Submitted:
22 October 2024
Posted:
23 October 2024
You are already at the latest version
Abstract
Vulvar carcinoma is a rare disease, meeting the criteria of a “rare cancer”. The incidence has been increasing, especially in women <60 years of age. Squamous cell carcinoma (VSCC) accounts for an overwhelming majority of vulvar carcinomas and is the focus of this review. As with many cancers, the increased understanding of molecular events during tumorigenesis has led to emergence of molecular subclassification of VSCC, which is subclassified into those tumors arising secondary to high risk human papillomavirus infection (HPV associated, or HPVa) and those which arise independent of HPV (HPVi), most commonly in the setting of a chronic inflammatory condition of the vulvar skin. This latter group of HPVi VSCC arises in most cases secondary to mutations in TP53, but recently attention has focused on the uncommon TP53 wildtype HPVi VSCC. These three molecular subtypes of VSCC (HPVa, HPVi p53 abnormal, HPVi p53 wild type), and their precursor lesions, cannot be diagnosed based on routine histopathological examination and immunostaining for p53 and p16, as surrogate markers for TP53 mutation and high-risk HPV infection, respectively, is essential. Molecular subtyping of VSCC shows high reproducibility and provides important prognostic information. The HPVa VSCC have the most favorable prognosis while the HPVi VSCC with TP53 mutations (p53abn) have the worst prognosis, and the HPVi VSCC with wild type TP53 (p53wt) have an intermediate prognosis. In this review, we discuss the evidence supporting this molecular subclassification and its implications for diagnosis and treatment of VSCC and its precursors.
Keywords:
Vulvar cancer
; squamous cell carcinoma
; p53
; p16
; human papillomavirus
; molecular
; classification
; prognosis
; radiation therapy
; surgery
Introduction
Vulvar cancer (VC) is an uncommon disease [1] and meets the criteria for „rare cancer“ according to the definition of the European Society for Medical Oncology: i.e. cancer with an incidence of <6 per 100.000 per year [2,3]. VC accounts for about 5.6% of all gynecologic malignancies with 6.470 estimated new cases for 2023 in the US [4]. An Australian study reported an 84% increase in the incidence from 1982-1984 to 2007-2009 in women younger than 60 years with no change in the VC incidence in women 60+ years [5,6]. Comparing the cancer registry data from 13 high-income countries over a 20-year period, Kang et al. [6] reported an overall increase of 4.6%, with an increase of 11.6% in women <60 years of age, but no change was in women aged 60+ years.
There has been no recent change in the overall survival of vulvar cancer patients [7]. Regardless of tumor stage and treatment approaches, an analysis of the SEER-data sets between 2000 and 2007 reported a 5-year overall survival of 60.6% (45.7% at 10 years and 33.1% at 15 years) [8]. The vast majority of VC are squamous cell carcinomas (VSCC); [8,9,10]. Within that histologic subtype, the most important development during the last 10 years has been the recognition of distinct histopathogenetic pathways [9,10,11,12]; these pathways are associated with distinct precursor lesions, different responses to treatment, and different outcomes [11,13,14,15,16,17,18,19,20,21]. Here, we summarize the clinicopathologic features of the different molecular subtypes of VSCC, including their impact on diagnosis and treatment.
Molecular Subtypes of VSCC
Although it has been recognized that VSCC can be either associated with high-risk human papillomavirus infection (HPVa) infection, or independent of HPV (HPVi) since the early 1990s [22,23], it has only recently been appreciated that VSCC and squamous cell carcinomas at other body sites e.g. the oropharynx [24,25,26], differ significantly from HPVi squamous cell carcinomas arising at the same body site. It is only in the 5th edition of the WHO Classification of Female Genital Tumours [27] that VSCC and its precursor lesions were subclassified as HPVi or HPVa (Figure 1a; [27]).
The move from the previously morphology-based classification of VSCC to an etiology/molecular-based classification (Figure 1b) allows for more precise prognostication characterisation [10,12,13,17] and also happened for cervical squamous cell carcinomas and adenocarcinomas. (Figure 1a and b; [27](). This change was subsequently adopted by the International Collaboration on Cancer Reporting (ICCR; [28]), the College of American Pathologists [28,29], as well as by the most recent update of the guidelines of the European Society of Gynaecological Oncology for the management of patients with vulvar cancer [30].
The molecular subclassification of VSCC defines at least two distinct subtypes (for details and diagnostic approach please see below; Figure 1b). Briefly, the first, most common but aggressive molecular subtype is HPV-independent and associated with a TP53-mutation, and consequent resulting in an aberrant p53-protein expression on immunohistochemistry. The second, less common but also less aggressive subtype with a better prognosis, is HPV-associated and based on an associated with high-risk HPV infection, showing shows a better prognosis and p16-protein overexpression [9,10,13,15].
This molecular subclassification has been implemented at sites outside the female genital tract where there is HPVa squamous cell carcinoma, e.g. penis [31] as well as head and neck cancers [26,32,33,34]. While most HPVi VSCC have mutations in TP53, associated with mutation pattern expression of p53 protein on immunostaining, Sand et al. [35] evaluated p16 and p53 expression in 18 studies of VSCC and found that 54% of the tumors were HPVi with mutation pattern p53 expression and 38% were HPVa with immunohistochemical p16 overexpression, however, 8% of VSCC are neither p16 negative with mutant pattern p53, or p16 positive with wild type 53, and this points to a third molecular subtype of VSCC i.e. HPVi (p16 negative) and p53 wild type.
Nooji et al. [36] first reported on this third molecular subtype of VSCC. They performed a targeted NGS-analysis of VSCC and its precursors and found a higher frequency of NOTCH1- and HRAS-mutations in HPVi p53wt VSCC compared to HPVi p53abn VSCC; the authors therefore suggested that NOTCH1- and HRAS-mutations might act as driver mutational events independent of TP53 which was later supported by another study [14]). Furthermore, high rates (up to 71%) of NOTCH1-mutations have been reported to occur in penile cancer, a male tumor with many similarities to VSCC [37].
The prognosis of the three molecular subtypes of VSCC (HPVa, HPVi p53abn and HPVi p53wt) has shown that HPVa VSCC has the most favorable prognosis, HPVi p53abn the worst prognosis, and HPVi p53wt an intermediate prognosis [12,17,36,38] and molecular analyses were performed [14,36]. As a result, there is growing acceptance of routine classification of VSCC and its precursors into one of these three molecular subtypes (see Figure 2).
Diagnosis of Molecular Subtypes of VSCC
The molecular subclassification of VSCC is based on a routine use of molecular markers, specifically immunostaining for both p53 and p16 in all cases. Ambiguous staining results may require additional in situ-analyses for HPV and/ or TP53 sequencing.
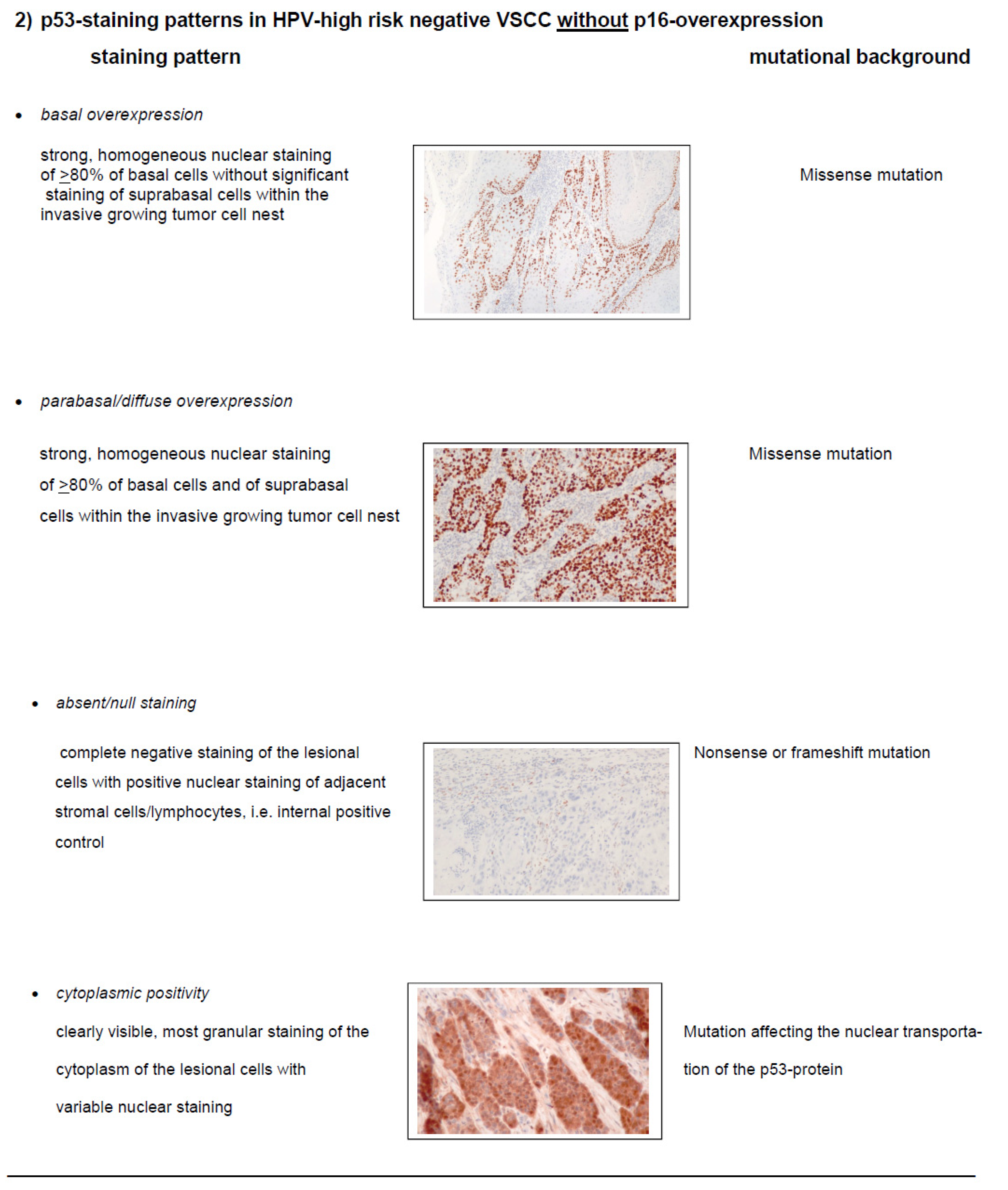
The immunohistochemical evaluation of p53 is performed as a pattern-based analysis rather than a simple positive or negative staining. The different staining patterns are summarized in Table 1, and when interpreted according to these recommendations shows a strong correlation with TP53 mutational status.

Immunohistochemical staining for p16 has been recommended, as a surrogate marker of high risk HPV infection, as part of the routine stratification of VSCC by the International Collaboration on Cancer Reporting (ICCR), the International Federation of Gynecology and Obstetrics (FIGO) and the WHO [1,13,16,27,28,39,40].
Within vulvar intraepithelial neoplasia (VIN) lesions, p16 is considered overexpressed when there is a block-like staining, i.e. strong nuclear and cytoplasmic staining of all lesional cells from the basal layer upwards through at least one-third of the epithelial thickness [41,42]. In invasive or metastatic VSCC, p16 overexpression is recognized when moderate or intense nuclear and cytoplasmic staining is detected in 70% or more of the tumor cells [9,42]. That interpretation of p16-staining in invasive carcinoma is based on the recommendations for head and neck squamous cell carcinoma by the American Society of Clinical Oncology and the College of American Pathologists [25]. Foci of keratinization within the VSCC should be excluded from consideration (Figure 3, [9]).
