
Submitted:
31 October 2024
Posted:
01 November 2024
You are already at the latest version
Abstract
Background: Transcranial direct current stimulation (tDCS) is a non-invasive brain stimulation for treatment-resistant obsessive-compulsive disorder (OCD). We aim to compare treatment out-comes with newly developed dual-stie cathodal tDCS over the orbitofrontal cortex (OFC) and pre-supplementary motor area (pre-SMA) and two previously reported montages (cerebel-lum-OFC and pre-SMA) in patients with treatment-resistant OCD. Methods: Eighteen OCD pa-tients were randomly allocated to receive twice-daily 2mA/20min sessions for 10 consecutive weekdays with the active cathode placed on the cerebellum-OFC, bilaterally pre-SMA or OFC-pre-SMA tDCS. The primary outcome was the change of the Yale-Brown Obsessive–Compulsive Scale (Y-BOCS). Resting electroencephalogram (EEG) was recorded to obtain the default mode network (DMN) via low resolution electromagnetic tomography. Each patient re-ceived one-week and one-month follow-ups after 2-week stimulation. Results: At the end of stimulation, the Y-BOCS scores in the cerebellum-OFC, pre-SMA, and OFC-pre-SMA tDCS groups (each group, n=6) was decreased 14.15 ± 13.31, 7.4 ± 9.59, and 20.75 ± 8.70 %, respectively but no significant differences were found between groups. In the OFC-pre-SMA tDCS group, OC symptoms significantly decreased by a mean of -20.75% immediately after the 20th tDCS session and the improvement remained 1 week and 1 month after tDCS. For EEG source functional connectivity (FC) analyses, increased FC within the frontal network was found after OFC-pre-SMA tDCS whereas decreased FC within the DMN was observed after cerebellum-OFC tDCS. Conclusions: Dual-site cathodal tDCS over the OFC and pre-SMA might be the promising montage to treat patients with treatment-resistant OCD. Future studies using randomized sham-controlled designs are needed.
Keywords:
electroencephalogram
; functional connectivity
; obsessive-compulsive disorder
; pre-supplementary motor area
; transcranial direct current stimulation
1. Introduction
Obsessive-compulsive disorder (OCD), being characterized by distressing obsessions/compulsions and typically starting between childhood and early adulthood, is a common, chronic, and disabling disorder with high proportions of treatment resistance. Around one-third of OCD patients fail to benefit significantly from first-line treatment, e.g., serotonin reuptake inhibitors (SRIs) or cognitive behavioral therapy (CBT). Combining, augmenting, and switching strategies as second-line treatments also fail to bring much benefit for these patients. A high proportion of treatment resistance in OCD patients has prompted a search for novel treatment strategies, such as repetitive transcranial magnetic stimulation (rTMS), which is a non-invasive brain stimulation (NIBS) technique and has been approved by the US Food and Drug Administration (FDA) using H7 or double-cone coil for treatment-resistant OCD [1].
Transcranial direct current stimulation (tDCS) is a promising, safe, tolerable, easy to use, and cost-effective NIBS with scarce evidence for OCD. tDCS applies a weak direct current on the scalp and through the brain and rapidly leads to shifts in resting membrane potentials that may alter cortical excitability and the function of neural systems. The facilitation of depolarization or hyperpolarization of cortical pyramidal cell somas by radial current flow contributes to increased or decreased cortical excitability of the brain regions under the anode or cathode [2]. tDCS has local effects on the modulation of excitation-inhibition balance at the stimulation site as well as produces physiological effects at the network level [3]. By application simultaneous stimulation of tDCS over different ares, tDCS could modulate brain activity and connectivity within large widespread brain network. For example, facilitatory anodal tDCS over the primary motor cortex (M1) with inhibitory cathodal tDCS of the contralateral frontopolar cortex resulted in signicantly increased functional connectivity within premotor, motor, and sensormotor areas of the simulated hemisphere [4]. Furthermore, cathodal stimulation of bilateral inferior parietal lob nodes of the default mode network (DMN) decreased the frequency of negative mind-wandering thoughts about the past [5]. Repeated tDCS with inter-session interval can prolong the after-effects and behavioral effects of tDCS by modifying the efficacy of N-methyl-D-aspartate receptor and is increasingly used for therapeutic applications in neuropsychiatric disorders [6]. Taken together, tDCS might alleviate targeted symptoms through alteration molecular mechanism and brain connectivity.
Neuroimaging studies have identified abnormal activity and connectivity within the orbito-fronto-striato-pallido-thalamic network in patients with OCD, including decreased activity in the parietal cortex and cerebellum as well as increased activity in the supplementary motor area (SMA), anterior cingulate cortex (ACC), orbitofrontal cortex (OFC), and the caudate [7]. In a randomized sham-controlled study on 21 patients with treatment-resistant OCD receiving 10 sessions (twice daily) of 2mA for 20 mins over a 3-month follow-up period, cerebellum-OFC tDCS applied with the cathode over the orbitofrontal cortex (OFC) and the anode over the right cerebellum induced a significant acute reduction of OCD symptoms immediately after the tDCS regimen compared to sham stimulation [8]. In randomized sham-controlled study on 43 patients with treatment-resistant OCD receiving 20 daily sessions of 2mA for 30 mins over an 8-week follow-up period, pre-SMA tDCS applied with the cathode over the supplementary motor area (SMA) and the anode over the left deltoid induced a significant reduction of OCD symptoms compared to sham stimulation [9]. The first meta-analysis of eight studies including four randomized controlled trials (RCTs) and four open-label trials on 241 patients with OCD showed that the pooling data demonstrated large effect of tDCS in reducing OCD symptoms, but active tDCS was not superior to sham at the end of treatment when considering only the RCTs. High variability of tDCS montages and small sample sizes might explain the lack of positive effect when comparing active to sham tDCS. The pre-SMA was most used montage in the meta-analysis study, followed by cerebellum-OFC and SMA. As the cortico-striatal-thalamic-cortical (CTSC) neurocircuitry plays a key role in OCD, repetitive transcranial magnetic simulation (rTMS) studies showed sequential bilateral rTMS may yielde a more significant improvement than unilateral rTMS in OCD symptoms [10]. Based on multiple circuits involved in OCD and rTMS studies, we proposed that dual-site tDCS stimulation, which related to CTSC, may benefit more than previous commonly used montage such as cerebellum-OFC and SMA. Furthermore, given the high variability of tDCS montages as a limitation for OCD treatment, previous studies applied a computer modeling analysis to evaluate the electric field (EF) strengths in specific brain structures associated with OCD symptoms. EF analysis found that montages using the main electrode over the SMA with an extracephalic reference electrode might lead to stronger EFs. Therefore, application of an extracephalic positioning as reference electrode might provide better efficacy in reducing OCD symptoms. Future randomized controlled studies are encouraged to investigate better tDCS montages/protocols (e.g., tDCS simultaneously targeting multiple OCD-related structures) in larger sample sizes [11]. To our knowledge, no study has investigated the effects of concurrent dual-site cathodal tDCS over the OFC and pre-SMA (OFC-pre-SMA tDCS) with extracephalic reference electrode in patients with treatment-resistant OCD.
Consideration the involvement of CTSC abnormalities in the pathogenesis of OCD, majority of the neuropsychological studies have focused on these circuits. Several studies suggests that patients with OCD demonstrated consistently neuropsychological deficits in executive function, processing speed, sustained attention, and nonverbal memory deficits [12]. Some commonly used neuropsychological tests were adopted in patients with OCD. For example, a study of 40 patients with OCD performing the Tower of London test of planning suggests that patients have a selective deficit in generating alternative strategies when they make a mistake compared than healthy controls [13]. Another study reported executive and working memory deficits measured by Stroop test in patients with OCD associated with treatment resistance [14]. Furthermore, heart rate variability (HRV), a tool to assess information about alterations in the function of autonomous nervous system, may be a potential physiological biomarker of GAD. Studies showed patients with OCD responded to treatment have a higher parasympathetic tone compared those with not response to treatment [15]. Taken together, by application of neuropsychological and neurological test, we could not only understand the cognitive deficit and autonomic nervous system activity in patients with OCD but also examine the potential effect of intervention (e.g. tDCS in the present study) on them.
The aim of this study was to investigate the effectiveness of OFC-pre-SMA tDCS and another two previously reported tDCS montages (i.e., cerebellum-OFC tDCS and pre-SMA tDCS) in patients with treatment-resistant OCD. The null hypothesis was that there was no difference in the effectiveness of treating OCD symptoms when comparing the interventions of three different tDCS montages. As a secondary aim, the neuropsychological and neurophysiological changes were also measured after the tDCS interventions.
