Submitted:
24 October 2024
Posted:
28 October 2024
You are already at the latest version
Abstract
Myo-inositol (MYO) and D-chiro-inositol (DCI) are the two most significant isomeric forms of inositol, playing a critical role in intracellular signaling. MYO is the most abundant form of inositol in nature; DCI is produced from MYO through epimerization by an insulin-dependent enzyme. Recently, it has been demonstrated that inositols may influence oocyte maturation, improve intracellular Ca2+ oscillation in the oocytes and have been proposed as potential interventions for restoring spontaneous ovulation. MYO concentration in human follicular fluid is considered a bioindicator of oocyte quality. In the ovary, DCI modulates the activity of aromatase thus regulating androgen synthesis. Under physiological conditions, MYO/DCI ratio is maintained at 40:1 in the plasma. In women with PCOS, MYO/DCI ratio lowers to 0:2:1, contributing to elevated androgen production. By regulating FSH signaling, MYO administration increases the number of high-quality embryos available for transfer in poor responder patients. Finally, by acting downstream to insulin signaling inositol administration during pregnancy may represent a novel strategy for counteracting gestational diabetes. These findings show that diet supplementation with inositols may be a promising strategy to address female infertility and sustain healthy pregnancy.
Keywords:
Myo-Inositol
; D-chiro-Inositol
; fertility
; oocytes
; in vitro fertilization
; gestational diabetes mellitus
; PCOS
1. Introduction
Infertility is defined by the World Health Organization (WHO) as the inability to conceive after 1 year (or longer) of unprotected intercourse [1]. Infertility affects up to 17.5% of the global population, with a notable impact on quality of life and psychological well-being. Advances in assisted reproductive technologies (ART), such as in vitro fertilization (IVF) and intracytoplasmic sperm injection (ICSI), improved pregnancy outcomes; however, the success rates remain suboptimal [1].
Recently, the role of inositol, particularly Myo-inositol (MYO), has been investigated for its potential to enhance fertility outcomes. Inositols are a group of nine stereoisomers, with MYO and DCI being the most prevalent in nature. MYO can be obtained from dietary sources, primarily corn, nuts, and fruits, or synthesized from D-glucose within the human body by various tissues such as the brain, liver, kidneys, mammary glands and testes [2]. Inositols play a critical role in cellular signaling and has garnered significant interest for its potential benefits in fertility treatments [3,4]. MYO is crucial for cellular metabolism, its presence being essential for the biosynthesis of numerous molecular components within the biochemical machinery [5]. One significant effect of MYO on human physiology is its regulation of several molecular pathways directly linked to reproductive functions [6]. An international consensus meeting reaffirmed that the quality of the oocytes and embryos in assisted reproduction may be improved when inositol supplementation is used during the IVF treatment [7]. Different studies have demonstrated that inositol influences oocyte maturation and can be proposed as a potential novel intervention for restoring spontaneous ovulation [8]. Inositols can decrease androgen production in theca cells by enhancing steroidogenesis [9]. Additionally, MYO supplementation can improve intracellular Ca2+ oscillation in mouse oocytes [10]. This has also been demonstrated in mouse oocytes in which it improves the meiotic progression [10]. Furthermore, high concentrations of MYO in human follicular fluid are considered a bioindicator of elevated oocyte quality [11].
This review synthesizes the current evidence on inositol's efficacy in fertility treatments, focusing on its biochemical mechanisms, clinical applications, impact on pregnancy outcomes and gestational diabetes.
2. Biological functions of Inositols in female reproductive system
Inositol is a polyalcohol with the formula C6H12O6 that exists in the form of nine isomers (cyclohexane-1,2,3,4,5,6-hexol) (Figure 1).
It is largely present in cereals such as corn, fruits, vegetables, milk derived products, meat, legumes and dried fruit [12] (Table 1). Inositols are crucial compounds that support female fertility and physiological pregnancy [13]. In mammals, MYO is the most abundant inositol isomer, being present in nearly all tissues. It is especially abundant in the brain, blood, fat, kidney, lung, ovaries, and testes, where it is involved in multiple cellular pathways [14]. DCI is frequently found as a trace element in all tissues containing MYO and is the second most represented inositol isomer [13]. Researchers discovered that MYO/DCI concentration ratios are high in tissues with high energy demand from extracellular glucose; on the contrary they are low in tissues that store glycogen as the primary source of glucose [14,15].
Both MYO and DCI inositol isomers are precursors of membrane phosphoglycans (PG), MYO-PG and DCI-PG, which are primarily involved in cellular signaling cascades [15], transmitting extracellular stimuli to cellular organelles [24]. The main functions of the inositol cascades are in the signaling of insulin [25], gonadotropins [15,26], and cytoskeletal rearrangement processes [27]. Consequently, inositols constitute the mediators of crucial processes such as energy metabolism, cellular motility, and, in the ovary, follicular development throughout the advancement of the menstrual cycle. Appropriate glucose levels and relative metabolic processes are important for follicle maturation and female fertility [28], to confer proper cellular motility essential during embryogenetic processes, such as neural tube closure [29], and to maintain a physiological pregnancy [30].
Impaired inositol and/or glycosylphosphatidylinositol (GPI) metabolism and abnormal inositol-phosphoglycans (IPG-P) production are observed, respectively, in women with polycystic ovary syndrome (PCOS) and in obese patients independently of PCOS, contributing to insulin resistance and dysmetabolic processes, which are considered as important hallmarks of female infertility.
In virtue of its action as an insulin sensitizer, MYO exerts positive effects on obesity, decreasing body weight and leptin secretion while increasing HDL cholesterol [31]. In the ovary, MYO enhances FSH action via anti-Müllerian hormone (AMH), and is abundant in follicular fluid, improving oocyte and embryo quality. As a strong antioxidant (increasing superoxide dismutase, catalase, and glutathione), it improves cell morphology, growth, and lipid synthesis in cell membranes.
Presence of DCI is guaranteed in all tissues via MYO conversion catalyzed by the activity of an insulin-dependent epimerase. Each organ of the human body has a specific MYO to DCI ratio related to its function [15]. High levels of DCI are observed in glycogen storage organs. In case of insulin resistance, the activation of epimerase is hampered in non-reproductive tissues, thereby obstructing the conversion of MYO to DCI. This leads to reduced levels of DCI, which diminishes glycogen synthesis and increases overall blood glucose levels, increasing insulin release but exacerbating insulin resistance. In the normal ovary, the typical MYO/DCI ratio is maintained by the insulin-epimerase axis around 100:1. In patients with insulin resistance, the ovary retains its normal insulin sensitivity contrary to other tissues. According to this phenomenon, known as the ovarian paradox (Figure 2), in these patients the ovary maintains a normal insulin sensitivity and hyperinsulinemia overstimulates ovarian cell epimerase, causing an excess of DCI at the expense of MYO and reducing the MYO to DCI ratio to 0.2:1 [5]. This imbalance leads to increased androgen synthesis due to higher DCI levels and impairs FSH signaling and oocyte quality due to MYO depletion. Indeed, several studies determined that MYO represents a valid non hormonal therapeutic approach to PCOS, as such or in treatments combining MYO and DCI in the respective ratio of 40:1. This treatment restores the menstrual cycle and ovulation, increases progesterone and SHBG, and decreases LH, testosterone, and insulin levels [32].
