Submitted:
21 October 2024
Posted:
22 October 2024
Read the latest preprint version here
Abstract
Object: Due to the fact that glioma surgery requires manipulation of the brain parenchyma and the expression of inflammatory mediators, there is often a possibility of central nervous system (CNS) infection occurring after surgery. Previous studies on CNS infections related to neurosurgery have uniformly explored the risk factors for CNS infections in all neurosurgery surgeries that require craniotomy, but have not explored the risk factors and clinical characteristics of CNS infections after glioma resection.
Methods: We included patients who underwent glioma resection from January 2015 to March 2023, systematically recorded population characteristics, clinical, surgical, laboratory and survival data, analyzed high-risk factors for postoperative CNS infections, summarized cerebrospinal fluid characteristics, antibiotic use, and explored whether CNS infections affects the long-term prognosis of glioma patients after surgery.
Results:All 337 patients underwent glioma resection, and 61 patients (18.1%) developed CNS infections after surgery. Ventricle Opening, post-op other systemic infections, post-op maximum cavity diameter, and peripheral blood Monocyte% are independent risk factors for postoperative CNS infections. The median protein content in cerebrospinal fluid of patients with CNS infections is 1.73g/L ([IQR] 1.03-3.06), the median glucose content is 2.7mmol/L ([IQR] 1.90-3.70), and the median WBC is 1478×106cells/L ([IQR] 467-4204.25×106), with a median percentage of multinucleated cells of 84.1% ([IQR] 74.55% -90.83%). Meropenem and Vancomycin are the most commonly used antibiotics, with an average usage time of 7.79 days and 8.41 days, respectively. Survival analysis suggests that the occurrence of CNS infections does not affect the long-term prognosis of glioma patients after surgery.
Conclusions: This study separately explored the risk factors for CNS infections in patients with glioma after surgery, instead of all diseases which need craniotomy,and summarized their cerebrospinal fluid characteristics and antibiotic use. Although CNS infection is only one of the possible complications during the treatment of gliomas, we believe that this will make a certain contribution to neurosurgeons' individualized prevention, diagnosis, and treatment of patients in the diagnosis and treatment of gliomas.
Keywords:
glioma
; central nervous system infection
; risk factors
; antibiotic
1. Introduction
Central nervous system(CNS) infection may occur in patients undergoing neurosurgical surgery. Previous studies have reported an incidence of CNS infections after neurosurgery ranging from 0.3% to 25.0% [1,2,3], but these studies were conducted in all neurosurgery patients rather than in a single disease, and the proportion of meningiomas in these studies is relatively high.
Glioma is the most common primary brain malignant tumor [4], and its treatment method is to preserve the maximum range of functional surgical resection, as well as to decide whether to undergo radiotherapy and chemotherapy early based on the patient's condition after surgery [5]. For surgery, glioma is different from meningioma, as it requires surgery on the brain parenchyma and requires a longer surgical time. The use of corticoids after surgery may increase the likelihood of postoperative CNS infection in patients [6,7]. Once CNS infection occurs, it can lead to an extension of the patient's hospitalization time, an increase in hospitalization costs, a delay in the patient's radiotherapy and chemotherapy process, an increase in the risk of death and the probability of neurological impairment [8,9].
Therefore, this study explored the high-risk factors for developing CNS infections in glioma patients after surgery, including clinical characteristics, laboratory test results, surgical related data, etc. At the same time, it summarized the cerebrospinal fluid characteristics and antibiotic use of postoperative CNS infections in glioma patients, and explored whether the occurrence of CNS infection affects the prognosis of glioma patients.
2. Methods
2.1. Identification of Patients
This study was completed at Peking Union Medical College Hospital. 337 patients with gliomas who underwent tumor resection from January 2015 to March 2023 were included consecutively, and no deaths occurred during hospitalization. Patients undergoing biopsy were not included. Among the these patients, 114 were glioblastomas, 89 were astrocytomas, 73 were oligodendrogliomas, 22 were ganglionic gliomas, and a total of 39 were other types of gliomas. This study is a clinical retrospective study, so we are not able to provide informed consents from all the patients (whose data are used for research). But the study has obtained ethical approval from The Ethics Review Committee of Peking Union Medical College Hospital, Chinese Academy of Medical Sciences, with ethical code K23C1427.
2.2. Data Abstraction
The diagnosis of CNS infection is determined based on the diagnostic criteria outlined in the Centers for Disease Control and Prevention [10] definitions. Specifically, these criteria include:
1. A definitive diagnosis of CNS infection is established when cerebrospinal fluid (CSF) cultures yield positive results for microorganisms.
2. In cases where CSF cultures are negative, but the patient exhibits following clinical signs or symptoms, the diagnosis of CNS infection can still be confirmed:(a)Fever (> 38℃); (b)Headache; (c)Signs of meningeal irritation; (d) An increased white blood cell (WBC) count in the CSF; (e) Elevated protein levels and/or decreased glucose levels in the CSF; (f) Detection of pathogens on Gram stain of CSF samples; (g) A positive blood culture for microorganisms can also lead to a definitive diagnosis of CNS infections. Among these criteria, meeting at least one condition from (a, b, c) and (d, e, f, g) respectively is sufficient for a definitive diagnosis.
We established a standardized database wherein we extracted clinical information from patients' cases and medical records. The recorded preoperative patient information includes age, gender, BMI, and the following clinical characteristics: whether they have a primary glioma, the presence of diabetes or other systemic diseases, prior history of radiotherapy and chemotherapy, steroid use, whether they had other organ infections, whether the tumor exhibited necrosis, maximum tumor diameter, and the absolute WBC count in the blood routine results upon admission. Intraoperative clinical characteristics encompass surgery duration, the occurrence of ventricle opening, and frontal/ethmoid opening, as well as the insertion of a tumor cavity catheter. Postoperative clinical characteristics involve external drain duration, the occurrence of other systemic infections, seizures, steroid use, maximum cavity diameter, and whether further surgeries were conducted. The datasets analysed during the current study can be found in Supplementary Materials.
2.3. Statistical Analysis
Data analysis was carried out using R language (version 4.2.2). Continuous variables were compared using the Student t-test or Mann-Whitney U-test, while categorical variables were compared using Fisher's exact test (Table 1). Variables with p-values<0.05 were included in a multivariable logistic regression to calculate OR and 95%CI, in order to determine whether they are independent risk factors for the occurrence of CNS infections (Table 2). Data on proteins, glucose, white blood cells, and other variables in the cerebrospinal fluid of patients who developed CNS infections were presented using medians and IQR. Treatment durations for various antibiotics were displayed using means. Kaplan-Meier survival analysis was employed to explore whether CNS infections had an impact on the prognosis of patients after glioma surgery.
