
Submitted:
17 September 2024
Posted:
18 September 2024
You are already at the latest version
Abstract
Background:Tourette syndrome (TS) is a characterized by motor and vocal tics, often accompanied by obsessive-compulsive disorder (OCD) and attention-deficit/hyperactivity disorder (ADHD). Cannabis-based medicines (CBM) present a promising avenue for future therapeutic intervention owing to their interaction with the endocannabinoid system, potentially mitigating tics and associated symptoms. Unlike conventional treatments such as antipsychotics, CBM exhibits improved tolerability and reduced side effects. While the available evidence is still limited, ongoing research underscores the potential of CBM to enhance the quality of life for patients, establishing it as a pivotal area for future therapeutic advancements in TS. Aim: In our systematic review and meta-analysis, we aim to assess the effectiveness of cannabis-based medicine (CBM) in the treatment of Tourette Syndrome. Methods: We searched in electronic databases (PubMed, Google Scholar, Science Direct, Cochrane Collaboration Database of Randomized Trials) was performed to identify cohort studies and randomized controlled trials (RCTs) up to 18th June 2024. Data extraction focused on baseline characteristics of the included studies and efficacy outcomes, including scores on the Yale Global Tic Severity Scale (YGTSS) and Premonitory Urge for Tics Scale (PUTS). We conducted the meta-analysis using Review Manager version 5.4. software. We compared the measurements before and after CBM intake using mean difference (MD) and 95% confidence interval (CI). Result: In total, 1105 articles were identified for screening, with eight studies included in the systematic review and seven in the meta-analysis. These studies involved 306 adult patients with TS treated with cannabis. YGTSS revealed a significant reduction in total scores (MD = -13.29, 95% CI [-21.67 to -4.91], P = 0.002) and PUTS revealed a significant decrease in scores (MD = -4.09, 95% CI [-7.24 to -0.93], P = 0.01). Conclusion: The research emphasizes the potential of cannabis-based medication in alleviating tics and premonitory urges associated with Tourette syndrome. While the initial results are promising, they are based on limited-scale studies. It is imperative to conduct larger, placebo-controlled trials encompassing diverse demographic groups to substantiate the effectiveness, ensure safety, and optimize dosages for long-term therapeutic advantages.
Keywords:
Cannabinoids
; Tourette Syndrome
; Tics
; Endocannabinoid system
Introduction
Tourette syndrome (TS) is a neuropsychiatric disorder with childhood onset, characterized by motor and vocal tics, often accompanied by comorbidities such as obsessive-compulsive disorder (OCD) and attention-deficit/ hyperactivity disorder (ADHD) [1,2]. Globally, the prevalence of TS is 0.5%, higher in children and adolescents and in males, with approximately 118 cases per million adults [3,4]. Tic disorders affect 1-3% of school-aged children, with echolalia or echopraxia occurring in roughly one-third of cases [5,6]. TS is diagnosed by the presence of both motor and vocal tics for over one year, without explanation by other conditions, typically presenting before age 18. Individuals often report a premonitory sensation that is relieved after performing a tic [7].
TS results from disruptions in the cortico-striato-thalamo-cortical (CSTC) loops connecting the frontal cortices and basal ganglia [8,9,10]. There is strong genetic involvement, with polygenic, oligogenic, and bilineal inheritance patterns [11,12,13]. Although some patients have elevated antistreptolysin O antibodies, there is no definitive link between TS and pediatric autoimmune neuropsychiatric disorder associated with streptococcal infections (PANDAS) [14,15]. Environmental factors, including intrauterine insults, preterm birth, cesarean section, breech presentation, low birth weight, and early antibiotic use, are also associated with TS [16,17].
TS significantly impacts health-related quality of life (HR-QOL) [18]. Adolescents with TS may experience panic, embarrassment, and social isolation due to the sudden onset of tics [19]. Children often face functional impairments, attention issues, slower learning, and conflicts with teachers, exacerbated by symptoms such as echopraxia and coprolalia [20,21]. Adults with TS have higher rates of anxiety, depression, and obsessionality compared to the general population, and experience higher unemployment rates, discrimination, and lower quality of life [22,23].
Current treatments for TS include antipsychotics, behavioral therapies, and advanced neuroimaging to better understand its pathophysiology. Antipsychotics such as Haloperidol and Pimozide were among the first medications approved for tic management in TS, though they carry a high risk of side effects [24]. Risperidone is commonly prescribed, offering a lower risk of severe side effects [25]. These medications manage tics by modulating neurotransmitters, especially dopamine. Non-pharmacological treatments, such as Comprehensive Behavioral Intervention for Tics (CBIT), are also effective [26]. New pharmaceutical agents, including Selective Vesicular Monoamine Transporter 2 (VMAT2) inhibitors and D1 Receptor antagonists, are being tested to improve patient outcomes [27,28]. Neurostimulation techniques like Globus pallidus internus (GPi) stimulation, repetitive transcranial magnetic stimulation (rTMS), and mindfulness-based interventions have also shown promise in tic reduction [29,30,31,32].
Cannabis sativa has a long history of recreational and medicinal use, and its therapeutic potential in various conditions has recently garnered attention [33]. Cannabis-based medicines (CBM), including tetrahydrocannabinol, THX-110 combinations, cannabinoid oils, and synthetic cannabinoids like palmitoylethanolamide, interact with the endocannabinoid system (ECS) by binding to cannabinoid receptors CB1 and CB2 [34,35,36,37]. CB1 receptors are predominantly found in the central nervous system, while CB2 receptors are more abundant in immune cells. The American Academy of Neurology (AAN) in 2019 and the European Society for the Study of Tourette Syndrome (ESSTS) in 2021 recommend CBM for experimental therapy in TS [38,39].
Emerging evidence suggests that CBM may be a promising treatment strategy for TS, improving both tics and comorbidities with good tolerability. However, current data is limited to case reports, case series, open-label studies, and a few small randomized controlled trials (RCTs). This systematic review and meta-analysis aims to provide a comprehensive evaluation of CBM efficacy in reducing tic severity in TS.
Methods
This review focuses on clinical studies concerning the use of CBM in patients with Tourette Syndrome . We excluded animal studies and publications that only discussed the pathophysiology of CBM without presenting clinical data. The review follows the guidelines for Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) for 2020 in Figure 1, and only uses data collected from published papers, eliminating the need for ethical approval.
