Submitted:
29 September 2024
Posted:
01 October 2024
You are already at the latest version
Abstract
The aim of the present review is to investigate the role of a toothpastes containing enzymes and proteins in supplementing natural salivary defenses. A systematic review was conducted using PRISMA with PROSPERO ID code CRD42024558854. An exhaustive search of PubMed, Web Of Science, and Scopus, using the PICO format was carried out. The used MeSH were enzymes; AND proteins; AND toothpaste. In vivo studies on humans analyzing the gum effects of a toothpaste containing enzymes and proteins, in the English language, published in the last 10 years were included. The search period started on 04 June 2024 and ended on 20 July 2024. The risk of bias was evaluated according to the Revised Cochrane risk-of-bias tool for randomized trials (RoB 2.0) while non-randomized studies were evaluated with the Cochrane risk-of-bias tool in Non-Randomized Studies (ROBINS-I). From a total of 62 studies, 3 were included. Two RCTs and had low and medium risk of bias, the N-RCT had low risk of bias. With the limitations of the present study, a toothpaste containing enzymes and proteins can improve gum health after 12 week and after 12 months, the role against black stains seemed not to be confirmed.
Keywords:
Enzymes
; Gingivitis
; Lactoferrin
; Lactoperoxidase
; Lysozyme
; Toothpaste
1. Introduction
The human oral cavity harbors a diverse microbiome, which plays a crucial role in maintaining oral health. The oral microbiome is a complex ecosystem composed of various microorganisms, including bacteria, fungi, viruses, and archaea. Among these, bacteria are the most studied, with over 700 species identified to date [1].
In a healthy individual, the oral microbiome exists in a state of dynamic equilibrium, with beneficial species outweighing harmful ones. This bacterial diversity is essential for preventing the overgrowth of single species, which could lead to disease. However, this delicate balance can be disrupted by various factors, including poor oral hygiene, host susceptibility, and environmental factors, leading to dysbiosis, a condition characterized by a shift towards a microbiome dominated by harmful species [2].
Gingivitis is an example of an oral condition caused by dysbiosis. In individuals with gingivitis, the plaque accumulated at the gingival margin leads to inflammation and a higher abundance of proteolytic and often obligate anaerobic species. [3]
Saliva contributes to shape the composition and function of the oral microbiome. It acts as the first line of defense against invading pathogens and provides a means to maintain homeostasis within the oral environment. Its protective properties stem from its components, including enzymes, proteins, and antimicrobial peptides [4].
One of the key defense mechanisms of saliva is the lactoperoxidase system (LPO system). This enzymatic system catalyzes the oxidation of thiocyanate ion, present in saliva, to hypothiocyanite, a potent antimicrobial agent, in the presence of hydrogen peroxide [5]. The hypothiocyanite produced by the LPO system demonstrates a broad-spectrum antibacterial activity against a diverse array of bacterial species, including those implicated in dental caries and periodontal diseases. This antimicrobial efficacy underscores the significance of the LPO system in safeguarding oral health. Hydrogen peroxide itself is an antimicrobial agent, produced by both the human host and some members of the oral microbiome, and contributes to oral defense by oxidizing thiocyanate to hypothiocyanite, a process that has been widely discussed in the literature. The hypothiocyanite produced by the LPO system exhibits antibacterial activity against a wide range of bacteria, including those associated with caries and periodontal diseases [6,7].
In addition to the LPO system, saliva contains several other enzymes and proteins that contribute to antimicrobial defense. Lysozyme in saliva breaks down bonds in peptidoglycan, a component of bacterial cell walls, leading to bacterial lysis and inhibiting the metabolic activity of various oral pathogens. Lactoferrin, an iron-binding glycoprotein present in saliva, sequesters free iron in the oral environment, depriving bacteria of this essential nutrient and limiting their growth. Moreover, lactoferrin exhibits direct bactericidal activity against specific cariogenic and periodontal pathogenic bacteria. Immunoglobulins, particularly secretory IgA (sIgA), are another crucial component of salivary defenses. sIgA binds to bacteria, preventing them from adhering to oral surfaces, and neutralizes bacterial toxins, thereby preventing tissue invasion and maintaining microbial balance [8].
An interesting study by Soares RV et al. [9] stated that salivary micelles have a distinct protein composition compared to whole saliva, containing a subset of proteins known to be important for the innate immune system. These proteins include high molecular weight proteins (MG2 and secretory IgA), intermediate molecular weight proteins (lactoferrin, amylase, and glycosylated proline-rich protein), and low molecular weight proteins (lysozyme).
Given the importance of saliva in maintaining oral health, toothpastes with enzymes and proteins have been developed to augment the natural salivary defenses [1]. These toothpastes typically contain enzymes such as amyloglucosidase, glucose oxidase, and lactoperoxidase, as well as proteins like lactoferrin and lysozyme, mimicking the enzyme and protein composition naturally present in saliva. The inclusion of these enzymes and proteins in toothpastes aims to enhance the natural defense system of saliva and promote a healthy oral environment. Amyloglucosidase and glucose oxidase have been shown to work synergistically to increase the production of hydrogen peroxide in saliva, thereby enhancing the activity of the lactoperoxidase system [10].
