Submitted:
29 October 2024
Posted:
30 October 2024
You are already at the latest version
Abstract
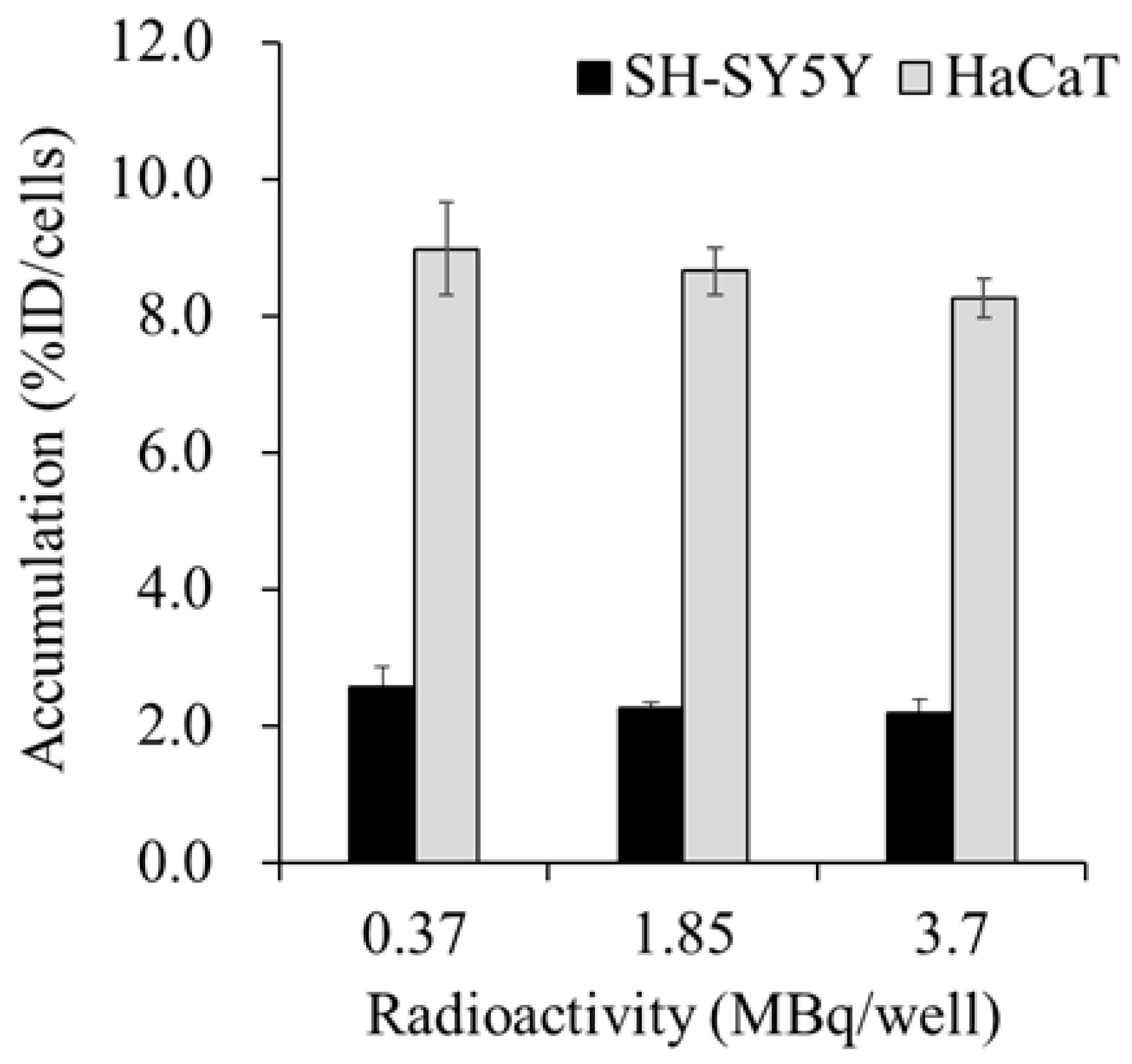
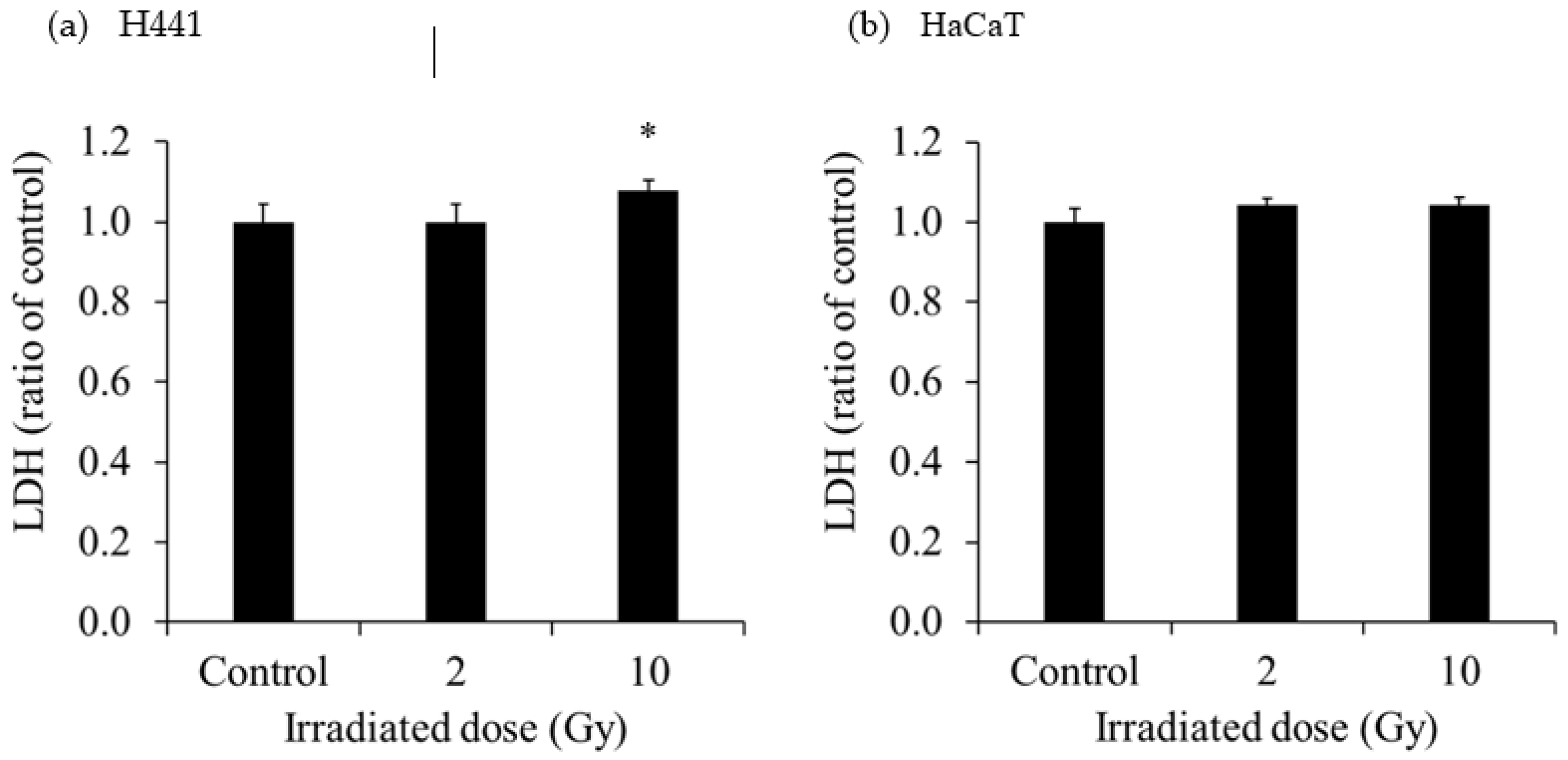
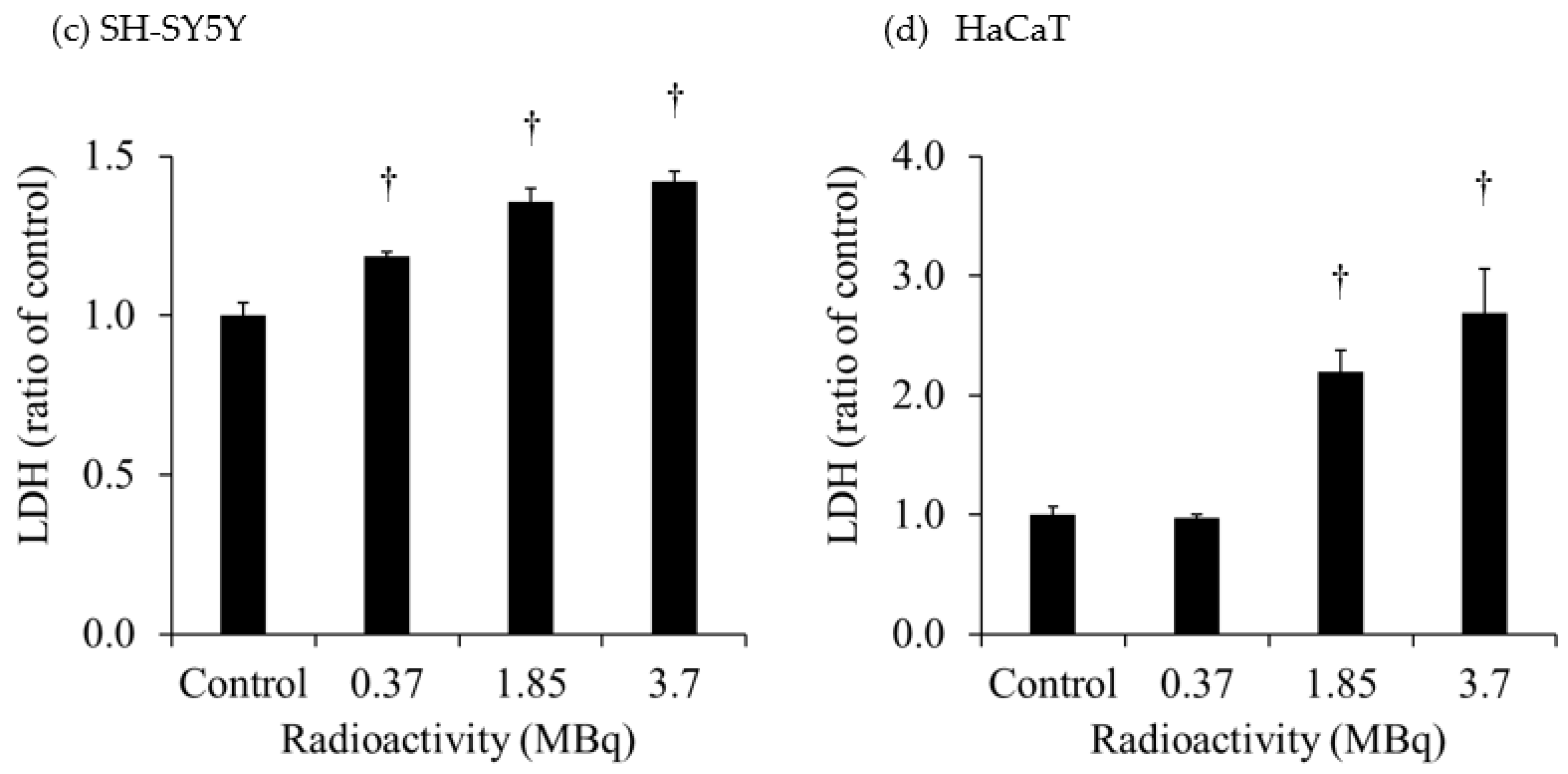
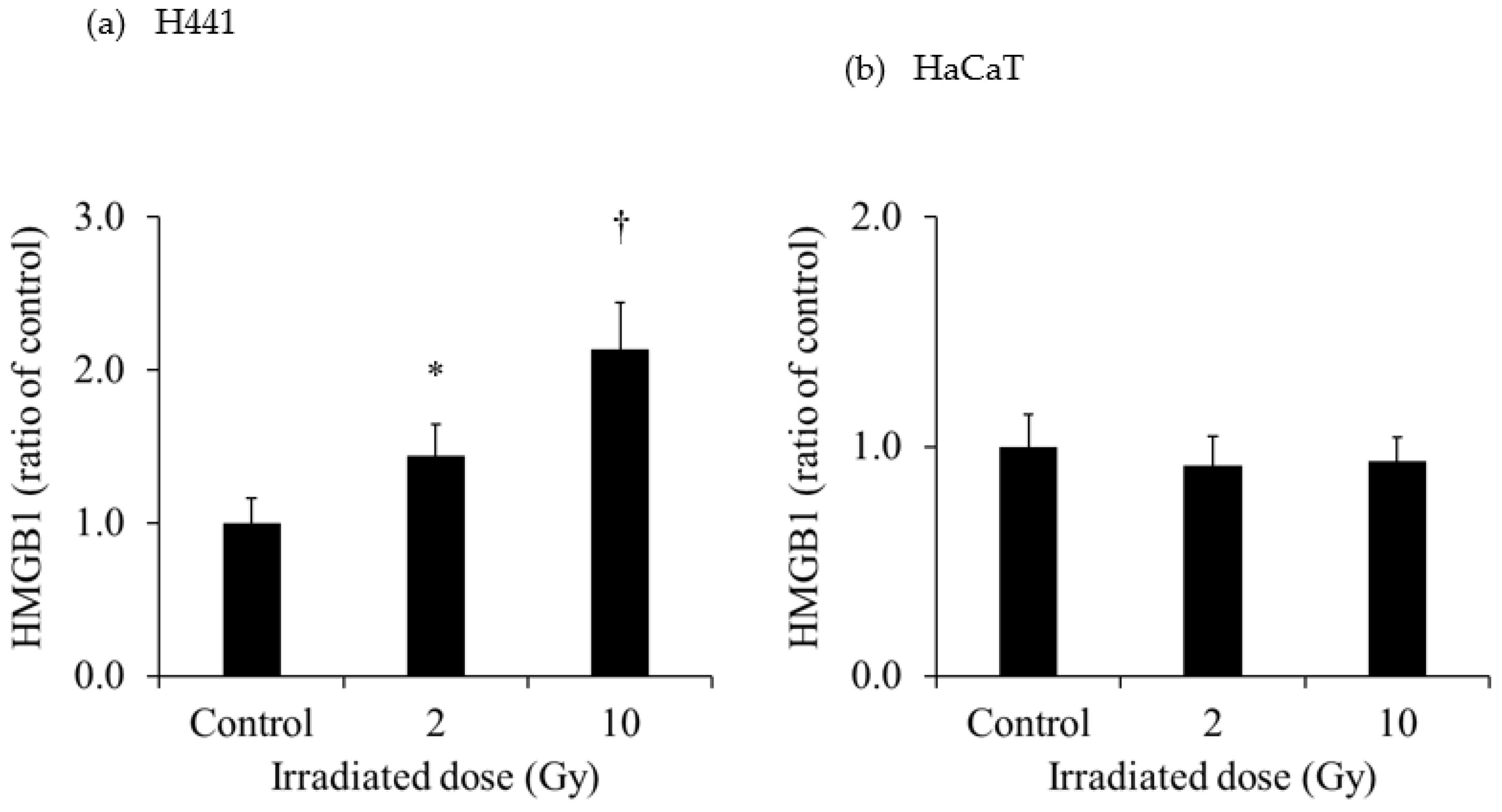
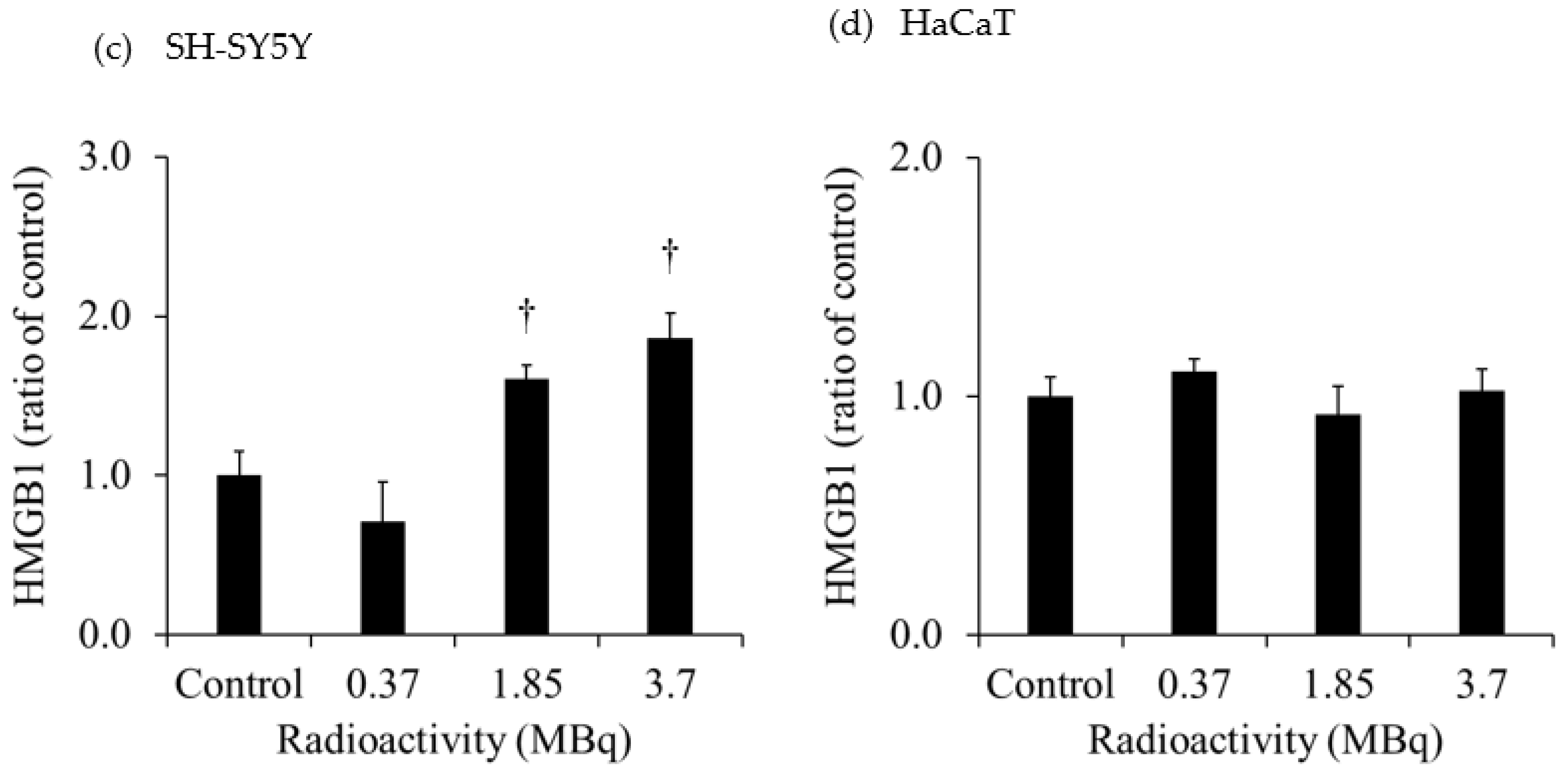
The rare abscopal effect during radiotherapy is thought to be caused by the release of immune-stimulated