2. Materials and Methods
2.1. Participants
The trial was approved by the ethics committee of Tri-Service General Hospital, Taipei, Taiwan registered (ClinicalTrials.gov ID: NCT05595421). The inclusion criteria were: (1) eligible participants aged 20-65 with the primary clinical diagnosis of DSM-5-defined obsessive-compulsive disorder, (2) being treatment-resistant, as revealed by a Yale-Brown Obsessive and Compulsive Scale score (Y-BOCS) >16 despite at least two selective serotonin reuptake inhibitor (SSRI) trials of adequate dose and duration (or refusal to take medication for personal choice) and having been offered prior cognitive behavior therapy (CBT) by a trained practitioner, (3) the dosages of undergoing psychopharmacological medications having remained unchanged for 1 month before the beginning of the trial and remaining unchanged throughout the entire duration of the study, and (4) agreement to participate in the study and provide the written informed consent. The exclusion criteria were: (1) having contraindications for transcranial electrical stimulation or transcranial magnetic stimulation, e.g., pacemakers, metallic or magnetic pieces in the head/brain, ear implants and other implantable brain medical devices, (2) pregnancy or breastfeeding at enrollment, (3) having active substance use disorder (in exception to caffeine and/or tobacco), (4) having a history of seizures, (5) having a history of intracranial neoplasms or surgery, or a history of severe head injuries or cerebrovascular diseases, (6) skin lesions on scalp at the area of electrode application, and (7) having unstable medical conditions at enrollment. Participants received a compensation of $66.67 if they properly completed the study.
2.2. tDCS Intervention
The study was a randomized, single-blind, clinical trial comparing different montages of transcranial direct current stimulation on treatment-resistant obsessive–compulsive disorder. Participants were randomized to one of the three groups: (1) cerebellum-OFC tDCS, (2) pre-SMA tDCS, and (3) OFC-pre-SMA tDCS. Figure 1 illustrated the modeling of electric field distribution across three tDCS groups. Stimulation sessions were applied using a DC stimulator (neuroConn, Ilmeneau, GmbH). All patients received twice-daily sessions separated by at least 1 h for 10 consecutive weekdays. We chose twice-daily stimulation instead of daily simulation because of previous studies showing better efficacy with twice-daily stimulation than once a day. For example, in a double-blind randomized study of 93 vascular depression receiving tDCS stimulation for 10 consecutive working days showed twice-daily stimulation achieved a significantly greater symptoms improvement than daily stimulation and sham group [16]. Furthermore, twice-daily tDCS stimulation boosts cortical plasticity and improves memory in a study of 124 patients with Alzheimer`s disease [17]. Therefore, we chose twice-daily sessions in the present study. Each session of tDCS consisted of a direct current of 2 mA delivered for 20 min. In the cerebellum-OFC tDCS group, two 7 × 5 cm (35 cm2) sponge electrodes soaked in a saline solution (0.9% NaCl) were applied with the anode placed over the right cerebellum (i.e., 3 cm below the inion and 1 cm right from the midline) and the cathode over FP1 according to the international 10–20 system (i.e, the left OFC). In the pre-SMA tDCS group, the cathode (5 × 5 cm) was placed on the sagittal midline at 15% of the distance between inion and nasion anterior to Cz (vertex) to target the bilateral presupplementary motor area (pre-SMA). The reference electrode (5 × 7 cm) was placed on the lateral surface of the patients’ right deltoid. In the OFC-pre-SMA tDCS group, the stimulator is connected to a 2 × 1 wire adaptor (Equalizer Box, NeuroConn). The first cathode (5 × 5 cm) was placed over the sagittal midline at 15% of the distance between inion and nasion anterior to Cz (vertex). The second cathode (5 × 7 cm) was placed over FP1. The reference electrode (5 × 7 cm) was placed on the lateral surface of the right deltoid. Study outcomes are measured by a clinical rater (HAC) blinded to the group assignment. The adverse effects of tDCS were measured by a well-established tool [18]. The timeline for treatment and assessments is provided in Figure 2.
2.3. Clinical Outcome Measures
The primary outcome measure was the change in the score of the Yale-Brown Obsessive-Compulsive Scale (Y-BOCS) from baseline to the end of stimulation. Y-BOCS is a 10-item scale designed to assess obsessions and compulsions by measuring the severity and type of symptoms of OCD patients over the past seven days. Total Y-BOCS scores range from 0 to 40, with higher scores indicating greater severity of OCD symptoms. Scores on the obsession and compulsion subscales range from 0 to 20, but only the total Y-BOCS score is interpreted [19]. Other clinical measures included the changes from baseline in the score of self-reporting OCD Visual Analog Scale (OCD-VAS), Hamilton Depression Rating Scale (HAM-D), Hamilton Anxiety Rating Scale (HAM-A), and World Health Organization Quality of Life-BREF (WHO-BREF). We included HAMD-D, HAM-A, and WHO-BREF because patients with OCD tended to comorbid depression and anxiety symptoms, which both may contribute lower quality of life [20].
2.4. Neuropsychological Outcomes
Neuropsychological outcomes were measured with Color Trails Test (CTT) for assessing sustained visual attention [21], Stroop Color Word Test (SCWT) for assessing selective attention and cognitive flexibility [22], Connors’ Continuous Performance Test –2nd Edition (CPT-II) for assessing concentration, sustained attention, response inhibition and impulsivity [23], Tower of London-Drexel University Test 2nd Edition (TOLDXtm) [24] for assessing executive functioning, especially concerning the ability of planning, processing, and problem-solving skills, and the Digit Symbol Substitution Test (DSST) for assessing attention, executive function, and processing speed.
2.5. Neurophysiological Outcomes
2.5.1. Heart Rate Variability (HRV)
The participants sat quietly in a light-controlled, soundproof room and breathe spontaneously. After a 20-minute rest, two electrodes were placed on the right and left arm just below the elbow and a ground electrode placed below the wrist on the right arm with a lead I electrocardiogram taken for 5 minutes. An HRV analyzer (LR8Z11, Yangyin Corp., Taipei, Taiwan) acquired, stored, and processed the electrocardiography signals. The power spectral analysis was performed using a non-parametric fast Fourier transformation to obtain high-frequency power (HF, 0.15–0.40 Hz) to represent vagal control of HRV.
2.5.2. Electroencephalogram (EEG)
Resting-state EEG was collected using a 19-channel EEG (Neuro Prax® TMS/tES compatible full band DC-EEG system, NeuroConn GmbH, Ilmenau, Germany) with Ag/AgCl sintered ring electrodes placed according to the international 10–20 system, using a sampling frequency of 4000 Hz, an analogue-digital precision of 24 bits, and an analogous 0–1200 Hz bandpass filter. Patients sat comfortably in a recliner in a light and sound-attenuated room. The participants were instructed not to drink caffeinated beverages one hour before EEG recording and alcohol 24 hours before recording to avoid caffeine- or alcohol-induced changes in the EEG stream.
The reference and ground electrodes were placed at the tip of the nose and Fpz, respectively. Horizontal electrooculogram (HEOG) recorded by two electrodes will be placed at 1 cm from the outer canthi of both eyes. Two electrodes will be placed above and below the left eye, respectively, to record the blinks and vertical electrooculogram (VEOG). The impedance of each electrode will be checked to remain below 5 kΩ. Patients were instructed to stay relaxed in a state of mind wandering with their eyes closed and resting-state EEG was recorded for 5 min. Offline, the data were downsampled to 256 Hz, band-pass filtered to 1–100 Hz, and analog 60 Hz-notch filtered using EEGLAB v2020.0 [25]. Artifact subspace reconstruction (ASR) was used to automatically detected and removed bad channels [26]. Independent component analysis (ICA) followed by ICLabel [27] was used to automatically remove artifacts caused by muscle activity, heartbeats, eye movements, and eye blinks. Only accepted epochs of eyes-closed rsEEG data were chosen for electrical source estimation.
2.5.3. Functional Connectivity Analysis in EEG Source Space
EEG-source estimate and connectivity analysis were performed using the exact low resolution electromagnetic tomography (eLORETA) algorithm, linear inverse solution for scalp-recorded EEG signals that has no localization error to point sources under noise-free conditions [28]. Cortical regions of interest (ROIs) for connectivity analysis were determined a priori based on previous studies reporting dysfunctional connectivity within the default mode network (DMN) and frontal network (FN) in OCD [29]. A voxel-wise approach was adopted to determine ROIs (4 from the DMN and 5 from the FN) by including all gray matter voxels within a 20mm radius of the seed points (see their MNI coordinates in Table 2). Time series with the average current density of all voxels from each ROI were calculated for subsequent computation of functional connectivity. Functional connectivity between each pair of ROIs was defined as the lagged non-linear coherence of intracortical EEG-source estimates. Only the lagged coherence was considered as physiological connectivity between ROIs because instantaneous (or zero-lag) coherence can be caused by the intrinsic artifacts due to low spatial resolution of the eLORETA solution and non-physiological effects such as volume conduction [28]. Only the non-linear part of lagged coherence was considered because this measure was based on normalized Fourier transforms and did not take into account any amplitude information. Previous research has linked non-linear lagged coherence with a fundamental process of neural communication associated with synaptic plasticity [30]. The lagged non-linear coherence was calculated for the EEG delta (1.5–4 Hz), theta (4–8 Hz), alpha (8–12 Hz), beta 1 (12–30 Hz), beta 2 (20–30 Hz) and gamma (30–80 Hz) frequency bands.
2.6. Sample Size Calculation
Sample size is estimated using data from previous research on tDCS in treating OCD to obtain the comparisons between baseline and endpoints of active treatment group [7]. In an open-label trial by Bation et al., cerebellum-OFC tDCS largely improved OCD symptoms (effect size= 1.21) [31]. In a randomized controlled trial by Da Silva et al., pre-SMA tDCS also largely improved OCD symptoms (effect size= 1.05 for the active group) [9]. In this trial, OFC-pre-SMA tDCS was assumed to have additive treatment effects of cerebellum-OFC tDCS and pre-SMA tDCS. With these assumptions, a large difference was estimated between the tDCS interventions with three different montages. G*power 3.1.9.4 is used to calculate the sample size of ANOVA (fixed effects, omnibus, one-way) for the primary outcome measurement with effect size f = 0.6, alpha error probability = 0.05, power (1- beta error probability) = 0.8, and number of groups = 3. The calculated total sample size is 30. Thus, a sample of 36 (N=12 in each group, please see ClinicalTrials.gov ID: NCT05595421) would be required assuming a 16% dropout rate. The trial stopped early before it attained its planned sample size because researchers failed to timely enroll eligible participants, and consequently funding vanished.