Accuracy of Molecular Subclassification of VSCC
Given its concordance with in situ-detection methods for HPV of up to 100%, p16-overexpression is considered a reliable surrogate marker for high-risk HPV infection [38,39,43,44]. The above mentioned p16-immunostaining has been reported to have a sensitivity of 97.4% to 100% and a specificity of 96.6% to 98.7% for assessment of HPV status [13,40]. Very rarely, complete absence of p16-overexpression may be seen in HPVa carcinomas of the lower female genital tract [45]; this may be caused by loss of heterozygosity [46], rarely by point-mutations of the p16-gene or silencing of the gene by promotor hypermethylation [47].
In VSCC p53 immunostaining interpretation has to be performed using a pattern-based analysis, defining two wildtype and four aberrant staining patterns (see Table 1). The aberrant p53-patterns show a strong correlation with TP53 sequencing analyses in VSCC (95% agreement) [15]. Another study reported a 97% accuracy of p53 immunostaining to predict TP53 mutations in VSCC [48].
It is important to note that molecular classification is not possible based on hematoxylin-and-eosin stained slides [16,18,40,49]. Therefore, the use of p16 and p53 immunohistochemistry is necessary for the correct molecular subtyping of VSCC. Using the combination of these two immunostains to diagnose the three different molecular subtypes (Figure 2). Yang et al. [13] reported that 95.6% (215/225) of VSCC could be readily classified as one of the three subtypes by using p16- and p53-immunostaining alone. Thompson et al. [19] demonstrated a good interobserver correlation for the immunohistochemical classification of VSCC into one of three molecular subtypes using p16 and p53 immunohistochemistry, with a kappa value of 0.74. In cases with ambiguous immunohistochemical staining results, it is sometimes necessary to examine more than one area of the tumor, and more than one tissue block [13]. Importantly, immunohistochemistry for p53 and p16 is inexpensive, readily available, represents a robust method with a standardised technical work-up, and the results are usually available within 24 hours [16,18].
In cases with ambiguous staining results (<5% of the cases), additional molecular evaluation may be required [13]. An algorithmic approach to use of further molecular testing (in situ hybridization or sequencing) as suggested by Yang et al. [13] is summarized in Figure 4.
One final consideration in molecular subtyping of VSCC is, that HPV high risk-negative but p53abn VSCC may show both immunohistochemical overexpression of p16 and mutant pattern p53 expression, so called double-positivity. The frequency of these cases ranges between 0% [21,50], 4.2% [13] and 6.8% [51] and may be underestimated at this time. With regards to the mechanism of double positivity, p16 is frequently overexpressed in high-grade serous ovarian cancer, and <1% of these tumors harbor a CDKN2A mutation, so that the p16 overexpression is thought to be secondary to dysregulation secondary to underlying p53 and/or Rb mutations [52]. In VSCC, Yang et al. [13] reported a CDKN2A (frameshift) mutation in two out of five of their double-positive cases. Clearly, the reason for double-positive staining in VSCC requires further research but the small number of cases reported to date suggests that the combination of p16 positivity and mutant pattern p53 staining is usually seen in HPVi p53abn VSCC.
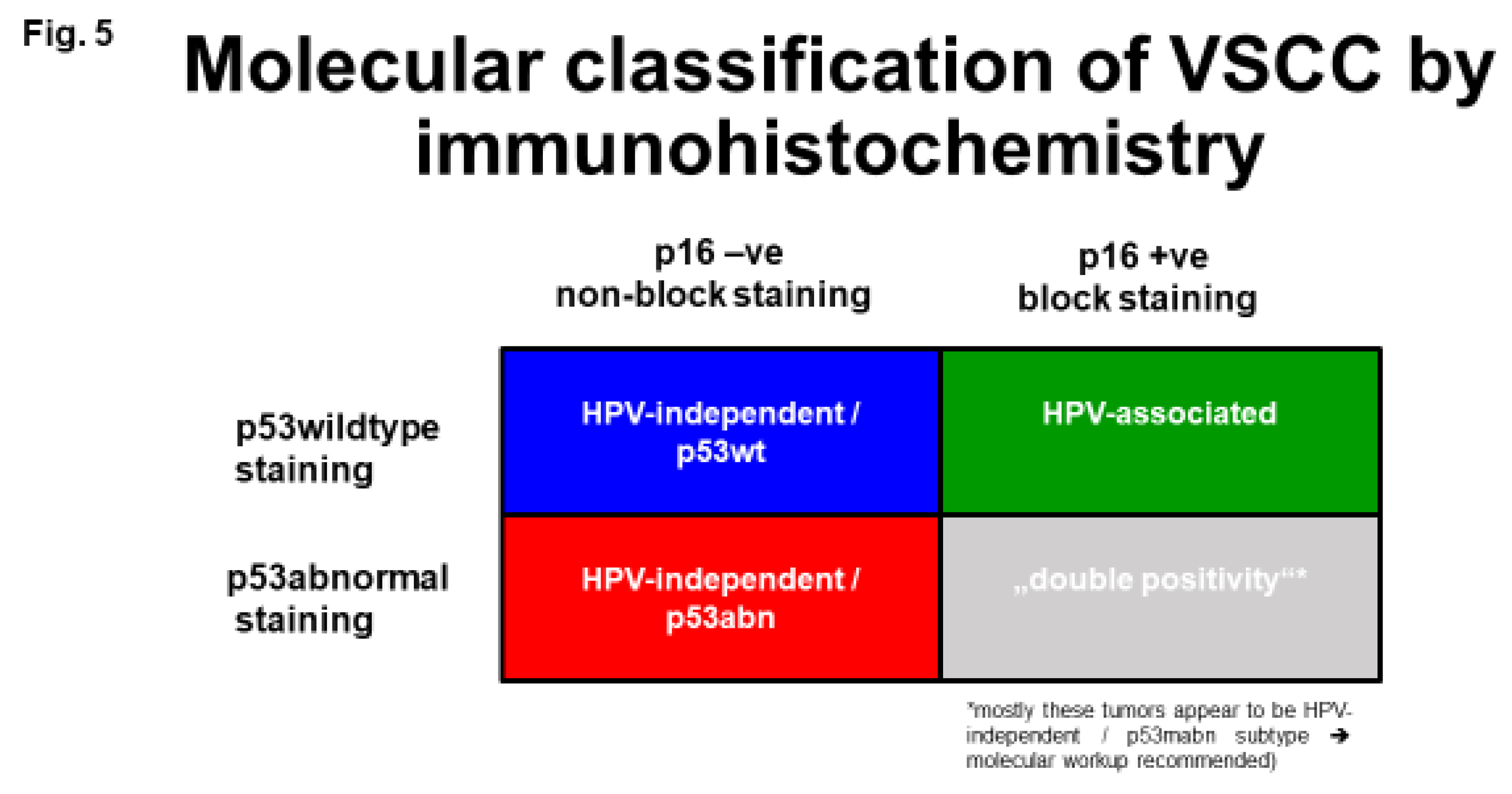
Figure 5.
Immunohistochemical classification of VSCC in its molecular subtypes (for details please see text and Figure 4 and Figure 6, Table 1).
Prognostic Impact of Molecular Subtyping
It is now accepted that the HPV status of VSCC is associated with a highly significant impact on prognosis (e.g. [16,18,19,35,50,51,54,55] and has been the subject of two meta-analyses. Cao et al. [56] reported a higher overall survival (RR = 0.53, (95%CI [0.35-0.80]; p=0.003) for HPVa/p16-positive tumors. Sand et al. [35] reported a pooled hazard ratio of 0.40 (95% CI [0.29-0.55]) for p16-positive VSCC and of 1.81 (95% CI [1.22-2.68]) for tumors with mutant pattern p53 expression tumors.
McAlpine et al. [18] reported a significantly worse survival in HPVi, p53-driven VSCC in the era after moving away from en-bloc radical vulvectomy. The study (n=197) compared two surgical approaches: radical vulvectomy with en- bloc resection of the vulva and groins (called long-horn-excision; group 1) versus a localised radical vulvectomy with separate incisions for vulva and both groins (so called triple incision; group 2). HPVa tumors were shown to have a superior progression-free (HR 0.17; p<0.001), disease-specific (HR 0.08; p<0.001) and overall survival (HR 0.24; p<0.001) in the group treated with less radical surgery. In contrast, no prognostic relevance of HPV-status observed in the group treated with the more radical surgical approach. 30-40% of the patients received adjuvant radiation therapy in both groups, with no reported inter-group differences in the radiation technique. With the radical surgical technique of a vulvar field resection (VFR), the extent of the resection (partial, total or extended) and regional lymph node sampling is based on the understanding of embryonic and fetal development, aiming to resect the ontogenetic cancer field. Early evidence showed that VFR without adjuvant radiotherapy compares favorably to standard multimodal treatment [64]. The study of Thompson et al. [19] reported equivalent outcomes in HPVa and HPVi p53abn VSCCs treated with the VFR-based surgical approach. These results are consistent with the previous study of McAlpine et al. [18] and the hypothesis that a radical primary resection leads to an improved outcome for those patients with a high-risk molecular subtype of VSCC i.e. HPVi p53abn. Ultimately, however, a prospective clinical trial of different surgical approaches is needed to adequately test the hypothesis that more radical surgery leads to an improved outcome for patients with HPVi VSCC and that equivalently favorable outcomes can be achieved in selected cases of younger patients with HPVa VSCC through less aggressive surgery with adjuvant radiotherapy.
With regards to adjuvant radiotherapy, Dohopolski et al. [57] examined 39 patients with adjuvant external beam (chemo-) RT and reported an in-field relapse rate of 72.2% for HPVi and 59.1% for HPVa tumors (p=0.062) as well as a five-year progression-free survival of 22.1% versus 63.5% (p=0.072). Two other studies mainly included patients treated with adjuvant radiation only. Yap et al. ([58] ; 26/40 with adjuvant RT only) described a locoregional relapse rate of 81.2% for HPVi versus 15.4% for HPVa VSCC (p=0.003). Similar results were reported by Lee et al. ( [59]; 28/57 with adjuvant RT only), with a local recurrence rate of 75% versus 19% (p<0.01). Twenty-four of 75 patients in the study of Lindell et al. [60] underwent adjuvant RT and showed a significantly better recurrence-free, disease-specific and overall survival in HPVa tumors (p<0.03). In a cohort of 73 patients with a median tumor size of 5.0 cm treated initially with radiotherapy, a complete clinical response rate of 63.6% was reported in HPVa versus 35.0% in HPVi VSCC [51]. In patients with a neoadjuvant treatment approach (n=63) the pathologic complete response rate was 53.8% versus 31.4% (p=0.067, HPVa/p16+ve versus HPVi/p16-ve, respectively). Proctor et al. [54] reported a higher complete clinical response rate in 48 patients with definitive (chemo-) radiation for HPVa (72.2%) versus 42.9% in HPVi VSCC. A case of a HPVa VSCC with a dramatic clinical response to chemoradiation is illustrated in Figure 7. It should be noted that these studies, while strongly suggesting a difference in radiosensitivity between HPVa and HPVi VSCC, are retrospective and there are not randomized prospective studies of VSCC where molecular subtype has been determined.
HPV-Independent, p53 Wild Type VSCC: Clinical Features
Most studies exploring the prognostic impact of molecular subtypes in VSCC have not subdivided the HPVi VSCC into p53abn and p53wt, so that data comparing all three molecular subtypes are still limited. Some studies exclude HPVi p53wt tumors from the analyses because of their rarity [19]. Both, Hinten et al. [11] and Barlow et al. [17] reported details of HPVi p53wt tumors that molecular subtype only within the supplementary material, not within the main analyses.
