
Submitted:
25 October 2024
Posted:
29 October 2024
You are already at the latest version
Abstract
Background: Anorectal malformations (ARMs) are often associated with tethered cord syndrome (TCS). This study focused on children with ARM to explore the risk factors for the co-occurrence of TCS and to investigate the impact of untethering surgery on anorectal function among these children.
Methods: A retrospective analysis was conducted on 130 children with ARM treated at Fujian Provincial Children's Hospital (Fujian Hospital of Shanghai Children's Medical Center) from May 2021 to January 2024. A total of 114 children were included in the study on the basis of the inclusion and exclusion criteria. The patients were divided into two groups according to the presence of TCS: the ARM group (n=83) and the ARM+TCS group (n=31). to explore the risk factors for the co-occurrence of ARM and TCS. All children diagnosed with TCS underwent untethering surgery regardless of symptoms. Anorectal function was compared between the ARM and ARM+TCS groups.
Results: In the multivariate analysis, intermediate or high-type ARM increased the risk of children with ARM having TCS, with an OR of 3.571, 95% CI from 0.106 to 0.738, and p= 0.010. Additionally, the presence of other malformations also increased the risk of children with ARM having TCS (p=0.026). When the ARM+TCS group was compared with the ARM group, children with low-type ARM in the ARM+TCS group exhibited a significant improvement in constipation following untethering surgery (p=0.043). However, when children with intermediate or high-type ARM were compared, the anorectal function of the children in both groups was comparable.
Conclusions: Intermediate or high-type ARM and the presence of other malformations are risk factors for the co-occurrence of TCS in children with ARM. In children with low-type ARM, those with TCS and ARM showed significant improvement in constipation after untethering surgery compared with those with ARM without TCS. We recommend that children with relevant conditions actively undergo untethering surgery.
Keywords:
Anorectal malformations (ARMs)
; tethered cord syndrome (TCS)
; risk factors
; anorectal function
; children
1. Introduction
Anorectal malformations (ARMs) are a type of congenital disease involving abnormalities of the anus and rectum, with an incidence of 1 in 5,000 to 1 in 2,000. The occurrence of this malformation may be related to genetic factors and environmental factors during pregnancy (such as viral infections, chemical substances, nutritional status, etc.). In addition, the mother’s age, socioeconomic status, and lifestyle may also be associated with the risk of ARM occurrence. This type of malformation usually occurs due to developmental disorders during the embryonic period, resulting in a narrow anal opening, covered by skin or absent [1]. ARMs are often associated with other malformations, with an incidence rate of 28% to 72%, commonly including urogenital, cardiac, and spinal limb malformations [2,3,4]. Between 20% and 60% of ARMs are associated with TCS [5,6]. TCSs are a group of neurological dysfunctions and deformities caused by congenital factors that lead to tethering of the spinal cord or conus, with a wide variety of signs and symptoms, such as scoliosis, lower back pain, difficulty walking, leg weakness, and bowel and bladder dysfunction. The natural history of untreated children is often characterized by a worsening of neurological function with age, and untethering surgery can often halt clinical deterioration and may reverse it [7,8]. TCS is also a congenital disease, and by linking these two conditions, we can see that they both involve abnormalities in embryonic development. The ARM and TCS may share certain risk factors, which are currently unknown.
With respect to the treatment of ARM, surgery is the only effective method. However, due to the complex pathological types of ARMs, their postoperative efficacy is often uncertain. After anoplasty, issues such as anal stenosis, rectal mucosal eversion, and anal incontinence may arise, leading to defecation dysfunction [9]. TCS occurs when the spinal cord is abnormally tethered by tissue, limiting its movement. This condition can also lead to bowel control disorders, including constipation or incontinence [8]. TCS requires surgical treatment aimed at untethering the spinal cord, removing the lesion, preventing the progression of the condition and improving neurological function as much as possible. When children have both ARM and TCS, anorectal function after untethering surgery has not been effectively evaluated, and there is controversy over whether to perform untethering surgery [10,11].
This study retrospectively reviewed the medical history, imaging data, and follow-up information of children with ARM treated at Fujian Provincial Children’s Hospital, aiming to explore the risk factors for the comorbidity of TCS. By comparing the postoperative defecation symptoms of the relevant children, this study explored whether untethering surgery could improve the anorectal function of children with ARM combined with TCS, which also provides a basis for the clinical management of children with ARM and TCS.