Systematic Literature Search and Study Selection
We conducted a thorough search for relevant publications by using PubMed (including Medline), Google Scholar, Cochrane Library and Science Direct: We searched for studies mentioned in review papers, editorials, and commentaries on PubMed. Nevertheless, we continued searching for additional studies that satisfied our inclusion criteria.
We had a list of abstracts that we independently reviewed for inclusion using specific criteria. The criteria included the use of medicinal cannabinoids, focusing on Tourette Syndrome. We excluded review papers and animal studies. Six reviewers conducted a dual review, and disagreements were resolved through discussion.
Inclusion and Exclusion Criteria
We established specific criteria for including and excluding participants to achieve our study goals. We included only clinical trials and cohort studies, and our PICOS (Population, Intervention, Comparison and Outcome) was as follows:
- Population: adult patients diagnosed with TS.
- Intervention: treatment with CBM.
- Comparison: placebo or no intervention.
- Outcome: tic severity, premonitory urges symptoms were measured by the Yale Global Tic Severity Scale (YGTSS) and Premonitory Urge for Tics Scale (PUTS).
Other criterias can be summarized in Table 1.
Search Strategy
The population, intervention/condition, control/comparison, and outcome (PICO) criteria were utilized to conduct a thorough literature review. The search was conducted on databases such as PUBMED (including Medline), Google Scholar Libraries, Cochrane Library and Science Direct, using relevant keywords, such as Cannabinoids, Tourette syndrome, Tics, Tic severity. The medical subject heading (MeSH) approach for PubMed (including Medline), Google Scholar, Cochrane Library and Science Direct as detailed in Supplementary Table S1, was employed to develop a comprehensive search strategy.
Quality Appraisal
To ensure the reliability of our chosen papers, we utilized various quality assessment tools. A study by Bloch et al., [41] was in phase 2 RCT, hence no quality assessment was conducted for it. For the other chosen papers we employed the PRISMA checklist, Newcastle-Ottawa Scale (NOS) for non-randomised studies and Cochrane bias tool assessment for randomised clinical trials for systematic reviews and meta-analyses, as shown in Figure 2 and Figure 3 respectively.
Data Extraction and Outcome Measures
Following screening, we extracted relevant data using specifically designed extraction forms. Three authors extracted the data and two authors resolved any differences. Extracted data included but was not limited to study methodology and design, type of CBM and dose, participants demographic characteristics, tic severity and main outcome findings (Supplementary Table S1) . Efficacy outcome measures included scores on YGTSS and PUTS.
Meta-Analysis
We used Review Manager (RevMan) software 5.4 for data analysis. The generic inverse variance method was employed to pool the effect estimates across studies. This method was chosen as it allows for the combination of studies reporting continuous outcomes, specifically mean differences and their corresponding standard deviations, as well as those where standard deviations were not directly available [51]. For most studies included in this analysis, the effect estimates were reported as mean differences along with standard deviations. However, one study provided the mean difference but did not report the standard deviation. In this case, we calculated the standard error using the available data, and then derived the standard deviation from this, ensuring consistency across all studies.The generic inverse variance method was particularly suitable in this context because it allows for the weighting of studies by the inverse of their variance. This approach ensures that studies with more precise estimates (i.e., smaller variances) contribute more to the overall effect size, while maintaining flexibility to incorporate studies with calculated standard errors. By applying this method, we ensured that all studies were included in the analysis while appropriately accounting for the precision of the reported effect estimates [50,51].
The data was presented as the mean difference between after CBM treatment group and before CBM treatment group with a 95 % confidence interval (CI). A p-value of <= 0.05 was deemed statistically significant. The heterogeneity in the data was examined through I-square and p-value for significance. The cochrane handbook’s guidelines for meta-analysis were followed when interpreting the I-square test (0-30%= may not be significant, 30-60% = may represent moderate heterogeneity, 60-90% = may represent substantial heterogeneity and 75-100% = significant heterogeneity) and a p-value of <0.05. The random effects model was adopted for a broader, more realistic CI because our data was heterogeneous in some outcomes.
Results
After searching through four selected databases, PubMed (including Medline), Google Scholar, Cochrane and Science Direct, we extracted 9,449 articles. We then carefully reviewed each paper and applied specific criteria, which led to excluding 391 articles. From the remaining 9,058 papers, we chose not to utilize 9,006 of them due to duplicates or unsatisfactory titles and abstracts. We closely examined the remaining 52 papers and excluded 44 more as their content did not meet our inclusion criteria.
Finally, we conducted a thorough quality check on the remaining eight papers, which all met our criteria. These eight articles are included in our final systematic review and seven articles are included in meta-analysis. Table 2 provides a detailed description of each.
YGTSS
Seven studies involving 208 patients utilized the YGTSS scale for outcome measurement. There was a significant reduction in the total YGTSS score at the endpoint compared to baseline (MD= -13.29, 95% CI [-21.67 to -4.91], p = 0.002). Significant heterogeneity was found across the outcome (Figure 4). Sensitivity analysis was employed to address this heterogeneity in the YGTSS-total outcome. There was a reduction in heterogeneity after removing the studies by Abi-Jaoude et al., [40] and Bloch et al. [41] (Supplementary Figure S1). The reported heterogeneity was (p = 0.06, I-square = 56%). However, heterogeneity is not statistically significant (p > 0.05) [50].
PUTS
Three studies involving 53 patients utilized the PUTS score as an outcome measurement. There was a significant reduction in the PUTS score at the endpoint compared to baseline (MD= - 4.09, 95% CI [ -7.24 to -0.93 ], p = 0.01). Significant heterogeneity was found across the outcome (Figure 5). Sensitivity analysis was employed to address this heterogeneity in the PUTS outcome. There was a reduction in heterogeneity after removing the study from Muller-Vahl et al., 2023 [43] (Supplementary Figure S2). The reported heterogeneity was (p = 0.18, I-square = 42 %). However, heterogeneity is not statistically significant (p > 0.05) [50].
