
Submitted:
09 November 2024
Posted:
13 November 2024
You are already at the latest version
Abstract
Metabolic dysfunction-associated steatotic liver disease (MASLD) has become increasingly recognized as a postoperative complication in patients undergoing pancreatic surgeries, particularly pancreaticoduodenectomy (PD). Given MASLD’s prevalence and impact on liver function and postoperative outcomes, understanding its incidence, risk factors, and potential interventions is critical for patient care. This study reviewed the relation between MASLD and PD. Studies indicate that MASLD’s incidence ranges from 13.2% to 31% in post-PD patients, with notable variation influenced by factors such as sex, body mass index, and nutritional deficiencies. PD, performed to treat pancreatic or bile duct disease, is associated with considerable postoperative physiological changes. These include disruptions in pancreatic enzyme production, which can impair digestion, metabolism, and potentially contribute to MASLD in susceptible patients. Patients with MASLD post-PD show lower liver-to-spleen attenuation ratios on imaging and often require intensified pancreatic enzyme replacement. A scoring system based on risk factors has been developed to identify patients at higher risk of MASLD and guide preventive nutritional support. MASLD is a prevalent complication post-PD that impacts recovery and treatment continuity in cancer patients. Early risk stratification, tailored enzyme therapy, and ongoing monitoring may reduce MASLD-related liver impairment, enhancing patient outcomes.
Keywords:
NAFLD
; Pancreas
; Bile duct
; Hepatic Steatosis
; Outcome
Background
Metabolic dysfunction-associated steatotic liver disease (MASLD), formerly known as non-alcoholic fatty liver disease (NAFLD), has emerged as a significant global health concern, affecting approximately 25-40% of the world’s population [1,2]. This chronic liver condition is closely associated with metabolic syndrome, obesity, and type 2 diabetes mellitus [3]. As the prevalence of MASLD continues to rise, its impact on various aspects of patient care, including surgical outcomes, has become increasingly apparent [2,4,5].
Pancreaticoduodenectomy (PD), also known as the Whipple procedure, is a complex surgical intervention primarily used to treat pancreatic cancer and other periampullary malignancies. This procedure involves the removal of the head of the pancreas, along with portions of the duodenum, bile duct, and occasionally part of the stomach[6]. Given the intricate nature of this operation and its potential for complications, understanding the influence of comorbidities such as MASLD on surgical outcomes is crucial.
This review aims to explore the intersection of MASLD and PD, and the prevalence of hepatic steatosis post-PD.
Metabolic Dysfunction-Associated Steatotic Liver Disease
MASLD prevalence is increasing in parallel with the obesity epidemic and metabolic syndrome[2]. Recent epidemiological studies estimate notable variations across different regions and ethnicities[7,8].
The rising prevalence of MASLD is closely associated with several well-established risk factors. Obesity, particularly central adiposity, is the most significant contributor, with studies showing that up to 90% of severely obese individuals may have some degree of hepatic steatosis. Type 2 diabetes mellitus is another major risk factor, with an estimated 55-70% of patients with type 2 diabetes also having MASLD. Other important risk factors include insulin resistance, dyslipidemia, and metabolic syndrome [2,3,9].
Genetic factors also play a crucial role in MASLD susceptibility[10]. Genome-wide association studies have identified several genetic variants associated with increased risk, including PNPLA3, TM6SF2, and MBOAT7 (Figure 1) [11,12,13]. These genetic factors may explain the variability in MASLD prevalence and severity among different ethnic groups.
Age and sex are additional factors influencing MASLD prevalence[14]. The condition is more common in older individuals, with a peak prevalence typically observed in the fifth to sixth decades of life[15,16]. While earlier studies suggested a higher prevalence in men[17], recent data indicate that postmenopausal women may be at increased risk, possibly due to hormonal changes affecting lipid metabolism[18].
MASLD encompasses a spectrum of liver pathology, ranging from simple steatosis to more advanced stages characterized by inflammation, fibrosis, and ultimately cirrhosis[19]. The progression of MASLD is typically described in several stages, including simple steatosis, steatohepatitis, fibrosis, and cirrhosis [19,20,21].
Simple Steatosis is initial stage and is characterized by excessive fat accumulation in hepatocytes, typically affecting more than 5% of liver cells. While often considered benign, recent evidence suggests that even simple steatosis may not be entirely innocuous[22,23].
Steatohepatitis involves hepatic fat accumulation accompanied by inflammation and hepatocyte injury[24]. It is characterized histologically by ballooning degeneration of hepatocytes, inflammatory infiltrates, and often the presence of Mallory-Denk bodies[25,26].
Progressive inflammation and cellular injury lead to the activation of hepatic stellate cells and the deposition of extracellular matrix, resulting in fibrosis[27]. The degree of fibrosis can range from mild (stage F1) to severe (stage F4 or cirrhosis) [28].
Cirrhosis is the most advanced stage of MASLD, characterized by extensive fibrosis, distortion of the liver architecture, and impaired liver function [29]. Cirrhosis significantly increases the risk of hepatocellular carcinoma and liver failure [30].
The progression of MASLD is not linear, and not all individuals with simple steatosis will progress to more advanced stages. Factors influencing disease progression include the severity of metabolic dysfunction, genetic predisposition, and lifestyle factors such as diet and physical activity [31,32].
Recent research has also highlighted the dynamic nature of MASLD progression, with the potential for disease regression, particularly in earlier stages, through lifestyle modifications and improved metabolic control[33,34]. However, once significant fibrosis has developed, the potential for reversal becomes more limited[35].