2. Materials and Methods
2.1 Patients
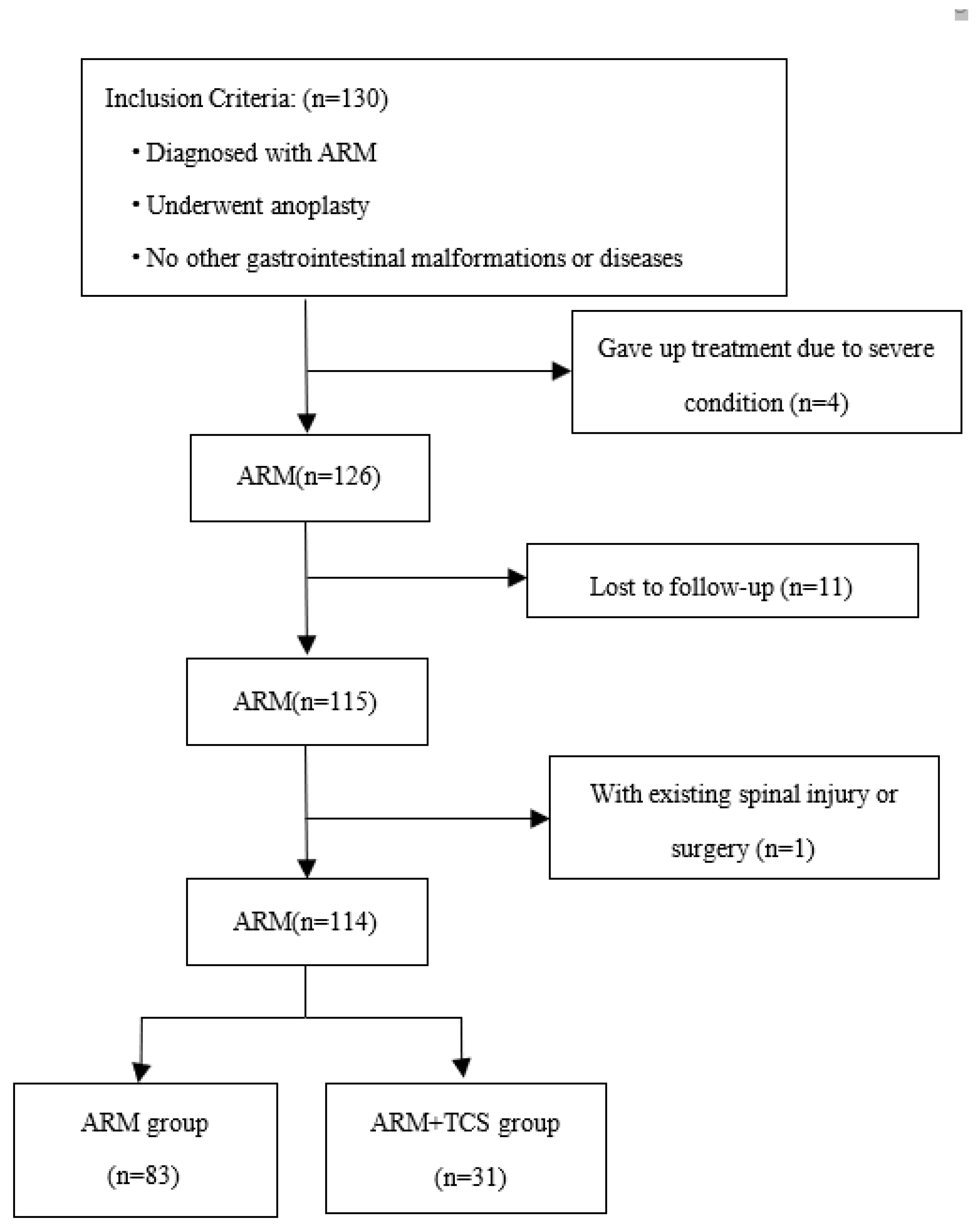
This study was approved by the Medical Ethics Committee of Fujian Provincial Children’s Hospital (No. 2024ETKLRK07005), and all legal guardians of the children signed the informed consent form for this clinical study. This retrospective analysis focused on 130 children with ARM admitted to Fujian Provincial Children’s Hospital (Fujian Hospital of Shanghai Children’s Medical Center) from May 2021 to January 2024. The inclusion criteria for case selection were as follows: ① complete medical history and lumbar sacral MRI examination; ② all children underwent anoplasty; and ③ absence of gastrointestinal structural abnormalities or diseases other than ARM. The exclusion criteria were as follows: ① children who abandoned treatment due to severe illness; ② exclusion of children with a history of spinal cord injury or surgery; and ③ were lost to follow-up. A total of 114 children met the inclusion and exclusion criteria, including 83 children in the ARM group and 31 children in the ARM+TCS group (Figure 1).