2.7. Statistics
SPSS Statistics 24.0 software (IBM SPSS Inc., Chicago, IL, USA) was used for all analyses. Univariate analyses of variance (ANOVAs) were conducted to compare demographic data, clinical variables at baseline, and the changes in outcome measures after tDCS between the three tDCS groups. The chi-squared tests were used to examine between-group differences in discrete variables. The null hypothesis was rejected with p<0.05 for the primary outcome measure (i.e., the change of the Y-BOCS score from baseline to the end of stimulation). A significant effect would be followed by post hoc analyses where Bonferroni corrections were applied for multiple testing. For the within-group comparisons of continuous variables, paired t-tests were used for parametric variables, and the Wilcoxon Signed Rank tests for nonparametric variables. In these analyses, we did not apply corrections for multiple comparisons due to the nature of exploratory testing. To compare the EEG source functional connectivity between each ROIs (in each frequency band) at the end of stimulation to that at baseline, paired t tests were used. The statistical nonparametric mapping (SnPM) methodology included in the eLORETA software was used to adjust for multiple comparisons by implementing a non-parametric permutation procedure (5000 randomizations). The level of significance for the analyses conducted was set at p=0.05 (two-tailed).
3. Results
3.1. Sample Characteristics
Of the 64 screened patients, 41 were eligible. Only 18 accepted to participate in the trial and were randomly allocated to receive cerebellum-OFC (n=6), pre-SMA (n=6) or OFC-pre-SMA tDCS (n=6). All of them completed 20 sessions of the trial. There were no significant between-group differences in the sociodemographic and clinical characteristics at baseline (Table 1). No participant drops out from this study.
3.2. Primary Outcome
At the end of stimulation, the percentage of Y-BOCS score reduction in the cerebellum-OFC, pre-SMA, and OFC-pre-SMA tDCS groups was 14.15 ± 13.31, 7.4 ± 9.59, and 20.75 ± 8.70 %, respectively. When comparing the three groups, there were no significant differences in the percentage change of Y-BOCS score at the end of stimulation (F=2.32, p=0.13, Figure 3). The results were similar at the one-week follow-up (F=0.61, p=0.56) and at the one-month follow-up (F=0.13, p=0.88). Regarding the difference of Y-BOCS raw score from the baseline, within-group analyses showed that Y-BOCS score significantly reduced at the end of stimulation in the cerebellum-OFC (t = -2.70, p =0.043) and OFC-pre-SMA (t = -4.68, p =0.005) tDCS groups. The effects for both groups persisted until the end of the trial (all p values < 0.05). The reduction in Y-BOCS score was not significant at the end of stimulation in the pre-SMA tDCS group (t = -1.90, p =0.12) but reached significance at the one-week (t = -2.65, p =0.045) and one-month (t = -2.62, p =0.047) follow-ups. When comparing the three groups, there were no significant differences in the change of Y-BOCS raw score from baseline at the end of stimulation (F=1.63, p=0.23), the one-week follow-up (F=0.88, p=0.48) and at the one-month follow-up (F=0.20, p=0.82).
3.3. Secondary Outcomes
The changes in the score of HAMD, HAMA, OCD-VAS, and all WHOQOL-BREF subdomains at the end of stimulation and follow-up visits were not significantly different between the cerebellum-OFC, pre-SMA, and OFC-pre-SMA tDCS groups (all p values > 0.05). Within-group analyses showed that compared to baseline, OCD-VAS scores at the end of stimulation (t=-4.70, p=0.005), at the one-week follow-up (t=-3.89, p=0.011) and at the one-month follow-up (t=-2.70, p=0.043) were significantly reduced in the OFC-pre-SMA tDCS group. The psychological domain score of WHOQOL at the one-month follow-up (t=2.99, p=0.031) was significantly increased in the pre-SMA tDCS group. When comparing the three groups, there were no significant differences in the change of performance in cognitive tests and HF-HRV at the end of stimulation (F=0.11, p=0.90). Within-group analyses showed that compared to baseline, CTT Color 2 time (t=5.91.20, p=0.002) and CPT-II d’ (z=2.20, p=0.03) at the end of stimulation were significantly decreased and increased in the pre-SMA tDCS group.
3.4. Safety and Tolerability
tDCS was well tolerated by the patients, no serious adverse event was observed.
There were no significant differences between the occurrences of treatment-emergent adverse events in the three tDCS groups (Table 3).
3.5. EEG Source Functional Connectivity Analyses
Significant differences between baseline and the end of stimulation emerged for within-DMN connectivity in the cerebellum-OFC tDCS group. Non-linear lagged coherence between a region in the anterior cingulate gyrus (ACC) and a region in the right inferior parietal lobule (IPL) in the beta 1 frequency band (12–20 Hz) was decreased at the end of stimulation compared to baseline (t = -3.83, p = 0.012; Figure 4A). In the OFC-pre-SMA tDCS group, within-FN connectivity significantly changed from baseline to the end of stimulation. Non-linear lagged coherence between a region in the right superior/middle frontal gyrus (rSFG) and a region in the left superior/middle frontal gyrus (lSFG) in the beta 2 frequency band (20–30 Hz) was increased at the end of stimulation compared to baseline (t = 3.77, p = 0.013; Figure 4B). Neither within-DMN nor within-FN connectivity significantly changed from baseline to the end of stimulation in the pre-SMA tDCS group.

Table 2.
MNI coordinates for the seeds from the default mode network (DMN) and frontal network (FN).
Table 2.
MNI coordinates for the seeds from the default mode network (DMN) and frontal network (FN).
| Network | Anatomic structure | Side | |||
|---|---|---|---|---|---|
| data | Anterior cingulate gyrus (ACC) | Mid | 0 | 53 | 0 |
| Posterior cingulate gyrus (PCC) | Mid | 0 | -53 | 29 | |
| Inferior parietal lobule (IPL) | R | 60 | -40 | 27 | |
| Inferior parietal lobule (IPL) | L | -60 | -40 | 27 | |
| Anterior cingulate gyrus (ACC) | Mid | 0 | 41 | 0 | |
| Superior/middle frontal gyrus (SFG) | R | 31 | 36 | 38 | |
| Superior/middle frontal gyrus (SFG) | L | -31 | 36 | 38 | |
| Medial frontal gyrus (MFG) | R | 14 | 48 | -4 | |
| data | Medial frontal gyrus (MFG) | L | -14 | 48 | -4 |
4. Discussion
Our study is the first to investigate the effectiveness of concurrent dual-site cathodal tDCS over the OFC and pre-SMA (OFC-pre-SMA tDCS) applied as a therapeutic tool to reduce OC symptoms in patients with treatment-resistant OCD. Our study is also the first to compare the clinical effects among three kinds of tDCS montages (cerebellum-OFC, OFC-pre-SMA, and pre-SMA tDCS) in treating OCD.
The present study provided the preliminary results, showing the novel dual-site OFC-pre-SMA cathodal tDCS contributed to higher OC symptoms reduction than previous commonly adopted montage (cerebellum-OFC and pre-SMA tDCS). Some reasons might explain the higher efficacy in the treatment of OCD using the novel montage. First, the OFC-pre-SMA cathodal tDCS montage could induce higher EFs and allow the current flow to penetrate more deeply into the brain [7]. Second, dual-site tDCS montage stimulated more brain regions involving in the CTSC neurocircuitry of OCD, leading to higher reduction of OC symptoms [10]. Notably, the results should be cautious because there is no sham control group in the present study. Placebo response is not negligible in the brain stimulation trial. However, it is well-known that studies showed reduced placebo response was observed for OCD than other psychiatric diagnoses [32]. The present study enrolled treatment-resistant OCD, which may make the symptoms more resistant to further intervention.
Our results indicated tDCS using different montages was safe and tolerable in treating patients with treatment-resistant OCD. Although the improvement of OCD symptoms at the end of stimulation was not significantly different between the three tDCS groups, OFC-pre-SMA tDCS was considered the most promising montage in this study. In the OFC-pre-SMA tDCS group, clinician-rated OC symptoms significantly decreased by a mean of -20.75% immediately after the 20th tDCS session and the improvement remained 1 week and 1 month after tDCS. The results were similar for the self-rated OC symptoms as well. Moreover, our findings provided neurophysiological evidence that EEG beta-2 band functional connectivity within the frontal network (i.e., between the right and left SFG) was significant increased at the end of OFC-pre-SMA tDCS. Previous EEG research has indicated decreased EEG lagged non-linear coherence at the beta 2 frequency within frontal brain regions for OCD patients in comparison to healthy individuals [29]. Non-linear coherence represents a synaptic plasticity-associated basic process of neural communication while non-linear coherence at beta frequency is especially vital for the encoding and retrieval of memory as well as information maintenance [29]. A lack of synchronization for the oscillatory cycle of neuronal populations in the frontal network reflects an altered intra and inter-hemispheric neuronal communication within these areas during rest and may imply a pathomechanism related to OCD. Taken together, findings reported herein are helpful for developing novel neurobiologically based intervention strategies for OCD. Future randomized clinical trials are needed to investigate whether OFC-pre-SMA tDCS improve OC symptoms through rectifying abnormal frontal network synchronization in patients with treatment-resistant OCD.
