
Submitted:
06 October 2024
Posted:
08 October 2024
You are already at the latest version
Abstract
Background and clinical significance: Guyon's canal syndrome is a pathological condition caused by compression of the ulnar nerve at the level of the wrist. It is less frequent than other compression syndromes of the upper limb (cubital and carpal tunnel), and different causative agents, including vascular lesions, are described. Among these, aneurysm of the ulnar artery is described in the literature as an infrequent aetiology.
Case Presentation: We report the case of a 25-year-old young man with Guyon's canal syndrome caused by an aneurysm of the ulnar artery, who underwent surgical decompression of the Guyon's canal without intervening on the aneurysm. The postoperative course was free of complications, and the patient reported satisfaction, with reduced symptoms. Clinical examination and ultrasound imaging showed mass reduction of the aneurysm in the postoperative period, which appears to be an evolution hitherto undocumented in the literature.
Conclusions: Many treatments are available for Guyon's canal syndrome. Past medical and surgical treatments, duration and severity of symptoms, causes, and pathogenesis are important for the therapeutic choice. Surgical treatment based on ligament section and lysis of the Guyon's canal downstream, without any action on the aneurysm and with ulnar artery preservation, determined a reduction in terms of volume, relief of the symptoms, and patient satisfaction.
With this case we describe a surgical therapeutic option for the treatment of Guyon's canal syndrome caused by an aneurysm of the ulnar artery, in which surgery is limited to canal decompression and consequential aneurism mass reduction with concomitant relief of symptoms.
Keywords:
Guyon's canal syndrome
; Hypothenar Hammer Syndrome
; Ulnar artery Aneurysm
1. Introduction and Clinical Significance
The ulnar nerve originates at C8-T1 and is a terminal branch of the brachial plexus, it reaches the hand via Guyon’s canal to provide motor and sensory innervation to the hand and digits. Guyon’s canal is a less frequent site of ulnar nerve compression injury, second to the cubital tunnel at the level of the medial epicondyle of the humerus.
The boundaries of Guyon’s canal include its anatomic “roof”, the palmar or volar carpal ligament, and its “floor”, the flexor retinaculum or transverse carpal ligament. The transverse carpal ligament runs deep to Guyon’s canal ulnarly (medially) at the level of the wrist while its radial (lateral) portion runs superficial to the median nerve, forming the "roof" of the carpal tunnel.
The Pisiform bone, Piso-hamate ligament, and abductor digiti minimi represent the ulnar boundary, while the hook of the hamate (hamulus) represents the radial boundary.
There are many potential deleterious stimuli to the distal ulnar nerve, including compression, inflammation, trauma, or vascular insufficiency. Aetiologies include:
Ganglion Cyst; the hook of hamate Fracture/Displacement; Tumours (lipoma); Repetitive trauma (Cyclist's handlebar external compression); Aberrant Muscle (e.g., abductor digiti minimi) or excess fat tissue within the canal; Ulnar artery thrombosis or aneurysm (e.g., Hypothenar Hammer Syndrome, a rare occupational or recreational malady, resulting from repetitive microtrauma to the ulnar artery at the level of Guyon's canal) [1,2]. Guyon’s canal syndrome is a relatively rare peripheral ulnar neuropathy that involves injury to the distal portion of the ulnar nerve as it travels through a narrow anatomic corridor at the wrist and is usually treated through canal decompression and possible therapy of the associated lesion. With this case report we describe a case of aneurysm-associated ulnare nerve compression at the Guyon’s canal, successfully treated with simple decompression through canal decompression.
2. Case Presentation
A 25-year old right hand dominant patient presented to the plastic surgery department, with several symptoms compatible with Guyon’s canal syndrome.
The patient was a manual worker, who was suffering from an aneurysm in the volar region of the left-hand ulnar artery of approximately 19 mm at maximum diameter, between the deep subcutaneous tissue and the muscle of the hypothenar eminence, with the presence of a 4mm thrombus on the posterior wall, confirmed both by ultrasound and MRI. He did not report any pathology, no allergies and no G6PDH deficiency, he was a smoker.