2.2 Data Collection
All the data were sourced from the hospital’s big data platform, WeChat platform, and postoperative follow-up. The following information was extracted: (1) Demographic characteristics, including sex, age at surgery, gestational age, and number of pregnancies. (2) Disease information encompassing wing spread classification, Krickenberger classification, TCS type, and the presence of other malformations. (3) Maternal and paternal reproductive history, including parental age at conception, mode of conception, abnormal pregnancy history, history of maternal diseases, labor, active smoking or passive smoking during pregnancy, folic acid supplementation, maternal infection in early pregnancy, and parental education level. All the children were followed up at least half a year after anoplasty and 3 months after untethering surgery, and bowel movement symptoms, which included constipation, soiling, and voluntary bowel movement, were assessed via the Krickenbeck clinical scoring system. Voluntary bowel movement ability was only recorded if the child met all three conditions: feeling of urge, capacity to verbalize, and ability to hold stools.
All pediatric patients underwent lumbosacral 3.0T magnetic resonance imaging (MRI) scans with adequate sedation prior to examination. The images collected included axial, sagittal, and coronal T1-weighted imaging (T1WI) and T2-weighted imaging (T2WI) of the lumbosacral region. The assessments and reports were made by senior pediatric neuroradiologists to determine the presence of TCS. The types of TCS included: spinal lipomas (SLs), spinal diastematomyelia, meningocele, myelomeningocele, lipomyelomeningocele, meningomyelocele, syringomyelia, low conus position (below the T2 level and over 3 months of age), and a thickened filum terminale (greater than 2 mm).
2.2.1 Research Design
Patients were divided into two groups according to the presence or absence of TCS in patients with ARM: the ARM group and the ARM+TCS group. The demographic characteristics, disease information, and maternal pregnancy history of the patients in both groups were collected. Univariate and multivariate analyses were conducted to explore the risk factors for ARM combined with TCS. Although the regularity of ARM combined with TCS has been identified, the impact of untethering surgery on the anorectal function of affected children is unknown. Therefore, we assessed anorectal function in ARM patients with TCS after untethering surgery and compared it with that of ARM patients without TCS.
2.2.2 Statistical analysis
Statistical analysis was performed via SPSS software version 24.0. Categorical variables are represented by frequencies and rates, intergroup comparisons were made using the chi-square test, and ordinal variables were analyzed with the rank sum test. Logistic regression analysis was employed to analyze the risk factors for ARMs combined with TCS. A p value of less than 0.05 (two-tailed) was considered statistically significant.
2.2.3 Results
Risk factors for ARMs associated with TCS
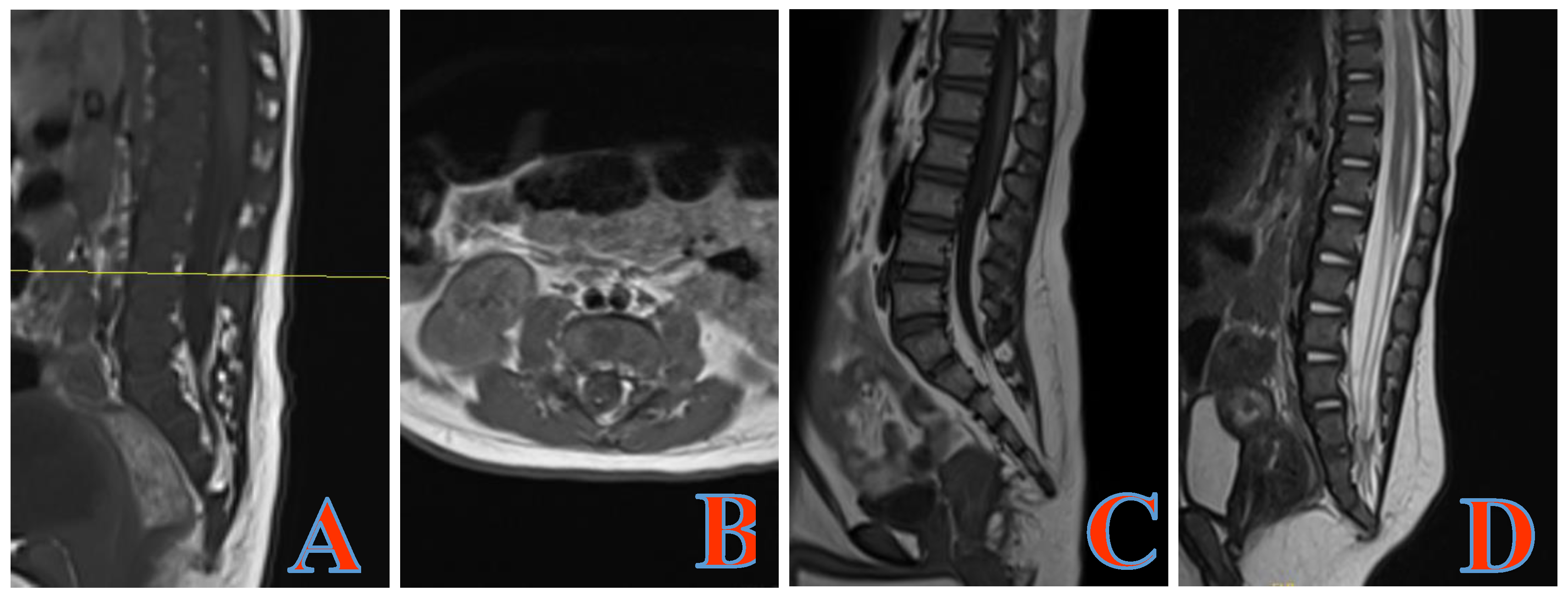
Among 114 children with ARM, 31 cases (27.2%) were associated with TCS, of which 30 cases were SL (4 cases were type III, 26 cases were type IV), and 1 case was syringomyelia (Figure 2).
