Submitted:
15 November 2024
Posted:
18 November 2024
You are already at the latest version
Abstract
Hepatocellular carcinoma (HCC) covers a malignant form of primary liver cancer. Intricate networks linking to the host immune system may be associated with the pathogenesis of HCC. A huge amount of interdisciplinary medical information for the treatment of HCC has been accumulated over the most recent years. For example, advances in new immunotherapy have improved the result of treatment for the HCC. Advantageously, this approach can be combined with standard conventional treatments such as surgical resection to improve the therapeutical consequence. However, several toxic effects of the treatments may stand a significant threat to human health. Now, the shift in mindset is important for the concept of superior cancer therapy, in which probiotics-therapy may be inspired at least within the warranty of safety. The interplay among the gut microbiota and immune system could affect the efficacy of several anticancer treatments including immune checkpoint therapy via the alteration of Th17 cell functions against various malignant tumors. Here, some of the recent anticancer techniques are discussed, in which the growth of HCC might be effectively repressed with safety.
Keywords:
hepatocellular carcinoma
; cancer therapy
; immune checkpoint
; probiotics
; gut microbiota
; ROS
; engram theory
; NAFLD
1. Introduction
Main liver cancers containing hepatocellular carcinoma (HCC) are the second most lethal cancer in global. The HCC is nearly constituting more than 3 quarters of malignant cases, which is so aggressive malignancy that it has been a social healthcare problem [1]. Medical treatments for HCC are decided on the clinical stages of the disease. Local therapies such as resection including hepatectomy, ablation, and/or irradiation are the traditional treatment for the early stages of HCC [2]. Surgical management may be the most vital method for HCC patients to achieve long-term survival. However, the 5-year survival rate might not be satisfactory with considerable rate of patients relapsing within 5 years [3]. In addition, the HCC is frequently detected at the point of unresectable advanced stages [4], which may be rendering the cure rate extremely low [5]. Thoughtlessly, systematic palliative management might be the opportunity for most patients with radical-stages of HCC [6]. Although the viral hepatitis, hepatitis B virus (HBV) and hepatitis C virus (HCV), is one of the most substantial reason for the development of HCC, alcoholic liver disease (ALD) and/or nonalcoholic fatty liver disease (NAFLD) may also be the conspicuous reason for the development of HCC [7]. The ingestion of high fat in addition to bacterial endotoxins might be the probable pathogenesis of NAFLD and HCC [8]. In addition, liver fibrosis, aflatoxin-induced liver toxicity, diabetes, smoking, and immune-related diseases including autoimmune hepatitis could also be important risk factors for HCC [9,10]. Interestingly, increasing evidence has directed to an important role of the gut microbiota and/or their various metabolites in the development of HCC. Because an imbalance in the composition of gut microbiota may result in chronic inflammation and/or the development of NAFLD or HCC [11,12] (Figure 1).
Preoperative medical factors such as anesthesia, hypothermia, and systemic inflammatory responses may support to the micro-relapse of early cancers [13]. In addition, a problem of surgical removal of tumors may be the risk of detaching cancer cells into systemic circulation [13]. Occult microscopic cancers in different organs including prostate and/or breast are common in over-all population [14]. Under these conditions, an immunotherapy synergizes with radiotherapy enhancing their antitumor reactions with favorable clinical consequences [15]. Subsequently, not all patients may exhibit greater efficiencies of the combined radioimmunotherapy [16,17]. Hence, further optimization might be more helpful [18]. In general, cancer therapy promotes reactive oxygen species (ROS) [19], which could produce more or less inflammation in non-target organs [20]. Additionally, cytotoxic lymphocytes, neutrophils, and/or macrophages might move to the inflammation spot to clear damaged cells [21]. Inflammatory cells may secrete various chemokines, cytokines, and growth factors, which could accidentally promote the cell growth of tumors. [22]. In these ways, resection surgery is the primary treatment method, however, which has a high recurrence rate. Adverse reactions of anti-cancer drugs may occur more severely than those of other treatment drugs, which might furthermore damage healthy cells. In addition, the treatment effect would be reduced and/or even vanished by the development of drug resistance [23]. Some arrangement of chemotherapeutic drugs with radiation therapy had been one of the most promising strategies giving improved survival of various cancers [24].
Inventions in technology and operative technique have required to further improve survival [25]. Particularly, newfangled treatments with few side effects had been immediately required. Here, we discuss some of the recent anticancer procedures or tactics, which could effectively contribute to the inhibition of HCC growth. This paper also attempts to generalize modern cancer therapeutics in terms of hypothetical cancer physiology. We then fall into the specific effects of future concept for the superior cancer treatment with the combination of probiotics proficiency.
2. Possible Recent Cancer Therapies Against Hepatocellular Carcinoma
Photothermal therapy (PTT) and photodynamic therapy (PDT) are relatively new strategies for cancer therapy, which are therapeutic methods with low toxicities utilizing photosensitizers preferentially accumulating in tumor tissue. The PTT and PDT have gradually emerged because of their spatial selectivity and/or relatively lower resistance, which could be utilized in the combination with other therapeutic modalities such as chemotherapy and/or immunotherapy. Usually, the PTT uses photosensitizers with specific light absorption to convert into heat energy for eliminating cancer cells, while the PDT exploits photosensitizers to yield ROS in the existing of particular wavelengths of light. The PTT could cause relatively little damage to surrounding healthy cells, since thermal effects only occur when specific light is applied in the presence of photosensitizers [26]. When the tumor tissues are exposed to the specific light, the activated photosensitizers might produce ROS in the usage of PDT, which could damage tumor cells and/or the neovascularization to tumores [27]. Photosensitizers for PTT and/or PDT may contain several nanoparticles, metal materials, and carbon-based materials [28]. Prostate cancer is one of the most common cancers in men and is asymptomatic in the early stage of the cancer with favorable indication of PTT/PDT therapies. PTT/PDT might considerably improve the outcome even in advanced prostate cancer with reduced systemic toxicity. In addition to these therapies, laser-induced PTT against HCC has attracted extensive attentions because of its strong tissue penetration with favorable biosafety [29]. Moreover, several data have also confirmed the inhibitory effect of PDT in tumor cells growth both in HCC and cholangiocarcinoma [30].
Procedures with immune checkpoint inhibition might be one of the most successful therapies for a number of cancers [31], which may activate specific immune cells such as CD3+ T-cell via the inhibition of a family of signaling receptors expressed on the surface of lymphocytes [32]. The signaling of immune checkpoints is indispensable in preventing excessive immune responses that could result in damaging to the host tissues [33]. Hence, their inhibition has been recognized to be a potent therapeutic mechanism in certain tumors [34]. Frequently used immune checkpoint inhibitors against various tumors may be made up of beneficial monoclonal antibodies such as ipilimumab, which can target the immune checkpoint of programmed cell death protein-1 (PD-1) and/or cytotoxic T-lymphocyte-associated protein 4 (CTLA4) [35]. Immunotherapy with these immune checkpoint inhibitors has been developed to applications in patients with a wide range of advanced cancers including Hodgkin's lymphoma, melanoma, non-small cell lung cancer, and head and neck squamous cell carcinoma [36]. It is amazing that application of the immunotherapy could achieve complete responses within an approximately 30% of patients [37]. Immune checkpoint inhibitors have been also permitted for the clinical usage as to HCC treatment, which have revealed considerable efficacy in many clinical trials afterwards [38]. Thus far, programmed cell death ligand 1 (PD-L1), CTLA-4, PD-1, and/or several other immune molecules seems to be connected with their effectiveness for the advanced cancer therapy, also being associated to the modification of tumor microenvironment [39]. Each treatments could result in the stimulation of an anti-cancer immune system for killing cancer cells [40]. Favorably, almost few side effect has been noticed except reversible minor adverse events [41,42,43]. Mechanistically, the physiological association between the PD-1/PD-L1 pathway and both Th17/Treg cells has been shown, which may suggest a crucial role of PD-1/PD-L1 in the regulation of Th17/Treg cells [44]. Likewise, CTLA-4 therapy could also support Th17 cells [45]. In addition, the obstruction of CTLA-4 signaling could further inhibit the function of Treg cells [46]. Amazingly, IL-17 and its main supply Th17 cells could upregulate PD-L1 expression, which may impede the efficacy of the immunotherapy [47]. Furtheremore, Th17 cells are unaffected to a steroid therapy [48]. Interaction of PD-1 with PD-L1 might trigger a reduction of PI3K signaling in T-lymphocytes leading to the introduction of Treg cells [49]. Th17 cells can ultimately differentiate into suppressive Treg cells [50], which may provide as a source of tumor-associated Treg cells. Therefore, excessive inflammation with Th17 cells might play imperative roles in some of inflammation-associated carcinogenesis [51], also targeting several specific antigens presented in malignant cancer cells [52]. The strategies to overcome this immune therapy-resistance of cancer cells seem to be moving toward an intensified strategy comprising a procedure with low adverse events.
With recent advances, chimeric antigen receptor (CAR) immunotherapy has similarly become a favorable modality for patients with refractory cancers. CAR immunotherapies commonly utilize synthetic constructs that can bind to a specific target antigen in a major histocompatibility complex (MHC) independent manner. In general, the MHC could trigger a strong T cell activation directing to the removal of target cells. The successful results of CAR-T cell therapy in relapsed and/or refractory B-cell malignancies have shifted the paradigm of this immunotherapy by appearing the medical attention for the treatment of various solid tumors [53,54]. Afterward, the CAR-T immunotherapy has also achieved promising success in the treatment of HCC [55,56]. Identification of more specific targets in HCC might improve the therapeutic potential of CAR-T in the future [57].
Oncolytic virus therapy characterizes an effectual immunotherapeutic approach againse cancers. The oncolytic virus may stimulate antitumor responses both through tumor cell-specific cell lysis and by the activation of certain immune system. Some viruses are naturally capable of killing cancer cells [58]. With the genetic engineering modification, virus mutants with oncolytic activity could be just restricted to tumor cells, which might reduce the virus-induced non specific toxicity in normal tissues/organs. There is growing evidence that the success of oncolytic virus therapy may depend on the tumor microenvironment [58], which is considered to be the most promising cancer treatment along with surgery, chemotherapy, and radiotherapy [59]. Some evidence for the application of oncolytic viruses therapy in HCC have been suggested [60]. In addition, oncolytic vaccinia virus could significantly enhance the cytotoxicity in HCC through the activation of PI3K/AKT signaling pathways [61].
