
Submitted:
16 November 2024
Posted:
18 November 2024
You are already at the latest version
Abstract
Hyponatremia, a common electrolyte imbalance in older adults, results from physiological aging, medication use, and comorbidities, with significant implications for morbidity and quality of life. This narrative review aims to explore the impact of dietary habits and nutritional deficiencies on the development and management of hyponatremia in this population. A literature search identified relevant studies addressing sodium balance, dietary intake, and nutrition related risk factors. Key findings reveal that low sodium and age-related changes, increase vulneratbility to hyponatremia and its associated risks, including cognitive decline and falls. Nutritional strategies, such as opti-mizing sodium and protein intake and reducing processed food consumption, may offer preven-tative benefits. Future research should focus on tailored dietary interventions and establishing so-dium intake guidelines specific to older adults. Implementing such strategies could improve health outcomes and reduce healthcare costs associated with hyponatremia in older populations.
Keywords:
hyponatremia
; frailty
; geriatric
; sarcopenia
1. Introduction
Hyponatremia is defined as a serum sodium level below 135 mEq/L and is a common occurrence in older adults.[1] Globally, an estimated 703 million people are age 65 and older. This number is expected to double by 2050, which may further strain healthcare systems.[2] The prevalence of hyponatremia is around 8% in the general population but rises sharply in older adults, particularly in hospital settings, where it can range from 15% to 30%.[3] In community-dwelling older individuals aged 75 and above, the prevalence reaches approximately 11.6%.[4] Hyponatremia is more frequently observed in patients in acute-care hospital, critical care units, ambulatory-care settings, and geriatric populations than in the general population.[1,5,6] The prevalence of hyponatremia increases with age.[7] Its prevalence is about 18% in older adults compared to 2.98% in younger groups. Strategies for hospitalized older adults should include plans that optimize sodium balance and prevent adverse outcomes associated with hyponatremia, such as cognitive impairment, falls, and increased morbidity.[8]
This condition is of great clinical concern as it increases the risk of morbidity and mortality, cognitive decline, falls, and fractures, which significantly impair quality of life and increase healthcare costs by up to 20%.[9] This review aims to explore the relationship between dietary habits, nutritional deficiencies, and hyponatremia in older adults, summarizing the implications for clinical practice and prevention.
Sodium is critical in maintaining cellular homeostasis, fluid balance, nerve function, and circulatory pressures. The bioavailability of sodium is reduced as individuals get older. Physiological changes, such as decreased glomerular filtration rate (GFR), impaired sodium conservation, and reduced sodium bioavailability contribute to this reduction.[10] Older adults are vulnerable to hyponatremia due to factors such as malnutrition, chronic diseases, and polypharmacy. The presence of impaired dietary intake, especially if low in sodium and protein consumption increases the risk of hyponatremia. This is evident in conditions such as “tea and toast” syndrome. The syndrome results from an insufficient intake of key nutrients, that result in sodium depletion due to a fluid imbalance.[1]
The clinical consequences of hyponatremia in older adults are significant. Hyponatremia impacts cognitive function and may result in delirium. In the hospital setting this could result in increased length of hospital stay increasing the risk of institutionalization, functional dependence, and mortality. [11] Therefore, understanding the role of dietary habits and nutritional deficiencies in developing hyponatremia is needed to develop effective prevention and management strategies tailored to this vulnerable population.
2. Methods
This narrative review was conducted to explore the relationship between dietary habits, nutritional deficiencies, and the incidence of hyponatremia in older adults. The aim was to provide a comprehensive understanding of the topic of diverse sources available in MedSurg literature, focusing on clinically relevant insights. A comprehensive literature search was conducted using PubMed, focusing on articles published in peer-reviewed journals. Key words included “hyponatremia,” “older adults,” “dietary sodium,” “nutritional deficiency,” “sarcopenia,” and “fluid balance.” Additional searches were performed using terms related to “frailty” and “malnutrition” to ensure the inclusion of studies addressing broad aspects of hyponatremia in the older populations. Our approach focused on summarizing findings from clinically significant studies to offer a broad perspective on how dietary and nutritional factors may impact hyponatremia. Articles were chosen based on their relevance, the insights they offered into the interaction between nutrition, sodium balance, and the hyponatremia risks in older adults.
