Submitted:
20 September 2024
Posted:
24 September 2024
You are already at the latest version
Abstract
Sputum induction (SI) is a non-invasive technique to obtain lower airway samples from people who do not spontaneously produce sputum. Since its introduction in 1958, its use has significantly increased for various respiratory conditions, especially with the establishment of standardized techniques. It has been used in pediatric research since 2002, starting with asthma studies. It is a safe and repeatable procedure for non-expectorating children. The ability to analyze both cellular and fluid components of sputum provides valuable information about lung diseases. This work reviews the utility of sputum induction in pediatric respiratory research and its potential clinical applications. We also discuss the safety, tolerability, and side effects profile of the procedure, emphasizing its significance in pediatric respiratory research. Despite the valuable insights gained from SI studies, challenges remain for widespread clinical utilization, requiring further refinement of the technique and increased accessibility in clinical settings.
Keywords:
Induced sputum
; airway inflammation
; respiratory
; children
Introduction
Sputum induction (SI) is a technique used to obtain lower airway samples for clinical or research purposes. SI was initially used for diagnosing lung cancer, Pneumocystis carinii pneumonia (PCP) in HIV patients [1,2] and evolved into a prominent tool for studying airway inflammation in asthma [3]. Later, the ability to analyze both cellular and fluid components of sputum yielded deeper insights into airway inflammatory profiles by identifying types of inflammatory cells and markers [4,5,6]. The establishment of standardized techniques has further enhanced the quality and reproducibility of SI samples [7,8,9]. Consequently, SI has emerged as a valuable method for assessing airway inflammation in various respiratory diseases, including infectious diseases, asthma, COPD, and interstitial lung disease [10].
In the realm of pediatric studies, SI is a non-invasive, repeatable, and safe technique for sampling the airways, especially in non-expectorating children. In the past, collecting sputum for diagnosis of respiratory infections was not commonly practiced in children. However, the true potential of SI has emerged with its application in studying asthma in children following successful attempts to examine the inflammatory response in asthma [7,11]. Its use has significantly increased with various respiratory conditions since the alignment between SI and spontaneously expectorated samples in characterizing airway infection and inflammation is well-established [12]. Moreover, SI samples have been recognized as a practical substitute for bronchoalveolar lavage (BAL) for acquiring culture samples from children with cystic fibrosis due to the enhanced yield and quality of sputum samples [13]. SI samples were also used in comparison with bronchoalveolar lavage results for diagnosing pulmonary tuberculosis [14]Taken together, SI provides a distinctive opportunity as a method to assess airway inflammation in the field of pediatric respiratory medicine, particularly in children who do not spontaneously produce sputum.
We aimed to review the utility of SI samples in research and its potential clinical applications, along with safety, tolerability, and side effects profile of the procedure and highlight its significance in pediatric respiratory medicine. This article summarizes studies demonstrating strong evidence for research value of sputum induction (SI) in evaluating various respiratory diseases in children. Although many of these studies focused on asthma, cystic fibrosis, and pulmonary tuberculosis; there is also evidence to support the use of SI in a diverse range of respiratory diseases in children. The insights gained from these endeavors not only redefine our diagnostic capabilities but also underscore the potential of personalized respiratory care in children, marking a new era by evaluating diseases non-invasively.
Safety of Sputum Induction in Children
While safety concerns may arise when considering SI for airway sampling in children, it is considered a safe procedure based on previous studies with children, especially when conducted by trained professionals [15]. The administration of this procedure entails implementing measures to minimize potential side effects. For instance, the procedure should be performed by healthcare professionals who are experienced in the technique and managing any potential effects. Another such measure includes pretreatment with beta2-agonist medications to further improve success and tolerability for children [7]. This commitment to the safety of SI is reflected in large-scale studies. Across 22 studies exploring SI for various conditions including asthma, tuberculosis, HIV, pneumonia, and cystic fibrosis, no serious adverse events were reported in over 1,800 children [16]. This large-scale evidence highlights the procedural safety of SI. Furthermore, a study involving 250 children aged 6-24 months with pulmonary tuberculosis reported the safety of SI in this age group, even during acute illness [17].
Although there may be initial concerns, comprehensive evidence strongly supports its safety in children. Conducted by trained professionals with proper precautions, it offers a valuable tool to get information about lung diseases in children.
Tolerance of Sputum Induction in Children
Evaluating tolerance in children undergoing SI necessitates a variety of flexible methods due to their age and developmental level. Therefore, subjective or objective assessments of the tolerability of the procedure have been implemented in studies with children. In subjective assessments, measures were assessed by both parents and healthcare professionals, utilizing tools like the Wong-Baker Faces Pain Rating Scale, Likert scales, or the Alert, Voice, Pain, Unresponsive [AVPU] scale [18,19,20]These scales allow for a nuanced understanding of the child's experience during the procedure. Studies indicated high subjective tolerance, such as in a study over 90% of procedures deemed "very easy" or "easy" by healthcare professionals [21].
Objective assessments, focusing on physiological parameters like respiratory rate, heart rate, oxygen saturation, and FEV1, offer additional insights. A study by Ronchetti et al. involving children with cystic fibrosis aged 6 months to 18 years demonstrated no significant changes in these parameters during the procedure, supporting its good tolerance, objectively [19]. Further, high tolerance for the procedure was also reported based on both parent and physiotherapist scores on the Likert Scale in the same study [19].
Both subjective and objective assessments revealed high tolerability, only 5% of patients in studies found the procedure overly uncomfortable and patients did not complete the procedure due to discomfort, demonstrating its high tolerability in pediatric populations [16].
Side Effects of Sputum Induction in Children
While sputum induction is a valuable tool in research and clinical practice of respiratory diseases in children, it is important to be aware of potential side effects. During SI, various temporary and manageable side effects might occur including a salty taste in the mouth, unpleasant experiences leading to discontinuation, vomiting, dizziness, anxiety, cough, dyspnea, wheezing, bronchospasm, or decline in FEV1. The most frequently reported side effects are cough and wheezing [11,21,22,23,24]. In addition, vomiting and epistaxis are commonly reported side effects in studies facilitating nasopharyngeal/oropharyngeal suctioning (Table 1).
The primary potential serious complication of SI is bronchospasm in patients with underlying asthma or reactive airway disease. While a decline in lung function (FEV1) may occur, it typically resolves quickly [12]. Previous studies have compared the side effects of SI with and without pretreatment with β2-agonist. These studies reported that only a small proportion of children experienced a fall in lung function of 10% or more from baseline without pretreatment [22,25] However, the implementation of pretreatment with β2-agonists has significantly improved the success rate and tolerability of the procedure in children. As a result, it has become an element of the SI protocol [7].
In summary, the vast majority of children experience minimal or no side effects from sputum induction. Although a small proportion of patients may not complete the procedure due to side effects, pretreatment with bronchodilators significantly reduces respiratory concerns, such as a decline in FEV1, in asthmatic children.
Utilization of Sputum Induction in Children with Respiratory Diseases
SI samples can provide information about both cellular and molecular mechanisms, making it a valuable tool particularly in respiratory disease research. It can also be utilized in clinical practice such as microbiological yield. It is helpful to obtain airway sampling in children who do not provide spontaneous sputum with a success rate differing based on the child's age group (Figure 1).
Sputum samples can be utilized for biomarkers of inflammation, infection, and airway remodeling, providing insights into the disease activity, summarized in Table 1.
We summarized utility of sputum induction below in a variety of respiratory diseases in children:
- 1.
- Asthma
Asthma is the most common chronic disease in children globally and one of the main causes of hospitalization in children aged < 5 years. Notably, the prevalence of asthma has exhibited a significant increase over the past two decades [26]. In the realm of pediatric asthma research, SI has been utilized in children since the first description of the technique in adult asthma patients [3]. Thereafter, there has been an increasing interest in the utilization of SI and its implications in research and clinical practice. Initial studies explored inflammatory markers in SI samples, like sputum cell counts, including eosinophils and neutrophils, and eosinophil cationic protein (ECP) levels to understand their correlation with asthma phenotypes and severity[11,22,27]. One such study by Drews et al [28] reported that nonatopic children exhibited a predominantly neutrophilic cell pattern. In contrast, eosinophilia emerged as a hallmark of airway inflammation in the majority of atopic children not treated with inhaled steroids, aligning with confirmed asthma phenotypes based on the ISAAC questionnaire[22]. Building on previous research, further studies evaluated an extended panel of inflammation markers in induced sputum to further refine the identification of phenotypes in asthmatic children [29].
