Submitted:
17 September 2024
Posted:
17 September 2024
You are already at the latest version
Abstract
Background: The COVID-19 pandemic led to rapid growth in telemental health services and investment in digital mental health technologies. Digital mental health technologies could expand access to mental health care amid increasing provider deficit by providing tools for expedited psychiatric symptom assessment and treatment augmentation. This systematic review explores the recent evidence for the use of scalable digital tools, including virtual reality, neurofeedback training, wearables, mobile apps, digital phenotyping, and machine learning for PTSD symptom assessment, diagnosis, and treatment. Methods: A PubMed search identified studies on digital technologies with current or future potential for scalability (accessible through a small, digital device without the virtual or in-person presence of a mental health care provider)–and PTSD diagnosis, symptom assessment, or symptom treatment as the primary outcome. Thirty-five studies inform this review. Results: Virtual reality exposure therapy is efficacious for combat-related PTSD treatment. Conclusions of studies investigating apps and neurofeedback training are limited by low sample size and methodological heterogeneity. Machine learning models demonstrate capability in detecting PTSD symptoms via passively collected data from smartphones, wearables, and actively collected data from patient speech, writing, and videos, but standardization of data collection and modeling are needed before application to clinical settings. Conclusions: Advancements in scalable digital tools could address barriers in healthcare access and improve patient engagement by providing asynchronous assessment and treatment augmentation. Future research utilizing diverse patient populations in standardized controlled trials is needed to determine evidence-based protocols for implementation.
Keywords:
digital health
; mental health
; PTSD
; virtual reality
; digital phenotyping
Introduction
Posttraumatic stress disorder (PTSD) is a psychiatric disorder characterized by chronic intrusive memories, hyperarousal, disrupted emotion regulation, depressed mood, and autonomic dysfunction following exposure to a traumatic event (American Psychiatric Association, 2013). Up to 90% of the urban U.S. population is exposed to trauma at some point in their lives, and the lifetime prevalence of developing PTSD is nearly 9% (Kilpatrick et al., 2013; Kessler et al., 2005). Globally, the rate of PTSD varies, with countries affected by war and of low socio-economic status showing considerably higher rates (Koenen et al., 2017). Current treatment guidelines for PTSD endorse pharmacotherapy with selective serotonin reuptake inhibitors (SSRIs) or selective norepinephrine inhibitors (SNRIs) in conjunction with trauma-focused exposure therapy or cognitive behavioral therapy (Martin et al., 2021; Department of Veterans Affairs & Department of Defense, 2023). However, only a minority of patients experience long-term remission of their symptoms (Watkins et al., 2018). These approaches may also be particularly limited for treating veterans and patients with chronic PTSD (Forbes et al., 2019; Watts et al., 2013). Although psychotherapy methods utilizing a trauma-oriented approach are effective for treating PTSD (Watts et al., 2013; Bisson et al., 2013; Orr et al., 2002; Lee et al., 2016; Jericho et al., 2022), these practices require an extensive amount of training on behalf of the provider. Given the regional disparities in access to trained mental health professionals in the U.S. and globally, many patients are unable to receive an effective amount or method of trauma-focused therapy (Adrilla et al., 2018; Keynejad et al., 2018, Kazdin et al., 2011; Cully et al., 2010). The pandemic-driven growth of remote telemental health services has helped ameliorate these geographic barriers for some patient populations (Di Carlo et al., 2021; Jones et al., 2020), as teletherapy has been shown to be as efficacious as in-person services for treating depression, anxiety, and PTSD (Giovanetti et al., 2022; Acierno et al., 2021; de Oliveira et al., 2023). Indeed, due to the complex nature of PTSD and its limited response to current treatments, more frequent and intensive therapy sessions may best improve treatment responses (Hendriks et al., 2018). However, increasing the frequency of teletherapy is not feasible considering the growing shortage of mental health providers (Satiani et al., 2018). Consequently, it is imperative to optimize the distribution of healthcare resources and enhance the efficacy of current therapeutic approaches. One potential solution is through leveraging the increasing capabilities of digital technology.
The ubiquity of smartphones and advancements in digital technology, including wearables and artificial intelligence (AI), pave the way for innovative automated diagnostic approaches. Digital phenotyping techniques allow for an automated, non-intrusive evaluation of patient symptoms during their day-to-day lives through measuring patterns in data collected from smartphones and wearables to create a digital signature (Torous et al., 2017; Reinersten et al., 2018; Sheikh et al., 2021). Several models have used this approach to accurately predict the presence of mood disorders (Jacobsen et al., 2019), suicidal thoughts (Kleiman et al., 2018), and relapses in substance use (Hsu et al., 2020) and psychosis (Barnett et al., 2018). Additionally, these data streams can be combined with “active” data collection, prompting patient engagement through written, vocal, or video inputs (Bedi et al., 2015; Kamath et al., 2022). Ultimately, these innovations could offer healthcare professionals the capacity to enhance diagnostic precision, evaluate a large number of patients, and intervene in a timely manner (Le Glaz et al., 2021).
Other scalable digital tools, such as virtual reality (VR), mobile apps, and neurofeedback training (NFT) could offer innovative approaches to PTSD treatment augmentation in a patient-directed manner. VR and augmented reality (AR) therapies can supplement or replace prolonged exposure (PE) therapy by immersing the user into a customizable, interactive three-dimensional environment. These immersive environments can integrate realistic elements of a patient’s traumatic experience that would otherwise be difficult or unsafe for extinction training, making this technology particularly suitable for veterans with combat-related trauma. Indeed, past reviews have suggested comparable efficacy to PE for this patient population (Kothgassner et al., 2019; Eshuis et al., 2020). With adequate oversight and patient training, virtual reality exposure therapy (VRET) could be completed at home and without the presence of a mental health service provider (Jones et al., 2020; Goreis et al., 2020). Meanwhile, mobile apps require little to no training to use and are a low-cost way to widely distribute psychoeducation, teach self-guided psychological exercises, and disseminate wellness surveys. Recent research shows promise in their potential for these tools to help reduce symptoms of depressive, anxiety, and pain (Torous et al., 2021; Ioannou et al., 2020). Other approaches, such as NFT, have seen limited use outside of research settings, but may soon be more widely available with decreasing costs and increasing capabilities of at-home electroencephalograph (EEG) headsets. NFT involves detecting an individual’s EEG activity while they attempt to endogenously produce a predetermined brain rhythm. When this rhythm is achieved, the user’s behavior is reinforced with a visual, auditory, or game stimulus. Consistent training of particular brain states and metacognitive skills has been shown to modulate autonomic arousal, and therefore, may be useful as an auxiliary tool for PTSD intervention (Marzbani et al., 2016).
How these technologies can be best implemented in clinical practice remains to be determined; however, they present a unique opportunity to provide patients with self-directed therapy, to limit provider burden, and to enhance efficacy of mid-level providers. While the application of the aforementioned technologies in mental health (Torous et al., 2021) and PTSD have been reviewed in other contexts (Bourla et al., 2018; Wu et al., 2023; Meyerbröker et al., 2021; Morland et al., 2020; Ramos-Lima et al., 2020; Wickersham et al., 2019), these reviews highlighted a single tool (Wu et al., 2023; Meyerbröker et al., 2021; Morland et al., 2020; Wickersham et al., 2019), require updating (Bourla et al., 2018), or did not focus on scalable digital tools specifically (Wu et al., 2023; Morland et al., 2020; Ramos-Lima et al., 2020). In this paper, we present a review of recent findings of scalable digital tools, encompassing digital phenotyping, wearable devices, natural language processing, facial feature detection, virtual and augmented reality, neurofeedback training, and mobile apps in their current capacities for predicting PTSD diagnosis, monitoring symptoms, and augmenting treatment. We discuss the evolving landscape of digital technology and the requisites for applying scalable tools to clinical practice.

Table 1.
Definitions of selected scalable digital technologies.
| Selected Technology | Definition |
| Digital Phenotyping | Mobile phone data, such as the number and length of calls and texts, accelerometry, GPS, and voice quality, can be used in conjunction with machine learning algorithms to predict, differentiate, and track mental illness. |
| Wearables | Devices that measure skin conductance, EKG, heart-rate, heart-rate variability, and EEG to detect changes in respiration, cardiac activity, and circadian rhythm. These data can be used to provide information about an individual’s autonomic function, a potentially useful indicator for PTSD severity and treatment outcomes. |
| Natural language processing (NLP) and Facial detection | AI-assisted analysis of the tone, content, quality, and sophistication of patient speech and writing can be used to identify different mood states, detect presence of psychiatric symptoms, and predict future behavior. Facial recognition can also detect facial valence and mood state in response to questions or emotional stimuli to predict diagnostic status and symptom severity. |
| Immersive technologies (VR, AR, 3DMR) | Use of an immersive head-mounted display (HMD), 180-degree monitors, or projection goggles can aid extinction training by recreating virtual environments and/or projecting virtual objects relevant to a patient’s traumatic experience onto the real-life environment. Can be used in conjunction with a treadmill (3MDR) or with other sensory information to increase environmental immersion and reduce avoidance behaviors. |
| Neurofeedback Training | EEG, when used with a computer interface, can provide real-time data of patient brain activity. Patients can learn to modulate their brain activity in response to stimuli presented through the computer interface when targeted brain rhythms are achieved. |
| Apps | Mobile platforms accessed via smartphone that screen for psychiatric symptoms, provide psychoeducation, coping strategies, CBT, and additional treatment resources. |
Table 2.
Summary of studies included in review. Summary of 35 studies on scalable digital technologies for the assessment and treatment of PTSD published 2017-2022.
Table 2.
Summary of studies included in review. Summary of 35 studies on scalable digital technologies for the assessment and treatment of PTSD published 2017-2022.