- Understanding Hyponatremia in Older Adults
-
Overview of Sodium Balance and Regulation in the BodySerum sodium is vital for maintaining fluid balance, regulating nerve and muscle cell function, and facilitating the transport of substrate across membranes.[7] Its critical roles influence hyponatremia's acute and chronic manifestations. A rapid decrease in serum sodium within 48 hours can lead to symptoms such as headaches, nausea, vomiting, and potentially progress to seizures and coma.[1] Chronic hyponatremia can manifest as fatigue, cognitive impairment, and gait deficits, leading to falls, osteoporotic fractures, and many associated symptoms.[12,13,14,15,16]
-
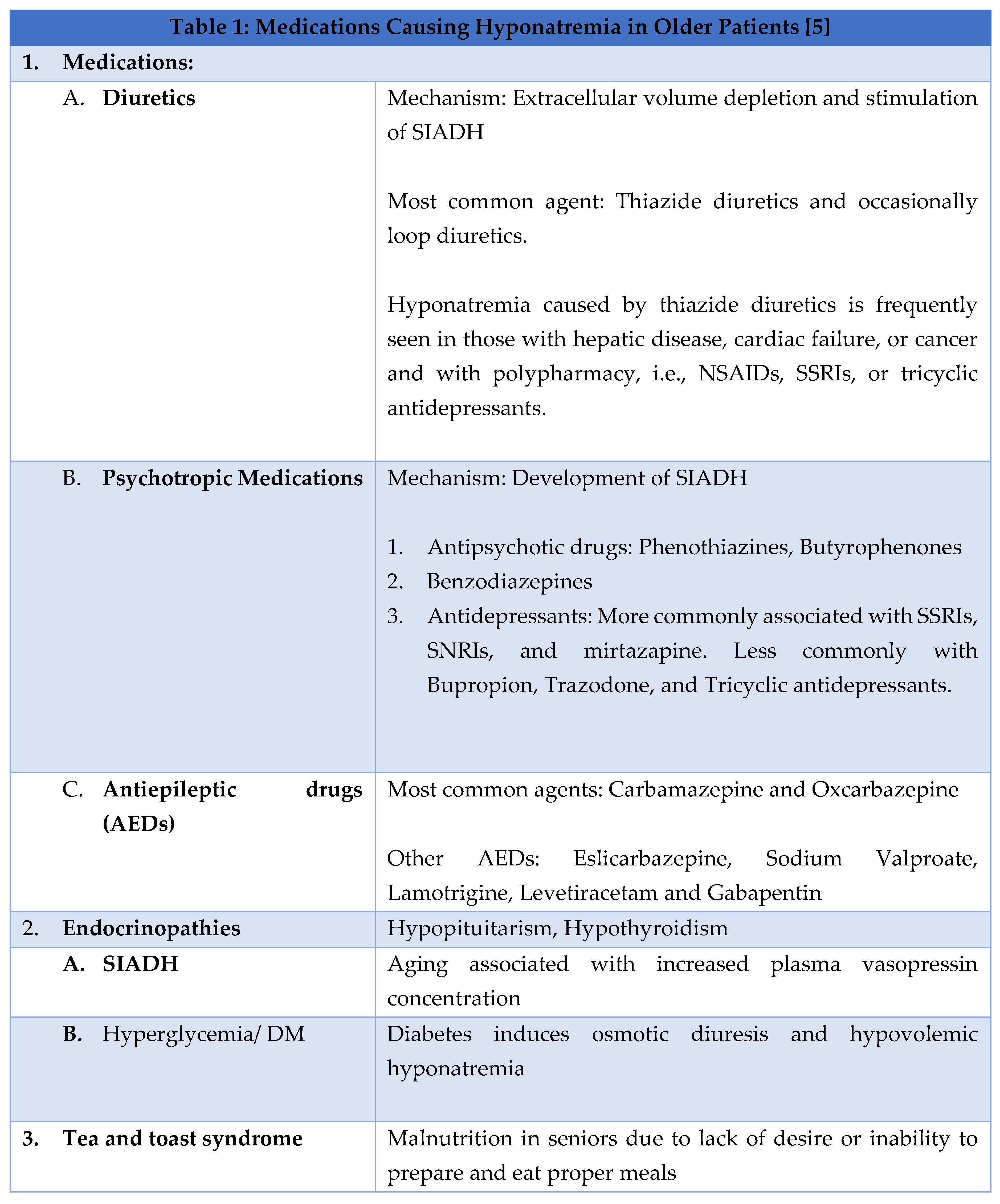
Factors Contributing to Hyponatremia in the older adultAge is an independent risk factor for hyponatremia in older adults, often due to medications, endocrinopathies, syndrome of inappropriate antidiuretic hormone secretion (SIADH), and malnutrition, and at times leading to the development of 'tea and toast' syndrome.[1] Some common causes of hyponatremia are given in Table 1.
-
“Tea and Toast” HyponatremiaOne notable example of a dietary habit leading to malnutrition and hyponatremia in older adults is the “tea and toast” syndrome. Tea and toast are typically deficient in sodium, protein, and other vital nutrients. Older individuals whose primary diet consists of such a diet increase their risk of developing hyponatremia. [17] Such a dietary pattern is often seen in older adults with poor appetite, difficulty preparing meals, or limited access to diverse food sources. A “tea and toast” diet results in sodium depletion. This in combination with excessive water intake, results in dilution of sodium levels in the blood, creating fluid imbalance, causing hyponatremia. Additionally, protein deficiency in such diets exacerbates malnutrition, contributing further to sarcopenia and frailty.[18,19]
-
Hyponatremia and FallsHyponatremia that is symptomatic is readily diagnosed and managed. Mild chronic hyponatremia presents a more significant challenge because of its links to adverse outcomes. Hyponatremia increases the risks of falls by contributing to neurocognitive impairment, which can cause gait instability and decreased attention span.[20] This has substantial implications for geriatric care, as falls are a common medical concern among older adults.[21] Falls affect 30-60% of older adults living independently in the community yearly.[22] The outcomes of such falls in older adults can include hip fractures, hospitalizations, head injuries, and the need for admission to long-term care facilities.[21] Furthermore, prospective data from the Rotterdam Study demonstrated a significant association between baseline mild hyponatremia and recent falls, as well as both vertebral and incidental non-vertebral fractures.[12] Epidemiological and experimental evidence has shown that chronic mild hyponatremia is an independent risk factor for osteoporosis, as it increases bone osteoclastic activity in a hyponatremic environment.[23] Chronic mild hyponatremia is associated with extended hospital stays, functional independence, and increased mortality in individuals with chronic disease and those admitted in the Intensive Care Unit (ICU) settings.[12,23,24,25]
- 2.