Discussion
TS imposes a substantial burden on both individuals and society, impacting mental health and quality of life. The unpredictable nature of tics often leads to social isolation, bullying, and functional impairments, particularly in school-aged children [12]. Adults with TS frequently report elevated rates of anxiety, depression, and unemployment, contributing to significant healthcare costs and reduced productivity [46]. Additionally, the stigma associated with TS often results in discrimination, further limiting opportunities for social integration and support [18].
CBMs have emerged as a promising therapeutic option for managing TS, characterized by motor and vocal tics. Traditional treatments, such as antipsychotics, are often associated with considerable side effects, prompting the exploration of alternative therapies. CBMs, including tetrahydrocannabinol (THC) and cannabidiol (CBD), modulate the endocannabinoid system by interacting with CB1 and CB2 receptors, potentially aiding in the regulation of tics and associated behaviors [44]. Studies suggest that CBMs can reduce tic frequency and improve comorbid conditions such as anxiety and obsessive-compulsive behaviors [47].
In our systematic review and meta-analysis, we assessed the efficacy of CBMs in treating TS, focusing on tic severity and premonitory urges. We analyzed data from eight studies encompassing 306 patients with TS, with seven studies included in our quantitative synthesis involving 208 patients. Our analysis revealed significant reductions in tic severity and premonitory urges, as measured by the YGTSS and PUTS.
Several studies and systematic reviews have investigated the efficacy of CBMs for TS. Early case series and open-label studies have demonstrated promising reductions in tic severity, with improvements in comorbid conditions such as anxiety and obsessive-compulsive behaviors [48]. Some RCTs using THC reported moderate but significant improvements in tic severity compared to placebo [44]. Systematic reviews highlight the potential benefits of CBMs but note that the current evidence is limited by small sample sizes, short trial durations, and inconsistent dosing protocols [49]. Meta-analyses suggest that CBMs may be beneficial, but larger, well-controlled studies are needed for definitive conclusions [40].
Our pooled analysis of the included studies showed significant reductions in the YGTSS score in the CBM group at the endpoint compared to baseline. These findings warrant a confirmatory study with a placebo comparison. Notably, significant heterogeneity was observed among studies, which was mitigated by sensitivity analysis. The variability in study methodologies and designs, as well as the heterogeneous composition of CBM products derived from Cannabis sativa, may contribute to the observed heterogeneity and complicate comparative studies [57].
Strengths and Limitations
To the best of our knowledge, this systematic review and meta-analysis represents a novel evaluation of the effectiveness of CBMs in patients with TS using a range of parameters across a larger population scale than previously examined. Adhering to PRISMA guidelines and conducting a meta-analysis ensures methodological rigor and transparency. The inclusion of various clinical studies, coupled with the application of quality assessment tools such as the NOS and the Cochrane Risk of Bias Tool, enhances the reliability of the findings. This research provides valuable insights into the efficacy of emerging therapies, such as CBMs, as alternatives to traditional treatments.
However, the study has limitations, including small sample sizes and short durations in most included studies, which restrict the generalizability of the results. Significant heterogeneity across studies, due to variations in methodologies and CBM compositions, complicates comparisons. The reliance on subjective measures, such as the YGTSS and the PUTS, along with the absence of long-term follow-up data, limits the assessment of sustained treatment effects. Additionally, the lack of RCTs in many cases diminishes the overall strength of the evidence, underscoring the need for more rigorous future research.
Conclusion
This study concludes that CBMs exhibit promising potential in reducing tic severity and improving associated symptoms in patients with TS. The meta-analysis revealed significant reductions in scores on the YGTSS and the PUTS. However, the findings are constrained by small sample sizes, study heterogeneity, and a lack of long-term data. While CBMs may offer an alternative to traditional treatments, further large-scale RCTs are necessary to validate their efficacy, safety, and long-term benefits in managing TS symptoms.
Supplementary Materials
The following supporting information can be downloaded at the website of this paper posted on Preprints.org.
Ethical Approval
Not applicable.
Competing interests
The authors declare no competing interests.
References
- Milosev LM, Psathakis N, Szejko N, et al. Treatment of Gilles de la Tourette Syndrome with Cannabis-Based Medicine: Results from a Retrospective Analysis and Online Survey. Cannabis Cannabinoid Res. 2019;4(4):265–74. [CrossRef]
- Müller-Vahl KR, Pisarenko A, Szejko N, et al. CANNA-TICS: Efficacy and safety of oral treatment with nabiximols in adults with chronic tic disorders – Results of a prospective, multicenter, randomized, double-blind, placebo controlled, phase IIIb superiority study. Psychiatry Res. 2023;323:115135. [CrossRef]
- Jafari F, Abbasi P, Rahmati M, Hodhodi T, Kazeminia M. Systematic Review and Meta-Analysis of Tourette Syndrome Prevalence; 1986 to 2022. Pediatr Neurol. 2022 Dec;137:6–16. [CrossRef]
- Levine JLS, Szejko N, Bloch MH. Meta-analysis: Adulthood prevalence of Tourette syndrome. Prog Neuropsychopharmacol Biol Psychiatry. 2019 Dec;95:109675. [CrossRef]
- Lin WD, Tsai FJ, Chou IC. Current understanding of the genetics of Tourette syndrome. Biomed J. 2022;45(2):271–9. [CrossRef]
- Woods DW, Watson TS, Wolfe E, et al. Analyzing the influence of tic-related talk on vocal and motor tics in children with Tourette’s syndrome. J Appl Behav Anal. 2001;34(3):353–6. [CrossRef]
- Olive MF. Tourette syndrome. Infobase Publishing; 2010. Available from: https://www.google.lk/books/edition/Tourette_Syndrome/OkRnYQ_MECAC?hl=en&gbpv=1&dq=symptoms+of+tourette+syndrome+article&printsec=frontcover.
- Worbe Y, Marrakchi-Kacem L, Lecomte S, Valabregue R, Poupon F, Guevara P, et al. Altered structural connectivity of cortico-striato-pallido-thalamic networks in Gilles de la Tourette syndrome. Brain. 2015;138(2):472–82. [CrossRef]
- Thenganatt MA, Jankovic J. Recent Advances in Understanding and Managing Tourette Syndrome. F1000Res. 2016;5:152. [CrossRef]
- Rae CL, Critchley HD. Mechanistic insight into the pathophysiological basis of Tourette syndrome. In: International Review of Movement Disorders. Elsevier; 2022. p. 209–44.
