
Submitted:
15 November 2024
Posted:
18 November 2024
You are already at the latest version
Abstract
In quiet standing the central nervous system implements a pre-programmed ankle strategy of postural control to maintain upright balance and stability. This strategy comprises a synchronized common neural drive delivered to synergistically grouped muscles. This study evaluated connectivity between EMG signals of unilateral and bilateral homologous muscle pairs of the lower legs during various standing balance conditions using magnitude squared coherence (MSC). The leg muscles examined included the right and left tibialis anterior (TA), medial gastrocnemius (MG), and soleus (S). MSC is a frequency domain measure that quantifies the linear phase relation between two signals and was analyzed in the alpha (8 – 13 Hz), beta (13 – 30 Hz), and gamma (30 – 100 Hz) neural frequency bands for feet together and feet tandem, with eyes open and eyes closed conditions. Results showed that connectivity in the beta, and lower and upper gamma bands (30 – 100 Hz) was influenced by standing balance conditions and indicative of a neural drive originating from the motor cortex. Instability was evaluated by comparing less stable standing conditions with a baseline - eyes open feet together stance. Changes in connectivity in the beta and gamma bands were found to be most significant in the muscle pairs of the back leg during tandem stance regardless of dominant foot placement. MSC identified the MG:S muscle pair as significant for the right and left leg. The results of this study provided insight into the neural mechanism of postural control.
Keywords:
postural control
; balance
; ankle strategy
; common neural drive
; magnitude squared coherence
1. Introduction
The evolution of the human bipedal stance and the ability to maintain standing balance during activities of daily living were simultaneous. The standing posture of humans is characterized by a narrow base of support, a higher location of the center of mass, and a propensity for biomechanical instability. Functional decline with age increases postural sway [1,2]. Furthermore, elderly individuals and patients with neurological and musculoskeletal disorders have demonstrated poor balance control [3,4,5,6] and have a high fall risk [7,8,9,10,11]. Therefore, to prevent falls, the biomechanics and neural control of quiet standing balance in healthy young and elderly adults and individuals with disease, e.g., neuropathology, needs to be clarified.
The central nervous system (CNS) is complex [12] and must facilitate the integration of visual, vestibular, and somatosensory information to coordinate muscle actions associated with static postures and dynamic movements. However, the musculoskeletal system comprises approximately 700 muscles crossing over 300 joints. To generate movement individual muscles are activated via the coordination of thousands of individual motor units (MU) through their motor pools. Thus, to achieve specific behavioral goals through muscle action redundancy creates a degree of freedom (DoF) problem [13,14]. This redundancy problem arises from a large number of possible muscle combinations that could be recruited, i.e., coordinated patterns, to accomplish an identical postural or movement goal. Therefore, a one-to-one correspondence between a specific movement task and its solution pattern cannot exist. Bernstein's [13] hierarchical control theory suggested that the CNS implemented specific functional control structures to limit the DoF at four levels: muscle tone, muscle synergies, space, and actions [13,15]. The organization of these synergies appears to be dictated by the constraints presented at higher levels of environmental space and desired actions [15]. The neural mechanisms that organize and control human standing posture and movement have not been entirely elucidated.
In the motor control literature, the term synergy often refers to conceptually different processes that potentially operate in parallel across different levels but within Bernstein’s framework of flexible hierarchical control [15]. The simplest definition of muscle synergies (the definition we will assume) is groups of muscles that act together to complete a similar act or function. The notion that muscle synergies are described as functional “structures” that contain the minimal number of muscles needed to generate a movement and accomplish a behavioral goal is a hallmark of neurophysiological approaches to explain coordinated movement. These neurophysiological approaches presume that muscle synergies result in the translation of task-level neural commands into execution-level muscle activation patterns as the “solution” to the DoF problem [16]. Latash et al. [16] suggested that Bernstein’s view that the “elimination of redundant DoF” was the central issue of motor control [13] misrepresented the value of motor variability, and offered an alternative view of muscle synergies. Thus, if an element, i.e., muscle, introduced an error into the common output, other elements would change their contributions to minimize the original error; systems that function according to that principle and demonstrate error compensation among the elements would be called synergies. This notion of compensatory elements was referred to as the “principle of abundance”, which suggests that all the elements (DoFs) always participate in all the tasks, assuring both stability and flexibility, i.e., variability, of the performance; in essence, rendering the redundancy problem irrelevant [16,17].
Latash et al.’s [16] departure from the traditional view of synergy as the correlation of coupling among individual motor elements led to a redefinition of synergies as “neural organizations that ensure task-specific covariation of elemental variable providing for the desired stability properties of an important output (performance variable)” [18]. This departure contributed to the uncontrolled manifold hypothesis, which assumes that, when a controller of a multi-element system, e.g., CNS, wants to stabilize a particular value of a performance variable, it selects a subspace within the state space of the elements such that, within the subspace, the desired value of the variable is constant. This subspace is the uncontrolled manifold (UCM) [16]. Within the manifold, the elements are not individually controlled and are free to vary within the bounds of the performance parameter, which resolves the need to control the DoF. In this case, the CNS “allows” multiple movement options within an acceptable range of end effector output; work in the UCM context emphasizes end-point control. Krishnamoorthy et al. [19,20], applied the UCM concept to examine the hypothesis that shifts in the center of pressure (COP) during multiple standing tasks in young adults were controlled, i.e., stabilized, using a small subset of central variables (muscle modes or M-modes). Electromyographic activity and principal component analysis of 11 postural muscles (tibialis anterior, medial and lateral gastrocnemius, soleus, vastus medialis and lateralis, rectus and biceps femoris, semitendinosus, rectus abdominis, and erector spinae), found three principal components that were associated with a push back M-mode, a push forward M-mode, and a mixed M-mode, i.e., synergies. Each M-mode had a distinctive set of muscle groups associated with changes in muscle activity in reaction to postural sway, i.e., shifts in the COP.
In attempts to elucidate the role muscle synergies might play in addressing the DoF problem several different approaches have been used. Krishnamoorthy et al. [19] used integrated electromyography (EMG) of several postural muscles and principal component analysis (PCA) to define muscle (or M) modes. Torres-Oviedo and Ting [21] used non-negative matrix factorization to identify muscle synergies related to human postural control to examine the intra- and inter-trial variation, while Boonstra et al. [22] decomposed EMG envelopes from ten leg muscles using non-negative matrix factorization (NNMF) and PCA to estimate the number muscle synergies during a variety of standing activities. Others have used muscle EMG data as input for event-driven intermittent feedback control [23] or neuromechanical [24] models.
In the last three decades, efforts to understand how the CNS controls synergistic muscle activity have focused on examining the role of common neural drives that synchronously activate motor pools of individual muscles in a functional synergy as a single unit at various frequencies [25,26,27,28,29,30,31]. The assumption driving these works is based on the principle that neural oscillations are synchronized by the CNS to achieve large-scale integration among cortical and subcortical components that control the recruitment of muscles, i.e., agonists and antagonists, to optimize performance. A common neural drive that simultaneously activates multiple motor pools also synchronizes their firing rate [32]. The frequency ranges associated with neural drive oscillations indicate their signal origin in the CNS [26], as shown in Table 1.1.1. The strength of neural synchronization from these frequency bands is identified through connectivity analysis, i.e., EMG-EMG coherence (magnitude square coherence). Methods using corticomuscular coherence (CMC) and intermuscular coherence (IMC) have been used to investigate common input to groups of muscles related to quiet bipedal standing [33,34], ballet postures [35], squatting [36], heel rise tasks [37], as well as sitting and standing tasks in patients with Parkinson’s disease [38]. The ensuing extended background and related review will focus on IMC related to investigations on human balance during quiet bipedal standing.
1.1. Extended Background
Human balance refers to a state of equilibrium where the center of pressure (COP) oscillates about the body’s center of mass (COM) that lies within a base of support (BOS) to prevent a fall [39,40,41,42,43,44,45]. Stability is the inherent ability to achieve, maintain, and/or restore a balanced state to avoid a fall [44]. Generally, the body becomes unstable and unbalanced if the COM is displaced outside the BOS; although we acknowledge that during locomotion the COM routinely falls outside of the BOS. Notably, the COP is directly related to foot placement or orientation. When one foot is in contact with the standing surface the net COP is below that foot. When both feet are in contact the net COP is between the two feet and each foot has its COP weight distribution [40]. Posture describes the orientation of the multi-segmental human body relative to gravity [40]. Note that balance and posture are often used interchangeably and in combination to assess and define the stability/instability of normal healthy humans.
Due to a relatively large COM located at two-thirds of the body height above ground, humans are inherently unstable bipeds that need a continuously acting control system to maintain balance and stability [40,46]. The postural control system consists of complex motor skills coordinated by the CNS that integrate the interaction of multiple sensorimotor processes [44]. The failure of this system results in the loss of balance, i.e., instability, which may lead to a fall. The exact mechanism of how the CNS coordinates and regulates postural control is still relatively unknown, as previously alluded to.
Postural control is a learned complex motor skill organized hierarchically by the CNS that constantly adapts and manages the interaction of multiple sensorimotor processes, e.g., visual, vestibular, and somatosensory, derived from an individual’s expectations, goals, cognitive factors, and prior experiences [45]. The main function of postural control is to promote postural orientation and equilibrium of the multi-segmented musculoskeletal system by implementing anticipatory and/or compensatory control strategies [46,47]. Postural orientation involves active control of the body’s center of mass relative to gravity, the support surface, the sensory environment, and internal references, while postural equilibrium refers to the coordination of sensorimotor strategies used to stabilize the body’s COM during internally and externally triggered perturbations to balance [46] (Figure 1.1).
The model in Figure 1.1 illustrates the compensatory and anticipatory strategies that are implemented following unpredictable or predictable perturbations, respectively. Internal perturbations are caused by voluntary movement where specific limbs are moved, whereas external perturbations result from unexpected changes to the sensory environment. During these movements, neighboring skeletal segments may become displaced, affecting overall balance [46,47]. The anticipatory movement strategy implements a feedforward control mechanism, in advance, that predicts the degree of compensation, i.e., adaptation, needed to maintain stability before voluntary movements.
The visual, vestibular, and somatosensory systems work together continuously to reweigh sensory input and actively manage the control system to combat changes in the sensory environment [13,46]. The ability to re-weigh sensory information depending on the sensory context is important for maintaining balance equilibrium relative to the present sensory environment [46]. The effects of external perturbations become predictable after repeated implementation of protective actions; when this happens the compensatory strategy becomes a new anticipatory strategy. Two common “fixed-support” strategies include the ankle and hip strategies. For example, to maintain balance from internal or small external perturbations when standing on a firm surface, the ankle plantar/dorsiflexor muscles are recruited (Table 1.2). If the COM shifts significantly, and the ankle strategy is unable to provide adequate compensation, the hip strategy is used to flex or extend the hip in an effort to realign the COM within the BOS [40.47]. If both the ankle and hip strategies are inadequate, a “change-in-support” strategy is employed as the individual takes a step to restore balance.
Cognitive, sensory, or motor impairments related to aging, injury, neurological disease, and traumatic brain injury create deficits in postural control. Identifying the musculoskeletal, neurological, and pathophysiological changes related to disease is central to understanding the causes and consequences of balance disorders and, thus, their management [47]. Studying balance in healthy and elderly or impaired individuals has provided a significant understanding of the postural control system and its impairments [22,38,48,49,50].
Maintaining a quiet, upright bipedal stance is a fundamental activity of daily living. The single inverted pendulum (SIP) biomechanical model has been accepted as a suitable model to quantify the angle strategy present during the maintenance of balance, i.e., controlling the continuous oscillation of the COP around the COM (postural sway) during quiet standing [39,40,41,42,43,51]. Although passive ankle stiffness has been identified as an important factor in the control of quiet stance [41], others have suggested that ankle stiffness was insufficient [52,53]. Thus, it appears that the ankle strategy for controlling a quiet stance may depend primarily on ankle musculature. Notably, Winter et al. [40,41] demonstrated that in tandem stance, as opposed to normal bipedal standing, the ankle invertors/evertors and hip abductors/adductors were prominent in controlling postural sway. Despite validation of the SIP, several studies have suggested that stabilization of quiet stance is complex, cannot be explained wholly by the SIP model, and is associated with accelerations and moments at both the knee and hip joints [54,55,56,57,58,59,60,61,62]. Despite these challenges, Morasso et al. [63] have shown that although the single inverted pendulum model may be “literally” false because it does not account for ankle-hip coordination, it is functionally correct and pragmatically acceptable for experimental studies that focus on the postural oscillations of the center of mass.
The single inverted pendulum model validation and precision has been widely accepted by the biomechanics community and used extensively as a framework for measuring postural sway in both the antero-posterior (A/P) and medio-lateral (M/L) directions to study the balance of persons with and without musculoskeletal and neurological impairments. Postural sway refers to the involuntary oscillations of the human body during quiet stance as measured by movements of the COP around the COM. The location of the COP under each foot, with respect to foot orientation, is a direct reflection of the neural mechanisms of postural control [40]. Previous research on quiet bipedal stance has generally focused on determining and examining a variety of metrics related to the COP, e.g., oscillations in the A/P and M/L directions, that might provide insight into postural control [64]. Winter et al. [41,42], whose work has been corroborated by others [21,49,51,65], demonstrated that the ankle dorsi- and plantarflexors partially controlled the A/P oscillations of the COP while loading/unloading at the hip joint controlled M/L oscillations. Other investigators examined COP metrics, as well as selected lower leg muscle electromyographic (EMG) activity when individuals stood with feet staggered or in tandem [41,66,67,68,69,70,71,72,73,74]. A summary of the results from studies investigating quiet tandem stances demonstrated that, as opposed to bipedal quiet stance, tandem standing led to 1) an increase in the COP A/P and M/L excursions, and these tended to be greater in eyes-closed (EC) compared to eyes-open (EO) conditions, 2) greater intra- and intertrial (between individuals) variability in COP excursion; less so with EO, 3) a greater vertical ground reaction force associated with the rear foot, 4) greater EMG activity in the tibialis anterior (TA), peroneus longus (PL), and soleus (Sol), in general, but greater yet in the rear limb for TA and Sol, 5) greater EMG activity with EC and with an increase in M/L excursion, except for Sol, which was tonically active regardless of changes in COP oscillations, 6) greater cross-correlation of TA and PL, than Sol, with M/L oscillations, and 7) the EMG of homonymous muscles of the two legs were out-of-phase, which suggests a mutual push-pull action of the muscle pairs. These data suggest that: i) despite large inter-trial and inter-participant variability, the neural commands to the leg muscles during tandem stance imply a task-sharing rule, whereby the Sol keeps the body upright while the back-and-forth activity of the TA and PL controls the COM in the frontal plane, ii) the asymmetry of the mechanical constraints on the feet as a function of stance organize coordination patterns of feet COPs while the degree of adaptive variation between the feet COPs is dependent on both mechanical and vision constraints, and iii) asymmetrical loading under each foot may result in different joint compliance properties, i.e., inherent stiffness, that in turn influence the fluctuations of the individual feet COPs and the net COP. This information is valuable because it provides insight into the normal functioning and control of normal quiet balance, and provides valid and reliable methods that can be used to assess individuals with musculoskeletal and neurological impairments.
As a signal of a train of motor unit action potentials (MUAP) that represents a muscle’s response elicited from a neural drive, the shape and firing rate of MUAPs in the EMG signal can potentially provide valuable information about how the CNS coordinates muscle activation, i.e., muscle synergies. As demonstrated in the tandem stance research just reviewed, increased MUAP recruitment is directly related to increased EMG magnitude. Therefore, a distinct relationship between muscle activation and CNS control must exist that would allow for the indirect extraction of synaptic input signals received by motor neurons from EMG signals. Connectivity analysis methods, such as corticomuscular (CMC) and intermuscular (IMC) coherence take advantage of the indirect measure of neural drive within the EMG signals [30,75,76]. The existence of synchronous neural drives can be deduced from comparing IMC between various EMG signals of specific muscles within a functional unit, i.e., synergists. Therefore, the EMG signals of postural control muscles that control quiet bipedal stances could provide valuable insight into how the CNS may synchronize and regulate motor control [77].
Coherence analysis quantifies the strength of the common oscillation between two signals; thus, EMG-EMG coherence quantifies the common oscillatory inputs to the motor neurons in a frequency band [28]. EMG-EMG coherence is estimated from the auto-and cross-spectra of the EMG signals x and y (, , and ) as [26].
As noted earlier (Table 1.1), muscular coherence in each frequency band is generated by various brain areas, i.e., spinal, subcortical, and cortical, thus, IMC can theoretically provide estimates of the neural origin and interconnections that contribute to functional motor tasks.