damage-associated molecular patterns, such as high mobility group box-1 protein (HMGB1), from cancer cells. Although external irradiation of cancer cells increases HMGB1 release, it is not clear if HMGB1 is released from cells after administering 131I-labeled m-iodobenzylguanidine (131I-MIBG) as an internal targeted radiotherapeutic agent. This study aimed to determine if HMGB1 is released from human-derived cancer and normal cells after administering 131I-MIBG. Methods: Extracellular lactate dehydrogenase (LDH) and HMGB1 released from H441 (human-derived lung adenocarcinoma cell line) and HaCaT (human keratinocyte cell line) 1 day after 2- and 10-Gy X-ray irradiation were measured. Accumulations of 131I-MIBG in SH-SY5Y (human-derived neuroblastoma cell line) and HaCaT were measured 60 min after administering 131I-MIBG (0.37, 1.85, 3.7 MBq/well). Extracellular LDH and HMGB1 released from SH-SY5Y and HaCaT 1 day after administering 131I-MIBG were also measured. Results: The extracellular LDH and HMGB1 released from H441 after 10-Gy X-ray irradiation were significantly increased. However, the extracellular LDH and HMGB1 released from HaCaT after 2-Gy and 10-Gy X-ray irradiation were not increased. After administering 1.85 MBq and 3.7 MBq 131I-MIBG, the extracellular LDH and HMGB1 released from SH-SY5Y were both significantly increased, but only the extracellular LDH released from HaCaT was significantly increased. Conclusions: HMGB1 was released from neuroblastomas but not from normal cells after 131I-MIBG administration, suggesting that a combination of 131I-MIBG and immunotherapy may be feasible.