Our study showed that the YBOCS score decreased by a mean of -14.15% after the 20th session of cerebellum-OFC tDCS. Abnormalities in cerebellum and OFC have been implicated in the pathophysiology of OCD. Neuroimaging studies in patients with OCD reported hyperactive OFC, hypoactive cerebellum, dysconnectivities between right and left cerebellar areas, and between the OFC and the cerebellum [7]. tDCS targeting the right cerebellum and the left OFC has been reported as an efficient approach to alleviate symptoms in patients with OCD, possibly through its modulation of a large interconnected corticosubcortical network involved in the pathophysiology of OCD. By using head models for optimally targeting current delivery to structures of interest, earlier research on tDCS computational analysis has revealed that tDCS using pre-SMA montage activate most of the areas related to OCD [33]. As opposed to pre-SMA montage, a recent study of electric field (EF) modeling analyses indicates cerebellum-OFC tDCS montage can induce a stronger EF intensity in the right dorsolateral prefrontal cortex and bilateral SMA/pre-SMA [7]. In a randomized sham-controlled double-blind study, patients with treatment-resistant OCD received 10 sessions of either active cerebellum-OFC tDCS (2 mA, 20-min, and two sessions per day) or sham [8]. The results indicated that cerebellum-OFC tDCS was not superior to sham in inducing a long-lasting reduction of symptoms (over a 12-week period) in patients with treatment-resistant OCD though it induced a significant acute reduction of OCD symptoms immediately after the tDCS regimen compared to sham stimulation. Taken together, future studies are encouraged to investigate if more number of sessions (e.g., 30 sessions) with more extended periods of treatment (e.g., 6 weeks) can positively influence the efficacy of cerebellum-OFC tDCS in treating in patients with treatment-resistant OCD.
The clinical benefit after cerebellum-OFC tDCS of the present study was also supported by significant reduction of EEG beta-1 band DMN connectivity between a region in the ACC and right IPL. Aberrant DMN has a crucial role in psychological process related to pathophysiological mechanisms of OCD and dysregulation DMN may contribute aberrant self-referential processing and preoccupation of self-oriented intrusive obsessive thoughts in OCD patients [34]. Neuroimaging studies have observed increased functional connectivity within the DMN in patient with OCD [35]. Similarly, increased DMN connectivity, which should be deactivated during cognitive task performance, was found when OCD patients received reward processing [36]. Regarding IPL, another study showed OCD patients had higher DMN connectivity between right IPL and left ventral medial PFC, which being with ACC, and both are involved in emotional and reward processing and decision making [37,38]. Notably, both thinned IPL and deficient neurite density in the right IPL among adult patients with OCD were reported [39,40]. It has been proposed that IPL plays an important role in regulation internal thought and external information. A lack of cognitive flexibility related to dysfunction of parietal cortex was found in patients with OCD, leading to excessive absorption with internally generated fears that are disharmony with evidence present in the external cues [41]. In sum, the present study showed cerebellum-OFC tDCS improved OCD symptoms after the end of stimulation and results were supported by neurophysiological evidence of reduction of EEG beta-1 band DMN functional connectivity.
Notably, the YBOCS score only decreased by a mean of -7.4% after the 20th session of pre-SMA tDCS. Previous studies reported cathodal pre-SMA stimulation reduced OC symptoms measured by mean Y-BOCS severity scores significantly than anodal stimulation, ranging from 20.1% (2mA/20 min for 20 sessions) [42]to 26.4% (2mA/30 min for 10 sessions) [43]. However, one double blinded, randomized, sham controlled study showed excitatory anodal tDCS stimulation reduced OC severity by 22.06% [44]. The inconsistency between studies might be derived from small sample sizes, lack of sham group, treatment duration, and variability of tDCS montage. For example, study by Gowda et al using anode over left pre-SMA with cathode over right supra-orbital area may lead to a different direction of the current flow, explaining the beneficial effect in reducing OC symptoms via excitatory anodal tDCS [44]. However, this could not explain the different between ours and study by D'Urso G et al, which both studies used same montage but much lower OC symptoms reduction in the present study (7.4% vs 20.1%). Another interesting finding of the present study was the pre-SMA tDCS was the only montage to produce delayed tDCS effects, reducing Y-BOCS by 14.4% and 22.8% in one-week and one-month follow-up period. It may take weeks to demonstrate efficacy using bilateral pre-SMA. The after-effects of tDCS have been linked to non-synaptic mechanisms involving neurogenesis [45]. Taken together, it is unclear whether an anode or cathode over pre-SMA is the most suitable montage to treat OCD patients. Therefore, it is important to tailored montage to the individuals by applying EF modeling analysis accounting for interindividual anatomical variability and follow-up period to detect possible after-effects of tDCS was warranted, particularly for pre-SMA region.
Our study had limitations. The first is the small sample size and the non-controlled, single-blind study design. The placebo response in the participants was not addressed because both the tDCS administer and patients were aware of the assigned treatment. The clinical response might have been inflated due to an expectancy bias. Nevertheless, it is expected that sham tDCS will show a low response in treatment-resistant patients with severe OCD severity given that greater OCD severity was associated with less sham responses. Second, small sample sizes might provide inadequate statistical power to detect significant difference in OCD symptoms reduction between three different intervention montage. However, the present study is the hypothesis-driven research to reveal that novel dual-site cathodal tDCS over the OFC and pre-SMA might be the most promising intervention in treatment resistance OCD accompany by pathophysiological evidence from EEG. The study provides valuable research direction in patient with treatment resistance OCD. Third, the study did not apply OCD symptom provocation before a tDCS session. The benefits of exposure therapies before rTMS intervention have been revealed. Future studies are advised to investigate the benefits of OC symptoms provocation in combination with tDCS. Third, EEG fails to detect sources of electrical activity in deep structures (e.g., striatum, thalamus and cerebellum) as well as the network connectivity in the areas. Furthermore, EEG findings in the present study may be not so conclusive due to small sample sizes and lower statistical power to detect differences. Future studies with large sample size to confirm our current findings are warranted.
5. Conclusions
We suggested that future studies should examine the efficacy in larger samples of treatment-resistant OCD and explore the efficacy of concurrent dual-site cathodal tDCS over the OFC and pre-SMA (OFC-pre-SMA tDCS) in treating OC symptoms using randomized sham-controlled designs.
Ethics approval:
All experimental procedures conformed to the standards set by the latest revision of the Declaration of Helsinki and were approved by the ethics committee of Tri-Service General Hospital (protocol code: 1-108-03-001 and date of approval: April 12, 2019).
Author Contributions
Conception and design of study: Chuan-Chia Chang, Hsin-An Chang; Acquisition of data: Hsin-An Chang; Analysis and/or interpretation of data: Chuan-Chia Chang, Hsin-An Chang; Drafting the manuscript: Che-Sheng Chu; Revising the manuscript critically for Important intellectual content: Yen-Yue Lin, Cathy Chia-Yu Huang, Yong-An Chung, Sonya Youngju Park and Wei-Chou Chang; Approval of the version of the manuscript to be Published: Hsin-An Chang.
Funding
This study was supported in part by grants from Advanced National Defense Technology & Research Program, Medical Affairs Bureau, Ministry of National Defense (MND-MAB-D-113074), National Science and Technology Council of Taiwanese Government (NSTC-112-2314-B-016-017-MY3, NSTC-112-2314-B-075B-006), Kaohsiung Veterans General Hospital (KSVGH113-069, KSVGH112-123, KSVGH112-124), and Tri-Service General Hospital (TSGH-A-112011). The funders had no role in the design of the study; in the collection, analyses, or interpretation of data; in the writing of the manuscript, or in the decision to publish the results.
Data Availability Statement
The datasets generated during and/or analyzed during the current study are available from the corresponding author on reasonable request.
Acknowledgments
We appreciate all the patients who have participated in this study. The authors also acknowledge the PET-MRI support from the Department of Radiology at Tri-Service General Hospital
Conflicts of Interest
The Authors declare that there is no conflict of interest.