In his work history he reported being a gutter worker.
The patient reported chronic pain in the left hand with paresthesia localized predominantly to the volar region of the left hand, and the 3rd, 4th, and 5th fingers.
Pain, discomfort and paresthesia were present for over 1.5 years. Ultrasound imaging allowed the diagnosis of an ulnar artery aneurysm of approximately 19 mm (Figure 1)
The treatment consisted of a locoregional block, with volar incision to the palm under regional anaesthesia, sedation, and arm tourniquet, followed by section of the volar carpal ligament and dissection of the ulnar fascicle to the depth and distal part of the Guyon’s canal, with separation of the aneurysmatic artery from the nerve (Figure 2).
The patient was discharged after one day of hospitalization with the recommendation to carry out ultrasound scans in the following months. The postoperative course was caracterized by immediate improvement of neurological symptoms (reduction of pain and improvement of sensitivity).
In particular, two months post operative ultrasonography proved the reduction of the aneurysm from 19mm to 16,3mm (Figure 3) and a three month post operative ultrasonography a further reduction at 16mm (Figure 4). Six months after the procedure the patient is completely pain-free and with full sensation recovery to the ulnar area of his hand.
3. Discussion
Our proposed hypothesis is that manual labor, with chronic work of repetitive percussion on the hook of the hamate of the left hand, has gradually caused inflammation that has determined chronic oedema, with stagnation of fluids that has led to fibrosis with narrowing of the Guyon's canal and this has had repercussions on the ulnar artery that has been narrowed downstream causing an aneurysmal dilation upstream, thus leading to the formation of this aneurysm over the time.
In the literature there are many medical and surgical therapies proposed for the treatment of hypothenar hammer syndrome.
Conservative treatment options are used for patients who are not at risk for tissue loss, necrosis, or active ischemia. Conservative treatments include activity modification, smoking cessation, pain control, calcium channel blockers, ⍺-blockers, β-blockers, and steroids.
Intravenous and oral vasodilators, including prostaglandins and prostacyclin, have been used to decrease sympathetic tone and vasospasm [3]
Nonoperative treatment employs a percutaneous approach. One technique directs intra-arterial thrombolytics to the site of ulnar artery thrombosis. Catheter-directed thrombolytic administration with recombinant tissue plasminogen activator or urokinase is performed in this therapeutic option. These intra-arterial treatments are less invasive, but they often do not resolve the neurological symptoms underlying Guyon’s canal syndrome. Furthermore, they are not without complications; in particular, complications of thrombolytic therapy include access site hematoma and bleeding. [3]
Regarding surgical treatment, a similar case was addressed by Zied et al [4], who reported a case of a young man, diagnosed with Guyon's canal syndrome caused by an ulnar artery aneurysm, who underwent surgical decompression. The surgical treatment consisted of opening and releasing the roof of Guyon's canal with removal of the aneurysm with good post-operative results. However, this approach resulted in the sacrifice of the ulnar artery, which was ligated, with a consequent reduction in vascular flow to the hand.
Another treatment proposed for hypothenar hammer syndrome due to an aneurysm of ulnar artery is the simple ligation of the ulnar artery [5].
A different surgical approach was discussed by Hui-chou HG et al [6] through resection of the abnormal arterial segment with ligation of vessel or reconstruction with venous [7] or arterial grafts [8]. But this kind of surgery requires an expert microsurgery team (which is not always available in a plastic surgery department) and/or surgical robot [10] and may be subject to complications, like numbness in the donor site, neuroma formation, graft failure, thrombosis [8], and hypertrophic scar formation.
Our goal was to save the artery by performing a simple decompression at the level of the roof of Guyon's canal through the section of piso-hamate ligament and volar carpal ligament in such a way as to cause a reduction downstream of the compression with reduction of pressure and therefore reduction of the aneurysm itself, thus saving the ulnar artery. (Figure 2)
4. Conclusions
In conclusion, the authors propose a conservative surgery for the treatment of Guyon's canal syndrome caused by an ulnar artery aneurysm, through a simple decompression of the roof of the canal downstream, with a reduction of the upstream pressure thereby obtaining a significant reduction in the diameter of the aneurysm, proved by ultrasonography.