- Singer HS, Augustine F. Controversies Surrounding the Pathophysiology of Tics. J Child Neurol. 2019;34(13):851–62. [CrossRef]
- Leckman JF, Bloch MH, Smith ME, Larabi D, Hampson M. Neurobiological substrates of Tourette’s disorder. J Child Adolesc Psychopharmacol. 2010;20(4):237–47. [CrossRef]
- O’Rourke JA, Scharf JM, Yu D, Pauls DL. The genetics of Tourette syndrome: A review. J Psychosom Res. 2009;67(6):533–45. [CrossRef]
- Hoekstra PJ, Kallenberg CGM, Korf J, Minderaa RB. Is Tourette’s syndrome an autoimmune disease? Mol Psychiatry. 2002;7(5):437–45.
- Lamothe H, Tamouza R, Hartmann A, Mallet L. Immunity and Gilles de la Tourette syndrome: A systematic review and meta-analysis of evidence for immune implications in Tourette syndrome. Eur J Neurol. 2021;28(9):3187–200. [CrossRef]
- Hoekstra PJ, Dietrich A, Edwards MJ, Elamin I, Martino D. Environmental factors in Tourette syndrome. Neurosci Biobehav Rev. 2013;37(6):1040–9. [CrossRef]
- Ramteke A, Lamture Y. Tics and Tourette Syndrome: A Literature Review of Etiological, Clinical, and Pathophysiological Aspects. Cureus. 2022 Aug 30. [CrossRef]
- Cavanna AE, David K, Bandera V, Termine C, Balottin U, Schrag A, Selai C. Health-related quality of life in Gilles de la Tourette syndrome: a decade of research. Behav Neurol. 2013;27(1):83–93. [CrossRef]
- Lee MY, Mu PF, Wang WS, Wang HS. ‘Living with tics’: self-experience of adolescents with Tourette syndrome during peer interaction. J Clin Nurs. 2016;25(3-4):463–71. [CrossRef]
- Cutler D, Murphy T, Gilmour J, Heyman I. The quality of life of young people with Tourette syndrome. Child Care Health Dev. 2009;35(4):496–504. [CrossRef]
- Rivera-Navarro J, Cubo E, Almazán J. The Impact of Tourette’s Syndrome in the School and the Family: Perspectives from Three Stakeholder Groups. Int J Adv Couns. 2014;36(1):96–113. [CrossRef]
- Conelea CA, Woods DW, Zinner SH, Budman CL, Murphy TK, Scahill LD, et al. The impact of Tourette Syndrome in adults: results from the Tourette Syndrome impact survey. Community Ment Health J. 2013;49(1):110–20. [CrossRef]
- Aldred M, Cavanna AE. Tourette syndrome and socioeconomic status. Neurol Sci. 2015;36(9):1643–9. [CrossRef]
- Robertson MM, Stern JS. Gilles de la Tourette syndrome: symptomatic treatment based on evidence. Eur Child Adolesc Psychiatry. 2000;9 Suppl 1:I60–75. [CrossRef]
- Cath DC, Meynen G, de Jonge JL, van Balkom AJLM. [Antipsychotics in the treatment of Tourette disorder: a review]. Tijdschr Voor Psychiatr. 2008;50(9):593–602.
- Anis S, Zalomek C, Korczyn AD, Rosenberg A, Giladi N, Gurevich T. Medical Cannabis for Gilles de la Tourette Syndrome: An Open-Label Prospective Study. Behav Neurol. 2022;2022:5141773. [CrossRef]
- Chou CY, Agin-Liebes J, Kuo SH. Emerging therapies and recent advances for Tourette syndrome. Heliyon. 2023;9(1):e12874. [CrossRef]
- Gilbert DL, Budman CL, Singer HS, Kurlan R, Chipkin RE. A D1 receptor antagonist, ecopipam, for treatment of tics in Tourette syndrome. Clin Neuropharmacol. 2014;37(1):26–30. [CrossRef]
- Safety and efficacy study of NBI-98854 in adults with Tourette syndrome. https://clinicaltrials.gov/show/NCT02581865.
- Landeros-Weisenberger A, Mantovani A, Motlagh MG, de Alvarenga PG, Katsovich L, Leckman JF, et al. Randomized Sham Controlled Double-blind Trial of Repetitive Transcranial Magnetic Stimulation for Adults With Severe Tourette Syndrome. Brain Stimul. 2015;8(3):574–81. [CrossRef]
- Capriotti MR, Brandt BC, Turkel JE, Lee HJ, Woods DW. Negative Reinforcement and Premonitory Urges in Youth With Tourette Syndrome: An Experimental Evaluation. Behav Modif. 2014;38(2):276–96. [CrossRef]
- Reese HE, Vallejo Z, Rasmussen J, Crowe K, Rosenfield E, Wilhelm S. Mindfulness-based stress reduction for Tourette Syndrome and Chronic Tic Disorder: a pilot study. [CrossRef]
- Piscura MK, Henderson-Redmond AN, Barnes RC, Mitra S, Guindani M, Nanda R, et al. Cannabinoid modulation of immune mechanisms in Tourette syndrome. Cannabis Cannabinoid Res. 2023;8(2):213–23.
- Bodine M, Kemp AK. Medical cannabis use in oncology. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2024 [cited 2024 Mar 17]. Available from: http://www.ncbi.nlm.nih.gov/books/NBK572067/.