Studies have demonstrated that toothpastes containing enzymes and proteins can positively influence the composition of the oral microbiome, leading to an increase in the abundance of bacteria associated with gingival health and a decrease in bacteria associated with periodontal diseases A randomized clinical trial by Adams SE et al. [1] showed that a toothpaste containing enzymes and proteins led to a significant increase in 12 taxa associated with gingival health, including Neisseria spp. bacteria, and a significant decrease in 10 taxa associated with periodontal diseases, including Treponema spp. bacteria over a 14-week period. These shifts in the oral microbiome composition were associated with improvements in gingival health, as evidenced by reduced gingival inflammation, gingival bleeding, and plaque accumulation.
Moreover, toothpastes containing enzymes and proteins have been shown to enhance the antibacterial activity of saliva. For example, an in vitro study reported that treatment with a toothpaste containing enzymes and proteins increased hypothiocyanite levels in saliva, suggesting enhanced activity of the lactoperoxidase system. Furthermore, this study demonstrated that the enzymes and proteins in the toothpaste adversely affected the bacterial membrane integrity in Streptococcus mutans and Fusobacterium nucleatum, two bacteria commonly associated with caries and periodontal diseases [11].
The role of oral hygiene regimens on the diversity of the human oral microbiome is well investigated in literature. The subgingival plaque analysis conducted by Min K. et al. [12] highlighted the potential significance of mechanical flossing in maintaining oral health. Through viable bacterial enumeration utilizing vPCR, the study demonstrated that flossing can synergistically enhance the efficacy of mouthrinsing in reducing the total bacterial load and the abundance of F. nucleatum below the gingival margin. Moreover, flossing exhibited a selective inhibitory effect on Porphyromonas gingivalis. These findings were corroborated by clinical assessments of bleeding and inflammation further emphasizing the role of mechanical flossing in controlling subgingival plaque in conjunction with mouthrinsing.
The aim of the present review was to assess if a toothpastes containing enzymes and proteins can supplement the natural oral defenses, promoting a balanced oral microbiome and contributing to the management of gum health.
2. Materials and Methods
A systematic review was conducted using the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines for systematic reviews and meta-analysis [13] and registered on PROSPERO—International prospective register of systematic reviews—with the ID code CRD42024558854.
2.1. Literature Search
The objective of the literature browsing was to define pertinent studies analyzing the effect of a toothpaste containing enzymes and proteins on gum health in the last ten years. An exhaustive search of PubMed, Web Of Science, and Scopus, using the Patient/Population/Problem, Intervention, Comparison, and Outcome (PICO) format, was conducted.
• Population: humans of all ages;
• Intervention: gingivitis and gum health;
• Comparator: toothpaste without enzymes and proteins tested in humans;
• Outcomes: possible effects of a toothpaste with enzymes and proteins on gingivitis and gum health.
The following MeSH (Medical Subject Headings) were used: enzymes; AND proteins; AND toothpaste. The search period started on 04 June 2024 and ended on 20 July 2024.
2.2. Eligibility Criteria
The inclusion criteria were as follows: all in vivo studies on humans analyzing the gum effects of a toothpaste containing enzymes and proteins, in the English language, published in the last 10 years.
The following served as exclusion criteria: research about periodontitis, peri-implantitis, toothpaste with other technologies; papers about oral probiotics and non-oral environments; systematic reviews; metanalyses; editorials; abstracts; book chapters; papers not in English.
2.3. Data Extraction
Studies were appraised by two reviewers independently (S.D., M.D.), and a matrix of relevant data was produced. In cases of reviewer disagreement, consensus was sought, and if necessary, a third reviewer provided a final decision. Data extraction included general details corresponding to the properties of the studies (e.g., author, year of publication, sources of funding) and specific details about the type of enzymes and proteins used, gingival condition of the population investigated, time of administration and follow-up.
2.4. Quality Assessment
The risk of bias was evaluated according to the Revised Cochrane risk-of-bias tool for randomized trials (RoB 2.0) [14]. This tool is structured into five domains of bias, focusing on different aspects of trial design, conduct, and reporting. Within each domain, a series of questions ('signalling questions') aim to elicit information about features of the trial that are relevant to risk of bias. A proposed judgement about the risk of bias arising from each domain is generated by an algorithm, based on answers to the signalling questions. Judgement can be 'Low' or 'High' risk of bias, or can express 'Some concerns'. Non-randomized studies were evaluated with the Cochrane risk-of-bias tool in Non-Randomized Studies (ROBINS-I) [15].
3. Results
3.1. Study Selection
The starting search supplied a total of 62 studies: 20 from PubMed, 18 from Web of Science, and 24 from Scopus. No studies were deleted due to being ineligible by automation tools, while 17 studies were removed because of duplication. Overall, 36 studies were removed for other reasons, for example, for analyzing other molecules such as triclosan, stannous fluoride, phytocannabinoids, triclosan. A total of 9 studies accessed the screening phase, and a total of 6 studies were withdrawn because they failed to demonstrate any data of interest, for example, because they were conducted in vitro, in animals, for postbiotics or for chemotherapy induced oral mucositis. Eligibility was assigned to 3 studies based on their abstracts, no studies were erased for being systematic reviews, abstracts or editorials. For this reason, a total of 3 studies were incorporated for the inclusion phase (Figure 1) and analyzed according to their full text.
3.2. Detailed Results
Regarding the population age, 33% (1/3) of studies referred to young adults (< 25 y.o.), 33% (1/3) referred to adults (30-40 y.o.), and 33% enrolled people from all ages (18-56 y.o.). None of the studies selected investigated some gender differences. Regarding the periodontal indexes used, 66% (2/3) used the Modified Gingival Index (MGI), the gingival Bleeding Index (BI) and plaque assessments by use of the Modified Quigley and Hein index; 33% (1/3) used Decayed Missing Filled Teeth (DMFT) index, Gingival Bleeding Index (GBI) and Plaque Control Record. Only one study involved a cut-off value for MGI ranged 2.00-2.75. Just 33% (1/3) examined the effect of the test toothpaste on black stains. All the studies excluded subjects with systemic illness, periodontitis and ongoing antibiotic intake in the last 3 months. Follow-up period was heterogeneous: from 12 weeks, 14 weeks to one year.