Keywords:
1. Introduction
2. Materials and Methods
2.1. Cancer Cell Lines
2.2. X-Ray Irradiation of H441 and HaCaT
2.3. Administration and Accumulation of 131I-MIBG in SH-SY5Y and HaCaT Cells
2.4. Lactate Dehydrogenase (LDH) Assay
2.5. HMGB1 Assay
2.6. Statistical Analysis
3. Results
4. Discussion
5. Conclusion
Author Contributions
Funding
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Brix, N.; Tiefenthaller, A.; Anders, H.; Belka, C.; Lauber, K. Abscopal, immunological effects of radiotherapy: Narrowing the gap between clinical and preclinical experiences. Immunol Rev 2017, 280, 249–279. [Google Scholar] [CrossRef]
- Nelson, B.E.; Adashek, J.J.; Lin, S.H.; Subbiah, V. The abscopal effect in patients with cancer receiving immunotherapy. Medicine 2023, 4, 233–244. [Google Scholar] [CrossRef]
- Ashrafizadeh, M.; Farhood, B.; Eleojo Musa, A.; Taeb, S.; Najafi, M. Damage-associated molecular patterns in tumor radiotherapy. Int Immunopharmacol 2020, 86, 106761. [Google Scholar] [CrossRef]
- Pol, J.; Vacchelli, E.; Aranda, F.; Castoldi, F.; Eggermont, A.; Cremer, I.; Sautès-Fridman, C.; Fucikova, J.; Galon, J.; Spisek, R.; Tartour, E.; Zitvogel, L.; Kroemer, G.; Galluzzi, L. Trial watch: Immunogenic cell death inducers for anticancer chemotherapy. Oncoimmunology 2015, 4, e1008866. [Google Scholar] [CrossRef]
- Krysko, D.V.; Garg, A.D.; Kaczmarek, A.; Krysko, O.; Agostinis, P.; Vandenabeele, P. Immunogenic cell death and DAMPs in cancer therapy. Nat Rev Cancer 2012, 12, 860–875. [Google Scholar] [CrossRef]
- Horner, E.; Lord, J.M.; Hazeldine, J. The immune suppressive properties of damage associated molecular patterns in the setting of sterile traumatic injury. Front Immunol 2023, 14, 1239683. [Google Scholar] [CrossRef]
- Wang, X.; Ji, J.; Zhang, H.; Fan, Z.; Zhang, L.; Shi, L.; Zhou, F.; Chen, W.R.; Wang, H.; Wang, X. Stimulation of dendritic cells by DAMPs in ALA-PDT treated SCC tumor cells. Oncotarget 2015, 6, 44688–44702. [Google Scholar] [CrossRef]
- Cha, J.H.; Chan, L.C.; Li, C.W.; Hsu, J.L.; Hung, M.C. Mechanisms controlling PD-L1 expression in cancer. Mol Cell 2019, 76, 359–370. [Google Scholar] [CrossRef]
- Malmberg, R.; Zietse, M.; Dumoulin, D.W.; Hendrikx, J.J.M.A.; Aerts, J.G.J.V.; van der Veldt, A.A.M.; Koch, B.C.P.; Sleijfer, S.; van Leeuwen, R.W.F. Alternative dosing strategies for immune checkpoint inhibitors to improve cost-effectiveness: a special focus on nivolumab and pembrolizumab. Lancet Oncol 2022, 23, e552–e561. [Google Scholar] [CrossRef]
- Muñoz-Unceta, N.; Burgueño, I.; Jiménez, E.; Paz-Ares, L. Durvalumab in NSCLC: Latest evidence and clinical potential. Ther Adv Med Oncol 2018, 10, 1758835918804151. [Google Scholar] [CrossRef]