| Study | Technology | Purpose | Sample Demographic | Method | Findings | Notes |
| Natural Language Processing (NLP) and Facial Feature Interpretation | ||||||
| [Schultebraucks et al. (2022)] | Voice and audio feature extraction with ML | PTSD and MDD diagnostic prediction post-trauma | 81 patients admitted to an emergency department of a Level-1 Trauma Unit following a life-threatening traumatic event | The audio and video of the patient responses to five open-ended questions acted as an input for a deep neural network which was trained to extract facial features of emotion and their intensity, speech prosody, movement parameters, and natural language content. | The algorithm was able to predict a CAPS-5 PTSD diagnosis with an AUC of .90 as well as depression status with an AUC of .86 | |
| [Marmar et al. (2019)] | Speech extraction with ML | PTSD detection from recordings of clinical interviews (with clinical psychologist) | Warzone veterans—52 with PTSD and 77 without | RF algorithm to predict PTSD presence based on speech features in clinical interviews | AUC of .954 and classification accuracy of 89.1%. Probability of PTSD was higher for markers that indicated slower, more monotonous speech, less change in tonality, and less activation | |
| [Gavrilescu et al. (2019)] | Facial microexpression detection with ML | PTSD, anxiety, depression detection | 128 caucasian, half male. 20 with MDD, 19 GAD, 17 PTSD | Multi-layered ML algorithm used to predict presence of PTSD, MDD, or anxiety through analyzing facial features while subjects watched emotion-inducing or emotion-neutral videos | The model was able to discriminate with 93% accuracy between healthy subjects and those affected by Major Depressive Disorder (MDD) or Post-traumatic Stress Disorder (PTSD), and 85% for Generalized Anxiety Disorder (GAD) | |
| [He et al. (2017)] | Natural language processing | PTSD detection from patient narratives | 300 Veterans- half with diagnosed PTSD | Used NLP and text mining using “N-gram” features approach on patient writing narratives to predict likelihood of PTSD diagnosis | AUCs of the four text classifiers—DT, NB, SVM, and PSM—were .68, .90, .86 and .94 respectively | N-gram features count the number of co-occurring words within a given window of word. DT: decision tree; NB: naive Bayes; SVM: support vector machine; PSM: product score model |
| [He et al. (2019)] | Natural language processing | PTSD detection from patient narratives and online-survey responses | 99 trauma survivors, 34 with a self-reported PTSD diagnosis and 65 without PTSD | Used PSM model on patient writing narratives alone or in conjunction with responses to a 21-question online-survey to predict presence of PTSD diagnosis | Analysis of patient text-responses alone yielded an accuracy of 84%, and a sensitivity of 100% while combining online survey responses with Bayesian modeling increased accuracy to 97%. | |
| [Sawalha et al. (2022)] | Natural language processing | PTSD detection from interview transcripts | 188 individuals with PTSD, 87 without. Used text data from a popular dataset, the Audio/Visual Emotion Challenge and Workshop [(AVEC 2019)] (23) | Sentiment text analysis (sub-branch of NLP) gathered from computer conducted semi-structured interview to detect PTSD | Achieved highest mean accuracy rate of 80.4%, with an AUC of .80 and an F1 score of .85 and .72 for the non-PTSD and PTSD groups, respectively. | |
| Digital phenotyping | ||||||
| [Place et al. (2017)] | Digital phenotyping using smartphone | PTSD and depression symptom prediction | 73 participants (67% male, 33% veterans) who reported at least one symptom of PTSD or depression on the Primary Care PTSD Screen (PC-PTSD) or the Patient Health Questionnaire (PHQ-2) | Participants were given an Android device to use as their normal phone. A mobile app app gathered data on messaging, outgoing calls, location, device use, speaking rate, and voice quality during normal phone use in addition to weekly voicemail diary entries for a period of 12 weeks. | Fatigue, interest in activities, and social connectedness were predicted using LASSO regression trained on data (GPS, messages sent, outgoing calls) from the prior week with AUCs of .56, .75, and .83 respectively. Depressed mood was predicted from audio data with an AUC of .74 | |
| [Friedman et al. (2020)] | Digital phenotyping using smartphone | PTSD diagnostic prediction | 228 Females, 150 with PTSD+emotional instability and history of child abuse, 35 healthy trauma controls with child abuse history, and 45 healthy controls | Passively-collected smartphone-based GPS data of distance travelled from home over a period of seven days | Average time away from home and distance traveled from home did not correlate with avoidance symptoms (PCL5-7 item). Both trauma-exposed groups stayed closer to their homes on weekends when compared to controls (PTSD: b = -0.618, p = .004; HTC: b = − 0.593, p = .032), with only the PTSD group differing significantly from controls on weekdays (b = − 0.340, p = .048). Including covariates for depression and health status dropped this relationship out of significance |
|
| [Lekkas and Jacobson (2021)] | Digital phenotyping using smartphone | PTSD diagnostic prediction | 185 females, 150 with PTSD and 35 healthy trauma controls (same as above, but without healthy control group) | Used leave one subject out (LOSO) and k-fold cross-validation on GPS data tracking daily time spent away from home and maximum distance travelled from home to predict PTSD diagnostic likelihood using data from Friedman et al., 2020 | Diagnostic group status predicted with an AUC = .816, sensitivity = .743, specificity = .8, and an accuracy = .771. | |
| Wearables | ||||||
| [Hinrichs et al. (2017)] | Mobile skin conductance | PTSD diagnostic prediction | 63 trauma-exposed patients in the emergency department (51% male, 76% Black). Motor vehicle accident was most commonly reported trauma (65.1%) | Feasibility study for measuring skin conductance (SC) via mobile device (eSense) in emergency department patients who had experienced a trauma approximately 1 year before | Individuals with PTSD showed significantly greater SCR than individuals without PTSD during trauma interview (P = .006). The AUC for the ROC curve analysis for SCR on PTSD diagnosis was 0.79 (p = .001). SCR during trauma interview also correlated positively with PTSD symptom total score on the PSS(b = 0.42, p = .001). | SCR: Skin Conductance Reactivity, PSS: PTSD Symptom Scale |
| [Hinrichs et al. (2019)] | Mobile skin conductance | PTSD diagnostic prediction | 107 trauma-exposed patients in the emergency department (56% male, 82% Black). Motor vehicle accident was the most commonly reported trauma (59%) | Used mobile SC (eSense) to predict the future incidence of PTSD in emergency department patients who had experienced a trauma within the past 12 hours. Used a series latent growth mixture modeling (LGMM) to classify participants into future PTSD symptom trajectories | SCR during trauma interview was significantly correlated with the probability of being in the chronic PTSD trajectory (r = 0.489, p < 0.000001; AUC = .90), with SCR being the most significant predictor of the chronic PTSD trajectory (p < 0.00001) when controlling for demographic and clinical measures. | |
| [Wiltshire et al. (2022)] | Mobile skin conductance | PTSD symptom assessment | 62 trauma-exposed children (54% male, 79% black, average age 9.11, SD = 0.37) | Measured SC using eSense in trauma-exposed children during a standardized trauma interview | Degree of trauma exposure was significantly correlated with SCR (i.e., change in SCL from baseline to maximum SCL) during the TESI-C interview (r(55) = 0.30, p = .023, ) trauma exposure alone significantly predicted SCR after controlling for other variables, R2change = 0.129, F (1,50)change = 8.31, p = .006. Hyperarousal symptoms predict SCL habituation r2 = .05, F(1,48) change = 4.31, p = .043 | SCL habituation is difference between maximum SC and end of interview SC. |
| [Grasser et al. (2022)] | Mobile skin conductance | PTSD symptom assessment | 86 refugee youth (aged 7-17, 41.8% male, all Arab) with an average of 4 traumatic experiences | Measured SC using eSense in trauma-exposed children during a standardized trauma interview | Trauma exposure was significantly associated with SCR during trauma interview (R2 = .084, p = .042). SCR during trauma interview was positively correlated with reexperiencing (R2 = .127, p = .028), and hyperarousal symptoms (R2 = .123, p = .048) | |
| [Cakmak et al. (2021)] | Wrist-worn sensor | PTSD diagnostic prediction | 1618 emergency department patients with recent (<72hour) trauma-exposure (36% male) | Collected survey and HRV data from ED patients recently exposed to trauma and used these data with a machine learning model (SVM log regression, Multilayer perceptron) to detect PTSD diagnostic status in the 8 weeks following trauma | AUC of .74 in predicting PTSD at 8wk using survey, only .54 with HRV, and .73 when combining survey and HRV | |
| [Tsanas et al. (2020)] | Wrist-worn sensor | PTSD symptom tracking | 42 participants with PTSD (38% male), 43 traumatized controls, and 30 healthy controls. | Wrist-worn sensor detecting actigraphy, light, and temperature data over 7 days | Participants with PTSD showed more fragmented sleep patterns and greater intraday variability compared with traumatized and healthy control groups, showing statistically significant (p < .05) and strong associations (|R| > 0.3). | |
| [Reinersten et al. (2017)] | Ambulatory ECG (Holter) monitor | PTSD diagnostic prediction | 24 male veterans with clinical diagnosis of PTSD and 25 healthy controls | Detected heart rate variability (HRV) features (statistical moments, power spectral density components, entropy, and acceleration / deceleration capacity) using a 24-hour Holter monitor to create a machine learning model for predicting PTSD diagnostic status | Using logistic regression models on an out-of-sample test set data yielded an AUC of 0.86 for detecting PTSD diagnostic status. 24-hours of data from sample yielded AUC of 0.72 and random segments resulted in AUC of .67 | |
| [Sadeghi et al. (2022)] | Smartwatch | PTSD symptom detection | 99 veterans with PTSD diagnosis (83% male) | Used a smartwatch-based app to collect data related to heart rate, body acceleration, and self-reported hyperarousal events over several days to create machine learning models for predicting onset of PTSD hyperarousal events | Of several machine learning algorithms (Random Forest, Support Vector Machine, Logistic Regression and XGBoost), XGBoost had the best performance in detecting onset of PTSD symptoms with 83% accuracy and an AUC of 0.70, where average heart rate, minimum heart rate and average body acceleration were the greatest predictors. | Model was trained on a subset of the sample (70%) and tested on the remaining participants (30%). |
| Immersive Technologies | ||||||
| [McLay et al. (2017)] | VR head-mounted display (HMD) | PTSD treatment | 83 active-duty service members (100% male) combat-related PTSD randomized to VRET (n = 42) or control (n = 41) | VRET + PE + in vivo exposure vs control group that viewed a moving image on computer during imaginal exposure. Participants completed 8-12 90-minute sessions over nine weeks. | Both treatment groups showed significant reduction in CAPS scores after nine weeks of treatment and at three-month follow up (p < .001), but there were no between-group differences. | |
| [Bisson et al. (2020)] | 3MDR (VRET+ EMDR + treadmill) | PTSD treatment | 42 veterans (all male) with treatment-resistant combat-related PTSD randomized to 3MDR (n = 21) or waitlist control (n=21). | During exposure, instead of immersing in the VR environment, participants viewed an image of the VR environment on a computer screen while walking on treadmill (3MDR). Participants received two preparation sessions followed by six 60 minute 3MDR sessions and one concluding session over nine weeks. Control group received intervention after 12 weeks. | At week 12, difference in mean CAPS scores between the immediate and delayed 3MDR arms was 9.56 (95% CI [− 17.15, −1.97], p = .014) with an estimated effect size of d = 0.65. These effects were maintained at 26 week follow-up. PCL-5 (−11.67, 95% CI [–20.06, −3.27], p = .006), GAD-7 (-5.14, 95% CI [−9.42, −0.86], p = .0018) and insomnia (ISI; -7.34, 95% CI [−10.64, −4.01], p < .001) also were improved at 12 weeks. |
3MDR: multimodal motion-assisted exposure therapy. |
| Van [Gelderen et al. (2020)] | 3MDR (VRET+ EMDR + treadmill) | PTSD treatment | 42 veterans (98% male) with treatment-resistant combat-related PTSD randomized to 3MDR (n = 21) or waitlist control (n = 21) | Same protocol as Bisson et al. except control group consisted of treatment as usual without trauma-related treatment. Both groups received similar amount of treatment hours. Experimental group received six 70-90 minute sessions over six weeks with an option of continuing up to 10 weeks. | Greater decrease in CAPS scores in 3MDR group vs control group at 16 weeks (F(1,37) = 6.43, p = .016; d = 0.83). PCL-5 was not significant (F(1,37) = 2.51, p = .121; d = 0.51) | |