3. A New Concept for the Cancer Therapy
Oncology is one of the most interdisciplinary research fields. In addition, a wide range of diagnostic and/or treatment technologies are accessible. Even though cancer has been comprehensively studied in these ways, a shift in mindset might be required for the concept of forthcoming cancer therapy. The efficacy of treatment procedures might principally depend on the balance between cure efficacy and toxicity. In this meaning, probiotics could have been used at least as an adjunctive therapy for the cancer treatments [62,63]. Humans and bacteria have a symbiotic relationship, which sustain substantial influences on our health. Interestingly, some bacteria strains have been identified to possess therapeutic capability for anticancer activities [64]. Residential bacteria have been identified everywhere in tissues even including brains, kidneys, placenta, and/or breast [65]. Some bacteria could surely affect the growth of solid tumors. On the contrary, it has been shown that Helicobacter pylori has been proved to increase the risk of developing gastric cancer [65]. In addition, enterotoxins of B. fragilis may contribute to the cancer development through the activation of signal transducer and activator of transcription (STAT) signaling [66]. However, certain commensal bacteria may inhibit the development and/or progression of inflammatory bowel disease-related cancer [67]. Similarly, it has been reported that Saccharomyces boulardii (S. boulardii) may effectively reduce the carcinogenesis in an AOM/DSS induced mouse model [68]. In addition, Clostridium butyricum could enforce the inhibitory effect on the inflammation in mouse intestine [69]. A strain of Salmonella typhimurium could cause cell death for prostate cancer cell lines via various mechanisms [70]. Moreover, Clostridium novyi could also cause direct cytotoxicity via the disruption of lipid bilayers of cancer cells [71]. Interestingly, the therapeutic bacteria could positively colonize in hypoxic areas of malignant tumors [72]. It has been shown that the combination of Salmonella typhimurium with traditional cancer chemotherapies could prolong the survival in mice [73]. Consequently, many bacteria-based cancer therapies have proceeded through clinical trials [74]. In addition, the application of bacteria-based cancer therapies may cover several side effects in the treatment of radiotherapy and/or chemotherapy [74]. Particularly, certain probiotics could reduce the incidence of cancer therapy-related side effects such as oral mucositis and/or diarrhea [75]. Studies regarding E. coli, Salmonella Typhimurium, Salmonella Clostridium and other strains have demonstrated that bacteria-based cancer therapies combined with radiotherapy could reduce radiation-associated adverse damages [76,77], which could also improve the therapeutic effect and prognosis [78,79]. However, the behavior of association with cancer cells, bacteria, and immune cells during the bacteria-based cancer therapies should need more in-depth investigation.
It has been reported that interrelationship between the immune system and the gut microbiome could determine the effectiveness of the cancer immunotherapy [80]. Therefore, modulation of the gut microbiome could optimize therapeutic outcomes upon immune-checkpoints blockade therapy. For example, it has been reported that L. acidophilus combined with anti-CTLA4 antibody blockade could enhance the antitumor immunity by synergistically improving antitumor T cell immunity in mouse model [81]. In addition, the antitumor effects of CTLA4 blockade may be determined by Bacteroides species including B. thetaiotaomicron and/or B. fragilis [82]. Consistenly, malignant tumor cells in antibiotic-treated mice had no response to CTLA4 blockade, suggesting that the beneficial bacteria may be deceased by the use of antibiotics [82,83]. Thus, savage with the B. fragilis could retrieve the effectiveness of CTLA4 blockade [83]. In addition, F. prausnitzii has anti-inflammatory properties recognized in colitis model animals [84], in which butyrate produced by the F. prausnitzii could improve the Th17/Treg balance for exhibiting anti-inflammatory effects [85]. In these ways, the relationship between gut microbiota and cancer treatment has been studied [86].
4. Epigenetics with Gut Microbiota Involved in Superior Cancer Therapy
Evolving evidence connects a crucial role of gut microbiota in liver inflammation and/or the development of HCC [87]. Undoubtedly, the gut-liver axis might be the vital mechanism by which the gut microbiota could promote various liver diseases including HCC [88]. For instance, dietary cholesterol could induce the alteration of gut bacterial metabolites, which might be involved in NAFLD-associated HCC [89]. In addition, gut microbiota dysfunction may trigger a neutrophils accumulation into the gut epithelium that could change the composition of inflammatory cytokine, which may activate the T helper 17 (Th17) cells [90]. The intra-tumoral areas of HCC might be often in an immunosuppressive situation [[91], which contain an amount of regulatory T (Treg) cells developing a link to help the immune escaping [[92]. Correspondingly, increased quantities of Th17 cells have been detected in tumor tissue [[93] and/or even in peripheral blood [[94] of the patients with HCC, however, which might be linked to negative disease outcomes [93,95]. Comparable results have also been observed in animal models, whereby limiting expansion of Th17 cells might decrease the growth of transplanted liver tumors in animal model [[96]. The gut may be a possible site of Th17 cell production. In addition, gut microbiota might influence the differentiation of Th17 cells via regulating the function of dendritic cells [97]. Accordingly, there may be an intricate association between the development of Th17 cells and the progression of HCC with the role of gut microbiota (Figure 2).
The resource of tumor-associated immune Th17 cells might be also linked to the gut [98]. Furthermore, Th17 cells appear to be associated with the HCC development, possibly via facilitating the angiogenesis of tumors [96,99]. Remarkably, modification of the gut microbiota could assist to avoid the incidence of the HCC [100]. Therefore, the alteration of gut microbiota may coincidentally induce the tumor development. Actually, gut bacterial metabolites have been known to play a role in the carcinogenesis of various cancers [101,102]. Besides, adjustment of gut microbiota reveals effective procedure of strengthening the anti-tumor immunity, which implies a close linking between gut microbiota and the oncopathogenic mechanisms of tumors [103]. The usage of several methods including probiotics and/or the fecal microbiota transplantation (FMT) may develop new models with the potential expediency available for HCC therapy. Especially, Th17 cells appear to be an advanced therapeutic target against certain situations of cancer-promotion such as excess production of ROS and/or severe inflammation. Tactics with employing probiotics and/or FMT could be advantageous at least to slow down the growth of HCC.
Collecting evidence shows the association of dysbiosis in the HCC development. Some intestinal bacteria isolated from patients with NASH may present an increase in Klebsiella pneumoniae strains [104]. In addition, the predominant bacteria in patients with HCC-cirrhosis are Clostridium and Paraprevotellaceae family [105]. Depletion of these bacteria by antibiotics might prevent the HCC progression. In addition, some of antibiotic treatments may decrease the liver tumor growth via the control of natural killer T cell accumulation [106]. Now, the gut microbiome has appeared as an important factor regulating antitumor immunity governing the efficacy of chemo- and/or novel immunotherapies [107,108,109]. Liver may possibly be exposed to bacterial components and their metabolites via the portal vein, in which the gut microbiome could regulate to the development of HCC [110,111]. Therefore, gut commensal bacteria are potential targets for controlling the liver tumorigenesis. Interestingly, it has been shown that patients with HCC have been identified to possess a higher proportion of Akkermansia muciniphila and Ruminococcaceae spp. [112]. The function of commensal bacteria might play a key role in keeping the cancer related immune homeostasis in the host [113].
5. Relationship Between Gut Microbiota and Epigenetics for the Superior Therapy Against HCC
Epigenetic regulations incorporating modifications in DNA methylation, epigenetic silencing of microRNAs, histone phosphorylation, and histone acetylation may be innate alterations in gene expression [114]. These regulations have been realized to play a substantial role in carcinogenesis and/or for antitumor immunity [115]. Therefore, the application of epigenetic technology could be promising for enhancing the effectiveness of existing immunotherapies. It is becoming clear that epigenetics can play a significant role in carcinogenesis by altering the gene expression [116,117,118]. Tumoral bacteria may lead to cancer initiation and/or development by inducing the epigenetic alterations as well as the modulation of host immunity [119]. For example, some events from gut microbiota have been shown in considerable responses by CD4+/CD8+ T cell effector subpopulations [120]. On the other hand, pathogenic bacteria could play a significant role in the dysregulation of the epigenetic machinery of their target cells. Alterations in the gene expression pattern can interfere with the activity of several immune responses [121]. In addition, gut microbiota could enhance the effector cytokine production by adjustment of their epigenetic signatures [122]. The gut microbiota may also affect immune responses both directly and indirectly via the microbiota-derived metabolites [123]. Roles of gut microbiome in cancer should be understand more precisely and more research in this field might be required.
Epigenetics with the adjustment of gut microbiota may be a favorable modulator of cancer therapies. For example, it has been shown that combining PTT with an epigenetic therapy could provoke advantageous immunomodulatory responses that result in improved survival in mice, in which the epigenetic therapy could improve the response to PTT by delaying the timing of tumor recurrence [124]. Similarly, it has also been shown that epigenetic modification of tumour antigens levels may be a novel approach to further enhance the effectiveness of PDT cancer therapy [125]. Moreover, epigenetic treatments based on administration of methyltransferase inhibitors in combination with PDT could offer effective mechanisms leading to development of antitumor immunity with potentiated antitumor effects [126]. Other new modalities of targeted therapy and/or immunotherapy such as CAR-T cell treatment, cancer vaccines, and/or oncolytic viral treatment might be also favorable with the appropriate gut microbiome for the epigenetic modification of tumour antigens levels, which could be some extra weapons against aggressive tumors [127]. Probiotics have been found to be helpful in many diseases, however, they do not always seem to be absolutely safe [128,129]. Consideration of risk-benefit ratio before setting this therapy should be recommended. Supervision is also mandatory to assess the security and effectiveness of the alteration of gut microbiome [130]. For example, probiotics could be responsible for systemic infections including inflammatory diseases and/or sepsis [131]. Probiotic bacteria have been also recognized as spontaneous factors of endometritis, urinary tract infections, meningitis, and spleen abscesses [132,133]. In addition, probiotic bacteria may result in chronic diarrhea, which might very slightly increase the risk of colorectal cancer [134]. Through interference with commensal microflora appropriately, they could result in honorable performances in the host.
6. Future Perspectives
The treatment of HCC has been drastically changing. Likewise, immunotherapy has turned out a breakthrough to inhibit the growth of tumor cells by activating an antitumor immunity for various cancers, which has revolutionized treatment strategies with increasing the chance of survival for cancer patients. [135]. These immunotherapies might also improve the survival of the HCC even in advanced stages [136]. Moreover, this strategy could be further empowered by an adapted patient selection. Gut microbiota-derived metabolites such as short-chain fatty acids (SCFAs) could be involved in the control of inflammation, which might be associated with the immune power shift beneficial for the cancer treatment [137]. Certain diet may also be responsible for the gut dysbiosis which is an important factor for the therapeutic outcomes [138]. In addition, commensal bacteria are imperative in coordinating antitumor responses in the tumor microenvironment [139,140], which is the key interface between cancer cells and anticancer T-cells [141]. In this regards, we have reported an interesting relatiohship among the gut microbiota, cancer cells and immune T-cells by an “engram theory” for the innovative treatment of colon cancer in mice model [67,142] (Figure 3). Further investigations are required to understand the molecular mechanisms to develop treatment strategies and to get favorable clinical outcomes, which should focus on the design of patient-tailored cancer therapeutics by manipulating diverse microbiota-derived molecules.
Many studies have been shown that the important crosstalks between cancer cells and cancer stem cells in a tumor microenvironment [143]. Cancer stem cells have been shown to develop neovascularization by expressing various angiogenic factors for the tumor growth [144]. Come to think of it, the progression of cancers may rely on the function of some host components such as gut microbiota and/or tumor microenvironment with close relation each other. Again, a shift in mindset may be required for the concept of forthcoming cancer therapy. Probiotics may be now promising not only for the cancer therapy, but also for the treatment of neurodegenerative disorders [145]. Henceforth, we now believe that the application of probiotics and/or FMT could expand for the treatment of autoimmune disease and the related inflammatory diseases. Consequently, huge number of researchers need to be united to comprehend the molecular mechanisms as well as to obtain some clues of therapeutic intervention against those intractable diseases.