3. Clinical Applications of Inositols in fertility treatments and healthy pregnancy
3.1. Inositols and Polycystic Ovary Syndrome (PCOS)
PCOS is the most prevalent endocrine disorder in women of reproductive age [31]. According to the Rotterdam criteria, its current definition requires at least two of the following clinical manifestations: chronic ovulatory disorder (oligo-ovulation to anovulation, and amenorrhea), presence of polycystic ovaries at the ultrasound examination, and hyperandrogenism [31], leading to the identification of four different phenotypes, with only three of them (A, B, and C) exhibiting hyperandrogenism (Figure 3). In recent years, these criteria have faced criticism. Indeed, the etiopathogenesis of these four Phenotypes is still under debate, and it has been proposed that Phenotype D may be caused by changes in gonadotrophin or insulin-like growth factor 1 levels. Finally, Phenotype D, which does not present hyperandrogenism, is more frequently associated with insulin resistance than Phenotypes A, B, and C [33].
The use of inositols is currently considered to be an experimental therapy for PCOS patients. In particular, the use of MYO is well validated in PCOS, especially for Phenotype D [33].
Insulin resistance and compensatory hyperinsulinemia seem to have a central role in PCOS pathogenesis, contributing both directly and indirectly to the development of hyperandrogenism and related clinical features. The increased production of androgens is an inherent property of theca cells, which is further exacerbated by excess luteinizing hormone (LH) and hyperinsulinemia. A functional result of PCOS hormonal imbalances is the failure to select a dominant follicle, leading to the accumulation of selectable follicles and the characteristic polycystic ovaries seen on ultrasonography. This follicular arrest results from a lack of follicle-stimulating hormone (FSH) action and/or premature LH action. Studies have highlighted the role of anti-Müllerian hormone (AMH) in inhibiting the follicular response to FSH [31], and the increased sensitivity of follicles to LH consequent to hyperinsulinism.
As anticipated, several studies have shown that MYO supplementation improves insulin sensitivity, reduces hyperandrogenism, and restores ovulatory function in women with PCOS, thereby enhancing fertility potential [34]. This effect is enhanced in overweight patients by the MYO-DCI combination, at both the metabolic and reproductive level [35].
In PCOS patients, insulin sensitivity and physiological androgen levels are improved by treatments with metformin (MET), but the gastrointestinal side effects of this compound limit its use [36]. Having no side effects at the recommended dosages, MYO and DCI represent at present the optimal nutraceutical alternative [31]. MYO is known to decrease LH and androgen levels, the LH/FSH ratio, and levels of testosterone and androstenedione as well as insulin resistance [4,37]. MYO helps re-establish ovulatory menstrual cycles, especially in obese women with PCOS, thereby facilitating spontaneous pregnancies through adequate luteal phase progesterone production [34]. When ovulation is induced in PCOS women with hyperinsulinemia, MYO enhances ovarian sensitivity to gonadotropins reducing the required doses of FSH and LH [8,38]. Furthermore, MYO reduces estradiol levels on the day of ovulation, avoiding ovarian hyperstimulation, and finally reduces the number of intermediate-sized follicles.
At the cellular level, MYO improvements include better oocyte quality and maturation, increased cleavage rate, improved embryo development (expanded blastocyst), higher embryo quality, and increased pregnancy rates in women with PCOS [39]. Chiu et al. [11] demonstrated a correlation between MYO concentration in follicular fluid and oocyte and embryo quality in women undergoing assisted reproduction without PCOS diagnosis. The same researcher showed that MYO supplementation promotes meiotic progression in mouse GV oocytes by enhancing intracellular Ca2+ oscillation, leading to the completion of meiosis [10]. A randomized controlled involving PCOS patients undergoing assisted reproduction demonstrated that treatment with MYO prior to induction of ovulation resulted in a significantly higher percentages of oocytes in metaphase II (MII) stage, fertilization rates and good quality embryos. The expression of three genes associated with good oocyte quality (PGK1, RGS2 and CDC42) was significantly higher in the MYO-treated group, although no significant difference in reactive oxygen species concentration in follicular fluid was noted, suggesting that MYO's effect on oocyte quality is independent of its antioxidant action [40]. Although a meta-analysis specifically focused on women with PCOS undergoing ICSI found the evidence for MYO's efficacy to be inconclusive [41,42], two additional meta-analyses support the impact of MYO among women with PCOS undergoing IVF/ICSI [8,43].
The effect of combined MYO-DCI supplementation on improving oocyte quality, embryo quality, and pregnancy outcomes in women with PCOS undergoing ART has also been explored in several studies [39,44,45], including a study involving a murine PCOS model [46] with the general conclusion that the two molecules together provide improved outcomes, but only by keeping DCI levels low, at the optimal MYO/DCI ratio of 40:1 [46]. Opposite effects are observed when high doses of DCI are administered (ovarian paradox), as observed both on human patients and mice [47].
The Bhide meta-analysis [43], which included 18 trials, confirmed that MYO/DCI administration for three months prior to ovarian stimulation reduces the required FSH doses for follicular response, lowers estradiol levels on the day of ovulation triggering, reduces the risk of ovarian hyperstimulation, and decreases the number of cancelled cycles. However, it did not find significant effects on regarding the number of oocytes, MII oocytes, top-grade embryos and clinical pregnancy rate. Since the study underscored the high heterogeneity of the included trials, large multicenter randomized controlled trials are necessary to evaluate the impact of inositol administration on clinical pregnancy and live birth rates in ART.
3.2. Inositols in ovarian response to hormonal stimulation by exogenous gonadotropins during Assisted Reproductive Technologies (ART)
Diminished ovarian response, affecting 9–24% of women undergoing ART, is a significant challenge in treating infertile patients [48,49]; this condition is characterized by an inadequate response to exogenous gonadotropins or a low ovarian reserve, considering age, ovarian biomarkers (antral follicle count [AFC] and AMH), and the ovarian response in previous stimulation cycles, as defined by the Patient-Oriented Strategies Encompassing Individualized Oocyte Number (POSEIDON) classification [50]. The low quantity and quality of retrieved oocytes after ovarian stimulation, along with very low fertilization rates following ICSI, are major factors contributing to the reduced success rate of ART in poor responders patients [51,52]. Oocyte quality is influenced by factors such as nuclear and mitochondrial genome integrity and the ovarian and follicular microenvironment, which affect cytoplasmic maturation [53]. Numerous studies have assessed various interventions aimed at improving reproductive outcomes for poor responders undergoing ART, but there is insufficient evidence to confirm their effectiveness [54]. Common interventions, such as pretreatment with compound oral contraceptives, adjuvant growth hormone (GH) or GH-releasing factors therapy, and corticosteroids, often result in only minor or statistically insignificant improvements [55]. Inositol has been shown to influence oocyte maturation and is suggested as a potential new intervention for restoring spontaneous ovulation [56]. Indeed, MYO seems to improve intracellular Ca2+ oscillation. As Ca2+ oscillation plays a critical role in normal fertilization and embryogenesis, this could be the proposed mechanism through which MYO enhances fertilization rate and embryo quality [57]. In accordance, treatment with MYO, starting three months before ovarian stimulation, showed promising results in improving reproductive outcomes in ICSI cycles for poor responder patients [56]. Several studies have demonstrated that women receiving MYO supplementation starting one month before the ICSI cycle and continuing until the ovulation trigger had a significant enhancement in fertilization rates and in the production of top grade embryos in comparison to untreated patients [44,49,57,58].
