Submitted:
13 November 2024
Posted:
14 November 2024
You are already at the latest version
Abstract
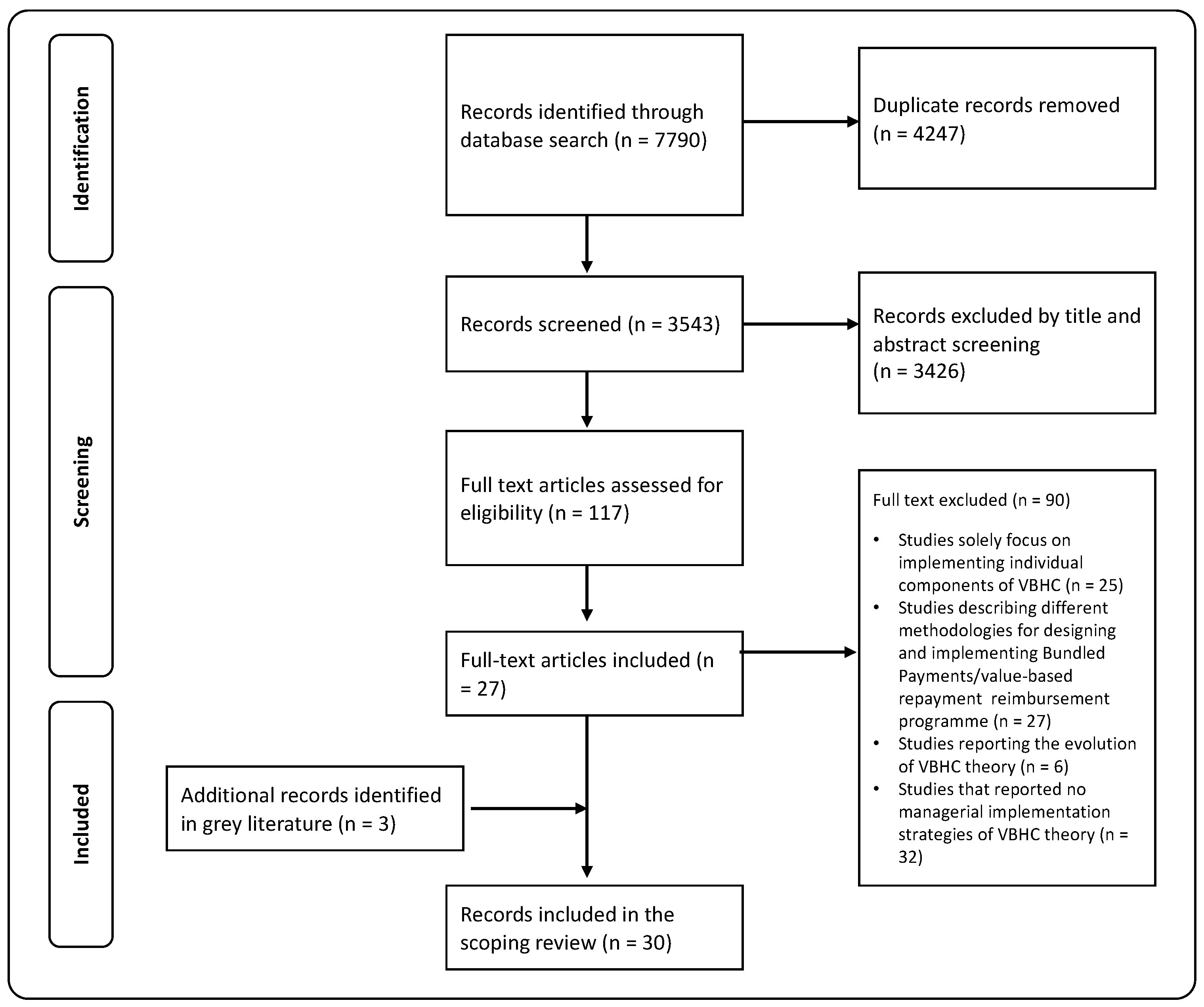
Background/Objectives: The principles of value-based Healthcare (VBHC) have received widespread endorsement, lead-ing healthcare organizations worldwide to shift their strategies towards them. However, despite growing recognition and acceptance, the actual implementation of value-based approaches varies widely. This research aims to identify studies that address the implementation of VBHC at dif-ferent levels (healthcare policymakers, hospital administrators, and healthcare providers), fo-cusing on each level’s relative strategies; Methods: To this end, a scoping review was conducted in accordance with the PRISMA extension for Scoping Reviews checklist. The electronic databases of Web of Science, PubMed, MEDLINE and Scopus were searched to identify relevant publica-tions in English from January 2006 to 31 July 2023; Results: We identified 30 eligible studies. Findings are organized into four main macro strategic levels, each comprising specific dimen-sions and operational approaches. Fourteen articles analyzed the role of government commitment in VBHC implementation, while six articles focused on regional integrated care systems. The role of hospitals was described in sixteen records; Conclusions: Our study suggests that a compre-hensive approach is necessary for the successful implementation of VBHC. Hospitals emerge as pivotal in this shift, requiring organizational and attitudinal changes among healthcare profes-sionals. However, a complete transition towards VBHC that ensures a seamless patient manage-ment throughout the entire care delivery value chain, necessitates government involvement in terms of state legislation, reimbursement methods, and hospital networking.