In pediatric asthma management, there is a substantial body of research literature exploring the use of SI to find an effective management strategy, since it offers a non-invasive, safe, and repeatable method for measuring airway inflammation. Sputum cell counts facilitated to the prediction of therapeutic responses, particularly eosinophil counts. SI samples have emerged as a valuable metric for monitoring asthma exacerbations and determining the efficacy of asthma control therapy in children with asthma [30] Sputum eosinophil counts were correlated with frequency of exacerbations, as well as hospitalization rates in pediatric asthma [31]. In parallel, further studies have delved into whether a management strategy could be established using SI samples to reduce asthma exacerbations [32,33] In subgroup analyses, researchers compared asthma control strategies including sputum eosinophil count versus clinical symptom control. Although statistical significance was not achieved due to limited statistical power, they reported correlation with sputum eosinophil counts and reduction in the number of participants experienced asthma exacerbations, decreased number of exacerbations and hospitalization rates [33,34]. Further, a Cochrane Database systematic review conducted by Petsky et al. highlighted the inadequacy of available data for tailoring asthma medications based on sputum eosinophilia in children [34].
Further exploration has been made using SI samples which included expression of vascular endothelial growth factor (VEGF), monitoring particulate matter accumulation in the lungs, flow cytometric analysis and regulatory T cells and cytokines in asthmatic children [35,36,37,38]. Notably, sputum VEGF expression significantly exceeded levels during quiescence, and both were higher than the corresponding levels of the control group during asthma exacerbation [35]. Further, innate lymphoid cells (ILC2) were significantly higher in the airways of children with severe asthma suggesting they could be a potential therapeutic target [37].
In the pursuit of refining SI techniques, recent publications have compared different methodologies, particularly in adolescents. A study evaluating physiotherapy techniques (oscillatory positive expiratory pressure, forced expiration, and acceleration of expiratory flow) for sputum induction in well-controlled asthmatic children and adolescents found no significant differences in inflammation outcomes [39]. These efforts mark a continuous stride toward optimizing SI practices in the field of pediatric asthma research. In addition, the cost-effectiveness of SI in asthma management is supported by economic analyses, demonstrating healthcare-related savings that outweigh the costs associated with sputum induction and processing [13,40].
In summary, SI has emerged as a valuable tool in pediatric asthma research. It allows direct assessment of airway inflammation non-invasively, aiding in phenotype identification, monitoring disease activity, and optimizing treatment plans, particularly in patients with severe or difficult-to-treat asthma. Its clinical application is limited due to standardization in techniques, logistical and technical considerations. But it still has the potential to pave the way for personalized treatment approaches and potentially reduce healthcare costs. Well-designed randomized controlled trials (RCTs) are needed to definitively establish the use of SI in guiding treatment decisions across diverse asthma severities and endotypes. Additionally, rapid advancements in sample analysis hold promise for even more personalized and effective asthma management in children.
- 2.
- Cystic Fibrosis
Cystic fibrosis (CF) is a life-shortening, multisystem disease, that prominently affects the lungs leading to progressive obstructive lung disease characterized by chronic infections and inflammation, impaired host defense, and tissue damage [41] [42,43]. Effective sampling of the lower airways is essential to characterize infection and inflammation in the management of respiratory health in CF. Sputum samples provide accurate information about infection and inflammation, but young children with CF, particularly < 6 years do not expectorate sputum spontaneously. In the era of CFTR modulator therapy, this has also presented a challenge in older children. Therefore, effective sampling of the lower airway can still be problematic in pediatric patients with CF.
Oropharyngeal cough swab or throat swab is a simple, and well-tolerated technique for bacterial surveillance of the CF lung in non-expectorating children. However, a study reported a sensitivity of 44% for concurrent bronchoalveolar lavage (BAL) cultures, suggesting their limited representation of the lower airways [44]. Therefore, there has been an increasing interest in sputum induction, as a safe and cost-effective technique for sampling the lower airway in children who are unable to expectorate spontaneously [45]. The three largest studies comparing cough swabs with induced sputum in children identified additional organisms on induced sputum in 31-42% of cases [46,47,48,49]
Although fiberoptic bronchoscopy with BAL is considered as the gold standard for lower airway sampling, it is a costly and invasive technique that requires anesthesia. BAL-based microbiology surveillance programs are of interest internationally, but little evidence strongly supports their routine use in CF care [16]. As an alternative, SI sampling holds promise for obtaining lower airway samples in non-productive children with CF. However, studies comparing paired BAL samples reported inconclusive results from providing similar microbiologic yield to BAL to being not highly sensitive or specific as routine surveillance for detection of lower airway pathogens in young children with cystic fibrosis [50,51]. Further, lower airway microbiota has been studied with a conclusion of SI capturing a microbiota signature representative of the lower airway in 80% of cases when compared to paired BAL samples [52], polymicrobial infection and gram negative organisms were detected more frequently in SI samples when compared to paired oropharyngeal swabs [53]. Furthermore, the CF-Sputum Induction Trial (CF-SpIT) study compared approaches to lower airway sampling in children with CF, aged 6 months to 18 years using concurrent samples from cough swabs, sputum-induction, and single-lobe, two-lobe, and six-lobe bronchoalveolar lavage [19]. The proportion of pathogens isolated by sputum induction and two-lobe bronchoalveolar lavage was reported as largely equivalent. In addition, a 5-year prospective observational cohort study involving children with CF aged 5-17 years concluded that induced sputum is useful for early detection of Non-tuberculous mycobacteria (NTM) previously never isolated, particularly in non-expectorating children [54].
In CF, SI samples were also used to assess airway inflammation, as well as to monitor disease activity by analyzing inflammation markers and measurement of cytokine concentrations in sputum [12,55,56,57]. Further, an adult study utilized SI samples to define the sputum immune profile of CF patients using single-cell RNA sequencing (scRNAseq) and significant differences in the sputum immune cell repertoire were demonstrated between patients with CF and healthy adults [58]. Subsequently, a successful implementation of this innovative approach was reported in the pediatric CF population to investigate the host defense and uncover the drivers behind hyperinflammatory state in CF lungs[59]. In addition, SI samples were employed for determining airway drug concentrations[60] and as non-invasive outcome measures to evaluate treatment response, such as following intravenous antibiotic therapy [61].
Given that progressive lung disease begins at younger ages, lower airway sampling plays a crucial role in managing CF lung disease. Sputum induction (SI) emerges as a promising tool to obtain lower airway samples in non-expectorating children with CF for research or clinical purposes. In the era of CFTR modulator therapy, despite recent advancements in clinical care, a knowledge gap still exists in understanding the driving mechanisms of the hyperinflammatory state and innate immune defects in CF. In addition, the mechanisms of action that underlie the impact of CFTR modulators on the immune response have not been elucidated yet. A better understanding of the inflammatory response and the initial host-defense defects in the airways of patients with CF could identify new therapeutic targets supported by advances in laboratory techniques and cutting-edge technologies, including finding effective therapies for patients with CF who are not eligible for CFTR modulators. SI still holds promise for gaining deeper insight into the pathogenesis of CF lung disease by utilizing samples from the site of inflammation.
- 3.
- Pneumonia
Pneumonia is a major health concern, causing significant morbidity and mortality in children, particularly in resource-limited countries [62] Accurate diagnosis of the causative agent is crucial for proper treatment and preventing further complications. Despite advancements in rapid diagnostic tests for viruses and atypical bacteria, detecting bacterial causes in children with pneumonia remains challenging. Sputum microscopy and culture, commonly used in adults, are rarely used in children due to difficulties in obtaining specimens [63,64]. Also, they are only recommended in hospitalized children due to their low diagnostic yield. While isolating pathogens from blood, pleural effusion, or bronchial lavage fluid can be used to determine causative pathogens, these methods have limitations. Blood cultures rarely yield bacteria (less than 10%) and obtaining pleural effusion or bronchial lavage fluid requires invasive procedures, making them impractical for routine use [64,65].