| [Difede et al. (2022)] | VR head-mounted display (HMD) | PTSD treatment | 192 veterans (90% male) with treatment-resistant combat-related PTSD randomized to VRET (n = 97) or PE (n = 95) | “Wizard of Oz protocol.” Participants received two preparatory sessions followed by seven 90-minute weekly sessions, with 30-45 minutes of exposure and 30 minutes of processing discussion. At session 3, participants received either D-cycloserine or placebo | Both treatment groups improved CAPS scores (F (1,190) = 51.18, p < 0.001), but there we differences between groups (F(1,190) = 2.36, p = .126). Therapy-by-MDD interaction (F = 4.07, p = .045) suggested that VRE was more effective for depressed participants (CAPS mean difference = .51, 95% CI [1.17, 5.86], p = .004, effect size = 0.14) but PE was more effective for nondepressed participants (CAPS mean symptom difference = −8.87 [95% CI [−11.33, −6.40], p < .001, effect size = −0.44) | “Wizard of Oz” protocol: During VRET, patients verbally describe events of their traumatic memory in the first person to the therapist, who customizes the VR scene to match the patient’s memory. D-cycloserine (DCS) is a partial agonist at the N-methyl-D-aspartate (NMDA) glutamate receptor. |
| Neurofeedback Training | ||||||
| [Nicholson et al. (2020)] | Neurofeedback Training | PTSD treatment | 36 civilians with PTSD (28% male) were randomized to experimental NFT (n = 18) or sham NFT (n = 18) and compared to healthy controls (n= 36). Military occupational trauma (n = 3), first responder occupational trauma (n = 2), and civilian physical/sexual abuse or neglect (n = 13) | Digitally-guided alpha-rhythm desynchronization neurofeedback measured from the parietal lobe vs sham neurofeedback. Minimum of 17 20-minute weekly NFT training sessions for 20 weeks | No significant difference in CAPS score reductions from pre- vs. post NFT training between the experimental and sham groups (F(1.42, 48.37) = 0.911, η2 = 0.026, ns). Only the experimental group showed significant CAPS-total scores from pre- to post-NFT (t(17) = 3.00, p < .008, dz = 0.71) and from pre-NFT to the 3-month follow-up (t(17) = 3.24, p < .005, dz = 0.77). Higher remission rates in experimental group vs sham group (61% vs 33%). Aberrant connectivity in large-scale brain networks trended towards normalization post-treatment | |
| [Leem et al. (2021)] | Neurofeedback Training | PTSD treatment | 22 adults with PTSD (10% male) randomized to NFT group (n = 10) or waitlist-control (n=9). Domestic violence trauma (n = 16), traffic accident (n = 2), school violence (n = 1) | Audio-based NFT training activation of parietal lobe alpha- and theta-rhythms and suppression of beta-rhythms. 16 50-minute sessions (30 minutes active and 20 minutes resting) over eight weeks | After eight weeks of treatment, scores on the Korean Version of the PTSD Checklist-5 (PCL-5-K) improved more in the NFT group than in the waitlist control group (NSRT group: 24.90 ± 13.13 vs. waitlist control group: 4.11 ± 9.03; p < 0.01), and this difference was maintained at one month follow-up. Measures of anxiety (BAI, p < .01), depression (BDI, p < .01), and quality of life (QOl-EQ-VAS, p <.01) were also significantly improved in the NFT group compared to waitlist controls at one-month follow-up. | |
| [Fruchtman-Steinbok et al. (2021)] | Neurofeedback Training | PTSD treatment | 59 adults with PTSD randomized to three groups: Trauma-script feedback interface (Trauma-NFT; n = 13), neutral feedback interface (Neutral-NFT; n = 14), and a waitlist control group of No-NF (n = 13) |
Trauma-oriented NFT protocol in which experimental group listening to an audio clip of a personal trauma-interview. Another group listened to neutral music. Down-regulation of amygdalar activity (AmygEFP) reduced the volume of the audio clip. 15 40-minute sessions over 13 weeks | Both NFT groups showed reductions in CAPS scores compared to controls (F(2,34) = 6.21, p = .005, η2 = 0.26), with a marginal difference between the NFT groups (p = .07). Relative to No-NF control, Trauma-NF showed the largest decrease in symptoms (−35.13%; p = .001), followed by Neutral-NF (−19.48%; p = .04). Both NFT groups also improved on anxiety (STAI), and only the Neutral-NFT group significantly improved on depression (BDI), where Trauma-NFT showed a marginal improvement. Neither experimental group significantly improved in emotional regulation or alexithymia. | EEG recording used a machine-learning based modeling of previous EEG sessions recorded in conjunction with fMRI, which allowed EEG-alone to be related to predicted decreases in amygdalar fMRI BOLD activity |
| [Rogel et al. (2020)] | Neurofeedback Training | PTSD treatment | 37 children (aged 6-13 years old, 65% male) with PTSD randomized to NFT group (n = 20) and treatment as usual control (n = 17). Chronic neglect (n = 33), impaired caregiver (n = 33), separation from primary caregiver (n =35), physical abuse, and domestic violence were most commonly reported traumas | Audio and visual NFT training inhibition of delta-, theta-, and beta- rhythms and the activation of each individual’s maximal amplitude alpha-rhythm in the parietal cortex vs. treatment as usual. 24 6-12 minute sessions of biweekly NFT over 12 weeks | After 12 weeks, fewer NFT participants met diagnostic criteria for PTSD compared to controls, as assessed by K-SADS (10/16 controls vs 4/16 NFT, p = .033). At one-month follow-up, this difference was no longer significant (7/14 controls vs 10/15 NFT, p = .362) | |
| du [Bois et al. (2021)] | Neurofeedback Training | PTSD treatment | 29 adults with PTSD randomized into three groups: Neurofeedback (n =1 0), Motor-imagery (n = 10), and control (n = 9) | Videogame-based NFT protocol training alpha-rhythm suppression over the parietal cortex vs motor imagery (MI) game training mu- and beta-rhythm modulation over the sensorimotor cortex. Six to seven 20-minute sessions | Only the NFT group showed significant reductions in PTSD symptom severity in four of the seven clinical measures: the PCL-5 (p = .005, d = 2.24), the PC-PTSD for DSM-5 (p = .005, d = 3.1), the Harvard Trauma questionnaire (p = .005, d = 2.41), and the 10-item CD-RISC (p = .041, d = −0.4). Significant differences between NFT and MI groups in their pre- and post-intervention differences in two of the seven clinical questionnaires (PCL-5 [p = .001, d = 2.22] and HTQ [p = .001, d = 2.19]). | Conducted outside of the clinical setting (in public buildings |
| Mobile Apps | ||||||
| [Pacella-LaBarbara et al. (2020)] | PTSD coach mobile app | PTSD treatment | 64 trauma-exposed patients in the emergency department assigned to PTSD Coach (n = 33) or treatment as usual (TAU; n = 31) | Patients used the PTSD coach app ad libitum for one month | At 1- and 3-month follow-ups, there were no significant PTSD symptom differences between groups, as assessed via the abbreviated 8-item PTSD checklist. Although, at 3-month follow-up, black participants assigned to the intervention group (n = 21) reported marginally lower PTSD symptoms (95% CI [−0.30, 37.77] and higher self-coping efficacy (95% CI [−58.20, −3.61]) according to a nine-item scale created by the authors. | |
| [Hensler et al. (2021/2022)] | Swedish version of PTSD coach mobile app | PTSD treatment |
179 adults in Sweden with trauma in the past two years assigned to have access to a Swedish version of PTSD coach (n = 89) or waitlist control (n = 90) | Participants were assessed twice daily with questions about self-reported health as well as app usage and use of strategies for 21 consecutive days | After 24 days, there were no significant differences in self-reported health between the two groups. A follow-up study using the same participant data revealed significant differences in posttraumatic stress in the group with access to the PTSD coach for three months (d = −0.45, 95% CI [−0.70, −0.20]), as assessed by the PCL-5. Participants with access to the app were also more likely to experience clinical improvements (χ²1,150) = 4.62; p = .03 (2(1, 150) = 4.62; p = .03) and less likely to meet diagnostic criteria for probable PTSD compared to waitlist controls (2(1, 150) = 7.74; p = .005). |
|
| [Kuhn et al. (2017)] | PTSD Coach mobile app | PTSD treatment | 120 trauma-exposed participants with elevated PCL-C scores asigned to PTSD coach access (n=60) or waitlist control (n=60) | Participants were assessed for PTSD symptom scores with PCL-C after three months of ad libitum use | After three months, participants with access to the app showed significant reductions in PCL-C scores compared to waitlist controls (F(1, 117) = 4.55, p = .035). Mean scores did not significantly differ after the waitlist controls received treatment (t(118) = 0.73, p = .466). The PTSD Coach group also showed significant reductions in depression symptoms (PHQ-8; F(1,117) = 8.34, p = .005). | |
| [Cox et al. (2019)] | Mobile app-based mindfulness program | PTSD treatment | 80 ICU patients discharged after being treated for cardiorespiratory failure, divided between mobile mindfulness (n=31), telephone mindfulness (n=31), or psychoeducation (n=18) | The patients were each allocated to a month-long treatment program; either mobile mindfulness, therapist-led telephone-based mindfulness, or psychoeducation. Patients were assessed with patient health questionnaire and Post Traumatic Stress Scale (PTSS) at 3-month follow-up. | At 3-month follow-up, clinically insignificant decreases in all groups on PTSS: mobile (−2.6, 95% CI[−6.3, 1.2]), telephone (−2.2, 95% CI [−5.6, 1.2]), education (−3.5, 95% CI [−8.0, 1.0]). | |
| [Elbogen et al. (2019)] | CALM mobile app | PTSD management | 112 dyads of veterans and their support person completed this study. Of the veteran participants, 90% were male with an average age of 36.52. | Participants were instructed to follow the novel CALM program for six months and had a mobile device to access apps supplementary to their program. Active control group participants received psychoeducational material and did visual memory training. | Both the experimental group (p < 0.001) and the active control group (p = 0.002) improved on PTSS. Among secondary outcomes, there was a larger decrease in anger over 6 months compared the control (B= −5.27, p = .008). Family/friends reported that veterans randomized to CALM engaged fewer maladaptive interpersonal behaviors (eg, aggression) over 6 months than the control (B = −2.08, p = .016). | CALM: Cognitive Applications for Life Management, TBI: Traumatic Brain Injury |
| [Niles et al. (2020)] | “Resolving Psychological Stress”(RePS) mobile app | PTSD management | 689 patients with PTSD symptoms in the United States (20% male) assigned to have personalized ABM (n = 234), non-personalized ABM (n = 219), or placebo (n = 236) | RePS mobile app trained attention bias by presenting participants with two words, where at least one was neutral, and one associated with threat. Both words were neutral in placebo condition, and in the personalized ABM, the threat word was chosen based on what the model predicted to be most threatening to the participant. Participants were instructed to use the app for 21 days. | After 21 days of training, all three groups showed reductions in PCL-5 scores from baseline (p < .001), but not at 5 week follow-up (p= .484). There were no significant difference in PCL-5 scores between the groups (p = .786) | |
| Van der [Meer et al. (2017)] | Smart Assessment on your Mobile (SAM) | PTSD and depression identification | 89 trauma-exposed participants in the Netherlands consisting of 88 police officers and 1 ambulance worker (75.3% male) | SAM was used to assess PTSD symptoms, general functioning, depression, etc. and involves a shortened, Dutch version of the PCL-5. Participants completed the SAM on average 5.6 days before completing in-person CAPS-5 interview | There was 77.5% agreement between the CAPS-5 and the PCL-5 in SAM. Also, participants with a clinician-rated PTSD diagnosis had significant higher scores on the PCL-5 (mean = 43.10, SD = 13.55) than participants without a PTSD diagnosis (mean = 25.75, SD = 11.01), (t = −6.43, p < .001) | |
| [Röhr et al. (2021)] | Sanadak mobile app | PTSD management | 133 trauma-exposed Syrian refugees residing in Germany aged 18-65 divided into an intervention group n = 65, and a control group n = 68. Participants were 61.7% male | Sanadak is a smartphone-based mobile app that provides CBT-based self-help in the Arabic language. Participants were allocated to either an intervention group that used the Sanadak app for four weeks or a control group that received psychoeducational reading material. |
After 4 weeks, no significant difference found between the intervention group using the Sanadak app (n = 65) and the psychoeducation control group (n = 68) on the PDS-5 (mean difference= –0.39, 95% CI [–3.24, 2.46], p = .79) | |
Methods
To identify recent articles using digital technologies for PTSD diagnosis, symptom assessment, and treatment, a PubMed search was conducted in February of 2023 screening for original research publications between 2017 and 2022. Query of PubMed used the terms “PTSD” OR “posttraumatic stress disorder” AND “digital phenotyping” OR “wearable” OR “sensor” OR “digital technology” OR “virtual reality” OR “augmented reality” OR “mobile app” OR “machine learning” OR “artificial intelligence” OR “neurofeedback” OR “facial recognition” OR “natural language processing.” These criteria were specified to human trials with full text available in English, and abstract review ensured original research was conducted with the aforementioned digital technologies–defined as digital technologies that have current or future potential for scalability (meaning a patient could feasibly gain access to the use of the technology through the purchase or provision of a small, digital device [i.e., wristband, tablet, headset, smartphone, or computer] and use it without the virtual or in-person presence of a mental health care provider)–and PTSD diagnosis, symptom assessment, or symptom treatment as the primary outcome.