3. Results
3.1. Study Population and Procedure Characteristics
This study included 337 patients who met the inclusion criteria. Table 1 presents their baseline characteristics and variables with statistically significant differences. Among these patients, 43.3% were female. Postoperatively, 61 patients (18.1%) were diagnosed with CNS infections. The median age of patients without CNS infections was 47 years (IQR: 34-57), while the median age of patients with CNS infections was 46 years (IQR: 34-55). Patients with primary gliomas accounted for a significant proportion in both groups (83.70% and 83.61%). Regarding the surgical procedures, the median surgery duration for patients without CNS infections was 5 hours (IQR: 4.0-6.3), with a 17.39% ventricle opening rate, additionally, 34.42% of patients had external drainage placement, and 6.52% underwent frontal or ethmoid sinus opening. Patients who developed CNS infections had a median surgery duration of 5.5 hours (IQR: 4.7-7.0), with a 47.54% ventricle opening rate, furthermore, 60.66% of these patients had external drainage placement, and 6.56% underwent frontal or ethmoid sinus opening.
3.2. Risk Factors of CNS Infections
Table 1 provides an overview of all the variables that were assessed for their association with the risk of CNS infections after surgeries. Variables with p-values<0.05, which demonstrated a statistically significant relationship with the occurrence of CNS infections, include monocyte% in preoperative peripheral blood, maximum tumor diameter, surgery duration, ventricle opening, tumor cavity catheter insertion, external drain duration, postoperative other systemic infections, postoperative maximum cavity diameter, and multiple hospital surgeries. The multivariable logistic regression result reveals that the independent risk factors include ventricle opening (OR 2.97, p < 0.01), postoperative other systemic infections (OR 4.03, p = 0.01), a larger postoperative maximum cavity diameter (OR 1.03, p = 0.02), and a higher monocyte % (OR 1.19, p = 0.04) (Table 2).
3.3. CSF Features in Patients with CNS Infections
In patients who developed CNS infections, the median cerebrospinal fluid (CSF) protein content was 1.73g/L (IQR: 1.03-3.06), the median CSF glucose content was 2.7mmol/L (IQR: 1.90-3.70), the median CSF chloride content was 120mmol/L (IQR: 116.00-122.00), the median CSF white blood cell count was 1478×106 cells/L (IQR: 467×106-4204.25×106), and the median percentage of polymorphonuclear cells (multinucleated cells) was 84.1% (IQR: 74.55%-90.83%) (Table 3).
3.4. Microbiology of CNS Infections and Antibiotics Use
Among the 61 patients with CNS infections, only 3 cases had positive microbiological culture results. The identified pathogens included Staphylococcus haemolyticus, Staphylococcus epidermidis, and Acinetobacter baumanii. (Table 4).
A total of 50 individuals received antibiotic treatment, 5 patients did not receive antibiotics due to the decision of the attending physician, and 6 cases were not included in the statistics due to the complexity of antibiotic usage. Vancomycin was the most frequently used antibiotic for Gram-positive bacteria, with a total of 43 administrations and an average duration of use of 7.79 days. Meropenem was the most commonly used antibiotic for Gram-negative bacteria, with 27 administrations and an average duration of use of 8.41 days (Table 5).
3.5. Survival Prediction
We conducted long-term follow-up on the surgical patients, and in our study cohort, there were a total of 107 individuals with survival data. Among these, 91 individuals did not experience CNS infections, and 83 of them reached the survival endpoint (91.21%), with a median survival of 1260 days. On the other hand, 16 individuals developed CNS infections, and all of them reached the survival endpoint (100%), with a median survival of 1348 days. Kaplan-Meier survival analysis revealed that there was no significant difference in prognosis between the two groups (Figure 1).
4. Discussion
4.1. Prevalence of CNS Infections after Craniotomy for Gliomas
In this study population, the postoperative incidence of CNS infections after glioma resection was 18.1%, with a cerebrospinal fluid (CSF) culture positivity rate of 0.9%. This rate falls within the range of probabilities reported in previous literature for CNS infections of post-craniotomy, which varies from 0.3% to 25.0% [1,2,3,11]. It's important to note that the low CSF culture positivity rate of 0.9% doesn't definitively rule out the occurrence of CNS infections in CSF culture-negative patients. Therefore, The diagnostic approach we employ for central nervous system infections involves observing whether patients present relevant clinical symptoms (fever, headache, meningeal signs) in conjunction with an increased white blood cell count, elevated protein content, and/or decreased glucose content in the CSF. This approach allows for an early diagnosis and the initiation of appropriate antibiotic treatment, facilitating the rapid recovery and discharge of patients to prevent potential exacerbation of intracranial infections or the emergence of infections in other areas during their hospitalization, however, this also contributes to an increased diagnostic rate of CNS infections.
4.2. Risk Factors
The multivariable logistic regression result indicates that ventricle opening, postoperative other systemic infections, postoperative maximum cavity diameter, and monocyte% are independent risk factors for the occurrence of CNS infections after glioma resection.
Ventricle opening often occurs in patients with tumors invading the ventricles or the surrounding brain tissue, and this is a unique situation in brain parenchymal tumors. Given that glioma resection surgery aims to remove the tumor as extensively as possible, there is a possibility of damaging the ventricular wall. While procedures like ventriculoperitoneal shunting and external ventricular drainage may also open the ventricles, they do not establish direct communication between the ventricular system and the cerebrospinal fluid circulation within the brain parenchyma. In the retrospective study conducted by Omri Maayan [12], which included 1209 patients who underwent tumor resection surgery, the role of Ventricle Opening as an independent risk factor for postoperative CNS infections was not addressed. However, our research findings contradict this, and the disparity in results may be attributed to the fact that they included patients with various types of brain tumors, with a significant proportion being meningioma patients. Meningioma surgery typically does not require ventricular wall disruption. In contrast, our study exclusively involved patients with gliomas, demonstrating differences in patient populations, thus leading to different conclusions. Currently, there is no existing literature reporting on studies related to the risk factor of ventricle opening in the development of postoperative CNS infections in glioma patients. Nonetheless, this outcome suggests that in cases where ventricular opening occurs during glioma resection surgery and patients present symptoms, such as fever, headache, and meningeal signs, timely consideration of lumbar puncture and antibiotic administration is warranted. Furthermore, if the disruption of the ventricular wall is not an essential surgical procedure, it may be advisable to minimize such interventions.