3. Results
3.1. Risk factors for ARMs associated with TCS
Among 114 children with ARM, 31 cases (27.2%) were associated with TCS, of which 30 cases were SL (4 cases were type III, 26 cases were type IV), and 1 case was syringomyelia (Figure 2). Seventy-five patients (65.79%) had other malformations (including congenital heart disease, urogenital system malformations, skeletal system malformations, Down syndrome, VATER association, etc.), with 47 patients having one additional malformation and 28 patients having two or more additional malformations.
Figure 2.
Type IV SL: The conus medullaris is in a normal position, and there is partial fatty degeneration of the filum terminale, with punctate high signals appearing on the axial T1WI. (A, B) Type III SL: The lipoma is located below the conus medullaris, merging with the subcutaneous fat through the sacral hiatus, and the entire length of the filum terminale has undergone fatty degeneration. (C) The conus medullaris has experienced dilation of the central canal. (D) SL, spinal lipomas; T1WI, T1-weighted images.
Figure 2.
Type IV SL: The conus medullaris is in a normal position, and there is partial fatty degeneration of the filum terminale, with punctate high signals appearing on the axial T1WI. (A, B) Type III SL: The lipoma is located below the conus medullaris, merging with the subcutaneous fat through the sacral hiatus, and the entire length of the filum terminale has undergone fatty degeneration. (C) The conus medullaris has experienced dilation of the central canal. (D) SL, spinal lipomas; T1WI, T1-weighted images.
The results of the univariate analysis affecting the combination of ARM and TCS are as follows (Table 1). Intermediate or high-type ARM and the presence of other malformations are associated with an increased risk of ARM combined with TCS. However, there was no statistically significant difference between the two groups in terms of age, parental reproductive age, maternal nonadherence to folic acid supplementation, history of infection in early pregnancy, abnormal pregnancy history, active smoking or passive smoking history, maternal education level, multiple pregnancy, conception method, labor, gestational age, or history of maternal diseases.
All variables were included in the multivariate analysis. Intermediate or high-type ARM also increased the risk of ARM children having TCS, with an OR of 3.571, 95% CI from 0.106 to 0.738, and a p value of 0.010. Additionally, the presence of other malformations also increases the risk of ARM children having TCS, with a p value of 0.026 (Table 2).

Table 1.
Univariate analysis of risk factors for ARMs combined with TCS.
| Variables | ARM group(n=83) | ARM+TCS group(n=31) | OR | 95% CI | p |
| Sex | |||||
| Female | 32(38.55) | 12(38.71) | 0.332 | (0.072-1.540) | 0.159 |
| Male | 51(61.45) | 19(61.29) | |||
| Maternal age at childbirth (years) | |||||
| <35 | 62(74.70) | 26(83.87) | 1.949 | (0.155-7.334) | 0.545 |
| >=35 | 21(25.30) | 5(16.13) | |||
| Paternal age at childbirth (years) | |||||
| <35 | 51(61.45) | 24(77.42) | 1.065 | (0.155-7.334) | 0.949 |
| >=35 | 32(38.55) | 7(22.58) | |||
| Education level of mother | |||||
| Elementary school | 6(7.23) | 3(9.68) | Ref | Ref | 0.722 |
| Junior high school | 24(28.92) | 9(29.03) | 0.402 | (0.059-2.741) | 0.352 |
| High school | 21(25.30) | 5(16.13) | 0.616 | (0.074-5.117) | 0.654 |
| University or Above | 32(38.55) | 14(45.16) | 0.818 | (0.117-5.725) | 0.839 |
| Active smoking or passive smoking | |||||
| Yes | 22(26.51) | 11(35.48) | 2.431 | (0.737-8.021) | 0.145 |
| No | 61(73.49) | 20(64.52) | |||
| Taking folic acid on time | |||||
| Yes | 34(40.96) | 6(19.35) | 2.640 | (0.679-10.268) | 0.161 |