Keywords:
1. Introduction
2. Materials and Methods
2.1. Search Strategy
2.2. Study Eligibility
- They examined how government policies, network structures, and regulatory frameworks can support the transition to VBHC.
- They focused on hospital management strategies before implementation and throughout the process of adopting and sustaining VBHC practices.
- We have excluded studies:
- Solely focusing on implementing individual components of VBHC.
- Describing different methodologies for designing and implementing bundled payments/value-based repayment program reimbursement.
- Reporting the evolution of VBHC theory.
- Not reporting on any managerial implementation strategies of VBHC theory.
2.3. Study Selection
2.4. Quality Appraisal
2.5. Data Extraction, Analysis and Reporting
- Study identification (first author, title, publication year).
- Study characteristics (country, study design).
- Level of analysis (system level, hospital level).
- Disease area (if relevant).
- Dimensions analyzed.
- Barriers and/or success factors.
3. Results
Literature Synthesis
4.1. Government Commitment in Policies Definition
4.2. Organizational Vision and Cultural Integration
4.3. Operational Excellence
4.4. VBHC Assessment
4. Discussion
5. Conclusions
Author Contributions
Appendix A
Appendix B
References
- Larsson, S.; Lawyer, P.; Silverstein, M.B. From Concept to Reality: Putting Value-Based Health Care into Practice in Sweden. 2010, Boston Consulting Group.
- H: ME; Teisberg EO Redefining Health Care: Creating Value-Based Competition on Results; Boston: Harvard Business School Press, 2006.
- Porter, M.E. Value-Based Health Care Delivery. Annals of Surgery 2008, 248, 503–509. [Google Scholar] [CrossRef] [PubMed]
- Lega, F.; De Pietro, C. Converging Patterns in Hospital Organization: Beyond the Professional Bureaucracy. Health Policy 2005, 74, 261–281. [Google Scholar] [CrossRef] [PubMed]
- van Staalduinen, D.; van den Bekerom, P.; Groeneveld, S.; Kidanemariam, M.; Stiggelbout, A.; Van den Akker-van Marle, M. The Implementation of Value-Based Healthcare: A Scoping Review. BMC HEALTH SERVICES RESEARCH 2022, 22. [Google Scholar] [CrossRef] [PubMed]
- Plsek, P.E.; Greenhalgh, T. The Challenge of Complexity in Health Care. BMJ 2001, 323, 625–628. [Google Scholar] [CrossRef] [PubMed]
- Porter, M.; Lee, T. The Strategy That Will Fix Health Care. HARVARD BUSINESS REVIEW 2013, 91, 50–70. [Google Scholar]
- Krebs, F.; Engel, S.; Vennedey, V.; Alayli, A.; Simic, D.; Pfaff, H.; Stock, S. ; Cologne Res & Dev Network CoRe Net Transforming Health Care Delivery towards Value-Based Health Care in Germany: A Delphi Survey among Stakeholders. HEALTHCARE 2023, 11. [Google Scholar] [CrossRef]
- Ramos, P.; Savage, C.; Thor, J.; Atun, R.; Carlsson, K.; Makdisse, M.; Neto, M.; Klajner, S.; Parini, P.; Mazzocato, P. It Takes Two to Dance the VBHC Tango: A Multiple Case Study of the Adoption of Value-Based Strategies in Sweden and Brazil. SOCIAL SCIENCE & MEDICINE 2021, 282. [CrossRef]
- Larsson, S.; Clawson, J.; Howard, R. Value-Based Health Care at an Inflection Point: A Global Agenda for the Next Decade. Catalyst non-issue content 2023, 4.