3.3. Quality Assessment Results
The risk of bias assessment of the two included RCTs was carried out using the Cochrane RoB 2.0 tool. The study of Carelli M. et al. [16] was classified as having some concerns regarding the reported results, the study of Daly S. et al. [17] had low risk of bias. The details are presented in Figure 2. The overall risk of bias, with each category presented as percentages is presented in Figure 3.
The risk of bias assessment of the included N-RCT was carried out using the Cochrane ROBINS I tool. The study of Pedersen AML. et al. [18] was classified as having low risk of bias.
4. Discussion
Oral health balance is shaped by the oral microbiome. This review aimed to investigate the impact of a proteins and enzyme-containing toothpaste on individuals with gingivitis, focusing on clinical periodontal indices as indicators of oral health status. A healthy oral microbiome maintains a dynamic equilibrium, where beneficial species predominate over harmful ones. This microbial diversity is crucial for preventing the overgrowth of single species, which can lead to disease such as gingivitis [19].
The protective attributes of saliva are derived from a diverse array of components, including enzymes, proteins, and antimicrobial peptides [20]. The formation of dental plaque or biofilm is a key element in the pathomechanism of gingivitis and periodontitis.
The literature provides evidence that salivary LPO possesses the capacity to inhibit biofilm formation at various stages of its development [21]. Owing to its ability to adsorb onto the salivary pellicle [22], the LPO system has been demonstrated to effectively prevent the adhesion of precursor cariogenic microorganisms [23]. Comparable studies have been conducted on both single- and multispecies biofilms. Cawley et al. established that the LPO system, in conjunction with lactoferrin, lysozyme, and bovine milk immunoglobulins, can inhibit the formation of single-species S. mutans biofilms. However, when applied to multispecies biofilms (which more closely resemble in vivo biofilms), the LPO system resulted in a reduction of microbial viability without affecting biofilm mass [4]. This discrepancy can be attributed to the LPO system's ability to kill microorganisms while being unable to inactivate glucosyltransferases, the extracellular bacterial enzymes responsible for synthesizing glucans, the structural components of the biofilm matrix [24].
Additionally, by disrupting the bonds within peptidoglycan, lysozyme induces bacterial lysis, leading to the rupture of bacterial cells and the inhibition of their metabolic activities [25]. Lactoferrin, a glycoprotein present in saliva with an iron-binding affinity, sequesters free iron within the oral environment, thereby depriving bacteria of this essential nutrient and restricting their growth. It demonstrates direct bactericidal activity against specific cariogenic and periodontal pathogens [26].
Another critical component of the salivary defense system is represented by sIgA that bind to bacteria, thereby preventing their adherence to oral surfaces and neutralizing bacterial toxins. This dual action contributes to the prevention of tissue invasion and the maintenance of microbial balance within the oral cavity [27]. Due to the relevance of the saliva into the complex oral ecosystem, dentifrices with natural enzymes and proteins were developed. Enzymes typically contained in these products are glucose oxidase, lactoperoxidase and amyloglucosidase, as well as proteins like lactoferrin and lysozyme, mirroring the enzyme and protein composition found in saliva [28].
Regarding the studies included in the present review, Carelli et al. [16] in a 14-week RCT assessed that using a toothpaste containing enzymes and salivary proteins did not reveal significant alterations in the oral microbiota or oral health of test subjects compared to controls. While a reduction in certain pathogenic bacteria (P. gingivalis, P. intermedia, A. actinomycetemcomitans, A. naeslundii, T. forsythia, T. denticola, Actinomyces spp., Veillonella spp.) was observed in the saliva of test subjects, no changes were noted in dental plaque. These findings were interpreted by the authors as the test toothpaste may have limited efficacy against planktonic bacteria in saliva but may have little or no impact on the bacteria that form dental plaque biofilm. However, the study was limited to a small sample of 16 patients with black stains followed for a short time.
The RCT by Daly S. et al. [17] indicates that brushing with a toothpaste containing natural proteins and enzymes is more effective in preventing gingivitis than a commercially available fluoride toothpaste with strong anti-plaque properties and does so without any adverse side effects. Even if the sample size is adequate, 229 participants, in this case the follow-up period was solely of 13 weeks.
Finally, the N-RCT of Pedersen AML et al. [18] stated that a consistent use of a fluoride toothpaste containing enzymes and proteins for at least a year is linked to better gum health than other fluoride toothpastes without these additional ingredients. Nevertheless, the current study and the previous one exclusively included participants with good oral health and no need for treatment for periodontitis or dental caries. Consequently, the findings may not be applicable to individuals with overt oral diseases like periodontitis or dental caries. Additionally, none of the studies included collected data on socioeconomic status, a known factor influencing oral health [29] and the composition of the oral microbiota [30]. Based on the reviewed studies, toothpastes containing enzymes and salivary proteins show promise in improving oral health. However, the evidence is limited by factors such as small sample sizes, short follow-up periods, and a focus on participants with good oral health.