Postoperative infections involving systems other than the central nervous system primarily included respiratory system infections and urinary tract infections. Among the 337 patients, a total of 14 patients developed postoperative pneumonia, and 5 patients experienced urinary tract infections. Notably, 8 of the patients who had postoperative pneumonia and 1 patient with a urinary tract infection subsequently developed symptoms related to meningitis and were diagnosed with CNS infections. The most common pathogen in pneumonia combined with CNS infections is Streptococcus pneumoniae [1,13,14,15,16,17]. This pathogen is commonly colonized in the nasopharynx [15] and can lead to pneumonia when there is an immune abnormality in the host. Due to its invasive nature, once it enters the bloodstream, it can proliferate, leading to the disruption of the blood-brain barrier (BBB) and entry into the cerebrospinal fluid, causing CNS infections [13,14]. In Bradford D. Gessner's study [14], researchers were able to simultaneously culture the same Streptococcus pneumoniae pathogen in patients who had both pneumonia and CNS infections. Research on urinary tract infections combined with CNS infections has primarily been conducted in infants. Previous studies have reported an extremely low incidence rate, approximately less than 0.1% [18,19,20,21,22]. This low incidence can be attributed to the fact that the most common pathogen in urinary tract infections is uropathogenic Escherichia coli (UPEC) [18,23]. The specific characteristics of its pathogenic mechanisms, the flushing action of urine, and the robust immune function of the urinary tract epithelium are likely the main reasons for this low incidence [23,24]. This suggests that when patients develop pneumonia postoperatively, it is essential to strengthen respiratory management while also monitoring for symptoms of CNS infections.
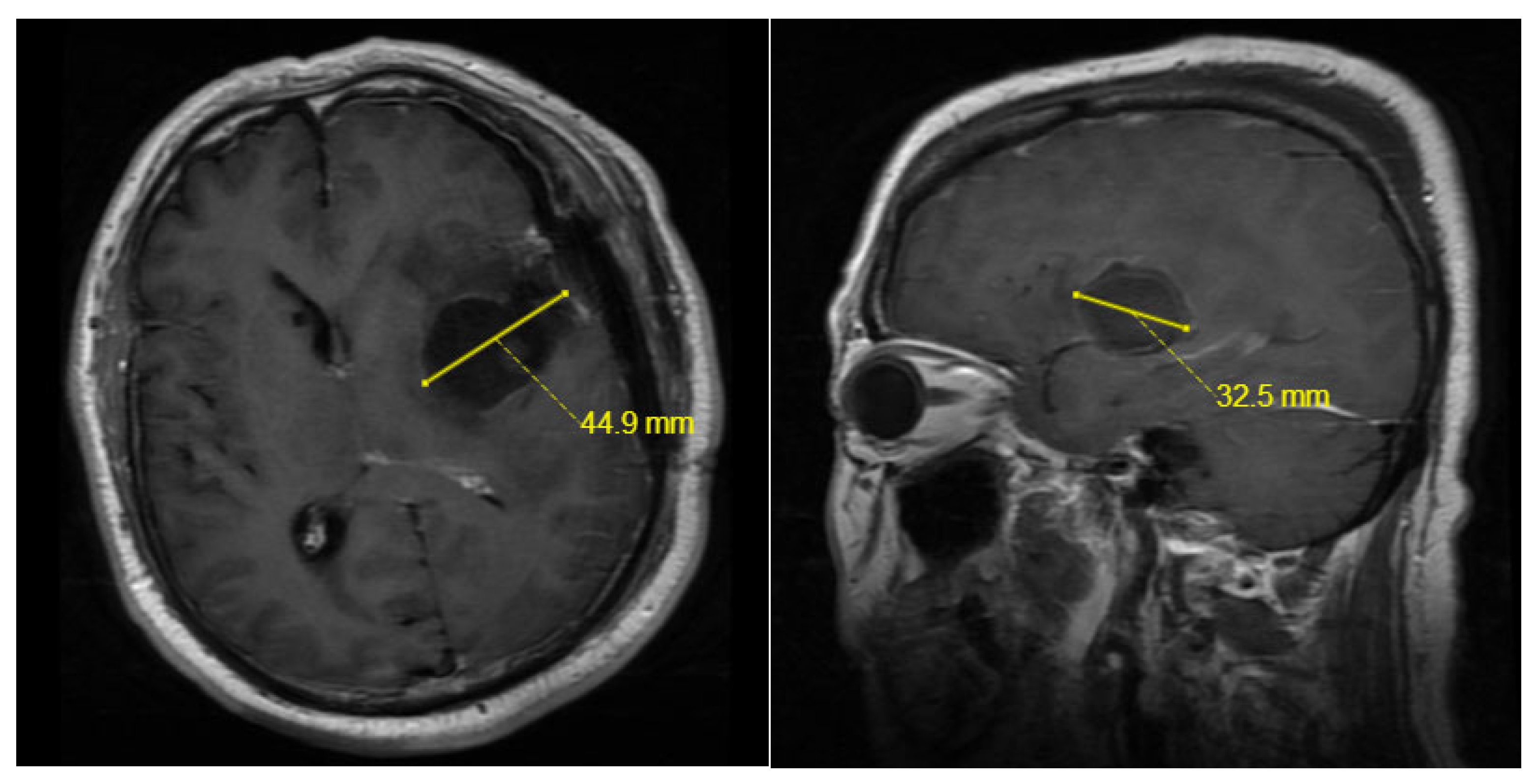
The post-operation maximum cavity diameter of a tumor on MRI, to some extent, reflects the volume of the residual cavity after tumor resection [25,26] (Figure 2). However, there is no existing literature reporting a relationship between it and the occurrence of postoperative CNS infections in glioma patients. It can be speculated that a larger postoperative residual cavity volume might be associated with a longer surgical duration, greater exposure of brain tissue and larger surgical trauma. These factors could potentially contribute to the risk of postoperative CNS infections. A longer surgical duration and increased exposure of brain tissue can elevate the likelihood of contact between bacteria in the air and exposed tissues. A larger surgical trauma results in the production of more inflammatory substances and a more intense immune response. Conversely, the preoperative maximum tumor diameter is not an independent risk factor for postoperative CNS infections in glioma patients. This may be due to the surgical principle of preserving functional areas in glioma resection [5,27] and the presence of brain shift phenomenon [28]. So in many cases, the postoperative residual cavity volume does not necessarily correlate with the size of the tumor itself.