Overview of Pancreaticoduodenectomy
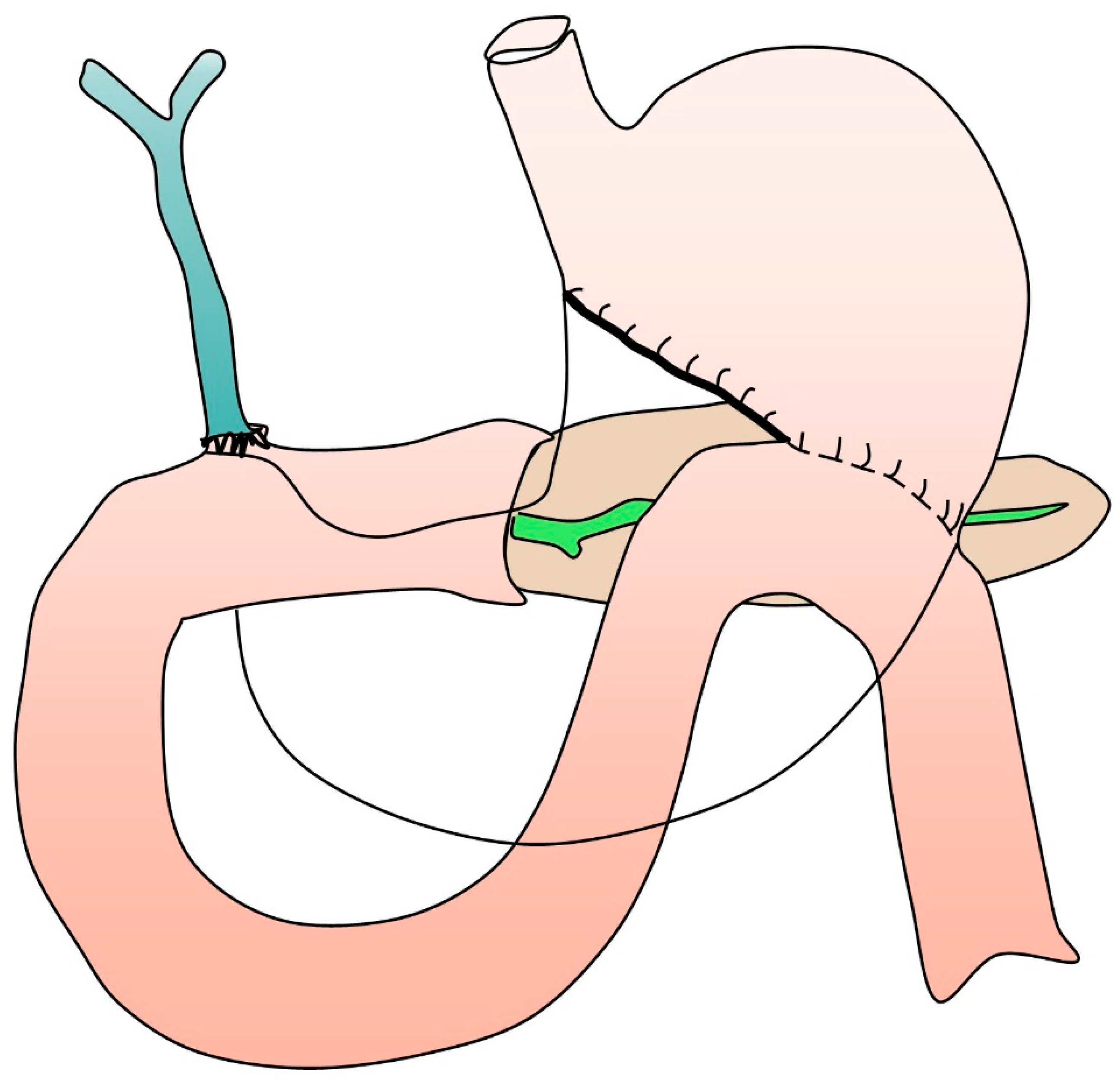
Pancreaticoduodenectomy remains one of the most complex and challenging abdominal surgeries performed today (Figure 2) [6]. This intricate operation involves the removal of the head of the pancreas, the duodenum, the gallbladder, and part of the bile duct, followed by a complex reconstruction of the gastrointestinal tract[36]. Recent advances in surgical techniques, including minimally invasive approaches, have improved outcomes and expanded the procedure’s applicability[37,38]. A 2024 meta-analysis by Tang et al. demonstrated that robotic PD is associated with reduced blood loss and shorter hospital stays compared to open surgery, albeit with longer operative times[39].
The primary indication for PD remains the treatment of malignant neoplasms of the pancreatic head, distal common bile duct, and periampullary region[40]. However, its application has expanded to include select benign conditions such as chronic pancreatitis and intraductal papillary mucinous neoplasms (IPMNs) with high-risk features[41]. Studies highlighted the importance of precise patient selection, showing that adherence to evidence-based criteria for resection of IPMNs can significantly reduce unnecessary surgeries while maintaining oncological safety[42,43].
Despite advancements in surgical techniques and perioperative care, PD is associated with significant morbidity[44]. The most dreaded complication remains postoperative pancreatic fistula (POPF), occurring in 5-30% of cases and potentially leading to life-threatening sequelae[45,46]. A study demonstrated that transpapillary pancreatic duct stenting did not significantly reduces the rate of clinically relevant POPF in patients[47]. Other common complications include delayed gastric emptying, postpancreatectomy hemorrhage, and surgical site infections[48,49]. Recent data from high-volume centers report mortality rates below 5%, with five-year survival rates for pancreatic adenocarcinoma improving to 20-30% in selected patients, particularly those receiving multimodal therapy[50,51].
The landscape of PD continues to evolve, with ongoing research focusing on personalized approaches to patient care. Studies explored the use of circulating tumor DNA (ctDNA) analysis for early detection of recurrence following PD, potentially allowing for more timely interventions [52,53,54,55]. Additionally, the integration of artificial intelligence in preoperative planning and intraoperative decision-making is an exciting frontier[56,57]. The potential of machine learning algorithms to predict POPF risk with higher accuracy than traditional scoring systems, paving the way for tailored perioperative management strategies[58,59,60,61].