The utility of SI as a tool for identifying the cause of childhood community-acquired pneumonia (CAP) is controversial. While some studies have shown promise, other studies have presented conflicting findings[20,63,66,67,68,69]. Several factors can explain these discrepancies: the risk of contamination from the upper respiratory tract, lower diagnostic utility in parenchymal diseases compared to airway diseases, the possibility of polymicrobial infection, incidental carriage of potentially pathogenic microorganisms due to physiological differences in the airways of young children, and the lack of a fully developed immune system in young patients.
A study with 101 children with CAP reported a high microbiological yield of (90%) SI samples, suggesting its potential as a diagnostic method [66]. Another study found SI to be safe and feasible in young children, with a good yield (70.3%) of bacteria from high-quality sputum samples [67]. Similarly, a recent study by Ogawa et al [68] suggests that bacteria isolated from good-quality sputum are more likely to be the true cause of CAP in children. Overall, previous research shows an average success rate of 62% to 79% in isolating pathogens, 15–25% being bacterial etiology from sputum specimens using SI [65,67]. However, some studies present contrasting results. The Pneumonia Etiology Research for Child Health (PERCH) study, a large-scale investigation across seven countries, highlighted safety, utility, and quality assessment of SI in resource-limited settings for children aged 1-59 months[20,63,69]. The study found significant variations in obtaining good quality sputum samples. Analyzing PERCH data, Murdoch et al [63] concluded that routine SI cultures are unreliable for diagnosing pneumonia in young children. Additionally, their comparison of paired SI and nasopharyngeal/oropharyngeal (NP/OP) swab samples from hospitalized children with severe pneumonia showed minimal additional diagnostic value from SI using PCR, compared to just NP/OP swabs [69]. Another study suggested that SI cultures rarely match cultures from sterile body sites, indicating isolated pathogens might reflect throat/mouth bacteria rather than the true cause of pneumonia [64]. In addition, despite showing high rates of bacteria isolation in sputum specimens, SI results may not always reflect the cause of pneumonia. Studies reported a lack of consistent correlation between positive SI cultures and chest X-rays, other diagnostic tests, disease progression, or treatment decisions [67]. Additionally, the presence of both viruses and bacteria in 66% of sputum samples highlights the challenges [70]. This could be due to co-infections, bacteria from the throat/mouth contaminating the sample, or colonization of the upper respiratory tract.
Identifying the cause of childhood pneumonia is challenging. Notably, most studies investigating SI involved severe cases or hospitalized children. The lack of a gold standard for diagnosing pneumonia etiology in children further complicates the issue. While PCR testing is more sensitive to viruses than cultures, it cannot definitively rule out a bacterial infection, especially in severe cases. The possibility of concomitant bacterial-viral infection further complicates and adds more challenges. SI shows some promise, but limitations exist. While new potent techniques such as clinical metagenome next-generation sequencing (mNGS) are on the horizon, future research is needed to validate and develop new and reliable diagnostic tests for accurate pathogen identification in children with pneumonia.
- 4.
- Opportunistic Infections in Immunocompromised Children
Induced sputum samples were also utilized in immunocompromised children with pneumonia. Studies show SI effectively detects Pneumocystis jirovecii (PCP) in such reaching high sensitivity with PCR testing [71,72]. A study involving HIV-positive children with pneumonia showed SI to be as effective as gastric lavage (GA) for diagnosing Mycobacterium tuberculosis and superior to nasopharyngeal aspirate (NPA) for identifying PCP [73].
- 5.
- Pulmonary tuberculosis
Pulmonary tuberculosis (TB) remains a major global health issue and still carries diagnostic challenges, particularly in children [74] While the World Health Organization (WHO) recommends sputum smear analysis for acid-fast bacilli (AFB) and culture in pulmonary TB diagnosis, this method often fails in children due to difficulty in producing sputum samples and lower bacterial presence (paucibacillary disease). This results in inadequate diagnosis and hinders effective treatment. For young children, gastric aspirate (GA) is the primary method for obtaining samples for culture. However, it is invasive and unpleasant, requires hospitalization and other methods like bronchoscopy are even more so, with limited accessibility in TB-endemic areas and concern of transmission.
Several studies were conducted to compare methods for the diagnosis of TB In children who are unable to expectorate sputum including SI, GA, nasopharyngeal aspiration (NPA), BAL or pleural/lymph node biopsy (PLNB). Sputum induction has been identified as an effective technique for isolating Mycobacterium tuberculosis in infants and children, and repeated SI may be just as useful as multiple gastric lavage samples [17,21,75,76]. Studies also suggest that a single SI sample can yield similar results to three gastric lavages [77]. Combining sputum induction with gastric aspiration might further improve Mycobacterium tuberculosis detection in hospitalized young children with acute severe pneumonia [78]. Further, a comprehensive review reported SI detects more TB cases than GA or NPA when the likelihood of TB (presumptive TB score) is low to moderate [79]. However, a meta-analysis revealed considerable inconsistency among studies comparing these techniques indicating difficulty in arriving at a definitive conclusion regarding the effectiveness of SI for diagnosing TB in children. Although the average TB detection rate appears to be 79%, this value may not be reliable due to the significant variation between studies [80].
While BAL sampling can be a preferred method for adults who do not produce sputum or have negative sputum smear analysis, its yield in diagnosing pulmonary TB in children is only 10%–22% [81]. On the other hand, sputum collected from children through nasopharyngeal aspiration or sputum induction has been reported to have a diagnostic yield of 20%–30% [77]. Adult studies comparing sputum induction (SI) and BAL samples in pulmonary TB diagnosis have shown that SI has an equal or greater diagnostic yield than BAL, with fewer risks and lower costs [81]. Moreover, one pediatric study, albeit with a small sample size, reported that SI samples were superior in detecting TB compared to bronchial brushing based on AFB smear, mycobacterial culture, and real-time PCR analyses [82]. A recent meta-analysis also reported that SI has similar accuracy to bronchoscopy-obtained samples in diagnosing sputum smear-negative pulmonary TB [83].
In the fight against pediatric TB, early diagnosis is the most effective control strategy. However, limitations in existing diagnostic tests call for new, accessible diagnostic tools, especially for children in diverse populations globally. This urgency is further amplified by the rising threat of drug-resistant TB in low- and middle-income countries, which requires accurate microbiological confirmation for tailoring appropriate treatment. This need has prompted the WHO to prioritize the development of a rapid, non-sputum-based diagnostic solution for childhood TB. As a result, promising new techniques are emerging, such as the Mycobacterium tuberculosis Host Response prototype cartridge (Cepheid MTB-HR), a finger-stick blood analysis based on mRNA transcriptomic signatures [84]. However, its reported sensitivity of 29.6% requires further studies. While it is recommended that clinical expertise, provider skills, patient age and developmental level should guide the choice of diagnostic method, SI can still be considered, particularly in resource-limited settings as a cost-effective, faster tool [81]. Despite the promise of recent advancements that can also improve the diagnostic yield of SI samples, further investigations are necessary to optimize cost, accessibility, and delivery location, particularly in tuberculosis-endemic countries. The fight against childhood TB requires ongoing efforts to improve diagnostic tools.
- 6.
- Other respiratory diseases
Several other studies have been performed on the potential of sputum analysis in understanding various respiratory conditions in children.
A study focused on children with obstructive sleep apnea (OSA) revealed a significant increase in the percentage of sputum neutrophils in these children and a significant positive correlation with the degree of neutrophilic airway inflammation and the severity of OSA [85]. This underscores the potential of SI samples in elucidating the inflammatory processes associated with OSA in children, indicating a promising avenue for future investigations.
Another study included preschool children with chronic airway diseases highlighted the advantages of sputum induction over cough swabs [18]. It demonstrated that SI is safe, feasible, and non-invasive, with successful sample collection in 95% of cases to assess both bacterial and viral infection.