Thus, MYO supplementation increases the number of high-quality embryos available for transfer, potentially leading to higher cumulative pregnancy rates in poor responder patients, a topic that warrants further investigation in future studies.
3.3. Impact of inositols administration on gestational diabetes mellitus
Over the past 50 years, the prevalence of obesity, type 2 diabetes, and gestational diabetes mellitus (GDM) among women of childbearing age has dramatically increased [59]. A rising number of pregnant women are now at risk for these conditions, characterized by insulin resistance, hyperinsulinemia, inflammation, and elevated oxidative stress [59]. During pregnancy, insulin resistance naturally increases due to the release of placental hormones, which aim to promote nutrient utilization by the fetus, particularly in the second and third trimesters. However, this pregnancy-associated insulin resistance is also the primary pathogenic mechanism leading to the development of GDM. Patients with GDM excrete significantly more urinary inositol during the first trimester compared to those with normal pregnancies, indicating altered insulin effects on inositol metabolism in this group [60]. Based on these findings, a randomized controlled study was conducted with pregnant women diagnosed with GDM between 24 and 28 weeks of gestation to evaluate the impact of MYO supplementation on insulin resistance parameters. Insulin resistance (evaluated via HOMA-IR) and circulating adiponectin levels were measured. Compared to the control group, the MYO supplementation group showed a significant reduction in HOMA-IR, fasting plasma glucose, insulin levels and a greater increase in circulating adiponectin levels after 8 weeks of treatment with 4 g MYO per day [61]. Fraticelli et al. [62] recently discovered that pregnant women with GDM treated with 4g of MYO showed significant improvement in insulin resistance and less weight gain during pregnancy compared to those treated with DCI (500 mg) or a MYO/DCI combination (1100 mg/27.6 mg) [62]. Despite promising clinical results, little is known about the bioavailability and optimal dosage of MYO. The maximum daily intake is currently up to 4 g, and splitting this dose into two administrations may provide full-day coverage. Further research is needed to determine if some pharmaceutical forms of MYO are more effective than others.
4. Dietary intake, safety and tolerability of Inositols
As previously mentioned, depending on the spatial orientation of its six hydroxyl groups, inositol exists in nature in nine different stereoisomeric forms [63]. The main type of inositol in food that is nutritionally significant is MYO. MYO was once thought to be a member of the vitamin B family. However, it is no longer regarded as a necessary food because the human liver and kidney generate it beginning with d-glucose at a rate of up to 4-5 g/day [64]. Inositol is mostly found in animal products in its free form or as phosphatidylinositol, a phospholipid that contains inositol. In contrast, inositol is preferentially found in plant-derived foods as inositol hexaphosphate (IP6). The main phosphorus storing molecule in seeds is IP6. According to estimates, a western diet offers roughly 1 g of MYO [65], an insufficient inositol intake. As shown previously in Table 1, fresh fruits, vegetables, and seeds (beans, grains, pseudo-cereals, and nuts) contain the highest concentration of myo-inositol, primarily in their aleurone layer [17]. Myo-inositol can be found in whole-grain cereals [17].Compared to other cereals, myo-inositol is higher in oats and bran. However, processing techniques have an impact on the overall quantity of free myo-inositol absorbed with cereals [17]. Additionally, microbial phytases hydrolyze up to 66% of dietary phytates in humans in the large intestine and stomach [66] . Therefore, the amount of free myo-inositol and D-chiro-inositol that is not broken down by bacteria determines how much of each is absorbed. Concurrently, genetic factors, unbalanced diets, and certain medications have contributed to inositol depletion, which is linked to various pathological conditions. Several studies have highlighted the positive effects of dietary supplementation with MYO in diseases associated with its depletion, such as insulin resistance, PCOS, diabetes, GDM, depression, and metabolic syndrome. These studies have evaluated different forms, combinations, and dosages of inositols, yielding variable results [67]. In clinical practice, dietary supplements typically contain no more than 4 g/day of inositol. However, studies on patients with depressive disorders have used much higher doses, up to 12–18 g/day, without significant adverse events and with additional clinical benefits [68]. The U.S. Food and Drug Administration (FDA) has classified MYO as Generally Recognized As Safe (GRAS), indicating it meets the safety standards of the Federal Food, Drug, and Cosmetic Act (FFDCA). Studies have shown that doses as high as 30 g/day may cause only mild gastrointestinal symptoms in the first month. The commonly used clinical dose of 4 g/day is completely free of side effects [68]. Given the various mechanisms contributing to inositol depletion, it is crucial to identify the primary cause to provide the most effective therapeutic strategy. When genetic alterations result in fewer inositol transporters or decreased activity, a tailored therapeutic approach with multiple daily administrations can prevent rapid saturation and subsequent inositol reduction [69]. In cases of poor intestinal absorption of inositols due to glucose competition, it is recommended to take inositol supplements away from meals to avoid competitive absorption during high glucose levels [70]. This strategy can improve glucose metabolism in patients with diabetes and insulin resistance by reducing postprandial glucose levels and increasing peripheral insulin sensitivity [70]. Defective intestinal absorption of inositols may also be linked to gut dysbiosis, leading to inflammation and micronutrient malabsorption. In such cases, concomitant supplementation of inositols (MYO and DCI) and prebiotics can enhance intestinal health and overcome absorption issues [71]. Studies in mouse models of obesity and women with PCOS have shown that combining MYO, DCI, and α-lactalbumin (α-LA) can improve intestinal absorption and enhance the beneficial effects on reproductive and metabolic health possibly due to changes in tight junctions’ permeability [71].
5. Conclusions
Inositols, particularly MYO, have emerged as a valuable adjunct in fertility treatments. Its ability to improve oocyte quality, embryo development, and clinical pregnancy rates makes it a promising option for women undergoing ART. This review provides a comprehensive overview of the current understanding of inositol's role in enhancing fertility, highlighting its potential benefits and safety profile for women undergoing fertility treatments. MYO and DCI have been shown to stimulate ovulation and restore the normal menstrual cycle in infertile women, especially those with PCOS. Additionally, MYO supplementation helps women undergoing ART by enhancing the quality of their oocytes and embryos. MYO lowers the risk of metabolic disorders like GDM during pregnancy, which can result in miscarriages or stillborn children. Since it has been demonstrated that large doses of DCI administered over an extended period raise testosterone levels, DCI supplementation for PCOS women should be carefully considered and should only be used for short-term treatments for all other patient types. Infact, DCI is effective in causing ovulation in these patients. DCI is a safe substitute for medications in anovulatory women to promote ovulatory activity.
The integration of inositols into fertility protocols offers a novel approach to enhancing reproductive outcomes and addressing the challenges of infertility. Further research is warranted to establish standardized dosing regimens and to explore its potential benefits in diverse populations.
Author Contributions
“Conceptualization, G.D, A.B.; writing—review and editing, M.P; G.C.; G.D.E.; C.T.; A.B.; visualization, M.P. and G.D.E.; supervision, G.D.; A.B. All authors have read and agreed to the published version of the manuscript.”.
Funding
This research received no external funding.
Institutional Review Board Statement
Not applicable.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Ombelet, W. WHO Fact Sheet on Infertility Gives Hope to Millions of Infertile Couples Worldwide. Facts Views Vis Obgyn 12, 249–251.