- The Role of Dietary Habits in Hyponatremia
Sodium is naturally present in various foods, and its intake can vary based on dietary habits. Familiar sources of dietary sodium include processed and packaged foods, often high in added salt. Table salt, used in cooking or as a seasoning, primarily contributes to sodium intake. Additionally, sodium-rich foods include salty snacks (such as chips and pretzels), canned soups, pickles, cured meats (such as bacon, ham, and sausages), cheese, and certain condiments (like soy sauce). Some natural foods, such as shellfish, dairy products, and vegetables like beets and celery, also provide smaller amounts of sodium.[26] For older adults at risk of hyponatremia it is important to manage the intake of these foods.
-
The Impact of Low Sodium Diets on Older AdultsLower dietary sodium intake amongst community-dwelling older adults was associated with poorer cognitive function, especially in those over 80. [27] . Cognitive impairments may affect executive functions, potentially impacting intermediate activities of daily living such as financial management. Given the risk of cognitive decline in older adults, even minor changes in cognitive ability because of low sodium intake could have significant health implications. Despite the known benefits of reducing dietary sodium for hypertension, the impact of hyponatremia on cognitive function underscores the need for further investigation.[28,29] Low nutritional sodium levels may negatively influence insulin regulation and the renin-angiotensin and sympathetic systems, potentially affecting cognitive function.[30,31,32] A recent study found a J-shaped relationship between sodium intake, cardiovascular disease and mortality. Individuals consuming more than 6 g of sodium per day and those consuming less than 3 g daily were found to have an increased risk of death and cardiovascular events.[33] Although further research is required, previous studies indicate a potential J-shaped relationship between sodium intake and cognitive function in older adults.[34,35,36] In a recent study involving older adults (average age 70 +- 12 years), adding a low-dose diuretic to angiotensin II receptor blockers for hypertension management significantly lowered serum sodium levels in individuals with low dietary salt intake.[37] As a result reducing dietary sodium intake to low levels may impair an individual's ability to maintain homeostasis, which could result in cognitive changes. This is especially concerning for older adults on medications that effect sodium levels. Reduced sodium intake has also been associated with a higher risk of cardiovascular events and mortality, regardless of blood pressure levels.[23,38]
-
Sodium-Rich Foods and Their Effects on HyponatremiaIncreased sodium intake elevates intra-glomerular pressure, which can contribute to or worsen chronic kidney damage, heightening the risk of progressive kidney disease.[39] High sodium intake is a recognized risk factor for developing such conditions. Specifically, in postmenopausal women in Korea,[36,38] excessive sodium intake (>2000 mg) was found to lead to increased urinary excretion (> 2 g/day), resulting in hypercalciuria and raising the risk of osteoporosis.[40] Additionally, excessive salt consumption has been linked to the development of hypertension[41,42] and, consequently, to a higher risk of cardiovascular disease, particularly in individuals with hypertension and older adults.[23] Lowering sodium intake has been shown to reduce both systolic and diastolic blood pressure, especially in hypertensive and normotensive individuals.[41]
-
The Role of Ultra-Processed Foods in Sodium IntakeThe increased availability and consumption of ultra-processed foods has contributed to higher sodium intake in the general population. This increase is beyond the recommended dietary intake of sodium. Ultra-processed foods include packaged snacks, ready-to-eat meals, processed meats, instant noodles, and fast foods. These often contain high levels of added sodium to enhance the flavor and prolong shelf life. [43] This trend is concerning for older adults who have multiple chronic conditions (MCC), as excessive sodium intake from these foods can exacerbate hypertension, cardiovascular disease, and renal impairment.
Consumption of ultra-processed foods could lead to both hyponatremia and hypernatremia, in older adults, especially those with MCC, especially if on multiple medications. Thus, it is crucial for dietary interventions targeting sodium management in to consider reducing ultra-processed food intake while promoting whole, minimally processed foods that support healthier sodium levels and overall nutrition.[43]
- 3.