Author Contributions
Conceptualization, MN, AF, and SM; original draft preparation and editing, MN and SM; visualization, MN and SM; supervision, SM. Each author (MN, AF, and SM) has participated sufficiently in this work of drafting the article and/or revising the article for the important rational content. Then, all authors gave final approval of the version to be submitted. Finally, all authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
Not applicable.
Acknowledgments
Not applicable.
Conflicts of Interest
The authors declare that they have no competing financial interests.
Abbreviations
HCV hepatitis C virus ()
| CAR | chimeric antigen receptor |
| CTLA4 | cytotoxic T-lymphocyte-associated protein 4 |
| FMT | fecal microbiota transplantation |
| HBV | hepatitis B virus |
| HCC | hepatocellular carcinoma |
| LPS | lipopolysaccharide |
| MHC | major histocompatibility complex |
| NAFLD | nonalcoholic fatty liver disease |
| PD-1 | programmed cell death protein-1 |
| PD-L1 | programmed cell death protein ligand-1 |
| PDT | photodynamic therapy |
| PTT | photothermal therapy |
| ROS | reactive oxygen species |
| SCFAs | short-chain fatty acids |
| STAT | signal transducer and activator of transcription |
| Th17 | T helper 17 cell |
| TLRs | toll-like receptors |
| Treg | regulatory T cell |
| VEGF | vascular endothelial growth factor A |
References
- Bray, F.; Ferlay, J.; Soerjomataram, I.; Siegel, R.L.; Torre, L.A.; Jemal, A. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. 2018, 68(6), 394–424. [Google Scholar] [CrossRef] [PubMed]
- Canale, M.; Ulivi, P.; Foschi, F.G.; Scarpi, E.; De Matteis, S.; Donati, G.; Ercolani, G.; Scartozzi, M.; Faloppi, L.; Passardi, A.; et al. Clinical and circulating biomarkers of survival and recurrence after radiofrequency ablation in patients with hepatocellular carcinoma. Crit Rev Oncol Hematol. 2018, 129, 44–53. [Google Scholar] [CrossRef]
- Choi, J.W.; Lee, J.M.; Lee, D.H.; Yoon, J.H.; Kim, Y.J.; Lee, J.H.; Yu, S.J.; Cho, E.J. Radiofrequency ablation using internally cooled wet electrodes in bipolar mode for the treatment of recurrent hepatocellular carcinoma after locoregional treatment: A randomized prospective comparative study. PLoS One. 2020, 15(9), e0239733. [Google Scholar] [CrossRef] [PubMed]
- Ilagan, C.H.; Goldman, D.A.; Gönen, M.; Aveson, V.G.; Babicky, M.; Balachandran, V.P.; Drebin, J.A.; Jarnagin, W.R.; Wei, A.C.; Kingham, T.P.; et al. Recurrence of Hepatocellular Carcinoma After Complete Radiologic Response to Trans-Arterial Embolization: A Retrospective Study on Patterns, Treatments, and Prognoses. Ann Surg Oncol. 2022, 29(11), 6815–6826. [Google Scholar] [CrossRef] [PubMed]
- Bruix, J.; Qin, S.; Merle, P.; Granito, A.; Huang, Y.H.; Bodoky, G.; Pracht, M.; Yokosuka, O.; Rosmorduc, O.; Breder, V.; et al. Regorafenib for patients with hepatocellular carcinoma who progressed on sorafenib treatment (RESORCE): a randomised, double-blind, placebo-controlled, phase 3 trial. Lancet. 2017, 389(10064), 56–66. [Google Scholar] [CrossRef]
- Hu, W.Y.; Wei, H.Y.; Li, K.M.; Wang, R.B.; Xu, X.Q.; Feng, R. LINC00511 as a ceRNA promotes cell malignant behaviors and correlates with prognosis of hepatocellular carcinoma patients by modulating miR-195/EYA1 axis. Biomed Pharmacother. 2020, 121, 109642. [Google Scholar] [CrossRef]
- Ma, C.; Kesarwala, A.H.; Eggert, T.; Medina-Echeverz, J.; Kleiner, D.E.; Jin, P.; Stroncek, D.F.; Terabe, M.; Kapoor, V.; ElGindi, M.; et al. NAFLD causes selective CD4(+) T lymphocyte loss and promotes hepatocarcinogenesis. Nature. 2016, 531(7593), 253–257. [Google Scholar] [CrossRef] [PubMed]
- Mehal, W.Z. The Gordian Knot of dysbiosis, obesity and NAFLD. Nat Rev Gastroenterol Hepatol. 2013, 10(11), 637–644. [Google Scholar] [CrossRef]
- Villanueva, A. Hepatocellular Carcinoma. N Engl J Med. 2019, 380(15), 1450–1462. [Google Scholar] [CrossRef] [PubMed]
- Chen, W.; Desert, R.; Ge, X.; Han, H.; Song, Z.; Das, S.; Athavale, D.; You, H.; Nieto, N. The Matrisome Genes From Hepatitis B-Related Hepatocellular Carcinoma Unveiled. Hepatol Commun. 2021, 5(9), 1571–1585. [Google Scholar] [CrossRef] [PubMed]
- Quesada-Vázquez, S.; Bone, C.; Saha, S.; Triguero, I.; Colom-Pellicer, M.; Aragonès, G.; Hildebrand, F.; Del Bas, J.M.; Caimari, A.; Beraza, N.; et al. Microbiota Dysbiosis and Gut Barrier Dysfunction Associated with Non-Alcoholic Fatty Liver Disease Are Modulated by a Specific Metabolic Cofactors' Combination. Int J Mol Sci. 2022, 23((22)), 13675. [Google Scholar] [CrossRef] [PubMed]
- Guo, X.; Okpara, E.S.; Hu, W.; Yan, C.; Wang, Y.; Liang, Q.; Chiang, J.Y.L.; Han, S. Interactive Relationships between Intestinal Flora and Bile Acids. Int J Mol Sci. 2022, 23(15), 8343. [Google Scholar] [CrossRef] [PubMed]
- Tohme, S.; Simmons, R.L; Tsung, A. Surgery for Cancer: A Trigger for Metastases. Cancer Res. 2017, 77(7), 1548–1552. [Google Scholar] [CrossRef]
- Goldstein, M.R.; Mascitelli, L. Surgery and cancer promotion: are we trading beauty for cancer? QJM. 2011, 104(9), 811–815. [Google Scholar] [CrossRef]
- Shaverdian, N.; Lisberg, A.E.; Bornazyan, K.; Veruttipong, D.; Goldman, J.W.; Formenti, S.C.; Garon, E.B.; Lee, P. Previous radiotherapy and the clinical activity and toxicity of pembrolizumab in the treatment of non-small-cell lung cancer: a secondary analysis of the KEYNOTE-001 phase 1 trial. Lancet Oncol. 2017, 18(7), 895–903. [Google Scholar] [CrossRef]
- Seiwert, T.Y.; Kiess, A.P. Time to Debunk an Urban Myth? The "Abscopal Effect" With Radiation and Anti-PD-1. J Clin Oncol. 2021, 39(1), 1–3. [Google Scholar] [CrossRef]
- Chen, D.; Verma, V.; Patel, R.R.; Barsoumian, H.B.; Cortez, M.A.; Welsh, J.W. Absolute Lymphocyte Count Predicts Abscopal Responses and Outcomes in Patients Receiving Combined Immunotherapy and Radiation Therapy: Analysis of 3 Phase 1/2 Trials. Int J Radiat Oncol Biol Phys. 2020, 108(1), 196–203. [Google Scholar] [CrossRef]
- Zhai, D.; An, D.; Wan, C.; Yang, K. Radiotherapy: Brightness and darkness in the era of immunotherapy. Transl Oncol. 2022, 19, 101366. [Google Scholar] [CrossRef]
- Terasaki, Y.; Ohsawa, I.; Terasaki, M.; Takahashi, M.; Kunugi, S.; Dedong, K.; Urushiyama, H.; Amenomori, S.; Kaneko-Togashi, M.; Kuwahara, N.; et al. Hydrogen therapy attenuates irradiation-induced lung damage by reducing oxidative stress. Am J Physiol Lung Cell Mol Physiol. 2011, 301(4), L415–426. [Google Scholar] [CrossRef] [PubMed]
- Lundgren, S.; Karnevi, E.; Elebro, J.; Nodin, B.; Karlsson, M.C.I.; Eberhard, J.; Leandersson, K.; Jirström, K. The clinical importance of tumour-infiltrating macrophages and dendritic cells in periampullary adenocarcinoma differs by morphological subtype. J Transl Med. 2017, 15(1), 152. [Google Scholar] [CrossRef]
- Ryter, S.W.; Kim, H.P.; Hoetzel, A.; Park, J.W.; Nakahira, K.; Wang, X.; Choi, A.M. Mechanisms of cell death in oxidative stress. Antioxid Redox Signal. 2007, 9(1), 49–89. [Google Scholar] [CrossRef] [PubMed]
- Siegel, R.J.; Singh, A.K.; Panipinto, P.M.; Shaikh, F.S.; Vinh, J.; Han, S.U.; Kenney, H.M.; Schwarz, E.M.; Crowson, C.S.; Khuder, S.A.; et al. Extracellular sulfatase-2 is overexpressed in rheumatoid arthritis and mediates the TNF-α-induced inflammatory activation of synovial fibroblasts. Cell Mol Immunol. 2022, 19(10), 1185–1195. [Google Scholar] [CrossRef]
- Raguz, S.; Yagüe, E. Resistance to chemotherapy: new treatments and novel insights into an old problem. Br J Cancer. 2008, 99(3), 387–391. [Google Scholar] [CrossRef]
- Choy, H.; Kim, D.W. Chemotherapy and irradiation interaction. Semin Oncol. 2003, 30(4 Suppl 9), 3–10. [Google Scholar] [CrossRef]
