Submitted:
02 November 2024
Posted:
05 November 2024
You are already at the latest version
Abstract
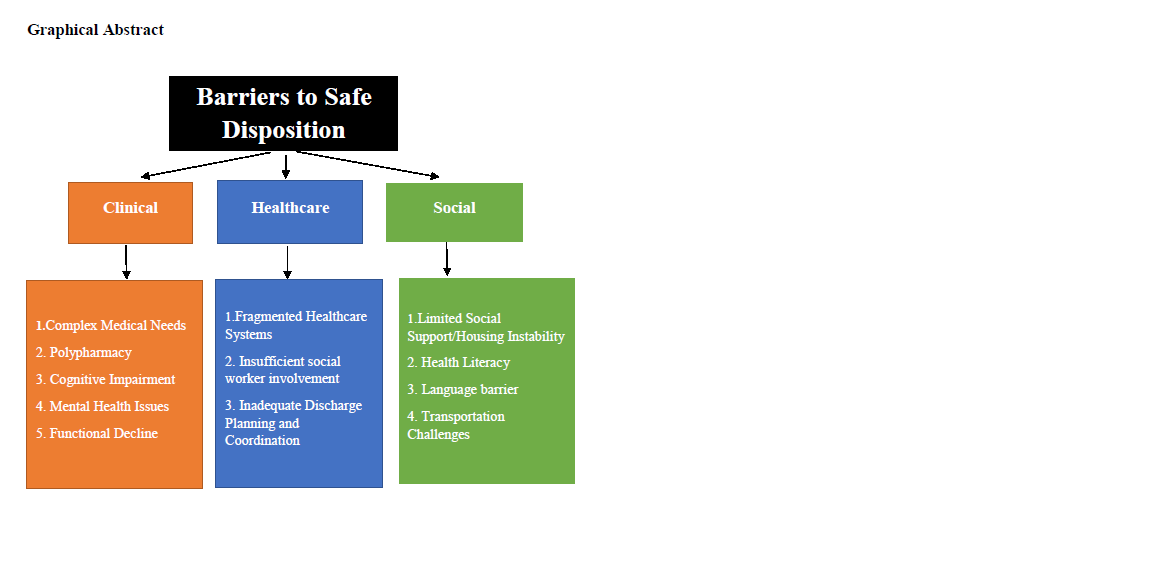
The safe transition of older adults from hospital to home or other care settings is a critical aspect of healthcare that significantly impacts patient outcomes. Barriers to safe social disposition may include clinical, healthcare system, or social factors. Despite advances in medical care, many older adults face these barriers during the transition process, which can lead to adverse health events, re-admission, and decreased quality of life. This review explores the obstacles to safe disposition for older adults post-hospitalization and discusses potential strategies to mitigate these issues.
Keywords:
Older adults
; Barriers
; Safe disposition
; Hospitalization
Introduction
The aging population is proliferating, leading to an increased number of elderly patients requiring hospitalization. According to the World Health Organization (WHO) 2024 world report on aging and health, individuals aged 65 and older will outnumber youth and are projected to reach 2.1 billion by 2050 compared to 1 billion in 2020 [1]. Many factors are playing a role in older adults’ health, ranging from physical and social environments – including their homes and communities- to personal characteristics – including gender, race, socioeconomic status, and genetic factors. Physical and social environments can affect health directly or through barriers or incentives that impact opportunities, decisions, and health behavior. Older patients suffer from more morbidities than younger patients, leading to prolonged hospitalization and increased healthcare needs [2]. Safe disposition—transitioning patients from hospital care to their homes or other care environments—is vital for ensuring continuity of care and optimizing health outcomes. A safe disposition process may prevent errors during care transitions that are often preventable, leading to a reduced risk of re-admissions and adverse drug events after discharge [3,4]. However, numerous barriers can impede this process, necessitating a comprehensive understanding of older adults' challenges in the post-hospitalization phase. Efficient discharge planning is an essential component of high-quality inpatient care, especially in older adults with multimorbidity and complex medical needs [5]. Efficient discharge planning aims to improve a patient's quality of life by ensuring continuity of care and reducing the rate of readmissions and/or complications, which may decrease the healthcare system's financial burden [6,7]. This review highlights the multifaceted barriers to safe disposition in older adults’ post-hospitalization and emphasizes the importance of coordinated efforts to improve care transitions.