- Steinmann, G.; Daniels, K.; Mieris, F.; Delnoij, D.; van de Bovenkamp, H.; van Der Nat, P. Redesigning Value-Based Hospital Structures: A Qualitative Study on Value-Based Health Care in the Netherlands. BMC HEALTH SERVICES RESEARCH 2022, 22. [Google Scholar] [CrossRef]
- Cossio-Gil, Y.; Omara, M.; Watson, C.; Casey, J.; Chakhunashvili, A.; Gutiérrez-San Miguel, M.; Kahlem, P.; Keuchkerian, S.; Kirchberger, V.; Luce-Garnier, V.; et al. The Roadmap for Implementing Value-Based Healthcare in European University Hospitals—Consensus Report and Recommendations. Value in Health 2022, 25, 1148–1156. [Google Scholar] [CrossRef]
- Tricco, A.C.; Lillie, E.; Zarin, W.; O’Brien, K.K.; Colquhoun, H.; Levac, D.; Moher, D.; Peters, M.D.J.; Horsley, T.; Weeks, L.; et al. PRISMA Extension for Scoping Reviews (PRISMA-ScR): Checklist and Explanation. Ann Intern Med 2018, 169, 467–473. [Google Scholar] [CrossRef]
- Arksey, H.; O’Malley, L. Scoping Studies: Towards a Methodological Framework. International Journal of Social Research Methodology 2005, 8, 19–32. [Google Scholar] [CrossRef]
- Munn, Z.; Peters, M.D.J.; Stern, C.; Tufanaru, C.; McArthur, A.; Aromataris, E. Systematic Review or Scoping Review? Guidance for Authors When Choosing between a Systematic or Scoping Review Approach. BMC Medical Research Methodology 2018, 18, 143. [Google Scholar] [CrossRef]
- Ng, S. A Qualitative Study on Relationships and Perceptions between Managers and Clinicians and Its Effect on Value-Based Healthcare within the National Health Service in the UK. HEALTH SERVICES MANAGEMENT RESEARCH 2022, 35, 251–258. [Google Scholar] [CrossRef] [PubMed]
- Conrad, D.; Grembowski, D.; Gibbons, C.; Marcus-Smith, M.; Hernandez, S.; Chang, J.; Renz, A.; Lau, B.; dela Cruz, E. A Report On Eight Early-Stage State And Regional Projects Testing Value-Based Payment. HEALTH AFFAIRS 2013, 32, 998–1006. [Google Scholar] [CrossRef]
- de Vries, E.; Drewes, H.; Struijs, J.; Heijink, R.; Baan, C. Barriers to Payment Reform: Experiences from Nine Dutch Population Health Management Sites. HEALTH POLICY 2019, 123, 1100–1107. [Google Scholar] [CrossRef]
- Phillips, R.; Cyr, J.; Keaney, J.; Messina, L.; Meyer, T.; Tam, S.; Korenda, K.; Darrigo, M.; Kumar, P.; Challapalli, S. Creating and Maintaining a Successful Service Line in an Academic Medical Center at the Dawn of Value-Based Care: Lessons Learned From the Heart and Vascular Service Line at UMass Memorial Health Care. ACADEMIC MEDICINE 2015, 90, 1340–1346. [Google Scholar] [CrossRef]
- Griffiths, E.; Odelade, O.; Gostkorzewicz, J.; Cordero, L. Demonstrating Proof of Concept for Value-Based Agreements in Europe: Two Real-World Cases. INTERNATIONAL JOURNAL OF TECHNOLOGY ASSESSMENT IN HEALTH CARE 2023, 39. [Google Scholar] [CrossRef]
- Conrad, D.; Grembowski, D.; Hernandez, S.; Lau, B.; Marcus-Smith, M. Emerging Lessons From Regional and State Innovation in Value-Based Payment Reform: Balancing Collaboration and Disruptive Innovation. MILBANK QUARTERLY 2014, 92, 568–623. [Google Scholar] [CrossRef]
- Nilsson, K.; Bååthe, F.; Andersson, A.E.; Wikström, E.; Sandoff, M. Experiences from Implementing Value-Based Healthcare at a Swedish University Hospital – a Longitudinal Interview Study. BMC Health Serv Res 2017, 17, 169. [Google Scholar] [CrossRef]
- Leao, D.; Cremers, H.; van Veghel, D.; Pavlova, M.; Hafkamp, F.; Groot, W. Facilitating and Inhibiting Factors in the Design, Implementation, and Applicability of Value-Based Payment Models: A Systematic Literature Review. MEDICAL CARE RESEARCH AND REVIEW 2023. [CrossRef]
- Daniels, K.; van der Voort, M.; Biesma, D.; van der Nat, P. Five Years’ Experience with Value-Based Quality Improvement Teams: The Key Factors to a Successful Implementation in Hospital Care. BMC HEALTH SERVICES RESEARCH 2022, 22. [Google Scholar] [CrossRef]
- Theunissen, L.; Cremers, H.-P.; Dekker, L.; Janssen, H.; Burg, M.; Huijbers, E.; Voermans, P.; Kemps, H.; Van Veghel, D. Implementing Value-Based Health Care Principles in the Full Cycle of Care: The Pragmatic Evolution of the Netherlands Heart Network. Circulation: Cardiovascular Quality and Outcomes 2023, 16, E009054. [Google Scholar] [CrossRef] [PubMed]
- Conrad, D.; Vaughn, M.; Grembowski, D.; Marcus-Smith, M. Implementing Value-Based Payment Reform: A Conceptual Framework and Case Examples. MEDICAL CARE RESEARCH AND REVIEW 2016, 73, 437–457. [Google Scholar] [CrossRef] [PubMed]
- van Veghel, D.; Soliman-Hamad, M.; Schulz, D.; Cost, B.; Simmers, T.; Dekker, L. Improving Clinical Outcomes and Patient Satisfaction among Patients with Coronary Artery Disease: An Example of Enhancing Regional Integration between a Cardiac Centre and a Referring Hospital. BMC HEALTH SERVICES RESEARCH 2020, 20. [Google Scholar] [CrossRef] [PubMed]