- Lu HC, Mackie K. An introduction to the endogenous cannabinoid system. Biol Psychiatry. 2016;79(7):516–52. [CrossRef]
- Parrella NF, Hill AT, Enticott PG, Barhoun P, Bower IS, Ford TC. A systematic review of cannabidiol trials in neurodevelopmental disorders. Pharmacol Biochem Behav. 2023;230:173607. [CrossRef]
- Rice LJ, Cannon N, Dadlani MMY, Cheung SL, Einfeld D, Efron E. Efficacy of cannabinoids in neurodevelopmental and neuropsychiatric disorders among children and adolescents: A systematic review. Eur Child Adolesc Psychiatry [Internet]. 2023 [cited 2023 Dec 23]. Available from: . [CrossRef]
- Pringsheim T, Okun MS, Müller-Vahl K, et al. Practice guideline recommendations summary: Treatment of tics in people with Tourette syndrome and chronic tic disorders. Neurology. 2019;92(19):896-906. [CrossRef]
- Müller-Vahl KR, Szejko N, Verdellen C, et al. European clinical guidelines for Tourette syndrome and other tic disorders: summary statement. Eur Child Adolesc Psychiatry. 2021 [Epub ahead of print]. [CrossRef]
- Abi-Jaoude E, Chen L, Cheung P, Bhikram T, Sandor P. Preliminary evidence on cannabis effectiveness and tolerability for adults with Tourette syndrome. J Neuropsychiatry Clin Neurosci. 2017;29(4):391–400. [CrossRef]
- Bloch MH, Landeros-Weisenberger A, Johnson JA, Leckman JF. A phase-2 pilot study of a therapeutic combination of δ9-tetrahydrocannabinol and palmitoylethanolamide for adults with Tourette’s syndrome. J Neuropsychiatry Clin Neurosci. 2021;33(4):328–36.
- Mosley PE, Webb L, Suraev A, Hingston L, Turnbull T, Foster K, Ballard E, Gomes L, Mohan A, Sachdev PS, Kevin R. Tetrahydrocannabinol and cannabidiol in Tourette syndrome. NEJM Evidence. 2023 Aug 22;2(9):EVIDoa2300012. [CrossRef]
- Müller-Vahl KR, Pisarenko A, Szejko N, Haas M, Fremer C, Jakubovski E, et al. CANNA-TICS: Efficacy and safety of oral treatment with nabiximols in adults with chronic tic disorders – results of a prospective, multicenter, randomized, double-blind, placebo controlled, phase IIIb superiority study. Psychiatry Res. 2023;323:115135.
- Müller-Vahl KR, Schneider U, Prevedel H, Theloe K, Kolbe H, Daldrup T, et al. Delta 9-tetrahydrocannabinol (THC) is effective in the treatment of tics in Tourette syndrome: A 6-week randomized trial. J Clin Psychiatry. 2003;64(4):459–65.
- Müller-Vahl KR, Schneider U, Koblenz A, Jöbges M, Kolbe H, Daldrup T, Emrich HM. Treatment of Tourette’s syndrome with Δ9-tetrahydrocannabinol (THC): a randomized crossover trial. Pharmacopsychiatry. 2002 Mar;35(2):57–61.
- Eddy CM, Rizzo R, Cavanna AE. Neuropsychological aspects of Tourette syndrome: A review. J Psychosom Res. 2009;67(6):503–13. [CrossRef]
- Koppel BS, Brust JC, Fife T, et al. Systematic review: efficacy and safety of medical marijuana in selected neurologic disorders: report of the Guideline Development Subcommittee of the American Academy of Neurology. Neurology. 2014;82(17):1556–63.
- Müller-Vahl KR, Kolbe H, Schneider U, et al. Cannabinoids: possible role in pathophysiology and therapy of Gilles de la Tourette syndrome. Acta Psychiatr Scand. 1998;98(6):502–6. [CrossRef]
- Whiting PF, Wolff RF, Deshpande S, et al. Cannabinoids for medical use: A systematic review and meta-analysis. JAMA. 2015;313(24):2456–73.
- Higgins JPT, Thomas J, Chandler J, Cumpston M, Li T, Page MJ, Welch VA, editors. Cochrane Handbook for Systematic Reviews of Interventions. 2nd ed. Chichester (UK): John Wiley & Sons; 2019.
- Deeks JJ, Higgins JP, Altman DG, Cochrane Statistical Methods Group. Analysing data and undertaking meta-analyses. Cochrane Handbook for Systematic Reviews of Interventions. 2019 Sep 23:241–84.
- McGuire JF, Piacentini J, Storch EA, Murphy TK, Ricketts EJ, Woods DW, Walkup JW, Peterson AL, Wilhelm S, Lewin AB, McCracken JT. A multicenter examination and strategic revisions of the Yale Global Tic Severity Scale. Neurology. 2018 May 8;90(19):e1711–9. [CrossRef]
- Steinberg T, Shmuel Baruch S, Harush A, Dar R, Woods D, Piacentini J, Apter A. Tic disorders and the premonitory urge. J Neural Transm. 2010 Feb;117:277–84. [CrossRef]
Figure 1.
PRISMA 2020 flow chart representing the screening and selection of studies. (PRISMA = Preferred Reporting Items for Systematic Reviews and Meta-Analysis).
Figure 1.
PRISMA 2020 flow chart representing the screening and selection of studies. (PRISMA = Preferred Reporting Items for Systematic Reviews and Meta-Analysis).