Clinical Barriers
- Complex Medical Needs: Multimorbidity (the coexistence of multiple chronic diseases) exists in 35% to 80% of older adults [8]. Multimorbidity causes disability, poor quality of life, and high health care utilization and costs, thereby complicating the discharge process [9]. In addition, very old patients present with dementia, limiting their ability to understand discharge instructions, which leads to a major challenge for the services provided [10].
- Polypharmacy and Medication Reconciliation: Polypharmacy is defined as using more medications than are medically necessary and may include medicines that are not indicated, are ineffective, or constitute a therapeutic duplication. There is no standard cut point about the number of medications, but in most studies, five or more drugs are defined as polypharmacy [11,12]. Polypharmacy is common among older adults due to multimorbidity. Hajjar E et al., in their study of 384 elderly hospitalized patients, found that 58.6% of patients took one or more unnecessary prescribed drugs [13]. Polypharmacy leads to adverse drug events, increased healthcare costs, medication non-adherence, functional decline, and increased risk of cognitive impairment and falls [14]. Inadequate medication reconciliation during discharge can result in medication errors, non-adherence, and subsequent health complications [15].
- Cognitive Impairment: Decline in mental performance is typical in older adults, and older patients hospitalized with stroke, heart failure, or lung disease have an increased risk for cognitive decline. The cognitive decline can lead to confusion and non-compliance with treatment recommendations. The mental deterioration may also be caused by delirium in hospitalized elderly patients [16]. Delirium is a potent risk factor for hospital-related complications, including more extended hospitalizations, unplanned ICU admission, discharge to a nursing facility, and all-cause mortality [17].
- Mental Health Issues: About 15% of the population above 60 years suffer from mental disorders that may be depression, anxiety, loneliness, or substance abuse, with depression being the most prevalent [18,19]. Suicide rates in older adults are as high or higher than in young individuals, the major contributory factors being physical illness, functional impairment, and stressful life events [20]. A study by Lin P et al. found that the incidence of mental problems in older hospitalized patients was 78%, and 53.8% of older patients with chronic diseases take negative coping styles that can aggravate the negative impact of the disease [21].
- Functional decline: Functional decline (FD), defined as a loss of independence in one or more basic activities of daily living (ADL), is a severe problem among hospitalized older adults. About 20%-30% of older adults experience a functional decline at hospital discharge, leading to increased dependency on ADLs, inpatient length of stay, hospital readmission rate, and mortality; the oldest old revealed the highest functional decline [22,23]. A meta-analysis by Geyskens L et al. identified living in a nursing home, instrumental activities of daily living (IADL) impairment, history of falls, cognitive impairment, dementia, delirium, malnutrition, hypoalbuminemia, comorbidity, and the presence of pressure ulcers as significant risk factors for functional decline [24].
Healthcare System Barriers
- Fragmented Healthcare Systems: Lack of proper communication with patients and caregivers, improper coordination among healthcare providers, and resources not being distributed according to patients' actual needs can result in disjointed care and unsafe transitions, leading to decreased patient satisfaction, longer lengths of stay, increased healthcare costs, and increased mortality [25,26,27].
- Insufficient social worker involvement: Social workers play a crucial role in the discharge process of older patients by evaluating their social, emotional, and economic needs, collaborating with healthcare teams to develop discharge plans, connecting patients and caregivers with community resources, and advocating for the rights and needs of older patients, by providing education to patients and families about the discharge process and arranging follow up visits to monitor the patient’s well-being [28]. Barriers to hospital discharge can arise from insufficient involvement of social workers.
- Inadequate Discharge Planning and Coordination: Comprehensive discharge planning is an essential feature of healthcare systems. The aim is to improve the coordination of services from the hospital to the community to ensure seamless discharge for the patient, resulting in a decreased length of stay in the hospital and a reduced rate of re-admissions [29]. Older adults have more complex needs, may have multiple comorbidities, and often take longer to recover following an illness, requiring more focused discharge planning to get them home or to a long-term care facility [30]. Discharge summaries are frequently delayed, of deficient quality regarding follow-up plans, and with improper medication reconciliation, which leads to confusion among patients and caregivers and may result in decreased compliance with the treatment and increased readmission rates [15,31].