- Joardar, S.; Duarah, P.; Purkait, M.K. Recent Advances in Myo-Inositol Recovery and Purification from Agricultural Sources as Potential Dietary Supplements: A Review. Sustainable Chemistry and Pharmacy 2023, 36, 101331. [Google Scholar] [CrossRef]
- Brusco, G.F.; Mariani, M. Inositol: Effects on Oocyte Quality in Patients Undergoing ICSI. An Open Study. Eur Rev Med Pharmacol Sci 2013, 17, 3095–3102. [Google Scholar] [PubMed]
- Zacchè, M.M.; Caputo, L.; Filippis, S.; Zacchè, G.; Dindelli, M.; Ferrari, A. Efficacy of Myo-Inositol in the Treatment of Cutaneous Disorders in Young Women with Polycystic Ovary Syndrome. Gynecological Endocrinology 2009, 25, 508–513. [Google Scholar] [CrossRef] [PubMed]
- Unfer, V.; Carlomagno, G.; Rizzo, P.; Raffone, E.; Roseff, S. Myo-Inositol Rather than D-Chiro-Inositol Is Able to Improve Oocyte Quality in Intracytoplasmic Sperm Injection Cycles. A Prospective, Controlled, Randomized Trial. Eur Rev Med Pharmacol Sci 2011, 15, 452–457. [Google Scholar] [PubMed]
- Granata, R.; Settanni, F.; Biancone, L.; Trovato, L.; Nano, R.; Bertuzzi, F.; Destefanis, S.; Annunziata, M.; Martinetti, M.; Catapano, F.; et al. Acylated and Unacylated Ghrelin Promote Proliferation and Inhibit Apoptosis of Pancreatic Beta-Cells and Human Islets: Involvement of 3’,5’-Cyclic Adenosine Monophosphate/Protein Kinase A, Extracellular Signal-Regulated Kinase 1/2, and Phosphatidyl Inositol 3-Kinase/Akt Signaling. Endocrinology 2007, 148, 512–529. [Google Scholar] [CrossRef]
- Bevilacqua, A.; Carlomagno, G.; Gerli, S.; Montanino Oliva, M.; Devroey, P.; Lanzone, A.; Soulange, C.; Facchinetti, F.; Carlo Di Renzo, G.; Bizzarri, M.; et al. Results from the International Consensus Conference on Myo-Inositol and D-Chiro-Inositol in Obstetrics and Gynecology--Assisted Reproduction Technology. Gynecol Endocrinol 2015, 31, 441–446. [Google Scholar] [CrossRef]
- Laganà, A.S.; Garzon, S.; Casarin, J.; Franchi, M.; Ghezzi, F. Inositol in Polycystic Ovary Syndrome: Restoring Fertility through a Pathophysiology-Based Approach. Trends Endocrinol Metab 2018, 29, 768–780. [Google Scholar] [CrossRef]
- Cheang, K.I.; Baillargeon, J.-P.; Essah, P.A.; Ostlund, R.E.; Apridonize, T.; Islam, L.; Nestler, J.E. Insulin-Stimulated Release of D-Chiro-Inositol-Containing Inositolphosphoglycan Mediator Correlates with Insulin Sensitivity in Women with Polycystic Ovary Syndrome. Metabolism 2008, 57, 1390–1397. [Google Scholar] [CrossRef]
- Chiu, T.T.Y.; Rogers, M.S.; Briton-Jones, C.; Haines, C. Effects of Myo-Inositol on the in-Vitro Maturation and Subsequent Development of Mouse Oocytes. Hum Reprod 2003, 18, 408–416. [Google Scholar] [CrossRef]
- Chiu, T.T.Y.; Rogers, M.S.; Law, E.L.K.; Briton-Jones, C.M.; Cheung, L.P.; Haines, C.J. Follicular Fluid and Serum Concentrations of Myo-Inositol in Patients Undergoing IVF: Relationship with Oocyte Quality. Hum Reprod 2002, 17, 1591–1596. [Google Scholar] [CrossRef]
- Zuluaga, A.M.; Mena-García, A.; Soria Monzón, A.C.; Rada-Mendoza, M.; Chito, D.M.; Ruiz-Matute, A.I.; Sanz, M.L. Microwave Assisted Extraction of Inositols for the Valorization of Legume By-Products. LWT 2020, 133, 109971. [Google Scholar] [CrossRef]
- Gambioli, R.; Forte, G.; Aragona, C.; Bevilacqua, A.; Bizzarri, M.; Unfer, V. The Use of D-Chiro-Inositol in Clinical Practice. Eur Rev Med Pharmacol Sci 2021, 25, 438–446. [Google Scholar] [CrossRef] [PubMed]
- Beemster, P.; Groenen, P.; Steegers-Theunissen, R. Involvement of Inositol in Reproduction. Nutr Rev 2002, 60, 80–87. [Google Scholar] [CrossRef] [PubMed]
- Larner, J. D-Chiro-Inositol--Its Functional Role in Insulin Action and Its Deficit in Insulin Resistance. Int J Exp Diabetes Res 2002, 3, 47–60. [Google Scholar] [CrossRef] [PubMed]
- Gonzalez-Uarquin, F.; Kenéz, Á.; Rodehutscord, M.; Huber, K. Dietary Phytase and Myo-Inositol Supplementation Are Associated with Distinct Plasma Metabolome Profile in Broiler Chickens. Animal 2020, 14, 549–559. [Google Scholar] [CrossRef]
- Clements, R.; Darnell, B. Myo-Inositol Content of Common Foods: Development of a High-Myo-Inositol Diet. The American journal of clinical nutrition 1980, 33, 1954–1967. [Google Scholar] [CrossRef]
- Dikeman, C.; Bauer, L.; Fahey, G. Carbohydrate Composition of Selected Plum/Prune Preparations. Journal of agricultural and food chemistry 2004, 52, 853–859. [Google Scholar] [CrossRef]
- Ratiu, I.A.; Al-Suod, H.; Ligor, M.; Ligor, T.; Krakowska, A.; Górecki, R.; Buszewski, B. Simultaneous Determination of Cyclitols and Sugars Following a Comprehensive Investigation of 40 Plants. Food Anal. Methods 2019, 12, 1466–1478. [Google Scholar] [CrossRef]
- Soria, A.C.; Sanz, M.L.; Villamiel, M. Determination of Minor Carbohydrates in Carrot (Daucus Carota L.) by GC–MS. Food Chemistry 2009, 114, 758–762. [Google Scholar] [CrossRef]
- Indyk, H.E.; Saldo, S.C.; White, P.M.; Dole, M.N.; Gill, B.D.; Woollard, D.C. The Free and Total Myo-Inositol Contents of Early Lactation and Seasonal Bovine Milk. International Dairy Journal 2016, 56, 33–37. [Google Scholar] [CrossRef]
- Byun, S.M.; Jenness, R. Estimation of Free Myo-Inositol in Milks of Various Species and Its Source in Milk of Rats (Rattus Norvegicus). J Dairy Sci 1982, 65, 531–536. [Google Scholar] [CrossRef] [PubMed]
- Ruiz-Aceituno, L.; Rodríguez-Sánchez, S.; Ruiz-Matute, A.I.; Ramos, L.; Soria, A.C.; Sanz, M.L. Optimisation of a Biotechnological Procedure for Selective Fractionation of Bioactive Inositols in Edible Legume Extracts. Journal of the Science of Food and Agriculture 2013, 93, 2797–2803. [Google Scholar] [CrossRef] [PubMed]
- Dinicola, S.; Chiu, T.T.Y.; Unfer, V.; Carlomagno, G.; Bizzarri, M. The Rationale of the Myo-Inositol and D-Chiro-Inositol Combined Treatment for Polycystic Ovary Syndrome. J Clin Pharmacol 2014, 54, 1079–1092. [Google Scholar] [CrossRef] [PubMed]