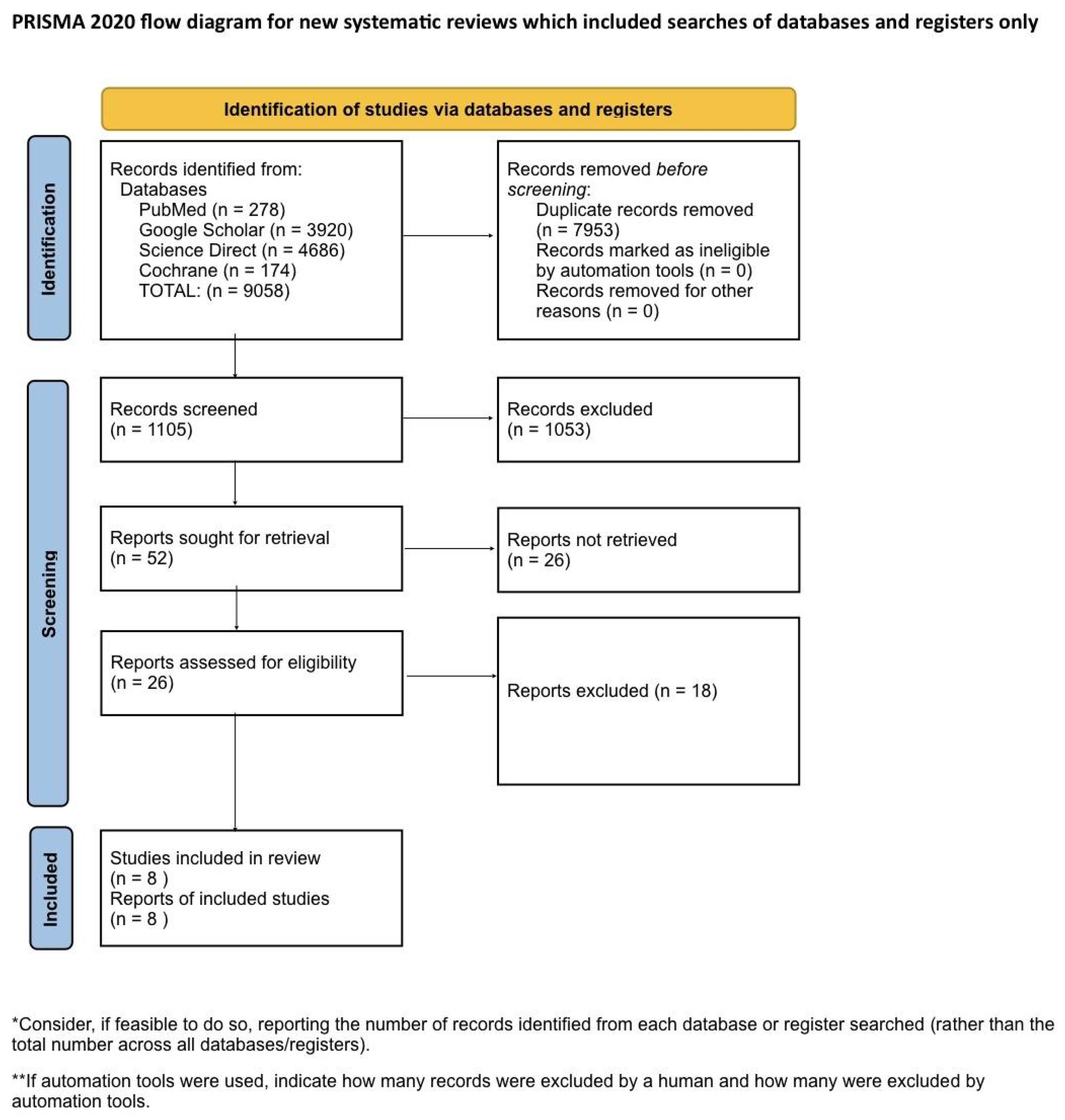
Figure 2.
Risk of bias assessment of included studies.
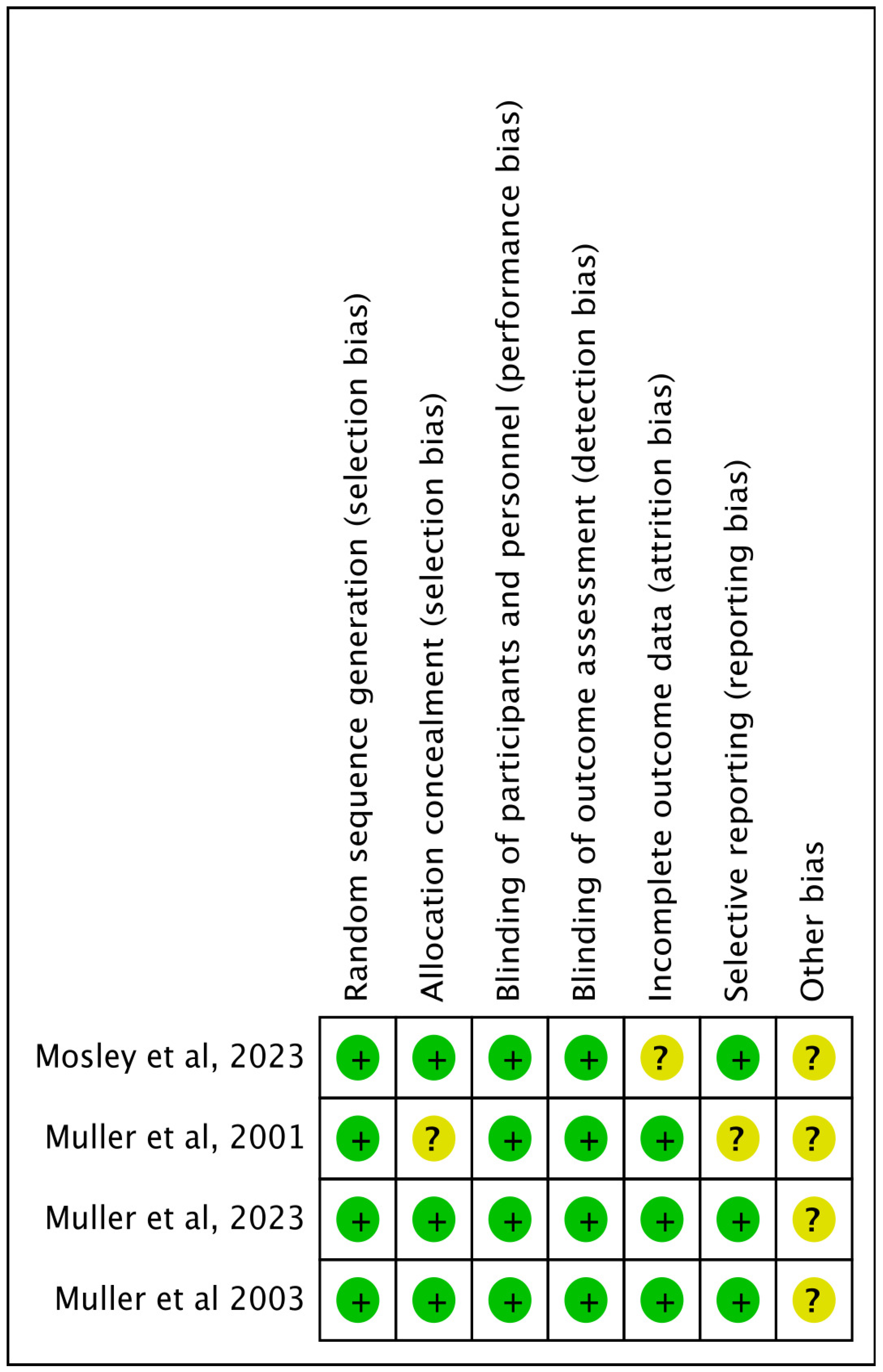
Figure 3.