Social Barriers
- Limited Social Support/Housing Instability: Older adults turn to their families for help, neighbors, and finally to formal sources of social support such as social workers. Family can support older patients by providing care to the patient and working together with the health care team, thereby ensuring safe discharge [32]. Many elderly patients lack robust social networks or family support systems, crucial for ensuring safety and adherence to post-discharge plans. Isolation can hinder recovery and increase the risk of readmission. Unsafe living conditions, homelessness, overburdened caregivers, financial strain on caregivers, and geographic distance from the patient are some of the factors that can lead to prolonged hospitalization, increased healthcare utilization, and unsafe discharge. [33].
- Health Literacy: Inadequate health literacy is recognized as a stronger predictor of poor health than age, income, employment status, education level, or race and is an independent factor for 30-day hospital reutilization after discharge [34,35]. Patients with low health literacy may not follow the medical instructions provided to them at their hospital discharge, and the consequent inability to attend follow-up visits and delays in seeking medical attention may lead to increased all-cause mortality [36,37]. Older patients have a significantly higher rate of inadequate health literacy than younger patients, which may be attributed to the decline in comprehension, memory, and word recognition abilities [38,39]. A study by Shahid R et al. showed that in patients over 65 years of age, 45.6% had inadequate health literacy, and 22.8% had marginal health literacy [38].
- Language barrier: Due to poor communication, patients with limited English proficiency have a poor understanding of follow-up visits and medications post-discharge. This leads to longer hospital stays and higher readmission rates [40,41]. The combination of low educational/health literacy with a language barrier places many patients in ‘double jeopardy’ of not understanding critical information and increasing risks at discharge [41].
- Transportation Challenges: Access to reliable transportation is often a significant barrier for older adults seeking follow-up care or rehabilitation services. Limited mobility can prevent them from attending appointments and adhering to treatment plans. Annually, transportation barriers prevent 3.6 million people in the United States from obtaining medical care [42]. Transportation is the third most cited barrier to accessing health services for older adults [43]. Studies have shown that individuals who are older, less educated, female, minority, or low-income, or have a combination of these characteristics are affected more by transportation barriers [44]. Transportation challenges may include limited availability and routes, overcrowding on trains and buses, safety issues, high fares cost, lack of a personal vehicle, long travel distances, lengthy waiting times, and inconvenient time schedules [43,44].
Strategies to Mitigate Barriers
- Enhanced Discharge Planning/Interprofessional Team Collaboration: The goal of efficient discharge planning is to improve a patient's quality of life by ensuring continuity of care and reducing the rate of unplanned readmissions and/or complications, which may decrease the healthcare system's financial burden [7]. Effective collaboration is the key to successful discharge planning. Initiating discharge planning upon admission involving a multidisciplinary team, patients, and families can ensure that all aspects of a patient’s care are addressed. This is particularly important for older adults with a more complex discharge plan and requires more assistance in executing the necessary elements [45]. Comprehensive geriatric assessment by thorough evaluation of the patient’s medical, cognitive, social, and functional needs and implementing standardized discharge planning protocols can improve transition safety [46].
- Medication Reconciliation Efforts: Medication reconciliation is a formalized process that considers all the drugs taken and to be taken by the patient when drafting a new prescription. Establishing robust medication reconciliation processes during discharge can ensure that patients and caregivers understand the medication regimen [47]. Integrating skilled pharmacists into allied healthcare teams can identify and address medication-related problems [48]. The objective is to prevent medication errors by promoting the transmission of complete and accurate patient medication information among healthcare professionals at each transition point in the care pathway.
- Patient and Caregiver Communication and Education: Proper communication about the disease process and discharge planning and providing education and resources for family caregivers can empower them to support older adults’ post-hospitalization, ensuring better adherence to care plans and improving outcomes. In addition, family members taking on caring roles should be given information about support systems that can support them emotionally and practically. The different aspects of being a carer should be discussed in family meetings to gauge the family’s understanding and preparedness for the role of caregiving [49,50].
- Patient-centered Care: Discharge safety is an evaluative concept, and therefore, one should consider a patient’s values about well-being, risk, and a meaningful life. Our findings support that increasing patients' medication understanding in their preferred language is an essential component of interventions to prevent medication errors and reduce re-hospitalizations [41].