| No | 49(59.04) | 25(80.65) | |||
| Abnormal pregnancy history | |||||
| Yes | 23(27.71) | 6(19.35) | 0.627 | (0.181-2.175) | 0.462 |
| No | 60(72.29) | 25(80.65) | |||
| Mode of conception | |||||
| Natural | 77(92.77) | 28(90.32) | 0.380 | (0.047-5.117) | 0.365 |
| Assisted | 6(7.23) | 3(9.68) | |||
| Multiple pregnancy | |||||
| Yes | 2(2.41) | 1(3.23) | 1.317 | (0.051-34.285) | 0.869 |
| No | 81(97.59) | 30(96.77) | |||
| Infection in early pregnancy | |||||
| Yes | 17(20.48) | 12(38.71) | 0.379 | (0.102-1.412) | 0.148 |
| No | 66(79.52) | 19(61.29) | |||
| Maternal diseases | |||||
| Yes | 15(18.07) | 4(12.90) | 0.954 | (0.174-5.226) | 0.957 |
| No | 68(81.93) | 27(87.10) | |||
| Gestational age(weeks) | |||||
| <37 | 17(20.48) | 4(12.90) | 0.378 | (0.076-1.875) | 0.234 |
| >=37 | 66(79.52) | 27(87.10) | |||
| Labor |
|||||
| Vaginal birth |
50(60.24) | 19(61.29) | 0.726 | (0.213-2.476) | 0.609 |
| Cesarean section |
33(39.76) | 12(38.71) | |||
| Wingspread classification | |||||
| Low | 66(79.52) | 14(45.16) | 0.117 | (0.029-0.468) | 0.002 |
| Intermediate or high | 17(20.48) | 17(54.84) | |||
| Krickenberger classification | |||||
| Rectourethral fistula | 13(15.66) | 7(22.58) | Ref | Ref | 0.966 |
| Rectovesical fistula | 3(3.61) | 3(9.68) | 0.998 | ||
| Rectovaginal fistula | 2(2.41) | 1(3.23) | 0.998 | ||
| Anal stenosis | 9(10.84) | 3(9.68) | 0.998 | ||
| Perineal fistula | 30(36.14) | 7(22.58) | 0.999 | ||
| Rectourethrovaginal fistula | 25(30.12) | 8(25.81) | 0.999 | ||
| Rectal atresia | 1(1.20) | 2(6.45) | 0.999 | ||
| Presence of other malformations | |||||
| No | 36(43.37) | 3(9.68) | Ref | Ref | 0.014 |
| One type | 32(38.55) | 15(48.39) | 6.528 | (1.571-27.130) | 0.010 |
| Two types or more | 15(18.07) | 13(41.94) | 7.701 | (1.686-35.171) | 0.008 |
The values are presented as numbers and percentages (%). TCS, tethered cord syndrome; ARM, anorectal malformation; OR, odds ratio; CI, confidence interval.
Table 2.
Multivariate analysis of risk factors for ARMs combined with TCS.
| Variables | B | SE | OR | 95% CI | p |
| Wingspread classification | 1.273 | 0.495 | 3.571 | (0.106-0.738) | 0.010 |
| Presence of other malformations | |||||
| No | Ref | Ref | Ref | Ref | 0.026 |
| One type | 1.335 | 0.615 | 3.801 | (1.139-12.688) | 0.030 |
| Two types or more | 1.743 | 0.669 | 5.716 | (1.541-21.210) | 0.009 |
SE, standard error; OR, odds ratio; CI, confidence interval.
3.2 Anorectal function with an ARM combined with TCS after untethering surgery
Patients with low-type ARM underwent one-stage anoplasty, whereas those with intermediate- or high-type ARM underwent a multistage treatment protocol (stage one involves a colostomy of the transverse colon, stage two involves anoplasty, and stage three involves closure of the colostomy). All patients in the ARM+TSC group underwent tethered cord release following surgical treatment of the ARM, with a median age of 29.7 months (ranging from 2 to 120 months) at the time of surgery. One patient with cerebrospinal fluid leakage from the incision site was cured with a pressure dressing. We did not assess preoperative anorectal function, as most patients were too young. In terms of constipation, children in the ARM+TCS group demonstrated significantly better anorectal function than those in the ARM group with low-type ARM (Table 3). When anorectal function was compared between the two groups of children with intermediate or high-type ARM, there was a decrease in the proportion of children with the ability to defecate independently, without constipation or fecal soiling. No statistically significant difference was observed between the two groups (Table 3).
Table 3.