MASLD in Patients After Undergoing Pancreaticoduodenectomy
The precise etiology of steatotic liver disease following PD remains elusive; however, researchers have postulated that postoperative malnutrition, stemming from pancreatic exocrine insufficiency, may be a contributing factor[62]. Isolated cases of hepatic failure secondary to steatohepatitis have been documented as a potential complication following PD, though such occurrences are infrequent[63].
The prevalence of MASLD in patients who have undergone PD has garnered increasing attention in recent years, as the metabolic consequences of this complex surgery become more apparent.
The development and impact of MASLD following pancreatic surgery, particularly PD, have garnered attention due to significant implications for patient outcomes. Tanaka’s findings underline a 23% prevalence of MASLD in patients post-PD, observing that non-obesity and absence of hyperlipidemia characterize this form of MASLD. A crucial association with pancreatic exocrine insufficiency was noted, with pancreatic enzyme supplementation significantly reducing steatosis and restoring biochemical balance. This suggests that pancreatic enzyme insufficiency may be a vital contributor to MASLD after PD and highlights the potential of enzyme therapy as a targeted intervention for patients with post-PD MASLD[64].
Expanding on this, Kato et al. [65] documented MASLD incidence at 19.6% following total pancreatectomy (TP), identifying female sex, elevated BMI, and postoperative diarrhea as independent risk factors. In Kato’s study, MASLD resolved spontaneously in 37.9% of patients within a year, indicating a potential self-limiting course in certain cases. This variation in disease trajectory emphasizes the need to consider individual patient risk profiles and demonstrates that postoperative MASLD may differ in severity and duration depending on specific patient factors [65].
Nakagawa’s study reported a MASLD incidence of 25% after PD, underscoring that postoperative pancreatic exocrine insufficiency (PEI) is the sole independent risk factor for MASLD. The correlation between MASLD incidence and low liver-to-spleen CT attenuation ratios suggests that imaging markers may serve as valuable predictors for MASLD in patients undergoing PD. These findings echo Tanaka’s results and underscore PEI as a crucial factor, potentially necessitating more consistent and rigorous management of enzyme replacement postoperatively[66].
In efforts to predict MASLD risk, Kato et al. proposed a postoperative scoring system, identifying pancreatic adenocarcinoma and postoperative diarrhea as significant predictors. Kato’s system correlates higher scores with increased MASLD prevalence (up to 93% for scores of 7–10), supporting a preventative approach by highlighting patients who would benefit most from nutritional intervention. This proactive strategy is especially relevant, as these patients are at higher risk of progressing from MASLD to NASH, complicating recovery and increasing liver disease burden[67].
Huang and colleagues emphasized that MASLD can disrupt essential adjuvant chemotherapy in cancer patients, with MASLD patients experiencing higher chemotherapy discontinuation rates (55.9%) than non-MASLD patients. This underscores MASLD’s significant clinical impact, particularly in cancer patients, where treatment delays can adversely affect prognosis. Huang’s findings reinforce the need for integrated management strategies addressing both MASLD prevention and continuity of cancer therapy to optimize patient outcomes post-surgery[68].
Additionally, Fujii’s radiomics-based study highlights preoperative CT-derived radiomic features as potential predictors for MASLD post-PD. By incorporating both clinical and radiomic parameters, Fujii’s predictive model achieved higher precision (72.7%) and recall (66.7%) than a solely clinical model, suggesting that advanced imaging techniques could improve MASLD risk stratification. This radiomics approach represents a step towards personalized risk assessment, allowing for targeted preventive measures in high-risk patients[69].
In a Belgian cohort, D’Cruz reported a 31% MASLD prevalence post-pancreatic surgery, with persistent cases observed up to two years postoperatively. The study linked MASLD occurrence to preoperative liver enzyme levels and weight loss, suggesting that long-term follow-up is essential[70]. These findings underscore that MASLD can present as both an early and late complication, necessitating prolonged monitoring and potential intervention to mitigate its progression and impact on liver function.
In a recent study by Shibata et al.[71], the incidence and clinical characteristics of hepatic steatosis following pancreatectomy, researchers have shed light on this growing concern in post-operative care. The study, which involved 104 patients who underwent pancreatic surgery, revealed that 20% of participants developed hepatic steatosis postoperatively. Notably, the research identified several risk factors for the development of hepatic steatosis, including a low neutrophil-to-lymphocyte ratio (NLR) in the overall cohort, and younger age, higher lymphocyte-to-monocyte ratio, and lymph node metastasis specifically in patients who underwent pancreaticoduodenectomy. These findings suggest a potential link between immune-nutritional parameters and the risk of postoperative hepatic steatosis, which could have significant implications for patient monitoring and management. The study also evaluated the effectiveness of pancrelipase administration at 900mg/day as a treatment for hepatic steatosis, with promising results. While some patients improved with dose escalation, others showed improvement without it, indicating that individualized treatment approaches may be necessary. However, it is important to note that the sample size for this aspect of the study was relatively small, and further research with larger cohorts is needed to confirm these findings and establish optimal dosing strategies for pancreatic enzyme replacement therapy in preventing and treating postoperative hepatic steatosis.
Izumi’s study emphasizes the impact of postoperative body mass index (BMI) and pancreatic cancer on the risk of MASLD following PD. The study’s data, which includes 101 patients, reveals that a lower postoperative BMI is linked to fat deposition (Hazard ratio (HR) of 0.56, p = 0.042), while pancreatic cancer presents as a strong risk factor for MASLD (HR 4.42, p = 0.034)[72]. These findings highlight how weight management and cancer-associated metabolic stress can exacerbate liver complications after PD, suggesting that BMI maintenance might serve as an important focus in postoperative care.