Figure 2.
The maximum diameter of the postoperative tumor cavity on MRI is determined by taking the longer length between the maximum diameter in the axial plane and the maximum diameter in the sagittal plane. As shown in the image below, the maximum diameter of the postoperative tumor cavity on MRI is 44.9mm.
Figure 2.
The maximum diameter of the postoperative tumor cavity on MRI is determined by taking the longer length between the maximum diameter in the axial plane and the maximum diameter in the sagittal plane. As shown in the image below, the maximum diameter of the postoperative tumor cavity on MRI is 44.9mm.
Surprisingly, what astonished us was that the Monocyte% in the peripheral blood of patients preoperatively is also one of the independent risk factors for postoperative CNS infections in glioma resection. Upon reviewing the relevant literature, it is known that monocytes play a role in the body's immune response and mediate the production of pro-inflammatory mediators such as interleukins, tumor necrosis factor, interferon, and others [29,30]. Marija Djukic's research [31] mentions that in mice, monocytes from the peripheral circulation can migrate into the brain under the chemotaxis of inflammatory mediators in the cerebrospinal fluid. They can directly participate in the inflammatory process or differentiate into microglial cells to exacerbate inflammation. In the context of Salmonella infection-related CNS infections, higher levels of monocytes were found to accumulate and infiltrate brain tissue, while levels of neutrophils, dendritic cells, T cells, B cells, and natural killer cells were lower [32].
While surgery duration, the placement of external drains, and the preoperative tumor's maximum diameter may not be independent risk factors for postoperative CNS infections, the results of the univariate analysis still suggest that they are risk factors for postoperative CNS infections. Therefore, in the clinical diagnostic and treatment process, they should still be given due attention.
In comparison to previous literature [6,33,34], this study did not conclude that diabetes and the use of steroids are risk factors for postoperative CNS infections. This difference in findings may be due to the higher rate of corticosteroid usage and the lower number of diabetes patients in our study. In cases where patients do not have specific medical conditions, we typically administer dexamethasone treatment within 7 days postoperatively. This treatment can manage peritumoral cerebral edema and related neurological deficits, allowing patients to maintain a good mental state, engage in early physical rehabilitation, and promote postoperative recovery [35]. In our study cohort, only 18 patients had diabetes.
4.3. The Characteristics of Cerebrospinal Fluid and the Use of Antibiotics
Elevated protein levels, decreased glucose levels, and an increased white blood cell count often indicate the possibility of bacterial CNS infections [36]. In our dataset, the protein levels were above the normal range, the glucose levels were close to the lower limit of the normal range, and the white blood cell count and the percentage of polymorphonuclear cells were higher than the normal range, which essentially aligns with the characteristics of CNS infections [2,36,37,38]. The near-normal glucose levels may be due to some patients having higher blood glucose levels during the lumbar puncture procedure. The 3 patients with positive microbiological cultures had the following pathogens: Staphylococcus haemolyticus, Staphylococcus epidermidis and Acinetobacter baumanii. Staphylococcus haemolyticus and Staphylococcus epidermidis are both common pathogens in hospital-acquired infections [39,40,41]. These two pathogens showed sensitivity to most antibiotics commonly used against gram-positive bacteria. On the other hand, Acinetobacter baumanii is known to be resistant to many antibiotics. This resistance can make infections caused by Acinetobacter baumanii challenging to treat. It's important to select appropriate antibiotics and treatment strategies based on the antibiotic sensitivity profile of the specific strain of Acinetobacter baumanii in the patient. 50 patients received antibiotics, with the most commonly used antibiotic for gram-positive bacteria being Vancomycin. For gram-negative bacteria, the most frequently used antibiotics were Meropenem and Cefperazone. The combination therapy of Meropenem and Vancomycin was the most commonly used among these patients. Meropenem is commonly used to treat infections in critically ill patients and those that are not effectively responsive to other antibiotics. In our clinical practice, we have observed that when other antibiotics, such as ceftriaxone and cefotaxime, prove ineffective in treating CNS infections, Meropenem often exhibits better efficacy [42,43]. Our criteria for discontinuing antibiotics are as follows: normal body temperature, absence of headache symptoms, negative meningeal signs, CSF white blood cell count <100/L, and normalization of protein and glucose levels.
It is worth discussing that some patients postoperatively, upon developing symptoms related to CNS infections, exhibit bloody cerebrospinal fluid (CSF) following a lumbar puncture. CSF cytological analysis shows a significant increase in both white blood cell and red blood cell counts. Inexperienced physicians may find it challenging to differentiate whether the patient's symptoms result from the stimulating effects of bloody CSF on the nervous system or from the additional occurrence of CNS infections. In comparison to patients with subarachnoid hemorrhage due to ruptured aneurysms, whose CSF characteristics exhibit the typical features of bloody CSF, primarily characterized by a significant increase in red blood cells and rare abnormal elevations in white blood cells [44,45], our case with subarachnoid hemorrhage presented a CSF sample with 45×106 red blood cells/L and only 0.104×106 white blood cells/L. Therefore, when both red and white blood cell counts are elevated in bloody CSF, priority should be given to considering the possibility of CNS infections.
4.4. Survival Analysis
Due to the need for postoperative radiation therapy and chemotherapy in glioma patients, the occurrence of postoperative CNS infections is likely to delay the timing of patients' receipt of these treatments. Therefore, we explored whether the occurrence of postoperative CNS infections in glioma patients would affect their prognosis. Among the 337 patients, a total of 107 patients had survival data, with 91 not experiencing CNS infections and 16 developing CNS infections. Kaplan-Meier survival analysis showed no significant difference between the two groups. We did not find any relevant literature reporting a correlation between the occurrence of CNS infections in gliomas and patient prognosis. Irene S. Kourbeti's study mentioned that in patients undergoing various types of craniotomies, the occurrence of infections in other sites postoperatively was not significantly correlated with patient prognosis [6].