The toothpaste tested in the studies included in this review contains fluoride and a mild surfactant Steareth-30 instead of sodium lauryl sulfate (SLS). In recent in vitro and in vivo studies Steareth-30 caused minimal gingival sloughing as compared to SLS [31]. However, patients were not asked directly to rate their experience following use of this toothpaste in terms of satisfaction with the taste or any oral discomfort, this is a limitation of all the studies included that should be addressed in future clinical studies.
Overall, while the evidence suggests that toothpastes containing enzymes and salivary proteins can be beneficial for oral health, further research is needed to fully understand their efficacy, particularly in individuals with existing oral diseases.
Limitations
One of the challenges encountered in our analysis was the variability in periodontal indices used across the studies, making it difficult to directly compare and draw definitive conclusions. The presence of heterogeneous samples, different ages, different kinds of clinical measurements, different follow-up were all confounding factors. Additionally, the diversity about the inclusion criteria for participants in the included studies represents a severe bias and makes comparison between studies unclear.
Clinical Relevance
The present systematic review highlighted that a toothpaste with an enzymatic technology (amyloglucosidase, glucose oxidase, and lactoperoxidase) as well as salivary proteins (lysozyme and lactoferrin) could be useful and effective in preventing gingivitis and in the managing of gingival inflammation both in the short and long term, thanks to the proved reduction of the Modified Gingival Index (MGI), Bleeding Index (BI), Plaque Index (PI).
5. Conclusions
The evidence available about the use of toothpaste with enzymes and proteins on gum health is poor. Only three studies were eligible for the present review purpose, and one of them presented some concerns for the quality assessment. The other two studies shared the idea that a toothpaste based on enzymes and proteins could be more effective in plaque and gingival inflammation control than a standard fluoride dentifrice. Despite these limitations, the positive findings regarding gum health improvement suggest that a toothpaste containing enzymes and proteins could be a valuable addition to oral care regimens. Moreover, future well-designed clinical studies are needed to assess the behavior of gingival indexes and microbiological changes in people using a toothpaste with enzymes and proteins.
Author Contributions
Conceptualization, S.D; methodology, S.D.; validation, S.D., M.D.; formal analysis, S.D.; investigation, S.D.; data curation, S.D.; writing—original draft preparation, S.D., M.D.; writing—review and editing, S.D.; supervision, M.D.; project administration, S.D. All authors have read and agreed to the published version of the manuscript.” Please turn to the CRediT taxonomy for the term explanation. Authorship must be limited to those who have contributed substantially to the work reported.
Funding
This research received no external funding.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Adams SE, Arnold D, Murphy B, Carroll P, Green AK, Smith AM, Marsh PD, Chen T, Marriott RE, Brading MG. A randomised clinical study to determine the effect of a toothpaste containing enzymes and proteins on plaque oral microbiome ecology. Sci Rep. 2017 Feb 27;7:43344. PMID: 28240240; PMCID: PMC5327414. [CrossRef]
- Lynge Pedersen AM, Belstrøm D. The role of natural salivary defences in maintaining a healthy oral microbiota. J Dent. 2019 Jan;80 Suppl 1:S3-S12. PMID: 30696553. [CrossRef]
- Sanz M, Beighton D, Curtis MA, Cury JA, Dige I, Dommisch H, Ellwood R, Giacaman RA, Herrera D, Herzberg MC, Könönen E, Marsh PD, Meyle J, Mira A, Molina A, Mombelli A, Quirynen M, Reynolds EC, Shapira L, Zaura E. Role of microbial biofilms in the maintenance of oral health and in the development of dental caries and periodontal diseases. Consensus report of group 1 of the Joint EFP/ORCA workshop on the boundaries between caries and periodontal disease. J Clin Periodontol. 2017 Mar;44 Suppl 18:S5-S11. PMID: 28266109. [CrossRef]
- Cawley A, Golding S, Goulsbra A, Hoptroff M, Kumaran S, Marriott R. Microbiology insights into boosting salivary defences through the use of enzymes and proteins. J Dent. 2019 Jan;80 Suppl 1:S19-S25. Epub 2018 Oct 30. PMID: 30389429. [CrossRef]
- Thomas EL, Milligan TW, Joyner RE, Jefferson MM. Antibacterial activity of hydrogen peroxide and the lactoperoxidase-hydrogen peroxide-thiocyanate system against oral streptococci. Infect Immun. 1994 Feb;62(2):529-35. PMID: 8300211; PMCID: PMC186138. [CrossRef]
- Wertz PW, de Szalay S. Innate Antimicrobial Defense of Skin and Oral Mucosa. Antibiotics (Basel). 2020 Apr 3;9(4):159. PMID: 32260154; PMCID: PMC7235825. [CrossRef]
- Ihalin R, Loimaranta V, Tenovuo J. Origin, structure, and biological activities of peroxidases in human saliva. Arch Biochem Biophys. 2006 Jan 15;445(2):261-8. Epub 2005 Aug 2. PMID: 16111647. [CrossRef]
- van 't Hof W, Veerman EC, Nieuw Amerongen AV, Ligtenberg AJ. Antimicrobial defense systems in saliva. Monogr Oral Sci. 2014;24:40-51. Epub 2014 May 23. PMID: 24862593. [CrossRef]
- Soares RV, Lin T, Siqueira CC, Bruno LS, Li X, Oppenheim FG, Offner G, Troxler RF. Salivary micelles: identification of complexes containing MG2, sIgA, lactoferrin, amylase, glycosylated proline-rich protein and lysozyme. Arch Oral Biol. 2004 May;49(5):337-43. PMID: 15041480. [CrossRef]
- Marsh PD, Do T, Beighton D, Devine DA. Influence of saliva on the oral microbiota. Periodontol 2000. 2016 Feb;70(1):80-92. PMID: 26662484. [CrossRef]
- Nandlal B, Anoop NK, Ragavee V, Vanessa L. In-vitro Evaluation of toothpaste containing enzymes and proteins on inhibiting plaque re-growth of the children with high caries experience. J Clin Exp Dent. 2021 Jan 1;13(1):e43-e47. PMID: 33425230; PMCID: PMC7781222. [CrossRef]
- Min K, Bosma ML, John G, McGuire JA, DelSasso A, Milleman J, Milleman KR. Quantitative analysis of the effects of brushing, flossing, and mouthrinsing on supragingival and subgingival plaque microbiota: 12-week clinical trial. BMC Oral Health. 2024 May 17;24(1):575. PMID: 38760758; PMCID: PMC11102210. [CrossRef]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. Syst. Rev. 2021, 10, 372.