- McGuigan, A.; Kelly, P.; Turkington, R.C.; Jones, C.; Coleman, H.G.; McCain, R.S. Pancreatic cancer: A review of clinical diagnosis, epidemiology, treatment and outcomes. World J Gastroenterol. 2018, 24(43), 4846–4861. [Google Scholar] [CrossRef] [PubMed]
- Jung, H.S.; Verwilst, P.; Sharma, A.; Shin, J.; Sessler, J.L.; Kim, J.S. Organic molecule-based photothermal agents: an expanding photothermal therapy universe. Chem Soc Rev. 2018, 47(7), 2280–2297. [Google Scholar] [CrossRef] [PubMed]
- Fan, Z.; Zhuang, C.; Wang, S.; Zhang, Y. Photodynamic and Photothermal Therapy of Hepatocellular Carcinoma. Front Oncol. 2021, 11, 787780. [Google Scholar] [CrossRef]
- Li, X.; Lovell, J.F.; Yoon, J.; Chen, X. Clinical development and potential of photothermal and photodynamic therapies for cancer. Nat Rev Clin Oncol. 2020, 17(11), 657–674. [Google Scholar] [CrossRef]
- Dun, X.; Liu, S.; Ge, N.; Liu, M.; Li, M.; Zhang, J.; Bao, H.; Li, B.; Zhang, H.; Cui, L. Photothermal effects of CuS-BSA nanoparticles on H22 hepatoma-bearing mice. Front Pharmacol. 2022, 13, 1029986. [Google Scholar] [CrossRef]
- Casini, A.; Leone, S.; Vaccaro, R.; Vivacqua, G.; Ceci, L.; Pannarale, L.; Franchitto, A.; Onori, P.; Gaudio, E.; Mancinelli, R. The Emerging Role of Ferroptosis in Liver Cancers. Life (Basel). 2022, 12(12), 2128. [Google Scholar] [CrossRef] [PubMed]
- Kaufmann, S.H.E.; Dorhoi, A.; Hotchkiss, R.S.; Bartenschlager, R. Host-directed therapies for bacterial and viral infections. Nat Rev Drug Discov. 2018, 17(1), 35–56. [Google Scholar] [CrossRef] [PubMed]
- Dyck, L.; Mills, K.H.G. Immune checkpoints and their inhibition in cancer and infectious diseases. Eur J Immunol. 2017, 47(5), 765–779. [Google Scholar] [CrossRef] [PubMed]
- Wei, S.C.; Duffy, C.R.; Allison, J.P. Fundamental Mechanisms of Immune Checkpoint Blockade Therapy. Cancer Discov. 2018, 8(9), 1069–1086. [Google Scholar] [CrossRef] [PubMed]
- Ribas, A.; Wolchok, J.D. Cancer immunotherapy using checkpoint blockade. Science. 2018, 359(6382), 1350–1355. [Google Scholar] [CrossRef]
- Korman, A.J.; Peggs, K.S.; Allison, J.P. Checkpoint blockade in cancer immunotherapy. Adv Immunol. 2006, 90, 297–339. [Google Scholar] [PubMed]
- Bagchi, S.; Yuan, R.; Engleman, E.G. Immune Checkpoint Inhibitors for the Treatment of Cancer: Clinical Impact and Mechanisms of Response and Resistance. Annu Rev Pathol. 2021, 16, 223–249. [Google Scholar] [CrossRef]
- Andrews, L.P.; Yano, H.; Vignali, D.A.A. Inhibitory receptors and ligands beyond PD-1, PD-L1 and CTLA-4: breakthroughs or backups. Nat Immunol. 2019, 20(11), 1425–1434. [Google Scholar] [CrossRef]
- Donisi, C.; Puzzoni, M.; Ziranu, P.; Lai, E.; Mariani, S.; Saba, G.; Impera, V.; Dubois, M.; Persano, M.; Migliari, M.; et al. Immune Checkpoint Inhibitors in the Treatment of HCC. Front Oncol. 2021, 10, 601240. [Google Scholar] [CrossRef] [PubMed]
- Lai, E.; Astara, G.; Ziranu, P.; Pretta, A.; Migliari, M.; Dubois, M.; Donisi, C.; Mariani, S.; Liscia, N.; Impera, V.; et al. Introducing immunotherapy for advanced hepatocellular carcinoma patients: Too early or too fast? Crit Rev Oncol Hematol. 2021, 157, 103167. [Google Scholar] [CrossRef] [PubMed]
- Greten, T.F.; Lai, C.W.; Li, G.; Staveley-O'Carroll, K.F. Targeted and Immune-Based Therapies for Hepatocellular Carcinoma. Gastroenterology. 2019, 156(2), 510–524. [Google Scholar] [CrossRef]
- Katariya, N.N.; Lizaola-Mayo, B.C.; Chascsa, D.M.; Giorgakis, E.; Aqel, B.A.; Moss, A.A.; Uson Junior, P.L.S.; Borad, M.J.; Mathur, A.K. Immune Checkpoint Inhibitors as Therapy to Down-Stage Hepatocellular Carcinoma Prior to Liver Transplantation. Cancers (Basel). 2022, 14(9), 2056. [Google Scholar] [CrossRef] [PubMed]
- Abdelrahim, M.; Esmail, A.; Saharia, A.; Abudayyeh, A.; Abdel-Wahab, N.; Diab, A.; Murakami, N.; Kaseb, A.O.; Chang, J.C.; Gaber, A.O.; et al. Utilization of Immunotherapy for the Treatment of Hepatocellular Carcinoma in the Peri-Transplant Setting: Transplant Oncology View. Cancers (Basel). 2022, 14(7), 1760. [Google Scholar] [CrossRef] [PubMed]
- Hewitt, D.B.; Rahnemai-Azar, A.A.; Pawlik, T.M. Potential experimental immune checkpoint inhibitors for the treatment of cancer of the liver. Expert Opin Investig Drugs. 2021, 30(8), 827–835. [Google Scholar] [CrossRef]
- Zhang, Y.; Liu, Z.; Tian, M.; Hu, X.; Wang, L.; Ji, J.; Liao, A. The altered PD-1/PD-L1 pathway delivers the 'one-two punch' effects to promote the Treg/Th17 imbalance in pre-eclampsia. Cell Mol Immunol. 2018, 15(7), 710–723. [Google Scholar] [CrossRef] [PubMed]
- Kim, S.T.; Chu, Y.; Misoi, M.; Suarez-Almazor, M.E.; Tayar, J.H.; Lu, H.; Buni, M.; Kramer, J.; Rodriguez, E.; Hussain, Z.; et al. Distinct molecular and immune hallmarks of inflammatory arthritis induced by immune checkpoint inhibitors for cancer therapy. Nat Commun. 2022, 13(1), 1970. [Google Scholar] [CrossRef] [PubMed]
- Okiyama, N.; Tanaka, R. Immune-related adverse events in various organs caused by immune checkpoint inhibitors. Allergol Int. 2022, 71(2), 169–178. [Google Scholar] [CrossRef]
- Li, S, Na. Targeting interleukin-17 enhances tumor response to immune checkpoint inhibitors in colorectal cancer. Biochim Biophys Acta Rev Cancer. 2022, 1877(4), 188758. [Google Scholar] [CrossRef] [PubMed]
- Ramesh, R.; Kozhaya, L.; McKevitt, K.; Djuretic, I.M.; Carlson, T.J.; Quintero, M.A.; McCauley, J.L.; Abreu, M.T.; Unutmaz, D.; Sundrud, M.S. Pro-inflammatory human Th17 cells selectively express P-glycoprotein and are refractory to glucocorticoids. J Exp Med. 2014, 211(1), 89–104. [Google Scholar] [CrossRef]
- Melin, A.; Routier, É.; Roy, S.; Pradere, P.; Le Pavec, J.; Pierre, T.; Chanson, N.; Scoazec, J.Y.; Lambotte, O.; Robert, C. Sarcoid-like Granulomatosis Associated with Immune Checkpoint Inhibitors in Melanoma. Cancers (Basel). 2022, 14(12), 2937. [Google Scholar] [CrossRef] [PubMed]
- Downs-Canner, S.; Berkey, S.; Delgoffe, G.M.; Edwards, R.P.; Curiel, T.; Odunsi, K.; Bartlett, D.L.; Obermajer, N. Suppressive IL-17A+Foxp3+ and ex-Th17 IL-17AnegFoxp3+ Treg cells are a source of tumour-associated Treg cells. Nat Commun. 2017, 8, 14649. [Google Scholar] [CrossRef]
- Saenz, S.A.; Local, A.; Carr, T.; Shakya, A.; Koul, S.; Hu, H.; Chourb, L.; Stedman, J.; Malley, J.; D'Agostino, L.A.; et al. Small molecule allosteric inhibitors of RORγt block Th17-dependent inflammation and associated gene expression in vivo. PLoS One. 2021, 16(11), e0248034. [Google Scholar] [CrossRef] [PubMed]
- Kendall, T.; Verheij, J.; Gaudio, E.; Evert, M.; Guido, M.; Goeppert, B.; Carpino, G. Anatomical, histomorphological and molecular classification of cholangiocarcinoma. Liver Int. 2019, 39 Suppl 1, 7–18. [Google Scholar] [CrossRef]
- Yoo, H.J.; Harapan, B.N. Chimeric antigen receptor (CAR) immunotherapy: basic principles, current advances, and future prospects in neuro-oncology. Immunol Res. 2021, 69(6), 471–486. [Google Scholar] [CrossRef] [PubMed]
- Huang, R.; Wang, X.; Zhang, X. Unity brings strength: Combination of CAR-T cell therapy and HSCT. Cancer Lett. 2022, 549, 215721. [Google Scholar] [CrossRef] [PubMed]
- Chung, H.; Jung, H.; Noh, J.Y. Emerging Approaches for Solid Tumor Treatment Using CAR-T Cell Therapy. Int J Mol Sci. 2021, 22(22), 12126. [Google Scholar] [CrossRef] [PubMed]
- Sun, B.; Yang, D.; Dai, H.; Liu, X.; Jia, R.; Cui, X.; Li, W.; Cai, C.; Xu, J.; Zhao, X. Eradication of Hepatocellular Carcinoma by NKG2D-Based CAR-T Cells. Cancer Immunol Res. 2019, 7(11), 1813–1823. [Google Scholar] [CrossRef] [PubMed]
- Jose, A.; Bavetta, M.G.; Martinelli, E.; Bronte, F.; Giunta, E.F.; Manu, K.A. Hepatocellular Carcinoma: Current Therapeutic Algorithm for Localized and Advanced Disease. J Oncol. 2022, 2022, 3817724. [Google Scholar] [CrossRef]