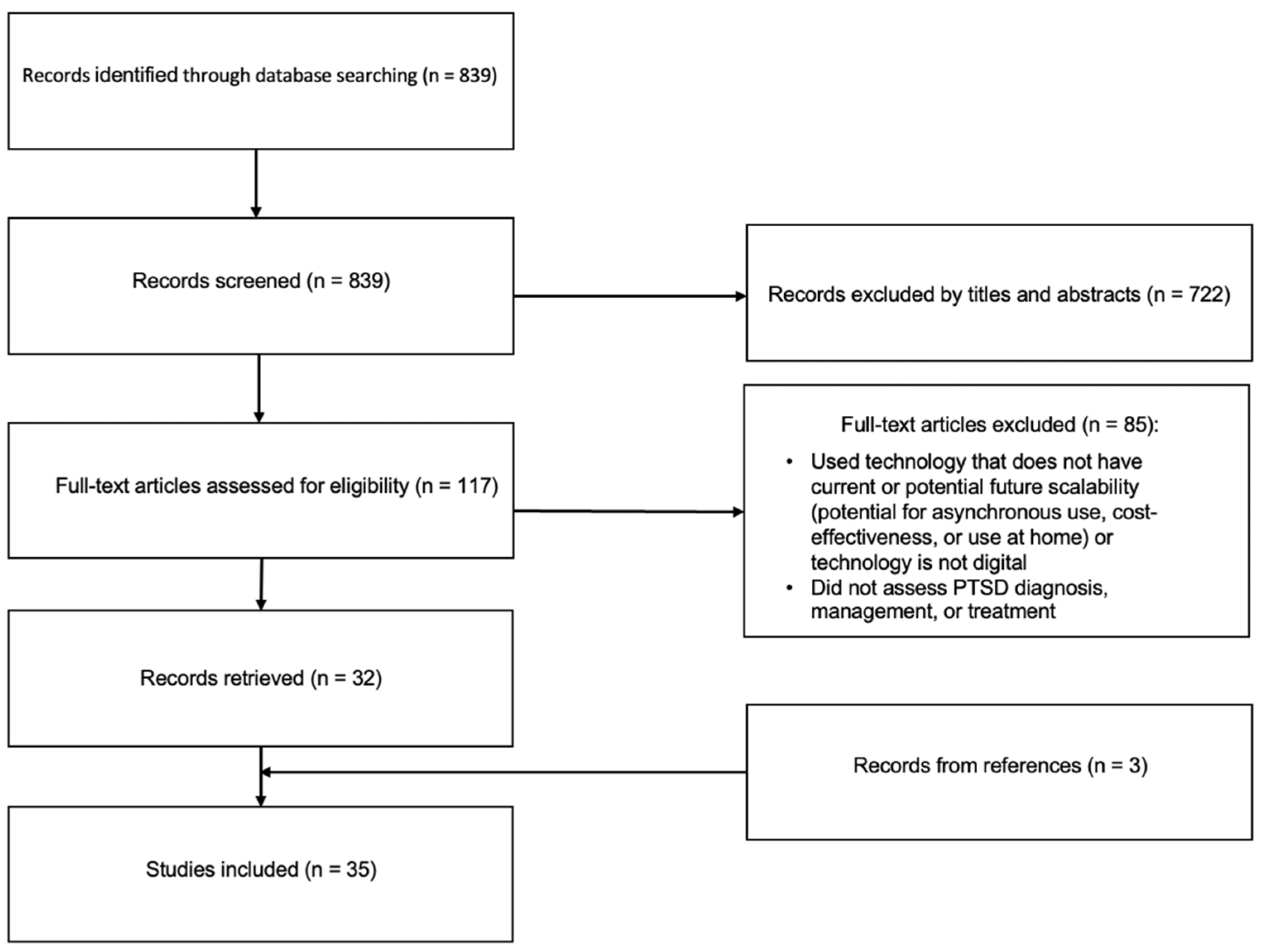
Figure 1.
Our Pubmed search generated 839 publications, 722 of which were screened out during title and abstract screening. The remaining 117 articles were screened for full-text, and 85 of these were rejected because they were outside the scope of the review (focused on other psychiatric disorders), used a digital tool that does not have potential scalability (neuroimaging, vagal nerve stimulation, teletherapy, TMS). An additional three articles found from citation trails were included, bringing the total number of studies informing this review to 35.
Figure 1.
Our Pubmed search generated 839 publications, 722 of which were screened out during title and abstract screening. The remaining 117 articles were screened for full-text, and 85 of these were rejected because they were outside the scope of the review (focused on other psychiatric disorders), used a digital tool that does not have potential scalability (neuroimaging, vagal nerve stimulation, teletherapy, TMS). An additional three articles found from citation trails were included, bringing the total number of studies informing this review to 35.
Each study was independently screened by LB and IR for author bias and for adherence to inclusion and exclusion criteria. If the two authors disagreed on the fit of a study for inclusion, AJ decided whether to include the study. We then categorized the articles as “immersive technologies” (VR and AR), “digital phenotyping,” “wearables,” “neurofeedback training,” “natural language processing and facial feature interpretation,” and “mobile apps.”
Results
Digital Tools for PTSD Diagnosis and Symptom Assessment
Digital Phenotyping
Our search identified three studies using data collected from smartphones to predict the presence of PTSD or PTSD symptoms. All studies used GPS data to some extent and were conducted in civilian populations. Place et al., (2017) gathered various data types generated through regular phone use in a sample with PTSD and depression symptoms and created a regression model that predicted presence of depressed mood, fatigue, interest in activities, and social connectedness with acceptable area under the receiver operating characteristic curve (AUC) of 0.74, 0.56, 0.75, and 0.83 respectively (see de Hond, 2022 for description of AUC interpretation) with PTSD diagnosis verified by the Structured Clinical Interview for Mental Disorders (SCID). Another study used GPS data to compare mobility patterns of women with PTSD, those with a history of child abuse but mentally healthy, and healthy controls, finding significant differences in distance traveled from home in the trauma-exposed groups compared to controls, especially during weekends (Friedmann et al., 2020). However, these differences were influenced by depression and health status in some cases. A third study used these GPS data to feed a machine learning algorithm to successfully differentiate between PTSD and control groups with high accuracy and predictive value (AUC = 0.82) (Lekkas et al., 2021).
Wearables
We reviewed four studies using digital skin conductance collected digitally via iPad (eSense app); three studies collecting pulse data with a wrist-worn sensor or Holter monitor; and one study measuring actigraphy, light, and temperature with a wrist-worn sensor.
Skin conductance data may aid PTSD diagnosis prediction in emergency department patients who had been exposed to trauma, with one research team achieving an AUC of 0.7 when using a regression model based on skin conductance reactivity (Hinrichs et al., 2017) and an AUC of 0.9 in a different sample two years later (Hinrichs et al., 2019). The other two studies highlighted the utility of using various skin conductance metrics for PTSD symptom prediction in children, finding skin conductance reactivity during a standardized trauma interview correlated with the number of traumatic events experienced and with PTSD symptoms in a sample of predominantly Black youth (Wiltshire et al., 2022) and in a sample of youth refugees (Grasser et al., 2022).
Investigations into pulse data and heart rate variability (HRV) through wearable sensors yielded variable results in predicting PTSD diagnosis; one study on 1618 emergency department patients with recent trauma exposure showed an AUC of 0.56 using a machine learning model based on sensor-based features, which improved to 0.79 when combined with clinical survey data (Cakmak et al., 2021). Another study using HRV data from 24-hour ECG monitoring demonstrated potential in distinguishing PTSD in a sample of male veterans with combat-related PTSD, with a model reaching an AUC of 0.86 when applied to an out-of-sample dataset and 0.72 when applied to the sample group (Reinertsen et al., 2017). Sadeghi et al., used data from smartwatches tracking heart rate and body acceleration, and to develop a machine learning model for predicting PTSD hyperarousal events in a cohort of 99 veterans (Sadeghi et al., 2022). The best performing machine learning model achieved an 83% accuracy and an AUC of 0.70 in predicting the occurrence of a PTSD hyperarousal event compared to self-report. The model identified higher average heart rate, higher minimum heart rate, and increased body acceleration as key predictive factors for the onset of PTSD hyperarousal symptoms.
Tsanas et al. demonstrated potential utility in tracking sleep with wearables for diagnostic purposes (Tsanas et al., 2020). Using sensors to measure actigraphy, light, and temperature, PTSD patients were seen to have more fragmented sleep patterns compared to traumatized and healthy controls.
Natural Language Processing (NLP) and Facial Feature Interpretation
Our literature search revealed six studies aiming to use machine learning to analyze speech, facial expression, or word choice to diagnose or predict PTSD trajectory (Schultebraucks et al., 2022; He et al., 2017; He et al., 2019; Sawalha et al., 2022; Marmar et al., 2019; Gavrilescu & Vizireanu, 2019).
Multiple studies have successfully used speech features and facial expressions, captured from recorded responses to interviews or prompts, to predict PTSD diagnoses. These predictions were benchmarked against gold-standard assessments such as the Clinician-Administered PTSD Scale (CAPS) and the PTSD Checklist for DSM-5 (PCL-5). For instance, Marmar et al. (2019) used Random Forest modeling to analyze objective speech features such as monotony of speech, hesitations, and energy variations during Clinician-Administered PTSD Scale (CAPS) interviews. The algorithm reached a sensitivity of 0.90, specificity of 0.88, AUC of 0.95, and an overall correct classification rate of 89.1%, finding participants with PTSD had slower, more monotonous speech, less change in tonality, and less activation. Meanwhile, Schultebraucks et al. (2022) achieved similar results using facial features of emotion and their intensity, speech prosody, movement parameters, and natural language content collected from participant video responses to five open-ended questions one month after experiencing a life-threatening traumatic event. The authors used a deep neural network model that predicted a PCL-5 PTSD diagnosis and depression diagnosis with AUC of 0.90 and .86 respectively. Another study by Gavrilescu & Vizireanu (2019) also demonstrated feasible diagnostic accuracy without provider intervention by applying machine learning to differentiate facial expressions common to patients with either PTSD, generalized anxiety disorder (GAD), or MDD. Using a multi-layered neural network-based architecture detecting facial features from videos of 128 participants watching emotionally-stimulating videos, the researchers were able to obtain an accuracy of 93% in predicting MDD and PTSD, and over 85% accuracy in predicting GAD.