Numerous studies have used IMC analysis to identify synchronization and common neural drive to various postural muscles during a variety of quiet standing tasks in young healthy adults [22,32,33,34,48,49,65,79,80,81,82,83,84,85,86,87]. Most studies [22,33,34,48,49,65,81,82,83,84,85] examined common tasks such as quiet bipedal standing; one implemented unipedal [81] or bipedal standing with eyes closed [49,65,80,82], and compared with natural bipedal standing. Other standing tasks included shifting the center of pressure within the base of support [78], dual tasks and standing at a height [22], and tandem stance [83,86,87]. In general, EMG-EMG coherence increased as the base of support narrowed, e.g., unipedal and tandem standing, and the difficulty in standing increased [83,84,86,87]. Significant coherence was observed primarily in the delta band, regardless of the muscle pair [65,79,86], which is thought to reflect synchronous activity of the motor neuron pool [88]. Notably, beta band coherence, which is thought to reflect activity in the corticospinal tract [26,28], i.e., control from the cortex, varied with the complexity of the standing tasks. Since significant beta band coherence was demonstrated in standing tasks characterized by a narrow base of support [83,86,87], cortical control of standing may increase as the difficulty of the standing task increases. Two studies reported increased coherence during eyes-closed conditions [48,80,86], while others reported no change [65] or the opposite effect [48]. Two studies [48,81] investigated muscle pairs across joints according to M-mode components. The delta band was the most common frequency band of interest for coherence analysis, although many studies also examined alpha, beta, and gamma bands. Yet, the specific frequency band values were researcher-dependent. Most studies selected 0-5 Hz for the coherence analysis of the delta band, and approximately 50% of the studies chose 15-35 Hz for the beta band [77].
Several other studies compared intermuscular coherence analysis of quiet standing tasks between young and elderly healthy adults [50,80,89,90,91,92,93,94]. Significant differences were noted between the young and elderly. For example, Obata et al [80] reported a significant coherence of 0-4 Hz for both groups in bilateral and unilateral plantarflexors, while a coherence of 8-12 Hz was found only for the elderly group in bilateral muscle pairs. Watanabe et al [92] also found that during bipedal standing, the delta band coherence of the plantarflexor pairs was greater in elderly adults and that the delta band coherence was greater in unipedal than in bipedal stance for both age groups, but greater in elders compared to younger adults. Degani et al [90] determined the IMC of synergistic muscle groups and found that young adults presented with significant coherence in the 0-5 Hz frequency band in the soleus and biceps femoris pair, whereas the older adults presented with coherence in the 0-10 Hz frequency range. These studies have also clearly shown that EMG-EMG coherence was related to increased postural sway during standing in elders and that older adults appeared to selectively increase the corticospinal drive to lower leg muscles to cope with increased postural sway.
Determining biomechanical metrics related to bipedal quiet standing, i.e., A/P and M/L excursions of the center of pressure, has been successful in describing control of the body’s center of mass relative to its base of support. A significant amount of that work included the description and analysis of lower leg muscle electromyography in examining both natural and tandem standing postures. In the past two decades, the use of intermuscular coherence has been used extensively in attempts to clarify neural mechanisms related to postural control of quiet stance in young and elderly healthy adults. Most of these studies focused their analysis on normal bipedal standing postures, but only two examined the EMG-EMG coherence of paired lower leg muscles during tandem standing. This study’s goal was to extend the work of Nandi et al. and Ohja et al. [83,86]. Therefore, the primary purpose of this study was to examine how the functional connectivity of lower leg muscle pairs would change during increased levels of standing postural instability. It has been shown that muscle pairs in the rear leg demonstrate greater connectivity, however, the role of the dominant leg has not been examined. Therefore, secondarily, we assessed the role of the dominant leg in maintaining tandem standing balance. Investigating functional connectivity using magnitude square coherence may add valuable insight to existing hypotheses of neural mechanisms related to the maintenance of balance and the postural control system mediated by integrated somatic neuromuscular systems.
2. Materials and Methods
2.1. Participants
Eight healthy young adults (age: 24.8 ± 3.3 years; height 171.0 ± 10.5 cm; body mass: 71.0 ± 13.5 kg) volunteered following informed consent. However, only six individuals (2 males and 4 females), aged 18 – 34, and of varying physical activity levels, were included in the final data analysis; data from two individuals was corrupted and were not included in the final analysis. All participants were considered healthy without a history of neurological or muscular disorders or recent previous injuries. Before data collection commenced, leg/foot dominance for each participant was determined based on the leg with which they preferred to kick a ball. A follow-up task of standing on one leg was implemented for participants who were unable to determine a preference from the previously asked questions. Three participants were right-leg and three left-leg dominant. The Human Research Review Committee approved this study, Institutional Review Board, Office of Research Compliance and Integrity, at Grand Valley State University (18-246-H).
2.2. Experimental Protocol
Participants completed five 30-second trials of six different balancing conditions (Table 2.1) starting with eyes open, feet together (EOFT) to quantify a stable baseline to compare to other balance conditions. A 30-second break was implemented between trials and a 2-minute break between each condition. Test conditions were not randomly ordered but were completed in the order they were listed across all participants. Balance tasks were performed barefoot, and arms were positioned with the shoulders flexed slightly and elbows fully flexed so that the index finger pointed towards the ipsilateral shoulders.
2.3. Data Acquisition
Surface electromyographic (EMG) signals (1200 Hz), motion trajectories (120 Hz), and ground reaction forces (1200 Hz; Advanced Mechanical Technology Inc., Watertown, MA) were synchronized using Vicon NEXUS motion capture software v2.8 (Oxford Metrics, Oxford, UK). Only EMG data were used for analysis in this study.
Electrical activity was recorded from the left (L) and right (R) tibialis anterior (TA), medial gastrocnemius (MG), and soleus (S) muscles [95]. These muscles were chosen because of their prominent role in standing postural control [39,40,43]. Before the application of the surface electrodes, the skin of the lower legs was shaved to remove excessive hair and cleaned with rubbing alcohol. Electrodes were secured to the skin with hypoallergenic tape and circumferentially secured using sports prewrap tape. Electrodes (interelectrode distance of 17 mm) were placed parallel to muscle fiber direction by the primary researcher according to SENIAM recommendations [96], and supervised by the laboratory research director with 20 years of experience. Accurate electrode placement was verified by performing manual muscle tests for each muscle. The reference, i.e., ground, electrode was secured to the patella on one of the lower extremities.
The MA-411 pre-amplifiers (double differential with Common Mode Rejection Ratio > 100 dB at 65 Hz, noise < 1.2 µV, and input impedance > 100,000 MΩ) were used to record data which incorporates both radio frequency interference filters and electrostatic discharge protection circuity that helps to eliminate motion artifacts and cable noise, providing the most reliable EMG signal (Motion Lab Systems Inc., Baton Rouge, LA). The pre-amplifiers were interfaced with the MA300-XVI EMG patient unit acquisition system. The patient unit of the MA-411 implemented a 500 Hz low-pass anti-aliasing filter on the raw EMG before transmitting it to the desktop unit where the signal was further filtered with a 10 Hz high-pass filter. All recorded EMG signals were analyzed in the frequency domain using MATLAB R2018a (The MathWorks, Natick, MA) for the following neural frequency bands (Table 2.2) and muscle pairs (Table 2.3) to observe the presence of synchronized correlated neural drives.
2.4. Data Analysis
MATLAB’s Welch’s power spectral density (PSD) estimator was used to visually analyze the frequency content of the raw 30-second EMG data collected for baseline condition, for all muscles, and each subject to identify any noise artifacts. A 60 Hz 2nd-order Butterworth notch filter with a 0.2 Hz bandwidth was used to remove the powerline interference at 60 Hz.
Magnitude squared coherence (MSC) measures the linearity of the phase relation between two signals x and y in the frequency domain defined by
is MSC, is the cross-spectrum power and and are the auto-spectrums of input signals x and y at frequency f. MSC values range between 0 and 1, where 0 indicates no linear relationship and 1 is a perfect linear relationship. The use of intermuscular, EMG-EMG, coherence provides insight into the connectivity between EMG signals of neighboring leg muscles.
MSC was calculated from MATLAB’s built-in MSC function that estimates using Welch’s overlapped periodogram method. The MSC spectrum was estimated for the whole 30 seconds of all filtered EMG data for each muscle pair listed in Table 2.1 across the neural frequency range (0 – 100 Hz) for each standing condition, and each subject. Magnitude squared coherence was estimated from a two-second Hamming window, with a 25% overlap. This created 19 window segments of 2400 data points and a frequency resolution of 0.5 Hz. Each neural frequency range was averaged across its MSC spectrum to generate a singular coherence value for that range. The functional block diagram for data and statistical analysis is illustrated in Figure 2.1.
2.5. Statistical Analysis
Statistical analysis and graphics were performed with R Statistical Software (v4.4.0; R Core Team 2024) [97] running in RStudio: Integrated Development Environment for R [98]. Raw data for each set of five independent trials across the six test conditions within the nine muscle pairs and six frequency bands for each participant was examined for the magnitude and variation of coherence measurements. We noted that the 10 Hz high-pass filter masked significant EMG-EMG coherence in the delta and theta frequency bands so these data were dropped from the main analysis. Based on observations of the full data set, we also determined that data from two muscle pair groups would not be included in our final analyses due to insufficient EMG connectivity. The resulting charts of five independent trials across the six test conditions within the seven muscle pairs and four frequency bands for each of the six subjects are included in the Appendix A, with only participant #3 (PO3) data included in section 3.1 (Figure 3.3.1). A single graphic (Figure 3.3.1) with all data from this reduced set of data was generated to help visualize inter-trial and inter-participant variation. Analysis was done on 168 sets of thirty coherence values from the six conditions and five independent trials within each participant, frequency band, and muscle group. The primary goal of the analysis was to determine under what conditions the mean coherence differed from the baseline EOFT condition. This implied the use of a Dunnett's test. Assumptions of normality (Shapiro tests) and homogeneity of variance (Levene's test) were performed on each data set with failures of assumptions graphed using Q-Q plots and boxplots. Given the exploratory nature of this study and the mild nature of deviations from the statistical assumptions, we chose to apply parametric methods without transformation for simplicity. Dunnett's test results are summarized graphically with an array of 95% Dunnett's confidence interval charts (Figures 3.2.1 to 3.2.6) each showing the interval for the mean difference between the less stable condition (ECFT, EOTanDB, ECTanDB, EOTanDF, and ECTanDF) and the baseline EOFT condition, i.e., the interval for the increase in coherence for each of the less stable conditions. Intervals associated with a significant (p-value < 0.05) are colored blue. Note: ANOVA F-tests were performed but rejected too frequently, i.e., a significant F-test often did not result in any significant Dunnett's intervals. This is because the F-test looks at all possible pairs of conditions, not just the five comparisons of interest but all 15 possible combinations.
3. Results
3.1. Overview of EMG-EMG Muscular Coherence Across Participants
After reviewing the magnitude squared coherence for each muscle pair and all participants across the test conditions and frequency bands we decided to focus the analysis on only the alpha, beta, lower gamma, and upper gamma frequency bands. We eliminated analysis of the delta and theta frequency bands because we believed that the default low- and high-pass filters built into the EMG pre-amplifiers resulted in the loss of meaningful data. Moreover, the left medial gastrocnemius: right medial gastrocnemius and left soleus: right soleus muscle pair MSC data were not part of our final analysis. This section will present an overview of the muscular coherence patterns across participants, based on our observations of the results. Because of the variability of the muscular coherence data (details to be discussed in subsection 3.3), we cannot illustrate overall patterns from a representative participant. However, we will provide the muscular coherence data from Participant #3 to assist the reader in their review of all participant data that can be found in the Appendix A.
The qualitative-based analysis noted the following EMG-EMG muscular coherence patterns (Figure 3.1.1):
- Consistently greater coherence between muscle pairs in the tandem stance postures compared to the feet together stance postures
- Consistently greater coherence in the LMG: LS and RMG: RS muscle pairs across the beta, lower gamma, and upper gamma frequency bands for tandem stance postures in both eyes open and closed conditions, without discernable differences between eyes open and eyes closed
- Demonstrable evidence of coherence between antagonistic muscle pairs, e.g., LTA: LS, primarily in the tandem stance postures.
3.2. Comparison of EMG-EMG Muscular Coherence Across Conditions
The primary purpose of this project was to examine whether muscular coherence differed between a baseline standing posture (EOFT) and less stable standing postures, e.g., tandem standing postures with eyes open and closed. A Dunnett's inferential analysis demonstrated selected significant differences in muscular coherence between more and less stable standing postures across select muscle pairs and test conditions. In this section, we will present data from all six participants and summarize our major findings.
For Participant #1 there was a consistent difference between tandem standing (dominant leg back) and the baseline condition with greater coherence for the RMG: RS muscle pair across all frequency bands. Surprisingly, greater coherence for the LMG: LS muscle pair was only evident for a couple of test conditions in the lower and upper gamma frequency bands (Figure 3.2.1).
Participant #2 demonstrated different patterns. For instance, 1) there were no differences in coherence in the alpha frequency band, 2) greater coherence in less stable standing postures for LTA: LS muscle pair was seen in the beta band, and 3) a mix of greater and lesser coherence in less stable standing postures for the RTA: RMG and RTA: RS in the beta and lower and upper gamma bands. However, no differences in coherence in the LMG: LS and RMG: RS muscle pairs in the less stable postures as we saw for P01 (Figure 3.2.2).
For Participants #3 (Figure 3.2.3) and #4 (Figure 3.2.4) we observed significant differences in coherence between the less stable standing postures and the baseline for six muscle pairs, primarily in the beta, lower gamma, and upper gamma frequency bands. Unlike P01, which demonstrated greater coherence in both the LMG: LS and RMG: RS muscle pairs, P03 showed less coherence in the LMG: LS muscle pair but greater coherence in the RMG: RS muscle pair. P04, however, showed inconsistent coherence differences in the LMG: LS muscle pair, in comparison to P03. Both P03 and P04 consistently showed greater coherence in the LTA: LMG, LTA: LS, RTA: RS, and LTA: RTA muscle pairs in the beta and lower and upper gamma frequency bands.
Participant #5 (Figure 3.2.5) and #6 (Figure 3.2.6) were similar to P01 in demonstrating greater coherence primarily in the LMG: LS and RMG: RS muscle pairs for less stable standing postures across all frequency bands. P05 showed reduced coherence only for the RTA: RMG muscle pair in tandem standing in the beta band, whereas P06 showed reduced coherence for the same muscle pair in the beta and lower and upper gamma bands. Participant #6 was distinguished from P05 in that there was a trend toward greater coherence in the LTA: RTA muscle pair in less stable standing postures in the beta and lower and upper gamma bands.
In summary, from subsections 3.1 and 3.2: 1) generally, there appear to be notable differences between the six participants in terms of how the coherence of muscle pairs changed in the tandem, i.e., less stable, standing postures, 2) muscular coherence significantly increased in selected muscle pairs in the tandem standing postures, 3) the most common muscle pairs affected by the tandem standing postures were LMG: LS and RMG: RS, 4) muscular coherence between antagonistic muscles, e.g., LTA: LS, during the tandem standing tasks suggests a more complex motor control pattern during less stable standing postures, 5) there did not appear to be differences in changed muscular coherence in the tandem eyes open and eyes closed conditions, and 6) changed muscular coherence in muscles pairs did not appear to be different when the dominant leg was placed on the rear or front forceplate.