5. Conclusions
In this study, we have identified the significance of ventricular opening during glioma resection in relation to the occurrence of postoperative CNS infections. Additionally, we have found that parameters such as post-op other systemic infections, post-op maximum cavity diameter, and monocyte % have predictive value for postoperative CNS infections. We have summarized the cerebrospinal fluid (CSF) characteristics of patients who develop CNS infections, providing a reference for the diagnosis of CNS infections in cases where CSF microbiological cultures yield negative results.
Furthermore, we have proposed that Meropenem is an effective treatment for postoperative CNS infections following glioma surgery. Importantly, our study has shown that CNS infections does not impact the prognosis of glioma patients. We believe that these findings will assist neurosurgeons in the personalized prevention, diagnosis, and treatment of postoperative CNS infections in glioma patients.
6. Limitations
This study is a retrospective analysis conducted at a single center, with the primary population being glioma patients rather than encompassing all patients undergoing craniotomy. In the survival analysis, only 107 patients had available survival data. So we are planning to establish prospective cohort studies to explore whether there are opportunities for optimization in clinical practice to further reduce the incidence of postoperative CNS infections in glioma patients. For instance, we will focus on interventions related to the independent risk factors identified in this analysis. An example is studying whether increasing the duration of prophylactic antibiotic use in patients with ventricular opening can lower the incidence of CNS infections. And further investigation will involve a stratified analysis based on tumor tissue type and grade to explore whether postoperative CNS infections impacts patient outcomes.
Ethics Approval and Consent to Participate
This study is a clinical retrospective study, so we are not able to provide informed consents from all the patients (whose data are used for research). But the study has obtained ethical approval from The Ethics Review Committee of Peking Union Medical College Hospital, Chinese Academy of Medical Sciences, with ethical code K23C1427. The statement regarding consent waiver can be found in related files. The full name of the committee/IRB which waived the need for informed consent: The Ethics Review Committee of Peking Union Medical College Hospital, Chinese Academy of Medical Sciences.
Supplementary Materials
The following supporting information can be downloaded at: Preprints.Org.
Author Contributions
Methodology, X.G.; formal analysis, X.Z. and Z.Z.; data curation, H.W. and L.G.; writing—original draft preparation, X.Z. Z.Z. X.G. H.W. and L.G.; writing—review and editing, Y.W. F.G. and W.M.; supervision, Y.W. and F.G.; funding acquisition, W.M. All authors have read and agreed to the published version of the manuscript.
Funding
This work was funded by the National High-Level Hospital Clinical Research Funding (2022-PUMCH-A-019) for Yu Wang and by the National High-Level Hospital Clinical Research Funding (2022-PUMCH-B-113) for Wenbin Ma.
Conflicts of Interest
All authors declared no conflict of interest.
Consent for Publication
All authors consent to the publication of this manuscript in the Journal of Clinical Medicine.
Availability of Data and Materials
The datasets analysed during the current study can be found in Supplementary Materials.
References
- MC, R. M. EA, and F. FA, - Hospital-acquired meningitis in patients undergoing craniotomy: incidence. - Am J Infect Control. 2002 May;30(3):158-64. (- 0196-6553 (Print)): p. - 158-64. [CrossRef]
- AM, K. et al. - Risk factors for adult nosocomial meningitis after craniotomy: role of antibiotic. - Neurosurgery. 2006 Jul;59(1):126-33; discussion 126-33. (- 1524-4040 (Electronic)): p. - 126-33; discussion 126-33.
- McClelland S, r. and H. WA, - Postoperative central nervous system infection: incidence and associated factors. - Clin Infect Dis. 2007 Jul 1;45(1):55-9. Epub 2007 May 21. (- 1537-6591 (Electronic)): p. - 55-9. [CrossRef]
- X, G. et al. - Clinical updates on gliomas and implications of the 5th edition of the WHO. - Front Oncol. 2023 Mar 14;13:1131642. eCollection, (- 2234-943X (Print)): p. - 1131642. [CrossRef]
- C, H. et al. - NCCN Guidelines® Insights: Central Nervous System Cancers, Version 2.2022. - J Natl Compr Canc Netw. 2023 Jan;21(1):12-20. (- 1540-1413 (Electronic)): p. - 12-20. [CrossRef]
- IS, K. et al. - Infections in patients undergoing craniotomy: risk factors associated with. - J Neurosurg. 2015 May;122(5):1113-9. Epub 2014 Oct, (- 1933-0693 (Electronic)): p. - 1113-9. [CrossRef]
- S, G. and H. R, - The Use of Adjunctive Steroids in Central Nervous Infections. - Front Cell Infect Microbiol. 2020 Nov 23;10:592017. (- 2235-2988 (Electronic)): p. - 592017.
- ML, D. et al. - Acute bacterial meningitis in adults. A review of 493 episodes. - N Engl J Med. 1993 Jan 7;328(1):21-8. (- 0028-4793 (Print)): p. - 21-8. [CrossRef]
- KW, W. et al. - Post-neurosurgical nosocomial bacterial meningitis in adults: microbiology.
- TC, H. A. M, and D. MA, - CDC/NHSN surveillance definition of health care-associated infection and criteria. - Am J Infect Control. 2008 Jun;36(5):309-32. (- 1527-3296 (Electronic)): p. - 309-32. [CrossRef]
- WM, T. et al. - CSF markers for diagnosis of bacterial meningitis in neurosurgical postoperative. - Arq Neuropsiquiatr. 2006 Sep;64(3A):592-5. (- 0004-282X (Print)): p. - 592-5. [CrossRef]
- O, M. et al. - Additive risk of surgical site infection from more than one risk factor following. - J Neurooncol. 2023 Apr;162(2):337-342. Epub 2023, (- 1573-7373 (Electronic)): p. - 337-342. [CrossRef]
- B, Y. et al. - Blood‒Brain Barrier Pathology and CNS Outcomes in Streptococcus pneumoniae. - Int J Mol Sci. 2018 Nov 11;19(11):3555. (- 1422-0067 (Electronic)): p. T - epublish. [CrossRef]
- RA, H. et al. - The role of pneumolysin in pneumococcal pneumonia and meningitis. - Clin Exp Immunol. 2004 Nov;138(2):195-201. (- 0009-9104 (Print)): p. - 195-201. [CrossRef]
- D, F. and W. GW, - Invasive Pneumococcal and Meningococcal Disease. - Infect Dis Clin North Am. 2019 Dec;33(4):1125-1141. (- 1557-9824 (Electronic)): p. - 1125-1141.