-
Nutritional Deficiencies and HyponatremiaAs people age, their metabolic and organ reserves universally decline. A diet that may be suitable for a young adult could become harmful for the same individual later in life. Failure to adjust diet and lifestyle accordingly can result in maladaptation, where the body struggles to compensate, leading to the development of various chronic conditions common in older adults, such as hypertension (HTN), diabetes (DM), cardiovascular disease (CVS), and chronic kidney disease (CKD).[44] According to the Dietary Guidelines Advisory Committee (DGAC), nearly half of all American adults, approximately 117 million individuals, have one or more chronic diseases that could be prevented with dietary improvements.[45] In an aging population, diet-induced health problems have a more significant impact due to reduced adaptability from age-related metabolic capacity and organ function declines. This contributes to the increased prevalence of chronic conditions like HTN, atherosclerotic vascular diseases, and CKD in older adults. Poor diets are the primary driver of the chronic disease burden in the United States. Currently, only 1% of Americans meet the criteria for ideal CVS health; 46% have HTN, around 50% have prediabetes or DM, and approximately 14% have CKD. Adjusting nutrient intake in the modern diet can mitigate risks of maladaptation, such as acid accumulation, excessive salt intake, potassium (K+) and fiber deficiency, and dehydration, significantly improving overall health.[44]
Salt and water regular are closely intertwined. Serum sodium (Na+) concentration reflects water balance and is the primary determinant of serum osmolality. In the kidney, arginine vasopressin (AVP) and tonicity enhancer element binding protein (TonEBP or NFAT5) work independently and together to maintain regular water absorption, maintaining serum Na+ concentration within the 135-145 mEq/L range. AVP regulates water and retains Na+, affecting volume balance.[44]
The modern diet is deficient in potassium (K+).[46] A low or low-normal serum or plasma K+ concentration resulting from insufficient intake can stimulate kidney NH3/NH4+ production and activate the RAAS, contributing to system inflammation, protein catabolism, CKD development, and, in patients with CKD, accelerating its progression.[47]
Chronic low-grade under-hydration has been linked to impaired cognitive performance, reduced cognition, perceived fatigue, and a lack of energy.[48] Underhydration also increases vulnerability to suboptimal adaptation or maladaptation, leading to kidney dysfunction and other health complications, particularly during physical stress or exposure to hot climates. It is not surprising that chronic under-hydration is also associated with nephrolithiasis,[49] as well as an increased risk of metabolic syndrome and CKD.[44,50,51] Fortunately, studies have shown that the adverse effects of a poor diet can be minimized through dietary modification, specifically by reducing overconsumption of salt and animal products while increasing unrefined plant foods and hydration. Increasing dietary intake of fruits and vegetables enhances both base equivalents and K+ in body fluids, associated with lower blood pressure and reduced risk of CVS diseases, including heart failure (HF) and overall mortality.[23,52,53,54,55,56]
-
Protein Energy Malnutrition and Hyponatremia in the ElderlySarcopenia is an age-related decline in skeletal muscle mass and function.[28] The European Working Group on Sarcopenia in Older People (EWGSOP) characterizes sarcopenia as a "progressive and widespread skeletal muscle condition linked to a higher risk of undesirable consequences, such as falls, fractures, physical impairment, and mortality.[57] Sarcopenia has an estimated prevalence of 9 to 18% in people aged sixty-five and older, increasing to 50% in those aged over eighty. Moreover, it has been postulated that beyond 50 years of age, muscle mass is lost at an approximate rate of 1-2% per year.[58] Some of the risk factors for sarcopenia include age, female sex, history of smoking, little to no exercise, particularly endurance training, and specific nutritional deficiencies.[57]
With increasing age, skeletal muscle size and number decrease, including reduced skeletal muscle precursor cells.[59] The causes of sarcopenia are multifaceted. Decreased activity among older people,[59] protein-calorie malnutrition and overnutrition,[19] hormonal declines such as decreased IGF-1, DHEA-sulfate, testosterone, and estrogen levels,[21] and increased inflammatory biomarkers [22] are believed to be critical contributors to the development of sarcopenia. Sarcopenia results in impaired mobility, functional dependence, and increase injury episodes among older adults. Muscle atrophy and decreased muscle strength, especially in the lower limbs, contribute to an increasing incidence of falls, that may result in fractures and other disabilities.[24] Moreover, a higher incidence of functional decline and an increased length of hospitalization are also reported among sarcopenic individuals. Sarcopenia has also been identified as a significant cause of mortality, particularly among those older than seventy-nine.[27]
Sarcopenia has been described as a potential cause of hyponatremia in the literature. Since muscle content represents the body's central potassium reserve, low potassium levels are seen in individuals with sarcopenia. Low potassium content leads to a shift of sodium intracellularly and an inappropriate release of antidiuretic hormone (ADH). These two mechanisms contribute to the development of hyponatremia.[60] On the other hand, hyponatremia may also lead to sarcopenia. As mild hyponatremia is frequently encountered among the geriatric population, its high propensity to cause sarcopenia makes it imperative for physicians to address the condition in a clinical setting.[61] Frailty, closely linked to sarcopenia, is related to hyponatremia, although the mechanism is not well established. Hyponatremia acts as both a causative and a prognostic factor in managing sarcopenia and frailty.[58]
- b.
-
Hyponatremia-Related DeficienciesElectrolyte abnormalities are observed in a considerable percentage of hyponatremic patients independent of the cause of hyponatremia. In one study, more than half of patients with diuretic-induced hyponatremia exhibited at least one additional electrolyte abnormality.[62] Chronic diuretic usage is frequently associated with hyponatremia, which may also be linked to reduced intracellular potassium reserves. In a small group of patients with chronic congestive heart failure, magnesium replacement alone was sufficient to correct this hyponatremia.[63] The most common disorders associated with hyponatremia include hypophosphatemia, hypokalemia, and hypomagnesemia.
- 4.
-
Assessing adequate fluid intake in older adultsThere is no simple or universally accepted method for measuring hydration levels in older adults.[64] For example, HF patients may need to check daily weight, along with daily fluid intake and output, to ensure they are not retaining excess fluid. Similarly, individuals with chronic kidney stones must monitor their hydration levels to prevent stone formation, aiming for a daily urine output of 2.5 liters in adults.
- 5.
-
Broader Risk Factors and Consideration for Hyponatremia in Older AdultsAge-related physiological changes and dietary factors are key to the development of hyponatremia in older adults. Other significant factors that include hydration status, physical activity, chronic disease, socioeconomic status, healthcare coverage, and education levels.[1] Inadequate hydration can lead to hypernatremia, while excessive fluid intake may cause dilutional hyponatremia, especially in individuals with impaired kidney function or HF. It is important for older adults with impaired renal function or those taking medications that affect fluid balance to maintain a balance between fluid intake and sodium levels.[65]
Sedentary behavior can exacerbate sarcopenia, especially in older adults. [66] Regular physical activity, whether mild or moderate, improves circulation and supports kidney function, aiding in sodium and fluid homeostasis.[67] Chronic diseases are more common in this populations and complicate sodium balance. Medications such as diuretics and antihypertensives, often increase sodium loss. Therefore, fluid management becomes challenging for older adults with MCC.