3.3. Intertrial and Intersubject EMG-EMG Muscular Coherence Variability
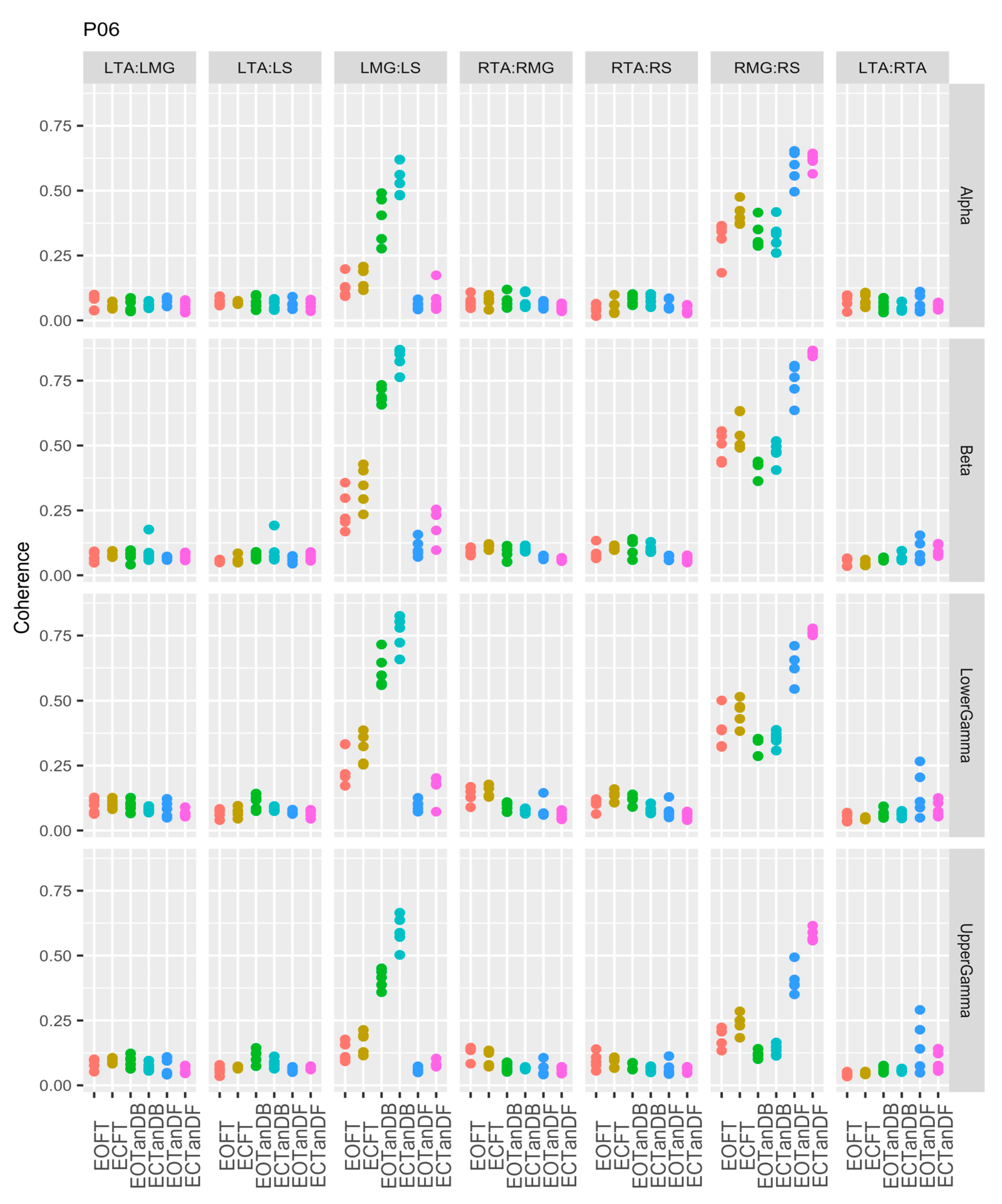
Previously, we identified inter-trial and inter-participant variability (Appendix A) and in subsection 3.2 we noted differences in muscular coherence patterns across our six participants. In Figure 3.3.1 we again demonstrated the notable biological variability as individuals adapt to changes in standing postures. The greatest variability is seen in the LMG: LS and RMG: RS muscle pairs across all frequency bands. As it turns out these were the muscle pairs that were most affected by the less stable standing postures. Figure 3.3.1. also shows that P06 appeared to have the most variability between trials particularly for the LMG: LS and RMG: RS muscle pairs.
4. Discussion
A significant incidence of falls related to the effects of aging, and degenerative and neurological disease is a major problem worldwide [3,4,5,6,7,8,9,10,11]. Since falls have been associated with a reduced ability to control postural sway [1,2], acquiring insight into the neurological mechanisms of standing balance and postural control is important. Previous research has addressed many aspects of biomechanical and central nervous systems' control of postural sway for both normal and elderly individuals based on the inverted pendulum model [39,40] for natural quiet standing postures [19,22,33,45,46,65,80,89], as well as the more difficult tandem stance [71,83,86,87]. In tandem standing it has been shown that EMG-EMG coherence of selected lower leg muscles is greater than natural standing and that larger vertical ground reaction forces exist under the rear foot. However, it is unclear what role the dominant leg/foot plays concerning maintaining a tandem standing posture. Having additional insight on tandem standing in healthy individuals is important to help baseline our understanding of different standing postures, and because this posture can be used as a tool to test those with musculoskeletal and neurological diseases who have impaired balance. Therefore, this project examined 1) how functional connectivity of lower leg muscle pairs, i.e., EMG-EMG coherence, would change with greater standing posture challenges and 2) the role of the dominant leg in maintaining tandem standing posture. Our results showed consistently greater coherence in the beta, lower gamma, and upper gamma frequency bands, particularly between the medial gastrocnemius and soleus muscle pairs bilaterally in the tandem stance posture; without discernable differences between eyes open or closed conditions. Although EMG-EMG coherence of muscle pairs was typically greater in the rear leg, functional connectivity did not appear to be different when the dominant leg was in the rear or fore position during tandem standing.
In his seminal work on the coordination and regulation of movement, Berstein [13] highlighted the complexity of the CNS and its challenge to manage the degree of freedom (DoF) redundancy. Bernstein’s hierarchical control theory suggested that the CNS governed specific functional control structures, which may minimize the DoF problem [13,15,99]. Latash and colleagues [16,17,18,100], acknowledged the DoF issue and, noting the variability in human movement, claimed that a DoF problem did not exist. Their alternative, called the “principal of abundance” suggested that all the elements, i.e., DoFs, always participated in all tasks, so that performance stability and flexibility, i.e., variability, could be optimized depending on the functional demands. Latash et al.’s [16,100] uncontrolled manifold hypothesis (UCM) was an attempt to define muscle synergies better and provide a method to examine the control of movement patterns related to an infinite number of activities. Krishnamoorthy et al. [19,20] examined shifts in the center of pressure and EMG activity of several postural muscles, using UCM to explore the role of muscle synergies during different standing tasks. They identified three muscle synergy patterns, i.e., muscle (or M) modes, that involved the control of antero-posterior postural sway. Other methods using EMG of postural muscles and principal component analysis (PCA) and/or non-negative matrix factorization (NNMF) [21,22] have also attempted to refine the ability to identify muscle synergies related to the control of quiet standing posture. In the last three decades, this work segued to research that used the EMG signal to examine the spectral information about motor neuron firing and the motor unit action potentials [101,102]. Thus, common presynaptic inputs to motor neuron pools of two or more muscles can synchronize their firing frequency, where the strength of such synchronization becomes apparent in the coherence, i.e., a measure of correlation in the frequency domain, between trains of action potentials discharged by motor neurons innervating two muscles. Common neural inputs to different muscles can then be inferred based on intermuscular (IMC or EMG-EMG) methods to examine the role of common neural drives that synchronously activate motor pools of individual muscles in a functional synergy [25,26,27,28,29,30,31].
If, from a neurological perspective, standing balance is maintained by functional synergies through the coordinated action of lower leg muscles, we assume that neural control may be simplified by the synchronized, i.e., common inputs, activation of muscles comprising a functional synergy as a single unit, rather than separate neural signals to each muscle [25,49,79,101]. From a biomechanical perspective, the single inverted pendulum (SIP) model, using the EMG of lower leg muscles, has been used to study quiet stance [39,40,41,42,43,51]. These studies have shown that during a natural quiet stance, i.e., standing with feet apart, the antero-posterior postural sway is controlled primarily by the lower leg muscles, e.g., dorsi- and plantarflexors. Whereas, medio-lateral sway is controlled by the ankle invertors/evertors and loading/unloading at the hip joint. While the results of this early work provided valuable insights into an aspect of postural control it insufficiently did so because of methodological limitations. Research using IMC based on the SIP has significantly increased our understanding of quiet standing postural control, under a variety of conditions, in young [22,32,33,34,48,49,65,79,80,81,82,83,84,85,86,87] and older adults [50,80,89,90,91,92,93,94] by providing information on the neural inputs to muscles at different frequencies that are characteristic of activity in different areas of the central nervous system, i.e., cortical, subcortical, spinal. Therefore, the source of presynaptic common inputs can be inferred based on the frequencies at which EMG-EMG coherences have emerged [26]. For example, during quiet standing coherence of select lower leg muscle pairs has been reported in the 0-5 Hz (delta), 6-15 (alpha) Hz, and 13-30 (beta) Hz bands. Delta and alpha frequency bands are thought to reflect subcortical inputs [80,101], and although alpha frequency bands may also involve corticospinal contributions, the beta band primarily is thought to reflect corticospinal control [77]. As standing task difficulty increases, e.g., tandem stance, significant beta band coherence is evident [83,86,87] and corticospinal excitability of the lower leg muscles has also been shown to increase [103].
Since our research involved two standing tasks more difficult than natural quiet standing, i.e., feet together and tandem, under both eyes open and closed conditions, it is most relevant to discuss our findings relative to previous research that examined the EMG-EMG coherence of lower leg muscles during quiet tandem standing postures [83,86,87]. Although we collected ground reaction force data in our cohort we have not presented those results here. However, in a previous publication using data from the same cohort as ours, Tipton et al. [104] showed that approximate entropy (ApEn) and velocity of the center of pressure (COP) in both the antero-posterior and medio-lateral directions were significantly increased in three less stable (more difficult) standing positions: feet together eyes close, and tandem with eyes open and eyes closed. An increase in ApEn suggests a more variable time series and less predictable pattern associated with a novel movement pattern, e.g., tandem standing. The COP findings in Tipton et al.’s report are consistent with many previous studies on the biomechanical and neurological challenges of tandem standing in non-impaired, healthy adults [41,66,67,68,69,70,71,72,73,74].
Ojha et al. [86] studied healthy young adults using a protocol very similar to ours. That is, they synchronized the motion capture of various standing barefoot postural stances and the collection of ground reaction forces and EMG of the tibialis anterior (AT), soleus (S), and medial gastrocnemius (MG) muscles, bilaterally. Their tandem stance data, however, only reflected when the dominant foot was on the rear force plate. Ojha used wavelet decomposition to extract the neural frequency bands: delta, theta, alpha, beta, and gamma, and magnitude squared coherence to examine common neural inputs to co-acting muscle pairs bilaterally: LAT-LMG, LAT-LS, LMG-LS, RAT-RMG, RAT-RS, LAT-RAT, LMG-RMG, AND LS-RS (where L = left and R = right). Tests for EMG cross-talk between muscle pairs were negligible. They showed that with increased postural challenges, i.e., eyes closed and tandem stances, the EMG signal density increased in all muscles, and coherence between muscle pairs trended higher in the least stable stances. There was greater coherence between muscle pairs of the same leg in the lower frequency band, i.e., delta, particularly for the right, i.e., dominant limb. Furthermore, coherence between RMG and RS was greater under all conditions [86].
Our study extended Ojha et al.’s results and tested a potential role the dominant limb might play in maintaining postural stability in the same postural conditions. Although we did not analyze the coherence in the delta and theta frequency bands, our results showed increased coherence between all muscle pairs in the tandem stance position compared to the baseline (or control) posture, i.e., feet together eyes open. Moreover, there was consistently greater coherence in the LMG: LS and RMG: RS muscle pairs across the beta, lower gamma, and upper gamma frequency bands for tandem stance postures in both the eyes open and eyes conditions, although there were no discernible differences in coherence when the eyes were open or closed. Kerkman et al. [32] also reported increased connectivity at higher frequency components (11-21 Hz and 21-60 Hz), but within and between lower leg and torso synergies. They suggested higher frequency components may reflect propriospinal pathways. Our coherence results in the beta and gamma frequency bands were different than what Ojha et al. reported, suggesting that future research might attempt to replicate our findings with a larger sample. We also reported coherence between antagonistic muscle pairs, e.g., LTA: LS, primarily in the tandem stance postures. This suggests that increased stiffness produced by these co-actions may be needed for less stable postures. When we looked at the possible role of the dominant limb it was apparent that muscle pair coherences were not different when the dominant limb was placed over the rear or forward forceplate. Finally, perhaps consistent with Latash et al.’s principle of abundance [16,17], we identified consistent inter-trial and inter-participant variability in muscle coherence patterns across our six participants, which was similar to what Torres-Oviedo and Ting reported [21,105]. These results may be indicative of the CNS’s ability to use all the elements, i.e., DoFs, in all of the postural tasks used in this project to ensure both flexible responses and standing stability.
In another comparable study, Nandi et al. [83] collected ground reaction force (COP) and surface EMG from six muscles, on the dominant side only, (soleus, Sol; lateral gastrocnemius, LG; tibialis anterior, TA; peroneus longus, PL; biceps femoris, BF; rectus femoris, RF) under four conditions (standing in stocking feet), in random order: 1) tandem stance with the dominant foot posterior, 2) wide stance (feet shoulder width apart), 3) narrow stance (feet together), and 4) one leg stance (dominant foot). Single-pair EMG-EMG coherence was estimated for the agonist-agonist (AG-AG) pairs: Sol-LG, Sol-PL, LG-PL, and agonist-antagonist (AG-ANT) pairs: Sol-TA, LG-TA, PL-TA, and RF-BF in the 0-55 Hz range; reflecting subcortical/spinal, and corticospinal inputs at 0-5 and 6-15 Hz and 6-15 and 16-40 Hz, respectively. They found that coherence was greater in the AG-AG compared to the AG-ANT muscle pairs in all frequency bands, suggesting that the system preferred functional synergies consistent with reciprocal rather than stiffness control. Coherence increased with stance difficulty but only in the AG-ANT muscle pairs in the delta band (0-5 Hz), reflecting subcortical input. Whereas, greater coherence in the AG-AG group, with increasing postural challenges, was noted in the beta and lower gamma bands (16-40 Hz), reflecting corticospinal inputs. Although we did not examine the coherence of the AG-ANT invertor/evertor antagonist muscle pair, e.g., PL-TA, our findings and conclusions are similar to Nandi et al. [83].
Tsiouri et al. [87] suggested that although the role of large muscle groups in postural control was substantial, the contribution of the toe flexors was underappreciated. To date, they have been the only group to examine the coherence of both ankle and intrinsic foot muscles in the control of standing balance. They included young healthy adults, collecting ground reaction forces (COP) and EMG activity of the flexor digitorum brevis (FDB), soleus (SOL), medial gastrocnemius (MG), and tibialis anterior (TA) while barefoot under four stance conditions: bipedal, tandem, one-legged (dominant leg), and on toes. Coherence of rectified EMG signals in the 0-60 Hz band, but with two frequency bands of interest, i.e., 0-5 Hz and 10-20 Hz, was determined for the SOL/FDB muscle pair. They showed that COP sway and the EMG activity in all muscles were greater for the three more difficult postural stances and that significant coherence between the SOL and FDB was found in both frequency bands. Notably, the increased coherence with increased stance challenges was greater in the 10-20 Hz (or beta) band. Their coherence findings are consistent with previously cited papers and underscore the importance of the FDB muscles in control of standing balance, as well as their relationship with the soleus.
Our study was not without methodological limitations. Future studies will need to include a larger sample size and test individuals with various other conditions, e.g., aging and musculoskeletal and neurological impairments. Unfortunately, because the raw EMG signals in this study were filtered we were unable to examine coherence in the lower frequency band ranges, so future work will need to re-examine this issue. On the other hand, we believe the fidelity of analysis of the other frequency band ranges was preserved. We did not examine our EMG for cross-talk because our protocol was identical to Ojha et al.’s [86]; perhaps this assumption needs to be examined. Winter [41] suggested that the ankle invertor/evertor muscles were critical in the control of medio-lateral postural sway, yet we did not test the activity of any ankle evertors, e.g., peroneus longus. Future research using our protocol should include ankle invertor/evertor muscles. We defined leg dominance as the leg one would kick a ball with, yet there is no consensus on the definition of leg dominance as some have suggested that the dominant leg is the one used to stand on one leg. Finally, since our test conditions were not randomly organized a learning effect may have biased our results.