- EW, G. et al. - Pneumonia, Meningitis, and Septicemia in Adults and Older Children in Rural. - Clin Infect Dis. 2023 Feb 18;76(4):694-703. (- 1537-6591 (Electronic)): p. - 694-703. [CrossRef]
- C, Z. et al. - Simultaneous Detection of Key Bacterial Pathogens Related to Pneumonia and. - Front Cell Infect Microbiol. 2018 Apr 5;8:107. (- 2235-2988 (Electronic)): p. - 107. [CrossRef]
- A, R. et al. - Infant Escherichia coli urinary tract infection: is it associated with. - Arch Dis Child. 2022 Mar;107(3):277-281. (- 1468-2044 (Electronic)): p. - 277-281. [CrossRef]
- M, T. P. A, and C. N, - Question 1. How common is co-existing meningitis in infants with urinary tract. - Arch Dis Child. 2011 Jun;96(6):602-6. (- 1468-2044 (Electronic)): p. - 602-6. [CrossRef]
- SS, W. B. DN, and C. AT, - Prevalence of Concomitant Acute Bacterial Meningitis in Neonates with Febrile. - J Pediatr. 2017 May;184:199-203. Epub 2017 Feb, (- 1097-6833 (Electronic)): p. - 199-203. [CrossRef]
- J, N. et al. - Risk of Meningitis in Infants Aged 29 to 90 Days with Urinary Tract Infection: A. - J Pediatr. 2019 Sep;212:102-110.e5. Epub 2019, (- 1097-6833 (Electronic)): p. - 102-110.e5. [CrossRef]
- PL, A. et al. - Prevalence of Urinary Tract Infection, Bacteremia, and Meningitis Among Febrile. - JAMA Netw Open. 2023 May 1;6(5):e2313354. (- 2574-3805 (Electronic)): p. - e2313354.
- LK, M. and H. DA, - Urinary Tract Infection: Pathogenesis and Outlook. - Trends Mol Med. 2016 Nov;22(11):946-957. Epub, (- 1471-499X (Electronic)): p. - 946-957. [CrossRef]
- GS, B. et al. - Tissue Immunity in the Bladder. - Annu Rev Immunol. 2022 Apr 26;40:499-523. (- 1545-3278 (Electronic)): p. - 499-523.
- PC, P. et al. - Rotating Gamma System Irradiation: A Promising Treatment for Low-grade Brainstem. - In Vivo. 2017 Sep-Oct;31(5):957-960. (- 1791-7549 (Electronic)): p. - 957-960. [CrossRef]
- Y, L. et al. - Expression of VEGF and MMP-9 and MRI imaging changes in cerebral glioma. - Oncol Lett. 2011 Nov;2(6):1171-1175. Epub 2011 Aug 17. (- 1792-1074 (Print)): p. - 1171-1175. [CrossRef]
- D, K. et al. - Technical principles in glioma surgery and preoperative considerations. - J Neurooncol. 2016 Nov;130(2):243-252. Epub 2016, (- 1573-7373 (Electronic)): p. - 243-252. [CrossRef]
- S, I. et al. - Tractography for Subcortical Resection of Gliomas Is Highly Accurate for Motor. - Cancers (Basel). 2021 Apr 9;13(8):1787. (- 2072-6694 (Print)): p. T - epublish. [CrossRef]
- JP, A. et al. - Inflammatory Monocytes and Neutrophils Regulate Streptococcus suis-Induced. - Infect Immun. 2020 Feb 20;88(3):e00787-19. Print 2020, (- 1098-5522 (Electronic)): p. T - epublish. [CrossRef]
- G, L. et al. - Cytokine and immune cell profiling in the cerebrospinal fluid of patients with. - J Neuroinflammation. 2019 Nov 14;16(1):219. (- 1742-2094 (Electronic)): p. - 219. [CrossRef]
- M, D. et al. - Circulating monocytes engraft in the brain, differentiate into microglia and. - Brain. 2006 Sep;129(Pt 9):2394-403. Epub 2006 Aug 3. (- 1460-2156 (Electronic)): p. - 2394-403. [CrossRef]
- TJ, B. et al. - Salmonella Meningitis Associated with Monocyte Infiltration in Mice. - Am J Pathol. 2017 Jan;187(1):187-199. Epub, (- 1525-2191 (Electronic)): p. - 187-199. [CrossRef]
- JL, S. M. CR, and A. DJ, - Surgical Site Infection Prevention: A Review. - JAMA. 2023 Jan 17;329(3):244-252. (- 1538-3598 (Electronic)): p. - 244-252. [CrossRef]
- R, M. et al. - The safety and efficacy of dexamethasone in the perioperative management of. - J Neurosurg. 2021 Sep 24;136(4):1062-1069. Print, (- 1933-0693 (Electronic)): p. - 1062-1069. [CrossRef]
- KS, D. and K. PU, - Optimal Management of Corticosteroids in Patients with Intracranial Malignancies. - Curr Treat Options Oncol. 2020 Jul 30;21(9):77. (- 1534-6277 (Electronic)): p. - 77. [CrossRef]
- HR, M. and B. SD, - Aseptic and Bacterial Meningitis: Evaluation, Treatment, and Prevention. - Am Fam Physician. 2017 Sep 1;96(5):314-322. (- 1532-0650 (Electronic)): p. - 314-322.
- JM, C. et al. - Repeat lumbar puncture in adults with bacterial meningitis. - Clin Microbiol Infect. 2016 May;22(5):428-33. (- 1469-0691 (Electronic)): p. - 428-33. [CrossRef]
- OH, H.O. et al. - Development of a prediction rule for diagnosing postoperative meningitis: a. - J Neurosurg. 2018 Jan;128(1):262-271. Epub 2017, (- 1933-0693 (Electronic)): p. - 262-271. [CrossRef]
- HO, E. et al. - Clinical Infections, Antibiotic Resistance, and Pathogenesis of Staphylococcus. - Microorganisms. 2022 May 31;10(6):1130. (- 2076-2607 (Print)): p. T - epublish. [CrossRef]
- CR, H. et al. - Coagulase-negative staphylococcal meningitis in adults: clinical characteristics. - Infection. 2005 Apr;33(2):56-60. (- 0300-8126 (Print)): p. - 56-60. [CrossRef]
- R, S. et al. - Outcome following postneurosurgical Acinetobacter meningitis: an institutional. - Neurosurg Focus. 2019 Aug 1;47(2):E8. (- 1092-0684 (Electronic)): p. - E8. [CrossRef]
- CM, B. L.-W. KA, and K. SJ, - Meropenem: a review of its use in the treatment of serious bacterial infections. - Drugs. 2008;68(6):803-38. (- 0012-6667 (Print)): p. - 803-38. [CrossRef]
- GG, Z. et al. - Comparative review of the carbapenems.