References
- Zhou, S.; Fang, Y. Efficacy of Non-Invasive Brain Stimulation for Refractory Obsessive-Compulsive Disorder: A Meta-Analysis of Randomized Controlled Trials. Brain Sci. 2022, 12, 7. [Google Scholar] [CrossRef] [PubMed]
- Nitsche, M.A.; Fricke, K.; Henschke, U.; Schlitterlau, A.; Liebetanz, D.; Lang, N. , et al. Pharmacological modulation of cortical excitability shifts induced by transcranial direct current stimulation in humans. J Physiol. 2003, 553, 293–301. [Google Scholar] [CrossRef] [PubMed]
- Sehatpour, P.; Dondé, C.; Hoptman, M.J.; Kreither, J.; Adair, D.; Dias, E. , et al. Network-level mechanisms underlying effects of transcranial direct current stimulation (tDCS) on visuomotor learning. Neuroimage. 2020, 223, 117311. [Google Scholar] [CrossRef] [PubMed]
- Polanía, R.; Nitsche, M.A.; Paulus, W. Modulating functional connectivity patterns and topological functional organization of the human brain with transcranial direct current stimulation. Hum Brain Mapp. 2011, 32, 1236–1249. [Google Scholar] [CrossRef]
- Chou, T.; Hooley, J.M.; Camprodon, J.A. Transcranial direct current stimulation of default mode network parietal nodes decreases negative mind-wandering about the past. Cognit Ther Res. 2020, 44, 10–20. [Google Scholar] [CrossRef]
- Nitsche, M.A.; Cohen, L.G.; Wassermann, E.M.; Priori, A.; Lang, N.; Antal, A. , et al. Transcranial direct current stimulation: State of the art 2008. Brain Stimul. 2008, 1, 206–223. [Google Scholar] [CrossRef]
- Pinto, B.S.; Cavendish, B.A.; da Silva, P.H.R.; Suen, P.J.C.; Marinho, K.A.P.; Valiengo, L.; et al. The Effects of Transcranial Direct Current Stimulation in Obsessive-Compulsive Disorder Symptoms: A Meta-Analysis and Integrated Electric Fields Modeling Analysis. Biomedicines 2022, 11, 1. [Google Scholar] [CrossRef]
- Bation, R.; Mondino, M.; Le Camus, F.; Saoud, M.; Brunelin, J. Transcranial direct current stimulation in patients with obsessive compulsive disorder: A randomized controlled trial. Eur Psychiatry. 2019, 62, 38–44. [Google Scholar] [CrossRef]
- Silva, R.; Brunoni, A.R.; Goerigk, S.; Batistuzzo, M.C.; Costa, D.; Diniz, J.B. , et al. Efficacy and safety of transcranial direct current stimulation as an add-on treatment for obsessive-compulsive disorder: a randomized, sham-controlled trial. Neuropsychopharmacology. 2021, 46, 1028–1034. [Google Scholar] [CrossRef]
- Grassi, G.; Moradei, C.; Cecchelli, C. Will Transcranial Magnetic Stimulation Improve the Treatment of Obsessive-Compulsive Disorder? A Systematic Review and Meta-Analysis of Current Targets and Clinical Evidence. Life (Basel). 2023, 13, 7. [Google Scholar] [CrossRef]
- Acevedo, N.; Bosanac, P.; Pikoos, T.; Rossell, S.; Castle, D. Therapeutic Neurostimulation in Obsessive-Compulsive and Related Disorders: A Systematic Review. Brain Sci. 2021, 11, 7. [Google Scholar] [CrossRef] [PubMed]
- Benzina, N.; Mallet, L.; Burguière, E.; N'Diaye, K.; Pelissolo, A. Cognitive Dysfunction in Obsessive-Compulsive Disorder. Curr Psychiatry Rep. 2016, 18, 80. [Google Scholar] [CrossRef] [PubMed]
- Veale, D.M.; Sahakian, B.J.; Owen, A.M.; Marks, I.M. Specific cognitive deficits in tests sensitive to frontal lobe dysfunction in obsessive-compulsive disorder. Psychol Med. 1996, 26, 1261–1269. [Google Scholar] [CrossRef]
- Doolub, D.; Vibert, N.; Botta, F.; Razmkon, A.; Bouquet, C.; Wassouf, I. , et al. High treatment resistance is associated with lower performance in the Stroop test in patients with obsessive-compulsive disorder. Front Psychiatry. 2023, 14, 1017206. [Google Scholar] [CrossRef]
- Olbrich, H.; Jahn, I.; Stengler, K.; Seifritz, E.; Colla, M. Heart rate variability in obsessive compulsive disorder in comparison to healthy controls and as predictor of treatment response. Clin Neurophysiol. 2022, 138, 123–131. [Google Scholar] [CrossRef]
- Zanardi, R.; Poletti, S.; Prestifilippo, D.; Attanasio, F.; Barbini, B.; Colombo, C. Transcranial direct current stimulation: A novel approach in the treatment of vascular depression. Brain Stimul. 2020, 13, 1559–1565. [Google Scholar] [CrossRef]
- Li, X.; Chen, L.; Yu, K.; Zhuang, W.; Zhu, H.; Xu, W. , et al. Impact of twice-a-day transcranial direct current stimulation intervention on cognitive function and motor cortex plasticity in patients with Alzheimer's disease. Gen Psychiatr. 2023, 36, e101166. [Google Scholar] [CrossRef]
- Brunoni, A.R.; Amadera, J.; Berbel, B.; Volz, M.S.; Rizzerio, B.G.; Fregni, F. A systematic review on reporting and assessment of adverse effects associated with transcranial direct current stimulation. Int J Neuropsychopharmacol. 2011, 14, 1133–1145. [Google Scholar] [CrossRef]
- Goodman, W.K.; Price, L.H.; Rasmussen, S.A.; Mazure, C.; Fleischmann, R.L.; Hill, C.L.; The Yale-Brown Obsessive Compulsive Scale, I.; et al. Development, use, and reliability. Arch Gen Psychiatry. 1989, 46, 1006–1011. [Google Scholar] [CrossRef]
- Remmerswaal, K.C.P.; Batelaan, N.M.; Hoogendoorn, A.W.; van der Wee, N.J.A.; van Oppen, P.; van Balkom, A. Four-year course of quality of life and obsessive-compulsive disorder. Soc Psychiatry Psychiatr Epidemiol. 2020, 55, 989–1000. [Google Scholar] [CrossRef]
- Maj, M.; D'Elia, L.; Satz, P.; Janssen, R.; Zaudig, M.; Uchiyama, C. , et al. Evaluation of two new neuropsychological tests designed to minimize cultural bias in the assessment of HIV-1 seropositive persons: a WHO study. Arch Clin Neuropsychol. 1993, 8, 123–135. [Google Scholar] [CrossRef] [PubMed]
- Scarpina, F.; Tagini, S. The Stroop Color and Word Test. Front Psychol. 2017, 8, 557. [Google Scholar] [CrossRef] [PubMed]
- López-Luengo, B.; González-Andrade, A.; García-Cobo, M. Not All Differences between Patients with Schizophrenia and Healthy Subjects Are Pathological: Performance on the Conners' Continuous Performance Test. Arch Clin Neuropsychol. 2016, 31, 983–995. [Google Scholar] [CrossRef] [PubMed]
- García-Alba, J.; Esteba-Castillo, S.; Castellanos López, M.; Janssen, R.; Zaudig, M.; Uchiyama, C. , et al. Validation and Normalization of the Tower of London-Drexel University Test 2nd Edition in an Adult Population with Intellectual Disability. Span J Psychol. 2017, 20, E32. [Google Scholar] [CrossRef]
- Delorme, A.; Makeig, S. EEGLAB: an open source toolbox for analysis of single-trial EEG dynamics including independent component analysis. J Neurosci Methods. 2004, 134, 9–21. [Google Scholar] [CrossRef]
- Chang, C.Y.; Hsu, S.H.; Pion-Tonachini, L.; Jung, T.P. Evaluation of Artifact Subspace Reconstruction for Automatic Artifact Components Removal in Multi-Channel EEG Recordings. IEEE Trans Biomed Eng. 2020, 67, 1114–1121. [Google Scholar] [CrossRef]
- Pion-Tonachini, L.; Kreutz-Delgado, K.; Makeig, S. ICLabel: An automated electroencephalographic independent component classifier, dataset, and website. Neuroimage. 2019, 198, 181–197. [Google Scholar] [CrossRef]