Social determinants of health significantly impact factors that are essential for managing hyponatremia including access to healthcare services, nutritional counseling, and medications. Older adults from lower socioeconomic backgrounds are less likely to have access to preventative healthcare. Limited or no healthcare coverage further complicates the situation and creates barriers to medical care, including medication reconciliation and dietary consultations. This may delay the diagnosis of hyponatremia resulting in worsening complications.[68] Older adults with lower education levels may need help understanding the steps necessary to maintain sodium balance or how medications can affect their levels.[69] Improving health education, access to health care, and providing adequate health coverage, particularly for vulnerable populations, is crucial to ensure the self-management of chronic diseases.
- 6.
- Screening, Diagnosis, and Management of Hyponatremia in Older Adults
Diagnosing hyponatremia in older adults includes a thorough history. History should include an assessment of food and fluid intake, with particular attention to salt intake and any underlying medical conditions that may contribute to sodium imbalances, such as CHF, liver disease, and renal impairment. Hyponatremia is diagnosed by checking serum sodium concentration. Once a diagnosis of hyponatremia is established, the underlying cause is evaluated by testing urine osmolality and other electrolytes.
Management of hyponatremia includes both the treatment of underlying cause and the sodium imbalance itself. Increasing dietary sodium and protein can benefit patients with mild chronic hyponatremia, especially if their diet is low in sodium intake. Correcting nutritional deficiencies in people with protein malnutrition is necessary for restoring sodium balance and supporting overall health.
For patients with dilutional hyponatremia, the treatment is through fluid restriction. This is especially used for management of patients with hyponatremia due to HF and SIADH, where water retention exacerbates sodium dilution.[65] In more severe cases, such as acute symptomatic hyponatremia, careful administration of hypertonic saline may be required under close medical supervision to avoid complications like osmotic demyelination syndrome.
The prevention of hyponatremia in older adults focuses on dietary education and modification. Older adults should be encouraged to maintain a balanced sodium, protein, and fluid intake while avoiding excessive consumption of processed foods high in sodium. Education on the potential effects of medications, such as diuretics and psychotropic drugs that can alter sodium balance is also crucial.[1] Regular monitoring of sodium levels in high risk individuals, such as those with MCC, may help prevent the development of more severe forms of hyponatremia.
3. Results
This review highlights how dietary habits increase the risk of hyponatremia in older adults. Aging impacts sodium regulation due to physiological changes, like reduced GFR and decreased sodium conversation. These age-related changes are linked to an increased prevalence of hyponatremia, particularly in those with comorbidities such as kidney disease and HF. While low sodium intake is beneficial for managing HTN, it may increase the risk of cognitive decline and impair physical function in older adults. There is a J-shaped relationship between sodium levels and health outcomes, where both very high and very low sodium intake can negatively impact health, particularly in those over 80.
The review also shows how inadequate intake of protein and essential nutrients contributes to conditions like sarcopenia and “tea and toast syndrome”, which exacerbate sodium imbalances and increase susceptibility to hyponatremia. Low potassium levels and sarcopenia can both be cause and consequences of chronic hyponatremia. Additionally, increased consumption of ultra-processed foods is associated with higher sodium intake and adverse health outcomes. For older adults, balancing sodium intake to prevent both, hyponatremia and hypernatremia is crucial, especially given the high prevalence of HTN and CVS disease in the population. Lastly, factors such as hydration, physical activity, chronic disease management, and socioeconomic status play significant roles in incidence an management of hyponatremia in older adults.
There is a complex interplay between dietary habits, nutritional deficiencies, and the risk of hyponatremia in older adults. While low sodium intake and specific nutritional deficiencies contribute to vulnerability, factors such as age-related physiological changes and socioeconomic influences further complicate management strategies.
4. Discussion: Recommendations for Managing Hyponatremia in Older Adults
The findings of this review underscore the complex relationship between dietary habits, nutritional deficiencies, and hyponatremia in older adults. The aging process introduces physiological changes-such as decreased GFR and impaired sodium conservation-that make sodium balance challenging to maintain. Coupled with common dietary patterns, like low sodium and protein intake, older adults face an increased risk of hyponatremia, leading to outcomes that range from cognitive impairment to heightened fall risk. These insights relevel the importance of viewing dietary and nutritional factors as integral component in the prevention and management of hyponatremia.
Managing hyponatremia in this population presents unique challenges. Clinicians must carefully balance sodium intake, particularly in older adults with comorbidities, such as HTN, CKD, and frailty. Polypharmacy further complicates the scenario as diuretics and antidepressants exacerbate sodium depletion. These complexities highlight the need for a nuanced approach, one that considers both dietary sodium intake and broader nutritional factors while navigating the risks associated with high sodium intake for cardiovascular health.
Future strategies in managing hyponatremia should focus on targeted dietary interventions. Emphasizing adequate sodium and protein intake, while limiting ultra-processed foods, may help address the nutritional gaps that increase vulnerability to hyponatremia. Educational initiatives tailored to older adults and caregivers could enhance awareness and adherence to sodium balance guidelines, equipping them with practical strategies for dietary adjustments. An interdisciplinary approach, involving dieticians, physician and caregivers, is also essential, supporting personalized care that reflects each patients unique health status and nutritional needs.