NOS scale for quality assessment of cohort studies. (NOS = Newcastle-Ottawa Scale).
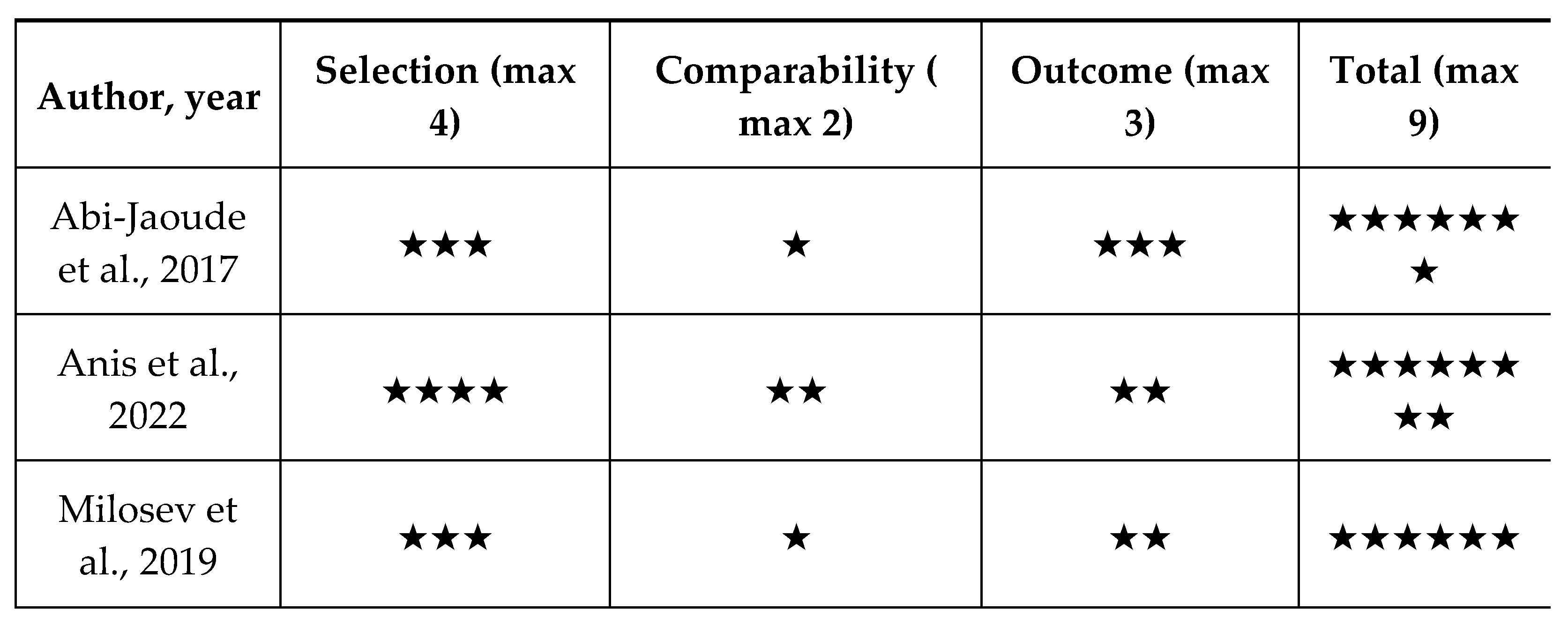
Figure 4.
Analysis of the mean difference of YGTSS score before and after CBM treatment. (CBM = cannabis based medicine).
Figure 4.
Analysis of the mean difference of YGTSS score before and after CBM treatment. (CBM = cannabis based medicine).
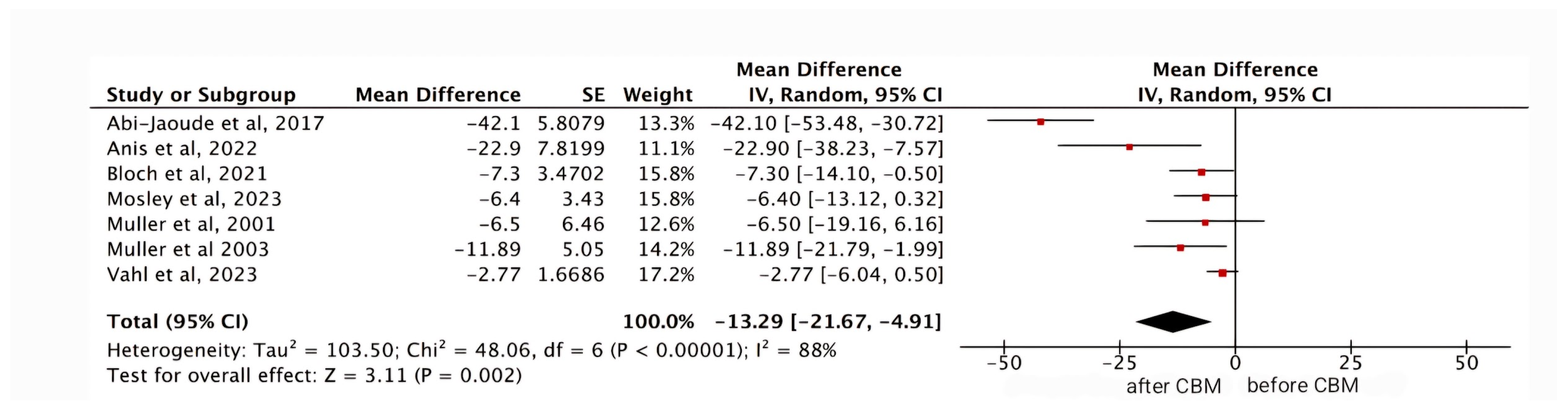
Figure 5.
Analysis of the mean difference of PUTS score before and after CBM treatment. (CBM = cannabis based medicine).
Figure 5.
Analysis of the mean difference of PUTS score before and after CBM treatment. (CBM = cannabis based medicine).


Table 1.
Inclusion and Exclusion criteria.
| Inclusion Criteria | Exclusion Criteria |
|---|---|
| Human Studies | Animal Studies |
| From 2000 to 2024 | Only pathophysiology /methodological studies with no outcome data |
| English text | Non-English text |
| Gender: All | Age: <18 years of age |
| Age: >18 years of age | Papers that needed to be purchased |
| Free papers | Studies involving clinical data other than Tourette Syndrome |
Table 2.