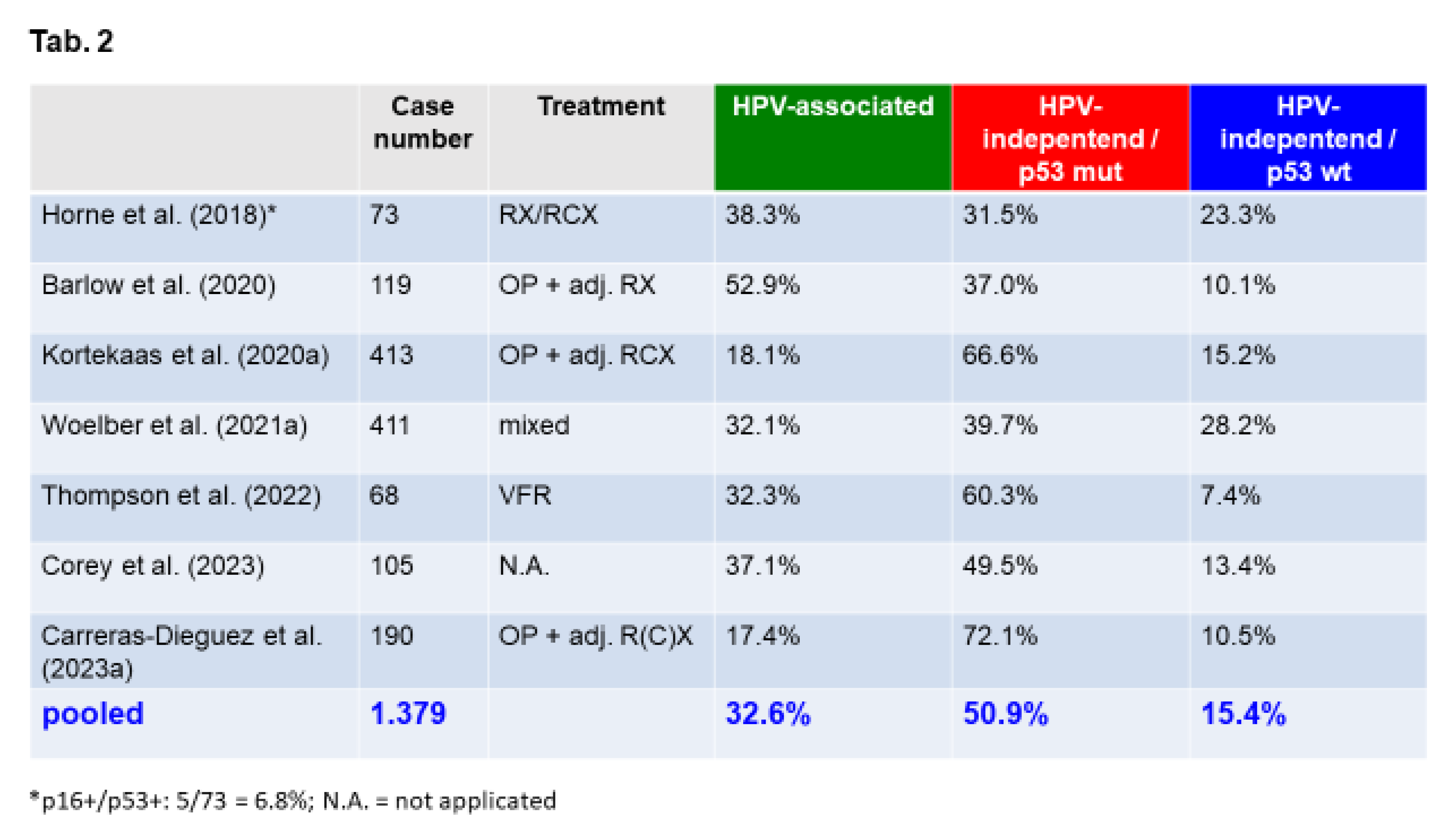
As noted previously, HPVi p53wt is the least common of the three subtypes (see Table 2).
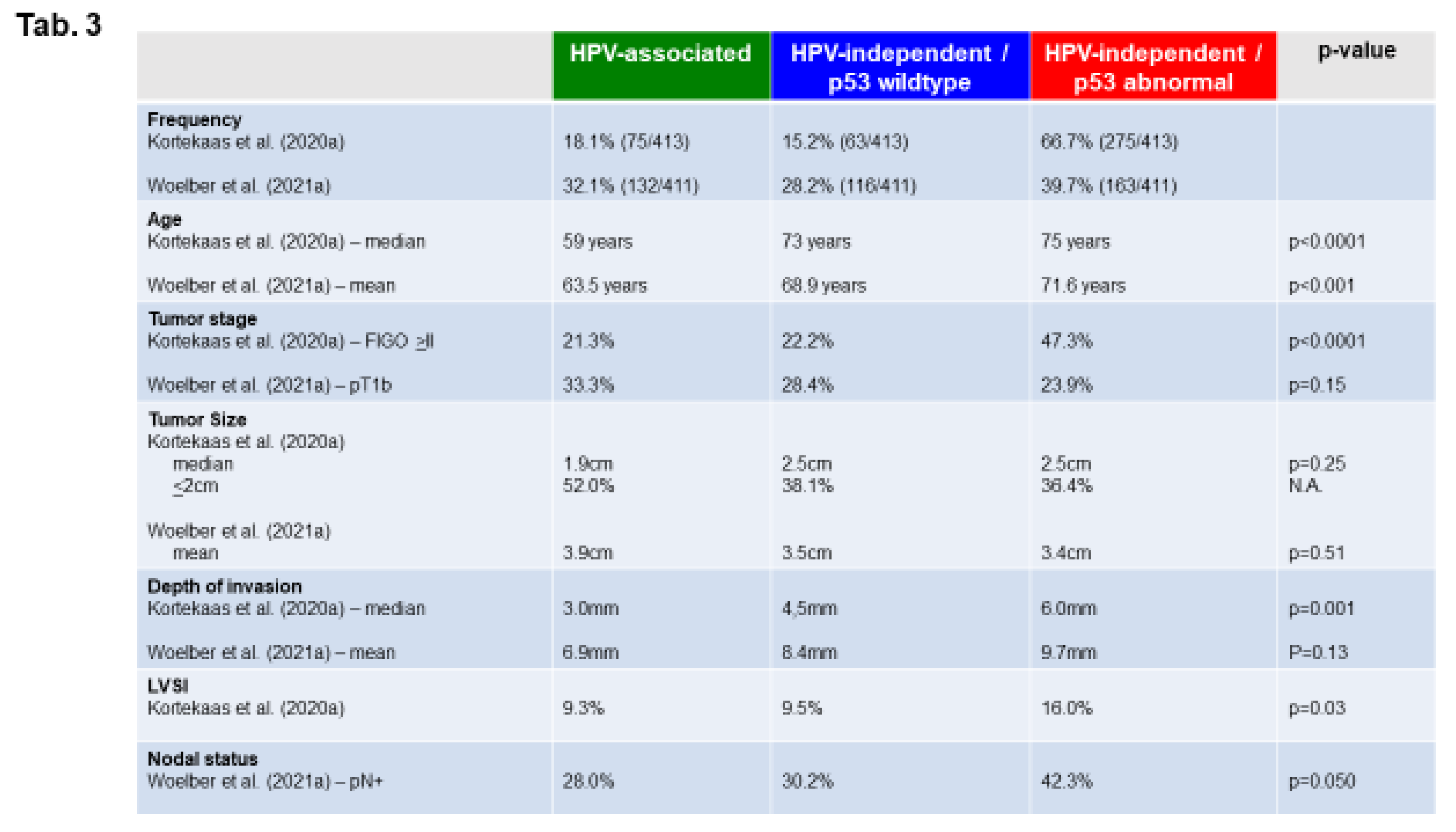
To illustrate the clinicopathologic findings for the tree-tiered molecular classification of VSCC, Table 3 summarizes the results of two recent large studies analysing n=413 cases [12] and n=411 cases [38], respectively.
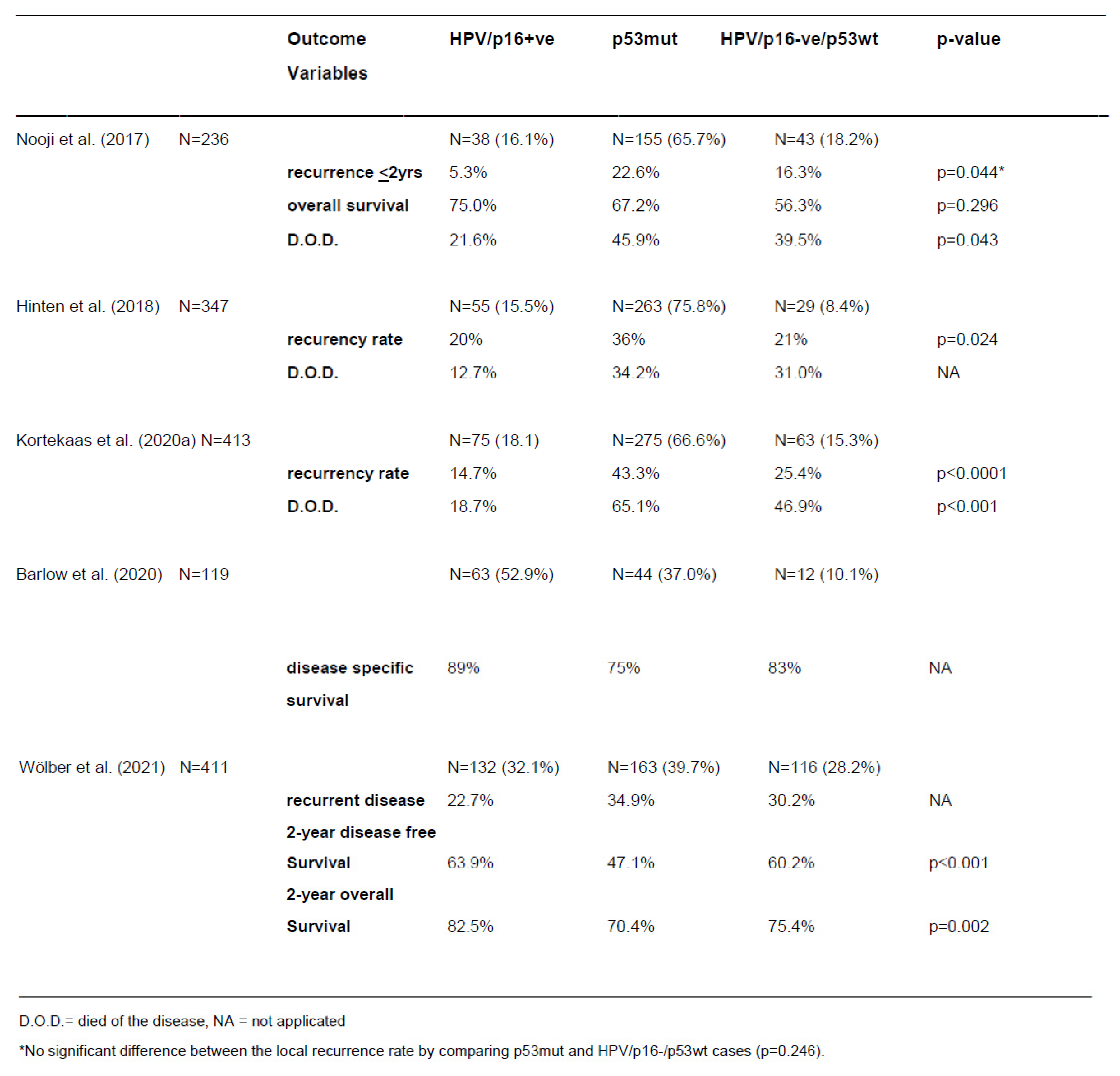
Nooji et al. [36] evaluated a series of 236 VSCC and reported a three times higher rate of local recurrence in HPVi p53wt and four times higher recurrence rate in HPVi p53abn VSCC compared to HPVa cancers (p=0.044). There was better overall survival at 5 years in HPVa VSCC compared to HPVi p53wt (HR 2.16; p=0.049) or HPVi p53abn VSCC (HR 3.43; p<0.001) in the study of Kortekaas et al. [12]). Comparing the two HPVi molecular subtypes, p53wt VSCC also had a better 5-year overall survival than p53abn tumors (HR 0.63; p=0.06), and p53wt tumors showed a longer recurrence-free period compared to p53abn VSCC (HR 0.43; p=0.003; [12]). In multivariate analysis, the three-tiered molecular classification of VSCC correlated significantly with the risk of recurrence irrespective of other clinicopathologic factors (e.g. tumor stage, tumor size, depth of invasion, inguinal lymph node involvement). Interestingly, recurrent disease occurred locally in all three molecular subtypes.