Further research is warranted to refine sodium intake guidelines specifically for geriatric populations. Studies investigating optimal sodium thresholds could help balance the risks of both hypertension and hyponatremia, while also examining how dietary modifications impact sodium balance and overall health in frail older adults. As healthcare costs and aging-related challenges continue to grow, preventive care practices that incorporate dietary education and support, may play a crucial role in mitigating the impact of hyponatremia on quality of life and healthcare systems.
5. Conclusions
In conclusion, this review highlights the multifaceted relationship between dietary habits, nutritional deficiencies, and the development of hyponatremia in older adults. We explored how age-related physiological changes, combined with suboptimal sodium and protein intake, elevate the risk of sodium imbalance, leading to adverse health outcomes, including cognitive decline, falls, and increased morbidity. Effective prevention and management strategies must emphasize personalized dietary education and improved nutritional support tailored to this vulnerable population. By addressing these dietary risks and focusing on sodium and protein adequacy, healthcare providers can contribute to better health outcomes, reduce hospitalizations, and improve the quality of life for older adults. Future research should further investigate targeted dietary interventions to refine preventive care practices and support healthier aging in populations at risk of hyponatremia.
Author Contributions
Conceptualization, N.J.; literature search and review, M.A., M.A., N.B.M., S.T.R., D.K., and R.F.; writing—original draft preparation, M.A., M.A., N.B.M., S.T.R., D.K., and R.F..; writing—review and editing, N.J..; All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
Not applicable.
Acknowledgments
Not applicable.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Filippatos TD, Makri A, Elisaf MS, Liamis G. Hyponatremia in the elderly: challenges and solutions. Clin Interv Aging. 2017;12:1957-1965. [CrossRef]
- United Nations DoEaSA, Population Division. World Population Ageing 2019 Highlights. World Population Ageing.
- 2019: Highlights. 2019;ST/ESA/SER.A/430.
- Zhang X, Li XY. Prevalence of hyponatremia among older inpatients in a general hospital. Eur Geriatr Med. Aug 2020;11(4):685-692. [CrossRef]
- Soriano TA, DeCherrie LV, Thomas DC. Falls in the community-dwelling older adult: a review for primary-care providers. Clin Interv Aging. 2007;2(4):545-54. [CrossRef]
- Rondon H, Badireddy M. Hyponatremia. StatPearls. 2022.
- Peri A. Management of hyponatremia: causes, clinical aspects, differential diagnosis and treatment. Expert Rev Endocrinol Metab. Jan 2019;14(1):13-21. [CrossRef]
- Strazzullo P, Leclercq C. Sodium. Adv Nutr. Mar 1 2014;5(2):188-90. [CrossRef]
- Gunathilake R, Oldmeadow C, McEvoy M, et al. Mild hyponatremia is associated with impaired cognition and falls in community-dwelling older persons. J Am Geriatr Soc. Oct 2013;61(10):1838-9. [CrossRef]
- Montero-Odasso M, van der Velde N, Martin FC, et al. World guidelines for falls prevention and management for older adults: a global initiative. Age Ageing. Sep 2 2022;51(9)doi:10.1093/ageing/afac205.
- Upadhyay A, Jaber BL, Madias NE. Epidemiology of hyponatremia. Semin Nephrol. May 2009;29(3):227-38. [CrossRef]
- Soiza RL, Cumming K, Clarke JM, Wood KM, Myint PK. Hyponatremia: Special Considerations in Older Patients. J Clin Med. Aug 18 2014;3(3):944-58. [CrossRef]
- Renneboog B, Sattar L, Decaux G. Attention and postural balance are much more affected in older than in younger adults with mild or moderate chronic hyponatremia. Eur J Intern Med. Jun 2017;41:e25-e26. [CrossRef]
- Renneboog B, Musch W, Vandemergel X, Manto MU, Decaux G. Mild chronic hyponatremia is associated with falls, unsteadiness, and attention deficits. Am J Med. Jan 2006;119(1):71 e1-8. [CrossRef]
- Hoorn EJ, Rivadeneira F, van Meurs JB, et al. Mild hyponatremia as a risk factor for fractures: the Rotterdam Study. J Bone Miner Res. Aug 2011;26(8):1822-8. [CrossRef]
- Hoorn EJ, Liamis G, Zietse R, Zillikens MC. Hyponatremia and bone: an emerging relationship. Nat Rev Endocrinol. Oct 25 2011;8(1):33-9. [CrossRef]
- Gosch M, Joosten-Gstrein B, Heppner HJ, Lechleitner M. Hyponatremia in geriatric inhospital patients: effects on results of a comprehensive geriatric assessment. Gerontology. 2012;58(5):430-40. [CrossRef]
- Verbalis JG, Goldsmith SR, Greenberg A, et al. Diagnosis, evaluation, and treatment of hyponatremia: expert panel recommendations. Am J Med. Oct 2013;126(10 Suppl 1):S1-42. [CrossRef]
- Robinson S, Granic A, Cruz-Jentoft AJ, Sayer AA. The role of nutrition in the prevention of sarcopenia. Am J Clin Nutr. Nov 2023;118(5):852-864. [CrossRef]
- Robinson S, Cooper C, Aihie Sayer A. Nutrition and sarcopenia: a review of the evidence and implications for preventive strategies. J Aging Res. 2012;2012:510801. [CrossRef]
- Shamliyan T, Talley KM, Ramakrishnan R, Kane RL. Association of frailty with survival: a systematic literature review. Ageing Res Rev. Mar 2013;12(2):719-36. [CrossRef]
- McIntire KL, Hoffman AR. The endocrine system and sarcopenia: potential therapeutic benefits. Curr Aging Sci. Dec 2011;4(3):298-305. [CrossRef]
- Jo E, Lee SR, Park BS, Kim JS. Potential mechanisms underlying the role of chronic inflammation in age-related muscle wasting. Aging Clin Exp Res. Oct 2012;24(5):412-22. [CrossRef]
- (WHO) WHO. World Report on Ageing and Health. 2015.