Comparison of defecation symptoms between the two groups with low ARM.
| Variables | ARM group(n=65) | ARM+TCS group (n=14) |
χ2/Z | p |
| Soiling | ||||
| No | 35(53.85) | 9(64.28) | -0.589 | 0.556 |
| Grade 1 once or twice per week | 12(18.46) | 2(14.29) | ||
| Grade 2 Every day, no social problem | 10(15.38) | 1(7.14) | ||
| Grade 3 Constant, social problem | 8(12.31) | 2(14.29) | ||
| Constipation | ||||
| No | 21(32.31) | 9(64.28) | -2.020 | 0.043 |
| Grade 1 Manageable by changes in diet | 19(29.23) | 2(14.29) | ||
| Grade 2 Requires laxatives | 11(16.92) | 2(14.29) | ||
| Grade 3 Resistant to diet and laxatives | 14(21.54) | 1(7.14) | ||
| Voluntary bowel movements | ||||
| No | 22(33.85) | 3(21.43) | 0.821 | 0.365 |
| Feeling of urge、 Capacity to verbalize、Hold defecation | 43(66.15) | 11(78.57) |
The values are presented as numbers and percentages (%). ARM, anorectal malformation; TCS, tethered cord syndrome.
Table 4.
Comparison of defecation symptoms between the two groups with intermediate- or high-type ARM.
Table 4.
Comparison of defecation symptoms between the two groups with intermediate- or high-type ARM.
| Variables | ARM group(n=18) | ARM+TCS group (n=17) |
χ2/Z | p |
| Soiling | ||||
| No | 8(44.44) | 6(35.29) | -0.434 | 0.665 |
| Grade 1 once or twice per week | 5(27.78) | 5(29.41) | ||
| Grade 2 Every day, no social problem | 2(11.11) | 4(23.53) | ||
| Grade 3 Constant, social problem | 3(16.67) | 2(11.77) | ||
| Constipation | ||||
| No | 5(27.78) | 7(41.18) | -0.326 | 0.744 |
| Grade 1 Manageable by changes in diet | 7(38.88) | 3(17.65) | ||
| Grade 2 Requires laxatives | 3(16.67) | 5(29.41) | ||
| Grade 3 Resistant to diet and laxatives | 3(16.67) | 2(11.76) | ||
| Voluntary bowel movements | ||||
| No | 12(66.67) | 7(41.18) | 2.289 | 0.130 |
| Feeling of urge、 Capacity to verbalize、Hold defecation | 6(33.33) | 10(58.82) |
The values are presented as numbers and percentages (%). ARM, anorectal malformation; TCS, tethered cord syndrome.
4. Discussion
ARM is caused by abnormal development of the anorectal region during the embryonic period, and while the exact etiology is currently unclear; it is currently believed to be the result of the combined action of genetic and environmental factors [12]. ARM often coexists with multiple malformations, including TCS. Based on the results of this study, the author believes that the risk factors for the coexistence of ARM with TCS in children have the following characteristics:
1. The proportion of children in the ARM+TCS group who took folic acid promptly was lower than that in the ARM group, although there was no significant difference between the two groups. Folic acid is an essential substance for the development of the nervous system during the embryonic stage. Deficiency can affect the fetal nervous system, leading to the occurrence of TCS [13]. Many pregnant women only discover their pregnancy after a delayed menstrual period, at which time they are already 5-6 weeks postovulation, and the neural tube has already closed, making it too late to begin taking folic acid. [14].
2. The prevalence of TCS is greater in children with intermediate or high-type ARM, and the occurrence of TCS is not related to the Krickenbeck classification, which is consistent with the literature [15,16]. The probability of TCS in children with intermediate or high-type ARM is 3.571 times greater than that of children with low-type ARM. When children with ARM are found to have multiple system malformations, the risk of TCS is greater, and screening for TCS should receive more attention at this time.
3. This study revealed that the incidence rate of TCS in children with ARM is approximately 27.2%, which is close to the results reported in domestic and international literature (20% to 60%), but it is much higher than the incidence rate of TCS in newborns (2.5/10000 to 2.7/1000) [17]. Given the high detection rate of TCS, it is recommended that all children with ARM undergo lumbosacral MRI before surgery. In addition to the timely identification of children with TCS, MRI has high accuracy in the preoperative typing of ARM, assessment of sphincter development, and accurate location of fistulas [5,18,19]. Some scholars believe that sacrococcygeal ultrasound has high specificity for diagnosing TCS, but sacrococcygeal ultrasound cannot accurately detect filar lipomatosis, and its sensitivity is relatively low [20]. Furthermore, sacrococcygeal ultrasound must be conducted before ossification of the posterior arch of the lumbar vertebrae, a time window that is usually only three months.
4. In this study, out of 31 cases of TCS, 30 cases were classified as spinal lipomas. All of these SLs are Type III or Type IV [21]. During embryonic development, the formation of the primary neural tube occurs between approximately 17 and 26 days postovulation, and the formation of the secondary neural tube occurs between 26 and 49 days postovulation [22,23]. Failure of the cloacal septum to divide leads to ARM, which occurs between 5 and 8 weeks postovulation and overlaps with the late stage of secondary neural tube formation. Therefore, when an ARM is associated with a TCS, the type of TCS is typically Type III or Type IV SL, which occurs after primary neural tube formation.