In conclusion, we believe that the use of connectivity analysis provides insight into how the CNS functions to control the multi-segmented musculoskeletal system under a variety of quiet standing postures. We have contributed additional evidence that the CNS can implement a common neural drive to simultaneously synchronize and activate key ankle muscles needed to maintain postural stability during internal perturbations, e.g., tandem stance with eyes closed. Some of our data corroborated previously published works, yet our data also uniquely suggests that muscle coherence in the lower and upper gamma frequency ranges may be related to the control of tandem standing. Additionally, it appears that functional muscle synergies are more important than simply limb dominance, although our data corroborate earlier studies that showed that in tandem standing greater muscle activity occurs in the rear leg. The coherence analysis in this study was unable to identify changes in antagonistic or bilateral homologous connectivity with increasing instability, suggesting that perhaps additional information theoretic measures, e.g., mutual information (MI) might be useful in future research. Finally, the inter-trial and participant variability appears to be consistent with the principle of abundance suggesting that formal information theory analysis of these data may be warranted. Our study results with young healthy adults suggest that clinical testing of tandem balance tasks might be a useful adjunct to the clinical measure of balance for individuals with musculoskeletal and neurological impairments.
Author Contributions
Conceptualization, DM, SR, GA; Methodology, DM, SR, GA; Software, DM; Validation, DM; Formal Analysis, DM; SR, GA, DWZ; Resources, GA; Data curation, DM, SR; Writing (original draft) – DM; Writing (review and editing), DM, SR, GA, DWZ; Visualization – DM, SR, DWZ; Supervision, SR, GA, DWZ; Project administration, SR, GA; All authors have read and agreed to the published version of the Manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
The study was conducted following the Declaration of Helsinki, and approved by the Institutional Review Board of Grand Valley State University(18-246-H) for studies involving humans.
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
The data presented in this study are available on request from the corresponding author due to restrictions imposed by our institution on retired faculty.
Acknowledgments
We acknowledge University administrative support for the use of equipment and materials needed for motion capture in the Biomechanics and Motor Performance Laboratory and all study participants.
Conflicts of Interest
The authors declare no conflicts of interest.
Appendix A
EMG-EMG muscular coherence for each participant: 5 trials, over 6 test conditions (EOFT = eyes open feet together; ECFT = eyes closed feet together; EOTanDB = eyes open tandem dominant leg back; ECTanDB = eyes closed tandem dominant leg back; EOTanDF = eyes open tandem dominant leg forward; ECTanDF = eyes closed tandem dominant leg forward, for all muscle pair combinations (LMG/RMG = left/right medial gastrocnemius; LS/RS = left/right soleus; LTA/RTA = left/right tibialis anterior), and across 4 frequency bands: alpha (8-13) Hz, beta ([13-30 Hz), lower gamma (30-60 Hz), upper gamma (60-100 Hz).
Figure A1.
EMG-EMG muscular coherence for participant#1 (P01).
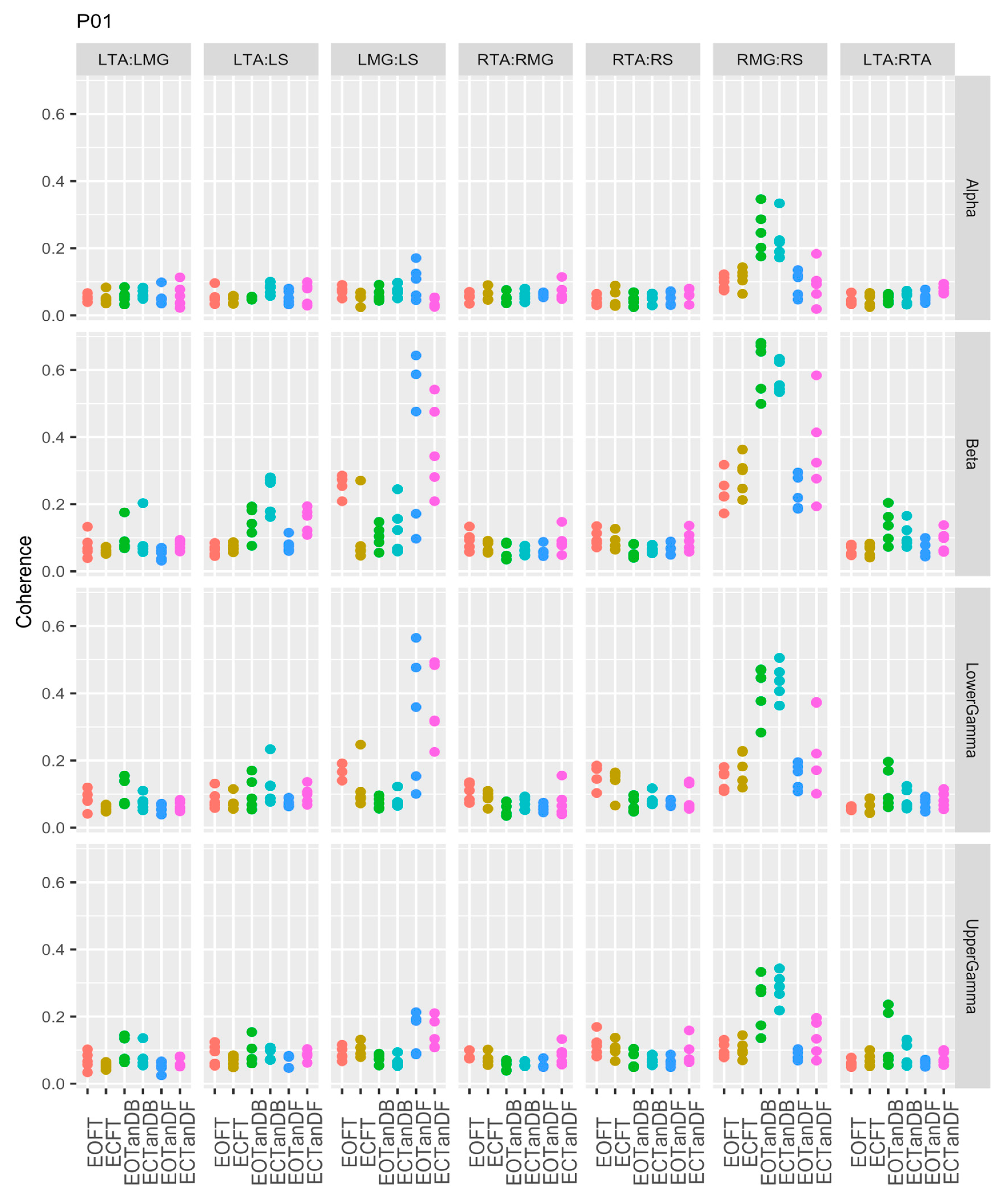
Figure A2.
EMG-EMG muscular coherence for participant#2 (P02).
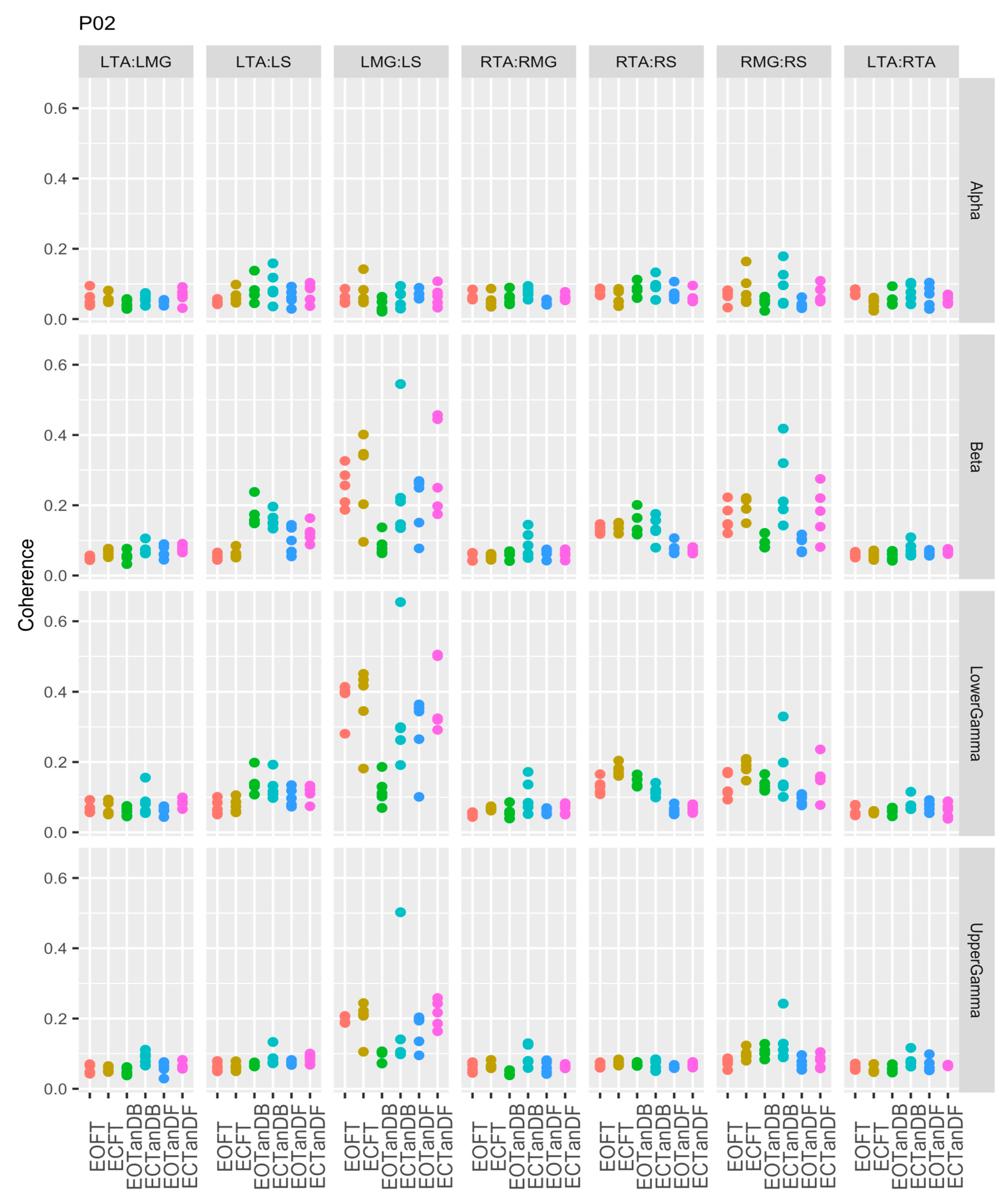
Figure A3.
EMG-EMG muscular coherence for participant#3 (P03).
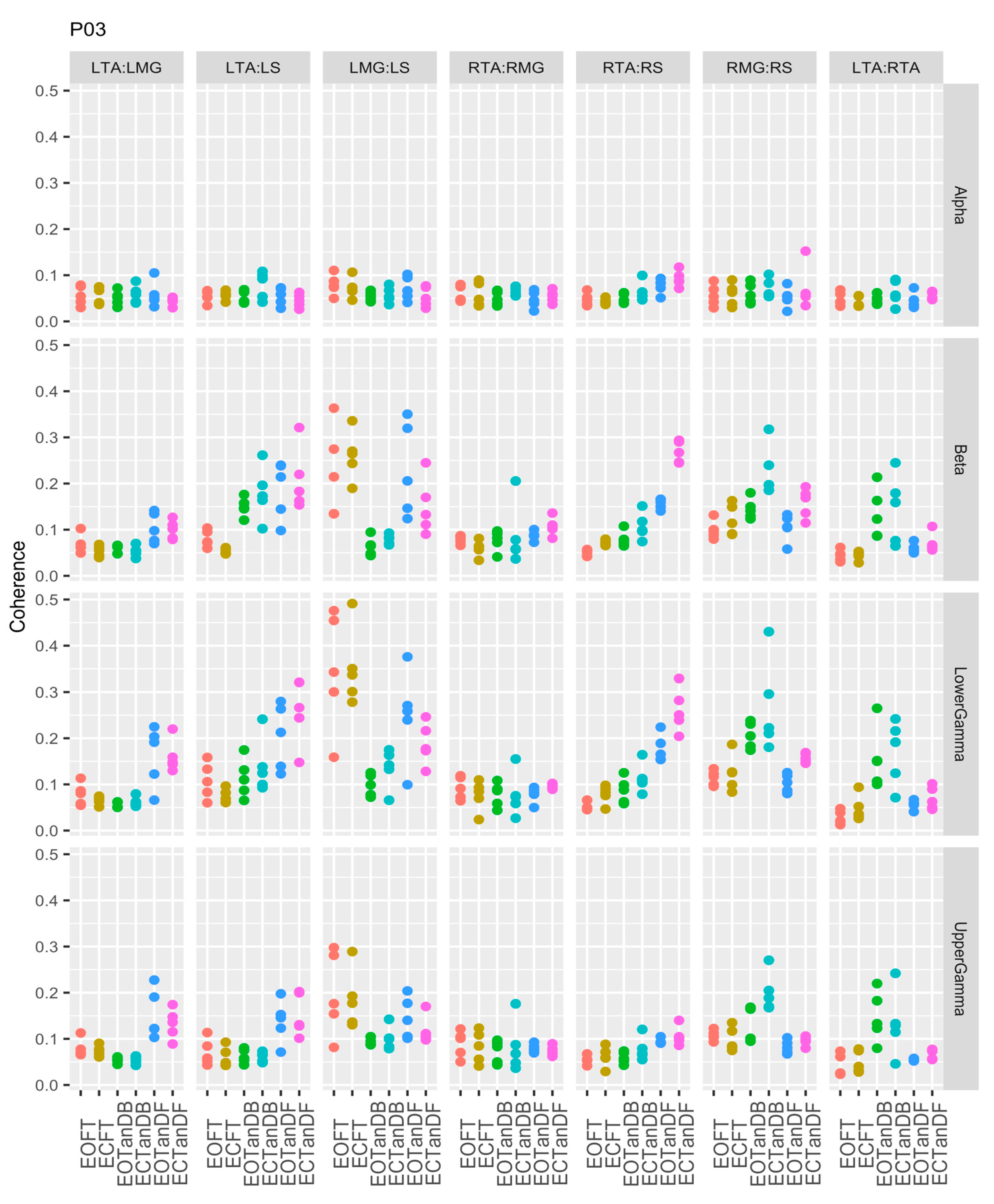
Figure A4.
EMG-EMG muscular coherence for participant#4 (P04).

Figure A5.
EMG-EMG muscular coherence for participant#5 (P05).
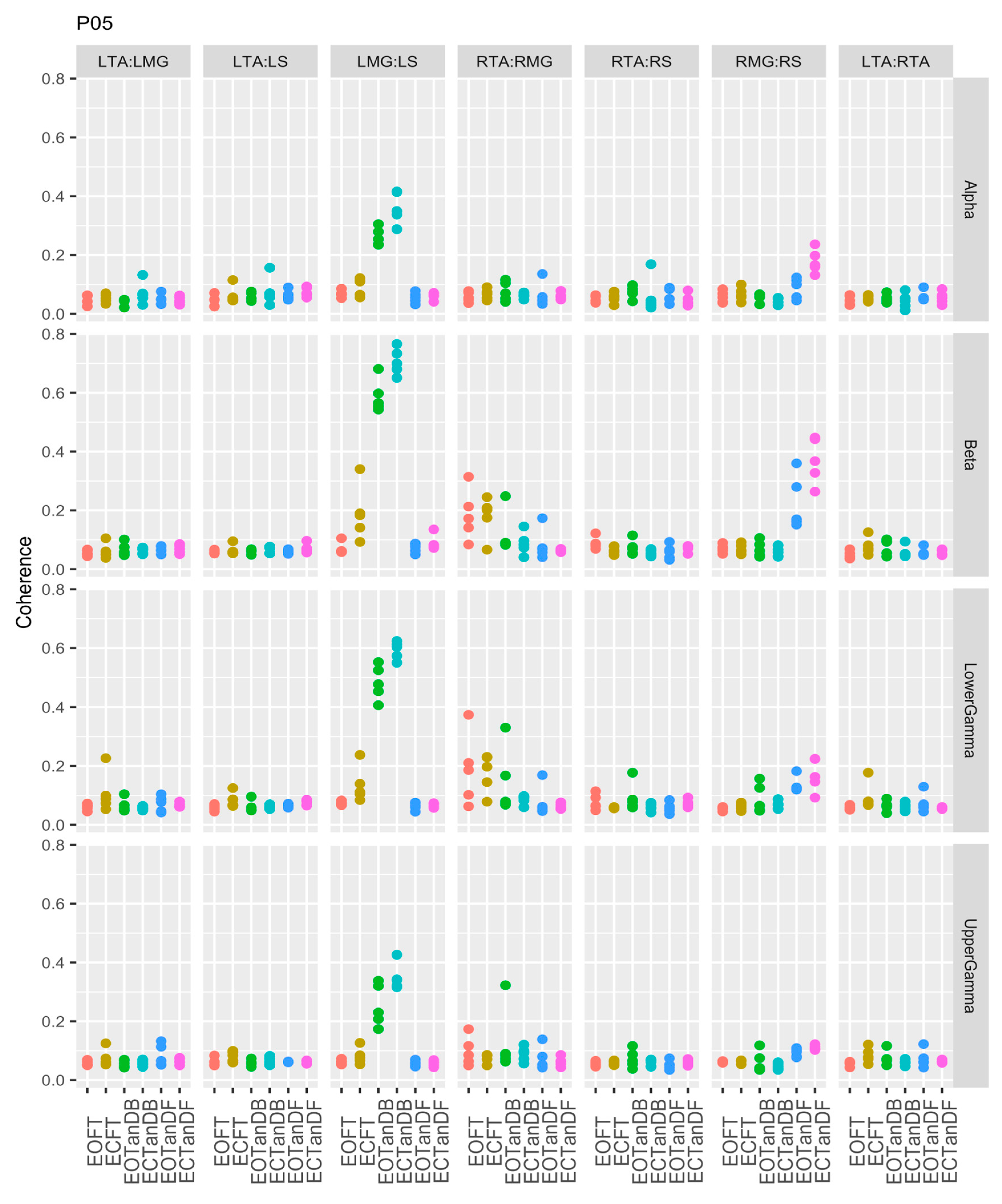
Figure A6.