Three studies demonstrate the potential in remote and automated PTSD diagnosis through textual analysis, with one study Sawalha et al. implementing an artificial, human-controlled avatar to ask emotionally-valenced questions over a video conference call. The researchers achieved a top accuracy of 80.4% and an AUC of 0.80 using natural language processing (NLP) techniques on transcripts generated from the interviews. Similarly, He et al. (2017) analyzed text responses of veterans’ written self-narratives detailing their trauma and current symptoms using four different machine learning models. The product score model achieved the greatest accuracy of 82% compared to clinical interview and the highest AUCs recorded for the support vector machine (0.90) and product score model (0.94). In a follow up study in non-veterans using the product square model, He et al. (2019) showed the diagnostic utility of self-narratives is increased when combined with online survey responses, improving the diagnostic accuracy from 84% to 97%.
Mobile Apps
The ubiquity of mobile smartphones provides an opportunity for incorporating scalable screening for psychiatric disorders, and one study assessed the use of a mobile app for PTSD diagnostic screening. Van der Meer et al. (2017) introduced SAM, a mobile app for screening PTSD and depression, in 88 trauma-exposed first responders. SAM showed a 77.5% agreement with the gold standard, and participants with a clinician-rated PTSD diagnosis had higher SAM-administered PCL-5 scores.
Digital Tools for PTSD Treatment Augmentation
Immersive Technology (VR, AR, 3DMR)
All six studies reviewed here included samples consisting solely of active duty service members or combat veterans (van Gelderen et al., 2020; McLay et al., 2017; Bisson et al., 2020; Difede et al., 2022, Loucks et al., 2019), as they were the only trials that met inclusion criteria (see methods section). All virtual reality exposure therapy (VRET) sessions were conducted in the presence of a trained therapist, with two studies utilizing the “Wizard of Oz” protocol in which the therapist can control the ambient environment (location, time of day, sounds, etc.).
Difede et al. compared PE to VRET in a RCT of 192 veterans with treatment-resistant combat-related PTSD, where the VRET group was placed in a VR environment relevant to their trauma and completed imaginal exposure (Difede et al., 2022). As participants recounted their traumatic event, the therapist customized the environment to match their description. In addition, at the first intervention session, participants received either a cognitive enhancer, D-cycloserine (partial NMDA glutamate receptor agonist), or a placebo. After nine weeks of treatment, participants in both groups improved significantly in CAPS scores, but, in accordance with previous work comparing VRET to PE (Kothgassner et al., 2019), there were no significant differences between the groups. Interestingly, depressed patients were more likely to benefit from VRET (p = .004, effect size = 0.14), while nondepressed patients were more likely to benefit from PE (p < .001, effect size = −0.44). The cognitive enhancer did not significantly impact treatment outcomes.
Three studies reported using multimodal motion-assisted exposure therapy (3MDR), which consists of a VRET protocol making use of eye-movement desensitization (EMDR) while walking on a treadmill (van Gelderen et al., 2020; McLay et al., 2017; Bisson et al., 2020). In a study of 81 active-duty service members with PTSD, McLay et al. studied 3MDR therapy integrating olfactory and motor stimuli and showed significant reductions in CAPS scores at 12 week follow-up, but not significantly different from compared to a control exposure therapy group that viewed a moving image on a computer screen (McLay et al., 2017). Bisson et al. and Van Gelderen et al. both followed the same 3MDR protocol in which 42 veterans selected 12 images that evoked memories of the traumatic event (Bisson et al., 2020; van Gelderen et al., 2020). While immersed, participants walked through a tunnel in a virtual outdoor environment and were presented with trauma-related images. Both of these studies found significant reductions in CAPS scores in 3MDR groups compared to waitlist controls (p = .021, d=.65) (Bisson et al., 2020) and controls who received non-trauma related treatment (p = .016, d = 0.83) (van Gelderen et al., 2020).
One open arm trial of 15 veterans tested the feasibility of using VRET for military sexual trauma and found significant reductions in CAPS (d = 1.11) and PCL-5 scores (d = 1.14) as well as depressive scores (d = 0.94), but these differences were insignificant at three-month follow up (Loucks et al., 2019). The study had a high drop-out rate with only 9 participants completing the trial.
No completed clinical trials were found that used augmented reality (AR) for PTSD treatment. However, there are pilot findings of augmented reality exposure therapy applied to real-life situations for treating behavioral avoidance in patients with PTSD ([name deleted to maintain the integrity of the review process], 2023).
Mobile Apps
The ubiquity of mobile smartphones provides an opportunity for incorporating scalable treatment augmentation without the need for an adjunct health professional. Previous investigations have explored mobile apps as tools for delivering education, self-guided psychological exercises, wellness surveys, and more (Röhr et al., 2021; Cox et al., 2019). The following papers explore the efficacy of downloadable mobile apps in PTSD treatment.
Four of the nine studies reviewed here utilized the PTSD coach (Kuhn et al., 2017; Hensler et al., 2021; Hensler et al., 2022; Pacella-LaBarbara et al., 2020), an app developed by the U.S. Department of Veterans Affairs’ National Center for PTSD and the Department of Defense’s DHA Connected Health (Kuhn et al., 2014). The app consists of several modules designed to improve patient education about PTSD, track PTSD symptoms over time, and provide patients with self-management exercises inspired by cognitive behavioral therapy.
In one of the first RCTs of PTSD Coach, Kuhn et al. recruited a sample of 120 trauma-exposed participants and found that users of the app experienced significant reductions in PTSD and depression symptom scores over three months as assessed by the PCL-C and PHQ-8 (effect sizes 0.41 and 0.45 respectively) (Kuhn et al., 2017). In another study, Hensler et al. studied 179 trauma-exposed adults and found that after 24 days, there were no reported differences in self-reported health between the experimental and control groups (Hensler et al., 2021). In a follow-up study using the same participant data, an intent-to-treat analysis revealed participants with access to the app for three months were more likely to experience clinical improvements (p = .03) and less likely to meet diagnostic criteria for probable PTSD compared to waitlist controls (p = .005) (Hensler et al., 2022). Lastly, Pacella-LaBarbara et al. studied PTSD Coach in 61 patients within 24 hours of experiencing a motor vehicle collision. At 1- and 3-month follow-up, there were no significant PTSD symptom differences between groups. Notably, 76% of those who had used the app reported it to be extremely helpful, but only 67% of subjects assigned to the app group had used the app at least once (Pacella-LaBarbara et al., 2020).
Cox et al. explored a self-directed mobile mindfulness app in a sample of 80 adult patients who had been treated for cardiorespiratory failure and underwent ICU management. Participants were each allocated to a month-long treatment program of mobile mindfulness, therapist-led telephone-based mindfulness, or education about critical illness. At one and three-month follow-ups, all groups showed clinically insignificant decreases on the PTSS (Cox et al., 2019).
Elbogen et al. investigated cognitive rehabilitation using the CALM program on 112 veterans with traumatic brain injury and PTSD. While both the experimental and psychoeducation control groups showed significant reductions in CAPS scores (p < .001 and p = .002, respectively), CALM was not significantly more effective (Elbogen et al., 2019).
Niles et al. used a mobile-based cognitive training intervention, attention-bias modification (ABM), for PTSD management. The ABM program involved flashing a neutral word and a threatening word simultaneously to participants, who were instructed to direct attention to the neutral word. Participants were assigned to ABM with personalized threatening words, non-personalized ABM, or placebo with two neutral words. After 21 days of training, all three groups had significant reductions in PCL-5 scores from baseline (p < .001), but there were no significant differences among the groups (Niles et al., 2020).
Röhr et al. assessed the Sanadak mobile app in a sample of 133 Syrian refugees with PTSD. After four weeks, no significant difference was found between the Sanadak app group and the psychoeducation control group on the PDS-5 (p = .79) (Röhr et al., 2021).
Neurofeedback
Our search revealed five studies investigating EEG-NFT for the treatment of PTSD. We did not include studies using fMRI as the primary training tool, as it is not scalable (see inclusion criteria).
Two studies investigating alpha-rhythm suppression over the parietal cortex found significant decreases in PTSD symptoms. Nicholson et al. (2020) showed 20 weeks of NFT in a civilian sample led to significant reductions in CAPS-total scores from pre- to post-NFT (p < .008, d = 0.71) and at three-month follow-up (p < .005, d = 0.77), but there was no significant difference in CAPS score reductions compared to sham groups (η2 = 0.026). Another smaller study in 29 Rwandans with PTSD also showed large effect sizes in pre- to post-NFT PTSD scores on the PTSD Checklist for DSM-5 (PCL-5) (p =0.005, d = 2.24), the Primary care PTSD screen for DSM-5 (PC-PTSD) (p =0.005, d = 3.1), and the Harvard Trauma questionnaire (p =0.005, d = 2.41) (du Bois et al., 2021). However, while this study reported that only the NFT group showed significant reductions in PTSD symptoms and that there were significant reductions between the NFT group and the active control group (motor imagery), there were no reported differences between the NFT group and waitlist controls.
As opposed to alpha suppression, Leem et al. (2021) studied activation of parietal cortex alpha-rhythms. Following eight weeks of training, PTSD symptoms (measured through a Korean version of the PCL-5) improved more in the NFT group than in the waitlist control group (p <.01), and this difference was maintained at one month follow-up along with measures of depression, anxiety, and quality of life. Similarly, Rogel et al. (2020) assessed parietal alpha activation and concurrent theta, beta, and delta suppression in a sample of 37 children with PTSD. After twelve weeks, fewer NFT participants met diagnostic criteria for PTSD compared to controls, but this difference was not maintained at one-month follow-up.
Previous fMRI studies suggest downregulation of the amygdala during exposure to trauma-cues could improve PTSD symptoms (Gerin et al., 2016; Nicholson et al., 2021). Fruchtman-Steinbok et al. (2021) developed an EEG NFT model that correlated with fMRI-amygdala activity in which successful suppression of amygdala activity reduced the volume of audio recorded from trauma-interviews. Following 15 sessions of NFT, both neutral NFT and trauma-interview NFT groups showed significant reductions in CAPS scores compared to waitlist controls (p = .005, η2 = 0.26), with a significant difference between trauma-NFT and controls (p = .001) and a marginal difference between neutral-NFT and controls (p = .07). These reductions in CAPS scores were maintained at three and six-month follow up but were not significant (p = .07).
Interestingly, although all five studies showed significant reductions in PTSD symptoms, only one study showed a correlation between brain activity changes and symptoms, with Nicholson et al. finding a negative correlation between total CAPS score reduction and salience network activity post-NFT (p = 0.015).
Discussion
The current review sought to investigate the efficacy of scalable digital technological tools for predicting PTSD diagnosis, monitoring symptoms, and augmenting treatment. This review surveyed a broad array of technologies to offer an update on the most promising digital tools, leading to the inclusion of studies from direct patient care through randomized controlled trials to feasibility studies applying machine learning. Considering the nascent stage of numerous technologies examined in this review, most research identified are pilot studies, which exhibit a wide variation in study design and methods. This made cross-study comparisons difficult. Furthermore, most studies did not directly compare the digital intervention to other methods of therapy or diagnosis, meaning conclusions of their effectiveness are limited.