Table 4 summarizes the prognostic data for the three-tiered molecular classification of VSCC extracted obtained from the literature.
Future Directions
Different targeted treatment approaches have been reported for VSCC (e.g. targeting EGFR (erlotinib), VEGF (bevacizumab), PD-L1 (pembrolizumab; [62])). However, treatment results of targeted therapy in VSCC are currently too limited to know if the different molecular subtypes can guide targeted therapy choices [30,62,63]. Evaluating biomarkers related to immune checkpoint therapy Corey et al. [21] reported no significant differences in mismatch repair defiency (dMMR/MSI-H), tumor mutational burden and PD-L1-expression within the three different molecular subtypes.
There are some results showing that the NOTCH-pathway may serve as a potential therapeutic target [37] through its inhibition by the sarco-endoplasmic reticulum Ca2+-ATPase (SERCA) modulators [64]. The recently described third molecular pathway of VSCC may therefore be targetable by SERCA-modulators. Additionally, HRAS mutations are prevalent within the molecular pathway of HPVi p53wt VSCC [36]. HRAS is involved in the RTK/RAS/PIK3-CA-pathway, targetable by selective mTOR-inhibitors [65]. Treatment recommendations based on the molecular subtyping are not in the most recent update of the guidelines of the European Society of Gynaecological Oncology for the management of patients with vulvar cancer [30], but for this to happen there will first have to be incorporation of molecular subtyping of VSCC into future studies.
Conclusions
In more than 95% of cases, VSCC can be reliably subclassified reliably into one of three different molecular subtypes by immunohistochemistry alone [13,48,53]. Immunostaining for both p16 AND p53 is required for molecular subtype diagnosis [13,16] and attention to recent improvements in interpretation of both of these immunomarkers is critical (see Table 1 and Figure 5 and Figure 6) [39,53,66,67]. While the molecular subtypes of VSCC are of prognostic significance, more data is needed in order to assess whether molecular subtype can guide extent of surgery or choice of adjuvant therapy as is the case with molecular classifcation of other tumors types such as breast or endometrial carcinoma. Generating such data will be facilitated with routine accurate molecular classification of all VSCC; this is particularly critical for cases included in research studies/clinical trials. The impact of the three-tiered molecular subclassification of VSCC is schematically summarized in Figure 8.
References
- Olawaiye, A.B.; Cuello, M.A.; Rogers, L.J. Cancer of the vulva: 2021 update. Int. J. Gynaecol. Obstet. 2021, 155 Suppl 1, 7–18. [Google Scholar] [CrossRef]
- Gatta, G.; Capocaccia, R.; Trama, A.; Martínez-García, C. The burden of rare cancers in Europe. Adv. Exp. Med. Biol. 2010, 686, 285–303. [Google Scholar] [CrossRef] [PubMed]
- Eslick, G.D. What is a Rare Cancer? Hematol. Oncol. Clin. North Am. 2012, 26, 1137–1141. [Google Scholar] [CrossRef] [PubMed]
- Siegel, R.L.; Miller, K.D.; Wagle, N.S.; Jemal, A. Cancer statistics, 2023. CA Cancer J. Clin. 2023, 73, 17–48. [Google Scholar] [CrossRef] [PubMed]
- Barlow, E.L.; Kang, Y.-J.; Hacker, N.F.; Canfell, K. Changing Trends in Vulvar Cancer Incidence and Mortality Rates in Australia Since 1982. Int. J. Gynecol. Cancer 2015, 25, 1683–1689. [Google Scholar] [CrossRef]
- Kang, Y.-J.; Smith, M.; Barlow, E.; Coffey, K.; Hacker, N.; Canfell, K. Vulvar cancer in high-income countries: Increasing burden of disease. Int. J. Cancer 2017, 141, 2174–2186. [Google Scholar] [CrossRef]
- Mancini, S.; Bucchi, L.; Zamagni, F.; Baldacchini, F.; Crocetti, E.; Giuliani, O.; Ravaioli, A.; Vattiato, R.; Preti, M.; Tumino, R.; et al. Trends in Net Survival from Vulvar Squamous Cell Carcinoma in Italy (1990-2015). J. Clin. Med. 2023, 12. [Google Scholar] [CrossRef]
- Scampa, M.; Kalbermatten, D.F.; Oranges, C.M. Squamous Cell Carcinoma of the Vulva: A Survival and Epidemiologic Study with Focus on Surgery and Radiotherapy. J. Clin. Med. 2022, 11. [Google Scholar] [CrossRef]
- Singh, N.; Gilks, C.B. Vulval squamous cell carcinoma and its precursors. Histopathology 2020, 76, 128–138. [Google Scholar] [CrossRef]
- Wei, K.X.; Hoang, L.N. Squamous and Glandular Lesions of the Vulva and Vagina: What's New and What Remains Unanswered? Surg. Pathol. Clin. 2022, 15, 389–405. [Google Scholar] [CrossRef]
- Hinten, F.; Molijn, A.; Eckhardt, L.; Massuger, L.F.A.G.; Quint, W.; Bult, P.; Bulten, J.; Melchers, W.J.G.; Hullu, J.A. de. Vulvar cancer: Two pathways with different localization and prognosis. Gynecol. Oncol. 2018, 149, 310–317. [Google Scholar] [CrossRef] [PubMed]
- Kortekaas, K.E.; Bastiaannet, E.; van Doorn, H.C.; van Vos Steenwijk, P.J. de; Ewing-Graham, P.C.; Creutzberg, C.L.; Akdeniz, K.; Nooij, L.S.; van der Burg, S.H.; Bosse, T.; et al. Vulvar cancer subclassification by HPV and p53 status results in three clinically distinct subtypes. Gynecol. Oncol. 2020, 159, 649–656. [Google Scholar] [CrossRef] [PubMed]
- Yang, H.; Almadani, N.; Thompson, E.F.; Tessier-Cloutier, B.; Chen, J.; Ho, J.; Senz, J.; McConechy, M.K.; Chow, C.; Ta, M.; et al. Classification of Vulvar Squamous Cell Carcinoma and Precursor Lesions by p16 and p53 Immunohistochemistry: Considerations, Caveats, and an Algorithmic Approach. Mod. Pathol. 2023, 36, 100145. [Google Scholar] [CrossRef] [PubMed]
- Salama, A.M.; Momeni-Boroujeni, A.; Vanderbilt, C.; Ladanyi, M.; Soslow, R. Molecular landscape of vulvovaginal squamous cell carcinoma: new insights into molecular mechanisms of HPV-associated and HPV-independent squamous cell carcinoma. Mod. Pathol. 2022, 35, 274–282. [Google Scholar] [CrossRef]
- Tessier-Cloutier, B.; Pors, J.; Thompson, E.; Ho, J.; Prentice, L.; McConechy, M.; Aguirre-Hernandez, R.; Miller, R.; Leung, S.; Proctor, L.; et al. Molecular characterization of invasive and in situ squamous neoplasia of the vulva and implications for morphologic diagnosis and outcome. Mod. Pathol. 2021, 34, 508–518. [Google Scholar] [CrossRef]
- Allo, G.; Yap, M.L.; Cuartero, J.; Milosevic, M.; Ferguson, S.; Mackay, H.; Kamel-Reid, S.; Weinreb, I.; Ghazarian, D.; Pintilie, M.; et al. HPV-independent Vulvar Squamous Cell Carcinoma is Associated With Significantly Worse Prognosis Compared With HPV-associated Tumors. Int. J. Gynecol. Pathol. 2020, 39, 391–399. [Google Scholar] [CrossRef]
- Barlow, E.L.; Lambie, N.; Donoghoe, M.W.; Naing, Z.; Hacker, N.F. The Clinical Relevance of p16 and p53 Status in Patients with Squamous Cell Carcinoma of the Vulva. J. Oncol. 2020, 2020, 3739075. [Google Scholar] [CrossRef]
- McAlpine, J.N.; Leung, S.C.Y.; Cheng, A.; Miller, D.; Talhouk, A.; Gilks, C.B.; Karnezis, A.N. Human papillomavirus (HPV)-independent vulvar squamous cell carcinoma has a worse prognosis than HPV-associated disease: a retrospective cohort study. Histopathology 2017, 71, 238–246. [Google Scholar] [CrossRef]
- Thompson, E.F.; Hoang, L.; Höhn, A.K.; Palicelli, A.; Talia, K.L.; Tchrakian, N.; Senz, J.; Rusike, R.; Jordan, S.; Jamieson, A.; et al. Molecular subclassification of vulvar squamous cell carcinoma: reproducibility and prognostic significance of a novel surgical technique. Int. J. Gynecol. Cancer 2022, 32, 977–985. [Google Scholar] [CrossRef]
- Carreras-Dieguez, N.; Saco, A.; del Pino, M.; Pumarola, C.; Del Campo, R.L.; Manzotti, C.; Garcia, A.; Marimon, L.; Diaz-Mercedes, S.; Fuste, P.; et al. Vulvar squamous cell carcinoma arising on human papillomavirus-independent precursors mimicking high-grade squamous intra-epithelial lesion: a distinct and highly recurrent subtype of vulvar cancer. Histopathology 2023, 82, 731–744. [Google Scholar] [CrossRef]
- Corey, L.; Wallbillich, J.J.; Wu, S.; Farrell, A.; Hodges, K.; Xiu, J.; Nabhan, C.; Guastella, A.; Kheil, M.; Gogoi, R.; et al. The Genomic Landscape of Vulvar Squamous Cell Carcinoma. Int. J. Gynecol. Pathol. 2023, 42, 515–522. [Google Scholar] [CrossRef] [PubMed]
- Kurman, R.J.; Toki, T.; Schiffman, M.H. Basaloid and warty carcinomas of the vulva. Distinctive types of squamous cell carcinoma frequently associated with human papillomaviruses. Am. J. Surg. Pathol. 1993, 17, 133–145. [Google Scholar] [CrossRef] [PubMed]
- Toki, T.; Kurman, R.J.; Park, J.S.; Kessis, T.; Daniel, R.W.; Shah, K.V. Probable nonpapillomavirus etiology of squamous cell carcinoma of the vulva in older women: a clinicopathologic study using in situ hybridization and polymerase chain reaction. Int. J. Gynecol. Pathol. 1991, 10, 107–125. [Google Scholar] [CrossRef] [PubMed]
- Giannella, L.; Di Giuseppe, J.; Delli Carpini, G.; Grelloni, C.; Fichera, M.; Sartini, G.; Caimmi, S.; Natalini, L.; Ciavattini, A. HPV-Negative Adenocarcinomas of the Uterine Cervix: From Molecular Characterization to Clinical Implications. Int. J. Mol. Sci. 2022, 23. [Google Scholar] [CrossRef] [PubMed]
- Fakhry, C.; Lacchetti, C.; Rooper, L.M.; Jordan, R.C.; Rischin, D.; Sturgis, E.M.; Bell, D.; Lingen, M.W.; Harichand-Herdt, S.; Thibo, J.; et al. Human Papillomavirus Testing in Head and Neck Carcinomas: ASCO Clinical Practice Guideline Endorsement of the College of American Pathologists Guideline. J. Clin. Oncol. 2018, 36, 3152–3161. [Google Scholar] [CrossRef]
- Perri, F.; Longo, F.; Caponigro, F.; Sandomenico, F.; Guida, A.; Della Vittoria Scarpati, G.; Ottaiano, A.; Muto, P.; Ionna, F. Management of HPV-Related Squamous Cell Carcinoma of the Head and Neck: Pitfalls and Caveat. Cancers (Basel) 2020, 12. [Google Scholar] [CrossRef]
- Lokuhetty, D.; White, V.A.; Watanabe, R. Female genital tumours, 5. edition, 2020, ISBN 9789283245049.