EMG-EMG muscular coherence for participant#6 (P06).
References
- Masui, T.; Hasegawa, Y.; Matsuyama, Y.; Sakano, S.; Kawasaki, M.; Suzuki, S. ; Gender differences in platform measures of balance in rural-dwelling elders. Arch Gerontol Geriatr 2005, 41, 201–209. [Google Scholar] [CrossRef] [PubMed]
- Roman-Liu, D. Age-related changes in the range and velocity of postural sway. Arch Gerontol Geriatr 2018, 77, 68–80. [Google Scholar] [CrossRef] [PubMed]
- Lamont, R.M.; Morris, M.E.; Menz, H.B.; McGinley, J.L.; Brauer, S.G. Falls in people with Parkinson’s disease: a prospective comparison of community and home-based falls. Gait Posture 2017, 55, 62–67. [Google Scholar] [CrossRef] [PubMed]
- Gazibara, T.; Tepavcevic, D.K.; Svetel, M.; Tomic, A.; Stankovic, I.; Kostic, V.S.; Pekmezovic, T. Near-falls in people with Parkinson’s disease: circumstances, contributing factors and association with falling. Clin Neurol Neurosurg 2017, 161, 51–55. [Google Scholar] [CrossRef] [PubMed]
- De Lima, F.; Melo, G.; Fernandes, D.A.; Santos, G.M.; Neto, F.R. Effects of total knee arthroplasty for primary knee osteoarthritis on postural balance: a systematic review. Gait Posture 2021, 89, 139–160. [Google Scholar] [CrossRef] [PubMed]
- Camicioli, R.; Morris, M.E.; Pieruccini-Farina, F.; Montero-Odasso, M.; Son, S.; Buzaglo, D.; Hausdorff, J.M.; Nieuwboer, A. Prevention of falls in Parkinson’s Disease: guidelines and gaps. Move Disord Clin Pract 2023, 10, 1459–1469. [Google Scholar] [CrossRef] [PubMed]
- Weerdesteyn, V.; de Niet, M.; van Duijuhoven, H.J.R.; Geurts, A.C.H. Falls in individuals with stroke. J Rehabil Res Dev 2008, 45, 1195–1214. [Google Scholar] [CrossRef]
- Ambrose, A.F.; Paul, G.; Hausdorff, J.M. Risk factors for falls among older adults: a review of the literature. Maturitas 2013, 75, 51–61. [Google Scholar] [CrossRef]
- Gale, C.R.; Cooper, C. Sayer, A.A. Prevalence and risk factors for falls in older men and women: the longitudinal study of ageing. Age Ageing 2016, 45, 789–794. [Google Scholar] [CrossRef]
- Moutzouri. M.; Gleeson, N., Billis, E., Tsepis, E., Panoutsopoulou, I., Eds.; Gliatis, J. The effect of total knee arthroplasty on patient’s balance and incidence of falls: a systematic review. Knee Surg Sports Traumatol Arthrosc 2017, 25, 3439–3451. [Google Scholar] [CrossRef]
- Salari, N.; Darvishi, N.; Ahmadipanah, M.; Shohaimi, S.; Mohammadi, M. Global prevalence of falls in older adults: a comprehensive systematic review and meta-analysis. J Orthop Surg Res 2022, 17, 334. [Google Scholar] [CrossRef]
- Sporns, O.; Chialvo, D.R.; Kaiser, M.; Hilgetag, C.C. Organization, development and function of complex brain networks. Trends Cogn Sci 2004, 8, 418–425. [Google Scholar] [CrossRef] [PubMed]
- Berstein, N. The Coordination and Regulation of Movements, 1st ed., Pergamon Press Ltd, Oxford, UK, 1967.
- Wang, Z.; Ko, J.H.; Challis, J.H.; Newell, K.M. The degrees of freedom problem in human standing posture: collective and component dynamics. PloS One 2014, 9, e85414. [Google Scholar] [CrossRef] [PubMed]
- Bruton, M. O’Dwyer, N. Synergies in coordination: a comprehensive overview of neural, computational, and behavioral approaches. J Neurophsyiol 2018, 120, 2761–2774. [Google Scholar] [CrossRef] [PubMed]
- Latash, M.L.; Scholz, J.P.; Schöner, G. Motor control strategies revealed in the structure of motor variability. Exerc Sport Sci Rev 2002, 30, 26–31. [Google Scholar] [CrossRef] [PubMed]
- Latash, M.L. The bliss (not the problem) of motor abundance (not redundancy). Exp Brain Res 2012, 217, 1–5. [Google Scholar] [CrossRef]
- Latash, M.L. Motor synergies and the equilibrium-point hypothesis. Mot Contr 2020, 14, 294–2010. [Google Scholar] [CrossRef]
- Krishnamoorthy, V.; Goodman, S.; Zatsiorsky, V. Latash, M.L. Muscle synergies during shifts of the center of pressure by standing persons: identification of muscle modes. Biol Cybern 2003, 89, 152–161. [Google Scholar] [CrossRef]
- Krishnamoorthy, V.; Latash, M.L.; Scholz, J.P.; Zatsiorsky, V.M. Muscle synergies during shifts of the center of pressure by standing persons. Exp Brain Res 2003, 152, 281–292. [Google Scholar] [CrossRef]
- Torres-Oviedo, G. and Ting, L.H. Muscle synergies characterizing human postural responses. J Neurophysiol 2007, 98, 2144–2156. [Google Scholar] [CrossRef]
- Boonstra, T.W.; Danna-Dos-Santos, A.; Xie, H.; Roerdink, M.; Stins, J.F.; Breakspear, M. Muscle networks: connectivity analysis of EMG activity during postural control. Sci Rep 2016, 5, 17830. [Google Scholar] [CrossRef]
- Tanabe, H.; Fujii, K.; Kouzaki, M. Intermittent muscle activity in the feedback loop of postural control system during natural quiet standing. Sci Rep 2017, 7, 10631. [Google Scholar] [CrossRef] [PubMed]
- Ting, L.H. and McKay, J.L. Neuromechanics of muscle synergies for posture and movement. Curr Opin Neurobiol 2007, 17, 622–628. [Google Scholar] [CrossRef] [PubMed]
- De Luca, C.J.; Erim, Z. Common drive in motor units of a synergistic muscle pair. J Neurophysiol 2002, 87, 2200–2204. [Google Scholar] [CrossRef] [PubMed]
- Grosse, P.; Cassidy, M.J.; Brown, P. EEG-EMG, MEG-EMG and EMG-EMG frequency analysis: physiological principles and clinical applications. Clin Neurophysiol 2002, 113, 1523–1531. [Google Scholar] [CrossRef] [PubMed]
- Farmer, S.F.; Halliday, D.M.; Conway, B.A.; Stephens, J.A.; Rosenburg, J.R. A review of recent applications of cross-correlation methodologies to human motor unit recording. J Neurosi Methods 1997, 74, 175–187. [Google Scholar] [CrossRef]
- Farmer, S.G. Rhythmicity, synchronization and binding in human and primate motor systems. J Physiol 1998, 509 (Pt 1) Pt 1, 3–14. [Google Scholar] [CrossRef]
- Bizzi, E.; Cheung, V.C.K. The neural origin of muscle synergies. Front Comput Neurosci 2013, 7–2013. [Google Scholar] [CrossRef]
- Boonstra, T.W. The potential of corticomuscular and intermuscular coherence for research on human motor control. Front Hum Neurosci 2013, 7–2013. [Google Scholar] [CrossRef]
- Laine, C.M. and Valero-Cuevas, F.J. Intermuscular coherence reflects functional coordination. J Neurophysiol 2017, 118, 1775–1783. [Google Scholar] [CrossRef]
- Kerkman, J.N.; Daffertshofer, A.; Gollo, L.L.; Breakshpear, M.; Boonstra, T.W. ; Network structure of the human musculoskeletal system shapes neural interactions on multiple time scales. Sci Adv 2018, 4, eaat0497. [Google Scholar] [CrossRef]
- Mochizuki, G.; Semmler, J.G.; Ivanova, T.D.; Garland, S.J. Low-frequency common modulation of soleus motor unit discharge is enhanced during postural control in humans. Exp Brain Res 2006, 175, 584–595. [Google Scholar] [CrossRef] [PubMed]
- Mochizuki, G.; Ivanova, T.D.; Garland, S.J. Factors affecting the common modulation of bilateral motor unit discharge in human soleus muscles. J Neurophysiol 2007, 97, 3917–3925. [Google Scholar] [CrossRef] [PubMed]
- Tanabe, H.; Fujii, K, .; Kouzaki, M. Joint coordination and muscle activities of ballet dancers during tiptoe standing. Motor Control 2017, 21, 72–89. [Google Scholar] [CrossRef] [PubMed]
- Kenville, R.; Maudrich, T.; Vidaurre, C.; Maudrich, D.; Villringer, A.; Ragert, P.; et al. Intermuscular coherence between homologous muscles during dynamic and static movement periods of bipedal squatting. J Neurophsiol 2020, 124, 1045–1055. [Google Scholar] [CrossRef] [PubMed]
- Hug, F.; Del Vecchio, A.; Avrillon, S.; Farina, D.; Tucker, K. Muscles from the same muscle group do not necessarily share common drive: evidence from the human triceps surae. J Appl Physiol 2021, 130, 342–354. [Google Scholar] [CrossRef] [PubMed]
- Formaggio, E.; Masiero, S. Volpe, D.; Demertzis, E.; Gallo, L.; Del Felice, A. Lack of inter-muscular coherence as axial muscles in Pisa Syndrome. Neurol Sci 2019, 40, 1465–1468. [Google Scholar] [CrossRef] [PubMed]
- Winter, D.A.; Prince, F.; Stergiou, P.; Powell, C. Medial-lateral and anterior-posterior responses associated with centre of pressure changes in quiet standing. Neursci Res Comm 1993, 12, 141–148. [Google Scholar]
- Winter, D. Human balance and posture control during standing and walking. Gait Posture 1995, 3, 193–214. [Google Scholar] [CrossRef]
- Winter, D.A.; Prince, G.; Frank, J.S.; Powell, C.; Zabjek, K.F. Unified theory regarding A/P and M/L balance in quiet stance. J Neurophysiol 1996, 75, 2334–2343. [Google Scholar] [CrossRef]
- Winter, D.A.; Patla, A.E.; Prince, F.; Ishac, M.; Krystyna, G.-P. Stiffness control of balance in quiet standing. J Neurophysiol 1998, 80, 1211–1221. [Google Scholar] [CrossRef] [PubMed]
- Winter, D.A.; Patla, A.E.; Ishac, M.; Gage, W.H. Motor mechanisms of balance during quiet standing. J Electromyogr Kinesiol 2003, 13, 49–56. [Google Scholar] [CrossRef]
- Pollock, A.S.; Durward, B.R.; Rowe, P.J.; Paul, J.P. What is balance? Clin Rehabil 2000, 14, 402–406. [Google Scholar] [CrossRef]
- Ivanenko, Y.; Gurfinkel, V.S. Human postural control. Front Neurosci 2018, 12, 171. [Google Scholar] [CrossRef]
- Horak, F.B. Postural orientation and equilibrium: what do we need to know about neural control of balance to prevent falls. Age Aging 2006, 35 (Suppl. S2), ii7–ii11. [Google Scholar] [CrossRef]
- Carpenter, M.G.; Murnaghan, C.D.; Inglis, J.T. Shifting the balance: evidence of an exploratory role for postural sway. Neurosci 2010, 171, 196–204. [Google Scholar] [CrossRef] [PubMed]
- Boonstra, T.W.; Roerdink. M.; Daffertshofer, A.; van Vugt, B.; van Werven, G.; Beek, P.J. Low-alcohol doses reduce common 10- to 15-Hz input to bilateral leg muscles during quiet standing. J Neurophysiol 2008, 100, 2158–2164. [Google Scholar] [CrossRef]
- Danna-Dos-Santos, A.; Degani, A.M.; Boonstra, T.W.; Mochizuki, L.; Harney, A.M.; Schmeckpeper, M.M.; Tabor, L.C.; Leonard, C.T. The influence of visual information on multi-muscle control during quiet stance: a spectral analysis approach. Exp Brain Res 2015, 233, 657–669. [Google Scholar] [CrossRef]
- Nojima, I.; Suwa, Y.; Sugiura, H.; Noguchi, T.; Tanabe, S.; Mima, T.; Watanabe, T. Smaller muscle mass is associated with increase in EMG-EMG coherence of the leg muscle during unipedal stance in elderly adults. Hum Mov Sci 2020, 71, 102614. [Google Scholar] [CrossRef]
- Warnica, M.J.; Weaver, T.B.; Prentice, S.D.; Laing, A.C. The influence of ankle muscle activation on postural sway during quiet stance. Gait Posture 2014, 39, 1115–1121. [Google Scholar] [CrossRef]
- Loram, I.D.; Lakie, M. Direct measurement of human ankle stiffness during quiet standing: intrinsic mechanical stiffness is insufficient for stability. J Physiol 2002, 545, 1041–1053. [Google Scholar] [CrossRef]
- Vlutters, M.; Boonstra, T.A.; Scouten, A.C.; van der Kooij, H. Direct measurement of the intrinsic ankle stiffness during standing. J Biomech 2015, 48, 1258–1263. [Google Scholar] [CrossRef] [PubMed]
- Aramake, Y.; Nozaki, D.; Masani, K.; Sato, T.; Nakazawa, K.; Yano, H. Reciprocal angular acceleration of the ankle and hip joints during quiet standing in humans. Exp Brain Res 2001, 136, 463–473. [Google Scholar] [CrossRef] [PubMed]
- Creath, R.; Kiemel, T.; Horak, F.; Peterka, R.; Jeka, J. A unified view of quiet and perturbed stance: simultaneous co-existing excitable modes. Neurosci Lett 2005, 377, 75–80. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Y.; Kiemel, T.; Jeka, J. The influence of sensory information on two-component coordination during quiet stance. Gait Posture 2007, 26, 263–271. [Google Scholar] [CrossRef] [PubMed]
- Pinter, H.J.; van Swigchem, R.; van Soest, A.J.K.; Rozendaal, A. The dynamics of postural sway cannot be captured using a one-segment inverted pendulum model: a PCA on segment rotations during unperturbed stance. J Neuophysiol 2008, 100, 3197–3208. [Google Scholar] [CrossRef]
- Gunther, M.; Grimmer, S.; Siebert, T.; Blickhan, R. All joints contribute to quiet stance: a mechanical analysis. J Biomech 2009, 42, 2739–2746. [Google Scholar] [CrossRef]
- Sasagawa, S.; Ushiyama, J.; Kouzaki, M.; Kanehisa, H. Effect of hip motion on the body kinematics in the sagittal plane during human quiet standing. Neurosci Lett 2009, 450, 27–31. [Google Scholar] [CrossRef]