- Community Support Programs: Developing community resources and support networks can help address social barriers. Community support programs should be able to cover the following services: 1. Interventions to optimize functional capacity and independence. 2. Slow-stream rehabilitation. 3. Case managers for caregiver support and home health services. 4. Addressing transportation, housing, and food security issues [51].
- Telehealth and Remote Monitoring: Utilizing telehealth services is a cost-effective way to facilitate follow-up care, making it easier for elderly patients to connect with healthcare providers without needing transportation. Telehealth significantly improves health outcomes in terms of readmission rates, mortality rates, and quality of life in older adults at high risk of readmission [52].
Conclusion
The safe disposition of older adults’ post-hospitalization is fraught with barriers that can significantly impact health outcomes. By recognizing the clinical, healthcare system, and social challenges that older adults face, healthcare providers can implement targeted strategies to enhance the transition process. Addressing these barriers improves patient safety, reduces readmission rates, and contributes to a higher quality of life for elderly patients. Continued research and policy efforts are essential to develop effective interventions that support safe transitions in this vulnerable population.
Funding
No funding was received.
Acknowledgments
None.
Conflicts of Interest
None.
References
- World Health Organization. World report on aging and health. 2024.
- O'Connell Francischetto E, Damery S, Davies S, Combes G. Discharge interventions for older patients leaving hospital: protocol for a systematic meta-review. Syst Rev. 2016, 5, 46. [Google Scholar] [CrossRef] [PubMed]
- Greenwald JL, Denham CR, Jack BW. The hospital discharge: a review of a high-risk care transition with highlights of a reengineered discharge process. J Patient Saf. 2007, 97-106.
- Agency for Healthcare Research and Quality. Readmissions and Adverse Events After Discharge. https://psnet.ahrq.gov/primer/readmissions-and-adverse-events-after-discharge.
- Yam C, Wong E, Cheung A, et al. Framework and components for effective discharge planning system: a Delphi methodology. BMC Health Serv Res 2012, 12, 396.
- Hunter T, Nelson JR, Birmingham J. Preventing readmissions through comprehensive discharge planning. Prof Case Manag. 2013, 18, 56–63. [Google Scholar] [CrossRef] [PubMed]
- Gonçalves-Bradley DC, Lannin NA, Clemson LM, Cameron ID, Shepperd S. Discharge planning from hospital. Cochrane Database Syst Rev. 2016, 2016, CD000313. [Google Scholar]
- Smith, S. , O'Dowd T. : Chronic diseases: what happens when they come in multiples?. Br J Gen Pract 2007, 57, 268–270. [Google Scholar]
- Marengoni A, von Strass E, Rizzato D, Winblad B, Fratiglioni L. The impact of chronic multimorbidity and disability on functional decline and survival in elderly persons A community-based, longitudinal study. J. Intern. Med. 2009, 265, 288–295. [Google Scholar] [CrossRef]
- Boyd, C.M. , Darer J., Boult C., Fried L.P., Boult L., Wu A.W.: Clinical practice guidelines and quality of care for older patients with multiple comorbid diseases: implications for performance pay. JAMA 2005, 294, 716–724. [Google Scholar] [CrossRef]
- Tjia J, Velten SJ, Parsons C, et al. Studies to reduce unnecessary medication use in frail older adults: a systematic review. Drugs Aging. 2013, 30, 285–307. [Google Scholar] [CrossRef]
- Schäfer L, Paulitsch M, Hanf M, Dinh TS, Klein A-A, Klasing S, Seidling H, Voigt K, van den Akker M. Polypharmacy in Older Patients with Multimorbidity: The Agreement Between Patient and General Practitioner-Reported Drugs Observed in a Pilot cRCT. International Journal of Environmental Research and Public Health. 2024, 21, 1389. [Google Scholar] [CrossRef]
- Hajjar E, Hanlon JT, Sloane RJ, et al. Unnecessary drug use in frail older people at hospital discharge. J Am Geriatr Soc. 2005, 53, 1518–1523. [Google Scholar] [CrossRef] [PubMed]
- Maher RL, Hanlon J, Hajjar ER. Clinical consequences of polypharmacy in the elderly. Expert Opin Drug Saf. 2014, 13, 57–65. [Google Scholar] [CrossRef] [PubMed]
- Michaelsen MH, McCague P, Bradley CP, Sahm LJ. Medication Reconciliation at Discharge from Hospital: A Systematic Review of the Quantitative Literature. Pharmacy (Basel). 2015, 3, 53–71. [Google Scholar]
- Chodosh J, et al. Cognitive decline in high-functioning older persons is associated with an increased risk of hospitalization. J Am Geriatr Soc. 2004, 52, 1456–1462. [Google Scholar] [CrossRef] [PubMed]
- Inouye SK, Westendorp RG, Saczynski JS. Delirium in elderly people. Lancet. 2014, 383, 911–922. [Google Scholar] [CrossRef]
- World Health Organization. World report on aging and health. 2018.