- Howells, A.; Marelli, G.; Lemoine, N.R.; Wang, Y. Oncolytic Viruses-Interaction of Virus and Tumor Cells in the Battle to Eliminate Cancer. Front Oncol. 2017, 7, 195. [Google Scholar] [CrossRef]
- Luo, C.; Wang, P.; He, S.; Zhu, J.; Shi, Y.; Wang, J. Progress and Prospect of Immunotherapy for Triple-Negative Breast Cancer. Front Oncol. 2022, 12, 919072. [Google Scholar] [CrossRef]
- Zhou, Y.; Wang, Q.; Ying, Q.; Zhang, X.; Chen, K.; Ye, T.; Li, G. Effects of Oncolytic Vaccinia Viruses Harboring Different Marine Lectins on Hepatocellular Carcinoma Cells. Int J Mol Sci. 2023, 24(4), 3823. [Google Scholar] [CrossRef]
- Zheng, X.; Xu, W.; Ying, Q.; Ni, J.; Jia, X.; Zhou, Y.; Ye, T.; Li, G.; Chen, K. Oncolytic Vaccinia Virus Carrying Aphrocallistes vastus Lectin (oncoVV-AVL) Enhances Inflammatory Response in Hepatocellular Carcinoma Cells. Mar Drugs. 2022, 20(11), 667. [Google Scholar] [CrossRef] [PubMed]
- Qi, X.; Liu, Y.; Hussein, S.; Choi, G.; Kimchi, E.T.; Staveley-O'Carroll, K.F.; Li, G. The Species of Gut Bacteria Associated with Antitumor Immunity in Cancer Therapy. Cells. 2022, 11(22), 3684. [Google Scholar] [CrossRef] [PubMed]
- Wang, Z.; Li, L.; Wang, S.; Wei, J.; Qu, L.; Pan, L.; Xu, K. The role of the gut microbiota and probiotics associated with microbial metabolisms in cancer prevention and therapy. Front Pharmacol. 2022, 13, 1025860. [Google Scholar] [CrossRef]
- Luo, M.; Chen, X.; Gao, H.; Yang, F.; Chen, J.; Qiao, Y. Bacteria-mediated cancer therapy: A versatile bio-sapper with translational potential. Front Oncol. 2022, 12, 980111. [Google Scholar] [CrossRef] [PubMed]
- Nejman, D.; Livyatan, I.; Fuks, G.; Gavert, N.; Zwang, Y.; Geller, L.T.; Rotter-Maskowitz, A.; Weiser, R.; Mallel, G.; Gigi, E.; et al. The human tumor microbiome is composed of tumor type-specific intracellular bacteria. Scinence. 2020, 368(6494), 973–980. [Google Scholar] [CrossRef] [PubMed]
- Kaźmierczak-Siedlecka, K.; Daca, A.; Fic, M.; van de Wetering, T.; Folwarski, M.; Makarewicz, W. Therapeutic methods of gut microbiota modification in colorectal cancer management - fecal microbiota transplantation, prebiotics, probiotics, and synbiotics. Gut Microbes. 2020, 11(6), 1518–1530. [Google Scholar] [CrossRef]
- Ikeda, Y.; Taniguchi, K.; Yoshikawa, S.; Sawamura, H.; Tsuji, A.; Matsuda, S. A budding concept with certain microbiota, anti-proliferative family proteins, and engram theory for the innovative treatment of colon cancer. Explor Med. 2022, 3, 468–478. [Google Scholar] [CrossRef]
- Wang, C.; Li, W.; Wang, H.; Ma, Y.; Zhao, X.; Zhang, X.; Yang, H.; Qian, J.; Li, J. Saccharomyces boulardii alleviates ulcerative colitis carcinogenesis in mice by reducing TNF-α and IL-6 levels and functions and by rebalancing intestinal microbiota. BMC Microbiol. 2019, 19(1), 246. [Google Scholar] [CrossRef]
- Shi, Y.; Xu, L.Z.; Peng, K.; Wu, W.; Wu, R.; Liu, Z.Q.; Yang, G.; Geng, X.R.; Liu, J.; Liu, Z.G.; et al. Specific immunotherapy in combination with Clostridium butyricum inhibits allergic inflammation in the mouse intestine. Sci Rep. 2015, 5, 17651. [Google Scholar] [CrossRef] [PubMed]
- Uchugonova, A.; Zhang, Y.; Salz, R.; Liu, F.; Suetsugu, A.; Zhang, L.; Koenig, K.; Hoffman, R.M.; Zhao, M. Imaging the Different Mechanisms of Prostate Cancer Cell-killing by Tumor-targeting Salmonella typhimurium A1-R. Anticancer Res. 2015, 35(10), 5225–5229. [Google Scholar]
- Li, L.; You, L.S.; Mao, L.P.; Jin, S.H.; Chen, X.H.; Qian, W.B. Combing oncolytic adenovirus expressing Beclin-1 with chemotherapy agent doxorubicin synergistically enhances cytotoxicity in human CML cells in vitro. Acta Pharmacol Sin. 2018, 39(2), 251–260. [Google Scholar] [CrossRef] [PubMed]
- Wang, X.; Liu, Z.; Sui, X.; Wu, Q.; Wang, J.; Xu, C. Elemene injection as adjunctive treatment to platinum-based chemotherapy in patients with stage III/IV non-small cell lung cancer: A meta-analysis following the PRISMA guidelines. Phytomedicine. 2019, 59, 152787. [Google Scholar] [CrossRef] [PubMed]
- Din, M.O.; Danino, T.; Prindle, A.; Skalak, M.; Selimkhanov, J.; Allen, K.; Julio, E.; Atolia, E.; Tsimring, L.S.; Bhatia, S.N.; et al. Synchronized cycles of bacterial lysis for in vivo delivery. Nature. 2016, 536(7614), 81–85. [Google Scholar] [CrossRef] [PubMed]
- McNerney, M.P.; Doiron, K.E.; Ng, T.L.; Chang, T.Z.; Silver, P.A. Theranostic cells: emerging clinical applications of synthetic biology. Nat Rev Genet. 2021, 22(11), 730–746. [Google Scholar] [CrossRef] [PubMed]
- Lu, Y.; Luo, X.; Yang, D.; Li, Y.; Gong, T.; Li, B.; Cheng, J.; Chen, R.; Guo, X.; Yuan, W. Effects of probiotic supplementation on related side effects after chemoradiotherapy in cancer patients. Front Oncol. 2022, 12, 1032145. [Google Scholar] [CrossRef] [PubMed]
- Burdelya, L.G.; Krivokrysenko, V.I.; Tallant, T.C.; Strom, E.; Gleiberman, A.S.; Gupta, D.; Kurnasov, O.V.; Fort, F.L.; Osterman, A.L.; Didonato, J.A.; et al. An agonist of toll-like receptor 5 has radioprotective activity in mouse and primate models. Science. 2008, 320(5873), 226–230. [Google Scholar] [CrossRef]
- Abdollahi, H. Beneficial effects of cellular autofluorescence following ionization radiation: hypothetical approaches for radiation protection and enhancing radiotherapy effectiveness. Med Hypotheses. 2015, 84(3), 194–198. [Google Scholar] [CrossRef]
- Bettegowda, C.; Dang, L.H.; Abrams, R.; Huso, D.L.; Dillehay, L.; Cheong, I.; Agrawal, N.; Borzillary, S.; McCaffery, J.M.; Watson, E.L.; et al. Overcoming the hypoxic barrier to radiation therapy with anaerobic bacteria. Proc Natl Acad Sci U S A. 2003, 100(25), 15083–15088. [Google Scholar] [CrossRef]
- Poonacha, K.N.T.; Villa, T.G.; Notario, V. The Interplay among Radiation Therapy, Antibiotics and the Microbiota: Impact on Cancer Treatment Outcomes. Antibiotics (Basel). 2022, 11(3), 331. [Google Scholar] [CrossRef]
- Lee, S.H.; Cho, S.Y.; Yoon, Y.; Park, C.; Sohn, J.; Jeong, J.J.; Jeon, B.N.; Jang, M.; An, C.; Lee, S.; et al. Bifidobacterium bifidum strains synergize with immune checkpoint inhibitors to reduce tumour burden in mice. Nat Microbiol. 2021, 6(3), 277–288. [Google Scholar] [CrossRef]
- Zhuo, Q.; Yu, B.; Zhou, J.; Zhang, J.; Zhang, R.; Xie, J.; Wang, Q.; Zhao, S. Lysates of Lactobacillus acidophilus combined with CTLA-4-blocking antibodies enhance antitumor immunity in a mouse colon cancer model. Sci. Rep. 2019, 9(1), 20128. [Google Scholar] [CrossRef] [PubMed]
- Ahmadi, Badi, S.; Moshiri, A.; Ettehad, Marvasti, F.; Mojtahedzadeh, M.; Kazemi, V.; Siadat, S.D. Extraction and Evaluation of Outer Membrane Vesicles from Two Important Gut Microbiota Members, Bacteroides fragilis and Bacteroides thetaiotaomicron. Cell J 2020, 22(3), 344–349. [Google Scholar]
- Vétizou, M.; Pitt, J.M.; Daillère, R.; Lepage, P.; Waldschmitt, N.; Flament, C.; Rusakiewicz, S.; Routy, B.; Roberti, M.P.; Duong, C.P.; et al. Anticancer immunotherapy by CTLA-4 blockade relies on the gut microbiota. Science. 2015, 350(6264), 1079–1084. [Google Scholar] [CrossRef]
- Zhang, M.; Qiu, X.; Zhang, H.; Yang, X.; Hong, N.; Yang, Y.; Chen, H.; Yu, C. Faecalibacterium prausnitzii inhibits interleukin-17 to ameliorate colorectal colitis in rats. PLoS One. 2014, 9(10), e109146. [Google Scholar] [CrossRef]
- Zhou, L.; Zhang, M.; Wang, Y.; Dorfman, R.G.; Liu, H.; Yu, T.; Chen, X.; Tang, D.; Xu, L.; Yin, Y.; et al. Faecalibacterium prausnitzii Produces Butyrate to Maintain Th17/Treg Balance and to Ameliorate Colorectal Colitis by Inhibiting Histone Deacetylase 1. Inflamm Bowel Dis. 2018, 24(9), 1926–1940. [Google Scholar] [CrossRef] [PubMed]