- Pascual-Marqui, R.D.; Lehmann, D.; Koukkou, M.; Kochi, K.; Anderer, P.; Saletu, B. , et al. Assessing interactions in the brain with exact low-resolution electromagnetic tomography. Philos Trans A Math Phys Eng Sci. 2011, 369, 3768–3784. [Google Scholar]
- Olbrich, S.; Olbrich, H.; Adamaszek, M.; Jahn, I.; Hegerl, U.; Stengler, K. Altered EEG lagged coherence during rest in obsessive-compulsive disorder. Clin Neurophysiol. 2013, 124, 2421–2430. [Google Scholar] [CrossRef]
- Fell, J.; Axmacher, N. The role of phase synchronization in memory processes. Nat Rev Neurosci. 2011, 12, 105–118. [Google Scholar] [CrossRef]
- Bation, R.; Poulet, E.; Haesebaert, F.; Saoud, M.; Brunelin, J. Transcranial direct current stimulation in treatment-resistant obsessive-compulsive disorder: An open-label pilot study. Prog Neuropsychopharmacol Biol Psychiatry. 2016, 65, 153–157. [Google Scholar] [CrossRef] [PubMed]
- Sugarman, M.A.; Kirsch, I.; Huppert, J.D. Obsessive-compulsive disorder has a reduced placebo (and antidepressant) response compared to other anxiety disorders: A meta-analysis. J Affect Disord. 2017, 218, 217–226. [Google Scholar] [CrossRef] [PubMed]
- Senço, N.M.; Huang, Y.; D'Urso, G.; Parra, L.C.; Bikson, M.; Mantovani, A. , et al. Transcranial direct current stimulation in obsessive-compulsive disorder: emerging clinical evidence and considerations for optimal montage of electrodes. Expert Rev Med Devices. 2015, 12, 381–391. [Google Scholar] [CrossRef] [PubMed]
- Szechtman, H.; Woody, E. Obsessive-compulsive disorder as a disturbance of security motivation. Psychol Rev. 2004, 111, 111–127. [Google Scholar] [CrossRef]
- Fan, J.; Zhong, M.; Gan, J.; Liu, W.; Niu, C.; Liao, H. , et al. Altered connectivity within and between the default mode, central executive, and salience networks in obsessive-compulsive disorder. J Affect Disord. 2017, 223, 106–114. [Google Scholar] [CrossRef]
- Koch, K.; Reeß, T.J.; Rus, O.G.; Gürsel, D.A.; Wagner, G.; Berberich, G. , et al. Increased Default Mode Network Connectivity in Obsessive-Compulsive Disorder During Reward Processing. Front Psychiatry. 2018, 9, 254. [Google Scholar] [CrossRef]
- Hein, T.P.; Gong, Z.; Ivanova, M.; Fedele, T.; Nikulin, V.; Herrojo Ruiz, M. Anterior cingulate and medial prefrontal cortex oscillations underlie learning alterations in trait anxiety in humans. Commun Biol. 2023, 6, 271. [Google Scholar] [CrossRef]
- Koçak, O.M.; Kale, E.; Çiçek, M. Default Mode Network Connectivity Differences in Obsessive-compulsive Disorder. Activitas Nervosa Superior. 2012, 54, 118–124. [Google Scholar] [CrossRef]
- Boedhoe, P.S.W.; Schmaal, L.; Abe, Y.; Alonso, P.; Ameis, S.H.; Anticevic, A. , et al. Cortical Abnormalities Associated With Pediatric and Adult Obsessive-Compulsive Disorder: Findings From the ENIGMA Obsessive-Compulsive Disorder Working Group. Am J Psychiatry. 2018, 175, 453–462. [Google Scholar] [CrossRef]
- Zhang, X.; Zhou, J.; Chen, Y.; Guo, L.; Yang, Z.; Robbins, T.W. , et al. Pathological Networking of Gray Matter Dendritic Density With Classic Brain Morphometries in OCD. JAMA Netw Open. 2023, 6, e2343208. [Google Scholar] [CrossRef]
- O'Connor, K.; Aardema, F. Fusion or confusion in obsessive compulsive disorder. Psychol Rep. 2003, 93, 227–232. [Google Scholar] [CrossRef] [PubMed]
- D'Urso, G.; Brunoni, A.R.; Mazzaferro, M.P.; Anastasia, A.; de Bartolomeis, A.; Mantovani, A. Transcranial direct current stimulation for obsessive-compulsive disorder: A randomized, controlled, partial crossover trial. Depress Anxiety. 2016, 33, 1132–1140. [Google Scholar] [CrossRef] [PubMed]
- Harika-Germaneau, G.; Heit, D.; Chatard, A.; Thirioux, B.; Langbour, N.; Jaafari, N. Treating refractory obsessive-compulsive disorder with transcranial direct current stimulation: An open label study. Brain Behav. 2020, 10, e01648. [Google Scholar] [CrossRef] [PubMed]
- Gowda, S.M.; Narayanaswamy, J.C.; Hazari, N.; Bose, A.; Chhabra, H.; Balachander, S. , et al. Efficacy of pre-supplementary motor area transcranial direct current stimulation for treatment resistant obsessive compulsive disorder: A randomized, double blinded, sham controlled trial. Brain Stimul. 2019, 12, 922–929. [Google Scholar] [CrossRef] [PubMed]
- Ardolino, G.; Bossi, B.; Barbieri, S.; Priori, A. Non-synaptic mechanisms underlie the after-effects of cathodal transcutaneous direct current stimulation of the human brain. J Physiol. 2005, 568, 653–663. [Google Scholar] [CrossRef]
Figure 1.
3D representations of electric field simulation for different montages of tDCS with a current intensity of 2mA: (A) cerebellum-OFC tDCS (anode over the right cerelellum and cathode over the left OFC), (B) pre-SMA tDCS (cathode over the bilateral pre-SMA and reference electrode over the lateral surface of the right deltoid), and (C) OFC-pre-SMA tDCS (the first cathode over the pre-SMA, the second cathode over left OFC, and the reference electrode over the lateral surface of the right deltoid). The computational models of cortical electric fields were estimated using HD-Explore® software (Soterix Medical, New York, NY, USA), which utilizes a finite element model of brain current flow based on an MRI-derived MNI 152 template head. OFC, the orbitofrontal cortex; pre-SMA, presupplementary motor area.
Figure 1.
3D representations of electric field simulation for different montages of tDCS with a current intensity of 2mA: (A) cerebellum-OFC tDCS (anode over the right cerelellum and cathode over the left OFC), (B) pre-SMA tDCS (cathode over the bilateral pre-SMA and reference electrode over the lateral surface of the right deltoid), and (C) OFC-pre-SMA tDCS (the first cathode over the pre-SMA, the second cathode over left OFC, and the reference electrode over the lateral surface of the right deltoid). The computational models of cortical electric fields were estimated using HD-Explore® software (Soterix Medical, New York, NY, USA), which utilizes a finite element model of brain current flow based on an MRI-derived MNI 152 template head. OFC, the orbitofrontal cortex; pre-SMA, presupplementary motor area.
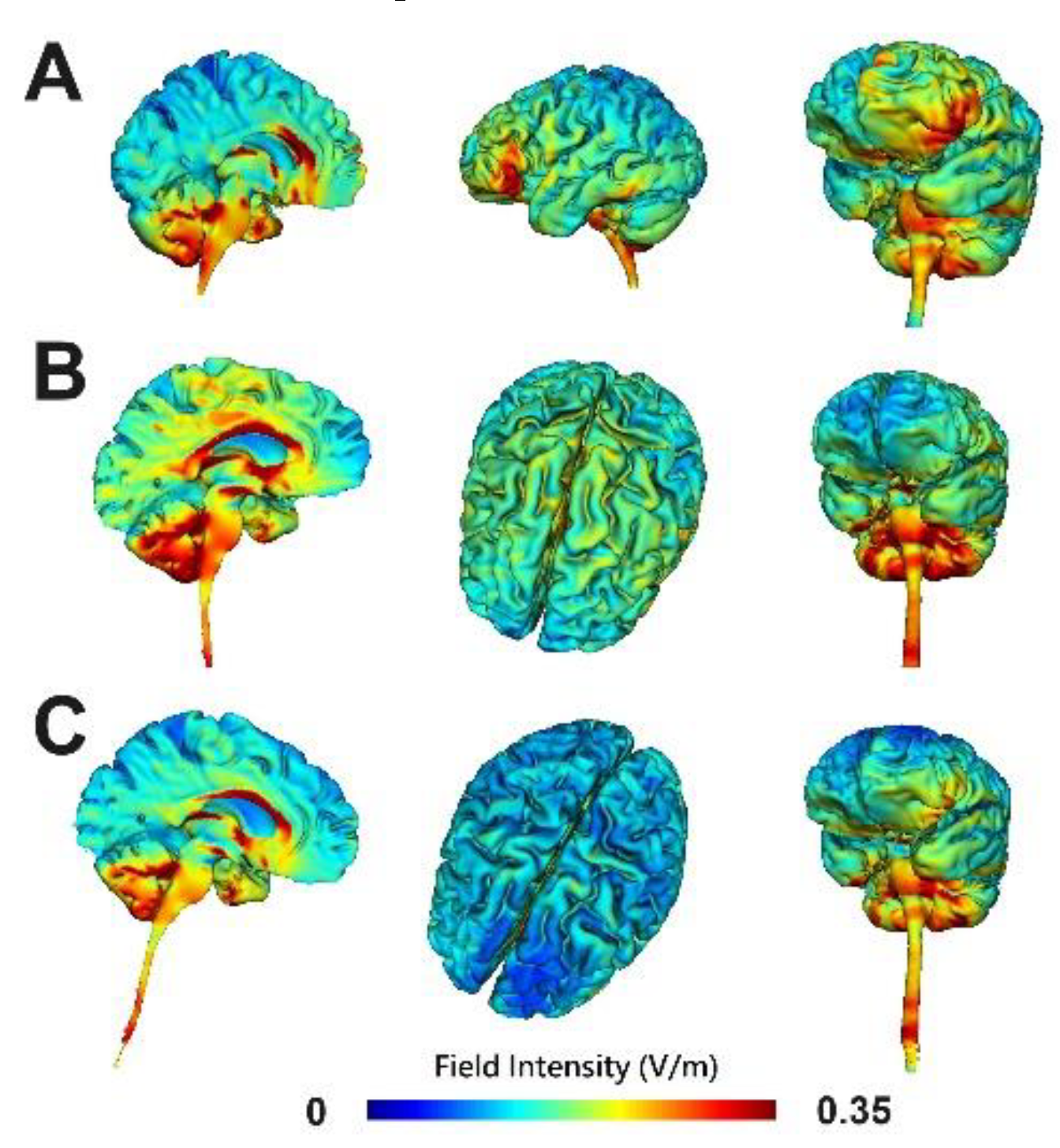
Figure 2.
Timeline for treatment and assessments. Abbreviations: D, day; tDCS, transcranial direct current stimulation; Y-BOCS, Yale-Brown Obsessive Compulsive Scale; OCD-VAS, Obsessive-Compulsive Disorder Visual Analog Scale; HAM-D, Hamilton Depression Rating Scale; HAM-A, Hamilton Anxiety Rating Scale; WHOQOL-BREF, World Health Organization Quality of Life-BREF; CTT, Color Trails Test; SCWT, Stroop Color Word Test; CPT-II, Connors’ Continuous Performance Test –2nd Edition; TOL, Tower of London-Drexel University Test 2nd Edition (TOLDXtm); DSST, Digit Symbol Substitution Test; HRV, heart rate variability; EEG, Electroencephalography.