- Sterne JAC, Savović J, Page MJ, Elbers RG, Blencowe NS, Boutron I, Cates CJ, Cheng HY, Corbett MS, Eldridge SM, Emberson JR, Hernán MA, Hopewell S, Hróbjartsson A, Junqueira DR, Jüni P, Kirkham JJ, Lasserson T, Li T, McAleenan A, Reeves BC, Shepperd S, Shrier I, Stewart LA, Tilling K, White IR, Whiting PF, Higgins JPT. RoB 2: a revised tool for assessing risk of bias in randomised trials. BMJ. 2019 Aug 28;366:l4898. PMID: 31462531. [CrossRef]
- Sterne JA, Hernán MA, Reeves BC, Savović J, Berkman ND, Viswanathan M, Henry D, Altman DG, Ansari MT, Boutron I, Carpenter JR, Chan AW, Churchill R, Deeks JJ, Hróbjartsson A, Kirkham J, Jüni P, Loke YK, Pigott TD, Ramsay CR, Regidor D, Rothstein HR, Sandhu L, Santaguida PL, Schünemann HJ, Shea B, Shrier I, Tugwell P, Turner L, Valentine JC, Waddington H, Waters E, Wells GA, Whiting PF, Higgins JP. ROBINS-I: a tool for assessing risk of bias in non-randomised studies of interventions. BMJ. 2016 Oct 12;355:i4919. PMID: 27733354; PMCID: PMC5062054. [CrossRef]
- Carelli M, Zatochna I, Sandri A, Burlacchini G, Rosa A, Baccini F, Signoretto C. Effect of A Fluoride Toothpaste Containing Enzymes and Salivary Proteins on Periodontal Pathogens in Subjects with Black Stain: A Pilot Study. Eur J Dent. 2024 Feb;18(1):109-116. Epub 2023 Mar 4. PMID: 36870327; PMCID: PMC10959611. [CrossRef]
- Daly S, Seong J, Newcombe R, Davies M, Nicholson J, Edwards M, West N. A randomised clinical trial to determine the effect of a toothpaste containing enzymes and proteins on gum health over 3 months. J Dent. 2019 Jan;80 Suppl 1:S26-S32. PMID: 30696552. [CrossRef]
- Pedersen AML, Darwish M, Nicholson J, Edwards MI, Gupta AK, Belstrøm D. Gingival health status in individuals using different types of toothpaste. J Dent. 2019 Jan;80 Suppl 1:S13-S18. PMID: 30696551. [CrossRef]
- Kilian M, Chapple IL, Hannig M, Marsh PD, Meuric V, Pedersen AM, Tonetti MS, Wade WG, Zaura E. The oral microbiome - an update for oral healthcare professionals. Br Dent J. 2016 Nov 18;221(10):657-666. PMID: 27857087. [CrossRef]
- Helmerhorst EJ, Oppenheim FG. Saliva: a dynamic proteome. J Dent Res. 2007 Aug;86(8):680-93. PMID: 17652194. [CrossRef]
- Magacz M, Kędziora K, Sapa J, Krzyściak W. The Significance of Lactoperoxidase System in Oral Health: Application and Efficacy in Oral Hygiene Products. Int J Mol Sci. 2019 Mar 21;20(6):1443. PMID: 30901933; PMCID: PMC6472183. [CrossRef]
- Haberska K, Svensson O, Shleev S, Lindh L, Arnebrant T, Ruzgas T. Activity of lactoperoxidase when adsorbed on protein layers. Talanta. 2008 Sep 15;76(5):1159-64. Epub 2008 May 21. PMID: 18761171. [CrossRef]
- Roger V., Tenovuo J, Lenander-Lumikari M, Söderling E, Vilja P. Lysozyme and lactoperoxidase inhibit the adherence of Streptococcus mutans NCTC 10449 (serotype c) to saliva-treated hydroxyapatite in vitro. Caries Research, 1994, 28.6: 421-428.
- Korpela A, Yu X, Loimaranta V, Lenander-Lumikari M, Vacca-Smith A, Wunder D, Bowen WH, Tenovuo J. Lactoperoxidase inhibits glucosyltransferases from Streptococcus mutans in vitro. Caries Res. 2002 Mar-Apr;36(2):116-21. PMID: 12037368. [CrossRef]
- Justiz Vaillant AA, Sabir S, Jan A. Physiology, Immune Response. 2024 Jul 27. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2024 Jan–. PMID: 30969623.