In fact, with this technique, there is a progressive and significant improvement in the clinical symptoms, without sacrificing the ulnar artery which is an important artery for the vascularization of the hand, the sacrifice of which can lead not only to a deficit in the perfusion of the hand and fingers (acutely), but also to alterations in sensitivity and problems of thermoregulation, mild muscle atrophy and ischemic pain (chronically).
Author Contributions
EG performed the planning and editing of the study, AG, MA, PS contributed with the editing, English grammar revision and literature search, FB carried out the surgery and supervised the study
Funding
This research received no external funding.
Institutional Review Board Statement
Ethical review for this case report was not required by the Ethics Committee of Medical University of Cagliari. The patient’s data have been anonymized.
Informed Consent Statement
Written informed consent has been obtained from the patient to publish this paper.
Data Availability Statement
The original data presented in the study are included in the case report, further inquiries can be directed to the corresponding author.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Dreizin D, Jose J. Hypothenar hammer syndrome. Am J Orthop (Belle Mead NJ). 4: Erratum in: Am J Orthop (Belle Mead NJ). 2012, 41, 2012.
- Monacelli G, Rizzo MI, Spagnoli AM, Monarca C, Scuderi N. Ulnar artery thrombosis and nerve entrapment at Guyon's canal: our diagnostic and therapeutic algorithm. In Vivo, 7: 24. [PubMed]
- Clifford PC, Martin MF, Sheddon EJ, et al. Treatment of vasospastic disease with prostaglandin E1. Br Med J. [CrossRef]
- Zied M, Farouk C, Mohsen C, Wajdi C, Ali H, Wael G. Guyon's canal syndrome resulting from an ulnar artery aneurysm: A case report. Int J Surg Case Rep. 1099. [CrossRef]
- Houshian S, Mahdi BH. Hypotenar hammer syndrome [Hypothenar hammer syndrome]. Ugeskr Laeger, 4: 16; 161, 4643. [CrossRef]
- Hui-Chou HG, Mc Clinton MA. Current options for treatment of hypothenar hammer syndrome. Hand Clin. [CrossRef]
- Malgras B, Mlynski A, Pierret C, Fossat S, de Kérangal X. Syndrome du marteau hypothénarien: cas clinique et revue de la littérature [Hypothenar hammer syndrome: case report and review of the literature]. J Mal Vasc, 2: 39. [CrossRef]
- Temming JF, van Uchelen JH, Tellier MA. Hypothenar hammer syndrome: distal ulnar artery reconstruction with autologous descending branch of the lateral circumflex femoral artery. Tech Hand Up Extrem Surg, 2: 15. [CrossRef]
- Facca S, Liverneaux P. Robotic assisted microsurgery in hypothenar hammer syndrome: a case report. Comput Aided Surg. [CrossRef]
- Athlani L, De Almeida YK, Maschino H, Dap F, Dautel G. Hypothenar hammer syndrome: A case of a late complication after surgery. Hand Surg Rehabil. [CrossRef]
Figure 1.
Preoperative ultrasonography, D1 shows the length of ulnar artery aneurysm (19mm).