Figure 2.
Timeline for treatment and assessments. Abbreviations: D, day; tDCS, transcranial direct current stimulation; Y-BOCS, Yale-Brown Obsessive Compulsive Scale; OCD-VAS, Obsessive-Compulsive Disorder Visual Analog Scale; HAM-D, Hamilton Depression Rating Scale; HAM-A, Hamilton Anxiety Rating Scale; WHOQOL-BREF, World Health Organization Quality of Life-BREF; CTT, Color Trails Test; SCWT, Stroop Color Word Test; CPT-II, Connors’ Continuous Performance Test –2nd Edition; TOL, Tower of London-Drexel University Test 2nd Edition (TOLDXtm); DSST, Digit Symbol Substitution Test; HRV, heart rate variability; EEG, Electroencephalography.
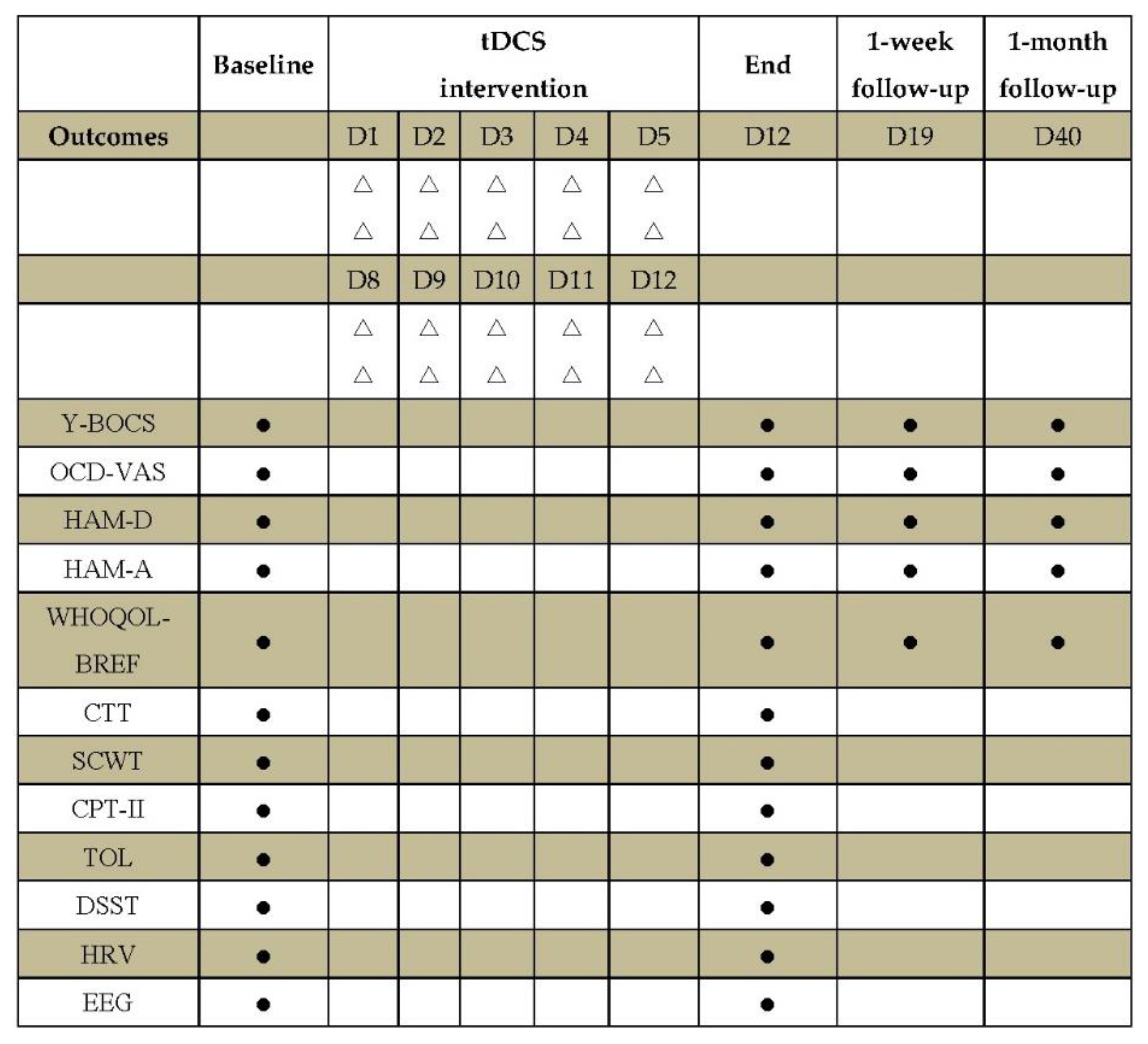
Figure 3.
This is a figure. Schemes follow the same formatting.
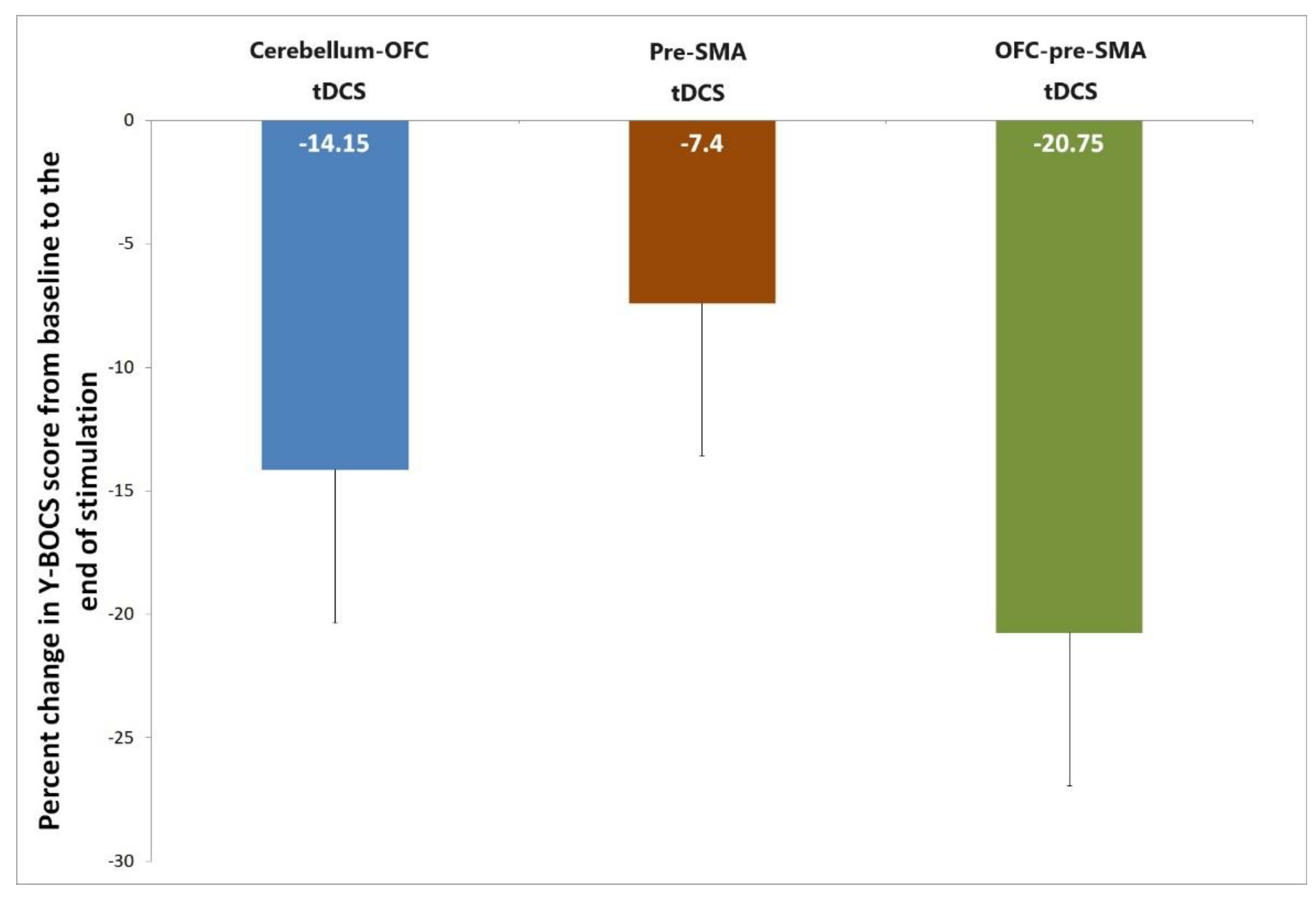
Figure 4.
(A) The cerebellum-OFC tDCS (anode over the right cerelellum and cathode over the left OFC) group had significant decreases in beta-1 band (12-20Hz) nonlinear lagged coherence within the default mode network (DMN) from baseline to the end of stimulation, specifically between the anterior cingulate cortex (ACC) and right inferior parietal lobule (IPL). (B) The OFC-pre-SMA tDCS (the first cathode over the pre-SMA, the second cathode over left OFC, and the reference electrode over the lateral surface of the right deltoid) group had significant increases in beta-2 band (20-30Hz) nonlinear lagged coherence within the frontal network (FN) from baseline to the end of stimulation, specifically between the right and left superior frontal gyrus (SFG). The figure was created using eLORETA and BrainNet Viewer. Error bars indicated standard deviations.