- Ramenzoni LL, Hofer D, Solderer A, Wiedemeier D, Attin T, Schmidlin PR. Origin of MMP-8 and Lactoferrin levels from gingival crevicular fluid, salivary glands and whole saliva. BMC Oral Health. 2021 Aug 5;21(1):385. PMID: 34353321; PMCID: PMC8340507. [CrossRef]
- Jalil RA, Ashley FP, Wilson RF, Wagaiyu EG. Concentrations of thiocyanate, hypothiocyanite, 'free' and 'total' lysozyme, lactoferrin and secretory IgA in resting and stimulated whole saliva of children aged 12-14 years and the relationship with plaque accumulation and gingivitis. J Periodontal Res. 1993 Mar;28(2):130-6. PMID: 8478785. [CrossRef]
- Paqué PN, Schmidlin PR, Wiedemeier DB, Wegehaupt FJ, Burrer PD, Körner P, Deari S, Sciotti MA, Attin T. Toothpastes with Enzymes Support Gum Health and Reduce Plaque Formation. Int J Environ Res Public Health. 2021 Jan 19;18(2):835. PMID: 33478112; PMCID: PMC7835853. [CrossRef]
- Petersen PE, Bourgeois D, Ogawa H, Estupinan-Day S, Ndiaye C. The global burden of oral diseases and risks to oral health. Bull World Health Organ. 2005 Sep;83(9):661-9. Epub 2005 Sep 30. PMID: 16211157; PMCID: PMC2626328.
- Belstrøm D, Holmstrup P, Nielsen CH, Kirkby N, Twetman S, Heitmann BL, Klepac-Ceraj V, Paster BJ, Fiehn NE. Bacterial profiles of saliva in relation to diet, lifestyle factors, and socioeconomic status. J Oral Microbiol. 2014 Apr 1;6. PMID: 24765243; PMCID: PMC3974179. [CrossRef]
- Green A, Crichard S, Ling-Mountford N, Milward M, Hubber N, Platten S, Gupta AK, Chapple ILC. A randomised clinical study comparing the effect of Steareth 30 and SLS containing toothpastes on oral epithelial integrity (desquamation). J Dent. 2019 Jan;80 Suppl 1:S33-S39. PMID: 30696554. [CrossRef]
Figure 1.
PRISMA flowchart.
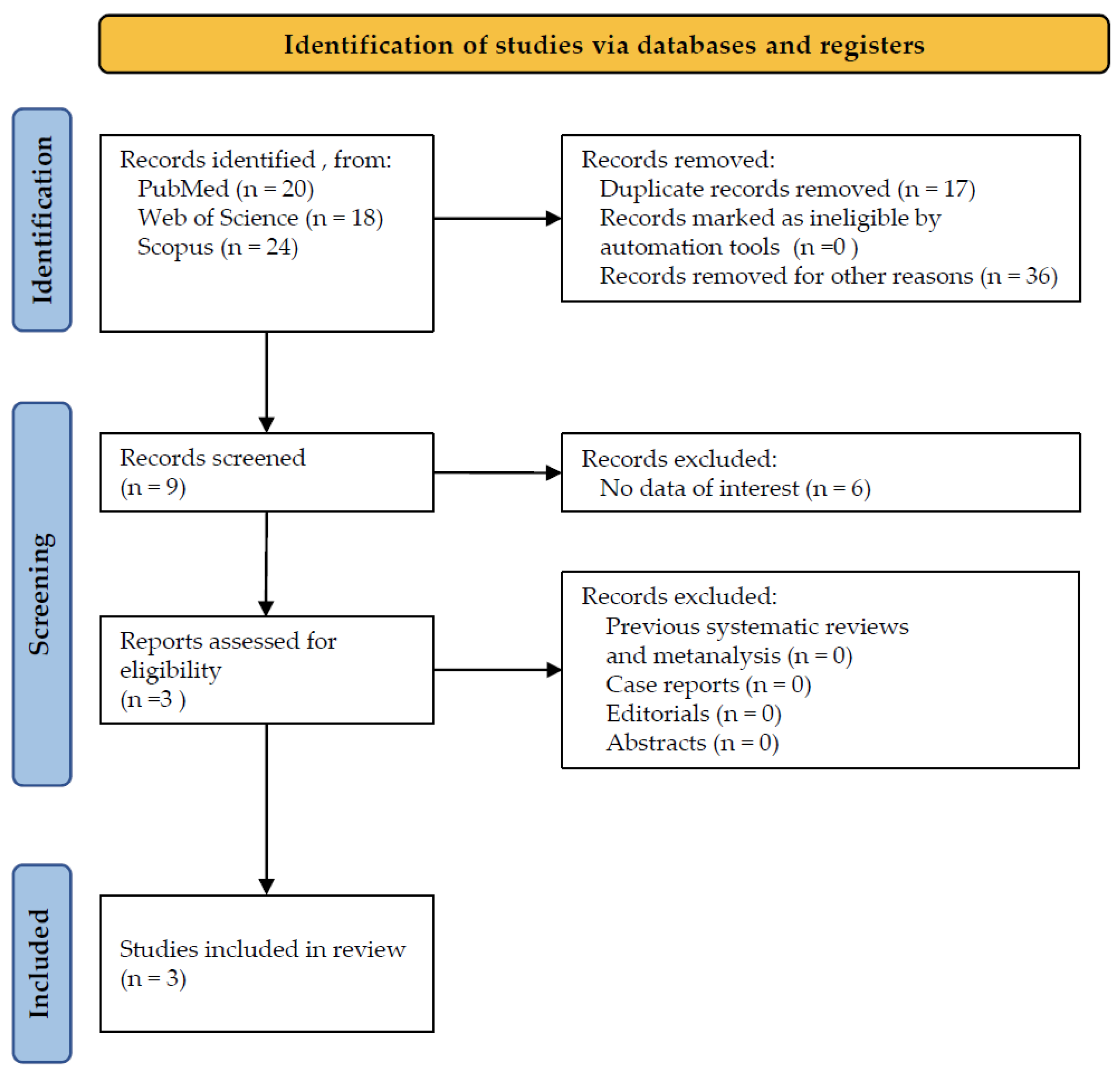
Figure 2.