- Bosanac, I.; Michikawa, T.; Mikoshiba, K.; Ikura, M. Structural Insights into the Regulatory Mechanism of IP3 Receptor. Biochim Biophys Acta 2004, 1742, 89–102. [Google Scholar] [CrossRef]
- Ulloa-Aguirre, A.; Reiter, E.; Crépieux, P. FSH Receptor Signaling: Complexity of Interactions and Signal Diversity. Endocrinology 2018, 159, 3020–3035. [Google Scholar] [CrossRef]
- Casarini, L.; Santi, D.; Brigante, G.; Simoni, M. Two Hormones for One Receptor: Evolution, Biochemistry, Actions, and Pathophysiology of LH and hCG. Endocr Rev 2018, 39, 549–592. [Google Scholar] [CrossRef]
- Cogram, P.; Hynes, A.; Dunlevy, L.P.E.; Greene, N.D.E.; Copp, A.J. Specific Isoforms of Protein Kinase C Are Essential for Prevention of Folate-Resistant Neural Tube Defects by Inositol. Hum Mol Genet 2004, 13, 7–14. [Google Scholar] [CrossRef]
- Nikolopoulou, E.; Galea, G.L.; Rolo, A.; Greene, N.D.E.; Copp, A.J. Neural Tube Closure: Cellular, Molecular and Biomechanical Mechanisms. Development 2017, 144, 552–566. [Google Scholar] [CrossRef]
- Unfer, V.; Dinicola, S.; Laganà, A.S.; Bizzarri, M. Altered Ovarian Inositol Ratios May Account for Pathological Steroidogenesis in PCOS. Int J Mol Sci 2020, 21, 7157. [Google Scholar] [CrossRef]
- Merviel, P.; James, P.; Bouée, S.; Le Guillou, M.; Rince, C.; Nachtergaele, C.; Kerlan, V. Impact of Myo-Inositol Treatment in Women with Polycystic Ovary Syndrome in Assisted Reproductive Technologies. Reprod Health 2021, 18, 13. [Google Scholar] [CrossRef]
- Nordio, M.; Basciani, S.; Camajani, E. The 40:1 Myo-Inositol/D-Chiro-Inositol Plasma Ratio Is Able to Restore Ovulation in PCOS Patients: Comparison with Other Ratios. Eur Rev Med Pharmacol Sci 2019, 23, 5512–5521. [Google Scholar] [CrossRef] [PubMed]
- Myers, S.H.; Russo, M.; Dinicola, S.; Forte, G.; Unfer, V. Questioning PCOS Phenotypes for Reclassification and Tailored Therapy. Trends in Endocrinology & Metabolism 2023, 34, 694–703. [Google Scholar] [CrossRef]
- Papaleo, E.; Unfer, V.; Baillargeon, J.-P.; De Santis, L.; Fusi, F.; Brigante, C.; Marelli, G.; Cino, I.; Redaelli, A.; Ferrari, A. Myo-Inositol in Patients with Polycystic Ovary Syndrome: A Novel Method for Ovulation Induction. Gynecol Endocrinol 2007, 23, 700–703. [Google Scholar] [CrossRef] [PubMed]
- Benelli, E.; Del Ghianda, S.; Di Cosmo, C.; Tonacchera, M. A Combined Therapy with Myo-Inositol and D-Chiro-Inositol Improves Endocrine Parameters and Insulin Resistance in PCOS Young Overweight Women. Int J Endocrinol 2016, 2016, 3204083. [Google Scholar] [CrossRef]
- Bevilacqua, A.; Bizzarri, M. Physiological Role and Clinical Utility of Inositols in Polycystic Ovary Syndrome. Best Pract Res Clin Obstet Gynaecol 2016, 37, 129–139. [Google Scholar] [CrossRef]
- Minozzi, M.; D’Andrea, G.; Unfer, V. Treatment of Hirsutism with Myo-Inositol: A Prospective Clinical Study. Reprod Biomed Online 2008, 17, 579–582. [Google Scholar] [CrossRef]
- Zheng, X.; Lin, D.; Zhang, Y.; Lin, Y.; Song, J.; Li, S.; Sun, Y. Inositol Supplement Improves Clinical Pregnancy Rate in Infertile Women Undergoing Ovulation Induction for ICSI or IVF-ET. Medicine (Baltimore) 2017, 96, e8842. [Google Scholar] [CrossRef]
- Colazingari, S.; Treglia, M.; Najjar, R.; Bevilacqua, A. The Combined Therapy Myo-Inositol plus D-Chiro-Inositol, Rather than D-Chiro-Inositol, Is Able to Improve IVF Outcomes: Results from a Randomized Controlled Trial. Arch Gynecol Obstet 2013, 288, 1405–1411. [Google Scholar] [CrossRef]
- Akbari Sene, A.; Tabatabaie, A.; Nikniaz, H.; Alizadeh, A.; Sheibani, K.; Mortezapour Alisaraie, M.; Tabatabaie, M.; Ashrafi, M.; Amjadi, F. The Myo-Inositol Effect on the Oocyte Quality and Fertilization Rate among Women with Polycystic Ovary Syndrome Undergoing Assisted Reproductive Technology Cycles: A Randomized Clinical Trial. Arch Gynecol Obstet 2019, 299, 1701–1707. [Google Scholar] [CrossRef]
- Artini, P.G.; Di Berardino, O.M.; Papini, F.; Genazzani, A.D.; Simi, G.; Ruggiero, M.; Cela, V. Endocrine and Clinical Effects of Myo-Inositol Administration in Polycystic Ovary Syndrome. A Randomized Study. Gynecol Endocrinol 2013, 29, 375–379. [Google Scholar] [CrossRef]
- Mendoza, N.; Pérez, L.; Simoncini, T.; Genazzani, A. Inositol Supplementation in Women with Polycystic Ovary Syndrome Undergoing Intracytoplasmic Sperm Injection: A Systematic Review and Meta-Analysis of Randomized Controlled Trials. Reprod Biomed Online 2017, 35, 529–535. [Google Scholar] [CrossRef] [PubMed]
- Bhide, P.; Pundir, J.; Gudi, A.; Shah, A.; Homburg, R.; Acharya, G. The Effect of Myo-Inositol/Di-Chiro-Inositol on Markers of Ovarian Reserve in Women with PCOS Undergoing IVF/ICSI: A Systematic Review and Meta-Analysis. Acta Obstet Gynecol Scand 2019, 98, 1235–1244. [Google Scholar] [CrossRef] [PubMed]
- Papaleo, E.; Unfer, V.; Baillargeon, J.-P.; Fusi, F.; Occhi, F.; De Santis, L. Myo-Inositol May Improve Oocyte Quality in Intracytoplasmic Sperm Injection Cycles. A Prospective, Controlled, Randomized Trial. Fertil Steril 2009, 91, 1750–1754. [Google Scholar] [CrossRef] [PubMed]
- Pacchiarotti, A.; Carlomagno, G.; Antonini, G.; Pacchiarotti, A. Effect of Myo-Inositol and Melatonin versus Myo-Inositol, in a Randomized Controlled Trial, for Improving in Vitro Fertilization of Patients with Polycystic Ovarian Syndrome. Gynecol Endocrinol 2016, 32, 69–73. [Google Scholar] [CrossRef] [PubMed]
- Bevilacqua, A.; Dragotto, J.; Giuliani, A.; Bizzarri, M. Myo-Inositol and D-Chiro-Inositol (40:1) Reverse Histological and Functional Features of Polycystic Ovary Syndrome in a Mouse Model. J Cell Physiol 2019, 234, 9387–9398. [Google Scholar] [CrossRef]