However, not all studies have found SI to be equally informative. For instance, a study by Ervine et al in 2009, which focused on children with gastroesophageal reflux (GER), concluded that SI may induce physiological GER in healthy children. Consequently, the analysis of pepsin in sputum obtained through induction was deemed not useful in investigating reflux-related respiratory disease [86].
In the context of bronchiolitis obliterans (BO), Rosewich and colleagues conducted the first study evaluating sputum samples in affected children. Their research revealed a neutrophilic inflammation with elevated levels of proinflammatory cytokines compared to healthy controls. Additionally, significant correlations were observed between sputum biomarker levels and the presence of small airway disease in children with BO [87].
Lastly, amidst the COVID-19 pandemic, a review article highlighted using SI for the evaluation of selected patients. Due to the generation of aerosols and cough maneuvers involved in the process, a multidisciplinary consensus on sputum induction biosafety was issued to ensure the safety of healthcare workers and patients alike [88].
Conclusion & Future Directions
Sputum induction (SI) offers a safe and non-invasive way to examine the lower airways in children with lung diseases. This technique can yield valuable insights into airway inflammation and infectious processes in research settings. Additionally, SI samples can be utilized with a variety of conventional and new techniques including but not limited to DNA extraction on the microbiome, enzyme-linked immunosorbent assay (ELISA), flow cytometry, mass cytometry, fluorescence in situ hybridization (FISH), and single-cell sequencing to investigate underlying mechanisms of different respiratory diseases, which ultimately could lead to the development of novel treatment strategies and improved disease management. Future avenues for utilizing SI in pulmonary medicine may focus on diseases such as Children's Interstitial and Diffuse Lung Disease (cHILD) and the pulmonary involvement of systemic conditions, such as connective tissue diseases and inflammatory bowel syndromes. In addition, SI can be a powerful tool for characterizing the lower airway microbiota in conjunction with state-of-the-art sequencing techniques.
However, challenges remain for widespread clinical utilization of sputum induction. Although it stands out for its cost-effectiveness, accessibility, and repeatability as a research tool, the procedure demands well-trained personnel and can be time-consuming. Further effort is needed to refine the technique for its accessibility in clinical settings, bridging the gap between research and everyday patient care.
Author Contributions
TKK and CJB conceptualized the study. TKK performed literature review and wrote the manuscript. All authors edited, revised and approved the final manuscript.
References
- Pitchenik, A.E.; Ganjei, P.; Torres, A.; Evans, D.A.; Rubin, E.; Baier, H. Sputum examination for the diagnosis of Pneumocystis carinii pneumonia in the acquired immunodeficiency syndrome. Am Rev Respir Dis 1986, 133, 226–229. [Google Scholar] [CrossRef] [PubMed]
- Bickerman, H.A.; Sproul, E.E.; Barach, A.L. An aerosol method of producing bronchial secretions in human subjects: a clinical technic for the detection of lung cancer. Dis Chest 1958, 33, 347–362. [Google Scholar] [CrossRef] [PubMed]
- Pin, I.; Gibson, P.G.; Kolendowicz, R.; Girgis-Gabardo, A.; Denburg, J.A.; Hargreave, F.E.; Dolovich, J. Use of induced sputum cell counts to investigate airway inflammation in asthma. Thorax 1992, 47, 25–29. [Google Scholar] [CrossRef]
- Pavord, I.D.; Pizzichini, M.M.; Pizzichini, E.; Hargreave, F.E. The use of induced sputum to investigate airway inflammation. Thorax 1997, 52, 498–501. [Google Scholar] [CrossRef]
- Spanevello, A.; Migliori, G.B.; Sharara, A.; Ballardini, L.; Bridge, P.; Pisati, P.; Neri, M.; Ind, P.W. Induced sputum to assess airway inflammation: a study of reproducibility. Clin Exp Allergy 1997, 27, 1138–1144. [Google Scholar] [CrossRef]
- Gibson, P.G.; Henry, R.L.; Thomas, P. Noninvasive assessment of airway inflammation in children: induced sputum, exhaled nitric oxide, and breath condensate. Eur Respir J 2000, 16, 1008–1015. [Google Scholar] [PubMed]
- Gibson, P.G.; Grootendor, D.C.; Henry, R.L.; Pin, I.; Rytila, P.H.; Wark, P.; Wilson, N.; Djukanovic, R. Sputum induction in children. Eur Respir J Suppl 2002, 37, 44s–46s. [Google Scholar] [CrossRef]
- Paggiaro, P.L.; Chanez, P.; Holz, O.; Ind, P.W.; Djukanovic, R.; Maestrelli, P.; Sterk, P.J. Sputum induction. Eur Respir J Suppl 2002, 37, 3s–8s. [Google Scholar] [CrossRef] [PubMed]
- Djukanovic, R.; Sterk, P.J.; Fahy, J.V.; Hargreave, F.E. Standardised methodology of sputum induction and processing. Eur Respir J Suppl 2002, 37, 1s–2s. [Google Scholar] [CrossRef]
- Fireman, E. Induced sputum as a diagnostic tactic in pulmonary diseases. Isr Med Assoc J 2003, 5, 524–527. [Google Scholar]
- Wilson, N.M.; Bridge, P.; Spanevello, A.; Silverman, M. Induced sputum in children: feasibility, repeatability, and relation of findings to asthma severity. Thorax 2000, 55, 768–774. [Google Scholar] [CrossRef] [PubMed]
- Sagel, S.D.; Kapsner, R.; Osberg, I.; Sontag, M.K.; Accurso, F.J. Airway inflammation in children with cystic fibrosis and healthy children assessed by sputum induction. Am J Respir Crit Care Med 2001, 164, 1425–1431. [Google Scholar] [CrossRef] [PubMed]
- Brightling, C.E. Clinical applications of induced sputum. Chest 2006, 129, 1344–1348. [Google Scholar] [CrossRef] [PubMed]
- Conde, M.B.; Soares, S.L.; Mello, F.C.; Rezende, V.M.; Almeida, L.L.; Reingold, A.L.; Daley, C.L.; Kritski, A.L. Comparison of sputum induction with fiberoptic bronchoscopy in the diagnosis of tuberculosis: experience at an acquired immune deficiency syndrome reference center in Rio de Janeiro, Brazil. Am J Respir Crit Care Med 2000, 162, 2238–2240. [Google Scholar] [CrossRef] [PubMed]
- Suri, R.; Marshall, L.J.; Wallis, C.; Metcalfe, C.; Shute, J.K.; Bush, A. Safety and use of sputum induction in children with cystic fibrosis. Pediatr Pulmonol 2003, 35, 309–313. [Google Scholar] [CrossRef]
- Forton, J. Induced sputum in young healthy children with cystic fibrosis. Paediatr Respir Rev 2015, 16 Suppl 1, 6–8. [Google Scholar] [CrossRef]