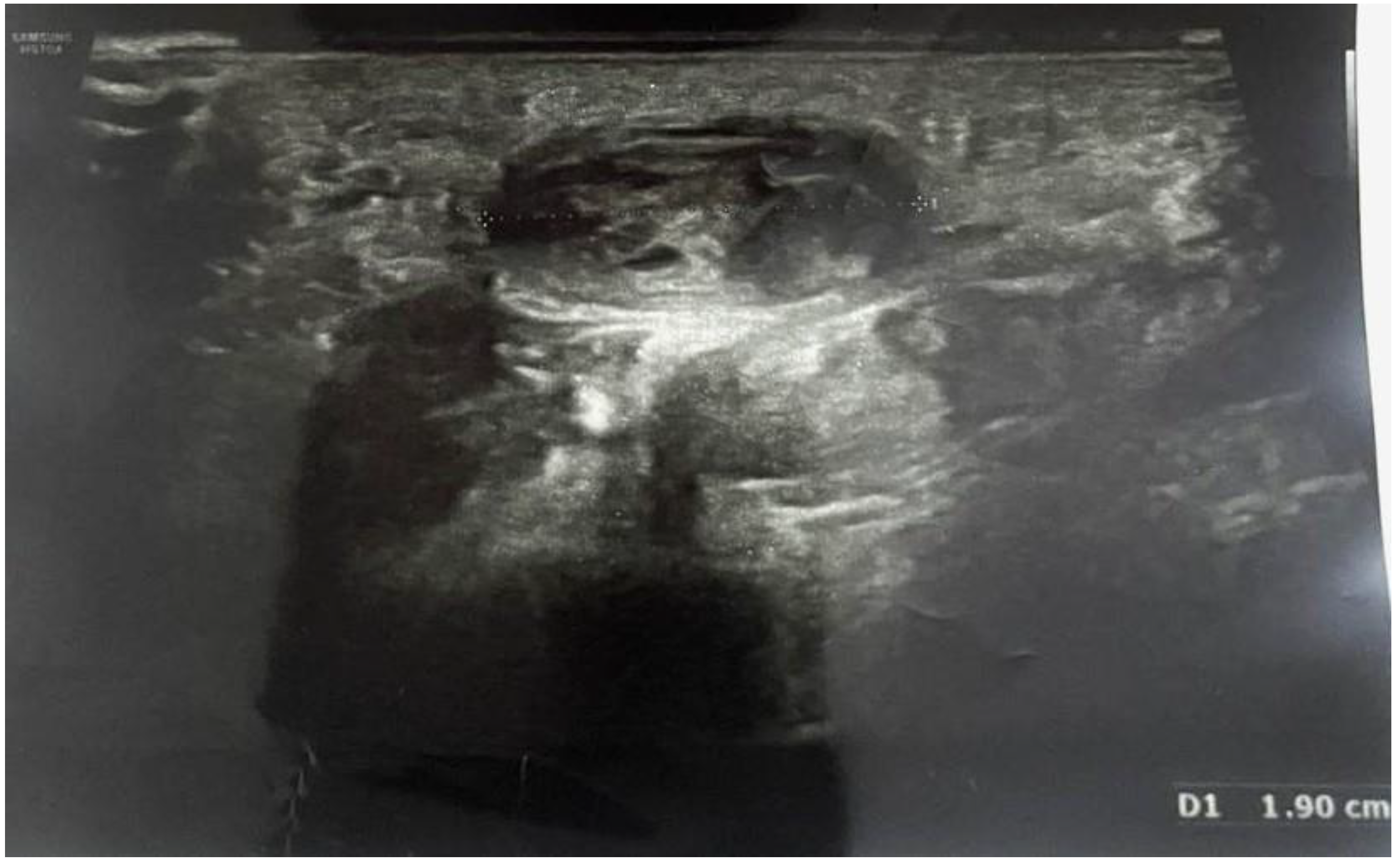
Figure 2.
Intraoperatory view; the aneurysm of the ulnar artery was identified. Dissection of the subcutaneous planes to expose ulnar nerve while preserving the ulnar nerve integrity. Complete section of the volar carpal ligament, and the most distal segment of the piso-hamate ligament.
Figure 2.
Intraoperatory view; the aneurysm of the ulnar artery was identified. Dissection of the subcutaneous planes to expose ulnar nerve while preserving the ulnar nerve integrity. Complete section of the volar carpal ligament, and the most distal segment of the piso-hamate ligament.

Figure 3.
Two month post operative ultrasonography shows a reduction of ulnar artery aneurysm, from 19mm to 16.3mm.
Figure 3.
Two month post operative ultrasonography shows a reduction of ulnar artery aneurysm, from 19mm to 16.3mm.

Figure 4.
Three month post operative ultrasonography shows a reduction of ulnar artery aneurysm, from 16.3mm to 16.0mm.
Figure 4.
Three month post operative ultrasonography shows a reduction of ulnar artery aneurysm, from 16.3mm to 16.0mm.

Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