- van der Nat, P.; van Veghel, D.; Daeter, E.; Crijns, H.; Koolen, J.; Houterman, S.; Soliman, M.; de Mol, B. ; Meetbaar Beter Study Grp Insights on Value-Based Healthcare Implementation from Dutch Heart Care. INTERNATIONAL JOURNAL OF HEALTHCARE MANAGEMENT 2020, 13, 189–192. [Google Scholar] [CrossRef]
- van Veghel, H.; Dekker, L.; Theunissen, L.; Janssen, J.; Burg, M.; Huijbers, P.; Voermans, P.; van der Wees, P.; Cremers, H. Introducing a Method for Implementing Value Based Health Care Principles in the Full Cycle of Care: Using Atrial Fibrillation as a Proof of Concept. INTERNATIONAL JOURNAL OF HEALTHCARE MANAGEMENT 2022, 15, 1–9. [Google Scholar] [CrossRef]
- Lansdaal, D.; van Nassau, F.; van der Steen, M.; de Bruijne, M.; Smeulers, M. Lessons Learned on the Experienced Facilitators and Barriers of Implementing a Tailored VBHC Model in a Dutch University Hospital from a Perspective of Physicians and Nurses. BMJ OPEN 2022, 12. [Google Scholar] [CrossRef]
- van Veghel, D.; Daeter, E.; Bax, M.; Amoroso, G.; Blaauw, Y.; Camaro, C.; Cummins, P.; Halfwerk, F.; Hamer, I.; de Jong, J.; et al. Organization of Outcome-Based Quality Improvement in Dutch Heart Centres. EUROPEAN HEART JOURNAL-QUALITY OF CARE AND CLINICAL OUTCOMES 2020, 6, 49–54. [Google Scholar] [CrossRef]
- Kissam, S.; Beil, H.; Cousart, C.; Greenwald, L.; Lloyd, J. States Encouraging Value-Based Payment: Lessons From CMS’s State Innovation Models Initiative. MILBANK QUARTERLY 2019, 97, 506–542. [Google Scholar] [CrossRef]
- Chatfield, J.; Longenecker, C.; Fink, L.; Gold, J. Ten CEO Imperatives for Healthcare Transformation: Lessons From Top-Performing Academic Medical Centers. JOURNAL OF HEALTHCARE MANAGEMENT 2017, 62, 371–383. [Google Scholar] [CrossRef]
- Zipfel, N.; Van Der Nat, P.B.; Rensing, B.J.W.M.; Daeter, E.J.; Westert, G.P.; Groenewoud, A.S. The Implementation of Change Model Adds Value to Value-Based Healthcare: A Qualitative Study. BMC Health Services Research 2019, 19. [Google Scholar] [CrossRef]
- Nilsson, K.; Bååthe, F.; Erichsen Andersson, A.; Sandoff, M. The Need to Succeed – Learning Experiences Resulting from the Implementation of Value-Based Healthcare. LHS 2018, 31, 2–16. [Google Scholar] [CrossRef] [PubMed]
- Randazzo, G.; Brown, Z. Transitioning From Volume to Value: A Strategic Approach to Design and Implementation. Nursing administration quarterly 2016, 40, 130–136. [Google Scholar] [CrossRef] [PubMed]
- Goretti, G.; Marinari, G.; Vanni, E.; Ferrari, C. Value-Based Healthcare and Enhanced Recovery After Surgery Implementation in a High-Volume Bariatric Center in Italy. OBESITY SURGERY 2020, 30, 2519–2527. [Google Scholar] [CrossRef]
- Nilsson, K.; Baathe, F.; Andersson, A.; Sandoff, M. Value-Based Healthcare as a Trigger for Improvement Initiatives. LEADERSHIP IN HEALTH SERVICES 2017, 30, 364–377. [Google Scholar] [CrossRef]
- Collden, C.; Hellstrom, A. Value-Based Healthcare Translated: A Complementary View of Implementation. BMC HEALTH SERVICES RESEARCH 2018, 18. [Google Scholar] [CrossRef]
- Gray, C.F.; Parvataneni, H.K.; Bozic, K.J. Value-Based Healthcare: “Physician Activation”: Healthcare Transformation Requires Physician Engagement and Leadership. Clinical Orthopaedics and Related Research 2020, 478, 954–957. [Google Scholar] [CrossRef]
- Keswani, A.; Koenig, K.; Bozic, K. Value-Based Healthcare: Part 1-Designing and Implementing Integrated Practice Units for the Management of Musculoskeletal Disease. CLINICAL ORTHOPAEDICS AND RELATED RESEARCH 2016, 474, 2100–2103. [Google Scholar] [CrossRef]
- Hurh, J.; Ko, Y.; Lee, S. Value-Based Healthcare: Prerequisites and Suggestions for Full-Fledged Implementation in the Republic of Korea. JOURNAL OF THE KOREAN MEDICAL ASSOCIATION 2017, 60, 826–840. [Google Scholar] [CrossRef]
- Nilsson, K.; Baathe, F.; Andersson, A.; Sandoff, M. The Need to Succeed - Learning Experiences Resulting from the Implementation of Value-Based Healthcare. LEADERSHIP IN HEALTH SERVICES 2018, 31, 2–16. [Google Scholar] [CrossRef]
- The Past and Future of the Affordable Care Act | Health Care Economics, Insurance, Payment | JAMA | JAMA Network Available online:. Available online: https://jamanetwork.com/journals/jama/fullarticle/2533697 (accessed on 6 March 2024).
- van de Ven, W.P.M.M.; Beck, K.; Buchner, F.; Schokkaert, E.; Schut, F.T. (Erik); Shmueli, A. ; Wasem, J. Preconditions for Efficiency and Affordability in Competitive Healthcare Markets: Are They Fulfilled in Belgium, Germany, Israel, the Netherlands and Switzerland? Health Policy 2013, 109, 226–245. [Google Scholar] [CrossRef]
- Garattini, L.; Martini, M.B.; Nobili, A. Integrated care: la strada giusta per il futuro? Recenti Progressi in Medicina 2021, 112, 615–618. [Google Scholar] [PubMed]