- Kaźmierczak-Siedlecka, K.; Skonieczna-Żydecka, K.; Hupp, T.; Duchnowska, R.; Marek-Trzonkowska, N.; Połom, K. Next-generation probiotics - do they open new therapeutic strategies for cancer patients? Gut Microbes. 2022, 14(1), 2035659. [Google Scholar] [CrossRef]
- Behary, J.; Raposo, A.E.; Amorim, N.M.L.; Zheng, H.; Gong, L.; McGovern, E.; Chen, J.; Liu, K.; Beretov, J.; Theocharous, C.; et al. Defining the temporal evolution of gut dysbiosis and inflammatory responses leading to hepatocellular carcinoma in Mdr2 -/- mouse model. BMC Microbiol. 2021, 21(1), 113. [Google Scholar] [CrossRef]
- Ponziani, F.R.; Bhoori, S.; Castelli, C.; Putignani, L.; Rivoltini, L.; Del Chierico, F.; Sanguinetti, M.; Morelli, D.; Paroni, Sterbini, F.; Petito, V.; et al. Hepatocellular Carcinoma Is Associated With Gut Microbiota Profile and Inflammation in Nonalcoholic Fatty Liver Disease. Hepatology. 2019, 69(1), 107–120. [Google Scholar] [CrossRef]
- Zhang, X.; Coker, O.O.; Chu, E.S.; Fu, K.; Lau, H.C.H.; Wang, Y.X.; Chan, A.W.H.; Wei, H.; Yang, X.; Sung, J.J.Y.; et al. Dietary cholesterol drives fatty liver-associated liver cancer by modulating gut microbiota and metabolites. Gut. 2021, 70(4), 761–774. [Google Scholar] [CrossRef]
- Rezasoltani, S.; Yadegar, A.; Asadzadeh Aghdaei, H.; Reza, Zali, M. Modulatory effects of gut microbiome in cancer immunotherapy: A novel paradigm for blockade of immune checkpoint inhibitors. Cancer Med. 2021, 10(3), 1141–1154. [Google Scholar] [CrossRef]
- Wu, Y.; Zheng, L. Dynamic education of macrophages in different areas of human tumors. Cancer Microenviron. 2012, 5(3), 195–201. [Google Scholar] [CrossRef] [PubMed]
- Ahmed, F.; Steele, J.C.; Herbert, J.M.; Steven, N.M.; Bicknell, R. Tumor stroma as a target in cancer. Curr Cancer Drug Targets. 2008, 8(6), 447–453. [Google Scholar] [CrossRef]
- Zhang, J.P.; Yan, J.; Xu, J.; Pang, X.H.; Chen, M.S.; Li, L.; Wu, C.; Li, S.P.; Zheng, L. Increased intratumoral IL-17-producing cells correlate with poor survival in hepatocellular carcinoma patients. J Hepatol. 2009, 50(5), 980–989. [Google Scholar] [CrossRef]
- Zhao, F.; Hoechst, B.; Gamrekelashvili, J.; Ormandy, L.A.; Voigtländer, T.; Wedemeyer, H.; Ylaya, K.; Wang, X.W.; Hewitt, S.M.; Manns, M.P.; et al. Human CCR4+ CCR6+ Th17 cells suppress autologous CD8+ T cell responses. J Immunol. 2012, 188(12), 6055–6062. [Google Scholar] [CrossRef]
- Liao, R.; Sun, J.; Wu, H.; Yi, Y.; Wang, J.X.; He, H.W.; Cai, X.Y.; Zhou, J.; Cheng, Y.F.; Fan, J.; et al. High expression of IL-17 and IL-17RE associate with poor prognosis of hepatocellular carcinoma. J Exp Clin Cancer Res. 2013, 32(1), 3. [Google Scholar] [CrossRef] [PubMed]
- Kuang, D.M.; Peng, C.; Zhao, Q.; Wu, Y.; Chen, M.S.; Zheng, L. Activated monocytes in peritumoral stroma of hepatocellular carcinoma promote expansion of memory T helper 17 cells. Hepatology. 2010, 51(1), 154–164. [Google Scholar] [CrossRef] [PubMed]
- Michaelis, L.; Treß, M.; Löw, H.C.; Klees, J.; Klameth, C.; Lange, A.; Grießhammer, A.; Schäfer, A.; Menz, S.; Steimle, A.; et al. Gut Commensal-Induced IκBζ Expression in Dendritic Cells Influences the Th17 Response. Front Immunol. 2021, 11, 612336. [Google Scholar] [CrossRef]
- Sung, C.Y.; Lee, N.P.; El-Nezami, H. Regulation of T helper 17 by bacteria: an approach for the treatment of hepatocellular carcinoma. Int J Hepatol. 2012, 2012, 439024. [Google Scholar] [CrossRef]
- Gu, F.M.; Li, Q.L.; Gao, Q.; Jiang, J.H.; Zhu, K.; Huang, X.Y.; Pan, J.F.; Yan, J.; Hu, J.H.; Wang, Z.; et al. IL-17 induces AKT-dependent IL-6/JAK2/STAT3 activation and tumor progression in hepatocellular carcinoma. Mol Cancer. 2011, 10, 150. [Google Scholar] [CrossRef]
- Qin, H.; Yuan, B.; Huang, W.; Wang, Y. Utilizing Gut Microbiota to Improve Hepatobiliary Tumor Treatments: Recent Advances. Front Oncol. 2022, 12, 924696. [Google Scholar] [CrossRef]
- Mikó, E.; Vida, A.; Bai, P. Translational aspects of the microbiome-to be exploited. Cell Biol Toxicol. 2016, 32(3), 153–156. [Google Scholar] [CrossRef] [PubMed]
- Kovács, T.; Mikó, E.; Vida, A.; Sebő, É.; Toth, J.; Csonka, T.; Boratkó, A.; Ujlaki, G.; Lente, G.; Kovács, P.; et al. Cadaverine, a metabolite of the microbiome, reduces breast cancer aggressiveness through trace amino acid receptors. Sci Rep. 2019, 9(1), 1300. [Google Scholar] [CrossRef] [PubMed]
- Yu, L.X.; Schwabe, R.F. The gut microbiome and liver cancer: mechanisms and clinical translation. Nat Rev Gastroenterol Hepatol. 2017, 14(9), 527–539. [Google Scholar] [CrossRef]
- Yuan, J.; Chen, C.; Cui, J.; Lu, J.; Yan, C.; Wei, X.; Zhao, X.; Li, N.; Li, S.; Xue, G.; et al. Fatty Liver Disease Caused by High-Alcohol-Producing Klebsiella pneumoniae. Cell Metab. 2019, 30(4), 675–688.e7. [Google Scholar] [CrossRef] [PubMed]
- Lapidot, Y.; Amir, A.; Nosenko, R.; Uzan-Yulzari, A.; Veitsman, E.; Cohen-Ezra, O.; Davidov, Y.; Weiss, P.; Bradichevski, T.; Segev, S.; et al. Alterations in the Gut Microbiome in the Progression of Cirrhosis to Hepatocellular Carcinoma. mSystems. 2020, 5(3), e00153–20. [Google Scholar] [CrossRef] [PubMed]
- Ma, C.; Han, M.; Heinrich, B.; Fu, Q.; Zhang, Q.; Sandhu, M.; Agdashian, D.; Terabe, M.; Berzofsky, J.A.; Fako, V.; et al. Gut microbiome-mediated bile acid metabolism regulates liver cancer via NKT cells. Science. 2018, 360(6391), eaan5931. [Google Scholar] [CrossRef]
- Routy, B.; Le Chatelier, E.; Derosa, L.; Duong, C.P.M.; Alou, M.T.; Daillère, R.; Fluckiger, A.; Messaoudene, M.; Rauber, C.; Roberti, M.P.; et al. Gut microbiome influences efficacy of PD-1-based immunotherapy against epithelial tumors. Science. 2018, 359(6371), 91–97. [Google Scholar] [CrossRef]
- Gopalakrishnan, V.; Spencer, C.N.; Nezi, L.; Reuben, A.; Andrews, M.C.; Karpinets, T.V.; Prieto, P.A.; Vicente, D.; Hoffman, K.; Wei, S.C.; et al. , Gut microbiome modulates response to anti-PD-1 immunotherapy in melanoma patients. Science. 2018, 359(6371), 97–103. [Google Scholar] [CrossRef]
- Matson, V.; Fessler, J.; Bao, R.; Chongsuwat, T.; Zha, Y.; Alegre, M.L.; Luke, J.J.; Gajewski, T.F. The commensal microbiome is associated with anti-PD-1 efficacy in metastatic melanoma patients. Science. 2018, 359(6371), 104–108. [Google Scholar] [CrossRef]
- Yoshimoto, S.; Loo, T.M.; Atarashi, K.; Kanda, H.; Sato, S.; Oyadomari, S.; Iwakura, Y.; Oshima, K.; Morita, H.; Hattori, M.; et al. Obesity-induced gut microbial metabolite promotes liver cancer through senescence secretome. Nature. 2013, 499(7456), 97–101. [Google Scholar] [CrossRef]
- Dapito, D.H.; Mencin, A.; Gwak, G.Y.; Pradere, J.P.; Jang, M.K.; Mederacke, I.; Caviglia, J.M.; Khiabanian, H.; Adeyemi, A.; Bataller, R.; et al. Promotion of hepatocellular carcinoma by the intestinal microbiota and TLR4. Cancer Cell. 2012, 21(4), 504–516. [Google Scholar] [CrossRef] [PubMed]
- Zheng, Y.; Wang, T.; Tu, X.; Huang, Y.; Zhang, H.; Tan, D.; Jiang, W.; Cai, S.; Zhao, P.; Song, R.; et al. Gut microbiome affects the response to anti-PD-1 immunotherapy in patients with hepatocellular carcinoma. J Immunother Cancer. 2019, 7(1), 193. [Google Scholar] [CrossRef] [PubMed]
- Fernandes, M.R.; Aggarwal, P.; Costa, R.G.F.; Cole, A.M.; Trinchieri, G. Targeting the gut microbiota for cancer therapy. Nat Rev Cancer. 2022, 22(12), 703–722. [Google Scholar] [CrossRef] [PubMed]
- Dai, E.; Zhu, Z.; Wahed, S.; Qu, Z.; Storkus, W.J.; Guo, Z.S. Epigenetic modulation of antitumor immunity for improved cancer immunotherapy. Mol Cancer. 2021, 20(1), 171. [Google Scholar] [CrossRef]
- Burr, M.L.; Sparbier, C.E.; Chan, K.L.; Chan Y.C.; Kersbergen, A.; Lam E.Y.N.; Azidis-Yates E.; Vassiliadis D.; Bell C.C.; Gilan O.; et al. An evolutionarily conserved function of polycomb silences the MHC class I antigen presentation pathway and enables immune evasion in cancer. Cancer Cell. 2019, 36(4), 385–401. e8.