- Hoang, L.; Webster, F.; Bosse, T.; Focchi, G.; Gilks, C.B.; Howitt, B.E.; McAlpine, J.N.; Ordi, J.; Singh, N.; Wong, R.W.-C.; et al. Data Set for the Reporting of Carcinomas of the Vulva: Recommendations From the International Collaboration on Cancer Reporting (ICCR). Int. J. Gynecol. Pathol. 2022, 41, S8–S22. [Google Scholar] [CrossRef]
- Krishnamurti, U.G.; Crothers, B.A.; Otis, C.N.; Birdsong, G.G.; Movahedi-Lankarani, S.; Klepeis, V. Protocol for the Examination of Specimens From Patients With Primary Carcinoma of the Vulva. Available online: chrome-extension://efaidnbmnnnibpcajpcglclefindmkaj/https://documents.cap.org/protocols/Vulva_4.2.0.0.REL_CAPCP.pdf (accessed on 27 November 2023).
- Oonk, M.H.M.; Planchamp, F.; Baldwin, P.; Mahner, S.; Mirza, M.R.; Fischerová, D.; Creutzberg, C.L.; Guillot, E.; Garganese, G.; Lax, S.; et al. European Society of Gynaecological Oncology Guidelines for the Management of Patients with Vulvar Cancer - Update 2023. Int. J. Gynecol. Cancer 2023, 33, 1023–1043. [Google Scholar] [CrossRef] [PubMed]
- Sand, F.L.; Rasmussen, C.L.; Frederiksen, M.H.; Andersen, K.K.; Kjaer, S.K. Prognostic Significance of HPV and p16 Status in Men Diagnosed with Penile Cancer: A Systematic Review and Meta-analysis. Cancer Epidemiol. Biomarkers Prev. 2018, 27, 1123–1132. [Google Scholar] [CrossRef]
- Sung, S.-Y.; Kim, Y.-S.; Kim, S.H.; Lee, S.J.; Lee, S.-W.; Kwak, Y.-K. Current Evidence of a Deintensification Strategy for Patients with HPV-Related Oropharyngeal Cancer. Cancers (Basel) 2022, 14. [Google Scholar] [CrossRef] [PubMed]
- Garnaes, E.; Frederiksen, K.; Kiss, K.; Andersen, L.; Therkildsen, M.H.; Franzmann, M.B.; Specht, L.; Andersen, E.; Norrild, B.; Kjaer, S.K.; et al. Double positivity for HPV DNA/p16 in tonsillar and base of tongue cancer improves prognostication: Insights from a large population-based study. Int. J. Cancer 2016, 139, 2598–2605. [Google Scholar] [CrossRef] [PubMed]
- Larsen, C.G.; Jensen, D.H.; Carlander, A.-L.F.; Kiss, K.; Andersen, L.; Olsen, C.H.; Andersen, E.; Garnæs, E.; Cilius, F.; Specht, L.; et al. Novel nomograms for survival and progression in HPV+ and HPV- oropharyngeal cancer: a population-based study of 1,542 consecutive patients. Oncotarget 2016, 7, 71761–71772. [Google Scholar] [CrossRef] [PubMed]
- Sand, F.L.; Nielsen, D.M.B.; Frederiksen, M.H.; Rasmussen, C.L.; Kjaer, S.K. The prognostic value of p16 and p53 expression for survival after vulvar cancer: A systematic review and meta-analysis. Gynecol. Oncol. 2019, 152, 208–217. [Google Scholar] [CrossRef] [PubMed]
- Nooij, L.S.; Haar, N.T. ter; Ruano, D.; Rakislova, N.; van Wezel, T.; Smit, V.T.H.B.M.; Trimbos, B.J.B.M.Z.; Ordi, J.; van Poelgeest, M.I.E.; Bosse, T. Genomic Characterization of Vulvar (Pre)cancers Identifies Distinct Molecular Subtypes with Prognostic Significance. Clinical Cancer Research 2017, 23, 6781–6789. [Google Scholar] [CrossRef] [PubMed]
- Chahoud, J.; Gleber-Netto, F.O.; McCormick, B.Z.; Rao, P.; Lu, X.; Guo, M.; Morgan, M.B.; Chu, R.A.; Martinez-Ferrer, M.; Eterovic, A.K.; et al. Whole-exome Sequencing in Penile Squamous Cell Carcinoma Uncovers Novel Prognostic Categorization and Drug Targets Similar to Head and Neck Squamous Cell Carcinoma. Clinical Cancer Research 2021, 27, 2560–2570. [Google Scholar] [CrossRef] [PubMed]
- Woelber, L.; Prieske, K.; Eulenburg, C.; Oliveira-Ferrer, L.; Gregorio, N. de; Klapdor, R.; Kalder, M.; Braicu, I.; Fuerst, S.; Klar, M.; et al. p53 and p16 expression profiles in vulvar cancer: a translational analysis by the Arbeitsgemeinschaft Gynäkologische Onkologie Chemo and Radiotherapy in Epithelial Vulvar Cancer study group. Am. J. Obstet. Gynecol. 2021, 224, 595.e1–595.e11. [Google Scholar] [CrossRef] [PubMed]
- Cheng, A.S.; Karnezis, A.N.; Jordan, S.; Singh, N.; McAlpine, J.N.; Gilks, C.B. p16 Immunostaining Allows for Accurate Subclassification of Vulvar Squamous Cell Carcinoma Into HPV-Associated and HPV-Independent Cases. Int. J. Gynecol. Pathol. 2016, 35, 385–393. [Google Scholar] [CrossRef] [PubMed]
- Santos, M.; Landolfi, S.; Olivella, A.; Lloveras, B.; Klaustermeier, J.; Suárez, H.; Alòs, L.; Puig-Tintoré, L.M.; Campo, E.; Ordi, J. p16 overexpression identifies HPV-positive vulvar squamous cell carcinomas. Am. J. Surg. Pathol. 2006, 30, 1347–1356. [Google Scholar] [CrossRef]
- Darragh, T.M.; Colgan, T.J.; Thomas Cox, J.; Heller, D.S.; Henry, M.R.; Luff, R.D.; McCalmont, T.; Nayar, R.; Palefsky, J.M.; Stoler, M.H.; et al. The Lower Anogenital Squamous Terminology Standardization project for HPV-associated lesions: background and consensus recommendations from the College of American Pathologists and the American Society for Colposcopy and Cervical Pathology. Int. J. Gynecol. Pathol. 2013, 32, 76–115. [Google Scholar] [CrossRef]
- Singh N, Gilks B, Wong RWC, McCluggage WG, Herrington C. Interpretation of p16 Immunohistochemistry In Lower Anogenital Tract Neoplasia. Available online: chrome-extension://efaidnbmnnnibpcajpcglclefindmkaj/https://www.bgcs.org.uk/wp-content/uploads/2019/06/Final-BAGP-UKNEQAS-cIQC-project-p16-interpretation-guide-2018.pdf (accessed on 6 May 2024).
- Jordan, R.C.; Lingen, M.W.; Perez-Ordonez, B.; He, X.; Pickard, R.; Koluder, M.; Jiang, B.; Wakely, P.; Xiao, W.; Gillison, M.L. Validation of methods for oropharyngeal cancer HPV status determination in US cooperative group trials. Am. J. Surg. Pathol. 2012, 36, 945–954. [Google Scholar] [CrossRef]
- Prigge, E.-S.; Arbyn, M.; Knebel Doeberitz, M. von; Reuschenbach, M. Diagnostic accuracy of p16INK4a immunohistochemistry in oropharyngeal squamous cell carcinomas: A systematic review and meta-analysis. Int. J. Cancer 2017, 140, 1186–1198. [Google Scholar] [CrossRef] [PubMed]
- Nicolás, I.; Saco, A.; Barnadas, E.; Marimon, L.; Rakislova, N.; Fusté, P.; Rovirosa, A.; Gaba, L.; Buñesch, L.; Gil-Ibañez, B.; et al. Prognostic implications of genotyping and p16 immunostaining in HPV-positive tumors of the uterine cervix. Mod. Pathol. 2020, 33, 128–137. [Google Scholar] [CrossRef] [PubMed]
- Poetsch, M.; Schuart, B.-J.; Schwesinger, G.; Kleist, B.; Protzel, C. Screening of microsatellite markers in penile cancer reveals differences between metastatic and nonmetastatic carcinomas. Mod. Pathol. 2007, 20, 1069–1077. [Google Scholar] [CrossRef] [PubMed]
- Poetsch, M.; Hemmerich, M.; Kakies, C.; Kleist, B.; Wolf, E.; vom Dorp, F.; Hakenberg, O.W.; Protzel, C. Alterations in the tumor suppressor gene p16(INK4A) are associated with aggressive behavior of penile carcinomas. Virchows Arch. 2011, 458, 221–229. [Google Scholar] [CrossRef]
- Kortekaas, K.E.; Solleveld-Westerink, N.; Tessier-Cloutier, B.; Rutten, T.A.; Poelgeest, M.I.E.; Gilks, C.B.; Hoang, L.N.; Bosse, T. Performance of the pattern-based interpretation of p53 immunohistochemistry as a surrogate for TP53 mutations in vulvar squamous cell carcinoma. Histopathology 2020, 77, 92–99. [Google Scholar] [CrossRef]