- Dykstra, PA. Older adult loneliness: myths and realities. European Journal of aging. 2009, 6, 91–100. [Google Scholar] [CrossRef]
- Shah, A. The relationship between suicide rates and age: an analysis of multinational data from the World Health Organization International. Int Psychogeriatr. 2007, 19, 1141–1152. [Google Scholar] [CrossRef]
- Lin P, Su Z, Zhang JL, Zhang J, Jin R, Guo N. Investigation on the mental health of the elderly and analysis of its influencing factors. Chin J Clin Health. 2022, 25, 355–358. [Google Scholar]
- Loyd C, Markland AD, Zhang Y et al. Prevalence of hospital-associated disability in older adults: a meta-analysis. J Am Med Dir Assoc 2020, 21, 455–461.
- Covinsky KE, et al. Loss of independence in activities of daily living in older adults hospitalized with medical illnesses: increased vulnerability with age. J Am Geriatr Soc. 2003, 51, 451–458. [Google Scholar] [CrossRef] [PubMed]
- Geyskens L, Jeuris A, Deschodt M, et al. Patient-related risk factors for in-hospital functional decline in older adults: A systematic review and meta-analysis. Age and Ageing. 2022, 51, afac007. [Google Scholar] [CrossRef] [PubMed]
- Hansson A, Svensson A, Ahlström BH, Larsson LG, Forsman B, Alsén P. Flawed communications: health professionals’ collaboration experience in caring for frail elderly patients. Scand J Public Health. 2018, 46, 680–689. [Google Scholar] [CrossRef]
- Snow K, Galaviz K, Turbow S. Patient Outcomes Following Interhospital Care Fragmentation: A Systematic Review. J Gen Intern Med. 2020, 35, 1550–1558. [Google Scholar] [CrossRef]
- Cam, H, Wennlöf, B, Gillespie U. et al. The complexities of communication at hospital discharge of older patients: a qualitative study of healthcare professionals’ views. BMC Health Serv Res 2023, 23, 1211.
- Judd RG, Sheffield S. Hospital social work: contemporary roles and professional activities. Soc Work Health Care. 2010, 49, 856–871. [Google Scholar] [CrossRef]
- Chen H, Hara Y, Horita N, Saigusa Y, Kaneko T. An Early Screening Tool for Discharge Planning Shortened Length of Hospital Stay for Elderly Patients with Community-Acquired Pneumonia. Clin Interv Aging. 2021, 16, 443–450. [Google Scholar] [CrossRef]
- Courtney MD, Edwards HE, Chang AM, Parker AW, Finlayson K, Hamilton K. A randomized controlled trial to prevent hospital readmissions and loss of functional ability in high-risk older adults: a study protocol. BMC Health Serv Res. 2011, 11, 202. [Google Scholar]
- Caleres G, Bondesson Å, Midlöv P, Modig S. Elderly at risk in care transitions When discharge summaries are poorly transferred and used a descriptive study. BMC Health Serv Res. 2018, 18, 770. [Google Scholar]
- Li H, Stewart BJ, Imle MA, Archbold PG, Felver L. Families, and hospitalized elders: a typology of family care actions. Res Nurs Health. 2000, 3–16.
- Bražinová, I. , & Chytil, O.. The family as a source of social support for older adults: Implications for gerontological social work. Journal of Social Work 2024, 24, 339–356. [Google Scholar]
- American Medical Association. Health literacy: Report of the Council on Scientific Affairs. Ad Hoc Committee on Health Literacy for the Council on Scientific Affairs, American Medical Association. JAMA. 1999, 281, 552–557. [Google Scholar]
- Mitchell SE, Sadikova E, Jack BW, Paasche-Orlow MK. Health literacy and 30-day post-discharge hospital utilization. J Health Commun. 2012, 17 (Suppl 3), 325–338.