- Lang T, Streeper T, Cawthon P, Baldwin K, Taaffe DR, Harris TB. Sarcopenia: etiology, clinical consequences, intervention, and assessment. Osteoporos Int. Apr 2010;21(4):543-59. [CrossRef]
- Kowal P, Chatterji S, Naidoo N, et al. Data resource profile: the World Health Organization Study on global AGEing and adult health (SAGE). Int J Epidemiol. Dec 2012;41(6):1639-49. [CrossRef]
- Adminstration USFD. Sodium in Your Diet. Accessed 10/10/2024, 2024. https://www.fda.gov/food/nutrition-education-resources-materials/sodium-your-diet.
- Beaudart C, Zaaria M, Pasleau F, Reginster JY, Bruyere O. Health Outcomes of Sarcopenia: A Systematic Review and Meta-Analysis. PLoS One. 2017;12(1):e0169548. [CrossRef]
- Stamler J. The INTERSALT Study: background, methods, findings, and implications. Am J Clin Nutr. Feb 1997;65(2 Suppl):626S-642S. [CrossRef]
- Cook NR. Salt intake, blood pressure and clinical outcomes. Curr Opin Nephrol Hypertens. May 2008;17(3):310-4. [CrossRef]
- Patel SM, Cobb P, Saydah S, Zhang X, de Jesus JM, Cogswell ME. Dietary sodium reduction does not affect circulating glucose concentrations in fasting children or adults: findings from a systematic review and meta-analysis. J Nutr. Mar 2015;145(3):505-13. [CrossRef]
- Grassi G, Dell'Oro R, Seravalle G, Foglia G, Trevano FQ, Mancia G. Short- and long-term neuroadrenergic effects of moderate dietary sodium restriction in essential hypertension. Circulation. Oct 8 2002;106(15):1957-61. [CrossRef]
- Alderman MH, Madhavan S, Ooi WL, Cohen H, Sealey JE, Laragh JH. Association of the renin-sodium profile with the risk of myocardial infarction in patients with hypertension. N Engl J Med. Apr 18 1991;324(16):1098-104. [CrossRef]
- O'Donnell M, Mente A, Rangarajan S, et al. Urinary sodium and potassium excretion, mortality, and cardiovascular events. N Engl J Med. Aug 14 2014;371(7):612-23. [CrossRef]
- Haring B, Wu C, Coker LH, et al. Hypertension, Dietary Sodium, and Cognitive Decline: Results From the Women's Health Initiative Memory Study. Am J Hypertens. Feb 2016;29(2):202-16. [CrossRef]
- Fiocco AJ, Shatenstein B, Ferland G, et al. Sodium intake and physical activity impact cognitive maintenance in older adults: the NuAge Study. Neurobiol Aging. Apr 2012;33(4):829 e21-8. [CrossRef]
- Afsar B. The relationship between cognitive function, depressive behaviour and sleep quality with 24-h urinary sodium excretion in patients with essential hypertension. High Blood Press Cardiovasc Prev. Mar 2013;20(1):19-24. [CrossRef]
- Nakayama M, Tomiyama H, Kuwajima I, et al. Low salt intake and changes in serum sodium levels in the combination therapy of low-dose hydrochlorothiazide and angiotensin II receptor blocker. Circ J. 2013;77(10):2567-72. [CrossRef]
- Park SM, Joung JY, Cho YY, et al. Effect of high dietary sodium on bone turnover markers and urinary calcium excretion in Korean postmenopausal women with low bone mass. Eur J Clin Nutr. Mar 2015;69(3):361-6. [CrossRef]
- Suzuki H, Takenaka T, Kanno Y, Ohno Y, Saruta T. Sodium and kidney disease. Contrib Nephrol. 2007;155:90-101. [CrossRef]
- Kim SW, Jeon JH, Choi YK, et al. Association of urinary sodium/creatinine ratio with bone mineral density in postmenopausal women: KNHANES 2008-2011. Endocrine. Aug 2015;49(3):791-9. [CrossRef]
- Whelton PK, Appel LJ, Sacco RL, et al. Sodium, blood pressure, and cardiovascular disease: further evidence supporting the American Heart Association sodium reduction recommendations. Circulation. Dec 11 2012;126(24):2880-9. [CrossRef]
- O'Donnell M, Mente A, Yusuf S. Sodium intake and cardiovascular health. Circ Res. Mar 13 2015;116(6):1046-57. [CrossRef]
- Zhou X, Perez-Cueto FJA, Santos QD, et al. A Systematic Review of Behavioural Interventions Promoting Healthy Eating among Older People. Nutrients. Jan 26 2018;10(2). [CrossRef]
- Qian Q. Dietary Influence on Body Fluid Acid-Base and Volume Balance: The Deleterious "Norm" Furthers and Cloaks Subclinical Pathophysiology. Nutrients. Jun 16 2018;10(6). [CrossRef]
- Committee DGA. Scientific Report of the 2015 Dietary Guidelines Advisory Committee: Advisory Report to the Secretary of Health and Human Services and the Secretary of Agriculture. 2015.