- Rakislova, N.; Clavero, O.; Alemany, L.; Saco, A.; Quirós, B.; Lloveras, B.; Alejo, M.; Pawlita, M.; Quint, W.; del Pino, M.; et al. "Histological characteristics of HPV-associated and -independent squamous cell carcinomas of the vulva: A study of 1,594 cases". Int. J. Cancer 2017, 141, 2517–2527. [Google Scholar] [CrossRef]
- Carreras-Dieguez, N.; Saco, A.; del Pino, M.; Marimon, L.; Del López Campo, R.; Manzotti, C.; Fusté, P.; Pumarola, C.; Torné, A.; Garcia, A.; et al. Human papillomavirus and p53 status define three types of vulvar squamous cell carcinomas with distinct clinical, pathological, and prognostic features. Histopathology 2023, 83, 17–30. [Google Scholar] [CrossRef]
- Horne, Z.D.; Dohopolski, M.J.; Pradhan, D.; Bhargava, R.; Edwards, R.P.; Kelley, J.L.; Comerci, J.T.; Olawaiye, A.B.; Courtney-Brooks, M.B.; Bockmeier, M.M.; et al. Human papillomavirus infection mediates response and outcome of vulvar squamous cell carcinomas treated with radiation therapy. Gynecol. Oncol. 2018, 151, 96–101. [Google Scholar] [CrossRef]
- Gao, J.; Aksoy, B.A.; Dogrusoz, U.; Dresdner, G.; Gross, B.; Sumer, S.O.; Sun, Y.; Jacobsen, A.; Sinha, R.; Larsson, E.; et al. Integrative analysis of complex cancer genomics and clinical profiles using the cBioPortal. Sci. Signal. 2013, 6, pl1. [Google Scholar] [CrossRef]
- Tessier-Cloutier, B.; Kortekaas, K.E.; Thompson, E.; Pors, J.; Chen, J.; Ho, J.; Prentice, L.M.; McConechy, M.K.; Chow, C.; Proctor, L.; et al. Major p53 immunohistochemical patterns in in situ and invasive squamous cell carcinomas of the vulva and correlation with TP53 mutation status. Mod. Pathol. 2020, 33, 1595–1605. [Google Scholar] [CrossRef]
- Proctor, L.; Hoang, L.; Moore, J.; Thompson, E.; Leung, S.; Natesan, D.; Chino, J.; Gilks, B.; McAlpine, J.N. Association of human papilloma virus status and response to radiotherapy in vulvar squamous cell carcinoma. Int. J. Gynecol. Cancer 2020, 30, 100–106. [Google Scholar] [CrossRef] [PubMed]
- Woelber, L.; Prieske, K.; Eulenburg, C. zu; Corradini, S.; Petersen, C.; Bommert, M.; Blankenstein, T.; Hilpert, F.; Gregorio, N. de; Iborra, S.; et al. Adjuvant radiotherapy and local recurrence in vulvar cancer - a subset analysis of the AGO-CaRE-1 study. Gynecol. Oncol. 2022, 164, 68–75. [Google Scholar] [CrossRef] [PubMed]
- Cao, H.; Wang, S.; Zhang, Z.; Lou, J. Prognostic Value of Overexpressed p16INK4a in Vulvar Cancer: A Meta-Analysis. PLoS One 2016, 11, e0152459. [Google Scholar] [CrossRef] [PubMed]
- Dohopolski, M.J.; Horne, Z.D.; Pradhan, D.; Bhargava, R.; Edwards, R.P.; Kelley, J.L.; Comerci, J.T.; Olawaiye, A.B.; Courtney-Brooks, M.; Berger, J.L.; et al. The Prognostic Significance of p16 Status in Patients With Vulvar Cancer Treated With Vulvectomy and Adjuvant Radiation. Int. J. Radiat. Oncol. Biol. Phys. 2019, 103, 152–160. [Google Scholar] [CrossRef] [PubMed]
- Yap, M.L.; Allo, G.; Cuartero, J.; Pintilie, M.; Kamel-Reid, S.; Murphy, J.; Mackay, H.; Clarke, B.; Fyles, A.; Milosevic, M. Prognostic Significance of Human Papilloma Virus and p16 Expression in Patients with Vulvar Squamous Cell Carcinoma who Received Radiotherapy. Clin. Oncol. (R Coll. Radiol) 2018, 30, 254–261. [Google Scholar] [CrossRef] [PubMed]
- Lee, L.J.; Howitt, B.; Catalano, P.; Tanaka, C.; Murphy, R.; Cimbak, N.; DeMaria, R.; Bu, P.; Crum, C.; Horowitz, N.; et al. Prognostic importance of human papillomavirus (HPV) and p16 positivity in squamous cell carcinoma of the vulva treated with radiotherapy. Gynecol. Oncol. 2016, 142, 293–298. [Google Scholar] [CrossRef]
- Lindell, G.; Näsman, A.; Jonsson, C.; Ehrsson, R.J.; Jacobsson, H.; Danielsson, K.G.; Dalianis, T.; Källström, B.N.; Larson, B. Presence of human papillomavirus (HPV) in vulvar squamous cell carcinoma (VSCC) and sentinel node. Gynecol. Oncol. 2010, 117, 312–316. [Google Scholar] [CrossRef] [PubMed]
- Nooij, L.S.; Brand, F.A.M.; Gaarenstroom, K.N.; Creutzberg, C.L.; Hullu, J.A. de; van Poelgeest, M.I.E. Risk factors and treatment for recurrent vulvar squamous cell carcinoma. Crit. Rev. Oncol. Hematol. 2016, 106, 1–13. [Google Scholar] [CrossRef]
- Woelber, L.; Mathey, S.; Prieske, K.; Kuerti, S.; Hillen, C.; Burandt, E.; Coym, A.; Mueller, V.; Schmalfeldt, B.; Jaeger, A. Targeted Therapeutic Approaches in Vulvar Squamous Cell Cancer (VSCC): Case Series and Review of the Literature. Oncol. Res. 2021, 28, 645–659. [Google Scholar] [CrossRef]
- Mantovani, G.; Fragomeni, S.M.; Inzani, F.; Fagotti, A.; Della Corte, L.; Gentileschi, S.; Tagliaferri, L.; Zannoni, G.F.; Scambia, G.; Garganese, G. Molecular pathways in vulvar squamous cell carcinoma: implications for target therapeutic strategies. J. Cancer Res. Clin. Oncol. 2020, 146, 1647–1658. [Google Scholar] [CrossRef]
- Pagliaro, L.; Marchesini, M.; Roti, G. Targeting oncogenic Notch signaling with SERCA inhibitors. J. Hematol. Oncol. 2021, 14, 8. [Google Scholar] [CrossRef] [PubMed]
- Ribera-Cortada, I.; Guerrero-Pineda, J.; Trias, I.; Veloza, L.; Garcia, A.; Marimon, L.; Diaz-Mercedes, S.; Alamo, J.R.; Rodrigo-Calvo, M.T.; Vega, N.; et al. Pathogenesis of Penile Squamous Cell Carcinoma: Molecular Update and Systematic Review. Int. J. Mol. Sci. 2021, 23. [Google Scholar] [CrossRef] [PubMed]
- Singh, N.; Gilks, C.B.; Wong Wing-Cheuk, R.; McCluggage, W.G.; Herrington, C.S. Final-BAGP-UKNEQAS-cIQC-project-p16-interpretation-guide-2018 2018.
- Köbel, M.; Kang, E.Y. The Many Uses of p53 Immunohistochemistry in Gynecological Pathology: Proceedings of the ISGyP Companion Society Session at the 2020 USCAP Annual9 Meeting. Int. J. Gynecol. Pathol. 2021, 40, 32–40. [Google Scholar] [CrossRef] [PubMed]
Figure 1a.
Subdivision of squamous cell carcinomas of the lower female genital tract based on HPV-association according to the recommendations of the WHO-classification 2020 [27].
Figure 1a.
Subdivision of squamous cell carcinomas of the lower female genital tract based on HPV-association according to the recommendations of the WHO-classification 2020 [27].

Figure 1b.
Classification of VSCC from morphology-based to morpho-molecular classification, depending on the etiology of the disease using p16- and p53-immunohistochemistry [10,12,13,19].
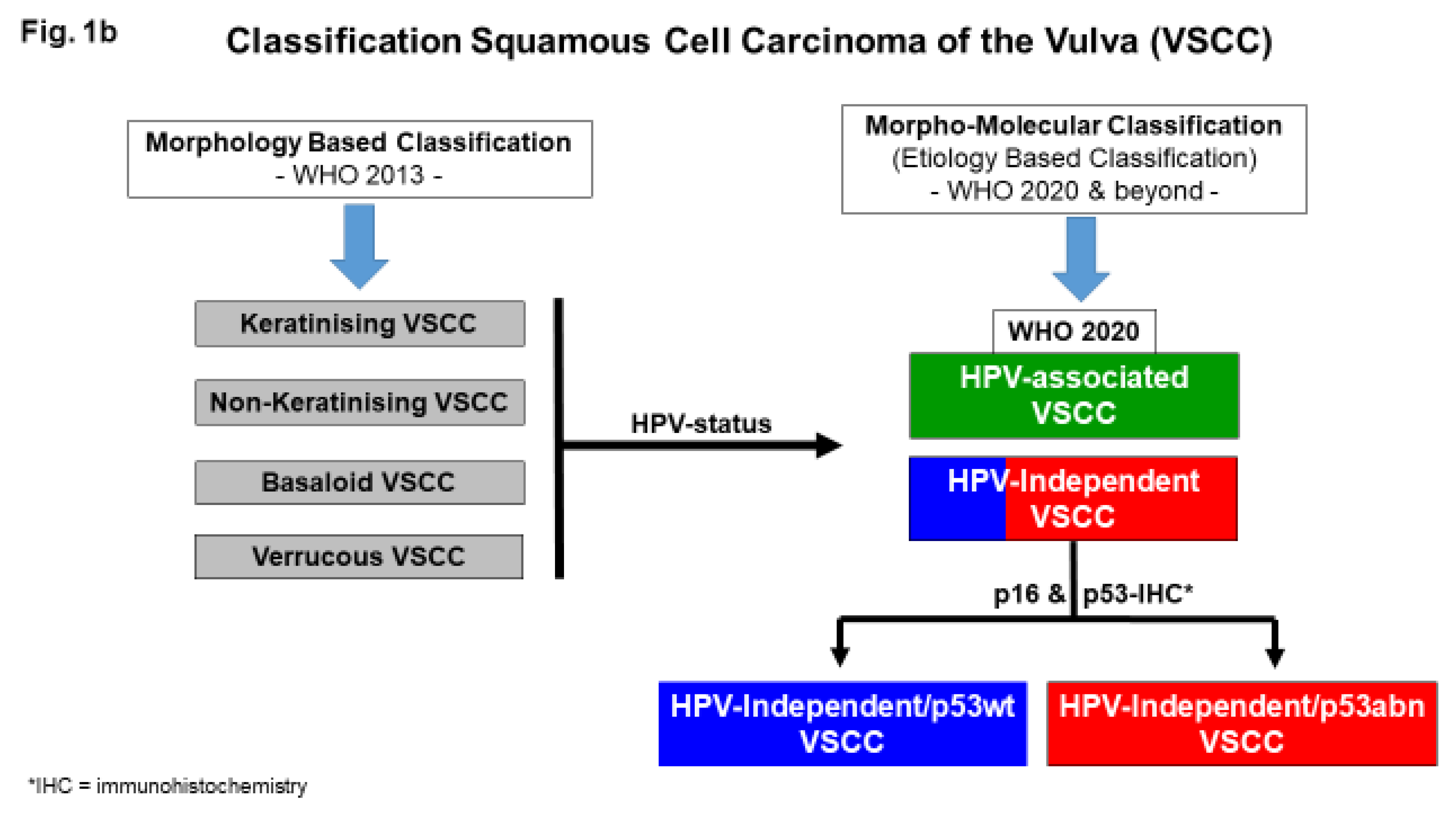
Figure 2.
Summary of the recently described three-tiered molecular classification of VSCC and its precursors (please see text) (uVIN = usual VIN, dVIN = differentiated VIN, vaVIN = verrucous VIN).
Figure 2.
Summary of the recently described three-tiered molecular classification of VSCC and its precursors (please see text) (uVIN = usual VIN, dVIN = differentiated VIN, vaVIN = verrucous VIN).