- Zar, H.J.; Hanslo, D.; Apolles, P.; Swingler, G.; Hussey, G. Induced sputum versus gastric lavage for microbiological confirmation of pulmonary tuberculosis in infants and young children: a prospective study. Lancet 2005, 365, 130–134. [Google Scholar] [CrossRef]
- Jochmann, A.; Artusio, L.; Robson, K.; Nagakumar, P.; Collins, N.; Fleming, L.; Bush, A.; Saglani, S. Infection and inflammation in induced sputum from preschool children with chronic airways diseases. Pediatr Pulmonol 2016, 51, 778–786. [Google Scholar] [CrossRef]
- Ronchetti, K.; Tame, J.D.; Paisey, C.; Thia, L.P.; Doull, I.; Howe, R.; Mahenthiralingam, E.; Forton, J.T. The CF-Sputum Induction Trial (CF-SpIT) to assess lower airway bacterial sampling in young children with cystic fibrosis: a prospective internally controlled interventional trial. Lancet Respir Med 2018, 6, 461–471. [Google Scholar] [CrossRef]
- DeLuca, A.N.; Hammitt, L.L.; Kim, J.; Higdon, M.M.; Baggett, H.C.; Brooks, W.A.; Howie, S.R.C.; Deloria Knoll, M.; Kotloff, K.L.; Levine, O.S.; et al. Safety of Induced Sputum Collection in Children Hospitalized With Severe or Very Severe Pneumonia. Clin Infect Dis 2017, 64, S301–S308. [Google Scholar] [CrossRef]
- Moore, H.A.; Apolles, P.; de Villiers, P.J.; Zar, H.J. Sputum induction for microbiological diagnosis of childhood pulmonary tuberculosis in a community setting. Int J Tuberc Lung Dis 2011, 15, 1185–1190. [Google Scholar] [CrossRef] [PubMed]
- Lex, C.; Payne, D.N.; Zacharasiewicz, A.; Li, A.M.; Wilson, N.M.; Hansel, T.T.; Bush, A. Sputum induction in children with difficult asthma: safety, feasibility, and inflammatory cell pattern. Pediatr Pulmonol 2005, 39, 318–324. [Google Scholar] [CrossRef] [PubMed]
- Joel, D.R.; Steenhoff, A.P.; Mullan, P.C.; Phelps, B.R.; Tolle, M.A.; Ho-Foster, A.; Mabikwa, V.; Kgathi, B.G.; Ncube, R.; Anabwani, G.M. Diagnosis of paediatric tuberculosis using sputum induction in Botswana: programme description and findings. Int J Tuberc Lung Dis 2014, 18, 328–334. [Google Scholar] [CrossRef]
- De Boeck, K.; Alifier, M.; Vandeputte, S. Sputum induction in young cystic fibrosis patients. Eur Respir J 2000, 16, 91–94. [Google Scholar] [CrossRef]
- Jones, P.D.; Hankin, R.; Simpson, J.; Gibson, P.G.; Henry, R.L. The tolerability, safety, and success of sputum induction and combined hypertonic saline challenge in children. Am J Respir Crit Care Med 2001, 164, 1146–1149. [Google Scholar] [CrossRef] [PubMed]
- Cao, Y.; Chen, S.; Chen, X.; Zou, W.; Liu, Z.; Wu, Y.; Hu, S. Global trends in the incidence and mortality of asthma from 1990 to 2019: An age-period-cohort analysis using the global burden of disease study 2019. Front Public Health 2022, 10, 1036674. [Google Scholar] [CrossRef]
- Covar, R.A.; Spahn, J.D.; Martin, R.J.; Silkoff, P.E.; Sundstrom, D.A.; Murphy, J.; Szefler, S.J. Safety and application of induced sputum analysis in childhood asthma. J Allergy Clin Immunol 2004, 114, 575–582. [Google Scholar] [CrossRef]
- Drews, A.C.; Pizzichini, M.M.M.; Pizzichini, E.; Pereira, M.U.; Pitrez, P.M.; Jones, M.H.; Sly, P.D.; Stein, R.T. Neutrophilic airway inflammation is a main feature of induced sputum in nonatopic asthmatic children. Allergy 2009, 64, 1597–1601. [Google Scholar] [CrossRef]
- Eller, M.C.N.; Vergani, K.P.; Saraiva-Romanholo, B.M.; Antonangelo, L.; Leone, C.; Rodrigues, J.C. Can inflammatory markers in induced sputum be used to detect phenotypes and endotypes of pediatric severe therapy-resistant asthma? Pediatr Pulmonol 2018, 53, 1208–1217. [Google Scholar] [CrossRef]
- Kansal, P.; Nandan, D.; Agarwal, S.; Patharia, N.; Arya, N. Correlation of induced sputum eosinophil levels with clinical parameters in mild and moderate persistent asthma in children aged 7-18 years. J Asthma 2018, 55, 385–390. [Google Scholar] [CrossRef]
- Green, R.H.; Brightling, C.E.; McKenna, S.; Hargadon, B.; Parker, D.; Bradding, P.; Wardlaw, A.J.; Pavord, I.D. Asthma exacerbations and sputum eosinophil counts: a randomised controlled trial. Lancet 2002, 360, 1715–1721. [Google Scholar] [CrossRef] [PubMed]
- Ciolkowski, J.; Stasiowska, B.; Mazurek, H. [Control of asthma symptoms and cellular markers of inflammation in induced sputum in children and adolescents with chronic asthma]. Pol Merkur Lekarski 2009, 26, 178–183. [Google Scholar] [PubMed]
- Fleming, L.; Wilson, N.; Regamey, N.; Bush, A. Use of sputum eosinophil counts to guide management in children with severe asthma. Thorax 2012, 67, 193–198. [Google Scholar] [CrossRef] [PubMed]
- Petsky, H.L.; Li, A.; Chang, A.B. Tailored interventions based on sputum eosinophils versus clinical symptoms for asthma in children and adults. Cochrane Database Syst Rev 2017, 8, CD005603. [Google Scholar] [CrossRef] [PubMed]
- Hossny, E.; El-Awady, H.; Bakr, S.; Labib, A. Vascular endothelial growth factor overexpression in induced sputum of children with bronchial asthma. Pediatr Allergy Immunol 2009, 20, 89–96. [Google Scholar] [CrossRef] [PubMed]
- Fireman, E.; Bliznuk, D.; Schwarz, Y.; Soferman, R.; Kivity, S. Biological monitoring of particulate matter accumulated in the lungs of urban asthmatic children in the Tel-Aviv area. Int Arch Occup Environ Health 2015, 88, 443–453. [Google Scholar] [CrossRef]
- Nagakumar, P.; Denney, L.; Fleming, L.; Bush, A.; Lloyd, C.M.; Saglani, S. Type 2 innate lymphoid cells in induced sputum from children with severe asthma. J Allergy Clin Immunol 2016, 137, 624–626. [Google Scholar] [CrossRef]
- Hamzaoui, A.; Ammar, J.; Hamzaoui, K. Regulatory T cells in induced sputum of asthmatic children: association with inflammatory cytokines. Multidiscip Respir Med 2010, 5, 22–30. [Google Scholar] [CrossRef]
- Felicio-Junior, E.L.; Barnabe, V.; de Almeida, F.M.; Avona, M.D.; de Genaro, I.S.; Kurdejak, A.; Eller, M.C.N.; Verganid, K.P.; Rodrigues, J.C.; Tiberio, I.; et al. Randomized trial of physiotherapy and hypertonic saline techniques for sputum induction in asthmatic children and adolescents. Clinics (Sao Paulo) 2020, 75, e1512. [Google Scholar] [CrossRef]
- Buendia, J.A.; Talamoni, H.L. Cost-utility of use of sputum eosinophil counts to guide management in children with asthma. J Asthma 2022, 59, 31–37. [Google Scholar] [CrossRef]
- Rowe, S.M.; Miller, S.; Sorscher, E.J. Cystic fibrosis. N Engl J Med 2005, 352, 1992–2001. [Google Scholar] [CrossRef] [PubMed]