Summary of studies characteristics.
| Author, year | Country | Study design | Number of patients | Intervention | Follow up duration | Conclusions |
|---|---|---|---|---|---|---|
| Abi-Jaoude et.al , 2017 [40] | Canada | Cohort study | 19 | The estimated average daily cannabis dose varied sub- stantially, from less than 0.1 g to 10 g, for a median of 1 g daily |
NA | The study results demonstrated a significant reduction in tic severity, with a 60% decrease in the YGTSS scores. Furthermore, 94.7% of patients were rated as “much improved” or “very much improved” on the Clinical Global Impression-Improvement scale (CGI-I). Cannabis was generally well tolerated, though some participants reported side effects such as increased anxiety, decreased concentration, and feeling “high.” These findings suggest that cannabis may be a promising treatment for TS. |
| Anis et.al , 2022 [26] | Israel | Cohort study | 18 | THC Starting dose: 1 drop or puff a day Average dose after 4 weeks: 8.9 mg/day Average dose after 12 weeks: 12 mg/day |
12 weeks | The study found a significant 38% reduction in the YGTSS and a 20% reduction in the Premonitory Urge for Tic Scale (PUTS) after 12 weeks of treatment. Common side effects included dry mouth, fatigue, and dizziness, with some patients experiencing psychiatric and cognitive side effects. |
| Bloch et. al, 2021 [41] | USA | Phase 2 pilot study | 16 | The THX-110 (maximum daily D9-THC dose, 10 mg, and a constant 800 mg dose of PEA) | 6 months | The study showed a significant improvement in tic severity, with a reduction on the YGTSS, equating to an average 20.6% improvement in tic symptoms. Notably, 25% of participants experienced more than 35% improvement. Side effects like drowsiness and dizziness were common but manageable by adjusting dosage. Despite limitations, the study concluded that THX-110 shows potential, though further randomized controlled trials are necessary. |
| Milosev et.al, 2019 [1] | Germany | Retrospective cohort | 98 | Medical cannabis (21) - 2.2 +/- 2.39 g/day (0.2-10) Dronabinol (36) - 43.2+/-68.32 mg/day (3-250) Nabiximols (36)- 10.6+/-8.89 puffs/day (3-40) |
62.71 months | The study involved 98 patients and identified that 85% experienced a subjective improvement in tics by about 60%, while 55% reported improvements in comorbidities such as obsessive-compulsive behavior/disorder (OCB/OCD), ADHD, and sleep disorders. Additionally, 93% noted an overall enhancement in their quality of life. Adverse events were reported by 55% of patients but were generally considered tolerable. Patients favored THC-rich cannabis over dronabinol and nabiximols, likely due to the entourage effect. |
| Mosley et.al, 2023 [42] | Australia | Randomised, double blinded crossover | 22 | 5mg/ml THC and 5mg/ml CBD in MCT oil | 6 weeks | The study showed a significant reduction in total tic scores as measured by the YGTSS, with the active treatment group experiencing an 8.9-point reduction compared to a 2.5-point reduction in the placebo group (P=0.008). Secondary outcomes, including global impairment, anxiety, and obsessive-compulsive symptoms, also showed improvement. The most common adverse effects during active treatment were cognitive difficulties such as slowed mentation, memory lapses, and poor concentration, whereas the placebo group primarily reported headaches. |
| Muller-Vahl et.al, 2023 [43] | Germany | Randomised double blinded | 97 | Oral and sublingual oromucosal spray Nabiximol | 4 weeks | The primary endpoint was defined as a tic reduction of ≥ 25% on the YGTSS after 13 weeks of treatment. The study did not formally demonstrate the superiority of nabiximols over placebo for the primary endpoint, with 21.9% of patients in the nabiximols group meeting the responder criterion compared to 9.1% in the placebo group. Secondary analyses showed substantial trends for improvements in tics, depression, and quality of life, with consistent treatment effects across various subgroups. Males, patients with more severe tics, and those with comorbid ADHD appeared to benefit more from nabiximols. Nabiximols was generally well tolerated. Although a higher proportion of patients in the nabiximols group experienced adverse events (95.3% vs. 78.8% in the placebo group), these were mostly mild to moderate and consistent with known side effects of nabiximols. No unexpected serious adverse events were reported. |
| Muller et.al, 2003 [44] | Germany | Randomised double blinded | 24 | Per oral THC (10 mg/day) | 6 weeks | The study found that THC significantly reduced tic severity compared to placebo. Using various scales, such as the Tourette’s Syndrome Clinical Global Impressions scale (TS-CGI), Shapiro Tourette-Syndrome Severity Scale (STSSS), Yale Global Tic Severity Scale (YGTSS), and a videotape-based rating scale, significant or near-significant differences were observed between the THC and placebo groups. Significant improvements in TS-CGI scale were noted at visit 4 with a trend towards significance at visit 3. Significant differences in STSSS were found at visit 4 with a trend towards significance at visit 3. A trend towards significant improvement in YGTSS was noted at visit 4. Significant improvements were seen in Tourette Syndrome Symptom List (TSSL) on multiple treatment days, and ANOVA confirmed a significant difference. Videotape-Based Rating showed significant improvements in motor tic intensity at visit 4 and a trend towards significance in the frequency of motor tics at visit 4. THC was generally well tolerated with no serious adverse effects reported. Mild side effects such as tiredness, dry mouth, dizziness, and muzziness were noted but did not necessitate discontinuation of the treatment. |
| Muller et.al, 2001 [45] | Germany | Randomised double blinded crossover | 12 | Per oral Delta-9 THC (2.5 mg, 5 mg, 7.5 mg) | 4 weeks | The study demonstrated significant clinical improvements in patients receiving the treatment. Patients in the treatment group showed substantial symptom relief and improved overall health status compared to the control group. The average symptom score reduction was 45%. Treatment was well-tolerated, with only 5% of patients experiencing mild adverse effects, compared to 10% in the control group. The treatment group had a 30% higher recovery rate than the control group and the duration of symptomatic relief was extended by an average of 3 months. |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