- Ahmed, A.; Tait, S.W.G. Targeting immunogenic cell death in cancer. Mol Oncol 2020, 14, 2994–3006. [Google Scholar] [CrossRef] [PubMed]
- Janho Dit Hreich, S.; Benzaquen, J.; Hofman, P.; Vouret-Craviari, V. To inhibit or to boost the ATP/P2RX7 pathway to fight cancer—that is the question. Purinergic Signal 2021, 17, 619–631. [Google Scholar] [CrossRef] [PubMed]
- Krysko, D.V.; Garg, A.D.; Kaczmarek, A.; Krysko, O.; Agostinis, P.; Vandenabeele, P. Immunogenic cell death and DAMPs in cancer therapy. Nat Rev Cancer 2012, 12, 860–875. [Google Scholar] [CrossRef] [PubMed]
- Sims, G.P.; Rowe, D.C.; Rietdijk, S.T.; Herbst, R.; Coyle, A.J. HMGB1 and RAGE in Inflammation and Cancer. Annu Rev Immunol 2010, 28, 367–388. [Google Scholar] [CrossRef]
- Schildkopf, P.; Frey, B.; Mantel, F.; Ott, O.J.; Weiss, E.M.; Sieber, R.; Janko, C.; Sauer, R.; Fietkau, R.; Gaipl, U.S. Application of hyperthermia in addition to ionizing irradiation fosters necrotic cell death and HMGB1 release of colorectal tumor cells. Biochem Biophys Res Commun 2010, 391, 1014–1020. [Google Scholar] [CrossRef]
- Dashnamoorthy, S.; Jeyasingh, E.; Rajamanickam, K. Validation of esophageal cancer treatment methods from 3D-CRT, IMRT, and Rapid Arc plans using custom Python software to compare radiobiological plans to normal tissue integral dosage. Rep Pract Oncol Radiother 2023, 28, 54–65. [Google Scholar] [CrossRef]
- López Alfonso, J.C.; Parsai, S.; Joshi, N.; Godley, A.; Shah, C.; Koyfman, S.A.; Caudell, J.J.; Fuller, C.D.; Enderling, H.; Scott, J.G. Temporally feathered intensity-modulated radiation therapy: A planning technique to reduce normal tissue toxicity. Med Phys 2018, 45, 3466–3477. [Google Scholar] [CrossRef]
- Wang, J.; Xie, K.H.; Ren, W.; Han, R.Y.; Xiao, L.H.; Yu, J.; Tan, R.Z.; Wang, L.; Liao, D.Z. Huanglian Jiedu plaster ameliorated X-ray-induced radiation dermatitis injury by inhibiting HMGB1-mediated macrophage-inflammatory interaction. J Ethnopharmacol 2023, 302, 115917. [Google Scholar] [CrossRef]
- Sgouros, G.; Bodei, L.; McDevitt, M.R.; Nedrow, J.R. Radiopharmaceutical therapy in cancer: clinical advances and challenges. Nat Rev Drug Discov 2020, 19, 589–608. [Google Scholar] [CrossRef]
- Bellavia, M.C.; Patel, R.B.; Anderson, C.J. Combined. targeted radiopharmaceutical therapy and immune checkpoint blockade: From preclinical advances to the clinic. J Nucl Med 2022, 63, 1636–1641. [Google Scholar] [CrossRef]
- DuBois, S.G.; Matthay, K.K. Radiolabeled metaiodobenzylguanidine for the treatment of neuroblastoma. Nucl Med Biol 2008, Suppl 1, S35–S48. [Google Scholar] [CrossRef]
- Wilson, J.S.; Gains, J.E.; Moroz, V.; Wheatley, K.; Gaze, M.N. A systematic review of 131I-meta iodobenzylguanidine molecular radiotherapy for neuroblastoma. Eur J Cancer 2014, 50, 801–815. [Google Scholar] [CrossRef]