Risk of bias of the RCTs included in the systematic review.
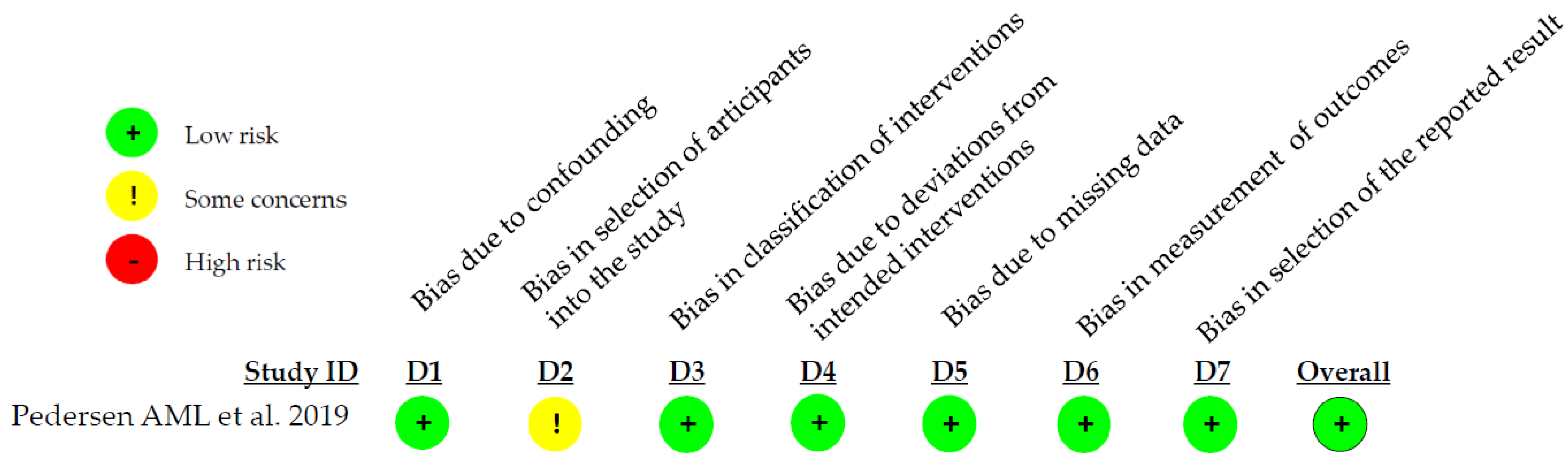
Figure 3.
Overall risk of bias, with each category presented as percentages.
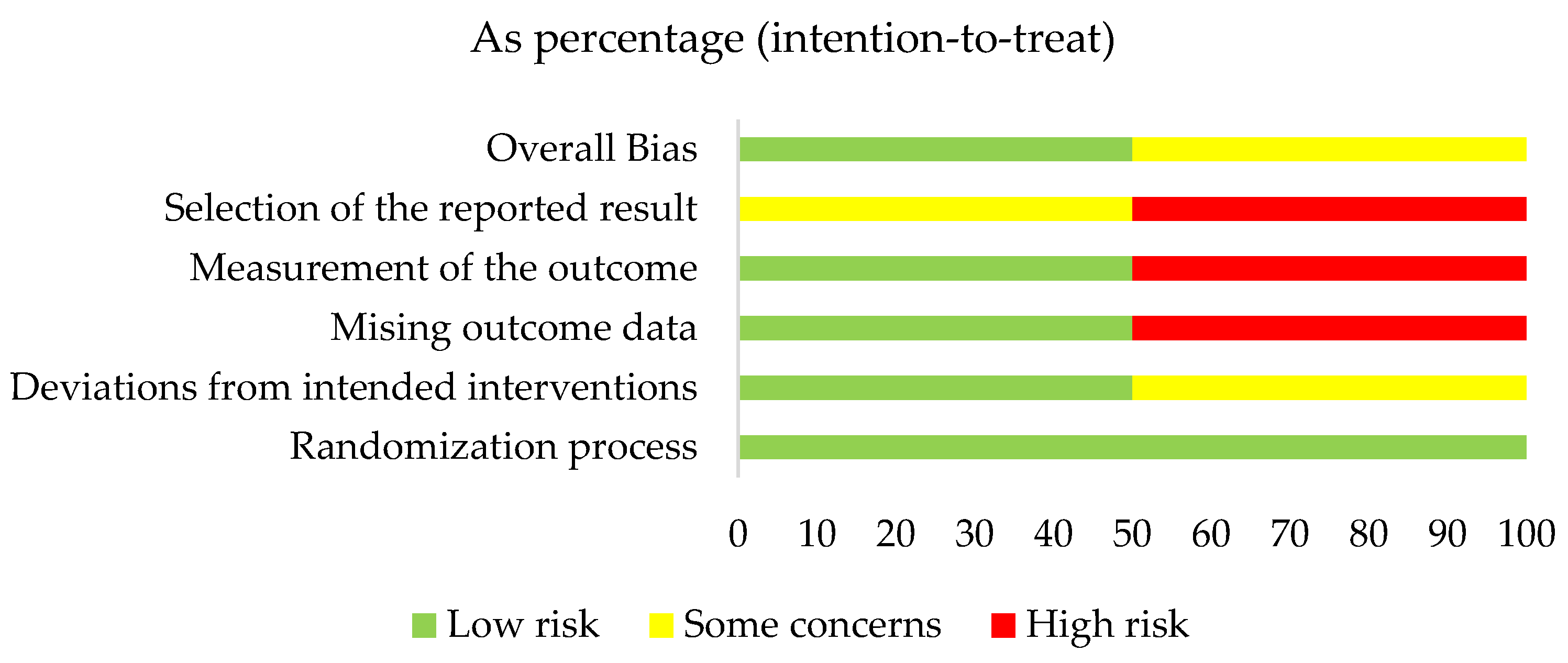
Figure 4.