- Chmiel, J.F.; Davis, P.B. State of the art: why do the lungs of patients with cystic fibrosis become infected and why can't they clear the infection? Respir Res 2003, 4, 8. [Google Scholar] [CrossRef] [PubMed]
- Stoltz, D.A.; Meyerholz, D.K.; Welsh, M.J. Origins of cystic fibrosis lung disease. N Engl J Med 2015, 372, 1574–1575. [Google Scholar] [CrossRef] [PubMed]
- Rosenfeld, M.; Emerson, J.; Accurso, F.; Armstrong, D.; Castile, R.; Grimwood, K.; Hiatt, P.; McCoy, K.; McNamara, S.; Ramsey, B.; et al. Diagnostic accuracy of oropharyngeal cultures in infants and young children with cystic fibrosis. Pediatr Pulmonol 1999, 28, 321–328. [Google Scholar] [CrossRef]
- Forton, J.T. Detecting respiratory infection in children with cystic fibrosis: Cough swab, sputum induction or bronchoalveolar lavage. Paediatr Respir Rev 2019, 31, 28–31. [Google Scholar] [CrossRef]
- Schultz, A.; Caudri, D. Cough swabs less useful but induced sputum very useful in symptomatic older children with cystic fibrosis. Lancet Respir Med 2018, 6, 410–411. [Google Scholar] [CrossRef]
- Mussaffi, H.; Fireman, E.M.; Mei-Zahav, M.; Prais, D.; Blau, H. Induced sputum in the very young: a new key to infection and inflammation. Chest 2008, 133, 176–182. [Google Scholar] [CrossRef]
- Ho, S.A.; Ball, R.; Morrison, L.J.; Brownlee, K.G.; Conway, S.P. Clinical value of obtaining sputum and cough swab samples following inhaled hypertonic saline in children with cystic fibrosis. Pediatr Pulmonol 2004, 38, 82–87. [Google Scholar] [CrossRef]
- Al-Saleh, S.; Dell, S.D.; Grasemann, H.; Yau, Y.C.; Waters, V.; Martin, S.; Ratjen, F. Sputum induction in routine clinical care of children with cystic fibrosis. J Pediatr 2010, 157, 1006–1011. [Google Scholar] [CrossRef]
- Blau, H.; Linnane, B.; Carzino, R.; Tannenbaum, E.L.; Skoric, B.; Robinson, P.J.; Robertson, C.; Ranganathan, S.C. Induced sputum compared to bronchoalveolar lavage in young, non-expectorating cystic fibrosis children. J Cyst Fibros 2014, 13, 106–110. [Google Scholar] [CrossRef]
- D'Sylva, P.; Caudri, D.; Shaw, N.; Turkovic, L.; Douglas, T.; Bew, J.; Keil, A.D.; Stick, S.; Schultz, A. Induced sputum to detect lung pathogens in young children with cystic fibrosis. Pediatr Pulmonol 2017, 52, 182–189. [Google Scholar] [CrossRef]
- Weiser, R.; Oakley, J.; Ronchetti, K.; Tame, J.D.; Hoehn, S.; Jurkowski, T.P.; Mahenthiralingam, E.; Forton, J.T. The lung microbiota in children with cystic fibrosis captured by induced sputum sampling. J Cyst Fibros 2022, 21, 1006–1012. [Google Scholar] [CrossRef]
- Hoppe, J.E.; Towler, E.; Wagner, B.D.; Accurso, F.J.; Sagel, S.D.; Zemanick, E.T. Sputum induction improves detection of pathogens in children with cystic fibrosis. Pediatr Pulmonol 2015, 50, 638–646. [Google Scholar] [CrossRef]
- Ahmed, M.I.; Kulkarni, H.; Shajpal, S.; Patel, D.; Patel, P.; Claydon, A.; Modha, D.E.; Gaillard, E.A. Early detection of non-tuberculous mycobacteria in children with cystic fibrosis using induced sputum at annual review. Pediatr Pulmonol 2019, 54, 257–263. [Google Scholar] [CrossRef]
- Sagel, S.D.; Wagner, B.D.; Anthony, M.M.; Emmett, P.; Zemanick, E.T. Sputum biomarkers of inflammation and lung function decline in children with cystic fibrosis. Am J Respir Crit Care Med 2012, 186, 857–865. [Google Scholar] [CrossRef]
- Lepissier, A.; Addy, C.; Hayes, K.; Noel, S.; Bui, S.; Burgel, P.R.; Dupont, L.; Eickmeier, O.; Fayon, M.; Leal, T.; et al. Inflammation biomarkers in sputum for clinical trials in cystic fibrosis: current understanding and gaps in knowledge. J Cyst Fibros 2022, 21, 691–706. [Google Scholar] [CrossRef]
- Giacalone, V.D.; Moncada-Giraldo, D.; Margaroli, C.; Brown, M.R.; Silva, G.L.; Chandler, J.D.; Peng, L.; Tirouvanziam, R.; Guglani, L.; Program, I.-C. Pilot study of inflammatory biomarkers in matched induced sputum and bronchoalveolar lavage of 2-year-olds with cystic fibrosis. Pediatr Pulmonol 2022, 57, 2189–2198. [Google Scholar] [CrossRef]
- Schupp, J.C.; Khanal, S.; Gomez, J.L.; Sauler, M.; Adams, T.S.; Chupp, G.L.; Yan, X.; Poli, S.; Zhao, Y.; Montgomery, R.R.; et al. Single-Cell Transcriptional Archetypes of Airway Inflammation in Cystic Fibrosis. Am J Respir Crit Care Med 2020, 202, 1419–1429. [Google Scholar] [CrossRef]
- Kockar Kizilirmak T., G. A. , Yin H., Bruscia E., Egan M., Britto-Leon C. Understanding Impact of CFTR Dysfunction on Airway Immune Cell Composition in Early Lung Disease Pathogenesis. In Proceedings of Am J Respir Crit Care Med; p. 6357.
- Ruddy, J.; Emerson, J.; Moss, R.; Genatossio, A.; McNamara, S.; Burns, J.L.; Anderson, G.; Rosenfeld, M. Sputum tobramycin concentrations in cystic fibrosis patients with repeated administration of inhaled tobramycin. J Aerosol Med Pulm Drug Deliv 2013, 26, 69–75. [Google Scholar] [CrossRef]
- Ordonez, C.L.; Henig, N.R.; Mayer-Hamblett, N.; Accurso, F.J.; Burns, J.L.; Chmiel, J.F.; Daines, C.L.; Gibson, R.L.; McNamara, S.; Retsch-Bogart, G.Z.; et al. Inflammatory and microbiologic markers in induced sputum after intravenous antibiotics in cystic fibrosis. Am J Respir Crit Care Med 2003, 168, 1471–1475. [Google Scholar] [CrossRef]
- Global Burden of Disease, C.; Adolescent Health, C.; Kassebaum, N.; Kyu, H.H.; Zoeckler, L.; Olsen, H.E.; Thomas, K.; Pinho, C.; Bhutta, Z.A.; Dandona, L.; et al. Child and Adolescent Health From 1990 to 2015: Findings From the Global Burden of Diseases, Injuries, and Risk Factors 2015 Study. JAMA Pediatr 2017, 171, 573–592. [Google Scholar] [CrossRef]
- Murdoch, D.R.; Morpeth, S.C.; Hammitt, L.L.; Driscoll, A.J.; Watson, N.L.; Baggett, H.C.; Brooks, W.A.; Deloria Knoll, M.; Feikin, D.R.; Kotloff, K.L.; et al. The Diagnostic Utility of Induced Sputum Microscopy and Culture in Childhood Pneumonia. Clin Infect Dis 2017, 64, S280–S288. [Google Scholar] [CrossRef]
- Green, A.; Cockroft, J.L.; Kaufman, R.A.; McCullers, J.A.; Arnold, S.R. Utility of Induced Sputum in Assessing Bacterial Etiology for Community-Acquired Pneumonia in Hospitalized Children. J Pediatric Infect Dis Soc 2022, 11, 274–282. [Google Scholar] [CrossRef]
- Tramper-Stranders, G.A. Childhood community-acquired pneumonia: A review of etiology- and antimicrobial treatment studies. Paediatr Respir Rev 2018, 26, 41–48. [Google Scholar] [CrossRef]