- Kaplan, R.S.; Porter, M.E. How to Solve the Cost Crisis in Health Care. Harv Bus Rev 2011, 89, 46–52, 54, 56-61 passim. [Google Scholar] [PubMed]
- Kaplan, R.S. Improving Value with TDABC. Healthc Financ Manage 2014, 68, 76–83. [Google Scholar]

| FIRST AUTHOR | TITLE | YEAR | COUNTRY | STUDY DESIGN | LEVEL OF ANALYSIS | MAIN DIMENSIONS ANALYZED | BARRIERS | SUCCESS FACTORS |
|---|---|---|---|---|---|---|---|---|
| Sze May Ng [16] | A qualitative study on relationships and perceptions between managers and clinicians and its effect on value-based healthcare within the national health service in the UK | 2022 | UK | A qualitative study | Hospital level | Vision and strategy Teamwork and interprofessional relationship |
There was often mistrust between clinicians and managers, with both being dismissive of each other's work. | Strong clinical leadership and medical engagement at all levels. Developed cultures where managers and clinicians are motivated and supported to work in partnerships. |
| Douglas Conrad [17] | A Report On Eight Early-Stage State And Regional Projects Testing Value-Based Payment | 2013 | US | A case study design | Government commitment | Value-based payment (VBP) | It requires time and resources, in addition to culture change. | State legislation can galvanize regional and state payment reform initiatives. Previous experience in the development, implementation, and evaluation of VBP models |
| Eline F de Vries [18] | Barriers to payment reform: Experiences from nine Dutch population health management sites | 2019 | Netherlands | A qualitative study | Government commitment | Value-based payment (VBP) | Information asymmetry as barrier towards payment reform. Hesitation to accept greater financial accountability. |
// |
| Robert A. Phillips [19] | Creating and Maintaining a Successful Service Line in an Academic Medical Center at the Dawn of Value-Based Care: Lessons Learned From the Heart and Vascular Service Line at UMass Memorial Health Care | 2015 | US | A case study design | Hospital level | Teamwork and interprofessional relationship | The traditional departmental structure made difficult to fully shift towards disease-oriented organization. | Dedicated leadership with accountability and responsibility for budget. |
| Elizabeth A. Griffiths [20] | Demonstrating proof of concept for value-based agreements in Europe: two real-world cases | 2023 | UK | A case study design | Government commitment | Value-based agreements (VBAs) | The limited experience of both parties in working together on VBAs. It took time to develop a dialogue between the relevant stakeholders and to determine partners willing to collaborate on scheme design. |
Engagement of core stakeholders (payers, manufacturers, and physicians) was critical. |
| Douglas Conrad [21] | Emerging Lessons From Regional and State Innovation in Value-Based Payment Reform: Balancing Collaboration and Disruptive Innovation | 2014 | UK | A qualitative study | Government commitment | Value-based payment (VBP) Development and implementation health IT infrastructure |
The prevalence of disparate EHR systems that are not interoperable or cannot adapt to one another. | Previous experience in the development, implementation, and evaluation of VBP models. Pressure from policymakers, regulators, and organized public and private purchasers. |
| Kerstin Nilsson [22] | Experiences from implementing valuebased healthcare at a Swedish University Hospital – a longitudinal interview study | 2017 | Sweden | A mixed (explorative and qualitative) design | Hospital level | Anchoring the new approach in the hospital organizational culture Cost measurement |
The lack of IT systems supporting VBHC. The traditional departmental structure made difficult to fully shift towards disease-oriented organization. Measure costs was particularly difficult to establish as the hospital accounting system only allowed data capture on an aggregated level. |
Leadership skills such as communication and motivation to get people involved step by step in developing the process. |
| Diogo LL Leao [23] | Facilitating and Inhibiting Factors in the Design, Implementation, and Applicability of Value-Based Payment Models: A Systematic Literature Review | 2023 | Netherlands | A Systematic Literature Review | Government commitment | Value-based payment (VBP) | It requires time and resources. | Previous experience in the development, implementation, and evaluation of VBP models. High motivation, engagement, and trust among involved stakeholders. Transparency and communication among involved stakeholders. |