- Suzuki, Y.; Nomura, T.; Casadio, M.; Morasso, P. Intermittent control with ankle, hip, and mixed strategies during quiet standing: a theoretical proposal based on a double inverted pendulum model. J Theor Biol 2012, 310, 55–79. [Google Scholar] [CrossRef]
- Sasagawa, S.; Shinya, M.; Nakazawa, K. Interjoint dynamic interaction during constrained human quiet standing by induced acceleration analysis. J Neurophysiol 2014, 111, 313–322. [Google Scholar] [CrossRef]
- Yamamoto, A.; Sasagawa, S.; Oba, N.; Nakazawa, K. Behavioral effect of knee joint motion on body’s center of mass during human quiet standing. Gait Posture 2015, 41, 291–294. [Google Scholar] [CrossRef]
- Morasso, P.; Cherif, A.; Zenzeri, J. Quiet standing: the single inverted pendulum model is not so bad after all. PLoS One 2019, 14, e0213870. [Google Scholar] [CrossRef] [PubMed]
- Yamamoto, T.; Smith, C.E.; Suzuki, Y.; Kiyono, K.; Tanahashi, T.; Sakoda, S.; Morasso, P.; Nomura, T. Universal and individual characteristics of posture sway during quiet standing in healthy young adults. Physiol Rep 2015, 3, 2015–e12329. [Google Scholar] [CrossRef]
- Saffer, M.; Kiemel, T.; Jeka, J. Coherence analysis of muscle activity during quiet stance. Exp Brain Res 2008, 185, 215–226. [Google Scholar] [CrossRef] [PubMed]
- Lord, S.R.; Rogers, M.W.; Howland, A.; Fitzpatrick, R. Lateral stability, sensorimotor function and falls in older people. J Am Geriatr Soc 1999, 47, 1077–81. [Google Scholar] [CrossRef] [PubMed]
- Jonsson, E.; Seiger, Å.; Hirschfeld, H. Postural steadiness and weight distribution during tandem stance in healthy young and elderly adults. Clin Biomech 2005, 20, 202–208. [Google Scholar] [CrossRef]
- Reynolds, R.F. The ability to voluntarily control sway reflects the difficulty of the task. Gait Posture 2010, 31, 78–81. [Google Scholar] [CrossRef]
- Sozzi, S.; Monti, A.; De Nunzio, A.M.; Do, M.-H.; Schieppati, M. Sensori-motor integration during stance: time adaptation of control mechanisms on adding or removing vision. Hum Mov Sci 2011, 30, 172–189. [Google Scholar] [CrossRef]
- Sozzi, S.; Do, M.C.; Monti, A.; Schieppati, A.M. Sensorimotor integration during stance: processing time of active or passive addition or withdrawal of vision or haptic information. Neurosci 2012, 212, 59–76. [Google Scholar] [CrossRef]
- Sozzi, S.; Honeine, J.-L.; Do, M.-C.; Schieppati, M. Leg muscle activity during tandem stance and the control of body balance in the frontal plane. Clin Neurophsiol 2013, 124, 1175–1186. [Google Scholar] [CrossRef]
- Wang, Z.; Newell, K.W. Phase synchronization of foot dynamics in quiet standing. Neurosci Lett 2012, 507, 47–51. [Google Scholar] [CrossRef]
- Wang, Z.; Jordan, K.; Newell, K.M. Coordination patterns of foot dynamics in the control of upright standing. Motor Control 2012, 16, 425–443. [Google Scholar] [CrossRef] [PubMed]
- Wang, Z.; Molenaar, P.M.C.; Newell, K.M. The effect of foot position and orientation on the inter- and intro-foot coordination in standing postures: a frequency domain PCA analysis. Exp Brain Res 2013, 230, 15–27. [Google Scholar] [CrossRef]
- Farina, D.; Negro, F.; Dideriksen, J.L. The effective neural drive to muscles is the common synaptic input to motor neurons. J Physiol 2014, 592 Pt 16, 3427–3441. [Google Scholar] [CrossRef]
- Farina, D.; Merletti, R.; Enoka, R.M. The extraction of neural strategies from the surface EMG: an update. J Appl Physiol 2014, 117, 1215–1230. [Google Scholar] [CrossRef]
- Yamanake, E.; Horiuchi, Y.; Nojima, I. EMG-EMG coherence during voluntary control of human standing tasks: a systematic scoping review. Front Neurosci 2023, 17, 1145751. [Google Scholar] [CrossRef]
- Boonstra, T.W.; Daffertshofer, A.; Roerdink, M.; Flipse, I.; Groenewoud, K.; Beek, P.J. Bilateral motor unit synchronization of leg muscles during a simple dynamic balance task. Eur J Neurosci 2009, 29, 613–622. [Google Scholar] [CrossRef] [PubMed]
- Danna-Dos-Santos, A.; Boonstra, T.W.; Degani, A.M.; Cardoso, V.S.; Magalhaes, T.; Mochizuki, L.; Leonard, C.T. Multi-muscle control during bipedal stance: an EMG-EMG analysis approach. Exp Brain Res 2014, 232, 75–87. [Google Scholar] [CrossRef]
- Obata, H. Abe, M.O.; Masani, K.; Nakazawa, K. Modulation between bilateral legs and within unilateral muscle synergists of postural muscle activity changes with development and aging. Exp Brain Res 2014, 232, 1–11. [Google Scholar] [CrossRef]
- García-Massó, X.; Pellicer-Chenoll, M.; Gonzalez, L.M.; Toca-Herrera, J.L. The difficulty of the postural control task affects multi-muscle control during quiet standing. Exp Brain Res 2016, 234, 1977–1986. [Google Scholar] [CrossRef]
- Noé, F.; García-Massó, X.; Paillard, T. Inter-joint coordination of posture on a seesaw device. J Electromyogr Kinesiol 2017, 34, 72–79. [Google Scholar] [CrossRef]
- Nandi, T.; Hortobagyi, T.; van Keeken, H.G.; Salem, G.J.; Lamoth, C.J.C. Standing task difficulty related increase in agonist-agonist and agonist-antagonist common inputs are driven by corticospinal and subcortical inputs respectively. Sci Rep 2019, 9, 2439. [Google Scholar] [CrossRef]
- Watanabe, T.; Saito, K.; Ishida, K.; Tanabe, S.; Nojima, I. Fatigue-induced decline in low-frequency common input to bilateral and unilateral plantar flexors during quiet standing. Neurosci Lett 2018, 686, 193–197. [Google Scholar] [CrossRef]
- Glass, S.M.; Wildman, L.; Brummitt, C.; Ratchford, K.; Westbrook, G.M.; Aron, A. Effects of global postural alignment on posture-stabilizing synergy and intermuscular coherence in bipedal standing. Exp Brain Res 2022, 240, 841–851. [Google Scholar] [CrossRef]
- Ojha, A.; Alderink, G.; Rhodes, S. Coherence between electromyographic (EMG) signals of anterior tibialis, soleus, and gastrocnemius during standing balance tasks. Front Hum Neurosci 2023, 17–2023. [Google Scholar] [CrossRef]
- Tsiouri, C.; Amiridis, I.G.; Kannas, T.; Varvariotis, N.; Sahinis, C.; Hazitaki, V.; Enoka, R.M. EMG coherence of foot and ankle muscles increases with a postural challenge in men. Gait Posture 2024, 113, 238–245. [Google Scholar] [CrossRef]
- Lowery, M.M.; Myers, L.J.; Erim, Z. Coherence between motor unit discharges in response to shared neural inputs. J Neurosci Methods 2007, 163, 384–391. [Google Scholar] [CrossRef]
- Degani, A.M.; Leonard, C.T.; Danna-Dos-Santos, A. The use of intermuscular coherence analysis as a novel approach to detect age-related changes on postural synergy. Neurosci Lett 2017, 656, 108–113. [Google Scholar] [CrossRef]
- Degani, A.M.; Leonard, C.T.; Danna-Dos-Santos, A. The effects of aging on the distribution and strength of correlated neural inputs to postural muscles during unperturbed bipedal stance. Exp Brain Res 2020, 238, 1537–1553. [Google Scholar] [CrossRef]
- Watanabe, T.; Saito, K.; Ishida, K.; Tanabe, S.; Nojima, I. Coordination of plantar flexor muscles during bipedal and unipedal stances in young and elderly adults. Exp Brain Res 2018, 236, 1229–1239. [Google Scholar] [CrossRef]
- Watanabe, T.; Saito, K.; Ishida, K.; Tanabe, S.; Nojima, I. Age-related declines in the ability to modulate common input to bilateral and unilateral plantar flexors during forward postural lean. Front Hum Neurosci 12, 254. [CrossRef]
- Walker, S.; Piitulainen, H.; Manlangit, T.; Avela, J.; Baker, S.N. Older adults show elevated intermuscular coherence in eyes-open standing but only young adults increase coherence in response to closing the eyes. Exp Physiol 2020, 105, 1000–1011. [Google Scholar] [CrossRef] [PubMed]
- Minamisawa, T.; Chiba, N.; Suzuki, E. ; Intra- and intermuscular coherence and body acceleration control in older adults during bipedal stance. Geriatrics 2021, 6, 114. [Google Scholar] [CrossRef]
- Perotto, A.O. Anatomical guide for the electromyographer, 3rd ed.; Charles C. Thomas: Springfield, IL, USA, 2011; pp. 154–167. [Google Scholar]
- Hermens, H.J.; Freriks, B.; Disselhorst-Klug, C.; Rau, G. Development of recommendations for SEMG sensors and sensor placement procedures. J Electromyogr Kinesiol 2000, 10, 361–74. [Google Scholar] [CrossRef] [PubMed]
- R Core Team (2024), R: A language and environment for statistical computing. R Foundation for Statistical Computing. Vienna, Austria. Htttps://www.R-project.org. (accessed 10 June 2024).
- Posit Team (2024), RStudio: Integrated Development Environment for R.Posit Software, PBC, Boston, MA. https://www.posit.co/. (accessed 10 June 2024). 10 June.
- Profeta, V.L.; Turvey, M.T. Bernstein’s levels of movement construction: a contemporary perspective. Hum Mov Sci 2018, 57, 111–133. [Google Scholar] [CrossRef] [PubMed]
- Scholz, J.P.; Schöner, G. The uncontrolled manifold concept: identifying control variables for a functional task. Exp Brain Res 1999, 126, 289–306. [Google Scholar] [CrossRef] [PubMed]
- Boonstra, T.W.; Breakspear, M. Neural mechanisms of intermuscular coherence implications for the rectification of surface electromyography. J Neurophysiol 2011, 107, 796–807. [Google Scholar] [CrossRef]
- Semmler, J.G. Motor unit synchronization and neuromuscular performance. Exerc Sport Sci Rev 2002, 30, 8–14. [Google Scholar] [CrossRef]
- Nandi, T.; Fisher, B.E.; Hortobágyi, T.; Salem, G.J. Increasing mediolateral standing sway is associated with increasing corticospinal excitability, and decreasing M1 inhibition and facilitation. Gait Posture 2018, 60, 135–140. [Google Scholar] [CrossRef]
- Tipton, N.; Alderink, G.; Rhodes, S. Approximate entropy and velocity of center of pressure to determine postural stability: a pilot study. Appl Sci 2023, 13, 9259. [Google Scholar] [CrossRef]
- Torres-Oviedo, G.; Ting, L.H. Subject-specific muscle synergies in human balance control are consistent across different biomechanical contexts. J Neurophysiol 2010, 103, 3084–3098. [Google Scholar] [CrossRef]
Figure 1.1.
Conceptual model of postural control.
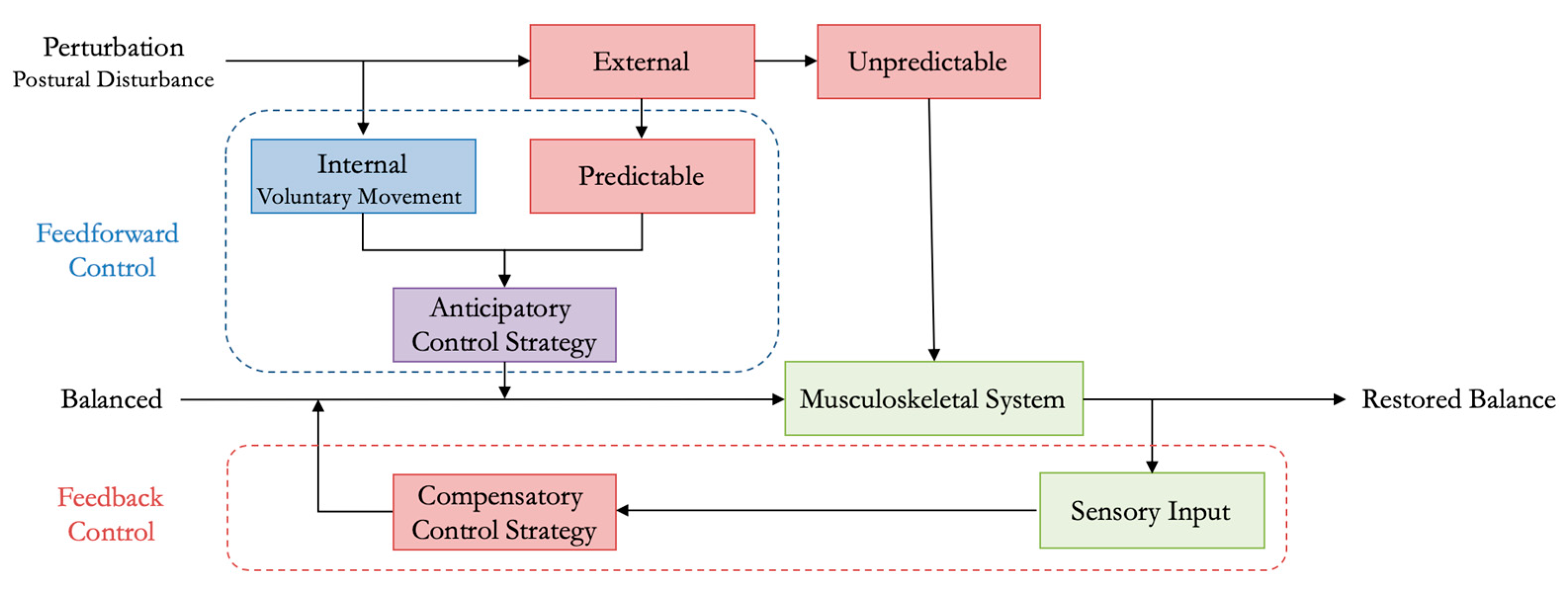
Figure 2.
Steps for data processing for each participant.

Figure 3.1.1.
EMG-EMG muscular coherence for Participant #3 (P03) for five trials over six conditions (EOFT = eyes open feet together; ECFT = eyes closed feet together; EOTanDB = eyes open tandem dominant leg back; ECTanDB = eyes closed tandem dominant leg back; EOTanDF = eyes open tandem dominant leg forward; ECTanDF = eyes closed tandem dominant leg forward) for all muscle pair combinations across four frequency bands: alpha (8-13 Hz), beta (13-30 Hz), lower gamma (30-60 Hz), and upper gamma (60-100 Hz). Note: LMG/RMG = left and right medial gastrocnemius; LS/RS = left and right soleus; LTA/RTA = left and right tibialis anterior.
Figure 3.1.1.
EMG-EMG muscular coherence for Participant #3 (P03) for five trials over six conditions (EOFT = eyes open feet together; ECFT = eyes closed feet together; EOTanDB = eyes open tandem dominant leg back; ECTanDB = eyes closed tandem dominant leg back; EOTanDF = eyes open tandem dominant leg forward; ECTanDF = eyes closed tandem dominant leg forward) for all muscle pair combinations across four frequency bands: alpha (8-13 Hz), beta (13-30 Hz), lower gamma (30-60 Hz), and upper gamma (60-100 Hz). Note: LMG/RMG = left and right medial gastrocnemius; LS/RS = left and right soleus; LTA/RTA = left and right tibialis anterior.

Figure 3.2.1.
Confidence intervals (CI) for mean differences in coherence between less stable, e.g., EOTanDB, standing postures and the baseline standing posture, i.e., EOFT for Participant #1 (PO1). Differences and their confidence intervals (CI) are presented as red (no significant difference) and blue (significantly different). The black horizontal line indicates zero difference, CI above zero indicates that the test condition was greater than the baseline, and CI below zero indicates that the test condition was less than the baseline.
Figure 3.2.1.
Confidence intervals (CI) for mean differences in coherence between less stable, e.g., EOTanDB, standing postures and the baseline standing posture, i.e., EOFT for Participant #1 (PO1). Differences and their confidence intervals (CI) are presented as red (no significant difference) and blue (significantly different). The black horizontal line indicates zero difference, CI above zero indicates that the test condition was greater than the baseline, and CI below zero indicates that the test condition was less than the baseline.