- Lahti, E.; Peltola, V.; Waris, M.; Virkki, R.; Rantakokko-Jalava, K.; Jalava, J.; Eerola, E.; Ruuskanen, O. Induced sputum in the diagnosis of childhood community-acquired pneumonia. Thorax 2009, 64, 252–257. [Google Scholar] [CrossRef]
- Kurade, A.; Dhanawade, S.; Shetti, S. Induced Sputum as a Diagnostic Tool in Pneumonia in Under Five Children-A Hospital-based Study. J Trop Pediatr 2018, 64, 510–515. [Google Scholar] [CrossRef]
- Ogawa, M.; Hoshina, T.; Abushawish, A.; Kusuhara, K. Evaluation of the usefulness of culture of induced sputum and the optimal timing for the collection of a good-quality sputum sample to identify causative pathogen of community-acquired pneumonia in young children: A prospective observational study. J Microbiol Immunol Infect 2023, 56, 1036–1044. [Google Scholar] [CrossRef]
- Thea, D.M.; Seidenberg, P.; Park, D.E.; Mwananyanda, L.; Fu, W.; Shi, Q.; Baggett, H.C.; Brooks, W.A.; Feikin, D.R.; Howie, S.R.C.; et al. Limited Utility of Polymerase Chain Reaction in Induced Sputum Specimens for Determining the Causes of Childhood Pneumonia in Resource-Poor Settings: Findings From the Pneumonia Etiology Research for Child Health (PERCH) Study. Clin Infect Dis 2017, 64, S289–S300. [Google Scholar] [CrossRef]
- Honkinen, M.; Lahti, E.; Osterback, R.; Ruuskanen, O.; Waris, M. Viruses and bacteria in sputum samples of children with community-acquired pneumonia. Clin Microbiol Infect 2012, 18, 300–307. [Google Scholar] [CrossRef]
- Das, C.K.; Mirdha, B.R.; Singh, S.; Seth, R.; Bagga, A.; Lodha, R.; Kabra, S.K. Use of Induced sputum to determine the prevalence of Pneumocystis jirovecii in immunocompromised children with pneumonia. J Trop Pediatr 2014, 60, 216–222. [Google Scholar] [CrossRef]
- LaRocque, R.C.; Katz, J.T.; Perruzzi, P.; Baden, L.R. The utility of sputum induction for diagnosis of Pneumocystis pneumonia in immunocompromised patients without human immunodeficiency virus. Clin Infect Dis 2003, 37, 1380–1383. [Google Scholar] [CrossRef] [PubMed]
- Zar, H.J.; Tannenbaum, E.; Hanslo, D.; Hussey, G. Sputum induction as a diagnostic tool for community-acquired pneumonia in infants and young children from a high HIV prevalence area. Pediatr Pulmonol 2003, 36, 58–62. [Google Scholar] [CrossRef] [PubMed]
- 2023, W.G.t.r. WHO Global Tuberculosis Report 2023. WHO report. Availabe online: https://www.who. 2023. [Google Scholar]
- Zar, H.J.; Tannenbaum, E.; Apolles, P.; Roux, P.; Hanslo, D.; Hussey, G. Sputum induction for the diagnosis of pulmonary tuberculosis in infants and young children in an urban setting in South Africa. Arch Dis Child 2000, 82, 305–308. [Google Scholar] [CrossRef] [PubMed]
- Al Zahrani, K.; Al Jahdali, H.; Poirier, L.; Rene, P.; Menzies, D. Yield of smear, culture and amplification tests from repeated sputum induction for the diagnosis of pulmonary tuberculosis. Int J Tuberc Lung Dis 2001, 5, 855–860. [Google Scholar]
- Hatherill, M.; Hawkridge, T.; Zar, H.J.; Whitelaw, A.; Tameris, M.; Workman, L.; Geiter, L.; Hanekom, W.A.; Hussey, G. Induced sputum or gastric lavage for community-based diagnosis of childhood pulmonary tuberculosis? Arch Dis Child 2009, 94, 195–201. [Google Scholar] [CrossRef]
- Moore, D.P.; Higdon, M.M.; Hammitt, L.L.; Prosperi, C.; DeLuca, A.N.; Da Silva, P.; Baillie, V.L.; Adrian, P.V.; Mudau, A.; Deloria Knoll, M.; et al. The Incremental Value of Repeated Induced Sputum and Gastric Aspirate Samples for the Diagnosis of Pulmonary Tuberculosis in Young Children With Acute Community-Acquired Pneumonia. Clin Infect Dis 2017, 64, S309–S316. [Google Scholar] [CrossRef]
- Ioos, V.; Cordel, H.; Bonnet, M. Alternative sputum collection methods for diagnosis of childhood intrathoracic tuberculosis: a systematic literature review. Arch Dis Child 2019, 104, 629–635. [Google Scholar] [CrossRef]
- Gonzalez-Angulo, Y.; Wiysonge, C.S.; Geldenhuys, H.; Hanekom, W.; Mahomed, H.; Hussey, G.; Hatherill, M. Sputum induction for the diagnosis of pulmonary tuberculosis: a systematic review and meta-analysis. Eur J Clin Microbiol Infect Dis 2012, 31, 1619–1630. [Google Scholar] [CrossRef]
- Lewinsohn, D.M.; Leonard, M.K.; LoBue, P.A.; Cohn, D.L.; Daley, C.L.; Desmond, E.; Keane, J.; Lewinsohn, D.A.; Loeffler, A.M.; Mazurek, G.H.; et al. Official American Thoracic Society/Infectious Diseases Society of America/Centers for Disease Control and Prevention Clinical Practice Guidelines: Diagnosis of Tuberculosis in Adults and Children. Clin Infect Dis 2017, 64, 111–115. [Google Scholar] [CrossRef]
- Chen, Q.P.; Ren, S.F.; Wang, X.F.; Wang, M.S. Comparison of bronchial brushing and sputum in detection of pediatric pulmonary tuberculosis. Ital J Pediatr 2016, 42, 11. [Google Scholar] [CrossRef]
- Luo, W.; Lin, Y.; Li, Z.; Wang, W.; Shi, Y. Comparison of sputum induction and bronchoscopy in diagnosis of sputum smear-negative pulmonary tuberculosis: a systemic review and meta-analysis. BMC Pulm Med 2020, 20, 146. [Google Scholar] [CrossRef] [PubMed]
- Olbrich, L.; Verghese, V.P.; Franckling-Smith, Z.; Sabi, I.; Ntinginya, N.E.; Mfinanga, A.; Banze, D.; Viegas, S.; Khosa, C.; Semphere, R.; et al. Diagnostic accuracy of a three-gene Mycobacterium tuberculosis host response cartridge using fingerstick blood for childhood tuberculosis: a multicentre prospective study in low-income and middle-income countries. Lancet Infect Dis 2024, 24, 140–149. [Google Scholar] [CrossRef] [PubMed]
- Li, A.M.; Hung, E.; Tsang, T.; Yin, J.; So, H.K.; Wong, E.; Fok, T.F.; Ng, P.C. Induced sputum inflammatory measures correlate with disease severity in children with obstructive sleep apnoea. Thorax 2007, 62, 75–79. [Google Scholar] [CrossRef] [PubMed]
- Ervine, E.; McMaster, C.; McCallion, W.; Shields, M.D. Pepsin measured in induced sputum-a test for pulmonary aspiration in children? J Pediatr Surg 2009, 44, 1938–1941. [Google Scholar] [CrossRef]
- Rosewich, M.; Zissler, U.M.; Kheiri, T.; Voss, S.; Eickmeier, O.; Schulze, J.; Herrmann, E.; Ducker, R.P.; Schubert, R.; Zielen, S. Airway inflammation in children and adolescents with bronchiolitis obliterans. Cytokine 2015, 73, 156–162. [Google Scholar] [CrossRef]
- Crespo-Lessmann, A.; Plaza, V.; Consensus, G. Multidisciplinary consensus on sputum induction biosafety during the COVID-19 pandemic. Allergy 2021, 76, 2407–2419. [Google Scholar] [CrossRef]
Figure 1.
The success rate of sputum induction by age groups (0-18 years).