There is increasing interest in the field of psychiatry for using machine learning and artificial intelligence to generate individualized approaches to symptom assessment through identifying digital biomarkers of disease, and many of the studies included in this review often leveraged machine learning approaches to enhance diagnostic prediction capabilities. However, the application of machine learning to psychiatry is still in its nascency, as there is limited consensus on standards for building, testing, and validating machine learning approaches (Koppe et al., 2021). For example, among the reviewed studies, the choice of machine learning algorithm greatly influenced predictive capability. In one study applying NLP to patient narratives, despite equivalent pre-processing of data inputs, four different commonly-used machine learning models varied widely in their predictive abilities when applied to the sample, as AUCs ranged from 0.68 to 0.94 (He et al., 2017). Although different data processing algorithms may be best suited given different data structures, there are still many unknowns about the different factors that influence model performance (Koppe et al., 2021). Nevertheless, the results of the reviewed studies support the potential for these digital technologies to supplement future clinical practice.
Studies of digital phenotyping and wearables showed promise in their ability to predict the presence of PTSD diagnosis or symptoms, with HRV showing the most consistent evidence. Of note, these technologies showed discriminant validity when applied to veteran cohorts and highly diverse civilian samples. For instance, studies on mobile skin conductance included samples of majority Black or Arab participants and showed potential in detecting PTSD diagnosis and in assessing symptom severity. Likewise, studies utilizing patient speech, writing, and facial features were also conducted in diverse civilian samples and showed a high degree of accuracy in detecting PTSD diagnosis using machine learning modeling.
One particular advantage to the use of these technologies for patient assessment is their potential to be incorporated into a clinic’s workflow with limited disruption to the patient or the provider (Rodriguez-Villa et al., 2020). If used in conjunction with in-person assessments, these technologies could provide a means of longitudinal symptom monitoring prior to or between appointments and for timely intervention. Indeed, the use of these data may be particularly helpful for assessing patients with PTSD, as avoidance behavior is a hallmark of the disorder. However, more work is needed in larger cohorts to establish standardized approaches to data collection and machine learning modeling before definitive conclusions can be drawn from this literature. These technologies should also be used to distinguish the presence of PTSD symptoms from other psychiatric symptoms before being deployed in clinical practice, as healthy controls were the comparison group in the majority of digital phenotyping, wearables, NLP, and facial recognition studies included in this review.
While the identification and assessment of digital biomarkers is an emerging trend in psychiatric research, the application of VR to PTSD is relatively more established. Previous reviews of VR for PTSD treatment have shown equivalent but not superior treatment outcomes to standard methodologies in treating veterans with combat-related trauma (Kothgassner et al., 2019; Eshuis et al., 2020), and this has been the general conclusion of studies informing this review. More studies of VRET are needed in diverse populations and in different types of trauma, as the majority of recent studies have been in military or veteran cohorts. Although combat environments are currently the easiest to recreate, there are some trials integrating stimuli for traumas related to sexual assault (Loucks et al., 2019) and motor vehicle accidents (Beck et al., 2007). It should also be noted that trials in this review had a trained counselor or therapist present during VRET sessions, and that unlike VRET for social phobias (Premkumar et al., 2021; Hildebrand et al., 2022), no PTSD trial to date has been conducted in a self-guided manner. As the capabilities of this technology and of generative artificial intelligence (i.e., ChatGPT) continue to advance, it may soon be possible to create customized scenarios in which digital characters interact with the patient, facilitating exposure therapy for interpersonal traumas in self-guided exposure format.
This review sought to include augmented reality (AR), but there have yet to be any published studies using this technology in patients with PTSD. AR may be uniquely suited for in vivo exposure therapy and real-life contextualization of exposure therapy, as patients can move freely and interact with trauma-relevant objects within the immediate environment. [name deleted to maintain the integrity of the review process] et al. has previously succeeded in the use of AR in single session treatment of simple phobias ([name deleted to maintain the integrity of the review process] et al., 2021) and recently developed a platform that allows for in vivo exposure therapy of social situations commonly avoided by people with PTSD ([name deleted to maintain the integrity of the review process], 2023).
Meanwhile, apps have been used extensively outside of the clinical setting and require limited training to use. However, as with other emerging digital tools, heterogeneity and limited evidence base currently limit conclusiveness about the effectiveness of apps. Most of the reviewed studies described an improvement in PTSD symptoms, and participants consistently described apps as easy to use. Despite their utility, apps are not used consistently or extensively, as most studies report a steep drop in usage several days after participants begin using an app. Adherence may best be addressed with consistent support from mental health provider or through greater use of gamification (Sandoval et al., 2017).
NFT makes use of gamification to promote engagement, and the studies informing this review showed small to moderate improvements in PTSD symptoms compared to waitlist controls. Nevertheless, studies were limited by small sample sizes and heterogeneity in study design. Participants within the same treatment arm also engaged in different meta-cognitive activities to achieve the goal-directed brain state, including focusing on colors, “quieting the mind,” or focusing on the reward stimulus, suggesting a lack of specificity in the neural processes and self-regulation skills being trained (Nicholson et al., 2020). The potential therapeutic mechanism of NFT remains unclear, and future studies will need to directly compare NFT protocols of activation and suppression of different neural oscillations, reinforcement schedules, and include active-control comparisons in order to better elucidate therapeutic potential.
Although this review highlights significant advancements in technological innovation in the field, these technologies have seen little use in the community setting and by clinicians. For example, VR emerged in the 1980s (Slater et al., 2016), but its use is mostly limited to major academic settings. The inertia and “resistance to technology,” lack of large-scale data, high cost, and technological complexity seem to be major obstacles in moving these technologies from academia into the community. Therefore, there is a need for greater focus in enhancing the usability, scalability, and cost of these technologies in order to transform them from laboratory and research innovations to tools of the future mental health professional.
This review has limitations. First, the conclusions from this review are limited due to sparse use of double blinding in these studies, which may be a product of interacting with digital technology and due to the nature of machine learning studies, as they were oriented towards diagnostic assessment. As such, use of sham digital treatments or data collection could be useful for future studies. Second, we elected to include a wide range of study designs, as opposed to limiting our search to randomized controlled trials (RCTs). Our goal was to provide an up-to-date view of the current capabilities of scalable digital technologies for PTSD and restricting inclusion criteria to RCTs would have limited our conclusions.
In conclusion, this review examined the use of digital technological interventions for assessing and treating PTSD. Increased availability of effective tools for assessing and treating PTSD is needed, and a number of digital technologies show promise in their ability to automate diagnosis and expand access to treatment augmentation. However, there is a need for further research into creating standardized, evidence-based protocols for these technologies to allow for greater dissemination. Likewise, more evidence comparing these digital technologies to standard practices in controlled settings is needed before they can be applied to clinical practice.
Funding
No funding was received for conducting this study.
Conflicts of Interest
AJ is an inventor of a patented AR technology with commercialization potentials. The patent and license to this technology is with Wayne State University. The authors declare that they have no other conflict of interest.
References
- Acierno, R., Jaffe, A. E., Gilmore, A. K., Birks, A., Denier, C., Muzzy, W.,... Tuerk, P. W. (2021). A randomized clinical trial of in-person vs. home-based telemedicine delivery of Prolonged Exposure for PTSD in military sexual trauma survivors. Journal of Anxiety Disorders, 83, 102461. [CrossRef]
- American Psychiatric Association, DSM-5 Task Force. (2013). Diagnostic and statistical manual of mental disorders: DSM-5. American Psychiatric Publishing, Inc.
- Andrilla, C. H. A., Patterson, D. G., Garberson, L. A., Coulthard, C., & Larson, E. H. (2018). Geographic variation in the supply of selected behavioral health providers. American Journal of Preventive Medicine, 54(6 Suppl 3), S199-S207. [CrossRef]
- Barnett, I., Torous, J., Staples, P., Sandoval, L., Keshavan, M., & Onnela, J. P. (2018). Relapse prediction in schizophrenia through digital phenotyping: A pilot study. Neuropsychopharmacology, 43(8), 1660-1666. [CrossRef]
- Beck, J. G., Palyo, S. A., Winer, E. H., Schwagler, B. E., & Ang, E. J. (2007). Virtual Reality Exposure Therapy for PTSD symptoms after a road accident: An uncontrolled case series. Behavior Therapy, 38(1), 39–48. [CrossRef]
- Bedi, G., Carrillo, F., Cecchi, G. A., Fernández Slezak, D., Sigman, M., Mota, N. B.,... Kortholm, J. (2015). Automated analysis of free speech predicts psychosis onset in high-risk youths. NPJ Schizophrenia, 1, 15030. [CrossRef]
- Bisson, J. I., Roberts, N. P., Andrew, M., Cooper, R., & Lewis, C. (2013). Psychological therapies for chronic post-traumatic stress disorder (PTSD) in adults. Cochrane Database of Systematic Reviews, 2013(12), CD003388. [CrossRef]
- Bisson, J. I., van Deursen, R., Hannigan, B., Kitchiner, N., Barawi, K., Jones, K.,... Humphreys, L. (2020). Randomized controlled trial of multi-modular motion-assisted memory desensitization and reconsolidation (3MDR) for male military veterans with treatment-resistant post-traumatic stress disorder. Acta Psychiatrica Scandinavica, 142(2), 141-151. [CrossRef]
- Bourla, A., Mouchabac, S., El Hage, W., & Ferreri, F. (2018). e-PTSD: An overview on how new technologies can improve prediction and assessment of Posttraumatic Stress Disorder (PTSD). European Journal of Psychotraumatology, 9(sup1), 1424448. [CrossRef]
- Cakmak, A. S., Alday, E. A. P., Da Poian, G., Rad, A. B., Metzler, T. J., Neylan, T. C.,et al. (2021). Classification and prediction of post-trauma outcomes related to PTSD using circadian rhythm changes measured via wrist-worn research watch in a large longitudinal cohort. IEEE Journal of Biomedical and Health Informatics, 25(8), 2866-2876. [CrossRef]
- Cox, C. E., Hough, C. L., Jones, D. M., Ungar, A., Reagan, W., Key, M. D., et al. (2019). Effects of mindfulness training programmes delivered by a self-directed mobile app and by telephone compared with an education programme for survivors of critical illness: A pilot randomised clinical trial. Thorax, 74(1), 33-42. [CrossRef]
- Cully, J. A., Jameson, J. P., Phillips, L. L., Kunik, M. E., & Fortney, J. C. (2010). Use of psychotherapy by rural and urban veterans. Journal of Rural Health, 26(3), 225-233. [CrossRef]
- de Hond, A. A. H., Steyerberg, E. W., & van Calster, B. (2022). Interpreting area under the receiver operating characteristic curve. The Lancet Digital Health, 4(12), e853-e855. [CrossRef]
- de Oliveira, P. B. F., Dornelles, T. M., Gosmann, N. P., & Camozzato, A. (2023). Efficacy of telemedicine interventions for depression and anxiety in older people: A systematic review and meta-analysis. International Journal of Geriatric Psychiatry, 38(5), e5920. [CrossRef]
- Department of Veterans Affairs & Department of Defense. (2023). VA/DOD Practice Guideline for Management of Posttraumatic Stress Disorder and Acute Stress Disorder (Version 3.0). U.S. Department of Veterans Affairs & U.S. Department of Defense.