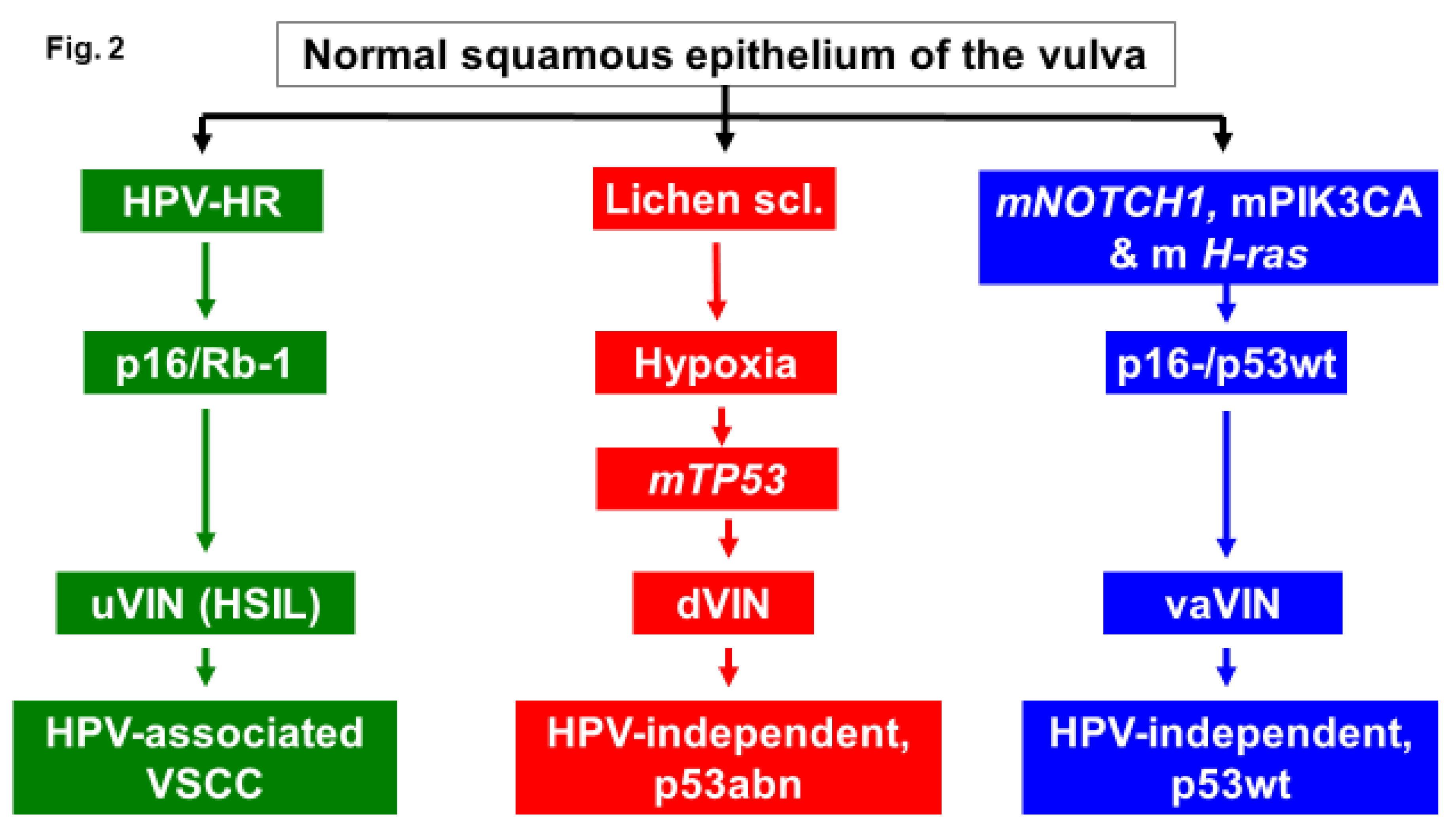
Figure 3.
Patterns of p16-overexpression on non-keratinising (a) and keratinising (b) VSCC, so- called block-like staining. Note that the keratinised areas stain negative for p16 pattern (asterix; see text).
Figure 3.
Patterns of p16-overexpression on non-keratinising (a) and keratinising (b) VSCC, so- called block-like staining. Note that the keratinised areas stain negative for p16 pattern (asterix; see text).
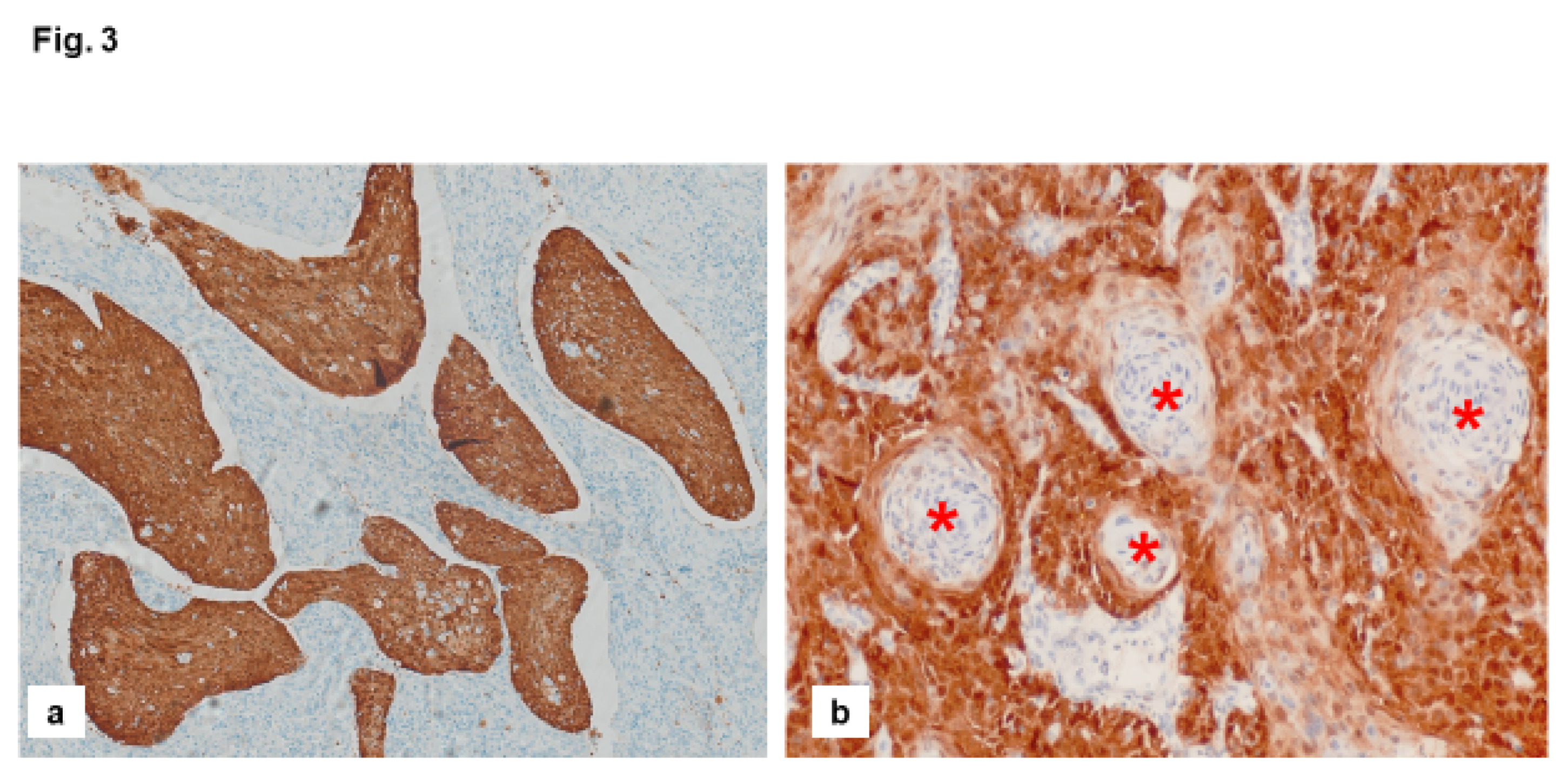
Figure 4.
Algorithmic approach for the three-tiered molecular subclassification of VSCC using p16 and p53 immunohistochemistry [13]. ISH = in situ hybridisation.
Figure 4.
Algorithmic approach for the three-tiered molecular subclassification of VSCC using p16 and p53 immunohistochemistry [13]. ISH = in situ hybridisation.
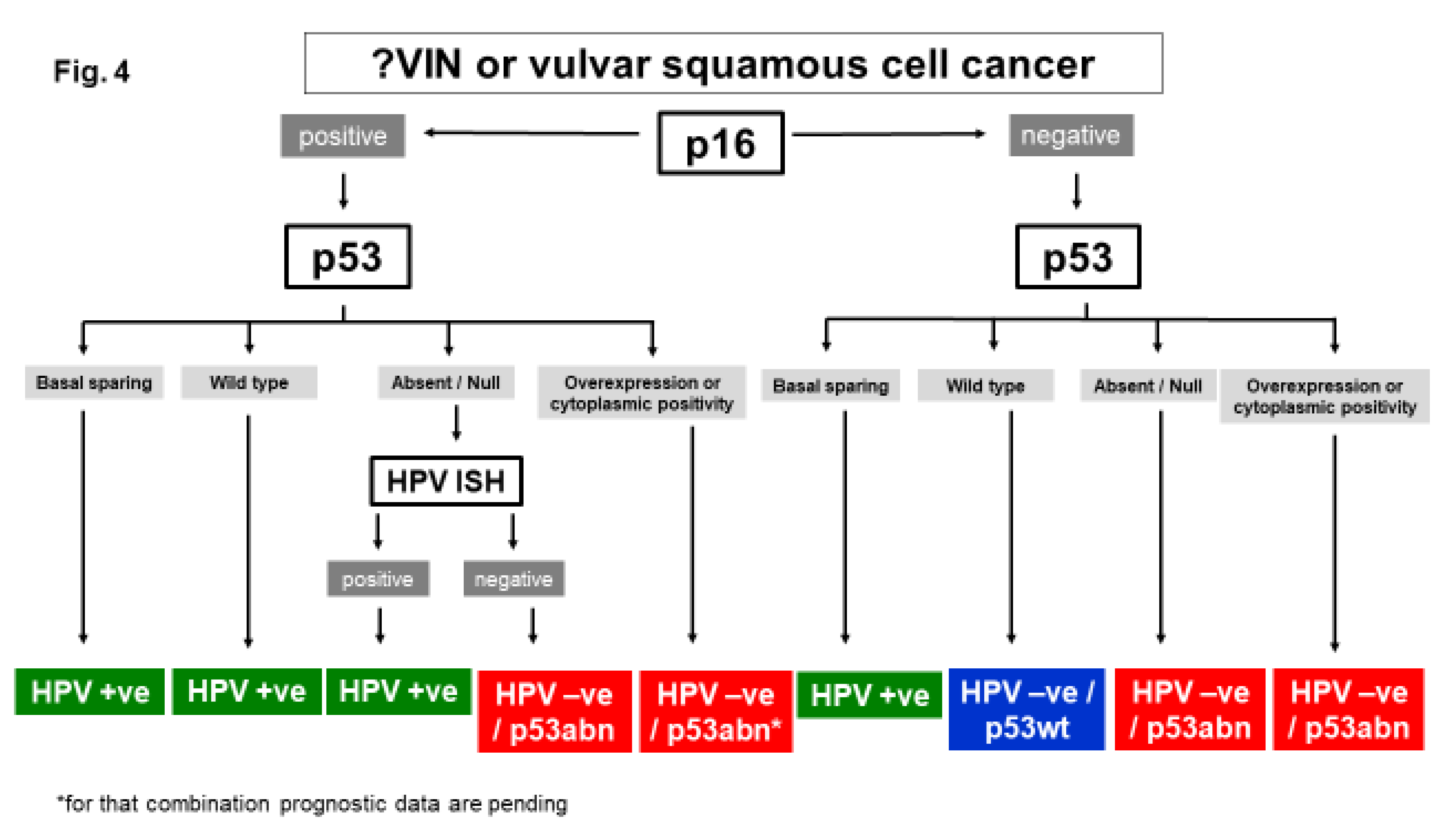
Figure 7.
year-old woman with a poorly differentiated squamous cell carcinoma (a; FIGO-stage IVA) with p16-block-type staining overexpression (b) and p53-wildtype expression staining pattern(scattered; c) on immunohistochemistry, treated by hypofractionated radiation with a total dose of 38 Gy and sequential chemotherapy consisting of 5 cycles carboplatin AUC 5 and paclitaxel 175 mg/m2. d) Prior treatment: 25cm x 10cm exophytic superficially ulcerated tumor. e) Partial clinical response after three months of treatment. f) Complete local clinical response after 10 months. There is no local recurrence within 363 months of follow-up.
Figure 7.
year-old woman with a poorly differentiated squamous cell carcinoma (a; FIGO-stage IVA) with p16-block-type staining overexpression (b) and p53-wildtype expression staining pattern(scattered; c) on immunohistochemistry, treated by hypofractionated radiation with a total dose of 38 Gy and sequential chemotherapy consisting of 5 cycles carboplatin AUC 5 and paclitaxel 175 mg/m2. d) Prior treatment: 25cm x 10cm exophytic superficially ulcerated tumor. e) Partial clinical response after three months of treatment. f) Complete local clinical response after 10 months. There is no local recurrence within 363 months of follow-up.