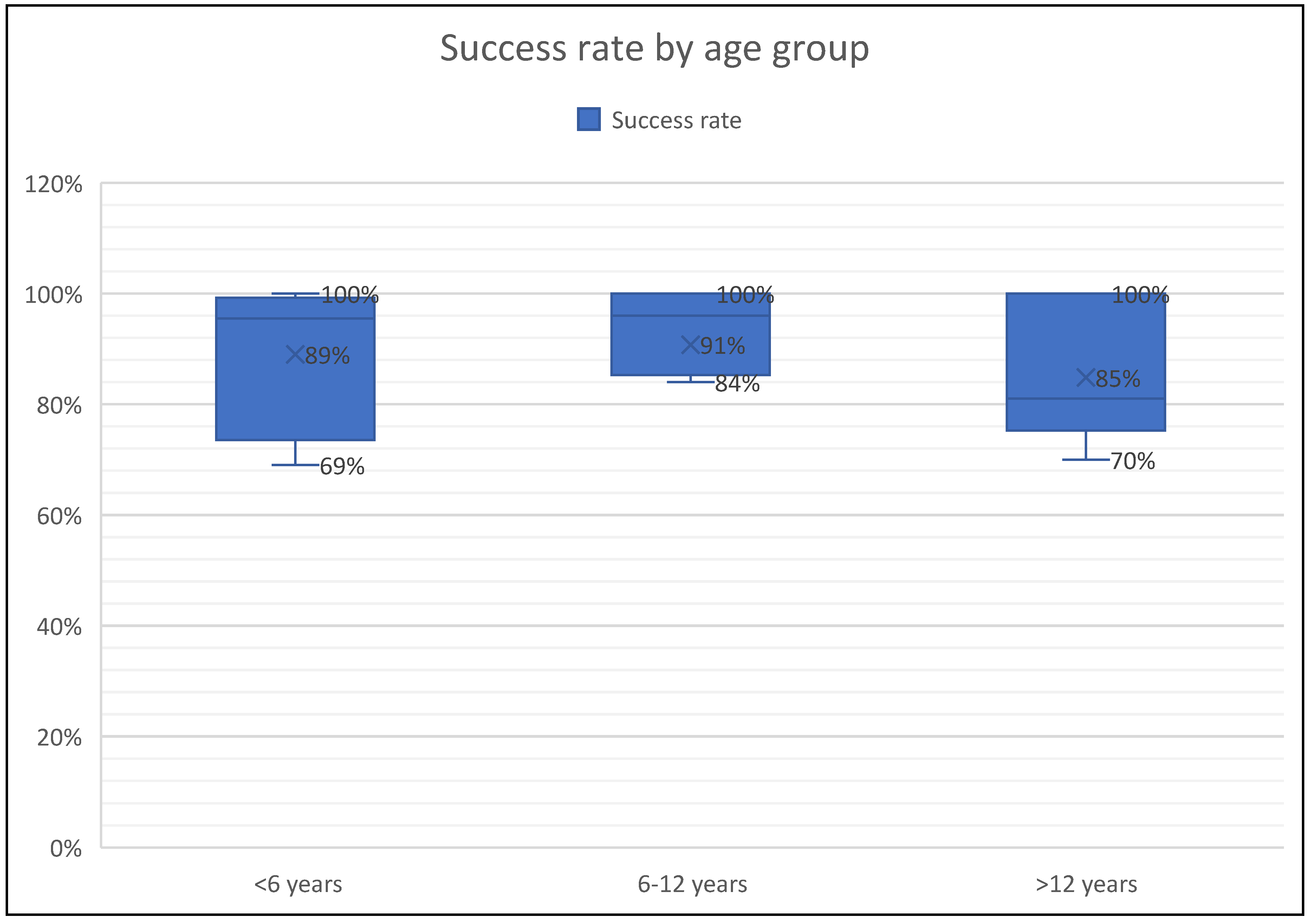

Table 1.
Summary of studies using sputum induction in children with respiratory diseases.
| First Author | N of subjects | Age (y) | Diseases | Analysis | Success rate | Side effects |
| De Boeck et al. (2000) [24] |
19 | 8.6 (4.3-15.2) | Cystic fibrosis | Microbiological yield | N/A | Salty taste Fall in FEV1>6 Fall in FEV1> Wheezing and cough(5.2%) |
| Wilson et al. (2000) [11] | Asthma:60 HC:27 |
10.2 (8.4-11) | Asthma | eosinophil counts and ECP levels | 61% | Dry cough |
| Jones PD et al. (2001) [25] | 53 | 7-16 (10.8) | Asthma | Safety and success of SI | 92% | Dry cough (3.7%) Fall in FEV1 >20% (3.7 %) |
| Sagel et al. (2001) [12] | CF:20 HC:11 |
6-12 | Cystic fibrosis | Total cell counts, ANC, IL-8, NE activity | 92% in CF 64% in HC |
Fall in FEV1 >10% (43%) Fall in FEV1 >20% (14%) |
| Covar R.A. et al. (2004) [27] | 117 | 13 (11-15) | Asthma | eosinophil counts, SPEos, ECP levels | 76.9% | Bronchospasm (7.7%) GI dyscomfort, nausea |
| Lex C et al. (2005) [22] | 38 | 6-16 | Asthma | Eosinophil, neutrophil counts | 73.6% | Dyspnea and wheezing (18.4%), Fall in FEV1>20% (7.8%) |
| Ciolkowski J et al. (2009) [32] | 154 | 8-21 | Asthma | Eosinophil, neutrophil counts | 78% | Not reported |
| Drews C.A et al. (2009) [28] | 77 | 12-13 | Asthma | eosinophil counts | 70.1% | Not reported |
| Ervine E et al. (2009) [86] | 21 | 8.7 (4-16) | GER | Pepsin | 100% | No side effects |
| Hossny E et al. (2009) [35] | Asthma:18 HC:34 |
9.8 (6-16) | Asthma | VEGF levels | 100% | Not reported |
| Lahti E et al. (2009) [66] | 101 | 3.4 (1.7-6.8) | CAP | Microbiological yield | 75.2% | unpleasant due to nasophayngeal aspiration |
| Hamzaoui et al. (2010) [38] | Asthma: 40 HC:20 |
11 (5-16.5) | Asthma | Treg cells, cytokines | 100% | Not reported |
| Moore et al. (2011) [21] | 270 | 3.2 (0.2-13 years | Pulmonary TB | Microbiological yield (Diagnosis of TB) | 99% | Mild epistaxis (15%), mild wheeze (0.6%), increased cough (6%) |
| Fleming et al. (2012) [33] |
45 | 13 (10.2-15.8) | Severe asthma | Eosinophils, neutrophil counts | 85% | Not reported |
| Das C.K et al. (2014) [71] | 105 | 74.5 ± 43.7 months | Intensive care with pneumonia | Microbiological yield (PCR assay) | 100% | Vomiting (8.5%), epistaxis (3.8%), transient bronchospasm(1.9%) |
| Joel et al. (2014) [23] | 1294 | 3.8 (<18 years) | Pulmonary TB | Microbiological yield (Diagnosis of TB) | 100% | Vomiting (0.5%), Mild epistaxis (0.4%), mild wheeze (0.08%), increased cough (0.17%) |
| Blau et al. (2014) [50] | 10 | 3 - 7.4 years | Cystic fibrosis | Microbiological yield | 91% | ‘Distressed’(n:2): crying and resisting somewhat. ‘Very distressed’ (n:1): crying and resisting a lot |
| Fireman E. et al. (2015) [36] | 136 | 12.6 ± 2.9 years | Asthma | Particulate matter level | 100% | Not reported |
| Jochmann et al. (2016) [18] | 64 | 2.7 (0.6 -6.3) | Chronic airway diseases | Microbiological yield | 96% | 4.6% (3/64) did not tolerate procedure, none |
| Nagakumar et al. (2016) [37] | Asthma:13 LRTI: 6 |
12.5 (8-16) years | Severe asthma | Flow cytometry | 100% | Not reported |
| D’Sylva et al. (2017) [51] | 57 | 3.3 (0.9-6.7) years |
Cystic fibrosis | Microbiological yield | 95% | Not reported |
| Murdoch et al. (2017) [63] | 3772 | 0.7 (0.1-5) | CAP | Microbiological yield | 69.1% | Transient drop in oxygen saturation (0.34%) |
| Eller et al. (2018) [29] | 40 | 12.8 (6-18) | Severe asthma | Total cell counts, IL-10, GM-CSF, IFN-gamma, and TNF-alpha | 70% | Not reported |
| Ronchetti et al., (2018) [19] | 124 | 8.2 (4.9-12.6) | Cystic fibrosis | Microbiological yield | 84% | upset(9%), mild wheeze(3%), vomiting(2%) transient dizziness(<1%) |
| Ahmed M.I et al. (2019) [54] | 42 | 11.4 (5-17) | Cystic fibrosis | Microbiological yield- NTM detection | 89% | Not reported |
| Felicio-Junior et al. (2020) [39] | 33 | 7-18 | Asthma | Differential cell count | 91% | No side effects |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