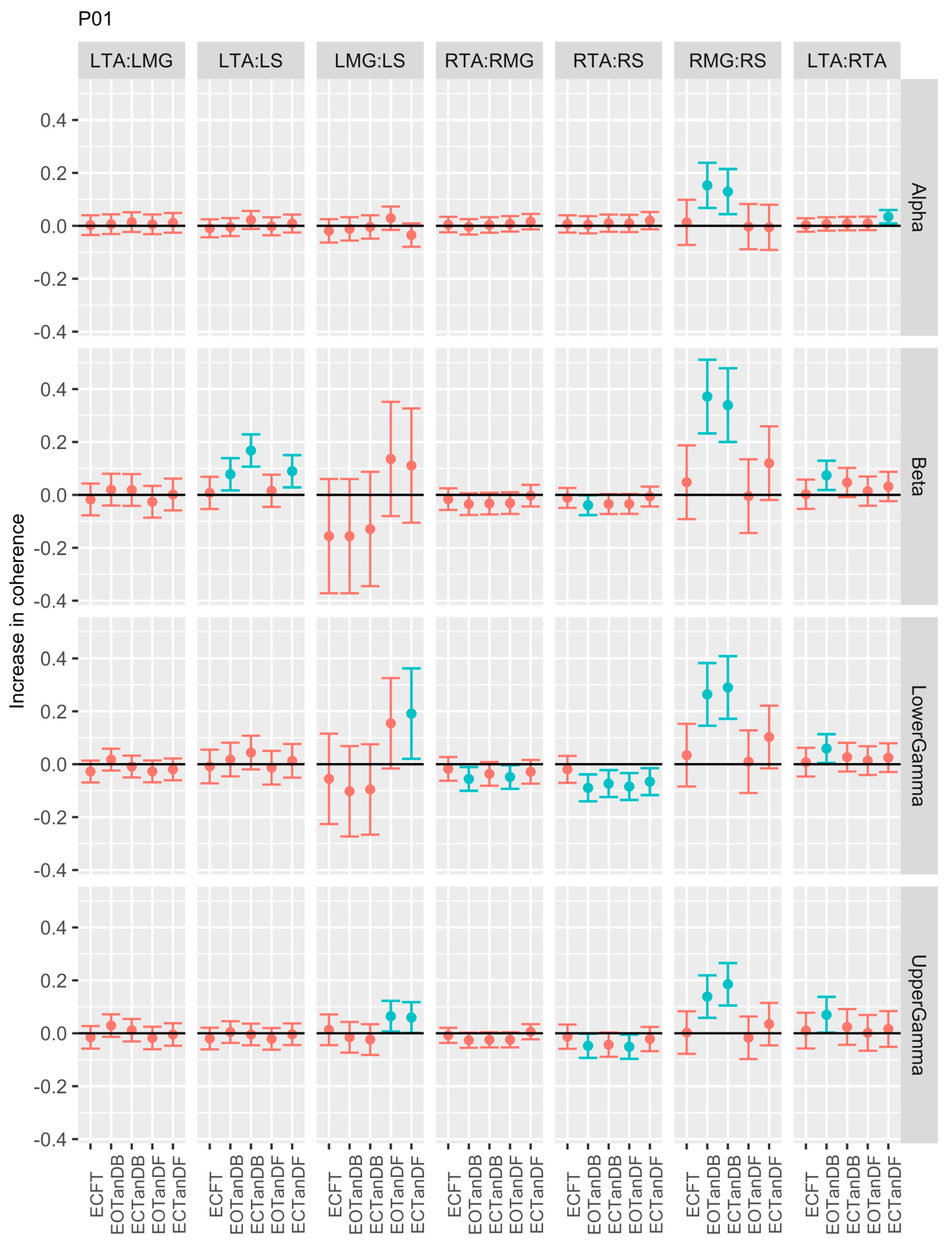
Figure 3.2.2.
Confidence intervals (CI) for mean differences in coherence between less stable, e.g., EOTanDB, standing postures and the baseline standing posture, i.e., EOFT for Participant #2 (PO2). Differences and their confidence intervals (CI) are presented as red (no significant difference) and blue (significantly different). The black horizontal line indicates zero difference, CI above zero indicates that the test condition was greater than the baseline, and CI below zero indicates that the test condition was less than the baseline.
Figure 3.2.2.
Confidence intervals (CI) for mean differences in coherence between less stable, e.g., EOTanDB, standing postures and the baseline standing posture, i.e., EOFT for Participant #2 (PO2). Differences and their confidence intervals (CI) are presented as red (no significant difference) and blue (significantly different). The black horizontal line indicates zero difference, CI above zero indicates that the test condition was greater than the baseline, and CI below zero indicates that the test condition was less than the baseline.
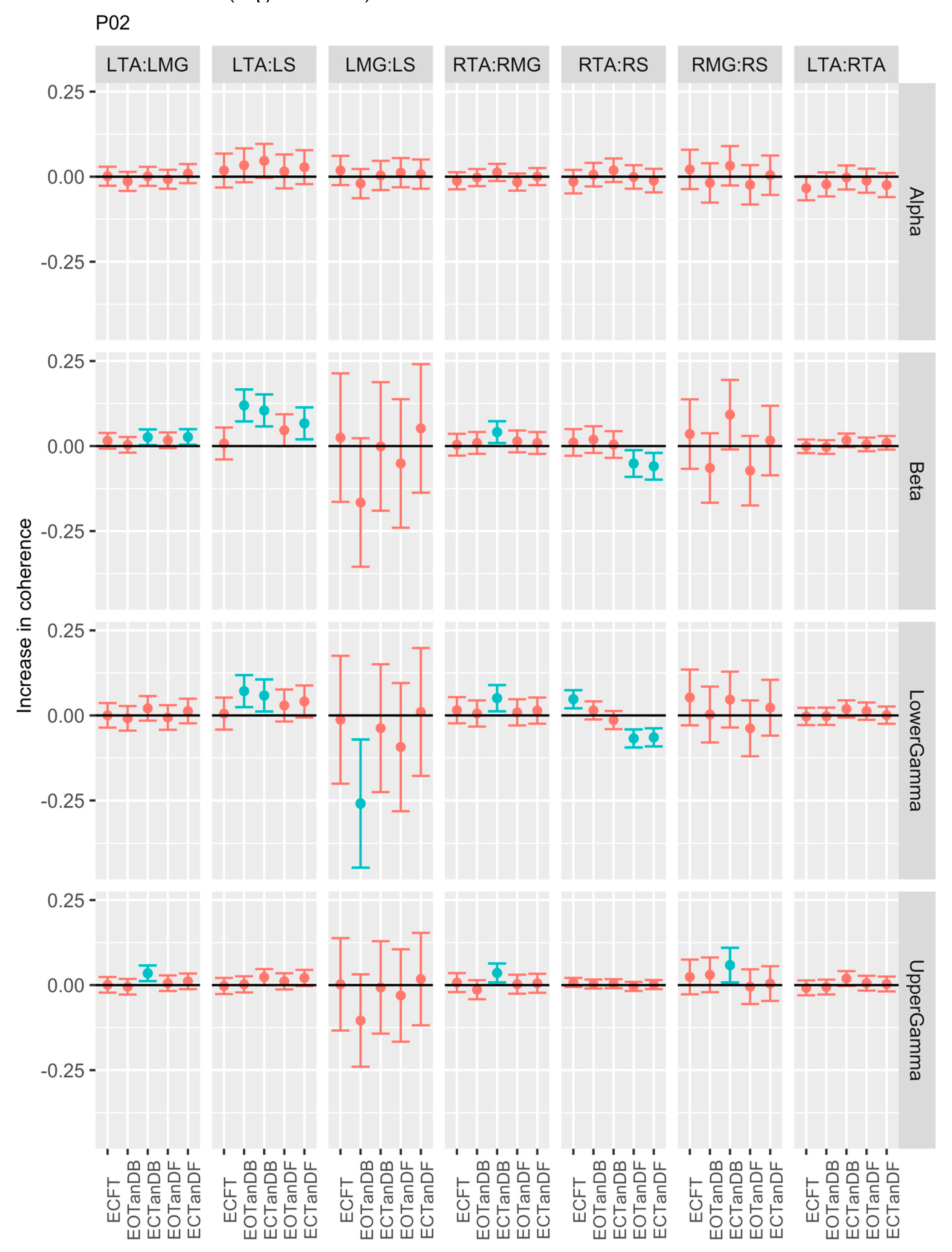
Figure 3.2.3.
Confidence intervals (CI) for mean differences in coherence between less stable, e.g., EOTanDB, standing postures and the baseline standing posture, i.e., EOFT for Participant #3 (PO3). Differences and their confidence intervals (CI) are presented as red (no significant difference) and blue (significantly different). The black horizontal line indicates zero difference, CI above zero indicates that the test condition was greater than the baseline, and CI below zero indicates that the test condition was less than the baseline.
Figure 3.2.3.
Confidence intervals (CI) for mean differences in coherence between less stable, e.g., EOTanDB, standing postures and the baseline standing posture, i.e., EOFT for Participant #3 (PO3). Differences and their confidence intervals (CI) are presented as red (no significant difference) and blue (significantly different). The black horizontal line indicates zero difference, CI above zero indicates that the test condition was greater than the baseline, and CI below zero indicates that the test condition was less than the baseline.
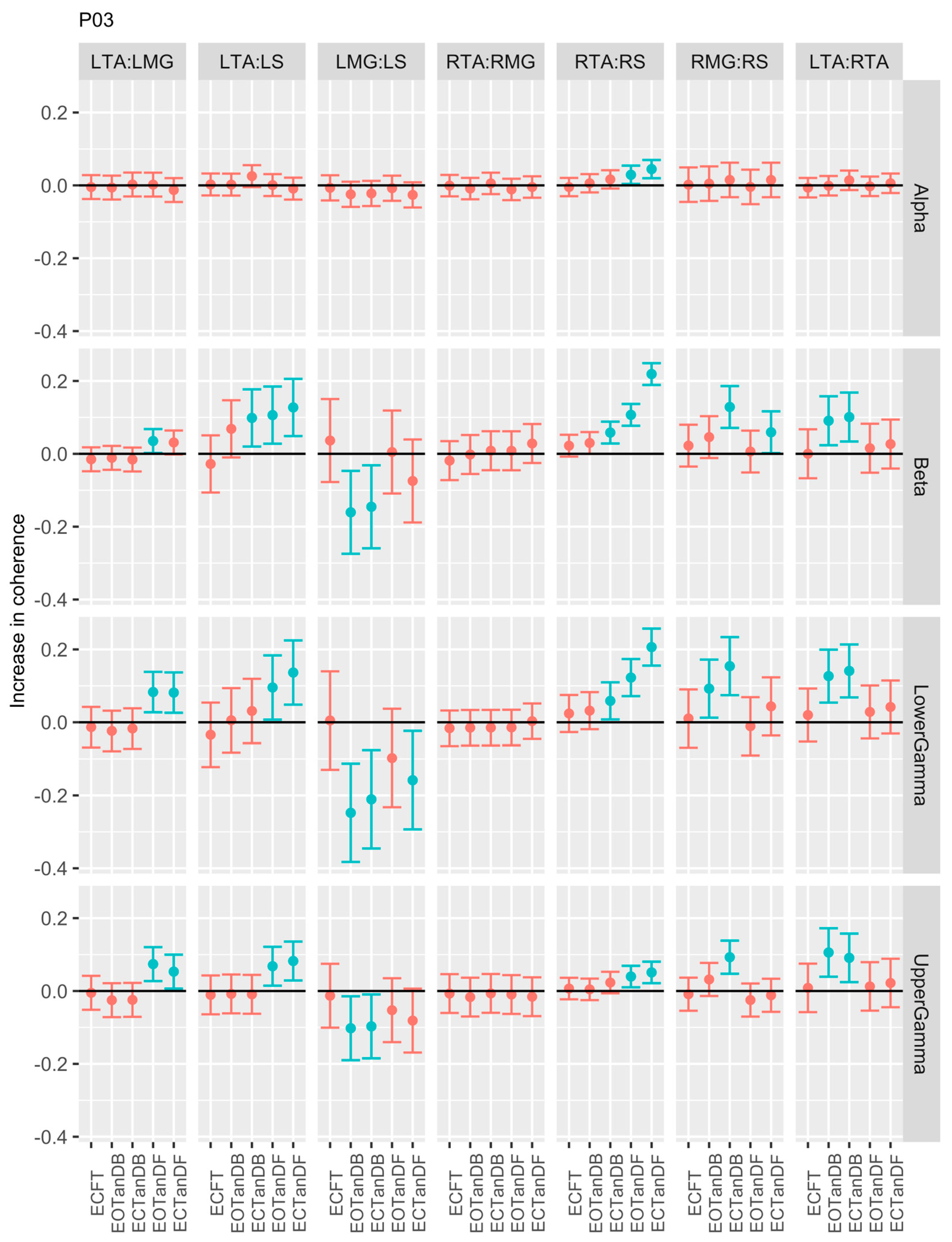
Figure 3.2.4.
Confidence intervals (CI) for mean differences in coherence between less stable, e.g., EOTanDB, standing postures and the baseline standing posture, i.e., EOFT for Participant #4 (PO4). Differences and their confidence intervals (CI) are presented as red (no significant difference) and blue (significantly different). The black horizontal line indicates zero difference, CI above zero indicates that the test condition was greater than the baseline, and CI below zero indicates that the test condition was less than the baseline.
Figure 3.2.4.
Confidence intervals (CI) for mean differences in coherence between less stable, e.g., EOTanDB, standing postures and the baseline standing posture, i.e., EOFT for Participant #4 (PO4). Differences and their confidence intervals (CI) are presented as red (no significant difference) and blue (significantly different). The black horizontal line indicates zero difference, CI above zero indicates that the test condition was greater than the baseline, and CI below zero indicates that the test condition was less than the baseline.
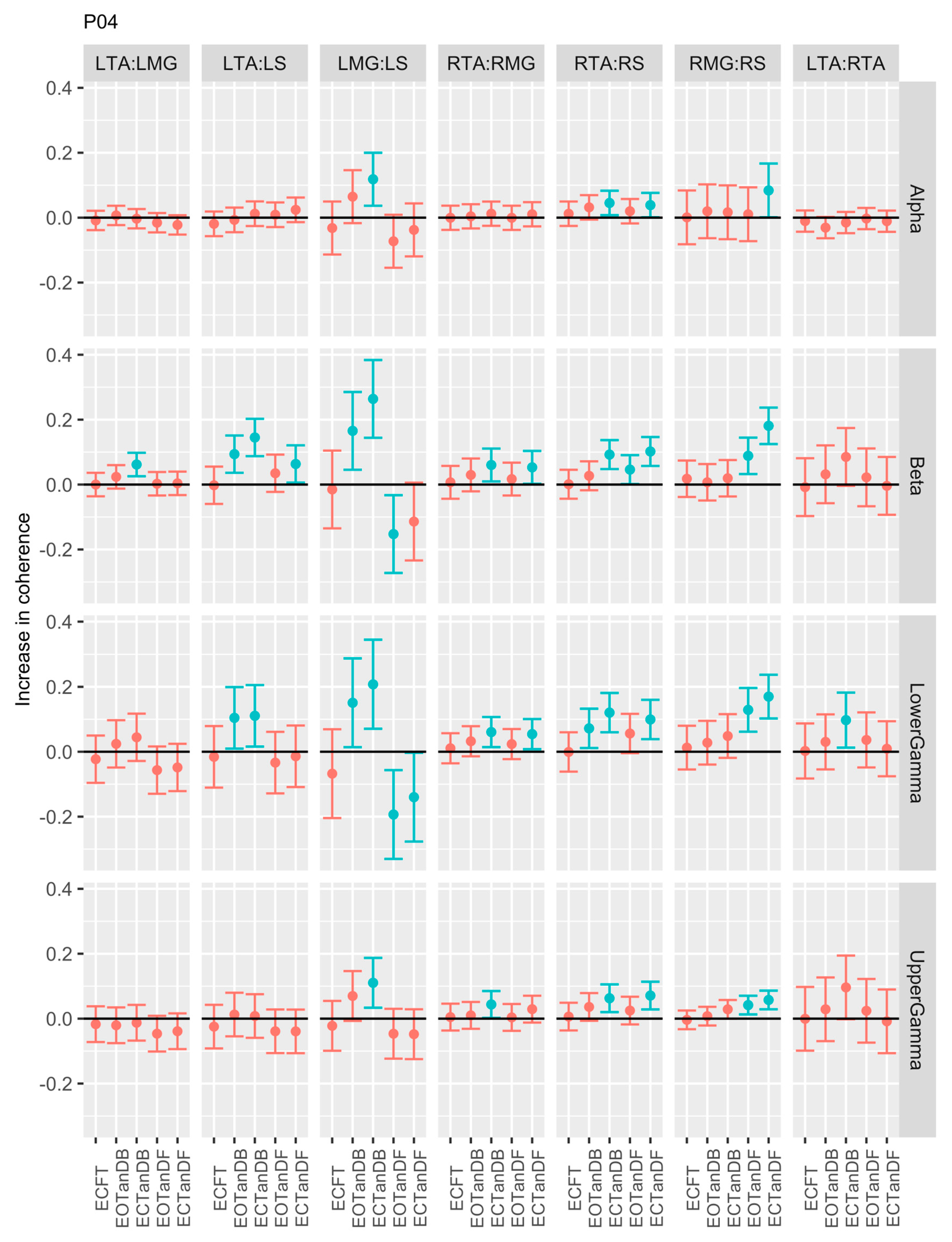
Figure 3.2.5.