- Greger, V.; Passarge, E.; Höpping, W.; Messmer, E.; Horsthemke, B. Epigenetic changes may contribute to the formation and spontaneous regression of retinoblastoma. Hum Genet. 1989, 83(2), 155–158. [Google Scholar] [CrossRef]
- Saito, Y.; Liang, G.; Egger, G.; Friedman, J.M.; Chuang, J.C.; Coetzee, G.A.; Jones, P.A. Specific activation of microRNA-127 with downregulation of the proto-oncogene BCL6 by chromatin-modifying drugs in human cancer cells. Cancer Cell. 2006, 9(6), 435–443. [Google Scholar] [CrossRef]
- Senga, S.S.; Grose, R.P. Hallmarks of cancer-the new testament. Open Biol. 2021, 11(1), 200358. [Google Scholar] [CrossRef]
- Wang, G.; He, X.; Wang, Q. Intratumoral bacteria are an important “accomplice” in tumor development and metastasis. Biochim. Biophys Acta Rev Cancer. 2023, 1878(1), 188846. [Google Scholar]
- Yang, F.; Yang, Y.; Chen, L.; Zhang, Z.; Liu, L.; Zhang, C.; Mai, Q.; Chen, Y.; Chen, Z.; Lin, T.; et al. The gut microbiota mediates protective immunity against tuberculosis via modulation of lncRNA. Gut Microbes. 2022, 14(1), 2029997. [Google Scholar] [CrossRef]
- Niller, H.H.; Minarovits, J. Patho-epigenetics of Infectious Diseases Caused by Intracellular Bacteria. Adv Exp Med Biol. 2016, 879, 107–130. [Google Scholar]
- Luu, M.; Schütz, B.; Lauth, M.; Visekruna, A. The Impact of Gut Microbiota-Derived Metabolites on the Tumor Immune Microenvironment. Cancers (Basel). 2023, 15(5), 1588. [Google Scholar] [CrossRef]
- Cerf-Bensussan, N.; Gaboriau-Routhiau, V. The immune system and the gut microbiota: Friends or foes? Nat Rev Immunol. 2010, 10(10), 735–744. [Google Scholar] [CrossRef]
- Ledezma, D.K.; Balakrishnan, P.B.; Cano-Mejia, J.; Sweeney, E.E.; Hadley, M.; Bollard, C.M.; Villagra, A.; Fernandes, R. Indocyanine Green-Nexturastat A-PLGA Nanoparticles Combine Photothermal and Epigenetic Therapy for Melanoma. Nanomaterials (Basel). 2020, 10(1), 161. [Google Scholar] [CrossRef]
- Wachowska, M.; Gabrysiak, M.; Muchowicz, A.; Bednarek, W.; Barankiewicz, J.; Rygiel, T.; Boon, L.; Mroz, P.; Hamblin, M.R.; Golab, J. 5-Aza-2'-deoxycytidine potentiates antitumour immune response induced by photodynamic therapy. Eur J Cancer. 2014, 50(7), 1370–1381. [Google Scholar] [CrossRef]
- Wachowska, M.; Muchowicz, A.; Golab, J. Targeting Epigenetic Processes in Photodynamic Therapy-Induced Anticancer Immunity. Front Oncol. 2015, 5, 176. [Google Scholar] [CrossRef]
- Trifylli, E.M.; Koustas, E.; Papadopoulos, N.; Sarantis, P.; Aloizos, G.; Damaskos, C.; Garmpis, N.; Garmpi, A.; Karamouzis, M.V. An Insight into the Novel Immunotherapy and Targeted Therapeutic Strategies for Hepatocellular Carcinoma and Cholangiocarcinoma. Life (Basel). 2022, 12(5), 665. [Google Scholar] [CrossRef]
- Hill, C.; Guarner, F.; Reid, G.; Gibson, G.R.; Merenstein, D.J.; Pot, B.; Morelli, L.; Canani, R.B.; Flint, H.J.; Salminen, S.; et al. Expert consensus document. The International Scientific Association for Probiotics and Prebiotics consensus statement on the scope and appropriate use of the term probiotic. Nat Rev Gastroenterol Hepatol. 2014, 11(8), 506–514. [Google Scholar] [CrossRef]
- Pace, F.; Macchini, F.; Massimo, Castagna, V. Safety of probiotics in humans: A dark side revealed? Dig Liver Dis. 2020, 52(9), 981–985. [CrossRef]
- Wallace, C.; Sinopoulou, V.; Gordon, M.; Akobeng, A.K.; Llanos-Chea, A.; Hungria, G.; Febo-Rodriguez, L.; Fifi, A.; Fernandez Valdes, L.; Langshaw, A.; et al. Probiotics for treatment of chronic constipation in children. Cochrane Database Syst Rev. 2022, 3(3), CD014257. [Google Scholar]
- Sun, F.; Zhang, Q.; Zhao, J.; Zhang, H.; Zhai, Q.; Chen, W. A potential species of next-generation probiotics? The dark and light sides of Bacteroides fragilis in health. Food Res Int. 2019, 126, 108590. [Google Scholar] [CrossRef]
- Bayer, A.S.; Chow, A.W.; Betts, D.; Guze, L.B. Lactobacillemia--report of nine cases. Important clinical and therapeutic considerations. Am J Med. 1978, 64(5), 808–813. [Google Scholar] [CrossRef] [PubMed]
- Dickgiesser, U.; Weiss, N.; Fritsche, D. Lactobacillus gasseri as the cause of septic urinary infection. Infection. 1984, 12(1), 14–16. [Google Scholar] [CrossRef]
- Tan, K.P.; Yang, M.; Ito, S. Activation of nuclear factor (erythroid-2 like) factor 2 by toxic bile acids provokes adaptive defense responses to enhance cell survival at the emergence of oxidative stress. Mol Pharmacol. 2007, 72(5), 1380–1390. [Google Scholar] [CrossRef]
- Hiam-Galvez, K.J.; Allen, B.M.; Spitzer, M.H. Systemic immunity in cancer. Nat Rev Cancer. 2021, 21(6), 345–359. [Google Scholar] [CrossRef]
- Reig, M.; Forner, A.; Rimola, J.; Ferrer-Fàbrega, J.; Burrel, M.; Garcia-Criado, Á.; Kelley, R.K.; Galle, P.R.; Mazzaferro, V.; Salem, R.; et al. BCLC strategy for prognosis prediction and treatment recommendation: The 2022 update. J Hepatol. 2022, 76(3), 681–693. [Google Scholar] [CrossRef] [PubMed]
- Jiang, X.; Zheng, J.; Zhang, S.; Wang, B.; Wu, C.; Guo, X. Advances in the Involvement of Gut Microbiota in Pathophysiology of NAFLD. Front Med (Lausanne). 2020, 7, 361. [Google Scholar] [CrossRef]
- Alexander, J.L.; Wilson, I.D.; Teare, J.; Marchesi, J.R.; Nicholson, J.K.; Kinross, J.M. Gut microbiota modulation of chemotherapy efficacy and toxicity. Nat Rev Gastroenterol Hepatol. 2017, 14(6), 356–365. [Google Scholar] [CrossRef]
- Mukaida, N. Intestinal microbiota: unexpected alliance with tumor therapy. Immunotherapy. 2014, 6(3), 231–233. [Google Scholar] [CrossRef] [PubMed]
- Iida, N.; Dzutsev, A.; Stewart, C.A.; Smith, L.; Bouladoux, N.; Weingarten, R.A.; Molina, D.A.; Salcedo, R.; Back, T.; Cramer, S.; et al. Commensal bacteria control cancer response to therapy by modulating the tumor microenvironment. Science. 2013, 342(6161), 967–970. [Google Scholar] [CrossRef] [PubMed]
- Pagadala, M.; Sears, T.J.; Wu, V.H.; Pérez-Guijarro, E.; Kim, H.; Castro, A.; Talwar, J.V.; Gonzalez-Colin, C.; Cao, S.; Schmiedel, B.J.; et al. Germline modifiers of the tumor immune microenvironment implicate drivers of cancer risk and immunotherapy response. Nat Commun. 2023, 14(1), 2744. [Google Scholar] [CrossRef]
- Yoshikawa, S.; Taniguchi, K.; Sawamura, H, Ikeda Y, Tsuji A, Matsuda S.Encouraging probiotics for the prevention and treatment of immune-related adverse events in novel immunotherapies against malignant glioma. Explor Target Antitumor Ther. 2022, 3(6), 817–827.
- Ayob, A.Z.; Ramasamy, T.S. Cancer stem cells as key drivers of tumour progression. J Biomed Sci. 2018, 25(1), 20. [Google Scholar] [CrossRef] [PubMed]
- Garza, Treviño, E.N.; González, P.D.; Valencia, Salgado, C.I.; Martinez, Garza, A. Effects of pericytes and colon cancer stem cells in the tumor microenvironment. Cancer Cell Int. 2019, 19, 173. [Google Scholar] [CrossRef]
- Yoshikawa, S.; Taniguchi, K.; Sawamura, H.; Ikeda, Y.; Tsuji, A.; Matsuda, S. A New Concept of Associations between Gut Microbiota, Immunity and Central Nervous System for the Innovative Treatment of Neurodegenerative Disorders. Metabolites. 2022, 12(11), 1052. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
A hypothetical representation and overview of the pathogenesis during the development of hepatocellular carcinoma (HCC). Hepatitis B virus (HBV), hepatitis C virus (HCV), alcoholic liver disease (ALD), and/or non-alcoholic fatty liver disease (NAFLD) as well as Th17/Treg balance and/or gut microbiota could independently contribute to the pathogenesis of HCC. Arrowhead indicates stimulation whereas double-arrowheads suggests bidirectional stimulation. Note that several important activities such as anti-inflammatory reaction pathway have been omitted for clarity.
Figure 1.
A hypothetical representation and overview of the pathogenesis during the development of hepatocellular carcinoma (HCC). Hepatitis B virus (HBV), hepatitis C virus (HCV), alcoholic liver disease (ALD), and/or non-alcoholic fatty liver disease (NAFLD) as well as Th17/Treg balance and/or gut microbiota could independently contribute to the pathogenesis of HCC. Arrowhead indicates stimulation whereas double-arrowheads suggests bidirectional stimulation. Note that several important activities such as anti-inflammatory reaction pathway have been omitted for clarity.
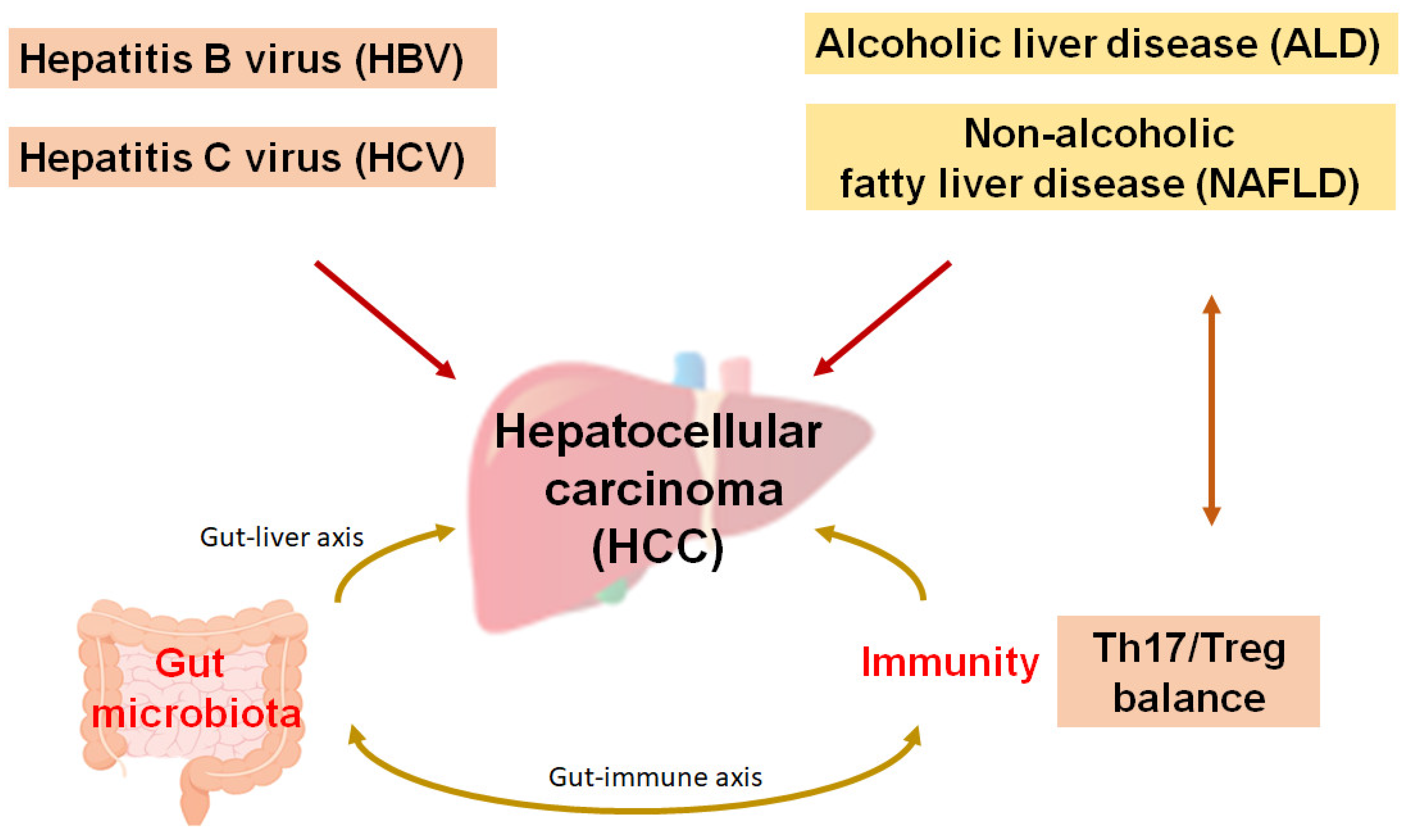
Figure 2.