| Kirsten Daniels [24] | Five years' experience with value-based quality improvement teams: the key factors to a successful implementation in hospital care | 2022 | Netherlands | A qualitative study | Hospital level | Vision and strategy Teamwork and interprofessional relationship Cost measurement |
The traditional departmental structure made difficult to fully shift towards disease-oriented organization. Hospital care is still paid according to pay-for-volume contracts, and budget responsibility still lies with the traditional functional departments. |
To have one team that addresses all quality-improvement related topics. |
| Luc Theunissen [25] | Implementing Value-Based Health Care Principles in the Full Cycle of Care: The Pragmatic Evolution of the Netherlands Heart Network | 2023 | Netherlands | A case study design | Regional integrated care system | Teamwork and interprofessional relationship Cost measurement |
The traditional departmental structure made difficult to fully shift towards disease-oriented organization. Hospital care is still paid according to pay-for-volume contracts, and budget responsibility still lies with the traditional functional departments. |
Platform where organizations can connect to share data and best practices. |
| Douglas Conrad [26] | Implementing Value-Based Payment Reform: A Conceptual Framework and Case Examples | 2015 | US | A Conceptual Framework and Case Examples | Government commitment | Value-based payment (VBP) | // | Clear and consistent communication about movement toward larger reforms. |
| Dennis van Veghel [27] | Improving clinical outcomes and patient satisfaction among patients with coronary artery disease: an example of enhancing regional integration between a cardiac centre and a referring hospital | 2020 | Netherlands | An observational cohort study design | Regional integrated care system | Integrated care | // | Trust and cooperation with other institutes. |
| P. B. van der Nat [28] | Insights on value-based healthcare implementation from Dutch heart care | 2020 | Netherlands | A case study design | Regional integrated care system | Integrated care | // | Trust and cooperation with other institutes. Platform where organizations can connect to share data and best practices. |
| H. P. A. van Veghel [29] | Introducing a method for implementing value based health care principles in the full cycle of care: Using atrial fibrillation as a proof of concept | 2020 | Netherlands | A case study design | Regional integrated care system | Integrated care | // | Platform where organizations can connect to share data and best practices. |
| Pedro Ramos [9] | It takes two to dance the VBHC tango: A multiple case study of the adoption of value-based strategies in Sweden and Brazil | 2021 | Sweden & Brasil | A comparative multiple case study | Hospital level | Teamwork and interprofessional relationship Cost measurement |
The traditional departmental structure made difficult to fully shift towards disease-oriented organization. Financing of care was not aligned with the care production and outcomes monitoring. |
The involvement of clinical staff was a crucial factor. |
| Dane Lansdaal [30] | Lessons learned on the experienced facilitators and barriers of implementing a tailored VBHC model in a Dutch university hospital from a perspective of physicians and nurses | 2021 | Netherlands | A descriptive qualitative study | Hospital level | Vision and strategy Support of information technology |
The usage of the EHR in daily practice. | Continued recognition of the usefulness of the VBHC implementation. |
| Dennis van Veghel [31] | Organization of outcome-based quality improvement in Dutch heart centres | 2020 | Netherlands | A mixed-method approach | Regional integrated care system | Quality improvement initiatives (QI) | Insufficient data infrastructure for successful outcome-based quality improvement. | // |
| Gijs Steinmann [11] | Redesigning value-based hospital structures: a qualitative study on value-based health care in the Netherlands | 2022 | Netherlands | A qualitative exploratory study | Hospital level | Teamwork and interprofessional relationship Cost measurement |
The traditional departmental structure made difficult to fully shift towards disease-oriented organization. Measuring costs was particularly difficult as the hospital accounting system only allowed data collection on an aggregated level. |
To have multiple leaders, each representing a particular organizational component. |
| Kissam SM [32] | States Encouraging Value-Based Payment: Lessons From CMS’s State Innovation Models Initiative | 2019 | US | A qualitative study | Government commitment | Value-based payment (VBP) | Lack of multipayer alignment around VBP models. Restrictions on the ability to share patient data across all care providers |