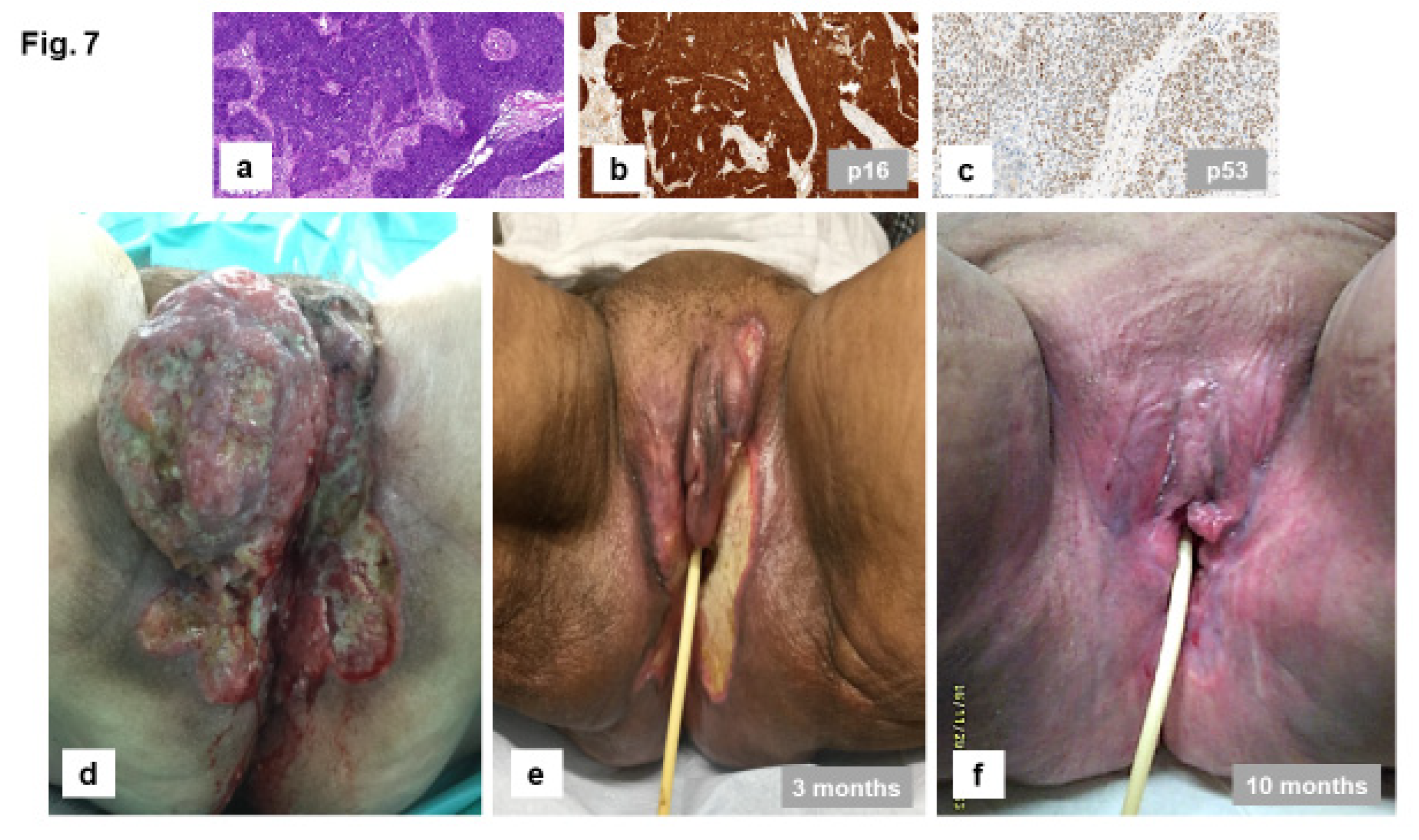
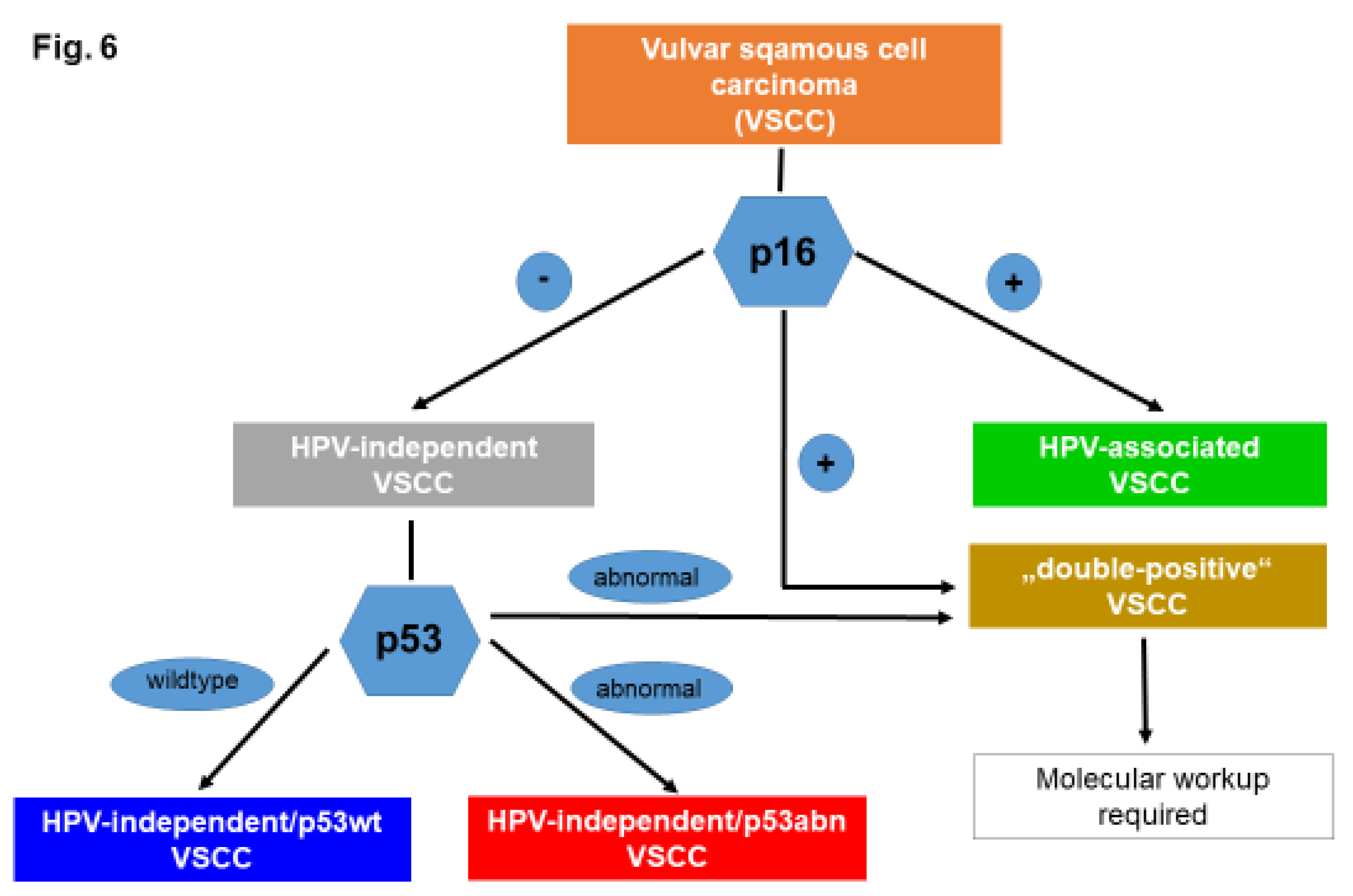
Figure 8.
Summary of the three-tiered molecular classification of VSCC.
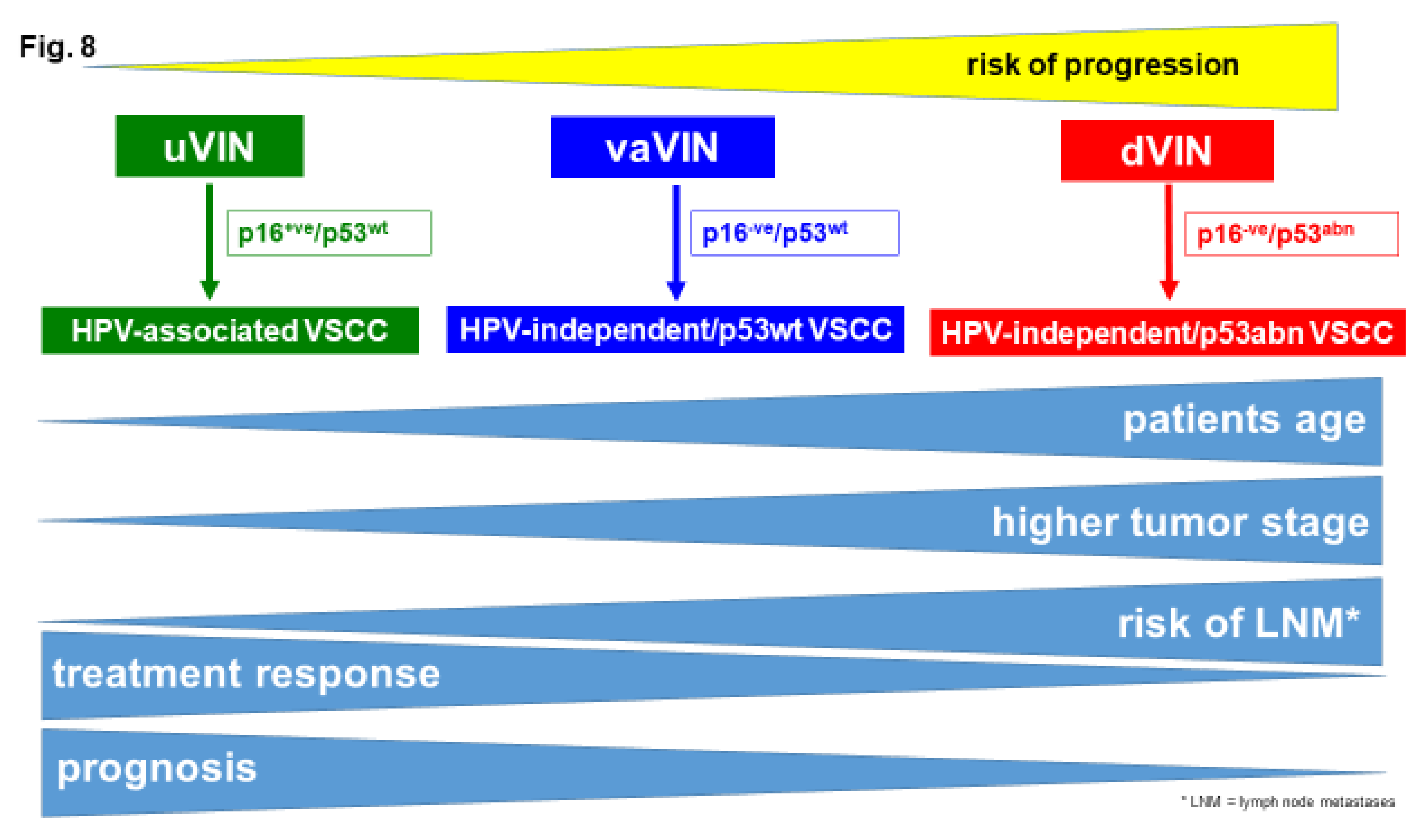

Table 2.
Frequency of the different molecular subtypes reported in the literature.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