- Di Carlo, F., Sociali, A., Picutti, E., Pettorruso, M., Vellante, F., Verrastro, V.,... Martinotti, G. (2021). Telepsychiatry and other cutting-edge technologies in COVID-19 pandemic: Bridging the distance in mental health assistance. International Journal of Clinical Practice, 75(1), e13716. [CrossRef]
- Difede, J., Rothbaum, B. O., Rizzo, A. A., Wyka, K., Spielman, L., Reist, C.,... D., Rizzo, A. A. (2022). Enhancing exposure therapy for posttraumatic stress disorder (PTSD): A comparison of virtual reality graded exposure with traditional imaginal exposure in a controlled trial. Journal of Consulting and Clinical Psychology, 90(1), 79-93. [CrossRef]
- du Bois, N., Bigirimana, A. D., Korik, A., Kéthina, L. G., Rutembesa, E., Mutabaruka, J., Mutesa, L., Prasad, G., Jansen, S., & Coyle, D. H. (2021). Neurofeedback with low-cost, wearable electroencephalography (EEG) reduces symptoms in chronic Post-Traumatic Stress Disorder. Journal of affective disorders, 295, 1319–1334. [CrossRef]
- Elbogen, E. B., Dennis, P. A., Van Voorhees, E. E., Blakey, S. M., Johnson, J. L., Johnson, S. C., et al. (2019). Cognitive Rehabilitation With Mobile Technology and Social Support for Veterans With TBI and PTSD: A Randomized Clinical Trial. Journal of Head Trauma Rehabilitation, 34(1), 1-10. [CrossRef]
- Eshuis, L. V., van Gelderen, M. J., van Zuiden, M., Nijdam, M. J., Vermetten, E., Olff, M., et al. (2021). Efficacy of immersive PTSD treatments: A systematic review of virtual and augmented reality exposure therapy and a meta-analysis of virtual reality exposure therapy. Journal of Psychiatric Research, 143, 516-527. [CrossRef]
- Foa, E. B., Chrestman, K. R., & Gilboa-Schechtman, E. (2008). Prolonged Exposure Therapy for Adolescents with PTSD Therapist Guide: Emotional Processing of Traumatic Experiences. Oxford University Press. [CrossRef]
- Forbes, D., Pedlar, D., Adler, A. B., Benner, C., Bryant, R., Busuttil, W., et al. (2019). Treatment of military-related post-traumatic stress disorder: Challenges, innovations, and the way forward. International Review of Psychiatry, 31(1), 95-110. [CrossRef]
- Friedmann, F., Santangelo, P., Ebner-Priemer, U., Hill, H., Neubauer, A. B., Rausch, S., et al. (2020). Life within a limited radius: Investigating activity space in women with a history of child abuse using global positioning system tracking. PLoS One, 15(5), e0232666. [CrossRef]
- Fruchtman-Steinbok, T., Keynan, J. N., Cohen, A., Jaljuli, I., Mermelstein, S., Drori, G., Routledge, E., Krasnoshtein, M., Playle, R., Linden, D. E. J., & Hendler, T. (2021). Amygdala electrical-finger-print (AmygEFP) NeuroFeedback guided by individually-tailored Trauma script for post-traumatic stress disorder: Proof-of-concept. NeuroImage. Clinical, 32, 102859. [CrossRef]
- Gavrilescu, M., & Vizireanu, N. (2019). Predicting Depression, Anxiety, and Stress Levels from Videos Using the Facial Action Coding System. Sensors (Basel, Switzerland), 19(17), 3693. [CrossRef]
- Gerin, M. I., Fichtenholtz, H., Roy, A., Walsh, C. J., Krystal, J. H., Southwick, S., & Hampson, M. (2016). Real-Time fMRI Neurofeedback with War Veterans with Chronic PTSD: A Feasibility Study. Frontiers in psychiatry, 7, 111. [CrossRef]
- Giovanetti, A. K., Punt, S. E. W., Nelson, E. L., & Ilardi, S. S. (2022). Teletherapy Versus In-Person Psychotherapy for Depression: A Meta-Analysis of Randomized Controlled Trials. Telemedicine Journal and e-Health, 28(8), 1077-1089. [CrossRef]
- Goreis, A., Felnhofer, A., Kafka, J. X., Probst, T., & Kothgassner, O. D. (2020). Efficacy of Self-Management Smartphone-Based Apps for Post-traumatic Stress Disorder Symptoms: A Systematic Review and Meta-Analysis. Frontiers in Neuroscience, 14, 3. [CrossRef]
- Grasser, L. R., Saad, B., Bazzi, C., Wanna, C., Suhaiban, H. A., Mammo, D., et al. (2022). Skin conductance response to trauma interview as a candidate biomarker of trauma and related psychopathology in youth resettled as refugees. European Journal of Psychotraumatology, 13(1), 2083375. [CrossRef]
- He, Q., Veldkamp, B. P., Glas, C. A., & de Vries, T. (2017). Automated Assessment of Patients’ Self-Narratives for Posttraumatic Stress Disorder Screening Using Natural Language Processing and Text Mining. Assessment, 24(2), 157–172. [CrossRef]
- He, Q., Veldkamp, B. P., Glas, C. A. W., & van den Berg, S. M. (2019). Combining Text Mining of Long Constructed Responses and Item-Based Measures: A Hybrid Test Design to Screen for Posttraumatic Stress Disorder (PTSD). Frontiers in Psychology, 10, 2358. [CrossRef]
- Hendriks, L., de Kleine, R. A., Broekman, T. G., Hendriks, G. J., & van Minnen, A. (2018). Intensive prolonged exposure therapy for chronic PTSD patients following multiple trauma and multiple treatment attempts. European Journal of Psychotraumatology, 9(1), 1425574. [CrossRef]
- Hensler, I., Sveen, J., Cernvall, M., & Arnberg, F. K. (2021). Ecological momentary assessment of self-rated health, daily strategies and self-management app use among trauma-exposed adults. European Journal of Psychotraumatology, 12(1), 1920204. [CrossRef]
- Hensler, I., Sveen, J., Cernvall, M., & Arnberg, F. K. (2022). Efficacy, Benefits, and Harms of a Self-management App in a Swedish Trauma-Exposed Community Sample (PTSD Coach): Randomized Controlled Trial. Journal of Medical Internet Research, 24(3), e31419. [CrossRef]
- Hildebrand, A. S., Roesmann, K., Planert, J., Machulska, A., Otto, E., & Klucken, T. (2022). Self-guided virtual reality therapy for social anxiety disorder: A study protocol for a randomized controlled trial. Trials, 23(1), 395. [CrossRef]
- Hinrichs, R., Michopoulos, V., Winters, S., Rothbaum, A. O., Rothbaum, B. O., Ressler, K. J., et al. (2017). Mobile assessment of heightened skin conductance in posttraumatic stress disorder. Depression and Anxiety, 34(6), 502-507. [CrossRef]
- Hinrichs, R., van Rooij, S. J., Michopoulos, V., Schultebraucks, K., Winters, S., Maples-Keller, J., et al. (2019). Increased Skin Conductance Response in the Immediate Aftermath of Trauma Predicts PTSD Risk. Chronic Stress (Thousand Oaks), 3, 2470547019844441. [CrossRef]
- Hsu, M., Ahern, D. K., & Suzuki, J. (2020). Digital Phenotyping to Enhance Substance Use Treatment During the COVID-19 Pandemic. JMIR Mental Health, 7(10), e21814. [CrossRef]
- Ioannou, A., Papastavrou, E., Avraamides, M. N., & Charalambous, A. (2020). Virtual Reality and Symptoms Management of Anxiety, Depression, Fatigue, and Pain: A Systematic Review. SAGE Open Nursing, 6, 2377960820936163. [CrossRef]
- Jacobson, N. C., Weingarden, H., & Wilhelm, S. (2019). Digital biomarkers of mood disorders and symptom change. NPJ Digital Medicine, 2, 3. [CrossRef]
- [name deleted to maintain the integrity of the review process]. (2021). Real-life contextualization of exposure therapy using augmented reality: A pilot clinical trial of a novel treatment method. Annals of Clinical Psychiatry, 33(4), 220-231. [CrossRef]
- [name deleted to maintain the integrity of the review process]. (2023). Augmented Reality Might Be the Future of Exposure Therapy for PTSD. Biological Psychiatry, 93(9, Supplement), S246. [CrossRef]
- Jericho, B., Luo, A., & Berle, D. (2022). Trauma-focused psychotherapies for post-traumatic stress disorder: A systematic review and network meta-analysis. Acta Psychiatrica Scandinavica, 145(2), 132-155. [CrossRef]
- Jones, C., Miguel-Cruz, A., Smith-MacDonald, L., Cruikshank, E., Baghoori, D., Chohan, A. K., et al. (2020). Virtual Trauma-Focused Therapy for Military Members, Veterans, and Public Safety Personnel With Posttraumatic Stress Injury: Systematic Scoping Review. JMIR mHealth and uHealth, 8(9), e22079. [CrossRef]
- Kamath, J., Leon Barriera, R., Jain, N., Keisari, E., & Wang, B. (2022). Digital phenotyping in depression diagnostics: Integrating psychiatric and engineering perspectives. World journal of psychiatry, 12(3), 393–409. [CrossRef]
- Kazdin, A. E., & Blase, S. L. (2011). Interventions and models of their delivery to reduce the burden of mental illness: Reply to commentaries. Perspectives on Psychological Science, 6(5), 507-510. [CrossRef]
- Kessler, R. C., Chiu, W. T., Demler, O., Merikangas, K. R., & Walters, E. E. (2005). Prevalence, severity, and comorbidity of 12-month DSM-IV disorders in the National Comorbidity Survey Replication. Archives of General Psychiatry, 62(6), 617-627. [CrossRef]
- Keynejad, R. C., Dua, T., Barbui, C., & Thornicroft, G. (2018). WHO Mental Health Gap Action Programme (mhGAP) Intervention Guide: A systematic review of evidence from low and middle-income countries. Evidence-Based Mental Health, 21(1), 30-34. [CrossRef]
- Kilpatrick, D. G., Resnick, H. S., Milanak, M. E., Miller, M. W., Keyes, K. M., & Friedman, M. J. (2013). National estimates of exposure to traumatic events and PTSD prevalence using DSM-IV and DSM-5 criteria. Journal of Traumatic Stress, 26(5), 537-547. [CrossRef]
- Kleiman, E. M., Turner, B. J., Fedor, S., Beale, E. E., Picard, R. W., Huffman, J. C., & Nock, M. K. (2018). Digital phenotyping of suicidal thoughts. Depression and anxiety, 35(7), 601–608. [CrossRef]
- Koenen, K. C., Ratanatharathorn, A., Ng, L., McLaughlin, K. A., Bromet, E. J., Stein, D. J.,... & Kessler, R. C. (2017). Posttraumatic stress disorder in the World Mental Health Surveys. Psychological Medicine, 47(13), 2260-2274. [CrossRef]
- Koppe, G., Meyer-Lindenberg, A., & Durstewitz, D. (2021). Deep learning for small and big data in psychiatry. Neuropsychopharmacology, 46(1), 176-190. [CrossRef]
- Kothgassner, O. D., Goreis, A., Kafka, J. X., Van Eickels, R. L., Plener, P. L., & Felnhofer, A. (2019). Virtual reality exposure therapy for posttraumatic stress disorder (PTSD): A meta-analysis. European Journal of Psychotraumatology, 10(1), 1654782. [CrossRef]
- Kuhn, E., Greene, C., Hoffman, J., Nguyen, T., Wald, L., Schmidt, J.,... & Ruzek, J. (2014). Preliminary evaluation of PTSD Coach, a smartphone app for post-traumatic stress symptoms. Military Medicine, 179(1), 12-18. [CrossRef]
- Kuhn, E., Kanuri, N., Hoffman, J. E., Garvert, D. W., Ruzek, J. I., & Taylor, C. B. (2017). A randomized controlled trial of a smartphone app for posttraumatic stress disorder symptoms. Journal of Consulting and Clinical Psychology, 85(3), 267-273. [CrossRef]