Confidence intervals (CI) for mean differences in coherence between less stable, e.g., EOTanDB, standing postures and the baseline standing posture, i.e., EOFT for Participant #5 (PO5). Differences and their confidence intervals (CI) are presented as red (no significant difference) and blue (significantly different). The black horizontal line indicates zero difference, CI above zero indicates that the test condition was greater than the baseline, and CI below zero indicates that the test condition was less than the baseline.
Figure 3.2.5.
Confidence intervals (CI) for mean differences in coherence between less stable, e.g., EOTanDB, standing postures and the baseline standing posture, i.e., EOFT for Participant #5 (PO5). Differences and their confidence intervals (CI) are presented as red (no significant difference) and blue (significantly different). The black horizontal line indicates zero difference, CI above zero indicates that the test condition was greater than the baseline, and CI below zero indicates that the test condition was less than the baseline.
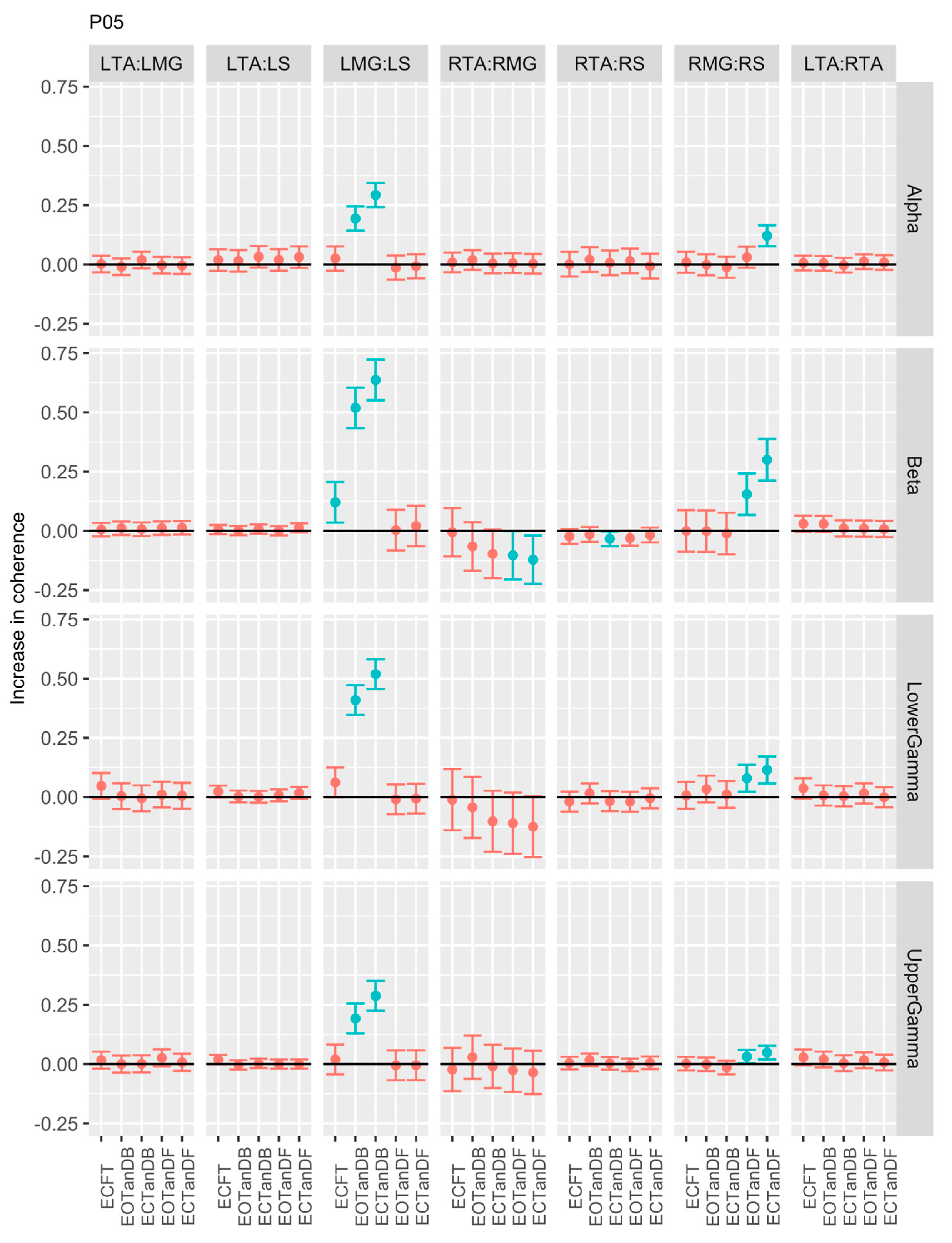
Figure 3.2.6.
Confidence intervals (CI) for mean differences in coherence between less stable, e.g., EOTanDB, standing postures, and the baseline standing posture, i.e., EOFT for Participant #6 (PO6). Differences and their confidence intervals (CI) are presented as red (no significant difference) and blue (significantly different). The black horizontal line indicates zero difference, CI above zero indicates that the test condition was greater than the baseline, and CI below zero indicates that the test condition was less than the baseline.
Figure 3.2.6.
Confidence intervals (CI) for mean differences in coherence between less stable, e.g., EOTanDB, standing postures, and the baseline standing posture, i.e., EOFT for Participant #6 (PO6). Differences and their confidence intervals (CI) are presented as red (no significant difference) and blue (significantly different). The black horizontal line indicates zero difference, CI above zero indicates that the test condition was greater than the baseline, and CI below zero indicates that the test condition was less than the baseline.
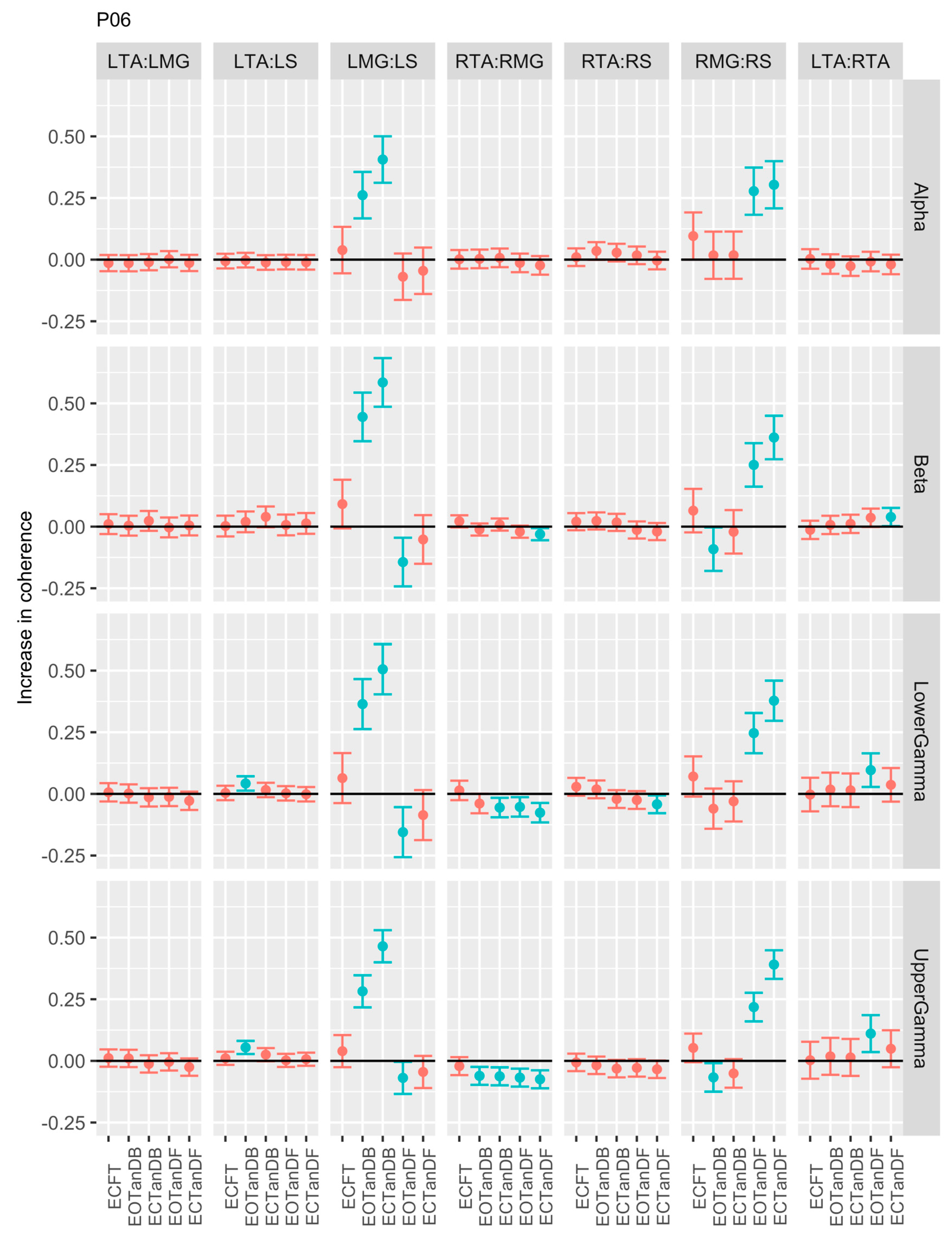
Figure 3.3.1.
Magnitude squared coherence for all six participants across five trials, and all muscle pairs for the alpha, beta, and lower and upper gamma frequency bands.
Figure 3.3.1.
Magnitude squared coherence for all six participants across five trials, and all muscle pairs for the alpha, beta, and lower and upper gamma frequency bands.
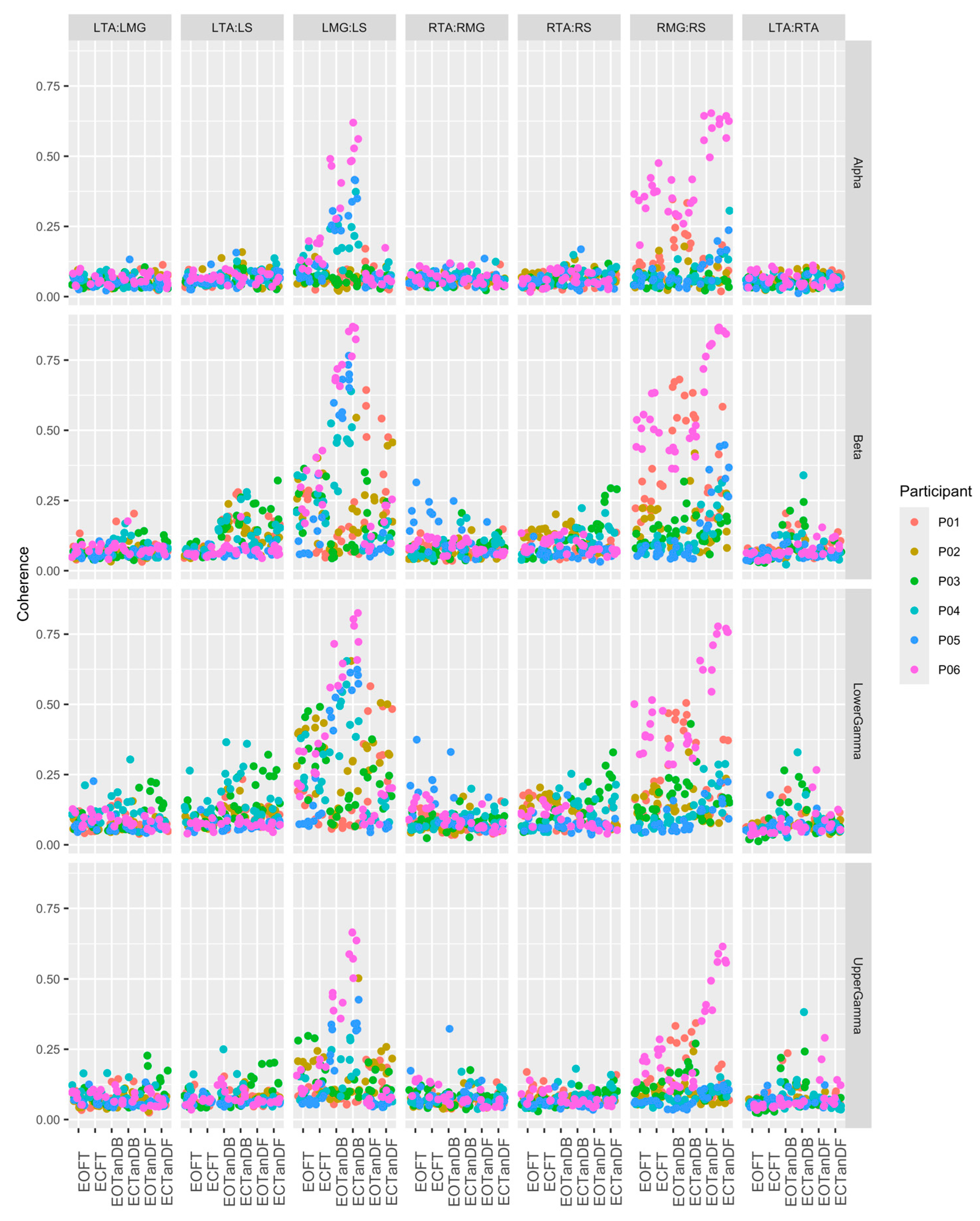

Table 1.1.
Neural Frequency Bands and Their Known Origin.
| Wave | Frequency (Hz) | Origin | Task Manifestation |
|---|---|---|---|
| Delta | 0.5 – 4 | Unknown | Isometric contraction, slow movements |
| Theta | 4 – 8 | Unknown | Isometric contraction, slow movements |
| Alpha | 8 – 13 | Unknown | Isometric contraction, slow movements |
| Beta | 13 – 30 | Motor cortex | Submaximal voluntary contraction |
| Lower Gamma | 30 – 60 | Motor cortex | Voluntary contraction, slow movements |
| Upper Gamma | 60 – 100 | Brainstem | Eye movement (60 – 90 Hz), respiration |
Table 1.
Plantarflexor (P) and Dorsiflexor (D) Muscles of the Lower Legs.
| Posterior Muscles | Anterior Muscles | Deep Anterior Muscles |
|---|---|---|
| Medial gastrocnemius (P) | Tibialis anterior (D) | Tibialis posterior (P) |
| Lateral gastrocnemius (P) | Fibularis longus (P) | Flexor digitorum longus (P) |
| Plantaris (P) | Extensor digitorum longus (D) | Flexor hallucis longus (P) |
| Soleus (P) | Fibularis brevis (P) | |
| Extensor hallucis longus (D) |
Table 2.1.
Quiet Standing Balance Test Conditions.
| Balance Condition | Description |
|---|---|
| EOFT | Eyes Open, Feet Together |
| ECFT | Eyes Closed, Feet Together |
| EOTanDF | Eyes Open, Feet Tandem, Dominant Foot Forward |
| ECTanDF | Eyes Closed, Feet Tandem, Dominant Foot Forward |
| EOTanDB | Eyes Open, Feet Tandem, Dominant Foot Back |
| ECTanDB | Eyes Closed, Feet Tandem, Dominant Foot Forward |
Table 2.2.
Neural Frequency Bands of Interest.
| Bands | Range (Hz) |
|---|---|
| Delta | 0 - 4 |
| Theta | 4 – 8 |
| Apha | 8 – 13 |
| Beta | 13 – 30 |
| Lower Gamma | 30 – 60 |
| Upper Gamma | 60 - 100 |
Table 2.3.
Muscle Pairs Analyzed.
| Left Unilateral | Right Unilateral | Bilateral Homologous |
|---|---|---|
| LTA:LMG | RTA:RMG | LTA:RTA |
| LTA:LS | RTA:RS | LMG:RMG |
| LMG:LS | RMG:RS | LS:RS |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