- KS, Y. and C. EM, - Diagnosis of acute stroke. - Am Fam Physician. 2015 Apr 15;91(8):528-36. (- 1532-0650 (Electronic)): p. - 528-36.
- B, S. C. EY, and N. G, - Cerebrospinal Fluid Analysis. - Am Fam Physician. 2021 Apr 1;103(7):422-428. (- 1532-0650 (Electronic)): p. - 422-428.
Figure 1.
Kaplan-Meier survival analysis of patients with and without meningitis(Unit: Days).
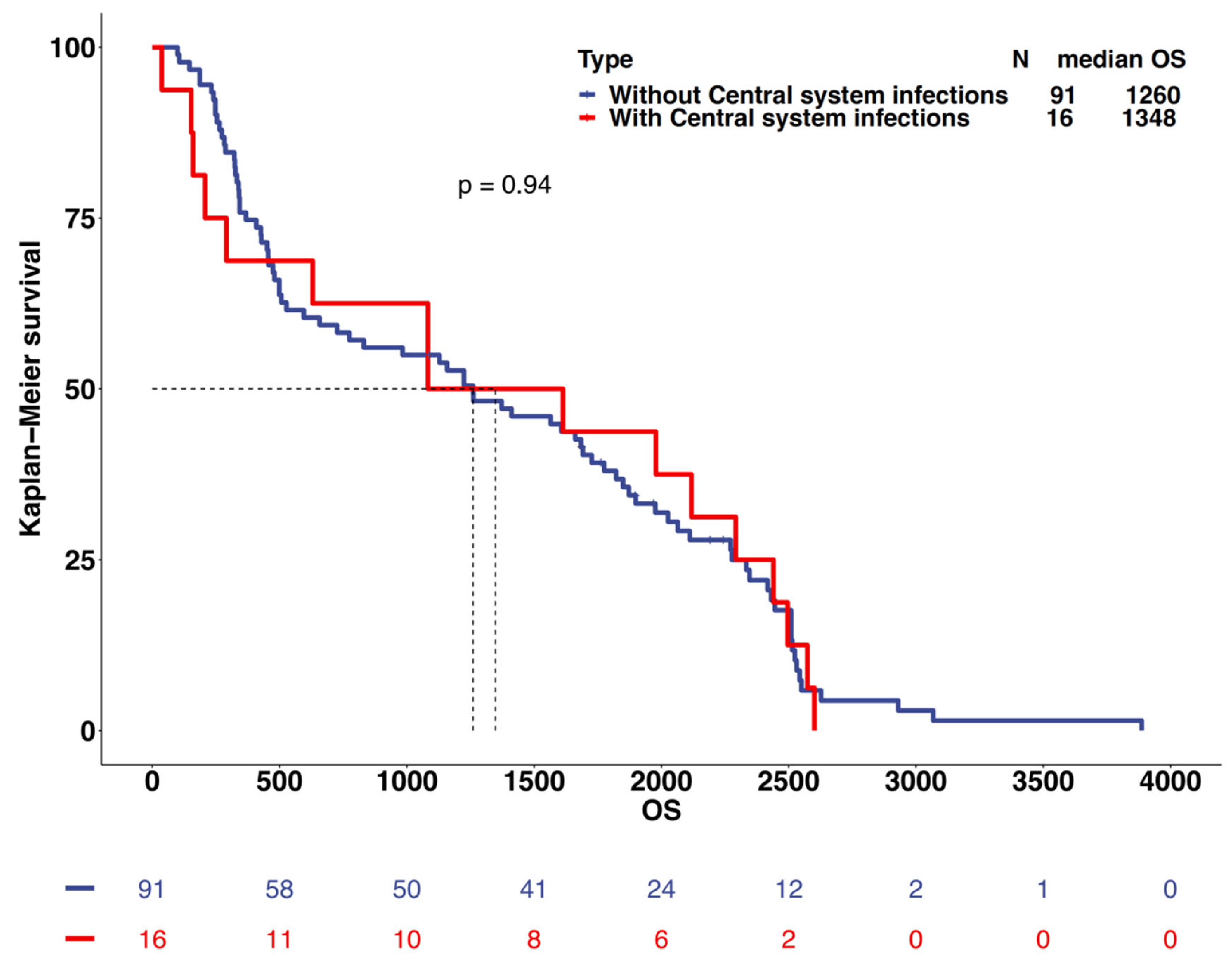

Table 1.
Comparison of the 2 groups regarding the development of CNS Infections. Continuous variables data are presented with n(%), while categorical variables data are represented by the Median[IQR]. Abbreviation: BMI=body mass index; Pre-op=pre-operation; Post-op=post-operation; The explanation of the Post op Maximum Cavity Diameter can be found in Figure 2.
Table 1.
Comparison of the 2 groups regarding the development of CNS Infections. Continuous variables data are presented with n(%), while categorical variables data are represented by the Median[IQR]. Abbreviation: BMI=body mass index; Pre-op=pre-operation; Post-op=post-operation; The explanation of the Post op Maximum Cavity Diameter can be found in Figure 2.