- Feng, L.; Li, S.; Wang, C.; Yang, J. Current status and future perspective on molecular imaging and treatment of neuroblastoma. Semin Nucl Med 2023, 53, 517–529. [Google Scholar] [CrossRef]
- Vinod, S.K.; Hau, E. Radiotherapy treatment for lung cancer: Current status and future directions. Respirology 2020, 25, 61–71. [Google Scholar] [CrossRef]
- Boukamp, P.; Petrussevska, R.T.; Breitkreutz, D.; Hornung, J.; Markham, A.; Fusenig, N.E. Normal keratinization in a spontaneously immortalized aneuploid human keratinocyte cell line. J Cell Biol 1988, 106, 761–771. [Google Scholar] [CrossRef]
- Sarudis, S.; Karlsson, A.; Bäck, A. Surface guided frameless positioning for lung stereotactic body radiation therapy. J Appl Clin Med Phys 2021, 22, 215–226. [Google Scholar] [CrossRef]
- Hamilton, T.; Zhang, J.; Wolf, J.; Kayode, O.; Higgins, K.A.; Bradley, J.; Yang, X.; Schreibmann, E.; Roper, J. Lung SBRT treatment planning: a study of VMAT arc selection guided by collision check software. Med Dosim 2023, 48, 82–89. [Google Scholar] [CrossRef]
- Donovan, E.K.; Swaminath, A. Stereotactic body radiation therapy (SBRT) in the management of non-small-cell lung cancer: Clinical impact and patient perspectives. Lung Cancer 2018, 9, 13–23. [Google Scholar] [CrossRef]
- Feng, Y.; Xiong, Y.; Qiao, T.; Li, X.; Jia, L.; Han, Y. Lactate dehydrogenase A: A key player in carcinogenesis and potential target in cancer therapy. Cancer Med 2018, 7, 6124–6136. [Google Scholar] [CrossRef]
- Schneider, K.S.; Groß, C.J.; Dreier, R.F.; Saller, B.S.; Mishra, R.; Gorka, O.; Heilig, R.; Meunier, E.; Dick, M.S.; Ćiković, T.; Sodenkamp, J.; Médard, G.; Naumann, R.; Ruland, J.; Kuster, B.; Broz, P.; Groß, O. The inflammasome drives GSDMD-independent secondary pyroptosis and IL-1 release in the absence of caspase-1 protease activity. Cell Rep 2017, 21, 3846–3859. [Google Scholar] [CrossRef]
- Pandit-Taskar., N.; Modak, S. Pandit-Taskar. N.; Modak, S. Norepinephrine transporter as a target for imaging and therapy. J Nucl Med 2017, 58, 39S–53S. [Google Scholar] [CrossRef] [PubMed]
- Kobayashi, M.; Mizutani, A.; Muranaka, Y.; Nishi, K.; Komori, H.; Nishii, R.; Shikano, N.; Nakanishi, T.; Tamai, I.; Kawai, K. Biological distribution of orally administered [123I]MIBG for estimating gastrointestinal tract absorption. Pharmaceutics 2021, 14, 61. [Google Scholar] [CrossRef] [PubMed]
- Kobayashi, M.; Mizutani, A.; Nishi, K.; Muranaka, Y.; Nishii, R.; Shikano, N.; Nakanishi, T.; Tamai, I.; Kleinerman, E.S.; Kawai, K. [131I]MIBG exports via MRP transporters and inhibition of the MRP transporters improves accumulation of [131I]MIBG in neuroblastoma. Nucl Med Biol 2020, 90–91, 49–54. [Google Scholar] [CrossRef] [PubMed]
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).