- Carlomagno, G.; Unfer, V.; Roseff, S. The D-Chiro-Inositol Paradox in the Ovary. Fertil Steril 2011, 95, 2515–2516. [Google Scholar] [CrossRef]
- Tarlatzis, B.C.; Zepiridis, L.; Grimbizis, G.; Bontis, J. Clinical Management of Low Ovarian Response to Stimulation for IVF: A Systematic Review. Hum Reprod Update 2003, 9, 61–76. [Google Scholar] [CrossRef]
- Caprio, F.; D’Eufemia, M.D.; Trotta, C.; Campitiello, M.R.; Ianniello, R.; Mele, D.; Colacurci, N. Myo-Inositol Therapy for Poor-Responders during IVF: A Prospective Controlled Observational Trial. J Ovarian Res 2015, 8, 37. [Google Scholar] [CrossRef]
- Humaidan, P.; Alviggi, C.; Fischer, R.; Esteves, S.C. The Novel POSEIDON Stratification of “Low Prognosis Patients in Assisted Reproductive Technology” and Its Proposed Marker of Successful Outcome. F1000Res 2016, 5, 2911. [Google Scholar] [CrossRef]
- Kailasam, C.; Keay, S.D.; Wilson, P.; Ford, W.C.L.; Jenkins, J.M. Defining Poor Ovarian Response during IVF Cycles, in Women Aged <40 Years, and Its Relationship with Treatment Outcome. Hum Reprod 2004, 19, 1544–1547. [Google Scholar] [CrossRef]
- Ata, B.; Yakin, K.; Balaban, B.; Urman, B. Embryo Implantation Rates in Natural and Stimulated Assisted Reproduction Treatment Cycles in Poor Responders. Reprod Biomed Online 2008, 17, 207–212. [Google Scholar] [CrossRef] [PubMed]
- Rienzi, L.; Balaban, B.; Ebner, T.; Mandelbaum, J. The Oocyte. Hum Reprod 2012, 27 Suppl 1, i2-21. [Google Scholar] [CrossRef]
- Pandian, Z.; McTavish, A.R.; Aucott, L.; Hamilton, M.P.; Bhattacharya, S. Interventions for “poor Responders” to Controlled Ovarian Hyper Stimulation (COH) in in-Vitro Fertilisation (IVF). Cochrane Database Syst Rev 2010, CD004379. [Google Scholar] [CrossRef] [PubMed]
- Kucuk, T.; Kozinoglu, H.; Kaba, A. Growth Hormone Co-Treatment within a GnRH Agonist Long Protocol in Patients with Poor Ovarian Response: A Prospective, Randomized, Clinical Trial. J Assist Reprod Genet 2008, 25, 123–127. [Google Scholar] [CrossRef] [PubMed]
- Ciotta, L.; Stracquadanio, M.; Pagano, I.; Carbonaro, A.; Palumbo, M.; Gulino, F. Effects of Myo-Inositol Supplementation on Oocyte’s Quality in PCOS Patients: A Double Blind Trial. Eur Rev Med Pharmacol Sci 2011, 15, 509–514. [Google Scholar] [PubMed]
- Nazari, L.; Salehpour, S.; Hosseini, S.; Saharkhiz, N.; Azizi, E.; Hashemi, T.; Ghodssi-Ghassemabadi, R. Effect of Myo-Inositol Supplementation on ICSI Outcomes among Poor Ovarian Responder Patients: A Randomized Controlled Trial. J Gynecol Obstet Hum Reprod 2020, 49, 101698. [Google Scholar] [CrossRef]
- Lisi, F.; Carfagna, P.; Oliva, M.M.; Rago, R.; Lisi, R.; Poverini, R.; Manna, C.; Vaquero, E.; Caserta, D.; Raparelli, V.; et al. Pretreatment with Myo-Inositol in Non Polycystic Ovary Syndrome Patients Undergoing Multiple Follicular Stimulation for IVF: A Pilot Study. Reprod Biol Endocrinol 2012, 10, 52. [Google Scholar] [CrossRef]
- Simmons, D. Diabetes and Obesity in Pregnancy. Best Pract Res Clin Obstet Gynaecol 2011, 25, 25–36. [Google Scholar] [CrossRef]
- Murphy, A.; Shamshirsaz, A.; Markovic, D.; Ostlund, R.; Koos, B. Urinary Excretion of Myo-Inositol and D-Chiro-Inositol in Early Pregnancy Is Enhanced in Gravidas With Gestational Diabetes Mellitus. Reprod Sci 2016, 23, 365–371. [Google Scholar] [CrossRef]
- Corrado, F.; D’Anna, R.; Di Vieste, G.; Giordano, D.; Pintaudi, B.; Santamaria, A.; Di Benedetto, A. The Effect of Myoinositol Supplementation on Insulin Resistance in Patients with Gestational Diabetes. Diabet Med 2011, 28, 972–975. [Google Scholar] [CrossRef]
- Fraticelli, F.; Celentano, C.; Zecca, I.A.; Di Vieste, G.; Pintaudi, B.; Liberati, M.; Franzago, M.; Di Nicola, M.; Vitacolonna, E. Effect of Inositol Stereoisomers at Different Dosages in Gestational Diabetes: An Open-Label, Parallel, Randomized Controlled Trial. Acta Diabetol 2018, 55, 805–812. [Google Scholar] [CrossRef] [PubMed]
- De Grazia, S.; Carlomagno, G.; Unfer, V.; Cavalli, P. Myo-Inositol Soft Gel Capsules May Prevent the Risk of Coffee-Induced Neural Tube Defects. Expert Opin Drug Deliv 2012, 9, 1033–1039. [Google Scholar] [CrossRef] [PubMed]
- Condorelli, R.A.; La Vignera, S.; Bellanca, S.; Vicari, E.; Calogero, A.E. Myoinositol: Does It Improve Sperm Mitochondrial Function and Sperm Motility? Urology 2012, 79, 1290–1295. [Google Scholar] [CrossRef] [PubMed]
- Bizzarri, M.; Fuso, A.; Dinicola, S.; Cucina, A.; Bevilacqua, A. Pharmacodynamics and Pharmacokinetics of Inositol(s) in Health and Disease. Expert Opin Drug Metab Toxicol 2016, 12, 1181–1196. [Google Scholar] [CrossRef] [PubMed]
- Schlemmer, U.; Jany, K.D.; Berk, A.; Schulz, E.; Rechkemmer, G. Degradation of Phytate in the Gut of Pigs--Pathway of Gastro-Intestinal Inositol Phosphate Hydrolysis and Enzymes Involved. Arch Tierernahr 2001, 55, 255–280. [Google Scholar] [CrossRef]
- Caputo, M.; Bona, E.; Leone, I.; Samà, M.T.; Nuzzo, A.; Ferrero, A.; Aimaretti, G.; Marzullo, P.; Prodam, F. Inositols and Metabolic Disorders: From Farm to Bedside. J Tradit Complement Med 2020, 10, 252–259. [Google Scholar] [CrossRef]
- Mukai, T.; Kishi, T.; Matsuda, Y.; Iwata, N. A Meta-Analysis of Inositol for Depression and Anxiety Disorders. Hum Psychopharmacol 2014, 29, 55–63. [Google Scholar] [CrossRef]
- Lepore, E.; Lauretta, R.; Bianchini, M.; Mormando, M.; Di Lorenzo, C.; Unfer, V. Inositols Depletion and Resistance: Principal Mechanisms and Therapeutic Strategies. Int J Mol Sci 2021, 22, 6796. [Google Scholar] [CrossRef]
- Bevilacqua, A.; Bizzarri, M. Inositols in Insulin Signaling and Glucose Metabolism. Int J Endocrinol 2018, 2018, 1968450. [Google Scholar] [CrossRef]
- Montanino Oliva, M.; Buonomo, G.; Calcagno, M.; Unfer, V. Effects of Myo-Inositol plus Alpha-Lactalbumin in Myo-Inositol-Resistant PCOS Women. J Ovarian Res 2018, 11, 38. [Google Scholar] [CrossRef]
Figure 1.