// |
| J. Seth Chatfield [33] | Ten CEO Imperatives for Healthcare Transformation: Lessons From Top-Performing Academic Medical Centers | 2017 | US | A mixed-method approach | Hospital level | Vision and strategy Anchoring the new approach in the hospital organizational culture |
// | To have a common shared vision and align goals at all the levels with that vision. Effective communication. |
| Nina Zipfel [34] | The implementation of change model adds value to value-based healthcare: a qualitative study | 2019 | Netherlands | A case study design | Hospital level | Vision and strategy Anchoring the new approach in the hospital organizational culture |
An implementation approach was lacking to guide improvement interventions. | Multi-stakeholders’ involvement in the design of the intervention played an important role in the success of the implementation. |
| Dorine J. van Staalduinen [5] | The implementation of value-based healthcare: a scoping review | 2022 | Netherlands | A scoping review | Hospital level | Anchoring the new approach in the hospital organizational culture | // | Creating and enhancing leadership was also considered essential in transforming to VBHC. |
| Kerstin Nilsson [35] | The need to succeed – learning experiences resulting from the implementation of value-based healthcare | 2018 | Sweden | An explorative design | Hospital level | Vision and strategy Cost measurement |
Measuring costs was particularly difficult as the hospital accounting system only allowed data collection on an aggregated level. | The importance of planning and preparation before starting the implementation process. |
| Geralyn Randazzo [36] | Transitioning From Volume to Value. A Strategic Approach to Design and Implementation | 2016 | US | A case study design | Regional integrated care system | Integrated care Support of information technology |
// | Platform where organizations can connect to share data and best practices. The Care Navigator role to assist the patients during their transition from the inpatient setting back to the community. |
| Giulia Goretti [37] | Value-Based Healthcare and Enhanced Recovery After Surgery Implementation in a High-Volume Bariatric Center in Italy | 2020 | Italy | A case study design | Hospital level | Teamwork and interprofessional relationship | // | Engaging patients and their representatives during the implementation work. |
| Kerstin Nilsson [38] | Value-based healthcare as a trigger for improvement initiatives | 2017 | Sweden | An explorative design study | Hospital level | Teamwork and interprofessional relationship | // | To create an open and trusting communication environment to succeed with developing processes. |
| Christian Colldén [39] | Value-based healthcare translated: a complementary view of implementation | 2018 | Sweden | A case study design | Hospital level | Support of information technology | The lack of IT systems supporting VBHC. | // |
| Chancellor F. Gray [40] | Value-based Healthcare: "physician Activation": Healthcare Transformation Requires Physician Engagement and Leadership | 2020 | US | Hospital level | Teamwork and interprofessional relationship | Communication barriers between the physician and nonphysician health system leaders. | // | |
| Aakash Keswani [41] | Value-based Healthcare: Part 1-Designing and Implementing Integrated Practice Units for the Management of Musculoskeletal Disease | 2016 | US | A case study design | Hospital level | Teamwork and interprofessional relationship | // | Engaging and activating patients throughout the care cycle, incorporating patients’ goals and preferences in treatment decisions (via SDM). Strong clinical leadership to promote teamwork, collaboration and joint accountability for patient outcomes and overall cost of care. |
| Joon Hurh [42] | Value-based healthcare: prerequisites and suggestions for full-fledged implementation in the Republic of Korea | 2017 | Republic of Korea | A case study design | Government commitment | Value-based payment (VBP) | // | Commitment and support from healthcare providers by normalizing payment rates for healthcare providers. |
| Strategic level | Dimension | Operational strategies | References |
|---|---|---|---|
| Government commitment in policies definition | Value-based payment (VBP) | Providing more guidance or assistance in payment reforms through a long-term vision with information on the implementation and potential impact of payment reforms. | [18,20,24,26] |
| Creating a sense of urgency for implementing payment reforms. | [18,21,23,26,42] | ||
| Defining national or local legislation. | [17,21,23,42] | ||
| Involving key stakeholders in the change process and implementation of the models. | [17,23] | ||