Fujii’s research identifies additional risk factors over time, examining a larger cohort of 196 patients and revealing that MASLD prevalence varies postoperatively: 12% at one month, rising to 21% at six months, then slightly dropping to 15% at one year. Significantly, female patients with decreased serum copper (Cu) appear to be at a higher risk across these time points, suggesting that micronutrient deficiencies and gender-specific responses to pancreatic exocrine insufficiency may drive MASLD progression. Fujii’s emphasis on copper reduction aligns with broader studies on micronutrient impacts on hepatic function, indicating that serum Cu levels could be monitored to identify at-risk groups[73].
Yoo’s study further distinguishes hepatic steatosis patterns, reporting a notable difference in MASLD occurrence between patients undergoing pylorus-preserving PD (PPPD) and those with bile duct resections (BDR). While PPPD patients showed a five-year MASLD incidence of 26.7%, BDR patients had only a 3.7% incidence (p < 0.001). Yoo’s findings suggest a link between the surgical technique and the sustained incidence of MASLD, indicating the need for multicenter studies to better understand the pathophysiological mechanisms behind these observed differences[74]. The persistence of MASLD in the PPPD cohort hints that PPPD may lead to prolonged changes in hepatic metabolism, possibly due to altered bile acid regulation or extended digestive changes.
Yu’s work on CT liver attenuation post-PD adds valuable insights into radiological changes associated with MASLD. Observing a significant decline in liver attenuation (from 52.3 to 47.6 Hounsfield units, p = 0.044) and a reduced liver-to-spleen attenuation ratio (1.12 to 1.01, p = 0.033), Yu suggests that these imaging biomarkers could serve as early indicators of MASLD onset post-PD[75].
Lastly, Ito’s findings spotlight intraoperative blood loss as an independent risk factor for MASLD development post-PD, with blood loss correlating strongly with the incidence of steatohepatitis (HR = 1.0001, p = 0.016)[76]. This critical link between surgical blood loss and MASLD risk underscores the importance of intraoperative management. Collectively, these studies underscore the multifactorial nature of MASLD post-PD, with risk factors spanning surgical, demographic, nutritional, and metabolic domains. Future studies could prioritize exploring the interactive effects of these variables, aiming to develop comprehensive MASLD prevention strategies for post-PD patients.
In an examination of MASLD in patients after pancreatoduodenectomy, recent findings have shed light on the prevalence, risk factors, and potential management strategies for this condition. A retrospective study of 120 patients who underwent pancreatoduodenectomy revealed a high occurrence rate of MASLD, with 38% of patients developing the condition postoperatively. Notably, the study identified several independent risk factors for MASLD development, including high body mass index, small pancreatic volume, prolonged operative time, and elevated aspartate aminotransferase/alanine aminotransferase ratio one month post-surgery. These findings underscore the importance of careful patient selection and perioperative management to mitigate the risk of MASLD. Interestingly, the study also explored the potential benefits of pancreatic enzyme supplementation therapy, suggesting a trend towards lower MASLD occurrence in patients receiving prophylactic supplementation (27% vs. 43%, p = 0.082). Furthermore, the recovery rates from MASLD were notably higher in patients receiving pancreatic enzyme supplementation therapy compared to those who did not (100% vs. 58%, p = 0.069), although the small sample size warrants cautious interpretation. The identification of predictive factors for MASLD recovery, such as small diameter main pancreatic duct and low serum amylase levels at postoperative day 28, provides valuable insights for tailoring postoperative management strategies. While these findings offer promising directions for clinical practice, further prospective studies with larger cohorts are necessary to validate these results and establish definitive guidelines for the prevention and management of MASLD in post-pancreatoduodenectomy patients[77].
In an examination of postoperative hepatic steatosis following total pancreatectomy, recent findings have shed light on the complex interplay of factors contributing to this condition. The study revealed that a significant proportion (37.2%) of patients developed hepatic steatosis post-surgery, accompanied by notable declines in nutritional status and body mass index. Intriguingly, the research identified several key risk factors beyond the previously established association with remnant pancreatic function. Female sex emerged as a significant predictor, suggesting potential hormonal or metabolic influences that warrant further investigation. Additionally, early postoperative serum albumin levels were found to be correlated with the development of hepatic steatosis, underscoring the critical role of nutritional status in post-surgical liver health. Perhaps most notably, the study highlighted the potential preventive effects of high-dose pancreatic enzyme replacement therapy on postoperative hepatic steatosis. This finding not only emphasizes the importance of managing pancreatic exocrine insufficiency but also opens up new avenues for targeted interventions to mitigate the risk of hepatic steatosis in pancreatomized patients. While these results provide valuable insights, it is important to note that the study’s relatively small sample size and focus on total pancreatectomy patients may limit its generalizability to other pancreatic surgeries. Future research should aim to validate these findings in larger, more diverse cohorts and explore the long-term implications of these risk factors and potential preventive strategies[78].
Collectively, these findings illustrate that MASLD is a prevalent and impactful complication following PD and TP, with a multifactorial etiology linked to PEI, patient demographics, and treatment factors. Improved predictive strategies, enzyme replacement therapy, and tailored postoperative care emerge as pivotal in managing MASLD, helping mitigate its impact on liver function and patient recovery trajectory.
Conclusion
In conclusion, this review underscores the significant interplay between MASLD and PD, highlighting a relationship that impacts postoperative outcomes. The prevalence of MASLD in patients undergoing PD presents unique challenges, influencing surgical decision-making and necessitating tailored perioperative management strategies. Moreover, the emergence of MASLD following PD introduces long-term metabolic and hepatic consequences that warrant close monitoring and proactive intervention.
Conflict of Interest
The author declare that they have no conflict of interest.
Funding
None.