Structures of the nine isomers of inositol.
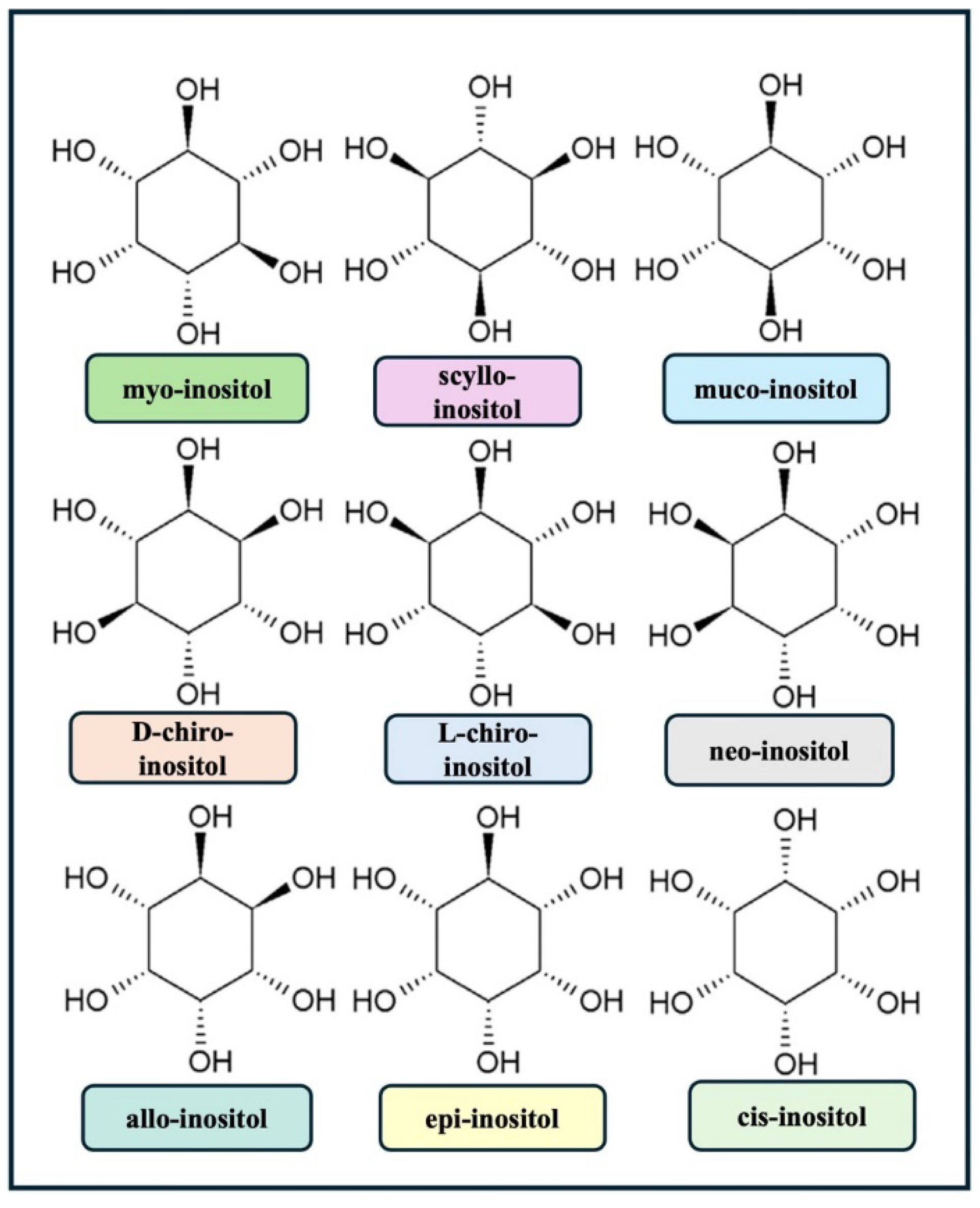
Figure 2.
In physiological conditions, when insulin binds to its receptor, inositol phosphoglycans are hydrolyzed from the cytoplasmic membrane, releasing MYO, which then promotes glucose uptake via the Glut-4 receptor. The enzyme epimerase simultaneously catalyzes the conversion of MYO to DCI, facilitating glycogen synthesis. In cases of insulin resistance, intracellular insulin signaling is down-regulated leading to a systemic shortage of DCI. By contrast, ovaries retain normal insulin sensitivity a phenomenon referred to as the "ovarian paradox". Therefore, in ovaries, hyperglycemic conditions induce an overstimulation of the insulin receptor, which enhances the conversion of MYO to DCI, resulting in an abnormal increase in DCI levels.
Figure 2.
In physiological conditions, when insulin binds to its receptor, inositol phosphoglycans are hydrolyzed from the cytoplasmic membrane, releasing MYO, which then promotes glucose uptake via the Glut-4 receptor. The enzyme epimerase simultaneously catalyzes the conversion of MYO to DCI, facilitating glycogen synthesis. In cases of insulin resistance, intracellular insulin signaling is down-regulated leading to a systemic shortage of DCI. By contrast, ovaries retain normal insulin sensitivity a phenomenon referred to as the "ovarian paradox". Therefore, in ovaries, hyperglycemic conditions induce an overstimulation of the insulin receptor, which enhances the conversion of MYO to DCI, resulting in an abnormal increase in DCI levels.