| Allocating significant resources toward payment and delivery system innovations. | [21] | ||
| Value-based agreements (VBAs) |
Legal/regulatory policies permitting innovative contracting (e.g., net price confidentiality). | [20] | |
| Policy supporting appropriate data capture and use to support contracting. | [20] | ||
| Collaborating and engaging with the medical device industry. | [42] | ||
| Organizational Vision and Cultural Integration |
Vision, strategy and governance structures | Having an official commitment to value-based redesign from the higher levels of the organization. | [11,16,24,30,34,35,38] |
| Embedding the adoption of the VBHC concept in the hospital strategy, policy documents, and planning and control. | [19,33] | ||
| Providing formal responsibility and mandate to a steering group with hospital representatives for the implementation of VBHC. | [5,16,19,24,25,27,29,30,31,33,34,35,39] | ||
| Empowerment of service line leadership with direct accountability and authority over programs and budgets. | [19,33] | ||
| Developing a tailored business plan to provide a structured process clear, goal-oriented and adaptable to each situation. | [9,24,33,34,39] | ||
| Being supported by consultancyies. | [5,22,34,35,39] | ||
| Starting with "experiments" and "pilots”. | [11,22,25,34,39] | ||
| Planning and preparation before starting the implementation process. | [35,38,39] | ||
| Anchoring the new approach to the hospital organizational culture | Staff training and education on the VBHC concept. | [5,11,19,24,31,33,35,36] | |
| Improving communication and information with staff about the change. | [5,22,25,33,35,36,37] | ||
| Providing time for healthcare professionals to work on the project and anchoring changes to their daily work. | [22,24,30,34,35] | ||
| Continued recognition of the usefulness of the VBHC implementation. | [30,35,38] | ||
| Starting with positive results. | [22,24,30,34] | ||
| Motivating people to get them involved step by step in developing the process. | [11,22,33] | ||
| Involving patients and their representatives in the implementation process. | [9,24,30,35,37,39,41] | ||
| Operational excellence | Standardize care pathways | Defining transmural care standard. | [9,26,27,29] |
| Hiring additional staff dedicated to care coordination to connect the territory and the hospital. | [17,26,32,36] | ||
| Participating in peer-to-peer learning collaboratives on implementing new delivery models or enhancing care coordination. | [32] | ||
| Planning and attendance of periodical networking meetings. | [26,29] | ||
| Defining and optimizing Critical Pathways (CPs). | [9,11,26,27,37,41] | ||
| Using liaison positions (such as “intermediary managers”) to enhance coordination between functional units. | [5,9,11,36,38] | ||
| Appling the lean-methodology. | [24] | ||
| Developing multidisciplinary teams |
Engaging all professionals involved in the different levels of one patient’s care | [9,19,34,38,41] | |
| Planning and attendance of regularly institutionalized meetings ("standing committees"). | [5,11,24] | ||
| Sharing workspace. | [24] | ||
| Creating multidisciplinary meetings to discuss complex patients. | [9,27] | ||
| IT support | Setting up innovative data sharing mechanisms to provide real time data to providers. | [17,18,20,21,26,42] | |
| Setting up care and information technology platforms to facilitate both patients and healthcare professionals. | [22,24,35,36] | ||
| Creating dashboards containing outcome measurements, PROMS/PREMS and costs. | [12, 29, 31] | ||
| Additional resources | Availability of additional support staff (data analysts/project leaders/care managers). | [9,24,35] | |
| VBHC assessment | Clinical Outcome measurement | Identifying and collecting relevant clinical outcome measurements. | [9,11,22,24,26,27,28,29,30,31,33,35,36,37,39,40] |
| Mapping the care processes for each respective group of patients. | [22,39] | ||
| Benchmarkingoutcome data among hospitals. | [11,24,28,31,39] | ||
| Obtaining, processing, and dispersing data in a time-efficient manner for internal reflection. | [11,28,30,31,33,40,41] | ||
| Explaining the clinical outcome measurements more pedagogically. | [43] | ||
| Simplifying PowerPoint presentations of outcomes measured. | [43] | ||
| Patient-reported measures | Collecting data regarding patient reported measures (PROMS e PREMs). | [24,26,27,30,37,40] | |
| Costs measurement | Measuring costs based on actual resource use over the full cycle of care for the patient's condition. | ||
| Audit & Feedback (A&F) | Performing “Audit and Feedback” (A&F). | [27,29] |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).