Figure 4.
(A) The cerebellum-OFC tDCS (anode over the right cerelellum and cathode over the left OFC) group had significant decreases in beta-1 band (12-20Hz) nonlinear lagged coherence within the default mode network (DMN) from baseline to the end of stimulation, specifically between the anterior cingulate cortex (ACC) and right inferior parietal lobule (IPL). (B) The OFC-pre-SMA tDCS (the first cathode over the pre-SMA, the second cathode over left OFC, and the reference electrode over the lateral surface of the right deltoid) group had significant increases in beta-2 band (20-30Hz) nonlinear lagged coherence within the frontal network (FN) from baseline to the end of stimulation, specifically between the right and left superior frontal gyrus (SFG). The figure was created using eLORETA and BrainNet Viewer. Error bars indicated standard deviations.
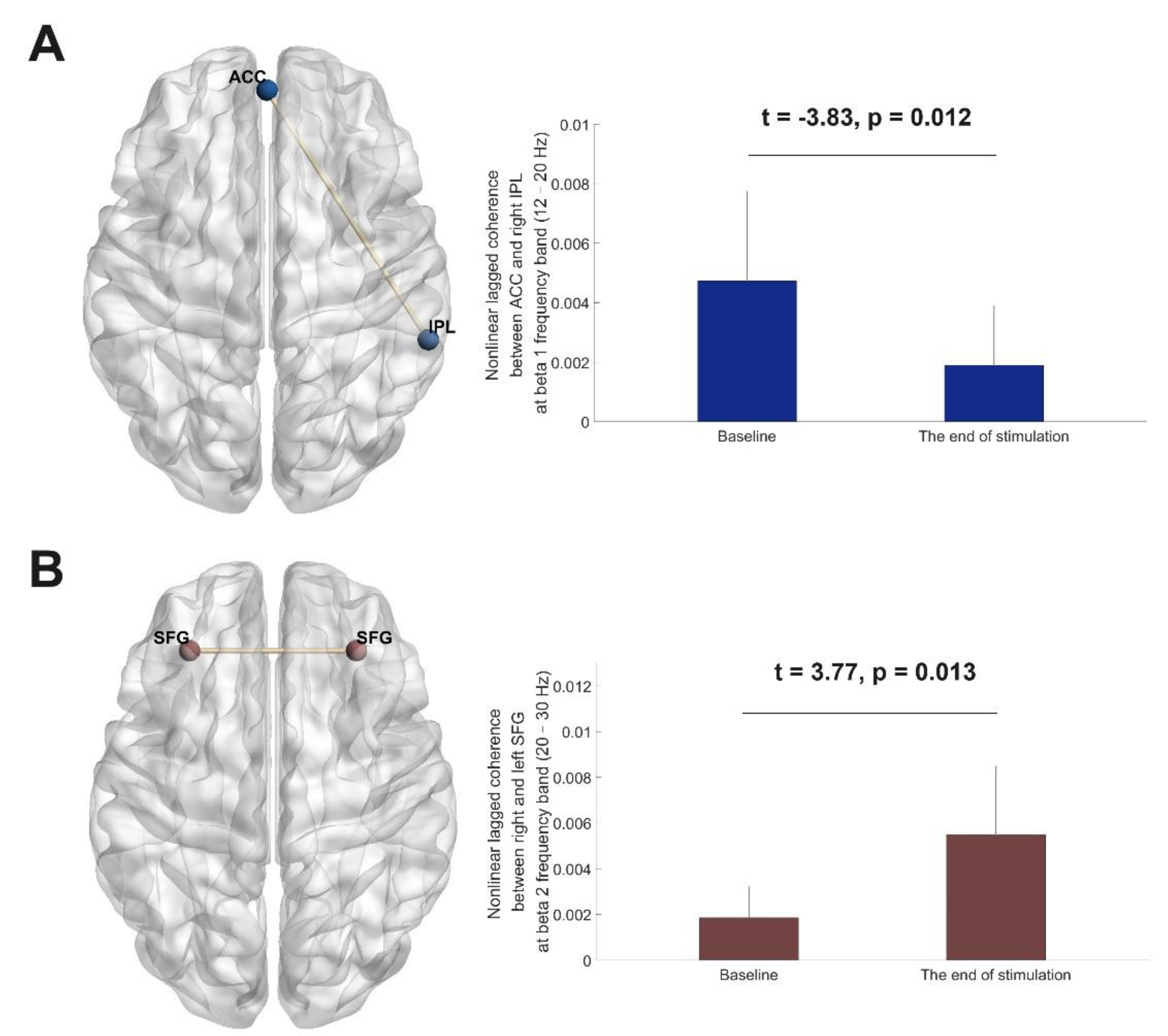
Table 1.
Sample characteristics at baseline.
| Variables | cerebellum-OFC tDCS | pre-SMA tDCS | OFC-pre-SMA tDCS | P value |
|---|---|---|---|---|
| Numbers | 6 | 6 | 6 | |
| Females (%) | 2(33.30%) | 1(16.70%) | 2(33.30%) | 0.76 |
| Age, years | 37.67±11.84 | 35.83±13.32 | 30.67±9.20 | 0.57 |
| Education level, years | 15.00±1.10 | 14.83±2.04 | 15.33±3.72 | 0.94 |
| Handedness(right-left) | 0/6 | 2/4 | 0/6 | 0.11 |
| Length of illness, years | 18.67±12.47 | 16.17±11.20 | 13.83±7.19 | 0.73 |
| Current pharmacological treatment | 0.55 | |||
| Monotherapy with SSRI or clomipramine, or combination of SSRI and clomipramine | 2 (33.30%) | 2 (33.30%) | 3 (50.0%) | |
| SSRI or clomipramine | ||||
| augmented with an antipsychotic | 2 (33.30%) | 4 (66.70%) | 3 (50.0%) | |
| Combination of SSRI and SNRI | 1 (16.70%) | 0 | 0 | |
| Combination of SSRI and NDRI | 1 (16.70%) | 0 | 0 | |
| Y-BOCS | 31.67±5.47 | 28.67±6.74 | 26.00±4.52 | 0.25 |
| OCD-VAS | 2.62±2.06 | 3.67±1.51 | 2.58±1.02 | 0.43 |
| HAMD | 10.67±7.45 | 9.00±5.10 | 7.00±4.38 | 0.56 |
| HAMA | 10.67±6.41 | 8.00±4.43 | 11.67±8.57 | 0.63 |
| WHOQOL-BREF | ||||
| Physical health | 18.83±2.64 | 18.17±2.99 | 17.17±3.31 | 0.63 |
| Psychology | 17.00±2.19 | 14.83±2.23 | 13.83±2.48 | 0.08 |
| Social relationships | 10.67±1.37 | 10.17±1.33 | 9.67±3.88 | 0.79 |
| Environment | 28.17±2.04 | 30.00±4.98 | 28.33±6.80 | 0.79 |
| TOL accuracy | 4.50±1.87 | 3.17±2.64 | 2.83±1.33 | 0.35 |
| TOL time | 233.17±52.97 | 240.67±77.59 | 233.67±88.17 | 0.98 |
| TOL score | 1.00±1.67 | 0.33±0.52 | 0.50±0.55 | 0.54 |
| DSST | 2.50±2.17 | 3.17±4.26 | 1.50±2.74 | 0.51 |
| CTT Color 1 time | 45.64±11.30 | 38.61±14.50 | 40.41±9.23 | 0.58 |
| CTT Color 2 time | 97.49±40.00 | 91.88±22.05 | 80.52±15.14 | 0.57 |
| CPT-II HRT | 434.70±56.06 | 401.84±68.95 | 383.78±78.38 | 0.45 |
| CPT-II Var | 11.56±11.77 | 8.12±6.37 | 6.82±2.26 | 0.57 |
| CPT-II d’ | 0.55±0.25 | 0.49±0.39 | 0.58±0.52 | 0.92 |
| SCWT Naming interference tendency | 0.16±0.15 | 0.44±0.34 | 0.31±0.35 | 0.28 |
| SCWT Reading interference tendency | 0.22±0.15 | 0.44±0.5 | 0.12±0.05 | 0.21 |
tDCS, transcranial direct current stimulation; SSRI, selective serotonin reuptake inhibitors; SNRI, serotonin and norepinephrine reuptake inhibitors; NDRI, norepinephrine and dopamine reuptake inhibitors; Y-BOCS, Yale-Brown Obsessive Compulsive Scale; OCD-VAS, Obsessive-Compulsive Disorder Visual Analog Scale; HAM-D, Hamilton Depression Rating Scale; HAM-A, Hamilton Anxiety Rating Scale; WHOQOL-BREF, World Health Organization Quality of Life-BREF; TOL, The Tower of London-Drexel University Test 2nd Edition (TOLDXtm); DSST, Digit Symbol Substitution Test; CTT, Color Trails Test; CPT-II, Connors’ Continuous Performance Test–2nd Edition; d’, detection; HRT, hit reaction time; VAR, variability; SCWT, Stroop Color Word Test; HF-HRV, high frequency power of heart rate variability [ln(ms2)].
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