| Variable | No CNS Infections | CNS Infections | p Value |
|---|---|---|---|
| No. of Procedures | 276 | 61 | |
| Age(yrs) | 47.00 [33.75, 57.00] | 46.00 [34.00, 55.00] | 0.67 |
| Female Sex | 123 (44.57%) | 23 (37.70%) | 0.40 |
| BMI | 24.03 [20.29, 27.77] | 24.76 [21.03, 28.49] | 0.17 |
| Primary Glioma | 231 (83.70%) | 51 (83.61%) | 1.00 |
| Diabetes mellitus | 16 (5.80%) | 2 (3.28%) | 0.63 |
| Comorbidities in Other Systems | 113 (40.94%) | 27 (44.26%) | 0.74 |
| Pre-op Radiotherapy | 40 (14.49%) | 12 (19.67%) | 0.41 |
| Pre-op Chemotherapy | 36 (13.04%) | 12 (19.67%) | 0.26 |
| Pre-op Steroid Use | 76 (27.54%) | 16 (26.23%) | 0.96 |
| Pre-op Concomitant Organ Infections | 3 (1.09%) | 3 (4.92%) | 0.13 |
| Pre-op Tumor Necrosis | 173 (62.68%) | 41 (67.21%) | 0.60 |
| Maximum Tumor Diameter(mm) | 41.60 [32.15, 55.00] | 49.50 [40.00, 60.00] | <0.01 |
| Surgery Duration(hours) | 5.00 [4.00, 6.30] | 5.50 [4.70, 7.00] | 0.01 |
| Ventricle Opened | 48 (17.39%) | 29 (47.54%) | <0.01 |
| Frontal/Ethmoid Opened | 18 (6.52%) | 4 (6.56%) | 1.00 |
| Tumor Cavity Catheter Insertion | 95 (34.42%) | 37 (60.66%) | <0.01 |
| External Drain Duration(days) | 0.00 [0.00, 1.00] | 1.00 [0.00, 3.00] | <0.01 |
| Post-op Other Systemic Infections | 10 (3.62%) | 11 (18.03%) | <0.01 |
| Post-op Seizures | 16 (5.80%) | 3 (4.92%) | 1.00 |
| Post-op Steroid Use | 254 (92.03%) | 59 (96.72%) | 0.31 |
| Post-op Maximum Cavity Diameter(mm) | 43.15 [33.77, 54.82] | 53.90 [46.90, 63.70] | <0.01 |
| Multiple Hospital Surgeries | 1 (0.36%) | 4 (6.56%) | <0.01 |
| Pre-op Blood Cell Tests | |||
| Absolute WBC Count (×10^9/L) | 6.20 [5.19, 7.74] | 6.53 [4.94, 8.17] | 0.57 |
| Absolute Lymphocyte Count(×10^9/L) | 1.74 [1.34, 2.22] | 1.68 [1.32, 2.12] | 0.38 |
| Lymphocyte % | 28.79 [18.92,38.66] | 27.20 [18.43,35.97] | 0.25 |
| Absolute Monocyte Count(×10^9/L) | 0.35 [0.28, 0.43] | 0.37 [0.30, 0.47] | 0.14 |
| Monocyte % | 5.60 [4.68, 6.50] | 6.30 [4.90, 6.90] | 0.03 |
| Absolute Neutrophil Count(×10^9/L) | 3.75 [2.83, 4.87] | 3.70 [2.89, 5.42] | 0.48 |
| Neutrophil % | 60.80 [54.05, 68.82] | 62.60 [56.00, 69.60] | 0.24 |
| Absolute Eosinophil Count (×10^9/L) | 0.09 [0.05, 0.15] | 0.08 [0.05, 0.14] | 0.76 |
| Eosinophil % | 1.50 [0.80, 2.50] | 1.50 [0.80, 2.60] | 0.94 |
| Absolute Basophil Count (×10^9/L) | 0.03 [0.02, 0.03] | 0.02 [0.02, 0.04] | 0.97 |
| Basophil % | 0.40 [0.30, 0.60] | 0.40 [0.20, 0.60] | 0.83 |
Table 2.
Multivariate analysis for the risk for meningitis.
| Variable | OR | CI | P |
|---|---|---|---|
| Ventricle Opened | 2.97 | 1.54-5.71 | <0.01 |
| Post-op Other Systemic Infections | 4.03 | 1.34-12.14 | 0.01 |
| Post-op Maximum Cavity Diameter | 1.03 | 1.01-1.06 | 0.02 |
| Monocyte % | 1.19 | 1.01-1.41 | 0.04 |
| Tumor Cavity Catheter Insertion | 1.63 | 0.66-4.02 | 0.29 |
| External Drain Duration | 1.07 | 0.84-1.38 | 0.57 |
| Maximum Tumor Diameter | 1.00 | 0.97-1.02 | 0.72 |
| Surgery Duration | 0.96 | 0.81-1.15 | 0.66 |
| Multiple Hospital Surgeries | 8.10 | 0.73-89.54 | 0.09 |
Table 3.
CSF characteristics of the 61 patients who had CNS infections.
| Variable | Median | IQR | Reference |
|---|---|---|---|
| Protein(g/L) | 1.73 | [1.03, 3.06] | 0.15-0.45 |
| Glucose(mmol/L) | 2.7 | [1.90, 3.70] | 2.4-4.5 |
| Chloride(mmol/L) | 120 | [116.00, 122.00] | 120-132 |
| WBC(10^6/L) | 1478 | [467, 4204.25] | 0-8 |
| Multinucleated Cell % | 84.1 | [74.55, 90.83] | <70 |
Table 4.
Pathogenic culture and drug sensitivity results of cerebrospinal fluid.
| Bacteria | Sensitive Antibiotics | Resistant Antibiotics |
|---|---|---|
| Staphylococcus haemolyticus | Gentamicin,Linezolid, Selectrin,Teicoplanin, Vancomycin |
Ciprofloxacin,Oxacillin, Erythromycin,Penicillin G |
| Staphylococcus epidermidis | Gentamicin,Linezolid, Vancomycin,Rifampicin, Selectrin,Teicoplanin |
Oxacillin,Penicillin G |
| Acinetobacter baumanii |
Minocycline,Tigecycline | Amikacin,Ceftazidime, Ciprofloxacin,Levofloxacin,Cefperazone-Sulbactam,Meropenem,Selectrin, Sulbactam-Ampicillin, Doxycycline,Cefepime, Imipenem,Tobramycin, Piperacillin-Tazobactam |
Table 5.
Antibiotic use in patients with meningitis.
| Antibiotic Varieties | Frequency of Use(n=50) | Average Time of Use(days) | |
|---|---|---|---|
| Gram-positive | Vancomycin | 43 | 7.79 |
| Linezolid | 4 | 7.75 | |
| Gram-negative | Meropenem | 27 | 8.41 |
| Cefperazone | 17 | 6.88 | |
| Ceftriaxone | 6 | 6.83 | |
| Ceftazidime | 7 | 8.43 | |
| Common Antibiotic Combinations | Meropenem+ Vancomycin |
23 | 8.13 |
| Cefperazone+ Vancomycin | 8 | 6.13 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