As surgical techniques and skills have progressed and the perioperative management of children with ARMs has increased, the complications associated with ARMs have seen significant improvement. However, postoperative constipation or fecal incontinence remain the most common complications affecting the quality of life of children with these malformations [24]. Numerous studies have reported on anorectal function in children with ARM who also have TCS after untethering surgery, with varying results [25,26]. We assessed defecation symptoms in children with ARM who underwent TCS following untethering surgery and compared them with those of ARM children without TCS. We discovered that in children with low-type ARM, those in the ARM+TCS group exhibited a significant improvement in constipation symptoms after untethering surgery compared with the children in the ARM group. When anorectal function was compared between the two groups of children with intermediate- or high-type ARM, no statistically significant difference was observed. The act of defecation is a complex physiological process that can be influenced by colonic motility, anorectal morphology, pelvic floor function, and sphincter function. Animal experiments also suggest that in severe ARM, the neural pathways that control defecation may not fully develop during the embryonic stage, and untethering surgery performed subsequently may not improve anorectal function [27]. We strongly recommend that children with ARM undergo untethering surgery upon diagnosis of TCS. This procedure can improve some symptoms in children with low-type ARM, and delayed intervention poses risks. New neurological deficits, such as urinary dysfunction, lower limb weakness, and foot deformities, can occur at any time as long as TCS is present. Furthermore, the use of neurophysiological monitoring can increase the safety of untethering surgery [28].
This study also has several limitations: 1. As a retrospective study, during the outpatient follow-up or WeChat follow-up process, many risk factors require the parents of the children to recall, and some factors are indeed difficult to remember accurately, leading to biases in the accuracy of some data; 2. Some risks involve sensitive social information, such as the mother’s smoking behavior, whether active or passive, and the real situation is likely to be more severe than what is reflected in the study; 3. Another limitation is that this study is a single-center study, and there are insufficient sample sizes for some groups, which may lead to biases in the research results; and 4. Due to the young age of many children, they are unable to complete anorectal manometry, resulting in a lack of objective examination results for anorectal function assessment.
In summary, having intermediate or high-type ARM and having other associated malformations are risk factors for the co-occurrence of TCS in children with ARM. Children with low-type ARM who also have TCS tend to have better anorectal function after untethering surgery than those with low-type ARM who do not have TCS. However, among children with intermediate or high-type ARM, anorectal function is comparable between the two groups.
Funding
Fujian Provincial Clinical Key Specialty Construction Project - Fujian Children’s Hospital Pediatric Neurosurgery [Min Wei Yi Zheng (2023) No. 1163].
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
Data supporting reported results are available on request in anonymized manner.
Acknowledgments
The authors thank the patients and their families for participating in this study.
Conflicts of Interest
The authors declare no conflict of interest. The authors have no personal circumstances or interests that may influence the representation or interpretation of the reported research results.
References
- MIYAKE Y, LANE G J, YAMATAKA A. Embryology and anatomy of anorectal malformations [J]. Semin Pediatr Surg, 2022, 31(6): 151226.
- LENA F, PELLEGRINO C, ZACCARA A M, et al. Anorectal malformation, urethral duplication, occult spinal dysraphism (ARM-UD-OSD): a challenging uncommon association [J]. Pediatr Surg Int, 2022, 38(10): 1487-94.
- LIAQAT N, WOOD R, FUCHS M. Hypospadias and anorectal malformation: A difficult combination [J]. J Pediatr Surg, 2023, 58(2): 228-30.
- DE BEAUFORT C M C, VAN DEN AKKER A C M, KUIJPER C F, et al. The Importance of Screening for Additional Anomalies in Patients with Anorectal Malformations: A Retrospective Cohort Study [J]. J Pediatr Surg, 2023, 58(9): 1699-707.
- ESPOSITO G, TOTONELLI G, MORINI F, et al. Predictive value of spinal bone anomalies for spinal cord abnormalities in patients with anorectal malformations [J]. J Pediatr Surg, 2021, 56(10): 1803-10.
- FANJUL M, SAMUK I, BAGOLAN P, et al. Tethered cord in patients affected by anorectal malformations: a survey from the ARM-Net Consortium [J]. Pediatr Surg Int, 2017, 33(8): 849-54.
- WEISBROD L J, THORELL W. Tethered Cord Syndrome (TCS) [M]. StatPearls. Treasure Island (FL) ineligible companies. Disclosure: William Thorell declares no relevant financial relationships with ineligible companies. 2024.
- CATMULL S, ASHURST J. Tethered Cord Syndrome [J]. Clin Pract Cases Emerg Med, 2019, 3(3): 297-8.