Acknowledgments
Special thanks to Dr. Seyed-Mohamad-Sadegh Mirahmadi and Dr. Reza Azarbad.
Authors’ Contributions
MS: Reviewing the literature, Methodology, Investigation, Conceptualization, Data curation, Formal analysis, Writing – the original draft, review & and editing, Designing the Figures.
References
- Younossi ZM, Kalligeros M, Henry L. Epidemiology of Metabolic Dysfunction Associated Steatotic Liver Disease. Clinical and Molecular Hepatology. 2024. [CrossRef]
- Miao L, Targher G, Byrne CD, Cao Y-Y, Zheng M-H. Current status and future trends of the global burden of MASLD. Trends in Endocrinology & Metabolism. 2024. [CrossRef]
- Mokhtare M, Abdi A, Sadeghian AM, Sotoudeheian M, Namazi A, Sikaroudi MK. Investigation about the correlation between the severity of metabolic-associated fatty liver disease and adherence to the Mediterranean diet. Clinical Nutrition ESPEN. 2023;58:221-7. [CrossRef]
- van Erpecum KJ, Dalekos GN. New horizons in the diagnosis and management of patients with MASLD. European Journal of Internal Medicine. 2024;122:1-2.
- Lionis C, Papadakis S, Anastasaki M, Aligizakis E, Anastasiou F, Francque S, et al. Practice Recommendations for the Management of MASLD in Primary Care: Consensus Results. Diseases. 2024;12:180. [CrossRef]
- Hüttner FJ, Fitzmaurice C, Schwarzer G, Seiler CM, Antes G, Büchler MW, et al. Pylorus-preserving pancreaticoduodenectomy (pp Whipple) versus pancreaticoduodenectomy (classic Whipple) for surgical treatment of periampullary and pancreatic carcinoma. Cochrane database of systematic reviews. 2016.
- Han MAT, Yu Q, Tafesh Z, Pyrsopoulos N. Diversity in NAFLD: a review of manifestations of nonalcoholic fatty liver disease in different ethnicities globally. Journal of Clinical and Translational Hepatology. 2020;9:71. [CrossRef]
- Yip TCF, Vilar-Gomez E, Petta S, Yilmaz Y, Wong GLH, Adams LA, et al. Geographical similarity and differences in the burden and genetic predisposition of NAFLD. Hepatology. 2023;77:1404-27. [CrossRef]
- Habib S. Team players in the pathogenesis of metabolic dysfunctions-associated steatotic liver disease: The basis of development of pharmacotherapy. World Journal of Gastrointestinal Pathophysiology. 2024;15.
- Ha S, Wong VW-S, Zhang X, Yu J. Interplay between gut microbiome, host genetic and epigenetic modifications in MASLD and MASLD-related hepatocellular carcinoma. Gut. 2024. [CrossRef]
- Sun B, Zhuang L. PNPLA3 is one of the bridges between TM6SF2 E167K variant and MASLD. Clinical and Molecular Hepatology. 2024. [CrossRef]
- Seko Y, Yamaguchi K, Shima T, Iwaki M, Takahashi H, Kawanaka M, et al. Clinical Utility of Genetic Variants in PNPLA3 and TM6SF2 to Predict Liver-Related Events in Metabolic Dysfunction-Associated Steatotic Liver Disease. Liver International. 2024.
- Longo M, Meroni M, Paolini E, Erconi V, Carli F, Fortunato F, et al. TM6SF2/PNPLA3/MBOAT7 loss-of-function genetic variants impact on NAFLD development and progression both in patients and in in vitro models. Cellular and Molecular Gastroenterology and Hepatology. 2022;13:759-88.
- Wang Z, Xu M, Hu Z, Shrestha UK. Prevalence of nonalcoholic fatty liver disease and its metabolic risk factors in women of different ages and body mass index. Menopause. 2015;22:667-73.
- Mitra S, De A, Chowdhury A. Epidemiology of non-alcoholic and alcoholic fatty liver diseases. Translational gastroenterology and hepatology. 2020;5.
- Gan L, Chitturi S, Farrell GC. Mechanisms and implications of age-related changes in the liver: nonalcoholic fatty liver disease in the elderly. Current gerontology and geriatrics research. 2011;2011:831536.
- Arun J, Clements RH, Lazenby AJ, Leeth RR, Abrams GA. The prevalence of nonalcoholic steatohepatitis is greater in morbidly obese men compared to women. Obesity surgery. 2006;16:1351-8.
- Polyzos SA, Goulis DG. Menopause and metabolic dysfunction-associated steatotic liver disease. Maturitas. 2024:108024.
- Lekakis V, Papatheodoridis GV. Natural history of metabolic dysfunction-associated steatotic liver disease. European Journal of Internal Medicine. 2024;122:3-10.
- Israelsen M, Francque S, Tsochatzis EA, Krag A. Steatotic liver disease. The Lancet. 2024;404:1761-78.
- Tacke F, Horn P, Wong VW-S, Ratziu V, Bugianesi E, Francque S, et al. EASL–EASD–EASO Clinical Practice Guidelines on the management of metabolic dysfunction-associated steatotic liver disease (MASLD). Journal of Hepatology. 2024.
- Geng Y, Faber KN, de Meijer VE, Blokzijl H, Moshage H. How does hepatic lipid accumulation lead to lipotoxicity in non-alcoholic fatty liver disease? Hepatology international. 2021;15:21-35.
- Liu Q, Bengmark S, Qu S. The role of hepatic fat accumulation in pathogenesis of non-alcoholic fatty liver disease (NAFLD). Lipids in health and disease. 2010;9:1-9.
- Fujii H, Kawada N. Inflammation and fibrogenesis in steatohepatitis. Journal of gastroenterology. 2012;47:215-25.