- Le Glaz, A., Haralambous, Y., Kim-Dufor, D. H., Lenca, P., Billot, R., Ryan, T. C.,... & Saporta, G. (2021). Machine learning and natural language processing in mental health: Systematic review. Journal of Medical Internet Research, 23(5), e15708. [CrossRef]
- Lee, D. J., Schnitzlein, C. W., Wolf, J. P., Vythilingam, M., Rasmusson, A. M., & Hoge, C. W. (2016). Psychotherapy versus pharmacotherapy for posttraumatic stress disorder: Systematic review and meta-analyses to determine first-line treatments. Depression and Anxiety, 33(9), 792-806. [CrossRef]
- Leem, J., Cheong, M. J., Lee, H., Cho, E., Lee, S. Y., Kim, G. W., & Kang, H. W. (2021). Effectiveness, Cost-Utility, and Safety of Neurofeedback Self-Regulating Training in Patients with Post-Traumatic Stress Disorder: A Randomized Controlled Trial. Healthcare (Basel, Switzerland), 9(10), 1351. [CrossRef]
- Lekkas, D., & Jacobson, N. C. (2021). Using artificial intelligence and longitudinal location data to differentiate persons who develop posttraumatic stress disorder following childhood trauma. Scientific Reports, 11(1), 10303. [CrossRef]
- Loucks, L., Yasinski, C., Norrholm, S. D., Maples-Keller, J., Post, L., Zwiebach, L.,... & Rothbaum, B. O. (2019). You can do that?!: Feasibility of virtual reality exposure therapy in the treatment of PTSD due to military sexual trauma. Journal of Anxiety Disorders, 61, 55–63. [CrossRef]
- Martin, A., Naunton, M., Kosari, S., Peterson, G., Thomas, J., & Christenson, J. K. (2021). Treatment guidelines for PTSD: A systematic review. Journal of Clinical Medicine, 10(18), 4175. [CrossRef]
- Marmar, C. R., Brown, A. D., Qian, M., Laska, E., Siegel, C., Li, M., Abu-Amara, D., Tsiartas, A., Richey, C., Smith, J., Knoth, B., & Vergyri, D. (2019). Speech-based markers for posttraumatic stress disorder in US veterans. Depression and anxiety, 36(7), 607–616. [CrossRef]
- Marzbani, H., Marateb, H. R., & Mansourian, M. (2016). Neurofeedback: A Comprehensive Review on System Design, Methodology and Clinical Applications. Basic and clinical neuroscience, 7(2), 143–158. [CrossRef]
- McLay, R. N., Baird, A., Webb-Murphy, J., Deal, W., Tran, L., Anson, H.,... & Johnston, S. (2017). A randomized, head-to-head study of virtual reality exposure therapy for posttraumatic stress disorder. Cyberpsychology, Behavior, and Social Networking, 20(4), 218-224. [CrossRef]
- Meyerbröker, K., & Morina, N. (2021). The use of virtual reality in assessment and treatment of anxiety and related disorders. Clinical Psychology & Psychotherapy, 28(3), 466–476. [CrossRef]
- Morland, L. A., Wells, S. Y., Glassman, L. H., Greene, C. J., Hoffman, J. E., & Rosen, C. S. (2020). Advances in PTSD treatment delivery: Review of findings and clinical considerations for the use of telehealth interventions for PTSD. Current Treatment Options in Psychiatry, 7(3), 221–241. [CrossRef]
- Nicholson, A. A., Ros, T., Densmore, M., Frewen, P. A., Neufeld, R. W. J., Théberge, J., Jetly, R., & Lanius, R. A. (2020). A randomized, controlled trial of alpha-rhythm EEG neurofeedback in posttraumatic stress disorder: A preliminary investigation showing evidence of decreased PTSD symptoms and restored default mode and salience network connectivity using fMRI. NeuroImage. Clinical, 28, 102490. [CrossRef]
- Niles, A. N., Woolley, J. D., Tripp, P., Pesquita, A., Vinogradov, S., Neylan, T. C.,... & Rauch, S. A. (2020). Randomized controlled trial testing mobile-based attention-bias modification for posttraumatic stress using personalized word stimuli. Clinical Psychological Science, 8(4), 756-772. [CrossRef]
- Orr, S. P., Metzger, L. J., & Pitman, R. K. (2002). Psychophysiology of post-traumatic stress disorder. Psychiatric Clinics of North America, 25(2), 271-293. [CrossRef]
- Pacella-LaBarbara, M. L., Suffoletto, B. P., Kuhn, E., Germain, A., Jaramillo, S., Repine, M.,... & Simon, N. M. (2020). A pilot randomized controlled trial of the PTSD Coach app following motor vehicle crash-related injury. Academic Emergency Medicine, 27(11), 1126-1139. [CrossRef]
- Place, S., Blanch-Hartigan, D., Rubin, C., Gorrostieta, C., Mead, C., Kane, J.,... & Fulcher, J. A. (2017). Behavioral indicators on a mobile sensing platform predict clinically validated psychiatric symptoms of mood and anxiety disorders. Journal of Medical Internet Research, 19(3), e75. [CrossRef]
- Premkumar, P., Heym, N., Brown, D. J., Battersby, S., Sumich, A., Huntington, B., Daly, R., & Zysk, E. (2021). The effectiveness of self-guided virtual-reality exposure therapy for public-speaking anxiety. Frontiers in Psychiatry, 12, 694610. [CrossRef]
- Ramos-Lima, L. F., Waikamp, V., Antonelli-Salgado, T., Passos, I. C., & Freitas, L. H. M. (2020). The use of machine learning techniques in trauma-related disorders: A systematic review. Journal of Psychiatric Research, 121, 159–172. [CrossRef]
- Reinertsen, E., Nemati, S., Vest, A. N., Vaccarino, V., Lampert, R., Shah, A. J.,... & Clifford, G. D. (2017). Heart rate-based window segmentation improves accuracy of classifying posttraumatic stress disorder using heart rate variability measures. Physiological Measurement, 38(6), 1061-1076. [CrossRef]
- Reinertsen, E., & Clifford, G. D. (2018). A review of physiological and behavioral monitoring with digital sensors for neuropsychiatric illnesses. Physiological Measurement, 39(5), 05TR01. [CrossRef]
- Rodriguez-Villa, E., Rauseo-Ricupero, N., Camacho, E., Wisniewski, H., Keshavan, M., & Torous, J. (2020). The digital clinic: Implementing technology and augmenting care for mental health. General Hospital Psychiatry, 66, 59-66. [CrossRef]
- Rogel, A., Loomis, A. M., Hamlin, E., Hodgdon, H., Spinazzola, J., & van der Kolk, B. (2020). The impact of neurofeedback training on children with developmental trauma: A randomized controlled study. Psychological trauma : theory, research, practice and policy, 12(8), 918–929. [CrossRef]
- Röhr, S., Jung, F. U., Pabst, A., Grochtdreis, T., Dams, J., Nagl, M.,... & Hinkelmann, L. (2021). A Self-Help App for Syrian Refugees With Posttraumatic Stress (Sanadak): Randomized Controlled Trial. JMIR mHealth and uHealth, 9(1), e24807. [CrossRef]
- Sadeghi, M., McDonald, A. D., & Sasangohar, F. (2022). Posttraumatic stress disorder hyperarousal event detection using smartwatch physiological and activity data. PLOS ONE, 17(5), e0267749. [CrossRef]
- Sandoval, L. R., Torous, J., & Keshavan, M. S. (2017). Smartphones for smarter care? Self-management in schizophrenia. The American Journal of Psychiatry, 174(8), 725-728. [CrossRef]
- Satiani, A., Niedermier, J., Satiani, B., & Svendsen, D. P. (2018). Projected workforce of psychiatrists in the United States: A population analysis. Psychiatric Services, 69(6), 710-713. [CrossRef]
- Sawalha, J., Yousefnezhad, M., Shah, Z., Brown, M. R. G., Greenshaw, A. J., & Greiner, R. (2022). Detecting Presence of PTSD Using Sentiment Analysis From Text Data. Frontiers in psychiatry, 12, 811392. [CrossRef]
- Sheikh, M., Qassem, M., & Kyriacou, P. A. (2021). Wearable, environmental, and smartphone-based passive sensing for mental health monitoring. Frontiers in Digital Health, 3, 662811. [CrossRef]
- Slater, M., & Sanchez-Vives, M. V. (2016). Enhancing our lives with immersive virtual reality. Frontiers in Robotics and AI, 3. [CrossRef]
- Torous, J., Bucci, S., Bell, I. H., Kessing, L. V., Faurholdt-Jepsen, M., Whelan, P.,... & Firth, J. (2021). The growing field of digital psychiatry: Current evidence and the future of apps, social media, chatbots, and virtual reality. World Psychiatry, 20(3), 318-335. [CrossRef]
- Torous, J., Onnela, J. P., & Keshavan, M. (2017). New dimensions and new tools to realize the potential of RDoC: digital phenotyping via smartphones and connected devices. Translational psychiatry, 7(3), e1053. [CrossRef]
- Tsanas, A., Woodward, E., & Ehlers, A. (2020). Objective characterization of activity, sleep, and circadian rhythm patterns using a wrist-worn actigraphy sensor: Insights into posttraumatic stress disorder. JMIR mHealth and uHealth, 8(4), e14306. [CrossRef]
- van der Meer, C. A. I., Bakker, A., Schrieken, B. A. L., Hoofwijk, M. C., & Olff, M. (2017). Screening for trauma-related symptoms via a smartphone app: The validity of Smart Assessment on your Mobile in referred police officers. International Journal of Methods in Psychiatric Research, 26(3), e1579. [CrossRef]
- van Gelderen, M. J., Nijdam, M. J., Haagen, J. F. G., & Vermetten, E. (2020). Interactive motion-assisted exposure therapy for veterans with treatment-resistant posttraumatic stress disorder: A randomized controlled trial. Psychotherapy and Psychosomatics, 89(4), 215-227. [CrossRef]
- Watkins, L. E., Sprang, K. R., & Rothbaum, B. O. (2018). Treating PTSD: A review of evidence-based psychotherapy interventions. Frontiers in Behavioral Neuroscience, 12, 258. [CrossRef]
- Watts, B. V., Schnurr, P. P., Mayo, L., Young-Xu, Y., Weeks, W. B., & Friedman, M. J. (2013). Meta-analysis of the efficacy of treatments for posttraumatic stress disorder. Journal of Clinical Psychiatry, 74(6), e541-e550. [CrossRef]
- Wickersham, A., Petrides, P. M., Williamson, V., & Leightley, D. (2019). Efficacy of mobile application interventions for the treatment of post-traumatic stress disorder: A systematic review. Digital health, 5, 2055207619842986. [CrossRef]
- Wiltshire, C. N., Wanna, C. P., Stenson, A. F., Minton, S. T., Reda, M. H., Davie, W. M., et al. (2022). Associations between children’s trauma-related sequelae and skin conductance captured through mobile technology. Behaviour Research and Therapy, 150, 104036. [CrossRef]
- Wu, Y., Mao, K., Dennett, L., Zhang, Y., & Chen, J. (2023). Systematic review of machine learning in PTSD studies for automated diagnosis evaluation. npj Mental Health Research, 2, 16. [CrossRef]
- Zoellner, L. A., Feeny, N. C., Bittinger, J. N., Bedard-Gilligan, M. A., Slagle, D. M., Post, L. M., et al. (2011). Teaching Trauma-Focused Exposure Therapy for PTSD: Critical Clinical Lessons for Novice Exposure Therapists. Psychological Trauma: Theory, Research, Practice, and Policy, 3(3), 300-308. [CrossRef]
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