Risk of bias of the N-RCT included in the systematic review.
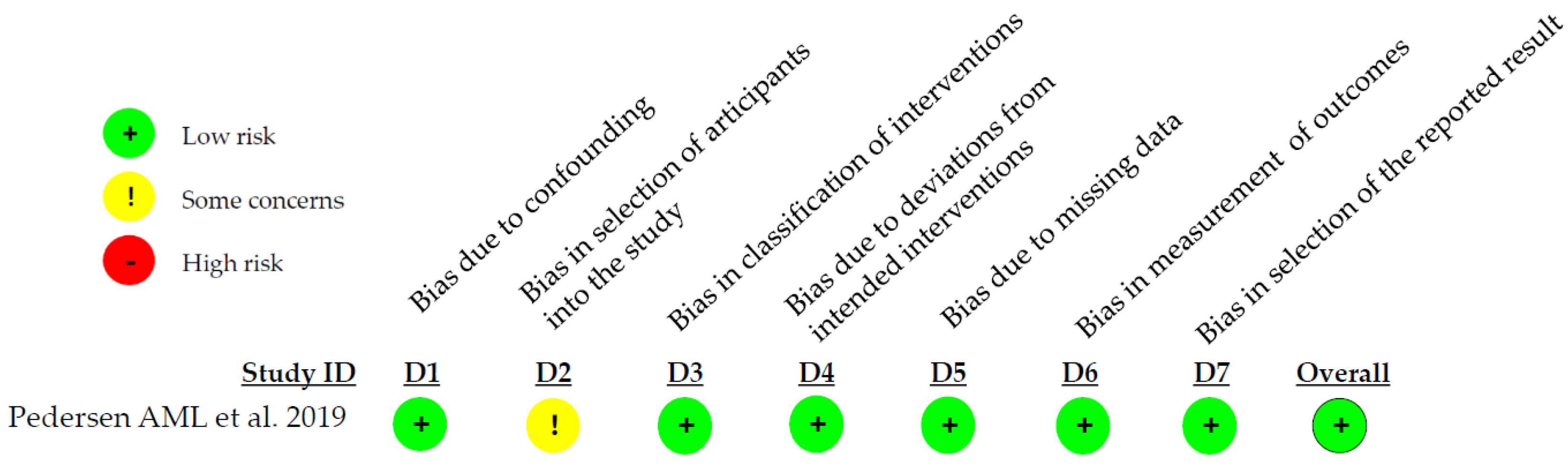

Table 1.
Main results. RCT, Randomized Controlled Trial. N-RCT, Non-Randomized Clinical Trial. DMFT, Decayed Missing Filled Teeth. GBI, Gingival Bleeding Index. MGI, Modified Gingival Index. BI, Bleeding Index. PI, Plaque Index. Age is expressed by mean value or range.
Table 1.
Main results. RCT, Randomized Controlled Trial. N-RCT, Non-Randomized Clinical Trial. DMFT, Decayed Missing Filled Teeth. GBI, Gingival Bleeding Index. MGI, Modified Gingival Index. BI, Bleeding Index. PI, Plaque Index. Age is expressed by mean value or range.
| Authors/Year | Study design |
Population /age |
Aim of administration | Follow-up | Systemic conditions |
|---|---|---|---|---|---|
| Carelli M. et al. 2024 [16] | RCT | 26/22,5 | Effects on DMFT, gingival indexes (GBI, Plaque control) and black stains | 14 weeks | Healthy |
| Daly S. et al. 2019 [17] | RCT | 229/32,6 | Effects on gingival indexes (MGI, BI, PI modified by Quigley and Hein) | 12 weeks | Healthy |
| Pedersen AML. et al. 2019 [18] | N-RCT | 305/18->56 | Effects on gingival indexes (MGI, BI, PI modified by Quigley and Hein) | 12 months | Healthy |
Table 2.
Summary of the included studies.
| Authors/Year | Conclusions |
|---|---|
| Carelli M. et al. 2024 [16] | Brushing with an electric toothbrush seemed to be more effective at reducing black stains compared to manual brush. This improvement was seen regardless of the toothpaste used. |
| Daly S. et al. 2019 [17] | Brushing with the enzyme and protein toothpaste resulted in lower plaque and bleeding indexes. |
| Pedersen AML. et al. 2019 [18] | Using a fluoride toothpaste containing enzymes and proteins for at least 1 year is associated with improved gum health compared to other fluoride toothpastes lacking these additional ingredients. |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