- Mouleeswaran K, Varghese J, Reddy MS. Atlas of Basic Liver Histology for Practicing Clinicians and Pathologists: Springer; 2023.
- Leow W-Q, Chan AW-H, Mendoza PGL, Lo R, Yap K, Kim H. Non-alcoholic fatty liver disease: the pathologist’s perspective. Clinical and Molecular Hepatology. 2023;29:S302. [CrossRef]
- Akkız H, Gieseler RK, Canbay A. Liver fibrosis: From basic science towards clinical progress, focusing on the central role of hepatic stellate cells. International Journal of Molecular Sciences. 2024;25:7873.
- Ahmad W, Ijaz B, Javed FT, Gull S, Kausar H, Sarwar MT, et al. A comparison of four fibrosis indexes in chronic HCV: development of new fibrosis-cirrhosis index (FCI). BMC gastroenterology. 2011;11:1-10.
- Pinzani M, Rosselli M, Zuckermann M. Liver cirrhosis. Best practice & research Clinical gastroenterology. 2011;25:281-90.
- Garrido A, Djouder N. Cirrhosis: a questioned risk factor for hepatocellular carcinoma. Trends in cancer. 2021;7:29-36. [CrossRef]
- Eslam M, El-Serag HB, Francque S, Sarin SK, Wei L, Bugianesi E, et al. Metabolic (dysfunction)-associated fatty liver disease in individuals of normal weight. Nature reviews Gastroenterology & hepatology. 2022;19:638-51.
- Verma MK, Tripathi M, Singh BK. Dietary Determinants of Metabolic Syndrome: Focus on the Obesity and Metabolic Dysfunction-Associated Steatotic Liver Disease (MASLD). 2024.
- Liu S, Wang J, Wu S, Niu J, Zheng R, Bie L, et al. The progression and regression of metabolic dysfunction-associated fatty liver disease are associated with the development of subclinical atherosclerosis: a prospective analysis. Metabolism. 2021;120:154779.
- Chai X-N, Zhou B-Q, Ning N, Pan T, Xu F, He S-H, et al. Effects of lifestyle intervention on adults with metabolic associated fatty liver disease: A systematic review and meta-analysis. Frontiers in Endocrinology. 2023;14:1081096.
- Tan Z, Sun H, Xue T, Gan C, Liu H, Xie Y, et al. Liver fibrosis: therapeutic targets and advances in drug therapy. Frontiers in cell and developmental biology. 2021;9:730176.
- Drebin JA, Strasberg SM. Techniques for biliary and pancreatic reconstruction after pancreaticoduodenectomy. Pancreatic Cancer: Springer; 2002. p. 171-80.
- Wang M, Cai H, Meng L, Cai Y, Wang X, Li Y, et al. Minimally invasive pancreaticoduodenectomy: a comprehensive review. International Journal of Surgery. 2016;35:139-46.
- Dai R, Turley RS, Blazer DG. Contemporary review of minimally invasive pancreaticoduodenectomy. World journal of gastrointestinal surgery. 2016;8:784.
- Tang G, Zhang L, Xia L, Zhang J, Chen R, Zhou R. Comparison of short-term outcomes of robotic versus open Pancreaticoduodenectomy: A Meta-Analysis of randomized controlled trials and Propensity-Score-Matched studies. International Journal of Surgery. 2024:10.1097.
- Shamali A, McCrudden R, Bhandari P, Shek F, Barnett E, Bateman A, et al. Pancreaticoduodenectomy for nonampullary duodenal lesions: indications and results. European Journal of Gastroenterology & Hepatology. 2016;28:1388-93.
- Jabłońska B, Szmigiel P, Mrowiec S. Pancreatic intraductal papillary mucinous neoplasms: Current diagnosis and management. World Journal of Gastrointestinal Oncology. 2021;13:1880.
- Salvia R, Burelli A, Perri G, Marchegiani G. State-of-the-art surgical treatment of IPMNs. Langenbeck's Archives of Surgery. 2021:1-10.
- Chen R, Xiao C, Song S, Zhu L, Zhang T, Liu R. The optimal choice for patients underwent minimally invasive pancreaticoduodenectomy: a systematic review and meta-analysis including patient subgroups. Surgical Endoscopy. 2024:1-17.
- Sharifi A, Bakhtiari Z. Complications (Pain intensity, Opioid usage, Bleeding, morbidity and mortality) following pancreaticoduodenectomy. Eurasian Journal of Chemical, Medicinal and Petroleum Research. 2023;2:266-74.
- Vallance AE, Young AL, Macutkiewicz C, Roberts KJ, Smith AM. Calculating the risk of a pancreatic fistula after a pancreaticoduodenectomy: a systematic review. Hpb. 2015;17:1040-8.
- Ke Z-x, Xiong J-x, Hu J, Chen H-y, Li Q, Li Y-q. Risk factors and management of postoperative pancreatic fistula following pancreaticoduodenectomy: single-center experience. Current medical science. 2019;39:1009-18.
- Guo C, Xie B, Guo D. Does pancreatic duct stent placement lead to decreased postoperative pancreatic fistula rates after pancreaticoduodenectomy? A meta-analysis. International Journal of Surgery. 2022;103:106707. [CrossRef]
- Marchegiani G, Di Gioia A, Giuliani T, Lovo M, Vico E, Cereda M, et al. Delayed gastric emptying after pancreatoduodenectomy: One complication, two different entities. Surgery. 2023;173:1240-7. [CrossRef]
- Simon R. Complications after pancreaticoduodenectomy. Surgical Clinics. 2021;101:865-74.
- Eguia E, Aranha GV, Abood G, Godellas C, Kuo PC, Baker MS. Do high-volume centers mitigate complication risk and reduce costs associated with performing pancreaticoduodenectomy in ethnic minorities? The American Journal of Surgery. 2021;222:153-8.
