BPC; for other abbreviations see materials and methods.
Table 2.
Clinical factors associated with the risk of unfavorable prostate cancer (PCa) pathology in 1047 patients treated with robot-assisted radical prostatectomy (RARP).
Table 2.
Clinical factors associated with the risk of unfavorable prostate cancer (PCa) pathology in 1047 patients treated with robot-assisted radical prostatectomy (RARP).
| Univariate analysis | Multivariate analysis | |||
|---|---|---|---|---|
| Statistics | OR (95% CI) | P-value | OR (95% CI) | P-value |
| Age (years) | 1.031 (1.005 - 1.059) | 0.021 | ||
| BMI (kg/m2) | 1.004 (0.946 - 1.065) | 0.907 | ||
| ASA 1 | Ref | |||
| ASA 2 | 1.344 (0.719 - 2.512) | 0.354 | ||
| ASA 3 | 2.744 (0.996 - 7.562) | 0.051 | ||
| PV (mL) | 0.989 (0.980 - 0.998) | 0.023 | ||
| PSA (ng/mL) | 1.091 (1.031 - 1.154) | 0.002 | ||
| PSAD (ng/mL2) | 40.796 (5.760 - 288.950) | <0.0001 | 9.004 (1.120 - 72.385) | 0.039 |
| Id-BPC (%/mL) | 2.187 (1.541 - 3.103) | <0.0001 | 1.512 (1.029 - 2.221) | 0.035 |
| ISUP 1 | Ref | Ref | ||
| ISUP > 1 | 13.081 (7.482 - 21.819) | <0.0001 | 10.596 (6.306 - 17.806) | <0.0001 |
| cT1 | Ref | Ref | ||
| cT2/3 | 3.057 (1.929 - 4.845) | 1.904 (1.160 - 3.127) | 0.011 | |
| cN0 | Ref | |||
| cN1 | 7.432 (1.019 - 54.202) | 0.048 |
Legend: OR, odds ratio; CI: confidence interval; Id-BPC: index density of percentage of biopsy positive cores; for other abbreviations see materials and methods.
Table 3.
Clinical factors associated with the risk of prostate cancer (PCa) progression in 1047 patients after robot-assisted radical prostatectomy.
Table 3.
Clinical factors associated with the risk of prostate cancer (PCa) progression in 1047 patients after robot-assisted radical prostatectomy.
| No PCa progression | Pca progression | Univariate analysis | Multivariate analysis | |||
|---|---|---|---|---|---|---|
| N (%) | 810 (77.4) | 237 (22.6) | HR (95% CI) | P-value | HR (95% CI) | P-value |
| Age (years) | 65 (59.7 - 70.0) | 65 (61 - 70) | 1.032 (1.011 - 1.052) | 0.002 | ||
| BMI (kg/m2) | 25.8 (23.9 - 28.1) | 25.6 (23.8 - 28.1) | 0.986 (0.947 - 1.027) | 0.502 | ||
| ASA 1 | 66 (8.1) | 22 (9.3) | Ref | |||
| ASA 2 | 668 (82.5) | 190 (80.2) | 0.876 (0.563 - 1.365) | 0.559 | ||
| ASA 3 | 76 (9.4) | 25 (10.5) | 1.336 (0.753 - 2.370) | 0.322 | ||
| PV (mL) | 40 (30 - 50) | 39 (30 - 50) | 1.005 (0.998 - 1.013) | 0.178 | ||
| PSA (ng/mL) | 6.3 (4.9 - 8.5) | 8 (5.4 - 12.5) | 1.038 (1.031 - 1.045) | <0.0001 | 1.027 (1.019 - 1.035) | <0.0001 |
| PSAD (ng/mL2) | 0.16 (0.11 - 0.23) | 0.21 (0.13 - 0.35) | 4.314 (3.198 - 5.820) | <0.0001 | ||
| Id-BPC (%/mL) | 0.74 (0.39 - 1.25) | 1.07 (0.57 - 1.81) | 1.468 (1.294 - 1.666) | <0.0001 | 1.561 (1.336 - 1.824) | <0.0001 |
| ISUP 1 | 308 (38) | 53 (22.3) | Ref | Ref | ||
| ISUP 2/3 | 432 (53.3) | 122 (51.5) | 2.785 (2.010 - 3.857) | <0.0001 | 2.618 (1.880 - 3.646) | <0.0001 |
| ISUP 4/5 | 70 (8.7) | 62 (26.2) | 6.658 (4.589 - 9.659) | <0.0001 | 4.709 (3.206 - 6.915) | <0.0001 |
| cT1 | 477 (58.9) | 123 (51.9) | Ref | Ref | ||
| cT2/3 | 333 (41.1) | 114 (48.1) | 2.131 (1.647 - 2.758) | <0.0001 | 1.549 (1.181 - 2.031) | 0.002 |
| cN0 | 775 (95.7) | 215 (90.7) | Ref | Ref | ||
| cN1 | 35 (4.3) | 22 (9.3) | 2.840 (1.824 - 4.421) | <0.0001 |
Legend: OR, odds ratio; CI, confidence interval; see also material and methods for explanations.
Table 4.
Multivariate analysis comparing the percentage of biopsy positive cores (BPC) and index density of BPC (Id-BPC) with the risk of unfavorable tumor pathology and prostate cancer (PCa) progression in 1047 patients treated with robot-assisted radical prostatectomy (RARP).
Table 4.
Multivariate analysis comparing the percentage of biopsy positive cores (BPC) and index density of BPC (Id-BPC) with the risk of unfavorable tumor pathology and prostate cancer (PCa) progression in 1047 patients treated with robot-assisted radical prostatectomy (RARP).
| Event occurrence | Id-BPC (%/mL) | BPC (%) |
|---|---|---|
| UNFAVOURABLE TUMOR PATHOLOGY | ||
| a) after adjusting for all clinical factors | ||
| OR (95% CI) | 1.566 (1.029 - 2.383) | 1.018 (1.006 - 1.031) |
| p-value | <0.0001 | <0.0001 |
| PROSTATE CANCER PROGRESSION | ||
| a) after adjusting for all clinical factors | ||
| HR (95% CI) | 1.587 (1.306 - 1.929) | 1.015 (1.008 - 1.021) |
| p-value | <0.0001 | <0.0001 |
| a) after adjusting for unfavorable pathology | ||
| HR (95% CI) | 1.365 (1.166 - 1.597) | 1.016 (1.010 - 1.022) |
| p-value | <0.0001 | <0.0001 |
Legend: OR, odds ratio; HR, hazard ratio; CI: confidence interval.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