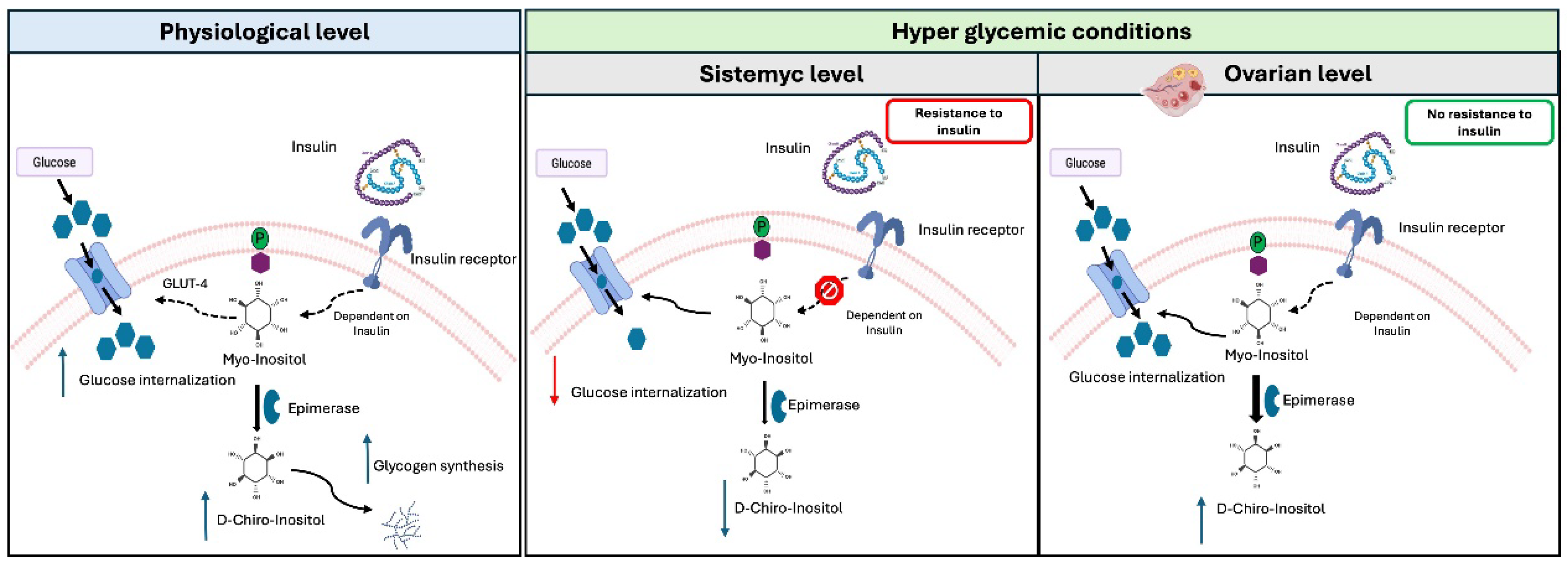
Figure 3.
Classic Rotterdam criteria. A Venn diagram showing the relationship between the four Rotterdam phenotypes. Abbreviations: PCOM, polycystic ovarian morphology.
Figure 3.
Classic Rotterdam criteria. A Venn diagram showing the relationship between the four Rotterdam phenotypes. Abbreviations: PCOM, polycystic ovarian morphology.
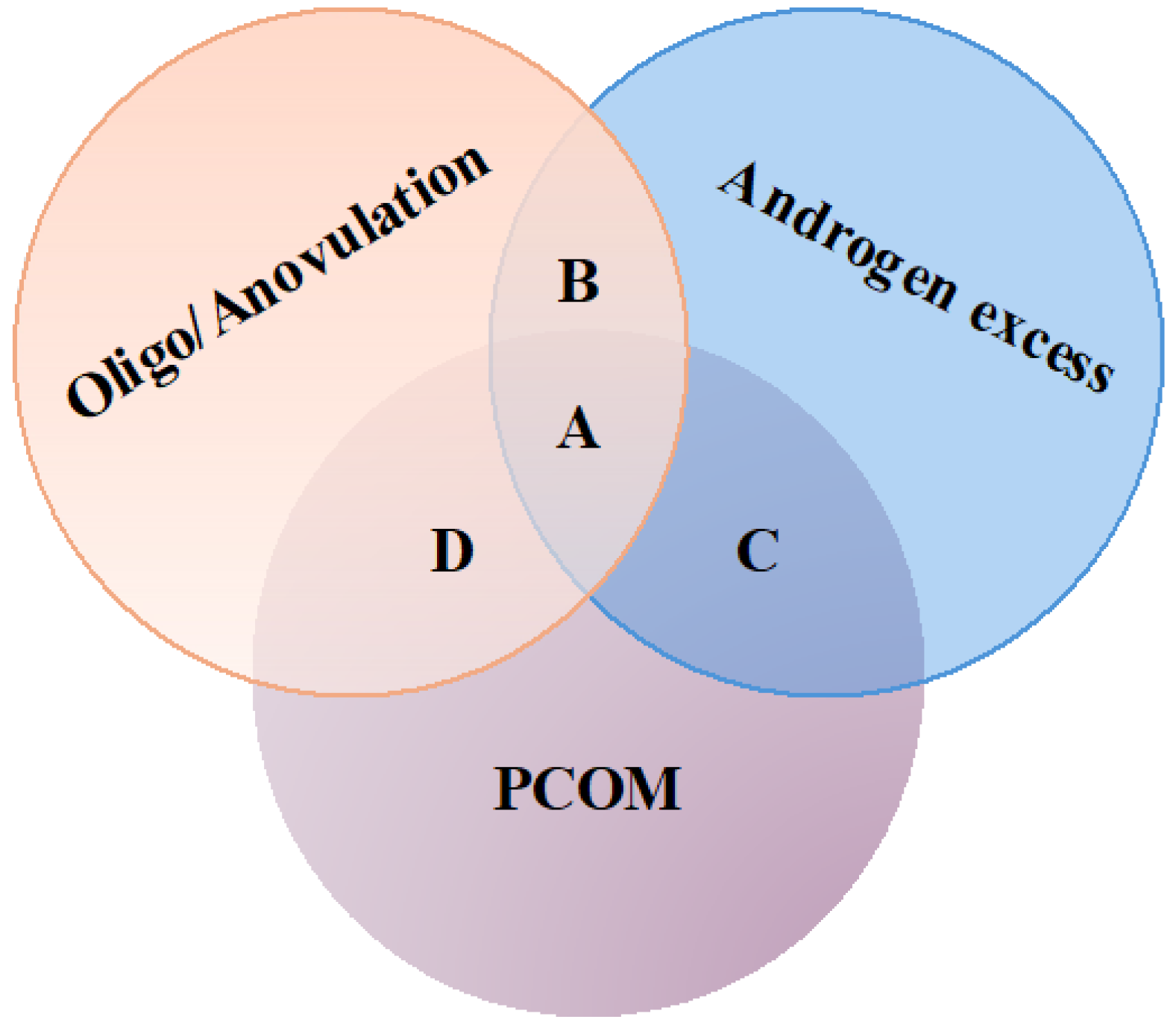

Table 1.
Principal source of inositol.
| Source | Quantity | References |
|---|---|---|
| Cereals | ||
| Rice bran | 7.85-8.52 mg/g | [16] |
| Fruits | ||
| Grapefruit juice | 120g of grapefruit juice provides about 468.8 mg of the compound | [17] |
| Fresh mandarin orange | 3.07 mg/g | [17] |
| Dates, palms, prunes | 46 mg/g | [18] |
| Vegetables | ||
| Lettuce | 1,07 mg/g | [19] |
| White onion | 0.6642 mg/g | [19] |
| Carrots | 2.2–9.8 mg/g | [20] |
| Milk derived products | ||
| Bovine milk | 5.3-8.7 mg/100 ml | [21] |
| Sweetened condensed milk | 0.26 mg/g | [22] |
| Meat | ||
| Beef liver | 0.64 mg/g | [17] |
| Legumes | ||
| Soybean | 1.22 mg/g in pod, 8 mg/g in seed | [12] |
| Dried fruit | ||
| Pine nuts | 0.7 mg/g | [23] |
| Peanut butter | 3.04 mg/g | [17] |
| Almond | 2.78 mg/g | [17] |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