- Panni RZ, Panni UY, Liu J, Williams GA, Fields RC, Sanford DE, et al. Re-defining a high volume center for pancreaticoduodenectomy. Hpb. 2021;23:733-8.
- Abdelrahim M, Esmail A, Xu J, Katz TA, Sharma S, Kalashnikova E, et al. Early relapse detection and monitoring disease status in patients with early-stage pancreatic adenocarcinoma using circulating tumor DNA. Journal of Surgery and Research. 2021;4:602-15. [CrossRef]
- Groot VP, Mosier S, Javed AA, Teinor JA, Gemenetzis G, Ding D, et al. Circulating tumor DNA as a clinical test in resected pancreatic cancer. Clinical Cancer Research. 2019;25:4973-84.
- Hata T, Mizuma M, Motoi F, Ohtsuka H, Nakagawa K, Morikawa T, et al. Prognostic impact of postoperative circulating tumor DNA as a molecular minimal residual disease marker in patients with pancreatic cancer undergoing surgical resection. Journal of Hepato-Biliary-Pancreatic Sciences. 2023;30:815-24.
- Yamaguchi T, Uemura K, Murakami Y, Kondo N, Nakagawa N, Okada K, et al. Clinical implications of pre-and postoperative circulating tumor DNA in patients with resected pancreatic ductal adenocarcinoma. Annals of Surgical Oncology. 2021;28:3135-44. [CrossRef]
- Vigia E, Ramalhete L, Filipe E, Bicho L, Nobre A, Mira P, et al. Machine learning-based model helps to decide which patients may benefit from pancreatoduodenectomy. Onco. 2023;3:175-88.
- Schlanger D, Graur F, Popa C, Moiș E, Al Hajjar N. The role of artificial intelligence in pancreatic surgery: A systematic review. Updates in Surgery. 2022;74:417-29.
- Shen Z, Chen H, Wang W, Xu W, Zhou Y, Weng Y, et al. Machine learning algorithms as early diagnostic tools for pancreatic fistula following pancreaticoduodenectomy and guide drain removal: A retrospective cohort study. International Journal of Surgery. 2022;102:106638.
- Verma A, Balian J, Hadaya J, Premji A, Shimizu T, Donahue T, et al. Machine Learning–based Prediction of Postoperative Pancreatic Fistula Following Pancreaticoduodenectomy. Annals of Surgery. 2024;280:325-31.
- Ashraf Ganjouei A, Romero-Hernandez F, Wang JJ, Casey M, Frye W, Hoffman D, et al. A machine learning approach to predict postoperative pancreatic fistula after pancreaticoduodenectomy using only preoperatively known data. Annals of surgical oncology. 2023;30:7738-47.
- Capretti G, Bonifacio C, De Palma C, Nebbia M, Giannitto C, Cancian P, et al. A machine learning risk model based on preoperative computed tomography scan to predict postoperative outcomes after pancreatoduodenectomy. Updates in Surgery. 2022:1-9.
- Kang CM, Lee JH. Pathophysiology after pancreaticoduodenectomy. World Journal of Gastroenterology: WJG. 2015;21:5794.
- Mori T, Ozawa E, Sasaki R, Shimakura A, Takahashi K, Kido Y, et al. Are transmembrane 6 superfamily member 2 gene polymorphisms associated with steatohepatitis after pancreaticoduodenectomy? JGH Open. 2024;8:e13113.
- Tanaka N, Horiuchi A, Yokoyama T, Kaneko G, Horigome N, Yamaura T, et al. Clinical characteristics of de novo nonalcoholic fatty liver disease following pancreaticoduodenectomy. Journal of gastroenterology. 2011;46:758-68.
- Kato H, Kamei K, Suto H, Misawa T, Unno M, Nitta H, et al. Incidence and risk factors of nonalcoholic fatty liver disease after total pancreatectomy: a first multicenter prospective study in Japan. Journal of Hepato-Biliary-Pancreatic Sciences. 2022;29:428-38.
- Nakagawa N, Murakami Y, Uemura K, Sudo T, Hashimoto Y, Kondo N, et al. Nonalcoholic fatty liver disease after pancreatoduodenectomy is closely associated with postoperative pancreatic exocrine insufficiency. Journal of Surgical Oncology. 2014;110:720-6.
- Kato H, Isaji S, Azumi Y, Kishiwada M, Hamada T, Mizuno S, et al. Development of nonalcoholic fatty liver disease (NAFLD) and nonalcoholic steatohepatitis (NASH) after pancreaticoduodenectomy: proposal of a postoperative NAFLD scoring system. Journal of hepato-biliary-pancreatic sciences. 2010;17:296-304.
- Huang K, Ma T, Qian T, Bai X, Liang T. Clinical significance and risk factors of nonalcoholic fatty liver diseases after pancreaticoduodenectomy: a Retrospective Cohort Study. HPB. 2024;26:S361-S2.
- Fujii T, Iizawa Y, Kobayashi T, Hayasaki A, Ito T, Murata Y, et al. Radiomics-based prediction of nonalcoholic fatty liver disease following pancreatoduodenectomy. Surgery Today. 2024:1-11.
- D’Cruz V, De Zutter A, Van den Broecke M, Ribeiro S, de Carvalho LA, Smeets P, et al. Prevalence of metabolic dysfunction-associated fatty liver disease after pancreatic surgery in a historical Belgian cohort and review of the literature. Acta Gastro-Enterologica Belgica. 2024;87.
- Shibata S, Takahashi Y, Oyama H, Minegishi Y, Tanaka K. Incidence and clinical characteristics of hepatic steatosis following pancreatectomy. The Showa University Journal of Medical Sciences. 2024;36:25-35.