A schematic representation and hypothetical overview of the immune checkpoint inhibitors against HCC. Certain gut microbiota could contribute to the potentiation of the immune checkpoint immunotherapy with the improvement of Th17/Treg immune cells’ balance. Some kinds of probiotics and/or fecal microbiota transplantation (FMT) could contribute to the alteration of gut microbial community for playing valuable roles to the potentiation of immune checkpoint therapy. Examples of certain beneficial microbial species with some effects on anti-cancer immune responses have been shown. Arrowhead indicates stimulation (or bidirectional stimulation), whereas ammerhead shows inhibition. Note that several important activities such as cytokine and/or chemokine production have been omitted for clarity.
Figure 2.
A schematic representation and hypothetical overview of the immune checkpoint inhibitors against HCC. Certain gut microbiota could contribute to the potentiation of the immune checkpoint immunotherapy with the improvement of Th17/Treg immune cells’ balance. Some kinds of probiotics and/or fecal microbiota transplantation (FMT) could contribute to the alteration of gut microbial community for playing valuable roles to the potentiation of immune checkpoint therapy. Examples of certain beneficial microbial species with some effects on anti-cancer immune responses have been shown. Arrowhead indicates stimulation (or bidirectional stimulation), whereas ammerhead shows inhibition. Note that several important activities such as cytokine and/or chemokine production have been omitted for clarity.
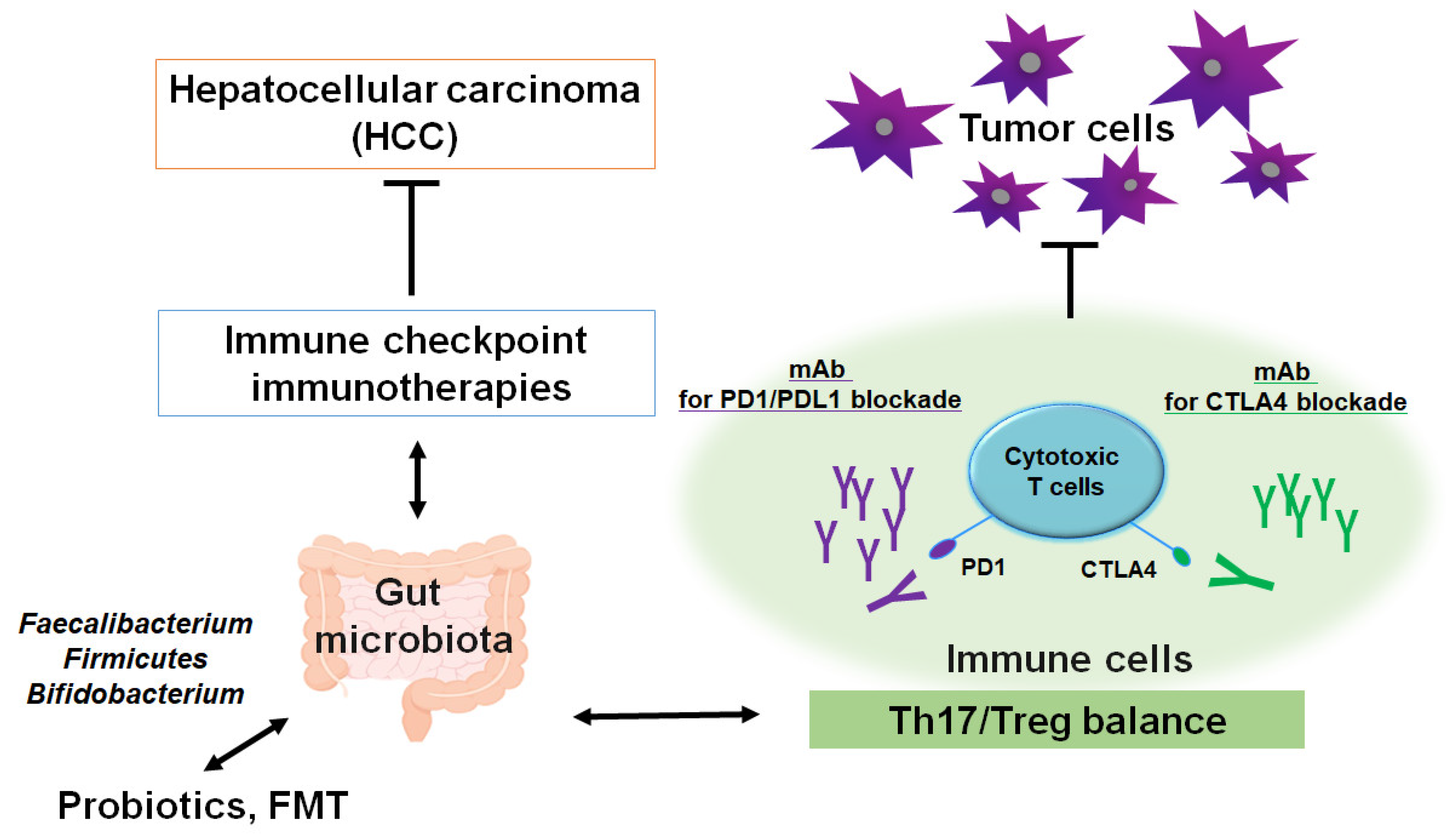
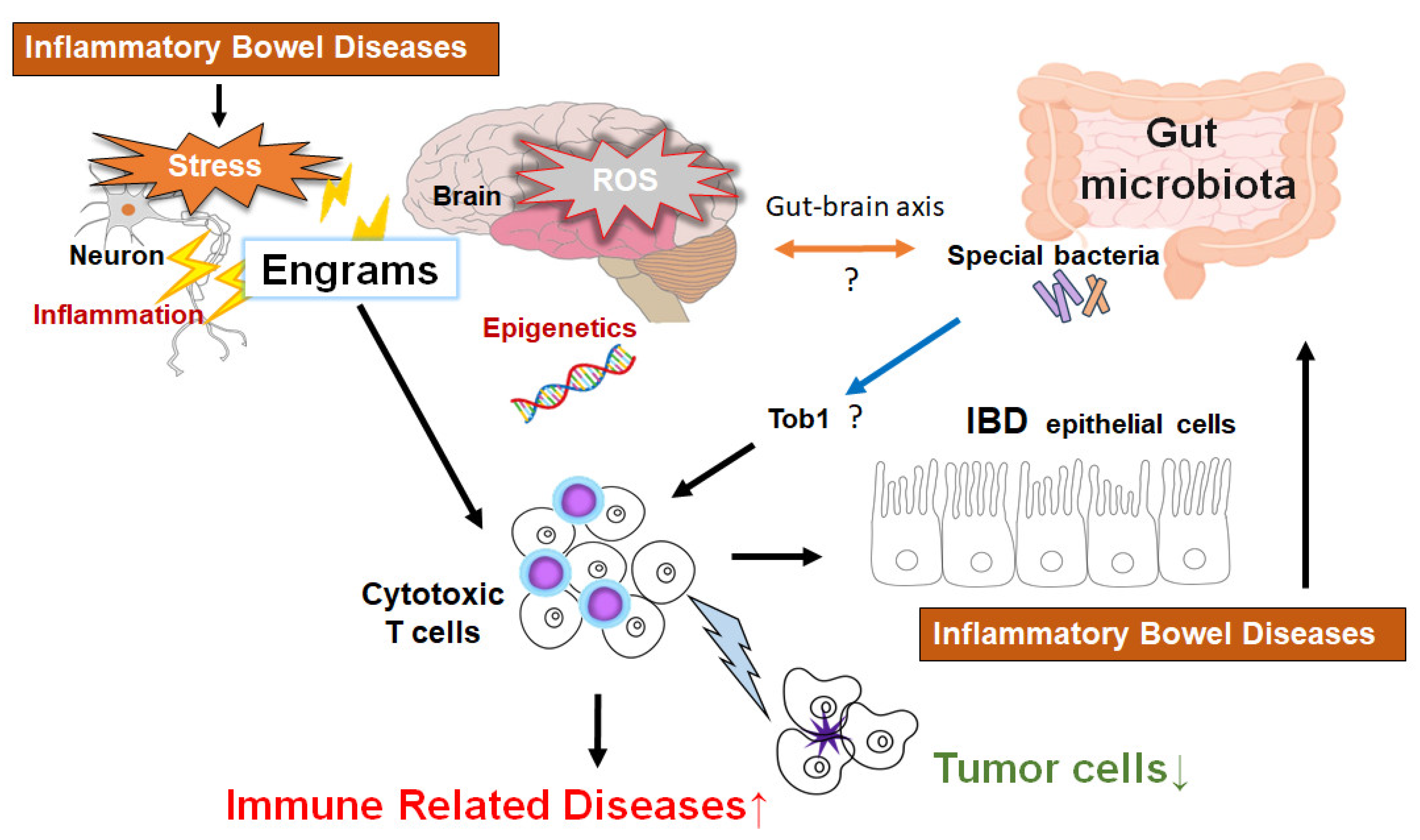
Figure 3.
Schematic representation of the hypothetical effects of gut microbiota and/or brain engrams for the activation of cytotoxic T cells in the pathogenesis of inflammatory bowel diseases. Engrams may be shaped in the condition of repeated inflammation with ROS and/or various oxidative stresses, which could employ active immune cells to damage colon epithelium, brain neurons, and/or cancer cells. If certain commensal bacteria in the gut could inhibit the expression of Tob1, an APRO family protein, which might consequently further stimulate the cytotoxic T cells for the reduction of tumors. Note that some critical pathways such as Wnt/beta-catenin signaling have been omitted for clarity. “?” means for authors’ speculation.
Figure 3.
Schematic representation of the hypothetical effects of gut microbiota and/or brain engrams for the activation of cytotoxic T cells in the pathogenesis of inflammatory bowel diseases. Engrams may be shaped in the condition of repeated inflammation with ROS and/or various oxidative stresses, which could employ active immune cells to damage colon epithelium, brain neurons, and/or cancer cells. If certain commensal bacteria in the gut could inhibit the expression of Tob1, an APRO family protein, which might consequently further stimulate the cytotoxic T cells for the reduction of tumors. Note that some critical pathways such as Wnt/beta-catenin signaling have been omitted for clarity. “?” means for authors’ speculation.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