- Millen BE, Abrams S, Adams-Campbell L, et al. The 2015 Dietary Guidelines Advisory Committee Scientific Report: Development and Major Conclusions. Adv Nutr. May 2016;7(3):438-44. [CrossRef]
- Qian Q. Inflammation: A Key Contributor to the Genesis and Progression of Chronic Kidney Disease. Contrib Nephrol. 2017;191:72-83. [CrossRef]
- Maughan RJ. Impact of mild dehydration on wellness and on exercise performance. Eur J Clin Nutr. Dec 2003;57 Suppl 2:S19-23. [CrossRef]
- Siener R, Hesse A. Fluid intake and epidemiology of urolithiasis. Eur J Clin Nutr. Dec 2003;57 Suppl 2:S47-51. [CrossRef]
- Wang CJ, Grantham JJ, Wetmore JB. The medicinal use of water in renal disease. Kidney Int. Jul 2013;84(1):45-53. [CrossRef]
- Thornton SN. Increased Hydration Can Be Associated with Weight Loss. Front Nutr. 2016;3:18. [CrossRef]
- Leenders M, Boshuizen HC, Ferrari P, et al. Fruit and vegetable intake and cause-specific mortality in the EPIC study. Eur J Epidemiol. Sep 2014;29(9):639-52. [CrossRef]
- Nguyen B, Bauman A, Gale J, Banks E, Kritharides L, Ding D. Fruit and vegetable consumption and all-cause mortality: evidence from a large Australian cohort study. Int J Behav Nutr Phys Act. Jan 25 2016;13:9. [CrossRef]
- Schwingshackl L, Schwedhelm C, Hoffmann G, et al. Food Groups and Risk of Hypertension: A Systematic Review and Dose-Response Meta-Analysis of Prospective Studies. Adv Nutr. Nov 2017;8(6):793-803. [CrossRef]
- Wang X, Ouyang Y, Liu J, et al. Fruit and vegetable consumption and mortality from all causes, cardiovascular disease, and cancer: systematic review and dose-response meta-analysis of prospective cohort studies. BMJ. Jul 29 2014;349:g4490. [CrossRef]
- Aaron KJ, Sanders PW. Role of dietary salt and potassium intake in cardiovascular health and disease: a review of the evidence. Mayo Clin Proc. Sep 2013;88(9):987-95. [CrossRef]
- Cruz-Jentoft AJ, Bahat G, Bauer J, et al. Sarcopenia: revised European consensus on definition and diagnosis. Age Ageing. Jul 1 2019;48(4):601. [CrossRef]
- Karakousis ND, Kostakopoulos NA. Hyponatremia in the frail. J Frailty Sarcopenia Falls. Dec 2021;6(4):241-245. [CrossRef]
- Walston JD. Sarcopenia in older adults. Curr Opin Rheumatol. Nov 2012;24(6):623-7. [CrossRef]
- Bertini V, Nicoletti C, Beker BM, Musso CG. Sarcopenia as a potential cause of chronic hyponatremia in the elderly. Med Hypotheses. Jun 2019;127:46-48. [CrossRef]
- Fujisawa C, Umegaki H, Sugimoto T, et al. Mild hyponatremia is associated with low skeletal muscle mass, physical function impairment, and depressive mood in the elderly. BMC Geriatr. Jan 6 2021;21(1):15. [CrossRef]
- Liamis G, Mitrogianni Z, Liberopoulos EN, Tsimihodimos V, Elisaf M. Electrolyte disturbances in patients with hyponatremia. Intern Med. 2007;46(11):685-90. [CrossRef]
- Solomon R. The relationship between disorders of K+ and Mg+ homeostasis. Semin Nephrol. Sep 1987;7(3):253-62.
- Cohen R, Fernie G, Roshan Fekr A. Fluid Intake Monitoring Systems for the Elderly: A Review of the Literature. Nutrients. Jun 19 2021;13(6). [CrossRef]
- Verbalis JG. Managing hyponatremia in patients with syndrome of inappropriate antidiuretic hormone secretion. J Hosp Med. Jul-Aug 2010;5 Suppl 3:S18-26. [CrossRef]
- Mo Y, Zhou Y, Chan H, Evans C, Maddocks M. The association between sedentary behaviour and sarcopenia in older adults: a systematic review and meta-analysis. BMC Geriatr. Dec 20 2023;23(1):877. [CrossRef]
- Costanti-Nascimento AC B-AL, Bragança-Jardim E, Pereira WO, Camara NOS, Amano MT. Physical exercise as a friend not a foe in acute kidney diseases through immune system modulation. Front Immunol. 2023;14(octo 20). [CrossRef] [PubMed] [PubMed Central]
- McMaughan DJ, Oloruntoba O, Smith ML. Socioeconomic Status and Access to Healthcare: Interrelated Drivers for Healthy Aging. Front Public Health. 2020;8:231. [CrossRef]
- Chesser AK, Keene Woods N, Smothers K, Rogers N. Health Literacy and Older Adults: A Systematic Review. Gerontol Geriatr Med. Jan-Dec 2016;2:2333721416630492. [CrossRef]
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