- TSUDA T, IWAI N, KIMURA O, et al. Bowel function after surgery for anorectal malformations in patients with tethered spinal cord [J]. Pediatr Surg Int, 2007, 23(12): 1171-4.
- DE BEAUFORT C M C, GROENVELD J C, MACKAY T M, et al. Spinal cord anomalies in children with anorectal malformations: a retrospective cohort study [J]. Pediatr Surg Int, 2023, 39(1): 153.
- INOUE M, UCHIDA K, OTAKE K, et al. Long-term functional outcome after untethering surgery for a tethered spinal cord in patients with anorectal malformations [J]. Pediatr Surg Int, 2017, 33(9): 995-9.
- LI J, GAO W, LIU X, et al. Clinical characteristics, prognosis, and its risk factors of anorectal malformations: a retrospective study of 332 cases in Anhui Province of China [J]. J Matern Fetal Neonatal Med, 2020, 33(4): 547-52.
- FARIA D J, SIMOES MDE J, TEIXEIRA L C, et al. Effect of folic acid in a modified experimental model of anorectal malformations adriamycin-induced in rats [J]. Acta Cir Bras, 2016, 31(1): 22-7.
- WU F, WANG Z, BI Y, et al. Investigation of the risk factors of anorectal malformations [J]. Birth Defects Res, 2022, 114(3-4): 136-44.
- DEWBERRY L, PENA A, MIRSKY D, et al. Sacral agenesis and fecal incontinence: how to increase the index of suspicion [J]. Pediatr Surg Int, 2019, 35(2): 239-42.
- RINTALA R J. Congenital anorectal malformations: anything new? [J]. J Pediatr Gastroenterol Nutr, 2009, 48 Suppl 2: S79-82.
- UCHIDA K, INOUE M, MATSUBARA T, et al. Evaluation and treatment for spinal cord tethering in patients with anorectal malformations [J]. Eur J Pediatr Surg, 2007, 17(6): 408-11.
- BISCHOFF A, PENA A, KETZER J, et al. The conus medullaris ratio: A new way to identify tethered cord on MRI [J]. J Pediatr Surg, 2019, 54(2): 280-4.
- METZGER G, COOPER J N, KABRE R S, et al. Inter-rater Reliability of Sacral Ratio Measurements in Patients with Anorectal Malformations [J]. J Surg Res, 2020, 256: 272-81.
- JEHANGIR S, ADAMS S, ONG T, et al. Spinal cord anomalies in children with anorectal malformations: Ultrasound is a good screening test [J]. J Pediatr Surg, 2020, 55(7): 1286-91.
- TOMINEY S, KALIAPERUMAL C, GALLO P. External validation of a new classification of spinal lipomas based on embryonic stage [J]. J Neurosurg Pediatr, 2020, 25(4): 394-401.
- MOROTA N, IHARA S, OGIWARA H. New classification of spinal lipomas based on embryonic stage [J]. J Neurosurg Pediatr, 2017, 19(4): 428-39.
- HERTZLER D A, 2ND, DEPOWELL J J, STEVENSON C B, et al. Tethered cord syndrome: a review of the literature from embryology to adult presentation [J]. Neurosurg Focus, 2010, 29(1): E1.
- SCHMITT F, SCALABRE A, MURE P Y, et al. Long-Term Functional Outcomes of an Anorectal Malformation French National Cohort [J]. J Pediatr Gastroenterol Nutr, 2022, 74(6): 782-7.
- TOTONELLI G, MESSINA R, MORINI F, et al. Impact of the associated anorectal malformation on the outcome of spinal dysraphism after untethering surgery [J]. Pediatr Surg Int, 2019, 35(2): 227-31.
- VILANOVA-SANCHEZ A, RECK C A, SEBASTIAO Y V, et al. Can sacral development as a marker for caudal regression help identify associated urologic anomalies in patients with anorectal malformation? [J]. J Pediatr Surg, 2018, 53(11): 2178-82.
- YANG Z, LI X, JIA H, et al. BMP7 is Downregulated in Lumbosacral Spinal Cord of Rat Embryos With Anorectal Malformation [J]. J Surg Res, 2020, 251: 202-10.
- HAN X, YUE X, WANG G, et al. Successfully treatment of tethered-cord syndrome secondary to progressive-development giant myelomeningocele by surgical repair with intraoperative neurophysiological monitoring in an infant [J]. Asian J Surg, 2023, 46(4): 1830-1.
Figure 1.
Inclusion and exclusion criteria for studies on ARM. ARM, Anorectal malformation; TCS, tethered cord syndrome.
Figure 1.
Inclusion and exclusion criteria for studies on ARM. ARM, Anorectal malformation; TCS, tethered cord syndrome.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