- Dewalt DA, Berkman ND, Sheridan S, Lohr KN, Pignone MP. Literacy and health outcomes: a systematic review of the literature. J Gen Intern Med. 2004, 19, 1228–1239. [Google Scholar] [CrossRef] [PubMed]
- Kripalani S, Jacobson TA, Mugalla IC, Cawthon CR, Niesner KJ, Vaccarino V. Health literacy and the quality of physician-patient communication during hospitalization. J Hosp Med. 2010, 5, 269–275. [Google Scholar] [CrossRef]
- Dani KA, Stobo DB, Capell HA, Madhok R. Audit of medical patient literacy in North Glasgow. Scott Med J. 2007, 52, 21–24. [Google Scholar] [CrossRef] [PubMed]
- Shahid, R. , Shoker M., Chu LM. et al. Impact of low health literacy on patients’ health outcomes: a multicenter cohort study. BMC Health Serv Res 2022, 22, 1148. [Google Scholar]
- Karliner LS, Kim SE, Meltzer DO, et al. Influence of language barriers on outcomes of hospital care for general medicine inpatients. J Hospital Medicine. 2010. [CrossRef]
- Karliner LS, Auerbach A, Nápoles A, Schillinger D, Nickleach D, Pérez-Stable EJ. Language barriers and understanding of hospital discharge instructions. Med Care. 2012, 50, 283–289. [Google Scholar] [CrossRef]
- American Hospital Association. Social Determinant of Health Series: Transportation and the Role of Hospitals. November 2017. http://www.hpoe.org/Reports-HPOE/2017/ sdoh-transportation-role-of-hospitals.pdf. Accessed October 10, 2018.
- Fitzpatrick AL, Powe NR, Cooper LS et al. Barriers to health care access among the elderly and who perceives them. American Journal of Public Health 2004, 94, 1788–1794. [Google Scholar] [CrossRef]
- Syed ST, Gerber BS, & Sharp LK. Traveling towards disease: Transportation barriers to health care access. Journal of Community Health 2013, 38, 976–993. [Google Scholar] [CrossRef]
- Bray-Hall S, Schmidt K, Aagaard E. Toward safe hospital discharge: transitions in care curriculum for medical students. J Gen Intern Med. 2010, 25, 878–881. [Google Scholar] [CrossRef]
- Ellis G, Whitehead MA, O’Neill D, Langhorne P, Robinson D. Comprehensive geriatric assessment for hospitalized older adults (review). Cochrane Database Syst. Rev. 0062. [CrossRef]
- Chiewchantanakit D, Meakchai A, Pituchaturont N, Dilokthornsakul P, Dhippayom T. The effectiveness of medication reconciliation to prevent medication error: A systematic review and meta-analysis. Res Soc Adm Pharm RSAP. 2020, 16, 886–894. [Google Scholar] [CrossRef] [PubMed]
- Tran-Nguyen S, Asha SE. A collaborative pharmacist-led intervention to prevent hospital readmissions among elderly patients discharged from the emergency department: a retrospective cohort study. Sci Rep 2024, 14, 15285. [Google Scholar] [CrossRef] [PubMed]
- Hagedoorn EI, Paans W, Jaarsma T, Keers JC, van der Schans C, Luttik ML. Aspects of family caregiving as addressed in planned discussions between nurses, patients with chronic diseases and family caregivers: A qualitative content analysis. BMC Nurs. 2017, 16, 37. [Google Scholar]
- Hickman LD, Phillips JL, Newton PJ, Halcomb EJ, Abed NA, Davidson PM. Multidisciplinary team interventions to optimize health outcomes for older people in acute care settings: A systematic review. Arch. Gerontol. Geriatr. 2015, 61, 322. [Google Scholar] [CrossRef]
- Guerin M, Grimmer K, Kumar S. Community services' involvement in the discharge of older adults from hospital into the community. Int J Integr Care. 2013, 13, e032. [Google Scholar]
- Soh YY, Zhang H, Toh JJY, Li X, Wu XV. The effectiveness of tele-transitions of care interventions in high-risk older adults: A systematic review and meta-analysis. Int J Nurs Stud. 2023, 139, 104428. [Google Scholar] [CrossRef]
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