- Izumi H, Yoshii H, Fujino R, Takeo S, Nomura E, Mukai M, et al. Factors contributing to nonalcoholic fatty liver disease (NAFLD) and fat deposition after pancreaticoduodenectomy: A retrospective analysis. Annals of Gastroenterological Surgery. 2023;7:793-9.
- Fujii Y, Nanashima A, Hiyoshi M, Imamura N, Yano K, Hamada T. Risk factors for development of nonalcoholic fatty liver disease after pancreatoduodenectomy. Annals of Gastroenterological Surgery. 2017;1:226-31.
- Yoo D-G, Jung B-H, Hwang S, Kim S-C, Kim K-H, Lee Y-J, et al. Prevalence analysis of de novo hepatic steatosis following pylorus-preserving pancreaticoduodenectomy. Digestive surgery. 2015;31:359-65. [CrossRef]
- Yu H-H, Shan Y-S, Lin P-W. Effect of pancreaticoduodenectomy on the course of hepatic steatosis. World journal of surgery. 2010;34:2122-7.
- Ito Y, Kenmochi T, Shibutani S, Egawa T, Hayashi S, Nagashima A, et al. Evaluation of predictive factors in patients with nonalcoholic fatty liver disease after pancreaticoduodenectomy. The American Surgeon. 2014;80:500-4.
- Sato T, Matsuo Y, Shiga K, Morimoto M, Miyai H, Takeyama H. Factors that predict the occurrence of and recovery from non-alcoholic fatty liver disease after pancreatoduodenectomy. Surgery. 2016;160:318-30.
- Hata T, Ishida M, Motoi F, Sakata N, Yoshimatsu G, Naitoh T, et al. Clinical characteristics and risk factors for the development of postoperative hepatic steatosis after total pancreatectomy. Pancreas. 2016;45:362-9. [CrossRef]
Figure 1.
Factors which plays crucial role in MASLD susceptibility.
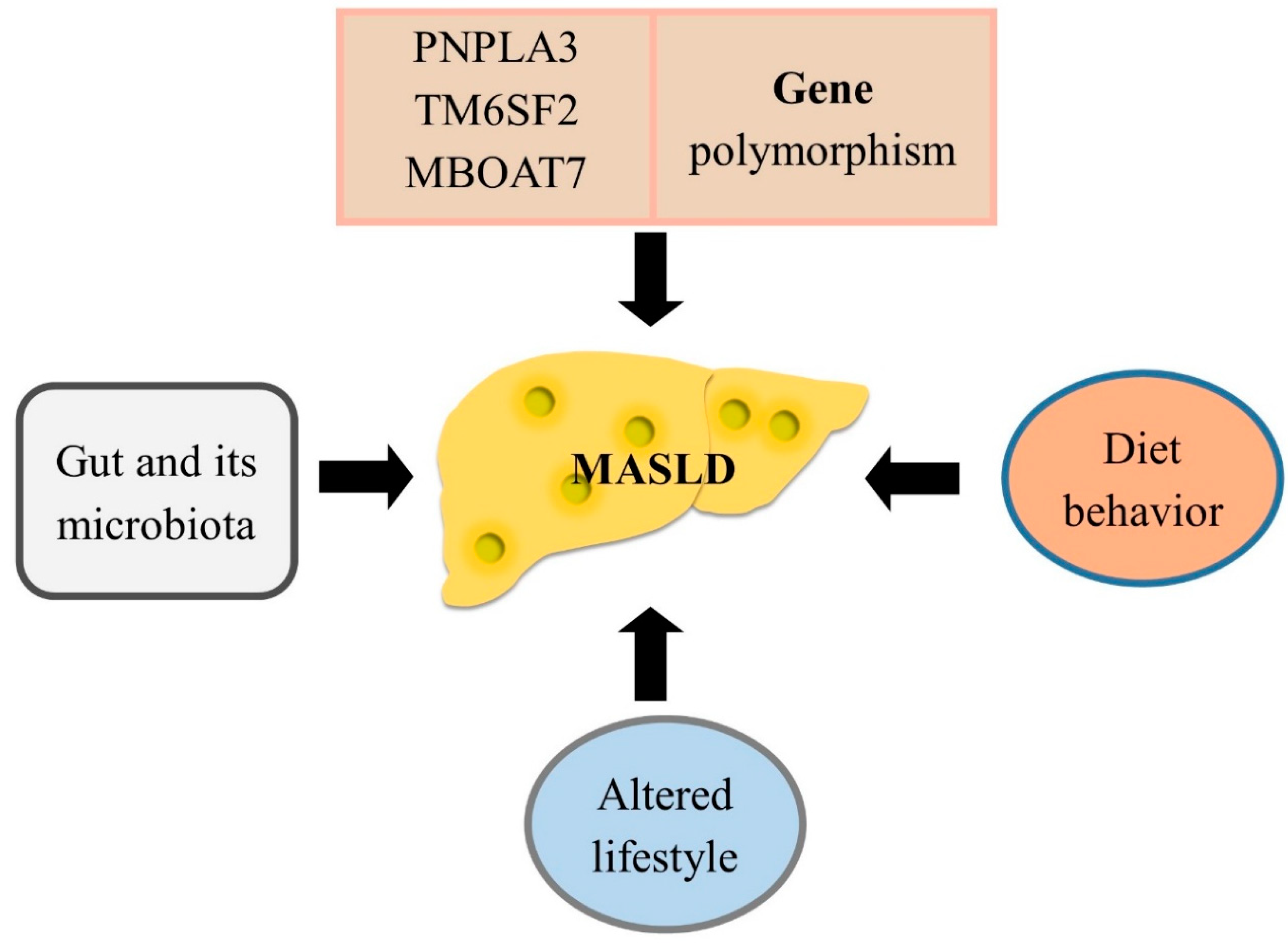
Figure 2.
The pancreaticoduodenectomy surgery procedure.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



